Embed Size (px)
Citation preview

TECHNICAL NOTE
Awake stereotactic brainstem biopsy via a contralateral, transfrontal,transventricular approach
E. A. C. PEREIRA, T. JEGAN, A. L. GREEN & T. Z. AZIZ
Oxford Functional Neurosurgery, Department of Neurological Surgery, John Radcliffe Hospital, Oxford, UK
AbstractThe authors describe a novel approach to stereotactic biopsy of lesions of the lateral pons and medial cerebellar peduncle,and its diagnostic success without morbidity. A contralateral approach laterally expands the accessible infratentorial area. Itmay also confer a theoretical reduction in neurological deficit with passage through non-dominant right hemisphere.
Key words: Brainstem tumour, contralateral transventricular approach, stereotactic biopsy.
Clinical details
A 70-year-old right-handed man collapsed at home,
losing consciousness for 10 min. History revealed 2
months of right-sided weakness. Examination of the
oriented patient demonstrated bilateral horizontal
nystagmus, left lower facial nerve paresis, right-sided
hemiparesis (power 4/5), pronator drift, brisk reflexes
and an upward right plantar. Dysphagia to solids,
and subsequent aspiration pneumonia, were mana-
ged by intravenous antibiotics and nasogastric feed-
ing. Dexamethasone was not commenced as the
patient remained orientated and a diagnosis of
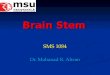
lymphoma had not been excluded. Magnetic reso-
nance imaging (MRI) showed extensive diffuse T2
high signal in the left pons, cerebral and middle
cerebellar peduncles, and some medullary extension
and fourth ventricle distortion without hydrocepha-
lus and minimal gadolinium enhancement (Fig. 1).
Single-voxel proton magnetic resonance spectro-
scopy (MRS) indicated markedly elevated choline
and decreased N-acetyl aspartate levels. A provi-
sional radiological diagnosis of diffuse low-grade
astrocytoma was made.
Informed patient consent was obtained to biopsy
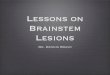
the lesion and gain diagnostic histology. Stereotactic
surgery was planned using a Cosman–Roberts–Wells
base ring, 1-mm slice stereotactic CT and Radionics
Stereoplan1 software (Fig. 2). A contralateral arc
was chosen and collar setting enabling entry at
the coronal suture. A 2.7-mm twistdrill craniostomy
was performed after subgaleal bupivicaine with
epinephrine infiltration and stab incision. With the
patient awake throughout the procedure, a 2-mm
diameter Radionics Nashold1 biopsy needle with 10-
mm side window was slowly passed to target. The
patient was conversant throughout 1 h with the base-
ring attached and 20 min procedure duration,
reporting no pain, or alteration in visual or facial
function. A single cannula pass was conducted and
three significant tissue samples obtained by aspira-
tion from each of four quadrants. After slow biopsy
needle withdrawal without subjective deficits, the
scalp was closed by single layer suture. Urgent frozen
section and subsequent histology confirmed diffuse
low-grade astrocytoma. The patient complained of
horizontal diplopia in the first few postoperative
hours; this resolved with commencement of dexa-
methasone and he remained mobile with improve-
ment of his pneumonia during the first postoperative
week. Further oncological management was arranged
including palliative radiotherapy (30 Gy in 10
fractions).
Discussion
Brainstem lesions comprise only 2% of all brain
tumours in adults with very variable pathology, in
contrast to children where they account for up to
15% of brain tumours with diagnoses often made by
MRI alone. In adults, preoperative radiological
diagnosis is incorrect in one in five cases and
histology desirable, frequently changing both man-
agement and prognosis. In general, the majority of
Correspondence: Dr E. A. C. Pereira, Oxford Functional Neurosurgery, Department of Neurological Surgery, West Wing, John Radcliffe Hospital, Oxford,
OX3 9DU, UK. Tel: þ44 (0) 1865 741166. Fax: þ44 (0) 1865 231885. E-mail: [email protected]
Received for publication 3 April 2008. Accepted 21 May 2008.
British Journal of Neurosurgery, August 2008; 22(4): 599 – 601
ISSN 0268-8697 print/ISSN 1360-046X online ª The Neurosurgical Foundation
DOI: 10.1080/02688690802220387
Br
J N
euro
surg
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/29/
14Fo
r pe
rson
al u
se o
nly.

