Embed Size (px)
Citation preview

Citation: Zaky A, Lang JD. Cardiac Dysfunction in Liver Transplantation. Austin J Anesthesia and Analgesia. 2014;2(1): 1007.
Austin J Anesthesia and Analgesia - Volume 2 Issue 1 - 2014ISSN : 2381-893X | www.austinpublishinggroup.orgZaky et al. © All rights are reserved
Austin Journal of Anesthesia and AnalgesiaOpen Access
Full Text Article
clinical background of cardiogenic shock as well as a biochemical picture characterized by distinctive elevation of serum lactate dehydrogenase and less of an elevation of serum bilirubin may help differentiate a primary hepatocellular etiology of cirrhosis from a secondary cardiogenic cause. Mechanistically, cardiac-induced hepatopathy is an extrahepatic post sinusoidal obstruction that impedes sinusoidal blood drainage leading to fibrosis. Cardiac-induced cirrhosis may also occur in left ventricular failure as a result of decreased forward flow to the liver leading to ischemicor hypoxic hepatitis.
Profiles of Cardiac Dysfunction in End Stage Liver Disease
Cirrhosis-aggravated cardiac disease
Coronary Artery Disease (CAD): The prevalence of CAD in patients with ESLD is equal to or greater than its prevalence in the general population, particularly among diabetics, with the range being between 2.5% to 27%, depending on the selection criteria. Reports on the impact of CAD on outcomes following liver transplantation have varied chronologically. A previous report by Plotkin [5]. Reported an overall mortality of 50% over a 1-3 year follow up period involving thirty two liver transplant recipients with angiographically-proven CAD. This high mortality rate occurred irrespective of the treatment modality for CAD. Interestingly, arecent multi-center cohort study by Wray [6] reported no significant differences in survival between liver transplant recipients with angiographically-proven obstructive CAD (≥50% stenosis) and those with non-obstructive CAD. Of intrigue, the obstructive coronary artery group demonstrated no statistically significant survival difference between patients with severe (>70% stenosis) and those with moderate CAD (50-70% stenosis). This apparent disagreement between the two studies can be explained by several factors. First, both studies reported on patients with coronary artery interventions prior to liver transplantation, but were not specifically designed to assess the effects of these interventions. Moreover, it could be that the significant improvement of management of coronary risk factors over the time between both studies may have contributed to the observed differences. Second, the study by Plotkin included only thirty two liver transplant candidates and did not include a control group. Third, the study by Wray suffered from several limitations including: the retrospective nature of the analysis leading to lack of adjustment for other covariates that affect survival, lack of adjustment for the interactions between centers and patient groups, lack of data on patients who underwent coronary interventions and did not undergo liver transplantation, and the risk of a classification bias based on co-classification of patients with non-obstructive CAD and normal coronaries as a single group. Taken together, more controlled studies are needed to assess the effects of different coronary interventions on the outcomes after liver transplantation.
Abbreviations
ESLD: End-Stage liver Disease; CAC: Cirrhosis-Associated Cardiomyopathy; POPH: Portopulmonary Hypertension; CAD: Coronary Artery Disease; INR: International Normalized Ratio; CABG: Coronary Artery Bypass Grafting
Introduction
The heart and the liver are mutually interactive organs both in health and disease [1]. For example, patients with chronic right heart failure may develop chronic congestive hepatopathy and cirrhosis, what has been previously termed, “cardiac cirrhosis” [2]. Conversely, patients with end-stage liver disease (ESLD) may develop a host of cardiovascular abnormalities[3]. The spectrum of heart diseases associated with liver cirrhosis includes 3 major groups:
1. Underlying heart disease aggravated by cirrhosis
2. Heart disease that is caused by a pathologic process that concomitantly affects the heart and the liver
3. Cirrhosis-associated cardiac disease, which may be vascular, myocardial or pericardial.
Liver transplantation is considered the definitive treatment of patients with ESLD. While considered a curative procedure, liver transplantationcan independently, contribute to further deterioration of pre-existing cirrhosis-associated cardiac dysfunction. These adverse effects occur as a result of acute changes in loading conditions, andthe liberation of inflammatory cytokines and other mediators during graft reperfusion [4]. Furthermore, following liver transplantation there is an increased risk of adverse cardiac events associated with chronic immunosuppressive therapy. Thus, patients such as these warrant a thorough cardiac evaluation prior to being deemed acceptable liver transplant candidates.
This review will discuss the following: profiles of cardiac dysfunction in ESLD with a specificfocus on coronary artery disease, and their preoperative evaluation and management.
It is important, though, to emphasize that cardiac failure may viciously precipitate liver failure. A temporal sequence of onset, a
Review Article
Cardiac Dysfunction in Liver TransplantationAhmed Zaky*, John D Lang
Department of Anesthesiology and Pain Medicine, University of Washington, USA
*Corresponding author: Ahmed Zaky, Department of Anesthesiology and Pain Medicine, VA Puget Sound Hospital/University of Washington, 1660 S Columbian way, Seattle, WA 98108, S-112-ANES, USA
Received: December 20, 2013; Accepted: January 03, 2014; Published: January 09, 2014
AustinPublishing Group
A

Austin J Anesthesia and Analgesia 2(1): id1007 (2014) - Page - 02
Zaky Austin Publishing Group
Submit your Manuscript | www.austinpublishinggroup.org
Risk stratification of patients with CAD undergoing liver transplantation
Multiple traditional and nontraditional cardiac risk factors have been identified in patients suffering from cirrhosis. Liver transplant candidates with more than one cardiac risk factor such as age>60, male gender, history of CAD, dyslipidemia, smoking, and diabetes has been associated with significant CAD [7]. Of these risk factors, diabetes mellitus (DM) has been specifically associated with asymptomatic coronary artery disease, with concomitant Type I DM, and CADassociated with 40% lower 5- year patient and graft survival rates [8]. Several non-traditional cardiac risk factors have been identified in patients with ESLD. In a recent retrospective case-control study, patients with non-alcoholic steatohepatitis (NASH) were more likely to be older, be morbidly obese, have hypertension, or have dyslipidemia compared with alcoholic cirrhosis. On multivariate analysis, NASH was associated with the development of a cardiovascular event (death from any cardiac cause, myocardial infarction, arrhythmias, stroke, cardiac arrest, and/or acute heart failure), independent of traditional risk cardiac risk, after liver transplantation [9], compared with patients with alcoholic cirrhosis. There were no significant differences between both groups in overall mortality, however. The association between NASH and traditional risk factors for CAD has been confirmed in other studies [10,11]. Prospective studies are needed to establish the role of NASH on cardiac-related events after liver transplantation. Multiple other nontraditional risk factors for CAD such as concomitant renal failure [12], elevated C-reactive protein [13], and intracoronary calcium [14] have been studied in patients with liver cirrhosis. The role of these factors as predictors versus as markers of cardiac-related morbidity and mortality remain to be investigated in larger studies.
Preoperative evaluation of patients with risk factors for CAD
The evaluation of cirrhosis patients with risk factors for CAD is a major clinical dilemma. This is because non-invasive cardiac testing has a low predictive value for angiographically-detectedobstructive CAD [15]. In addition, CAD that is caused by non-obstructive atherosclerotic plaques (<50% stenosis)which isnot detected by non-invasive testing, can be also responsible for acute coronary syndromes (unstable angina, myocardial infarction and sudden cardiac death) [16]. To further complicate issues, patients with myocardial perfusion defects and no angiographically-detected coronary lesions may succumb post-liver transplantation due to cardiovascular complications, primary graft failure and sepsis [17]. It is therefore crucial to exercise caution in interpreting a stress test in liver transplant candidates, even in the absence of angiographic evidence of coronary obstruction. To follow is a brief description of the diagnostic tests employed in the evaluation of liver transplant candidates with risk factors for CAD.
