Embed Size (px)
DESCRIPTION
Ayurvision-09 is a CME in Ayurveda on the topic Current Understanding and management of AVABAHUKA ( Painful shoulder syndromes). This e-souvenir of the CME covers the presentations by the resource persons.
Citation preview

AYURVISION 2009
AYURVISION - 2009
CME IN AYURVEDA ON
“CURRENT UNDERSTANDING AND MANAGEMENT OF
AVABAHUKA”
19th& 20th December 2009
SOUVENIR
Exploring the new frontiers in academic and scientific Ayurveda
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 1
DEPT. OF AYURVEDA, Kasturba Medical College,
Manipal University, Manipal

AYURVISION 2009
AYURVISION - 2009
CME IN AYURVEDA ON “CURRENT UNDERSTANDING AND MANAGEMENT OF AVABAHUKA”
ORGANIZED BY:-DEPT. OF AYURVEDA
Kasturba Medical CollegeManipal University
Manipal
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 2

AYURVISION 2009
From the desk of H. O. D……….
Ayurvision
A MISSION WITH A VISION
“It needed a scientific age for the world to appreciate the full dignity of Ayurveda as a holistic system of perfect health. Now it has become clear to the world of science that every thing in the universe has its basis in the ‘unified field’ and everything can be successfully handled from this one area. It is this that has authenticated Ayurveda’s holistic approach to perfect health for both individual and society. Ayurveda today stands as the technology of the ‘unified field’ for perfect health of the individual of the nation, and of the world as a whole”
- MaharishMahesh Yogi
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 3

AYURVISION 2009
1. Ayurveda is Intellectual Property of we Indians. Every Indian has the
right to protect it.
2. Scenario of Ayurvedic education- Practice and research. Too much
emphasis on modern medicine. Neglect of Ayurvedic tradition and
practice. Ayurvedic profession is looked down by the public greatly
because graduates of Ayurveda sideline their science and resort to
unethical practice of Modern Medicine. Emphasis needed to improve
the quality and standards of Ayurvedic Education, accountability of
the Profession and standardization of Ayurvedic medicines.
3. Graduates of Modern medicine must be exposed to the principles and
practice of Ayurveda, either during their graduation level training or
during their Internship period. Medical Council of India, IMA and
Central Council Of Indian Medicine should come to single platform
and discuss this issue, as to how to implement this proposal.
4. Ayurvision is a step towards standardizing Ayurvedic Clinical
methods, based on which depends the quality and standards of
Ayurvedic Practice and research.
5. International Scenario of Ayurveda – India has to create world class
teaching – training centers for the foreigners, otherwise other
countries will develop there own institutions and apply there own
regulatory norms, and India will be a looser at the end.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 4

AYURVISION 2009
6. Manipal University’s vision for future of Ayurveda - Create
atmosphere for exchange of views among different professionals.
Encourage multidisciplinary research and provide training to
practitioners of Medicine.
India has a large infrastructure for teaching and clinical care training under
Indian systems of Medicine and teaching and training has been availed of
according to the curriculum set up by the Central Council of Indian
Medicine. The diagnosis and treatment of various ailments, use of drugs and
Ayuvedic profession as a whole has its basis to the education based on
authoritative texts recognized for these systems, but, the scientific validation
of the treatment has not been done on a wide scale. The off take and output
from these institutions has so far been limited and has not been able to meet
the standards for scientific enquiry. In the present era of globalization and
development of a world market for Ayurveda as a whole (education, research
and medical care delivery), research and development is needed. It has
become more and more evident that the medical centers around the country
with the state of the art infrastructure to provide quality medical education,
clinical training and research are to be recognized as the center of excellence
and supported to conduct Ayurvedic teaching and training as per the
requirements of the CCIM. The same views and proposals have been
highlighted during various National and International Conferences.
- (views expressed by the Secretary ISM, Govt. Of India)
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 5

AYURVISION 2009
Through this Ayuvision we propose to explore the new frontiers in academic
and scientific Ayurveda.
Dr. M. S. Kamath MD (Ayu.)
Additional Professor & HeadDepartment of AyurvedaManipal UniversityKMC, Manipal.Tel. 0820 29 22105mail : [email protected]
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 6

AYURVISION 2009
AYURVISION-2009CME ON
“CURRENT UNDERSTANDING & MANAGEMENT OF AVABAHUKA”
19th and 20th of December 2009
Program Schedule
Day1. December 19, 2009Morning SessionSl No Time Events01 08.00-09.00 Registration
02 09:00-10:00 Inauguration
03 10.00-10:30 High Tea
04 10:30-11:30 “Imaging of Cervical Spine & Shoulder Joint by Dr.Charudutta Associate Professor, Dept of Radiology KMC, Manipal.
05 11:30-12:30 “Clinical approach to a painful Shoulder”by Dr.Vivek Pandey, Associate Professor, Dept of Orthopaedics, KMC, Manipal
06 12:30 – 01:45 LUNCH BREAK
After noon Session
Sl No Time Events01 02.00-3.00 pm “Understanding of Sirascha Akunchana &
Bahupraspandahari” by Dr.G.R.Vastrad,Prof, Dept of Kayachikitsa, Taranath Govt Ayurvedic Medical College, Bellary
02 03.00-4.00 pm. Poster Presentation (Competition for Delegates)
03 04.00-4.30 pm Tea Break
04 04.30-5.30 pm Live Demonstration of “Avabahuka” patients for Diagnosis and Management
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 7

AYURVISION 2009
Day 2. December 20, 2009Morning Session
Sl No Time Events01 09:00-10:00 “Differential Diagnosis of Avabahuka” by
Dr.S.G.Mangalagi, HOD, Post Graduate Studies in Kayachikitsa, Govt Ayurvedic Medical College, Mysore
02 10:00-10:30 Tea Break
03 10:30-11:30 “Understanding of Bahushirshagatavata according to Charaka” by Dr.Prasanna Mogasale, Asst Professor, Dept of Kayachikitsa, SDM College of Ayurveda,Udupi.
04 11:30-12:30 “Management of Avabahuka with Shamanaushadhis” by Dr.Prashanth Assistant Professor, Ayurveda Mahavidyalaya, Hubli, Karnataka
05 12:30-01:45 LUNCH BREAK
Afternoon Session
Sl No Time Events01 02:00-03:00 “Management of Avabahuka by
Panchakarma Chikitsa”by Dr.K.Govindan Namboodari, Prof. Dept of Kayachikitsa, GovtAyurvedicCollege, hiruvananthapuram, Kerala.
02 03:00-03:30 Collection of certificates by delegates
03 03:30- 04:30 Panel Discussion
04 04:30-05:00 Valedictory Function followed by High Tea
.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 8

AYURVISION 2009
Contents.
01. Managemet of Avabahuka’ Shamanoushadhis. Dr. Prasanth…………….. ………………………………………………………12
02. Differential Diagnosis of Avabahuka. Dr.S.G. Mangalagi,……… ………………………………………………………22
03. Management of Avabahuka by Panchakarma. Dr. K. Govindan Namboodari. ………………………………………………………35
04. Clinical Approach to a painful shoulder Dr. Vivek Pandey……………. ………………………………………………………45
05. Abstracts………………………………………….50
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 9

AYURVISION 2009
AYURVISION – 2009CME ON “CURRENT UNDERSTANDING & MANAGEMENT OF
AVABAHUKA” 19th and 20th of December 2009
Chair person : Dr. Sripathi R Rao Dean, KMC, Manipal.
Co- Chair person : Dr. M.S. Kamath HOD Dept. of Ayurveda, KMC, Manipal.
Hon’ able adviser and Scientific CommitteeChairmen: Dr. K J Malagi Members:Dr. Basavaraj – Associate Professor Dr.Kamath Madhusudan.- Assistant ProfessorDr. Sripathi Adiga. – Assistant ProfessorDr.Anupama.- Assistant Lecturer
Master of Ceremony: Dr. Anupama
Reception committee:Chairmen – Dr. Anupama Dr. Divya Dr. SapanaMrs. Laxmi Mr. Ganesh Mrs. Divya
Transport Committee & Accommodation Chairmen – Dr.Sripathi AdigaDr. RajeshDr. Shivangoud Dr. Amruta Dr. Prthibha B.PMr. Praveen,Mr Vasudev,Mrs Sangeeta
Food & Catering Committee:Chairmen – Dr. Kamath MadhusudhanDr. ShaileshDr. Prathibha P.KDr. Jayanthi TMr VadirajMrs. BharathiMiss.GayathriMrs Savitha
Prayer By:Dr. Prathibha P.KDr Narind KhajuriaDr. SapanaDr. Amruta
Poster session judges:1. Dr. Govindan Nambodari.2. Dr. Vastrad.3. Dr. Prashant
e-BOOK editor: Dr Kamath Madhusudhana.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 10

