Embed Size (px)
Citation preview

AVC : nouveautés thérapeutiques
Stroke: new therapies

L’édition de cet ouvrage a été rendue possible grâce à l’Institut Servier.This publication has been made possible through an educational grant from the Institut Servier.
L’éditeur ne pourra être tenu responsable de tout incident, tant aux personnes qu’aux biens, qui pourrait résulter soit de sa négligence, soit de l’utilisation de tous produits, méthodes, instructions ou idées décrits dans la publication. En raison de l’évolution rapide de la science médicale, l’éditeur recommande qu’une vérification intervienne pour les diagnostics et la posologie.The Publisher cannot be held responsible for any injury and/or damage to persons or property, which may result either from negligence or from the use or operation of any methods, products, instructions or ideas contained in the material herein. Because of the rapid advances in medical sciences, the Publisher recom mends that independent verification of diagnoses and drug dosages should be made.
© 2015 Springer Science + Business Media France Sarl. Tous droits réservés 22 Rue de Palestro75002 ParisFrance
Aucune partie de la présente publication ne peut être reproduite, diffusée ou enregistrée sous quelque forme ou par quelque moyen que ce soit, mécanique ou électronique, y compris par photocopie, enregistrement ou par des sys tèmes de stockage et de récupération de données, sans l’autorisation écrite de l’éditeur.No parts of this publication may be reproduced, transmitted or stored in any form or by any means, either mechanical or electronic, including photocopying, recording, or through an information storage and retrieval system, without the written permission of the publisher.
Impression : JouveImprimé en France
ISBN : 978-2-918172-11-6

Les colloques de L’Institut Servier
AVC : nouveautés thérapeutiques
Stroke: new therapies

Parus dans la même collection
La prévention et la protection dans la société du risque : le principe de précautionPrevention and protection in the risk society: the precautionary principle
ISBN : 2-84299-333-0
La recherche médicale à l’aube du XXIe siècle. Recherche médicale et modèle animalMedical research at the dawn of the 21st century. Medical research and animal models
ISBN : 2-84299-372-1
Vulnérabilité et vieillissement : comment les prévenir, les retarder ou les maîtriser ?Vulnerability and aging: can they be prevented, delayed or controlled?
ISBN : 2-84299-400-0
Le génome : avancées scientifiques et thérapeutiques et conséquences socialesThe genome: scientific and therapeutic developments and social consequences
ISBN : 2-84299-425-6
La révolution de la longévitéThe longevity revolution
ISBN : 2-84299-457-4
Le Cancer : nouvelles données, nouvelles stratégies, nouveaux espoirsCancer: recent evidence, innovative strategies, future hopes
ISBN : 2-84299-609-7
Ensemble face à la douleur. Prévention, traitement et prise en chargeUnited against pain. Prevention, treatment and management of pain
ISBN : 2-84299-705-0
L’obésité : un problème d’actualité, une question d’avenirObesity: an existing problem, a question for the future
ISBN : 2-84299-801-4
Actualités et perspectives en transplantationNews and prospects in transplantation
ISBN : 2-84299-942-1
Prévention de la dépendance fonctionnellePrevention of functional dependency
ISBN : 978-2-9528-747-8-6
Angiogenèse et anti-angiogenèseAngiogenesis and anti-angiogenesis
ISBN : 978-2-918172-24-6
La mémoireMemory
ISBN : 978-2-918172-52-9
Pharmacogénétique et pharmacogénomiquePharmacogenetics and pharmacogenomics
ISBN : 978-2-918172-03-1
Nanosciences en médecineNanosciences in medicine
ISBN : 978-2-918172-05-5
La SarcopénieSarcopenia
ISBN 978-2-918172-09-3
Vieillissement cutanéSkin ageing
ISBN 978-2-918172-10-9
La découverte et la vie

L’INSTITUT SERVIER
Fondateur : Docteur Jacques Servier
Délégué général : Madame Béatrice Guardiola
Comité scientifique
Président du Comité Scientifique : Professeur Pierre Godeau
Membres : Professeurs Michel Aubier, Jacques Barrat, Dominique Bellet, Jean-Pierre Bourdarias, Marie-Germaine Bousser, Jean-Marie Brogard, Bernard Devulder, Camille Francès, Jean-François Giudicelli, Philippe Grenier, Michel Haguenau, Pierre Lefebvre, Henri Lôo, Jean-Pierre Michel, Gérard Milhaud, Yves Pouliquen, Michel Safar, Jean-Paul Tillement, Richard Trèves, Yannis Tsouderos
La découverte et la vie
Life through Discovery

Auteurs
Pierre Godeau Président du Comité Scientifique de l’Institut Servier
Sonia Alamowitch Chef de Service de Neurologie et d’Urgences Neurovasculaires Hôpital Saint Antoine et Université Paris VI Pierre et Marie Curie Paris, France
Jean-François Pinel Service de Neurologie, CHU Pontchaillou Rennes, France
Christian Stapf Professeur de Neurologie Université Paris Diderot – Sorbonne Paris Cité
Unité Neurovasculaire et DHU Neurovasc Paris Sorbonne Service de Neurologie, APHP – Hôpital Lariboisière 2 rue Ambroise
Paré, 75475 Paris cedex 10, France Stroke Center / The Neurological Intitute Columbia University
Medical Center 710 West 168 Street, NI-615 New York, NY 10032, USA
Martin Ebinger Priv.-Doz. Dr. med. Dr. phil. Martin Ebinger Oberarzt der Klinik und Hochschulambulanz für Neurologie am
Campus Charité Mitte- Zusatzbezeichnung Notfallmedizin - Center for Stroke Research Berlin (CSB) Charité -
Universitätsmedizin Berlin | CCM Charitéplatz 1 | 10117 Berlin | Germany
François Proust Département de Neurochirurgie, Hôpital universitaire de Strasbourg, Strasbourg, France
Vianney Gilard, Département de Neurochirurgie, Hôpital universitaire de Rouen, Sophie Curey, Rouen, France Éléonore Tollard, Olivier Langlois
Isabelle Crassard Service de Neurologie, Hôpital Lariboisière, Paris, France
Philippe Marque Chef de Service de Médecine Physique et de Réadaptation, CHU Rangueil, Toulouse, France
Emmanuel Touzé Professeur de Neurologie et Inserm U919, Université de Caen Basse Normandie, CHU Côte de Nacre, Caen, France
France Woimant Service de Neurologie, Hôpital Lariboisière Paris, France
Sommaire
AVC : nouveautés thérapeutiques
Introduction : Les accidents vasculaires cérébrauxPierre Godeau ............................................................................................................ 13
Traiter l’ischémie cérébrale aiguëSonia Alamowitch ....................................................................................................... 17
AVC : nouveautés thérapeutiques : Après 20 ans de thrombolyse, quoi de neuf ?Jean-François Pinel .................................................................................................... 25
Traiter l’hémorragie cérébraleChristian Stapf ............................................................................................................ 38
Un scanner dans l’ambulance ? Thrombolyse pré-hospitalière et autres opportunitésMartin Ebinger ........................................................................................................... 45
Anévrisme rompu : clips ou microspires ?Vianney Gilard, Sophie Curey, Éléonore Tollard, Olivier Langlois, François Proust ........................................................................................................... 53
Traiter la thrombose veineuse cérébraleIsabelle Crassard ........................................................................................................ 65
Du nouveau en réhabilitation post-AVC ?Philippe Marque ......................................................................................................... 74
Prévenir l’infarctus cérébralEmmanuel Touzé ......................................................................................................... 84
Comment organiser le parcours de santé des patients victimes d’AVC ?France Woimant .......................................................................................................... 95


Contents
Stroke: new therapies
Introduction : Cerebrovascular accidentsPierre Godeau ............................................................................................................ 105
Treating acute cerebral ischaemiaSonia Alamowitch ....................................................................................................... 109
Stroke, new therapies: After twenty years of thrombolysis, what’s new?Jean-François Pinel .................................................................................................... 117
Treating Hemorrhagic strokeChristian Stapf ............................................................................................................ 130
A scanner in the ambulance? Prehospital thrombolysis and further opportunitiesMartin Ebinger ........................................................................................................... 136
Ruptured aneurysm: clips or coils?Vianney Gilard, Sophie Curey, Éléonore Tollard, Olivier Langlois, François Proust ........................................................................................................... 143
Treat cerebral venous thrombosisIsabelle Crassard ........................................................................................................ 154
What’s new in post-stroke rehabilitation?Philippe Marque ......................................................................................................... 163
Preventing cerebral infarctionEmmanuel Touzé ......................................................................................................... 173
Organising health care pathways for stroke victimsFrance Woimant .......................................................................................................... 183
AVC : nouveautés thérapeutiques

13
AVC : nouveautés thérapeutiquesStroke: new therapies© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
Les accidents vasculaires cérébraux
Pierre Godeau
Consacrer un colloque aux accidents vasculaires cérébraux (AVC) s’inscrit légitimement dans la continuité des travaux de L’Institut Servier. En effet, la majo-rité des thèmes retenus dans les années récentes concerne l’étude des conséquences du vieillissement et les AVC sont d’autant plus fréquents que l’on avance en âge. Avec une incidence annuelle de 150 000 cas en France, une prévalence d’environ 500 000 cas, les AVC posent un problème de Santé Publique de la plus haute impor-tance. En effet, leur fréquente gravité comportant un risque létal et celui de séquelles plus ou moins lourdes pouvant conduire à un handicap et à un état de dépendance fonctionnelle avec le spectre d’un séjour définitif en milieu hospitalier, représente pour la Société une charge financière considérable.
On ne peut négliger, d’autre part, le risque individuel de déficit intellectuel, voire de démence dans les années suivant un AVC, même en apparence peu sévère, et la fréquence d’état dépressif réactionnel avec le bouleversement de l’équilibre familial qui en résulte.
En regard de tous les paramètres conditionnant une évolution très variable d’un sujet à l’autre, il est rassurant de constater une amélioration importante du pronostic global reposant sur une prise en charge à la fois plus rapide et mieux adaptée, notamment dans le cadre des unités de soins spécialisées « Unités d’Urgences Neurovasculaires » ou « Stroke Units » et d’autre part d’une rééducation mieux conduite pour limiter les séquelles. Cependant, le « maillage » du territoire hexagonal reste trop irrégulier et trop lâche et les problèmes logistiques d’accès aux soins sont loin d’être résolus.
Une évaluation exacte des solutions à appliquer présuppose une classification précise des AVC comme l’a envisagé Marie-Germaine Bousser qui a été la cheville ouvrière de l’organisation de cette journée, retenant comme l’indique le titre : un AVC ou des AVC. Elle nous a rappelé qu’on pouvait classer les AVC en 5 catégories, schématiquement : 5 % d’hémorragies méningées, 15 % d’hémorragies cérébrales, 0,5 % de thromboses veineuses cérébrales et 78 % d’accidents ischémiques transi-toires (AIT) et d’infarctus cérébraux ces deux états, malgré la discordance de leur évolution, étant regroupés logiquement car représentant un continuum et procédant d’une prise en charge urgente et spécifique.
Certes, il n’est guère possible dans le cadre d’une journée d’épuiser le sujet des AVC et des aspects particuliers ont été volontairement exclus de notre programme. Tel a

Pierre Godeau
14
été le cas de la conduite à tenir en présence d’un AVC embolique, embol paradoxal par « patent foramen ovale » chez un sujet jeune. Longtemps objet de controverse, les cardiologues étant volontiers interventionnistes et les neurologues réservés. En effet, trois études prospectives avaient conclu à l’inutilité de l’occlusion de cette commu-nication interauriculaire. En réalité, le problème est en voie de solution depuis la fin 2013 où deux études multicentriques avec méta-analyse : l’une française [1] com-portant 1 224 patients versus 1 226 témoins traités médicalement et l’autre améri-caine [2] portant sur 1 150 patients traités versus 1 143 témoins après randomisation ont abouti aux même conclusions : les études précédentes manquaient de puissance et le nombre restreint d’accidents évolutifs ne permettait pas de conclusions valables. En revanche, les deux études récentes apportent la preuve statistique de l’efficacité de la fermeture par voie percutanée du PFO avec une réduction d’environ 1/3 du risque de récidive. Toutefois une légère augmentation du risque de fibrillation auriculaire a été objectivée dans les deux études, les conséquences n’en sont pas négligeables. C’est pourquoi l’étude française « close » se poursuit et permettra, nous l’espérons, d’aboutir à des recommandations précises dans les mois à venir.
Ceci nous conduit à quelques considérations générales sur les progrès en méde-cine et la communication interdisciplinaire. En cette année 2014 où l’on célèbre le centenaire de la guerre de 1914, il n’est pas inutile de revenir sur le concept de « balkanisation » de la médecine qui avait paru désuet et incompréhensible pour les jeunes générations mais remis au goût du jour. Ce vocable imagé mettait en vedette l’émiettement de la médecine en multiples spécialités concurrentes – ce qui n’est pas un défaut – mais parfois hostiles et repliées sur leur territoire restreint. Cette attitude est à distinguer de la subdivision de chaque spécialité d’organes conduisant à un approfondissement indispensable des connaissances et une adaptation idéale des multiples techniques modernes à un domaine de plus en plus étroit, phénomène irréversible et condition essentielle de progrès. Parallèlement, le retour à une globali-sation de la médecine s’avère indispensable et non pas opposé mais complémentaire de l’hyperspécialisation. C’est ainsi que la meilleure prise en charge des AVC relève autant des progrès de la prévention et de la suppression des facteurs de risque – ceux-ci ont été bien identifiés dans l’étude multicentrique interstroke [3], étude cas-contrôle réalisée dans 22 pays, les facteurs ne sont pas tout à fait les mêmes que ceux d’ordre cardiaque et coronariens évalués dans l’étude interheart. Quoiqu’il en soit, les progrès seront assurés par le développement de la diabétologie, le contrôle des erreurs métaboliques et diététiques, des hyperlipémies, de l’hypertension artérielle, des vasculopathies périphériques et coronaires, des maladies systémiques, la lutte contre le tabagisme et l’alcoolisme, des troubles du rythme cardiaque et du meilleur contrôle des troubles de l’hémostase en maintenant l’équilibre entre les risques de thrombose et d’hémorragie, ceci ne peut que faire l’objet d’une réflexion indivi-duelle et ne saurait alourdir inutilement le programme déjà chargé de ce symposium.

15
Les accidents vasculaires cérébraux
Rappelons simplement que la prise en charge de la fibrillation auriculaire permet-tra de réduire considérablement le risque des AVC de nature thromboembolique. Selon l’Ecole cardiologique de Bordeaux dont Michel Haissaguerre est le leader, la fibrillation auriculaire affecte 1 % de la population, soit 600 000 patients en France et 4 à 5 millions en Europe. Des chiffres même supérieurs, 750 000 en France ont été récemment rapportés par Jean-Marc Davy et coll au récent congrès de la Société de Cardiologie à Barcelone [4] avec une estimation de doublement de ce chiffre d’ici 2050. Si on admet que la FA est responsable de 20 % des AVC et que 30 % des patients en FA sont asymptomatiques, il est capital de sensibiliser les médecins généralistes à la détection de la FA et à solliciter un avis cardiologique au moindre doute. Sans perdre de vue les controverses sur les nouveaux anticoa-gulants qui s’atténueront lorsqu’on disposera en routine d’un contrôle biologique approprié, on peut évoquer le développement des techniques ablatives dont ont bénéficié 300 000 personnes en 2013 et dont les indications augmentent de façon exponentielles (plus de 20 % par an actuellement). Un autre procédé de prévention des AVC et des embolies périphériques liées à la fibrillation auriculaire consiste en l’occlusion de l’auricule gauche par un dispositif en nickel et titane qui se déploie comme un petit parapluie après introduction sous endoscopie trans-oesophagienne par voie transeptale. Ce dispositif Watchman a fait l’objet de l’étude prospective multicentrique américaine « PROTECT AF » dont le suivi à 3,8 années vient d’être publié aujourd’hui même dans le JAMA [5] et démontre sa supériorité vis-à-vis de la warfarine dans la fibrillation atriale non valvulaire.
Ces progrès qui devraient s’affirmer contribueront certainement à améliorer l’espérance de vie et particulièrement de vie en bonne santé, chère à notre ami Jean-Pierre Michel. Cependant, on ne doit pas oublier le risque croissant, mais pour le moment limité, d’AVC consécutifs à la prise de vaso-constricteurs – méphantamine d’usage heureusement limité, vaso-constricteurs nasaux d’intérêt thérapeutique incertain mais aux risques avérés, surtout prise de cocaïne qui multiplie par 6 ou 7 le risque d’AVC chez les patients de 15 à 49 ans comme l’ont signalé récemment nos confrères de Baltimore [6].
Mon propos est déjà trop long et il est temps de laisser la place à Marie-Germaine Bousser qui va évoquer rapidement le programme de cette journée avant de céder la place à Michel Haguenau qui va modérer cette matinée, Marie-Germaine lui succèdera cet après-midi et tirera in fine les conclusions de ce colloque qui sera certainement riche d’enseignements.
References
1 Beygui F, Labombarda F, Sabatier R, et al. A meta-analysis of randomized trials comparing percutaneous closure of patent foramen ovale to medical therapy. ESC Congrès 2013; abstract 90273.

Pierre Godeau
16
2 Renfigo-Moreno P, et al. Patent foramen ovale transcatheter closure vs. medical therapy on recurrent vascular events: a systematic review and meta-analysis of randomized controlled trials. Eur Heart J 2013;34:3342-52.
3 O’Donnell MJ, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case control study. Lancet 2010;376:112-23.
4 Davy JM, et al. The French screening campaign of atrial fibrillation in general practice assessment of predictive criteria for atrial fibrillation. ESC Congress, Barcelona 2014; abstract 4876.
5 Reddy VY, Severt H, Halperin J, et al. Percutaneous left atrial appendage closure vs warfarin for atrial fibrillation – A randomized clinical trial. JAMA 2014;312(19):1988-98.
6 Cheng G(Y-C) et al. Illicit cocaine use and risk of ischemic stroke: the stroke prevention in young adults study. International Stroke Conference, 12-14 February 2014; abstract.

17
AVC : nouveautés thérapeutiquesStroke: new therapies© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
Traiter l’ischémie cérébrale aiguë
Sonia Alamowitch (Paris)
1995 : daTe de naissance de la Thrombolyse
C’est en 1995 qu’une étude publiée par le National Institute of Neurological Disorders and Stroke (NINDS) a établi la preuve du bénéfice de la thrombolyse intraveineuse (IV) par l’activateur tissulaire recombinant du plasminogène (rt-PA) dans le traitement de phase aiguë de l’infarctus cérébral. Par rapport aux patients ayant reçu le placebo, les patients traités rt-PA en IV dans les 3 heures suivant la survenue des symptômes d’accident vasculaire cérébral (AVC) avaient environ 30 % de chances de plus de récupérer sans séquelles à 3 mois. [1]
Environ 10 ans plus tard, l’étude ECASS 3 a montré que la thrombolyse IV était efficace dans une fenêtre horaire un peu plus large, allant jusqu’à 4h30 après les premiers symptômes. [2]
PhysioPaThologie des infarcTus cérébraux : la zone de Pénombre ischémique
Les deux études citées ci-dessus ont montré que le facteur temps est un élément crucial dans l’efficacité de la thrombolyse IV. L’AVC ischémique est un phénomène dynamique. L’occlusion artérielle et le défaut d’irrigation sanguine qui s’en suit sont responsables de la souffrance du tissu cérébral dans le territoire du vaisseau concerné. Au centre de ce territoire, l’ischémie cérébrale conduit rapidement à une nécrose et à une perte de fonction irréversible. Il subsiste autour de cette lésion une zone dite de « pénombre ischémique » qui se trouve en état de sidération fonction-nelle durant quelques heures, pouvant évoluer vers la nécrose, mais restant viable si la perfusion est restaurée à temps. L’objectif de l’intervention thérapeutique est donc de tenter de reperfuser la zone d’ischémie en obtenant une désocclusion artérielle et, ainsi, de sauver la zone de pénombre ischémique. Plus cette intervention sera précoce, meilleures seront les chances de succès.

Sonia Alamowitch
18
Time is brain
Une méta-analyse portant sur près de 6 000 patients a été publiée en 2014. Elle confirme que la thrombolyse IV est efficace jusqu’à 4h30 après la survenue des symptômes d’ischémie cérébrale, mais que son bénéfice diminue au fil du temps. Ainsi, lorsque le traitement est instauré dans les 90 minutes qui suivent l’instal-lation des symptômes, il faut traiter quatre patients pour obtenir une récupération neurologique, alors qu’il faut en traiter 14 si le traitement est instauré entre 3 heures et 4h30 après. Au-delà de 4h30, le traitement n’a pas démontré son efficacité (cf. figure 1). [3]
La thrombolyse doit donc être instaurée le plus vite possible. C’est le concept du time is brain. Cet impératif a des implications majeures dans l’organisation de la prise en charge de toute suspicion d’infarctus cérébral. L’alerte thrombolyse suppose la mobilisation de toute la chaîne des secours pour accélérer au maximum la prise en charge pré et per-hospitalière des patients.
Parce que chaque minute compte, les patients doivent être adressés directement en Unité spécialisée (unité neuro-vasculaire, UNV) pour une évaluation clinique rapide par une équipe expérimentée en neurovasculaire. Ils doivent avoir une imagerie céré-brale en urgence qui va permettre d’affirmer le diagnostic, de vérifier qu’il n’existe pas de contre-indication, et ainsi, d’identifier les patients qui pourront bénéficier
1,00
0,8
1,0
1,2
1,5
1,6
1,8
2,0
2,2
2,4
2,6
2,8
3,0
1,5 2,0 2,5 3,0 3,5 4,0 4,5 5,0 5,5 6,0 6,5
Odd
s ra
tio
(95
% C
I)
Délai de traitement (h)
Interaction: χ12 = 5,80 (p = 0,016)
4h30
OR ajustés (95 %CI)
NPT pour Rankin 0–1
0–1h301h31–3h
3h01–4h304h31–6h
491421
2,84 (1,75–4,60)1,52 (1,10–2,11) 1,32 (1.09–1,61)1,22 (0,96–1,54)
figure 1. Effet du délai de traitement par l’alteplase sur l’évolution de l’AVC. [3]NPT : nombre de personnes à traiter.
19
Traiter l’ischémie cérébrale aiguë
du traitement. L’objectif est de parvenir à un délai de moins d’une heure entre l’arrivée du patient à l’hôpital et la thrombolyse IV (le temps « porte-seringue »). Cette véritable course contre la montre suppose une articulation étroite entre les services pré-hospitaliers qui vont adresser les patients (Samu) et l’équipe experte en neurovasculaire.
D’importants efforts d’organisation intra-hospitalière et de coordination avec les services de radiologie et d’urgences restent nécessaires. Ainsi, une étude américaine parue en 2011 ayant porté sur 25 504 patients victimes d’AVC ischémiques aigus traités par rt-PA entre 2003 et 2009 a montré que le temps porte-seringue était infé-rieur ou égal à 60 minutes dans seulement 26,6 % des cas. L’évolution était toutefois favorable puisqu’en 2003, ils n’étaient que 19,5 % contre 29,1 % en 2009. [4]
améliorer l’accès au TraiTemenT
raccourcir le délai de traitement
Il importe que les patients arrivent le plus tôt possible à l’hôpital. Dans cette pers-pective, ils doivent être capables d’identifier les symptômes d’AVC, et c’est tout le sens des campagnes d’alerte actuellement menées avec le message « vous ressentez brutalement une faiblesse d’un côté du corps, composez vite le 15 ». Cette injonc-tion suppose que le secteur pré-hospitalier (Samu, pompiers sur la région parisienne) soit en mesure d’identifier ces patients et de les adresser directement aux unités neurovasculaires. Certains centres en France expérimentent la téléthrombolyse : le malade est pris en charge en service d’urgences sans UNV tandis qu’un expert neurovasculaire sur un autre site l’évalue aux plans neurologique (téléconsulation) et radiologique (télé-transfert d’image) ; le cas échéant, il donne son feu vert pour la thrombolyse, sans perte de temps dans l’administration du traitement.
reconsidérer certaines contre-indications
Alors que l’AMM européenne du rt-PA pour l’infarctus cérébral aigu date de 2002, 5 % seulement des AVC bénéficient de ce traitement qui est le seul ayant démontré une efficacité en phase aiguë. Un des grands enjeux pour les années à venir sera de parvenir à augmenter ce pourcentage.
Une piste majeure d’amélioration serait de reconsidérer les contre-indications au rt-PA. Initialement, un grand nombre de patients a été exclu du traitement en raison de la crainte soulevée par le risque d’hémorragie cérébrale.
Avec un recul de 20 ans, et après la publication de nombreuses données, il apparaît que certaines de ces contre-indications ne sont pas pertinentes et que les reconsidérer pourrait porter à 20 % la population pouvant bénéficier du traitement. [5-8]

Sonia Alamowitch
20
Patients âgés de plus de 80 ans
La thrombolyse n’est pas indiquée dans l’AMM chez les patients âgés de plus de 80 ans alors qu’ils comptent pour plus de 30 % des AVC. Ces patients ont été exclus des essais thérapeutiques initiaux en raison d’un risque d’hémorragie cérébrale plus important dans cette population avec les traitements antithrombotiques. L’essai thé-rapeutique randomisé IST3 (International Stroke Trial) comparant l’injection IV de rt-PA contre placebo incluait 3 035 patients dont 1617 de plus de 80 ans. Il a montré que le bénéfice était significativement plus important chez les plus de 80 ans traités dans les 3 heures suivant l’installation des symptômes (p = 0,027). [9]
Dans les guidelines américaines, la thrombolyse IV n’est plus contre-indiquée avant 3 heures chez les plus de 80 ans [10] et cela devrait également être le cas en Europe d’ici peu de temps. Il est préconisé d’être prudent dans la deuxième partie de la fenêtre horaire, entre 3h et 4h30 (contre-indication relative) et de prendre en considération les autres contre-indications relatives.
Amélioration rapide de la symptomatologie ou symptômes modérés
Trente pour cent des patients avec infarctus cérébral et amélioration spontanée de leur état dans les heures qui suivent l’installation des symptômes ou présentant des symptômes modérés ont un handicap résiduel significatif à 3 mois (mRankin ≥ 2). Le risque de dégradation secondaire est particulièrement élevé en cas de persistance de l’occlusion artérielle car elle va être à l’origine d’une altération définitive de la zone de pénombre ischémique. [11-13]
Ainsi, s’il existe une occlusion artérielle, le traitement par rt-PA doit être instauré même en cas de NIHSS ≤ 4 ou d’amélioration spontanée des symptômes.
Indication de la thrombolyse IV : un patient sur deux dans une zone grise
Un excellent article publié en 2013 dans Brain soulignait qu’un quart des patients avec infarctus cérébral en phase hyper-aiguë a une indication indiscutable à la thrombolyse alors que celle-ci est contre-indiquée chez un autre quart. Un patient sur deux se situe donc dans une « zone grise » dans laquelle il va falloir évaluer la balance bénéfice/risque de saignement en fonction de l’étude en IRM-ARM du tandem état du parenchyme cérébral/perméabilité vasculaire.
La liste des contre-indications classiques de la thrombolyse rétrécit au fil du temps et les dix suivantes devraient être révisées :
– patients âgés de plus de 80 ans et de moins de18 ans, – femmes enceintes, – crise d’épilepsie au début de l’AVC, – déficit sévère (NIHSS > 25) sans infarctus étendu sur l’IRM cérébrale, – déficit mineur ou en cours d’amélioration avec occlusion artérielle à l’imagerie, – diabète et antécédent d’AVC,

21
Traiter l’ischémie cérébrale aiguë
– infarctus cérébral semi-récent de petite taille, – anévrisme intracrânien asymptomatique de petite taille, – traitement antivitamine K et INR < 1,7, – infarctus cérébral du réveil après horodatage de l’infarctus en IRM. [14]
les limites de la thrombolyse
La thrombolyse IV n’est pas efficace dans toutes les situations. Il est fréquent qu’elle ne permette pas une désobstruction durable en cas d’occlusion d’une artère de gros et moyen calibre, notamment du tronc basilaire, du segment M1 de l’artère cérébrale moyenne ou de la carotide interne. Dans ces situations, on observe un échec de la désocclusion ou une désocclusion initiale qui sera suivie d’une réocclusion dans 34 % des cas. [15]
La désocclusion artérielle peut être alors réalisée en allant directement, au cours d’une artériographie (neuroradiologie interventionnelle), au contact du caillot intra-artériel. Une thrombolyse chimique et/ou une thrombectomie mécanique intra-artérielles pourront alors être réalisées. Les systèmes de désobstruction méca-nique font appel soit à la thrombo-aspiration, soit au retrait mécanique de caillots par stents retriever. La stratégie thérapeutique privilégiée actuellement, appelée « Bridging therapy », consiste à débuter par une thrombolyse IV suivie d’un geste de désocclusion artérielle. Cette approche séduisante a fait l’objet d’études compa-ratives randomisées vis-à-vis de la thrombolyse IV. [16-18] Dans un premier temps, celles-ci ont montré que le traitement de désocclusion endovasculaire ne faisait pas mieux que la thrombolyse IV mais, en 2014, l’essai randomisé CLEAN a apporté des arguments pour valider cette stratégie thérapeutique. Dans cette étude menée aux Pays-Bas, le traitement standard (rt-PA IV) était comparé à un traitement combiné thrombolyse IV + désocclusion intra-artérielle chez 500 patients bien sélectionnés et traités très précocement (< 6h). Ses résultats montrent un bénéfice clinique très net pour le traitement combiné (OR : 1,65 ; IC 95 % : 1,21–1,30). Il faut souligner que le délai médian de thrombectomie, remarquablement court, n’était que de 4h30. [19, 20] Les résultats de plusieurs autres essais thérapeutiques sont attendus pour 2015.
les auTres TraiTemenTs de l’infarcTus cérébral en Phase aiguë
les anticoagulants
Les anticoagulants ont été en vogue il y a plus de 30 ans dans cette indication, mais les essais thérapeutiques ont montré qu’ils n’apportaient pas de bénéfice en phase aiguë et qu’ils n’ont que de rares indications (niveau de preuve faible).
Sonia Alamowitch
22
les antiagrégants plaquettaires
Aspirine seule
Des études publiées il y a plus de 10 ans ont montré que l’aspirine en phase aiguë de l’infarctus cérébral réduit légèrement le risque de récidive dont on sait qu’il est élevé dans les premiers jours qui suivent un premier infarctus cérébral (OR : 0,77 ; IC 95 % : 0,69–0,87 ; p ≤ 0,05). [21]
Associations d’antiagrégants plaquettaires
Une méta-analyse de 12 essais randomisés incluant 3 766 patients a comparé l’aspi-rine seule aux associations aspirine + dipyridamole et aspirine + clopidogrel. Par rapport à l’aspirine seule, les associations d’antiagrégants plaquettaires réduisaient légèrement le risque de récidive (OR : 0,67 ; IC 95 % : 0,49–0,93). La bithérapie était associée à une augmentation non significative des saignements majeurs (OR : 2,09 ; IC 95 % : 0,86–5,06). [22]
Les associations d’antiagrégants plaquettaires pourraient être bénéfiques en traitement très précoce de l’accident ischémique transitoire (AIT) ou de l’infarctus cérébral mineur. Un essai mené en Chine, contrôlé, randomisé, en double aveugle, contre placebo, a inclus 5 170 patients ayant fait un infarctus mineur ou un AIT à haut risque dans les 24 heures. Ils ont reçu une association clopidogrel + aspirine (clopidogrel à la dose initiale de 300 mg, puis 75 mg par jour pendant 90 jours, + aspirine à la dose de 75 mg par jour pendant les 21 premiers jours) ou un placebo + aspirine (75 mg par jour pendant 90 jours). À 90 jours, l’association s’est révélée supérieure à l’aspirine seule pour la prévention des AVC (HR : 0,68 ; IC 95 % : 0,57–0,81 ; p < 0,001). Des hémorragies de modérées à sévères se sont produites chez 0,3 % des patients dans les deux groupes. [23]
Cette étude a donc l’intérêt de montrer que la bithérapie en phase aiguë fait mieux que la monothérapie en prévention de la récidive d’AVC avec un rapport bénéfice-risque favorable. Nous avons donc là une piste pour le traitement de phase aiguë des infarctus cérébraux mineurs ou des AIT. Cinq essais thérapeutiques comparant l’aspirine et des associations d’antiagrégants plaquettaires dans ces indications sont actuellement en cours.
conclusion
Grâce à la thrombolyse IV, « guérir » près de 40 % des patients avec infarctus cérébral en cours de constitution est maintenant possible. La thrombolyse IV doit être instaurée très précocement. L’enjeu pour les années à venir est de parvenir à traiter plus vite et un plus grand nombre de patients. Les traitements endovasculaires ouvrent des perspectives thérapeutiques intéressantes et constitueront probablement

23
Traiter l’ischémie cérébrale aiguë
demain une nouvelle arme dans l’arsenal thérapeutique de phase aiguë pour des patients sélectionnés. Enfin, les stratégies d’association d’antiagrégants plaquet-taires instaurées en phase aiguë dans les accidents ischémiques mineurs pourraient réduire le risque de survenue d’un infarctus cérébral.
bibliographie
1 The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995;333:1581-7.
2 Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med 2008;359:1317-29.
3 Emberson J, Lees KR, Lyden P, et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet 2014;384:1929-35.
4 Fonarow GC, Smith EE, Saver JL, et al. Timeliness of tissue-type plasminogen activator therapy in acute ischemic stroke: patient characteristics, hospital factors, and outcomes associated with door-to-needle times within 60 minutes. Circulation 2011;123:750-8.
5 De Keyser J1, Gdovinová Z, Uyttenboogaart M, Vroomen PC, Luijckx GJ. Intravenous alteplase for stroke: beyond the guidelines and in particular clinical situations. Stroke 2007;38:2612-18.
6 Tong D. Are all IV thrombolysis exclusion criteria necessary? Being SMART about evidence-based medicine. Neurology 2011;76:1780-1.
7 Demaerschalk BM. Challenging the validity of imposing contraindications to thrombolysis for acute ischemic stroke. Neurology 2011;77:1862-3.
8 Wardlaw JM, Murray V, Berge E, et al. Recombinant tissue plasminogen activator for acute ischaemic stroke: an updated systematic review and meta-analysis. Lancet 2012;379:2364-72.
9 IST-3 collaborative group, Sandercock P, Wardlaw JM, et al. The benefits and harms of intra-venous thrombolysis with recombinant tissue plasminogen activator within 6 h of acute ischae-mic stroke (the third international stroke trial [IST-3]): a randomised controlled trial. Lancet 2012;379:2352-63.
10 Jauch EC, Saver JL, Adams HP Jr, et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013;44:870-947.
11 Rajajee V, Kidwell C, Starkman S, et al. Early MRI and outcomes of untreated patients with mild or improving ischemic stroke. Neurology 2006;67:980-4.
12 Nedeltchev K, Schwegler B, Haefeli T, et al. Outcome of stroke with mild or rapidly improving symptoms. Stroke 2007;38:2531-5.
13 Smith WS, Schwab S. Advances in stroke: critical care and emergency medicine. Stroke 2012;43:308-9.
14 Balami JS, Hadley G, Sutherland BA, Karbalai H, Buchan AM. The exact science of stroke thrombolysis and the quiet art of patient selection. Brain 2013;136:3528-53.
15 Alexandrov AV, Grotta JC. Arterial reocclusion in stroke patients treated with intravenous tissue plasminogen activator. Neurology 2002;59:862-7.
16 Broderick JP, Palesch YY, Demchuk AM, et al. Endovascular therapy after intravenous t-PA versus t-PA alone for stroke. N Engl J Med 2013;368:893-903.
17 Paciaroni M, Inzitari D, Agnelli G, et al. Intravenous thrombolysis or endovascular therapy for acute ischemic stroke associated with cervical internal carotid artery occlusion: the ICARO-3 study. J Neurol 2014. [Epub ahead of print]
Sonia Alamowitch
24
18 Kidwell CS, Jahan R, Gornbein J, et al. A trial of imaging selection and endovascular treatment for ischemic stroke. N Engl J Med 2013;368:914-23.
19 Fransen PS, Beumer D, Berkhemer OA, et al. MR CLEAN, a multicenter randomized clinical trial of endovascular treatment for acute ischemic stroke in the Netherlands: study protocol for a randomized controlled trial. Trials 2014;15:343.
20 Berkhemer OA, Fransen PS, Beumer D, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med 2015;372:11-20.
21 Sandercock P, Gubitz G, Foley P, Counsell C. Antiplatelet therapy for acute ischaemic stroke. Cochrane Database Syst Rev 2003;(2):CD000029.
22 Geeganage CM, Diener HC, Algra A, et al. Dual or mono antiplatelet therapy for patients with acute ischemic stroke or transient ischemic attack: systematic review and meta-analysis of rando-mized controlled trials. Stroke 2012;43:1058-66.
23 Wang Y, Wang Y, Zhao X, et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. N Engl J Med 2013;369:11-19.

25
AVC : nouveautés thérapeutiquesStroke: new therapies© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
AVC : nouveautés thérapeutiques : Après 20 ans de thrombolyse, quoi de neuf ?
Jean-François Pinel (Rennes)
La science du passé est le meilleur passeport pour l’avenir.Christine de Suède (XVIIème siècle)
La thrombolyse intraveineuse ne saurait se résumer à l’injection d’ une dose de 0.9 mg/kg d’alteplase (ou rtPA, Recombinant tissue Plasminogen Activator) à des patients présentant un accident vasculaire cérébral ischémique datant de moins de 4 heures 30. L’arrivée de cette thérapeutique a profondément modifié non seule-ment la neurologie vasculaire mais l’ensemble des services de neurologie dans leur structure et leur fonctionnement ; l’impact s’est étendu aux centres d’appel, aux ambulanciers, aux services d’urgence et aux services de radiologie.
Pourtant, les recommandations ne sont pas identiques dans tous les pays et les pratiques individuelles sont loin d’être homogènes ; la littérature est abondante, mais les études sur lesquelles elle s’appuie font l’objet de critiques qui pourraient aller jusqu’à remettre en question le bien-fondé des indications de la thrombolyse IV. Certaines agences nationales et sociétés savantes se proposent d’ailleurs de revoir leurs positions.
Il nous faut revisiter le passé.
Le déVeLoppement de LA thromboLyse IV
Après presque 20 ans, depuis la publication décisive de l’étude du NINDS dans le New England Journal of Medicine en décembre 1995 [1], nous pouvons retracer l’histoire très particulière de cette innovation.
Dès les années 60 apparaissent quelques publications sur l’utilisation d’agents thrombolytiques dans le traitement de l’accident vasculaire cérébral ; en 1988, G. del Zoppo [2] compile huit études, dont la dernière de T. Abe [3] semble très prometteuse puisque sur 58 patients, 48 sont améliorés sans complication hémor-ragique et sans décès ; il s’agit d’une étude en double aveugle, multicentrique, sans limite d’âge, où l’inclusion se fait dans les 15 jours suivants l’événement ; le
Jean-François Pinel
26
traitement est fait d’urokinase à faible dose sur six jours ; l’évaluation se base sur un score d’amélioration globale à un mois… Nous sommes très loin de la méthodologie des études ultérieures. Mais, à l’époque, tout en considérant qu’il était prématuré d’utiliser ces agents pharmacologiques, plusieurs auteurs se montraient optimistes pour l’avenir (J.C. Grotta [4] ; M. A. Sloan [5]) en évoquant déjà l’utilisation du rtPA et la perspective de combiner à la thrombolyse des agents protecteurs. A ce jour, les études sur les agents protecteurs ont toutes été négatives.
Dans les années 90 plusieurs études d’envergure seront menées, certaines avec la streptokinase (MAST-I 1995 [6], ASK 1996 [7], MAST-E 1996 [8]) d’autres avec le rtPA ( ECASS 1995 [9], ECASS II 1998 [10]) ; globalement elles seront toutes négatives ; certes, des sous analyses post-hoc ont pu montrer des tendances favorables, mais au prix d’ «arrangements méthodologiques» (modification du but principal de l’analyse pour ECASS II), voire de conflits ouverts et de scission entre les investigateurs (2 présentations des résultats avec des conclusions divergentes pour MAST-I [11]).
En fait, la véritable révolution avait été publiée en 1993 par P. Langhorne ; il prouvait l’intérêt de développer des unités neurovasculaires (UNV), structures apportant un bénéfice certain à l’ensemble des patients pris en charge. Malgré des études validées, démontrant le bénéfice du regroupement des moyens médicaux et paramédicaux pour tous les AVC, c’est la thrombolyse, qui, bien que concernant un faible pourcentage de patients, a été l’argument de poids pour développer les filières conduisant aux «stroke units» ; la mise en place de ces unités qui bénéficient à l’ensemble des patients présentant un AVC, qu’il soit ou non ischémique, qu’il soit ou non thrombolysé, aurait été beaucoup plus difficile sans l’image porteuse du caillot à «dissoudre».
Peu d’avancées concernaient la prise en charge médicamenteuse des accidents vasculaires cérébraux ischémiques en aigu ; les études qui concluront à l’efficacité, certes modeste, de l’aspirine étaient en cours et ne seront publiées que 2 ans plus tard en 1997 (études IST [12]et CAST [13]) et seul l’intérêt d’une héparine de bas poids moléculaire prescrite dès les 48 premières heures [14] venait d’être publiée dans une étude sur 300 patients ; l’efficacité sur l’évolution à six mois n’a cependant pas été confirmée par la suite.
C’est donc avec enthousiasme que la communauté médicale neurologique a accueilli l’étude du NINDS [1] montrant une efficacité, sur le pronostic fonctionnel à trois mois, du rtPA injecté dans les trois heures suivant la survenue de l’AVC.
Cependant, dès la publication, les critiques de fond ont été nombreuses : c’était la seule étude positive ; il y avait eu un changement de l’objectif principal après 291 inclusions ; on notait une absence d’efficacité sur les scores à 24 h et sur la mor-talité globale ; de plus, l’asymétrie des scores NIHSS à l’inclusion entre le groupe contrôle et le groupe traité pouvait expliquer à elle seule le résultat sur le score de

27
AVC : nouveautés thérapeutiques : Après 20 ans de thrombolyse, quoi de neuf ?
Rankin à 6 mois ; enfin, le «prix» à payer pour éviter 11 « morts ou dépendances » était de 6 hématomes intracrâniens et de 3 décès directement imputables au traite-ment, ces décès ne semblant pas toujours survenir chez les patients les plus graves. De plus, l’étude ne portait que sur 624 patients au total, alors que les cohortes de nos collègues cardiologues sur la thrombolyse étaient de 60 000 patients dans l’étude GISSI 2 dès 1990 [15] et de 41 000 patients dans l’étude GUSTO en1993 [16], étude qui comparait déjà les thrombolytiques entre eux.
Dans les années 1996 et 1997, plusieurs auteurs, respectés dans la communauté neurovasculaire, considéraient que la preuve permettant l’utilisation large de cette thérapeutique n’était pas apportée ; J van Gijn [17], tout en se réjouissant qu’on ait entrouvert une porte, trouvait qu’il était prématuré de conclure à la validité de la thrombolyse intraveineuse ; A. Furlan et G. Kanoti [18] affirmaient qu’il était trop tôt pour utiliser la thrombolyse intraveineuse en dehors d’études, et ce, malgré un avis favorable de la FDA ; L. Caplan et J.P. Mohr [19] jugeaient le traitement trop dangereux, sa mise en œuvre à grande échelle risquant d’entrainer trop de compli-cations, éventuellement mortelles pour un bénéfice seulement minime chez d’autres.
Pourtant, en Août 2000, les recommandations passaient d’un grade 2B à un grade 1 sans qu’il n’y ait eu d’études supplémentaires et alors que plusieurs publications remettaient de nouveau en cause les résultats de l’étude NINDS, reprenant en particu-lier le fait que le groupe placebo était initialement moins grave et que ce déséquilibre expliquait par lui-même les résultats de l’étude à trois mois. (Lenzer [20] ; Mann [21])
En 2002, dans le British Medical Journal, plusieurs auteurs (C. Warlow, J.M. Wardlaw [22] ; G.Trotter [23]) considéreront que ce qui est prouvé pour l’infarctus du myocarde ne l’est pas encore pour le cerveau, que le traitement devrait toujours être réservé à des patients très ciblés, que les bénéfices semblent avoir été exagérés dans la littérature et que d’autres études seraient nécessaires.
C’est dans ce climat que l’autorisation d’utilisation du rtPA dans les accidents vasculaires cérébraux ischémiques de moins de trois heures a été donnée en Europe en 2003. La Société Française Neurovasculaire avait émis ses recommandations [24] sur les résultats des méta-analyses : globalement « 14 morts ou dépendances » évi-tées tous les 100 patients traités ; certes, le risque d’hématomes intracrâniens (10 fois plus, dont 75 % mortels)et une «balance» d’un mort pour quatre bénéfices étaient reconnus, mais globalement, sous réserve de respecter les contre-indications et en particulier le délai de mise en œuvre du traitement, celui-ci devait être largement proposé sous la responsabilité d’une équipe formée.
Plusieurs séries furent alors publiées tentant de préciser les contre-indications, soulignant les risques en cas de violation de protocole [25, 26], s’interrogeant sur l’intérêt de former ou non des médecins urgentistes [27], et discutant déjà du cas spécifique du sujet âgé [28] ; ainsi, progressivement, la thrombolyse s’est dévelop-pée en France, conjointement à la mise en place des unités neurovasculaires.
Jean-François Pinel
28
Le très faible pourcentage de patients traités par la thrombolyse IV dans les 3 heures a justifié alors le déploiement d’une énergie considérable pour améliorer la phase préhospitalière, structurer la prise en charge en aigu dans les hôpitaux et revoir toutes les filières, ce dont a bénéficié l’ensemble des patients présentant un AVC, thrombolysé ou non. L’image même de la neurologie d’urgence et de la perception du neurologue s’est trouvée affectée par ces avancées ; deux références [29], dont l’une pastiche mimant la présentation d’un article du NEJM [30], resituent avec humour et bon sens la situation en 2002 et 2003 : «Thrombolysis for acute stroke has revolutionized the psychology of the specialty and this tendancy has impacted on other specialties. It remains to be seen if there is an equally beneficial effect on stroke patients. Until then, preventative treatment of hypertension, diabetes, and lifestyle modifications including smoking cessation and exercise are recommended both for neurologists and the general public”.
Le principal motif d’exclusion au traitement thrombolytique restait la limitation à trois heures ; les modèles laissaient penser que l’efficacité pourrait perdurer après injection plus tardive. L’étude ECASS III [31], publiée en 2008 a répondu à cette interrogation en montrant une efficacité sur le score de Rankin à 90 jours chez les patients traités entre 3 heures et 4 heures 30.
Puis, en 2012 une étude de grande envergure, IST-3 [32], pragmatique, internatio-nale, multicentrique, randomisée, en ouvert, portant sur 3 035 patients s’est attachée à savoir si nous pouvions étendre l’indication à tous les patients, quel que soit l’âge et ce jusqu’à six heures ; en fait, les patients, pour lesquels le médecin était convaincu de l’indication ou de la contre-indication, étaient exclus et seuls les patients pour lesquels existait un doute étaient inclus ; l’évaluation se faisait par l’équivalent d’une échelle de Rankin, en ouvert, le patient pouvant connaitre le traitement qu’il avait reçu ; les résultats, publiés en mai 2012, concluaient que la thrombolyse dans les six heures améliorait le pronostic fonctionnel et ce, quel que soit l’âge des patients ; in fine, 95 % des patients inclus n’étaient pas dans les critères d’indication approuvés dans la communauté européenne : 53 % étaient âgés de plus de 80 ans et 32 % avaient un score NIHSS supérieur ou égal à 16 (AVC graves). Le paradigme semblait dès lors s’inverser ; alors que jusqu’à présent le neurologue se posait en urgence la question de l’indication chez un patient présentant un accident vasculaire cérébral, la question devenait : quel patient ayant présenté un accident vasculaire cérébral ischémique de moins de six heures présente une contre-indication à la thrombolyse [33] ?
LA sItuAtIon ACtueLLe
Ces dernières années le nombre de publications sur le sujet a continué de croître, passant de 445 publications dans PubMed en 2010 à 572, 714, 846 les années sui-vantes et à plus de 900 en 2014. Si l’on tente de comparer les principaux sujets
29
AVC : nouveautés thérapeutiques : Après 20 ans de thrombolyse, quoi de neuf ?
abordés entre 2004 et 2014, on s’aperçoit que les aspects organisationnels sont toujours autant évoqués, que les articles traitant de l’imagerie sont moins fréquents et que de nouveaux sujets ont émergé en particulier l’association à un geste endo-vasculaire, le questionnement sur l’utilisation des thrombolytiques chez les patients sous anticoagulant oraux directs, la télémédecine… Les articles cliniques restent très présents : quel risque prend on à thrombolyser un patient dont le diagnostic d’accident vasculaire cérébral ischémique en aiguë est erroné [34-36] ? Y a-t-il des différences d’efficacité et de tolérance entre les patients caucasiens et les patients chinois [37, 38] ? Quelle est la sensibilité et la spécificité de l’I.R.M. à la phase aiguë [39] ? Quelle valeur accorder aux scores prédictifs de saignement intracrâ-nien [40] ? Doit-on thrombolyser les patients ayant un accident vasculaire peu invalidant [41] ? La thrombolyse a-t-elle un impact plus important sur les lésions de substance blanche ou sur celles de substance grise [42] ? L’imagerie peut-elle nous expliquer l’aggravation de certains patients malgré le traitement [43] ? Quelles sont les contre-indications relatives ou absolues, variables suivant les sociétés savantes et les pays [44] ?
Malgré 20 ans de recul et l’abondante littérature, force est de constater que l’atti-tude du neurologue dans ces situations particulières d’urgence reste très hétérogène. Une enquête réalisée en 2013 en Bretagne [45] interrogeant 30 neurologues exerçant en unité neurovasculaire à propos de 28 situations particulières (âge, terrain, sémio-logie, contre-indications relatives, particularités à l’I.R.M.) a montré un accord professionnel fort dans seulement 10 % des situations ; sur environ un tiers des cas il y avait une majorité relative, sur un autre tiers seules des tendances se dessinaient et pour le tiers restant la réponse thérapeutique était complètement aléatoire entre les praticiens. En fait, lors d’une thrombolyse, la crainte principale reste l’aggravation du patient par une hémorragie intracrânienne ; au décours du geste, on s’enquiert en premier lieu de la tolérance puis secondairement de l’efficacité éventuelle. Les modi-fications de pratique ont été insidieuses, souvent le fait d’expériences individuelles car les études rigoureuses ne peuvent se faire pour toutes les situations particulières : des contre-indications sont tombées car ne reflétant que les critères d’exclusion des études initiales, les critères neuroradiologiques des images au scanner (que la thrombolyse nous a appris à lire) se sont transformés en critères IRM différents, tout au moins pour les centres qui en bénéficient en urgence, ce qui participe également aux variations de pratique.
Pourtant, les recommandations des sociétés savantes sont régulièrement actua-lisées [46] et la Cochrane Library a publié des synthèses en 2000, 2003, 2009 et 2014 [47-50] ; ce dernier document de plus de 160 pages s’appuie sur 27 études portant elles-mêmes sur plus de 10 000 patients. Initialement, en 2000, la Cochrane Collaboration ne semblait pas convaincue dans ses conclusions par la thrombo-lyse intraveineuse, malgré l’étude NINDS publiée cinq ans auparavant. En 2014

Jean-François Pinel
30
la conclusion est plus tranchée : «le traitement thrombolytique donné dans les six heures après la survenue de l’accident vasculaire cérébral réduit la proportion de décès et de dépendance. Ce bénéfice est clair malgré l’augmentation des hémor-ragies intracrâniennes et des décès à 10 jours et aux évaluations finales. L’âge, les modifications au scanner ou la sévérité ne sont pas des contre-indications pour administrer le traitement en particulier dans les 4.5 premières heures».
Les questIons
Bien que bénéficiant d’une aide financière par le NHS, la Cochrane Collaboration précise que ses conclusions ne sont pas nécessairement celles de l’agence gouver-nementale ; ceci peut laisser penser que, malgré l’extrême rigueur méthodologique utilisée pour cette méta-analyse, il reste de la place pour des opinions plus nuancées.
Concernant l’extension de la fenêtre thérapeutique entre 3 heures et 4.5 heures suite à l’étude ECASS III, les controverses restent d’actualité ; une série d’articles parus dans Stroke en 2014 rappelle que la FDA n’a pas autorisé cette extension et qu’en l’absence de nouvelles études, assez peu probables, la question restera posée [51-53]. Parmi les interrogations sur cette étude, certains remarquent que le groupe placebo était un peu plus grave à l’entrée et que les patients de ce groupe avaient deux fois plus d’antécédents vasculaires cérébraux, que le pourcentage des hémor-ragies intracérébrales était particulièrement bas dans le groupe traité et que ceci était en partie dû à un changement spécifique de définition pour cette étude. Ces auteurs remarquent également qu’il s’agit de la seule étude positive, les autres, réalisées sur la même période montrant une surmortalité ayant conduit à leur interruption préma-turée ; un travail avec la desmoteplase [54], publié en 2009, cherchant également à étendre la fenêtre thérapeutique, a été négatif ; il a fait l’objet de beaucoup moins de commentaires et de diffusion n’étant retrouvé que 7 fois dans les titres de références ultérieures alors que l’étude ECASS III était citée 113 fois.
L’étude IST-3 [32] a fait l’objet de vives critiques et un article didactique [55], reprenant les interrogations méthodologiques qu’elle suscite lui a été consacré : description des biais, du principe de l’éligibilité sur l’incertitude, du passage d’une étude en double aveugle à une étude ouverte après 276 patients, de la définition d’un centre expérimenté s’il fait seulement plus de trois thrombolyses par an, de l’analyse ordinale faite secondairement changeant a posteriori le but principal de l’étude pour l’analyse, de la surmortalité lors des sept premiers jours pour cause «cérébrale» (p à 0.0001), des conflits d’intérêts éventuels.
D’autres opinions encore plus incisives, sinon virulentes, se retrouvent sur la toile [56, 57] ; souvent très argumentés, ces avis affirment qu’on ne doit pas conclure à une étude positive quand il n’y a pas de différence sur le critère principal prédéfini de «mort et dépendance» à six mois ; ils soulignent de plus que la méthodologie d’inclusion