Stress testingThe most recent report from the American Heart Association
[18] recommends performing a non-invasive cardiac stress test on patients with ESLD with >3 risk factors for CAD (age >60, diabetes, hypertension, left ventricular hypertrophy, history of CAD, smoking and dyslipidemia), regardless of functional status. Patients with proven ischemia on stress testing are then referred for coronary angiography todefinitively evaluate their coronary anatomy.
Stress testing describes the physical or pharmacologically-induced increase in myocardial oxygen demand to uncover areas of critically obstructed coronary artery disease. Ischemic myocardial areas manifest either as wall motion abnormalities detected by echocardiography or perfusion defects detected by radionuclidemyocardial perfusion scans. Pharmacologic stress may be induced by dobutamine, an inotrope, and a chronotrope or by coronary vasodilators such as adenosine ordipyridamole. The latter produces a ‘coronary steal’ from areas of coronary obstruction to areas of normal reactive coronary anatomy and hence precipitates ischemia. The more significant the coronary artery obstruction, the more predictive the stress test. Stress testing however, cannot identify non-obstructingatherosclerotic plaques even if they are morphologically vulnerable to rupture. Of stress tests currently being utilized, dobutamine stress echocardiography (DSE) has been the most studied.
Dobutamine stress echocardiography hasproduced inconclusive results in a large percentage of liver transplant candidates because of the inability to achieve predicted target heart rates or heart rate blood pressure product that are high enough to induce wall motion abnormalities. This physiologic limitation is attributed to failure of beta receptors to respond to sympathetic stimulation, a condition termed chronotropic incompetence [19]. Reports on the accuracy of DSE varied widely among studies as a result of the variability in patient selection criteria to perform DSE and end points used for its evaluation. In a retrospective study [15] of 105 patients with end-stage liver disease who underwent both DSE and coronary angiography, Harinstein et al. reported a low sensitivity (13%) and
Preoperative cardiac evaluation
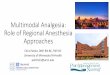
2-3 coronary risk factors
Dobutamine stress echocardiogram
Positive for ischemia
Negative for ischemia
Significant obstructive CAD
(>50%)
Coronary angiography
No significant obstructive
CAD
Proceed with OLT Consider revascularization versus
Synchronous CABG/OLT
Figure 1: Schematic diagram of preoperative evaluation of patients with CAD undergoing, OLT.CAD; coronary artery disease; OLT; orthotopic liver transplantation; CABG: coronary artery bypass grafting

Austin J Anesthesia and Analgesia 2(1): id1007 (2014) - Page - 03
Zaky Austin Publishing Group
Submit your Manuscript | www.austinpublishinggroup.org
intermediate negative predictive value (75%) for the detection of angiography-proven obstructive CAD. Interestingly, the specificity and positive predictive values of DSE increased significantly with the increase in the number of risk factors for CAD. A recent single-centered retrospective study [20] of 400 liver transplant candidates reported a fairly high NPV (89%) and a low sensitivity (14%) of preoperative DSE in predicting 30-day post-liver transplantation cardiac events (death/nonfatal myocardial infarctions). Of interest, none of the traditional risk factors for CAD were shown to predict the study outcomes on multivariate analysis. Furthermore, patients in these patients had low Model for End Stage Liver Disease (MELD) scores. The strong NPV of preoperative DSE for myocardial injury post-liver transplantation was confirmed in another retrospective study [21]. Taken together, a conclusively negative DSE (lack of wall motion abnormalities on reaching 85% of predicted heart rate response after dobutamine injection) in patients with low cardiac risk may reliably rule out ischemia or the development of cardiac events post-liver transplantation. A positive test on the other hand, may not necessarily be associated with these outcomes.
Assessment of myocardial perfusion using intravenous ultrasound contrast agents during real-time myocardial stress echocardiography (RTMSE) has been introduced for the assessment and prediction of cardiac events in patients with advanced liver disease. This technique, by combining wall motion abnormalities with perfusion defects is theorized to be a more sensitive measure of myocardial ischemia than DSE. In addition, adding a contrast agent to echocardiography improves image resolution and endocardial border detection,and thusovercomes 2 of the major limitations of DSE [22]. Tsutsui [23]. examined for the first time the prognostic power of myocardial perfusion imaging with RTMSE in patients undergoing OLT. An abnormal myocardial perfusion imaging was shown to be an independent predictor of in-hospital and 2-year mortality. Interestingly, adjusting for myocardial perfusion, wall motion abnormalities lost predicative value, denoting the higher predictive power of perfusion compared to wall motion abnormalities. Despite its appeal, myocardial perfusion with RTMSE needs to be further studied before being used routinely in liver transplant candidates.
Reports on myocardial perfusion stress testing in the form of nuclear single-photon emission computed tomography (SPECT) with the injection of vasodilators such as adenosine or dipyridamoleare conflicting and inconclusive [24-26]. One explanation for these conflicting results is the failure of adenosine or dipyridamole in achieving coronary vasodilation due to the underlying systemic vasodilation in advanced liver disease.
Coronary calcificationCalcium commonly deposits on coronary atherosclerotic
plaques. Thus, the degree of plaque calcification can be used to assess the severity of coronary obstruction, and hence the propensity of developing cardiac events after liver transplantation. Computerized tomography is used to measure coronary calcification and the amount of cardiac calcium detected is fit into scores that take into account the age and gender. Calcium scores can thus grade the severity of CAD. Cardiac calcium scores have a limited predictive value as a single screening test for CAD [27] . Cardiac calcium scoring may provide additive information to other CAD risk factors for the occurrence
of cardiac events (death, myocardial infarction or revascularization) [28]. It is also of value as a strong negative test; where cardiac calcium scores of zero are associated with < 50% coronary artery stenosis [29]. A recent study of 101 patients with ESLD showed a strong relationship between cardiac calciumscore and multiple specific cardiac risk factors (age, systolic blood pressure, fasting glucose levels, some elements of metabolic syndrome). In this study, the cardiac calcium score revealed a high prevalence of asymptomatic CAD in patients undergoing assessment for liver transplantation [14]. Taken together, the role of calcium cardiac score is auxiliary at best. More studies are needed to explore its role in the prediction of cardiac events in patients with end stage liver disease.
Coronary angiography
Coronary angiography can be performed despite coagulopathy, although at the price of increased risks of bleeding and contrast-induced nephropathy [30,31]. Sharma and colleagues [31] investigated the safely of cardiac catheterization in patients awaiting liver transplantation and compared them with matched controls with normal liver function. Patients in the study group had a significantly elevated serum creatinine, lower hemoglobin levels and higher international normalized ratios (INR) compared with matched controls. Compared with controls, the study group had a significantly higher rate of vascular complications, transfusions and major bleedings [31]. A trans-radial approach to coronary angiography has been suggested as a potential approach to decrease bleeding complications in ESLD patients [32]. Also, cardiac CT angiography is emerging as a non-invasive alternative to coronary angiography for the assessment of CAD in patients with ESLD [33]. However, more studies are needed to establish its role in pre-transplant evaluation.
Aspects of treatment of liver transplant candidates with cardiac risk factors
There is no current consensus on what gradeof coronary lesion requires intervention and what intervention might be the most useful in patients with ESLD. Coronary revascularization should be considered in liver transplant candidates when the lack of revascularization presents a prohibitive risk factor for liver transplantation. Available options are: medical management, percutanoeus revascularization and coronary artery bypass grafting (CABG).
Medical management
Aspirin in the doses used for cardiovascular protection may affect platelet function and worsen thrombocytopenia commonly occurring in patients with ESLD [34]. The use of angiotensin converting enzyme inhibitors and angiotensin receptor blockers may worsen renal function in patients with ESLD especially those suffering from hepatorenal syndrome, as well as worsening the systemic vasodilation characteristic of ESLD [35].
