-
7/30/2019 Axillary Dissection vs No Axillary Dissection in Women
With Invasive Breast Cancer and Sentinel Node Metastasis (
1/7
ORIGINAL CONTRIBUTION
Axillary Dissection vs No Axillary Dissectionin Women With
Invasive Breast Cancerand Sentinel Node MetastasisA Randomized
Clinical Trial
Armando E. Giuliano, MD
Kelly K. Hunt, MD
Karla V. Ballman, PhD
Peter D. Beitsch, MD
Pat W. Whitworth, MD
Peter W. Blumencranz, MD
A. Marilyn Leitch, MD
Sukamal Saha, MD
Linda M. McCall, MS
Monica Morrow, MD
AXILLARY LYMPH NODE DISSEC-tion (ALND) has been part
ofbreastcancersurgery sincethedescriptionof theradicalmas-
tectomy.1 ALNDreliably identifiesnodal
metastases and maintains regional con-trol,2,3 but the
contribution of localtherapy to breast cancer survival is
con-troversial.4,5 TheEarlyBreastCancerTri-alists Collaborative
Group synthesizedfindings from 78 randomized con-trolled trials,
concluding that local con-trol of breastcancer was associated
withimproved disease-specific survival.6
ALND, as a means for achieving lo-cal disease control, carries
an indisput-able andoften unacceptable risk of com-plications such
as seroma, infection,and
lymphedema.7-9
Sentinel lymph nodedissection (SLND) was therefore devel-oped to
accurately stage tumor-draining axillary nodes with less mor-bidity
than ALND.10 SLND alone is
theacceptedmanagementforpatientswhose
Author Affiliations: John Wayne Cancer Institute atSaint Johns
Health Center, Santa Monica, California(Dr Giuliano); M. D.
Anderson Cancer Center, Hous-ton, Texas (Dr Hunt); Mayo Clinic
Rochester, Roch-ester, Minnesota (Dr Ballman); DallasSurgical
Group,Dallas, Texas (Dr Beitsch); Nashville Breast
Center,Nashville, Tennessee (Dr Whitworth); Morton PlantHospital,
Clearwater, Florida (Dr Blumencranz); Uni-versity of Texas
Southwestern Medical Center, Dallas
(Dr Leitch); McLaren Regional Medical Center, Michi-ganState
University, Flint (Dr Saha);American Collegeof Surgeons Oncology
Group, Durham, North Caro-lina (Ms McCall); and Memorial
Sloan-KetteringCancer Center, New York, New York (Dr
Morrow).Corresponding Author:Armando E. Giuliano, MD,JohnWayne
Cancer Institute at Saint Johns Health
Cen-ter,2200SantaMonicaBlvd,SantaMonica, CA
90404([email protected]).
Context Sentinel lymph node dissection (SLND) accurately
identifies nodal metas-tasis of early breast cancer, but it is not
clear whether further nodal dissection affectssurvival.
Objective To determine the effectsof complete axillary lymph
node dissection (ALND)
on survival of patients with sentinel lymph node (SLN)
metastasis of breast cancer.Design, Setting, and Patients The
American College of Surgeons Oncology GroupZ0011 trial, a phase 3
noninferiority trial conducted at 115 sites and enrolling
patientsfrom May 1999 to December 2004. Patients were women with
clinical T1-T2 invasivebreast cancer, no palpable adenopathy, and 1
to 2 SLNs containing metastases iden-tified by frozen section,
touch preparation, or hematoxylin-eosin staining on perma-nent
section. Targeted enrollment was 1900 women with final analysis
after 500 deaths,but the trial closed early because mortality rate
was lower than expected.
Interventions All patients underwent lumpectomy and tangential
whole-breast irra-diation. Those with SLNmetastases identified by
SLNDwere randomized to undergo ALNDor no further axillary
treatment. Those randomized to ALND underwent dissection of 10or
more nodes. Systemic therapy was at the discretion of the treating
physician.
Main Outcome Measures Overall survival was the primary end
point, with a non-inferiority margin of a 1-sided hazard ratio of
less than 1.3 indicating that SLND alone
is noninferior to ALND. Disease-free survival was a secondary
end point.Results Clinical and tumor characteristics were similar
between 445 patients ran-domized to ALND and 446 randomized to SLND
alone. However, the median num-ber of nodes removed was 17 with
ALND and 2 with SLND alone. At a median fol-low-up of 6.3 years
(last follow-up, March 4, 2010), 5-year overall survival was
91.8%(95% confidence interval [CI], 89.1%-94.5%) with ALND and
92.5% (95% CI, 90.0%-95.1%) with SLND alone; 5-year disease-free
survival was 82.2% (95% CI, 78.3%-86.3%) with ALND and 83.9% (95%
CI, 80.2%-87.9%) with SLND alone. The haz-ard ratio for
treatment-related overall survival was 0.79 (90% CI, 0.56-1.11)
withoutadjustment and0.87 (90% CI, 0.62-1.23) after adjustingfor
age and adjuvant therapy.
Conclusion Among patients with limited SLN metastatic breast
cancer treated withbreast conservation and systemic therapy, the
use of SLND alone compared with ALNDdid not result in inferior
survival.
Trial Registration clinicaltrials.gov Identifier:
NCT00003855
JAMA. 2011;305(6):569-575 www.jama.com
For editorial comment see p 606.
