Embed Size (px)
Citation preview

D ISK HEMORRHAGES ARE MORE FREQUENT IN PATIENTS
with normal-tension glaucoma than other types ofglaucoma and normal control subjects. Disk hemorrhage isclosely associated with retinal nerve fiber layer defect inthe location and size of peripapillary atrophy and is asignificantly negative prognostic factor in patients withnormal-tension glaucoma.1–2 Branch retinal vein occlusiondoes not seem to be related to intraocular pressure (IOP)and primary open-angle glaucoma, especially when occur-ring at an arteriovenous crossing.3 Conversely, in open-angle glaucoma patients, Sonnsjo and associates4 notedthat the incidence of retinal venous occlusion (10.5%) washigher than in control subjects (1.3%) and that diskhemorrhage was also present in some cases (29 of 1,026cases). These researchers hypothesized that disk hemor-rhage is the thrombosis of very small vessels. However,there has been no report dealing with branch retinal veinocclusion in normal-tension glaucoma patients with diskhemorrhage.
From July 2001 to June 2002, during diagnostic workupfor normal-tension glaucoma patients in the GlaucomaClinic of Seoul National University Hospital, 15 cases ofnormal-tension glaucoma with disk hemorrhage in one eyewere detected, four of which showed combined branchretinal vein occlusion in the contralateral eye. Twenty-four hour IOP measurement, fundus examination, retinalnerve fiber layer photography, stereo disk photography,Humphrey visual field analysis, confocal scanning lasertomography, and fluorescein angiography were performedfor all four patients.
Table 1 shows the clinical characteristics of the fourpatients. Mean age was 57 � 10 years (range, 47–71 years).Three patients (75%) had systemic hypertension. Twopatients had bilateral normal-tension glaucoma and thusbranch retinal vein occlusion in normal-tension glaucomaeyes. Three patients showed occlusion occurring at thearteriovenous crossing and one patient at the optic cup.Mean cup-to-disk ratio ranged from 0.5 to 0.8. There wasno significant difference in IOP between the disk hemor-rhage eyes and the contralateral eyes with branch retinalvein occlusion. All four patients had bilateral peripapillaryatrophy and retinal nerve fiber layer defects collocatedwith the disk hemorrhage (Figure 1).
To the best of our knowledge, this is the first report ofdisk hemorrhage in normal-tension glaucoma associatedwith contralateral branch retinal vein occlusion. Thesecases suggest the possibility that some disk hemorrhages innormal-tension glaucoma may have a pathogenic mecha-nism in common with branch retinal vein occlusion andmay likewise be caused by thrombosis of very small vessels.
REFERENCES
1. Sugiyama K, Tomita G, Kitazawa Y, Onda E, Shinohara H,Park KH. The associations of optic disk hemorrhage withretinal nerve fiber layer defect and peripapillary atrophy in
normal-tension glaucoma. Ophthalmology 1997;104:1926–1933.
2. Ishida K, Yamamoto T, Sugiyama K, Kitazawa Y. Disk hem-orrhage is a significantly negative prognostic factor in normal-tension glaucoma. Am J Ophthalmol 2000;129:707–714.
3. Beaumont PE, Kang HK. Cup-to-disk ratio, intraocular pres-sure, and primary open-angle glaucoma in retinal venousocclusion. Ophthalmology 2002;109:282.
4. Sonnsjo B, Krakau CE. Arguments for a vascular glaucomaetiology. Acta Ophthalmol 1993;71:433–444.
Autoclavable Wide-angle ContactLens for Vitreous SurgeryVinay A. Shah, MD, andKakarla V. Chalam, MD
PURPOSE: To evaluate an autoclavable self-stabilizingwide-angle contact lens for vitrectomy.DESIGN: Observational study.METHOD: The wide-angle contact lens has two lens pieceswithin a high temperature-resistant (150 C) plasticcasing. The inferior lens with footplates is made ofacrylic and the superior of glass. During surgery the lensis used as the self-stabilizing wide-angle contact lens withimproved stability on the eye.RESULT: The lens enables the surgeon to address theperipheral retina with less dependence on the assistant.The lens is sterilizable by autoclaving. The field of viewof the wide-angle lens is 106 degrees static and 127degrees dynamic view.CONCLUSION: The autoclavable self-stabilizing wide-anglelens reduces the cost and time for sterilization. (Am JOphthalmol 2004;137:359–360. © 2004 by ElsevierInc. All rights reserved.)
GOOD VISUALIZATION OF THE FUNDUS IS CRUCIAL FOR
successful vitreous surgery. Wide-field viewing withan appropriate contact lens is a major advance in thisdirection. Sterilization of these lenses is traditionally doneeither by ethylene oxide gas or chemically by glutaralde-hyde 2% or povidone iodine 5%.1 Sterilization with steamautoclaving is cost effective, fast, and widely used. How-ever, it cannot be used for presently available wide-angle,self-stabilizing lenses.2 We describe a new autoclavableself-stabilizing, wide-angle lens for vitreous surgery.