31
AVC : nouveautés thérapeutiques : Après 20 ans de thrombolyse, quoi de neuf ?
aurait dû favoriser le traitement dans le bras thrombolyse (puisqu’étaient exclus les patients contre-indiqués par l’expertise du médecin) et qu’il n’est donc pas sérieux d’étendre les résultats à «tous» les patients dans la «vraie vie». De plus, l’absence de relation entre l’efficacité et le délai d’administration, remet très largement en cause les résultats de l’étude ECASS III, déjà très critiquée : de fait, les auteurs d’IST-3 [32] reconnaissent qu’entre 3 heures et 4h30, le traitement semble délétère…
Toutes ces interrogations à propos de l’étude ECASS III et surtout d’IST-3 conduisent à s’interroger sur la réalité même de l’efficacité de la thrombolyse intraveineuse [58] ; globalement sur les 12 études importantes, 6 ne montrent aucun bénéfice, 4 sont arrêtées prématurément pour effets délétères et 2, bien que déclarées positives, restent très discutables dans leur conclusion au vue de la méthodologie utilisée pour analyser les données [59].
Ainsi, les critiques de l’étude pivot du NINDS de 1995 reviennent au premier plan ; une analyse argumentée par de nombreux graphiques, reprenant l’ensemble des données sources, conclut presque 15 ans après … qu’il n’est pas possible de sta-tuer sur une efficacité de la thrombolyse IV dans les accidents vasculaires cérébraux ischémiques [60] .
R. Shinton dans le Lancet en août 2014 [61] analyse à nouveau l’étude NINDS et l’étude IST-3, reprend les critiques antérieures et conclut que la preuve du béné-fice de la thrombolyse reste très précaire et que si la prise en charge des accidents vasculaires cérébraux par les unités neurovasculaires est efficiente, les autorités de régulation doivent revoir l’ensemble du dossier du rtPA.
C’est ce que semble annoncer D. Cohen et H. Macdonald dans le British Médical Journal en septembre 2014 concernant l’agence de régulation britannique [62] ; dans une lettre de l’Internal Medecine Journal, en août 2014 [63], D. Fatovich rapporte que le collège américain des médecins urgentistes va revoir ses recommandations et que le collège australien de médecine d’urgence considère que la thrombolyse IV ne fait plus partie du traitement standard de l’accident vasculaire cérébral ischémique.
C’est dans ce contexte, avec ces incertitudes, qu’il nous faut prendre en charge nos patients : décision difficile ; C. Shamy [64], à propos d’une enquête auprès de 70 neurologues de la province de l’Ontario, montre le manque d’homogénéité des attitudes, ce qu’avait reflété notre petite étude en Bretagne ; curieusement dans notre étude le fait pour le praticien de croire en un rapport bénéfice/risque élevé ou faible ne changeait pas son taux d’indication dans les 28 situations proposées ; la décision médicale reste un art sinon mystérieux, du moins difficile.
ConCLusIon
Cet article s’est attaché à étudier les éventuels bénéfices directs de la thrombolyse intraveineuse, il faut reconnaître que l’existence de cette thérapeutique a été un

Jean-François Pinel
32
formidable moteur pour la prise en charge de tous les accidents vasculaires céré-braux : le développement des unités neurovasculaires avec un personnel dédié, la mise en place de filières d’amont et d’aval, la création de postes pour des médecins neurovasculaires, la mise en place de gardes et d’astreintes pour tous les patients neurologiques, le développement de la neuroradiologie avec des scanners et des
sous-groupe événement / nombre de patients rapport des cotes
ajusté (IC à 99 %)
Valeur de
p ajustée rt-PA Contrôle
Âge (ans) 0,029
≤ 80 331/698 (47,4%) 346/719 (48,1%) 0,92 (0,67–1,26)
> 80 223/817 (27,3%) 188/799 (23,5%) 1,35 (0,97–1,88)
score nIhss 0,003
0–5 221/304 (72,7%) 232/308 (75,3%) 0,85 (0,52–1,38)
6–14 276/728 (37,9%) 268/724 (37,0%) 1,08 (0,81–1,45)
15–24 50/402 (12,4%) 33/421 (7,8%) 1,73 (0,93–3,20)
≥ 25 7/81 (8,6%) 1/65 (1,5%) 7,43 (0,43–129,00)
probabilité prévue de mauvais résultats à six mois 0,009
< 0,4 256/351 (72,9%) 290/377 (76,9%) 0,81 (0,52–1,26)
0,4–0,5 88/169 (52,1%) 76/160 (47,5%) 1,20 (0,68–2,13)
0,5–0,75 127/361 (35,2%) 118/357 (33,1%) 1,10 (0,73–1,65)
> 0,75 83/634 (13,1%) 50/624 (8,0%) 1,73 (1,07–2,82)
délai jusqu’à la randomisation (h) 0,613
0–3 132/431 (30,6%) 95/418 (22,7%) 1,64 (1,03–2,62)
3–4,5 182/577 (31,5%) 226/600 (37,7%) 0,73 (0,50–1,07)
>4,5 240/507 (47,3 %) 213/500 (42,6%) 1,31 (0,89–1,93)
phase de l’étude 0,479
En aveugle 34/136 (25,0%) 38/140 (27,1%) 0,91 (0,42–1,98)
Ouverte 520/1379 (37,7%) 496/1378 (36,0%) 1,14 (0,89–1,45)
Centre disposant d’une expérience dans la thrombolyse 0,911
Non 313/940 (33,3%) 309/950 (32,5%) 1,10 (0,82–1,48)
Oui 241/575(41,9%) 225/568 (39,6%) 1,14 (0,78–1,66)
total 554/1515 (36,6%) 534/1518 (35,2%) 1,12 (0,89–1,41)
Figure 1. Etude IST-3. Effet du traitement sur le critère principal («en vie et indépendant», Oxford Handicap Score 0,1,2). Aucune significativité sur la population totale et les sous-groupes ; tendance non significative à l’aggravation chez les sujets de moins de 80 ans, les déficits mineurs, les patients traités entre 3 h et 4 h 30. [32]
0,4 1,0 3,0
En faveur du contrôle
En faveur du rt-PA
33
AVC : nouveautés thérapeutiques : Après 20 ans de thrombolyse, quoi de neuf ?
I.R.M. disponibles 24 heures sur 24, 7 jours sur 7, le développement de la neurora-diologie interventionnelle, l’impact sur l’enseignement et sur la recherche et enfin la perception de l’AVC dans la population… tout ceci est à verser en partie au crédit de la thrombolyse intraveineuse. En ce sens, l’impact positif de cette thérapeutique, qui, in fine, ne concerne toujours qu’une minorité d’AVC, a très largement dépassé le strict bénéfice des patients traités par alteplase.
Cette mise en perspective des publications passées ne saurait déboucher sur des recommandations médicales. Elle vise seulement à rappeler que notre objecti-vité est très relative et que la rigueur nécessaire au progrès de la science médicale n’exclut pas de s’interroger sur nos perceptions voire nos a priori. Concernant les accidents vasculaires cérébraux ischémiques, force est de reconnaitre la logique de la reperméabilisation en urgence du vaisseau thrombosé pour éviter l’extension de l’infarctus dans la zone de pénombre ; pour autant, il nous faut rester vigilant dans notre perception de la littérature et ne pas en faire des prophéties auto-réalisatrices ; nous devons osciller entre le strict respect de la méthodologie des études cliniques (coûteuses et difficiles à renouveler) et les analyses post-hoc pour extraire a pos-teriori des données. La démarche qui nous a conduit de l’étude NINDS en 1995, approuvant le traitement dans les 3 heures, à l’étude ECASS III étendant la fenêtre à 4.5 heures puis l’étude IST-3 voulant élargir cette fenêtre jusqu’à 6 heures pour tous les patients peut aussi se revisiter en remontant dans le temps… mais l’histoire
0 %
–40
–20
0
20
40
50 % 100 %
Aggravation
Cha
ngem
ent
à 90
jou
rs d
u N
IHSS
Placebo < 90 mn (n = 145)
tPA < 90 mn (n = 157)
Placebo 90–180 mn (n = 167)
tPA 90–180 mn (n = 155)
Amélioration
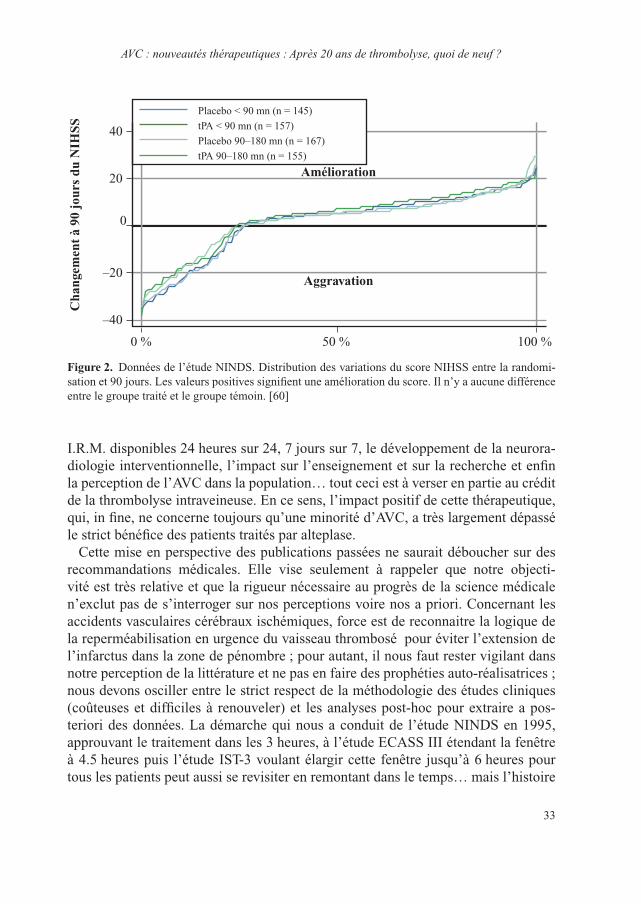
Figure 2. Données de l’étude NINDS. Distribution des variations du score NIHSS entre la randomi-sation et 90 jours. Les valeurs positives signifient une amélioration du score. Il n’y a aucune différence entre le groupe traité et le groupe témoin. [60]

Jean-François Pinel
34
avance et si le regard vers le passé est toujours riche d’enseignement, il n’est pas envisageable de remettre tout à plat et de revenir à la période d’avant 1995.
Quelques interrogations de fond subsistent : quand les méta-analyses ont peu de sens (méthodologies différentes, déséquilibre dans le nombre de patients entre les études…), quel poids donner aux études positives et négatives (NINDS, ECASS, DIAS 2) ? Peut-on occulter les modifications de protocoles en cours d’études (NINDS, IST-3) ? Devons-nous porter autant d’intérêt aux analyses statistiques post-hoc qui font basculer le résultat des études de négatif à positif (IST-3 ; Figure 1) ou de positif à négatif (NINDS ; Figure 2) ? Comment concilier les recommandations des Sociétés Savantes et des organismes nationaux de régula-tion quand, à partir de la même littérature, les avis ne concordent pas (extension à 4.5 heures de la thrombolyse IV) ?
A ces questions sans réponse simple, il faudrait ajouter la problématique majeure représentée par le passage des recommandations au traitement d’un patient donné, mais ce serait ouvrir un autre débat largement discuté dans la littérature. Enfin, les techniques évoluant et la thrombolyse intraveineuse ayant montré ses limites, les interrogations concernent maintenant le champ des thrombectomies mécaniques associées à la thrombolyse IV [65]…
Le bon sens a de l’avenir.
bibliographie
1 The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995;333(24):1581-7.
2 del Zoppo GJ. Investigational use of tPA in acute stroke. Ann Emerg Med 1988;17(11): 1196-201.
3 Abe T, Kazama M, Naito I. Clinical evaluation for efficacy of tissue culture urokinase (TCUK) on cerebral thrombosis by means of multicenter double-blind study. Blood Vessel 1981;12:321-41.
4 Grotta J. Can raising cerebral blood flow improve outcome after acute cerebral infarction? Stroke 1987;18:264-7.
5 Sloan MA. Thrombolysis and stroke. Past and future. Arch Neurol 1987;44(7):748-68.6 Italy (MAST-I) Group. Randomised controlled trial of streptokinase, aspirin, and combi-
nation of both in treatment of acute ischaemic stroke. Multicentre Acute Stroke Trial. Lancet 1995;346(8989):1509-14.
7 Donnan GA, et al. Streptokinase for acute ischemic stroke with relationship to time of administra-tion: Australian Streptokinase (ASK) Trial Study Group. JAMA 1996;276(12):961-6.
8 The Multicenter Acute Stroke Trial–Europe Study Group. Thrombolytic therapy with streptoki-nase in acute ischemic stroke. N Engl J Med 1996;335(3):145-50.
9 Hacke W, et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The European Cooperative Acute Stroke Study (ECASS). JAMA 1995;274 (13):1017-25.

35
AVC : nouveautés thérapeutiques : Après 20 ans de thrombolyse, quoi de neuf ?
10 Hacke W, et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian Acute Stroke Study Investigators. Lancet 1998;352(9136):1245-51.
11 Tognoni GR, Roncaglioni MC. Dissent: an alternative interpretation of MAST-I. Multicentre Acute Stroke Trial–Italy Group. Lancet 1995;346:1515.
12 International Stroke Trial Collaborative Group. The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke. Lancet 1997;349(9065):1569-81.
13 CAST (Chinese Acute Stroke Trial) Collaborative Group. CAST: randomised placebo-control-led trial of early aspirin use in 20,000 patients with acute ischaemic stroke. Lancet 1997;349 (9066):1641-9.
14 Kay R, et al. Low-molecular-weight heparin for the treatment of acute ischemic stroke. N Engl J Med 1995;333(24):1588-93.
15 Gruppo Italiano per lo Studio della Streptochinasi nell’Infarto Miocardico (GISSI). Effectiveness of intravenous thrombolytic treatment in acute myocardial infarction. Lancet 1986;1(8478): 397-402.
16 The GUSTO Investigators. An international randomized trial comparing four thrombolytic strate-gies for acute myocardial infarction. N Engl J Med 1993;329(10):673-82.
17 van Gijn J. Thrombolysis in ischemic stroke: double or quits? Circulation 1996;93(9):1616-17.18 Furlan AJ, Kanoti G. When is thrombolysis justified in patients with acute ischemic stroke? A
bioethical perspective. Stroke 1997;28(1):214-18.19 Caplan LR, et al. Should thrombolytic therapy be the first-line treatment for acute ischemic
stroke? Thrombolysis – not a panacea for ischemic stroke. N Engl J Med 1997;337(18):1309-10; discussion 1313.
20 Lenzer J. Alteplase for stroke: money and optimistic claims buttress the “brain attack” campaign. BMJ 2002;324(7339):723-9.
21 Mann J. Truths about the NINDS study: setting the record straight. West J Med 2002;176(3):192-4.22 Warlow C, Wardlaw J. Therapeutic thrombolysis for acute ischaemic stroke. BMJ 2003;326
(7383):233-4.23 Trotter G. Why were the benefits of tPA exaggerated? West J Med 2002; 176(3):194-7.24 Société française Neurovasculaire. Recommandations pour l’utilisation du thrombolytic treatment
intra-veineux dans l’accident ischémique cérébral. Rev Neurol 2000;156:1178-85.25 Albers GW, et al. Intravenous tissue-type plasminogen activator for treatment of acute stroke:
the Standard Treatment with Alteplase to Reverse Stroke (STARS) study. JAMA 2000;283(9): 1145-50.
26 Katzan IL, et al. Use of tissue-type plasminogen activator for acute ischemic stroke: the Cleveland area experience. JAMA 2000;283(9):1151-8.
27 Akins PT, et al. Can emergency department physicians safely and effectively initiate thrombolysis for acute ischemic stroke? Neurology 2000;55(12):1801-5.
28 Tanne D, et al. Intravenous tissue plasminogen activator for acute ischemic stroke in patients aged 80 years and older: the tPA stroke survey experience. Stroke 2000;31(2):370-5.
29 Brewer PV, Vadeboncoeur A. PsychOSocial effecTs Of aCute stroke thrombolysIS programs on neurologists and Emergency physicians: A proSpectIve comparativE cohoRt (POST ‘OC IS EASIER) study. Can J Emerg Med 2003;133.
30 Brewer PV, Vadeboncoeur A. The psycho-social effects on the Neurology community secondary to the use of tPA for stroke: A prospective cohort study. http://www.mail-archive.com/[email protected]/msg00340/NINDS_RAW_DATA.PDF, 2002.

Jean-François Pinel
36
31 Hacke W, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med 2008;359(13):1317-29.
32 Sandercock P, et al. The benefits and harms of intravenous thrombolysis with recombinant tissue plasminogen activator within 6 h of acute ischaemic stroke (the third international stroke trial [IST-3]): a randomised controlled trial. Lancet 2012;379(9834):2352-63.
33 Leys D, Cordonnier C. rt-PA for ischaemic stroke: what will the next question be? Lancet 2012; 379(9834):2320-1.
34 Tsivgoulis G, et al. Safety and outcomes of intravenous thrombolysis in stroke mimics: a 6-year, single-care center study and a pooled analysis of reported series. Stroke 2011;42(6):1771-4.
35 Zinkstok SM, et al. Safety of thrombolysis in stroke mimics: results from a multicenter cohort study. Stroke 2013;44(4):1080-4.
36 Guerrero WR, Savitz SI. Tissue-type plasminogen activator for stroke mimics: continuing to be swift rather than delaying treatment to be sure. Stroke 2013;44(5):1213-14.
37 Chao AC, et al. Outcomes of thrombolytic therapy for acute ischemic stroke in Chinese patients: the Taiwan Thrombolytic Therapy for Acute Ischemic Stroke (TTT-AIS) study. Stroke 2010;41(5):885-90.
38 Liao X, et al. Standard-dose intravenous tissue-type plasminogen activator for stroke is better than low doses. Stroke 2014;45(8):2354-8.
39 Simonsen CZ, et al. Sensitivity of diffusion- and perfusion-weighted imaging for diagnosing acute ischemic stroke is 97.5%. Stroke 2015;46:98-101.
40 Strbian D, et al. Symptomatic intracranial hemorrhage after stroke thrombolysis: comparison of prediction scores. Stroke 2014;45(3):752-8.
41 Greisenegger S, et al. Thrombolysis in patients with mild stroke: results from the Austrian Stroke Unit Registry. Stroke 2014;45(3):765-9.
42 Tisserand M, et al. Is white matter more prone to diffusion lesion reversal after thrombolysis? Stroke 2014;45(4):1167-9.
43 Tisserand M, et al. Mechanisms of unexplained neurological deterioration after intravenous thrombolysis. Stroke 2014;45:3527-34.
44 Frank B, et al. Thrombolysis in stroke despite contraindications or warnings? Stroke 2013;44(3):727-33.
45 Vannier SR, T, Pinel JF. Enquete auprès des UNV bretonnes sur la thrombolysis off-label. Poster 18eme journées de la SFNV, Paris, 2013.
46 Jauch EC, et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013;44(3):870-947.
47 Wardlaw JM, del Zoppo G, Yamaguchi T. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev 2000;(2):CD000213.
48 Wardlaw JM, et al. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev 2003;(3):CD000213.
49 Wardlaw JM, et al. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev 2009;(4):CD000213.
50 Wardlaw JM, et al. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev 2014;(7):CD000213.
51 Schellinger PD, Kohrmann M. 4.5-Hour time window for intravenous thrombolysis with recom-binant tissue-type plasminogen activator is established firmly. Stroke 2014;45(3):912-13.
52 Wechsler LR. The 4.5-hour time window for intravenous thrombolysis with intravenous tissue-type plasminogen activator is not firmly established. Stroke 2014;45(3):914-15.

37
AVC : nouveautés thérapeutiques : Après 20 ans de thrombolyse, quoi de neuf ?
53 Selim MH, Molina CA. Thrombolysis in the 3- to 4.5-hour window: what do ECASSkeptics want? Stroke 2014;45(3):916-17.
54 Hacke W, et al. Intravenous desmoteplase in patients with acute ischaemic stroke selected by MRI perfusion-diffusion weighted imaging or perfusion CT (DIAS-2): a prospective, randomised, double-blind, placebo-controlled study. Lancet Neurol 2009;8(2):141-50.
55 Radecki RPC, YG, Press, GM. rt-PA and stroke: does IST-3 make it all clear or muddy the waters? Answers to the November 2012 Journal Club questions. Ann Emerg Med 2013;(4):489-98.
56 http://emergencymedicineireland.com/lytics-in-stroke/.57 http://www.smartem.org/podcasts/smart-thrombolytics-stroke-update.58 Hoffman JR, Cooper RJ. How is more negative evidence being used to support claims of
benefit: The curious case of the third international stroke trial (IST-3). Emerg Med Australas 2012;24(5):473-6.
59 Fatovich DM. Believing is seeing: stroke thrombolysis remains unproven after the third International Stroke Trial (IST-3). Emerg Med Australas 2012;24(5):477-9.
60 Hoffman JR, Schriger DL. A graphic reanalysis of the NINDS Trial. Ann Emerg Med 2009;54(3):329-36; 336 e1-35.
61 Shinton R. Questions about authorisation of alteplase for ischaemic stroke. Lancet 2014;384(9944):659-60.
62 Cohen D, Macdonald H. UK drug agency announces review of use of alteplase after stroke. BMJ 2014;349:g5355.
63 Fatovich DM, Brown SG. Stroke thrombolysis remains unproven: per ardua, ad astra. Intern Med J 2014;44(12a):1261-2.
64 Shamy MC, Jaigobin CS. The complexities of acute stroke decision-making: a survey of neurolo-gists. Neurology 2013;81(13):1130-3.
65 Fransen PS, et al. MR CLEAN, a multicenter randomized clinical trial of endovascular treatment for acute ischemic stroke in the Netherlands: study protocol for a randomized controlled trial. Trials 2014;15:343.
38
AVC : nouveautés thérapeutiquesStroke: new therapies© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
Traiter l’hémorragie cérébrale
Christian Stapf (Paris)
L’hémorragie cérébraLe : un aVc à hauT risque
Les accidents vasculaires cérébraux (AVC) représentent la troisième cause de mor-talité et la première cause d’invalidité dans nos sociétés. De 70 à 90 % des AVC sont de nature ischémique. Si elle est plus rare, l’hémorragie cérébrale est une forme particulièrement grave d’AVC avec une mortalité comprise entre 30 et 60 % dans les 30 premiers jours (contre 15 à 20 % dans les infarctus cérébraux) et de lourds déficits neurologiques à long terme.
Avec le vieillissement de la population, et en partie secondairement à la prescrip-tion de plus en plus fréquente d’anticoagulants, le taux annuel d’hémorragies céré-brales augmente progressivement. Les facteurs de risque d’hémorragie cérébrale les plus fréquents sont l’hypertension artérielle (60–70 % des cas), l’abus d’alcool, le tabagisme et d’autres prédispositions comme l’angiopathie amyloïde.
Au cours des 24 premières heures d’une hémorragie cérébrale spontanée, le volume de l’hématome progresse d’au moins un tiers dans 38 % des cas. Cette progression de l’hématome constitue un facteur associé à un plus mauvais pronostic en termes de mortalité à la phase aiguë et de morbidité à long terme.
Prise en charge ThéraPeuTique
Toute hémorragie cérébrale a une cause sous-jacente
Au cours des 40 dernières années, plusieurs classifications ont été proposées pour les AVC ischémiques, permettant de catégoriser les infarctus cérébraux en fonction de leur étiologie selon les classifications de l’Harvard Stroke Registry / NINDS Stroke Databank, de l’Oxford Community Stroke Project classification (OCSP), de la classification TOAST (Trial of Org 10172 in Acute Stroke Treatment) ou de l’a-s-C-o (Atherosclerosis, Small vessel disease, Cardiac source, Other cause).
En revanche, les classifications des hémorragies cérébrales se limitent à la prise en compte de leur localisation (intracérébrale / sous-arachnoïdienne / intraventriculaire ou lobaire / profonde) et à une catégorisation étiologique sommaire qui oppose les
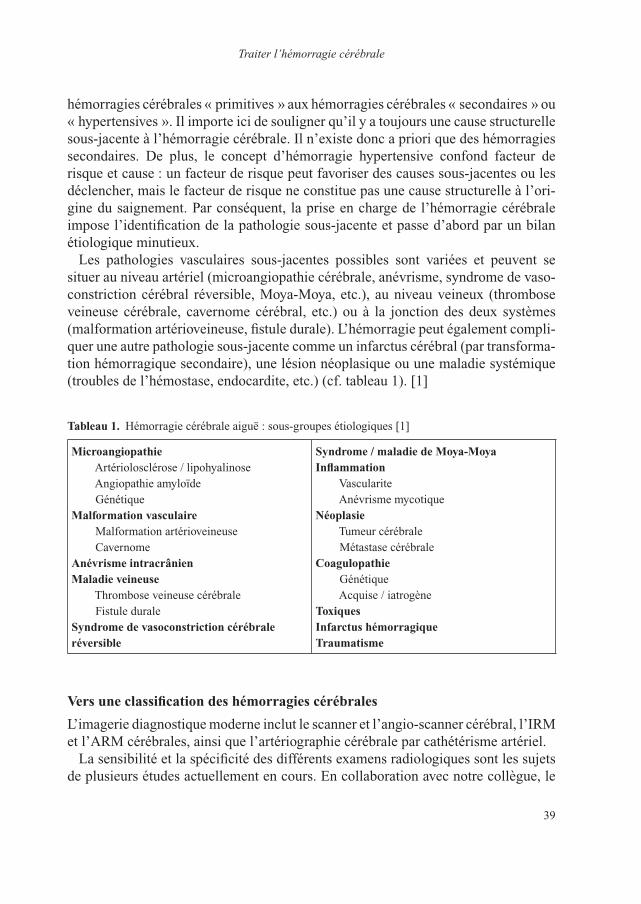
39
Traiter l’hémorragie cérébrale
hémorragies cérébrales « primitives » aux hémorragies cérébrales « secondaires » ou « hypertensives ». Il importe ici de souligner qu’il y a toujours une cause structurelle sous-jacente à l’hémorragie cérébrale. Il n’existe donc a priori que des hémorragies secondaires. De plus, le concept d’hémorragie hypertensive confond facteur de risque et cause : un facteur de risque peut favoriser des causes sous-jacentes ou les déclencher, mais le facteur de risque ne constitue pas une cause structurelle à l’ori-gine du saignement. Par conséquent, la prise en charge de l’hémorragie cérébrale impose l’identification de la pathologie sous-jacente et passe d’abord par un bilan étiologique minutieux.
Les pathologies vasculaires sous-jacentes possibles sont variées et peuvent se situer au niveau artériel (microangiopathie cérébrale, anévrisme, syndrome de vaso-constriction cérébral réversible, Moya-Moya, etc.), au niveau veineux (thrombose veineuse cérébrale, cavernome cérébral, etc.) ou à la jonction des deux systèmes (malformation artérioveineuse, fistule durale). L’hémorragie peut également compli-quer une autre pathologie sous-jacente comme un infarctus cérébral (par transforma-tion hémorragique secondaire), une lésion néoplasique ou une maladie systémique (troubles de l’hémostase, endocardite, etc.) (cf. tableau 1). [1]
Tableau 1. Hémorragie cérébrale aiguë : sous-groupes étiologiques [1]
microangiopathie Artériolosclérose / lipohyalinose Angiopathie amyloïde Génétiquemalformation vasculaire Malformation artérioveineuse Cavernomeanévrisme intracrânienmaladie veineuse Thrombose veineuse cérébrale Fistule duralesyndrome de vasoconstriction cérébrale réversible
syndrome / maladie de moya-moyainflammation Vascularite Anévrisme mycotiquenéoplasie Tumeur cérébrale Métastase cérébralecoagulopathie Génétique Acquise / iatrogèneToxiquesinfarctus hémorragiqueTraumatisme
Vers une classification des hémorragies cérébrales
L’imagerie diagnostique moderne inclut le scanner et l’angio-scanner cérébral, l’IRM et l’ARM cérébrales, ainsi que l’artériographie cérébrale par cathétérisme artériel.
La sensibilité et la spécificité des différents examens radiologiques sont les sujets de plusieurs études actuellement en cours. En collaboration avec notre collègue, le
Christian Stapf
40
Pr Charlotte Cordonnier (CHRU Lille), nous travaillons actuellement avec plusieurs centres européens, à une première classification étiologique, et nous essayons de définir les critères diagnostiques permettant d’établir une étiologie « possible », « probable » ou « définitive ».
hiérarchiser les examens d’imagerie
D’après des données issues d’une cohorte de 152 patients prospectifs, l’imagerie scannographique nous a permis de porter un diagnostic étiologique chez 3 % des patients, l’imagerie par IRM/ARM chez 63 %, et la réalisation d’une artériographie chez 6 % des patients, soit un total de 72 % de diagnostics étiologiques précis pour des hémorragies cérébrales normalement classifiées en « primitives » ou « hypertensives ».
Il faut souligner que 21 % de ces diagnostics modifiaient immédiatement les modalités de prise en charge des patients.
Les examens d’imagerie ont été répétés 3 à 4 mois plus tard chez les patients demeurés sans diagnostic étiologique, après résorption de l’hématome (il peut arriver que ce dernier masque la cause du saignement). Ainsi, alors qu’une artériographie initiale d’apparence normale, une seconde artériographie effectuée après résorption de l’hématome pourra, par exemple, révéler une malformation artérioveineuse ou un cavernome cérébral pouvant être traité et guéri.
En résumé, notre pratique doit être définie par le fait qu’il n’existe que des hémor-ragies secondaires et les notions d’hémorragies « primaires » ou « hypertensives » doivent être évitées. Le bilan d’imagerie a pour but de permettre la visualisation de la cause de l’hémorragie. Certains diagnostics étiologiques doivent être portés en urgence car ils vont influer sur la décision thérapeutique aiguë (anévrismes, infarctus hémorragique, maladies veineuses, maladies systémiques…). En outre, toute cause identifiée a des implications à long terme comme l’éradication de la lésion lorsque cela est possible (anévrisme, MAV, cavernome, fistule durale…) et la prise en charge des facteurs de risque lorsqu’ils sont présents (hypertension, tabagisme…).
Vers une prise en charge thérapeutique ciblée
Le spot-sign
Un diagnostic de maladie des petites artères va être porté chez la grande majorité des patients. Ces patients sont à risque d’aggravation rapide selon la cascade d’événe-ments suivante : augmentation de volume (effet de masse), inondation ventriculaire, hydrocéphalie secondaire, hypertension intracrânienne et, au pire, engagement cérébral entraînant le décès du patient. Il importe, en conséquence, de stopper ce processus. Un signe radiologique appelé « spot-sign » est actuellement évalué en tant que facteur prédictif d’expansion hémorragique. [2] Une étude observation-nelle multicentrique publiée en 2012, menée chez 268 patients avec hémorragie
41
Traiter l’hémorragie cérébrale
cérébrale, a ainsi montré la présence du spot-sign dans les hématomes aigus chez un quart des patients (23 %). La présence du spot-sign était prédictive de l’expansion de l’hématome avec une sensibilité de 51 % et une spécificité de 85 %. La mortalité à 3 mois était de 43,4 % chez les patients spot-sign positifs contre 19,6 % chez les patients spot-sign négatifs (HR : 2,4, intervalle de confiance à 95 % : 1,4–4,0 ; p = 0,002). [3]
La prise en charge
Correction des facteurs de risque
Une atteinte des petites artères cérébrales est souvent consécutive à l’effet des fac-teurs de risque vasculaire qui ont entraîné la dégénérescence et finalement la rupture de la paroi artérielle. Le contrôle de ces facteurs de risque et, plus particulièrement, de l’hypertension artérielle est primordial pour éviter la progression de l’atteinte des petites artères et des complications hémorragiques. Pour rappel, il a été montré qu’une diminution de 10 mmHg de la pression systolique ou de 5 mmHg de pression diastolique permet de prévenir 80 % des hémorragies cérébrales sur cinq ans.
Stopper l’extravasation et la croissance de l’hématome
– Hémostase localeDes résultats prometteurs de l’administration très précoce (< 4 heures après le début des signes cliniques) d’un facteur hémostatique, le facteur VII activé recombinant (FVIIa), ont été rapportés dans une étude de phase II randomisée évaluant la tolérance et l’efficacité. La progression du volume de l’hématome cérébral était nettement moindre dans le groupe traité que dans le groupe pla-cebo avec une efficacité significative sur les critères cliniques de dépendance ou de mortalité. [4]Néanmoins, une étude de phase III de confirmation n’a pas retrouvé d’effet favorable sur l’évolution clinique. [5]D’autres traitements hémostatiques sont actuellement en cours d’évaluation, y compris la transfusion de plaquettes chez les patients victimes d’une hémor-ragie cérébrale aiguë dans un contexte de traitement antiplaquettaire en vigueur (étude PATCH). En attendant les résultats des études en cours, le traitement hémostatique ne peut pas être recommandé dans l’hémorragie cérébrale aiguë.
– Évacuation neurochirurgicale L’évacuation chirurgicale de l’hématome est réalisée au cas par cas, mais sans preuve scientifique quelle que soit la méthode : évacuation par craniotomie ouverte ou par voie endoscopique sous contrôle stéréotaxique. L’étude interna-tionale STICH (Surgical Trial in Intracerebral Haemorrhage) a inclus un total de plus de 1000 patients et a comparé l’évacuation chirurgicale précoce à la prise
Christian Stapf
42
en charge médicale conservative dans les 72 heures d’une hémorragie cérébrale sus-tentorielle spontanée (sans malformation vasculaire sous-jacente). La méthode chirurgicale était laissée à l’appréciation des neurochirurgiens qui ont opté pour une craniotomie dans la grande majorité des cas (77 %). L’étude n’a pas permis de montrer de différence entre la chirurgie et le traitement médical des hémorragies cérébrales sus-tentorielles (toutes localisations confondues), sur la mortalité, ni sur la dépendance évaluée à 6 mois. [6]De la même façon, l’étude STICH II (n = 597 patients avec hématome lobaire de moins de 12 heures) n’a montré aucune différence de morbi-mortalité entre les modalités de prise en charge avec ou sans chirurgie. Une étude évaluant la chirurgie « minimalement invasive » sur l’hématome est actuellement en cours et une évaluation de l’hémicraniectomie décompressive après une hémorragie sus-tentorielle est en préparation. [7]
– Traitement antihypertenseurPlusieurs études non contrôlées ont suggéré l’existence d’une corrélation négative entre la pression artérielle et la détérioration neurologique chez les patients hospitalisés en unité de soins intensifs neurovasculaires (USINV) pour hémorragie intracérébrale spontanée. Les résultats de l’étude randomisée pilote INTERACT (Intensive Blood Pressure Reduction in Acute Cerebral Haemorrhage Trial) ont ainsi montré que chez 404 patients traités par antihy-pertenseur moins de 6 heures après la survenue des symptômes de l’hémorragie cérébrale (tension artérielle systolique cible < 140 mmHg), la progression du volume de l’hématome était moindre par rapport au groupe contrôle. [8]Finalement, l’étude INTERACT 2, un essai randomisé international incluant 2 839 patients, a mis en évidence une forte tendance à l’amélioration de la morbi-mortalité (odds ratio 0,87 ; IC 95 % : 0,75–1,01 ; p = 0,006) chez des patients traités par abaissement rapide de la tension artérielle systolique (tension cible < 140 mmHg en moins de 60 minutes) et une amélioration significative de l’évolution neurologique sur l’échelle de Rankin à 3 mois (odds ratio 0,87 ; IC 95 % : 0,77–1,00 ; p = 0,04). [9]Dans l’attente des résultats d’un autre essai randomisé en cours, les recomman-dations actuelles en cas d’hémorragie cérébrale aiguë favorisent l’application immédiate d’un traitement antihypertenseur ciblant une tension systolique inférieure à 140 mmHg en moins de 40 minutes. [10]
implications pratiques
– Il convient de garder à l’esprit que toute hémorragie cérébrale a une cause structurelle sous-jacente qu’il faut dépister par un bilan adéquat. Des facteurs de risque favorisent et ou modifient certaines causes, mais il importe de ne

43
Traiter l’hémorragie cérébrale
pas confondre causes et facteurs de risque. Les notions d’hémorragies « primi-tives » ou « hypertensives » doivent donc être évitées.
– Le bilan diagnostique a pour but de permettre la visualisation étiologique et la mise en œuvre d’une prise en charge thérapeutique ciblée. La présence du spot-sign peut servir de facteur prédictif de l’expansion de l’hématome.
– L’hémostase locale et l’évacuation chirurgicale de l’hématome n’ont pas fait la preuve de leur efficacité.
– En revanche, il apparaît aujourd’hui clairement que le traitement antihyperten-seur aigu permet une amélioration de la morbi-mortalité. Il doit être intense (traitement IV en bolus puis en continu) pour permettre une baisse de la pression artérielle systolique en dessous de 140 mmHg en moins d’une heure. Il doit être administré sous une surveillance tensionnelle étroite (mesure de la pression artérielle toutes les 15 minutes durant une heure). Le protocole appli-qué doit être bien défini et connu de toute l’équipe soignante. Comme dans la thrombolyse, la rapidité est un facteur déterminant et il faut éviter les délais entre l’imagerie et la mise en œuvre du traitement antihypertenseur. Dans cette situation, l’esprit d’équipe est crucial.
– Le traitement doit être administré au sein d’une USINV et il faut que le contrôle des chiffres tensionnels soit durable, pendant les premières 24 heures (bénéfices en phase aiguë < 24 h), puis les premiers jours (bénéfices en phase post-aiguë < 7 jours) et enfin, à vie (bénéfices à long terme : prévention).
– La mise à jour des recommandations de l’AHA/ASA est en cours de rédac-tion. Les recommandations européennes (ESO) ont été publiées en 2014. [11] Un comité français du nom de SFNV vient de se constituer dans le but d’émettre des recommandations.
bibliographie
1 Al-Shahi Salman R1, Labovitz DL, Stapf C. Spontaneous intracerebral hemorrhage. BMJ 2009; 339:b2586.
2 Wada R, Aviv RI, Fox AJ, et al. CT angiography “spot sign” predicts hematoma expansion in acute intracerebral hemorrhage. Stroke 2007;38:1257-62.
3 Demchuk AM, Dowlatshahi D, Rodriguez-Luna D, et al. Prediction of haematoma growth and outcome in patients with intraHemorrhagic stroke using the CT-angiography spot sign (PREDICT): a prospective observational study. Lancet Neurol 2012;11:307-14.
4 Mayer SA, Brun NC, Begtrup K, et al. Recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med 2005;352:777-85.
5 Mayer SA, Brun NC, Begtrup K, et al. Efficacy and safety of recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med 2008;358:2127-37.
6 Mendelow AD, Gregson BA, Fernandes HM, et al. Early surgery versus initial conserva-tive treatment in patients with spontaneous supratentorial intracerebral haematomas in the

Christian Stapf
44
International Surgical Trial in IntraHemorrhagic stroke (STICH): a randomised trial. Lancet 2005;365:387-97.
7 Mendelow AD, Gregson BA, Rowan EN, et al. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial lobar intracerebral haematomas (STICH II): a randomised trial. Lancet 2013;382:397-408.
8 Anderson CS, Huang Y, Arima H, et al. Effects of early intensive blood pressure-lowering treatment on the growth of hematoma and perihematomal edema in acute intracerebral hemorrhage: the Intensive Blood Pressure Reduction in Acute Hemorrhagic stroke Trial (INTERACT). Stroke 2010;41:307-12.
9 Anderson CS, Heeley E, Huang Y, et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N Engl J Med 2013;368:2355-65.
10 Manning L, Hirakawa Y, Arima H, et al. Blood pressure variability and outcome after acute intraHemorrhagic stroke: a post-hoc analysis of INTERACT2, a randomised controlled trial. Lancet Neurol 2014;13:364-73.
11 Steiner T, Al-Shahi Salman R, Beer R, et al. European Stroke Organisation (ESO) guidelines for the management of spontaneous intracerebral hemorrhage. Int J Stroke 2014;9:840-55.
45
AVC : nouveautés thérapeutiquesStroke: new therapies© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
Un scanner dans l’ambulance ? Thrombolyse pré-hospitalière et autres opportunités
Martin Ebinger (Berlin)
InTrodUcTIon
Les accidents vasculaires cérébraux (AVC) sont une cause majeure de mortalité et d’invalidité dans le monde [1]. La thrombolyse par administration intraveineuse d’activateur du plasminogène tissulaire (tPA) est un traitement largement disponible, scientifiquement fondé et légalement autorisé, qui réduit le risque d’invalidité per-manente après un AVC ischémique [2, 3]. Toutefois, les effets de la thrombolyse dépendent fortement du temps [4]. A chaque minute de retard du traitement, les chances d’un bon résultat s’amenuisent [5-7]. Par conséquent, le tPA doit être admi-nistré le plus tôt possible après le début des symptômes. Dans l’idéal, le traitement sera entamé immédiatement dès le premier contact avec le patient, c’est-à-dire quand l’ambulance arrive pour emmener le patient à l’hôpital. Étant donné que le tableau clinique ne permet pas de distinguer avec fiabilité un AVC ischémique d’un AVC hémorragique, une tomodensitométrie (TDM) est requise avant le traitement [8]. D’autre part, le traitement par tPA est associé au risque redouté d’hémorragie intra-cérébrale symptomatique (HICs). Cela exige une grande expérience clinique si l’on choisit cette option thérapeutique. Un neurologue habitué au traitement des AVC aigus, capable de traiter correctement les complications possibles et formé à la médecine d’urgence réunit toutes les qualités requises dans un contexte pré-hospitalier. En 2012, le Dr Silke Walter et ses collègues de Hombourg, dans la Sarre (Allemagne), ont été les premiers à publier sur des traitements par tPA au moyen d’une “Unité Mobile AVC”, qui est une ambulance équipée d’un scanner et d’un laboratoire embarqué. Ces pionniers de l’équipe du Pr Klaus Fassbender ont démontré d’excellents gains de temps par rapport aux soins classiques [9].
Martin Ebinger
46
Thrombolyse pré-hospITalIère
La thrombolyse pré-hospitalière, dans une ambulance spécialisée dans le traitement des AVC, est réalisable, sûre, et réduit le délai entre l’alerte et le traitement. Cela a été démontré récemment par une étude prospective, appelée PHANTOM-S [10]. Dans cette étude, conçue et supervisée par le Pr Heinrich Audebert de la Charité (Allemagne), les semaines ont été randomisées par blocs au STEMO ou aux soins habituels. «STEMO» (Stroke Emergency Mobile) désigne le Mobile d’Urgence AVC (Figure 1), ambulance équipée d’un scanner, d’un laboratoire embarqué et d’une connexion de télé-médecine. Une équipe spécialisée est à son bord. Cette équipe se compose d’un neurologue urgentiste, d’un technicien en radiologie et d’un paramédical. Par UMTS, le STEMO est relié à un neuro-radiologue par téléphone. Au centre d’orientation de Berlin, régi par le Département des Pompiers de Berlin, un algorithme précédemment développé et validé pour la reconnaissance des AVC a été employé pendant les appels d’urgence [11]. Si l’orienteur suspectait un AVC dans les 4 heures suivant le début des symptômes ou lorsque le début des symptômes était inconnu, l’alerte AVC était activée. Cela entraînait la mobilisation du STEMO
1
Figure 1. Le Mobile d’Urgence AVC (STEMO) devant la porte de Brandebourg à Berlin (Allemagne) (par sbdsgn.de; avec l’aimable autorisation de MEYTEC GmbH, Werneuchen, Allemagne).
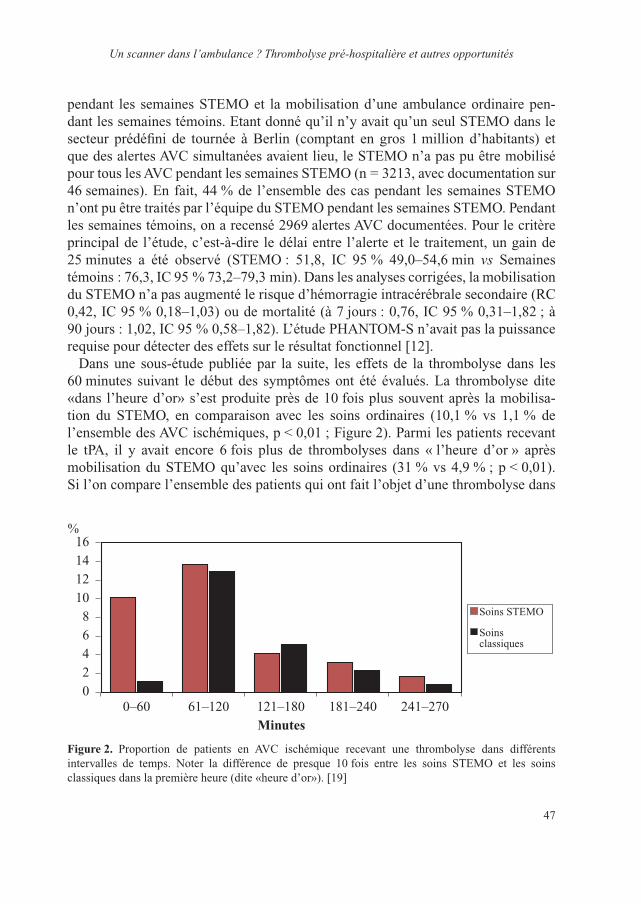
47
Un scanner dans l’ambulance ? Thrombolyse pré-hospitalière et autres opportunités
pendant les semaines STEMO et la mobilisation d’une ambulance ordinaire pen-dant les semaines témoins. Etant donné qu’il n’y avait qu’un seul STEMO dans le secteur prédéfini de tournée à Berlin (comptant en gros 1 million d’habitants) et que des alertes AVC simultanées avaient lieu, le STEMO n’a pas pu être mobilisé pour tous les AVC pendant les semaines STEMO (n = 3213, avec documentation sur 46 semaines). En fait, 44 % de l’ensemble des cas pendant les semaines STEMO n’ont pu être traités par l’équipe du STEMO pendant les semaines STEMO. Pendant les semaines témoins, on a recensé 2969 alertes AVC documentées. Pour le critère principal de l’étude, c’est-à-dire le délai entre l’alerte et le traitement, un gain de 25 minutes a été observé (STEMO : 51,8, IC 95 % 49,0–54,6 min vs Semaines témoins : 76,3, IC 95 % 73,2–79,3 min). Dans les analyses corrigées, la mobilisation du STEMO n’a pas augmenté le risque d’hémorragie intracérébrale secondaire (RC 0,42, IC 95 % 0,18–1,03) ou de mortalité (à 7 jours : 0,76, IC 95 % 0,31–1,82 ; à 90 jours : 1,02, IC 95 % 0,58–1,82). L’étude PHANTOM-S n’avait pas la puissance requise pour détecter des effets sur le résultat fonctionnel [12].
Dans une sous-étude publiée par la suite, les effets de la thrombolyse dans les 60 minutes suivant le début des symptômes ont été évalués. La thrombolyse dite «dans l’heure d’or» s’est produite près de 10 fois plus souvent après la mobilisa-tion du STEMO, en comparaison avec les soins ordinaires (10,1 % vs 1,1 % de l’ensemble des AVC ischémiques, p < 0,01 ; Figure 2). Parmi les patients recevant le tPA, il y avait encore 6 fois plus de thrombolyses dans « l’heure d’or » après mobilisation du STEMO qu’avec les soins ordinaires (31 % vs 4,9 % ; p < 0,01). Si l’on compare l’ensemble des patients qui ont fait l’objet d’une thrombolyse dans
02468
101214
%16
0–60 61–120 121–180 181–240 241–270Minutes
Soins STEMO
Soins classiques
Figure 2. Proportion de patients en AVC ischémique recevant une thrombolyse dans différents intervalles de temps. Noter la différence de presque 10 fois entre les soins STEMO et les soins classiques dans la première heure (dite «heure d’or»). [19]

Martin Ebinger
48
« l’heure d’or » aux patients traités plus tardivement, il n’y avait pas de différence statistiquement significative en termes d’hémorragie intracérébrale secondaire et de mortalité à 7 jours ou 90 jours. Toutefois, les analyses corrigées de l’âge, du sexe, de la fibrillation auriculaire et du NIHSS ont révélé un RC de 1,93 (IC 95 % 1,09–3,41) pour le retour au domicile après mobilisation du STEMO [13]. Bien que ce ne soit là que le résultat d’une analyse exploratoire utilisant un paramètre indirect (le retour au domicile), il correspond bien à l’association solidement établie entre la précocité du traitement et la qualité des résultats [4, 5, 7]. D’autres études, ayant la puissance requise pour détecter des différences de résultats fonctionnels entre les groupes, sont nécessaires pour démontrer les effets d’une thrombolyse pré-hospitalière dans « l’heure d’or » (et après) sur le résultat fonctionnel.
TrIage
Le triage est une importante tâche pré-clinique, qui permet de s’assurer que les patients reçoivent le traitement optimal tout en utilisant au mieux les ressources. Habituellement, les patients sont orientés vers l’hôpital le plus proche. Dans l’idéal, ils sont admis dans l’hôpital adéquat le plus proche. Dans le cas d’un AVC ischémique aigu, l’hôpital adéquat est celui qui dispose d’une unité spécialisée dans l’AVC. Dans le cas d’un AVC hémorragique, un hôpital doté d’un service de neurochirurgie serait souhaitable et, de plus en plus, les patients présentant une oblitération des grosses artères sont transférés dans des centres capables de réaliser une revascularisation mécanique après le début d’un traitement IV par tPA.
Le concept de STEMO augmente le taux de reconnaissance des AVC, facilite l’admission d’un patient donné dans l’hôpital adéquat et permet d’instaurer un temps de traitement critique pendant le transport. Par exemple, les patients sous anticoagulants oraux présentant une hémorragie intra-cérébrale peuvent faire l’objet d’un diagnostic fiable dans le contexte pré-hospitalier et l’inversion de l’anti-coa-gulation peut démarrer avant l’arrivée à l’hôpital. Une réduction énergique de la pression artérielle peut être obtenue pendant le transport. Les résultats de l’essai INTERACT2 tendent à prouver qu’un traitement plus précoce procure là encore le plus grand bénéfice dans les AVC hémorragiques [14]. Si l’angiographie par TDM à bord du STEMO révèle une oblitération des grosses artères (p. ex. AIC ou M1), le patient peut être amené au laboratoire de cathétérisation le plus proche pour une revascularisation mécanique après la mise en œuvre d’un traitement par tPA. Le Dr Matthias Wendt, l’un des neurologues urgentiste du STEMO, a récemment conduit une étude formelle des effets de la mobilisation du STEMO sur les hospita-lisations. Comparant les admissions après mobilisation du STEMO aux admissions pendant les soins ordinaires, il a observé des différences significatives en faveur du STEMO pour les admissions des victimes d’un AVC ischémique dans des hôpitaux
49
Un scanner dans l’ambulance ? Thrombolyse pré-hospitalière et autres opportunités
dotés d’unités AVC et les admissions des victimes d’un AVC hémorragique dans des hôpitaux dotés d’un service de neurochirurgie, (Wendt et al., manuscrit soumis à publication).
Une plaTe-Forme de recherche pré-hospITalIère
Le STEMO est plus qu’un outil pour accélérer la thrombolyse, avoir des aperçus sur les effets de la thrombolyse dans « l’heure d’or » ou améliorer le triage des patients. C’est une plate-forme de recherche idéale. Plusieurs agents neuroprotecteurs n’ont pas réussi jusqu’ici l’épreuve des essais cliniques. L’une des raisons à cela pourrait être l’utilisation tardive d’agents potentiellement thérapeutiques par rapport à l’appli-cation réussie dans les études chez l’animal. Le STEMO pourrait offrir l’opportunité d’une rencontre très précoce entre les victimes d’un AVC et les experts, permettant le démarrage de traitements expérimentaux. Bien que son résultat soit neutre, l’essai FAST-Mag du Pr Jeff Saver, de l’Université de Californie à Los Angeles (UCLA), est un excellent exemple de la conduite d’un essai à grande échelle sur les neuro-protecteurs dans un contexte pré-hospitalier [15, 16]. L’utilisation d’ambulances équipées d’un scanner peut accroître la puissance de telles études à l’avenir, en sélectionnant les patients appropriés sur la base de critères d’imagerie. Outre l’essai de nouveaux médicaments ou de nouvelles interventions, comme le refroidissement précoce, le STEMO a déjà mis en évidence certains bio-marqueurs qui pourraient être utiles ou non pour étayer le diagnostic d’AVC. Par exemple, Michal Rozanski, un autre neurologue à bord du STEMO de Berlin, a récemment étudié la sensibilité et la spécificité de la protéine acide fibrillaire gliale (PAFG) pour distinguer les AVC ischémiques des hémorragies intra-cérébrales. Alors que les données préliminaires suggéraient que la sensibilité était plutôt faible, la présence de taux de PAFG supé-rieurs à 0,29 ng/ml s’avère être un indicateur fiable d’un AVC hémorragique [17]. D’autre part, la copeptine, extrémité N-terminale de la vasopressine, ne s’est pas révélée utile pour distinguer les AVC ischémiques des pseudo-AVC, des urgences vasculaires et non-vasculaires ou des fenêtres temporelles précoces et tardives après un AVC (Wendt, manuscrit soumis à publication).
rapporT coûT/eFFIcacITé
Les nouvelles avancées ont toujours un certain prix, et il est plus que justifié de se demander quels sont les coûts générés par les concepts de thrombolyse pré-hospita-lière. Ces coûts doivent alors être pesés au regard des bénéfices attendus et réellement obtenus. Jusqu’ici, les analyses coût/efficacité du concept STEMO se sont appuyées sur des extrapolations. Néanmoins, les premières analyses ont été menées et elles

Martin Ebinger
50
suggèrent un incrément du ratio coût/efficacité (ICER) raisonnable pour chaque année de vie (corrigée de la qualité, QALY) gagnée avec le STEMO. Ces analyses ont été conduites en collaboration avec une équipe de recherche danoise d’Odense, et publiées récemment par Dorte Gyrd-Hansen et al. [18]. En se basant sur la collecte de tous les reçus disponibles, le coût annuel net du concept STEMO était de 963 954 €. A partir des données d’essais randomisés contre placebo du tPA, les nombres de sujets à traiter pour éviter une invalidité ont été utilisés pour calculer l’effet que pourrait avoir la thrombolyse pré-hospitalière sur le résultat fonctionnel. Selon cette approche, la plus haute fréquence des thrombolyses et la plus haute proportion de patients traités précocement pourraient éviter 18 cas d’invalidité par an. Ces 18 cas s’élèvent à 29,7 QALY gagnées, soit un ICER de 32 456 € par QALY. Que ce prix à payer soit acceptable ou non, cela ne relève pas de la recherche médicale : cela dépend de la volonté d’une société à financer la prévention des invalidités. Cette décision politique dépend en outre de la disponibilité de contre-mesures alternatives concurrentes, qui nécessitent également un financement. En général, cependant, les ICER situés au-dessous de 50 000–100 000 $US (aux Etats-Unis) ou de 30 000 £ (au Royaume-Uni) semblent acceptables dans de nombreux pays occidentaux. Etant donné que la seule analyse coût/efficacité, à ce jour, du concept de thrombolyse pré-hospitalière repose sur des extrapolations (d’abord, du nombre d’invalidités évitées, et ensuite, de l’équation de +1,77 QALY pour chaque invalidité évitée), il est clair que d’autres études sont nécessaires pour constituer un terrain solide pour les décideurs. Ces études devront tenir compte non seulement des effets de la throm-bolyse pré-hospitalière, mais aussi de traitements tels que la réduction de la pression artérielle en cas d’AVC hémorragique, comme l’a souligné le Pr Marie-Germaine Bousser lors du Colloque de L’Institut Servier, AVC : nouveautés thérapeutiques, à Paris (France), le 20 novembre 2014.
conclUsIon
La thrombolyse pré-hospitalière dans les ambulances équipées d’un scanner est faisable, sûre, réduit le délai entre l’alerte et le traitement, augmente le nombre de thrombolyses et renforce les chances de thrombolyse dans « l’heure d’or ». L’imagerie dans l’ambulance permet une hospitalisation “sur mesure” dans les dif-férents établissements et un traitement d’urgence spécifique pendant le transport. Le STEMO est une intéressante plate-forme de recherche “sur le front” qui, d’un point de vue sociétal, est sans doute un sage investissement. Cela dit, le domaine de la thrombolyse pré-hospitalière est en pleine évolution et d’autres études sont nécessaires pour prouver le bénéfice en termes d’invalidités épargnées et de ren-tabilité. L’intégration des concepts de thrombolyse pré-hospitalière dans les soins courants exige des recherches d’accompagnement pour répondre à ces questions
51
Un scanner dans l’ambulance ? Thrombolyse pré-hospitalière et autres opportunités
et pour identifier l’usage optimal d’ambulances spécialisées pour le traitement des AVC. Dans le monde entier, les chercheurs préparent différents projets dans divers contextes. Ainsi, à Paris (France), le Dr Guillaume Turc et le Pr Jean- Louis Mas ont fait une demande de crédits pour lancer leur projet de thrombolyse pré-hospitalière, appelé ASPHALT [Acute stroke: prehospital vs. inhospital intravenous thrombolyse (AVC aigu : thrombolyse par administration intraveineuse, pré-hospitalière vs hospi-talière)] – superbe acronyme pour ouvrir la route d’un meilleur traitement des AVC !
références
1 Feigin VL, Forouzanfar MH, Krishnamurthi R, et al. Global and regional burden of stroke during 1990-2010: findings from the Global Burden of Disease Study 2010. Lancet 2014;383(9913): 245-54.
2 The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995;333(24):1581-7.
3 Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med 2008;359(13):1317-29.
4 Emberson J, Lees KR, Lyden P, et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet 2014;384(29):1929–1935.
5 Saver JL, Fonarow GC, Smith EE, et al. Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke. JAMA 2013;309(23):2480-8.
6 Saver JL. Time is brain-quantified. Stroke 2006;37(1):263-6.7 Meretoja A, Keshtkaran M, Saver JL, et al. Stroke thrombolysis: save a minute, save a day. Stroke
2014;45(4):1053-8.8 Runchey S, McGee S. Does this patient have a hemorrhagic stroke?: clinical findings distinguishing
hemorrhagic stroke from ischemic stroke. JAMA 2010;303(22):2280-6.9 Walter S, Kostopoulos P, Haass A, et al. Diagnosis and treatment of patients with stroke in a mobile
stroke unit versus in hospital: a randomised controlled trial. Lancet Neurol 2012;11(5):397-404.10 Ebinger M, Rozanski M, Waldschmidt C, et al. PHANTOM-S: the prehospital acute neurological
therapy and optimization of medical care in stroke patients – study. Int J Stroke 2012;7(4):348-53.11 Krebes S, Ebinger M, Baumann AM, et al. Development and validation of a dispatcher identifica-
tion algorithm for stroke emergencies. Stroke 2012;43(3):776-81.12 Ebinger M, Winter B, Wendt M, et al. Effect of the use of ambulance-based thrombolysis on time to
thrombolysis in acute ischemic stroke: a randomized clinical trial. JAMA 2014;311(16):1622-31.13 Ebinger M, Wendt M, Rozanski M, et al. Golden hour-thrombolysis by starting treatment before
hospital arrival: the Pre-Hospital Acute Neurological Treatment and Optimization of Medical care in Stroke study (PHANTOM-S). Stroke 2014;45(Suppl 1):A104.
14 Anderson CS, Heeley E, Huang Y, et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N Engl J Med 2013;368(25):2355-65.
15 Saver JL, Starkman S, Eckstein M, et al. Methodology of the Field Administration of Stroke Therapy – Magnesium (FAST-MAG) phase 3 trial: Part 1 – rationale and general methods. Int J Stroke 2014;9(2):215-19.
16 Saver JL, Starkman S, Eckstein M, et al. Methodology of the Field Administration of Stroke Therapy – Magnesium (FAST-MAG) phase 3 trial: Part 2 – prehospital study methods. Int J Stroke 2014;9(2):220-5.

