Embed Size (px)
Citation preview

CLINICAL AND DIAGNOSTIC LABORATORY IMMUNOLOGY, Jan. 1994, p. 38-43 Vol. 1, No. 11071-412X/94/$04.00+0Copyright © 1994, American Society for Microbiology
Autoimmune Hemolytic Anemia in ChronicMucocutaneous Candidiasis
BENJAMIN I. OYEFARA,l12* HAEWON C. KIM,2'3'4 ROGER N. DANZIGER,1 2MARLAIN CARROLL,2'4 JEFFREY M. GREENE,' 2 AND
STEVEN D. DOUGLAS" 2'4Divisions ofAllergy, Immunology and Infectious Disease,' Hematology/Oncology,3 and
Clinical Laboratories,4 Children's Hospital of Philadelphia, and Department of Pediatrics,University of Pennsylvania Medical School,2 Philadelphia, Pennsylvania 19104
Received 7 July 1993/Returned for modification 13 August 1993/Accepted 22 September 1993
Chronic mucocutaneous candidiasis is an immunodeficiency disease characterized by T-cell dysregulationand chronic superficial candidal infections. We report on three patients with chronic mucocutaneouscandidiasis who developed autoantibodies to erythrocytes. Our first patient, a 19-year-old female, developedautoimmune hemolytic anemia (AIHA) that required multiple courses of treatment, including corticosteroids,intravenous immunoglobulin, and danazol. During the last exacerbation of AIHA, intensive treatment withcorticosteroids and intravenous immunoglobulin failed and yet the patient responded to plasmapheresis. Oursecond patient, a 21-year-old male, developed AIHA which responded to oral corticosteroid therapy. Our thirdpatient, a 6-year-old female without evidence of hemolysis, was found to have erythrocyte autoantibodies onroutine screening. These three patients had positive direct antiglobulin tests, and the first patient had bothimmunoglobulin G (IgG) and IgM erythrocyte autoantibodies, while the remaining two patients had only IgGautoantibody. This is the first report of the association of AIHA with chronic mucocutaneous candidiasis. Wesuggest that all patients with chronic mucocutaneous candidiasis be screened periodically for erythrocyteautoantibodies. Plasmapheresis, a safe ancillary procedure in the management of AIHA, may be life-saving insome cases. The occurrence of erythrocyte autoantibodies in mucocutaneous candidiasis may be related toimmunoregulatory disorders in this disease.
Chronic mucocutaneous candidiasis (CMC) is a rare heter-ogeneous disorder characterized by chronic and recurrentinfections of mucous membranes, nails, scalp, and skin withorganisms of the genus Candida (3, 24). Although Candidaalbicans is the usual organism that causes these infections, thevulnerability of these patients to a variety of other noncandidalinfections, some of which can be disseminated, has beenobserved (11, 15, 19, 22). Examples of such noncandidalinfectious agents include Staphylococcus aureus, Pneumococ-cus spp., Haemophilus influenzae, Mycobacterium avium intra-cellulare, Histoplasma capsulatum, Cryptococcus neoformans,herpes simplex virus, and Giardia lamblia.A wide variety of immunological abnormalities in patients
with CMC have been reported. The primary immune defect isbelieved to be an impairment in the T-cell response to Candidaorganisms and is characterized by cutaneous anergy to Candidaorganisms as well as diminished or absent lymphocyte prolif-erative response to Candida antigen (11, 25). Durandy et al.(14) demonstrated mannan-specific and mannan-induced T-cell-suppressive activity in 18 patients with CMC. These work-ers speculated that defective presentation of mannan, a can-didal antigen, by monocytes could result in the accumulation ofmannan, leading to the activation of specific T suppressor cellsand the consequent cellular immunodeficiency specific to C.albicans. Gupta (18) reported a deficiency of autologousmixed-lymphocyte reaction which was associated with in-creased suppressor T-cell activity or with functional deficiencyof helper T cells in four of six patients with CMC. A deficiency
* Corresponding author. Mailing address: Section of Immunology,Division of Allergy, Immunology and Infectious Diseases, Children'sHospital of Philadelphia, 34th Street & Civic Center Boulevard,Philadelphia, PA 19104. Phone: (215) 590-2135. Fax: (215) 590-3044.
of helper T cells (32) as well as excessive suppressor T-cellactivity (36) have also been reported in association with CMCby others. In addition, mononuclear cells with deficient expres-sion of CD2 but normal CD3 occur in CMC (30).