2011 American Medical Association. All rights reserved.
(Reprinted) JAMA, February 9, 2011Vol 305, No. 6 569
-
7/30/2019 Axillary Dissection vs No Axillary Dissection in Women
With Invasive Breast Cancer and Sentinel Node Metastasis (
2/7
sentinel lymph nodes (SLNs) are histo-logically free of tumor,
while ALND re-
mains the standard of care for patientswhose SLNs contain
metastases.11
Cancer biology is much better under-stood now than it was when
ALND wasintroduced. Biological factorsmay affectthe predilectionof
some malignant cellsto selectively invadelymph nodes ratherthan
visceral organs, just as certain tu-mor types metastasize to
certain organsandnot others.12 Recognitionof thecom-plexity of
tumor biology has changedcancer treatment, with more liberal useof
systemic therapy to treat occult can-
cer cells wherever they may be in thebody. Consequently, the
decisionto ad-minister systemic therapy is influencedby a variety
of patient- and tumor-related factors, with lymph node tumorstatus
influencing13,14 but not necessar-ilydictatingthe useof
chemotherapy.15-18
Other factors, such as early cancer de-tection by screening
mammography,have ledto earlier intervention in breastcancer,
reducing the incidence of nodalmetastases and even the number of
tu-mor-involved lymph nodes.19
These evolving concepts have calledinto question the need for
ALND.20,21 Avariety of algorithms have been devel-oped to help
clinicians decide whichpa-tients wouldbenefit from ALND.22-24
Re-view of Surveillance,Epidemiology, andEndResults data hasshown
that theuseof ALND for SLN metastases has de-creased in recent
years.25 No study has
conclusively demonstrated a survivalbenefit or detrimentfor
omitting ALND
when metastatic breast cancer is identi-fied by SLND. In the
late 1990s, theAmerican College of Surgeons Oncol-ogy Group
designed andbegan themul-ticenter Z0011 trial.Theprimary aimofthis
study was to determine the effectsof ALND on overall survival in
patientswith SLN metastases treated in the con-temporary era with
lumpectomy, adju-vant systemic therapy, and tangential-field
radiation therapy.
METHODS
Patient CharacteristicsThis multicenter, randomized phase 3trial
was registered with the NationalCancer Institute andapproved by
thein-stitutional review boards of participat-ing centers. All
patients provided writ-ten informed consent. Adult womenwith
histologically confirmed invasivebreastcarcinoma clinically 5 cm or
less,no palpable adenopathy, and an SLNcontaining metastatic breast
cancerdocumented by frozen section, touchpreparation, or
hematoxylin-eosin stain-
ing on permanent section were eligiblefor participation.
Patients with metas-tases identified initiallyor solely
withim-munohistochemical stainingwereineli-gible. Treatment with
lumpectomy tonegative margins (no tumor at ink) wasrequired. Women
wereineligible if theyhad 3 or more positive SLNs, mattednodes, or
gross extranodal disease, or if
they had received neoadjuvant hor-monal therapy or
chemotherapy.
Study Design and Treatment
Before randomization, all women un-derwent SLND and were
stratified ac-cordingto age (50 and50 years),es-trogen-receptor
status, and tumor size(1cm,1cmand2cm,or2 cm).Eligible women were
randomly as-signed to ALND or no further axillary-specific
interventionspecifically, nothird-field nodal irradiation.
ALNDwasdefinedas ananatomical level I andII dis-section including
at least 10 nodes. Allwomen were to receive whole-breastopposing
tangential-field radiationtherapy. The use of adjuvant
systemictherapy was determined by the treatingphysician and was not
specified in the
protocol.Patients most commonly entered the
study post-SLND following identifica-tion of metastases on final
pathology re-port. However, of the 891 registered pa-tients, 287
were registered pre-SLNDand assigned to treatment after
intraop-erative documentation of SLN metasta-ses. Patients in this
group subsequentlyfound to have 3 or more tumor-involvedlymph nodes
were included in theanaly-sis. Patientswereassessed for
diseasere-currence according to standard clinical
practice.History and physical examina-tion were performed every
6 months forthe first 36 months and yearly thereaf-ter. Annual
mammography was re-quired; other testing was based on symp-toms and
investigator preference.
Study End Points
The primary end point was overall sur-vival, defined as the time
from random-ization until death from any cause. Ashort-term primary
end point was oc-currence of surgical morbidities. The
study plan was to report surgical mor-bidities following the
completion of ac-crual and prior to overall survival re-porting
after receiving permissionfromthe data and safety monitoring
com-mittee. These morbidities have beenreported.10
A secondary end point was disease-free survival, defined as the
time from
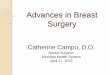
Figure 1. Study Flow
420 Included in primary analysis
25 Excluded (withdrew prior to surgery)
436 Included in primary analysis
10 Excluded (withdrew prior to surgery)
445 Randomized to receive ALND420 Received ALND as
randomized
25 Withdrew prior to surgery
446 Randomized to receive SLND alone436 Received SLND alone
as randomized
10 Withdrew prior to surgery
92 Lost to follow-up2 Discontinued intervention
1 Refused after randomizationbut prior to surgery
1 Consent obtained afterpatient registered
74 Lost to follow-up3 Discontinued intervention
2 Refused after randomizationbut prior to surgery
1 Opted for alternative therapy
891 Patients randomized
ALND indicates axillary lymph node dissection; SLND, sentinel
lymph node dissection.
SENTINEL NODE DISSECTION IN INVASIVE BREAST CANCER
570 JAMA, February 9, 2011Vol 305, No. 6 (Reprinted) 2011
American Medical Association. All rights reserved.
-
7/30/2019 Axillary Dissection vs No Axillary Dissection in Women
With Invasive Breast Cancer and Sentinel Node Metastasis (
3/7
randomization to death or first docu-mented recurrence of breast
cancer.Breast cancer recurrence was catego-rized as locoregional
disease (tumor inthe breast or ipsilateral supraclavicu-lar,
subclavicular, internal mammary,
or axillary nodes) or distant metasta-ses. Disease-free survival
and its com-ponents (locoregional disease and dis-tant metastases)
are reported insteadofthe protocol-specified secondary endpoint
(eg, distant diseasefree sur-vival) to facilitate comparison
withother studies.