The use of statins has raised concerns of worsening liver function [36]. Recent data, however suggest their safety in patients with advanced liver disease provided there is adequate monitoring of liver function [37]. Some concerns have arisen regarding reports of severe rhabdomyolysis with the concomitant use of statins and some anti-rejection medications that inhibit hepatic cytochrome p450 enzyme [38]. Adequately powered randomized trials are needed regarding the safety of the use of statins in ESLD patients.

Austin J Anesthesia and Analgesia 2(1): id1007 (2014) - Page - 04
Zaky Austin Publishing Group
Submit your Manuscript | www.austinpublishinggroup.org
Beta blockers have been shown to be protective against the occurrence of cardiac events post-liver transplantation. A recent observational study has shown a protective role of beta blockers in cardiac patients with ESLD[20].Non-selective beta blockers are of proven benefit in ESLD patients with esophageal varices [39]. However, more trials are needed to determine the dosage and timing of initiation of beta blockersas cardio-protective agents in liver transplant candidates.
Percutanoeus revascularizationThere is a tendency to favor the use of baremetal stents (BMS) over
drug-eluting stents (DES) to limit the duration of dual antiplatelet therapy in the form of aspirin and clopidogrel in the setting of coagulopathy frequently encountered in patients with ESLD. This however may curtail the beneficial effects of DES especially in situations when the risk of restenosis from BMS is deemed to be too high; patients with diabetes, complex lesions (bifurcations and left main), long lesions in small caliber vessels and the treatment of in-stent restenosis [40].
Coronary Artery Bypass Grafting (CABG)
CABG surgery is associated with significant morbidity and mortality in patients with ESLD compared with those without ESLD. Early reports suggest a mortality of 30-40% and morbidity of up to 70-100% [41]. Studies have consistently shown a proportionately high mortality and morbidity (including but not limited to: ascites, cardiac tamponade, pleural effusion, bleeding, and encephalopathy) with worsening Child and MELD classification in patients undergoing CABG prior to liver transplantation [42-45]. A ‘cut-off’ Child score >7 was found to have a sensitivity and specificity of 86 % and 92%, respectively for mortality with a PPV and NPV of 67% and 97%, respectively in some studies. Some studies have reported less mortality with off pump CABG (OPCAB) in patients with advanced Child classification [46]. Several pre- and intraoperative predictors of morbidity and mortality were identified in ESLD patients undergoing CABG; low platelet counts, higher MELD scores, lower serum cholinesterase levels, cardiopulmonary bypass time, and aortic cross clamp time [47]. Taken together, lower cirrhosis severity scores are associated with lower morbidity and mortality compared with more advanced scores. In the latter group of patients, OPCAB may be offered, however at the expense of an elevated risk of mortality and morbidity.
Combined CABG and liver transplantation has been scarcely reported in the literature. In a case series of patients with severe triple vessel diseaseand ESLD, there were no intraoperative deaths. At 25-months of follow up, there was an 80% graft- and patient-survival (one patient died of recurrent Hepatitis C). Overall average length of staywas 21 days [48].
Cardiac surgery can be performed after liver transplantation with an acceptable risk [49]. In a case series of 15 liver transplant recipients who underwent cardiac surgery, there were no early deaths, no rejection episodes, or increase in wound infection rates. At a mean of 26.5 months of follow up, 13.3% had died, and 255 developed recurrent angina [49].
Systemic Diseases Affecting the Heart and the Liver Alcoholic Heart and Muscle Disease
Reported incidences of alcoholic cardiomyopathy range from 21% to 32% of dilated cardiomyopathy in surveys conducted at referral centers [50]. Heavy alcohol drinking (> 90 g/d) may lead to cardiac structural abnormalities such as: increased myocyte apoptotic cell death, decreased calcium sensitivity, and decreased myofibril function, and myocardial fibrosis [51-53].
Clinical features
The clinical symptoms and signs are similar to heart failure due to other causes. Echocardiographic findings include: decreased ejection fraction, impaired mean fractional shortening, increased left ventricular mass, increase left atrial dimensions, all manifesting as impaired both systolic and diastolic function. In advanced cases, echocardiography shows: 4-chamber dilatation, normal or decreased left ventricular wall thickness. Supraventricular arrhythmias are common in alcoholic cardiomyopathy. Causes of death are progressive chronic heart failure and sudden cardiac death [53].
Treatment
Abstinence from alcohol in the early stages may lead to significant improvement of left ventricular ejection fraction [54]. The treatment of alcoholic cardiomyopathy is similar to heart failure of other etiologies. End stage heart failure is an indication for cardiac transplantation. Unfortunately, alcohol relapses are common [55].
Cirrhosis-associated Cardiac DiseasesCirrhosis-associated Cardiomyopathy (CAC)
Cirrhosis-associated cardiomyopathy (CAC) describes cardiac
Cardiac dysfunction in patients suffering fromcirrhosis characterized by impaired contractile responsiveness to stress and/or altered diastolic relaxation with associated electrophysiological abnormalities in the absence of other known cardiac disease.
Diagnostic criteria:
Systolic dysfunction
• Blunted increase in cardiac output with exercise, volume challenge or pharmacological stimuli
• Resting EF <55%
Diastolic dysfunction
• E/A < 1• Prolonged deceleration time (> 200 msec)• Prolonged isovolumetric relaxation time (< 80 msec)
Supportive criteria
• Electrophysiological abnormalities• Chronotropic incompetence• Electromechanical uncoupling• Prolonged QTc interval• Enlarged left atrium• Increased myocardial mass• Increased BNP, pro-BNP• Increased Troponin I
Table 1 :WorkingDefinitionofCirrhosis-associatedCardiomyopathy[100].

Austin J Anesthesia and Analgesia 2(1): id1007 (2014) - Page - 05
Zaky Austin Publishing Group
Submit your Manuscript | www.austinpublishinggroup.org
dysfunction in patients with cirrhosis characterized by impaired contractile responsiveness to stress and/or altered diastolic function with electrophysiologic abnormalities in the absence of other known cardiac disease [56]. This syndrome is seen in approximately 40-50% of adult patients with cirrhosis [56]. The clinical manifestations of this syndrome correlate with the severity of cirrhosis [57].
Clinical characterization of cirrhosis-associated cardiomyopathy Cardiac dysfunction resulting from cirrhosis encompass: systolic dysfunction, diastolic dysfunction, and electrophysiological dysfunction (Table 1). Systolic dysfunction. According to the current working definition of cirrhosis-associated cardiomyopathy, systolic dysfunction describes a contractile defect that is uncovered by stress. The high resting cardiac output and lower filling pressures encountered in patients with cirrhosis is partially explained by low systemic vascular resistance and increased arterial compliance [3]. Physical exercise, however, is associated with a significant elevation of left ventricular filling pressures and a relatively smaller increase in cardiac output, ejection fraction and heart rate [58]. A less than optimal exercise-induced increase in ejection fraction in the presence of an exercise-induced lowering of afterload is a sign of left ventricular contractile dysfunction. Recently, cardiac magnetic resonance imaging (CMRI) and advanced echocardiography technologies have uncovered more of the subtleties of CAC. As assessed by CMRI, there is a modest increase in left ventricular mass, left ventricular end-diastolic and left atrial volumes [59]. A recent echocardiographic study using tissue Doppler imaging [60] revealed a significant increase in left ventricular end-diastolic diameter and a reduction in peak systolic velocity and systolic strain rate. Peak left ventricular systolic velocity and strain measured by tissue Doppler are considered more sensitive indices of left ventricular contractile function than the ejection fraction and cardiac index [61]. This is because these markers are more indicative of the more vulnerable longitudinally-arranged subendocardial fibers [61]. These findings strongly suggest resting structural and contractile changes in patients with cirrhosis that are not included in the current definition. Reduced systolic function may have prognostic implications such as the development of ascites and renal dysfunction [56].
Taken together, evidence exists demonstrating that contractile dysfunction in cirrhosis takes place under resting conditions and that it has prognostic implications.