AYURVISION 2009
PAPERSOF
RESOURCE PERSON
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 11

AYURVISION 2009
SHAMANA CHIKITSA IN APABAHUKA
DR.A.S.PRASHANTH
Professor
Department of Post Graduate StudiesAyurveda Maha VidyalayaHubli, Karnataka – 580024Telephone: 0836-2335575Mob: +91-94481-35575Mail: [email protected]
INTRODUCTION:Apabahuka is a disease that affects the Amsa Sandhi and is produced by the
Vata Dosha. Even though the term Apabahuka is not mentioned in the Nanatmaja
Vata Vyadhi, Acharya Susruta and others have considered Apabahuka as a Vata
Vyadhi. In Madhava Nidana two conditions of the disease has been mentioned –
Amsa Shosha and Apabahuka. Amsa Shosha can be considered as the preliminary
stage of the disease where loss or dryness of Sleshaka Kapha from Amsa Sandhi
occurs. In the next stage i.e., Apabahuka, due to the loss of Shleshaka Kapha
symptoms like Shoola during movement, restricted movement etc are manifested.
While commenting on these in Madhukosha Teeka it is mentioned that Amsa
Shosha is produced by Dhatu Kshaya i.e., Sudha Vata Janya and Apabahuka is
Vata Kapha Janya.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 12

AYURVISION 2009
LITERARY REVIEW:
In Charaka Samhita there is no direct reference regarding the disease
Apabahuka. But he gives the reference regarding the disease Bahushosha in Sutra
Sthana IN THE CONTEXT OF Nanatmaja Vata Vikaras.. In Sushruta Samhita
Samprapti, Lakshana and Chikitsa of Apabahuka has been discussed in detail in the
context of Vata Vyadhi. In Astanga Sangraha a complete description regarding the
disease has been dealt. Commentators like Arunadatta, Dalhana, Hemadri have
tried to analyze Apabahuka. Madava Nidana, Yogaratnakara, Vangasena Samhita
explained Apabahuka in Vata Vyadhi chapter. Madavakara was the first to
differentiate Apabahuka from Amsashosha. Other authors like Bhavamishra,
Sarangadara have discussed Apabahuka. The recent text like Gadanigraha,
Brihatnigantu Ratnakara explained Apabahuka.
NIRUKTI AND PARIBHASHA:
Nirukti and Paribhasha of Vata vyadhi is - “Vikrita vata janito asadharana vyadhi
vata vyadhi”
Extra ordinary disease resulting from Vikrita Vata is known as Vata Vyadhi.
Apabahuka comprises of two words 'Apa' and 'Bahuka'.
‘Apa’ means deterioration or dysfunction. The word 'Bahuka' means Muscular
gender. Thus Apabahuka can be defined as, Bahustambho Apabahuka / Bad arm,
stiffness in the arm joint.
NIDANA:
In case of Apabahuka Hetu may be classified into two groups;
Bahya Hetu – causing injury to the Marma or the region surrounding that.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 13

AYURVISION 2009
Abhyantara Hetu – indulging in Vata Prakopaka Nidana leading to vitiation of
Vata in that region.This may be again of Bahya Abhigataja(External cause) which
manifest Vyadhi or disease first and the other is Dosha Prakopajanya (Samshraya)
which in turn leads to Karmahani of Bahu.
VARIOUS NIDANAS OF VATAVYADHI AND VATA PRAKOPA FOR
APABAHUKA:
Aharaja(food) : Rasa- Katu, Tikta, Kashaya Rasa; Guna - Laghu, Ruksha, Sheeta,
Dravya; Adhaki, Chanaka, Kalaya, Masura, Mudga, Nishpava, Shuskashaka,
Tinduka; Matra – Abhojana, Alpashana, Vishamashana.
Viharaja (external) : Atiplavana, Atiprapatana, Atiprapidana, Ativichestitam,
Ativyayama, Kriyatiyoga, Mityayoga -Asama Chalana, Balavat Vigraha, Bhara
harana, Dukhasana, Vegadharana, Kalaja – Aparatra, Agantuja – Abhighataja,
Marmaghata.
SAMPRAPTI:As Apabahuka is considered as a Vata Vyadhi and Vata having Ashukari
Guna the Poorvaroopa like Bahupraspanditahara and Shoola may manifest mildly
or are totally absent. But the above symptoms are clearly manifested in the
Vyaktha Avastha or in Roopa Avastha of the Vyadhi in the Vyakta Sthana i.e in
the Amsa Pradesha.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 14

AYURVISION 2009
In this stage the Amsa Pradesha gets affected by aggravated Vata for which
Amsashosha occurs in the initial stage by the decrease of Shleshaka Kapha and
further leading to manifestations of Apabahuka by the symptoms like
Bahupraspanditahara and Shoola. There fore Madhava Nidana, Madhukosha
commentary has mentioned that Amsa Shosha and Apabahuka are the two stages
of the Vyadhi.
SAPEKSHA NIDANA:
Apabahuka is to be differentiated from the following disease conditions that
affect the upper limb.
Vishwachi
Amsa shosha
Ekanga vata
SADHYA ASADHYATA:
As Apabahuka is considered as Vatavyadhi which is a ‘Maharoga’ inspite of
effective treatment, will not yield good results, when it is associated with
Balamamsakshaya. Yogaratnakara says that Vatavyadhi is Sadhya, if it is of recent
onset and if the patient has good Bala.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 15

AYURVISION 2009
In Madhava Nidana, it is said that if patient is strong and without any
complications then the patient should be treated, as it is Sadhya for Chikitsa.
Sushruta and Madhavakara say that Shuddha Vataja Roga is Krichrasadhya,
Dhathukshayaja is Asadhya and Samsargaja is Sadhya. Bhava Prakasha and
Vagbhata opines the same. Even while explaining Vatavyadhi Chikitsa
Charakacharya has mentioned that all the Vatavyadhi after lapse of one year
becomes Krichrasadhya or Asadhya. Sadhyasadhyata can also be assessed by
considering Hetu, Poorvaroopa, Roopa, Dosha, Dushya etc. Thus Apabahuka in the
initial stage will become Sadhya and is Krichrasadhya or Asadhya after certain
period.
CHIKITSA:
The general line of treatment mentioned for Vatavyadhi in Ayurvedic
classics include Snehana (both internal and external), Swedana,
Mrudusamshodhana, Vasti, Sirovasti Nasya, etc. Charaka further says that
depending on the location and Dushya (tissue element vitiated by Vata) each
patient should be given specific therapies. Nasyakarma has been mentioned by
Vagbhata in Jatroordhva Vatavikaras. Three major approaches are made in the
management of Vatavyadhi.
1. Treatment of Kevala Vata
2. Treatment of Samsrusta Vata
3. Treatment of Avruta Vata
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 16

AYURVISION 2009
Ayurvedic classics explain the Chikitsa of Apabahuka as follows.
1. Nasya and Uttarabhaktika Snehapana are useful in the management of
Apabahuka.
2. Astanga Sangraha mentions Navana Nasya and Sneha Pana for Apabahuka.
3. Sushrutacharya advice Vatavyadhi Chikitsa for Apabahuka, except Siravyadha.
4. Chikitsa Sara Sangraha advice Nasya, Uttara bhaktika Snehapana and Sweda for
the treatment of Apabahuka.
5. Brumhana Nasya indicated in Apabahuka by Vagbhata
By considering the above references, following can be said as the line of treatment
of Apabahuka.
1. Nidana parivarjana
2. Abhyanga.
3. Swedana
4. Uttarabhaktika Snehapana
5. Nasyakarma
6. Shamanoushadhi.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 17