Statistical Analysis
The primary end point was overall sur-vival as a measure of
noninferiority ofno further axillary specified interven-tions
(SLND-alone group) compared
with the ALND group. Based on the lit-erature at the time of
study design, wehypothesized that overall survival was80% at 5
years for optimally treatedwomen with positive nodes.26-28
Clini-cal noninferiority was defined as theSLND-alone group having
a 5-year sur-vival of not less than 75% of that ob-served in the
ALND group. Noninferi-ority of the SLND-alone treatment wasalso
considered if the hazard ratio (HR)for mortality was less than 1.3
whencomparedwith ALND. An estimated 500
deaths were neededfor the study to have90%power to confirm
noninferiority ofSLND alone compared with ALND, withthe use of a
2-sided 90% confidence in-terval (CI) for the HR from a Cox
re-gression model.29 Specifically, if the90% CI for the HR was
below 1.3, thiswould indicate that patients undergo-ing SLND alone
do not have an unac-ceptably worse overall survival than pa-tients
undergoing SLND plus ALND.
The use of a 2-sided 90% CI corre-sponds to a 1-sided
significance level of
.05.
30
Theenrollment of 1900 patients in4 years with a minimum
follow-up pe-riod of5 yearswasinitiallyplanned. Fourformal
interimanalysesand 1 final analy-siswere planned foroverall
survival,andthe OBrien-Flemming-spending strat-egy was used to
generate stoppingboundaries for each planned analysis.Theoverall
study significancewasmain-
tained at .05. However, none of theplanned interim analyses were
per-formed beforethestudy wasclosedbasedon the recommendation of
the data andsafety monitoring committee. Because ofthis,a
singleterminal hypothesis test with
an
of .05 is applied to the data, whichmakes it consistent with the
plannedoverall significance level of .05 in theoriginal study
plan.
Ineligible patients were retained inall analyses (ie, both the
intent-to-treat analyses and the treatment-received analyses).
Kaplan-Meier sur-vival curves for overall survival werecompared by
log-rank test. The unad-justed HR (and 90% CI) was calcu-lated
using a Cox regression analysis,and noninferiority P values are
re-ported. As a secondary analysis, known
prognostic factors including adjuvanttreatment were included in
the Cox re-gression model to generate an ad-justed HR for overall
survival (with a90% CI and noninferiority P
values).Disease-freesurvival was analyzed usingKaplan-Meier curves
and univariableandmultivariable Cox regression analy-ses with 95%
CIs. The fact that therewere only 94 deaths limited the num-ber of
variables that could be used in amultivariable model without
affectingmodel stability. We created a base
model that included the treatmentgroup (SLND alone vs ALND),
age(50 vs 50 years), and whether thepatient received adjuvant
therapy (yesvs no) and added prognostic variablesto this model
individually. Only vari-ables obtained on 90% or more of
thepatients were included in the multi-variable analysis.
Locoregional recur-rence rates were compared with theFisher exact
test. Each analysis, otherthan analysis for the primary end pointof
overall survival, was performed with
2-sidedP
values, 5% significance, anda 95% CI; all analyses were
performedusing SASrelease 9.1(SAS Institute Inc,Cary, North
Carolina).
RESULTS
Patient Characteristics
The first patient was enrolled in May1999, and accrual closed in
December
2004 based on a recommendation of theindependent data and safety
monitor-ing committee because of concerns re-garding the extremely
low mortality
rate. Even if the trial had accrued thetargeted 1900 patients,
it would havetaken more than 20 years of follow-upto observe 500
deaths at the realizedevent rate. At the time of the decisionto
terminate the study there had beenno formal analysis comparing the
sur-vival experience between the 2 groups;the decision was based
solely on the ob-
Table 1. Baseline Patient and TumorCharacteristics by Study
Group
Characteristic
No. (%)
ALND(n = 420)
SLND Alone(n = 436)
Age, median (range), y 56 (24-92) 54 (25-90)
Missing 7 10Clinical T stage
T1 284 (67.9) 303 (70.6)
T2 134 (32.1) 126 (29.4)
Missing 2 7
Tumor size, median(range), cm
1.7 (0.4-7.0) 1.6 (0.0-5.0)
Missing 6 14
Receptor statusER/PR 256 (66.8) 270 (68.9)
ER/PR 61 (15.9) 54 (13.8)
ER/PR 3 (0.8) 4 (1.0)
ER/PR 63 (16.5) 64 (16.3)
Missing 37 44
LVIYes 129 (40.6) 113 (35.2)
No 189 (59.4) 208 (64.8)
Missing 102 115
Modified Bloom-Richardson score
1 71 (22.0) 81 (25.6)
2 158 (48.9) 148 (46.8)
3 94 (29.1) 87 (27.5)
Missing 97 120
Tumor typeInfiltrating ductal 344 (82.7) 356 (84.0)
Infiltrating lobular 27 (6.5) 36 (8.5)
Other 45 (10.8) 32 (7.5)
Missing 4 12
Lymph nodemetastases0 4 (1.2) 29 (7.0)
1 199 (58.0) 295 (71.1)
2 68 (19.8) 76 (18.3)
3 25 (7.3) 11 (2.7)
4 47 (13.7) 4 (1.0)
Missing 77 21
Abbreviations:ALND, axillarylymphnode dissection;
ER,es-trogenreceptor;LVI, lymphovascularinvasion; PR, proges-terone
receptor; SLND, sentinel lymph node dissection.
SENTINEL NODE DISSECTION IN INVASIVE BREAST CANCER
2011 American Medical Association. All rights reserved.
(Reprinted) JAMA, February 9, 2011Vol 305, No. 6 571
-
7/30/2019 Axillary Dissection vs No Axillary Dissection in Women
With Invasive Breast Cancer and Sentinel Node Metastasis (
4/7
served mortality rate for pooled datafromthe 2 groups. The date
of last fol-low-up for this analysis was March 4,2010.