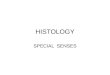
The wide-angle contact lens (Figure 1, A) has two lenspieces within a high temperature-resistant 302 F (150 C)plastic casing. The inferior part has an acrylic concavocon-vex lens with footplates (Figure 1, B; refractive index [RI]1.51). The concave contact surface has a radius of curva-
Accepted for publication July 22, 2003.From the Department of Ophthalmology, University of Florida College
of Medicine, Jacksonville, Florida.Inquiries to Kakarla V. Chalam, MD, Department of Ophthalmology,
University of Florida College of Medicine, 580 W. 8th Street, Jackson-ville, FL 32209; fax: (904) 244-9391; e-mail: [email protected]
BRIEF REPORTSVOL. 137, NO. 2 359
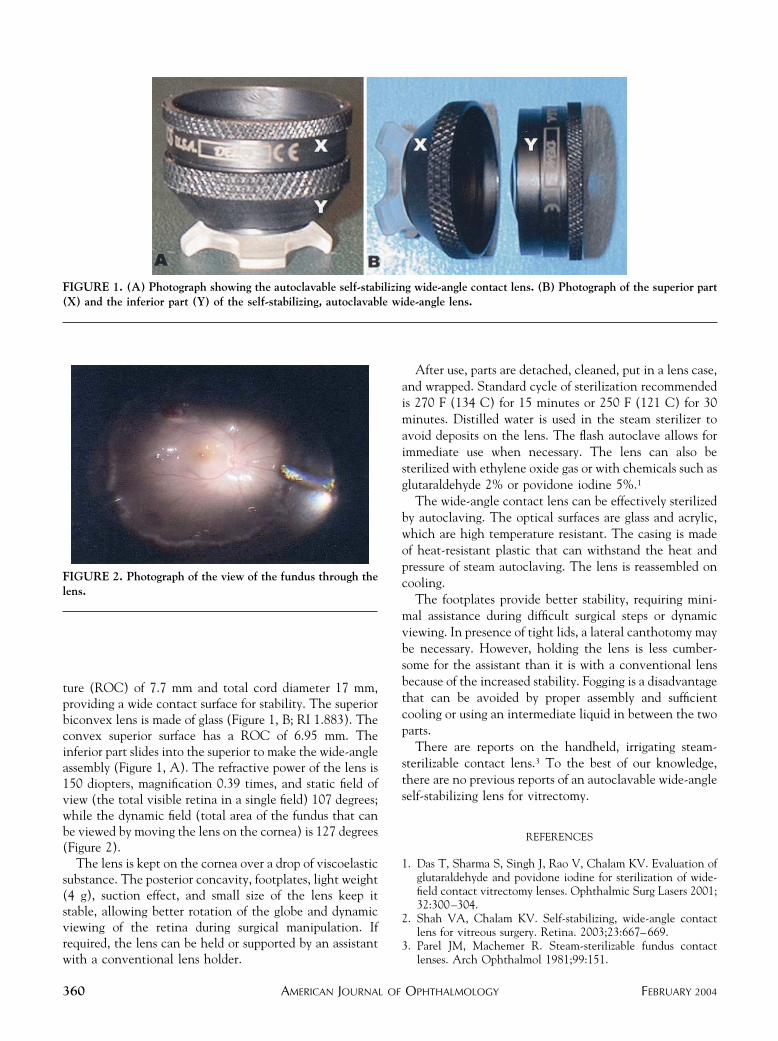
ture (ROC) of 7.7 mm and total cord diameter 17 mm,providing a wide contact surface for stability. The superiorbiconvex lens is made of glass (Figure 1, B; RI 1.883). Theconvex superior surface has a ROC of 6.95 mm. Theinferior part slides into the superior to make the wide-angleassembly (Figure 1, A). The refractive power of the lens is150 diopters, magnification 0.39 times, and static field ofview (the total visible retina in a single field) 107 degrees;while the dynamic field (total area of the fundus that canbe viewed by moving the lens on the cornea) is 127 degrees(Figure 2).
The lens is kept on the cornea over a drop of viscoelasticsubstance. The posterior concavity, footplates, light weight(4 g), suction effect, and small size of the lens keep itstable, allowing better rotation of the globe and dynamicviewing of the retina during surgical manipulation. Ifrequired, the lens can be held or supported by an assistantwith a conventional lens holder.
After use, parts are detached, cleaned, put in a lens case,and wrapped. Standard cycle of sterilization recommendedis 270 F (134 C) for 15 minutes or 250 F (121 C) for 30minutes. Distilled water is used in the steam sterilizer toavoid deposits on the lens. The flash autoclave allows forimmediate use when necessary. The lens can also besterilized with ethylene oxide gas or with chemicals such asglutaraldehyde 2% or povidone iodine 5%.1
The wide-angle contact lens can be effectively sterilizedby autoclaving. The optical surfaces are glass and acrylic,which are high temperature resistant. The casing is madeof heat-resistant plastic that can withstand the heat andpressure of steam autoclaving. The lens is reassembled oncooling.
The footplates provide better stability, requiring mini-mal assistance during difficult surgical steps or dynamicviewing. In presence of tight lids, a lateral canthotomy maybe necessary. However, holding the lens is less cumber-some for the assistant than it is with a conventional lensbecause of the increased stability. Fogging is a disadvantagethat can be avoided by proper assembly and sufficientcooling or using an intermediate liquid in between the twoparts.
There are reports on the handheld, irrigating steam-sterilizable contact lens.3 To the best of our knowledge,there are no previous reports of an autoclavable wide-angleself-stabilizing lens for vitrectomy.
REFERENCES
1. Das T, Sharma S, Singh J, Rao V, Chalam KV. Evaluation ofglutaraldehyde and povidone iodine for sterilization of wide-field contact vitrectomy lenses. Ophthalmic Surg Lasers 2001;32:300–304.
2. Shah VA, Chalam KV. Self-stabilizing, wide-angle contactlens for vitreous surgery. Retina. 2003;23:667–669.
3. Parel JM, Machemer R. Steam-sterilizable fundus contactlenses. Arch Ophthalmol 1981;99:151.
FIGURE 1. (A) Photograph showing the autoclavable self-stabilizing wide-angle contact lens. (B) Photograph of the superior part(X) and the inferior part (Y) of the self-stabilizing, autoclavable wide-angle lens.
FIGURE 2. Photograph of the view of the fundus through thelens.
AMERICAN JOURNAL OF OPHTHALMOLOGY360 FEBRUARY 2004