AYURVISION 2009
Some of the Shamanoushadhi explained in Texts:
Ashtanga Hrudaya:
Chikitsa Sutra:
'Apabaahou hitam nasyam snehascha uttarabhaktika:’ (A.H.Chi.21/44)
“Gudamanjaryaa khapuram vrushabeemoolam ca shishirajalapishtamNaavanavidhou prayojitam avabaahuka gala ruja arti haram” (Commentary)
“Dasamoola balaa maasha kwatham taila aajya mishritam Saayam bhuktwaa pibennasyam vishwachyaam avabaahuke” (Commentary)
“Prasaarinee tulaa kwathee taila prastham paya: samamDwimedaa mishi manjishthaa kushta raasnaa kucandanai:Jeevaka rushabha kaakolee yugula amaradarubhi:Kalkitai: vipacet sarva maarutaamaya naashanam” (A.H.Chi.21/65-66)
Balaa Tailam (A.H.Chi.21/73-81)
Cakradatta:
“Dasamoola balaa maasha kwatham taila aajya mishritam Saayam bhuktwaa pibennasyam vishwachyaam avabaahuke” (Vatavyadhi.25)
“Moolam balaayaastvatha paaribhadraat tathaa aatmaguptaa swarasam pibed vaaNasyantu yo maamsarasena kuryaan maasadasou vajra samaana baahu” (Vatavyadhi.26)
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 18

AYURVISION 2009
“Baahushoshe pibet sarpir bhuktvaa kalyaanakam mahat” (Vatavyadhi.28)
Vishvachi Chikitsa – Rakta mokshana (Vatavyadhi.57)
Trayodasanga Guggulu – Gridrasi baahu prishte hanu grahe...(Vatavyadhi.69-73)
Narayana Tailam – Hanusthambe Manyaasthambe... (Vatavyadhi.120-130)
Mahanarayana Tailam – Hanugraham... (Vatavyadhi.131-140)
Ketakyaadi Tailam – Asthi gata vatam... (Vatavyadhi.150)
Swalpamaasha Tailam – Baahuseersha gata vata... (Vatavyadhi.154-155)
Masha Tailam – Vishvaachyaam Apabaahuke... (Vatavyadhi.157-161)
Masha Tailam – Apabaahukahara... (Vatavyadhi.162-164)
Saptaprastha Brihatmaasha Tailam – Apabaahuke... (Vatavyadhi.165-172)
Prasaarini Tailam – Asheeti Vatavikaareshu... (Vatavyadhi.173-186)
Mahaamaasha Tailam – Vishvaachi... (Vatavyadhi.187-191)
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 19

AYURVISION 2009
Mahaamaasha Tailam – Apabaahuka Vishvaachyou... (Vatavyadhi.192-200)
Mahaaraajaprasaarini Tailam – (Vatavyadhi.258-264)
Bhaishajya Ratnavali:
Balaadi Kashayam – Baahushosha... (Bha.Rat.26/67)
Yogarajaguggulu Vati – Sarvaan Vataamayaan... (Bha.Rat.26/102-113, Sarngadhara)
Vatagajaankusha Ras – Apabaahuka Samgyakam... (Bha.Rat.26/114-118, Rasendra Sara Sam)
Brihat Vaata Chintaamani Ras – Vaata Rogam... (Bha.Rat.26/141-144)
Vaata Vidwamsa Ras – Manyaa Sthambam... (Bha.Rat.26/178-184, Rasendra Sara Sam)
Mahaakukkudamaamsa Tailam – Apabaahuke... (Bha.Rat.26/511-520)
Maashabalaadi Tailam – Hanusthambham Manyaasthambam... (Bha.Rat.26/551-556)
Vishagarbha Tailam – Hanusthambham Manyaasthambham... (Bha.Rat.26/560)
Balarishtam – Sarva Vata Roga hara... (Bha.Rat.26/572-574)
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 20

AYURVISION 2009
Sahasra Yogam:
Ashtavargam Kashayam
Prasaarinyadi Kashayam
Rasnadwigunabhaagam Kashayam
Ketakyaadi Tailam
Parinatakeri Ksheeraadi Tailam
Kaarpaasasthyaadi Tailam
Ksheerabala (101)
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 21

AYURVISION 2009
Differential Diagnosis of Apabahuka W.S.R. To Frozen
Shoulder
Dr. S. G. Mangalgi,Professor and HOD,Dept. of Postgraduate studies in Kayachikitsa, GAMC, Mysore
INTRODUCTION:
The present day world is full of stress and strain with increasing
competitions in all walks of life. This has led to many diseases which though do
not kill a person, but hamper one’s day to day life.
Vataja disorders include major neurological problems, few conditions of the
musculo-skeletal system, few psychosomatic problems and very few gastro-
intestinal problems. More precisely in vataja disorder multiple systems of the body
get affected.
Apabahuka is one of the Vatavyadhi which affects the normal functioning of
the upper limb. Agriculture still continues to be the prime occupation of people in a
developing country like India. Incidence of Apabahuka is more among people who
use their upper limbs to perform strenuous work.
Apabahuka comprises of two words 'apa' and 'bahuka'. Apa means Viyoga,
vikratou means Viyogou ie dysfunction, separation. Bahuka - pra cha koorparasya
urdhwadha bhagou iti vishnupurane means it starts from Koorparasandhi (elbow
joint) to Shoulder girdle.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 22

AYURVISION 2009
Thus Apabahuka can be defined as: stambho Apabahuka1 i.e. Stiffness in the
arm joint
To summarize the above discussion and considering the relevant clinical
feature, the term Apabahuka would mean "loss of function of bahusandhi i.e.
Praspanditahara (stiffness or disability in the arm).
By seeing the above definition of Apabahuka explained by our acharyas
correlates with the Frozen Shoulder/Adhesive Capsulitis explained in
contemporary science.
In clinical practice we do get the patients with the complaint of pain/
stiffness of shoulder joint/ upper arm in different conditions such as in infectious,
degenerative, and neurological problems. This requires a thorough differentiation
of these conditions for successful treatment.
Symptoms of Apabahuka/ Frozen Shoulder:
In case of Apabahuka sthanika laxana take important place, as compared to
sarvadaihika laxana. The cardinal features of Apabahuka are as follows.
i) Bahu Praspandidahara2
ii) Amsabandhana Shosha3
iii) Shoola4
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 23

AYURVISION 2009
Bahu Praspandidahara - This has three terms
Bahu - means upper limb
Prasapandana - means movement or chalana, this is considered under normal
function of vata in Sushruta Samhita.5
Praspandana shareerasya chalanam, idam vyanasya karma6
Dalhana commenting on this says that praspandana means chesta or
movement and chesta to akunchana - prasaranadi karma,7 this karma is maintained
by vyanavata in the limbs.8
Hara - means loss of / impaired / difficult. Thus, in the present context this may
be taken up as (i.e. praspandahara) difficulty in the movement or impaired or
loss of movement of the upper limb.
Amsabandhana Shosha:
Sushrutacharya considered this as a major laxanas in case of Apabahuka.
But, this is practically seen in the later part of the disease.
Shoola:
Although any of the texts do not mention about the shoola as one of the
laxana of Apabahuka, it is still a feature practically seen in Apabahuka patients.
Recent Ayurvedic texts like Chikitsa Sara Sangraha and Nidana Sara, clearly
mention about Savedana as a predominant laxanas of Apabahuka, along with other
laxanas.
Based on the symptomatology, we can correlate the condition Apabahuka
with that of frozen shoulder mentioned in modern classics as follows:
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 24

AYURVISION 2009
Symptoms
a) Gradual onset of shoulder stiffness
b) Pain manifest after significant Shoulder Range of movement lost
c) Pain well localized to rotator cuff
d) Pain radiation into deltoid and anterior arm
e) Pain interferes with sleep (unable to lie on shoulder)
Signs:
Inspection:
a) Patient holds arm protectively at side
b) Deltoid and Supraspinatous atrophy
Palpation:
a) Generalized pain at rotator cuff and biceps tendon
b) Limited range of movement
c) Loss of both active and passive shoulder range of movement (pathognomonic)
d) Restricted movement in all planes
e) Normal range of motion excludes adhesive Capsulitis as a diagnosis
Associated Findings:
Reflex Sympathetic Dystrophy, Hand Edema, coolness, and discoloration
Sapeksha Nidana:
There are some clinical conditions of modern science which may be
compared with that of Apabahuka. These may be categorized as follows.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 25