It has been speculated that the failure of Candida-stimulatedT cells to produce lymphokines may be the significant defect inCMC (23). Consistent with that hypothesis, Sander et al. (33)recently reported a marked regression of mucocutaneouscandidiasis in a patient with alopecia universalis, malignantthymoma, and mucocutaneous candidiasis who was treatedwith interleukin-2. Apart from the T-cell abnormalities, otherimmunologic defects in association with CMC include isolatedimmunoglobulin A (IgA) deficiency (4), deficient IgG responseto diphtheria immunization (5), IgG2 subclass deficiency (17),chemotactic defects (38), defective monocyte-mediated anti-body-dependent cellular cytotoxicity (31), the presence ofplasma inhibitor to lymphocyte transformation (9), and de-creased activity of total serum complement (13). Many of theseabnormal findings frequently return to normal after treatmentof the Candida infection, suggesting that some of these re-ported anomalies are epiphenomena and do not represent thebasic immunologic defect (3). However, Mobacken et al. (28)studied eight patients with CMC and found that clinicalimprovement after treatment with ketoconazole for 6 monthswas not associated with reversal of either the cutaneous anergyor the in vitro lymphoproliferative response to candidal anti-gen. Together, all these studies suggest that the fundamentalabnormality in CMC is a T-cell regulatory defect, but themolecular basis of the defect is unknown.The clinical manifestations of CMC are also variable, and at
least six different clinical variants have been described (24). Awide variety of autoimmune diseases have also been reportedin association with CMC. These include hypoparathyroidism,
38
on June 20, 2020 by guesthttp://cvi.asm
.org/D
ownloaded from

AUTOIMMUNE ANEMIA IN CHRONIC MUCOCUTANEOUS CANDIDIASIS 39
TABLE 1. Clinical characteristics of six patients with CMC
Case Age Age at Mode of Familynao. (Aygr) Sex diagnosis presentation history of Clinical complicationsno.(yr) ~~(MO) prsnainCMC1 19 F 6 Chronic oral, vaginal, and Negative Autoimmune hemolytic anemia, hypothyroidism
skin candidiasis2 21 M 14 Chronic Candida infection Negative Autoimmune hemolytic anemia, bronchiectasis, hypothyroidism,
of scalp and nails chronic sinusitis; died of respiratory failure secondary to dis-seminated aspergillosis
3 6 F 11 Chronic oral and skin can- Negative Bronchiectasis, failure to thrive; died of measles pneumonitis atdidal infection age 6 yr
4 7 F 13 Chronic oral candidiasis Negative Hypoparathyroidism, alopecia totalis, rheumatic fever, reactiveairways disease
5 5 F 8 Chronic oral, perineal, and Negative Cyclic neutropeniascalp candidiasis
6 17 M 8 Chronic oral and perineal Negative Meatal stenosis, delayed puberty, iron deficiency anemia, penicil-candidiasis lin allergy, bilateral inguinal hernia, atypical mycobacterial in-
fection of cervical and messenteric nodes; died of disseminatedMycobacterium avium-M. intracellulare infection
hypothyroidism, Addison's disease, diabetes mellitus, hypogo-nadism, chronic active hepatitis, alopecia totalis, perniciousanemia, aplastic anemia, and immune thrombocytopenia (7,12, 19, 39). Although a recent clinical review of cases through-out the United States (19) mentioned the occurrence oferythrocyte autoantibodies in CMC, clinical evidence of hemo-lysis was not cited. We report on three patients with CMC whodeveloped erythrocyte autoantibodies. Two of these patientsdeveloped exacerbations of acute hemolytic anemia that re-quired therapy. We also reviewed the records of our sixpatients with CMC to determine whether there were distinc-tive clinical or laboratory findings that could distinguish thosewho developed autoimmune hemolytic anemia (AIHA).