Diastolic dysfunction
Diastolic dysfunction is a prominent feature of CAC. This describes impairment of ventricular filling as a result of alterations in the receptive ventricular properties.
The underlying mechanism of diastolic dysfunction in cirrhosis is increased myocardial wall stiffness most likely due to myocardial hypertrophy, fibrosis and sub-endothelial edema [3] resulting in high filling pressures of the left ventricle and atrium and ultimately increasing the risk of pulmonary edema because of the backward failure.
Normally, the velocity of early rapid ventricular filling (denoted by E) is greater than the late filling phase that is dependent on atrial contraction (denoted by A) [62]. Therefore, E/A less than 1 may denote impaired ventricular relaxation. A low E/A, however, is highly
preload-sensitive. The American Society of Echocardiography has included tissue Doppler imaging criteria in the diagnosis of diastolic dysfunction [63]. Doppler tissue imaging measures the slow velocity high amplitude annular tissue motion (denoted by E’’) which is less affected by preload. An increase in the E’/E ratio has been used as a more sensitive measure of diastolic dysfunction [64].
Electrophysiological dysfunction
Electrophysiological dysfunction includes: prolonged QT interval, chronotropic incompetence and electromechanical dissociation. QT interval prolongation adjusted for heart rate (QTc) is found in approximately 50% of patients with cirrhosis [65]. It has been shown to be significantly related to the severity of liver disease, plasma norepinephrine levels, and the presence of portal hypertension [66]. Prolonged QT interval was independently associated with the risk of sudden death in cirrhosis, although the latter is relatively uncommon [65]. The most likely underlying mechanism is dysfunctional potassium channels prolonging the duration of action potential and QT interval [67]. Studies on the dispersion of QT interval (i.e., difference between the longest and shortest interval) report a normally maintained diurnal variation in patients with liver cirrhosis [68]. A recent retrospective study reported that prolonged QTc (>463 msec) independently predicted mortality from gastrointestinal bleeding [69]. Beta receptor blockade seems to restore a normal QT interval in some individuals [70]. Also, prolonged QTc is partly reversible by liver transplantation, despite being prolonged during the early phase of transplantation [71]
Chronotropic incompetence refers to the inability of the heart rate to respond to physiologic and pharmacologic demands such as exercise, head tilt, inotropes, and a higher than normal increase in plasma norepinephrine concentrations. The inability to increase the heart rate in response to demands may partially explain reduced cardiac output under these conditions. The time between the onset of electrical and mechanical systole is normally tightly controlled and is referred to as electromechanical coupling. A defect in electromechanical coupling leads to the dyssynchrony between electrical and mechanical systole. Bernardi [72] demonstrated prolongation of pre-ejection phase at rest, together with defective shortening with exercise in patients with cirrhosis denoting a defect in electromechanical coupling.
Aspects of treatment
To date, there are no clinical trials on the management of CAC.
Table2:DefinitionofPortopulmonaryHypertensionClinical evidence of portal hypertension, and:
MPAP>25mmHgatrestor>30mmHgonexercisePVR > 240 dynes.sec.cm-5
PCWP<15mmHgorTPG>12mmHgMPAP: mean pulmonary artery pressure, PVR: pulmonary vascular resistance, PCWP: pulmonary capillary wedge pressure
PAP: pulmonary artery pressure
Table3:ClassificationofPortopulmonaryHypertension
Severity Mean PAP (mm Hg)
Mild >25and<35
Moderate >35and<45
Severe ≥45

Austin J Anesthesia and Analgesia 2(1): id1007 (2014) - Page - 06
Zaky Austin Publishing Group
Submit your Manuscript | www.austinpublishinggroup.org
Patients in heart failure should be treated following guidelines for non-cirrhosis induced cardiac failure. Noteworthy, the use of afterload reducers may not be well-tolerated given the widespread and progressive vasodilation characteristic of cirrhosis. Short courses of non-selective beta blockers were shown to restore prolonged QT intervals towards normal [70]. No recommendation, however, for the chronic use of beta blockers can be made at the present time. Cardiac glycosides are less effective inotropes. A potential role for the aldosterone antagonist, K-canrenoate exists to reverse the RAAS-induced myocardial fibrosis in pre-ascitic cirrhosis [73]. Despite the theoretic appeal, more studies are needed to further explore this approach. Liver transplantation is associated with a recovery of CAC.
Portopulmonary Hypertension (POPH)Portopulmonary hypertension is a form of pulmonary arterial
hypertension (PAH) with increased pulmonary vascular resistance (PVR) or trans-pulmonary gradient (TPG) due to vasoconstriction and pulmonary vascular remodeling, all occurring in the setting of a clinical evidence of portal hypertension [74] (Tables 2, 3). It should be emphasized that portal hypertension is in itself associated with a hyperdynamic circulation, sodium retention and volume overload, all can cause PAH with normal TPG and PVR, and hence not classified as POPH. Portopulmonary hypertension is present in about 5% -10% of liver transplant candidates [75]. Approximately 5% of liver transplant candidates have moderate to severe PAH(mean pulmonary artery pressuremPAP- >35 mmHg), which has been considered a contraindication to OLT [76]. A preoperative mPAP 35 -50 mmHg has been associated with a 50% risk of mortality after liver transplantation [77]. AnmPAP of > 50 has been associated with nearly 100% mortality [77]. It is to be emphasized that right ventricular function is more important prognostically than absolute pulmonary artery values, since right ventricular function is the most important criterion in determining the likelihood of a successful graft [78]. Patients severe POPH may undergo combined heart-lung transplantation.
Diagnostic evaluation
Transthoracic echocardiography (TTE)
TTE with Doppler estimation of pulmonary artery systolic pressure (PASP) is the screening tool of choice for the detection of POPH [79]. An elevated PASP > 30 mmHg is suggestive of pulmonary hypertension. Additional finding on echocardiography include an enlarged or dilated right ventricle and evidence of right ventricular strain.
The accuracy of an echocardiography derived PASP of > 30 mmHg as a threshold cut-off for the diagnosis of POPH was associated with a sensitivity and specificity of 100 and 96%, respectively, among 165 liver transplant candidates. PPV and NPV at this cut off were 59% and 100%, respectively [80]. PASP is determined based on an estimate of right atrial pressure and peak tricuspid regurgitation velocity using the modified Bernoulli equation.
Given the low PPV and the poor correlation between TTE and catheterization values, all patients with echocardiographic findings suggestive of pulmonary hypertension should be referred to right cardiac catheterization for definitive diagnosis.
Right heart catheterization
Right heart catheterization is considered the gold standard for the diagnosis of POPH. It is important to rule out elevated PAP due to elevated left atrial pressures or to elevated cardiac output associated with ESLD. Measurement of the TPG is often used to achieve such a differentiation [81]. Also, a trial of diuresis can be given if PAOP is >15 mmHg with subsequent measurement of mPAP. If mPAP is > 35 mmHg, PVR > 3 Woods Units and PAOP < 15 mmHg, then mild POPH is diagnosed [82].
Radiologic studies
Chest radiography and computed tomography may show signs of right ventricular enlargement. Chest CT may also show increased pulmonary artery diameter, and increased segmental artery to bronchial ratios in multiple pulmonary lobes [81].
Electrocardiography
Signs of right heart strain, right axis deviation, right bundle branch block and first degree atrio-ventriuclar block may be seen [83].
