Embed Size (px)
DESCRIPTION
fat soluble vitamins
Citation preview

AVITAMINOSIS – FAT SOLUBLE
VITAMINS


A fat soluble vitamin.
CHEMISTRYVitamin – D is a sterol, it contains steroid nucleus
(Cyclopentanoperhydrophenanthrene ring)
Vitamin – D function like a hormone
Also referred to as antirachtic vitamin.
Forms of vitamins
Vitamin D2 (ergocalciferol)
Vitamin D3 (Cholecalciferol)

CH3
Ergocalciferol and Cholecalciferol are sources for
vitamin D activity and are referred as provitamins


Active form: the active form of vitamin D is
1,25 – Dihydroxycholecalciferol and is also
called as calcitriol.
Both hydroxylase enzymes (of liver and
kidney) require cytochrome P450, NADPH
and molecular oxygen for hydroxylation
process
Storage25 – hydroxycholecalciferol is the major
storage and circulatory form of vitamin D


CALCIUM – PHOSPHOROUS HOMEOSTASIS

DAILY REQUIREMENTS

Children - 10 gm/day or 400 IU/day
Adults - 5 gm/day or 200 IU/day
Pregnency,lactation -10 gm/day or 400 IU/day
Above the age of 60 yrs - 600 IU /day
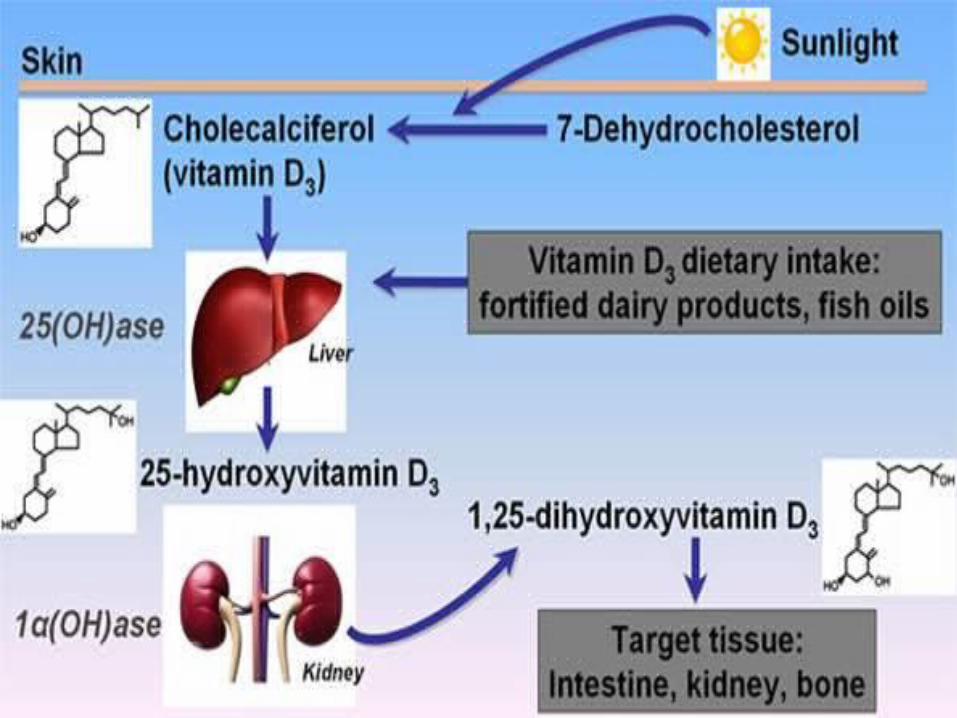
Sources of vitamin D:Exposure to sunlight produces cholecalciferol
Good sources includes – fatty fish, fish liver oils, egg yolk etc
Milk is a good source