Martin Ebinger
52
17 Rozanski M, Waldschmidt C, Kunz A, et al. Plasma Glial Fibrillary Acidic Protein(GFAP) for differentiation between hemorrhagic and ischemic strokes in pre-hospital stroke care. 9th World Stoke Congress, 22-25 October 2014, Poster 399.
18 Gyrd-Hansen D, Olsen KR, Bollweg K, et al. Cost-Effectiveness of Pre-hospital Thrombolysis. Results of the Pre-hospital Acute Neurological Treatment and Optimization of Medical care in Stroke (PHANTOM-S) Study. accepted. Neurology 2015;84(11):1090-1097.
19 Ebinger M, Kunz A, Wendt M, et al. Effects of Golden Hour Thrombolysis: a Prehospital Acute Neurological Treatment and Optimization of Medical Care in Stroke (PHANTOM-S) substudy. JAMA Neurol 2015;72(1):25-30.
53
AVC : nouveautés thérapeutiquesStroke: new therapies© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
Anévrisme rompu : clips ou microspires ?
Vianney Gilard1, Sophie Curey1, Éléonore Tollard1, Olivier Langlois1, François Proust2 (1Rouen, 2Strasbourg)
IntroductIon
Au cours des trois dernières décennies, les modalités du traitement endovasculaire se sont largement imposées dans le domaine de la pathologie neurovasculaire [1]. Les premiers résultats de l’étude ISAT (International Study Aneurysm Trial) confir-ment le rôle prédominant des microspires endovasculaires dans le traitement des anévrismes intracrâniens (IC) rompus [2, 3]. Différentes sociétés internationales ont par la suite formulé des prises de position favorisant ainsi une discussion entre les radiologues interventionnistes et les neurochirurgiens afin d’aboutir à une décision thérapeutique [4-8]. La dernière publication de l’ISAT [9], portant sur le risque tar-dif d’hémorragie sous-arachnoïdienne (HSA) récidivante, confirme l’intérêt de ces nouvelles stratégies avec un haut niveau de preuve. Ce changement dans la pratique médicale conduit à d’importantes conséquences pour le neurochirurgien vasculaire, mais également pour la neurochirurgie dans son ensemble.
Une meilleure compréhension de la place précise de la neurochirurgie vasculaire dans le traitement des anévrismes IC est essentielle pour développer des stratégies visant à préserver l’expertise chirurgicale dans nos services et à déterminer le cursus de la formation. L’objectif de cet article est d’analyser les enseignements et les limites de l’étude ISAT afin de préciser la place des clips microchirurgicaux dans le traitement des anévrismes cérébraux.
Quels sont les enseIgnements des études rAndomIsées ?
Le traitement comparatif des anévrismes IC rompus a été analysé dans quatre études randomisées [3, 9-11], ISAT constituant la principale étude interna-tionale. L’objectif de toutes ces études a été de désigner la procédure la plus sûre entre la mise en place de microspires endovasculaires et celle de clips micro- chirurgicaux.
Vianney Gilard, Sophie Curey, Éléonore Tollard, Olivier Langlois, François Proust
54
dépendance et décès post-thérapeutiques
Après une phase pilote entre mai 1997 et avril 2002, la cohorte ISAT, publiée pour la première fois en 2002 [2], a été composée de 2 143 patients en bon état général lors de l’admission (94 % de grades 1 à 3 sur l’échelle WFNS), qui présentaient des anévrismes rompus de petite taille dans la circulation antérieure (97,3 %), et qui ont été randomisés dans un groupe endovasculaire (n = 1 073) et un groupe micro-chirurgical (n = 1 070). Cette étude, qui a recruté 2 500 patients, afin d’atteindre une puissance statistique de 90 % à un niveau de signification de 0,01 % pour la détection d’une amélioration de 25 % à un an, a été interrompue lors d’une ana-lyse intermédiaire programmée. Les résultats définitifs ont montré une réduction du risque relatif de dépendance ou de décès à un an de 23,9 % (p < 0,001) et une réduction du risque absolu de 7,4 % après un traitement endovasculaire, par rapport au clippage microchirurgical. Les décès à un an ont atteint respectivement 7 % et 7,9 % chez les patients des groupes endovasculaire et microchirurgical. Après un suivi moyen de neuf ans de la cohorte ISAT [9], le taux de mortalité à cinq ans a été significativement réduit dans la cohorte ayant reçu les microspires, et la proportion de patients autonomes a été similaire dans les deux bras. Les derniers résultats de l’étude ISAT portant sur le suivi à long terme (patients vivants à 10 ans), publiés en 2014 [12], ont montré que la probabilité d’être encore en vie et en bon état général (score sur l’Échelle de Rankin modifiée [modified Rankin Scale, mRS] 0 à 2), par rapport au décès ou à la dépendance, a été significativement supérieure pour le groupe ayant reçu le traitement endovasculaire, comparativement au clippage neurochirurgical.
Plus récemment, l’étude BRAT (Barrow Ruptured Aneurysm Trial), réalisée par des experts en neurochirurgie vasculaire cérébrale, a comparé une exclusion par clip (288 patients) à une embolisation par microspires (233 patients) [11]. Après un an, une réduction du risque absolu de 10,7 % (p = 0,03) a été observée après occlusion endovasculaire par rapport au clippage microchirurgical. À trois ans, cette réduction du risque absolu a été réduite à 5,8 %, sans signification statistique.
La section vasculaire française du département de neurochirurgie vasculaire a inclus 41 patients âgés de plus de 70 ans dans une étude randomisée comparant les deux procédures indiquées. À six mois, le résultat n’a pas été significativement différent entre les deux bras (p = 0,18), bien que la proportion de résultats favorables ait été supérieure après la mise en place de microspires endovasculaires.
ressaignement
L’objectif principal des différents traitements des anévrismes rompus vise à préve-nir une HSA récidivante, entraînant un taux de mortalité connu de 57 % chez ces patients [13].

55
Anévrisme rompu : clips ou microspires ?
L’étude ISAT a fourni un excellent éclairage sur les HSA récidivantes, en fraction-nant leur survenue en trois périodes : avant le traitement, au cours de la première année suivant le traitement et au-delà [3, 9]. Le risque relatif de ressaignement à partir de l’anévrisme cible au cours de la première année a été de 1,15 (IC à 95 % : 0,75 à 1,75) après la mise en place de microspires endovasculaires par rapport au clippage neurochirurgical. Ce résultat non significatif a pris en compte toutes les HSA récidivantes avant et après l’exclusion procédurale.
Au cours de la période pré-interventionnelle, des HSA récidivantes sont surve-nues plus fréquemment dans le bras du clippage (17 dans le bras des microspires vs 28 dans le bras du clippage), sans signification statistique (risque relatif : 0,6 ; IC 95 % : 0,33–1,1]. Dans la mesure où les caractéristiques initiales des deux groupes de traitement étaient appariées, la seule différence significative a été le délai entre la randomisation et l’exclusion de l’anévrisme (1,1 jour pour les microspires vs 1,7 jour pour le clippage) [2]. Cette augmentation du taux de récidive des HSA proportionnellement au délai avant l’exclusion a confirmé le risque majeur des reprises de saignements (qui atteignent environ 2 à 4 % par jour) au cours des quatre premières semaines suivant l’HSA initiale [14].
Après la procédure, le taux de ressaignement à un an a augmenté de manière signi-ficative dans le bras endovasculaire (test du χ2 de Pearson, p = 0,004) par rapport au bras du clippage. Ce taux de ressaignement élevé peut être lié au taux d’occlusions incomplètes après traitement endovasculaire, survenues chez 66 % des patients, contre un taux d’occlusions complètes de 82 % après traitement neurochirurgical, malgré seulement 49 % d’angiographies de contrôle pratiquées dans ce bras.
Au-delà d’un an, le ratio global des HSA récidivantes a diminué. Après un suivi à long terme des séries de l’étude ISAT (minimum de six ans et maximum de 14 ans), 17 patients ont présenté un ressaignement dans le bras endovasculaire par rapport à sept dans le bras du clippage, c’est-à-dire une incidence respective de 0,21 %/an et de 0,09 %/an [9].
Après un suivi de 10 ans, le risque cumulé de ressaignement à partir de l’anévrisme cible (anévrisme rompu initial) a été de 0,0216 pour les patients traités par des microspires endovasculaires et de 0,0064 pour ceux ayant bénéficié d’un clippage neurochirurgical [12].
L’étude BRAT n’a pas recherché les récidives d’hémorragie au cours de la pre-mière année suivant le traitement de l’anévrisme, mais aucune récidive d’HSA n’a été observée au cours de la deuxième ou de la troisième année dans les deux groupes de traitement [11].
Autres résultats de l’étude IsAt
Depuis 2005, les résultats des objectifs secondaires ont été rapportés pour les cohortes ISAT, notamment les résultats cognitifs, le sous-groupe de sujets

Vianney Gilard, Sophie Curey, Éléonore Tollard, Olivier Langlois, François Proust
56
âgés, les coûts et enfin l’extrapolation d’une stratégie globale pour les deux traitements.
L’analyse neuropsychologique a porté sur le sous-groupe N-ISAT issu des popula-tions ISAT de huit centres britanniques participant à ce protocole d’évaluation [15]. Ce sous-groupe a été représentatif des principales cohortes ISAT [16]. Les résultats ont confirmé l’existence commune d’une altération cognitive chez 32,1 % des patients présentant des résultats favorables (échelle modifiée de Rankin : 0–2). En effet, une réduction du risque relatif d’altération cognitive à un an de 31 % (p < 0,005) et une réduction du risque absolu de 12 % ont été observées après traitement endovascu-laire comparativement au clippage microchirurgical. En outre, un plus grand nombre de domaines cognitifs a été altéré dans le groupe neurochirurgical par rapport au groupe endovasculaire, principalement dans les domaines suivants : mémoire ver-bale, vitesse de traitement et aptitudes exécutives. Cette étude, qui a inclus des tests neuropsychologiques validés, a été la plus importante jamais effectuée comprenant une évaluation cognitive complète, contrairement à la sélection abrégée classique pratiquée dans les études randomisées.
L’analyse du sous-groupe des patients âgés de plus de 70 ans a suggéré de façon surprenante que l’avantage était moins élevé avec les microspires qu’avec le clip-page [3]. Cette question est pertinente pour plusieurs raisons : l’allongement de l’espérance de vie entraîne l’inclusion d’un nombre significatif de patients âgés présentant une HSA, l’incidence de l’HSA augmente avec l’âge [17], un traite-ment curatif a été bénéfique dans cette tranche d’âge par rapport à un traitement conservateur, malgré un risque majeur de résultats défavorables [18]. Néanmoins, le sous-groupe n’a pas été préspécifié dans le protocole ISAT, un sous-groupe de 278 patients randomisés âgés de plus de 65 ans a été l’objet d’une deuxième analyse secondaire [19]. Aucune différence n’a été observée en termes de taux d’autono-mie fonctionnelle entre le bras endovasculaire (60,1 %) et le bras neurochirurgical (56,1 %). Toutefois, les patients âgés présentant un anévrisme de l’artère cérébrale moyenne (ACM) et ayant bénéficié d’un clippage neurochirurgical ont montré une autonomie fonctionnelle significativement meilleure à un an que les patients ayant reçu des microspires. Pour les autres localisations, un test du χ² (artère cérébrale antérieure et artère communicante antérieure, p = 0,7 ; artère carotide interne [ACI] et artère communicante postérieure, p = 0,06) n’a pas mis en évidence de différence significative au niveau de l’autonomie fonctionnelle entre les deux bras. De plus, en ajoutant les patients présentant une occlusion de l’artère initiale, une migration des microspires et des problèmes thrombo-emboliques, le taux d’événements thrombo-emboliques a augmenté de manière significative après traitement endovasculaire (p = 0,01), bien qu’un taux inférieur de cas d’épilepsie et de pneumonie ait été observé. Ces résultats suggèrent que le clippage neurochirurgical devrait être le trai-tement privilégié pour les patients âgés présentant un anévrisme rompu de l’artère
57
Anévrisme rompu : clips ou microspires ?
cérébrale moyenne. Cependant, ces résultats ne peuvent pas être considérés comme provenant d’une étude randomisée valide, car le sous-groupe n’était pas initialement spécifié. C’est la raison pour laquelle un groupe de collaboration français a mis en œuvre une étude randomisée (www.clinicaltrial.gouv) comparant des traitements endovasculaire et neurochirurgical chez des patients âgés (≥ 70 ans) présentant des anévrismes rompus [20].
En ce qui concerne le coût du traitement, aucune différence significative à 12 mois n’a été observée entre les deux bras en Australie [21], au Canada [22] ou au Royaume-Uni [23]. Ces trois pays, sur la base des données de leurs patients enrôlés dans l’étude ISAT, ont fait état des mêmes observations : les patients ayant reçu des microspires ont généré des coûts supérieurs pour ce qui concerne les dépenses médicales, mais celles-ci ont été compensées par la réduction des coûts liés à la durée du séjour de la première procédure. Des observations similaires ont déjà été effectuées à la suite d’études rétrospectives [24, 25]. Par conséquent, un changement de paradigme du clippage neurochirurgical vers la mise en place de microspires endovasculaires ne modifie pas les coûts du traitement.
En résumé, l’étude ISAT s’est avérée être bien faite et puissante sur le plan sta-tistique. Sa large population randomisée a fourni un certain nombre de résultats robustes permettant de proposer des recommandations pour la prise en charge de certains types d’anévrismes rompus. Ces différentes publications confirment le rôle essentiel du traitement endovasculaire dans la prise en charge des anévrismes céré-braux rompus. Il apparaît clairement qu’il doit être proposé en première intention, aux patients et à leurs proches, une mise en place précoce de microspires, lorsque le sac anévrismal peut encore être traité par les deux procédures.
en résumé
Au cours des 20 dernières années, des études randomisées ont confirmé que les microspires endovasculaires constituaient une procédure de référence pour le traite-ment des anévrismes, dans la mesure où cette modalité diminue de manière signifi-cative le risque de morbidité et de mortalité par rapport au clippage microchirurgical. De plus, le risque de ressaignement à partir de l’anévrisme cible après 10 ans de suivi reste faible, et n’a pas été responsable d’une augmentation de la morbidité. La recommandation, formulée par une équipe multidisciplinaire composée de neurora-diologues interventionnels et de neurochirurgiens, consistait à proposer en première intention la mise en place de microspires endovasculaires lorsque le sac anévrismal pouvait être traité par les deux procédures [8]. L’impact mondial de l’étude ISAT sur la prise en charge des anévrismes IC explique la prédominance actuelle (47 à 81 %) des microspires endovasculaires [26-29]. La nouvelle génération de médecins en Europe et en Amérique du Nord est donc moins familière de la prise en charge chirurgicale de ces lésions.
Vianney Gilard, Sophie Curey, Éléonore Tollard, Olivier Langlois, François Proust
58
Néanmoins, après un suivi de 5 et 10 ans, aucune différence significative n’a été observée au niveau du taux de survivants autonomes entre le groupe endovasculaire (82 %) et le groupe de neurochirurgie (81 %). Malgré les prédictions alarmistes annonçant la disparition du clippage, censé être remplacé en 2014 par les microspires endovasculaires pour tous les anévrismes IC [30], en 2014 l’exclusion microchirur-gicale reste une modalité thérapeutique appropriée largement proposée à travers le monde [31], et elle est toujours considérée comme faisant partie intégrante de l’arse-nal thérapeutique des anévrismes IC, permettant ainsi de proposer une procédure adaptée à chaque patient. La prise en charge future des anévrismes IC nécessite le développement d’un programme de formation.
AvAncées dAns l’exclusIon mIcrochIrurgIcAle
Depuis le travail neurochirurgical fondamental décrivant le lambeau ptérional fronto-temporal permettant une approche de la partie antérieure du polygone de Willis [32], la procédure microchirurgicale s’est enrichie du concept d’approche mini-invasive et de la surveillance peropératoire par vidéo-angiographie au vert d’indocyanine (ICG). En outre, les procédures de revascularisation cérébrale doivent être intégrées à la prise en charge des anévrismes IC complexes comme étant une technique protectrice et préventive des complications ischémiques.
craniotomie mini-invasive
La craniotomie mini-invasive est une réponse de moyen terme entre un accès par ca-théter fémoral et la craniotomie. Le concept de craniotomie en trou de serrure, décrit par Pernansky et coll. [33], peut s’adapter aux anévrismes IC. Plusieurs options de craniotomie (mini-ptérionale, latérale supra-orbitaire et orbito-ptérionale) ont favo-risé le développement de l’approche supra-orbitaire sous-frontale [34]. L’approche supra-orbitaire est suffisante pour exposer les anévrismes de l’artère communicante antérieure, de l’artère carotide interne et de l’artère cérébrale moyenne ne présentant que peu ou pas de rétraction [35]. La difficulté a été d’obtenir une exposition adé-quate des anévrismes IC. Naturellement, cette craniotomie réduite reste indiquée en l’absence d’hypertension intracrânienne. Après une dissection limitée de la scissure latérale de Sylvius, facilitée par un coton, une chirurgie exovasculaire douce sous grossissement optique permet une incision par clivage de l’anévrisme. Outre cette approche supra-sourcilière, l’approche transcaverneuse transzygomatique prétem-porale a été présentée par Krisht et coll. [36] chez 50 patients atteints d’anévrismes basilaires complexes. Leurs résultats ont été impressionnants, estimant le traitement microchirurgical comme étant dépourvu de mortalité liée à la procédure et condui-sant à un pourcentage de 92 % de patients présentant un score de 0–2 sur l’échelle
59
Anévrisme rompu : clips ou microspires ?
de Rankin modifiée à 6 mois. La dissection du sac nécessite de grandes compétences techniques pour ajouter plusieurs mesures, notamment la résection de la circonvo-lution orbitaire interne, une craniotomie étendue, une dissection interhémisphérique et le contrôle des déchirures du collet de l’anévrisme par la technique du clippage avec coton (cotton-clipping) [37]. En ce qui concerne les techniques de clippage, les procédures ont évolué. Un nouveau concept de clip, basé sur un mécanisme d’ouverture inversé, permet une ouverture plus large des mâchoires du clip et une meilleure vision chirurgicale [38). L’utilisation d’un clip fenêtré peut s’avérer plus sûre dans la mesure où elle minimise la rétraction de la microvascularisation avant le clippage [39].
vidéo-angiographie peropératoire
La surveillance peropératoire concerne le vaisseau parent, mais également la micro-circulation. Une angiographie numérique peropératoire constitue la méthode de choix pour les diagnostics peropératoires de perméabilité vasculaire ou d’occlusion anévrismale, mais il n’est pas réaliste de proposer cette technique à tous les patients sans effectuer une sélection. Ce procédé ne peut pas devenir une méthode standard en raison de son coût élevé, de sa durée, de la nécessité d’un soutien logistique important et de son caractère invasif comportant un risque de complications (0,4 à 2,6 %) [40, 41]. Pour toutes ces raisons, la vidéo-angiographie microscopique au vert d’indocyanine est devenue un examen peropératoire de routine. La vidéo-an-giographie au vert d’indocyanine apporte des informations sur la perméabilité du vaisseau parent et l’existence de résidus anévrismaux. Raabe et coll. [42] ont montré que la sensibilité de la vidéo-angiographie était de 100 % et sa spécificité de 95 % pour le diagnostic d’une sténose de l’artère parent. En outre, cet examen apporte des informations sur les artères perforantes à l’interieur des champs opératoires et contribue à vérifier leur perméabilité [43]. Enfin, elle a été utilisée pour contrôler la perméabilité d’un pontage extracrânien-intracrânien [44]. Cette procédure de contrôle peropératoire est facile à mettre en œuvre, ne prenant en moyenne que deux minutes, et permet une évaluation sûre du résultat post-clippage. Le Doppler microvasculaire peropératoire est une technique fiable permettant d’analyser la vitesse et la turbulence du débit sanguin au cours de la mise en place du clip [45-47]. La débitmétrie Doppler, efficace grâce à sa rapidité et à son faible coût, permet immédiatement de reposer un clip en moins de deux minutes. Une analyse de contraste à granularité laser (laser speckle) permet d’évaluer immédiatement le débit sanguin cortical relatif [48, 49]. Ces procédures d’évaluation sont encore en développement. Enfin, un enregistrement électrophysiologique dans le territoire de l’artère cérébrale moyenne permet de vérifier la microperfusion corticale et l’absence de conséquences ischémiques, son efficacité apparaissant essentiellement dans les

Vianney Gilard, Sophie Curey, Éléonore Tollard, Olivier Langlois, François Proust
60
clippages temporaires [50, 51]. Toutes ces procédures peropératoires doivent être considérées comme complémentaires, et non pas concurrentes [52].
Procédures de revascularisation cérébrale
Ces procédures doivent évoluer vers une protection conceptuelle contre l’ischémie au cours de la prise en charge d’anévrismes IC complexes. Le pontage chirurgical a évolué du pontage extracrânien-intracrânien (EC-IC) vers le pontage intracrâ-nien-intracrânien (IC-IC). Depuis le pontage entre l’artère temporale superficielle et l’artère cérébrale moyenne [32], il s’est développé une deuxième génération de pontage qui utilise des greffons d’interposition veineux ou artériels en réponse aux limitations de flux. Une troisième génération de pontage est entièrement intracrâ-nienne, et utilise d’autres artères intracrâniennes sans mettre à contribution des artères donneuses extracrâniennes. La procédure de revascularisation cérébrale actuellement développée pour l’anévrisme géant ou les tumeurs de la base du crâne repose sur la technique ELANA afin d’éviter un clampage temporaire [53-57].
IndIcAtIon Actuelle du clIPPAge
L’indication du clippage doit être envisagée dans le cadre de la collaboration d’une équipe neurovasculaire, proposant un équilibre des compétences dans les procédures endovasculaires et microchirurgicales. Pour chaque patient, le traitement doit être discuté afin de proposer les modalités optimales adaptées à chaque anévrisme, mais les résultats de l’étude ISAT et les habitudes européennes actuelles ont privilégié les microspires endovasculaires lorsque l’efficacité des deux procédures semble équivalente. Dans ces conditions, le clippage microchirurgical est réservé à l’hyper-tension intracrânienne liée à un hématome intraparenchymateux anévrismal, à des anévrismes complexes, à une dysplasie des bifurcations artérielles, à des anévrismes traités par microspires avec recanalisation ainsi qu’à des anévrismes de grande taille voire géants.
Néanmoins, l’association de critères morphologiques et de certaines caractéris-tiques des patients peut contribuer à la prise de décision. Les critères morphologiques concernent l’approche vasculaire et les caractéristiques de l’anévrisme. L’approche vasculaire peut être problématique en cas d’athérosclérose ou de vaisseaux tortueux ajoutant une difficulté d’accès au sac anévrismal. Les caractéristiques de l’anévrisme peuvent conduire à privilégier l’approche endovasculaire ou microchirurgicale en fonction de la taille du collet ou de la projection contre le fond microvasculaire [58]. Les caractéristiques des patients sont également déterminées par l’âge et les comorbidités. Intuitivement, les microspires endovasculaires devraient préserver les fonctions cognitives dans le segment souche artériel et les artères perforantes,
61
Anévrisme rompu : clips ou microspires ?
notamment l’artère communicante antérieure ou l’artère basilaire. Le clippage pourrait être plus adapté aux anévrismes à base large de l’artère cérébrale moyenne. Enfin, les patients de moins de 40 ans devraient toujours être pris en charge par craniotomie et clippage.
La préservation de l’excellence et le développement de ces stratégies complexes imposent un effort significatif au niveau de la formation des médecins et du personnel paramédical. La section cérébrovasculaire des principales sociétés de neurochirurgie doit mettre en valeur plusieurs approches de formation, notamment la simulation, le partage des compétences, les réseaux de formation internationaux et l’élabora-tion d’un programme de formation commun avec nos confrères neuroradiologues interventionnels.
références
1 Prestigiacomo CJ. Historical perspectives: the microsurgical and endovascular treatment of aneurysms. Neurosurgery 2006;59(5 Suppl 3):S39-47; discussion S3-13.
2 Molyneux A, Kerr R, Stratton I, et al. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet 2002;360 (9342):1267-74.
3 Molyneux AJ, Kerr RS, Yu LM, et al. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 2005;366(9488):809-17.
4 Derdeyn CP, Barr JD, Berenstein A, et al. The International Subarachnoid Aneurysm Trial (ISAT): a position statement from the Executive Committee of the American Society of Interventional and Therapeutic Neuroradiology and the American Society of Neuroradiology. AJNR Am J Neuroradiol 2003;24(7):1404-8.
5 Dormont D, Bonafe A, Cognard C, et al. [What about the ISAT results?]. J Neuroradiol 2003;30(5):286-8.
6 Kirkpatrick PJ, Kirollos RW, Higgins N, Matta B. Lessons to be learnt from the International Subarachnoid Haemorrhage Trial (ISAT). Br J Neurosurg 2003;17(1):5-7.
7 Raabe A, Schmiedek P, Seifert V, Stolke D. German Society of Neurosurgery Section on Vascular Neurosurgery: Position Statement on the International Subarachnoid Hemorrhage Trial (ISAT). Zentralbl Neurochir 2003;64(3):99-103.
8 Albucher JF, Morin-Surroca M. Recommendation about treatment of ruptured cerebral aneurysm: endovascular coiling versus microsurgical clipping. Paris: French National Authority for Health; 2009.
9 Molyneux AJ, Kerr RS, Birks J, et al. Risk of recurrent subarachnoid haemorrhage, death, or dependence and standardised mortality ratios after clipping or coiling of an intracranial aneurysm in the International Subarachnoid Aneurysm Trial (ISAT): long-term follow-up. Lancet Neurol 2009;8(5):427-33.
10 Vanninen R, Koivisto T, Saari T, et al. Ruptured intracranial aneurysms: acute endovascular treatment with electrolytically detachable coils – a prospective randomized study. Radiology 1999;211(2):325-36.

Vianney Gilard, Sophie Curey, Éléonore Tollard, Olivier Langlois, François Proust
62
11 Spetzler RF, McDougall CG, Albuquerque FC, et al. The Barrow Ruptured Aneurysm Trial: 3-year results. J Neurosurg 2013;119(1):146-57.
12 Molyneux AJ, Birks J, Clarke A, et al. The durability of endovascular coiling versus neurosurgical clipping of ruptured cerebral aneurysms: 18 year follow-up of the UK cohort of the International Subarachnoid Aneurysm Trial (ISAT). Lancet 2014.
13 Johnston SC, Dowd CF, Higashida RT, et al. Predictors of rehemorrhage after treatment of ruptu-red intracranial aneurysms: the Cerebral Aneurysm Rerupture After Treatment (CARAT) study. Stroke 2008;39(1):120-5.
14 Bederson JB, Connolly ES, Jr., Batjer HH, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke 2009;40(3):994-1025.
15 Scott RB, Eccles F, Lloyd A, Carpenter K. From multidimensional neuropsychological outcomes to a cognitive complication rate: the International Subarachnoid Aneurysm Trial. Trials 2008;9:13.
16 Scott RB, Eccles F, Molyneux AJ, et al. Improved cognitive outcomes with endovascular coi-ling of ruptured intracranial aneurysms: neuropsychological outcomes from the International Subarachnoid Aneurysm Trial (ISAT). Stroke 2010;41(8):1743-7.
17 de Rooij NK, Linn FH, van der Plas JA, et al. Incidence of subarachnoid haemorrhage: a systema-tic review with emphasis on region, age, gender and time trends. J Neurol Neurosurg Psychiatry 2007;78(12):1365-72.
18 Proust F, Gerardin E, Derrey S, et al. Interdisciplinary treatment of ruptured cerebral aneurysms in elderly patients. J Neurosurg 2010;112(6):1200-7.
19 Ryttlefors M, Enblad P, Kerr RS, Molyneux AJ. International subarachnoid aneurysm trial of neurosurgical clipping versus endovascular coiling: subgroup analysis of 278 elderly patients. Stroke 2008;39(10):2720-6.
20 Proust F, Bracard S, Thines L, et al. [Aneurismal subarachnoid hemorrhage in the elderly subject. Should this patient participate in a randomized clinical trial?]. Neurochirurgie 2010;56(1):67-72.
21 Bairstow P, Dodgson A, Linto J, Khangure M. Comparison of cost and outcome of endovascular and neurosurgical procedures in the treatment of ruptured intracranial aneurysms. Australas Radiol 2002;46(3):249-51.
22 Javadpour M, Jain H, Wallace MC, et al. Analysis of cost related to clinical and angiographic outcomes of aneurysm patients enrolled in the international subarachnoid aneurysm trial in a North American setting. Neurosurgery 2005;56(5):886-94; discussion 94.
23 Wolstenholme J, Rivero-Arias O, Gray A, et al. Treatment pathways, resource use, and costs of endovascular coiling versus surgical clipping after aSAH. Stroke 2008;39(1):111-19.
24 Johnston SC. Effect of endovascular services and hospital volume on cerebral aneurysm treatment outcomes. Stroke 2000;31(1):111-17.
25 Ballet AC, Guerin J, Berge J, et al. [Neurosurgical and endovascular treatment of intracranial aneurysms: a cost analysis of two different strategies at the University Hospital of Bordeaux (France)]. Neurochirurgie 2002;48(5):419-25.
26 Mejdoubi M, Gigaud M, Tremoulet M, et al. Initial primary endovascular treatment in the mana-gement of ruptured intracranial aneurysms: a prospective consecutive series. Neuroradiology 2006;48(12):899-905.
27 Crocker M, Corns R, Hampton T, et al. Vascular neurosurgery following the International Subarachnoid Aneurysm Trial: modern practice reflected by subspecialization. J Neurosurg 2008;109(6):992-7.
28 Cowan JA, Jr., Ziewacz J, Dimick JB, et al. Use of endovascular coil embolization and surgical clip occlusion for cerebral artery aneurysms. J Neurosurg 2007;107(3):530-5.

63
Anévrisme rompu : clips ou microspires ?
29 O’Kelly CJ, Kulkarni AV, Austin PC, et al. The impact of therapeutic modality on outcomes following repair of ruptured intracranial aneurysms: an administrative data analysis. J Neurosurg 2010;113(4):795-801.
30 Maurice-Williams RS. Aneurysm surgery after the International Subarachnoid Aneurysm Trial (ISAT). J Neurol Neurosurg Psychiatry 2004;75(6):807-8.
31 Alshafai N, Cusimano MD, Falenchuk O. Global differences in the present and future manage-ment of cerebral aneurysms. World Neurosurgery 2013;80(6):717-22.
32 Krayenbuhl HA, Yasargil MG, Flamm ES, Tew JM, Jr. Microsurgical treatment of intracranial saccular aneurysms. J Neurosurg 1972;37(6):678-86.
33 Reisch R, Perneczky A. Ten-year experience with the supraorbital subfrontal approach through an eyebrow skin incision. Neurosurgery 2005;57(4):242-55 10.1227/01.NEU.0000178353.42777.2C.
34 Figueiredo EG, Deshmukh V, Nakaji P, et al. An anatomical evaluation of the mini-supraorbi-tal approach and comparison with standard craniotomies. Neurosurgery 2006;59(4 Suppl 2): ONS212-20; discussion ONS20.
35 Park J, Woo H, Kang DH, et al. Superciliary keyhole approach for small unruptured aneurysms in anterior cerebral circulation. Neurosurgery 2011;68(2 Suppl Operative):300-9; discussion 309.
36 Krisht AF, Krayenbuhl N, Sercl D, et al. Results of microsurgical clipping of 50 high complexity basilar apex aneurysms. Neurosurgery 2007;60(2):242-50; discussion 50-2.
37 Barrow DL, Spetzler RF. Cotton-clipping technique to repair intraoperative aneurysm neck tear: A technical note. Neurosurgery 2011;68(2 Suppl Operative):294-9; discussion 299.
38 Krammer MJ, Lumenta CB. The new aneurysm clip system for particularly complex aneurysm surgery: technical note. Neurosurgery 2010;66(6 Suppl Operative):336-8.
39 Zada G, Christian E, Liu CY, Giannotta SL. Fenestrated aneurysm clips in the surgical manage-ment of anterior communicating artery aneurysms: operative techniques and strategy. Clinical article. Neurosurg Focus 2009;26(5):E7.
40 Chiang VL, Gailloud P, Murphy KJ, et al. Routine intraoperative angiography during aneurysm surgery. J Neurosurg 2002;96(6):988-92.
41 Tang G, Cawley CM, Dion JE, Barrow DL. Intraoperative angiography during aneurysm surgery: a prospective evaluation of efficacy. J Neurosurg 2002;96(6):993-9.
42 Raabe A, Nakaji P, Beck J, et al. Prospective evaluation of surgical microscope-integrated intraoperative near-infrared indocyanine green videoangiography during aneurysm surgery. J Neurosurg 2005;103(6):982-9.
43 de Oliveira JG, Beck J, Seifert V, et al. Assessment of flow in perforating arteries during intracra-nial aneurysm surgery using intraoperative near-infrared indocyanine green videoangiography. Neurosurgery 2007;61(3 Suppl):63-72; discussion 73.
44 Woitzik J, Horn P, Vajkoczy P, Schmiedek P. Intraoperative control of extracranial-intra-cranial bypass patency by near-infrared indocyanine green videoangiography. J Neurosurg 2005;102(4):692-8.
45 Marchese E, Albanese A, Denaro L, et al. Intraoperative microvascular Doppler in intracranial aneurysm surgery. Surg Neurol 2005;63(4):336-42; discussion 42.
46 Holscher T, Ozgur B, Singel S, et al. Intraoperative ultrasound using phase inversion harmonic imaging: first experiences. Neurosurgery 2007;60(4 Suppl 2):382-6; discussion 6-7.
47 Amin-Hanjani S, Meglio G, Gatto R, et al. The utility of intraoperative blood flow measure-ment during aneurysm surgery using an ultrasonic perivascular flow probe. Neurosurgery 2008;62(6 Suppl 3):1346-53.
48 Hecht N, Woitzik J, Dreier JP, Vajkoczy P. Intraoperative monitoring of cerebral blood flow by laser speckle contrast analysis. Neurosurg Focus 2009;27(4):E11.
Vianney Gilard, Sophie Curey, Éléonore Tollard, Olivier Langlois, François Proust
64
49 Klein KU, Stadie A, Fukui K, et al. Measurement of Cortical Microcirculation during Intracranial Aneurysm Surgery by Combined Laser-Doppler Flowmetry and Photo-Spectrometry. Neurosurgery 2011.
50 Friedman WA, Chadwick GM, Verhoeven FJ, et al. Monitoring of somatosensory evoked poten-tials during surgery for middle cerebral artery aneurysms. Neurosurgery 1991;29(1):83-8.
51 Penchet G, Arne P, Cuny E, et al. Use of intraoperative monitoring of somatosensory evoked potentials to prevent ischaemic stroke after surgical exclusion of middle cerebral artery aneu-rysms. Acta Neurochir (Wien) 2007;149(4):357-64.
52 Gruber A, Dorfer C, Standhardt H, et al. Prospective comparison of intraoperative vascular monitoring technologies during cerebral aneurysm surgery. Neurosurgery 2011;68(3):657-73; discussion 73.
53 Abla AA, Lawton MT. Anterior cerebral artery bypass for complex aneurysms: an experience with intracranial-intracranial reconstruction and review of bypass options. Journal of Neurosurgery 2014;120(6):1364-77.
54 Bremmer JP, Verweij BH, Klijn CJ, et al. Predictors of patency of excimer laser-assisted nonoc-clusive extracranial-to-intracranial bypasses. Journal of Neurosurgery 2009;110(5):887-95.
55 Vajkoczy P, Korja M, Czabanka M, et al. Experience in using the excimer laser-assisted nonoc-clusive anastomosis nonocclusive bypass technique for high-flow revascularization: Mannheim-Helsinki series of 64 patients. Neurosurgery 2012;70(1):49-54; discussion 55.
56 van Doormaal TP, van der Zwan A, Redegeld S, et al. Patency, flow, and endothelialization of the sutureless Excimer Laser Assisted Non-occlusive Anastomosis (ELANA) technique in a pig model. Journal of Neurosurgery 2011;115(6):1221-30.
57 van Doormaal TP, van der Zwan A, van der Tweel I, et al. Optimization of the excimer laser assisted non-occlusive anastomosis (ELANA) flap retrieval rate. Lasers in Surgery and Medicine 2010;42(5):418-24.
58 Proust F, Debono B, Hannequin D, et al. Treatment of anterior communicating artery aneurysms: complementary aspects of microsurgical and endovascular procedures. J Neurosurg 2003;99(1): 3-14.

65
AVC : nouveautés thérapeutiquesStroke: new therapies© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
Traiter la thrombose veineuse cérébrale
Isabelle Crassard (Paris)
La thrombose veineuse cérébrale a longtemps été considérée comme une patholo-gie rare, de cause souvent infectieuse, de diagnostic très difficile (souvent porté à l’autopsie) et de pronostic extrêmement sombre. Cette perception a beaucoup évolué ces dernières années avec le développement des techniques de neuroradiologie et l’amélioration de la prise en charge thérapeutique.
Bref rappel sur les ThromBoses veineuses céréBrales
Données épidémiologiques
La thrombose veineuse cérébrale atteint des personnes de tous âges, du nouveau-né au vieillard, avec une moyenne d’environ 39 ans dans les grandes séries. Son sex ratio est de 2 à 3 femmes pour un homme avec un pic d’incidence chez la femme jeune en raison de facteurs de risque comme la contraception œstroprogestative et la grossesse.
Son incidence a récemment été évaluée aux Pays-Bas à 1,32 pour 100 000 per-sonnes/an, soit un taux similaire à celui de la méningite bactérienne. [1] Elle est par conséquent beaucoup plus fréquente que ne l’affirmaient les données classiques. En témoignent également les grandes séries récentes pour l’hôpital Lariboisière (inclusion de 450 patients) et la grande étude International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT) (inclusion de 624 cas dans 89 centres et 21 pays). Sa fréquence reste probablement sous-estimée, notamment pour les formes sans AVC.
la thrombose
Siège et étendue variables
La thrombose veineuse cérébrale présente des particularités vis-à-vis de la patho-logie artérielle. Son siège et son étendue sont très variables. Dans les séries ISCVT (n = 624) et Lariboisière (n = 450), l’atteinte concerne fréquemment les sinus latéraux (73 %) et le sinus sagittal supérieur (62–65 %), plus rarement les veines corticales (17–21 %), le système veineux profond (7–11 %) et, exceptionnellement, le sinus caverneux (2 %).
Isabelle Crassard
66
Il est très fréquent (plus de la moitié des cas) que plusieurs sinus et/ou veines soient thrombosé(e)s.
Enfin, en raison de la minceur de leurs parois, les veines corticales peuvent se dilater en cas de thrombose, ce qui entraine fréquemment une inversion de flux et le développement d’une circulation collatérale.
Causes et facteurs favorisants
Les thromboses veineuses cérébrales peuvent survenir dans de nombreuses patho-logies. Dans la série de Lariboisière, les causes peuvent être locales (traumatismes, malformations vasculaires, tumeurs… [9 %]), infectieuses (infections de voisinage ou générales telles que septicémie ou méningite [6,5 %]), liées à des maladies générales (lupus érythémateux systémique, maladie de Behcet, thrombophilies congénitales, coagulopathies, cancers, hémopathies, médicaments… [42 %]) et gynéco-obstétricales (grossesse, post-partum, contraception orale [22,5 %]).
Plusieurs causes ou facteurs favorisants peuvent être associés et un bilan complet est donc nécessaire. Malgré cela, aucun facteur favorisant n’est retrouvé dans 15 à 20 % des cas.
Polymorphisme clinique et évolutif
Les thromboses veineuses cérébrales se caractérisent par leur polymorphisme cli-nique et évolutif. Contrairement aux infarctus artériels, le mode d’installation est le plus souvent variable, sur quelques jours, et débute par une céphalée, présente dans 90 % des cas et pouvant s’associer à un œdème papillaire en cas d’hypertension intracrânienne. Plusieurs grandes présentations cliniques émergent : syndrome focal dans 50 à 80 % des cas, hypertension intracrânienne isolée dans 10 à 40 %, encé-phalopathie subaiguë dans 10 à 20 %. Une atteinte du sinus caverneux va donner des signes locaux neuro-ophtalmologiques.
Les formes inhabituelles représentent 15 à 20 % des présentations cliniques de thromboses veineuses cérébrales avec, par exemple, des signes neurologiques tran-sitoires ou des céphalées isolées.
Diagnostic
Les thromboses veineuses cérébrales étant caractérisées par la diversité de leur étio-logie et de leurs présentations cliniques, associant de façon variable céphalée, déficit focal, crise d’épilepsie, trouble de la conscience, leur diagnostic repose sur les tech-niques de neuroradiologie, en particulier l’IRM cérébrale associée à l’angio-IRM. L’IRM cérébrale montre des modifications de signal du sinus thrombosé. Celui-ci n’est pas visualisé sur les séquences d’AngioRM (cf. figure 1).
Des lésions du parenchyme (œdème diffus, œdème localisé, lésions hémorra-giques plus ou moins importantes) sont présentes dans 40 à 50 % des cas. Elles

67
Traiter la thrombose veineuse cérébrale
sont le plus souvent aspécifiques, rarement évocatrices et l’imagerie du parenchyme apporte surtout une aide au diagnostic différentiel. En revanche, des lésions comme l’atteinte bithalamique en cas de thrombose du système veineux profond et les petites
figure 1. Thrombose du sinus sagittal supérieur.Hypersignal du thrombus en séquence T1 (A) et T2 (B) ; hyposignal en séquence T2* (C) ; non visualisation du sinus sur l’Angio-RM (D).

