Embed Size (px)
Citation preview

Cancer Therapy: Preclinical
Augmentation of Immune Checkpoint CancerImmunotherapy with IL18Zhifeng Ma1,2,Wen Li1, Shinichi Yoshiya2, Yunfeng Xu1, Masaki Hata1, Yosif El-Darawish1,Tzvetanka Markova1, Kyosuke Yamanishi3, Hiromichi Yamanishi3, Hideaki Tahara4,Yoshimasa Tanaka5, and Haruki Okamura1
Abstract
Purpose: Recent clinical trials and animal models demonstrat-ed that immune checkpoint blockade enhanced effector cellresponses and tumor rejection; however, further developmentand improvement of cancer immunotherapy is necessary formorefavorable objective responses. In this study, we examined theeffect of IL18 on the antitumor effect of immune checkpointinhibitors.
Experimental Design: We examined the effect of IL18 on theperitoneal dissemination of CT-26 cells or tail vein injectionmetastasis of B16/F10 cells using antiprogrammed death-1ligand-1 (aPD-L1) and/or anti-CTL–associated antigen-4(aCTLA-4) mAbs.
Result: Massive ascites developed after intraperitoneal inocu-lation of CT-26, resulting in animal death within 30 days. Treat-ment of mice with aPD-L1 and/or aCTLA-4 significantly pro-longed their survival, and a combination of the antibodies and
IL18 provided a much greater therapeutic benefit. The combina-tion modality led to the accumulation of precursor of maturenatural killer (pre-mNK) cells in the peritoneal cavity togetherwith increased CD8þ T and decreased CD4þCD25þFoxp3þ
T cells. Depletion of the pre-mNK cells abrogated the therapeuticeffects and increased the number of CD4þCD25þFoxp3þ T cells.The combination treatment also suppressed tail vein injectionmetastasis of B16/F10 cells.
Conclusions: The results demonstrated that IL18 enhancedtherapeutic effects of immune checkpoint blockade against peri-toneal dissemination of carcinoma or tail vein injectionmetastasisof melanoma through accumulation of pre-mNK cells, memory-type CD8þ T cells, and suppression of CD4þCD25þFoxp3þ T cells.A combination of immune checkpoint inhibitors with IL18 maygive a suggestion to the development of next-generation cancerimmunotherapy. Clin Cancer Res; 22(12); 2969–80. �2016 AACR.
IntroductionT-cell responses are controlled by T-cell receptors (TCR) and
nonclonotypic immune coreceptors. Whereas costimulatoryreceptors such as CD28 and inducible T-cell costimulator (ICOS)amplify the transcriptional effects of TCR signaling, coinhibitoryreceptors including CTL-associated protein-4 (CTLA-4), pro-grammed death-1 (PD-1), lymphocyte activation gene 3 (LAG3),and T cell immunoglobulin andmucin domain 3 (TIM-3) reduceeffector functions. Tumor growth can thus be restricted by costi-mulatory signaling and facilitated by coinhibitory pathways.Tumor cells often usurp the coinhibitory system, also termed theimmune checkpoint, which controls the antitumor effects ofimmune effector cells (1–4).
Recently, research has focused on the development of cancerimmunotherapy that targets the immune checkpoint pathwaysusing mAbs, anti-CTLA4 (aCTLA-4), anti-PD-1 (aPD-1), and/oranti-PD-1 ligand-1 (aPD-L1; refs. 5–7). In clinical trials, aCTLA-4was shown to improve the overall survival rate in patientswith advanced melanoma, refractory to conventional therapies(8–10). Because CTLA-4 signaling is involved in the downregula-tion of T cells in the priming phase, the blockade of CTLA-4signaling promotes cytotoxic T cells; however, aCTLA-4 inducessevere adverse reactions (1–4). In contrast, the PD-1 pathwayplays an essential role in the regulationof immune cells, includingab T cells, gd T cells, andNK cells, in the effector phase. In a phase Iclinical trial of a fully human aPD-1/aPD-L1, objective responseswere observed in patients with melanoma, non–small cell lungcancer, renal cell cancer, bladder cancer (11, 12), non-Hodgkinlymphoma, Hodgkin lymphoma (13), esophageal cancer (14),and hepatocellular cancer (15). The nonredundant roles anddistinct adverse reactions of CTLA-4 and PD-1 pathways suggestthe potential of dual immune checkpoint blockade using a lowdose of CTLA-4 and a high dose of aPD-1 or aPD-L1 (16, 17).
Effective antitumor responses to treatments require not only ablockade of coinhibitory pathways, but also an increase in thenumber of immune effector cells. It has been demonstrated thatthe development, cytokine production, and cytotoxicity of effec-tor cells can bemodulated by various cytokines, such as IL2, IL12,IL15, IL18, and IL21. Among them, IL18 is a unique cytokine thatis maturated by inflammasome complexes (18, 19), and modu-lates antitumor responses (20–22). It is demonstrated that IL18markedly enhances the expansion of NK cells, CD8þCTLs, and gd
1Laboratory of Tumor Immunology and Immunotherapy, Hyogo Col-legeofMedicine, Hyogo, Japan. 2Department ofOrthopaedic Surgery,Hyogo College of Medicine, Nishinomiya, Hyogo, Japan. 3HirakataRyoikuen,Osaka, Japan. 4Department of Surgery andBioengineering,Institute of Medical Science, The University of Tokyo, Tokyo, Japan.5Center for Bioinformatics and Molecular Medicine, Graduate Schoolof Biomedical Sciences, Nagasaki University, Nagasaki, Japan.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corresponding Author: Haruki Okamura, Laboratory of Tumor Immunologyand Immunotherapy, Hyogo College of Medicine, Nishinomiya, Hyogo Province663-8501, Japan. Phone: 81-798-45-6744; Fax: 81-798-45-6746; E-mail:[email protected]
doi: 10.1158/1078-0432.CCR-15-1655
�2016 American Association for Cancer Research.
ClinicalCancerResearch
www.aacrjournals.org 2969
on April 12, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 11, 2016; DOI: 10.1158/1078-0432.CCR-15-1655

T cells which express IL18 receptors a/b chains and receptorscontaining immunoreceptor tyrosine-based activation motif(ITAM), and produce IFNg (23–27). In humans, IL18 promotesthe expansion of CD56brightCD11cþHLA-DRþ helper NK cells,which may be a human counterpart of mouse precursors ofmature natural killer (pre-mNK) cells, previously referred to asIFN-producing killer dendritic cells (28, 29). IL18-induced NK-lineage cells exhibit potent antitumor activity, although NK cellsexpressing inhibitory receptors, such as CTLA-4 and PD-1, mayhave regulatory functions. It is thus worthwhile to examine theeffect of IL18 on cancer immunotherapy using blocking mAbsspecific to coinhibitory pathways.