Deficiency of vitamin D causes rickets in
children and osteomalacia in adults
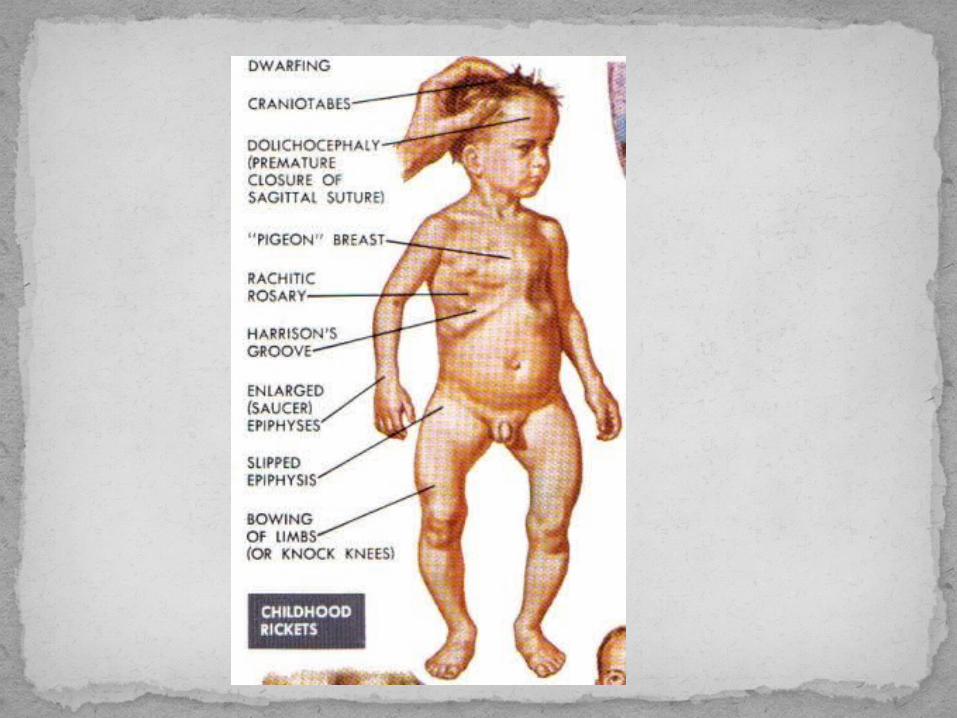
Rickets:
It is a vitamin D deficiency state in children
Causes: Dietary deficiency and non-
exposure to sunlight.



CLINICAL FEATURES

ORAL MANIFESTATIONS
Developmental abnormailities of dentin and enamel
Delayed eruptionMisalignment of teethHigh caries indexEnamel hypoplasiaEruption rate is retarded of both
deciduous and permanent teeth


Biochemical findings:
Decreased serum calcium (9-11mg/dl)Decreased plasma phosphorous (3-
4.5 mg/dl)Increased plasma alkaline
phosphatase (30-130 IU)

Also known as adult rickets
Bones affected – flat bones and diaphyses
of long bones
Etiology:
Inadequate exposure to sunlight
Low dietary intake
Malabsorption

RADIOGRAPHIC FEATURES
Asymmetric deformities of stress bearing bones.
Longitudinal hairline fractures.