Treatment Pulmonary vasodilators have been used in moderate and severe
POPH (mPAP> 35 mmHg) to lower mPAP and hence facilitate liver transplantation [84]. There is a paucity of randomized trials on the use of specific pulmonary vasodilators in patients with POPH. The current treatment centers on the use of prostanoids, endothelin antagonists and phosphodiesterase V inhibitors. Prostanoids induce pulmonary vasodilation and inhibit platelet aggregation leading to an increased risk of bleeding and systemic hypotension, respectively. Comparatively, they are more studied compared with other pulmonary vasodilators. They are very potent drugs that can be given by intravenous infusion or by inhalation. Some of the side effects include headaches, flushing, tachycardia and more importantly high output failure and mean pulmonary artery pressure as a result of the precipitous systemic vasodilation. In this particular case right heart catheterization may be indicated to differentiate whether increased pulmonary vascular resistance accompanies the increase in mean pulmonary artery pressure or it is simply resulting from elevated cardiac output. Endothelin antagonists inhibit the endothelin-1-induced vasoconstriction and vascular remodeling.Bosenten, an oral dual endothelin receptor antagonist, carries an FDA caution against its use in patients with moderate to severe liver dysfunction or elevated transaminases. Multiple reports have shown improvement in hemodynamics, exercise capacity with Bosentan with up to 3-fold increase in serum transaminases greater than the upper level of normal that responded to dose reduction or discontinuation [85, 86]. Endothelinanatagonists should be used with caution in patients with ESLD and post transplantation given their potential hepatotoxc effects unrevealed by the small series of patients in which they were studied. Phosphodiesterase V inhibitors such as sildenafil enhance nitric oxide-mediated vasodilation. They have been used successfully in small studies in variable doses [87]. Overall, given the paucity of evidence, pulmonary vasodilators should be used with caution in liver transplant candidates.
Liver transplantation may [88] or may not [89] reverse POHP.

Austin J Anesthesia and Analgesia 2(1): id1007 (2014) - Page - 07
Zaky Austin Publishing Group
Submit your Manuscript | www.austinpublishinggroup.org
Interestingly, there have been recent reports of de novo pulmonary hypertension post OLT. Unfortunately, this syndrome is associated with high mortality with no pre-operative clinical predictors for its development [90].
Pericardial disease
Fluid retention characteristic of ESLD frequently leads to ascites, pleural and pericardial effusions, of which the latter may be associated with cardiac tamponade. The diagnosis of cardiac tamponademay be challenging in patients with cirrhosis. This is because elevated right sided pressures may mask or delay right ventricular (and/or atrial) collapse despite the presence of underlying tamponade physiology [91]. Significant effusions should be treated by pericardiocentesis or pericardial window, and patients should be followed up by echocardiography.
Preoperative evaluation of liver transplant candidates: Current stance and future directions. The current literature lacks a definitive preoperative strategy that optimized perioperative outcomes in liver transplant candidates. This stems from the lack of randomized controlled trials investigating the utility of preoperative testing in high-risk liver transplant candidates. Additionally, there is a lack of consensus on what are risk factors that are associated with postoperative cardiac dysfunction. Adding to the difficulty, the literature is inconclusive on what constitutes a cardiac morbidity post OLT, eat alone the contribution of preoperative risk factors. Moreover, it yet remains to be proven whether new onset cardiac morbidities (secondary to immunosuppression, as an example) are really ‘new-onset’ versus ‘newly-diagnosed’. It is therefore understandable why the current guidelines for preoperative evaluation of liver transplant candidates do not stand on solid evidence-based recommendations. To follow are some examples of the current literature on cardiac testing in liver transplant candidates.
In a retrospective study Ripoll [92]observed that patients who developed an abnormal cardiac response defined by a coupled reduction in left ventricular stroke work index with an elevation of filling pressures to be more likely to be hyponatremic, and centrally hypovolemic. An abnormal cardiac response occurred most commonly after reperfusion and was associated with prolonged intubation. Although adding to the notion that an abnormal cardiac response may occur in the absence of an abnormal preoperative echocardiographic cardiac testing, this is study is criticized for being single centered, retrospective, lacking a control group, using non conventional limits for statistical significance, and the use of preload determined marker of left ventricular systolic dysfunction. In the absence of a baseline testing of what the author defined as an abnormal cardiac response, it is uncertain whether the attained response is exclusively due to ESLD. Another retrospective report [93] commented on intraoperative and 6-months postoperative cardiac morbidity. Cardiac morbidity was defined as pulmonary edema, arrhythmia, ischemia, pulmonary hypertension, and heart failure. Using multivariate regression analysis, the authors concluded that a highintegrated MELD score, occurrence of intraoperative cardiac complications, preoperative history of cardiac disease were all independent predictors of poor cardiac outcomes. Interestingly, serum sodium shown to be associated with worse outcomes in Ripoll’s study was not shown to be associated with poor outcome in
this study. This study is criticized based on its retrospective nature, lack of a control group, missing patient data, not reporting on the diagnostic modality used to determine baseline cardiac dysfunction, of only adjusting for age and gender in the multivariate regression model, and in not reporting baseline characteristics co-morbidities of the study cohort. Based on these limitations, firm conclusions on specific preoperative cardiac predictors are hard to be generalized.
Given the above-mentioned inherent limitations of dobutamine stress echocardiography in the preoperative evaluation of liver transplant candidates, it is not surprising that its use has produced mixed results. Umphry [94] reported that a failure to attain a heart rate greater than 82% of predicted and a maximum rate pressure product of 63.33 to be predictive of poor intra and postoperative cardiac outcomes. On the other hand, Findlay [21] reported more disappointing results by demonstrating failure of a positive preoperative dobutamine stress echocardiogram to predict cardiac morbidity in the form of myocardial injury. Again both studies suffer from the above-mentioned limitations of being retrospective and of reporting different definitions of cardiac outcomes at different time points in a small sample sized population. Therefore, there is a need for a standardized preoperative approach for risk stratifying liver transplant candidates and that this approach be prospectively tested.
Future directions
There has been a recent interest in identifying cardiac dysfunction at a subclinical level. Advanced echocardiographic techniques and magnetic resonance imaging are now gaining more popularity in detecting early mechanical dysfunction of the myocardium that is not detected by conventional echocardiographic techniques such as the ejection fraction.
Contrast magnetic resonance imaging has been shown to be superior than echocardiography in detecting smaller size perfusion defects not manifesting as wall motion abnormalities by echocardiography [95]. This is theorized to be due to a better detection of the extent of perfusion in the longitudinally arrangedsubendocardial fibers that are more prone to ischemia compared with circularly and radially arranged fibers.
In an interesting exploratory study, Reddy [96] demonstrated feasibility of what they called on-stop shop for cardiac, abdominal and vascular MRI in liver transplant candidates. More studies are needed to investigate the influence on outcomes of various techniques of cardiac MRI in the preoperative cardiac evaluation of liver transplant candidates.
One potential modality to detect subtle myocardial dysfunction in ESLD is to study the regional deformation of the left ventricle along different planes of motion. In this regard, the present assessment could be achieved by measuring strain and strain rate using advanced echocardiographic techniques, such as Doppler tissue imaging and speckle tracking echocardiography. Strain measures segmental myocardial deformation and strain rate measures the rate at which this deformation occurs [97]. Measuring strain across the longitudinal plane of motion has been shown to be a more sensitive measure of ischemia, fibrosis and hypertrophy compared to more global indicators of left ventricular systolic function, such as ejection fraction [97]. This is, in part, due to the arrangement of the more

Austin J Anesthesia and Analgesia 2(1): id1007 (2014) - Page - 08
Zaky Austin Publishing Group
Submit your Manuscript | www.austinpublishinggroup.org
vulnerable subendocardial fibers of the left ventricle across this plane of motion. Doppler tissue imaging used to measure myocardial velocities is angle-dependent and cannot be performed in retrospect. Speckle tracking imaging creates reflections and interferences between the ultrasound beam and the myocardial tissue ‘speckles’ that can be tracked retrospectively throughout the cardiac cycle and is angle-independent [98]. In a recent study in a pediatric population with septic shock, speckle tracking imaging modality was able to detect impaired myocardial performance that was not revealed by EF measurement [99]. Speckle tracking echocardiography may thus be a modality to explore in the preoperative evaluation of liver transplant candidates.