Prognosis of peritoneal dissemination of cancer is poor, eventhough a combination of cytoreduction with hyperthermic intra-peritoneal chemotherapy has become a standard therapy (30). Incontrast, there have been several studies examining immunother-apy for the treatment of peritoneal disseminated cancer (31–33).In this study, we examined the effect of IL18 on cancer immu-notherapy using aPD-L1 and/or aCTLA-4 in animal models ofperitoneal dissemination of CT-26 colon carcinoma, and ana-lyzed the mechanism underlying IL18-mediated enhancement ofantitumor activity.
Materials and MethodsAnimals and tumor cells
Six- to 8-week old male BALB/c and C57BL/6J mice werepurchased from Japan SLC (Hamamatsu). Mice were housed ina pathogen-free condition at 25�C under controlled lighting(12 hours light/12 hours dark), with free access to water andfood pellets. The CT-26 (CRL-2638), CT-26.CL25 (CRL-2639)mouse colon carcinoma cell lines, 4T1 (CRL-2539) mousebreast carcinoma cell line, and B16/F10 (CRL-6475) mousemelanoma cell line were purchased from the ATCC. The CT-26,CT-26.CL25, and 4T1 cells were maintained in RPMI1640medium (Nacalai Tesque, Inc.) supplemented with 10% FBS(BioWest), 100 units/mL penicillin, 100 mg/mL streptomycin
(Gibco BRL), B16/F10 cells were maintained in DMEM (Naca-lai Tesque, Inc.) supplemented with 10% FBS, 100 units/mLpenicillin, 100 mg/mL streptomycin at 37�C in a humidifiedatmosphere with 5% CO2.
ReagentsRecombinant mouse IL18 was provided by GlaxoSmithKline
PLC (Research Triangle Park), whereas mouse IL2 was purchasedfrom R&D Systems Inc. Anti-mouse CD152 (CTLA-4) antibody(aCTLA-4, clone UC10-4F10-11), anti-mouse CD274 (PD-L1)antibody (aPD-L1, clone 10F.9G2), and control isotype-matchedhamster IgGwere purchased fromBioXcell (BE0091). Rabbit anti-asialo GM1 (aGM1) was purchased from Wako Pure ChemicalIndustries Ltd (014-09801). Rabbit IgG was purchased fromMedical and Biological Laboratories Co., Ltd (PM035). Anti-mouse CD8 mAb (aCD8) was purchased from Santa Cruz Bio-technology, Inc. (clone 53-6.7).
Tumor cell implantation and immune checkpoint blockingSubconfluent CT-26, CT-26.CL25, 4T1, and B16/F10 cells
were harvested by detaching with 0.05% trypsin and 0.53mmol/L EDTA (trypsin-EDTA; Nacalai) or 0.25% trypsin and0.53 mmol/L EDTA (trypsin-EDTA; Nacalai) in Ca2þ, Mg2þ freeDulbecco PBS, pH 7.4 (Nacalai) and washed with PBS. Theviable cells were counted by Trypan Blue dye exclusion test andsuspended in PBS. CT-26 and 4T1 cell suspensions (5 � 104
cells in 250 mL of PBS) were intraperitoneally injected intoBALB/c mice, CT-26.CL25 cell suspensions (1 � 105 cells in100 mL of PBS) were subcutaneously injected into BALB/c mice,and B16/F10 cell suspensions (2 � 105 cells in 200 mL of PBS)were intravenously injected into C57BL/6J mice. After 3, 7, or10 days postinoculation, various doses of aCTLA-4, aPD-L1,and/or IL18 were intraperitoneally injected four times every4 days. For depletion of NK cells or CTL, aGM1 or aCD8 wasadministered to the mice. The abdominal perimeter was mea-sured to estimate the amount of ascites, and the survival ratewas monitored until 90 days postinoculation of tumor cells.
Cell preparation and cytokine assayPeritoneal exudate cells (PEC)were harvested from the abdom-
inal cavity and washed in 5 mL PBS three times. Red blood cellswere eliminated by ACK lysis buffer (500 mmol/L NH4Cl, 10mmol/L KHCO3, and 0.1 nmol/L Na2EDTA at pH 7.2––7.4), andthe resulting cells were washed three times with PBS. Cellsviability was assessed by Trypan Blue dye exclusion test. CT-26cells were lysed by repeated freezing and thawing, and the resul-tant cell debris was washed and resuspended in PBS. PECs werestimulated with the CT-26 cell preparation and cultured in theabsence or presence of IL12 (1 ng/mL) and/or IL18 (100 ng/mL)in RPMI1640medium supplemented with 10% FBS, L-glutamine(Gibco BRL), 100 units/mL penicillin, 100 mg/mL streptomycinand 10�5 mol/L 2-mercaptoethanol at 37�C in a humidifiedatmosphere with 5% CO2. After incubation, cytokines in theculture supernatants were measured using their correspondingELISA kits according to the manufacturer's instructions(PeproTech).
In vitro cytotoxicity assayCytotoxicity was assessed in vitro using the DELFIA EuTDA
Cytotoxicity Assay System (PerkinElmer Life Sciences,WallacOy).Briefly, CT-26 cells were labeled with a chelate prodrug for 10
Translational Relevance
Although immune checkpoint inhibitors are effective insome cancer patients, the efficacy may be further improvedin combination with other therapeutic modalities. In thecurrent study, we analyzed the effect of IL18 on the antitumoreffect of immune checkpoint blockade. IL18 is a cytokine ofIL1 family members and is formed by the action of activatedinflammasomes, but its physiologic roles are not completelyclarified. Recently, it was demonstrated that IL18 promotedthe expansion and survival of effector cells including NK, gd T,and CD8þ T cells. However, clinical efficacy of IL18 cancermonotherapy has been shown to be negligible. Here, we showthat IL18 efficiently augmented the expansion of effector cellsin the presence of immune checkpoint antibodies, andreduced the proportion of regulatory T cells. In addition,immune checkpoint inhibitors and IL18 synergistically inhib-ited the growth of tumor cells without significant adverseevents in animal models. The results strongly suggest that acombination of IL18 and immune checkpoint inhibitorscould be beneficial in treatment of cancer patients.
Ma et al.