AYURVISION 2009
1. Peri arthritis or frozen shoulder or adhesive Capsulitis.
2. Incomplete rupture of supraspinatous tendon
3. Lesions of the rotatory cuff
4. Sub acromial or subdeltoid bursitis
5. Sub coracoid bursitis
6. Painful shoulder
7. Bicipital tendinitis
8. Osteo arthritis of shoulder joint
9. Brachial plexus neuropathies
Differential diagnosis:
Apabahuka should be differentiated with the following diseased conditions
that affect the upper limb
.
1. Vishwachi:
‘Talam Pratyangulinam ya kandara bhahu pristata
Bahvoho Karmakshayakari viswachinama sa smritah”||9
Here, the pain starts from hasta tala and angulis and radiates in the kandaras
of prista region and manifest with karmakshaya. Range of movement is more
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 26

AYURVISION 2009
restricted in case of Viswachi than apabahuka, where pain is more in Apabahuka
than viswachi.
2. Shosha:
“Asmsa desha sthito vayuhu shoshayet amsa bandhanam”|10
Shosha was considered as a separate condition by Madhavakara and it has to
be differentiated from apabahuka by considering it as an independent entity. Where
the wasting of muscles itself is the cardinal feature, have to be noted. Shosha will
appear in the later stages of Apabahuka. But, Apabahuka may be a predisposing
factor for Shosha which intern does not end up with Apabahuka.
3. Ekangavata:
‘Ekangavatam tam vidyaat anye pakshavadham viduh: ||11
Karmahani of affected limb is the main feature seen ekangavata. In case of
apabahuka, karmakshaya of bahusandhi is the main characteristic feature observed.
Ekangavata can be compared with that of monoplegia where the lesion is not in the
bahusandhi which is an uppermotor neuron disorder.
MODERN PERSPECTIVE:
1. Biceps tendon rupture:
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 27

AYURVISION 2009
Symptoms - Painful snap at elbow following forceful elbow flexion, Swelling and
Tenderness occur proximal to elbow, sudden onset with sharp snapping sensation,
Pain and weakness of shoulder and arm
Signs:
A. Weak flexion at elbow: where in some flexion may be maintained.
B. Weak supination at forearm.
C. Bulbous swelling in upper arm on flexion
Localized bulge at distal biceps when elbow flexed
Bulge represents retracted biceps muscle belly
Except shoulder pain the above signs and symptoms are not their so it is not a frozen shoulder.
2.Biceps Tenosynovitis:
Occurs above the age 40 years due to repetitive throwing, causes
Anterolateral Shoulder Pain referred down anterior arm.
Signs:
A Tenderness over bicipital groove
B. Pain limits active and passive range of motion
C Maneuvers that stretch biceps elicit pain
Forceful external rotation with abduction
Arm extension with elbow extended
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 28

AYURVISION 2009
Shoulder pain referred to anterior arm and restriction of movements on both
active and passive movements are not seen in frozen shoulder, so it could be
excluded.
2. Subluxing Biceps Tendon:
Symptoms: There will be congenital presence of shallow groove in the bicipital
region, shoulder pain and stiffness, frequent reoccurrence of subluxation.
Signs: Forceful external rotation and abduction of shoulder are painful. Surgery is
the choice of management. But in case of frozen shoulder, there won’t be any
bicipital groove/subluxation are not seen where all modalities of movements are
afflicted.
3. Clavicle fracture:
H/o of trauma i.e. fall against lateral shoulder (most common), fall on
Outstretched Hand, direct blow to clavicle,
Symptoms:
Shoulder pain and swelling localized to fracture site, patient unable to lift arm due
to pain.
Presentation:
Holding the affected arm adducted and supported with the opposite hand.
Signs:
Gross clavicular deformity observed or palpated, localized swelling, bruising,
tenderness, and crepitation.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 29

AYURVISION 2009
Complications:
Neurovascular injury of affected arm, Pneumothorax Subcutaneous Emphysema
Chest X ray of Antiro-postirior view shows fracture site.
Except shouder pain, all features of above condition are not go in favor of
frozen shoulder; hence it could be easily differentiated.
4. Gleno Humeral Instability:
Symptom:
Typically occurs below the age of 40 years, lateral deltoid numbness and pain
Signs:
Shoulder apprehension Test is positive. X ray of shoulder shows either Hill-Sachs
Lesion, Shoulder Dislocation, Inferior glenoid avulsion Fracture.
5. Shoulder dislocation:
Usually there is history of trauma or generalized seizers present; Acromion
is much more prominent, humeral head fullness absent under deltoid, Leaves
prominent cavity. Severe pain in the shoulder with any range of motion, Arm
"locked" in place (may be cradled by other hand), Patient refuses to move arm. In
case of –
Anterior dislocation - Arm held externally rotated, anterior shoulder appears
full with anterior bulge, Space below acromion appears empty, internal rotation
painful
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 30

AYURVISION 2009
Posterior dislocation - Arm held in internal rotation, Forearm rests on
abdomen, Anterior shoulder flat, External rotation painful, Assess
neurovascular structures. X ray is the diagnostic.
6. Rotator Cuff Tendonitis:
Symptoms:
Pain worse at night, unable to lie on affected shoulder, locking sensation with
abduction, referred pain to deltoid.
Signs:
Tenderness at the insertion of supraspinatous, pain in the Acromioclavicular joints,
patient automatically turns palm up on abduction, and active "palm down"
abduction is painful. Intact muscle strength, Pain and crepitation worse between 60
to 120 degrees abduction, maximal compression of soft tissue in subacromial
space. X ray shows sclerosis at the tuberosity.
Based on the clinical features of above condition, we can easily distinguish it from
frozen shoulder.
7. Fracture of Proximal Humerus:
Symptoms:
Usually there is a history of trauma or fall is present, severe pain in the arm
provoked by any type of movement, stiffness of shoulder.
Signs:
Presence of signs like Swelling, echymosis and pain over shoulder are present. In
case of neuro vascular injury there is a sensory loss over the arm. Pallor of forearm
on examination reveals the injury of the brachial artery. AP view of X ray shows
fractured site.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 31

AYURVISION 2009
8.Osteo arthritis of Shoulder joint:
Symptoms-
Gradual onset of pain and stiffness, stiffness may significantly limit function when
advanced, chronic Shoulder Pain, Crepitus.
Signs :
Limited shoulder range of motion - active and passive. X ray shows degenerative
changes like narrowing of joint spaces, subchondral sclerosis and formation of
osteophytes.
7. Brachial Plexus Neuropathies:
Symptoms-
Severe Shoulder Pain or arm and neck pain worsens at night and is of short
duration. Shoulder weakness follows pain within 1 to 30 days.
Signs:
Atrophy of multiple shoulder muscle groups involved are deltoid muscle, rotator
cuff muscles, biceps muscle and triceps muscle Electromyogram shows neurogenic
atrophy.
8. Sub coracoids Bursitis:
Symptom:
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 32

AYURVISION 2009
The patient complains of pain in the region of the coracoid and there is definite
tenderness over the interval between two bones.
Signs: Chronic cases on which adhesions are present have marked limitations of
lateral rotation and abduction.
9. Sub Deltoid Bursitis:
Symptoms:
Pain in the shoulder on abduction and internal rotation of the humerus is severe at
night, and tender points of the shoulder which is usually felt near the insertion of
the deltoid muscle, rather than in the joint itself, although it may radiate wide.
Signs:
Point tenderness on the greater tuberosity which disappears under the acromion on
abduction (Dawbamis sign). This tenderness may be absent or it may be wide
spread over the deltoid region.
In some cases the patient gives a history of an injury to the shoulder. This usually
takes the form of a fall on the outstretched arm or stabbed shoulder. When the pain
follows an injury there is usually an interval of few days before it manifests itself.
Radiological imaging may show calcium deposits on the supraspinatous tendon.
CONCLUSION:
1. Apabahuka is a disease of shoulder joint with restricted movement.
2. Apabahuka can be compared with frozen shoulder
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 33