CASE REPORTS
Case 1. This patient is a 19-year-old caucasian female whoweighed 5 lb (ca. 2 kg) at birth after a full-term gestation. Atage 6 months, this patient developed generalized candidal skininfections that responded poorly to local therapy (Table 1).She also demonstrated cutaneous anergy to candidal antigen atthis time. A skin biopsy sample revealed C. albicans, and shewas admitted to the hospital and treated with intravenousamphotericin B. Transfer factor therapy was also initiatedduring this admission, using transfer factor that was preparedfrom her father, who had a positive delayed-type hypersensi-tivity (DTH) skin test to candidal antigen.When the patient was 4 years old and receiving transfer
factor, her DTH skin test to candidal antigen converted fromnegative to positive. Clinically, she had minimal candidal skininvolvement, although she was also receiving oral ketoconazoletherapy. In the same year, the patient developed hypothyroid-ism and was started on levothyroxine therapy. At age 6 years,she developed a persistent malar rash which was diagnosed as
acne rosacea. Serological tests for antinuclear and anti-DNAantibodies were negative at ages 6, 8, and 11 years. At age 10years, transfer factor therapy was stopped. She continued tohave recurrent episodes of oral thrush which responded to oralketoconazole treatment. At age 12 years, she developed her-pes/zoster in the T3 dermatome, which resolved withoutcomplications.At age 15 years, she had her first episode of Coombs'
test-positive hemolytic anemia and was admitted to the hospi-tal with a hemoglobin level of 2.9 g/dl, an elevated reticulocytecount, elevated indirect bilirubin, elevated lactic dehydroge-
nase, and a reduced serum haptoglobin level (Table 2). Thisepisode of hemolytic anemia was preceded by a few days ofviral upper respiratory tract infection. She was treated withintravenous gammaglobulin (1 g/kg/day) and intravenousmethylprednisolone (1 mg/kg every 12 h). She was also cau-tiously transfused with packed erythrocytes (3 ml/kg for fourdoses) between days 2 and 4 of admission. She improvedslowly, and by day 8 after admission, her hemoglobin level hadreached 12.2 g/dl. She was discharged on an oral prednisoneregimen (1 mg/kg/day), which was tapered off slowly over thenext 4 weeks. Serological tests for cytomegalovirus, Epstein-Barr virus, cryoglobulins, and cold agglutinins were negative.Determination of antinuclear antibodies during this admissiondemonstrated a titer of 1:80 (homogeneous). Other positiveautoantibodies included antimitochondrial, anti-smooth mus-
cle, antiparietal, and antithyroglobulin antibodies. Rheuma-toid factor and antimicrosomal antibody tests were negative(Table 3).At age 17 years, the patient had another exacerbation of
Coombs' test-positive hemolytic anemia during a viral syn-drome. She was admitted with a hemoglobin level of 4.6 g/dl,an elevated reticulocyte count, elevated indirect bilirubin,elevated lactic dehydrogenase, and a reduced serum haptoglo-bin level (Table 2). The patient demonstrated both IgG andIgM erythrocyte antibodies. An erythrocyte eluate was testedagainst a panel of erythrocyte antigens, and it reacted with allof the antigens (broad specificity). Treatment with intravenousgammaglobulin (1 g/kg/day) and intravenous methylpred-nisolone (1 mg/kg every 12 h) was started. On the third dayafter admission, intravenous gammaglobulin treatment wasdiscontinued because of worsening of her anemia, with a
hemoglobin level of 4.3 g/dl, and plasmapheresis was starteddaily for 5 days. A total of 360 ml of plasma per kg of body
TABLE 2. Hematologic data at time of active AIHA
Case Hemoglobin Reticulocyte Indirect Haptoglobin Lactate
no. (gIdl) count (%) blgrubl (mg/dl) (U/liter)
1 2.9 31.7 1.8 <8 1,1914.3 53.1 4.1 <7 5,148
2 6.2 50.6 3.1 <8 9103 12.2 1.8 0.2 NDa 667
a ND, not done.
VOL. 1, 1994
on June 20, 2020 by guesthttp://cvi.asm
.org/D
ownloaded from

40 OYEFARA ET AL.
TABLE 3. Autoantibodies in patients with CMC
Case Autoantibodies"no. ANA DAT MITO MUS PAR TG MICR
1 + + + + + + _2 + + - + _ _ -3 + + - + - - _4 - - + + + - _5 - - - + _6 + - - + _ _ _
" ANA, antinuclear antibodies; DAT, direct antiglobulin test (Coombs' test);MITO, antimitochondrial antibodies; MUS, anti-smooth muscle antibodies;PAR, antiparietal antibodies; TG, antithyroglobulin antibodies; MICR, antimi-crosomal antibodies.
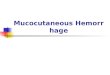
weight was exchanged over 5 days, with 5% human serumalbumin and physiologic saline as the replacement solution.For the last plasma exchange, 2 units of fresh frozen plasmawere infused to treat oozing from the catheter site due todepletion of clotting factors. Intravenous methylprednisolone(1 mg/kg every 12 h) treatment was continued throughout theperiod of admission. She improved very slowly, and by day 10after admission, her hemoglobin level had reached 8 g/dl (Fig.1). She was discharged on a regimen of oral prednisone (1mg/kg/day), and by day 41 of therapy, her hemoglobin level hadreached 12.2 g/dl. Alternate-day prednisone therapy was thenstarted. This patient continued to have evidence of chronic butcompensated hemolysis for several months after dischargefrom the hospital. A trial of danazol for several weeks wasunsuccessful in controlling her hemolysis. Splenectomy wassuggested as a therapeutic option, but the patient refused. Sheis currently off prednisone therapy, and her hemoglobin levelon 4 April 1993 was 11.2 g/dl, with a reticulocyte count of 2.5%.Case 2. The patient was a 21-year-old caucasian male, who
weighed 9 lb 6 oz (ca. 4 kg) at birth after a full-termuncomplicated pregnancy. At 14 months of age, he developedcandidal infections of his scalp and nails which persisted
14
z
0-i
0
w
m
12
10
8
6
4
PLASMAPHERESIS
FIG. 1. Response to therapy of patient 1 during the second episodeof hemolytic anemia. Intravenous methylprednisolone (1 mg/kg every12 h) and intravenous gammaglobulin (1 g/kg/day) were started on theday of admission. Gammaglobulin treatment was discontinued on day3 after admission, and plasmapheresis was started on the same day andcontinued for 5 days.