Clinical Features: Female more affected than maleRemodelling of bones in absence of adequate calcium. Bowing of long bones may occur due to weight of the bodyFlattening of pelvis bones may cause difficulty during labour
ORAL MANIFESTATIONSPeriodontitis reported in women suffering from osteomalacia
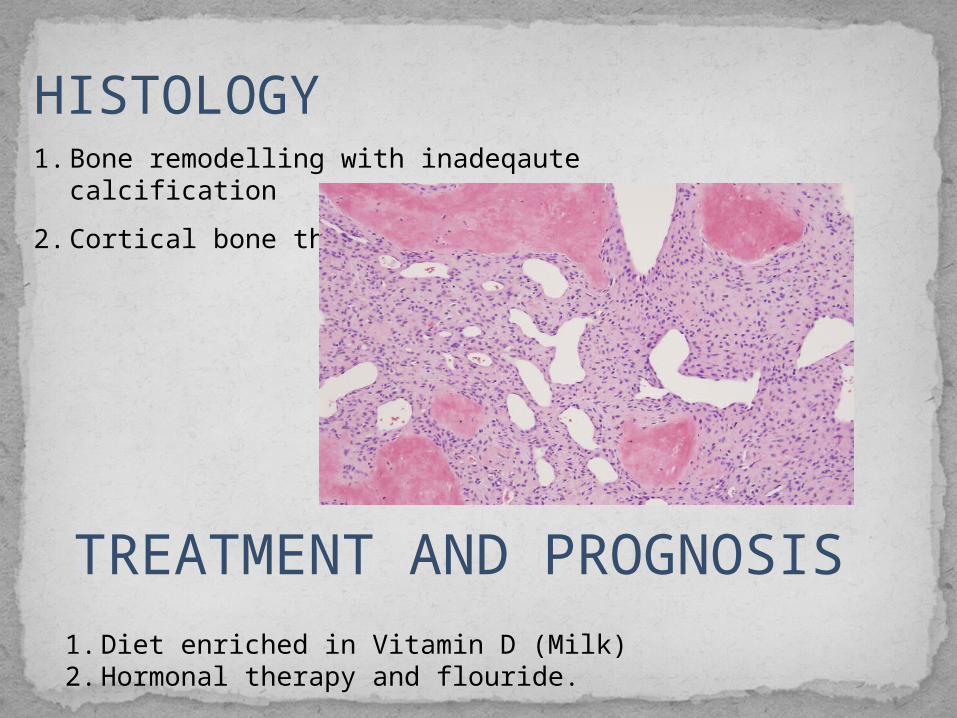
1. Diet enriched in Vitamin D (Milk)2. Hormonal therapy and flouride.
TREATMENT AND PROGNOSIS
HISTOLOGY1. Bone remodelling with inadeqaute calcification
2. Cortical bone thin.
Also known as Renal OsteodystrophyIn chronic renal failure, 1 α – hydroxylase
activity is decreased leading to decreased synthesis of 1,25 – DHCC
Painful crippling disease.TREATMENT AND PROGNOSISCondition is treated by giving 1,25 –
DHCC preparationsBut prognosis depends on the treatment
of underlying renal disease.

VITAMIN D RESISTANT RICKETS(FAMILIAL HYPOPHOSPHATSIA,
REFRACTORY RICKETS, PHOSPHATE DIABETES)
CHARACTERISED BY:1. Hypophostameia, hypophosphaturia 2. Familial ( x linked dominant)3. No response to vitamin D usual doses4. Decreased Ca and P absorption5. Dwarfism

CLINICAL FEATURES
DwarfismBowing of legsPseudofracturesSkull and sitting deformitiesMuscular weakness and atony may occur

ORAL MANIFESTATIONS
Formation of globular, hypocalcified dentinClefts in pulp horn regionWide root canal and pulp chambersPulp horns elongated and extending neat DEJ.Lamina dura absentAlveolar bone abnormal

High pulp horns and large pulp chambers are common in patients with x-linked hypophosphatemic dominant rickets


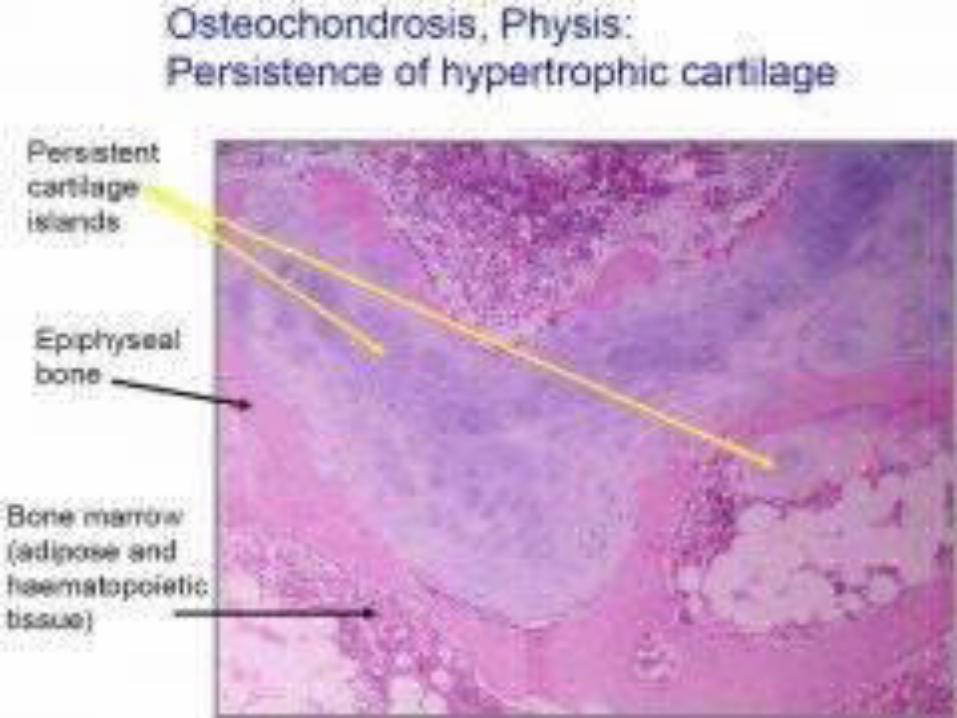
HISTOLOGICAL FEATURES
Cartilage plate and shaft of long bones altered
Failure of bone salt depositionRachitic metaphysis- Broad zone between cartilage cells and shaft.