AYURVISION 2009
3.Shoola though not told in the classics is one of the complaints that brings
patient to the doctor.
4. Samprapti and laxanas of Apabahuka and its physical examination can
better be understood and done with the help of modern medical techniques.
5.Apabahuka should be differentiated from other clinical conditions of
shoulder joint for successful treatment.
REFERENCES:
1. Nibandha Sangraha
2. A.Hr.Ni. 15/43
3. Su.Ni. 1/82
4. Su.Ni. 1/27
5. Su.Su.15/4
6. Su.Ni. 1/18
7. Su.Ni. 1/18 Dalhana
8. Cha.Chi. 28/9 - Chakrapani
9. Su.Ni.1
10.Ma.Ni.15/44
11.’Cha. chi.29.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 34

AYURVISION 2009
MANAGEMENT OF APABAHUKA BY PANCHAKARMA
Dr. K. Govindan Namboodiri,M.D(Ay).Prof.Dept of Kayachikitsa.Govt.Ayurvedic College.Trivendrum.
Apabahuka is a major disease come across with daily practice.Vitiated vata
situated at amsamoola causes loss of motor activities or difficulty in movements of
hand and wasting of associated muscles .Many pathological conditions seen now
has resemblance to apabahuka cervical spondylosis,periarthritis of
shoulder,adhesive capsulitis(frozen shoulder},injury to supraspinatus muscle etc
Management of apabahuka is achieved by adopting the treatment measures
vatavyadhi in general and specific treatment for apabahuka.
1.General treatment of vatavyadhi-Snehana,swedana,mrudusodhana etc.
2.Specific treatment of apabahuka- a)Nasyam
b)Auttarabhaktika sneham
When we consider the management by panchakarma let us take the poorvakarma
also.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 35

AYURVISION 2009
A).SNEHANA-
Snehana is adviced in nirama stage.If the disease is in sama stage rookshana and
pachana are done toattain the nirama stage .Then snehana is done.In vatavyadhi
both the bahyasneha and abhyantara sneha isneeded.
a)Abhyantara sneha
-It is the specific treatment of apabahuka. The sneha is adviced to consume after
food .The sneha taken after food cures the diseases occurring in the upper part of
the body .It also gives strength to the body parts of that region. Thailas and
yamaka(thaila+ghrita) are adviced for pana after food. The sneha cures the dhatu
sosha and promotes dhatupushti.It promotes agni and increases the strength of the
body.The following thailas are used in apabahuka for internal use.
1.Karpasasthyadi thailam
2.Ksheerabala prepared with thailam and ghritam.
3.Masha thailam.
b)Bahya snehana-
As in other vatavyadhis abhyanga is beneficial in apabahuka also .Specific thailas
are described for this purpose.
1.Karpasasthyadi thailam.
2.Jambeera thailam.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 36

AYURVISION 2009
3.Parinatakeriksheeradi thailam.
4.Balaguloochyadi thailam for head.
B)SWEDANA-
Swedana alleviates toda,ruk,stambha,graha etc. One specific sweda applied in
apabahuka is jambeerapindasweda.
Shashtikapindasweda is effective where sosha(wasting of muscle)is present.
SHASHTIKA PINDA SWEDA
The word ‘PINDA’ means bolus. Pinda sweda refers to the sudation performed by
bolus of drugs. Shashtika pinda sweda is performed in ekanga or sarvanga with the
bolus of boiled Shashtika shali with Balamoola kwatha and ksheera. The main
properties of Shashtika are snigdha, guru, sthira, sheeta and tridoshaghna. Though
a sweda karma, it has brimhana guna.
Materials required:
1. Shashtika shali-500g
2. Balamoola-750g
3. Water- Q. S.
4. Cow’s milk-3litres
5. Cotton cloth(45cm X 45cm)- 4 pieces
6. Threads(75cm)- 8
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 37

AYURVISION 2009
7.Vessels-
a. For preparing kwatha
b. For cooking rice
c. To heat the boluses in mixture of kwatha and milk during the
procedure (5 litres capacity with wide mouth made of bronze)
d. A plate for carrying heated pottali
7. Stove-1
8. Oil for talam- 10ml
9. Rasnadi choorna- 5g
10.Suitable oil for abhyanga-100ml
11.Coconut leaves/tongue cleaner-2
12.Tissue paper/towel- 2
13.Masseurs -2
14.Attendant - 1
Preparation of the medicine:
Balamoola kwatha-
750g of Balamoola is cleaned, crushed and boiled in 12 litres of water and reduced
to 3 litres.
Shashtika rice cooking-
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 38

AYURVISION 2009
In 1.5 litres of Balamoola kashaya and 1.5 litres of milk, 500 g of Shashtika rice
should be added and boiled till it becomes thick and semisolid. Sufficient quantity
of hot water can be used for proper cooking of the rice. Another method is that the
Shashtika rice can be semi cooked in pure water; gradually added milk and kwatha;
cooked again.
Preparation of the boluses:
The cooked rice should be divided into 4 equal parts and put into 4pieces of
cotton cloths. The three corners should be folded neatly together so as to come
under the fourth corner and the fourth fold is used to cover the other three corner
folds underneath. One end of the thread is held tight with left hand and the other
end is wound around the folds. In short, the boluses should be tied in such a way
that the mouth of the sac leaves a tuft at the top of the bundle, for holding it with
ease. Conventionally, the size of a bundle is half kernel of a moderate coconut.
Pre operative procedure:
The patient should be seated with leg extended over the droni and talam should be
applied with suitable oil. Abhyanga should be then performed with prescribed oil
for about 10 minutes. Out of 4 pottalis, 2 are kept in the mixture of Balamoola
kwatha and milk (1.5 litres of each was already kept for this purpose), which
should be put on a stove with moderate heat.
Procedure:
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 39

AYURVISION 2009
2 warm potalis should be gently applied in a synchronised manner by the two
therapists on two sides of droni. It is followed by a gentle massage with other hand.
They should ensure that the heat of the boluses is bearable to the patient by
touching them over the dorsum of their hand.
The temperature of the boluses should be maintained throughout the procedure by
continuous relay of the four boluses after reheating by dipping in milk kwatha
mixture.The process should be continued till the patient gets samyak swinna
lakshana or until the contents of the boluses exhausted. This procedure is done in
the seven positions as in kayaseka or as advised by the physician.
Duration:
45 minutes -1 hour, preferable time is in between 7-11 am and 4-6 pm. The
procedure can be stopped if the medicine in the boluses or the milk mixture is
exhausted.
Post operative procedure:
At the end of the procedure, the medicine remained over the body should be
scrapped of with the coconut leaves or with any similar device and the body is
wiped dry with tissue paper or soft towels. After that medicated oil should be
applied.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 40

AYURVISION 2009
Talam should be removed and Rasnadi choorna applied over the head.
Gandharvahastadi kashaya can be given for drinking. The patient should take
complete rest for at least half an hour, and then the patient is allowed to take warm
water bath.
Precautions:
1. During the preparation of the rice, care should be taken to avoid over/under
cooking and should be stirred frequently for the better extraction and
cooking.
2. Tie bolus firmly to avoid leaking of contents during rubbing.
3.The therapists in both the sides of the patient should massage with the bolus
in a synchronised manner.
4.Ensure uniformity of pressure and temperature on all the body parts
.5 Boluses should be applied with sufficient warmth (450C-50oC).
6.The therapy should be stopped at any time if the patient gets good
perspiration or shivering.
Complications and management:
1. Shivering: It usually occurs due to the uneven distribution of temperature or
prolonged time gap in between the taking up of new boluses; or if body is
exposed to cold breeze immediately after the procedure. Allow the patient to
take rest cover with a blanket and give warm liquid diet.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 41

AYURVISION 2009
2. Fainting: Due to increased body temperature or low heat threshold of the
patient or atiyoga of kriyakrama. Sprinkle cold water over the face and body,
and put thalam with appropriate medicated oil and choorna. Drakshadi
kashaya can be given internally.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 42

AYURVISION 2009
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 43

AYURVISION 2009
MRUDU SODHANA.
After snehana and swedana,mrudusodhana is done.For this Eranda thailam with
milk is adviced.
NASYAM.
The main panchakarma procedure in apabahuka is nasyam.Nasyam is indicated in
diseases affecting upper part of the body and head .Brimhana nasyam is adviced in
apabahuka.Thailas used for nasya are
1.Karpasasthyadi thailam.
2.Masha thailam.
3.Ksheerabala thailam.
Nasal passage is the route to head. It is also the site of orifices of most of
paranasal sinuses. Its mucosal epithelium is sensitive to variety of stimuli.The
medicines applied by nasya will have local action as well as deeper action at
neurological level.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 44