Clin Cancer Res; 22(12) June 15, 2016 Clinical Cancer Research2970
on April 12, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 11, 2016; DOI: 10.1158/1078-0432.CCR-15-1655

minutes, washed, and resuspended in RPMI1640 medium. ThePECs from mice which had been treated with mAbs and/or IL18were suspended in RPMI1640 medium. The resulting cells weremixed at the indicated effector/target ratios and incubated for 3hours at 37�C. The supernatants were mixed with europiumsolution and the time-resolved fluorescence was measured usingamultiplate reader. The percentage of specific lysis was calculatedas follows: [(experimental release – spontaneous release)/(max-imum release – spontaneous release)] � 100%.
Flow cytometryThe PECs were examined for cell surface markers using a FACS
flow cytometer. The cells were stained with FITC-conjugated anti-CD4 mAbs (GK1.5), APC-conjugated anti-CD4 mAbs (RM4-5),biotin-conjugated anti-CD8mAb (53–6.7), APC-conjugated anti-CD314/NKG2D mAb (CX5), FITC and APC-conjugated anti-bTCRmAb (H57-597), PE-conjugated Foxp3mAb (FJK-16s), APC-conjugated anti-streptavidin (catalog 17-4317-82), which werepurchased from eBioscience Inc. (San Diego). APC-conjugatedanti-CD8 mAb (53–6.7), PE and APC-conjugated anti-CD45R/B220 mAbs (RA3-6B2) were purchased from Biolegend Inc. (SanDiego). FITC-conjugated anti-CD11b mAb (M1/70), biotin-con-jugated anti-CD11c mAb (HL3), PE, APC and BB515-conjugatedanti-CD25 mAb (PC-61), FITC and PE-conjugated anti-CD49bmAbs (DX5), PE-conjugated anti-CD122 mAb (TM-b1), PE-con-jugated anti-NK1.1 mAb (PK136), and FITC-conjugated anti-Streptavidin Ab (catalog 554460) were purchased from BD Bios-ciences. The cellswere incubatedwith antibodies for 20minutes at4�C, and then analyzed using a FACS Calibur flow cytometer.Anti-mouse CD16/32mAb (clone: 93, eBioscience) was used as aFc blocker. The data were processed with CellQuest software (BDBiosciences).
Measurement by ImageJTodetermine tumor volume, the greatest longitudinal diameter
(length) and the greatest transverse diameter (width) were deter-mined using an ImageJ software 1.48 (NIH, Bethesda, MD).Tumor volume was calculated by the modified ellipsoidal for-mula: Tumor volume ¼ 1/2(length � width2).
Statistical analysisData were statistically analyzed by SPSS 20.0.0 software (IBM)
and expressed as means � SD. Two groups measurements wereanalyzed with a two-tailed Student t test, and the other groupswere analyzed using one-way ANOVA with Tukey multiple com-parison test. A P value < 0.05 was considered significant, NSdenotes nonsignificant. Survival was estimated using Kaplan–Meier followed by a log-rank test.
Study approvalAll mice were bred and maintained in our animal facility in
accordance with the guidelines for the care and use of experi-mental animals in Hyogo College of Medicine, Japan. All experi-ments were conducted with the approval of the Animal CareCommittee of Hyogo College of Medicine.
ResultsIL18 enhances antitumor activity elicited by aPD-L1 and/oraCTLA-4
The blockade of immune checkpoints such as PD-1 andCTLA-4signaling pathways induces clinical benefits in limited population
of patients with various cancers (11–15). Therefore, it is impor-tant that aPD-1/PD-L1- and/or aCTLA-4–based therapies areanalyzed in a wider range of patients. Because effective antitumorresponses require immune activation as well as immune check-point blockade, we examined the synergistic effect of IL18, whichwas demonstrated to enhance effector functions of immune cells(25,26,38,39) on the survival rate of preimplantedmice receivingaPD-L1 and/or aCTLA-4. To develop an in vivo model of perito-neal dissemination, mice were intraperitoneally inoculated withthe CT-26 colon carcinoma cells. When preimplanted mice wereadministered with control IgG, all mice died of peritoneal dis-semination of tumor cells accompanying pool of ascites andabdominal adhesions within 30 days (Fig. 1A and D and Sup-plementary Figs. S1A–S1D). Treatment of 3-day preimplantedmice with either IL18, aCTLA-4, or aPD-L1 alone demonstratedmodest therapeutic effect. It is of note that combination of IL18and CTLA-4 or PD-L1 blockade promoted tumor rejection withdefinite significance by at least day 90 (Fig. 1A and SupplementaryFigs. S1A and S1B). When 7-day preimplanted mice were treatedwith the combination therapy of IL18 and immune checkpointblockade, 40% and 80% of mice survived more than 90 days foraPD-L1 and aCTLA-4, respectively (Fig. 1B). Although dualblockade of PD-L1 and CTLA-4 pathways also had modest effectson the survival rate of 7-day preimplanted mice, the addition ofIL18 enhanced tumor rejection in all mice by day 90 (Fig. 1C).Although dual blockade of PD-L1 and CTLA-4 signaling elicitedtherapeutic effects on the survival rate of 10-day preimplantedmice, inclusion of IL18 further promoted tumor rejection in 20%of mice by at least 90 days (Fig. 1D).
To further analyze the mechanism underlying the antitumoractivity elicited by IL18 and immune checkpoint blockade, theoptimal doses of the recombinant proteins were determined inthe mouse model. When CT-26 preimplanted mice were treatedwith IL18 and aCTLA-4, all mice receiving 2 mg of IL18 and 50 or100 mg of aCTLA-4 survived until day 90, whereas lower doses ofIL18 andaCTLA-4 hadmoderate therapeutic effects. Similarly, allmice treatedwith 2mgof IL18 and200mgofaPD-L1 surviveduntilday 90 and reduced effects were observed with a lower aPD-L1dose (Supplementary Figs. S1E and S1F).
Moreover, combination of IL18 and dual blockade of PD-L1and CTLA-4 was effective also in the treatment of mice subcu-taneously injected with CT-26.CL25 cells (SupplementaryFigs. S1G and S1H), but the combination failed to prevent theabdominal growth of 4T1 cells (Fig. 1E). IL18 also enhancedthe therapeutic effect of immune checkpoint blockade by aPD-L1 and/or aCTLA-4 in the tail vein injection metastasis modelusing CT26 cells (data not shown) and in C57BL/6 miceinoculated with B16 mouse melanoma cells (Fig. 1F andSupplementary Fig. S1I).