Isabelle Crassard
68
hémorragies juxtacorticales, souvent bilatérales, sont très évocatrices de thrombose veineuse cérébrale.
Pronostic à 6 mois
Dans les séries Lariboisière et ISCVT, à 6 mois, une guérison complète est observée dans 75 et 46 % des cas respectivement, des séquelles mineures dans 16 et 40 %, des séquelles sévères dans 6 et 7 % et un décès dans 3 et 7 % des cas.
Le pronostic fonctionnel apparaît donc bon chez la majorité des patients et le taux de décès est beaucoup moins élevé que ne l’affirmaient les données classiques. Le décès est principalement causé par l’engagement consécutif à une lésion cérébrale importante, par une complication comme l’état de mal ou l’embolie pulmonaire, ou par la cause sous-jacente comme un cancer, une hémopathie ou une infection grave.
L’évolution à la phase aiguë est extrêmement variable et imprévisible. Un quart des patients s’aggravait à la phase aiguë dans la série ISCVT. Il importe donc d’évoquer le diagnostic de thrombose veineuse cérébrale de façon à mettre en route le traite-ment en urgence en cas de confirmation.
la prise en charge ThérapeuTique De la ThromBose veineuse céréBrale
Nous disposons à présent de recommandations européennes, publiées en 2010, et nord-américaines, publiées en 2011. [2, 3] Le traitement repose sur trois piliers : le traitement antithrombotique par l’héparine, le traitement symptomatique (cépha-lées, hypertension intracrânienne et épilepsie) et le traitement étiologique si besoin (infections, maladies générales).
le traitement antithrombotique
Place de l’héparine
Le traitement de la thrombose veineuse cérébrale par héparine a été longtemps controversé en raison des craintes suscitées par l’existence de formes hémorragiques. Depuis, des séries prospectives et rétroprospectives et deux études randomisées ont clairement établi que ces patients doivent pouvoir bénéficier d’un traitement par héparine.
L’étude Einhäupl publiée en 1991 a évalué l’anticoagulation par héparine intra-veineuse pour le traitement de la thrombose veineuse cérébrale aseptique dans un essai randomisé, contrôlé, en double aveugle, incluant 20 patients (10 héparine, 10 placebo). Il a été arrêté prématurément. Après trois mois, huit des patients trai-tés par héparine avaient complètement récupéré et deux présentaient des déficits neurologiques résiduels légers. Dans le groupe placebo, un patient seulement était

69
Traiter la thrombose veineuse cérébrale
complètement rétabli, six avaient des déficits neurologiques et trois étaient décédés (p < 0,01). Une étude rétrospective supplémentaire a été menée chez des patients atteints de thrombose veineuse cérébrale avec hémorragie intracrânienne. Le taux de décès chez les patients traités par héparine a été de 15 % contre 69 % chez ceux qui n’avaient pas eu le traitement. [4]
L’autre essai multicentrique, contrôlé contre placebo, en double aveugle, publié en 1999, a été mené par le Cerebral Venous Sinus Thrombosis Study Group. Il incluait 59 patients qui ont reçu soit une héparine de bas poids moléculaire (HBPM), soit un placebo pendant 3 semaines. Le traitement par HBPM a été suivi d’une anticoagu-lation orale pendant 3 mois.
Vingt-quatre pour cent des patients du groupe HBPM ont eu une évolution défa-vorable définie comme la mort ou un indice de Barthel inférieur à 15 (différence de risque : –4 % ; IC 95 % : –25–17 % ; NS). Après 12 semaines, 13 % des patients du groupe HBPM et 21 % du groupe placebo avaient eu une évolution défavorable définie comme la mort ou un score de handicap d’Oxford supérieur ou égal à 3 (différence de risque : –7 % ; IC 95 % ; –26–12 % ; NS). Il ne s’est pas produit de nouvelles hémorragies cérébrales symptomatiques. [5]
La méta-analyse des études évaluant l’héparine dans la thrombose veineuse céré-brale montre une réduction de 14 % du risque de décès (IC 95 % : –6–36 %) et de 16 % du risque de décès ou de handicap (IC 95 % : –6–37 %).
En conséquence, les recommandations proposent de traiter les patients atteints de thrombose veineuse cérébrale par héparine, héparine non fractionnée ou HBPM. [2, 3]
Comparaison de l’héparine non fractionnée et des HBPM
Une petite étude randomisée a comparé l’HBPM (n = 34) et l’héparine non frac-tionnée (HNF, n = 32) dans le traitement de la thrombose veineuse cérébrale. Le taux de décès a été de 19 % dans le groupe HNF contre 0 % dans le groupe HBPM. La récupération à trois mois a été plus importante dans le groupe HBPM (88 % vs 62,5 % ) et le taux d’hémorragies sévères a été de 9,5 % dans le groupe HNF contre 0 % dans le groupe HBPM. [6]
Malgré certaines faiblesses de l’étude, ces résultats apparaissent donc en faveur des HBPM.
Dans la série ISCVT, 302 patients ont été mis sous HNF et 119 sous HBPM. La récupération a été meilleure chez les patients traités par HBPM et les taux de décès et de nouvelles hémorragies intracrâniennes tendaient à être plus importants chez les patients sous HNF (cf. tableau 1). [7]
Les données disponibles incitent donc à préférer un traitement par HBPM en l’absence de contre-indication majeure (insuffisance rénale ou indication à un trai-tement chirurgical rapide).
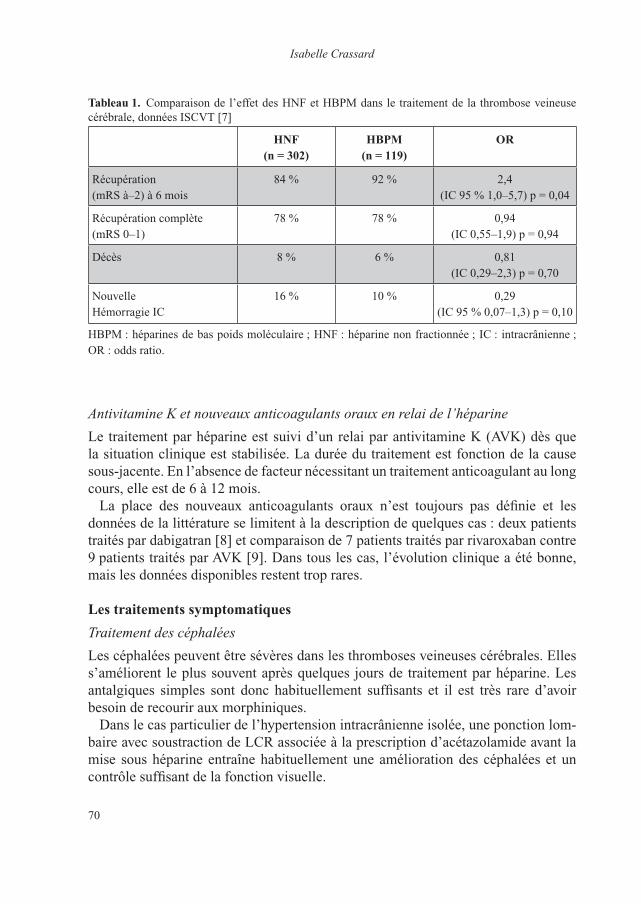
Isabelle Crassard
70
Antivitamine K et nouveaux anticoagulants oraux en relai de l’héparine
Le traitement par héparine est suivi d’un relai par antivitamine K (AVK) dès que la situation clinique est stabilisée. La durée du traitement est fonction de la cause sous-jacente. En l’absence de facteur nécessitant un traitement anticoagulant au long cours, elle est de 6 à 12 mois.
La place des nouveaux anticoagulants oraux n’est toujours pas définie et les données de la littérature se limitent à la description de quelques cas : deux patients traités par dabigatran [8] et comparaison de 7 patients traités par rivaroxaban contre 9 patients traités par AVK [9]. Dans tous les cas, l’évolution clinique a été bonne, mais les données disponibles restent trop rares.
les traitements symptomatiques
Traitement des céphalées
Les céphalées peuvent être sévères dans les thromboses veineuses cérébrales. Elles s’améliorent le plus souvent après quelques jours de traitement par héparine. Les antalgiques simples sont donc habituellement suffisants et il est très rare d’avoir besoin de recourir aux morphiniques.
Dans le cas particulier de l’hypertension intracrânienne isolée, une ponction lom-baire avec soustraction de LCR associée à la prescription d’acétazolamide avant la mise sous héparine entraîne habituellement une amélioration des céphalées et un contrôle suffisant de la fonction visuelle.
Tableau 1. Comparaison de l’effet des HNF et HBPM dans le traitement de la thrombose veineuse cérébrale, données ISCVT [7]
hnf (n = 302)
hBpm (n = 119)
or
Récupération (mRS à–2) à 6 mois
84 % 92 % 2,4 (IC 95 % 1,0–5,7) p = 0,04
Récupération complète (mRS 0–1)
78 % 78 % 0,94 (IC 0,55–1,9) p = 0,94
Décès 8 % 6 % 0,81 (IC 0,29–2,3) p = 0,70
Nouvelle Hémorragie IC
16 % 10 % 0,29 (IC 95 % 0,07–1,3) p = 0,10
HBPM : héparines de bas poids moléculaire ; HNF : héparine non fractionnée ; IC : intracrânienne ; OR : odds ratio.
71
Traiter la thrombose veineuse cérébrale
Traitement des crises épileptiques
Le traitement anticomitial est systématique en cas de crises épileptiques avérées. Le choix thérapeutique doit prendre en compte le risque d’interactions médicamen-teuses avec l’AVK. Il y a un consensus pour l’arrêt du traitement après un an en l’absence de nouvelle crise associée à un EEG normal.
le traitement étiologique
Le traitement étiologique est adapté à la cause sous-jacente lorsque cela est possible. Il est particulièrement important dans les formes septiques nécessitant une antibio-thérapie adaptée à la porte d’entrée, parfois associée à un traitement chirurgical. De même, un traitement spécifique sera nécessaire au cours de certaines maladies générales associées, cancer, hémopathies ou maladies systémiques par exemple.
prise en charge Des formes graves
La prise en charge décrite ci-avant est suffisante dans 90 % des cas. Il subsiste toutefois 10 % de formes graves dont la prise en charge est beaucoup plus difficile.
La gravité de ces formes peut être liée à leur étiologie, par exemple une maladie hématologique grave ou une anémie sévère par saignements chroniques.
Les thromboses veineuses cérébrales peuvent également prendre d’emblée des formes neurologiques graves ou s’aggraver secondairement avec un état de mal épileptique, une embolie pulmonaire…
Traitement chirurgical
Ce traitement peut être proposé chez des patients présentant à la phase aiguë des risques d’engagement cérébral dus soit à une importante lésion du parenchyme cérébral, soit à un œdème cérébral malin.
La décompression chirurgicale a été évaluée dans une étude rétrospective incluant 12 patients. Les formes malignes de thrombose veineuse cérébrale étaient définies comme suit : 1) présence de lésions corticales supratentorielles, 2) signes d’engage-ment clinique (altération de la conscience et dilatation pupillaire) et/ou radiologique, 3) d’emblée ou après aggravation malgré traitement par héparine.
Lors de l’aggravation maligne, tous les patients, sauf un, présentaient des lésions hémorragiques ; la déviation médiane du septum pellucidum était de 12 mm, cinq patients (dont trois ayant été opérés) présentaient une mydriase unilatérale et quatre (dont deux ayant été opérés) une mydriase bilatérale. Huit patients ont subi une décompression chirurgicale, externe (n = 4), externe et interne (n = 3) ou interne (n = 1). Les quatre patients n’ayant pas bénéficié de la décompression chirurgicale sont décédés dans les cinq jours suivant le diagnostic. Un patient opéré est décédé

Isabelle Crassard
72
d’une embolie pulmonaire. Les sept autres ont survécu avec une bonne récupération à 23,1 mois en médiane. [10]
Dans une étude incluant 69 patients (dont 31 cas de la littérature), une hémicra-niectomie décompressive a été effectuée chez 45 patients, une évacuation d’héma-tome chez 7 et les deux chez 17. Au dernier suivi (médiane, 12 mois), 37 % avaient un score de 0 à 1 à la modified Rankin Scale (mRS) et 56,5 % avaient un score mRS de 0 à 2, ce qui est un très bon résultat fonctionnel chez des patients initialement dans un état clinique gravissime. À cette date, 5,8 % étaient vivants avec un score de 4 à 5 et 15,9 % étaient décédés. Trois des neuf patients avec pupilles fixes bilatérales avaient complètement récupéré. [11]
La décompression chirurgicale apparaît ainsi pouvoir sauver des vies avec de bons résultats fonctionnels dans les thromboses veineuses cérébrales malignes.
Thrombolyse endovasculaire
L’utilisation des fibrinolytiques a été proposée dès 1971. Une méta-analyse publiée en 2003 a inclus 72 études, dont aucun essai contrôlé, pour un total de 169 patients. Les patients avaient été traités par urokinase (n = 127) ou activateur tissulaire du plasminogène (rt-PA, n = 37). Une thrombectomie avait été associée chez 16 patients. Leur état clinique était grave (coma : 28 %, encéphalopathie : 52 %, syndrome focal : 7 %, hypertension intracrânienne : 13 %). Trente-trois pour cent avaient une hémorragie à l’imagerie initiale et 31 % une atteinte du système veineux profond. Le pourcentage de patients décédés n’a été que de 6 % seulement et une bonne récupération clinique a été constatée dans 58 % des cas. [12]
Une nouvelle méta-analyse publiée en 2010 a inclus 15 études rétrospectives et prospectives de 5 à 20 patients chacune, pour un total de 156 patients dont 30 % présentaient une hémorragie à l’imagerie initiale. Ils ont été traités par urokinase dans 71 % des cas et par rt-PA dans 29 %. Les auteurs se sont plus particulièrement intéressés aux complications du traitement : hémorragies sévères (9,8 %), nouvelle hémorragie intracrânienne symptomatique (7,6 %), décès (9,2 %) dont la moitié liée à une nouvelle hémorragie. [13]
La place de ce traitement reste donc toujours à évaluer ; il reste réservé aux patients qui s’aggravent ou comateux malgré le meilleur traitement médical. Une étude ran-domisée est en cours, l’étude TO-ACT, dont les résultats devraient être disponibles en 2018. [14]
conclusion
La thrombose veineuse cérébrale est une maladie rare, mais son pronostic est bien meilleur que celui des infarctus artériels. Elle a de nombreuses causes possibles et
73
Traiter la thrombose veineuse cérébrale
une clinique peu spécifique. Le diagnostic doit être très souvent évoqué. Le trai-tement doit être débuté dès confirmation du diagnostic par l’imagerie. La prise en charge repose essentiellement sur l’héparine, même en cas d’hémorragie, associée aux mesures symptomatiques et étiologiques si nécessaire. Des traitements plus agressifs, comme la chirurgie décompressive, peuvent être proposés en cas d’œdème malin. Le traitement endovasculaire peut parfois être discuté mais sa place reste à évaluer.
Bibliographie
1 Coutinho JM, Zuurbier SM, Aramideh M, Stam J. The incidence of cerebral venous thrombosis: a cross-sectional study. Stroke 2012;43:3375-7.
2 Einhäupl K, Stam J, Bousser MG, et al. EFNS guideline on the treatment of cerebral venous and sinus thrombosis in adult patients. Eur J Neurol 2010;17:1229-35.
3 Saposnik G, Barinagarrementeria F, Brown RD, Jr, et al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2011;42:1158-92.
4 Einhäupl KM, Villringer A, Meister W, et al. Heparin treatment in sinus venous thrombosis. Lancet 1991;338:597-600.
5 de Bruijn SFTM, Stam J, for the Cerebral Venous Sinus Thrombosis Study Group. Randomized, Placebo-Controlled Trial of Anticoagulant Treatment With Low-Molecular-Weight Heparin for Cerebral Sinus Thrombosis. Stroke 1999;30:484-8.
6 Misra UK, Kalita J, Chandra S, et al. Low molecular weight heparin versus unfractionated hepa-rin in cerebral venous sinus thrombosis: a randomized controlled trial. Eur J Neurol 2012;19: 1030-6.
7 Coutinho JM, Ferro JM, Canhão P, et al. Unfractionated or low-molecular weight heparin for the treatment of cerebral venous thrombosis. Stroke 2010;41:2575-80.
8 Hon SF, Li HL, Cheng PW. Use of direct thrombin inhibitor for treatment of cerebral venous thrombosis. J Stroke Cerebrovasc Dis 2012;21:915.e11-5.
9 Geisbüsch C, Richter D, Herweh C, et al. Novel factor xa inhibitor for the treatment of cerebral venous and sinus thrombosis: first experience in 7 patients. Stroke 2014;45:2469-71.
10 Théaudin M, Crassard I, Bresson D, et al. Should decompression surgery be performed in mali-gnant cerebral venous thrombosis?: a series of 12 patients. Stroke 2010;41:727-31.
11 Ferro JM, Crassard I, Coutinho JM, et al. Decompression surgery in cerebrovenous thrombosis: a multicenter registry and a systematic review of individual patient data. Stroke 2011;42:2825-31.
12 Canhão P, Falcão F, Ferro JM. Thrombolytics for cerebral sinus thrombosis: a systematic review. Cerebrovasc Dis 2003;15:159-66.
13 Dentali F, Squizzato A, Gianni M, et al. Safety of thrombolysis in cerebral venous thrombosis. A systematic review of the literature. Thromb Haemost 2010;104:1055-62.
14 Coutinho JM, Ferro JM, Zuurbier SM, et al. Thrombolysis or anticoagulation for cerebral venous thrombosis: rationale and design of the TO-ACT trial. Int J Stroke 2013;8:135-40.
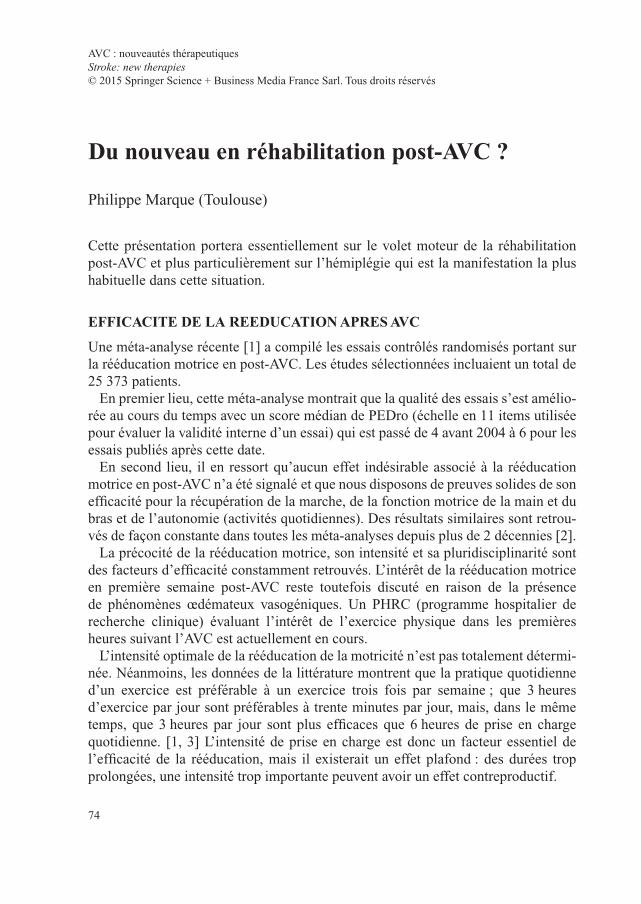
74
AVC : nouveautés thérapeutiquesStroke: new therapies© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
Du nouveau en réhabilitation post-AVC ?
Philippe Marque (Toulouse)
Cette présentation portera essentiellement sur le volet moteur de la réhabilitation post-AVC et plus particulièrement sur l’hémiplégie qui est la manifestation la plus habituelle dans cette situation.
EFFICACITE DE LA REEDUCATION APRES AVC
Une méta-analyse récente [1] a compilé les essais contrôlés randomisés portant sur la rééducation motrice en post-AVC. Les études sélectionnées incluaient un total de 25 373 patients.
En premier lieu, cette méta-analyse montrait que la qualité des essais s’est amélio-rée au cours du temps avec un score médian de PEDro (échelle en 11 items utilisée pour évaluer la validité interne d’un essai) qui est passé de 4 avant 2004 à 6 pour les essais publiés après cette date.
En second lieu, il en ressort qu’aucun effet indésirable associé à la rééducation motrice en post-AVC n’a été signalé et que nous disposons de preuves solides de son efficacité pour la récupération de la marche, de la fonction motrice de la main et du bras et de l’autonomie (activités quotidiennes). Des résultats similaires sont retrou-vés de façon constante dans toutes les méta-analyses depuis plus de 2 décennies [2].
La précocité de la rééducation motrice, son intensité et sa pluridisciplinarité sont des facteurs d’efficacité constamment retrouvés. L’intérêt de la rééducation motrice en première semaine post-AVC reste toutefois discuté en raison de la présence de phénomènes œdémateux vasogéniques. Un PHRC (programme hospitalier de recherche clinique) évaluant l’intérêt de l’exercice physique dans les premières heures suivant l’AVC est actuellement en cours.
L’intensité optimale de la rééducation de la motricité n’est pas totalement détermi-née. Néanmoins, les données de la littérature montrent que la pratique quotidienne d’un exercice est préférable à un exercice trois fois par semaine ; que 3 heures d’exercice par jour sont préférables à trente minutes par jour, mais, dans le même temps, que 3 heures par jour sont plus efficaces que 6 heures de prise en charge quotidienne. [1, 3] L’intensité de prise en charge est donc un facteur essentiel de l’efficacité de la rééducation, mais il existerait un effet plafond : des durées trop prolongées, une intensité trop importante peuvent avoir un effet contreproductif.

75
Du nouveau en réhabilitation post-AVC ?
Enfin, ces grandes méta-analyses insistent sur l’effet d’équipe. Une prise en charge pluridisciplinaire est nécessaire pour permettre l’abord de tous les aspects de la rééducation motrice. Elle implique, de façon coordonnée, kinésithérapeutes, ergothérapeutes, orthophonistes, neurologues et médecins de médecine physique et de réadaptation. [4]
QUELLE EST LA bONNE TEChNIQUE DE RééDUCATION POST-AVC ?
Les techniques de rééducation motrice classiques
Avant les années 2000, la rééducation motrice reposait sur plusieurs techniques empiriques (Bobath, Brunnstrom, Perfetti…) dont les concepts sont très diffé-rents et parfois même opposés. Ainsi, les techniques de Bobath et de Brunnstrom découlent d’approches radicalement opposées. Les efforts physiques, et donc le renforcement musculaire, sont prohibés dans la technique de Bobath, car ils sont supposés renforcer la spasticité. Les réactions réflexes sont inhibées et considérées comme archaïques. À l’inverse, les réactions réflexes sont utilisées et renforcées dans la technique de Brunnstrom car elles sont perçues comme de la motricité élé-mentaire dans cette méthode. Le renforcement de la spasticité qui peut en résulter est considéré comme transitoire et sans retentissement néfaste sur la motricité. Onze essais ont comparé ces différentes méthodes sans qu’aucune n’apparaisse supérieure à l’autre. [3, 5]
De même, le renforcement musculaire, qui est pénalisé dans la technique Bobath, a montré son efficacité chez le sujet hémiplégique avec un gain de force et des bénéfices fonctionnels. [6-8] Il a été démontré dans le même temps qu’il était bien toléré et qu’il n’aggravait pas la spasticité des patients. Cette dernière peut augmen-ter temporairement avec la fatigue au cours de l’exercice, mais cette majoration ne persiste pas au long cours. [9, 10]
En conséquence, s’il existait un consensus des méta-analyses cliniques autour de l’effet positif de la rééducation motrice après AVC, ces différents résultats mon-traient que le type d’exercice ou de technique de rééducation permettant d’obtenir cet effet restait largement méconnu.
Les modèles animaux
Modèle d’environnement enrichi chez le rat
Le modèle d’environnement enrichi consiste à élever des animaux en groupe, dans des cages spacieuses, disposant d’objets divers stimulant la curiosité, les manipula-tions, etc. Un tel milieu, où l’animal peut interagir socialement, favorisant l’explo-ration et un large éventail d’expériences, contribue à augmenter l’activité physique spontanée. Un dispositif de distribution imposant l’utilisation de la patte pour saisir
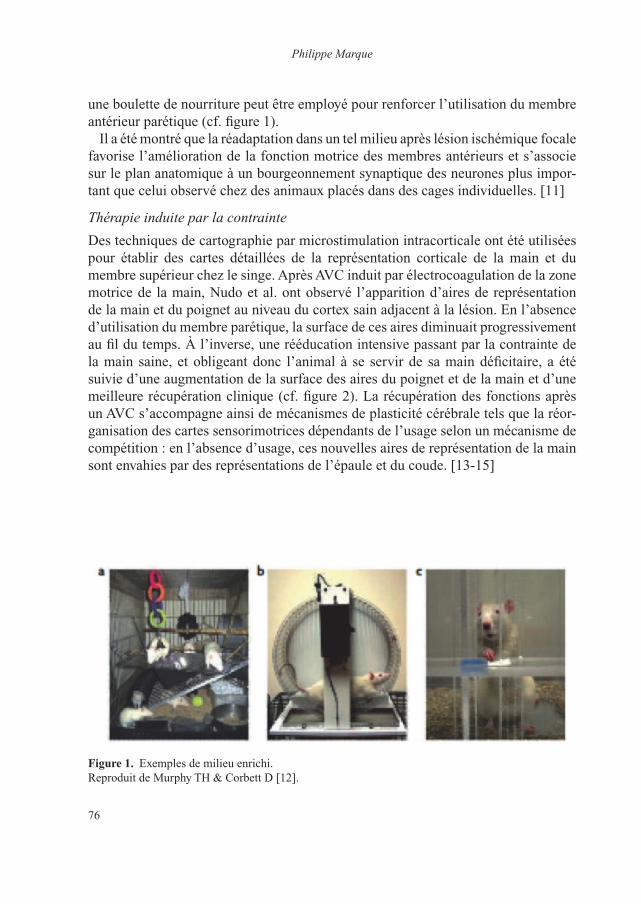
Philippe Marque
76
une boulette de nourriture peut être employé pour renforcer l’utilisation du membre antérieur parétique (cf. figure 1).
Il a été montré que la réadaptation dans un tel milieu après lésion ischémique focale favorise l’amélioration de la fonction motrice des membres antérieurs et s’associe sur le plan anatomique à un bourgeonnement synaptique des neurones plus impor-tant que celui observé chez des animaux placés dans des cages individuelles. [11]
Thérapie induite par la contrainte
Des techniques de cartographie par microstimulation intracorticale ont été utilisées pour établir des cartes détaillées de la représentation corticale de la main et du membre supérieur chez le singe. Après AVC induit par électrocoagulation de la zone motrice de la main, Nudo et al. ont observé l’apparition d’aires de représentation de la main et du poignet au niveau du cortex sain adjacent à la lésion. En l’absence d’utilisation du membre parétique, la surface de ces aires diminuait progressivement au fil du temps. À l’inverse, une rééducation intensive passant par la contrainte de la main saine, et obligeant donc l’animal à se servir de sa main déficitaire, a été suivie d’une augmentation de la surface des aires du poignet et de la main et d’une meilleure récupération clinique (cf. figure 2). La récupération des fonctions après un AVC s’accompagne ainsi de mécanismes de plasticité cérébrale tels que la réor-ganisation des cartes sensorimotrices dépendants de l’usage selon un mécanisme de compétition : en l’absence d’usage, ces nouvelles aires de représentation de la main sont envahies par des représentations de l’épaule et du coude. [13-15]
Figure 1. Exemples de milieu enrichi.Reproduit de Murphy TH & Corbett D [12].
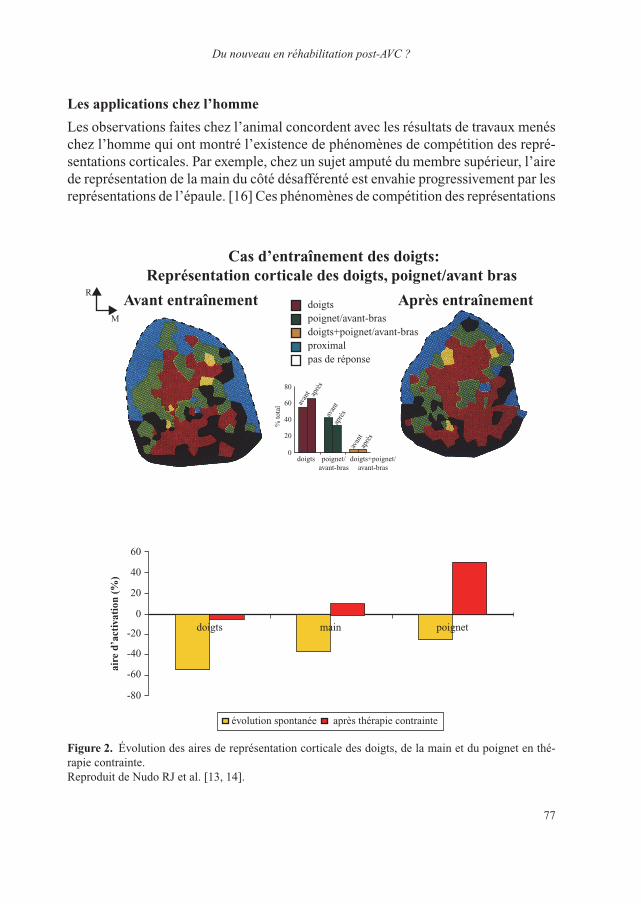
77
Du nouveau en réhabilitation post-AVC ?
Les applications chez l’homme
Les observations faites chez l’animal concordent avec les résultats de travaux menés chez l’homme qui ont montré l’existence de phénomènes de compétition des repré-sentations corticales. Par exemple, chez un sujet amputé du membre supérieur, l’aire de représentation de la main du côté désafférenté est envahie progressivement par les représentations de l’épaule. [16] Ces phénomènes de compétition des représentations
Cas d’entraînement des doigts:Représentation corticale des doigts, poignet/avant bras
Avant entraînement Après entraînementdoigtspoignet/avant-brasdoigts+poignet/avant-brasproximalpas de réponse
R
M
doigts
avan
t
avan
t
avan
t
% to
tal
0
20
40
60
80
poignet/avant-bras
doigts+poignet/avant-bras
aprè
s
aprè
s
aprè
s
doigts
évolution spontanée après thérapie contrainte
aire
d’a
ctiv
atio
n (%
)
-80
-60
-40
-20
0
20
40
60
main poignet
Figure 2. Évolution des aires de représentation corticale des doigts, de la main et du poignet en thé-rapie contrainte.Reproduit de Nudo RJ et al. [13, 14].

Philippe Marque
78
corticales s’installent très rapidement. Les potentiels évoqués moteurs (PEM) au niveau des muscles du bras de sujets normaux avant, pendant et après blocage par ischémie grâce à un garrot de l’avant-bras et de la main ont été enregistrés en vue d’étudier la chronologie des modifications. Les amplitudes des PEM du deltoïde ont rapidement augmenté avec l’installation de l’ischémie puis sont revenues à leur niveau antérieur à l’ablation du garrot. L’augmentation de la taille du PEM du deltoïde était inversement proportionnelle à la diminution de celui de l’abducteur du pouce induite par l’ischémie sous garrot. Dans le même temps, les PEM du bras controlatéral n’ont pas été affectés. [17]
Depuis ces travaux, la thérapie induite par la contrainte est largement employée en réhabilitation post-AVC. Cette méthode a été validée sur des effectifs impor-tants de patients. Ainsi, la cohorte de Taub, randomisée contre placebo, incluant plusieurs centaines de patients, montre une utilisation plus importante dans les activités de la vie quotidienne du membre supérieur parétique dans le groupe traité. [18] Parallèlement, et par mimétisme avec les études chez l’animal, les effets du traitement peuvent être objectivés par les techniques de cartographie par TMS. [19]
Les autres techniques
Le biofeedback par électromyogramme
Le biofeedback par électromyogramme est une technique faisant appel à des élec-trodes positionnées sur les muscles du patient pour générer un signal (visuel ou sonore) de feedback en réponse à l’activation du muscle. Elle bénéficie d’un bon niveau de validation et a un impact démontré sur la récupération après un AVC. [1]
Les robots de rééducation
La principale limite de la thérapie induite par la contrainte est de ne pouvoir s’adres-ser qu’à des malades conservant une fonction motrice résiduelle de bonne qualité, c’est-à-dire incluant une pince pouce index. Des outils permettant de mobiliser le membre paralysé sont nécessaires chez les autres patients. Les robots de rééducation ont ainsi pris une place croissante dans la littérature de réhabilitation au cours de ces quinze dernières années (cf. figures 3 et 4).
Pour les membres supérieurs, les méta-analyses montrent une amélioration du déficit moteur et de la fonction motrice dans les activités de la vie quotidienne. [20]
L’intérêt des robots de rééducation dans la récupération de la marche reste, toute-fois, controversé et les résultats des méta-analyses sont discordants. Les publications les plus récentes montrent que le bénéfice des robots de rééducation est faible chez les patients ayant conservé une déambulation résiduelle. En revanche, le bénéfice est significatif chez les patients totalement privés de marche et ayant bénéficié d’un traitement précoce. [21]

79
Du nouveau en réhabilitation post-AVC ?
Figure 3. Robot de rééducation employé dans la réhabilitation motrice des membres supérieurs [Société Médimex, Sainte-Foy-lès-Lyon, France].
Figure 4. Robot de rééducation employé dans la réhabilitation motrice des membres inférieurs [Société Médimex, Sainte-Foy-lès-Lyon, France].

Philippe Marque
80
LA PéRIODE CRITIQUE
Chez le nouveau-né, il existe des périodes critiques pour les apprentissages (lecture, langage, praxies) au-delà desquelles ceux-ci sont beaucoup plus difficiles. Ces observations peuvent être transposées chez le patient ayant fait un AVC.
Dans un travail clinique faisant appel à un paradigme expérimental utilisant des stimulations magnétiques transcrâniennes qui permettent d’évaluer la plasticité cérébrale chez le sujet hémiplégique, nous avons montré que le cerveau possède de fortes capacités plastiques trois mois après l’AVC, mais que ces capacités diminuent fortement à un an. [22]
Une étude menée chez le rat a évalué l’efficacité sur le résultat fonctionnel et les modifications neuromorphologiques de cinq semaines de réadaptation enrichie initiée au 5ème, 14ème ou 30ème jour après une ischémie focale. L’administration du traitement dès le 5ème jour a été suivie des meilleurs résultats et les possibilités de récupération étaient très diminuées au-delà de 15 jours. Ces données suggèrent qu’en post-AVC, le cerveau possède une sensibilité accrue au traitement de réadaptation précoce, mais que celle-ci diminue avec le temps. Ce phénomène mettrait en jeux des mécanismes facilitateurs et inhibiteurs de la plasticité cérébrale, les mécanismes facilitateurs entrant en action bien plus précocement que les mécanismes inhibiteurs. [23]
Au-delà de cette période, ces résultats ne signifient pas que plus aucune plasticité n’est possible mais que l’on retombe sur les mécanismes de régulation de ce phéno-mène et donc sur ces limites chez l’adulte.
QUE FERONS-NOUS DEmAIN ?
Les stimulations cérébrales
On distingue la stimulation magnétique transcrânienne dite répétitive (rTMS ; repe-titive Transcranial Magnetic Stimulation) et la stimulation transcrânienne à courant continu (tDCS ; transcranial Direct Current Stimulation).
L’utilisation des stimulations électriques s’inscrit dans une approche récente des prises en charge chez le cérébrolésé. L’existence d’une inhibition interhémisphé-rique a été démontrée non seulement au repos [24] mais aussi au cours d’un mou-vement [25]. Murase et al. [25] ont montré que la levée de l’inhibition interhémis-phérique observée chez des sujets sains dans les 20 ms qui précèdent le mouvement était diminuée ou absente chez des sujets hémiplégiques. Ce type de résultats rejoint certaines observations d’imagerie fonctionnelle qui, dans les 15 jours suivant une lésion vasculaire sous-corticale mettaient en évidence une augmentation d’activa-tion du cortex moteur du côté sain et une désactivation du cortex du côté lésé. [26]. Une hypothèse est proposée pour expliquer ces résultats. L’hyperactivation de l’hémisphère sain serait le résultat de la lésion de l’hémisphère controlatéral et de la
81
Du nouveau en réhabilitation post-AVC ?
diminution d’inhibition interhémisphérique qui en résulte. En retour, l’hémisphère sain hyperactivé serait responsable d’une augmentation de l’inhibition de l’hémis-phère lésé et d’une majoration du déficit moteur. Le concept de plasticité inadaptée est proposé pour décrire cette rupture de la balance interhémisphérique.
Si l’on accepte cette hypothèse, les interventions thérapeutiques chez l’hémiplé-gique, que ce soit par rééducation ou par stimulations cérébrales, doivent s’attacher à stimuler l’hémisphère lésé et/ou à inhiber l’hémisphère sain pour restaurer la balance interhémisphérique. Les stimulations cérébrales non invasives sont particulièrement adaptées à ce type de programme.
La rTMS consiste à émettre une série d’impulsions pendant un intervalle de temps donné de façon à modifier durablement l’activité de la région visée. Les post-effets sur l’amplitude des PEM et donc sur l’excitabilité du cortex dépendent de la fré-quence, de la durée et du nombre de stimulations appliquées : les stimulations par rTMS à basse fréquence (1 Hz) ont un effet inhibiteur, alors que les stimulations à haute fréquence ont un effet facilitateur.
La tDCS consiste à appliquer un courant continu de faible intensité au travers de 2 électrodes polarisées : l’électrode positive ou anode et l’électrode négative ou cathode. L’évaluation par PEM permet d’observer une augmentation de l’excitabilité corticale sous l’anode et une diminution de cette excitabilité sous la cathode. [27]
Hummel a mené une étude croisée, en double aveugle, contrôlée contre placebo, en vue de tester l’hypothèse selon laquelle la stimulation non-invasive du cortex moteur pourrait améliorer la fonction motrice dans la main parétique des patients avec AVC en phase chronique. La fonction motrice de la main a été mesurée à l’aide du test Jebsen Taylor hand function Test (JTT). Le JTT de la main parétique a été nettement amélioré avec la tDCS alors qu’il ne l’était pas dans le groupe placebo. Cet effet s’est prolongé au-delà de la période de stimulation. Il a été retrouvé chez tous les patients et était corrélé à une augmentation de l’excitabilité motrice corticale au sein de l’hémisphère atteint, exprimée sous forme de courbes de recrutement accrues et d’une réduction de l’inhibition intracorticale à court intervalle. [28]
De nombreux essais faisant appel à la rTMS ou à la tDCS ont été menés. Un cer-tain nombre d’entre eux sont décevants et n’ont pas montré les bénéfices attendus. Il subsiste de nombreuses questions auxquelles il faudra apporter une réponse comme le type de neuromodulation corticale pouvant être employé (rTMS facilitatrice ou inhibitrice, stimulation magnétique transcrânienne, stimulation associative pairée, tDCS) et les modalités de son utilisation.
Interface cerveau-machine et rééducation
Les interfaces cerveau-machine dites non invasives utilisent l’électro-encé-phalogramme (EEG) dans la suppléance des patients avec un grand handicap. Ces dis-positifs enregistrent l’activité cérébrale produite par une tâche mentale et fournissent

Philippe Marque
82
aux sujets un retour quantitatif et qualitatif de leur activité cérébrale pouvant leur permettre d’apprendre à la contrôler en vue de piloter différentes aides techniques.
L’équipe de Birbaumer, un pionnier de l’interface cerveau-machine, a mené une étude en double aveugle, contrôlée contre placebo, pour évaluer le bénéfice d’un entraînement quotidien avec l’interface cerveau-machine par rapport à la physiothé-rapie seule chez les patients souffrant de parésie sévère.
Trente-deux patients chroniques avec une faiblesse sévère du bras et de la main ont été inclus. Ils devaient tenter d’activer par l’imagination un mouvement d’extension du coude ou des doigts. Deux groupes étaient constitués : le groupe intervention où l’augmentation des fréquences β et µ dans l’activité EEG déclenchaient le fonc-tionnement d’un robot permettant de réaliser le geste choisi et un groupe SHAM où les mouvements du robot étaient indépendants des modifications de l’activité EEG. Les résultats ont été encourageants avec une amélioration du score moteur de Fugl-Meyer du membre supérieur et de l’index de latéralisation en IRMf correspondant à une meilleure activation de l’hémisphère lésé. [29]
L’utilisation des interfaces cerveau-machine en rééducation motrice apparaît comme une voie prometteuse.
CONCLUSION
Les modalités de la réhabilitation en post-AVC évoluent profondément avec une remise en cause des techniques traditionnelles portées par les équipes de kinésithé-rapie. Aujourd’hui, le maître-mot est use it or loose it et de nouveaux outils sont d’ores et déjà ou vont être disponibles.
bibliographie
1 Veerbeek JM, van Wegen E, van Peppen R, et al. What is the evidence for physical therapy posts-troke? A systematic review and meta-analysis. PLoS One 2014;9:e87987.
2 Ottenbacher KJ, Jannell S. The results of clinical trials in stroke rehabilitation research. Arch Neurol 1993;50:37-44.
3 Kwakkel G, van Peppen R, Wagenaar RC, et al. Effects of augmented exercise therapy time after stroke: a meta-analysis. Stroke 2004;35:2529-39.
4 Langhorne P, Bernhardt J, Kwakkel G. Stroke rehabilitation. Lancet 2011;377:1693-702.5 Kollen BJ, Lennon S, Lyons B, et al. The effectiveness of the Bobath concept in stroke rehabilita-
tion: what is the evidence? Stroke 2009;40:e89-97.6 Logigian MK, Samuels MA, Falconer J, Zagar R. Clinical exercise trial for stroke patients. Arch
Phys Med Rehabil 1983;64:364-7.7 Engardt M, Knutsson E, Jonsson M, Sternhag M. Dynamic muscle strength training in stroke
patients: effects on knee extension torque, electromyographic activity, and motor function. Arch Phys Med Rehabil 1995;76:419-25.
8 Sharp SA, Brouwer BJ. Isokinetic strength training of the hemiparetic knee: effects on function and spasticity. Arch Phys Med Rehabil 1997;78:1231-6.
83
Du nouveau en réhabilitation post-AVC ?
9 Brown DA, Kautz SA. Increased workload enhances force output during pedaling exercise in persons with poststroke hemiplegia. Stroke 1998;29:598-606.
10 Smith GV, Silver KH, Goldberg AP, Macko RF. “Task-oriented” exercise improves hamstring strength and spastic reflexes in chronic stroke patients. Stroke 1999;30:2112-18.
11 Biernaskie J, Corbett D. Enriched rehabilitative training promotes improved forelimb motor func-tion and enhanced dendritic growth after focal ischaemic injury. J Neurosci 2001;21:5272-80.
12 Murphy TH, Corbett D. Plasticity during stroke recovery: from synapse to behaviour. Nat Rev Neurosci 2009;10:861-72.
13 Nudo RJ, Milliken GW, Jenkins WM, Merzenich MM. Use-dependent alterations of movement representations in primary motor cortex of adult squirrel monkeys. J Neurosci 1996;16:785-807.
14 Nudo RJ, Wise BM, SiFuentes F, Milliken GW. Neural substrates for the effects of rehabilitative training on motor recovery after ischaemic infarct. Science 1996;272:1791-4.
15 Milliken GW, Plautz EJ, Nudo RJ. Distal forelimb representations in primary motor cortex are redistributed after forelimb restriction: a longitudinal study in adult squirrel monkeys. J Neurophysiol 2013;109:1268-82.
16 Kew JJ, Ridding MC, Rothwell JC, et al. Reorganization of cortical blood flow and transcranial magnetic stimulation maps in human subjects after upper limb amputation. J Neurophysiol 1994;72:2517-24.
17 Brasil-Neto JP, Cohen LG, Pascual-Leone A, et al. Rapid reversible modulation of human motor outputs after transient deafferentation of the forearm: a study with transcranial magnetic stimula-tion. Neurology 1992;42:1302-6.
18 Taub E, Uswatte G, Mark VW, Morris DM. The learned nonuse phenomenon: implications for rehabilitation. Eura Medicophys 2006;42:241-56.
19 Liepert J, Bauder H, Wolfgang HR, et alC. Treatment-induced cortical reorganization after stroke in humans. Stroke 2000;31:1210-16.
20 Mehrholz J, Hädrich A, Platz T, et al. Electromechanical and robot-assisted arm training for improving generic activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst Rev 2012;6:CD006876.
21 Mehrholz J, Elsner B, Werner C, et al. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst Rev 2013;7:CD006185.
22 Castel-Lacanal E, Marque P, Tardy J, et al. Induction of cortical plastic changes in wrist muscles by paired associative stimulation in the recovery phase of stroke patients. Neurorehabil Neural Repair 2009;23:366-72.
23 Biernaskie J, Chernenko G, Corbett D. Efficacy of rehabilitative experience declines with time after focal ischaemic brain injury. J Neurosci 2004;24:1245-54.
24 Ferbert A, Priori A, Rothwell JC, et al. Interhemispheric inhibition of the human motor cortex. J Physiol 1992;453:525-46.
25 Murase N, Duque J, Mazzocchio R, Cohen LG. Influence of interhemispheric interactions on motor function in chronic stroke. Ann Neurol 2004;55:400-9.
26 Loubinoux I, Carel C, Pariente J, et al. Correlation between cerebral reorganization and motor recovery after subcortical infarcts. Neuroimage 2003;20:2166-80.
27 Nitsche MA, Paulus W. Excitability changes induced in the human motor cortex by weak trans-cranial direct current stimulation. J Physiol 2000;527:633-9.
28 Hummel F, Celnik P, Giraux P, et al. Effects of non-invasive cortical stimulation on skilled motor function in chronic stroke. Brain 2005;128:490-9.
29 Ramos-Murguialday A, Broetz D, Rea M, et al. Brain–machine interface in chronic stroke reha-bilitation: a controlled study. Ann Neurol 2013;74:100-8.

84
AVC : nouveautés thérapeutiquesStroke: new therapies© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
Prévenir l’infarctus cérébral
Emmanuel Touzé (Caen)
Quand et comment Prévenir l’infarctus cérébral ?
Soixante-quinze pour cent des accidents vasculaires cérébraux (AVC) sont des pre-miers événements. La prévention primaire est donc essentielle, mais la prévention secondaire est également nécessaire avec un risque de récidive d’environ 3 % à 30 jours, 10 % à un an, 25 % à 5 ans et 40 % à 10 ans. [1]
La prévention doit être adaptée à la cause de l’infarctus cérébral. Les accidents ischémiques (infarctus et accident ischémique transitoire [AIT]) comptent pour 85 % des AVC. Leurs principales causes sont l’athérosclérose (20 %), la maladie des petites artères (25 %) et l’embolie d’origine cardiaque (20 %). Si la prise en charge de ces différents types d’AVC présente de nombreux points communs, elle va toutefois nécessiter la prise en compte de leurs spécificités.
Que l’on se situe en prévention primaire ou secondaire, quelle que soit l’origine de l’événement, la prévention repose sur trois piliers : 1) la prise en charge des facteurs de risque vasculaires, 2) les médicaments anti-agrégants plaquettaires et anticoagu-lants, 3) les techniques de revascularisation chirurgicales ou endovasculaires.
imPortance des facteurs de risQue
Les études épidémiologiques ont montré que dix facteurs de risque expliquent 90 % des infarctus cérébraux : l’hypertension, le tabagisme actif, l’obésité abdo-minale, l’inactivité physique, le diabète, la prise d’alcool, le stress psychologique, la dépression, des cardiopathies (fibrillation atriale [FA], flutter, infarctus du myocarde, maladie valvulaire rhumatismale, prothèse valvulaire) et le rapport apo B/A1. [2]
On distingue classiquement les facteurs de risque non modifiables et modifiables. Les premiers sont l’âge, l’origine ethnique, les facteurs génétiques, le sexe masculin, un petit poids à la naissance. Les seconds sont notamment l’hypertension artérielle (HTA), les cardiopathies, le diabète, les dyslipidémies, la sténose carotidienne, le tabagisme, l’obésité abdominale, l’inactivité physique.

85
Prévenir l’infarctus cérébral
la pression artérielle
L’hypertension artérielle, principal facteur de risque d’AVC
Les études épidémiologiques nous montrent que le facteur de risque majeur des AVC est l’HTA. Le risque augmente de façon continue avec le niveau de pression artérielle (PA). Une méta-analyse de 61 études en population générale incluant un total d’un million de sujets a montré que le risque de premier événement double pour chaque augmentation de 20 mmHg de la PA systolique (cf. figure 1). Une relation identique a été retrouvée pour la PA diastolique. Elle reste valide, quel que soit l’âge, sans qu’un seuil ait été véritablement identifié. [3]
1
2
4
8
16
64
32
128
25680–89 ans
70–79 ans
60–69 ans
50–59 ans
120 140 160 180
Mor
talit
é lié
e au
x A
VC
(R
isqu
e ab
solu
flo
ttan
t)
Pression artérielle systolique habituelle (mmHg)
figure 1. Relation entre la pression artérielle et le risque d’AVC. [3]
Emmanuel Touzé
86
La même relation est retrouvée après un premier AVC et, dans cette situation encore, le niveau de risque de récidive augmente avec le niveau de PA systolique ou diastolique. [4]
Les essais thérapeutiques ont, quant à eux, très largement démontré qu’en préven-tion primaire, faire baisser la PA permet une diminution continue du risque d’AVC : plus la baisse est importante, plus le risque diminue. [5]
Une réduction, même modeste, de la PA au niveau de la population au moyen de l’application systématique de mesures très simples (vigilance pondérale, diminution de la consommation de sel, activité physique, hygiène alimentaire [fruits, légumes, aliments riches en potassium], diminution de la consommation d’alcool) aurait un effet bénéfique très important. Une simple baisse de 5 mmHg de la PA systolique en population générale permettrait d’y réduire de 14 % le risque d’AVC.
En prévention secondaire, il est également largement démontré que faire baisser la PA après un AVC diminue le risque de récidive. [6, 7]
Quel niveau de pression artérielle en prévention secondaire ?
Dans la maladie coronaire, il semble que l’association entre niveau de PA et niveau de risque ait la forme d’une courbe en J avec, pour les pressions artérielles les plus basses, une possible augmentation du risque d’événement. Cette relation ne semblait pas retrouvée avec les AVC et les anciennes recommandations préconisaient, en prévention secondaire, de faire baisser la PA même chez des sujets normotendus, c’est-à-dire dont la PA est inférieure à 140/90 mmHg. Une analyse secondaire d’un grand essai thérapeutique incluant 20 330 patients, PROFESS TRIAL, a toutefois montré qu’en prévention secondaire, il existe une augmentation du risque d’AVC chez les patients ayant une pression artérielle inférieure à 120 mmHg, sans que l’on puisse affirmer un lien de causalité. [8]
Les résultats d’autres études sont cependant en faveur d’une baisse de la pression artérielle chez les sujets ayant une PA normale en prévention secondaire. Ainsi, l’étude SPS3, qui incluait 3 020 patients avec infarctus lacunaires objectivés à l’IRM, a évalué deux niveaux de pression artérielle cible (130–139 mmHg et < 130 mmHg) en prévention secondaire. Ses résultats montrent une diminution (non significa-tive) de l’incidence des récidives d’AVC chez les patients du groupe de PA cible < 130 mmHg (HR : 0,81 ; intervalle de confiance à 95 % : 64–1,03 ; p = 0,08). En revanche, le taux d’hémorragie intracérébrale a été considérablement réduit (HR : 0,37 ; intervalle de confiance à 95 % : 0,15–0,95, p = 0,03). Faire baisser la PA en dessous de 130 mmHg pourrait ainsi être bénéfique dans certaines situations. [9]
Ces résultats sont corroborés par ceux de l’étude ACCORD qui a évalué deux PA cible, inférieure à 120 mmHg et inférieure à 140 mmHg, chez 4 733 diabétiques de type 2. La fréquence annuelle des AVC a été de 0,32 % et 0,53 % respectivement (HR, 0,59 ; intervalle de confiance à 95 % : 0,39–0,89 ; p = 0,01). En revanche, les

87
Prévenir l’infarctus cérébral
taux annuels de décès toutes causes confondues étaient de 1,28 % et de 1,19 % res-pectivement (HR : 1,07 ; intervalle de confiance à 95 % : 0,85–1,35 ; p = 0,55). [10]
En conséquence, les nouvelles recommandations de l’American Heart Association/American Stroke Association (AHA/ASA) préconisent, en prévention secondaire, une baisse de la PA en dessous de 140 mmHg, mais considèrent qu’il est possible, dans certains types d’infarctus cérébraux comme l’accident lacunaire, d’abaisser les chiffres tensionnels en dessous de 130 mmHg. [11]
les dyslipidémies
De nombreuses études épidémiologiques ont montré que le cholestérol est un facteur de risque d’infarctus cérébral. Les essais thérapeutiques évaluant les statines ont permis de montrer très clairement qu’en prévention primaire, plus le LDL-cholestérol est abaissé, plus le risque d’événement vasculaire en général, dont les infarctus cérébraux, est diminué. Une méta-analyse récente a ainsi montré que pour chaque diminution de 1 mmol/l de LDL-cholestérol, le risque d’infarctus cérébral est abaissé de 21 %, quel que soit l’âge et le niveau de risque initial de la personne. [12]
En prévention secondaire, l’étude SPARCL, qui incluait 4 731 patients ayant fait un AVC ou un AIT dans les six mois précédant leur entrée dans l’étude, a également démontré que la diminution du LDL-cholestérol était associée à une baisse de l’ordre de 16 % du risque de récidive d’AVC à six ans (cf. figure 2). [13]
Le bénéfice de la diminution du LDL-cholestérol est donc bien démontré, tant en prévention primaire qu’en prévention secondaire.
En conséquence, les guidelines de l’AHA/ASA préconisent, en prévention primaire, de traiter par des statines tous les patients à haut risque. En prévention secondaire, les statines sont également recommandées chez les patients dont le LDL-cholestérol est à plus de 1 g/l, notamment si l’accident a une origine athéroscléreuse. [11]
De la même façon, la HAS préconise un traitement par statine en cas d’infarctus cérébral ou d’AIT non cardioembolique associé à un LDL-cholestérol supérieur ou égal à 1 g/l. La cible de LDL-cholestérol recommandée est inférieure à 1 g/l. Les patients diabétiques et les patients ayant un antécédent coronarien doivent bénéficier d’un traitement par statine quel que soit le taux de LDL-cholestérol.
Ce traitement est envisageable chez les patients ayant un LDL-cholestérol infé-rieur à 1 g/l et un infarctus cérébral ou un AIT associé à une maladie athéroscléreuse symptomatique. [14]
le diabète
Il est aujourd’hui clair que le contrôle de la glycémie chez le diabétique diminue le risque de complications microvasculaires, cependant le bénéfice sur les complica-tions macrovasculaires reste à démontrer, notamment pour ce qui concerne les AVC.

Emmanuel Touzé
88
Dans cette population, il a été jusqu’à récemment recommandé d’abaisser les chiffres tensionnels en dessous de 120/80 mmHg. À présent, les recommandations préconisent seulement une diminution en dessous de 140/90 mmHg. L’intérêt des statines chez ces patients doit être rappelé. [15]
l’inactivité physique et l’alimentation
Nous disposons d’un grand nombre de données issues d’études observationnelles montrant que l’activité physique intervient dans la prévention de l’AVC. Les guide-lines américaines de 2008 recommandent que les adultes pratiquent une activité phy-sique d’intensité modérée (par exemple, de la marche rapide) au moins 150 minutes par semaine ou une activité physique aérobie d’intensité élevée (par exemple, courir) 75 minutes par semaine ou une association équivalente d’activité physique aérobie d’intensités modérée et élevée.
Les recommandations 2013 de l’AHA/ASA sur les habitudes de vie en prévention du risque cardiovasculaire préconisent la pratique d’une activité physique aérobie pendant au moins 40 minutes au moins 3 à 4 jours par semaine dans le but de réduire la tension artérielle et d’améliorer le profil lipidique.
Pour les patients ayant subi un AVC ischémique ou un AIT et qui en sont capables, au moins trois à quatre séances par semaine d’exercice physique aérobie d’intensité
0 %1 2 3 4 5 6
4 %
8 %
12 %
16 %RR : 16 %
RR ajusté (IC 95 %)’ : 0,84 (0,71–0,99), p = 0,03
11,2 vs. 13,1 % : RAR = 1,9 %
Placebo (2366)
Statine (2365)
Années post-randomisation
AVC Fatal ou non fatal %
figure 2. Bénéfice du traitement hypocholestérolémiant en prévention secondaire des AVC. [13]
89
Prévenir l’infarctus cérébral
modérée à élevée permettent de réduire les facteurs de risque d’AVC. Les séances devraient durer 40 minutes en moyenne.
Pour les personnes souffrant d’un handicap après un AVC ischémique, la supervi-sion par un professionnel de santé tel qu’un physiothérapeute ou un professionnel de la réadaptation cardiaque, au moins à l’initiation du programme d’exercice, peut être envisagée.
Pour ce qui concerne l’alimentation, nous disposons également de nombreuses données issues d’études épidémiologiques et, dans une moindre mesure, d’essais randomisés. Les recommandations 2014 de l’AHA/ASA pour la prévention primaire de l’AVC précisent ainsi que :
– La réduction de la consommation de sodium et l’augmentation de l’apport en potassium sont recommandées pour abaisser la PA (classe I, niveau A).
– Un régime de type DASH, qui met l’accent sur les fruits, les légumes et les produits laitiers peu gras et la réduction des graisses saturées, est recommandé pour abaisser la tension artérielle (classe I, niveau A).
– Une alimentation riche en fruits et légumes, et ainsi riche en potassium, est bénéfique et peut réduire le risque d’accident vasculaire cérébral (classe I, niveau B).
– Un régime méditerranéen complété par des noix peut être envisagé pour la réduction du risque d’AVC (classe IIa, niveau B). [16]
les médicaments antithrombotiQues
Le deuxième pan de la prévention des AVC est représenté par deux grandes familles de médicaments : les antiagrégants plaquettaires pour les accidents non cardioembo-liques, et les anticoagulants pour les accidents cardioemboliques.
les antiagrégants plaquettaires
Le bénéfice des antiagrégants plaquettaires dans la prévention des infarctus cérébraux chez les patients ayant eu un infarctus cérébral ou un AIT est largement démontré. La question du choix de l’antiplaquettaire se pose toutefois. En prévention secondaire, nous disposons de trois options qui peuvent être considérées comme équivalentes : l’aspirine, le clopidogrel et l’association aspirine-dipyridamole. [17]
Des études d’association d’antiplaquettaires ont démontré qu’il n’y avait pas de bénéfice à associer l’aspirine au clopidogrel en raison d’une augmentation du risque hémorragique. En revanche, l’intérêt de cette association en phase aiguë d’accident mineur ou transitoire pour la prévention des récidives est débattu. Les résultats de plusieurs études sont favorables à cette stratégie, notamment une étude chinoise récemment publiée, menée chez 5 170 patients ayant fait un AIT ou un

Emmanuel Touzé
90
infarctus cérébral mineur dans les 24 heures. Ils ont reçu une association clopidogrel + aspirine (clopidogrel à la dose initiale de 300 mg, puis 75 mg par jour pendant 90 jours, plus aspirine à la dose de 75 mg par jour pendant les 21 premiers jours) ou un placebo plus aspirine (75 mg par jour pendant 90 jours). À 90 jours, l’association s’est révélée supérieure à l’aspirine seule pour la prévention des AVC (HR : 0,68 ; IC 95 % : 0,57–0,81 ; p < 0,001) (cf. figure 3). [18] Le traitement est préconisé par les recommandations 2014 de l’AHA/ASA pour la prévention des AVC chez les patients avec AVC et AIT. Il pourrait être proposé sur une courte période mais pas sur le long terme. [11]
les anticoagulants
Les anticoagulants sont essentiellement prescrits dans le contexte de la fibrillation atriale (FA). Cette dernière multiplie par cinq le risque d’infarctus cérébral. C’est une maladie du sujet âgé, la FA touchant moins de 0,5 % des sujets avant 50 ans
0,0
0,00
0,85
0,90
0,95
1,00
0
0
30
30
60
60
90
900,2
0,5
0,6
0,8
1,0
Aspirine
Aspirine
Surv
ivan
ts s
ans
réci
dive
d’A
VC
Jours depuis randomisation
Nb à risque
2586
2584
2307
2376
2287
2361
1906
1989Clopidogrel-aspirine
Hazard ratio, 0,68 (95 % CI, 0,57–0,81)P < 0,001
Clopidogrel-aspirine
figure 3. Intérêt d’une association aspirine + clopidogrel en phase aiguë d’un AIT ou d’un infarctus cérébral mineur. [18]
91
Prévenir l’infarctus cérébral
contre 5 à 15 % après 80 ans. [19] Après 70 ans, 30 % des patients ayant un AVC ischémique sont en FA contre 20 % tous âges confondus. [20] Les infarctus céré-braux liés à la FA sont associés à une mortalité à un mois de 32,5% contre 16,2 % sans FA. [21] Le handicap induit est plus sévère en cas d’infarctus cérébral avec FA versus sans FA. [20]
Nous disposons cependant d’un traitement très efficace avec les anticoagulants oraux. Les nombreuses études réalisées montrent que le traitement anticoagulant diminue de deux tiers (12 % vs 4 %) le risque d’événements emboliques cérébraux (RRR : 66 % ; IC 95 % : 43–80). [22]
Les nouveaux anticoagulants oraux ont été évalués dans de très larges études incluant plus de 10 000 patients. [23, 24] Ils s’avèrent non inférieurs aux AVK pour la prévention des AVC et certains auraient même une petite supériorité vis-à-vis des AVK en termes de prévention des infarctus cérébraux, mais ils présentent sur-tout le grand avantage d’être associés à un moindre risque d’hémorragie cérébrale. [25-29]
la revascularisation
La revascularisation concerne principalement la sténose carotidienne extracrâ-nienne. Celle-ci peut être asymptomatique en situation de prévention primaire, ou symptomatique dans un contexte de prévention secondaire.
La sténose carotidienne est dépistée chez des patients ayant une maladie vasculaire (maladie coronaire, artériopathie oblitérante des membres inférieurs, maladie de l’aorte), étant diabétiques ou ayant fait un AVC ou un AIT dans un autre territoire. La sténose carotidienne est qualifiée de symptomatique, si l’infarctus cérébral ou l’AIT est récent et est survenu dans le territoire de cette sténose.
Les deux situations sont totalement différentes. Grâce aux traitements médicaux disponible (statines, meilleure prise en charge des facteurs de risque en général), le risque d’événement dans le territoire de la sténose est extrêmement faible, inférieur à 1 %, en cas de sténose carotidienne asymptomatique. [30] Celle-ci constitue avant tout un marqueur de risque d’événements vasculaires (événement coronarien, décès d’origine vasculaire supérieur à 2 % par an). Le traitement est essentiellement médi-cal et le bénéfice de la chirurgie est extrêmement faible dans cette situation.
La sténose carotidienne symptomatique est en revanche associée à un risque très élevé de récidive d’événement dans les jours ou semaines qui suivent ce premier événement. [31-33] Dans cette situation, le bénéfice de la chirurgie est important, notamment en cas de sténose supérieure à 70 %. L’angioplastie stenting est une stra-tégie alternative. Elle est associée à un sur-risque de complications (AVC, décès) à court terme mais son efficacité à moyen et long terme est probablement équivalente à celle de la chirurgie.