Patients were enrolled from 115 in-stitutions, which
includedaffiliatesoftheCancer Trials Support Unit and
theNorthCentral Cancer TreatmentGroup.Of 891 patients, 445 were
randomly as-signed to the ALND group and 446 tothe SLND-alone group
(FIGURE 1).Thirty-five patients were excluded af-ter withdrawing
consent prior to sur-gery. The 103 ineligible patients wereincluded
in the analyses reported here.Because this was a noninferiority
trial,a more conservative analysis was per-
formed on the treatment-receivedsample (n = 813 patients); 32
patientsin the ALND group did not have ALND,and 11 patients in the
SLND-alonegroup had ALND. No qualitativedifferences were observed
betweentreatment-received sample and intent-to-treat
sampleanalyses,so only intent-to-treat results are reported.
Diseasecharacteristics at baselinewerewell bal-anced between the 2
groups(TABLE 1).
Treatment Results
There was an expected differencebetween ALND and SLND-alone
treat-ment groupsin total numberof removedlymph nodes and total
number oftumor-involved nodes; the median totalnumber of nodes
removed was 17 (in-terquartile range [IQR], 13-22) in theALND group
and 2 (IQR, 1-4) in theSLND-alone group.31 The median total
number of nodes with histologicallydemonstrated tumor
involvement (in-cluding SLNs) in the ALND group andSLND-alone group
was equal (1 [IQR,
1-2] for both groups). Hematoxylin-eosinstained tumor deposits
no largerthan 2 mm were defined as microme-tastases and were
identified in SLNs of137 of 365 patients (37.5%) in theALND group
comparedwith 164 of 366(44.8%) in the SLND-alone group(P=.05).In
the ALNDgroup, 97of 355patients(27.3%)had additional metas-tasis in
lymph nodes removed by ALND,including 10% of patients with
SLNmicrometastasis who had macroscopi-callyinvolved non-SLNs
removed. Total
nodal involvement is summarized inTable 1; 21.0% of patients
undergoingALND had 3 or more involved nodescompared
with3.7%undergoing SLNDalone. Four or more involved nodeswere seen
in 13.7% of patients receiv-ing ALND and 1.0% of those
receivingSLND alone.
Adjuvant systemic therapy was de-livered to 403 women (96.0%) in
theALND group and 423 women (97.0%)in the SLND-alone group.31 No
differ-ences in the proportion of women re-
ceiving endocrine therapy, chemo-therapy, or both were observed.
Thetypeof chemotherapyadministeredwassimilar in the 2 groups;
anthracycline-and taxane-based combination regi-mens were the most
common. The ma-jority of the women (n =605) receivedwhole-breast
radiation therapy: 263of 296 (88.9%) in the ALND group
and 277 of 309 (89.6%) in the SLND-alone group.
Overall Survival
At a median follow-upof 6.3years (IQR,5.2-7.7), there were 94
deaths (SLND-alone group, 42; ALND group,52). Theuseof SLND
alonecomparedwithALNDdid not appear to result in
statisticallyinferior survival (FIGURE2) (P=.008fornoninferiority).
The unadjusted HRcomparing overall survival between theSLND-alone
groupandthe ALNDgroupwas 0.79 (90% CI, 0.56-1.10), whichdidnot
cross the specifiedboundary of1.3(FIGURE 3). The 5-year overall
sur-vival rates were92.5%(95% CI, 90.0%-95.1%) in the SLND-alone
group and91.8% (95% CI, 89.1%-94.5%) in theALND group. This was
substantially
greater than the 80% anticipated at pro-tocol design. The HR for
overall sur-vival adjusting for adjuvant therapy(chemotherapy,
endocrine therapy,and/or radiation therapy) and age forthe
SLND-alone group compared withthe ALND group was 0.87 (90%
CI,0.62-1.23). The adjusted HRs compar-ing the SLND-alone group
with theALND group in the other multivari-able models ranged from
0.86 to 0.92(TABLE 2), all similar to the unad-just ed rate of
0.79. An exploratory
analysis revealed that treatment withALND vs SLND alone produced
no sta-tistically significant difference in out-come among patients
groupedby recep-tor status of the primary tumor (ER/PR or
ER/PR).
Disease-Free Survival
Disease-free survival (Figure 2) did notdiffer significantly
between treatmentgroups. The 5-year disease-free survivalwas 83.9%
(95% CI, 80.2%-87.9%) forthe SLND-alone group and82.2% (95%
CI, 78.3%-86.3%) for the ALND group(P=.14). The unadjusted HR
compar-ing the SLND-alone group with theALND group was 0.82 (95%
CI, 0.58-1.17),and the HR adjusted for adjuvanttreatment and age
was 0.88 (95% CI,0.62-1.25) (TABLE3). Theadjusted HRscomparing the
SLND-alone group withthe ALND group in the other multivari-
Figure 2. Survival of the ALND Group Compared With SLND-Alone
Group
100
90
80
40
50
70
60
30
20
Log-rankP=.25100
No. at riskALNDSLND alone
420436
1
408421
2
398411
3
391403
4
378387
5
313326
6
223226
7
141142
8
7474
Years
Alive
Survival,%
100
90
80
40
50
70
60
30
20
10
0
ALND
SLND alone Log-rankP=.14
420436
1
369395
2
335363
3
310337
4
286307
5
226231
6
152147
7
8381
8
3736
Years
Alive and Disease-Free
ALND indicates axillary lymph node dissection; SLND, sentinel
lymph node dissection.
SENTINEL NODE DISSECTION IN INVASIVE BREAST CANCER
572 JAMA, February 9, 2011Vol 305, No. 6 (Reprinted) 2011
American Medical Association. All rights reserved.
-
7/30/2019 Axillary Dissection vs No Axillary Dissection in Women
With Invasive Breast Cancer and Sentinel Node Metastasis (
5/7
able models ranged from 0.84 to 0.89(Table 3), all similar to
the unadjustedrateof0.82. Locoregionalrecurrenceandits correlates
have been previouslyreported.31 The5-yearratesoflocalrecur-rence
were 1.6% (95% CI, 0.7%-3.3%)
intheSLND-alonegroupand3.1%(95%CI, 1.7%-5.2%) in the ALND
group(P=.11). Locoregional recurrencefreesurvival at 5 years was
96.7% (95% CI,94.7%-98.6%)in theSLND-alone
groupand95.7%(95%CI,93.6%-97.9%)intheALND group (P=.28).
