Embed Size (px)
Citation preview

This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial research
and education use, including for instruction at the author'sinstitution and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier's archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/authorsrights

J A C C : C A R D I O V A S C U L A R I M A G I N G V O L . 1 2 , N O . 9 , 2 0 1 9
I S S N 1 9 3 6 - 8 7 8 X / $ 3 6 . 0 0
Author's Personal Copy
LETTERS TO THE EDITOR
Micro-Optical Coherence Tomography
for Endothelial Cell Visualization in
the Coronary Arteries
Coronary arteries are covered by a layer of endothelialcells (ECs) that have a thickness of approximately1 mm. Impairment of ECs is at the origin of coronaryatherosclerosis and its clinical manifestations. Thecurrent gold standard, scanning electron microscopy(SEM), has demonstrated that ECs form an endolumi-nal feature referred to as “endothelial pavementing”(1). However, the assessment of ECs in humans re-mains elusive because a clinical imagingmodality withsufficient resolution does not exist. This study inves-tigated the use of a new form of optical coherence to-mography (OCT), termed micro-OCT (mOCT) (2), whichoffers an axial resolution of 1 mm and a lateral resolu-tion of 2 mm, for evaluating EC morphology.
First, we stripped the endothelium from freshswine coronary segments with cyanoacrylate adhe-sive. Coronary segments were imaged 3 dimension-ally (3D) with mOCT. mOCT images were then3D-volume rendered using ImageJ (3). 3D mOCTallowed clear visualization of endothelial pavement-ing (Figure 1A, left top and middle panels) with cellsoriented parallel to the coronary flow direction(Figure 1A, left top and middle panels), not seen at thesites where ECs were stripped off (Figure 1A, top rightpanel). The surface roughness, measured as rootmean squared (RMS), diminished significantly at sitesof EC stripping compared with intact sites (3.4 � 0.1mm vs. 1.5 � 0.1 mm, p < 0.01). Subsequently, swinecoronary segments were processed for SEM and wereco-registered to the same area imaged by mOCT. Themorphology of ECs visualized by 3D mOCT was similarto that seen by SEM (Figure 1A, middle panels). 3DSEM data were computed from 2-dimensional SEMimages using intensity thresholding and Mountains-Map software (Digital Surf, Besançon, France). Forboth intact and stripped sites, strong positivecorrelations were noted between the RMS calculatedfor mOCT and SEM (R2 ¼ 0.95, p < 0.01; R 2¼ 0.97, p <
0.01, respectively) (Figure 1B, left top and bottomgraphs). We also used mOCT to explore ECmorphology in human cadaver coronary plaques.Conventional OCT cross sections were obtainedbefore mOCT to characterize human coronary lesion
tissue type. After standard OCT pullback, 1-cm-longcoronary segments (n ¼ 45) from 8 fresh cadaverhearts were opened and imaged in 3D with mOCT andco-registered with SEM. As per the correspondingstandard OCT images, the tissue type of each coro-nary segment was classified as intimal hyperplasia,fibrous plaque, fibroatheroma, or fibrocalcific plaque.Figure 1A, bottom panels, show typical endothelialmorphology of a fibrous plaque seen by 3D mOCT andco-registered SEM. mOCT RMS was significantly lowerover fibroatheroma and fibrocalcific plaquescompared with intimal hyperplasia and fibrous seg-ments (p < 0.01) (Figure 1B, right).
The major findings of the present study werethat: 1) 3D mOCT was capable of clearly visualizing ECmorphology that manifested endothelial pavement-ing in intact swine coronary arteries, as confirmed bysurface morphology seen by SEM; and 2) 3D mOCTimaging was able to identify and quantify ECmorphology overlying various human cadaver coro-nary lesions. These results suggest that mOCT couldbe useful for improving our understanding of the roleof ECs in the pathogenesis of the diverse manifesta-tions of coronary artery disease.