Emmanuel Touzé
92
l’asPirine en Prévention Primaire
L’aspirine a montré un bénéfice dans la prévention des événements vasculaires, notamment coronariens. [34] Curieusement, l’aspirine est associée à un bénéfice en prévention des événements coronaires chez l’homme alors que ce n’est pas le cas chez la femme. À l’inverse, l’aspirine est associée à un bénéfice en prévention primaire chez la femme, mais pas chez l’homme. En conséquence, les recommanda-tions de l’AHA/ASA pour la prévention primaire des AVC précise qu’il est possible de donner de l’aspirine chez les patients dont le risque vasculaire à 10 ans est supé-rieur à 10 % et qu’elle peut être proposée chez la femme en prévention d’un premier accident ischémique cérébral, en particulier chez les diabétiques. [11]
sPécificités des avc chez la femme
Chez la femme, les AVC sont plus nombreux (en raison de leur plus grande longévité), la morbi-mortalité associée est accrue avec une institutionnalisation plus fréquente. L’HTA est plus souvent en cause chez les plus de 60 ans. [35] Les femmes présentent des facteurs de risque spécifiques (grossesse, facteurs hormonaux, contraception, traitements hormonaux, ménopause précoce, migraine avec aura) et des causes spécifiques comme l’éclampsie. Ces spécificités chez la femme sont à la base de la campagne mondiale menée en 2014 « Je suis une femme, l’AVC me concerne ».
Qu’il s’agisse de patients de sexe masculin ou féminin, la prévention ne présente pas de grosse différence. Le bénéfice de la chirurgie prophylactique est très claire-ment plus faible chez la femme que chez l’homme en cas de sténose carotidienne asymptomatique. La contraception œstroprogestative et le traitement hormonal substitutif sont contre-indiqués après un infarctus cérébral ou un AIT, mais les pro-gestatifs purs sont possibles. L’aspirine peut être proposée en prévention primaire.
conclusion
Les moyens de prévention d’un premier événement ou d’une récidive sont globale-ment identiques, mais le bénéfice absolu va être différent en prévention primaire et en prévention secondaire.
Les progrès dans la prévention ont été majeurs au cours des 30 à 40 dernières années et ont permis une réelle réduction de l’incidence de la maladie, même si le nombre absolu de personnes touchées continue d’augmenter en raison du vieillisse-ment de la population.
Les nombreux facteurs de risque d’AVC sont des variables continues et cela a des implications pour la pratique. Ainsi, il peut être utile de faire baisser les chiffres tensionnels en dessous de la PA cible de façon à réduire encore le risque.

93
Prévenir l’infarctus cérébral
Si les avancées les plus récentes sont modestes, l’application rigoureuse des recommandations actuelles permettrait de réduire le risque d’événement.
bibliographie
1 Mohan KM, Wolfe CD, Rudd AG, et al. Risk and cumulative risk of stroke recurrence: a systema-tic review and meta-analysis. Stroke 2011;42:1489-94.
2 O’Donnell MJ, Xavier D, Liu L, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet 2010;376:112-23.
3 Lewington S, Clarke R, Qizilbash N, et al. Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002;360:1903-13.
4 Rodgers A, MacMahon S, Gamble G, et al. Blood pressure and risk of stroke in patients with cerebrovascular disease. The United Kingdom Transient Ischaemic Attack Collaborative Group. BMJ 1996;313:147.
5 Staessen JA, Wang JG, Thijs L. Cardiovascular protection and blood pressure reduction: a meta-analysis. Lancet 2001;358:1305-15.
6 Liu L, Wang Z, Gong L, et al. Blood pressure reduction for the secondary prevention of stroke: a Chinese trial and a systematic review of the literature. Hypertens Res 2009;32:1032-40.
7 Rashid P, Leonardi-Bee J, Bath P. Blood pressure reduction and secondary prevention of stroke and other vascular events: a systematic review. Stroke 2003;34:2741-8.
8 Ovbiagele B, Diener HC, Yusuf S, et al. Level of systolic blood pressure within the normal range and risk of recurrent stroke. JAMA 2011;306:2137-44.
9 SPS3 Study Group, Benavente OR, Coffey CS, et al. Blood-pressure targets in patients with recent lacunar stroke: the SPS3 randomised trial. Lancet 2013;382:507-15.
10 ACCORD Study Group, Cushman WC, Evans GW, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med 2010;362:1575-85.
11 Kernan WN, Ovbiagele B, Black HR, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014;45:2160-236.
12 Cholesterol Treatment Trialists’ (CTT) Collaborators, Mihaylova B, Emberson J, et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet 2012;380:581-90.
13 Amarenco P, Bogousslavsky J, Callahan A, III, et al. High-dose atorvastatin after stroke or tran-sient ischemic attack. N Engl J Med 2006;355:549-59.
14 HAS. Prévention vasculaire après un infarctus cérébral ou un AIT - Actualisation. Juillet 2014, mise à jour février 2015.
15 American Diabetes Association. Standards of medical care in diabetes—2013. Diabetes Care 2013;36(Suppl 1):S11-66.
16 Meschia JF, Bushnell C, Boden-Albala B, et al. Guidelines for the primary prevention of stroke: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014;45:3754-832.
17 Antithrombotic Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ 2002;324:71-86.
18 Wang Y, Wang Y, Zhao X, et al. Clopidogrel with aspirin in acute minor stroke or transient ische-mic attack. N Engl J Med 2013;369:11-9.

Emmanuel Touzé
94
19 Grau AJ, Weimar C, Buggle F, et al. Risk factors, outcome, and treatment in subtypes of ischemic stroke: the German stroke data bank. Stroke 2001;32:2559-66.
20 Lin HJ, Wolf PA, Kelly-Hayes M, et al. Stroke severity in atrial fibrillation. The Framingham Study. Stroke 1996;27:1760-4.
21 Marini C, De Santis F, Sacco S, et al. Contribution of atrial fibrillation to incidence and outcome of ischemic stroke: results from a population-based study. Stroke 2005;36:1115-19.
22 Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med 2007;146:857-67.
23 Turpie AG. New oral anticoagulants in atrial fibrillation. Eur Heart J 2008;29:155-65.24 Hankey GJ, Eikelboom JW. Antithrombotic drugs for patients with ischaemic stroke and transient
ischaemic attack to prevent recurrent major vascular events. Lancet Neurol 2010;9:273-84.25 Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial
fibrillation. N Engl J Med 2011;365:981-92.26 Connolly SJ, Ezekowitz MD, Yusuf S, et al. Newly identified events in the RE-LY trial. N Engl J
Med 2010;363:1875-6.27 Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial
fibrillation. N Engl J Med 2013;369:2093-104.28 Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrilla-
tion. N Engl J Med 2011;365:883-91.29 RCP Rivaroxaban, 2013.30 Naylor AR. Time to rethink management strategies in asymptomatic carotid artery disease. Nat
Rev Cardiol 2011;9:116-24.31 Blaser T, Hofmann K, Buerger T, et al. Risk of stroke, transient ischemic attack, and vessel
occlusion before endarterectomy in patients with symptomatic severe carotid stenosis. Stroke 2002;33:1057-62.
32 Fairhead JF, Mehta Z, Rothwell PM. Population-based study of delays in carotid imaging and surgery and the risk of recurrent stroke. Neurology 2005;65:371-5.
33 Marnane M, Ni Chroinin D, Callaly E, et al. Stroke recurrence within the time window recom-mended for carotid endarterectomy. Neurology 2011;77:738-43.
34 Antithrombotic Trialists’ (ATT) Collaboration, Baigent C, Blackwell L, et al. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet 2009;373:1849-60.
35 Bushnell C, McCullough LD, Awad IA, et al. Guidelines for the prevention of stroke in women: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014;45:1545-88.
95
AVC : nouveautés thérapeutiquesStroke: new therapies© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
Comment organiser le parcours de santé des patients victimes d’AVC ?
France Woimant (Paris)
Organiser le parcours de santé des personnes victimes d’accidents vasculaires cérébraux (AVC) est un véritable challenge. Il s’agit de planifier la prise en charge d’une pathologie à la fois urgente et chronique, et de plus, extrêmement fréquente et touchant tous les âges. En effet, si l’AVC est plus fréquent après 75 ans, il n’épargne pas l’enfant. Le parcours de santé doit pouvoir s’organiser dans la proximité, au mieux sur le territoire de santé du patient et/ou de son entourage, et ce depuis les actions ciblées de prévention, la phase hospitalière, jusqu’au retour au domicile.
Une pAthologie fréqUente, grAVe et CoûteUse
En France, presque 110 000 personnes sont hospitalisées chaque année pour un AVC [1]. Le nombre de personnes ayant des antécédents d’AVC a été estimé en France à 780 000, à partir des enquêtes déclaratives handicap – santé - ménages et handicap – santé - institution 2008–2009 [2]. Ces enquêtes montrent que deux-tiers des personnes victimes d’AVC gardent des séquelles qui, une fois sur deux, ne leur permettent plus d’effectuer une ou plusieurs activités de la vie quotidienne (telles que manger, marcher, se laver, s’habiller) [2]. Le score de Rankin modifié a été comparé chez les enquêtés selon qu’ils avaient ou non des antécédents d’AVC. Il était supérieur à 2 (correspondant à un handicap qui restreint significativement le mode de vie et/ou empêche une existence totalement indépendante) chez 34,4 % des personnes ayant un antécédent d’AVC (28 % des personnes vivant au domicile et 87,8 % de ceux en institution), versus 3,9 % des personnes sans antécédents d’AVC (3,1 % de ceux vivant à domicile et 71,6 % de ceux vivant en institution) [3]. Ces enquêtes montrent également que les personnes lourdement dépendantes avec un Rankin à 5 (correspondant à un Handicap sévère entraînant une dépendance totale et nécessitant une supervision permanente ) ont dans presque un quart des cas un antécédent d’AVC. Ces quelques chiffres montrent la sévérité de l’AVC qui reste la première cause de handicap acquis de l’adulte.
Ces séquelles participent largement au poids financier de l’AVC pour l’assurance maladie et la société. Les dépenses sanitaires et médicosociales annuelles liées à
France Woimant
96
l’AVC sont considérables, estimées en 2007 à 8,3 milliards d’euros : 5,9 milliards pour le secteur de soins (3 % des dépenses totales) et 2,4 milliards d’euros pour le secteur médico-social. En 2004, la dépense moyenne annuelle par patient en affection de longue durée (ALD) « accident vasculaire cérébral invalidant » était estimée à 9 642 euros (soit 14 % de plus qu’un patient sous ALD pour maladie d’Alzheimer) [4]. En 2007, le coût moyen des cas incidents d’AVC était estimé à 16 686 euros par patient durant la première année et le coût annuel des cas préva-lents à 8 099 euros par patient, ce coût variant avec l’importance des séquelles et du handicap [5].
Un pArCoUrs de sAnté des pAtients qUi débUte pAr lA préVention
La prévention reste la meilleure stratégie pour réduire l’incidence et les consé-quences des AVC. Le dépistage et le traitement des facteurs de risque sont les principaux éléments de cette prévention de l’AVC et de l’ensemble des maladies vasculaires (maladie coronarienne, artériopathie oblitérante des membres inférieurs, insuffisance rénale...). Les actions de prévention concernent tous les âges, depuis les enfants (actions dans les écoles) jusqu’aux personnes âgées et doivent être multicul-turelles pour s’adapter à tous. Les actions ciblées de prévention de l’AVC peuvent être aidées par des actions d’éducation thérapeutique menées en ambulatoire (par exemple sur l’hypertension artérielle, principal facteur de risque de l’AVC) ; ces actions sont d’autant plus aisées à mettre en place, que proposées à proximité du domicile du patient.
le pArCoUrs hospitAlier des AVC
A la phase aiguë, où chaque minute compte, l’organisation de la prise en charge doit également se faire dans la proximité, au mieux au sein des unités neuro-vas-culaires (UNV). Cent-quarante UNV sont programmées dans le cadre du plan AVC 2010–2014 ; elles ne seront, malheureusement pas toujours localisées à moins de 30 minutes du lieu de survenue de l’AVC. Aussi, la prise en charge initiale des AVC peut également être réalisée dans des établissements disposant de services d’urgences, situés à proximité du lieu de survenue de l’AVC. Ces établissements doivent disposer de personnel formé à l’AVC au sein des services d’urgences et de radiologie, d’un plateau de neuro-imagerie disponible en urgence 24h/24 et 7j/7 et d’outils de télémédecine adaptés [6]. Dans ces établissements disposant de services d’urgences mais n’ayant pas d’UNV, le traitement initial est décidé par urgentiste et neurologue après une visio-consultation et un transfert de la neuro-imagerie. Une fois le traitement initié, le patient est transféré en UNV.

97
Comment organiser le parcours de santé des patients victimes d’AVC ?
Après la phase aiguë, 30 % des patients sont transférés en soins de suite et de réadaptation [7] ; cette période qui dure le plus souvent plusieurs semaines est particulièrement difficile psychologiquement et ne doit donc pas éloigner le patient de son entourage [8]. De plus, le retour au domicile sera plus facile à organiser par un établissement de proximité qui aura une meilleure connaissance des ressources médico-sociales et sociales locales. Le retour au domicile, appuyé sur une hospitali-sation de jour, ne peut s’organiser que si l’établissement est à proximité du domicile du patient.
le retoUr AU domiCile
La prise en charge de l’AVC ne s’arrête pas à la sortie de l’hôpital, mais doit prendre en compte le retour et le maintien du patient au domicile ce qui amène à considérer la coordination ville – hôpital. Le retour au domicile est un moment difficile pour le patient et son entourage, qui réalisent le bouleversement qu‘a entraîné l’AVC dans la vie quotidienne, dans la vie familiale et professionnelle.
De nombreux éléments vont conditionner le maintien au domicile des patients. Parmi eux :
• le degré de handicap physique et cognitif,• la survenue de complications,• la participation de l’entourage,• la formation des aidants,• le soutien psychologique du patient et des différents intervenants.
Il est indispensable au décours de l’AVC d’organiser un suivi coordonné entre les acteurs de recours et les professionnels de proximité afin de prévenir les récidives, les complications et la perte d’autonomie. Une coopération est donc nécessaire entre les professionnels de soins et d’accompagnement [9] :
• professionnels de santé libéraux (médecin généraliste, neurologue, infirmier, kinésithérapeute, orthophoniste, ergothérapeute, psychologue, assistante sociale …),
• professionnels de santé des centres experts,• professionnels :
– des structures et services pour personnes handicapées : services d’accom-pagnement médico-social pour adultes handicapés (SAMSAH), services d’accompagnement à la vie sociale (SAVS), maisons départementales des personnes handicapées (MDPH)… ;
– des structures et services pour les personnes âgées dont les maisons pour l’autonomie et l’intégration des malades Alzheimer (MAIA), les centres
France Woimant
98
locaux d’information et de coordination (CLIC), les équipes médico- sociales de l’allocation personnalisée d’autonomie (APA) ;
– des organismes compétents dans la réorganisation du domicile,
• auxiliaires de vie, aides ménagères,• aidants…
de noUVelles orgAnisAtions se mettent en plACe poUr fACiliter le mAintien AU domiCile :
les équipes d’évaluation pour améliorer l’interface ville – hôpital
• Les évaluations pluriprofessionnelles post AVC hospitalières permettent de réaliser à distance de l’accident une évaluation pluriprofessionnelle par une équipe spécialisée dans la pathologie neuro-vasculaire et ce, en lien avec les professionnels libéraux. Les objectifs de cette évaluation sont : – faire le point sur la maladie vasculaire, les facteurs de risque vasculaire et
assurer la meilleure prévention secondaire ; – réaliser un bilan physique afin de définir un programme de suivi personnalisé ; – dépister les troubles de l’humeur (la dépression est très fréquente au décours
de l’AVC) ; – déterminer les capacités de réinsertion sociale et professionnelle ; – apprécier la qualité de vie du patient, celle de l’entourage et voir si les
aidants ont besoin d’un soutien ; – proposer, si nécessaire, un programme d’éducation thérapeutique ; – informer sur les associations de patients.
Ces évaluations s’adressent donc à tous les patients, y compris ceux n’ayant pas ou peu de séquelles afin de repérer des déficiences passées jusqu’alors inaperçues, mais pouvant être sources de handicaps et d’une désadaptation professionnelle et/ou sociale.
• Les équipes mobiles de soins de suite et réadaptation AVC, mises en place à titre expérimental dans quelques régions dont l’Île-de-France, interviennent principalement pour des prises en charge ponctuelles, dans des situations où les difficultés rencontrées peuvent compromettre le maintien au domicile. Elles sont composées de médecin, ergothérapeute, assistante sociale intervenant au domicile ou en institution. Leurs missions sont d’améliorer le maintien au domicile (évaluation des patients et des aidants), de préparer si nécessaire les hospitalisations et de prévoir ensuite le retour à domicile voire d’éviter des hospitalisations inutiles. Les évaluations sont réalisées en lien avec les profes-sionnels libéraux et les structures médico-sociales
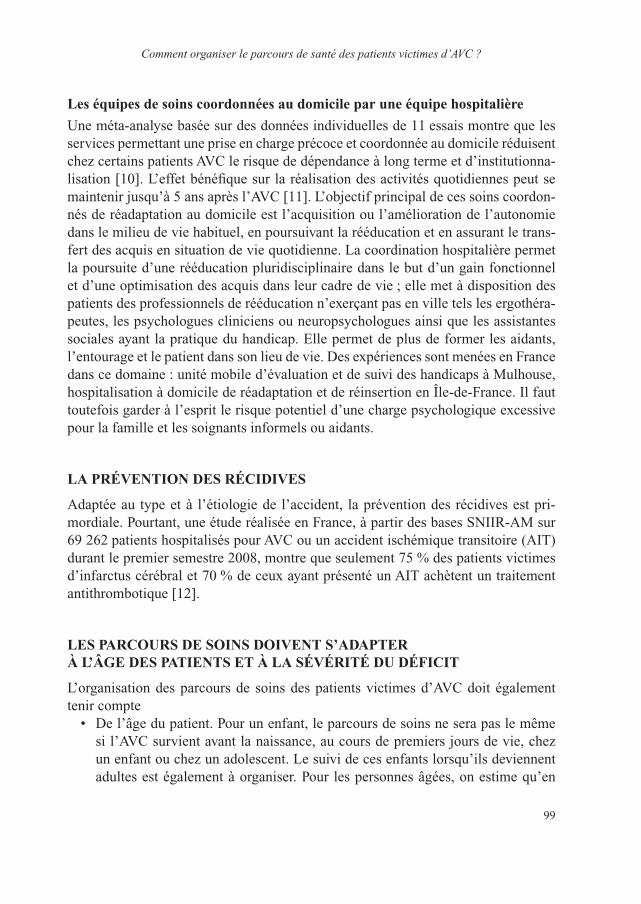
99
Comment organiser le parcours de santé des patients victimes d’AVC ?
les équipes de soins coordonnées au domicile par une équipe hospitalière
Une méta-analyse basée sur des données individuelles de 11 essais montre que les services permettant une prise en charge précoce et coordonnée au domicile réduisent chez certains patients AVC le risque de dépendance à long terme et d’institutionna-lisation [10]. L’effet bénéfique sur la réalisation des activités quotidiennes peut se maintenir jusqu’à 5 ans après l’AVC [11]. L’objectif principal de ces soins coordon-nés de réadaptation au domicile est l’acquisition ou l’amélioration de l’autonomie dans le milieu de vie habituel, en poursuivant la rééducation et en assurant le trans-fert des acquis en situation de vie quotidienne. La coordination hospitalière permet la poursuite d’une rééducation pluridisciplinaire dans le but d’un gain fonctionnel et d’une optimisation des acquis dans leur cadre de vie ; elle met à disposition des patients des professionnels de rééducation n’exerçant pas en ville tels les ergothéra-peutes, les psychologues cliniciens ou neuropsychologues ainsi que les assistantes sociales ayant la pratique du handicap. Elle permet de plus de former les aidants, l’entourage et le patient dans son lieu de vie. Des expériences sont menées en France dans ce domaine : unité mobile d’évaluation et de suivi des handicaps à Mulhouse, hospitalisation à domicile de réadaptation et de réinsertion en Île-de-France. Il faut toutefois garder à l’esprit le risque potentiel d’une charge psychologique excessive pour la famille et les soignants informels ou aidants.
lA préVention des réCidiVes
Adaptée au type et à l’étiologie de l’accident, la prévention des récidives est pri-mordiale. Pourtant, une étude réalisée en France, à partir des bases SNIIR-AM sur 69 262 patients hospitalisés pour AVC ou un accident ischémique transitoire (AIT) durant le premier semestre 2008, montre que seulement 75 % des patients victimes d’infarctus cérébral et 70 % de ceux ayant présenté un AIT achètent un traitement antithrombotique [12].
les pArCoUrs de soins doiVent s’AdApter à l’âge des pAtients et à lA séVérité dU défiCit
L’organisation des parcours de soins des patients victimes d’AVC doit également tenir compte
• De l’âge du patient. Pour un enfant, le parcours de soins ne sera pas le même si l’AVC survient avant la naissance, au cours de premiers jours de vie, chez un enfant ou chez un adolescent. Le suivi de ces enfants lorsqu’ils deviennent adultes est également à organiser. Pour les personnes âgées, on estime qu’en

France Woimant
100
2020, presque 30 % des personnes hospitalisées pour AVC auront plus de 85 ans, les parcours s’organisent en lien avec les filières gériatriques
• De la sévérité des AVC : l’organisation de la prise en charge des accidents ischémiques transitoires est bien différente de celle des AVC sévères [13]. Pour les AVC sévères admis initialement en réanimation, peuvent se discuter des décisions : – de limitations de soins, – de prélèvements d’organes (l’AVC est la cause principale de décès en mort
encéphalique), – d’admissions en services de soins palliatifs, – d’admissions en services de rééducation post réanimation, – d’admissions en unités de soins de longue durée, – d’hébergements permanents ou temporaires en structures médicosociales :
maison d’accueil spécialisé (MAS), foyer d’accueil médicalisé (FAM), en établissement d’hébergement pour personnes âgées dépendantes (EHPAD).
Comment Coordonner et Animer Ce pArCoUrs de sAnté des AVC
Les infirmières «coordinatrices» dans le parcours des AVC sont encore trop peu nombreuses. Pourtant, leur rôle est primordial lors du retour au domicile des patients victimes d’AVC. Leurs principales missions sont d’améliorer l’observance au traitement (médicamenteux et de rééducation), d’apprendre aux patients et à leur entourage les symptômes évocateurs de complications, qui lorsqu’elles surviennent, majorent encore le handicap. Ces infirmières appellent les patients après leur retour au domicile et/ ou participent à la consultation de suivi du neurologue. Elles sont un lien entre les professionnels de ville et de l’hôpital [14].
En cohérence avec le plan AVC 2010–2014, les animateurs de filières AVC contri-buent à construire un parcours de santé de qualité pour les victimes d’AVC. Leurs principales missions sont de :
– développer et coordonner la filière AVC autour des UNV, afin d’assurer la conti-nuité des soins, en améliorant les circuits hospitaliers et en organisant les liens avec la ville, le secteur médico-social et les associations de patients ;
– accroître la formation de l’ensemble des professionnels intervenant dans la filière ;
– mener sur chaque territoire des actions d’information pour le grand public.
En conclusion, la prise en charge du patient atteint d’accident vasculaire cérébral ne se limite pas à l’hospitalisation en phase aigüe en unité neuro vasculaire puis,

101
Comment organiser le parcours de santé des patients victimes d’AVC ?
si nécessaire, en services de soins de suites et de réadaptation. C’est l’ensemble du parcours de santé du patient victime d’un AVC qu’il faut organiser et planifier avec le malade, son entourage et de nombreux professionnels. Ce parcours doit pouvoir s’organiser dans la proximité, au mieux sur le territoire de santé. Structurer l’organi-sation territoriale de la prise en charge des AVC permet d’éviter des «ruptures» dans le parcours de santé des personnes victimes d’AVC, ruptures qui se soldent trop souvent par une hospitalisation en urgence dans un établissement peu adapté pour prendre en charge le problème. De nouvelles organisations se mettent en place dont l’enjeu est d’augmenter le nombre de patients pris en charge dans les filières AVC, en lien avec les professionnels libéraux, l’objectif étant de réduire le handicap post-AVC, et d’améliorer la qualité de vie des patients et de leur entourage. Sans oublier la prévention, qui reste la meilleure stratégie pour réduire le handicap lié aux AVC.
références
1 de Peretti C, Nicolau J, Tuppin P, et al. Evolutions de la prise en charge hospitalière des accidents vasculaires cérébraux en court séjour et en soins de suite et de réadaptation entre 2007 et 2009 en France. Presse Med 2012;41:491-503.
2 de Peretti C, Grimaud O, Tuppin P, et al. Prévalence des accidents vasculaires cérébraux et de leurs séquelles et impact sur les activités de la vie quotidienne: apports des enquêtes déclaratives Handicap-santé-ménages et Handicap-santé-institution. Bull Epidemiol Hebd 2012;1:1-6.
3 Schnitzler A, Woimant F, Tuppin P, de Peretti C. Prevalence of self-reported stroke and disability in the French adult population: a transversal study. PLoS One 2014;9(12):e115375.
4 Fery-Lemonnier E. Rapport ministériel sur la prévention et la prise en charge des accidents vasculaires cérébraux en France. Juin 2009.
5 Chevreul K, Durand-Zaleski I, Gouépo A, et al. Cost of stroke in France. Eur J Neurol 2013;20: 1094-100.
6 Circulaire N°DGOS/R4/R3/PF3/2012/106 du 6 mars 2012 relative à l’organisation des filières régionales de prise en charge des patients victimes d’accident vasculaire cérébral (CVA).
7 de Peretti C, Nicolau J, Holstein J, et al. Hospitalisations en soins de suite et de réadaptation en France après un accident vasculaire cérébral survenu en 2007. BEH 2010; 49-50:501-6.
8 Brainin M, Olsen TS, Chamorro A, et al. Organization of stroke care: education, referral, emergency management and imaging, stroke units and rehabilitation. European Stroke Initiative. Cerebrovasc Dis 2004;17(Suppl 2):1-14.
9 Gache K, Leleu H, Nitenberg G, et al. Main barriers to effective implementation of stroke care pathways in France: a qualitative study. BMC Health Serv Res 2014;14:95.
10 Langhorne P, Taylor G, Murray G, et al. Early supported discharge services for stroke patients: a meta-analysis of individual patients’ data. Lancet 2005;365:501-6.
11 Thorsén AM, Holmqvist LW, de Pedro-Cuesta J, von Koch L. A randomized controlled trial of early supported discharge and continued rehabilitation at home after stroke: five-year follow-up of patient outcome. Stroke 2005;36:297-303.
12 Moysan TV, de Peretti S, Woimant F. Caractéristiques et traitements des assurés du régime général hospitalisés pour accident vasculaire cérébral au cours du premier semestre 2008. Rev Neurol 2008;169:126-35.

France Woimant
102
13 Woimant F, Biteye Y, Chaine P, Crozier S. Severe stroke: which medicine for which results? Ann Fr Anesth Reanim 2014;33:102-9.
14 Cortes E, Woimant F. L’éducation du patient post-accident vasculaire cérébral. STV 2007;19:492-4.

Stroke: new therapies


105
Stroke: new therapiesAVC : nouveautés thérapeutiques© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
Cerebrovascular accidents
Pierre Godeau
Devoting a meeting to stroke perfectly fits into the ongoing work at Institut Servier. In fact, most of the themes over recent years have addressed the consequences of ageing, and stroke is all the more frequent with advancing age. With an incidence of 150,000 cases a year in France and a prevalence of about 500,000, stroke represents a major public health issue. Stroke often causes death or has sequelae that cause disability or loss of independence, with extended hospitalisation possible, imposing a considerable burden on health care resources.
Moreover, we cannot ignore the impact of personal loss of cognitive function— even dementia—following a stroke that was apparently mild. Reactional depression is a common consequence, along with resulting upheaval for the family unit.
Diverse factors determine prognosis, which varies hugely from one subject to another after a stroke but it is reassuring to observe that there has been significant improvement due to more timely and more effective management, especially in spe-cial Stroke Units. In addition, advances in re-education techniques have significantly attenuated the impact of sequelae. However, coordination across the country remains irregular and weak so logistical access-to-care deficiencies are far from resolved.
A precise assessment of possible solutions assumes an exact classification of cerebrovascular accidents (CVAs), which is addressed by Marie-Germaine Bousser who was the lynchpin in organising this meeting. Her question is “One cerebro-vascular accident or many”. She reminds us that CVAs can be assigned to one of five different categories with, broadly speaking, 5% due to meningeal haemorrhage, 15% to cerebral haemorrhage, 0.5% to cerebral venous thrombosis and transient ischaemic attack (TIA) or cerebral infarction accounting for 78%. The last two are grouped together because, despite their disparate evolution, they represent a continuum and both require urgent, specific management.
Of course, it is impossible to cover in just one day everything about stroke and certain topics have been deliberately left out of today’s programme, such as what to do when confronted by an embolic CVA in a young patient with patent foramen ovale (PFO). This has long been controversial with cardiologists tending to want to operate and neurologists being more reserved. Three prospective studies suggested that closing the communication is ineffective but two multicentre, meta-analytical studies published since the end of 2013 go a long way to resolving this controversy:

Pierre Godeau
106
the first was French [1] and compared 1,224 operated patients versus 1,226 medi-cally treated controls; the second, an American study, involved 1,150 treated patients and 1,143 controls after randomisation. Both came to the same conclusions, namely that the previous studies had lacked power and the number of accidents analysed was insufficient to allow any valid conclusions. In contrast, the two more recent studies provide solid evidence of the benefit of percutaneous PFO closure with a reduction of about one-third in the risk of recurrence. Nevertheless, a small increase in the risk of atrial fibrillation was detected in both studies and this should not be ignored. For that reason, the French Close Study is being continued and this will lead, one can hope, to the issuance of specific recommendations in coming months.
This leads to some general considerations on progress in medicine and communi-cation between different disciplines. In 2014 when we are celebrating the centenary of the Great War, it is useful to review the idea of the “Balkanisation” of medicine, which had seemed out-dated and incomprehensible to the young generations but is back in fashion. This picture points up the fragmentation of medicine into a series of competing specialisms; this is not a defect although specialisms are sometimes hostile to one another and inwardly focused on a small area of interest. Distinction should be made between this attitude and the subdivision of each specialism of organs lead-ing to the indispensable acquisition of greater knowledge and optimal adaptation of diverse modern methods to an increasingly narrow field—an irreversible trend that is essential for progress. In parallel, a return to the globalisation of medicine would seem to be indispensable and complementary—rather than counter—to hyperspe-cialisation. Thus, improving CVA management depends as much on progress on prevention and eliminating risk factors, as identified in the multicentre Interstroke Study [3], a case-control study conducted in 22 countries, which focused on factors somewhat different to the cardiac and coronary factors evaluated in the Interheart Study. In any case, progress is ensured with the development of knowledge about diabetes, improvements in metabolic and dietary issues as well as the management of hyperlipidaemia, hypertension, peripheral and coronary artery disease, systemic diseases, the fight against smoking and drinking, problems related to arrhythmia and better control of clotting function (to maintain a balance between the risks of thrombosis and haemorrhage), which can only be a subject of individual reflection and would unproductively encumber this meeting’s programme, which is already heavily loaded.
Let us just remember that managing atrial fibrillation (AF) can considerably reduce the risk of thromboembolic stroke. According to the Ecole Cardiologique de Bordeaux directed by Michel Haissaguerre, 1% of people have atrial fibrilla-tion, i.e. 600,000 people in France and 4–5 million across Europe. Even higher figures—750,000 in France—were reported recently by Jean-Marc Davy et al. at the recent European Society of Cardiology Conference in Barcelona [4] together with an

107
Cerebrovascular accidents
estimate that this figure will have doubled by 2050. Assuming that atrial fibrillation underlies 20% of CVAs and that 30% of patients with AF show no symptoms, it is important to raise the consciousness of general practitioners with respect to detect-ing AF, and they ought to be ready to seek specialist advice from a cardiologist if they are in the least doubt. Without ignoring the controversies related to the latest anticoagulants, which will be resolved when a suitable, routine laboratory test is available, mention could be made of the development of obliteration techniques, which 300,000 people underwent in 2013. The indications for such techniques are growing exponentially (currently by more than 20% a year). Another way of preventing stroke and peripheral embolization related to AF involves occluding the left atrium with a nickel-titanium device that deploys like a tiny umbrella after inser-tion via a trans-septal approach with transoesophageal endoscopic guidance. This Watchman device was assessed in the prospective American multicentre PROTECT AF study: results after 3.8 years of follow-up—published this very day in JAMA [5]—demonstrate its superiority over warfarin in non-valvular AF.
Consolidation and extension of such advances will prolong life expectancy and, in particular, improve life expectancy in good health, so dear to our colleague Jean-Pierre Michel. However, we should not forget the risk—limited but growing—of vasoconstrictor-induced CVA, associated with the use of methamphetamine (not yet widespread), nasal vasoconstrictors that are of dubious therapeutic value and have proved risks and, most importantly, cocaine that multiplies the risk of CVA in people aged between 15 and 49 by a factor of 6 or 7, as reported recently by our colleagues in Baltimore [6].
I have already spoken for too long and it is time to hear from Marie-Germaine Bousser, who will quickly go over today’s programme before Michel Haguenau moderates this morning’s session. Marie-Germaine will take over in the afternoon and, at the end of the day, she will review the conclusions from this meeting, which I hope will teach us all a great deal.
References
1 Beygui F, Labombarda F, Sabatier R, et al. A meta-analysis of randomized trials comparing percutaneous closure of patent foramen ovale to medical therapy. ESC Congrès 2013; abstract 90273.
2 Renfigo-Moreno P, et al. Patent foramen ovale transcatheter closure vs. medical therapy on recurrent vascular events: a systematic review and meta-analysis of randomized controlled trials. Eur Heart J 2013;34:3342-52.
3 O’Donnell MJ, et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 coun-tries (the INTERSTROKE study): a case control study. Lancet 2010;376:112-23.
4 Davy JM, et al. The French screening campaign of atrial fibrillation in general practice assess-ment of predictive criteria for atrial fibrillation. ESC Congress, Barcelona 2014; abstract 4876.

Pierre Godeau
108
5 Reddy VY, Severt H, Halperin J, et al. Percutaneous left atrial appendage closure vs warfarin for atrial fibrillation – A randomized clinical trial. JAMA 2014;312(19):1988-98.
6 Cheng G(Y-C) et al. Illicit cocaine use and risk of ischemic stroke: the stroke prevention in young adults study. International Stroke Conference, 12-14 February 2014; abstract.

109
Stroke: new therapiesAVC : nouveautés thérapeutiques© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
Treating acute cerebral ischaemia
Sonia Alamowitch (Paris)
1995: birTh of Thrombolysis
In 1995, the National Institute of Neurological Disorders and Stroke (NINDS) pub-lished an article that established the evidence in favour of intravenous (IV) throm-bolysis with recombinant tissue plasminogen activator (rt-PA) in the treatment of acute-phase cerebral infarction. Compared with patients given placebo, those given IV rt-PA within three hours of the onset of symptoms of stroke had a 30% better chance of recovering without sequelae after three months [1].
Some ten years later, the ECASS 3 Study showed that IV thrombolysis is effective over a slightly longer window, up to four-and-a-half hours after the first symptoms [2].
PhysioPaThology of cerebral infarcTion: The ischaemic Penumbra
Both of the above-mentioned studies showed that timing is essential for effective IV thrombolysis. Ischaemic stroke is a dynamic phenomenon. Occlusion of the artery and the resultant interruption of the blood supply distress brain tissue in the territory supplied by the vessel concerned. In the middle of this territory, cerebral ischaemia soon causes necrosis and irreversible functional impairment. Around this lesion there is a patch called the “ischaemic penumbra”, which is compromised for several hours and which can eventually become necrotic. However, the tissue remains viable for a while and it can be rescued if the blood supply is restored in time. The aim of therapeutic intervention is therefore to try to restore blood supply to the ischaemic patch by unblocking the artery and saving the tissue in the ischaemic penumbra. The earlier this is achieved, the greater the chance of success.
Time is brain
A meta-analysis covering nearly 6,000 patients was published in 2014. This confirms that IV thrombolysis is effective up to four-and-a-half hours after the
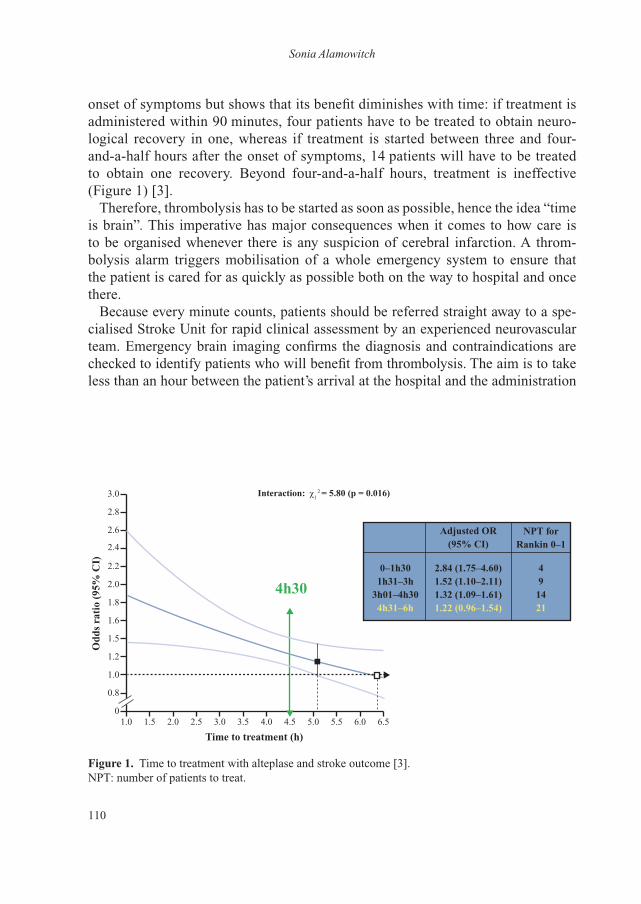
Sonia Alamowitch
110
onset of symptoms but shows that its benefit diminishes with time: if treatment is administered within 90 minutes, four patients have to be treated to obtain neuro-logical recovery in one, whereas if treatment is started between three and four-and-a-half hours after the onset of symptoms, 14 patients will have to be treated to obtain one recovery. Beyond four-and-a-half hours, treatment is ineffective (Figure 1) [3].
Therefore, thrombolysis has to be started as soon as possible, hence the idea “time is brain”. This imperative has major consequences when it comes to how care is to be organised whenever there is any suspicion of cerebral infarction. A throm-bolysis alarm triggers mobilisation of a whole emergency system to ensure that the patient is cared for as quickly as possible both on the way to hospital and once there.
Because every minute counts, patients should be referred straight away to a spe-cialised Stroke Unit for rapid clinical assessment by an experienced neurovascular team. Emergency brain imaging confirms the diagnosis and contraindications are checked to identify patients who will benefit from thrombolysis. The aim is to take less than an hour between the patient’s arrival at the hospital and the administration
1.00
0.8
1.0
1.2
1.5
1.6
1.8
2.0
2.2
2.4
2.6
2.8
3.0
1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0 5.5 6.0 6.5
Odd
s ra
tio
(95%
CI)
Time to treatment (h)
Interaction: χ12 = 5.80 (p = 0.016)
4h30
Adjusted OR (95% CI)
NPT for Rankin 0–1
0–1h301h31–3h
3h01–4h304h31–6h
491421
2.84 (1.75–4.60)1.52 (1.10–2.11) 1.32 (1.09–1.61)1.22 (0.96–1.54)
figure 1. Time to treatment with alteplase and stroke outcome [3].NPT: number of patients to treat.

111
Treating acute cerebral ischaemia
of IV thrombolysis, referred to as “door-to-needle time”. This race against time necessitates tight coordination between the emergency services (ambulance, etc.) and the neurovascular team.
Major effort is required in terms of organisation at the hospital and coordination with the radiology department and the emergency services. An American study published in 2011 covering 25,504 stroke victims administered rt-PA between 2003 and 2009 showed that door-to-needle time was less than an hour for only 26.6% of patients although the trend was positive since the percentage rose from 19.5% in 2003 to 29.1% in 2009 [4].
access To TreaTmenT
Time to treatment
It is vital that patients arrive at the hospital as soon as possible. For this, they them-selves have to be able to recognise the symptoms of stroke, which is the reason for current media campaigns based on the message “If you experience sudden weakness on one side of the body, call an ambulance straight away”. This assumes that the emergency services will be able to identify stroke victims and take them straight to a Stroke Unit. Some centres in France are trying out the idea of tele-thrombolysis: if a patient is picked up by an ambulance far from any Stroke Unit, a remote neurovas-cular expert oversees the neurological work-up (tele-consultation) and evaluates the radiological results (remote image transfer); the expert can then give the green light for thrombolytic treatment with a minimum of time lost.
reconsider the contraindications
Although rt-PA has been licensed for the treatment of acute cerebral infarction since 2002 in Europe, only 5% of stroke victims receive it—the only modality with demonstrated efficacy in the acute phase. One of the great challenges for the coming years is to raise this percentage.
One possible avenue for improvement would be to review the contraindications to rt-PA. Initially, many patients were denied treatment because of a fear of cerebral bleeding.
After 20 years of experience and the accumulation of information, some of the contraindications seem to be unwarranted and reconsidering them could already increase the fraction of victims that might benefit up to 20% [5-8].
Patients over 80
Thrombolysis is not licensed for patients over 80, a population that accounts for more than 30% of strokes. These patients were excluded from the early clinical trials
Sonia Alamowitch
112
because of the increased risk of cerebral haemorrhage on antithrombotic drugs. The randomised IST3 (International Stroke Trial) Study compared IV rt-PA with placebo in 3,035 patients, including 1,617 over 80 year-olds. This showed that benefit was significantly greater in this elderly sub-population if the drug was administered within three hours of the onset of symptoms (p = 0.027) [9].
The American guidelines no longer contraindicate IV thrombolysis within three hours in patients of over 80 [10] and this should happen in Europe soon. Caution is indicated in the next part of the window—between three hours and four-and-a-half hours—which is a relative contraindication to be weighed up in the light of other relative contraindications.
Rapid improvement in symptoms
Thirty per cent of patients with a cerebral infarction who show spontaneous improvement within a matter of hours of the onset of symptoms or who only ever show mild symptoms will have significant residual disability three months later (mRankin ≥ 2). The risk of secondary deterioration is particularly high if the artery remains occluded, causing permanent damage in the ischaemic penumbra [11-13].
For this reason, if an artery is blocked, rt-PA treatment should be started even if the NIHSS score is 4 or under, and even if there is spontaneous regression of the symptoms.
Indication for IV thrombolysis: one patient in two is borderline
An excellent article published in 2013 in Brain emphasised that, while thrombolysis is indubitably indicated in a quarter of patients with a cerebral infarction in the hyper-acute phase and indubitably contraindicated in another quarter, half of all pa-tients are borderline, necessitating assessment of the benefit-risk balance for bleed-ing on the basis of a MRI-MRA scan of the tandem state of the cerebral parenchyma/vascular permeability.
The list of contraindications to thrombolysis is shrinking with time and the follow-ing ten should be amended:
– patients over 80 and under 18, – pregnant women, – epileptic seizure at the beginning of the stroke, – severe deficit (NIHSS >25) without extended infarction observed on a brain
MRI scan, – minor or improving deficit with arterial occlusion detected by imaging, – diabetes or a history of stroke, – recent, small cerebral infarction, – small, asymptomatic intracranial aneurysm, – anti-vitamin K treatment or INR <1.7,
113
Treating acute cerebral ischaemia
– cerebral infarction on waking after MRI confirmation of the time of the infarction [14].
limitations of thrombolysis
IV thrombolysis is not always effective. It often fails to achieve sustained de-occlu-sion of a large or medium-calibre artery, especially the common basilar artery, the M1 segment of the common carotid artery and the internal carotid artery. In these situations, unblocking either fails or works initially with subsequent re-occlusion (observed in 34% of cases) [15].
The artery can be unblocked by directly intervening on the intra-arterial clot in the course of arteriography (interventional neuroradiology). Both chemical throm-bolysis and mechanical thrombectomy are options. Mechanical modalities include thrombo-aspiration and removal with a stent retriever. The currently preferred thera-peutic strategy is called bridging therapy, which involves IV thrombolysis followed by a procedure to unblock the artery. This approach has been compared with IV thrombolysis in a series of randomised studies [16-18]. The first studies showed that endovascular embolectomy was no better than IV thrombolysis, but in 2014 the randomised CLEAN trial provided evidence that this therapeutic modality was of benefit. In this Dutch study, standard treatment (IV rt-PA) was compared to a com-bination of IV thrombolysis + endovascular embolectomy in 500 carefully selected patients who were treated very early (within 6 hours). The results clearly show the superiority of combined treatment (OR: 1.65; 95% CI: 1.21–1.30) but it is important to note that the median time to thrombectomy was extremely short (four-and-a-half hours) [19, 20]. More clinical trial results are expected in 2015.
oTher ways of TreaTing acuTe-Phase cerebral infarcTion
anticoagulants
Anticoagulants were in fashion thirty years ago in this indication but therapeutic trials have shown that they bring no benefit in the acute phase and have but few indications (low level of evidence).
antiplatelet drugs
Aspirin
Studies from over ten years ago showed that administering aspirin in the acute phase of cerebral infarction slightly reduced the risk of recurrence (which is known to be likely in the days after a first cerebral infarction) (OR: 0.77; 95% CI: 0.69–0.87; p ≤ 0.05) [21].

Sonia Alamowitch
114
Combinations of antiplatelet drugs
A meta-analysis of 12 randomised trials covering a total of 3,766 patients compared aspirin on its own with combinations of aspirin + dipyridamole and aspirin + clopi-dogrel. Compared with aspirin alone, combination with an antiplatelet drug slightly reduced the risk of recurrence (OR: 0.67; 95% CI: 0.49–0.93) although bitherapy was associated with a statistically insignificant rise in major bleeding events (OR: 2.09; 95% CI: 0.86–5.06) [22].
Combinations of antiplatelet drugs could be of benefit in the very early stages of a transient ischaemic attack (TIA) or a minor cerebral infarction. A placebo-controlled, randomised, double-masked study in China was conducted on 5,170 patients who had had a minor infarct or a high-risk TIA in the last 24 hours. They were given either a combination of clopidogrel + aspirin (clopidogrel at an initial daily dosage of 300 mg then 75 mg for 90 days + aspirin at a daily dosage of 75 mg for the first 21 days) or placebo + aspirin (75 mg a day for 90 days). After 90 days, the combina-tion proved more effective than aspirin alone at preventing cerebrovascular accidents (CVA) (HR: 0.68; 95% CI: 0.57–0.81; p<0.001). Moderate-to-severe bleeding was seen in 0.3% of patients in each group [23].
This study shows that, in the acute phase, bitherapy is more effective than mono-therapy at preventing CVA recurrence with a positive benefit-risk ratio. This opens up an avenue for the treatment of minor cerebral infarctions or TIAs in the acute phase. Five different therapeutic trials comparing aspirin and combinations of anti-platelet drugs in these indications are currently under way.
conclusion
By virtue of IV thrombolysis, it might now be possible to “cure” nearly 40% of patients with cerebral infarction in the stage of progressive damage. IV thromboly-sis has to be started as soon as possible: the challenge for the coming years is to arrive at treating as many patients as possible as quickly as possible. Endovascular techniques are opening up promising therapeutic perspectives and these will prob-ably constitute a new weapon in tomorrow’s arsenal for the treatment of certain patients in the acute stage. Finally, administering combinations of antiplatelet drugs in the acute stage of a minor ischaemic accident could reduce the risk of full-blown cerebral infarction.
115
Treating acute cerebral ischaemia
references
1 The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995;333:1581-7.
2 Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med 2008;359:1317-29.
3 Emberson J, Lees KR, Lyden P, et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet 2014;384:1929-35.
4 Fonarow GC, Smith EE, Saver JL, et al. Timeliness of tissue-type plasminogen activator therapy in acute ischemic stroke: patient characteristics, hospital factors, and outcomes associated with door-to-needle times within 60 minutes. Circulation 2011;123:750-8.
5 De Keyser J1, Gdovinová Z, Uyttenboogaart M, Vroomen PC, Luijckx GJ. Intravenous alteplase for stroke: beyond the guidelines and in particular clinical situations. Stroke 2007;38:2612-18.
6 Tong D. Are all IV thrombolysis exclusion criteria necessary? Being SMART about evidence-based medicine. Neurology 2011;76:1780-1.
7 Demaerschalk BM. Challenging the validity of imposing contraindications to thrombolysis for acute ischemic stroke. Neurology 2011;77:1862-3.
8 Wardlaw JM, Murray V, Berge E, et al. Recombinant tissue plasminogen activator for acute ischaemic stroke: an updated systematic review and meta-analysis. Lancet 2012;379:2364-72.
9 IST-3 collaborative group, Sandercock P, Wardlaw JM, et al. The benefits and harms of intra-venous thrombolysis with recombinant tissue plasminogen activator within 6 h of acute ischae-mic stroke (the third international stroke trial [IST-3]): a randomised controlled trial. Lancet 2012;379:2352-63.
10 Jauch EC, Saver JL, Adams HP Jr, et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013;44:870-947.
11 Rajajee V, Kidwell C, Starkman S, et al. Early MRI and outcomes of untreated patients with mild or improving ischemic stroke. Neurology 2006;67:980-4.
12 Nedeltchev K, Schwegler B, Haefeli T, et al. Outcome of stroke with mild or rapidly improving symptoms. Stroke 2007;38:2531-5.
13 Smith WS, Schwab S. Advances in stroke: critical care and emergency medicine. Stroke 2012;43:308-9.
14 Balami JS, Hadley G, Sutherland BA, Karbalai H, Buchan AM. The exact science of stroke thrombolysis and the quiet art of patient selection. Brain 2013;136:3528-53.
15 Alexandrov AV, Grotta JC. Arterial reocclusion in stroke patients treated with intravenous tissue plasminogen activator. Neurology 2002;59:862-7.
16 Broderick JP, Palesch YY, Demchuk AM, et al. Endovascular therapy after intravenous t-PA versus t-PA alone for stroke. N Engl J Med 2013;368:893-903.
17 Paciaroni M, Inzitari D, Agnelli G, et al. Intravenous thrombolysis or endovascular therapy for acute ischemic stroke associated with cervical internal carotid artery occlusion: the ICARO-3 study. J Neurol 2014. [Epub ahead of print]
18 Kidwell CS, Jahan R, Gornbein J, et al. A trial of imaging selection and endovascular treatment for ischemic stroke. N Engl J Med 2013;368:914-23.
19 Fransen PS, Beumer D, Berkhemer OA, et al. MR CLEAN, a multicenter randomized clinical trial of endovascular treatment for acute ischemic stroke in the Netherlands: study protocol for a randomized controlled trial. Trials 2014;15:343.

Sonia Alamowitch
116
20 Berkhemer OA, Fransen PS, Beumer D, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med 2015;372:11-20.
21 Sandercock P, Gubitz G, Foley P, Counsell C. Antiplatelet therapy for acute ischaemic stroke. Cochrane Database Syst Rev 2003;(2):CD000029.
22 Geeganage CM, Diener HC, Algra A, et al. Dual or mono antiplatelet therapy for patients with acute ischemic stroke or transient ischemic attack: systematic review and meta-analysis of rand-omized controlled trials. Stroke 2012;43:1058-66.
23 Wang Y, Wang Y, Zhao X, et al. Clopidogrel with aspirin in acute minor stroke or transient ischemic attack. N Engl J Med 2013;369:11-19.