Surgical Morbidities
Paresthesias, shoulder pain, weakness,lymphedema, and axillary
web syn-drome are recognized morbidities ofALND.7-9 As previously
reported,10 therate of wound infections, axillary sero-
mas, and paresthesiasamong patientsintheZ0011 trial was higher
for theALNDgroup than for the SLND-alone group(70% vs25%,P.001).
Lymphedema inthe ALND group was significantly morecommonby
subjectivereport (P.001)and also tended to be higher by objec-tive
assessment of arm circumference.These findings are in accordance
withother randomized comparisons of SLNDwith vs without
ALND.32,33
COMMENTIn the American College of SurgeonsOncology Group Z0011
randomizedtrial, ALND did not significantly affectoverall or
disease-free survival ofpatients with clinical T1-T2 breast
can-
cerand a positiveSLNwho were treatedwith lumpectomy, adjuvant
systemictherapy, and tangential-field whole-breast radiation
therapy. These sur-vival findingsare consistent withthoseof
theNational SurgicalAdjuvant Breastand Bowel Project B04 trial, in
whichwomen with clinically negative nodeswere randomized to
treatment by radi-cal mastectomy, total mastectomy plusnodal
irradiation, or total mastectomywith delayed ALND if nodal
recur-rence was observed.4 Initially and ateach interim analysis
for up to 25 years
of follow-up, no statistically signifi-cant survival differences
were observedbetween any of the groups.For patientstreated in the
modern era, the rel-evanceofthe B04study,which includedpatients
with larger tumors undergo-ing mastectomy without adjuvant
sys-temic therapy, is uncertain, because anaxillary recurrence
after SLND inpatientswith a lower risk of deathfromdistant disease
might negatively affect
survival. ThefindingsfromZ0011 docu-ment the high rate of
locoregionalcon-trol achieved with modern multimo-dality therapy,
even without ALND.
Incontrast toB04,inwhich about 40%of patients in the radical
mastectomy
group were node-positive and the samenumber in the total
mastectomy groupwere assumed to be node-positive and5-year overall
survival was only about60%, 100% of patients in Z0011 hadnodal
involvement; yet the 5-year over-
Figure 3. Hazard Ratios Comparing OverallSurvival Between the
ALND and SLND-AloneGroups
1.0 1.30.5
Unadjusted
Adjusted
Hazard Ratio (90% CI)
for Overall Survival
2.0
Favors
SLND Alone
Favors
ALND
Blue dashed line at hazard ratio=1.3 indicates non-inferiority
margin;blue-tintedregionto theleft of haz-ard ratio=1.3 indicates
values for which SLND alonewouldbe considerednoninferior to SLND
plusALND.ALNDindicatesaxillarylymphnodedissection;CI,
con-fidenceinterval; SLND, sentinellymph nodedissection.
Table 2. Adjusted Hazard Ratios for Overall Survival Comparing
SLND-Alone vs ALND Groups
Model Variables
No.Adjusted HR
(90% CI)Noninferiority
P ValuePatients Events
Treatment group (SLND alone vs ALND), age (50 vs 50
y),adjuvantly treated (yes vs no)
839 92 0.87 (0.62-1.23) .03
Variables in row 1 primary tumor size (per 1 cm, continuous) 818
92 0.89 (0.62-1.25) .03
Variables in row 1 estrogen receptor status (negative vs
positive) 778 87 0.92 (0.64-1.30) .05
Variables in row 1 modified Bloom-Richardson score (1 vs 2 vs 3)
839 92 0.86 (0.61-1.21) .02
Variables in row 1 tumor type (ductal vs lobular vs other) 839
92 0.88 (0.63-1.25) .03
Abbreviations: ALND, axillary lymph node dissection; CI,
confidence interval; HR, hazard ratio; SLND, sentinel lymph node
dissection.
Table 3. Adjusted Hazard Ratios for Disease-Free Survival
Comparing SLND-Alone vs ALND Groups
Model Variables
No. Adjusted HR(95% CI) P ValuePatients Events
Treatment group (SLND alone vs ALND), age (50 vs 50
y),adjuvantly treated (yes vs no)
839 127 0.88 (0.62-1.25) .47
Variables in row 1 primary tumor size (per 1 cm, continuous) 818
125 0.86 (0.60-1.22) .40
Variables in row 1 estrogen receptor status (negative vs
positive) 778 117 0.84 (0.58-1.20) .33
Variables in row 1 modified Bloom-Richardson score (1 vs 2 vs 3)
839 127 0.87 (0.61-1.23) .43
Variables in row 1 tumor type (ductal vs lobular vs other) 839
127 0.89 (0.62-1.27) .52
Abbreviations: ALND, axillary lymph node dissection; CI,
confidence interval; HR, hazard ratio; SLND, sentinel lymph node
dissection.
SENTINEL NODE DISSECTION IN INVASIVE BREAST CANCER
2011 American Medical Association. All rights reserved.
(Reprinted) JAMA, February 9, 2011Vol 305, No. 6 573
-
7/30/2019 Axillary Dissection vs No Axillary Dissection in Women
With Invasive Breast Cancer and Sentinel Node Metastasis (
6/7
allsurvival wasmore than 90%. Further-more, a 19% rate of
axillary first failurewas observed in B04,4 whereas the axil-lary
nodal recurrencerate wasonly 0.9%in theSLND-alonegroup inZ0011.31
Theexcellent local and distant outcomes in
this study highlight the effects of mul-tiple changes in breast
cancer manage-ment during the interval between the 2studies. These
changes, which includeimproved imaging, moredetailed patho-logical
evaluation, improvedplanning ofsurgical and radiation approaches,
andmoreeffective systemic therapy, empha-size the need for ongoing
reevaluationof standard local therapy.
