Embed Size (px)
DESCRIPTION
CMS National Dry Run: Risk-Standardized Payment Measure: Acute Myocardial Infarction 30-day Episode of Care. August 13, 2013. Agenda. Introductions ( next) Purpose of Dry Run and Measure Proposed Implementation Dry R un Overview Measure Details Resources Questions and Answers. - PowerPoint PPT Presentation
Citation preview
August 13, 2013
CMS National Dry Run:Risk-Standardized Payment
Measure: Acute Myocardial Infarction
30-day Episode of Care
2
• Introductions (next)
• Purpose of Dry Run and Measure
• Proposed Implementation
• Dry Run Overview
• Measure Details
• Resources
• Questions and Answers
Agenda
3
• Centers for Medicare & Medicaid Services (CMS)
• Yale New Haven Health Services Corporation – Center for Outcomes Research and Evaluation (CORE)
• Mathematica Policy Research (MPR)
Introductions
4
• Introductions
• Purpose of Dry Run and Measure (next)
• Proposed Implementation
• Dry Run Overview
• Measure Details
• Resources
• Questions and Answers
Agenda
5
• Educate hospitals about new measures
• Provide hospitals with results and data
• Help hospitals interpret results and data
• Encourage hospitals to ask questions
Purpose of Dry Run
6
• Cost: the amount incurred in providing services
• Payment: the amount paid on behalf of a Medicare patient for health care services
• Risk-standardized payment: an amount that has been modified to make payments comparable across hospitals
Defining Common Terms
7
• Inpatient hospitalizations contribute to rising healthcare costs1, 2
• Payments reflect costs from Medicare’s perspective
• Variations in care patterns affect payments made by CMS