117
Stroke: new therapiesAVC : nouveautés thérapeutiques© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
Stroke, new therapies: After twenty years of thrombolysis, what’s new?
Jean-François Pinel (Rennes)
The science of the past is the best passport to the future.Christina of Sweden (XVIth Century)
Intravenous thrombolysis cannot be boiled down to injecting a dose of 0.9 mg/kg of alteplase (recombinant tissue plasminogen activator [rtPA]) to patients within four-and-a-half hours of an ischaemic stroke. The development of this treatment modality has profoundly changed not only vascular neurology but how all neurology departments operate as well as how they are structured: the impact has spread to call centres, emergency medical personnel and departments, and radiology services.
However, recommendations differ from country to country and individual prac-tices are far from uniform. Many articles have been published but the studies they report on have been subject to criticisms that could go as far as casting doubt on the validity of the indications for IV thrombolysis. Some national agencies and learned societies are considering reviewing their position.
So we need to go back over the past.
Development of Iv thrombolySIS
Going back to the publication nearly twenty years ago of the results of the NINDS Study in the New England Journal of Medicine in December 1995 [1], we can look at the very particular history of this innovation.
In the 1960s, a few articles were published on using thrombolytic agents in the treatment of stroke. In 1988, del Zoppo [2] compiled eight studies, including Abe’s last one [3], which reports on 58 patients, of whom 48 improved without bleed-ing complications or dying; this was a double-blind, multicentre study with no age restriction on patients who could be included up to 15 days after the event. The treatment given was low-dose urokinase for six days and the end point was based on global improvement after one month. This is very different from the methodology of later studies but, at the time, given that the use of such pharmacological agents

Jean-François Pinel
118
was very young, a number of experts declared themselves optimistic about the future (Grotta [4]; Sloan [5]), referring back to the prior use of rtPA and the possibility of combining protective agents with thrombolysis. To date, studies on protective agents have all given negative results.
In the 1990s, a number of important studies were carried out, some with strepto-kinase (MAST-I 1995 [6], ASK 1996 [7], MAST-E 1996 [8]) and others with rtPA (ECASS 1995 [9], ECASS II 1998 [10]); globally, these all gave negative results. Some post-hoc analyses might show a positive trend but only at the expense of meth-odological “tweaks” (e.g. modification of the endpoints of the analysis for ECASS II). This led to open conflict and a frank split between the investigators, with two different sets of results presented for MAST-I, each coming to different conclusions [11]).
In fact, the true revolution was reported in 1993 by Langhorne. This pointed up the value of developing Stroke Units, which afford some degree of help to all admitted patients. Despite validated studies demonstrating the benefit of bringing stroke-related resources—both medical and non-medical—together in one facility, it was thrombolysis that, even though it is only relevant to a small fraction of patients, swung the argument for creating avenues that led to the implantation of Stroke Units: setting up such units that help all victims of stroke—be it ischaemic or not, treated by thrombolysis or not—would have been far more difficult without the striking image of a clot to be “dissolved”.
There had been little progress in the pharmacology of treating acute-phase ischae-mic stroke. Studies that pointed up the modest efficacy of aspirin were still under way and would not be published until two years later in 1997 (IST [12] and CAST [13]) and the value of low molecular weight heparin prescribed within 48 hours [14] had only just been published with the results of a study on 300 patients; nevertheless, efficacy vis-à-vis outcome at Month 6 was not subsequently confirmed.
It was therefore with enthusiasm that neurologists welcomed the results of the NINDS Study [1] showing the benefit of injecting rtPA within three hours of the onset of a stroke vis-à-vis functional prognosis at Month 3.
However, from the day of publication, there was extensive fundamental criticism: it was the only positive study; the main objective was changed after 291 inclusions; no efficacy was manifest in scores after 24 hours or global mortality; the differential in NIHSS score between the treated and control groups at baseline could alone account for the Month 6 Rankin score result; and finally, the “price” to be paid to prevent 11 cases of death or dependence was 6 cases of intracranial haematoma and three deaths directly attributable to treatment (which did not necessarily strike patients with the most severe strokes). Finally, the study only covered a total of 624 patients while the cohorts of our cardiologist colleagues on thrombolysis were of the order of 60,000 patients in the 1990 GISSI 2 Study [15] and 41,000 in the 1993 GUSTO Study [16] (which already compared different thrombolytic agents).

119
Stroke, new therapies: After twenty years of thrombolysis, what’s new?
In 1996 and 1997, several experts respected in the neurovascular community con-sidered that there was insufficient evidence to justify generalisation of this treatment modality; van Gijn [17], while welcoming the fact that a door had been opened, found it premature to conclude that intravenous thrombolysis was effective; Furlan and Kanoti [18] believed that it was too early to use intravenous thrombolysis out-side of a research framework, despite FDA approval; Caplan and Mohr [19] deemed the treatment too risky and thought that widespread implementation could lead to too many complications (some life-threatening) for minor benefit in a fraction of patients.
Nevertheless, in August 2000, the recommendations were upgraded from 2B to 1 without any supplementary results and despite many experts casting doubt on the NINDS results, particularly pointing to the problem that the fact that the placebo group had been less seriously compromised at baseline could alone account for the month 3 results (Lenzer [20]; Mann [21]).
In 2002 in the British Medical Journal, a number of experts (Warlow, Wardlaw [22]; Trotter [23]) suggested that what had been demonstrated for myocardial infarc-tion had not yet been demonstrated for the brain, that this treatment should still be restricted to a tightly targeted patient population, that the benefits seem to have been exaggerated in the literature, and that further studies were warranted.
It is against this background that the administration of rtPA within three hours of an ischaemic stroke was licensed in Europe in 2003. The French Neurovascular Society issued guidelines [24] based on the results of meta-analyses: globally, "14 deaths or dependences" prevented for every 100 treated patients notwithstanding the risk of intracranial haematoma (ten-fold higher, including 75% fatal), a "balance" of one death for four patients benefitted was recognised but globally, as long as the contraindications were applied (in particular timing of the administration of treat-ment), thrombolysis should be widely provided as long as it was administered by a well-trained team.
A number of studies were then published to try to specify contraindications and emphasise the risks of failing to adhere to the treatment protocol [25, 26], while raising the issue of whether or not to train emergency physicians [27] and already debating the special case of the elderly [28]; in this way, the practice of thrombolysis grew in France in parallel to the set-up of Stroke Units.
The tiny fraction of patients who were managing to get administered IV throm-bolysis within three hours then justified a massive effort to improve the pre-hospital phase, restructure acute-phase care in the hospital and review all the channels used for stroke victims (whether treated by thrombolysis or not). The very image of emergency neurology and neurologists was changed by these advances. Two articles [29], one of which is a pastiche that mimics an article in the NEJM [30], re-viewed the situation in 2002 and 2003 with humour, "Thrombolysis for acute stroke
Jean-François Pinel
120
has revolutionized the psychology of the specialty and this tendency has impacted on other specialties. It remains to be seen if there is an equally beneficial effect on stroke patients. Until then, preventative treatment of hypertension, diabetes, and lifestyle modifications including smoking cessation and exercise are recommended both for neurologists and the general public".
The main reason for withholding thrombolytic treatment remained the three-hour time limit and models suggested that later administration might be effective. The ECASS III Study [31] published in 2008 answered this question by demonstrating effectiveness in terms of Rankin score on day 90 in patients treated between three hours and four-and-a-half hours after onset.
Then in 2012, the large-scale, pragmatic, international, multicentre, randomised, open-label IST-3 Study [32] on 3,035 patients set out to investigate whether the indication could be extended to all patients, whatever their age, and prolonged out to six hours. In practice, doctors excluded patients in whom they were sure of the indication or the contraindication and only borderline patients were included. Assessment was on the basis of an equivalent of the Rankin Scale and the trial was open-label in that the patient knew which treatment he or she had received. The article published in May 2012 came to the conclusion that thrombolysis within six hours improved functional prognosis whatever the patient’s age. Fully 95% of the patients included did not fulfil the criteria recommended in Europe: 53% were over 80 and 32% had a NIHSS score of 16 or over (a severe stroke). The paradigm seemed therefore to be reversed: hitherto in an emergency context, neurologists asked what the indication was in a stroke victim, but now the question had be-come in which patient who has had a stroke in the last six hours is thrombolysis contraindicated [33]?
Current SItuAtIon
The number of articles published on this subject has continued to grow in recent years, from 445 posted on PubMed in 2010 to 572, 714 and 846 in the following years, with more than 900 in 2014. Reviewing the main topics addressed between 2004 and 2014, it is clear that logistic issues are still as commonly brought up, the number of articles on imaging is declining and new subjects have emerged, includ-ing combining thrombolysis with an endovascular procedure, questions about using thrombolytic agents in patients on direct oral anticoagulants, and remote diagnosis and prescription (telemedicine). Clinical articles remain highly represented: what is the risk of administering thrombolysis to a patient wrongly diagnosed with acute-phase stroke [34-36]? Are there differences in efficacy and safety between Caucasians and Chinese subjects [37, 38]? How sensitive and specific is MRI in the acute phase [39]? What weight should be accorded to scores that predict intracranial

121
Stroke, new therapies: After twenty years of thrombolysis, what’s new?
haemorrhage [40]? Should thrombolysis be undertaken in a patient with a non-debilitating stroke [41]? Does thrombolysis have more impact on damage to white matter or grey matter [42]? Can imaging explain why some patients deteriorate despite treatment [43]? What are the most useful relative and absolute contraindica-tions because they vary between learned societies and from country to country [44]?
Despite 20 years of experience and an extensive literature, it has to be admitted that neurologists’ attitudes in these special emergency situations remain highly dis-parate. A survey carried out in Brittany in 2013 [45] put 28 specific scenarios—age, background factors, symptoms, relative contraindications, MRI details—to 30 neu-rologists working in a Neurovascular Unit. Consensus was only observed in 10% of these situations; in about one-third, there was a relative majority; in another third, trends could be observed; and in the last third, the different interviewees proposed entirely disparate therapeutic strategies. When thrombolysis was in question, the principal fear was exacerbation due to intracranial haemorrhage. In the course of administration, the main preoccupation was safety with efficacy only consid-ered secondarily. Modifications to practice were insidious, often due to personal experience because it is not possible to conduct rigorous trials in all situations. Contraindications were ignored because they only reflect exclusion criteria from the early studies. Neuroradiological scan-based criteria (that thrombolysis has taught us to read) have been changed to different MRI-based criteria, at least at centres that have the relevant equipment for emergencies (which also contributes to inconsistent practice).
Nevertheless, the learned societies regularly update their recommendations [46] and the Cochrane Library published summaries in 2000, 2003, 2009 and 2014 [47-50]; the latter document—of over 160 pages—covers 27 studies and a total of over 10,000 patients. Initially, in 2000, the Cochrane Collaboration did not seem to be convinced of the usefulness of intravenous thrombolysis, despite the NINDS Study published five years before. By 2014, their conclusion was more positive, “Thrombolytic therapy given up to six hours after stroke reduces the proportion of dead or dependent people. This overall benefit was apparent despite an increase in symptomatic intracranial haemorrhage, deaths at 10 days, and final assessments. Age, scan modifications or severity do not constitute contraindications to this treat-ment, especially in the first four-and-a-half hours".
QueStIonS
Although it is funded by the National Health Service, the Cochrane Collaboration stipulates that its conclusions are not necessarily the same as those of that organisa-tion so, despite the methodological rigour applied for this meta-analysis, there may be room for more equivocal opinions.
Jean-François Pinel
122
With respect to prolongation of the therapeutic window from three to four-and-a-half hours following the findings of the ECASS III Study, there is still controversy. A series of articles published in Stroke in 2014 points out that the FDA has not approved this extension and that, in the absence of new studies (which is unlikely), the question will persist [51-53]. Among the criticisms of this study, some experts note that the placebo group was in a slightly more serious condition at baseline, that patients in this group had two times as many cerebrovascular events in their past and that the percentage with intracerebral haemorrhage was particularly low in the treated group, partly due to a specific change in the definition for this study. These authors also point out that this was the only study with positive results; in other studies conducted at the same time, excess mortality led to premature termination. A project on desmoteplase [54] published in 2009 also sought to investigate prolong-ing the therapeutic window but gave negative results. This latter study attracted far less attention and it was only cited 7 times in subsequent reference titles whereas the ECASS III Study was cited 113 times.
The IST-3 Study [32] attracted more virulent criticisms and was attacked in a di-dactic article [55] that raises more methodological questions: description of skewing factors, of the principle of eligibility on the uncertainty, switch from a double-blind design to open-label after the inclusion of 276 patients, an experienced centre be-ing defined as one that administers thrombolysis just three times a year, the ordinal analysis being carried out secondarily, retrospectively changing the study’s main objective for the analysis, excess mortality in the first seven days for “cerebral” causes (p = 0.0001), and possible conflicts of interest.
Other even more critical—even virulent—opinions have been broadcast [56, 57]. Often well argued on the basis of solid evidence, these opinions affirm that the re-sults cannot be taken as positive if there is no difference in the pre-established month 6 “death and dependence” end point. They emphasise that the inclusion method must have favoured treatment in the thrombolysis arm (because patients in whom the physician concluded there was a contraindication were excluded) and it was not therefore legitimate to extrapolate the results to “all” patients in the “real world”. Moreover, the absence of any relationship between efficacy and time to administra-tion casts serious doubt on the ECASS III results, already heavily criticised. In fact, the authors of IST-3 [32] recognise that treatment between three and four-and-a-half hours seems to be harmful.
All these questions about ECASS III and to an even greater extent IST-3 shed doubt on the very issue of whether intravenous thrombolysis is really effective [58]; globally, out of the twelve relevant major studies, six showed no benefit, four had to be terminated prematurely because of adverse effects and the conclusions from the other two—despite their having been declared positive—remain highly debatable in the light of the methodology used for data analysis [59].
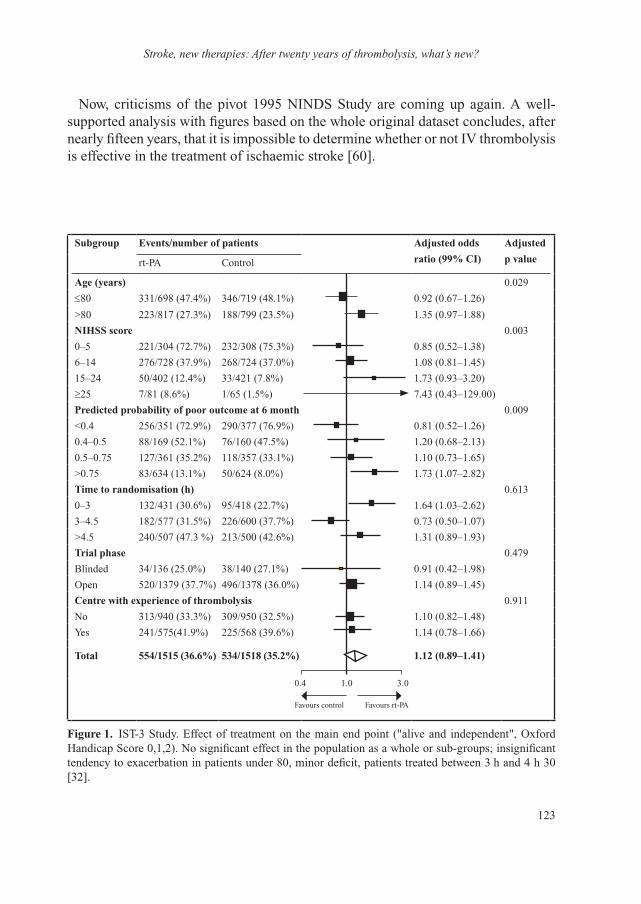
123
Stroke, new therapies: After twenty years of thrombolysis, what’s new?
Now, criticisms of the pivot 1995 NINDS Study are coming up again. A well-supported analysis with figures based on the whole original dataset concludes, after nearly fifteen years, that it is impossible to determine whether or not IV thrombolysis is effective in the treatment of ischaemic stroke [60].
Subgroup events/number of patients Adjusted odds
ratio (99% CI)
Adjusted
p value rt-PA Control
Age (years) 0.029
≤80 331/698 (47.4%) 346/719 (48.1%) 0.92 (0.67–1.26)
>80 223/817 (27.3%) 188/799 (23.5%) 1.35 (0.97–1.88)
nIhSS score 0.003
0–5 221/304 (72.7%) 232/308 (75.3%) 0.85 (0.52–1.38)
6–14 276/728 (37.9%) 268/724 (37.0%) 1.08 (0.81–1.45)
15–24 50/402 (12.4%) 33/421 (7.8%) 1.73 (0.93–3.20)
≥25 7/81 (8.6%) 1/65 (1.5%) 7.43 (0.43–129.00)
predicted probability of poor outcome at 6 month 0.009
<0.4 256/351 (72.9%) 290/377 (76.9%) 0.81 (0.52–1.26)
0.4–0.5 88/169 (52.1%) 76/160 (47.5%) 1.20 (0.68–2.13)
0.5–0.75 127/361 (35.2%) 118/357 (33.1%) 1.10 (0.73–1.65)
>0.75 83/634 (13.1%) 50/624 (8.0%) 1.73 (1.07–2.82)
time to randomisation (h) 0.613
0–3 132/431 (30.6%) 95/418 (22.7%) 1.64 (1.03–2.62)
3–4.5 182/577 (31.5%) 226/600 (37.7%) 0.73 (0.50–1.07)
>4.5 240/507 (47.3 %) 213/500 (42.6%) 1.31 (0.89–1.93)
trial phase 0.479
Blinded 34/136 (25.0%) 38/140 (27.1%) 0.91 (0.42–1.98)
Open 520/1379 (37.7%) 496/1378 (36.0%) 1.14 (0.89–1.45)
Centre with experience of thrombolysis 0.911
No 313/940 (33.3%) 309/950 (32.5%) 1.10 (0.82–1.48)
Yes 241/575(41.9%) 225/568 (39.6%) 1.14 (0.78–1.66)
total 554/1515 (36.6%) 534/1518 (35.2%) 1.12 (0.89–1.41)
figure 1. IST-3 Study. Effect of treatment on the main end point ("alive and independent", Oxford Handicap Score 0,1,2). No significant effect in the population as a whole or sub-groups; insignificant tendency to exacerbation in patients under 80, minor deficit, patients treated between 3 h and 4 h 30 [32].
0.4 1.0 3.0
Favours control Favours rt-PA

Jean-François Pinel
124
In the August 2014 Lancet [61], Shinton re-analysed the NINDS and IST-3 results. He goes back over the old criticisms and concludes that evidence in favour of the benefit of thrombolysis remains poor. He also concludes that, although Neurovascular Units efficiently care for victims of strokes, the regulatory agencies ought to review the whole case for rtPA.
This is what Cohen and Macdonald seemed to announce in the British Medical Journal in September 2014 with respect to the UK drug agency [62]. In an August 2014 letter to the Internal Medicine Journal [63], Fatovich reports that the American College of Emergency Physicians is going to review its recommendations and that the Australian College of Emergency Medicine considers that IV thrombolysis no longer constitutes part of the standard treatment for ischaemic stroke.
It is against this background of uncertainty that we have to look after our patients, a thorny problem. Shamy [64] conducted a survey of 70 neurologists in the Canadian Province of Ontario that showed highly disparate approaches as we observed in our small survey in Brittany. Curiously, in our study, believing in a high or low benefit-to-risk ratio did not change practitioners’ prescribing behaviour in terms of indication in the 28 scenarios proposed. Medical decision-making remains an art that, if not actually mysterious is, at any rate, difficult.
0%
–40
–20
0
20
40
50% 100%
Worse
90 D
ay c
hang
e in
NIH
SSPlacebo < 90 min (n = 145)
tPA < 90 min (n = 157)
Placebo 90–180 min (n = 167)
tPA 90–180 min (n = 155)
Improved
figure 2. Data from the NINDS Study. Distribution of changes in NIHSS score between randomisation and day 90. Positive values mean an improvement in score. There is no difference between the treated group and the control group [60].

125
Stroke, new therapies: After twenty years of thrombolysis, what’s new?
ConCluSIon
This article aims to weigh up the possible direct benefits of intravenous thrombolysis, but it is important to recognise that the existence of this therapeutic modality has been a magnificent engine in the management of strokes in general with the development of Neurovascular Units with dedicated staff, the establishment of channels upstream and downstream, the creation of posts for neurovascular specialists, the setting of precau-tions and deadlines for all neurological patients, the development of neuroradiology with CT scanners and MRI equipment available round the clock seven days a week, the development of interventional neuroradiology, impact on teaching and research, and finally how strokes are perceived by the general public. All this can, in part, be chalked up to intravenous thrombolysis. In this sense, the positive impact of this treatment modality—which ultimately only concerns a small fraction of strokes—has gone significantly beyond simple benefit to patients who are treated with alteplase.
This review of past publications does not target the medical recommendations. Its only aim is to point out that our objectivity is very relative and that the rigour required for progress in medical science does not preclude examination of our perceptions, even our prejudices. With ischaemic strokes, it is vital to recognise the value of urgent repermeabilisation of the thrombosed vessel to prevent spread of the infarct into the penumbral area. For all that, we must remain vigilant in our read-ing of the literature and avoid making self-fulfilling prophesies. We should switch between strict adherence to clinical trial methodology (costly and difficult to repeat) and post-hoc analyses to extract information retrospectively. The journey that has brought us from the 1995 NINDS Study (approval of treatment within three hours) to the ECASS III Study (extension of the window to four-and-a-half hours) and then the IST-3 Study (recommending prolongation of the window to six hours for all patients) could also be re-examined by going back over the past. But history moves on and although the past may have a lot to teach us, we cannot wipe the slate clean and just go back to the situation before 1995.
Some questions remain. When a meta-analysis lacks rationale (disparate meth-odologies, imbalance in population size between different studies), how should positive and negative studies (NINDS, ECASS, DIAS 2) be weighed up against one another? Should changes be made to the protocol while a study is under way (NINDS, IST-3)? Should so much interest be placed in post-hoc statistical analyses that reverse hitherto negative results (IST-3; Figure 1) and positive results (NINDS; Figure 2)? How to reconcile guidelines from learned societies with those of national regulatory agencies when, according to the literature, opinions diverge (extension of IV thrombolysis to four-and-a-half hours)?
To these questions with no simple answer, it is important to add the major issue of how to apply guidelines to the treatment of a given patient—which would open

Jean-François Pinel
126
another debate that is widely discussed in the literature. Finally, techniques evolve and since intravenous thrombolysis has been shown to have limitations, questions now focus on combining it with mechanical thrombectomy [65].
Common sense has a future.
references
1 The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995;333(24):1581-7.
2 del Zoppo GJ. Investigational use of tPA in acute stroke. Ann Emerg Med 1988;17(11): 1196-201.
3 Abe T, Kazama M, Naito I. Clinical evaluation for efficacy of tissue culture urokinase (TCUK) on cerebral thrombosis by means of multicenter double-blind study. Blood Vessel 1981;12:321-41.
4 Grotta J. Can raising cerebral blood flow improve outcome after acute cerebral infarction? Stroke 1987;18:264-7.
5 Sloan MA. Thrombolysis and stroke. Past and future. Arch Neurol 1987;44(7):748-68.6 Italy (MAST-I) Group. Randomised controlled trial of streptokinase, aspirin, and combina-
tion of both in treatment of acute ischaemic stroke. Multicentre Acute Stroke Trial. Lancet 1995;346(8989):1509-14.
7 Donnan GA, et al. Streptokinase for acute ischemic stroke with relationship to time of administra-tion: Australian Streptokinase (ASK) Trial Study Group. JAMA 1996;276(12):961-6.
8 The Multicenter Acute Stroke Trial–Europe Study Group. Thrombolytic therapy with streptoki-nase in acute ischemic stroke. N Engl J Med 1996;335(3):145-50.
9 Hacke W, et al. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The European Cooperative Acute Stroke Study (ECASS). JAMA 1995;274 (13):1017-25.
10 Hacke W, et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian Acute Stroke Study Investigators. Lancet 1998;352(9136):1245-51.
11 Tognoni GR, Roncaglioni MC. Dissent: an alternative interpretation of MAST-I. Multicentre Acute Stroke Trial–Italy Group. Lancet 1995;346:1515.
12 International Stroke Trial Collaborative Group. The International Stroke Trial (IST): a randomised trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke. Lancet 1997;349(9065):1569-81.
13 CAST (Chinese Acute Stroke Trial) Collaborative Group. CAST: randomised placebo-controlled trial of early aspirin use in 20,000 patients with acute ischaemic stroke. Lancet 1997;349 (9066):1641-9.
14 Kay R, et al. Low-molecular-weight heparin for the treatment of acute ischemic stroke. N Engl J Med 1995;333(24):1588-93.
15 Gruppo Italiano per lo Studio della Streptochinasi nell’Infarto Miocardico (GISSI). Effectiveness of intravenous thrombolytic treatment in acute myocardial infarction. Lancet 1986;1(8478): 397-402.
16 The GUSTO Investigators. An international randomized trial comparing four thrombolytic strate-gies for acute myocardial infarction. N Engl J Med 1993;329(10):673-82.
17 van Gijn J. Thrombolysis in ischemic stroke: double or quits? Circulation 1996;93(9):1616-17.18 Furlan AJ, Kanoti G. When is thrombolysis justified in patients with acute ischemic stroke? A
bioethical perspective. Stroke 1997;28(1):214-18.

127
Stroke, new therapies: After twenty years of thrombolysis, what’s new?
19 Caplan LR, et al. Should thrombolytic therapy be the first-line treatment for acute ischemic stroke? Thrombolysis – not a panacea for ischemic stroke. N Engl J Med 1997;337(18):1309-10; discussion 1313.
20 Lenzer J. Alteplase for stroke: money and optimistic claims buttress the “brain attack” campaign. BMJ 2002;324(7339):723-9.
21 Mann J. Truths about the NINDS study: setting the record straight. West J Med 2002;176(3):192-4.22 Warlow C, Wardlaw J. Therapeutic thrombolysis for acute ischaemic stroke. BMJ
2003;326(7383):233-4.23 Trotter G. Why were the benefits of tPA exaggerated? West J Med 2002; 176(3):194-7.24 Société française Neurovasculaire. Recommandations pour l’utilisation du thrombolytic treatment
intra-veineux dans l’accident ischémique cérébral. Rev Neurol 2000;156:1178-85.25 Albers GW, et al. Intravenous tissue-type plasminogen activator for treatment of acute stroke:
the Standard Treatment with Alteplase to Reverse Stroke (STARS) study. JAMA 2000;283(9): 1145-50.
26 Katzan IL, et al. Use of tissue-type plasminogen activator for acute ischemic stroke: the Cleveland area experience. JAMA 2000;283(9):1151-8.
27 Akins PT, et al. Can emergency department physicians safely and effectively initiate thrombolysis for acute ischemic stroke? Neurology 2000;55(12):1801-5.
28 Tanne D, et al. Intravenous tissue plasminogen activator for acute ischemic stroke in patients aged 80 years and older: the tPA stroke survey experience. Stroke 2000;31(2):370-5.
29 Brewer PV, Vadeboncoeur A. PsychOSocial effecTs Of aCute stroke thrombolysIS programs on neurologists and Emergency physicians: A proSpectIve comparativE cohoRt (POST ‘OC IS EASIER) study. Can J Emerg Med 2003;133.
30 Brewer PV, Vadeboncoeur A. The psycho-social effects on the Neurology community secondary to the use of tPA for stroke: A prospective cohort study. http://www.mail-archive.com/[email protected]/msg00340/NINDS_RAW_DATA.PDF, 2002.
31 Hacke W, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med 2008;359(13):1317-29.
32 Sandercock P, et al. The benefits and harms of intravenous thrombolysis with recombinant tissue plasminogen activator within 6 h of acute ischaemic stroke (the third international stroke trial [IST-3]): a randomised controlled trial. Lancet 2012;379(9834):2352-63.
33 Leys D, Cordonnier C. rt-PA for ischaemic stroke: what will the next question be? Lancet 2012; 379(9834):2320-1.
34 Tsivgoulis G, et al. Safety and outcomes of intravenous thrombolysis in stroke mimics: a 6-year, single-care center study and a pooled analysis of reported series. Stroke 2011;42(6):1771-4.
35 Zinkstok SM, et al. Safety of thrombolysis in stroke mimics: results from a multicenter cohort study. Stroke 2013;44(4):1080-4.
36 Guerrero WR, Savitz SI. Tissue-type plasminogen activator for stroke mimics: continuing to be swift rather than delaying treatment to be sure. Stroke 2013;44(5):1213-14.
37 Chao AC, et al. Outcomes of thrombolytic therapy for acute ischemic stroke in Chinese pa-tients: the Taiwan Thrombolytic Therapy for Acute Ischemic Stroke (TTT-AIS) study. Stroke 2010;41(5):885-90.
38 Liao X, et al. Standard-dose intravenous tissue-type plasminogen activator for stroke is better than low doses. Stroke 2014;45(8):2354-8.
39 Simonsen CZ, et al. Sensitivity of diffusion- and perfusion-weighted imaging for diagnosing acute ischemic stroke is 97.5%. Stroke 2015;46:98-101.
40 Strbian D, et al. Symptomatic intracranial hemorrhage after stroke thrombolysis: comparison of prediction scores. Stroke 2014;45(3):752-8.

Jean-François Pinel
128
41 Greisenegger S, et al. Thrombolysis in patients with mild stroke: results from the Austrian Stroke Unit Registry. Stroke 2014;45(3):765-9.
42 Tisserand M, et al. Is white matter more prone to diffusion lesion reversal after thrombolysis? Stroke 2014;45(4):1167-9.
43 Tisserand M, et al. Mechanisms of unexplained neurological deterioration after intravenous thrombolysis. Stroke 2014;45:3527-34.
44 Frank B, et al. Thrombolysis in stroke despite contraindications or warnings? Stroke 2013;44(3):727-33.
45 Vannier SR, T, Pinel JF. Enquete auprès des UNV bretonnes sur la thrombolysis off-label. Poster 18eme journées de la SFNV, Paris, 2013.
46 Jauch EC, et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013;44(3):870-947.
47 Wardlaw JM, del Zoppo G, Yamaguchi T. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev 2000;(2):CD000213.
48 Wardlaw JM, et al. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev 2003;(3):CD000213.
49 Wardlaw JM, et al. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev 2009;(4):CD000213.
50 Wardlaw JM, et al. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev 2014;(7):CD000213.
51 Schellinger PD, Kohrmann M. 4.5-Hour time window for intravenous thrombolysis with recom-binant tissue-type plasminogen activator is established firmly. Stroke 2014;45(3):912-13.
52 Wechsler LR. The 4.5-hour time window for intravenous thrombolysis with intravenous tissue-type plasminogen activator is not firmly established. Stroke 2014;45(3):914-15.
53 Selim MH, Molina CA. Thrombolysis in the 3- to 4.5-hour window: what do ECASSkeptics want? Stroke 2014;45(3):916-17.
54 Hacke W, et al. Intravenous desmoteplase in patients with acute ischaemic stroke selected by MRI perfusion-diffusion weighted imaging or perfusion CT (DIAS-2): a prospective, randomised, double-blind, placebo-controlled study. Lancet Neurol 2009;8(2):141-50.
55 Radecki RPC, YG, Press, GM. rt-PA and stroke: does IST-3 make it all clear or muddy the waters? Answers to the November 2012 Journal Club questions. Ann Emerg Med 2013;(4):489-98.
56 http://emergencymedicineireland.com/lytics-in-stroke/.57 http://www.smartem.org/podcasts/smart-thrombolytics-stroke-update.58 Hoffman JR, Cooper RJ. How is more negative evidence being used to support claims of
benefit: The curious case of the third international stroke trial (IST-3). Emerg Med Australas 2012;24(5):473-6.
59 Fatovich DM. Believing is seeing: stroke thrombolysis remains unproven after the third International Stroke Trial (IST-3). Emerg Med Australas 2012;24(5):477-9.
60 Hoffman JR, Schriger DL. A graphic reanalysis of the NINDS Trial. Ann Emerg Med 2009;54(3):329-36; 336 e1-35.
61 Shinton R. Questions about authorisation of alteplase for ischaemic stroke. Lancet 2014;384(9944):659-60.
62 Cohen D, Macdonald H. UK drug agency announces review of use of alteplase after stroke. BMJ 2014;349:g5355.
63 Fatovich DM, Brown SG. Stroke thrombolysis remains unproven: per ardua, ad astra. Intern Med J 2014;44(12a):1261-2.

129
Stroke, new therapies: After twenty years of thrombolysis, what’s new?
64 Shamy MC, Jaigobin CS. The complexities of acute stroke decision-making: a survey of neurolo-gists. Neurology 2013;81(13):1130-3.
65 Fransen PS, et al. MR CLEAN, a multicenter randomized clinical trial of endovascular treatment for acute ischemic stroke in the Netherlands: study protocol for a randomized controlled trial. Trials 2014;15:343.

130
Stroke: new therapiesAVC : nouveautés thérapeutiques© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
Treating Hemorrhagic stroke
Christian Stapf (Paris)
HemorrHagic sTroke: a HigH-risk sTroke Type
Stroke constitutes the third cause of mortality and the leading cause of disability in our society. Between 70% and 90% of cerebrovascular accidents (CVAs) are ischaemic. Although it is not as common, hemorrhagic stroke is a particularly serious type of CVA with a mortality rate of 30–60% within the first 30 days ( compared with 15–20% from cerebral infarct) and at times severe neurological deficit in the long term.
With the ageing of the population and, in parallel, the ever-more widespread prescription of anticoagulant drugs, the annual incidence of hemorrhagic stroke is steadily rising. The most important risk factors are arterial hypertension (60–70% of cases), heavy drinking and smoking as well as other predisposing factors such as cerebral amyloid angiopathy.
In the first 24 hours of a spontaneous hemorrhagic stroke, the volume of the hae-matoma grows by at least one-third in 38% of cases. Hematoma expansion is a factor that is associated with poor prognosis in terms of death in the acute phase as well as long-term morbidity.
TreaTmenT
any hemorrhagic stroke has an underlying cause
In the last forty years, various classification systems for ischemic stroke have been proposed to categorise cerebral infarcts according to aetiology, e.g. the Harvard Stroke Registry / NINDS Stroke Databank, the Oxford Community Stroke Project classification (OCSP), TOAST (Trial of Org 10172 in Acute Stroke Treatment) and ASCO (Atherosclerosis, Small vessel disease, Cardiac source, Other cause).
In contrast, classification systems for hemorrhagic stroke only take stock of their location (intracerebral / sub-arachnoid / intraventricular or lobar/deep) with an aetiological component limited to distinction between “primary” and “ secondary” or “hypertensive” hemorrhage. It is important to emphasise that hemorrhagic stroke always has an underlying structural cause so, in effect, all of them are secondary.

131
Treating Hemorrhagic stroke
In addition, the term “hypertensive hemorrhage” mixes up risk factor and cause: a risk factor can predispose to or trigger an underlying cause but it does not constitute a structural cause of the bleeding. In consequence, treating a case of hemorrhagic stroke necessarily involves identifying the underlying problem by means of a scru-pulous etiologic investigation.
Various vascular pathologies can cause cerebral bleeding, involving arteries (cer-ebral microangiopathy, aneurysm, reversible cerebral vasoconstriction syndrome, moya-moya disease, etc.), veins (cerebral venous thrombosis, cerebral cavernoma, etc.) or where the two systems meet (arteriovenous malformation, dural fistula). Bleeding can also be a complication of some other underlying problem like a cerebral infarction (through secondary hemorrhagic transformation), neoplasia or systemic disease (impaired clotting function, endocarditis, etc.) (Table 1) [1].
Table 1. Acute hemorrhagic stroke: etiologic sub-groups [1]
microangiopathy Arteriolosclerosis / lipohyalinosis Amyloid angiopathy GeneticVascular malformation Arteriovenous malformation Cerebral cavernous malformationintracranial aneurysmVenous disease Cerebral venous thrombosis Dural fistulareversible cerebral vasoconstriction syndrome
moya-moya diseaseinflammation Vasculitis Mycotic aneurysmneoplasia Brain tumour Cerebral metastasisHemostatic disorder Genetic Acquired/iatrogenicDrug-inducedHemorrhagic infarctionHead trauma
Towards a classification system for hemorrhagic stroke
Modern diagnostic imaging techniques include CT scanning and CT angiography, brain MRI and MRA and cerebral arteriography with arterial catheterisation.
The sensitivity and specificity of the various radiological techniques are currently being assessed in a series of ongoing studies. In collaboration with our colleague, Professor Charlotte Cordonnier (CHRU Lille), we are currently working with a num-ber of European centres on a first etiologic classification system and we are trying to define diagnostic criteria to establish an aetiology as Possible, Probable or Definite.
ranking imaging techniques
According to data derived from a prospective cohort of 152 patients, CT scan-ning allowed us to make an etiologic diagnosis in 3% of patients, MRI/MRA in

Christian Stapf
132
63% and arteriography in 6%, i.e. a total of 72% precise etiologic diagnoses in cases of hemorrhagic stroke traditionally classified as either “Primary” or “Hypertensive.”
It is important to emphasise that 21% of these diagnoses immediately impacted on how the patients were being managed.
In patients who could not originally be diagnosed etiologically, imaging exami-nations were repeated 3–4 months later after the hematoma had been re-absorbed (because it can mask the cause of the bleeding). For example, even though the initial arteriography might have looked normal, the same examination after re-ab-sorption of the hematoma could reveal an arteriovenous malformation or a cerebral cavernoma—which could be treated and cured.
To summarize, our practice ought to be conditioned by the fact that all hemorrhages are secondary and the idea of ”primary” or “hypertensive” hemorrhage should be avoided. The purpose of imaging is to visualise the cause of the bleeding. Some etiologic diagnoses need to be made immediately because they will affect treatment strategy in the acute phase, including aneurysm, haemorrhagic infarction, venous disease and systemic disease. In addition, any identified cause will have long-term implications such as repair of the lesion if that is possible (including aneurysm, arteriovenous malformation, cavernoma and dural fistula) and control of risk factors (arterial hypertension, smoking, etc.).
Towards targeted treatment
Spot-sign
Most patients will be diagnosed with small artery disease. These patients are at risk of rapid exacerbation through the following cascade of events: growth in volume (mass effect), ventricular inundation, secondary hydrocephalus, intracra-nial hypertension and, in the worst case, cerebral herniation leading to death of the patient. It is vital therefore to interrupt this process. A radiological phenomenon called spot sign is currently being assessed as a predictor of hemorrhagic expansion [2]. A multicentre, observational study published in 2012 on 268 patients with a hemorrhagic stroke reported finding the spot sign in the acute hematomas of one quarter of patients (23%). The presence of this spot sign was predictive of hematoma expansion with a sensitivity of 51% and a specificity of 85%. Mortality at 3 months was 43.4% in patients with the spot sign compared with 19.6% in those without it (HR: 2.4, 95% Confidence Interval: 1.4–4.0; p = 0.002) [3].
Management
Addressing risk factors
Involvement of small arteries in the brain is often due to the effect of vascular risk factors that have caused damage to arterial walls, ultimately leading to rupture.
133
Treating Hemorrhagic stroke
Controlling such risk factors, especially hypertension, is essential to prevent further damage to small arteries and bleeding complications. It should be borne in mind that reducing systolic blood pressure by 10 mmHg or diastolic pressure by 5 mmHg prevents 80% of Hemorrhagic strokes in five years.
Stop extravasation and expansion of the haematoma
– Local haemostasisPromising results have been obtained with very early administration (within four hours of the onset of symptoms) of a coagulation factor, namely recom-binant activated factor VII (FVIIa), in a randomised phase II study evaluating efficacy and safety. Cerebral haematoma volume grew markedly less in the treated group than in the placebo group with significant efficacy on clinical criteria of dependence and mortality [4].Nevertheless, a phase III confirmatory study failed to detect any positive effect on clinical outcome [5].Other hemostatic treatments are currently undergoing evaluation, including the transfusion of platelets to victims of an acute Hemorrhagic stroke while on anti-platelet therapy (the PATCH Study). Until the results are available, haemostatic treatment cannot be recommended in the treatment of acute Hemorrhagic stroke.
– Neurosurgical evacuation Hematomas are surgically drained on a case-by-case basis without any scientific evidence on any of the techniques used: evacuation via an open craniotomy or by endoscope with stereotactic guidance. The international STICH (Surgical Trial in IntraHemorrhagic stroke) Study included more than 1,000 patients and com-pared early surgical evacuation with conservative medical care within 72 hours of a spontaneous supratentorial hemorrhagic stroke (with no underlying vessel malformation). The choice of surgical technique was left up to the neurosur-geon, most of whom opted for craniotomy (77%). No difference was observed between surgery and medical treatment of supratentorial hemorrhagic stroke (all localisations) in terms of either mortality or dependence after six months [6].Similarly, the STICH II Study (n = 597 patients who developed a lobar hae-matoma in the preceding 12 hours) did not show any difference in morbidity or mortality between care including surgery and care without it. A study is currently under way to investigate a minimally invasive surgical technique to drain the hematoma and an evaluation of decompressive hemicraniotomy after a supratentorial hemorrhage is being prepared [7].
– Antihypertensive treatmentA number of uncontrolled studies have pointed to a correlation between blood pressure and neurological deterioration in Stroke Unit patients after a

Christian Stapf
134
spontaneous intracerebral hemorrhage. In the randomised, pilot INTERACT (Intensive Blood Pressure Reduction in Acute Hemorrhagic stroke Trial) pilot study on 404 patients given antihypertensive treatment within 6 hours of the onset of the symptoms of hemorrhagic stroke (target systolic blood pressure <140 mmHg), hematoma volume grew less than in the control group [8].Finally, the randomised, international INTERACT 2 trial involving 2,839 pa-tients showed a strong trend to improvement in morbidity and mortality (Odds Ratio 0.87; 95% CI: 0.75–1.01; p = 0.006) in patients treated to lower systolic blood pressure straight away (target <140 mmHg in less than 60 minutes) and significant improvement in neurological outcome as measured on the Rankin scale after three months (Odds Ratio 0.87; 95% CI: 0.77–1.00; p = 0.04) [9].While we are still waiting for the results of another randomised trial, current guidelines for acute Hemorrhagic stroke recommend immediately administering antihypertensive drugs to bring systolic blood pressure down below 140 mmHg in less than 40 minutes [10].
practical implications
– It is worth bearing in mind that any hemorrhagic stroke has an underlying structural cause that needs to be identified in an appropriate investigation. Risk factors may predispose to or affect certain causes but it is important not to mix up causes and risk factors. Therefore, ideas like “primary” and “ hypertensive” hemorrhage ought to be avoided.
– The purpose of the diagnostic work-up is to determine the aetiology of the bleeding and plan targeted therapy. The spot sign may be predictive of haema-toma expansion.
– Neither local haemostasis nor surgical drainage have been shown to be effective. – In contrast, it is now clear that antihypertensive treatment in the acute phase
improves morbidity and mortality. This should be intense (IV administration of a bolus dose followed by continuous infusion) to bring systolic blood pressure down below 140 mmHg within one hour. Throughout administration, blood pressure should be closely monitored (with blood pressure measured every 15 minutes during the first hour). All members of the care-providing team should be familiar with the therapeutic protocol. As with thrombolysis, time is key, and delays between imaging and the introduction of antihypertensive treatment should be minimised. In this situation, team spirit is crucial.
– This treatment should be administered in a dedicated Stroke Unit and blood pressure should be kept under control on a sustained basis: for the first 24 hours (acute phase benefits <24 hours) and then the next few days (post-acute phase benefit <7 days) and finally throughout the patient’s life (long-term benefit: on stroke prevention).
135
Treating Hemorrhagic stroke
– The AHA/ASA is in the process of updating its guidelines. European guidelines (ESO) were published in 2014 [11]. A French committee (SFNV) recently convened with a view to issuing recommendations.
references
1 Al-Shahi Salman R1, Labovitz DL, Stapf C. Spontaneous intracerebral hemorrhage. BMJ 2009; 339:b2586.
2 Wada R, Aviv RI, Fox AJ, et al. CT angiography “spot sign” predicts hematoma expansion in acute intracerebral hemorrhage. Stroke 2007;38:1257-62.
3 Demchuk AM, Dowlatshahi D, Rodriguez-Luna D, et al. Prediction of haematoma growth and outcome in patients with intraHemorrhagic stroke using the CT-angiography spot sign (PREDICT): a prospective observational study. Lancet Neurol 2012;11:307-14.
4 Mayer SA, Brun NC, Begtrup K, et al. Recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med 2005;352:777-85.
5 Mayer SA, Brun NC, Begtrup K, et al. Efficacy and safety of recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med 2008;358:2127-37.
6 Mendelow AD, Gregson BA, Fernandes HM, et al. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the International Surgical Trial in IntraHemorrhagic stroke (STICH): a randomised trial. Lancet 2005;365:387-97.
7 Mendelow AD, Gregson BA, Rowan EN, et al. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial lobar intracerebral haematomas (STICH II): a randomised trial. Lancet 2013;382:397-408.
8 Anderson CS, Huang Y, Arima H, et al. Effects of early intensive blood pressure-lowering treatment on the growth of hematoma and perihematomal edema in acute intracerebral hemorrhage: the Intensive Blood Pressure Reduction in Acute Hemorrhagic stroke Trial (INTERACT). Stroke 2010;41:307-12.
9 Anderson CS, Heeley E, Huang Y, et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N Engl J Med 2013;368:2355-65.
10 Manning L, Hirakawa Y, Arima H, et al. Blood pressure variability and outcome after acute intraHemorrhagic stroke: a post-hoc analysis of INTERACT2, a randomised controlled trial. Lancet Neurol 2014;13:364-73.
11 Steiner T, Al-Shahi Salman R, Beer R, et al. European Stroke Organisation (ESO) guidelines for the management of spontaneous intracerebral hemorrhage. Int J Stroke 2014;9:840-55.
136
Stroke: new therapiesAVC : nouveautés thérapeutiques© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
A scanner in the ambulance? Prehospital thrombolysis and further opportunities
Martin Ebinger (Berlin)
IntroductIon
Stroke is a leading cause of death and disability worldwide [1]. Thrombolysis with intravenous tissue plasminogen activator (tPA) is a widely available, evidence-based and licensed treatment that reduces the risk of permanent disability after ischaemic stroke [2, 3]. However, the effects of thrombolysis are time-dependent [4]. With every minute’s treatment delay, chances of a good outcome become less likely [5-7]. Therefore, tPA should be administered as early as possible after symptom onset. Ideally, treatment is started straight away at the first encounter with the patient, i.e. when the ambulance arrives to pick up the patient for hospital admission. Since clini-cal features cannot be used in order to distinguish reliably between ischaemic and haemorrhagic stroke, a computed tomography (CT) scan is required prior to treatment [8]. Furthermore, tPA treatment is associated with the feared risk of symptomatic intracerebral haemorrhage (sICH). This requires clinical expertise when choosing this treatment option. A neurologist experienced in acute stroke treatment, able to deal adequately with possibly occurring complications and trained in emergency medicine combines all the necessary expertise in a prehospital setting. In 2012, Silke Walter, MD, and her colleagues from Homburg, Saarland, Germany, were the first to report tPA treatments using a so-called mobile stroke unit, an ambulance equipped with a CT scanner and a point-of-care laboratory. These pioneers from Prof. Klaus Fassbender’s group demonstrated excellent time savings compared to regular care [9].
PrehosPItAl thrombolysIs
Prehospital thrombolysis in a specialized stroke ambulance is feasible, safe and reduces time from alarm to treatment. This was recently shown in a prospective study, called PHANTOM-S [10]. In this study, which was designed and supervised
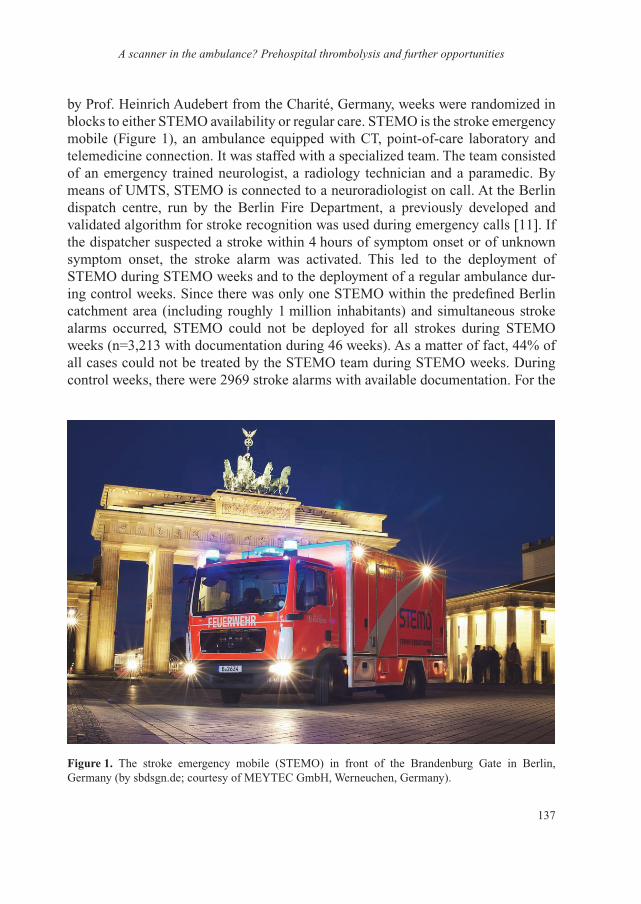
137
A scanner in the ambulance? Prehospital thrombolysis and further opportunities
by Prof. Heinrich Audebert from the Charité, Germany, weeks were randomized in blocks to either STEMO availability or regular care. STEMO is the stroke emergency mobile (Figure 1), an ambulance equipped with CT, point-of-care laboratory and telemedicine connection. It was staffed with a specialized team. The team consisted of an emergency trained neurologist, a radiology technician and a paramedic. By means of UMTS, STEMO is connected to a neuroradiologist on call. At the Berlin dispatch centre, run by the Berlin Fire Department, a previously developed and validated algorithm for stroke recognition was used during emergency calls [11]. If the dispatcher suspected a stroke within 4 hours of symptom onset or of unknown symptom onset, the stroke alarm was activated. This led to the deployment of STEMO during STEMO weeks and to the deployment of a regular ambulance dur-ing control weeks. Since there was only one STEMO within the predefined Berlin catchment area (including roughly 1 million inhabitants) and simultaneous stroke alarms occurred, STEMO could not be deployed for all strokes during STEMO weeks (n=3,213 with documentation during 46 weeks). As a matter of fact, 44% of all cases could not be treated by the STEMO team during STEMO weeks. During control weeks, there were 2969 stroke alarms with available documentation. For the
1
Figure 1. The stroke emergency mobile (STEMO) in front of the Brandenburg Gate in Berlin, Germany (by sbdsgn.de; courtesy of MEYTEC GmbH, Werneuchen, Germany).

Martin Ebinger
138
primary end-point of the study, i.e. alarm to treatment times, a 25 minute time reduc-tion was observed (STEMO deployment: 51.8, 95% CI: 49.0–54.6 min vs. control weeks: 76.3, 95% CI: 73.2–79.3 min). In adjusted analyses STEMO deployment did not entail an increased risk of secondary intracerebral haemorrhage (OR 0.42, 95% CI: 0.18–1.03), or mortality (within 7 days: 0.76, 95% CI: 0.31–1.82; within 90 days: 1.02, 95% CI: 0.58–1.82). The PHANTOM-S study was not powered to detect effects on functional outcome [12].
In a subsequently published sub-study, the effects of thrombolysis within the first 60 minutes of symptom onset were assessed. The so-called golden hour thrombolysis occurred about 10 times more often after STEMO deployment compared to regular care (10.1% vs. 1.1% of all ischaemic strokes, p<0.01; Figure 2). Among the patients receiving tPA, there was still a 6-fold increase in the proportion of golden hour thrombolysis after STEMO deployment compared to regular care (31% vs 4.9%; p<0.01). Comparing all patients who received golden hour thrombolysis to patients treated in later time windows there was no statistically significant difference in terms of secondary intracerebral haemorrhage, or mortality within 7 or 90 days. However, analyses adjusted for age, sex, atrial fibrillation and NIHSS, revealed an OR of 1.93 (95% CI: 1.09–3.41) for discharge to home after STEMO deployment [13]. While this is only the result of an exploratory analysis using a surrogate outcome parameter (discharge home) it fits well into the well-established association between earlier treatment and better outcomes [4, 5, 7]. Future studies powered for functional out-come differences between groups are necessary in order to demonstrate the effects of prehospital thrombolysis within and outside the golden hour on functional outcome.
02468
101214
%16
0–60 61–120 121–180 181–240 241–270Minutes
STEMO care
Conventional care
Figure 2. Proportion of patients with ischaemic stroke receiving thrombolysis in different time intervals. Note the almost 10-fold difference between STEMO care and conventional care within the first hour, the so-called golden hour [19].