Combinationof immune checkpoint blockadewith IL18 allowsfor an accumulation of the precursors of mNK cells
To elucidate the mechanism by which immune checkpointblockade combined with IL18 provides favorable therapeuticeffects, we next examined the number of PECs. When tumor-freemice were injected with a combination of aCTLA-4, aPD-L1, andIL18, no detectable increase in the number of PECs was observed(data not shown). Treatment of CT-26 preimplanted mice witheither IL18, aCTLA-4, or aPD-L1 alone induced modest accumu-lation of PECs. In contrast, there was a large accumulation of PECswhen CT-26 preimplanted mice were treated with a combination
IL18 plus anti-PD-L1 and anti-CTLA-4 Antibodies
www.aacrjournals.org Clin Cancer Res; 22(12) June 15, 2016 2971
on April 12, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 11, 2016; DOI: 10.1158/1078-0432.CCR-15-1655

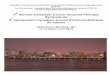
Figure 1.Effect of IL18 on the survival rate of preimplanted mice receiving aCTLA-4 and/or aPD-L1. BALB/c mice were intraperitoneally (i.p.) implanted with 5 � 104
CT-26 cells on day 0, isotype-matched IgG 100 mg, aCTLA-4 100 mg, aPD-L1 200 mg, IL18 2 mg alone or in various combinations in 250 mL of PBS wereintraperitoneally administered ondays 3, 7, 11, and 15 (A) or days 7, 11, 15, and 19 (B) followingCT-26 inoculation. Isotype-matched IgG 100mg,aCTLA-4 100mg,aPD-L1100 mg alone or combined with IL18 2 mg in 250 mL of PBS were administered on days 7, 11, 15, and 19 (C) or days 10, 14, 18, and 22 (D) following CT-26 inoculation.BALB/c mice were intraperitoneally implanted with 5 � 104 4T1 cells on day 0, isotype-matched IgG 100 mg, aCTLA-4 100 mg, aPD-L1 200 mg, IL18 2 mgalone or in various combinations in 250 mL of PBSwhichwere intraperitoneally administered on days 3, 7, 11, and 15 (E) following 4T1 inoculation. Each group included5 mice and survival rate of mice was monitored by day 90, Kaplan–Meier plots followed by log-rank P < 0.005 (A–C), P < 0.05 (D), P ¼ 0.088 (E). C57BL/6Jmice were intravenously injected with 2� 105 B16/F10 cells, isotype-matched IgG 100 mg, aCTLA-4 100 mg, aPD-L1 100 mg, and IL18 2 mg in different combinations in250 mL of PBS which were intraperitoneally administered on days 3, 7, 11, and 15 following B16/F10 inoculation. Each group included 5 mice and tumorvolumewasmeasured onday 28. Error bars representmean� SD; one-wayANOVAwith corresponding Tukeymultiple comparison test; � ,P<0.05; �� ,P <0.005 (F).Representative results of four independent experiments are shown (A–F).
Ma et al.
Clin Cancer Res; 22(12) June 15, 2016 Clinical Cancer Research2972
on April 12, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 11, 2016; DOI: 10.1158/1078-0432.CCR-15-1655

of immune checkpoint blockade with IL18 (Fig. 2A–C). Althoughthe accumulation of PECs reached a maximum at day 6 anddeclined thereafter, a subsequent injection of mAbs and IL18 onday 7 promoted reaccumulation of PECs and a sustained level ofPECs was observed even at day11. The number of CT26 tumorcells contained in the PECs of CT-26 preimplanted mice injectedwith control IgGwas significantly greater compared with themice
treated with combination of immune checkpoint blockade andIL18 (Fig. 2D and E).
To characterize the PECs recruited by the tumor cells, mAbs,and/or IL18, the cells were stained with mAbs specific for DX5(CD49b), B220 (CD45R), CD11b, CD11c, and NKG2D(CD314). It was of note that 10% to 30% of PECs comprisedDX5þB220þ NK cells 4 days after mAb plus IL18 administration
Figure 2.Accumulation of PECs after immune checkpoint blockade therapy combined with IL18. BALB/c mice were intraperitoneally (i.p.) injected with 5� 104 CT-26 cells in250 mL of PBS on day 0, isotype-matched IgG 100 mg, aCTLA-4 100 mg, aPD-L1 2 mg, IL18 2 mg alone or in various combinations in 250 mL of PBS whichwere intraperitoneally administered on days 3 and 7 following CT-26 inoculation (A–C). Each group included 5 mice and PECs were harvested and viable cells werecounted on days 4, 5, 6, 7, and 11. Error bars represent mean � SD; one-way ANOVA with corresponding Tukey multiple comparison test; � , P < 0.05 (A–C).Representative results of four independent experiments are shown (A–C). Isotype-matched IgG or aCTLA-4 plus aPD-L1 and IL18 were intraperitoneallyadministered into the tumor preimplanted mice 3 days following CT-26 inoculation. Each group included 5 mice and PECs were harvested and stained by Giemsastaining buffer, CT-26 cells number was counted on day 7 (D). Images are displayed at 20� or 40� magnification (E) and are representative of threeindependent experiments. Error bars represent mean � SD; two-tailed Student t test; � , P < 0.05 (D).
IL18 plus anti-PD-L1 and anti-CTLA-4 Antibodies
www.aacrjournals.org Clin Cancer Res; 22(12) June 15, 2016 2973
on April 12, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 11, 2016; DOI: 10.1158/1078-0432.CCR-15-1655

to CT26 cell-implanted mice (7 days postinoculation of CT26cells). In addition, B220 and NKG2D were expressed on themajority of the NK cells in the PECs and the expression levels ofB220, CD11b, and CD11c were significantly increased by theinjection of IL18 (Fig. 3A, Table 1, and Supplementary Fig. S2A).The expression of B220 on NK cells was further enhanced 8 daysafter mAbs plus IL18 administration (day 11 postinoculation ofCT 26 cells; Fig. 3B, Table 1). The B220þ NK cells also expressedCD11b, CD11c, and CD122 and were most likely to be pre-mNKcells (Table 2), formerly called IFNg-producing killer dendriticcells (28, 29).