Importantly, mOCT is a noncontact, 3D imagingtechnology that can ultimately be implemented incatheters to study ECs in living patients (4). 3D mOCTvisualization of ECs may allow a more precise capa-bility to predict plaque progression. Although theextent to which mOCT can visualize ECs beneaththrombus remains an open question, mOCT could alsobe helpful for making a more precise diagnosis ofcoronary “endothelial” erosion that has emerged asthe second most prevalent histopathological findingin acute coronary syndrome. The use of mOCT tech-nology to assess coronary stent strut endothelialcoverage may also help resolve current questions andcontroversies regarding stent healing and optimalantiplatelet therapy durations.
Kensuke Nishimiya, MD, PhDBiwei Yin, PhDZhonglie Piao, PhDJiheun Ryu, PhDHany Osman, MDHui Min Leung, PhDGargi Sharma, PhDChia Pin Liang, PhDJoseph A. Gardecki, PhDHui Zheng, PhDHiroaki Shimokawa, MD, PhDGuillermo J. Tearney, MD, PhD*

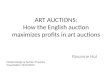
FIGURE 1 3D mOCT and SEM Images of Coronary Endothelial Cell Morphology
Intact: (+) EC pavementing Stripped: (-) EC pavementingy
x
3D-μOCT3D μOCT
3D-μOCT3D μOCT SEMSEM
3D-μOCT3D μOCT SEMSEM
Scale bars for top panels, 100 μm; middle and bottom panels, 25 μm
A
SwineCoronary
SwineCoronary
HumanFibrousPlaque
3D-μOCT3D μOCT
IntimalHyperplasia
(N = 26)
FibrousPlaque(N = 9)
FibrocalcificPlaque(N = 5)
Fibro-atheroma
(N = 5)
B
μOCT
RM
S (μ
m)
3D μOCT RMS (μm)
3D μOCT RMS (μm)
5.0
4.0
3.0
1.0
SEM
RM
S (μ
m)
2.0
Surface Roughness (Swine) Surface Roughness (Human)
R2 = 0.95p < 0.01
R2 = 0.97p < 0.01
2
2.5
3
2.5 3 3.5 4 4.5
15 intact sites
SEM
RM
S (μ
m)
18 stripped sites
0.5
1.5
2.5
0.5 1.5 2.5
(A) Three-dimensional (3D) micro-optical coherence tomography (mOCT) of an intact swine coronary artery showing endothelial cell (EC)
pavementing (top left panel). In contrast, a comparatively smooth surface is seen at the site of endothelial stripping (top right panel).
Endothelial pavementing of a swine coronary segment and human fibrous plaque visualized by 3D mOCT is similar to that seen by scanning
electron microscopy (SEM) (middle and bottom panels). Blood flow direction in the images of the swine coronary artery is depicted using
yellow arrows (middle panels), demonstrating an alignment of endothelial cells with flow. Scale bars, 100 mm (upper panels); 25 mm
(middle and bottom panels). (B) Scatter plots showing significant correlations between 3D mOCT and SEM root mean squared (RMS)
measurements in both 15 intact (left top graph) and 18 stripped sites (left bottom graph). Box plot of mOCT root mean squared for different
OCT-delineated coronary lesions (right). Statistical differences were examined using Wilcoxon signed rank test. Intimal hyperplasia root
mean squared (3.6 � 0.1 mm) was higher than that of fibrous plaque (3.0 � 0.2 mm) (p < 0.01), and both intimal hyperplasia and fibrous
plaque root mean squared were higher than those of fibrocalcific plaque (1.8 �0 .2 mm) and fibroatheroma (1.5 � 0.1 mm) (p < 0.01).