• Payments reported in conjunction with outcome quality measures, such as AMI mortality, will illuminate high-value care
1. Health Care Cost Institute, 2010; 2. Jha AK, et. al., Health Affairs, 2009
Why report a payment measure?
8
• AMI is a common and expensive condition among Medicare beneficiaries
• AMI episode requires care in hospital and post-discharge
• There is substantial variation in payments • In hospital practice patterns• Post-discharge care
Why measure payment for an acute myocardial infarction (AMI) episode?
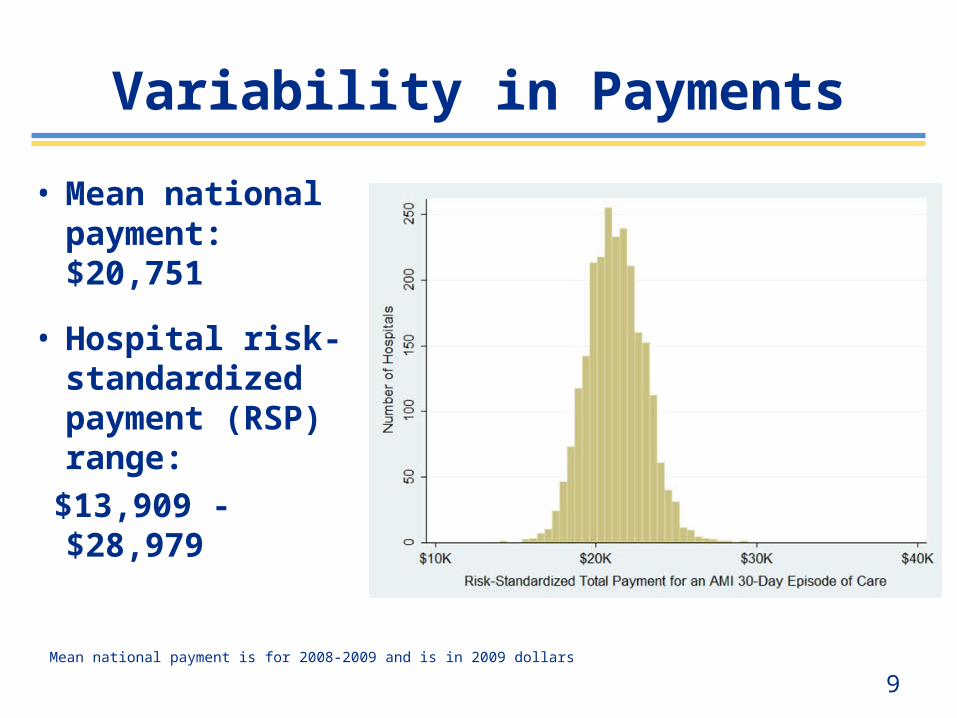
9Mean national payment is for 2008-2009 and is in 2009 dollars
• Mean national payment: $20,751
• Hospital risk-standardized payment (RSP) range:
$13,909 - $28,979
Variability in Payments
10
• Making care more affordable is a priority within the National Quality Strategy (NQS) and CMS Quality Strategy
• In response to the NQS, CMS is analyzing efficiency. Currently measures exist in the following programs:• Hospital Inpatient Quality Reporting Program• Hospital Value-Based Purchasing Program• Hospital Outpatient Quality Reporting Program• Physician Value-Based Modifier Program
• Support efforts to make payments and quality more transparent to consumers and providers
Addressing Affordable Care
11
• Introductions
• Purpose of Dry Run and Measure
• Proposed Implementation (next)
• Dry Run Overview
• Measure Details
• Resources
• Questions and Answers
Agenda
12
• In the IPPS FY 2014 Final Rule, CMS added the AMI payment measure to the Inpatient Quality Reporting (IQR) program
• If finalized, CMS will publicly report the measure results on Hospital Compare