ConclusionThe heart and liver are mutually interactive organs. The current
pre-liver transplant work up does not stem from a solid evidence. As a remedy, standardized definitions of risk profiles and cardiac morbidities should be prospectively investigated both short and long term. This standardization should go in line with the quest of newer modalities capable of diagnosing cardiac dysfunction at an early stage. The involvement of a multidisciplinary team of caregivers is a key to the success of this approach.References1. Ripoll C, Yotti R, Bermejo J, Bañares R. The heart in liver transplantation.
JHepatol.2011;54:810-822.
2. Kotin, P. andE.M.Hall. “Cardiac” or congestive cirrhosis of liver. Am JPathol. 1951; 27: 561-71.
3. Moller, S. and J.H. Henriksen. Cardiovascular dysfunction in cirrhosis.Pathophysiological evidence of a cirrhotic cardiomyopathy. Scand J Gastroenterol.2001;36:785-94.
4. Arranz J, Soriano A, Garcia I, García I, Concepción MT, et al. Effect of proinflammatory cytokines (IL-6, TNF-alpha, IL-1beta) on hemodynamicperformanceduringorthotopiclivertransplantation.TransplantProc.2003;35:1884-1887.
5. Plotkin JS, Scott VL, Pinna A, Dobsch BP, De Wolf AM, et al. Morbidity and mortality in patients with coronary artery disease undergoing orthotopic livertransplantation.LiverTransplSurg.1996;2:426-430.
6. Wray C, Scovotti JC, Tobis J, Niemann CU, Planinsic R, et al. Liver Transplantation Outcome in Patients With Angiographically Proven Coronary Artery Disease: A Multi-Institutional Study. Am J Transplant. 2013;13:184-191.
7. Tiukinhoy-Laing SD, Rossi JS, Bayram M, De Luca L, Gafoor S, et al. Cardiac hemodynamic and coronary angiographic characteristics of patients being evaluated for liver transplantation. Am J Cardiol. 2006; 98: 178-181.
8. Yoo,H.Y,P.J.Thuluvath.Theeffectofinsulin-dependentdiabetesmellituson outcome of liver transplantation. Transplantation. 2002; 74: 1007-1012.
9. VanwagnerLB,BhaveM,TeHS,FeinglassJ,AlvarezL,etal.Patientstransplanted for nonalcoholic steatohepatitis are at increased risk for postoperativecardiovascularevents.Hepatology.2012;56:1741-1750.
10. Targher G, Bertolini L, Padovani R, Rodella S, Zoppini G, et al., Prevalence of non-alcoholic fatty liver disease and its association with cardiovascular diseaseinpatientswithtype1diabetes.JHepatol.2010;53:713-718.
11. Targher, G, G. Arcaro. Non-alcoholic fatty liver disease and increased risk ofcardiovasculardisease.Atherosclerosis.2007;191:235-240.
12. Cholongitas E, Senzolo M, Patch D, Shaw S, O’Beirne J, et al. Cirrhotics admitted to intensive care unit: the impact of acute renal failure on mortality. EurJGastroenterolHepatol.2009;21:744-750.
13. Shimada K, Fujita M, Tanaka A, Yoshida K, Jisso S, et al. Elevated serum C-reactive protein levels predict cardiovascular events in the Japanese coronaryarterydisease(JCAD)study.CircJ.2009;73:78-85.
14. McAvoyNC, KocharN,McKillopG,NewbyDE,HayesPC. Prevalenceof coronary artery calcification in patients undergoing assessment fororthotopiclivertransplantation.LiverTranspl.2008;14:1725-1731.
15. Harinstein ME, Flaherty JD, Ansari AH, Robin J, Davidson CJ, et al.Predictive value of dobutamine stress echocardiography for coronary artery disease detection in liver transplant candidates. Am J Transplant. 2008; 8: 1523-1528.
16. Rubin DA, Schulman DS, Edwards TD, Starzl TE, Curtiss EI. Myocardial ischemiaafterorthotopiclivertransplantation.AmJCardiol.1994;74:53-56.
17. Guckelberger O, Byram A, Klupp J, Neumann UP, Glanemann M, et al. Coronary event rates in liver transplant recipients reflect the increasedprevalence of cardiovascular risk-factors. Transpl Int. 2005; 18: 967-974.
18. Lentine KL, Costa SP, Weir MR, Robb JF, Fleisher LA, et al. Cardiac disease evaluation and management among kidney and liver transplantation candidates: a scientific statement from the American Heart Associationand the American College of Cardiology Foundation. J Am Coll Cardiol. 2012;60:434-480.
19. Lee, S.S. Cardiac abnormalities in liver cirrhosis. West J Med. 1989; 151: 530-535.
20. SafadiA,HomsiM,MaskounW,LaneKA,SinghI,etal.Perioperativeriskpredictors of cardiac outcomes in patients undergoing liver transplantation surgery. Circulation. 2009; 120: 1189-1194.
21. Findlay JY, Keegan MT, Pellikka PP, Rosen CB, Plevak DJ. Preoperative dobutamine stress echocardiography, intraoperative events, and intraoperative myocardial injury in liver transplantation. Transplant Proc. 2005;37:2209-2213.
22. Marwick, T.H. Contrast stress echocardiography: completing the picturefrom image enhancement to improved accuracy and prognostic insight. Circulation.2005;112:1382-1383.
23. Tsutsui JM, Mukherjee S, Elhendy A, Xie F, Lyden ER. Value of dobutamine stress myocardial contrast perfusion echocardiography in patients with advanced liver disease. Liver Transpl. 2006; 12: 592-599.
24. Davidson CJ, Gheorghiade M, Flaherty JD, Elliot MD, Reddy SP, et al. Predictive value of stress myocardial perfusion imaging in liver transplant candidates.AmJCardiol.2002;89:359-360.
25. Aydinalp A, Bal U, Atar I, Ertan C, AktaÅŸ A, et al. Value of stress myocardial perfusion scanning in diagnosis of severe coronary artery disease in liver transplantationcandidates.TransplantProc.2009;41:3757-3760.
26. ZoghbiGJ,PatelAD,ErshadiRE,HeoJ,BynonJS,etal.Usefulnessofpreoperative stress perfusion imaging in predicting prognosis after liver transplantation.AmJCardiol.2003;92:1066-1071.
27. Taylor AJ, Burke AP, O’Malley PG, Farb A, Malcom GT, et al. A comparison of the Framingham risk index, coronary artery calcification, and culpritplaquemorphologyinsuddencardiacdeath.Circulation.2000;101:1243-1248.
28. KondosGT,HoffJA,SevrukovA,DaviglusML,GarsideDB,etal.Electron-beamtomographycoronaryarterycalciumandcardiacevents:a37-monthfollow-up of 5635 initially asymptomatic low- to intermediate-risk adults.Circulation.2003;107:2571-2576.
29. Cheng VY, Lepor NE, Madyoon H, Eshaghian S, Naraghi AL, et al.Presence and severity of noncalcified coronary plaque on 64-slicecomputed tomographic coronary angiography in patients with zero and low coronaryarterycalcium.AmJCardiol.2007;99:1183-1186.
30. MacDonald LA, Beohar N, Wang NC, Nee L, Chandwaney R, et al. A comparison of arterial closure devices to manual compression in liver transplantation candidates undergoing coronary angiography. J Invasive Cardiol.2003;15:68-70.

Austin J Anesthesia and Analgesia 2(1): id1007 (2014) - Page - 09
Zaky Austin Publishing Group
Submit your Manuscript | www.austinpublishinggroup.org
31. Sharma M, Yong C, Majure D, Zellner C, Roberts JP, Bass NM, et al. Safety of cardiac catheterization in patients with end-stage liver disease awaitinglivertransplantation.AmJCardiol.2009;103:742-746.