despite appropriate medical therapy. He was hospitalized forpneumonia at ages 3.5, 11, and 15 years. At age 15 years, hischest x-ray revealed chronic bronchiectasis. In the same year,he underwent a Caldwell-Luc surgical procedure for chronicsinusitis. Evaluation of his thyroid status at age 15 demon-strated hypothyroidism, for which levothyroxine therapy wasbegun. At ages 16.5, 18, and 21 years, he had exacerbations ofCoombs' test-positive hemolytic anemia, with dramatic de-creases in hemoglobin level. During the first episode, whichwas diagnosed on a routine follow-up visit, his hemoglobinlevel had decreased from 13 g/dl 6 months prior to that visit to6.2 g/dl. His reticulocyte count was 50.6%, the indirect biliru-bin level was 3.1 mg/dl, the haptoglobin level was <8 mg/dl,and the serum lactate dehydrogenase level was 910 U/liter(Table 2). This patient developed warm erythrocyte antibody(IgG) (Table 4). An erythrocyte eluate was tested against apanel of erthrocyte antigens, and it exhibited broad specificity.He responded well to oral prednisone given initially at a
dose of 2 mg/kg/day for the first 2 to 3 days, with a gradual dosereduction over the next 4 to 6 weeks. The second exacerbationof hemolysis, which was diagnosed by his private physician, alsoresponded well to oral prednisone therapy. His hemoglobinlevel during the clinic visit on 6 February 1992 was 13 g/dl, witha reticulocyte count of 1.2%, while on a maintenance dose ofprednisone (10 mg/day). The last exacerbation of hemolysisoccurred during the course of a lower respiratory tract infec-tion. His hemoglobin level on 14 June 1993 was 10.3 g/dl, witha reticulocyte count of 11.2%. His oral prednisone dose wasincreased to 50 mg/day, and by the fourth day of therapy, hishemoglobin level had increased to 11 g/dl, with a reticulocytecount of 6.8%. In July 1993, the patient died of respiratoryfailure secondary to disseminated aspergillosis.
Case 3. A 6-year-old caucasian female at age 11 months hada history of chronic oral and skin infections with Candidaorganisms which responded poorly to local therapy (Table 1).By age 24 months, she had started failing to thrive. In addition,she developed chronic sinopulmonary infection and candidalesophagitis. At age 5 years, the patient was admitted forpneumonia and required a left lower lobectomy because ofisolated bronchiectasis. A bronchoscopic culture at this timerevealed Pseudomonas aeruginosa. Prior to this time, cysticfibrosis had been ruled out by a normal sweat chloride test. Thepatient did well postlobectomy and was discharged.At age 6 years, she was readmitted for pneumonia which was
preceded by a viral upper respiratory tract infection. A sputumculture revealed Pseudomonas aeruginosa, and appropriateantibiotic therapy was begun. While in the hospital, the patienthad a complete immunologic reevaluation, including an au-toantibody screen. A positive Coombs' test was discovered, butthere was no clinical or laboratory evidence of hemolysis. Thepatient improved initially but ultimately died from measlespneumonitis despite intensive therapy with intravenous gammaglobulin, nebulized and intravenous ribavarin, and mechanicalventilatory support.
Autopsy revealed chronic bronchiectasis, giant cell pneumo-nia, chronic esophagitis, absent Hassall's corpuscles in thethymus, and absent follicles in lymph nodes and appendix.