AYURVISION 2009
CONCLUSION.
Apabahuka is a major disease described under vatavyadhi.The main symptoms
being pain,difficulty in/painful movements and later wasting of muscles.
Management of this disease is done by general treatment of vatavyadhi and
specific treatment for apabahuka. In Kerala the practitioners used many internal
and external medications which are described in Chikitsamanjari,Yogamrita etc.
These measures are efficacious in managing apabahuka.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 45

AYURVISION 2009
Clinical approach to a painful shoulder
Dr. Vivek Pandey, Associate prof.,Orthopaedic SurgeryKMC, Manipal
Normal shoulder function is needed for daily routine activities and sporting
actions. Over the years, the understanding of shoulder anatomy and function has
drastically improved and adjuncted with excellent imaging methods, the treatment
options have provided excellent outcomes in the shoulder problems.
The shoulder joint or gleno-humeral joint is a ball and socket joint. The glenoid or
socket is shallow and is inherently unstable. The stability is provided by various
ligaments, capsule, physical and muscular forces. These stabilizers also play role in
shoulder joint movement with adequate rhythm. Any disturbance in structural or
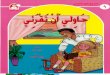
rhythmic support of the shoulder leads to a painful shoulder. Because there are
numerous structures that can cause shoulder pain, it is important that clinician
should narrow down into one or more of the following categories of shoulder pain.
(Image 1)
1. Rotator cuff musculature: tendinopathy / tears
2. Impingement
3. Biceps tendonitis
4. Stiffness: frozen shoulder
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 46

AYURVISION 2009
5. Acromio-clavicular and gleno-humeral joint arthritis
6. Disrupted scapula-humeral rhythm
7. Instability i.e. shoulder dislocation
8. Referred pain esp. from neck or others
A good clinical history and systematic examination of shoulder can establish the
diagnosis in most of the cases. A brief description of above listed problem will be
helpful in assessing the problem.
Rotator cuff pathology is more frequent in patients more than 30 years. Mostly,
supraspinatus and infraspinatus tendons are involved in tendinitis or tear.
Tendonitis or tendinopathy is usually seen in chronic overhead activities. They
present with pain usually with overhead activity. The pain is usually in the night
especially sleeping onto the side of affected shoulder. Cuff tears are seen with fall
on outstretched hand, rapid acceleration, and direct blow to shoulder or even after
long standing tendonitis. If there is complete tear, they present with weakness in
elevating shoulder. Partial cuff tears are more painful than full thickness tears.
Supraspinatus and infraspinatus muscle wasting is the key clinical feature. Resisted
abduction is painful with thumbs down position. Rotator cuff tendinopathy often
and partial cuff tears sometimes can be managed conservatively. Rehabilitation
plays an important role in treatment. Non responsive cuff problems or full
thickness cuff tears are best managed surgically. If a full thickness cuff tear is
ignored for long, it can lead to rotator cuff arthropathy which is a very difficult
condition to manage.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 47

AYURVISION 2009
Impingement means compression of rotator cuff and subacromial bursa between
humeral head and under surface of acromian. It is due to narrowed space or
thickened and inflamed structure. The clinical presentation is similar to rotator cuff
tendinopathy. However, neither muscle wasting nor weakness of muscle is seen.
Biceps tendinopathy is seen in more than 25 years of patients. It is aggravated by
lifting or carrying bags or overhead reaching. It can lead to spontaneous rupture.
Rotator cuff signs are absent and movements are full.
It is important to rule out affections of subscapularis muscle in chronic biceps
tendonitis or subluxating tendon.
Shoulder stiffness is usually due to frozen shoulder. These patients are usually
more than 40 years and often first time diagnosed to have diabetes by orthopaedic
surgeon as frozen shoulder could be the presenting feature.
There is usually long standing history of pain accompanied by global loss of
movement of shoulder joint. Night pain and global loss of movement is the key
feature and patient cannot lie on the affected side. Loss of rotations is the key
finding. Treatment is mostly conservative in form of analgesics, physiotherapy and
occasional intra-articular injections. Sometimes, manipulation under anaesthesia is
done to restore movements and minimize pain. Arthroscopic release is also a good
option in non-responders.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 48

AYURVISION 2009
Acromio-clavicular joint pain is quite common especially in patients more than 40
years of age. The pain is usually localized to the tip of shoulder. Treatment is
usually conservative, local steroid injections and sometimes arthroscopic resection.
Gleno-humeral arthritis is a feature of elderly population. It is associated with pain
and stiffness with arthritic changes on x-ray. Joint replacement is treatment of
choice for advance arthritis.
Disrupted scapular rhythm can give rise to vague pain around shoulder. It can be
diagnosed by clinical examination. Treatment is always conservative in form of
muscle strengthening exercises.
Image 1: algorithm to assess the shoulder pain
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 49

AYURVISION 2009
Shoulder instability is usually traumatic. It is more frequent in younger population.
Diagnosis of shoulder instability is not difficult to establish due to precise history
given by the patient. It is rarely accompanied by pain and night pain is usually not
the feature. The treatment is usually surgical.
Referred pain is one of the common entities to be kept in mind. The most common
area of referred pain is from neck. Cervical spondylitis and disc prolapse are the
common causes of neck pain. The patient will have neck pain which radiates to the
shoulder, arm and hand. The local examination of shoulder is normal whereas neck
movements are painful with or without radicular features. These patients may also
have night pain while lying on the side.
Other areas of referred pain are from chest and abdomen. Pancoast tumour of lungs
in an elderly can lead to shoulder pain. Chronic angina pain is also referred to the
shoulder on left side but with breathlessness, sweating etc. Chronic cholycystitis or
cholelithiasis can lead to right shoulder pain. Chronic splenic pain can lead to left
shoulder pain. So, a proper systemic evaluation is must.
A good history coupled with clinical examination usually establishes the diagnosis.
Non responsive shoulder pain or if cuff tear is suspected, it must be supplemented
with diagnostic ultrasound of the shoulder. Ultrasound is a cheap and quite
sensitive investigation in the hands of an expert sonologist. If necessary, MRI can
be done but MRI does not offer an exceptional advantage over ultrasound contrary
to the expected.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 50

AYURVISION 2009
Abstracts.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 51

AYURVISION 2009
Anatomy and applied anatomy of shoulder joint.
Dr. Sapna *, Dr. Jayanthi**, Dr. Anupama***.
______________________________________
ABSTRACT:
KEYWORDS: Visualization, understanding anatomy and applied anatomy. For obtaining better result while treating Avabahuka one should have sheer knowledge about anatomy and its applied aspects so that one can understand the different anatomical structures involved in the disease process; and thus select the appropriate treatment.. *PGCPK Scholar, Dept of Ayurveda KMC,Manipal.** PGCPK Scholar,Dept of Ayurveda,KMC,Manipal.*** Asst.Lecturer, Dept of Ayurveda,KMC,Manipal.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 52

AYURVISION 2009
A RARE TREATMENT MODALITY FOR APABAHUKA- SIRAVYADHA
Dr.Ranjith.R.P*,Dr.Ravishankar.A.G**. __________________________________________________________
Abstract.
Apabahuka is a painful condition of shoulder joints which restricts the
normal movements of upper limbs. Now a days reporting cases of Apabahuka are increasing
because of the life style. About 15-20% of working group of people are affected with shouider
pain. Most of the treatments such as Snehana, Swedana, Nasya and internal medication are time
consuming and results will be delayed.
Raktamokshana ( siravyadha) is an affective treatment to relieve the
signs and symptoms of Apabahuka immediatly and also it is an effective treatment in
raktaavritha condition.
Highlights of the poster:-
1. Raktamokshana as a treatment of Apabahuka as per Ayurvedic literature.
2. Action of Siravyadha in relieving various symptoms of Apabahuka.
3. Applicability of Siravyadha in Apabahuka in now a days medical
practice. .
Details will be presented in the poster with pictorial support and scientific explanations.
*2nd year M S scholar, Dept of Shalyatantra,Alvas Ayurveda College,Moodbidri.**Asst.Professor, Dept of Shalyatantra,Alvas Ayurveda College,Moodbidri.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 53