Proposed Implementation
13
• Introductions
• Purpose of Dry Run and Measure
• Proposed Implementation
• Dry Run Overview (next)
• Measure Details
• Resources
• Questions and Answers
Agenda
14
• Timeline: August 5 – September 4, 2013
• Access to Hospital-Specific Reports• QualityNet
• Results:• Hospital-Specific Report (HSR)• Measure Information and Instructions Report
• Resources:• Methodology reports, FAQs, other materials• [email protected]
Dry Run Overview
15
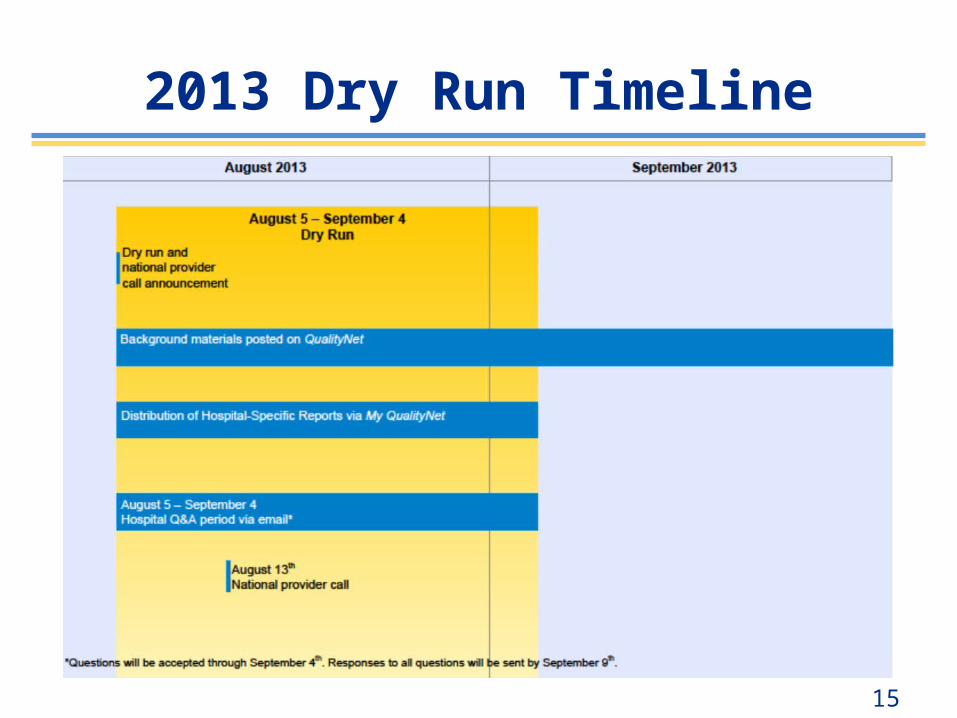
2013 Dry Run Timeline
16
• Introductions
• Purpose of Dry Run and Measure
• Dry Run Overview
• Measure Details (next)
• Proposed Implementation
• Resources
• Questions and Answers
Agenda
17
• Home health agency• Non-institutional providers (e.g., physicians and independent labs)• Durable medical equipment
• Inpatient• Skilled nursing facility• Outpatient• Hospice
• Hospital-level, risk-standardized payments for an AMI episode of care
• Admission to 30 days post-admission
• Includes payments for the index admission and post-discharge settings, including:
Measure Design
18
• Chronic Condition Warehouse (CCW) Data• Medicare administrative claims data
• 100% of patients with a primary discharge diagnosis of AMI
• Why use CCW?• Can follow patients across multiple care settings using a
unique patient identifier
Data Source
19
• Non-federal short-term acute care hospitals• Critical access hospitals (CAH) are included
• Dry run includes patients: • Discharged in 2008-2009 • ≥65 years of age• Principal discharge diagnosis of AMI (defined by
ICD-9 codes 410.xx, excluding 410.x2)• Randomly select one index admission per patient