Clinical and immunological characteristics of CMC pa-tients. As illustrated in Table 1, all the patients were diagnosedwithin the first 2 years of life, and as expected, they allpresented with chronic superficial candidal infections. In addi-tion, autoantibodies to various autoantigens were detected inall the patients (Table 3), but only two of the six patients (33%)developed AIHA.The patients also exhibited variable immunologic character-
istics (Tables 4, 5, and 6). An observation made for all the
CLIN. DIAGN. LAB. IMMUNOL.
on June 20, 2020 by guesthttp://cvi.asm
.org/D
ownloaded from

AUTOIMMUNE ANEMIA IN CHRONIC MUCOCUTANEOUS CANDIDIASIS 41
TABLE 4. Immunohematologic dataa
Direct antiglobulinCase Indirect Erythrocyteno. Poly- Anti- Anti- antiglobulin IgGspecific IgG C3d
1First episode + + + + + NA"Second episode +++ +++ + +C ++++
2 + + - + ++3 + + - + +
a -, no agglutination; + to + + + +, increasing degree of agglutination.NA, not available.
c IgG and IgM.
patients was cutaneous anergy to Candida antigens and otherantigens as well as defective lymphoproliferative response toCandida antigen. Lymphoproliferative responses to mitogenswere also impaired to a variable degree. There is no evidentimmunological predictor of AIHA.
RESULTS AND DISCUSSION
A wide range of autoimmune disorders have been reportedin association with CMC (7, 12, 19). This is the first report ofthe occurrence of clinically significant autoimmune hemolyticanemia in association with CMC. Two of six patients (33%)with CMC who were included in this study developed AIHAthat required therapy. Case 3 developed erythrocyte autoanti-bodies without clinical or laboratory evidence of hemolysis.AIHA is a clinical disorder characterized by the develop-
ment of erythrocyte autoantibodies, which result in decreasederythrocyte survival, ultimately leading to anemia (20). Theautoantibodies in AIHA may be warm-reacting IgG or cold-reacting IgM (16, 20). One of the patients developed both IgGand IgM erythrocyte autoantibodies, whereas the remainingtwo patients had only IgG autoantibody. Eluates preparedfrom the patients' erythrocytes confirmed the presence of IgGautoantibody which reacted with all the erythrocyte antigenstested.A review of clinical as well as immunologic markers in the six
patients with CMC did not yield any marker that distinguishesbetween the patients who developed AIHA and those who didnot. The occurrence of autoantibodies to various autoantigensin all six patients with CMC, including those who did not haveerythrocyte autoantibodies, is consistent with previous reportsthat patients with CMC are very likely to develop autoimmu-nity (7, 12, 19). Indeed, an attractive unifying hypothesis toexplain the heterogeneous features of CMC suggested anautoimmune disorder directed at the lymphoid apparatus,causing a cell-mediated defect which in turn results in chroniccandidiasis and progressive endocrinopathy (3).
Evidence from a number of animal model systems of auto-immunity has suggested that loss of effective suppressor T-cell
function can lead to autoimmune disease (26). Extensivestudies carried out in the New Zealand Black mice model ofautoimmunity and with hybrids produced by crossing NewZealand Black and New Zealand White mice have shed some
light on the pathogenesis of AIHA. New Zealand Black micespontaneously develop antierythrocyte antibodies by 3 monthsof age; the direct antiglobulin test is positive by 9 months ofage, and then typical signs of AIHA appear (37). The anti-erythrocyte autoantibodies are both IgG and IgM. Autoanti-bodies also develop in the hybrid mice. The pathogenesis ofautoantibody formation in these animals has been suggested tobe the result of loss of suppressor cell activity as they age,
which allows the development of forbidden clones of lympho-cytes with self-antigen specificity (26). Consistent with reportsby other investigators (4, 25), our patients with CMC havesome defects in T-cell immunity. The idea that the develop-ment of erythrocyte autoantibodies in these patients is relatedto some T-cell regulatory defects is therefore very attractive.
Therapeutic intervention in AIHA depends largely on theextent of symptoms, which correlate with the level and rate ofdestruction of erythrocytes. Overall, the goals of therapyinclude immediate restoration of adequate oxygen transport byincreasing circulatory erythrocyte mass; decreased destructionof opsonized erythrocytes; control of the population of B-cellsthat secrete the pathogenic autoantibody; and treatment of anyassociated underlying disease in secondary forms of AIHA(20). Corticosteroids constitute the cornerstone of treatmentfor both the primary and secondary forms of AIHA (20).Corticosteroids downregulate Fc receptor expression and thusdecrease the splenic clearance of erythrocytes that are opso-nized with IgG or C3b (5, 35). The second patient hadinsidious onset of hemolytic anemia which responded well totreatment with oral prednisone on three occasions. On theother hand, the first patient had a much more rapid onset ofsymptoms and more severe hemolytic anemia that requiredmultiple therapeutic modalities, including intravenous ste-roids, intravenous gammaglobulin, packed erythrocyte transfu-sion, and plasmapheresis. During the two admissions, intrave-nous gammaglobulin and intravenous steroids were started atalmost the same time. It is therefore impossible to comment onthe relative efficacy of these two forms of therapy for thispatient. Intravenous gammaglobulin has been used successfullyin the treatment of other autoimmune cytopenias, especiallyimmune thrombocytopenia (20). The proposed mechanismsfor its action include Fc receptor blockage, heightened T-suppressor function, anti-idiotypic counterregulation, and in-terference with the cytokine cascade (27). However, intrave-nous gammaglobulin has occasional but limited efficacy inAIHA (6). The observation that the first patient requiredpacked erythrocyte transfusion during the first admission andplasmapheresis during the second admission despite treatmentwith high-dose intravenous gammaglobulin tends to supportthe limited efficacy of this form of treatment in AIHA.