Phenotypic analyses of T cells in the PECs from preimplantedmice treated with mAbs and IL18
Analysis of the T-cell subsets in the PEC was undertaken bystaining the cell surface markers with mAbs. Although IL18 didnot affect the proportion of CD4þ cells in the PECs of miceadministrated aCTLA-4, IL18 strongly reduced CD4þ cells in thePECs stimulated by aPD-L1 or by aCTLA-4 plus aPD-L1 (Fig. 4Aand Supplementary Fig. S2B). CD4þ T cells occupied 10.95% �1.21% of the PECs from mice injected with aPD-L1 plus IL18 4days after CT-26 inoculation, although 20.35%� 2.16% of PECsfrom mice treated with aPD-L1 alone were CD4þ T cells. Thiseffect was pronounced when aCTLA-4 plus aPD-L1 regimen(23.18% � 2.76%) was compared with the aCTLA-4 plusaPD-L1 plus IL18 regimen (5.88% � 1.03%). This suggests thata combination of IL18 and immune checkpoint blockade potent-ly decreases CD4þ T-cell/effector T-cell ratios in the PECs (Fig. 4Aand Supplementary Fig. S2B). This was confirmed by measuringthe proportion of CD25þFoxp3þ cells in the PECs. Administra-tion of aCTLA-4 plus aPD-L1 reduced the proportion of CD25þ
Foxp3þ cells, whereas a combination of IL18 with the mAbsfurther reduced CD25þFoxp3þ cells. The proportion of CD25þ
Foxp3þ cells in the control IgG CD4þCD25þ PECs was 65.23%�3.11%, and this was reduced to 54.88% � 3.07% by aCTLA-4 plus aPD-L1, and further reduced to 47.67% � 3.15%by aCTLA-4 plus aPD-L1 plus IL18. In contrast, in the TCR-bchainþCD8þ cells, IL18 appeared to have no effect on theirproportion (Fig. 4A). The decrease in the proportion of CD4þ
CD25þFoxp3þregulatory T cells in the PECs by IL18was observedeven when they were analyzed 8 days after administrationof aCTLA-4 plus aPD-L1 with or without IL18 (51.03% �2.75%vs. 59.31%� 4.32%, respectively), whereas the proportionof the control was rather high (77.02% � 4.12%; Fig. 4B). Inaddition, the proportion of CD8þ T cells was decreased by IL18
Figure 3.Phenotypic analyses of NK cells in PECs derived from CT-26 preimplantedmice receiving immune checkpoint blocking mAbs and IL18. BALB/cmice were intraperitoneally (i.p.) injected with 5 � 104 CT-26 cells in250 mL of PBS on day 0. Isotype-matched IgG 100 mg, or aCTLA-4100 mg, aPD-L1 100 mg, with or without IL18 2 mg in 250 mL of PBS wereintraperitoneally administered 3 days following CT-26 inoculation. Fourdays later, PECs were harvested and examined for DX5 (CD49b), B220(CD45R) using a flow cytometer. TCR-b� fractions in the PECs were gatedand further examined for NKG2D (CD314) or CD11b (Mac-1) and CD11cexpression (A). Similarly, PECs prepared 8 days after administration ofmAbs and IL18 were analyzed by flow cytometry (B). Similar dot plotsdisplays are representative of three independent experiments(n ¼ 3; A and B).
Ma et al.
Clin Cancer Res; 22(12) June 15, 2016 Clinical Cancer Research2974
on April 12, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 11, 2016; DOI: 10.1158/1078-0432.CCR-15-1655

administration, although the expression of NKG2D on the CD8þ
T cells was slightly increased (Fig. 4B).
Functional analyses of PECs from preimplanted mice treatedwith immune checkpoint blocking mAbs and/or IL18
Because immune checkpoint blockade in combination withIL18 promoted accumulation of pre-mNK cells in the PECs andshifted the peritoneal environment from dominant suppressionto an inflammatory milieu ideal for immune effector cell-medi-ated tumor rejection, we next analyzed responses of PECs tovarious stimuli to determine their functions. The results showthat IFNg was released from the PECs derived from CT-26 mice.Treatment of mice with aCTLA-4 plus aPD-L1 enhanced theproduction of IFNg , and IL18 further promoted IFNg production(Supplementary Fig. S3A). In contrast, a high level of IL10 wasproduced by the PECs and the IL10 secretion was reduced whenmice were treated with immune checkpoint blocking mAbs. Thedecrease in IL10 production was more prominent in the presenceof IL18 (Supplementary Fig. S3B), and TGFb production was alsoattenuated by mAbs treatment. The addition of IL18 reduced thecytokine secretion to a background level (Supplementary Fig.S3C). A low level of IFNg was produced by PECs after adminis-tration of IL18 plus mAbs 10 days after tumor inoculation(Supplementary Fig. 3D). In contrast, a high level of TGFb wasproduced by PECs induced by control IgG, and the secretion ofTGFb was reduced when mice were treated with immune check-point blocking mAbs (Supplementary Fig. S3D).
Next, the effect of immune checkpoint blocking mAbs and/orIL18 on the cytotoxicity of PECs was determined. A combinationofaCTLA-4 andaPD-L1 slightly increased the tumoricidal activityof the PECs and the addition of IL18 markedly enhanced thecytotoxicity of PECs against CT-26 cells (Supplementary Fig. S4A).Repeated injection of aCTLA-4 plus aPD-L1 and/or IL18 revealedthat IL18 helped sustain a high level of antitumor activity of PECs(Supplementary Fig. S4B). On the basis of the results, it was most
likely that enhanced secretion of inflammatory cytokines andtumoricidal activity of the PECs were responsible for the protec-tion of mice from aggressive tumor cells.
Negation by pre-mNK cell deletion of the therapeutic effect ofimmune checkpoint blockade and IL18
We next attempted to identify cell subsets in the PECs respon-sible for tumor rejection and improved survival rate. Uponintraperitoneal inoculation of tumor cells and treatment byimmune checkpoint blockade and IL18, the pre-mNK cells wereaccumulated in the peritoneum as shown in Fig. 3. The resultprompted us to examine the effect of NK cell depletion on thesurvival rate and cytotoxic activity of effector cells in the PECs.After administration of aCTLA-4, aPD-L1, IL18, and control IgGinto CT-26 preimplanted mice, all mice survived more than 90days. In contrast, injection of anti-asialoGM1 Ab (aGM1) insteadof control IgG almost completely negated the therapeutic effect ofthe combination therapy, indicating that pre-mNK cells play apivotal role in tumor rejection (Fig. 5A). In addition, the cytotoxicactivity of the PECs against CT-26was significantly reduced by theaddition of aGM1 (Fig. 5B). Repeated injections of aGM1 furtherreversed the beneficial effects of the tumor immunotherapy usingimmune checkpoint blocking mAbs and IL18 (Fig. 5C).