The well-documented morbidityfrom ALND has led other
investiga-tors to explore alternative methods ofaxillary treatment
in patients withclini-
cally negative nodes, including radia-tion, systemic therapy,
and axillaryobservation. These have consistentlydemonstrated low
axillary failure rates,with no significant differences in
sur-vival.34,35 The International Breast Can-cerStudyGrouptrialof
ALND vs obser-vation is noteworthy becausemorethanhalf
ofthepatientsdid notreceivebreastor axillary radiotherapy. In women
60years and older receiving adjuvanttamoxifen butno
axillarytreatment, therateof axillary recurrence wasonly 3%,
andoverall survival was73% at a medianfollow-up of 6.6
years.36
The low rates of locoregional recur-rence at 5 years and the
nearly identi-cal overall and disease-free survival be-tween
treatment groups in Z0011would suggest that differences in
sur-vival between study groups are un-likely to emerge with longer
follow-up, because ALND would only affectsurvival by virtue of
improved locore-gional control. In theEarly Breast Can-cer
Trialists Collaborative Group over-
view, statistically significant survivaldifferences between
treatments at 15years were seen only when differencesin
locoregional recurrence betweentreatments were greater than 10% at
5years.6 Axillary recurrence is usually anearly event, occurring at
a median of14.8 months in B04; in that trial, only7 of 68 axillary
recurrences occurred
more than 5 years after study entry.4
Greco et al37 reported that median timeto axillary recurrence
was 30.6 monthsfor 401 patients who underwent breast-conserving
procedures and radiationtherapy with no axillary surgery. Re-
cent reports of long-term follow-up inrandomized trials confirm
these find-ings.38,39 Because the total locore-gional recurrence
rate in the Z0011SLND-alone group at 5 years is only2.5% compared
with 3.6% in the ALNDgroup, it is unlikely that further fol-low-up
would result in enough addi-tional recurrences to generate a
clini-cally meaningful survival differencebetween groups. The
absolute differ-ence in 5-year overall survival be-tween the
treatment groups in Z0011is 0.7%, numerically favoring the
SLND-
alone group. The HR for overall sur-vival comparing the
SLND-alonegroupwith the ALND group was 0.79 (90%CI, 0.56-1.10). The
worst HR (1.10) isless than 1.3, which was hypothesizedas the
inferiority margin threshold. Inessence, this meansthat the5-year
over-all survival for the SLND-alone groupmight be as low as 90.3%
if the true5-year overall survival for the ALNDgroup was 91.8% and
the HR as highas 1.10. Most importantly, there is nosuggestion that
rates of locoregional re-
currence, the mechanism by whichvariations in local therapy
result in sur-vival differences, differ between groupsto the extent
needed to produce sur-vival differences or are likely to do soin
the future. Taken together, this sug-gests that contemporary women
maysustain the morbidity of ALND with-out any meaningful
improvement insurvival rates. Limitations of the study,such as
failure to achieve target ac-crual and possible randomization
im-balance favoring theSLND-alone group,
must be considered. However, even inhigh-risk women (ER/PR) in
Z0011,preliminary analysis suggests no effectof elimination of ALND
on survival.
Despite limitationsof the Z0011 trial,its findingscould
haveimportant impli-cations for clinical practice. Examina-tion
oftheregionalnodes with SLNDcanidentify
hematoxylin-eosindetectedme-
tastases thatwould indicate a higher riskforsystemic disease
andtheneed forsys-temic therapy to reduce that risk. Re-sults from
Z0011 indicate that womenwith a positive SLN and clinical
T1-T2tumors undergoing lumpectomywith ra-
diation therapy followed by systemictherapy do not benefit from
the addi-tion of ALND in terms of local control,disease-free
survival, or overall sur-vival. The only additional
informationgained from ALND is the number ofnodes containing
metastases. This prog-nostic information is unlikelyto
changesystemic therapy decisions and is ob-tained at the cost of a
significant in-crease in morbidity.10 The only ratio-nale for ALND
in these patients wouldbe if the finding of additional nodal
me-tastases would result in changes in sys-
temic therapy. Because current guide-lines do not support
differences inadjuvant systemic therapy based on thenumber of
positive lymph nodes, ex-cept in some uncommon select sub-groups,40
ALND does not appear to bewarranted in this patient population.
The Z0011 trial did not include pa-tients undergoing mastectomy,
thoseundergoing lumpectomy without ra-diotherapy, those treated
with partial-breast irradiation, those receiving neo-adjuvant
therapy, and those receiving
whole-breast irradiation in the proneposition, in which the low
axilla is nottreated. In those patients, ALND re-mains standard
practice when SLNDidentifies a positive SLN. However,ALND may no
longer be justified forwomen who have clinical T1-T2 breastcancer
and hem ato xy l i n- eosi ndetected metastasis in the SLNand
whoare treated with breast-conserving sur-gery, whole-breast
irradiation, and ad-juvant systemic therapy. Implementa-tion of
this practice change would
improve clinical outcomes in thou-sands of women each year by
reduc-ing the complications associated withALND and improving
quality of lifewith no diminution in survival.
Author Contributions: Dr Giuliano had full access toallof
thedata in thestudyand takes responsibility forthe integrity of the
data and the accuracy of the dataanalysis.Study concept and design:
Giuliano.
SENTINEL NODE DISSECTION IN INVASIVE BREAST CANCER
574 JAMA, February 9, 2011Vol 305, No. 6 (Reprinted) 2011
American Medical Association. All rights reserved.