TABLE 5. Humoral immune data
Quantitative Ig titer Functional antibodies'Case no. Isohemagglutinins (titer)
IgG IgA IgM Tetanus Diphtheria Pneumococcal Haemophilus influenzae Rubella Mumps
1 1,820 324 607 - - - - + + ob
2 1,170 116 158 - - - + ND ND Anti-A (1:512), anti-B (1:8)3 1,040 99 130 - - + + ND ND Anti-A (1:64), anti-B (1:2)
a -, not protective; +, protective; ND, not determined.b Blood group AB.
VOL. 1, 1994
on June 20, 2020 by guesthttp://cvi.asm
.org/D
ownloaded from

42 OYEFARA ET AL.
TABLE 6. Cellular immune data for patients with CMC
Delayed-typeCD4 Lymphocyte stimulation (% of control) hypersensitivityCase Absolute lymphocyte count CD4/CD8 skin test'
no. count (cells/,J) count ratio(cells4i.l)(cells ,u) Phytohemag- Concanavalin Pokeweed Candida Diphtheria Tetanus Candida Otlbglutinin A mitogen antigen toxoid toxoid spp. the
1 1,184-2,880 1,129 1.5 70 47 60 10.5 6.2 6 NDC2 1,095-2,600 633 0.72 57 73 26 3 ND ND3 420-1,196 538 1.2 16 19 19 0 ND ND -4 1,353-3,692 652 1.3 96 67 79 25 ND 53 -5 1,056-4,080 1,323 2.09 147 155 102 0 0 7 -6 1,278-3,536 787 0.88 138 111 83 0.6 0 0
-, negative."Tetanus toxoid, diphtheria toxoid, and trichophyton extract.c ND, not done.
During the second admission, the first patient required dailyplasmapheresis for 5 days. Plasmapheresis acts by removingautoantibodies from the circulation, thereby slowing downhemolysis before the effects of corticosteroid or other immu-nosuppressive drugs are established (20). However, plasma-pheresis is more effective in AIHA caused by IgM autoanti-bodies, since, at any given time, most of the IgG autoantibodiesare bound to erythrocytes. Of note, the first patient had bothIgM and IgG autoantibodies. In addition, high-dose methyl-prednisolone was continued throughout the period of plasma-pheresis. It is therefore possible that plasmapheresis onlyslowed down hemolysis before the full effects of the steroidbecame established.The synthetic androgen danazol has been reported to be
effective in some patients with immune thrombocytopenia (34)and AIHA (2, 10). The proposed mechanisms for its actioninclude downregulation of Fc receptors in monocytes (34),immune modulation by normalization of CD4/CD8 lympho-cyte ratios (29), and increased resistance of erythrocyte mem-branes to osmotic lysis (2). However, an outpatient trial ofdanazol for our second patient was unsuccessful and had to bediscontinued because of the development of significant sideeffects, especially hirsutism.
In general, splenectomy is an alternative therapeutic optionfor patients with AIHA who require high maintenance pred-nisone doses (10 to 20 mg/day) or who have multiple andfrequent relapses or serious side effects from steroid therapy(20). Splenectomy removes a major portion of both the phago-cytic reticuloendothelial system and the autoantibody-producingB cells (20). At least 50% of patients with AIHA have a goodinitial response to splenectomy, but there is no clinical orlaboratory measurement that can predict who will benefit fromsplenectomy (20, 21). Our first patient refused splenectomy.
In conclusion, these case reports indicate that clinicallysignificant AIHA occurs in patients with CMC. We thereforesuggest that all patients with CMC be screened periodically forerythrocyte autoantibodies. When frank hemolysis occurs orpatients become refractory to corticosteroids and/or intrave-nous gammaglobulin, plasmapheresis should be considered asa therapeutic option before the addition of potent immuno-suppressive therapy, which could be detrimental for patientswho are already immunosuppressed. Further studies are
needed to elucidate the precise immunoregulatory defect thatis responsible for the development of erythrocyte autoantibod-ies in patients with CMC.