TREATMENT AND PROGNOSIS
1. High Doses of vitamin D (50,000 – 100,000 IU)
2. 25- hydroxycholecalciferol in lower doses more successful (10,000 – 25,000 IU) in combination with oral phosphate administration.
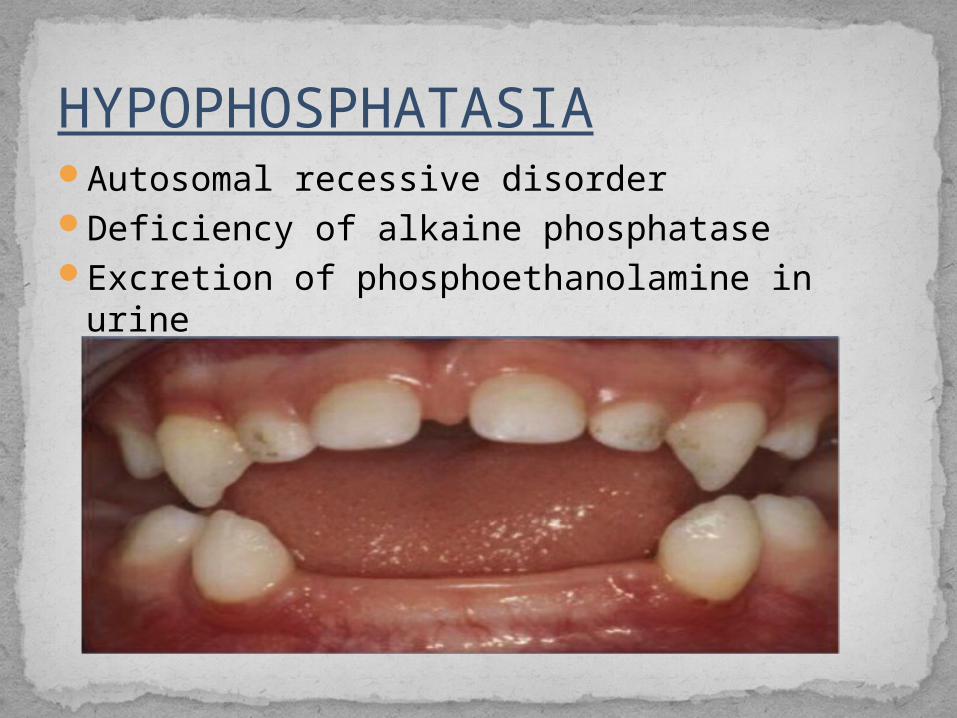
HYPOPHOSPHATASIAAutosomal recessive disorderDeficiency of alkaine phosphataseExcretion of phosphoethanolamine in urine