32. Rao SV, Cohen MG, Kandzari DE, Bertrand OF, Gilchrist IC.The transradial approach to percutaneous coronary intervention: historical perspective, current concepts, and future directions. J Am Coll Cardiol. 2010; 55: 2187-2195.
33. Coronary multidetector computed tomographic angiography to evaluate coronary artery disease in liver transplant candidates: methods, feasibility and initial experience. et al. Coronary multidetector computed tomographic angiography to evaluate coronary artery disease in liver transplant candidates: methods, feasibility and initial experience. J Cardiovasc Med (Hagerstown).2011;12:460-8.
34. Menguy R, Desbaillets L, Okabe S, Masters YF . Abnormal aspirin metabolism in patients with cirrhosis and its possible relationship to bleeding in cirrhotics. Ann Surg. 1972; 176: 412-418.
35. LeeJK,HsiehJF,TsaiSC,HoYJ,KaoCH.Effectsofsingledoseof50mgcaptoprilinpatientswithlivercirrhosisandascites.Hepatogastroenterology.2000; 47: 767-770.
36. Clarke AT, Mills PR . Atorvastatin associated liver disease. Dig Liver Dis. 2006;38:772-777.
37. Zachoval R, Gerbes AL, Schwandt P, Parhofer KG . Short-term effects of statin therapy in patients with hyperlipoproteinemia after liver transplantation:resultsofarandomizedcross-overtrial.JHepatol.2001;35:86-91.
38. Dopazo C, Bilbao I, Lázaro JL, Sapisochin G, Caralt M . Severe rhabdomyolysis and acute renal failure secondary to concomitant use of simvastatin with rapamycin plus tacrolimus in liver transplant patient. Transplant Proc. 2009; 41: 1021-1024.
39. Garcia-Tsao G, Sanyal AJ, Grace ND, Carey W; Practice Guidelines Committee of the American Association for the Study of Liver Diseases; Practice Parameters Committee of the American College of Gastroenterology . Prevention and management of gastroesophageal varicesandvaricealhemorrhageincirrhosis.Hepatology.2007;46:922-938.
40. Ehtisham J, Altieri M, Salamé E, Saloux E, Ollivier I . Coronary artery disease in orthotopic liver transplantation: pretransplant assessment and management. Liver Transpl. 2010; 16: 550-557.
41. Bizouarn P, Ausseur A, Desseigne P, Le Teurnier Y, Nougarede B . Early and late outcome after elective cardiac surgery in patients with cirrhosis. AnnThoracSurg.1999;67:1334-1338.
42. An Y, Xiao YB, Zhong QJ. Open-heart surgery in patients with liver cirrhosis. Open-heartsurgeryinpatientswithlivercirrhosis.2007;31:1094-1098.
43. SugimuraY,ToyamaM,KatohM,KatoY,HisamotoK.Analysisofopenheart surgery in patients with liver cirrhosis. Asian Cardiovasc Thorac Ann. 2012;20:263-268.
44. Filsoufi F, Salzberg SP, Rahmanian PB, Schiano TD, ElsiesyH . Earlyand late outcome of cardiac surgery in patients with liver cirrhosis. Liver Transpl.2007;13:990-995.
45. MorisakiA,HosonoM,SasakiY,KuboS,HiraiH .Risk factoranalysisin patients with liver cirrhosis undergoing cardiovascular operations. Ann Thorac Surg. 2010; 89: 811-817.
46. Hayashida N, Shoujima T, TeshimaH, Yokokura Y, Takagi K . Clinicaloutcome after cardiac operations in patients with cirrhosis. Ann Thorac Surg. 2004; 77: 500-505.
47. Suman A, Barnes DS, Zein NN, Levinthal GN, Connor JT . Predicting outcome after cardiac surgery in patients with cirrhosis: a comparison of Child-PughandMELDscores.ClinGastroenterolHepatol.2004;2:719-723.
48. AxelrodD, Koffron A, Dewolf A, Baker A, Fryer J . Safety and efficacyof combined orthotopic liver transplantation and coronary artery bypass grafting.LiverTranspl.2004;10:1386-1390.
49. Prabhakar G, Testa G, Abbasoglu O, Jeyarajah DR, Goldstein RM . The safety of cardiac operations in the liver transplant recipient. Ann Thorac Surg. 1998; 65: 1060-1064.
50. ReganTJ.Alcoholandthecardiovascularsystem.JAMA.1990;264:377-381.
51. Capasso JM, Li P, Guideri G, Malhotra A, Cortese R . Myocardial mechanical, biochemical, and structural alterations induced by chronic ethanolingestioninrats.CircRes.1992;71:346-356.
52. Delbridge LM, Connell PJ, Harris PJ, Morgan TO . Ethanol effects oncardiomyocyte contractility. Clin Sci (Lond). 2000; 98: 401-407.
53. Fauchier L, Babuty D, Poret P, Casset-Senon D, Autret ML . Comparison of long-term outcome of alcoholic and idiopathic dilated cardiomyopathy. Eur HeartJ.2000;21:306-314.
54. La Vecchia LL, Bedogni F, Bozzola L, Bevilacqua P, Ometto R . Prediction of recovery after abstinence in alcoholic cardiomyopathy: role of hemodynamic and morphometric parameters. Clin Cardiol. 1996; 19: 45-50.
55. Dew MA, DiMartini AF, Steel J, De Vito Dabbs A, Myaskovsky L . Meta-analysis of risk for relapse to substance use after transplantation of the liver or other solid organs. Liver Transpl. 2008; 14: 159-172.
56. MøllerS,HenriksenJH .Cirrhoticcardiomyopathy.JHepatol.2010;53:179-190.
57. LiuH,GaskariSA,LeeSS .Cardiacandvascularchanges incirrhosis:pathogenicmechanisms.WorldJGastroenterol.2006;12:837-842.
58. Wong F, Girgrah N, Graba J, Allidina Y, Liu P . The cardiac response to exercise in cirrhosis. Gut. 2001; 49: 268-275.
59. Møller S, Søndergaard L, Møgelvang J, Henriksen O, HenriksenJH.Decreasedrightheartbloodvolumedeterminedbymagneticresonanceimaging:evidenceofcentralunderfillingincirrhosis.Hepatology.1995;22:472-478.
60. Merli M, Calicchia A, Ruffa A, Pellicori P, Riggio O . Cardiac dysfunction in cirrhosis is not associated with the severity of liver disease. Eur J Intern Med.2013;24:172-176.
61. KazankovK,Holland-FischerP,AndersenNH,TorpP,SlothE.Restingmyocardialdysfunction incirrhosisquantifiedby tissueDoppler imaging.LiverInt.2011;31:534-540.
62. Garcia MJ1, Thomas JD, Klein AL . New Doppler echocardiographic applications for the study of diastolic function. J Am Coll Cardiol. 1998; 32:865-875.
63. Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK . Recommendations for the evaluation of left ventricular diastolic function by echocardiography.EurJEchocardiogr.2009;10:165-193.
64. Mahadevan G, Dwivedi G, Williams L, Steeds RP, Frenneaux M . Epidemiology and diagnosis of heart failure with preserved left ventricular ejectionfraction:rationaleanddesignofthestudy.EurJHeartFail.2012;14: 106-112.
65. Bernardi M, Maggioli C, Dibra V, Zaccherini G . QT interval prolongation in liver cirrhosis: innocent bystander or serious threat? Expert Rev GastroenterolHepatol.2012;6:57-66.
66. Bernardi M, Calandra S, Colantoni A, Trevisani F, Raimondo ML . Q-T interval prolongation in cirrhosis: prevalence, relationship with severity, andetiologyofthediseaseandpossiblepathogeneticfactors.Hepatology.1998;27:28-34.