REFERENCES1. Ahn, Y., L. F. Fernandez, C. I. Kim, et al. 1989. Danazol therapy
renders red cells resistant to osmotic lysis. FASEB J. 3:157-162.
2. Ahn, Y. S., W. J. Harrington, R. M. Mylvagamam, J. Ayab, andL. M. Paul. 1985. Danazol therapy for autoimmune hemolyticanemia. Ann. Intern. Med. 102:298-301.
3. Ammann, A. J., and R. Hong. 1989. Chronic mucocutaneouscandidiasis, p. 286-290. In E. R. Stiehm (ed.), Immunologicdisorders of infants and children, 4th ed. W. B. Saunders Com-pany, Philadelphia.
4. Aralamanthem, K., J. M. Dwyer, and M. Genel. 1979. Defectiveimmunoregulation in familial candidiasis endocrinopathy syn-drome. N. Engl. J. Med. 300:164-168.
5. Atkinson, J. B., A. D. Schreiber, and M. M. Frank 1973. Effects ofcorticosteroids and splenectomy on the immune clearance anddestruction of erythrocytes. J. Clin. Invest. 52:1509-1517.
6. Besa, E. C. 1988. Rapid transient reversal of anemia and long-termeffect of maintenance intravenous immunoglobulin for autoim-mune hemolytic anemia in patients with lymphoproliferative dis-orders. Ann. Intern. Med. 84:691-698.
7. Blizzard, R. M., and J. A. Gibbs. 1968. Candidiasis: studiespertaining to its association with endocrinopathies and perniciousanemia. Pediatrics 42:231-237.
8. Cahill, L. T., E. Ainbender, and P. R. Glad. 1974. Chronicmucocutaneous candidiasis: T cell deficiency associated with B celldysfunction in man. Cell. Immunol. 14:215-225.
9. Canales, L., R. 0. Middlemos, and J. M. Louro. 1969. Immuno-logical observations in chronic mucocutaneous candidiasis. Lancetii:567-571.
10. Chan, A. C., and K. Sack 1991. Danazol therapy in autoimmunehemolytic anemia associated with systemic lupus erythromatosus.J. Rheumatol. 18:280-282.
11. Chilgren, R. A., P. G. Quie, H. J. Meuwissen, R. A. Good, and R.Hong. 1969. The cellular immune defect in chronic mucocutane-ous candidiasis. Lancet i:1286-1288.
12. Deeg, H. J., L. G. Lum, J. Sanders, G. J. Levy, K. M. Sullivan, P.Beatty, D. Thomas, and R. Storb. 1986. Severe aplastic anemiaassociated with chronic mucocutaneous candidiasis. Transplanta-tion 41:583-586.
13. Drew, J. H. 1973. Chronic mucocutaneous candidiasis with abnor-mal function of serum complement. Med. J. Aust. 2:77-80.
14. Durandy, A., A. Fischer, F. LeDeist, E. Drouchet, and C. Griscelli.1987. Mannan-specific and mannan-induced T-cell supressive ac-tivity in patients with chronic mucocutaneous candidiasis. J. Clin.Immunol. 7:400-409.
15. Flynn, P. M., F. F. Barrett, and H. G. Herrod. 1987. Disseminatedhistoplasmosis in two patients with chronic mucocutaneous candi-diasis. Pediatr. Infect. Dis. J. 6:691-692.
16. Gibson, J. 1988. Autoimmune hemolytic anemia: current concepts.Aust. N. Z. J. Med. 18:625-637.
17. Gill, F. F., and J. M. Portnoy. 1989. An unusual combination ofimmunologic abnormalities in patients with chronic mucocutane-ous candidiasis. Ann. Allergy 63:98-100, 147-148.
18. Gupta, S. 1985. Autologous mixed lymphocyte reaction in man.XI. Deficiency of autologous mixed lymphocyte reaction andabnormalities of monoclonal antibody-defined T-cell subsets in
CLIN. DIAGN. LAB. IMMUNOL.
on June 20, 2020 by guesthttp://cvi.asm
.org/D
ownloaded from

AUTOIMMUNE ANEMIA IN CHRONIC MUCOCUTANEOUS CANDIDIASIS 43
chronic mucocutaneous candidiasis. Scand. J. Immunol. 21:525-530.
19. Herrod, H. G. 1990. Chronic mucocutaneous candidiasis in child-hood and complications of non-candidal infection: a report of thePediatric Immunodeficiency Collaboration Study Group. J. Pedi-atr. 116:377-382.