for patients with multiple admissions
Inclusion Criteria
20
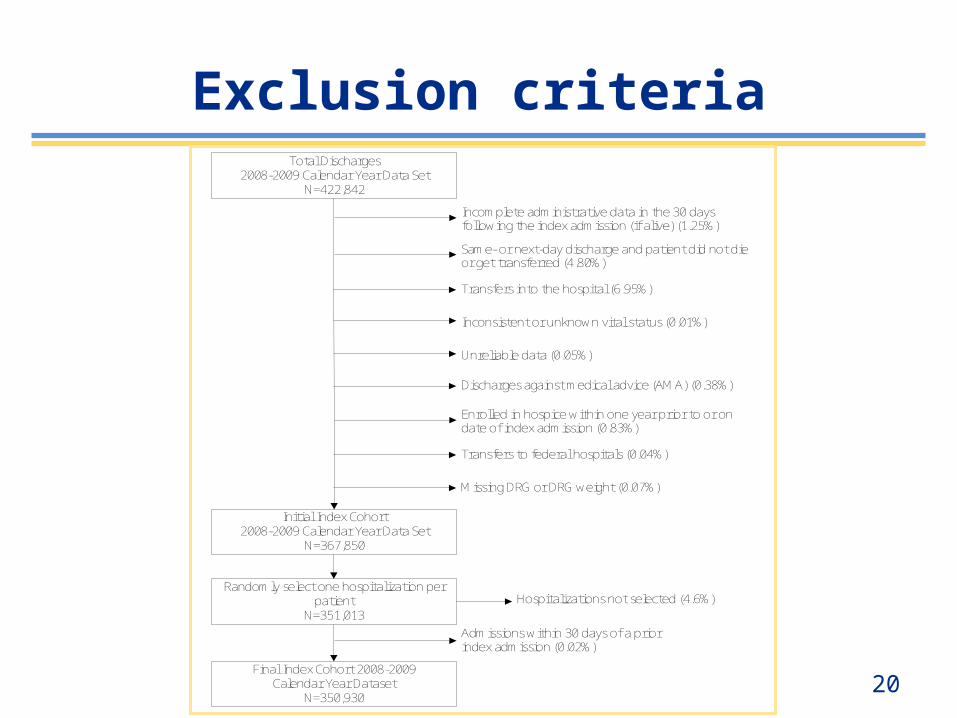
Enrolled in hospice within one year prior to or on date of index admission (0.83%)
Incomplete administrative data in the 30 days following the index admission (if alive) (1.25%)
Same- or next-day discharge and patient did not die or get transferred (4.80%)
Transfers into the hospital (6.95%)
Inconsistent or unknown vital status (0.01%)
Unreliable data (0.05%)
Discharges against medical advice (AMA) (0.38%)
Admissions within 30 days of a prior index admission (0.02%)
Transfers to federal hospitals (0.04%)
Initial Index Cohort 2008-2009 Calendar Year Data Set
N=367,850
Randomly select one hospitalization per patient
N=351,013Hospitalizations not selected (4.6%)
Final Index Cohort 2008-2009 Calendar Year Dataset
N=350,930
Total Discharges 2008-2009 Calendar Year Data Set
N=422,842
Missing DRG or DRG weight (0.07%)
Exclusion criteria
21
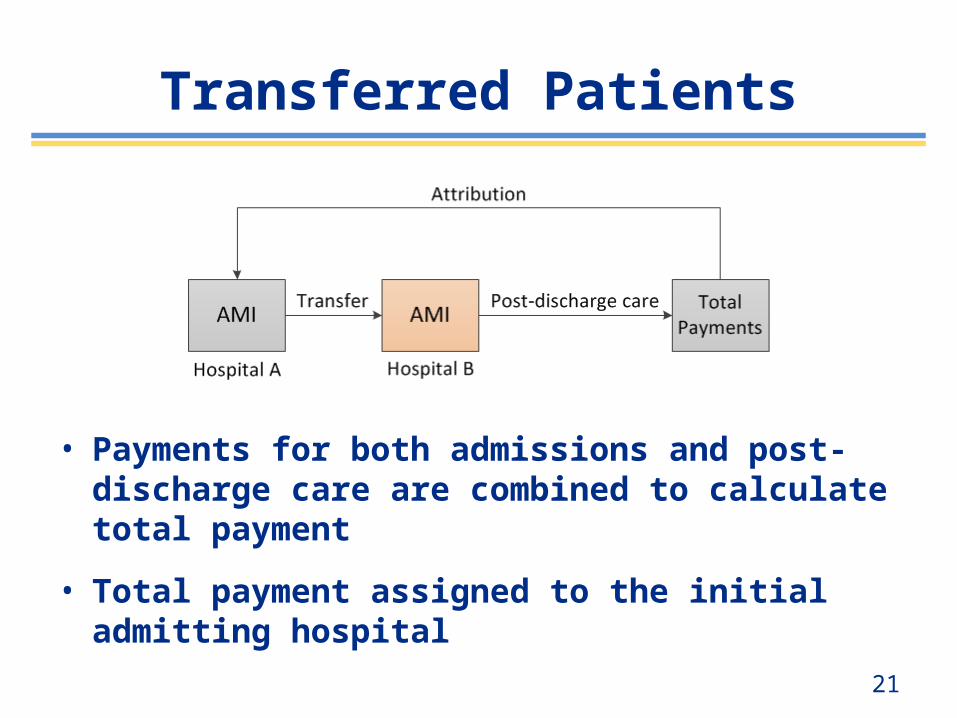
• Payments for both admissions and post-discharge care are combined to calculate total payment
• Total payment assigned to the initial admitting hospital
Transferred Patients
22
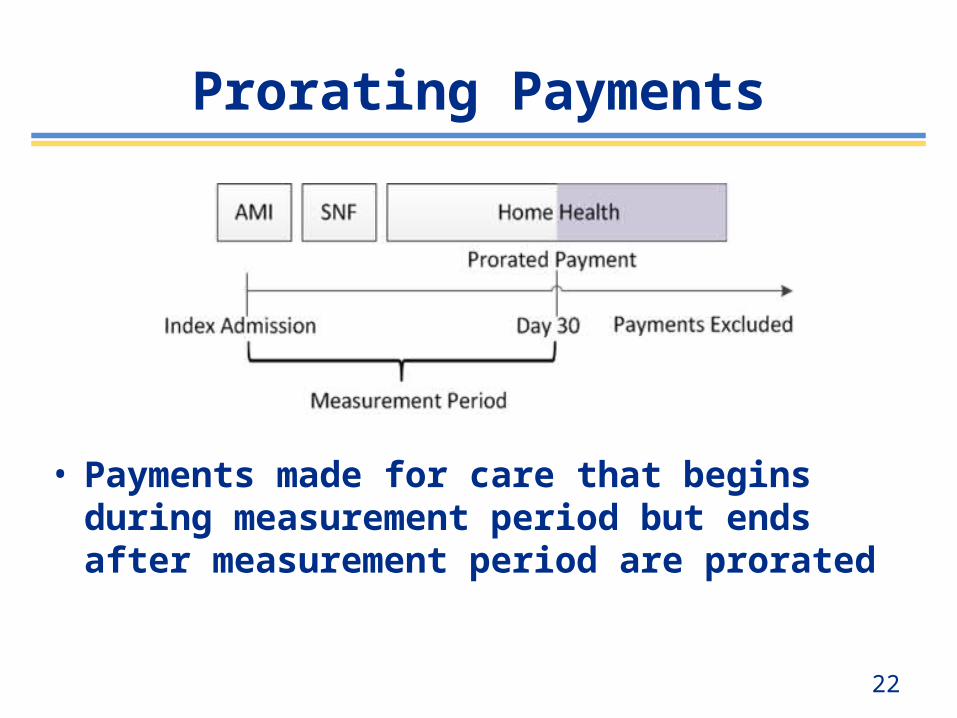
• Payments made for care that begins during measurement period but ends after measurement period are prorated
Prorating Payments
23
• Includes payments from admission to 30 days post-admission
• Incorporates claims from across all care settings
• Removes or averages payment adjustments unrelated to care• Geography (wage index, cost of living)• Policy adjustments (IME, DSH, etc.)