67. Genovesi S, Prata Pizzala DM, Pozzi M, Ratti L, Milanese M . QT interval prolongation and decreased heart rate variability in cirrhotic patients: relevance of hepatic venous pressure gradient and serum calcium. Clin Sci (Lond). 2009; 116: 851-859.
68. HansenS,MøllerS,BendtsenF,JensenG,HenriksenJH.Diurnalvariationand dispersion in QT interval in cirrhosis: relation to haemodynamic changes.JHepatol.2007;47:373-380.

Austin J Anesthesia and Analgesia 2(1): id1007 (2014) - Page - 010
Zaky Austin Publishing Group
Submit your Manuscript | www.austinpublishinggroup.org
69. Trevisani F, Di Micoli A, Zambruni A, Biselli M, Santi V . QT interval prolongation by acute gastrointestinal bleeding in patients with cirrhosis. LiverInt.2012;32:1510-1515.
70. Henriksen JH, Bendtsen F, Hansen EF, Møller S . Acute non-selectivebeta-adrenergic blockade reduces prolonged frequency-adjusted Q-T interval(QTc)inpatientswithcirrhosis.JHepatol.2004;40:239-246.
71. ShinWJ,KimYK,SongJG,KimSH,ChoiSS.AlterationsinQTintervalin patients undergoing living donor liver transplantation. Transplant Proc. 2011;43:170-173.
72. Bernardi M, Trevisani F, Santini C, Zoli G, Baraldini M, Ligabue A. Plasma norepinephrine, weak neurotransmitters, and renin activity during active tilting in liver cirrhosis: relationship with cardiovascular homeostasis and renalfunction.Hepatology.1983;3:56-64.
73. Pozzi M, Grassi G, Ratti L, Favini G, Dell’Oro R . Cardiac, neuroadrenergic, and portal hemodynamic effects of prolonged aldosterone blockade in postviral child A cirrhosis. Am J Gastroenterol. 2005; 100: 1110-1116.
74. Swanson KL, Krowka MJ . Screen for portopulmonary hypertension, especially in liver transplant candidates. Cleve Clin J Med. 2008; 75: 121-122,125-30,133passim.
75. Kuo PC, Plotkin JS, Gaine S, Schroeder RA, Rustgi VK . Portopulmonary hypertension and the liver transplant candidate. Transplantation. 1999; 67: 1087-1093.
76. SwansonKL,WiesnerRH,NybergSL,RosenCB,KrowkaMJ.Survivalin portopulmonary hypertension: Mayo Clinic experience categorized by treatmentsubgroups.AmJTransplant.2008;8:2445-2453.
77. Martínez-Palli G, Taurà P, Balust J, Beltrán J, Zavala E . Liver transplantation in high-risk patients: hepatopulmonary syndrome and portopulmonary hypertension.TransplantProc.2005;37:3861-3864.
78. Ramsay MA . Portopulmonary hypertension and hepatopulmonary syndrome, and liver transplantation. Int Anesthesiol Clin. 2006; 44: 69-82.
79. Rodríguez-RoisinR, KrowkaMJ,HervéP, FallonMB;ERSTask ForcePulmonary-Hepatic Vascular Disorders (PHD) Scientific Committee .Pulmonary-HepaticvascularDisorders(PHD).EurRespirJ.2004;24:861-880.
80. Torregrosa M, Genesca J, Gonzalez A, Evangelista A, Mora A . Role of Doppler echocardiography in the assessment of portopulmonary hypertension in liver transplantation candidates. Transplantation. 2001; 71: 572-574.
81. Mukhtar NA, Fix OK . Portopulmonary hypertension. J Clin Gastroenterol. 2011;45:703-710.
82. RavalZ,HarinsteinME,SkaroAI,ErdoganA,DeWolfAM.Cardiovascularrisk assessment of the liver transplant candidate. J Am Coll Cardiol. 2011; 58:223-231.
83. KuoPC,PlotkinJS,JohnsonLB,HowellCD,LaurinJM.Distinctiveclinicalfeatures of portopulmonary hypertension. Chest. 1997; 112: 980-986.
84. Porres-Aguilar M, Zuckerman MJ, Figueroa-Casas JB, Krowka MJ . Portopulmonaryhypertension:stateoftheart.AnnHepatol.2008;7:321-330.
85. HalankM,MiehlkeS,HoeffkenG,SchmeisserA,SchulzeM.Useoforal
endothelin-receptor antagonist bosentan in the treatment of portopulmonary hypertension. Transplantation. 2004; 77: 1775-1776.
86. Kuntzen C, Gülberg V, Gerbes AL . Use of a mixed endothelin receptor antagonist in portopulmonary hypertension: a safe and effective therapy? Gastroenterology. 2005; 128: 164-168.
87. CaddenIS,GreanyaED,ErbSR,ScudamoreCH,YoshidaEM.Theuseofsildenafiltotreatportopulmonaryhypertensionpriortolivertransplantation.AnnHepatol.2009;8:158-161.
88. Sugimachi K, Soejima Y, Morita K, Ueda S, Fukuhara T . Rapid normalization of portopulmonary hypertension after living donor liver transplantation. Transplant Proc. 2009; 41: 1976-1978.
89. UmedaN,KamathPS.Hepatopulmonarysyndromeandportopulmonaryhypertension.HepatolRes.2009;39:1020-1022.
90. Koch DG, Caplan M, Reuben A . Pulmonary hypertension after liver transplantation: case presentation and review of the literature. Liver Transpl. 2009; 15: 407-412.
91. AkinciSB,GaineSP,PostW,MerritWT,TanHP.Cardiactamponadeinan orthotopic liver recipient with pulmonary hypertension. Crit Care Med. 2002;30:699-701.
92. Ripoll C, Catalina MV, Yotti R, Olmedilla L, Pérez-Peña J . Cardiac dysfunction during liver transplantation: incidence and preoperative predictors. Transplantation. 2008; 85: 1766-1772.
93. Fouad TR, Abdel-Razek WM, Burak KW, Bain VG, Lee SS . Prediction of cardiac complications after liver transplantation. Transplantation. 2009; 87: 763-770.
94. Umphrey LG, Hurst RT, Eleid MF, Lee KS, Reuss CS, Hentz JG, etal. Preoperative dobutamine stress echocardiographic findings andsubsequent short-term adverse cardiac events after orthotopic liver transplantation. Liver Transpl. 2008; 14: 886-92.
95. Kim RJ, Wu E, Rafael A, Chen EL, Parker MA . The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction.NEnglJMed.2000;343:1445-1453.
96. Reddy ST, Thai NL, Fakhri AA, Oliva J, Tom KB . Exploratory use of cardiovascular magnetic resonance imaging in liver transplantation: a one-stopshopforpreoperativecardiohepaticevaluation.Transplantation.2013;96:827-833.
97. Sanderson JE, Fraser AG . Systolic dysfunction in heart failure with a normal ejection fraction: echo-Doppler measurements. Prog Cardiovasc Dis. 2006; 49: 196-206.
98. Helle-ValleT,CrosbyJ,EdvardsenT,LyseggenE,AmundsenBH,SmithHJ, et al. New noninvasive method for assessment of left ventricularrotation:speckletrackingechocardiography.Circulation2005;112:3149-3156.
99. Basu S, Frank LH, Fenton KE, Sable CA, Levy RJ, Berger JT. Two-dimensional speckle tracking imaging detects impaired myocardial performance in children with septic shock, not recognized by conventional echocardiography.PediatrCritCareMed.2011;13:259-264.
100. Moller,S.andJ.H.Henriksen,Cirrhoticcardiomyopathy.JHepatol.2010;53:179-190.
Citation: Zaky A, Lang JD. Cardiac Dysfunction in Liver Transplantation. Austin J Anesthesia and Analgesia. 2014;2(1): 1007.
Austin J Anesthesia and Analgesia - Volume 2 Issue 1 - 2014ISSN : 2381-893X | www.austinpublishinggroup.orgZaky et al. © All rights are reserved