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 9 , 2 0 1 9 Letters to the EditorS E P T E M B E R 2 0 1 9 : 1 8 7 8 – 9 8
1879
Author's Personal Copy

FIGURE 1 Worseni
(1) Initial cardiac mag
arrows); (2) cardiac m
after restriction of e
Letters to the Editor J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . 1 2 , N O . 9 , 2 0 1 9
S E P T E M B E R 2 0 1 9 : 1 8 7 8 – 9 8
1880
Author's Personal Copy
*Department of PathologyHarvard Medical School and Massachusetts GeneralHospitalWellman Center for Photomedicine55 Fruit StreetBoston, Massachusetts 02114E-mail: [email protected]://doi.org/10.1016/j.jcmg.2019.01.021
© 2019 by the American College of Cardiology Foundation. Published by Elsevier.
Please note: Dr. Tearney has reported receiving catheter materials from TerumoCorporation, with which Massachusetts General Hospital has a licensingarrangement and from which he has the rights to receive royalties; has receivedsponsored research funding from Vivolight and Canon Inc.; has reported afinancial or fiduciary interest in SpectraWave, a company developing anOCT-Near Infrared Reflectance Spectroscopy intracoronary imaging system andcatheter; and has reported consulting for SpectraWave; his financial or fiduciaryinterest was reviewed and is managed by the Massachusetts General Hospitaland Partners HealthCare in accordance with their conflict of interest policies. Drs.Tearney and Gardecki are named inventors on OCT and mOCT patents. All otherauthors have reported that they have no relationships relevant to the contents ofthis paper to disclose.
RE F E RENCE S
1. Pasternak RC, Baughman KL, Fallon JT, et al. Scanning electron microscopyafter transluminal angioplasty of normal canine coronary arteries. Am J Car-diol 1980;45:591–8.
2. Liu L, Gardecki JA, Nadkarni SK, et al. Imaging the subcellular structure ofhuman coronary atherosclerosis using micro-optical coherence tomography.Nat Med 2011;17:1010–4.
3. Schneider CA, Rasband WS, Eliceiri KW. NIH Image to ImageJ: 25 years ofimage analysis. Nat Methods 2012;9:671–5.
4. Yin B, Hyun C, Gardecki JA, et al. Extended depth of focus for coherence-based cellular imaging. Optica 2017;4:959–65.
Exercise Is Good for the Heart But Not for
the Inflamed Pericardium?
Pericarditis is a condition that has the potential to beassociated with significant morbidity and mortality
ng LGE on CMR With Exercise
netic resonance with late gadolinium enhancement (LGE) of the pericardium
agnetic resonance after ongoing exercise during medical therapy with worse
xercise without changes in medical therapy and improved late gadolinium en
(1). Unfortunately, little is known about thenonpharmacological therapies of pericarditis that goalong with traditional anti-inflammatory treatment,particularly the role of exercise restriction. CurrentU.S. and European guidelines are geared more towardathletic populations and recommend exercise re-striction until there is resolution of inflammation onthe basis of clinical, laboratory, and echocardio-graphic data (2,3). However, these guidelines arelargely based on expert consensus without strongtrial evidence to back them up, and limiting exercisein active individuals may not be desirable. Mostexplanations of the pathophysiology of exercise-induced harm are just postulated theories, theadverse effects of exercise-induced tachycardia andshear stress on the pericardium leading to worseninginflammation, or increased blood flow to the peri-cardium secondary to inflammation and resultingoxidative stress from free radicals. Studies have alsoreported a relationship between pericarditis and ge-netic variations of the immune system that can pre-dispose people to worsening inflammation fromenvironmental triggers such as exercise (4).
Although we do not yet have a large, robustlyanalyzed patient series, in our substantial experience,some patients receiving medical therapy whocontinue to exercise seem to show worsening lategadolinium enhancement on cardiac magnetic reso-nance (Figure 1), and they have higher inflammatorymarkers such as C-reactive protein and erythrocytesedimentation rate. The late gadolinium enhance-ment and elevated inflammatory markers tend toimprove with exercise restriction, a finding that maysupport the theory of a proinflammatory role for
in a case of active pericarditis during anti-inflammatory therapy (red
ning late gadolinium enhancement; (3) cardiac magnetic resonance
hancement.