CLINICAL FEATURES
BASED ON CLINICAL FEAUTURES, It is of three clinical forms
1. INFANTILE – severe rickets, hypercalcemia and death
2. CHILDHOOD – increased infection, growth retardation, rachitic rosary. Pulmonary, GI tract and renal disorders also present
3. ADULT – spontaneous feactures
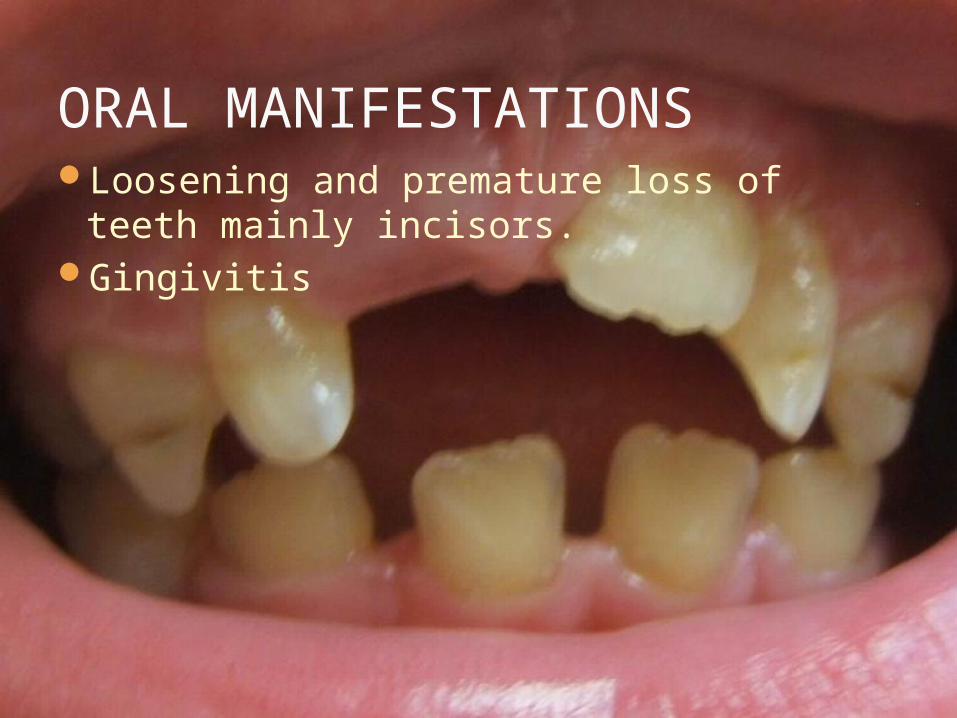
ORAL MANIFESTATIONSLoosening and premature loss of teeth
mainly incisors.Gingivitis
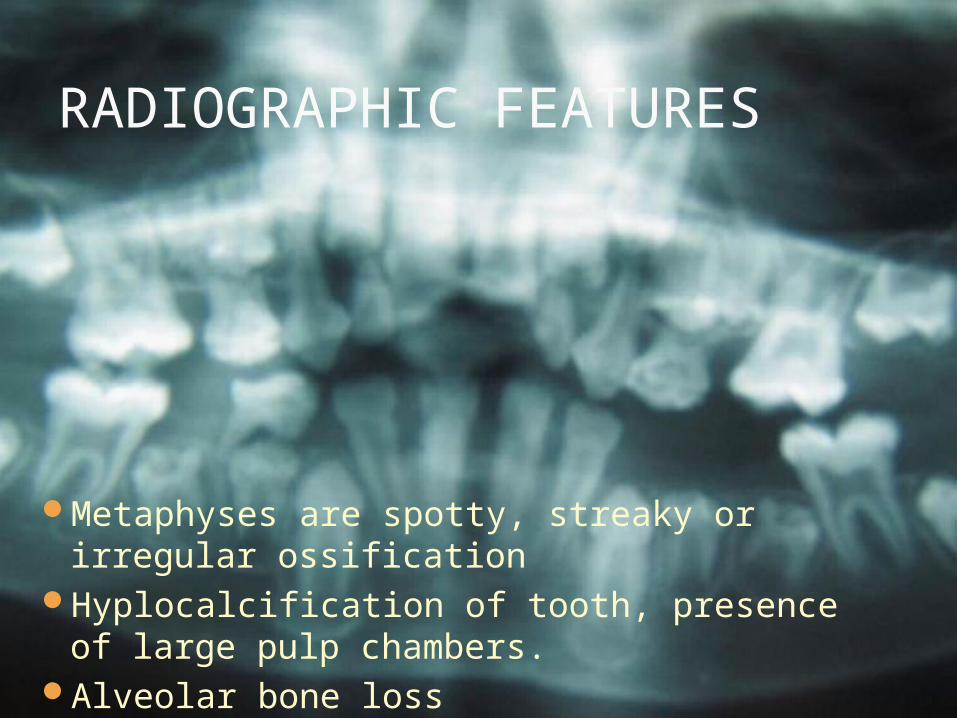
RADIOGRAPHIC FEATURES
Metaphyses are spotty, streaky or irregular ossification
Hyplocalcification of tooth, presence of large pulp chambers.
Alveolar bone loss