-
7/30/2019 Axillary Dissection vs No Axillary Dissection in Women
With Invasive Breast Cancer and Sentinel Node Metastasis (
7/7
Acquisition of data: Giuliano, Beitsch, Whitworth,Blumencranz,
Leitch, Saha, Morrow.Analysis and interpretation of data: Giuliano,
Hunt,Ballman, Whitworth, Leitch, McCall, Morrow.Draftingof
themanuscript:Giuliano, Ballman,Beitsch,Whitworth, Morrow.Critical
revision of the manuscript for importantintellectual
content:Giuliano, Hunt, Ballman,Beitsch,Whitworth, Blumencranz,
Leitch, Saha, McCall,
Morrow.Statistical analysis: Ballman,
McCall.Administrative,technical, or material support:Giuliano,Hunt,
Whitworth, Leitch, Saha.Study supervision: Giuliano,
Whitworth.Conflictof InterestDisclosures: All authorshave
com-pleted and submitted the ICMJE Form for Disclosureof Potential
Conflicts of Interest and none were re-ported.Funding/Support: This
study was supported by Na-tional Cancer Institute grant U10 CA
76001 to theAmerican College of Surgeons Oncology
Group(ACOSOG).Roleof theSponsor: TheNational CancerInstitute hadno
role in the design and conduct of the study; thecollection,
analysis, and interpretation of the data; orthe preparation,
review, or approval of the manu-script.Additional Contributions: We
thank the ACOSOGstaff,in particularthe leadership of Heidi Nelson,
MD(MayoClinic, Rochester, Minnesota), DavidOta,
MD(DukeUniversity,Durham,North Carolina),and SamuelA. Wells Jr, MD
(NationalCancer Institute, Bethesda,Maryland). All 3 of these
individuals contributed tostudy design, manuscript review, or both;
none re-ceived compensation for their contributions. We alsothank
all of the investigators and their site researchteams. Lastly,we
wishto thank thebravepatients withbreast cancer who participated in
this study and theircaregivers.
REFERENCES
1. Halsted WS. The results of radical operations forthe cure of
carcinoma of the breast. Ann Surg. 1907;46(1):1-19.2. Fisher B,
Wolmark N, Bauer M, Redmond C,GebhardtM. Theaccuracyof
clinicalnodalstaging and
of limited axillary dissection as a determinant of his-tologic
nodal status in carcinoma of the breast. SurgGynecol Obstet.
1981;152(6):765-772.3. GraversenHP, Blichert-Toft M, Andersen JA,
ZedelerK. Breast cancer: risk of axillary recurrence in
node-negative patients following partial dissection of theaxilla.
Eur J Surg Oncol. 1988;14(5):407-412.4. Fisher B, Jeong JH,
Anderson S, Bryant J, FisherER, Wolmark N. Twenty-five-year
follow-upof a ran-domized trialcomparingradical mastectomy,
totalmas-tectomy, and total mastectomy followed by irradiation.N
Engl J Med. 2002;347(8):567-575.5. Orr RK. The impact of
prophylactic axillary nodedissection on breast cancer survivala
Bayesianmeta-analysis. Ann Surg Oncol. 1999;6(1):109-116.6. Clarke
M,CollinsR, DarbyS, etal; EarlyBreastCan-cer
TrialistsCollaborativeGroup (EBCTCG).Effectsofradiotherapy and of
differences in the extent of sur-gery for early breast cancer on
local recurrence and15-year survival: an overviewof
therandomisedtrials.Lancet. 2005;366(9503):2087-2106.7. Yeoh EK,
Denham JW, Davies SA, Spittle MF. Pri-mary breast cancer:
complications of axillarymanagement. Acta Radiol Oncol.
1986;25(2):105-108.8. Lotze MT,Duncan MA,GerberLH, Woltering
EA,Rosenberg SA. Early versus delayed shouldermotion following
axillary dissection: a randomizedprospective study. Ann Surg.
1981;193(3):288-295.
9. Ivens D, Hoe AL, Podd TJ, Hamilton CR, Taylor I,Royle GT.
Assessment of morbidity from completeaxillary dissection. Br J
Cancer. 1992;66(1):136-138.10. Lucci A, McCall LM, Beitsch PD, et
al; AmericanCollege of Surgeons Oncology Group. Surgical
com-plicationsassociated with sentinel lymphnode dissec-tion (SLND)
plus axillary lymph node dissection com-pared with SLND alone in
the American College of
Surgeons Oncology Group trial Z0011. J Clin
Oncol.2007;25(24):3657-3663.11. Lyman GH, Giuliano AE, Somerfield
MR, et al;American Society of Clinical Oncology. American So-ciety
of Clinical Oncology guideline recommenda-tions for sentinel lymph
node biopsy in early-stagebreast cancer. J Clin Oncol.
2005;23(30):7703-7720.12. Fidler IJ. The pathogenesis of cancer
metastasis:the seed and soil hypothesis revisited. Nat RevCancer.
2003;3(6):453-458.13. AbramsJS. Adjuvant therapy forbreast
cancerresults from the USA consensus conference. BreastCancer.
2001;8(4):298-304.14. Goldhirsch A, Glick JH, Gelber RD, Senn HJ.
Meet-ing highlights: International Consensus Panel on theTreatment
of PrimaryBreast Cancer.J Natl Cancer
Inst.1998;90(21):1601-1608.15. Srlie T, Perou CM, Tibshirani R, et
al. Gene ex-
pression patterns of breast carcinomas distinguishtu-mor
subclasseswith clinical implications. ProcNatl AcadSci U S A.
2001;98(19):10869-10874.16. van de Vijver MJ, He YD, vant Veer LJ,
et al. Agene-expression signature as a predictor of survivalin
breast cancer. N Engl J Med. 2002;347(25):1999-2009.17. Albain KS,
Barlow WE, Shak S, et al; Breast Can-cerIntergroup of North
America. Prognosticand pre-dictive value of the 21-gene recurrence
score assayin postmenopausal women with node-positive,
oes-trogen-receptor-positive breast cancer on chemo-therapy:a
retrospectiveanalysis of a randomised trial.Lancet Oncol.
2010;11(1):55-65.18. Paik S,TangG, Shak S, etal. Gene
expressionandbenefit of chemotherapy in women with node-negative,
estrogen receptor-positive breast cancer.J Clin Oncol.
2006;24(23):3726-3734.19. Swedish Organised Service Screening
Evaluation
Group. Effectof mammographic service screeningonstage at
presentation of breast cancers in Sweden.Cancer.