Modulation of pre-mNK cell and CD4þCD25þ T-cellaccumulation by aGM1
The numbers of PECs were essentially the same betweenpreimplanted mice which had been injected with aGM1, fol-lowed by aCTLA-4, aPD-L1, and IL18, and those with controlIgG. The percentage of TCR-b�DX5þB220þ pre-mNK cells was,however, significantly reduced by the treatment with aGM1(Supplementary Fig. S5A). It is noteworthy that aGM1 marked-ly increased the accumulation of CD4þCD25þ T cells, and thatthe administration of aGM1 significantly reduced the numberof CD8þ T cells (Supplementary Fig. S5B). The results clearlydemonstrated that aGM1 treatment led to an increase in theratio of CD4þCD25þ regulatory T cells to TCR-b�DX5þB220þ
pre-mNK effector cells, shifting antitumor cellular responses toimmune suppression.
Immunosuppressive milieu induced by aGM1To examine the tumor environment in the peritoneum, cyto-
kine production was determined after administration of aGM1.When preimplanted mice were treated with immune checkpointblocking mAb plus IL18, the inclusion of aGM1 reduced thesecretion of IFNg from PECs (Supplementary Fig. S6A). In con-trast, the production of IL10 and TGFb was markedly enhanced(Supplementary Figs. S6B and S6C), demonstrating that aGM1converted the inflammatory environment in the peritoneum intoimmunosuppressive milieu.
Table 1. Percentage and absolute number of DX5þB220þ NK induced by IgG, aCTLA-4, aPD-L1, and IL18
IgG aCTLA-4þaPD-L1 aCTLA-4þaPD-L1þIL18
6 Days DX5þB220þ NK Percentage (%) 10.85 � 1.74 28.94 � 2.05a 35.57 � 3.12a,b
Absolute number (�106) 0.47 � 0.08 1.68 � 0.12a 4.05 � 0.36a,b
10 Days DX5þB220þ NK Percentage (%) 17.34 � 1.98 22.95 � 2.33a 27.11 � 2.64a,b
Absolute number (�106) 0.60 � 0.07 1.33 � 0.14a 3.11 � 0.30a,b
NOTE: CT-26 preimplanted mice were administrated IgG, aCTLA-4 plus aPD-L1 with or without IL18, PECs were harvested (same as Fig. 3), percentage ofDX5þB220þ NK cells were checked by using a flow cytometer. Data given are the average values from three independent experiments in triplicate.aP < 0.05, significant when compared with IgG group.bP < 0.05, significant when compared with aCTLA-4 plus aPD-L1 group.
Table 2. Surface markers of pre-mNK induced by IgG, aCTLA-4, aPD-L1, andIL18
IgG aCTLA-4þaPD-L1 aCTLA-4þaPD-L1þIL18
DX5 þ þþ þþþB220 þ þþ þþþCD11b þ þ þCD11c þþ þ þþþCD62L þ þ þCD69 þ þ þCD83 þ þ þCD122 þ þ þNKG2D þ þþ þþþNOTE: CT-26 preimplanted mice were administrated IgG, aCTLA-4 plus aPD-L1with or without IL18. Surface markers of pre-mNK cells were checked by using aflow cytometer.
IL18 plus anti-PD-L1 and anti-CTLA-4 Antibodies
www.aacrjournals.org Clin Cancer Res; 22(12) June 15, 2016 2975
on April 12, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 11, 2016; DOI: 10.1158/1078-0432.CCR-15-1655

Essential role of CD8þ T cells in tumor rejectionBecause aGM1 treatment decreased efficacy of immune check-
point blockade and IL18 with concomitant reduction of CD8þ Tcells, we analyzed the role of CD8þ T cells in tumor immuno-therapy. When preimplanted mice received aCTLA-4, aPD-L1,and IL18, these mice survived more than 90 days. The addition ofanti-CD8 mAb (aCD8), however, significantly reduced the sur-vival rate and all mice died within 32 days (Fig. 6A). In functionalanalyses, cytotoxic activity of the PECs derived frompreimplantedmice treated with aCTLA-4, aPD-L1, IL18, and aCD8 was signif-
icantly impaired, when compared with treatment without aCD8(Fig. 6B). The immune impairment in the PECswas observed even9 days after treatment (Fig. 6C), which strongly suggests thatCD8þ T cells played a critical role in antitumor responses.
Phenotypic analyses of PECs after treatment with aCD8Administration of aCD8 to mice receiving CT-26, aCTLA-4,
aPD-L1, and IL18 greatly reduced the CD8þ population in thePECs, whereas the proportion of CD4þ T cells was not signifi-cantly altered (Supplementary Fig. S7A). The proportion of TCR-
Figure 4.Phenotypic analyses of T cells in the PECs fromCT-26 preimplantedmice treatedwith immune checkpoint blockade and/or IL18. BALB/cmicewere intraperitoneallyinjected with 5 � 104 CT-26 cells in 250 mL of PBS on day 0. Isotype-matched IgG 100 mg, or either aCTLA-4 100 mg, aPD-L1 100 mg, with or withoutIL18 2 mg in 250 mL of PBSwere intraperitoneally administered 3 days after CT-26 inoculation. A, After additional 4 days, PECswere harvested and stained for TCR-b,CD4, CD25, and Foxp3, or TCR-b, CD8, and NKG2D. B, eight days after the treatment and examined for expression of surface molecules in the same way.Similar dot plots or histograms displays are representative of three independent experiments (n ¼ 3; A and B).
Ma et al.
Clin Cancer Res; 22(12) June 15, 2016 Clinical Cancer Research2976
on April 12, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 11, 2016; DOI: 10.1158/1078-0432.CCR-15-1655

b�B220þDX5þpre-mNK cellswas notmarkedly influencedby theaddition of aCD8 (Supplementary Fig. S7B), demonstrating thatthe accumulation of CD4þ T cells and pre-mNK cells in theperitoneumwas regulated by amechanism that is independent ofCD8þ T cells, and that the antitumor activity of the CD8þ T cellswas essential for tumor rejection.