139
A scanner in the ambulance? Prehospital thrombolysis and further opportunities
trIAge
Triage is an important preclinical task ensuring that patients receive the optimal treatment while at the same time resources are used wisely. Usually, patients are admitted to the nearest hospital. Ideally, they get admitted to the nearest adequate hospital. Adequate, in the case of an acute ischaemic stroke, is a hospital with a Stroke Unit. In the case of haemorrhagic stroke, a hospital with a department of neurosurgery may be desirable and, increasingly, patients with blockage of major arteries are transferred to centres with the ability to perform mechanical recanaliza-tion after the start of Iv tPA.
The STEMO concept enhances the recognition rate of stroke, facilitates admission to the adequate hospital in a given patient and allows for the start of time-critical treatment during transportation. For instance, patients with intracerebral bleeds on oral anticoagulation can be reliably diagnosed in the prehospital setting and reversal of anticoagulation can be started before hospital arrival. Aggressive blood pressure lowering can be achieved during transportation. Results from the INTERACT2 trial suggest that earlier treatment again provides the greatest benefit in haemorrhagic stroke [14]. If CT-angiography aboard the STEMO reveals occlusion of large arteries (e.g. ICA or M1) the patient can be brought to the next available catheter lab for mechanical recanalization after initiation of tPA treatment. Matthias Wendt, MD, one of the STEMO emergency trained neurologists, recently formally investigated the effects of STEMO deployment on hospital admission. Comparing admissions after STEMO deployment to admissions during regular care, he found significant differences for admissions of patients with ischaemic strokes to hospitals with Stroke Units and for admissions of patients with haemorrhagic strokes to hospitals with neurosurgery departments in favour of STEMO deployment (Wendt et al., submitted).
A PrehosPItAl reseArch PlAtForm
STEMO is more than a tool to speed up thrombolysis, to gain insights into the ef-fects of golden hour thrombolysis or to improve patient triage. It is an ideal research platform. Several neuroprotective agents have failed the acid test of clinical trials so far. One of the reasons for this may be the delayed use of potentially therapeutic agents compared to the successful application in animal studies. STEMO could offer the opportunity of a very early encounter between acute stroke patients and experts allowing the start of experimental agents. Although with a neutral outcome, the FAST-Mag trial by Prof. Jeff Saver from UCLA gave an excellent example of how a large scale prehospital neuroprotective trial can be performed [15, 16]. Using ambulances equipped with CT scanners may increase the power of such studies by selecting appropriate patients based on imaging criteria in the future. Apart from

Martin Ebinger
140
testing new drugs or interventions like early cooling, STEMO has already started to shed light on some biomarkers that may or may not be useful to support the diagnosis of stroke. For example, Michal Rozanski, another neurologist aboard the Berlin STEMO, recently investigated the sensitivity and specificity of glial fibrillary acidic protein (GFAP) to differentiate between ischaemic strokes and intracerebral haemorrhage. While preliminary data suggested that sensitivity was rather low, GFAP levels above 0.29 ng/ml were reliably indicative of haemorrhagic strokes [17]. Copeptin, the N-terminal end of vasopressin, on the other hand, did not turn out to be helpful when differentiating between ischaemic stroke and stroke mim-ics, vascular and non-vascular emergencies or later and earlier time windows after stroke (Wendt, submitted).
cost eFFectIveness
New developments always come at a certain price and it is more than justified to ask what costs the prehospital thrombolysis concepts create. These costs then have to be weighed against the expected and actual benefits achieved. Hitherto, cost effective-ness analyses of the STEMO concept had to rely on extrapolations. Nevertheless, first t analyses have been performed and suggest a reasonable incremental cost effectiveness ratio (ICER) for each quality adjusted life year (QALY) gained by STEMO. These analyses were performed in cooperation with a Danish research group from Odense and published recently by Dorte Gyrd-Hansen et al. [18]. Based on the collection of all available receipts, the net annual cost of the STEMO concept was €963,954. Using data from randomized placebo controlled trials of tPA, the numbers needed to treat in order to prevent disability were used to calculate the effect prehospital thrombolysis could have on functional outcome. According to this approach, the higher frequency of thrombolysis and the higher proportion of patients treated in early time windows could avoid 18 cases of disability per year. These 18 cases amount to 29.7 QALYs gained and this equates to an ICER of €32,456 per QALY. Whether or not this is an acceptable price to pay is beyond the scope of medical research and depends on the willingness of society to pay for the prevention of disability. This political decision is also subject to the availability of competing alternative countermeasures also requiring funding. In general, however, ICERs ranging below US$50,000–100,000 (in the USA) or £30,000 (in the UK) seem ac-ceptable in many western societies. Since the so far only cost-effectiveness analysis of the prehospital thrombolysis concept is based on extrapolations (first, number of avoided disabilities and, second, the equation of 1.77 QALY gain for every avoided disability) future studies are necessary to create a robust ground for decision makers. These studies may not only take into account the effects of prehospital thrombolysis

141
A scanner in the ambulance? Prehospital thrombolysis and further opportunities
but also treatments of other conditions such as blood pressure lowering in the case of haemorrhagic stroke, as Prof. Marie-Germaine Bousser pointed out during the Colloque de L’Institut Servier, AvC: nouveautés thérapeutiques, in Paris, France, 20 November 2014.
conclusIon
Prehospital thrombolysis in ambulances equipped with a CT scanner is feasible, safe, reduces time from alarm to treatment, increases the number of thrombolysis, and enhances the chances of golden hour thrombolysis. Imaging in the ambulance allows for tailored admission to different hospitals and specific emergency treat-ment during transport. The STEMO is an attractive “front line” research platform and from a societal point of view may be a wise investment. However, the field of prehospital thrombolysis is still evolving and future studies are needed to prove ben-efit in terms of avoided disability and cost-effectiveness. Integration of prehospital thrombolysis concepts into regular care requires accompanying research to answer these questions and to identify the optimal use of specialized ambulances for stroke treatment. Around the globe, researchers are preparing different projects in a variety of settings. In Paris, France, for example, Guillaume Turc, MD, and Prof. Jean-Louis Mas are applying for funding in order to start their prehospital thrombolysis project, called ASPHALT (Acute stroke: prehospital vs. inhospital intravenous thromboly-sis)—what a great acronym to pave the road for improved stroke treatment!
references
1 Feigin vL, Forouzanfar MH, Krishnamurthi R, et al. Global and regional burden of stroke during 1990-2010: findings from the Global Burden of Disease Study 2010. Lancet 2014;383(9913):245-54.
2 The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995;333(24):1581-7.
3 Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med 2008;359(13):1317-29.
4 Emberson J, Lees KR, Lyden P, et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet 2014;384(29):1929–1935.
5 Saver JL, Fonarow GC, Smith EE, et al. Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke. JAMA 2013;309(23):2480-8.
6 Saver JL. Time is brain-quantified. Stroke 2006;37(1):263-6.7 Meretoja A, Keshtkaran M, Saver JL, et al. Stroke thrombolysis: save a minute, save a day. Stroke
2014;45(4):1053-8.8 Runchey S, McGee S. Does this patient have a hemorrhagic stroke?: clinical findings distinguishing
hemorrhagic stroke from ischemic stroke. JAMA 2010;303(22):2280-6.

Martin Ebinger
142
9 Walter S, Kostopoulos P, Haass A, et al. Diagnosis and treatment of patients with stroke in a mobile stroke unit versus in hospital: a randomised controlled trial. Lancet Neurol 2012;11(5):397-404.
10 Ebinger M, Rozanski M, Waldschmidt C, et al. PHANTOM-S: the prehospital acute neurological therapy and optimization of medical care in stroke patients – study. Int J Stroke 2012;7(4):348-53.
11 Krebes S, Ebinger M, Baumann AM, et al. Development and validation of a dispatcher identifica-tion algorithm for stroke emergencies. Stroke 2012;43(3):776-81.
12 Ebinger M, Winter B, Wendt M, et al. Effect of the use of ambulance-based thrombolysis on time to thrombolysis in acute ischemic stroke: a randomized clinical trial. JAMA 2014;311(16):1622-31.
13 Ebinger M, Wendt M, Rozanski M, et al. Golden hour-thrombolysis by starting treatment before hospital arrival: the Pre-Hospital Acute Neurological Treatment and Optimization of Medical care in Stroke study (PHANTOM-S). Stroke 2014;45(Suppl 1):A104.
14 Anderson CS, Heeley E, Huang Y, et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N Engl J Med 2013;368(25):2355-65.
15 Saver JL, Starkman S, Eckstein M, et al. Methodology of the Field Administration of Stroke Therapy – Magnesium (FAST-MAG) phase 3 trial: Part 1 – rationale and general methods. Int J Stroke 2014;9(2):215-19.
16 Saver JL, Starkman S, Eckstein M, et al. Methodology of the Field Administration of Stroke Therapy – Magnesium (FAST-MAG) phase 3 trial: Part 2 – prehospital study methods. Int J Stroke 2014;9(2):220-5.
17 Rozanski M, Waldschmidt C, Kunz A, et al. Plasma Glial Fibrillary Acidic Protein(GFAP) for differentiation between hemorrhagic and ischemic strokes in pre-hospital stroke care. 9th World Stoke Congress, 22-25 October 2014, Poster 399.
18 Gyrd-Hansen D, Olsen KR, Bollweg K, et al. Cost-Effectiveness of Pre-hospital Thrombolysis. Results of the Pre-hospital Acute Neurological Treatment and Optimization of Medical care in Stroke (PHANTOM-S) Study. accepted. Neurology 2015;84(11):1090-1097.
19 Ebinger M, Kunz A, Wendt M, et al. Effects of Golden Hour Thrombolysis: a Prehospital Acute Neurological Treatment and Optimization of Medical Care in Stroke (PHANTOM-S) substudy. JAMA Neurol 2015;72(1):25-30.

143
Stroke: new therapiesAVC : nouveautés thérapeutiques© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
Ruptured aneurysm: clips or coils?
Vianney Gilard1, Sophie Curey1, Éléonore Tollard1, Olivier Langlois1, François Proust2 (1Rouen, 2Strasbourg)
IntRoductIon
In the past three decades, the field of endovascular treatment was largely ex-panded across the domain of neurovascular pathology [1]. The initial results of the International Study Aneurysm Trial (ISAT) confirm the predominant role of endo-vascular coiling in treating ruptured intracranial (IC) aneurysms [2, 3]. As a result of this, different societies across the world have established their position state-ments, favouring a concerted discussion between interventionists and neurosurgeons in reaching a decision [4-8]. The last publication from ISAT [9], about the late risk of recurrent subarachnoid haemorrhage (SAH), strengthens support for these new strategies with a high level of proof. This shift in medical practice leads to serious consequences for the vascular neurosurgeon but also for neurosurgery as whole.
A better understanding of the precise place of vascular neurosurgery in the field of IC aneurysm treatment is crucial to develop strategies with regard to preserving surgical expertise in our departments and to determining the course of scholarship. The objective of this paper is to analyse the lessons and limits of ISAT in order to de-termine the place of microsurgical clipping in the treatment of cerebral aneurysms.
What aRe the lessons fRom the RandomIzed studIes?
The comparative treatment of ruptured IC aneurysms has been analysed in four randomized studies [3, 9-11], ISAT being the predominant international study. The objective of all studies was to determine the safer procedures between endovascular coiling and microsurgical clipping.
dependency and death after treatment
After a pilot phase, the ISAT cohort published for the first time in 2002 [2], between May 1997 and April 2002, was composed of 2,143 patients in good clinical condi-tion at admission (94% in WFNS grade 1-3) with small ruptured aneurysms of the

Vianney Gilard, Sophie Curey, Éléonore Tollard, Olivier Langlois, François Proust
144
anterior circulation (97.3%), randomly assigned to an endovascular group (n = 1,073) and microsurgical group (n = 1,070). This trial, which recruited 2,500 patients to achieve a statistical power of 90% at a 0.01% level of significance to detect a 25% improvement in outcome at 1 year, was interrupted at a planned interim analysis. The definitive results were a reduction of the relative risk of dependence or death at 1 year of 23.9% (p<0.001) and an absolute risk reduction of 7.4% after endovascular treatment by comparison with microsurgical clipping. The case fatalities at 1 year were 7% and 7.9% among patients allocated to endovascular and microsurgical treatment. After a mean follow-up of 9 years of the ISAT cohort [9], the mortality rate at 5 years was significantly reduced in the coiling cohort, and the proportion of independent patients was similar in both arms. The last ISAT results addressing long-term follow-up (alive at 10 years), published in 2014 [12], reported that the probability of being alive with a good outcome (mRS 0–2) compared with death or dependence was significantly better for the group assigned to endovascular treat-ment than those assigned to neurosurgical clipping.
More recently, the Barrow Ruptured Aneurysm Trial (BRAT) conducted by experts in cerebrovascular neurosurgery compared 288 patients assigned to clip exclusion with 233 patients assigned to coil embolization [11]. At 1 year, an absolute risk reduction of 10.7% (p = 0.03) was observed after endovascular occlusion in com-parison with microsurgical clipping. At 3 years, this absolute risk reduction became 5.8% with no significance.
The French vascular section of vascular neurosurgery included 41 patients older than 70 years into a randomized study comparing the two procedures (submitted). At 6 months, the outcome was not significantly different between the two arms (p = 0.18), although the proportion of favourable outcomes was superior after en-dovascular coiling.
Recurrent subarachnoid haemorrhage
The primary objective of all treatment for ruptured aneurysms is to prevent a recur-rent SAH, which has a known mortality rate of 57% in these patients [13].
The ISAT study gives an excellent insight into recurrent SAH, dividing its occur-rence into three periods: before treatment, during the first year after treatment and beyond [3, 9]. The relative risk of rebleeding from the target aneurysm during the first year was 1.15 (95% CI: 0.75–1.75) after endovascular coiling in comparison with neurosurgical clipping. This non-significant result took into account all recur-rent SAHs before and after procedural exclusion.
In the course of the pre-procedural period, recurrent SAH occurred more fre-quently in the clipping arm (17 in the coiling arm vs. 28 in the clipping arm) with a non-significant level (relative risk: 0.6, 95% CI: 0.33–1.1). As the baseline char-acteristics of both treatment groups were matched, the only significant difference

145
Ruptured aneurysm: clips or coils?
was the timing delay between randomization and aneurysm exclusion (1.1 days for coiling vs. 1.7 days for clipping) [2]. This increasing rate of recurrence of SAH in proportion to the exclusion time confirmed the major risk of rebleeding (reaching ≈2–4% per day) during the first 4 weeks after the initial SAH [14].
After the procedure, the rebleeding rate at 1 year was significantly increased in the endovascular arm (χ2 Pearson test, p = 0.004) in comparison with the clipping arm. This high rebleeding rate could be related to the proportion of incomplete oc-clusion after endovascular treatment, which occurred in 66% of patients instead of a complete occlusion rate of 82% after neurosurgical treatment, despite only 49% of control angiography within this arm.
Beyond 1 year the global ratio of recurrent SAH decreased. After a long-term follow-up in the ISAT series (minimum of 6 years and maximum of 14 years), 17 patients experienced rebleeding in the endovascular arm compared with seven in the clipping arm, giving an incidence, respectively, of 0.21% per year and 0.09% per year [9].
At 10 years of follow-up, the cumulative risk of rebleeding from the target aneu-rysm (initial ruptured aneurysm) was 0.0216 for the patients treated by endovascular coiling and 0.0064 for those treated by neurosurgical clipping [12].
The BRAT study did not examined bleeding recurrence in the first year after an-eurysm treatment, but no recurrence of SAH was documented in the second or third year in either treatment group [11].
others results from Isat
Since 2005, the ISAT cohorts have reported secondary objectives such as the cogni-tive outcome, the elderly sub-group, the cost, and finally to extrapolate a global strategy for both treatments in the patients.
The neuropsychological analysis concerned the N-ISAT sub-sample drawn from ISAT enrolled in eight UK centres participating in this assessment protocol [15]. This sub-sample was representative of the main ISAT cohorts [16]. They confirmed the common existence of cognitive impairment in 32.1% of patients with favourable outcome (modified Rankin scale 0–2). Indeed, a reduction in the relative risk of cognitive impairment at 1 year of 31% (p<0.005) and an absolute risk reduction of 12% were observed after endovascular treatment in comparison with microsurgical clipping. Moreover, a greater number of cognitive domains were impaired in the neurosurgical group than the endovascular group, predominantly in the following domains: verbal memory, processing speed and executive skills. This study with valid neuropsychological tests was the largest ever study with full cognitive assess-ment as opposed to the classic short screening used in randomized studies.
The sub-group analysis of patients older than 70 years suggested surprisingly that there was less advantage for coiling than clipping [3]. This question is pertinent for several reasons: the longer life expectancies account for a significant number of elderly

Vianney Gilard, Sophie Curey, Éléonore Tollard, Olivier Langlois, François Proust
146
patients admitted with SAH, the incidence of SAH increases with advanced age [17], curative treatment was beneficial in this age class in comparison with conservative treatment despite a major risk of poor outcomes [18]. In spite of this, the sub-group was not pre-specified into the ISAT protocol, a sub-group of 278 randomly assigned patients older than 65 years was the subject of a second secondary analysis [19]. No difference was observed in the functional independence rate between the endo-vascular arm (60.1%) and the neurosurgical arm (56.1%). Nevertheless, the elderly patients with a middle cerebral artery (MCA) aneurysm who received neurosurgical clipping had a significantly better functional independence at 1 year than the coiled patients. For the other locations according to the χ2 test (anterior cerebral and anterior communicating artery, p = 0.7; internal carotid artery (ICA) and posterior com-municating artery, p = 0.06), no significant difference in functional independence was found between the two arms. Moreover, the thrombo-embolic event rate, when patients with parent artery occlusion, coil migration and thrombo-embolic problems were added, was significantly increased after endovascular treatment (p = 0.01), but a lower rate of epilepsy and pneumonia was observed. These results suggest that neurosurgical clipping should be the favoured treatment for elderly patients with ruptured aneurysm of the middle cerebral artery. However, these results may not be considered as coming from a valid randomized study, because the sub-group was not initially specified. For this reason, a French collaborative group developed a randomized study (www.clinicaltrial.gouv) between endovascular and neurosurgical treatment with regard to elderly patients (≥70 years) with ruptured aneurysms [20].
Regarding the cost of treatment, no significant difference at 12 months was found between both arms in Australia [21], Canada [22] or the UK [23]. These three coun-tries, using the data from their patients enrolled in ISAT, reported the same observa-tions: the coiled patients had higher costs related to medical expenses but this was offset by the reduction in cost related to the length of stay for the first procedure. Similar observations have already been reported from retrospective studies [24, 25]. Indeed, a change in paradigm from neurosurgical clipping to endovascular coiling does not lead to a change in the cost of treatment.
In summary, ISAT is a well-executed and statistically powerful study. Its large randomized population give some robust results to propose recommendations in the management of certain ruptured aneurysms. These different publications confirm the primary role of endovascular treatment in the management of ruptured cerebral aneurysms. It appears evident that patients and relatives should be proposed an early coiling in the first instance when the aneurysm sac is suitable for the two procedures.
In summary
During the past 20 years, randomized studies have confirmed endovascular coiling of aneurysms as a reference procedure, because this treatment significantly decreased the

147
Ruptured aneurysm: clips or coils?
risk of morbidity and mortality in comparison with microsurgical clipping. Moreover, the risk of rebleeding from the target aneurysm at 10 years of follow-up remained low and was not responsible for an increase in morbidity. The recommendation, by a mul-tidisciplinary team composed of interventional neuroradiologists and neurosurgeons, was to propose in the first instance endovascular coiling when the aneurysm sac is suitable for both procedures [8]. The worldwide impact of ISAT on the management of IC aneurysms explained the current predominance (47–81%) of endovascular coil-ing [26-29]. Consequently, the new generation of physicians in Europe and North America were less familiar with the surgical management of these lesions.
Nonetheless, at 5 and 10 years of follow-up, no significant difference in the rate of independent survivors was found between the endovascular group (82%) and the neurosurgery group (81%). Despite the alarmist predictions of the disappearance of clipping replaced by endovascular coiling for all IC aneurysms [30], in 2014 micro-surgical exclusion remains a suitable treatment largely proposed worldwide [31], and always considered as an element of the therapeutic arsenal against IC aneurysms in order to propose the suitable procedure for each patient. The future management of IC aneurysms requires the development of an educational programme.
advances In mIcRosuRgIcal exclusIon
Since the seminal neurosurgical work describing the fronto-temporal pterional flap to approach the anterior part of the circle of Willis [32], the microsurgical proce-dure has included in its arsenal the concept of a minimally invasive approach and intraoperative monitoring by indocyanine green (ICG) videoangiography. Moreover, the procedures of brain revascularization must be involved in the management of complex IC aneurysms as a protective and preventive technique against ischaemic complications.
minimally invasive craniotomy
Minimally invasive craniotomy is the response to the starkest contrast between femo-ral catheter access and craniotomy. The concept of keyhole craniotomy, described by Pernansky et al. [33], is suitable for IC aneurysms. Several options for craniotomy, minipterional, lateral supraorbital and orbito-pterional, have favoured the develop-ment of the supraorbital subfrontal approach [34]. The supraorbital approach is sufficient to expose the AcomA, the ICA and the MCA aneurysms with little or no retraction [35]. The challenge was to provide adequate exposure of IC aneurysms. Obviously, this small craniotomy remains indicated in the absence of intracranial hypertension. After a limited dissection of the sylvian fissure, helped by cotton, a gentle exovascular surgery under optical magnification permits a sharp and blunt
Vianney Gilard, Sophie Curey, Éléonore Tollard, Olivier Langlois, François Proust
148
dissection of the aneurysm. Besides this superciliary approach, the pretemporal transzygomatic transcavernous approach has been presented by Krisht et al. [36] for 50 patients with complex basilar aneurysms. Their results were impressive, valuing microsurgical treatment, with no procedure-related mortality and 92% of patients at a modified Rankin scale 0–2 at 6 months. The sac dissection requires a high technical skill in order to adjunct several measures such as gyrus rectus resection, extended craniotomy, interhemispheric dissection and control of aneurysm neck tear by the cotton-clipping technique [37]. Concerning clipping techniques, the procedures have evolved. A new design concept of clip, based on an inverted opening mechanism, allowed a wider opening of the clip jaw and better surgical vision [38]. The use of a fenestrated aneurysm clip can be safe in minimizing the retraction of microvasculari-zation before clipping [39].
Intraoperative videoangiography
Intraoperative monitoring concerned the parent vessel but also the microcirculation. Intraoperative digital subtraction angiography is the method of choice for intra-operative diagnoses of vessel patency or aneurysm occlusion, but to propose this procedure to unselected patients is unrealistic. This procedure may not become the standard procedure because of its expansive nature, time taken, the need for major logistical support and the invasive character of the procedure with its risk of compli-cations (0.4–2.6%) [40, 41]. For these reasons, microscope-based indocyanine green videoangiography is becoming a routine intraoperative procedure. Indocyanine green videoangiography provides information about the patency of the parent vessel and the existence of aneurysm remnants. Raabe et al. [42] showed that the sensitivity of vide-oangiography was 100% and the specificity was 95% to diagnose stenosis of the parent artery. Moreover, this procedure provides information about perforating arteries into the operative fields and helps verify their patency [43]. Finally, this procedure was used to verify the patency of extracranial-intracranial bypass [44]. This intraoperative control procedure is easy to apply, taking on average less than 2 minutes of time, and becomes a reliable assessment of the post-clipping result. The intraoperative micro-vascular Doppler is a reliable technique to analyse the velocity and turbulence of blood flow during the clip application [45-47]. Not being time-consuming and the low cost of Doppler flowmetry give to this procedure its efficiency and permits immediate clip reapplication in less than 2 minutes. Using a laser speckle contrast analysis may im-mediately assess relative cortical blood flow [48, 49], and these evaluation procedures are in development. Finally, the electrophysiology record in the territory of the middle cerebral artery allows verification of cortical microperfusion and the absence of is-chaemic consequences, and their efficiency appears essentially in temporary clipping [50, 51]. All these intraoperative procedures should be considered as complementary rather than competitive [52].
149
Ruptured aneurysm: clips or coils?
Brain revascularization procedures
These procedures are to evolve into a conceptual protection against ischaemia during the management of complex IC aneurysms. Bypass surgery has evolved since the extracranial-to-intracranial (EC-IC) bypass to intracranial-to-intracranial (IC-IC). From the superficial temporal artery-middle cerebral artery bypass [32], a second generation of bypass was developed using venous or arterial interposition grafts in response to flow limitations. A third generation of bypass is entirely intracranial, using other intracranial arteries without contribution from extracranial donor arter-ies. The procedure of cerebral revascularization currently developed for the giant aneurysm or cranial base tumours used the ELANA technique in order to avoid temporary clamping [53-57].
cuRRent IndIcatIon foR clIppIng
The indication for clipping must be envisaged in a collaborative neurovascular team that offers a balance of competence in the endovascular and microsurgical procedures. For each patient, treatment should be discussed in order to propose the optimal treatment directed to each aneurysm, but the results of ISAT and the current habit in Europe has favoured endovascular coiling when the two procedures seem equivalent in terms of efficiency. Within these conditions, microsurgical clipping is reserved for intracranial hypertension related to aneurysmal intraparenchymatous haematoma, complex aneurysms, dysplasia of arterial bifurcations, coiled aneu-rysms with recanalization and large and giant aneurysms.
Nevertheless, the combination of morphological criteria and patient characteristics may help in decision-making. Morphological criteria concerned the vascular ap-proach and the aneurysm features. The vascular approach may be made problematic by atherosclerosis or kinking vessels providing difficult access up to the aneurysm sac. The aneurysm characteristics may favour the endovascular or microsurgical approach according to the neck size, or the projection against the microvascular background [58]. The patient characteristics are also determined by age and co-morbidity. Intuitively, endovascular coiling would be expected to preserve cognitive functions in the arterial parent segment with perforating arteries such as the anterior communicating artery or basilar artery. The middle cerebral artery aneurysm, which is broad based, might be more suitable for clipping. Moreover, patients younger than 40 years of age should still be managed by craniotomy and clipping.
The preservation of the excellence and development of these complex strategies impose a significant effort in training medical and paramedical personnel. The cerebrovascular section of major neurosurgery societies must valorise several edu-cational approaches such as simulation, sharing expertise, international educational
Vianney Gilard, Sophie Curey, Éléonore Tollard, Olivier Langlois, François Proust
150
networks, and elaboration of a common educational programme with our neuroradi-ologist interventional colleagues.
References
1 Prestigiacomo CJ. Historical perspectives: the microsurgical and endovascular treatment of aneurysms. Neurosurgery 2006;59(5 Suppl 3):S39-47; discussion S3-13.
2 Molyneux A, Kerr R, Stratton I, et al. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet 2002;360 (9342):1267-74.
3 Molyneux AJ, Kerr RS, Yu LM, et al. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 2005;366(9488):809-17.
4 Derdeyn CP, Barr JD, Berenstein A, et al. The International Subarachnoid Aneurysm Trial (ISAT): a position statement from the Executive Committee of the American Society of Interventional and Therapeutic Neuroradiology and the American Society of Neuroradiology. AJNR Am J Neuroradiol 2003;24(7):1404-8.
5 Dormont D, Bonafe A, Cognard C, et al. [What about the ISAT results?]. J Neuroradiol 2003;30(5):286-8.
6 Kirkpatrick PJ, Kirollos RW, Higgins N, Matta B. Lessons to be learnt from the International Subarachnoid Haemorrhage Trial (ISAT). Br J Neurosurg 2003;17(1):5-7.
7 Raabe A, Schmiedek P, Seifert V, Stolke D. German Society of Neurosurgery Section on Vascular Neurosurgery: Position Statement on the International Subarachnoid Hemorrhage Trial (ISAT). Zentralbl Neurochir 2003;64(3):99-103.
8 Albucher JF, Morin-Surroca M. Recommendation about treatment of ruptured cerebral aneurysm: endovascular coiling versus microsurgical clipping. Paris: French National Authority for Health; 2009.
9 Molyneux AJ, Kerr RS, Birks J, et al. Risk of recurrent subarachnoid haemorrhage, death, or dependence and standardised mortality ratios after clipping or coiling of an intracranial aneurysm in the International Subarachnoid Aneurysm Trial (ISAT): long-term follow-up. Lancet Neurol 2009;8(5):427-33.
10 Vanninen R, Koivisto T, Saari T, et al. Ruptured intracranial aneurysms: acute endovascular treatment with electrolytically detachable coils – a prospective randomized study. Radiology 1999;211(2):325-36.
11 Spetzler RF, McDougall CG, Albuquerque FC, et al. The Barrow Ruptured Aneurysm Trial: 3-year results. J Neurosurg 2013;119(1):146-57.
12 Molyneux AJ, Birks J, Clarke A, et al. The durability of endovascular coiling versus neurosurgical clipping of ruptured cerebral aneurysms: 18 year follow-up of the UK cohort of the International Subarachnoid Aneurysm Trial (ISAT). Lancet 2014.
13 Johnston SC, Dowd CF, Higashida RT, et al. Predictors of rehemorrhage after treatment of rup-tured intracranial aneurysms: the Cerebral Aneurysm Rerupture After Treatment (CARAT) study. Stroke 2008;39(1):120-5.
14 Bederson JB, Connolly ES, Jr., Batjer HH, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke 2009;40(3):994-1025.

151
Ruptured aneurysm: clips or coils?
15 Scott RB, Eccles F, Lloyd A, Carpenter K. From multidimensional neuropsychological outcomes to a cognitive complication rate: the International Subarachnoid Aneurysm Trial. Trials 2008;9:13.
16 Scott RB, Eccles F, Molyneux AJ, et al. Improved cognitive outcomes with endovascular coil-ing of ruptured intracranial aneurysms: neuropsychological outcomes from the International Subarachnoid Aneurysm Trial (ISAT). Stroke 2010;41(8):1743-7.
17 de Rooij NK, Linn FH, van der Plas JA, et al. Incidence of subarachnoid haemorrhage: a system-atic review with emphasis on region, age, gender and time trends. J Neurol Neurosurg Psychiatry 2007;78(12):1365-72.
18 Proust F, Gerardin E, Derrey S, et al. Interdisciplinary treatment of ruptured cerebral aneurysms in elderly patients. J Neurosurg 2010;112(6):1200-7.
19 Ryttlefors M, Enblad P, Kerr RS, Molyneux AJ. International subarachnoid aneurysm trial of neurosurgical clipping versus endovascular coiling: subgroup analysis of 278 elderly patients. Stroke 2008;39(10):2720-6.
20 Proust F, Bracard S, Thines L, et al. [Aneurismal subarachnoid hemorrhage in the elderly subject. Should this patient participate in a randomized clinical trial?]. Neurochirurgie 2010;56(1):67-72.
21 Bairstow P, Dodgson A, Linto J, Khangure M. Comparison of cost and outcome of endovascular and neurosurgical procedures in the treatment of ruptured intracranial aneurysms. Australas Radiol 2002;46(3):249-51.
22 Javadpour M, Jain H, Wallace MC, et al. Analysis of cost related to clinical and angiographic outcomes of aneurysm patients enrolled in the international subarachnoid aneurysm trial in a North American setting. Neurosurgery 2005;56(5):886-94; discussion 94.
23 Wolstenholme J, Rivero-Arias O, Gray A, et al. Treatment pathways, resource use, and costs of endovascular coiling versus surgical clipping after aSAH. Stroke 2008;39(1):111-19.
24 Johnston SC. Effect of endovascular services and hospital volume on cerebral aneurysm treat-ment outcomes. Stroke 2000;31(1):111-17.
25 Ballet AC, Guerin J, Berge J, et al. [Neurosurgical and endovascular treatment of intracranial aneurysms: a cost analysis of two different strategies at the University Hospital of Bordeaux (France)]. Neurochirurgie 2002;48(5):419-25.
26 Mejdoubi M, Gigaud M, Tremoulet M, et al. Initial primary endovascular treatment in the man-agement of ruptured intracranial aneurysms: a prospective consecutive series. Neuroradiology 2006;48(12):899-905.
27 Crocker M, Corns R, Hampton T, et al. Vascular neurosurgery following the International Subarachnoid Aneurysm Trial: modern practice reflected by subspecialization. J Neurosurg 2008;109(6):992-7.
28 Cowan JA, Jr., Ziewacz J, Dimick JB, et al. Use of endovascular coil embolization and surgical clip occlusion for cerebral artery aneurysms. J Neurosurg 2007;107(3):530-5.
29 O’Kelly CJ, Kulkarni AV, Austin PC, et al. The impact of therapeutic modality on outcomes fol-lowing repair of ruptured intracranial aneurysms: an administrative data analysis. J Neurosurg 2010;113(4):795-801.
30 Maurice-Williams RS. Aneurysm surgery after the International Subarachnoid Aneurysm Trial (ISAT). J Neurol Neurosurg Psychiatry 2004;75(6):807-8.
31 Alshafai N, Cusimano MD, Falenchuk O. Global differences in the present and future manage-ment of cerebral aneurysms. World Neurosurgery 2013;80(6):717-22.
32 Krayenbuhl HA, Yasargil MG, Flamm ES, Tew JM, Jr. Microsurgical treatment of intracranial saccular aneurysms. J Neurosurg 1972;37(6):678-86.
33 Reisch R, Perneczky A. Ten-year experience with the supraorbital subfrontal approach through an eyebrow skin incision. Neurosurgery 2005;57(4):242-55 10.1227/01.NEU.0000178353.42777.2C.

Vianney Gilard, Sophie Curey, Éléonore Tollard, Olivier Langlois, François Proust
152
34 Figueiredo EG, Deshmukh V, Nakaji P, et al. An anatomical evaluation of the mini-supraorbital approach and comparison with standard craniotomies. Neurosurgery 2006;59(4 Suppl 2): ONS212 20; discussion ONS20.
35 Park J, Woo H, Kang DH, et al. Superciliary keyhole approach for small unruptured aneurysms in anterior cerebral circulation. Neurosurgery 2011;68(2 Suppl Operative):300-9; discussion 309.
36 Krisht AF, Krayenbuhl N, Sercl D, et al. Results of microsurgical clipping of 50 high complexity basilar apex aneurysms. Neurosurgery 2007;60(2):242-50; discussion 50-2.
37 Barrow DL, Spetzler RF. Cotton-clipping technique to repair intraoperative aneurysm neck tear: A technical note. Neurosurgery 2011;68(2 Suppl Operative):294-9; discussion 299.
38 Krammer MJ, Lumenta CB. The new aneurysm clip system for particularly complex aneurysm surgery: technical note. Neurosurgery 2010;66(6 Suppl Operative):336-8.
39 Zada G, Christian E, Liu CY, Giannotta SL. Fenestrated aneurysm clips in the surgical manage-ment of anterior communicating artery aneurysms: operative techniques and strategy. Clinical article. Neurosurg Focus 2009;26(5):E7.
40 Chiang VL, Gailloud P, Murphy KJ, et al. Routine intraoperative angiography during aneurysm surgery. J Neurosurg 2002;96(6):988-92.
41 Tang G, Cawley CM, Dion JE, Barrow DL. Intraoperative angiography during aneurysm surgery: a prospective evaluation of efficacy. J Neurosurg 2002;96(6):993-9.
42 Raabe A, Nakaji P, Beck J, et al. Prospective evaluation of surgical microscope-integrated intraop-erative near-infrared indocyanine green videoangiography during aneurysm surgery. J Neurosurg 2005;103(6):982-9.
43 de Oliveira JG, Beck J, Seifert V, et al. Assessment of flow in perforating arteries during intrac-ranial aneurysm surgery using intraoperative near-infrared indocyanine green videoangiography. Neurosurgery 2007;61(3 Suppl):63-72; discussion 73.
44 Woitzik J, Horn P, Vajkoczy P, Schmiedek P. Intraoperative control of extracranial-intrac-ranial bypass patency by near-infrared indocyanine green videoangiography. J Neurosurg 2005;102(4):692-8.
45 Marchese E, Albanese A, Denaro L, et al. Intraoperative microvascular Doppler in intracranial aneurysm surgery. Surg Neurol 2005;63(4):336-42; discussion 42.
46 Holscher T, Ozgur B, Singel S, et al. Intraoperative ultrasound using phase inversion harmonic imaging: first experiences. Neurosurgery 2007;60(4 Suppl 2):382-6; discussion 6-7.
47 Amin-Hanjani S, Meglio G, Gatto R, et al. The utility of intraoperative blood flow measure-ment during aneurysm surgery using an ultrasonic perivascular flow probe. Neurosurgery 2008;62(6 Suppl 3):1346-53.
48 Hecht N, Woitzik J, Dreier JP, Vajkoczy P. Intraoperative monitoring of cerebral blood flow by laser speckle contrast analysis. Neurosurg Focus 2009;27(4):E11.
49 Klein KU, Stadie A, Fukui K, et al. Measurement of Cortical Microcirculation during Intracranial Aneurysm Surgery by Combined Laser-Doppler Flowmetry and Photo-Spectrometry. Neurosurgery 2011.
50 Friedman WA, Chadwick GM, Verhoeven FJ, et al. Monitoring of somatosensory evoked poten-tials during surgery for middle cerebral artery aneurysms. Neurosurgery 1991;29(1):83-8.
51 Penchet G, Arne P, Cuny E, et al. Use of intraoperative monitoring of somatosensory evoked po-tentials to prevent ischaemic stroke after surgical exclusion of middle cerebral artery aneurysms. Acta Neurochir (Wien) 2007;149(4):357-64.
52 Gruber A, Dorfer C, Standhardt H, et al. Prospective comparison of intraoperative vascular monitoring technologies during cerebral aneurysm surgery. Neurosurgery 2011;68(3):657-73; discussion 73.

153
Ruptured aneurysm: clips or coils?
53 Abla AA, Lawton MT. Anterior cerebral artery bypass for complex aneurysms: an experience with intracranial-intracranial reconstruction and review of bypass options. Journal of Neurosurgery 2014;120(6):1364-77.
54 Bremmer JP, Verweij BH, Klijn CJ, et al. Predictors of patency of excimer laser-assisted nonoc-clusive extracranial-to-intracranial bypasses. Journal of Neurosurgery 2009;110(5):887-95.
55 Vajkoczy P, Korja M, Czabanka M, et al. Experience in using the excimer laser-assisted nonoc-clusive anastomosis nonocclusive bypass technique for high-flow revascularization: Mannheim-Helsinki series of 64 patients. Neurosurgery 2012;70(1):49-54; discussion 55.
56 van Doormaal TP, van der Zwan A, Redegeld S, et al. Patency, flow, and endothelialization of the sutureless Excimer Laser Assisted Non-occlusive Anastomosis (ELANA) technique in a pig model. Journal of Neurosurgery 2011;115(6):1221-30.
57 van Doormaal TP, van der Zwan A, van der Tweel I, et al. Optimization of the excimer laser assisted non-occlusive anastomosis (ELANA) flap retrieval rate. Lasers in Surgery and Medicine 2010;42(5):418-24.
58 Proust F, Debono B, Hannequin D, et al. Treatment of anterior communicating artery aneu-rysms: complementary aspects of microsurgical and endovascular procedures. J Neurosurg 2003;99(1):3-14.
154
Stroke: new therapiesAVC : nouveautés thérapeutiques© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
Treat cerebral venous thrombosis
Isabelle Crassard (Paris)
Cerebral venous thrombosis has been considered for a long time as a rare disease, often secondary to infection with a poor prognosis. It was very difficult to diagnose, diagnosis often only being made at autopsy. However, this perception has changed a great deal in recent years with new neuroradiological techniques coupled with improved treatment.
LiTTLe reminder abouT cerebraL venous Thrombosis
epidemiological data
Cerebral venous thrombosis can strike at any age from birth to old age with a mean age of 39 observed in the large studies. Its sex ratio is two to three women for every man, with a peak in incidence among young women because of specific risk factors, namely oestrogen-progestin birth control and pregnancy.
In the Netherlands, its incidence was recently estimated at 1.32 per 100,000 per-son-years, a rate similar to that of bacterial meningitis [1] and more common than suggested by the classic data. Further evidence comes from the large studies recently conducted by Lariboisière Hospital (450 patients included) and the large-scale International Study on Cerebral Vein and Dural Sinus Thrombosis (ISCVT), which covered 624 cases at 89 centres in 21 countries. Its frequency probably remains under-estimated, especially when it occurs without a stroke.
Thrombosis
Localisation and extent of involvement
Some of the features of cerebral venous thrombosis are distinct from those of arterial disease. Its localisation and the area affected are highly variable. In the ISCVT (n = 624) and the Lariboisière studies (n = 450), the lateral sinuses were involved in 73% of cases and the superior sagittal sinus in 62–65%. Less frequently, it involved the cortical veins (17–21%), the deep venous system (7–11%) or the cavernous sinus (2%).
In more than half of all cases, more than one sinus and/or vein is thrombosed.
155
Treat cerebral venous thrombosis
Because they have such thin walls, thrombosed cortical veins can become dilated and this often leads to reverse flow and development of a collateral circulatory pathway.
Causes and risk factors
Cerebral venous thrombosis can occur in a number of pathologies. The Lariboisière Study identified local causes (trauma, malformed vessels, tumours, etc. [9%]), infection (in neighbouring tissue or general infections like septicaemia or menin-gitis [6.5%]), systemic causes (systemic lupus erythematosus, Behcet’s disease, congenital thrombophilia, clotting disorders, cancer, haematological disorders, drug reactions, etc. [42%]) and gynaeco-obstetric causes (pregnancy, post-partum, oral contraceptives [22.5%]).
More than one cause or risk factor may be present so a full investigation is warranted. Even so, in 15–20% of cases, no risk factor is ever identified.
Polymorphism
Cerebral venous thrombosis is characterised by polymorphism in terms of both clinical picture and outcome. In contrast to arterial infarction, the mode of instal-lation is often variable and it can take a number of days. Onset is often marked by headache (observed in 90% of cases), possibly associated with papillary oedema if there is intracranial hypertension. Various clinical pictures are seen: focal syndrome in 50–80% of cases, isolated intracranial hypertension in 10–40% and sub-acute encephalopathy in 10–20%. Involvement of the cavernous sinus will give rise to local neuro-ophthalmological signs.
Some 15–20% of cases of cerebral venous thrombosis present atypically, e.g. as transient neurological signs or isolated headache.
Diagnosis
Because the aetiology and clinical picture are so varied in cerebral venous thrombo-sis (which can present as a combination of headache, focal deficit, epileptic seizures and impaired consciousness), diagnosis depends on neuroradiological techniques, in particular cerebral magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA). Cerebral MRI shows changes in the signal from the thrombosed sinus, which is not seen on the corresponding MRA image (Figure 1).
Parenchymatous lesions (diffuse or localised oedema, haemorrhagic lesions of varying size) are found in 40–50% of cases. These are usually aspecific and are rarely pathognomic so imaging of the parenchyma is mainly of use when it comes to differential diagnosis. However, lesions such as bithalamic involvement with thrombosis of the deep venous system and small juxtacortical haemorrhages (often bilateral) are highly suggestive of cerebral venous thrombosis.

Isabelle Crassard
156
Prognosis at six months
In the Lariboisière and ISCVT studies, full remission was observed at six months in 75% and 46% of cases, respectively, minor sequelae in 16% and 40%, severe sequelae in 6% and 7%, and death occurred in 3% and 7%.
Figure 1. Thrombosis of the superior sagittal sinus.Hypersignal from the thrombus in T1 (A) and T2 (B); hyposignal in T2* (C); sinus not seen in MRA (D).
157
Treat cerebral venous thrombosis
Function is conserved in most patients and death is far rarer than previously believed. The most common reason for death is a problem secondary to either significant brain damage (e.g. transtorial herniation), a status epilepticus, a pulmonary embolism or the underlying pathology (cancer, haematological disorder or severe infection).
How the acute phase evolves is variable and unpredictable. One-quarter of the ISCVT patients deteriorated in the acute phase. It is important to diag-nose cerebral venous thrombosis so that treatment can be started as soon as possible.
TreaTmenT oF cerebraL venous Thrombosis
Guidelines were published in Europe in 2010 and in North America in 2011 [2, 3]. Treatment relies on three strategies: antithrombotic heparin, managing symptoms (headache, intracranial hypertension and epilepsy) and treatment of the underlying condition (infection, systemic disease).
antithrombotic treatment
Heparin
For a long time, the place of heparin in the treatment of cerebral venous thrombosis was controversial because of fear of the existence of haemorrhagic forms. Since then, prospective and retrospective studies as well as two randomised studies have clearly established that patients benefit from heparin.
The randomised, controlled, double-blind Einhäupl Study published in 1991 assessed anticoagulation with intravenous heparin in the treatment of aseptic cerebral venous thrombosis in 20 patients (10 heparin, 10 placebo). The study was stopped early because, by three months, eight of the heparin patients had fully recovered and the other two showed mild, residual neurological deficit whereas, in the placebo group, only one patient had fully recovered, six had neurological deficit and three were dead (p<0.01). An additional retrospective study was conducted in patients with cerebral venous thrombosis associated with intracranial haemorrhage: 15% of patients treated with heparin died compared with 69% in the control group [4].
Another multicentric, placebo-controlled, double-blind study was published in 1999 by the Cerebral Venous Sinus Thrombosis Study Group. This included 59 patients who were given either low molecular weight heparin (LMWH) or placebo for three weeks. The course of LMWH was followed by oral anticoagulants for three months.
Twenty-four per cent of patients in the LMWH group had a negative outcome as defined by death or a Barthel Index of below 15 (risk differential: –4%; 95% CI: –25–17%; NS). After 12 weeks, 13% of patients in the LMWH group and 21% in the placebo group had a negative outcome as defined by death or an Oxford

Isabelle Crassard
158
Handicap Score of 3 or above (risk differential: –7%; 95% CI; –26–12%; NS). No new symptomatic cerebral haemorrhages were detected [5].
A meta-analysis of studies of heparin in cerebral venous thrombosis shows a 14% decrease in the risk of death (95% CI: –6–36%) and a 16% decrease in the risk of death or handicap (95% CI: –6–37%).
In consequence, the guidelines propose administering heparin to patients with cerebral venous thrombosis, either unfractionated heparin or LMWH [2, 3].
Comparison of unfractionated heparin and LMWH
A small randomised study compared LMWH (n = 34) and unfractionated heparin (UFH, n = 32) in the treatment of cerebral venous thrombosis. Mortality was 19% in the UFH group compared with zero in the LMWH group. More patients in the LMWH group had recovered by three months (88% vs 62.5%) and the incidence of severe bleeding was 9.5% in the UFH group compared with zero in the LMWH group [6].
Despite weaknesses, the results of this study seem to indicate that LMWH may be more effective.
In the ISCVT study, 302 patients were treated with UFH and 119 on LMWH. Recovery was better in patients on LMWH and both mortality and the incidence of new intra cranial haemorrhage were higher in the UFH group (Table 1) [7].
Therefore, the available data seem to encourage prescribing LMWH as long as there is no significant contraindication (kidney failure or imminent surgery).
Table 1. Comparison of UFH and LMWH in the treatment of cerebral venous thrombosis, data from the ISCVT [7]
uFh (n = 302)
LmWh (n = 119)
or
Recovery (mRS to 2) at 6 months
84% 92% 2.4 (95% CI: 1.0–5.7) p = 0.04
Complete recovery (mRS 0–1)
78% 78% 0.94 (95% CI: 0.55–1.9) p = 0.94
Deaths 8% 6% 0.81 (95% CI: 0.29–2.3) p = 0.70
New IC haemorrhage
16% 10% 0.29 (95% CI: 0.07–1.3) p = 0.10
LMWH: low molecular weight heparin; UFH: unfractionated heparin; IC: intracranial; OR: odds ratio.

159
Treat cerebral venous thrombosis
Vitamin K antagonists and new oral anticoagulants to follow up heparin
As soon as the clinical situation has stabilised, the patient is switched from heparin to a vitamin K antagonist (VKA). The length of this course of treatment will depend on the underlying cause: in the absence of any factor indicating long-term anticoagulant treatment, it is 6–12 months.
The place of the new oral anticoagulants is still undefined and the literature is lim-ited to reports on odd cases: two patients treated with dabigatran [8] and a comparison of 7 patients treated with rivaroxaban versus 9 patients treated with a VKA [9]. All of these patients improved but there is as yet not enough data to draw a solid conclusion.
symptomatic treatments
Headache
Headache can be severe in cerebral venous thrombosis but it usually gets better within a matter of days of starting heparin. Simple analgesics are usually adequate and morphine derivatives are rarely needed.
For the special case of isolated intracranial hypertension, cerebrospinal fluid is drained by lumbar puncture before the heparin: this is associated with the prescrip-tion of acetazolamide and usually improves the headache and helps control visual function.
Epileptic seizures
Antiepileptic treatment is always administered in a patient with epileptic seizures. Which drug is used should take into account interactions with the VKA. The consensus position is to stop treatment after one year as long as there have been no new seizures and EEG results are normal.
aetiological treatment
Whenever possible, the aetiological treatment should be adapted to the underlying condition. This is particularly important for septic forms that should be treated with effective antibiotics matching the entry point, and sometimes surgery. Similarly, specific treatment may be indicated for certain intercurrent systemic diseases, such as cancer and haematological disorders.
TreaTing severe Forms
The type of care described above suffices in 90% of cases but treating the 10% of patients with the severest forms is far more difficult.
Severity may be due to the aetiology, e.g. a serious haematological disorder or severe anaemia due to chronic bleeding.

Isabelle Crassard
160
Cerebral venous thrombosis can also present as a serious neurological problem from the outset or deteriorate secondarily to status epilepticus or pulmonary embolism.
surgery
Surgery can be considered in patients in the acute phase who are at risk of cerebral herniation, either because of major damage to the cerebral parenchyma or malignant cerebral oedema.
Surgical decompression was investigated in a retrospective study of 12 patients. Malignant forms of cerebral venous thrombosis were defined as: 1) presence of supratentorial cortical lesions; 2) evidence of clinical involvement (impaired consciousness, dilatation of the pupils) or radiological signs; 3) from the outset or after deterioration despite heparin treatment.
With malignant deterioration, all the patients bar one developed haemorrhagic le-sions; median deviation of the septum pellucidum was 12 millimetres, five patients (three of whom had been operated on) developed mydriasis on one side and four (two operated) on both sides. Eight patients underwent surgical decompression, ei-ther external (n = 4), external + internal (n = 3) or internal (n = 1). The four patients who were not operated on died within five days of diagnosis. One operated patient died of a pulmonary embolism but the other seven recovered well within a median time of 23.1 months [10].
In a study of 69 patients (including 31 case histories from the literature), decom-pressive hemicraniectomy was carried out in 45 of them, drainage of the haematoma in 7 and both procedures in 17. At the last follow-up (median = 12 months), 37% scored 0–1 on the modified Rankin Scale (mRS) with 56.5% scoring 0–2—a very good functional outcome given the patients’ clinical condition at baseline. On this date, 5.8% of the patients were alive with a score of 4–5, and 15.9% had died. Three of the 9 patients with both pupils fixed recovered fully [11].
Thus, surgical decompression seems to save lives and affords good functional outcomes in malignant cerebral venous thrombosis.
endovascular thrombolysis
Fibrinolytics have been in use since 1971. A meta-analysis published in 2003 covered 72 studies (including no controlled trials) and a total of 169 patients. The patients had been treated with urokinase (n = 127) or tissue plasminogen activator (rt-PA, n = 37). Thrombectomy was also performed in 16 patients. The patients were all in a serious clinical condition (coma: 28%, encephalopathy: 52%, focal syndrome: 7%, intracranial hypertension: 13%). Thirty-three per cent had bleeding on the initial imaging and there was deep venous system involvement in 31%. Only 6% of the patients died and good clinical recovery was documented in 58% [12].
161
Treat cerebral venous thrombosis
A new meta-analysis published in 2010 covered 15 retrospective and prospec-tive studies (each on 5–20 patients) with a total of 156 patients, 30% of whom had bleeding on the initial imaging. Of these, 71% were administered urokinase and 29% were administered rt-PA. The authors paid special attention to compli-cations of the treatment: severe bleeding (9.8%), new symptomatic intracranial haemorrhaging (7.6%) and death (9.2%, half of which cases were related to new bleeding) [13].
The place of this modality therefore remains to be established and it remains reserved for patients in a coma or whose condition deteriorates despite best medical treatment. A randomised study, the TO-ACT Study, is currently under way and the results should come out in 2018 [14].
concLusion
Cerebral venous thrombosis is a rare disease but its prognosis is far better than that of an arterial infarct. It can be caused by a variety of problems and its clinical picture is relatively non-specific. This diagnosis should be frequently considered. Treatment should be started as soon as the condition has been confirmed by imaging. Basic treatment is heparin (even when there is bleeding) combined with drugs to manage symptoms and, if possible, treatment of the underlying condition. More aggressive modalities such as decompression surgery may be considered in a patient with ma-lignant oedema. Endovascular thrombolysis may be considered although its place in treatment remains to be established.
references
1 Coutinho JM, Zuurbier SM, Aramideh M, Stam J. The incidence of cerebral venous thrombosis: a cross-sectional study. Stroke 2012;43:3375-7.
2 Einhäupl K, Stam J, Bousser MG, et al. EFNS guideline on the treatment of cerebral venous and sinus thrombosis in adult patients. Eur J Neurol 2010;17:1229-35.
3 Saposnik G, Barinagarrementeria F, Brown RD, Jr, et al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2011;42:1158-92.
4 Einhäupl KM, Villringer A, Meister W, et al. Heparin treatment in sinus venous thrombosis. Lancet 1991;338:597-600.
5 de Bruijn SFTM, Stam J, for the Cerebral Venous Sinus Thrombosis Study Group. Randomized, Placebo-Controlled Trial of Anticoagulant Treatment With Low-Molecular-Weight Heparin for Cerebral Sinus Thrombosis. Stroke 1999;30:484-8.
6 Misra UK, Kalita J, Chandra S, et al. Low molecular weight heparin versus unfractionated hepa-rin in cerebral venous sinus thrombosis: a randomized controlled trial. Eur J Neurol 2012;19: 1030-6.
7 Coutinho JM, Ferro JM, Canhão P, et al. Unfractionated or low-molecular weight heparin for the treatment of cerebral venous thrombosis. Stroke 2010;41:2575-80.
Isabelle Crassard
162
8 Hon SF, Li HL, Cheng PW. Use of direct thrombin inhibitor for treatment of cerebral venous thrombosis. J Stroke Cerebrovasc Dis 2012;21:915.e11-5.
9 Geisbüsch C, Richter D, Herweh C, et al. Novel factor xa inhibitor for the treatment of cerebral venous and sinus thrombosis: first experience in 7 patients. Stroke 2014;45:2469-71.
10 Théaudin M, Crassard I, Bresson D, et al. Should decompression surgery be performed in malig-nant cerebral venous thrombosis?: a series of 12 patients. Stroke 2010;41:727-31.
11 Ferro JM, Crassard I, Coutinho JM, et al. Decompression surgery in cerebrovenous thrombosis: a multicenter registry and a systematic review of individual patient data. Stroke 2011;42:2825-31.
12 Canhão P, Falcão F, Ferro JM. Thrombolytics for cerebral sinus thrombosis: a systematic review. Cerebrovasc Dis 2003;15:159-66.
13 Dentali F, Squizzato A, Gianni M, et al. Safety of thrombolysis in cerebral venous thrombosis. A systematic review of the literature. Thromb Haemost 2010;104:1055-62.
14 Coutinho JM, Ferro JM, Zuurbier SM, et al. Thrombolysis or anticoagulation for cerebral venous thrombosis: rationale and design of the TO-ACT trial. Int J Stroke 2013;8:135-40.