20. Hillyer, C. D., E. M. Berkman, and R. S. Schwartz. 1990. Auto-immune hemolytic anemia and cold agglutinin disease: autoanti-bodies, mechanisms and therapy. Clin. Aspects Autoimmun. 5:22-32.
21. Jandi, J. H., and M. E. Kaplan. 1960. The destruction of red cellsby antibodies in man. III. Quantitative factors influencing thepattern of hemolysis in vivo. J. Clin. Invest. 39:1145-1149.
22. Kauffinan, C. A., M. J. Shea, and P. T. Franne. 1981. Invasivefungal infections in patients with chronic mucocutaneous candidi-asis. Arch. Intern. Med. 141:1076-1078.
23. Kirkpatrick, C. H. 1988. Chronic mucocutaneous candidiasis.Antibiotic and immunologic therapy. Ann. N.Y. Acad. Sci. 544:471-480.
24. Kirkpatrick, C. H. 1989. Chronic mucocutaneous candidiasis. Eur.J. Clin. Microbiol. Infect. Dis. 8:448-456.
25. Kirkpatrick, C. H., R. R. Rich, and J. E. Bennett. 1971. Chronicmucocutaneous candidiasis: model building in cellular immunity.Ann. Intern. Med. 74:955-978.
26. Krakauer, R. S. 1978. Disorders of the suppressor cell system inautoimmunity. Ann. Intern. Med. 88:226-238.
27. Levinson, A. L. 1989. Mechanisms of action of intravenous immu-noglobulin in patients with autoimmune disease. Immunol. Up-dates 1:1-4.
28. Mobacken, H., L. Lindholm, and S. Moberg. 1987. Immunologicalstudies in chronic mucocutaneous candidiasis before and afterketoconazole treatment. Acta Dermato-Venereol. 67:257-260.
29. Mylvaganam, R., Y. S. Ahn, W. Harrington, and C. I. Kron. 1987.Immune modulation by danazol in autoimmune thrombocytope-nia. Clin. Immunol. Immunopathol. 42:281-287.
30. Noh, L M., S. H. Hussein, K. D. Siukumaran, I. Rose, and N.
Abdullah. 1991. Chronic mucocutaneous candidiasis with deficientCD2 but normal CD3 mononuclear cells. J. Clin. Lab. Immunol.35:89-93.
31. Rosenblatt, H. R., S. Ladisch, R. M. Albrecht, R. I. Lehrer, T. J.Fuscher, R. Hong, and E. R. Stiehm. 1979. Monocyte effectordefects in chronic mucocutaneous candidiasis (abstract). Pediatr.Res. 13:454.
32. Ruiz-Arguelles, A., J. R. Jett, and R. E. Ritts, Jr. 1983. Impairedgeneration of helper T-cells in a patient with chronic mucocuta-neous candidiasis and malignant thymoma. J. Clin. Lab. Immunol.10:165-169.
33. Sander, E., G. Prolla, A. R. Marques, T. Zelmanowitz, M.Zampese, and G. Schwartsmann. 1993. Reversal by interleukin-2of alopecia universalis, mucocutaneous candidiasis, and sexualimpotence in a patient with malignant thymoma. J. Natl. CancerInst. 85:673.
34. Schreiber, A. D., P. Chien, A. Tomask, and D. B. Cines. 1987.Effect of danazol in immune thrombocytopenia purpura. N. Engl.J. Med. 316:503-508.
35. Schreiber, A. D., J. Parsons, P. McDermot, et al. 1975. The effectof corticosteroids on the human monocyte IgG and complementreceptors. J. Clin. Invest. 56:1189-1197.
36. Stobo, J. D., S. Paul, R. E. VanScoy, and P. E. Hermans. 1976.Suppressor thymus-derived lymphocytes in fungal infection. J.Clin. Invest. 57:319-328.
37. Theofilopoulos, A. N., and F. J. Dixon. 1985. Murine models ofsystemic lupus erythematosus. Adv. Immunol. 37:269-290.
38. Vanscoy, R. E., H. R. Hill, R. E. Ritts, and P. G. Quie. 1975.Familial neutrophil chemotaxis defect, recurrent bacterial infec-tions, mucocutaneous candidiasis and hyperimmunoglobulin E.Ann. Intern. Med. 82:766-771.
39. Whitaker, J., B. H. Landing, V. M. Esselborn, and R. R. Williams.1956. Syndrome of familial juvenile hypoadrenocortism, hypopar-athyroidism and superficial moniliasis. J. Clin. Endocrinol. 16:1374-1387.
VOL. 1, 1994
on June 20, 2020 by guesthttp://cvi.asm
.org/D
ownloaded from