DiscussionImmunotherapy targeting immune checkpoint pathways is
effective in some cancer patients such as metastatic melanoma,lung cancer, and kidney cancer (1,11–15,31). The blockade ofimmune checkpoints like PD-1/PD-L1 and CTLA-4/CD80 path-ways reinvigorates immune effector cells and leads to tumorrejection (5–7). Even though dual blockade of the PD-1 andCTLA-4 pathways results in synergistic effects in antitumorresponses (16, 17), the therapeutic intervention fails to complete-ly eliminate malignant tumors. It is thus necessary to further
develop and improve immune checkpoint blocking therapy. Inthe current study, we demonstrated that IL18markedly improvedthe survival rate of preimplanted mice treated with aCTLA-4 andaPD-L1. In a tail vein injection metastasis model using B16melanoma cells, IL18 exerted a similar effect on treatment byimmune checkpoint blockade. In contrast, IL18 failed to enhancethe effect of immune checkpoint blockade against intraperitonealgrowth of 4T1 breast cancer cells. This indicated that the effect ofIL18 aswell as immune checkpoint blockade is not effective on allthe tumor cells type as is the fact that the therapy is not effective onall of the cancer patients. Although the reasons for differentresponses among tumor cell types, it seems that the efficacy ofthe therapy is dependent on whether the cancer is able to induceinflammatory responses or not. Inflammatogenic tumors may besusceptible to the therapy, whereas others may not respond to iteffectively. The strength of antigenicity may be dependent on thefrequency of antigenic mutation of the tumor cells, or on theintensity of PD-L1orCTLA4 in tumor cells, or on the expression of
Figure 5.Critical role of pre-mNK cells in the therapeutic effect of immune checkpoint blockade and IL18. BALB/c mice were injected with control rabbit IgG 50 mgor 50mLaGM1 in 250mLof PBSondays�1, 2, 6 and 10, 5� 104CT-26 cells in 250mLof PBSonday0, isotype-matched IgG 100mg,aCTLA-4 100mgplusaPD-L1 100mg,or combinedwith IL18 2 mg in 250 mL of PBS on days 3, 7, 11, and 15. Each group included 5mice and survival rate ofmicewasmonitored by day 90, Kaplan–Meier plotsfollowed by log-rank P < 0.005. A representative result of four independent experiments is shown (A). As shown in A, CT-26 preimplanted mice wereadministered with aGM1, aCTLA-4, aPD-L1, and IL18. PECs were harvested and examined on day 7 (B) or day 12 (C) for cytotoxic activity against CT-26 cellsat effector/target ratios of 3:1, 10:1, and 30:1 in decuplicate. Error bars represent mean � SD; two-tailed Student t test; � , P < 0.05. Representative resultsof three independent experiments are shown (B and C).
IL18 plus anti-PD-L1 and anti-CTLA-4 Antibodies
www.aacrjournals.org Clin Cancer Res; 22(12) June 15, 2016 2977
on April 12, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 11, 2016; DOI: 10.1158/1078-0432.CCR-15-1655

stress-inducedmolecules such asMICA/MICB (34). Thesemust befurther explored.
Although IL18 was originally discovered as an IFNg-inducingfactor (22, 24), precise physiologic functions of this cytokine havenot yet been fully elucidated. IL18 is converted to its mature formby the action of inflammasome complexes (18, 20, 21), which area caspase-1–activating apparatus composed of multiple proteins(19). They sense and respond to various stresses such as infection,reactive oxygen species, and tissue damage (20–22). In addition,they are linked to cellular metabolism and to events such aspyroptosis andmitochondria autophagy, regulating cell viability.IL18 may thus play an important role in the responses to cellularstress and is involved in maintenance of energy metabolismhomeostasis and in quality control of organelles, leading to cellsurvival and expansion of activated lymphocytes (25–27).
Beneficial effects of IL18 in immune checkpoint blockingtherapy may be attributable to multiple mechanisms includingactivation and expansion of cytotoxic pre-mNK cells, reduced
accumulation of regulatory T cells, and suppression ofsoluble inhibitor secretion such as IL10 and TGFb. In humans,IL18 promotes development and expansion of CD56high
CD11cþCD25highCD86highHLA-DRhighHLA-DQhigh NK cells(termed helper NK cells) in the presence of IL2, which in turnenhance the expansion of effector gd T cells (25–27). It is mostlikely that human helper NK cells are a counterpart of mousepre-mNK cells (28, 29). If this is the case, mouse pre-mNK cellsmay induce the development and expansion of effector T cells.Because both pre-mNK cells and effector T cells exhibitcytotoxic activity against tumor cells, IL18 unambiguouslypromotes induction of immune effector cells, leading to erad-ication of tumors.
It has been demonstrated that dual blockade of the PD-1 andCTLA-4pathways increased the immune effector cell/regulatory T-cell ratio in an animalmodel (16, 17). The addition of IL18 in thissystem further decreases the number of regulatory T cells,although the precise mechanism remains elusive. Thus, it will be
Figure 6.Critical role of CD8þ T cells in the therapeutic effect of immune checkpoint blockade and IL18. BALB/cmicewere injectedwithaCD8 100 mg in 250 mL of PBS on days�1, 2, 6 and 10, 5 � 104 CT-26 cells in 250 mL of PBS on day 0, isotype-matched IgG 100 mg, aCTLA-4 100 mg plus aPD-L1 100 mg and IL18 2 mg in 250 mL ofPBS on days 3, 7, 11, and 15. Each group included 5 mice and survival rate of mice was monitored by day 90, Kaplan–Meier plots followed by log-rank P < 0.005. Arepresentative result of four independent experiments is shown (A). Similar to A, CT-26 preimplanted mice were administered with aCD8, aCTLA-4, aPD-L1,and IL18. PECs were harvested and examined on day 7 (B) or day 12 (C) for cytotoxic activity against CT-26 cells at effector/target ratios of 3:1, 10:1, and30:1 in decuplicate. Error bars represent mean � SD; two-tailed Student t test; � , P < 0.05. Representative results of three independent experiments are shown(B and C).
Ma et al.
Clin Cancer Res; 22(12) June 15, 2016 Clinical Cancer Research2978
on April 12, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 11, 2016; DOI: 10.1158/1078-0432.CCR-15-1655

of interest to examine the relationship between increased pre-mNK and decreased regulatory T cells. Because the functions ofIL18 can be defined by the environment, it is likely that IL18simply enhanced the effect ofaCTLA-4 andaPD-L1, resulting in adecrease in the number of regulatory T cells. Similarly, effectivesuppression by IL18 of soluble inhibitor secretion is also achievedby the promotion of immunomodulatory effects of aCTLA-4 andaPD-L1.