AYURVISION 2009
Differential diagnosis in Avabahuka
Dr. Rajesh B*.,Dr. Prathibha B P**. Dr. Basavaraj Hadpad***.
Abstract. Keywords:- Avabahuka, Vyavachedaka nidana. In clinical practice, in order to diagnose a disease, we should have a clear understanding of many other diseases which may mimic a given disease condition. Same is the case with avabahuka. To make its correct diagnosis we should know the lakshanas of many other diseases also, which may resemble like avabahuka, so that we can differentiate one from the other and come to a correct and final diagnosis. *PGCPK Scholar, Dept of Ayurveda KMC,Manipal.** PGCPK Scholar,Dept of Ayurveda,KMC,Manipal.*** Associate professor, Dept of Ayurveda,KMC,Manipal.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 54

AYURVISION 2009
“Different treatment modalities in the management of Avabahuka”.
Dr. Prathibha P K*, Dr. Amrutha**, Dr. Shripathi Adiga H***.
Key words- vata vyadhi, management, different authors, various stages
Abstract –
Avabahuka, in spite of being included under Vata Vyadhis, shoulders numerous therapeutic procedures as a result of the timely work, wit, and experience of different authors.The management of the disease appears to be of different shades as the result of the varied interpretation of its doshic predominance and understanding of its samprapthi.
The copious drugs vow to the optimum utilization of the same in various stages of the disease.As science always endures change for sounder work, there exists immense scope for the proper understanding and therapeutic enhancement in terms of avabahuka.Here, is one such earnest attempt.
*PGCPK Scholar, Dept of Ayurveda KMC,Manipal.** PGCPK Scholar,Dept of Ayurveda,KMC,Manipal.*** Assistant professor, Dept of Ayurveda,KMC,Manipal.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 55

AYURVISION 2009
Modern Correlations of Apabahuka
Dr Parvathy.S.P*,Dr. Zenica D’souza**.__________________________________________________________________
Abstract:Apabahuka is one among the nanatmaja vatavyadhi.Very limited information is available about this particular disease in the classics. It is mentioned for the first time by Acharya Susrutha.There is no mentioning about the disease in Caraka Samhitha. According to Susruta the features include Amsa sosha and Siraakunchana. Ashtanga Hrudayakara defines the disease in the similar way as Susrutha did, adding up another characteristic as Bahu praspanditahara. Clinically the features of Apabahuka are found in many conditions such as Scapulo Humeral Muscular Dystrophy, Osteoarthritis of Shoulder etc., the details of which will be illustrated in the poster presentation.
*2nd Year P G Scholar of dept of Panchakarma,Alvas Ayurveda Medical College, Moodabidri..** Asst. Professor and HOD, Dept of Panchakarma,Alvas Ayurveda Medical College,Moodabidri.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 56

AYURVISION 2009
CURRENT UNDERSTANDING OF AVABAHUKA AND ITS AYURVEDIC MANAGEMENT
*Dr. Savita B. Bhosale ** Dr. R. S. Hiremath ***Dr. Nataraj
Abstract:Avabahuka considered, as one of the vatavyadhi and Sushurta is the first author who explained
nidana and samprapti of avabahuka under vatavyadhi. The vyadhi found mainly in amsa pradesh
(scapular region) characterized with pain, restricted movement of shoulder joint etc that can be
correlated with many pathological conditions of shoulder joint and scapular region. The exact
correlation of avabahuka with underlying modern pathology is not possible but it is always
necessary to put forward nearest postulation to use the objective diagnostic tools and its further
progression of disease process. For this purpose a update interpretation of ayurvedic avabahuka
may be beneficial.
The management as claimed by Ayurvedic physician’s posses it own peculiarity i.e. to eliminate
the Dooshika diathesis by means of Nasya and to revert the process of the dosa dusya
sammurchhana by a better scientific regimen. So in this paper critical analysis of avabahuka and
its management with modern clinical conditions will be discussed in detail.
* P.G Scholar, dept of Rasashastra, K.L.E’S B.M.Kakanwadi Ayurveda Mahavidyalaya
Belgaum.
** Asst. Professor, Dept of Rasashastra, K.L.E’S B.M.Kakanwadi Ayurveda Mahavidyalaya
Belgaum.
*** Lecturer, Dept of Dravyaguna, K.L.E’S B.M.Kakanwadi Ayurveda Mahavidyalaya
Belgaum.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 57

AYURVISION 2009
Understanding Avabahuka under the aegis of contemporary modern science.
Dr Narind*, Dr K. J. Malagi**.________________________________________________________
Keywords: - Avabahuka, Bahu karma kshyakari, contemporary modern science, Syndrome
Abstract: -
Avabahuka, one of the Vata vyadhis explained in the Ayurvedic classics, can be better understood when it is considered as a syndrome rather than a single disease.‘Bahu karma kshayakari’, i.e., inappropriate or even lack of functioning of either one or both the upper limbs is the cardinal feature of the disease.
Contemporary modern sciences enumerate a number of conditions where in either retarded or complete absence of the functioning of the upper limbs are evident.
Here is an earnest attempt to understand the same.
** PGCPK Scholar,Dept of Ayurveda,KMC,Manipal.*** Associate professor, Dept of Ayurveda,KMC,Manipal.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 58

AYURVISION 2009
VARIOUS WAYS TO TREAT APABAHUKA
DR.Priya chandan* ,Dr Zenica**, __________________________________________________________________
Apabahuka , which is a disease condition mainly affecting cervical and shoulder regions, thereby it disturbs the day to day activities. Relief from the symptoms of Apabahuka such as pain, restricted movements etc is essential for leading routine life properly. So thinking about remedies to give relief to such patients is necessary. Here I am doing a small try for the same. Main points to be discussed- (i).Various treatment modalities mentioned in Ayurvedic literatures. (ii) The effects of each treatment modalities. Above mentioned topics will be presented in the poster with the support of scientific and pictorial details.
*2nd Year P G Scholar of dept of Panchakarma,Alvas Ayurveda Medical College, Moodabidri..** Asst. Professor and HOD, Dept of Panchakarma,Alvas Ayurveda Medical College,Moodabidri.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 59

AYURVISION 2009
VISION ON NIDANA & SAMPRAPTHI OF AVABAHUKA
Dr Shivanagouda.S.H *,Dr Madhusudan Kamath**,Dr Shripathi Adiga***.
Abstract :
Key words- disease, nidana, samprapthi, treatment, humors.
Avabahuka, one among the 80 vata vyadhis explained in the ayurvedic classics, incorporates various salient virtues which have always posed problems for the thorough understanding of the disease and formulation of the treatment modalities.
The quest for knowledge in the learned has always encouraged them to reach the zenith in their field of interest. Likewise, Ayurvedic scholars have pin pointed the importance of nidana in the manifestation of diseases and the need to get rid of them initially, as a means of treatment of the disease. The classics explain the same as ‘ nidana parimarjanameva chikitsa’.And also, the apt understanding of the stages in the manifestation of the disease, the humors involved in the same, are all of vitality while planning the treatment of the disease. This view is put forth as ‘samprapthi vighatanameva chikitsa’ in the precious classics of ayurveda, the science of life.
Considering the same in terms of the disease avabahuka, the vision regarding the nidana and samprapthi of the disease is in par with its treatment, in terms of importance. This is an attempt to understand the same.
* PGCPK Scholar,Dept of Ayurveda,KMC,Manipal.** Assistant professor, Dept of Ayurveda,KMC,Manipal.*** Assistant professor, Dept of Ayurveda,KMC,Manipal.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 60

AYURVISION 2009
CURRENT CLINICAL UNDERSTANDING OF APABAHUKA
Dr.Kiran kumar Agadi*.
Abstract.
Keywords:Methods of Diagnosis of Apabahuka.Clinical examinations.Abyanga
sweda and Nasya.Physiotherapy.
Present era is an era of stress. Modern day life style and modern gadgets and competitions in all
walks of life has made man’s life more strenuous than before. It is also responsible for increase
in the incidence of many diseases. Most of these diseases may not be life threatening but hamper
day to day life and human productivity. Apabahuka is one among such diseases, which is
agonizing and affects normal routine work of human being.
Apabahuka is one of the Vatavyadhi, which affects the normal functioning of the upper limb,
especially movements around the shoulder girdle. Pain and stiffness around shoulder girdle
usually develops gradually over several months to a year, it may also progress rapidly in some
patients. Pain may also interference with sleep of individuals.
In contemporary medical science, there are lot of treatment strategies described for its
management. But still the available methods are not satisfactory. Most of the methods are
palliative and there is a high rate of reoccurrence of the problem. On the point of this view
clinical diagnosis of Apabahuka and its management is taken in to consideration for presentation.
Objectives of the poster
Nidanas of Apabahuka. Roopa of Apabahuka. Samprapti ghatakas of Apabahuka. Clinical examinations of Apabahuka. Investigations in Apabahuka. Management of Apabahuka. Pathya – Apathyas of Apabahuka.
* Second year P.G. Scholar.,G.A.M.C. Mysore 21
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 61

