Embed Size (px)
DESCRIPTION
Autism Spectrum Disorders: An Introduction Rhea Paul, Ph.D., CCC-SLP Southern Connecticut State University Yale Child Study Center Feb. 11-15, 2008 [email protected]. Diagnostic Concepts: Pre 1940. Insanity of Childhood (Maudsley, 1867) Dementia Praecox (Kraeplin, 1893) - PowerPoint PPT Presentation
Citation preview

Autism Spectrum Disorders: An Introduction
Rhea Paul, Ph.D., CCC-SLPSouthern Connecticut State University
Yale Child Study CenterFeb. 11-15, 2008

Diagnostic Concepts: Pre 1940
•Insanity of Childhood (Maudsley, 1867)•Dementia Praecox (Kraeplin, 1893)•Dementia Praecocissima (DeSanctis,
1906)•Dementia Infantilis (Heller, 1908)•Childhood Schizophrenia (Potter,
1930)

A Brief History of Autism: Kanner (1943)
“There is from the start an extreme autistic aloneness (p. 33)… these children have come into the world with innate inability to form the usual, biologically provided affective contact with people, just as other children come into the world with innate physical or intellectual handicaps (p. 42-43).”
described echolalia pronoun reversals inappropriate word usages noted better abilities with objects
than with people

A Brief History of Autism: Kanner (1943) Autism first used by Leo Kanner (1943) to
describe a syndrome of "disturbances in affective contact," observed in eleven boys who
lacked the dysmorphology often seen in mental retardation,
lacked social motivation toward communication and interaction.
Did well on some parts of IQ tests leading to speculation they were not MR
Kanner borrowed autism from Bleuler (1950), used to describe the withdrawal into fantasy world seen in
people with schizophrenia. Kanner's report stated that autism was an inborn, constitutional
disorder, but choice of terminonology led to some confusion about the
source of the deficits in autism.

Hans Asperger At about the same time, a German psychiatrist
reported a similar syndrome (Asperger, 1944) Boys reported to be highly intelligent and verbal but socially inept Like “little professors” Noticed similar profile in their fathers
Asperger’s report was not translated from the German until the 1980s it had little impact on the literature on autistic syndromes in the
English speaking world. Still a matter of debate:
Do the intelligent boys with well-developed language, poor social skills, and obsessive interests have something different from Kanner’s autism?
Or merely a variety of autism in high functioning individuals?

A Brief History of Autism: 1950s Work on autism through the 1960s dominated by
psychoanalysts (e.g., Bettelheim, 1967) focused on the theory that autism was caused by
"refrigerator mothers.” Other mental illnesses were also seen this way; e.g.,
schizophrenia Kanner's boys came from upper middle class, often
intellectual families, reinforcing suggestion that autism was the result of cold parenting.
In the 1970s research began to show that autism, properly diagnosed, can be seen in all social classes in every part of the world
At the same time, grassroots efforts by parents to dispel “refrigerator mother” myth Parents of children with autism had other, normal children

A Brief History of Autism: 60s-70s
1970s Rutter, Wing researched cognitive and linguistic impairments
This led to behavioral/educational Rx Wing’s patterns of autistic presentation
Aloof Passive Active but odd
Cohen, others, began neurobiological research

A Brief History of Autism: 70s-90s
1990s focus on interrelated core symptoms: socio-communicative, social-cognitive dysfunctions
DSM-IV criteria (1994): triad of impairments Impairment in social interaction Impairment in communication Restricted, repetitive and stereotyped patters of behaviors,
interests, and activities ICD-10 criteria: PDD defined by
abnormal and/or impaired development that is manifest before the age of 3 years
abnormal functioning social interaction communication restricted, repetitive behavior

Etiology of Autism: A brief history
Early focus on parentsPsychodynamic viewsBUT evidence against
No abnormalities in child careNo major personality problemsNo obvious deficits in parenting
By 1970's a large body of evidence favoring neurobiological etiology

1990s-present: Biological Influences
It is now clear that the disorders seen in autism originate in the child, not the parents.
Neurochemical differences are seen in pts. (hyperserotonemia) Head size and brain differences are subtle, but measureable Prenatal abnormalities (trophoblasts)
Research on the genetics of autism suggests there are heritable factors that convey a susceptibility (Rutter, Bailey, Simonoff, & Pickles, 1997).
Social, communicative, and cognitive difficulties seen in varying degrees in parents, siblings, and other relatives (Broader autism phenotype-BAP)
Although genetic factors contribute to appearance of autism, it can also be associated with other medical conditions.
25% of individuals with autism develop seizure disorders (Rapin, 1991). Tuberous sclerosis (abnormal tissue growth) associated with autism The co-occurrence of autism and Fragile X syndrome (the most common
heritable form of mental retardation) is higher than would be expected (Dykens & Volkmar, 1997).

A Brief History of Autism: 90s-present DSM-IV Field Trial
to validate diagnostic criteria
Definition of syndromes and subgroups within PDD spectrum
New areas of research: Neuroimaging Genetics Event-related
potentials Theory of Mind;
neuropsychology Early identification
and intervention Treatment research
Psychopharmacology Behavioral/
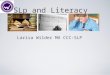
EducationalFig. 1. AV emotional stimuli greater than AV bouncing ball perception; arrows point to the right STS
STS

EtiologyAutism as a final common pathway
CNS Pathologyseizures, "soft" sign, reflexes, EEG abnormalities
Other medical conditionsinfectious, structural, chromosomal, etc.Strongest associations: Fragile X (1%) & Tuberous sclerosis
Genetic Factors Need for testable neurobiological hypotheses and mechanisms

Diagnostic Concepts: Post 1940
•Early Infantile Autism (Kanner, 1943)•Autistic Psychopathy (Asperger, 1944)•Atypical Personality (Rank, 1949)•Pervasive Developmental Disorder
(APA, 1980)•Autism Spectrum Disorders (2000s)

Behavioral Features
Severe social deficitsCommunication deficits (verbal and
nonverbal)Unusual responses to environmentInsistence on SamenessStereotyped movements Special interests/preoccupations

Social Disturbance
Distinctive & greater than expected given MASome social skills emerge with timeTypes
AloofPassiveActive but Odd
Deficits inmutual gazejoint attentiontheory of mind

Triad of Symptoms that Define Autism in DSM-IV Severe, qualitative impairment in
social interaction Qualitative impairment in
communication Delayed language = autism or PDD-NOS No language delay = AS
Restrictive, repetitive or stereotyped behaviors or interests

Empirical Bases for DSM-IV Field Trial: Volkmar et al., 1994
Multiple sites 977 patients with autism, other pervasive
developmental disorders, and other disorders standard coding system used 125 raters with range of experience Patterns of agreement among existing diagnostic
systems examined International Classification of Diseases (ICD), 10th
Revision, most closely approximated the clinicians' diagnoses
Inclusion of other disorders within pervasive developmental disorders appeared justified
Modifications in the ICD-10 definition were made; DSM-IV definition made equivalent

Normal Social Development
• From the first days of life infants are profoundly sociable• Human face/voice are the most interesting stimuli in the environment• Early emergence of • Selective attention to faces and voices• Social reciprocity: mutual gaze, smiling• Attachments to familiar people• Social-communicative skills

Early Acquired Social SkillsJoint attention, attachment,
imitation

Normal Social Interaction: Infants

Normal Social Interaction: Toddlers

Normal Social Interaction: Preschoolers

Normal Social Interaction: Language Delay: Brittany

Normal Social Interaction: Language Delay

Autism Every Day video http://www.milestonevideo.tv/nonprofi
t.php