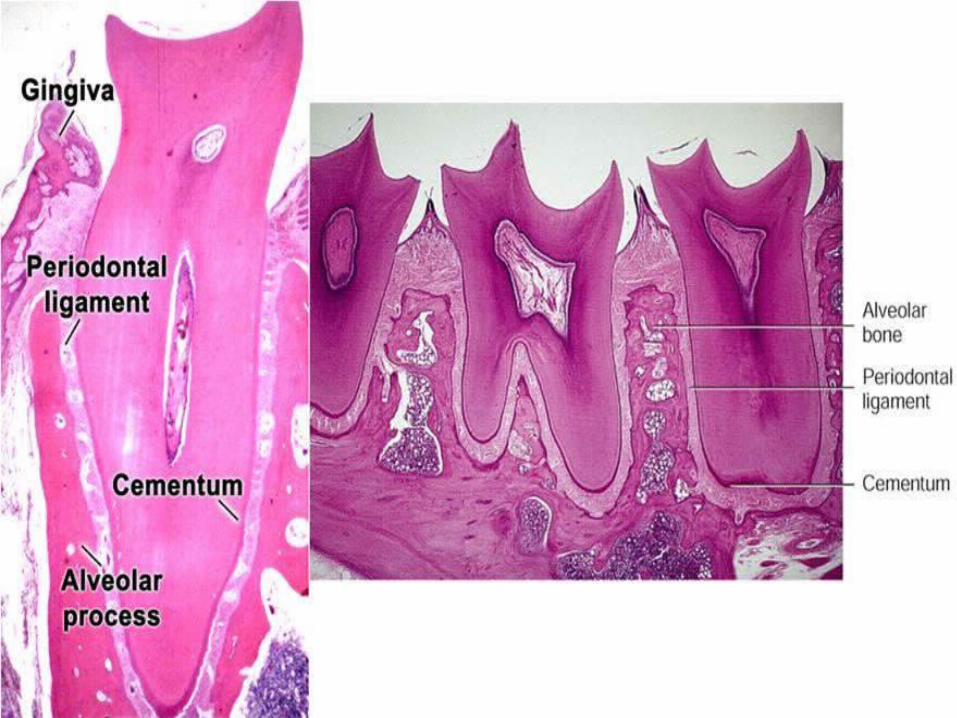
HISTOLOGYIncrease width of cartilage with widening
of hypertrophic cell zonePenetration of cartilage by marrowLarge amount of inadequately calcified
osteoid .Absence of cementum or some poorly
formed cementum.
TREATMENT
Partial improvement by high doses of vitamin D
Moderate improvement by oral dosinf of phosphate
Prognosis not good.

PSEUDOHYPOPHOSPHATASIA
Similar to hypophosphatasia but with normal serum alkaline phosphatase
Osteopathy of long bones and skullExfoliation of decidous teethHypercalcemiaPhosphoethanolaminuria
Vitamin D is stored mainly in liver
Vitamin D is most toxic in overdoses
Toxic effects include demineralization of bones and
increased calcium absorption from intestine,
leading increased plasma calcium (hypercalcemia)
Hypercalcemia is associated with deposition of
calcium in many soft tissues such as kidney and
arteries
It leads to formation of stones (renal calculi)
High consumption is associated with loss of
appetite, nausea, increased thirst, loss of weight etc

Calcitriol is considered as an important
calciotropic hormone, while cholecalciferol
is the prohormone
1. Vitamin D3 (cholecalciferol) is synthesized
in the skin by the UV – rays of sunlight
2. The biologically active form of vitamin D,
calcitriol is produced in the kidney
3. Calcitriol has target organs-intestine, bone
and kidney

4. Calcitriol action is similar to that of steroid
hormones
It binds to a receptor in the cytosol and the
complex acts on DNA to stimulate the
synthesis of calcium binding protein
5. Calcitriol synthesis is self-regulated by a
feedback mechanism i.e., calcitriol
decreases its own synthesis
6. Actinomycin D inhibits the action of calcitriol,
calcitriol exerts its effect on DNA leading to
the synthesis of RNA (transcription)