2007;109(11):2205-2212.20. Fisher B, Montague E, Redmond C, et al.
Com-parison of radical mastectomy with alternativetreatments for
primary breast cancer: a first reportof results from a prospective
randomized clinicaltrial. Cancer. 1977;39(6)(suppl):2827-2839.21.
Rutgers EJ. Sentinel node biopsy: interpretationandmanagementof
patientswith immunohistochem-istry -po sit iv e se n tin e l n o d
e s a n d th o se withmicrometastases. J Clin Oncol.
2008;26(5):698-702.22. van laParra RF,ErnstMF, Bevilacqua JL,et al.
Vali-dation of a nomogram to predict the risk of nonsen-tinel lymph
node metastases in breast cancer pa-tients with a positive sentinel
node biopsy: validationof the MSKCC breast nomogram. Ann Surg
Oncol.2009;16(5):1128-1135.23. Amanti C, Lombardi A, Maggi S, et
al. Is com-plete axillary dissection necessaryfor all patients
withpositive findings on sentinel lymphnode biopsy? vali-dation of
a breast cancer nomogramfor predicting thelikelihood of a
non-sentinel lymphnode. Tumori. 2009;95(2):153-155.24. Coutant C,
Olivier C, Lambaudie E, et al. Com-parison of models to predict
nonsentinel lymph nodestatus in breast cancer patients with
metastatic sen-tinel lymph nodes: a prospective multicenter study.J
Clin Oncol. 2009;27(17):2800-2808.25. RescignoJ, Zampell
JC,AxelrodD. Patternsof ax-
illary surgical care for breast cancer in the era of sen-tinel
lymph node biopsy. Ann Surg Oncol. 2009;16(3):687-696.26. Fisher B,
Redmond C, Poisson R, et al. Eight-year results of a randomized
clinical trial comparingtotal mastectomy and lumpectomy with or
withoutirradiation in the treatment of breast cancer. N Engl JMed.
1989;320(13):822-828.27. Early Breast Cancer TrialistsCollaborative
Group.
Systemic treatment of early breast cancer by hor-monal,
cytotoxic, or immune therapy: 133 ran-domised trialsinvolving31,000
recurrences and24,000deaths among 75,000 women. Lancet.
1992;339(8785):71-85.28. Early Breast Cancer TrialistsCollaborative
Group.Systemic treatment of early breast cancer by hor-monal,
cytotoxic, or immune therapy: 133 ran-domised trialsinvolving31,000
recurrences and24,000deaths among 75,000 women. Lancet.
1992;339(8784):1-15.29. Rubinstein LV,Gail MH,SantnerTJ.
Planningtheduration of a comparative clinical trial with loss to
fol-low-up and a period of continued observation.J Chronic Dis.
1981;34(9-10):469-479.30. Kaji AH, Lewis RJ. Are we looking for
superior-ity, equivalence, or noninferiority? asking the
rightquestion and answering it correctly.
AnnEmergMed.2010;55(5):408-411.
31. Giuliano AE, McCall L, Beitsch P, et al. Locore-gional
recurrence after sentinel lymph node dissec-tionwith or without
axillary dissectionin patientswithsentinel lymph node metastases:
the American Col-lege of Surgeons Oncology Group Z0011 random-ized
trial. Ann Surg. 2010;252(3):426-433.32. FleissigA, Fallowfield LJ,
Langridge CI, et al. Post-operative arm morbidity and quality of
life: results ofthe ALMANAC randomised trial comparing sentinelnode
biopsy with standard axillary treatment in themanagement of
patients with early breast cancer.Breast Cancer Res Treat.
2006;95(3):279-293.33. Veronesi U, Paganelli G, Viale G, et al. A
ran-domized comparison of sentinel-nodebiopsy with rou-tine
axillary dissection in breast cancer. N EnglJ
Med.2003;349(6):546-553.34. Veronesi U, Orecchia R, Zurrida S, et
al. Avoid-ing axillary dissection in breast cancer surgery: a
ran-domizedtrial to assess therole of axillaryradiotherapy.
Ann Oncol. 2005;16(3):383-388.35. Martelli G, Boracchi P, De
Palo M, et al. A ran-domized trial comparing axillary dissection to
no ax-illary dissection in older patients withT1N0 breast
can-cer:results after 5 years of follow-up. AnnSurg.
2005;242(1):1-9.36. Rudenstam CM, Zahrieh D, Forbes JF, et al;
In-ternational Breast Cancer Study Group. Randomizedtrial comparing
axillary clearance versus no axillaryclearancein older patients
with breastcancer: first re-sults of International BreastCancer
Study Group Trial10-93. J Clin Oncol. 2006;24(3):337-344.37.
GrecoM, Agresti R, Cascinelli N, et al.Breast can-cer patients
treated without axillary surgery: clinicalimplications and biologic
analysis. Ann Surg. 2000;232(1):1-7.38. Martelli G, Miceli R,
Daidone MG, et al. Axillarydissection versus no axillary dissection
in elderly pa-tientswith breast cancer and no palpable axillary
nodes:results after 15 years of follow-up [published onlineahead of
print July 23,2010]. AnnSurgOncol.
2010.doi:10.1245/s10434-010-1217-7.39. Veronesi U, Viale G,
Paganelli G, et al. Sentinellymph node biopsy in breast cancer:
ten-year resultsof a randomized controlled study. Ann Surg.
2010;251(4):595-600.40. Goldhirsch A, Ingle JN, Gelber RD, Coates
AS,Thrlimann B, Senn HJ; Panel Members. Thresholdsfortherapies:
highlightsof theSt GallenInternationalExpert Consensuson the
primary therapyof earlybreastcancer 2009. Ann Oncol.
2009;20(8):1319-1329.
SENTINEL NODE DISSECTION IN INVASIVE BREAST CANCER
2011 American Medical Association. All rights reserved.
(Reprinted) JAMA, February 9, 2011Vol 305, No. 6 575