adult brainstem tumours are not amenable to
surgical resection, making stereotactic biopsy an
attractive procedure for obtaining pathological tissue.
Stereotactic biopsy of brainstem lesions has been
performed for four decades with high diagnostic and
low complication rates. Its utility has been demon-
strated in non-enhancing diffuse astrocytomas as half
of those presumed to be low grade on MRI have been
high grade at biopsy.1 Proton MRS can be technically
limited at the skull base due to artefact from adjacent
tissues. Our experience of awake brainstem biopsies
is without operative mortality and with transient
neurological sequelae in 10% of patients, all of which
resolved either on cannula movement or within a few
hours of surgery.2 Our rationale is that biopsy-related
morbidity is reduced by keeping the patient awake
during the procedure, monitoring them clinically for
subjective reports of altered perception and assessing
them for weakness. Furthermore, reports of facial
paraesthesia, diplopia or oscillopia confirm anatomi-
cal localization. However, we have not had cause to
stop surgery due to intraoperative morbidity detected
by subjective reports from the awake patient.
The stereotactic approach to brainstem lesions is
traditionally ipsilateral and either transfrontal trans-
cortical, suboccipital transcerebellar or transtent-
orial. The transtentorial approach is now hardly
used, as its path crosses vital vasculature and cranial
nerves, and may cause pain with effortful tentorial
puncture. The suboccipital route can cause patient
discomfort with dissection of overlying musculature,
and requires patient positioning that makes intuba-
tion and general anaesthesia often necessary. The
transfrontal approach with the patient reclined or
supine is therefore favoured for awake surgery;
however, the ipsilateral route becomes limited to
midline regions of pons and medulla by the tentorial
incisura. A contralateral, transfrontal, extraventricu-
lar approach to the lateral pons enabling a wider
infratentorial pathological area to be sampled without
tentorial limitation or puncture has been described in
six patients without morbidity or mortality.3
We have not experienced the theoretically in-
creased risks of haemorrhage and target shift in
traversing a lateral ventricle that are thought to justify
a solely extraventricular intraparenchymal approach
over a transventricular one. In this case, the
transventricular trajectory was felt to give the best
chance of obtaining multiple biopsies in a single pass
with target shift unlikely in the confined infratentorial
space around the pons A contralateral transventri-
cular route does not increase distance from cranial
insertion point to target unlike an extraventricular
route, although no significant correlation has been
described between needle tract length and morbidity.
In this case, a contralateral approach might theore-
tically also have reduced biopsy-related morbidity by
passage through the non-dominant right hemisphere,
FIG. 1. (A) Axial T2-MRI. (B) Gadolinium-enhanced coronal T1-MRI showing a diffuse left pontine space occupying lesion.
600 E. A. C. Pereira et al.
Br
J N
euro
surg
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/29/
14Fo
r pe
rson
al u
se o
nly.

although we would not limit the procedure to left
infratentorial lesions.
Declaration of interest: The authors report no
conflicts of interest. The authors alone are respon-
sible for the content and writing of the paper.
References
1 Samadani U, Stein S, Moonis G, Sonnad SS, Bonura P,
Judy KD. Stereotactic biopsy of brain stem masses: decision
analysis and literature review. Surg Neurol 2006;66:484–90;
discussion 491.
2 Shad A, Green A, Bojanic S, Aziz T. Awake stereotactic biopsy
of brain stem lesions: technique and results. Acta Neurochir
(Wien) 2005;147:47–9; discussion 49–50.
3 Amundson EW, McGirt MJ, Olivi A. A contralateral, trans-
frontal, extraventricular approach to stereotactic brain-
stem biopsy procedures. Technical note. J Neurosurg
2005;102: 565–70.
FIG. 2. Contralateral, transfrontal, transventricular trajectory to the lateral pons.
Contralateral transventricular awake brainstem biopsy 601
Br
J N
euro
surg
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
SUN
Y S
tate
Uni
vers
ity o
f N
ew Y
ork
at S
tony
Bro
ok o
n 10
/29/
14Fo
r pe
rson
al u
se o
nly.