163
Stroke: new therapiesAVC : nouveautés thérapeutiques© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
What’s new in post-stroke rehabilitation?
Philippe Marque (Toulouse)
This presentation mostly concerns the motor aspects of post-stroke rehabilitation, and specifically the hemiplegia, which is the most common feature in this situation.
EFFICACY OF REHABILITATION FOLLOWING A STROKE
A recent meta-analysis [1] has compiled the randomised controlled trials on motor rehabilitation post-stroke. The studies selected included a total of 25,373 patients.
Firstly, this meta-analysis showed that the quality of trials has improved over time, with a median PEDro score (an 11 item scale used to assess the internal validity of the trial), which has increased from 4 before 2004 to 6 for trials published after that date.
Secondly, it appears that no adverse effects associated with motor rehabilitation post-stroke have been reported and that we have solid evidence that it is effective in recovering walking, hand and forearm motor function and independence (activities of daily living). Similar results have been consistently found in all of the meta-analyses over more than 2 decades [2].
Factors involved in efficacy that are consistently found are early institution of motor rehabilitation, together with its intensity and a multi-disciplinary approach. The utility of motor rehabilitation in the first week post-stroke, however, remains contentious, because of the existence of a vasogenic oedema. A PRHC (hospital clinical research programme) assessing the merits of physical exercise in the initial hours following the stroke is currently ongoing.
The optimal intensity of motor rehabilitation has not been entirely established, although published findings show that daily exercise is preferable to exercise three times per week, that 3 hours of exercise per day are preferable to thirty minutes per day, although at the same time, the 3 hours per day are more effective than 6 hours of daily management [1, 3]. The intensity of care is therefore an essential component of the effectiveness of rehabilitation, although a ceiling effect is seen as excessively long rehabilitation times or excessive intensity may have a counter-productive effect.
Finally, these large meta-analyses have emphasised the team effect. Multi-disciplinary care is needed in order to approach all aspects of motor rehabilitation,

Philippe Marque
164
and involve a coordinated approach by physiotherapists, ergotherapists, orthopho-nists, neurologists and physical medicine and rehabilitation physicians [4].
WHAT IS THE RIGHT POST-STROKE TECHNIQUE?
Conventional motor rehabilitation techniques
Before 2000, motor rehabilitation was based on several empirical techniques (Bobath, Brunnstrom, Perfetti, etc.), which involve very different and occasionally opposing concepts. The Bobath and Brunnstrom techniques are developed from radically different approaches. Physical exercise and therefore muscle strengthening are prohibited in the Bobath technique, as these are assumed to increase the spastici-ty. Reflex reactions are inhibited and considered to be archaïc. Conversely, reflex reactions are used and reinforced in the Brunnstrom technique, as these are seen as the elementary motility in this method. The increased spasticity that may result from this is considered to be transient and not to have adverse consequences on motility. Eleven trials have compared these different methods, although none has emerged as being superior to the other [3, 5].
Similarly, muscle strengthening, which is penalised with the Bobath technique, has been shown to be effective in hemiplegic patients with a gain in strength and functional benefits [6-8]. At the same time, it has been shown to be well tolerated and not to worsen patients’ spasticity, which may increase temporarily with fatigue during exercise, although this increase does not persist in the long term [9, 10].
As a result, while there is a consensus from the clinical meta-analyses about the positive effect of motor rehabilitation after stroke, the different results show that the type of exercise or re-education technique used to obtain this effect are still largely unknown.
Animal models
Enriched environment model in the rat
The enriched environment model involves rearing animals in a group in spacious cages with various objects to stimulate their curiosity and manipulation, etc. This environment in which the animals can interact socially promotes exploration and a large range of experiences and helps to increase spontaneous physical activity. Any dispensing device requiring the animal’s paw be used in order to grasp a feed pellet can be used to strengthen the use of a paretic anterior limb (see Figure 1).
Rehabilitation in such an environment after a local ischaemic injury has been shown to promote the improvement in anterior limb muscle function and is associ-ated anatomically with greater synaptic budding of neurones than is seen in animals that are housed in individual cages [11].

165
What’s new in post-stroke rehabilitation?
Constraint-induced therapy
Intracortical micro stimulation mapping techniques have been used to produce de-tailed maps of the cortical representation of the hand and upper limb in the monkey. Nudo and colleagues found that after electrocoagulation-induced stroke of the hand motor area, areas representing the hand and wrist developed in the healthy cortex adjacent to the injury. If the paretic limb was not used, the surface area of these regions reduced gradually over time. Conversely, in the case of rehabilitation with constraint of the healthy hand, requiring the animal to use its deficient hand was accompanied by an increase in the surface area of the hand and wrist regions and better clinical recovery (see Figure 2).
Recovery of functions following a stroke is therefore accompanied by cerebral plasticity mechanisms such as reorganisation of the sensory motor maps, which are dependent on use through a competitive mechanism: if not used, these new areas representing the hand are taken over by representations of the shoulder and elbow [13-15].
Applications in humans
Animal findings are consistent with the results of work carried out in humans, which show the existence of competitive cortical representation effects. In an arm amputee, for example, the area in the side in which the afferent hand signal has been removed is gradually invaded by representations of the shoulder [16]. These competitive cortical representation effects develop very rapidly. Motor Evoked Potentials (MEP) in the forearm muscles of normal people before, during and after blockade through ischaemia produced by a forearm and hand tourniquet have been recorded in order to study the chronology of the changes. Deltoid muscle MEP amplitudes increased
Figure 1. Example of the enriched environment. Reproduced from Murphy and Corbett [12].

Philippe Marque
166
rapidly as the ischaemia was produced and then returned to their previous levels when the tourniquet was removed. The increase in magnitude of the deltoid MEP was inversely proportional to the reduction in the amplitude of the abductor pollicis produced by the tourniquet-induced ischaemia. During the same time period the MEPs for the contralateral arm were not changed [17].
Since these studies were performed, constraint-induced therapy has been widely used in post-stroke rehabilitation and the method has been validated on large num-bers of patients. The cohort of Taub et al., which was randomly assigned against a
Digit training cases:digit, Wrist/Forearm representations
Pre-training Post-trainingdigitwrist/fadigit+wrist/faproximalno response
R
M
digit
pre
pre
pre
% to
tal
0
20
40
60
80
wrist/fa digit+w/fa
post
post
post
fingers
spontaneous change after constraint therapy
Act
ivat
ion
area
(%
)
-80
-60
-40
-20
0
20
40
60
hand wrist
Figure 2. Change in cortical representation areas for the fingers, hand and wrist in constraint therapy. Reproduced from Nudo and colleagues [13, 14].
167
What’s new in post-stroke rehabilitation?
placebo, included several hundreds of patients and showed greater use of the paretic upper limb in activities of daily living in the treatment group [18]. In parallel, and mimi cking animal studies, the effects of treatment can be demonstrated using tran-scranial magnetic stimulation (TMS) mapping techniques [19].
Other techniques
Electromyogram biofeedback
Electromyogram biofeedback is a technique using electrodes positioned on the patient’s muscles to generate a feedback signal (visual or auditory) in a response to activation of the muscle. It has been well validated and has a demonstrable impact on recovery after a stroke [1].
Rehabilitation robots
The major limitation of constraint-induced therapy is that it can only be used in patients who have good quality, preserved residual motor function, i.e. one that includes the thumb–index finger pinch. Tools that mobilise the paralysed limb are required in other patients. Rehabilitation robots have therefore gained an increas-ingly large place in the rehabilitation literature over the past 15 years (see Figures 3 and 4).
For the upper limbs, the meta-analyses show improvement in motor deficit and motor function in activities of daily living [20].
The utility of re-education robots in recovery of gait, however, remains controver-sial and the results of meta-analyses are inconsistent. The most recent publications show that re-education robots have little benefit in patients who have preserved residual walking ability, although significant benefit is achieved in patients who have been totally deprived of their walking ability and are treated early [21].
THE CRITICAL PERIOD
There are critical periods for learning in new-born infants (reading, language, pra-xia), beyond which these are far more difficult. These findings can be extrapolated to patients who have suffered a stroke.
We have shown in a clinical study using an experimental paradigm with TMS to assess cerebral plasticity in hemiplegic patients that the brain has extensive plastic capacity three months after the stroke, although this capacity has fallen greatly at one year post-stroke [22].
A study in the rat has assessed the effectiveness of enriched rehabilitation started on the fifth, 14th or 30th day after local ischaemia on functional results and neuro-morphological changes. Administration of the treatment from day 5 produced better

Philippe Marque
168
Figure 3. Re-education robot used in upper limb motor rehabilitation. [Médimex company, Sainte-Foy-lès-Lyon, France].
Figure 4. Re-education robot used in lower limb motor rehabilitation. [Médimex company, Sainte-Foy-lès-Lyon, France].

169
What’s new in post-stroke rehabilitation?
results and the possibilities for recovery fell greatly beyond 15 days. These findings suggest that post-stroke the brain has greater sensitivity to early rehabilitation therapy but that this falls over time. This phenomenon is believed to involve mechanisms that facilitate and inhibit cerebral plasticity, the facilitating mechanisms coming into action far earlier than the inhibitory mechanisms [23].
Beyond this period, the results do not mean that no plasticity is possible but that regulatory mechanisms for this effect come into play, resulting in these limitations in adults.
WHAT WILL WE BE DOING IN THE FUTURE?
Cerebral stimulations
Repetitive transcranial magnetic stimulation (rTMS) can be distinguished from transcranial direct current stimulation (tDCS).
Electrical stimulations are used in a recent approach for treating the brain-damaged patient. Inter-hemispheric inhibition has been demonstrated not only at rest [24] but also during movement [25]. Murase et al. [25] showed that the removal of inter-hemispheric inhibition seen in healthy people in the 20 ms before movement was reduced or absent in hemiplegic patients. This type of result is consistent with some functional image findings, which show increased activation of the motor cortex from the healthy side and inactivation of the cortex on the injured side during the 15 days after a sub-cortical vascular injury [26]. A hypothesis has been advanced to explain these results, through which over-activation of the healthy hemisphere is the result of the injury to the contralateral hemisphere and the reduced inter-hemispheric inhibi-tion that occurs as a result of this. Following this, the overactive healthy hemisphere would cause an increasing inhibition of the injured hemisphere and an increase in the motor deficit. The concept of an appropriate plasticity has been proposed to describe this upset in the intra-hemispheric balance.
If we accept this hypothesis, therapeutic interventions in hemiplegic patients either through rehabilitation or cerebral stimulation must aim to stimulate the injured hemi-sphere and/or inhibit the healthy hemisphere in order to restore the inter-hemispheric balance. Non-invasive cerebral stimulations are particularly suitable for this type of programme.
rTMS involves emitting a series of impulses over a given period of time in order to produce lasting change to the activity of the targeted region. The after effects on MEP amplitude and therefore on the excitability of the cortex depend on the frequency, duration and number of stimulations applied. Low-frequency rTMS stimulations (1 Hz) have an inhibitory effect, whereas high-frequency stimulations have a facilitating effect.

Philippe Marque
170
tDCS involves applying a continuous low-intensity current through 2 polarised electrodes: the positive electrode or anode and the negative electrode or cathode. MEP assessment demonstrates an increase in cortical excitability beneath the anode and reduced excitability beneath the cathode [27].
Hummel and colleagues carried out a double blind placebo-controlled crossover study to test the hypothesis through which non-invasive stimulation of the motor cortex could improve motor function in the paretic hand of stroke patients in the chronic phase. Motor function in the hand was measured using the Jebsen Taylor hand function test (JTT). The JTT in the paretic hand improved considerably with tDCS but did not improve in the placebo group. This effect lasted beyond the stimu-lation period, was found in all patients and correlated with an increase in cortical motor excitability in the affected hemisphere, seen as increased recruitment curves and a reduction in the short-term intracortical inhibition [28].
Many studies using rTMS or tDCS have been carried out. Some of these have been disappointing and have not shown the expected benefits. Many questions remain to be answered such as the type of cortical neuromodulation that can be used (fa-cilitating or inhibitory rTMS, transcranial magnetic stimulation, paired associative stimulation, tDCS) and the means of using these.
Brain–machine interface and rehabilitation
So-called non-invasive brain–machine interfaces use an electroencephalogram (EEG) in the treatment of patients with severe handicap. These devices record the cerebral activity by a mental task and provide the patients with quantitative and qualitative feedback about their cerebral activity, enabling them to learn to control this with a view to running various technical aids.
The group working with Birbaumer, a pioneer in the brain–machine interface, has carried out a double blind placebo-controlled trial to assess the benefit of daily train-ing with the brain–machine interface compared to physiotherapy alone in patients with severe paresis.
Thirty-two chronic patients with severe arm and hand weakness were included. The patients were asked to activate an elbow or finger extension movement through their imagination. Two patient groups were established: the intervention group in which the increase in β and µ frequencies in the EEG activity triggered the functioning of a robot enabling the chosen movement to be performed, and a sham group in which the robot movements were independent of changes in EEG activity. Encouraging results were obtained with an improvement in the Fugl–Meyer motor score for the upper limb and lateralisation index on functional magnetic resonance imaging represent-ing improved activation of the injured hemisphere [29].
The use of brain–machine interfaces in motor rehabilitation appears to be a prom-ising approach.

171
What’s new in post-stroke rehabilitation?
CONCLUSION
Post-stroke rehabilitation methods are changing profoundly, bringing into question the conventional techniques used by physiotherapy teams. The current strap line is ‘use it or lose it’, and new tools are already available or will become available.
References
1 Veerbeek JM, van Wegen E, van Peppen R, et al. What is the evidence for physical therapy post-stroke? A systematic review and meta-analysis. PLoS One 2014;9:e87987.
2 Ottenbacher KJ, Jannell S. The results of clinical trials in stroke rehabilitation research. Arch Neurol 1993;50:37-44.
3 Kwakkel G, van Peppen R, Wagenaar RC, et al. Effects of augmented exercise therapy time after stroke: a meta-analysis. Stroke 2004;35:2529-39.
4 Langhorne P, Bernhardt J, Kwakkel G. Stroke rehabilitation. Lancet 2011;377:1693-702.5 Kollen BJ, Lennon S, Lyons B, et al. The effectiveness of the Bobath concept in stroke rehabilita-
tion: what is the evidence? Stroke 2009;40:e89-97.6 Logigian MK, Samuels MA, Falconer J, Zagar R. Clinical exercise trial for stroke patients. Arch
Phys Med Rehabil 1983;64:364-7.7 Engardt M, Knutsson E, Jonsson M, Sternhag M. Dynamic muscle strength training in stroke
patients: effects on knee extension torque, electromyographic activity, and motor function. Arch Phys Med Rehabil 1995;76:419-25.
8 Sharp SA, Brouwer BJ. Isokinetic strength training of the hemiparetic knee: effects on function and spasticity. Arch Phys Med Rehabil 1997;78:1231-6.
9 Brown DA, Kautz SA. Increased workload enhances force output during pedaling exercise in persons with poststroke hemiplegia. Stroke 1998;29:598-606.
10 Smith GV, Silver KH, Goldberg AP, Macko RF. “Task-oriented” exercise improves hamstring strength and spastic reflexes in chronic stroke patients. Stroke 1999;30:2112-18.
11 Biernaskie J, Corbett D. Enriched rehabilitative training promotes improved forelimb motor func-tion and enhanced dendritic growth after focal ischaemic injury. J Neurosci 2001;21:5272-80.
12 Murphy TH, Corbett D. Plasticity during stroke recovery: from synapse to behaviour. Nat Rev Neurosci 2009;10:861-72.
13 Nudo RJ, Milliken GW, Jenkins WM, Merzenich MM. Use-dependent alterations of movement representations in primary motor cortex of adult squirrel monkeys. J Neurosci 1996;16:785-807.
14 Nudo RJ, Wise BM, SiFuentes F, Milliken GW. Neural substrates for the effects of rehabilitative training on motor recovery after ischaemic infarct. Science 1996;272:1791-4.
15 Milliken GW, Plautz EJ, Nudo RJ. Distal forelimb representations in primary motor cortex are redistributed after forelimb restriction: a longitudinal study in adult squirrel monkeys. J Neurophysiol 2013;109:1268-82.
16 Kew JJ, Ridding MC, Rothwell JC, et al. Reorganization of cortical blood flow and transcra-nial magnetic stimulation maps in human subjects after upper limb amputation. J Neurophysiol 1994;72:2517-24.
17 Brasil-Neto JP, Cohen LG, Pascual-Leone A, et al. Rapid reversible modulation of human motor outputs after transient deafferentation of the forearm: a study with transcranial magnetic stimula-tion. Neurology 1992;42:1302-6.
18 Taub E, Uswatte G, Mark VW, Morris DM. The learned nonuse phenomenon: implications for rehabilitation. Eura Medicophys 2006;42:241-56.

Philippe Marque
172
19 Liepert J, Bauder H, Wolfgang HR, et alC. Treatment-induced cortical reorganization after stroke in humans. Stroke 2000;31:1210-16.
20 Mehrholz J, Hädrich A, Platz T, et al. Electromechanical and robot-assisted arm training for improving generic activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst Rev 2012;6:CD006876.
21 Mehrholz J, Elsner B, Werner C, et al. Electromechanical-assisted training for walking after stroke. Cochrane Database Syst Rev 2013;7:CD006185.
22 Castel-Lacanal E, Marque P, Tardy J, et al. Induction of cortical plastic changes in wrist muscles by paired associative stimulation in the recovery phase of stroke patients. Neurorehabil Neural Repair 2009;23:366-72.
23 Biernaskie J, Chernenko G, Corbett D. Efficacy of rehabilitative experience declines with time after focal ischaemic brain injury. J Neurosci 2004;24:1245-54.
24 Ferbert A, Priori A, Rothwell JC, et al. Interhemispheric inhibition of the human motor cortex. J Physiol 1992;453:525-46.
25 Murase N, Duque J, Mazzocchio R, Cohen LG. Influence of interhemispheric interactions on motor function in chronic stroke. Ann Neurol 2004;55:400-9.
26 Loubinoux I, Carel C, Pariente J, et al. Correlation between cerebral reorganization and motor recovery after subcortical infarcts. Neuroimage 2003;20:2166-80.
27 Nitsche MA, Paulus W. Excitability changes induced in the human motor cortex by weak tran-scranial direct current stimulation. J Physiol 2000;527:633-9.
28 Hummel F, Celnik P, Giraux P, et al. Effects of non-invasive cortical stimulation on skilled motor function in chronic stroke. Brain 2005;128:490-9.
29 Ramos-Murguialday A, Broetz D, Rea M, et al. Brain–machine interface in chronic stroke reha-bilitation: a controlled study. Ann Neurol 2013;74:100-8.

173
Stroke: new therapiesAVC : nouveautés thérapeutiques© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
Preventing cerebral infarction
Emmanuel Touzé (Caen)
When to Prevent cerebral infarction and hoW?
Seventy-five per cent of cerebrovascular accidents (CVA) are first events. Primary prevention is therefore vital but secondary prevention too is as necessary given the high rate of recurrence: about 3% within 30 days, 10% within a year, 25% within 5 years and 40% within 10 years [1].
Preventive measures have to match the cause of the cerebral infarct. Ischaemic accidents (infarcts and transient ischaemic attacks [TIAs]) account for 85% of CVAs. The main causes are atherosclerosis (20%), disease of the small arteries (25%) and emboli from the heart (20%). Although management of these different types of CVA has common features, specificities nevertheless have to be taken into account.
Be it for primary or secondary prevention and whatever the cause of the event, prevention depends on three issues: 1) managing vascular risk factors; 2) anti-platelet and anticoagulant drugs; 3) surgical and endovascular revascularisation techniques.
imPortance of risk factors
Epidemiological surveys have shown that just ten risk factors account for 90% of cerebral infarcts, namely hypertension, current smoking, abdominal obesity, lack of physical exercise, diabetes, alcohol consumption, psychological stress, depression, heart disease (atrial fibrillation [AF], flutter, myocardial infarction, rheumatic valve disease, heart valve replacement) and apo B/apo A1 ratio [2].
Traditionally, distinction has been made between modifiable and unmodifi-able risk factors. The former are age, racial origin, genetic factors, gender (being male) and low birth weight. The latter include hypertension (HT), heart disease, diabetes, dyslipidaemia, carotid stenosis, smoking, abdominal obesity and lack of exercise.

Emmanuel Touzé
174
blood pressure
Hypertension is the main risk factor for CVA
Epidemiological surveys show that HT is the main risk factor for CVA. The risk rises linearly with blood pressure (BP). A meta-analysis of 61 studies of the general population covering over a million subjects showed that the risk of a first event dou-bles with every 20 mmHg increase in systolic BP (Figure 1); the same relationship is observed with diastolic BP. This is true at all ages although no threshold has really been determined [3].
The same relationship is also seen after a first CVA and again the risk of recurrence rises with both systolic and diastolic BP [4].
1
2
4
8
16
64
32
128
25680–89 years
70–79 years
60–69 years
50–59 years
120 140 160 180
CVA
mor
talit
y (a
bsol
ute
floa
ting
ris
k)
Usual systolic blood pressure (mmHg)
figure 1. Blood pressure and risk of CVA [3].
175
Preventing cerebral infarction
It has been clearly shown in clinical trials that decreasing BP reduces the risk of a CVA with the greater the decrease in BP, the greater the reduction in CVA risk [5].
Even a modest reduction in BP across a population as a result of systematic im-plementation of very simple measures (weight control, reducing salt intake, physical exercise, a healthy diet [fruits, vegetables, potassium-rich foodstuffs], reducing alcohol consumption) would have a huge positive impact. A simple reduction of 5 mmHg in systolic BP across the population as a whole would reduce the incidence of CVA by 14%.
In secondary prevention too, it has been clearly shown that decreasing BP after a CVA reduces the risk of recurrence [6, 7].
Target blood pressure in secondary prevention
In coronary heart disease, the relationship between BP and risk draws a J-shaped curve with increased risk at very low BP as well as at high values. This relationship does not seem to apply to CVAs and the old guidelines on secondary prevention recommended lowering BP even in normotensive patients, i.e. below 140/90 mmHg. Secondary analysis of data from the large-scale PROFESS therapeutic trial, which covered 20,330 patients who had already had a CVA showed that the risk of recur-rence was higher in patients with BP below 120 mmHg although no causal relation-ship could be established [8].
However, results from other studies on secondary prevention show benefit from reducing BP in normotensive patients. The SPS3 Study on 3,020 patients with a MRI-confirmed lacunar infarct evaluated two BP targets (130–139 mmHg and <30 mmHg) in secondary prevention. The results showed an insignificant decrease in the incidence of recurrent CVA in the <130 mmHg target group (HR: 0.81; 95% Confidence Interval: 64–1.03; p = 0.08). On the other hand, the incidence of in-tracerebral bleeding was considerably reduced (HR: 0.37; 95% Confidence Interval: 0.15–0.95, p = 0.03). Thus, lowering BP to below 130 mmHg could be of benefit in certain situations [9].
These results are corroborated by those of the ACCORD Study, which also focused on two BP targets—below 120 mmHg and below 140 mmHg—in 4,733 patients with type 2 diabetes. The respective annual incidences of CVA were 0.32% and 0.53% (HR: 0.59; 95% Confidence Interval: 0.39–0.89; p = 0.01) but annual death rates (all causes) were, respectively, 1.28% and 1.19% (HR: 1.07; 95% Confidence Interval: 0.85–1.35; p = 0.55) [10].
In consequence, the new American Heart Association/American Stroke Association (AHA/ASA) guidelines on secondary prevention recommend lowering BP to below 140 mmHg, and in some situations such as lacunar infarct, to below 130 mmHg [11].

Emmanuel Touzé
176
dyslipidaemia
Many epidemiological studies have shown high cholesterol to be a risk factor for cerebral infarction. The therapeutic trials conducted to evaluate statins clearly showed that for primary prevention, the greater the decrease in low-density lipo-protein (LDL)-cholesterol, the greater the reduction in the risk of vascular events in general, including that of cerebral infarction. A recent meta-analysis showed that, for every 1 mmol/l drop in LDL-cholesterol, the risk of cerebral infarction is reduced by 21%, whatever the subject’s age or baseline risk level [12].
With respect to secondary prevention, the SPARCL Study, which covered 4,731 patients who had had a CVA or a TIA in the six months preceding inclusion, also showed that lowering LDL-cholesterol was associated with a reduction of the order of 16% in the risk of recurrent CVA within six years (Figure 2) [13].
The benefit of lowering LDL-cholesterol is therefore clearly demonstrated in both primary and secondary prevention.
AHA/ASA guidelines recommend giving all high-risk patients statins for primary prevention, and for secondary prevention in patients whose LDL-cholesterol is above 1 g/l, especially if the accident was associated with atherosclerosis [11].
Similarly, the French Supreme Health Authority recommends statin treatment for patients who have had a non-cardioembolic cerebral infarct or TIA associated with a LDL-cholesterol level of 1 g/l or higher. The recommended LDL-cholesterol target
0%1 2 3 4 5 6
4%
8%
12%
16%RR : 16%
Adjusted RR (95% CI): 0.84 (0.71–0.99), p = 0.03
11.2 vs. 13.1% : RAR = 1.9%
Placebo (2,366)
Statin (2,365)
Years after randomisation
CVA, fatal or not (%)
figure 2. Lowering cholesterol in secondary CVA prevention [13].
177
Preventing cerebral infarction
is below 1 g/l. Patients with diabetes and those with a history of coronary heart disease should be on a statin whatever their LDL-cholesterol.This treatment should be considered in a patient with LDL-cholesterol below 1 g/l who has experienced a cerebral infarct or TIA associated with symptomatic athero-sclerotic disease [14].
diabetes
It is now clear that controlling blood glucose reduces the risk of microvascular com-plications in diabetics although benefit vis-a-vis macrovascular problems remains to be demonstrated, especially with respect to CVAs.
Until recently, bringing BP down below 120/80 mmHg was recommended in this population but now the recommended reduction is only to below 140/90 mmHg. The value of statins in these patients ought to be emphasised [15].
lack of exercise and diet
We have a great deal of information from observational studies that suggest that ex-ercise prevents CVAs. The 2008 American guidelines recommend that adults should exercise moderately (e.g. brisk walking) for at least 150 minutes a week or perform intense, aerobic activity (e.g. running) for 75 minutes a week (or some combination of the two).
The 2013 AHA/ASA lifestyle guidelines for the prevention of cardiovascular dis-ease recommend at least 40 minutes of aerobic exercise three or four times a week in order to reduce BP and improve lipid profile
If possible, patients who have had an ischaemic CVA or TIA should do three or four sessions of moderate to intense, aerobic physical exercise to address CVA risk factors. Each session should last 40 minutes on average.
For patients who have a deficit after an ischaemic CVA, supervision by a profes-sional (e.g. a physical therapist or expert in cardiac re-education) might be advisable, at least at the beginning of the exercise programme.
Similarly on diet, there is a body of data from epidemiological studies and, to a lesser extent from randomised studies. The 2014 AHA/ASA guidelines on primary CVA prevention recommend:
– Cutting down sodium intake and raising potassium intake to lower BP (class I, level A).
– A DASH-type diet, which emphasises fruit, vegetables and dairy products, coupled with reducing saturated fat intake, to lower BP (class I, level A).
– A diet rich in fruit and vegetables, which is therefore rich in potassium and can reduce the risk of CVA (class I, level B).
– A Mediterranean diet complemented with nuts to reduce CVA risk (class IIa, Level B) [16].
Emmanuel Touzé
178
antithrombotic drugs
The second aspect of CVA prevention is represented by two big families of me-dicinal products, namely antiplatelet drugs for non-cardioembolic accidents, and anticoagulants for cardioembolic accidents.
antiplatelet drugs
Antiplatelet drugs have been solidly demonstrated as being effective at preventing cerebral infarction in patients who have already had a cerebral infarct or a TIA. Nevertheless, the question of which drug to prescribe arises. In secondary preven-tion, three options can be considered as equivalent, i.e. aspirin, clopidogrel and a combination of aspirin and dipyridamole [17].
Studies of combinations of antiplatelet drugs have shown that combining aspirin with clopidogrel affords no advantage and raises the risk of bleeding. On the other hand, this combination may help prevent recurrence if administered in the acute phase of a minor or transient accident although this is not established. The results of some studies support this strategy, in particular a recently published Chinese study of 5,170 patients who had had a TIA or a minor cerebral infarct in the preceding 24 hours. They were given either a combination of clopidogrel + aspirin (clopidogrel at an initial dose of 300 mg then 75 mg daily for 90 days + aspirin at a daily dosage of 75 mg for the first 21 days) or placebo + aspirin (75 mg a day for 90 days). After 90 days, the combination proved more effective than aspirin alone at preventing cer-ebrovascular accidents (CVA) (HR: 0.68; 95% CI: 0.57–0.81; p<0.001) (Figure 3) [18]. The treatment is recommended in the 2014 AHA/ASA guidelines to prevent CVA in patients with a history of either CVA or TIA; it can be offered for a short course but not for long-term treatment [11].
anticoagulants
Anticoagulants are essentially prescribed to manage atrial fibrillation (AF), which increases the risk of cerebral infarction by a factor of five. This is a problem of the elderly, affecting fewer than 0.5% of people under 50 as opposed to 5–15% of over 80 year-olds [19]. After 70 years of age, 30% of patients who have had an ischaemic CVA suffer from AF compared with 20% of patients across all ages [20]. Cerebral infarction associated with AF has a mortality rate within one month of 32.5% compared with 16.2% without AF. [21]. The resultant disability following cerebral infarction is worse in those with AF than in those without it [20].
However, oral anticoagulant drugs represent a very effective treatment modal-ity. It has been shown in many studies that anticoagulant therapy reduces the risk of a cerebral embolic event by two-thirds (12% vs 4%) (RRR: 66%; 95% CI: 43–80) [22].
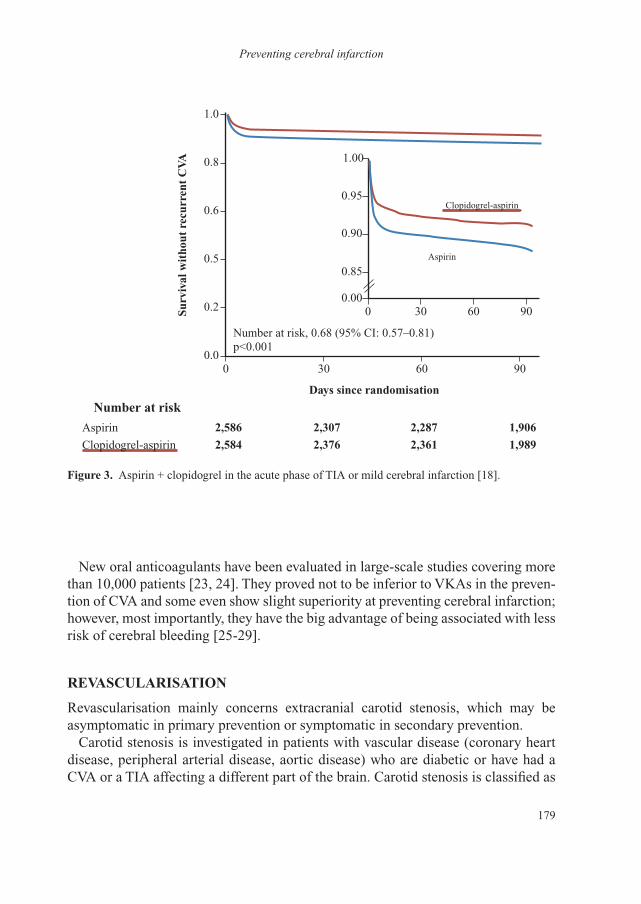
179
Preventing cerebral infarction
New oral anticoagulants have been evaluated in large-scale studies covering more than 10,000 patients [23, 24]. They proved not to be inferior to VKAs in the preven-tion of CVA and some even show slight superiority at preventing cerebral infarction; however, most importantly, they have the big advantage of being associated with less risk of cerebral bleeding [25-29].
revascularisation
Revascularisation mainly concerns extracranial carotid stenosis, which may be asymptomatic in primary prevention or symptomatic in secondary prevention.
Carotid stenosis is investigated in patients with vascular disease (coronary heart disease, peripheral arterial disease, aortic disease) who are diabetic or have had a CVA or a TIA affecting a different part of the brain. Carotid stenosis is classified as
0.0
0.00
0.85
0.90
0.95
1.00
0
0
30
30
60
60
90
900.2
0.5
0.6
0.8
1.0
Aspirin
Aspirin
Surv
ival
wit
hout
rec
urre
nt C
VA
Days since randomisation
Number at risk
2,586
2,584
2,307
2,376
2,287
2,361
1,906
1,989Clopidogrel-aspirin
Number at risk, 0.68 (95% CI: 0.57–0.81)p<0.001
Clopidogrel-aspirin
figure 3. Aspirin + clopidogrel in the acute phase of TIA or mild cerebral infarction [18].
Emmanuel Touzé
180
symptomatic if the cerebral infarct or TIA was recent and involved the same territory as the stenosis.
The two situations are completely different. Thanks to the treatment modalities available (statins, general improvement in risk factor management), the risk of an event in the territory of the stenosis is extremely low—below 1% for asymptomatic carotid stenosis [30]. Above all, this constitutes a marker for the risk of vascular events (a coronary event, death due to a vascular problem over 2% a year). Treatment is essentially medical and the benefit of surgery is extremely low in this situation.
On the other hand, symptomatic carotid stenosis is associated with a very high incidence of recurrence within days or weeks of the first event [31-33]. In this situ-ation, surgery is of great benefit, especially if the artery is narrowed by more than 70%. Angioplastic stenting is an alternative strategy although it has an excess risk of complications (CVA, death) in the short term; nevertheless, it is probably as effec-tive as surgery in the medium and long terms.
asPirin and Primary Prevention
Aspirin has been shown to be effective at preventing vascular events, especially coronary events [34]. Curiously, aspirin helps prevent coronary events in men but not women, whereas it is beneficial for primary prevention in women but not men. In consequence, the AHA/ASA guidelines on primary CVA prevention state that aspirin can be given to patients with a ten-year vascular risk of over 10%, and to women in order to prevent a first ischaemic accident, especially women with diabetes [11].
sPecificities of cva in Women
CVAs are more common in women (because they live longer) and the associated morbidity and mortality are worse as well as institutionalisation being a more com-mon consequence. HT is the most common cause in women of over 60 [35]. Women have specific risk factors (pregnancy, endocrine factors, contraception, hormone treatment, early menopause, migraine with aura) as well as specific causes like eclampsia. These specificities were addressed in a global campaign in 2014 with the message, “I’m a woman, stroke affects me”.
Prevention does not differ much between men and women. Prophylactic surgery for asymptomatic carotid stenosis is clearly of less benefit in women than it is in men. Oestrogen-progestin contraception and hormone replacement treatment are contraindicated after a cerebral infarct or TIA although pure progestin is safe. For primary prevention, aspirin can be proposed.
181
Preventing cerebral infarction
conclusion
The ways of preventing a first event or recurrence are globally identical but the absolute benefit will differ in primary and secondary prevention.
There has been massive progress in prevention over the last 30–40 years, resulting in a real reduction in the incidence of the disease although the absolute number affected is inexorably rising because of ageing of the population.
Many of the risk factors for CVA are continuous variables, which have practical implications, e.g. it could be worth lowering BP below the recommended target to cut the risk down further.
Although recent advances have been more modest, rigorous application of existing recommendations will reduce the scope of the problem.
references
1 Mohan KM, Wolfe CD, Rudd AG, et al. Risk and cumulative risk of stroke recurrence: a system-atic review and meta-analysis. Stroke 2011;42:1489-94.
2 O’Donnell MJ, Xavier D, Liu L, et al. Risk factors for ischaemic and intracerebral haemor-rhagic stroke in 22 countries (the INTERSTROKE study): a case-control study. Lancet 2010;376: 112-23.
3 Lewington S, Clarke R, Qizilbash N, et al. Prospective Studies Collaboration. Age-specific rel-evance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002;360:1903-13.
4 Rodgers A, MacMahon S, Gamble G, et al. Blood pressure and risk of stroke in patients with cerebrovascular disease. The United Kingdom Transient Ischaemic Attack Collaborative Group. BMJ 1996;313:147.
5 Staessen JA, Wang JG, Thijs L. Cardiovascular protection and blood pressure reduction: a meta-analysis. Lancet 2001;358:1305-15.
6 Liu L, Wang Z, Gong L, et al. Blood pressure reduction for the secondary prevention of stroke: a Chinese trial and a systematic review of the literature. Hypertens Res 2009;32:1032-40.
7 Rashid P, Leonardi-Bee J, Bath P. Blood pressure reduction and secondary prevention of stroke and other vascular events: a systematic review. Stroke 2003;34:2741-8.
8 Ovbiagele B, Diener HC, Yusuf S, et al. Level of systolic blood pressure within the normal range and risk of recurrent stroke. JAMA 2011;306:2137-44.
9 SPS3 Study Group, Benavente OR, Coffey CS, et al. Blood-pressure targets in patients with recent lacunar stroke: the SPS3 randomised trial. Lancet 2013;382:507-15.
10 ACCORD Study Group, Cushman WC, Evans GW, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med 2010;362:1575-85.
11 Kernan WN, Ovbiagele B, Black HR, et al. Guidelines for the prevention of stroke in patients with stroke and transient ischemic attack: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014;45:2160-236.
12 Cholesterol Treatment Trialists’ (CTT) Collaborators, Mihaylova B, Emberson J, et al. The effects of lowering LDL cholesterol with statin therapy in people at low risk of vascular disease: meta-analysis of individual data from 27 randomised trials. Lancet 2012;380:581-90.
13 Amarenco P, Bogousslavsky J, Callahan A, III, et al. High-dose atorvastatin after stroke or tran-sient ischemic attack. N Engl J Med 2006;355:549-59.
Emmanuel Touzé
182
14 HAS. Prévention vasculaire après un infarctus cérébral ou un AIT—Actualisation. Juillet 2014, mise à jour février 2015.
15 American Diabetes Association. Standards of medical care in diabetes—2013. Diabetes Care 2013;36(Suppl 1):S11-66.
16 Meschia JF, Bushnell C, Boden-Albala B, et al. Guidelines for the primary prevention of stroke: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014;45:3754-832.
17 Antithrombotic Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of an-tiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ 2002;324:71-86.
18 Wang Y, Wang Y, Zhao X, et al. Clopidogrel with aspirin in acute minor stroke or transient is-chemic attack. N Engl J Med 2013;369:11-9.
19 Grau AJ, Weimar C, Buggle F, et al. Risk factors, outcome, and treatment in subtypes of ischemic stroke: the German stroke data bank. Stroke 2001;32:2559-66.
20 Lin HJ, Wolf PA, Kelly-Hayes M, et al. Stroke severity in atrial fibrillation. The Framingham Study. Stroke 1996;27:1760-4.
21 Marini C, De Santis F, Sacco S, et al. Contribution of atrial fibrillation to incidence and outcome of ischemic stroke: results from a population-based study. Stroke 2005;36:1115-19.
22 Hart RG, Pearce LA, Aguilar MI. Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med 2007;146:857-67.
23 Turpie AG. New oral anticoagulants in atrial fibrillation. Eur Heart J 2008;29:155-65.24 Hankey GJ, Eikelboom JW. Antithrombotic drugs for patients with ischaemic stroke and transient
ischaemic attack to prevent recurrent major vascular events. Lancet Neurol 2010;9:273-84.25 Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial
fibrillation. N Engl J Med 2011;365:981-92.26 Connolly SJ, Ezekowitz MD, Yusuf S, et al. Newly identified events in the RE-LY trial. N Engl J
Med 2010;363:1875-6.27 Giugliano RP, Ruff CT, Braunwald E, et al. Edoxaban versus warfarin in patients with atrial
fibrillation. N Engl J Med 2013;369:2093-104.28 Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrilla-
tion. N Engl J Med 2011;365:883-91.29 RCP Rivaroxaban, 2013.30 Naylor AR. Time to rethink management strategies in asymptomatic carotid artery disease. Nat
Rev Cardiol 2011;9:116-24.31 Blaser T, Hofmann K, Buerger T, et al. Risk of stroke, transient ischemic attack, and vessel
occlusion before endarterectomy in patients with symptomatic severe carotid stenosis. Stroke 2002;33:1057-62.
32 Fairhead JF, Mehta Z, Rothwell PM. Population-based study of delays in carotid imaging and surgery and the risk of recurrent stroke. Neurology 2005;65:371-5.
33 Marnane M, Ni Chroinin D, Callaly E, et al. Stroke recurrence within the time window recom-mended for carotid endarterectomy. Neurology 2011;77:738-43.
34 Antithrombotic Trialists’ (ATT) Collaboration, Baigent C, Blackwell L, et al. Aspirin in the primary and secondary prevention of vascular disease: collaborative meta-analysis of individual participant data from randomised trials. Lancet 2009;373:1849-60.
35 Bushnell C, McCullough LD, Awad IA, et al. Guidelines for the prevention of stroke in women: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014;45:1545-88.

183
Stroke: new therapiesAVC : nouveautés thérapeutiques© 2015 Springer Science + Business Media France Sarl. Tous droits réservés
Organising health care pathways for stroke victims
France Woimant (Paris)
Organising the health care pathway of stroke victims is a big challenge. It involves planning the management of a pathology that is both urgent and chronic as well as being extremely common and striking people of all ages. Although strokes are more common after the age of 75, children are not invulnerable. The health care pathway has to be organised on a local basis, ideally in the patient’s health care region, and this applies from targeted prevention through hospitalisation to going back home.
COmmOn, seriOus and expensive
In France, almost 110,000 people are admitted into hospital every year with a stroke [1]. The number of French people who have had a stroke has been estimated at 780,000 on the basis of surveys of disability – health – households and disabil-ity—health—institution in 2008–2009 [2]. These surveys show that two-thirds of stroke victims experience sequelae and, in one case in two, such sequelae stop them carrying out one or more daily activities such as eating, walking, washing or getting dressed [2]. In these surveys, modified Rankin Scores were compared according to whether or not the subject had a history of stroke. The score was over 2 (corresponding to handicap that significantly restricts lifestyle or precludes full independence) in 34.4% of those with a history of stroke (28% of those living at home and 87.8% of those in an institution) compared with 3.9% of people with no history of stroke (3.1% of those living at home and 71.6% of those in an institu-tion) [3]. These surveys also show that almost a quarter of highly dependent patients with a Rankin Score of 5 (corresponding to severe handicap with total dependence requiring permanent supervision) have had a stroke. These figures alone illustrate the scope of the stroke problem, which is the main cause of acquired disability in adults.
Sequelae account for a large part of the financial burden that stroke imposes on the health insurance system and society. Annual stroke-related health care and medi-cosocial expenditure is high, estimated at 8.3 billion euros in 2007: e5.9 billion to the health care sector (3% of the overall budget) and e2.4 billion for medicosocial

France Woimant
184
services. In 2004, mean annual expenditure per patient classified as having the Long-Term Condition (LTC) “debilitating stroke” was estimated at 9,642 euros (i.e. 14% more than for a patient with the LTC “Alzheimer’s disease”) [4]. In 2007, the mean cost of an incident case of stroke over the first year was 16,686 euros and the annual cost of a prevalent case was 8,099 euros although this varies enormously according to the sequelae and the degree of disability [5].
a pathway that starts with preventiOn
Prevention remains the best way of reducing the incidence and repercussions of stroke. Screening for and managing risk factors are the main issues when it comes to preventing strokes and indeed all cardiovascular diseases (coronary heart disease, peripheral arterial occlusive disease, kidney failure, etc.). Preventive measures concern all ages, from childhood (school programmes) to old age. These need to be multiculturally structured to reach everyone. Targeted stroke preventive measures can be backed up by outpatient education, e.g. focusing on hypertension, which is the main risk factor for stroke. Such actions are all the more accessible if they are provided close to the patient’s home.
hOspital
In the acute phase when every minute counts, care should also be organised locally, ideally at a Stroke Unit (SU). One hundred and forty SUs are to be established in the framework of the 2010–2014 National Stroke Plan. But unfortunately, this will not ensure one within a 30-minute journey of anywhere a stroke could occur. Patients may also be first seen at a nearby establishment with an Emergency Department. These should have appropriately trained staff in both the Emergency and Radiology Departments together with neuro-imaging facilities available around the clock, seven days a week, as well as appropriate remote diagnosis and therapeutic advice possibilities (telemedicine) [6]. In establishments with an Emergency Department but no SU, initial treatment is prescribed by the emergency physician and a neurolo-gist after a visio-consultation and transfer of neuro-imaging results. Once treatment has been started, the patient is transferred to a SU.
After the acute phase, 30% of patients are transferred to a rehabilitation unit [7]; this period usually lasts weeks and is psychologically stressful so the patient should not be taken far away from his or her family and friends [8]. Moreover, discharge home will be easier to organise from a nearby establishment, which will be more familiar with local medicosocial and social resources. The return home with support through rehabilitation unit can only be organised if the establishment is close to the patient’s home.

185
Organising health care pathways for stroke victims
returning hOme
Stroke management does not end with discharge from the hospital and it should take into account the return of the patient back to his or her home so coordination be-tween independent health professionnals and the hospital is important. Going back home is a difficult time for patient and family who are only just beginning to realise how the stroke is going to disrupt the daily routines of their professional and family lives.
Many factors will determine whether or not the patient will be able to stay at home, including:
• the degree of physical disability and cognitive deficit,• complications,• help at home,• training of carers,• psychological support for the patient and carers.
Following a stroke, it is essential to organise coordinated follow-up between local support workers and professional health care providers in order to prevent recur-rence, complications and loss of independence. Close cooperation is therefore very important between health care professionals and support workers [9]:
• independent professional health care providers (general practitioners, neurologists, nurses, physical therapists, speech therapists, occupational thera-pists, psychologists, social workers, etc.),
• health care professionals from centres of excellence,• professionals from:
– structures and services for the disabled: medicosocial support services for disabled adults (SAMSAH, services d’accompagnement médico-social pour adultes handicapés), social life support services (SAVS, services d’accompagnement à la vie sociale), Departmental homes for the disabled (MDPH, maisons départementales des personnes handicapées), etc.;
– structures and services for the elderly such as home for the independence and integration of Alzheimer’s patients (MAIA, maisons pour l’autonomie et l’intégration des malades Alzheimer), local information and coordina-tion centres (CLIC, centres locaux d’information et de coordination) and medicosocial teams for personalised allocation of independence (APA, allocation personnalisée d’autonomie);
– organisations that adapt homes.
• home help, cleaners,• carers, etc.

France Woimant
186
new OrganisatiOns tO help keep patients at hOme
assessment of how to improve coordination between hospital and the independent sector
• Post-stroke multidisciplinary assessment in the hospital involves evaluation by a team specialising in neurovascular disease working together with independent professional health care providers. The aims of the assessment are to:
– review the disease situation, identify vascular risk factors and plan secondary prevention measures;
– perform a physical work-up to define a personalised care programme; – monitor for mood problems (depression is very common after a stroke); – assess capacities for social and professional reintegration; – assess the quality of life of the patient and his/her family and friends, and
see if the carers need support; – if necessary, offer therapeutic education; – give information about patient support groups.
These assessments are relevant to all patients, even those who have no sequelae because they will bring to light past, hitherto unrecognised, deficiencies that could lead to disability or the loss of social and professional adaptability.
• Mobile stroke follow-up care and rehabilitation teams have been established on an experimental basis in certain regions including the Île-de-France region around Paris. These teams mainly come in to provide short-term help to over-come difficulties that might threaten the patient’s ability to stay at home. They consist of a physician, an occupational therapist and a social worker who come to the home or carry out their work at an institution. Their job is to improve conditions in the home (assessment of the patient and carers), to prepare for hospital admissions (avoiding unnecessary admissions) and organise the return home. These assessments are undertaken in collaboration with independent professionals and medicosocial structures.
Care teams coordinated at home with the hospital team
A meta-analysis based on individual data from 11 trials showed that services aimed at providing early, coordinated care in the home cut down the risk of long-term dependence and institutionalisation in some stroke patients [10]. The beneficial ef-fect vis-à-vis daily activities can persist to five years after the stroke [11]. The main objective of this type of coordinated rehabilitation in the home is the acquisition and enhancement of independence in daily life through rehabilitation and by ensuring that what we have learned is applied to daily life. Hospital coordination permits continued multidisciplinary rehabilitation with a goal of improved function and opti-misation of acquired knowledge in the context of patients’ lives. It makes it possible

187
Organising health care pathways for stroke victims
for patients to access professional re-educators that are not found in independent practice such as occupational therapists, clinical psychologists, neuropsychologists and social workers experienced with disability. It also helps train carers and those who live with the patient. Experiments have been conducted on this in France: a mobile disability assessment and follow-up unit in Mulhouse, hospitalisation to home rehabilitation and reintegration in Île-de-France. It is nevertheless important to remember the possible risk of placing an excessive psychological burden on the family as well as professional and informal carers.
preventing reCurrenCe
Preventive measures that match the type of the stroke and its aetiology are essential. However, studies conducted in France using SNIIR-AM databases and covering 69,262 patients admitted into hospital after a stroke or a transient ischaemic attack (TIA) in the first six months of 2008 showed that only 75% of victims of a cerebral infarct and 70% of those who experienced a TIA were prescribed an antithrombotic drug [12].
health Care Channels Ought tO be adapted tO the patient’s age and the seriOusness Of the defiCit
How stroke victims are channelled through the health care system ought to take into account:
• The patient’s age. For a child, the channel will not be the same if the stroke occurs before birth, in the first days of life, in a child or in a teenager. These children should also be monitored through adulthood. For the elderly, it is estimated that in 2020, almost 30% of people admitted into hospital for stroke will be over 85 so stroke care pathways ought to be organised in coordination with geriatric channels.
• The severity of the stroke. Organisation of the care for a TIA is quite different from that of a severe stroke [13]. For patients with a severe stroke who are admitted straight into an intensive care unit, the following options need to be considered: – limitation of care; – organ donation (stroke is the leading cause of brain death); – transfer to a palliative care unit; – transfer to a post-intensive care rehabilitation unit; – transfer to a long-term care unit; – permanent or temporary accommodation in a specialised medicosocial
structure: a reception house (MAS, maison d’accueil spécialisé), a
France Woimant
188
medicalised reception home (FAM, foyer d’accueil médicalisé) or a home for the dependent elderly (EHPAD, établissement d’hébergement pour personnes âgées dépendantes).
hOw tO COOrdinate and run the strOke Care pathway
Nurse “coordinators” in stroke care are still too few in number. Nevertheless, their role is central when stroke victims return home. Their main jobs are to ensure compliance with treatment (drugs and rehabilitation) and tell patients and fam-ily members about signs of developing complications, which might exacerbate the disability. These nurses call patients after they have gone back home and/or attend the consultation with a neurologist. They provide a link between professionals at the hospital and in the independent sector [14].
In line with the 2010–2014 Stroke Plan, coordinators involved in the stroke care pathway are helping to build an effective health care pathway for stroke victims. Their main jobs are to:
– develop and coordinate the stroke pathway around SUs in order to ensure con-tinuous care by improving hospital circuits and creating links with independent practitioners, the medicosocial sector and patient support groups;
– enhance training of all the professionals involved in the pathway; – organise mass educational campaigns for the general public across the country.
In conclusion, looking after patients after a stroke is not limited to admission into a Stroke Unit during the acute phase and then if necessary, in follow-up care and rehabilitation departments. The whole of the stroke victim’s health care pathway needs to be organised and planned together with the patient, his or her family and a variety of different health care professionals. This pathway should be local, ide-ally within the health care region. Structuring the regional organisation of stroke care will prevent gaps in the pathway, which too often ends up with emergency admission into an establishment that is poorly suited to coping with the attendant problems. In collaboration with independent professional health care providers, new organisations are being set up to raise the proportion of patients who are chan-nelled into stroke-specific pathways, the aim being to reduce disability after stroke and improve patients’ quality of life as well as that of their family and friends; not to forget prevention, which remains the best way of reducing stroke-related disability.
189
Organising health care pathways for stroke victims
references
1 de Peretti C, Nicolau J, Tuppin P, et al. Evolutions de la prise en charge hospitalière des accidents vasculaires cérébraux en court séjour et en soins de suite et de réadaptation entre 2007 et 2009 en France. Presse Med 2012;41:491-503.
2 de Peretti C, Grimaud O, Tuppin P, et al. Prévalence des accidents vasculaires cérébraux et de leurs séquelles et impact sur les activités de la vie quotidienne: apports des enquêtes déclaratives Handicap-santé-ménages et Handicap-santé-institution. Bull Epidemiol Hebd 2012;1:1-6.
3 Schnitzler A, Woimant F, Tuppin P, de Peretti C. Prevalence of self-reported stroke and disability in the French adult population: a transversal study. PLoS One 2014;9(12):e115375.
4 Fery-Lemonnier E. Rapport ministériel sur la prévention et la prise en charge des accidents vasculaires cérébraux en France. Juin 2009.
5 Chevreul K, Durand-Zaleski I, Gouépo A, et al. Cost of stroke in France. Eur J Neurol 2013;20: 1094-100.
6 Circulaire N°DGOS/R4/R3/PF3/2012/106 du 6 mars 2012 relative à l’organisation des filières régionales de prise en charge des patients victimes d’accident vasculaire cérébral (CVA).
7 de Peretti C, Nicolau J, Holstein J, et al. Hospitalisations en soins de suite et de réadaptation en France après un accident vasculaire cérébral survenu en 2007. BEH 2010; 49-50:501-6.
8 Brainin M, Olsen TS, Chamorro A, et al. Organization of stroke care: education, referral, emergency management and imaging, stroke units and rehabilitation. European Stroke Initiative. Cerebrovasc Dis 2004;17(Suppl 2):1-14.
9 Gache K, Leleu H, Nitenberg G, et al. Main barriers to effective implementation of stroke care pathways in France: a qualitative study. BMC Health Serv Res 2014;14:95.
10 Langhorne P, Taylor G, Murray G, et al. Early supported discharge services for stroke patients: a meta-analysis of individual patients’ data. Lancet 2005;365:501-6.
11 Thorsén AM, Holmqvist LW, de Pedro-Cuesta J, von Koch L. A randomized controlled trial of early supported discharge and continued rehabilitation at home after stroke: five-year follow-up of patient outcome. Stroke 2005;36:297-303.
12 Moysan TV, de Peretti S, Woimant F. Caractéristiques et traitements des assurés du régime général hospitalisés pour accident vasculaire cérébral au cours du premier semestre 2008. Rev Neurol 2008;169:126-35.
13 Woimant F, Biteye Y, Chaine P, Crozier S. Severe stroke: which medicine for which results? Ann Fr Anesth Reanim 2014;33:102-9.
14 Cortes E, Woimant F. L’éducation du patient post-accident vasculaire cérébral. STV 2007;19:492-4.