Payment Calculation
24
• Goal is to assess payments influenced by clinical decisions
• Payment adjustments such as wage index are unrelated to clinical decisions/practice patterns of care
• Using actual payments would not allow for a fair comparison across hospitals
Removing Payment Adjustments
25
• To isolate differences in payments that reflect practice patterns, the measure estimates payments by:
• Stripping: • Removing geographic adjustments• Removing policy adjustments
• Standardizing: • Average payments across geographic areas
when geographic differences cannot be removed
Removing Payment Adjustments: Stripping/Standardizing
26
• Accounts for differences in patient characteristics and comorbidities across hospitals
• Includes:• Secondary diagnosis codes from index admission
(except for potential complications of care)• All diagnosis codes from previous year from:
• acute inpatient hospital stays• hospital outpatient care• physician, radiology, and laboratory services
Risk Adjustment
27
• Calculating risk-standardized payment (RSP)
Risk-Standardized Payments
28
• Categories of measure results:• Less than U.S. average national payment
• No different than U.S. average national payment
• Greater than U.S. average national payment
• Number of cases too small (<25 cases)
• Final RSP reported with interval estimate
Categorizing Hospital Results
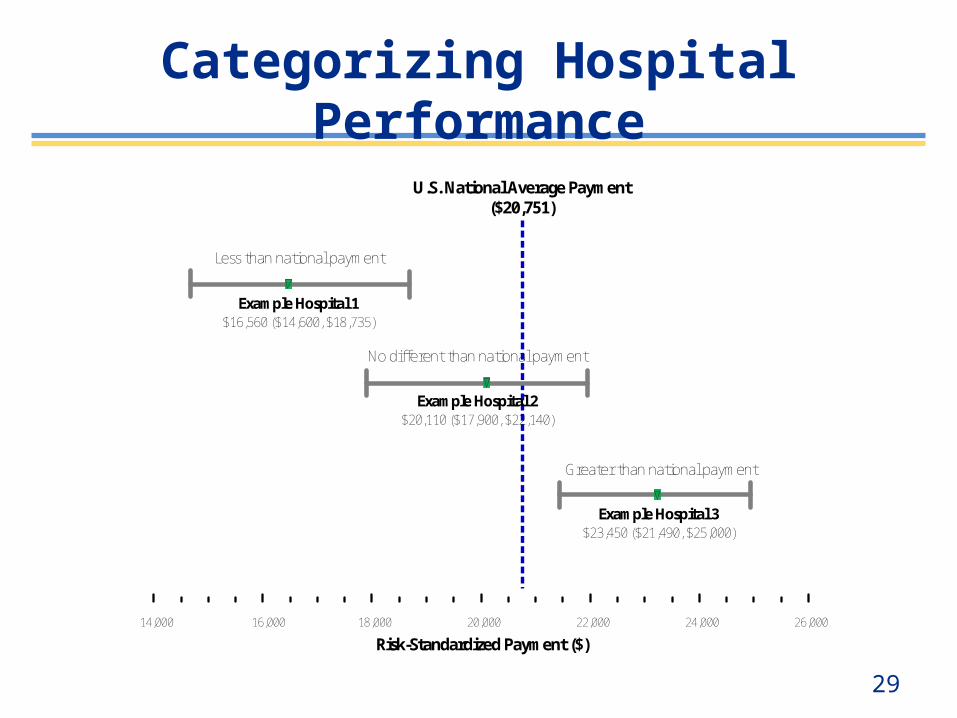
29
Risk-Standardized Payment ($)
U.S. National Average Payment($20,751)
Less than national payment
Example Hospital 1$16,560 ($14,600, $18,735)
Example Hospital 2$20,110 ($17,900, $22,140)
Greater than national payment
Example Hospital 3$23,450 ($21,490, $25,000)
No different than national payment
14,000 16,000 18,000 20,000 22,000 24,000 26,000
Categorizing Hospital Performance
30
• Introductions
• Purpose of Dry Run and Measure
• Proposed Implementation
• Dry Run Overview
• Measure Details
• Resources (next)
• Questions and Answers
Agenda
32
• Email Q&A period
August 5 – September 4, 2013
Note: Please do NOT email or attach to emails any patient identifiable information
Questions & Comments
33
Questions?














![[Slideshare] fardh'ain(august-2013-batch)#2(tauuheed)-13-september-2013](https://img.pdfslide.us/doc/110x75/546a48b6af7959ae538b4f2f/slideshare-fardhainaugust-2013-batch2tauuheed-13-september-2013.jpg)