AYURVISION 2009
A CRITICAL ANALYSIS OF AVABAHUKA AND ITS MANAGEMENT - AN AYURVEDIC APPROACH.
DR. SUPRIYA .U. PRABHU DESSAI*.
ABSTRACT:
KEYWORDS: - Shoulder pain, Avabahuka.
Shoulder pain is a presenting complaint among adults in outpatient settings. It can be defined as pain in and around the articular surfaces of the shoulder girdle , including the glenohumeral, acromioclavicular, sternoclavicular joints and the scapulothoracic articulation. Common causes of chronic shoulder pain include rotator cuff strain or tear, biceps tendonitis, subacromial bursitis, glenohumeral osteoarthritis, impingement syndrome and adhesive capsulitis. The condition can produce substantial disability and difficulty with activities of daily living. This conditions can be correlated with Avabahuka- under both saam and niraam conditions. The elaborate descriptions are available in our classics to manage pain, in which the vaata is the main culprit as our acharya’s say, “na vaatena vina shula”. So, here an effort is made to overcome shoulder pain, one of the most common occupational disorders, by ayurvedic management, to relieve pain and stiffness and to improve function.
*PG Scholar,Dept of Kayachikitsa,SDM College of Ayurveda,Udupi
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 62

AYURVISION 2009
AYURVISION 2009Guests/ Resource Persons List
01.Dr. Charudatta. Asst .Prof, Dept. of Radiology, KMC,Manipal. 02.Dr. Vivek Pandey, Associate Professor, Dept. of Orthopaedics, KMC,Manipal.
03.Dr. G.R. Vastrad, Prof, Dept of Kayachikisa, Taranath Govt. Ayurvedic Medical Colleg,Bellary. 04.Dr.S.G. Mangalagi, HOD, Post Graduate Studies in Kayachikitsa, Govt Ayurvedic College, Mysore
05.Dr. Prasanth, Assistant Prof, Department of Kayachikitsa, Ayurveda Mahavidyalaya, Hubli.
06.Dr. K. Govindan Namboodari, Prof. Dept. Kayachiktisa, Govt. Ayurvedic College, Thiruvananthapuram.
07.Prasanna Mogasale. Asst Prof.Dept of PG Studies in Kayachikitsa, SDM College of Ayurveda.Udupi.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 63

AYURVISION 2009
AYURVISION – 2009LIST OF DELEGATES REGISTERED
Sl. No. Name Place01. Dr. Rajesh , BAMS (PGCPK) PGCPK – Manipal02. Dr. Divya Nayak , BAMS (PGCPK) PGCPK – Manipal03. Dr. Shailesh, BAMS (PGCPK) PGCPK – Manipal04. Dr. Amruta , BAMS (PGCPK) PGCPK – Manipal05. Dr. Pratibha P. K, BAMS (PGCPK) PGCPK – Manipal06. Dr. Sapana Singh, BAMS (PGCPK) PGCPK – Manipal07. Dr. Narind Khajuria, BAMS (PGCPK) PGCPK – Manipal08. Dr. Pratibha B. P, BAMS (PGCPK) PGCPK – Manipal09. Dr. Shivan Gouda S. H, BAMS (PGCPK) PGCPK – Manipal10. Dr. Jayanti Tripati, BAMS (PGCPK) PGCPK – Manipal11. Agamya S Udupi 12. Dr. Akarshani A. M (MD) Mysore 13. Dr. Sidram M Guled (MD) Mysore 14. Dr. Shivanand K Pyati (MD) Mysore 15. Dr. Chitralatha (MD) Mysore 16. Dr. Triveni (MD) Mysore 17. Dr. Kiran Kumar Agadi (MD) Mysore 18. Dr. Mahesh Sharma M N (MD) Mysore 19. Dr. Sowmya S Bhat (MD) Mysore 20. Dr. Anil Kumar H K (MD) Mysore 21. Dr. Shubharani M (MD) Mysore22. Dr. Geetha Kumari S (MD) Mysore 23. Dr. Sween , PGCPK Haryana 24. Dr. Supriya , PGCPK Goa25. Dr. Arun J Wilson (MD) Moodbidri 26. Dr. Shweta A H (MD) Moodbidri
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 64

AYURVISION 2009
27. Arifa M P (MD) Moodbidri28. Dr. Rebu K Joseph (MD) Moodbidri29. Dr. Swapna Gunjal (MD) Moodbidri30. Dr. Susha John (MD) Moodbidri31. Dr. Parvathy S. P (MD) Moodbidri32. Dr. Priya Chandran (MD) Moodbidri33. Dr. R. P Ranjit (MD) Moodbidri34. Dr. Savitha B Bhonsle BAMS, PGCPK Belgaum35. Dr. Aravind M. C, BAMS, PGCPK Mumbai 36. Dr. Poornima Desai , BAMS, PGDPK Goa37. Dr. Rashmila Chindakar , BAMS Goa 38. Dr. Zenica , M. D Moodbidri39. Dr. Nayana, BAMS, PGCPK Moodbidri40. Dr. Anjali , BAMS, PGCPK Bangalore 41. Dr. Premanand, BAMS, PGCPK Tamil Nadu42. Dr. Anil Tamannavar , BAMS, PGCPK Gadag 43. Mrs. Savitha A Tamannavar, LLB Gadag 44. Dr. Ramesh Konkeri, MD Belgaum45. Dr. Laxmi R Konkeri , BAMS Belgaum 46. Dr. Meera, BAMS, PGDPK USA47. Dr. Akiko, BAMS Japan 48. Dr. Vijay Kumar B, BAMS Bellary 49. Dr. Deepak S Mummigatti, MD Dharwad50. Dr. Neeta D. Mummigatti , BAMS Dharwad 51. Dr. B. M. Anuradha, BAMS, PGCPK Belur52. Dr. Prakash Naik, BAMS Udupi53. Dr. Praveen Kumar, (MD) Hubli 54. Dr. Sivakumar, (MD) Hubli55. Dr. Vivekananda, BAMS Kannur 56. Dr. Vidyoth, BAMS Pallikannur
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 65

AYURVISION 2009
INSPIRED BY LIFE
“ EXPLORING THE NEW FRONTIERS IN ACADEMIC & SCIENTIFIC AYURVEDA”
CME ON “AVABAHUKA”ON 19th & 20th DEC AT K.M.C. OF UNIVERSITY OF MANIPAL, THE SOARING FOUNTAIN OF KNOWLEDGE
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 66

AYURVISION 2009
MAY THIS CME BE A GREAT OPPORTUNITY TO IGNIT MINDS TO DISCOVER & EXCEL WHILE ENCOURAGING
THE SPIRIT OF RESEACH & INNOVATION !
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 67

AYURVISION 2009
WITH BEST COMPLIMENTS FROM
Dr Kusala Wijesundara on behalf of AMDA Peace Clinic at Bodhgaya with the pure sense of “Sri Lankan Fellow ship” & “So go - Fu jo spirit”
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 68

AYURVISION 2009
POSTERS
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 69

AYURVISION 2009
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 70

AYURVISION 2009
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 71

AYURVISION 2009
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 72

AYURVISION 2009
Best Compliments From:
MR. VIDYAVANTH KAMATHAuthorised Dealer Kottakkal Arya Vaidya SalaOpp. Corporation, Bank, Manipal
The Himalaya Drug Company.
SG Phyto pharma Pvt Ltd.
Millenium Herbal Care Ltd.
Vasu Health Care Pvt Ltd.
Organized by Department of Ayurveda, Kasturba Medical College & Hospital, Manipal 73