Upon engagement with its receptor, IL18 activates p38 MAPK,PI3K/AKT, and ERK pathways as well as the MyD88-IRAK-TRAF6signaling pathway (35–37). IL18 thus executes multiple signalsinvolved in cellular viability, growth, differentiation, migration,and cytokine secretion. In addition, IL18 activates signals relatedto Bcl-2 and Bcl-XL, which may account for the protection oflymphocytes from activation-induced cell death and pro-grammed cell death (25, 26, 38, 39), resulting in a large accumu-lation of PECs. Because efficient cytokine production is oftenaccompanied by large expansion of cytokine-producing cells,immune effector cells like pre-mNK cells may be expanded viathe Bcl family molecule-mediated signals executed by IL18.
It is worth noting that IL18-deficient mice are prone to thedevelopment of spontaneous tumors, and that IL18 has potentantitumor activity. The cytokine, however, fails to directly act onand eradicate tumor cells, suggesting that IL18 activates andexpand immune effector cells and indirectly exhibits antitumoractivity. In line with the findings, depletion of pre-mNK cells orCD8þ T cells reversed antitumor effects of immune checkpointblockade plus IL18 therapy. Althoughpre-mNK cells accumulatedin the peritoneum after the therapy, the number of CD8þ T cellswas rather reduced. This is possibly because CD8þ T cells withouttumor specificity were not infiltrated into the tumor, even thougha substantial number of tumor-specific T cellsweremobilized intothe peritoneum.
It has been demonstrated that dual blockade of the PD-1 andCTLA-4pathways increased the immune effector cell/regulatory T-cell ratio in an animal model (16, 17). In the current study, theaddition of IL18 in this system further decreases the number ofregulatory T cells, although the precise mechanism remains elu-sive. Thus, it will be of interest to examine the relationshipbetween increased pre-mNK and decreased regulatory T cells.
On the other side, it was shown that IL18-induced NK cellsexpress PD-1 and are immunoablative (40, 41). Therefore, it isnecessary to examinewhether IL18 inducesNK cells susceptible toregulation by PD-L1–expressing cells such as tumor cells. In fact,IL18 was shown to suppress immune responses to cancer throughinduction of PD-1 and immunoablative NK cells (34, 40). How-ever, many studies indicate that IL18 has a dual role in cancerimmunology depending on the context, one is anticancer activityand the other is tumor-promoting activity (42). Our currentresults demonstrated that IL18 canpromote the anticancer activityof immune checkpoint inhibitors. Although themechanismmustbe elucidated in detail, it was considered that the expansion ofeffector cells such asNK cells by IL18 could overcome the immune
suppression byPD-1,whichmaybe upregulated by IL18. The dualrole of IL18 in tumor immunologymust be analyzed. Thismay berelated with the dual roles of NK cells, induction of tolerance oractivation of immunity.
In addition to cellular immunity, cytokines appear to play anessential role in the rejection of tumors. In fact, the addition ofIL18 to immune checkpoint blockade therapy converts the tumorenvironment from one of suppression to one of inflammatorymilieu, leading to efficient rejection of tumors. In contrast, inclu-sion of aGM1 or aCD8 reversed the cytokine milieu, suggestingthat pre-mNK cells and CD8þ T cells play an important role indetermining the tumor environment. Taken together, IL18 is notmerely a cytokine producer, but a key factor to modulate antitu-mor activity via the transcription network downstreamof the IL18receptor during immune checkpoint blockade therapy. Althoughmuch needs to be done to elucidate the divergent roles of IL18 atthe molecular level, inclusion of IL18 in immune checkpointblockade therapy may extend the currently evolving treatmentlandscape of cancer.
Disclosure of Potential Conflicts of InterestH. Tahara reports receiving a commercial research grant from and has
received speakers bureau honoraria from Ono Pharmaceuticals. No potentialconflicts of interest were disclosed by the other authors.
Authors' ContributionsConception and design: Z. Ma, W. Li, M. Hata, Y. El-Darawish, H. OkamuraDevelopment of methodology: Z. Ma, W. Li, Y. Xu, M. Hata, Y. El-Darawish,H.OkamuraAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): Z. Ma, W. Li, Y. Xu, M. Hata, Y. El-Darawish,T. Markova, K. Yamanishi, H.OkamuraAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): Z. Ma, W. Li, M. Hata, Y. El-Darawish, T. Markova,K. Yamanishi, H. Tahara, Y. Tanaka, H. OkamuraWriting, review, and/or revision of the manuscript: Z. Ma, W. Li, M. Hata,K. Yamanishi, H. Tahara, Y. Tanaka, H. OkamuraAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): Z. Ma, W. Li, S. Yoshiya, M. Hata, H. OkamuraStudy supervision: Z. Ma, W. Li, M. Hata, H. Okamura
AcknowledgmentsThe authors thank Ms. Naomi Gamachi, Fumiko Yoshida, Atsuko Tama-
moto, and Emi Yamaguchi for expert technical assistance and thank GlaxoS-mithKline PLC (Research Triangle Park, NC) for providing the recombinantmouse IL18.
Grant SupportThis work was supported by JSPS KAKENHI by grant number 24390306.The costs of publication of this article were defrayed in part by the
payment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received July 15, 2015; revised December 2, 2015; accepted December 27,2015; published OnlineFirst January 11, 2016.
References1. Mellman I, Coukos G, Dranoff G. Cancer immunotherapy comes of age.
Nature 2011;480:480–9.2. Makkouk A, Weiner GJ. Cancer immunotherapy and breaking immune
tolerance: new approaches to an old challenge. Cancer Res 2015;75:5–10.
3. LeMercier I, Lines JL, Noelle RJ. BeyondCTLA-4 and PD-1, the generation Zof negative checkpoint regulators. Front Immunol 2015;6:418.
4. Zhou E, Huang Q, Wang J, Fang C, Yang L, Zhu M, et al. Up-regulation ofTim-3 is associated with poor prognosis of patients with colon cancer. Int JClin Exp Pathol 2015;8:8018–27.
IL18 plus anti-PD-L1 and anti-CTLA-4 Antibodies
www.aacrjournals.org Clin Cancer Res; 22(12) June 15, 2016 2979
on April 12, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 11, 2016; DOI: 10.1158/1078-0432.CCR-15-1655

5. Leach DR, Krummel MF, Allison JP. Enhancement of antitumor immunityby CTLA-4 blockade. Science 1996;271:1734–6.
6. van Elsas A, Sutmuller RP, Hurwitz AA, Ziskin J, Villasenor J, Medema JP,et al. Elucidating the autoimmune and antitumor effectormechanisms of atreatment based on cytotoxic T lymphocyte antigen-4 blockade in combi-nation with a B16 melanoma vaccine: comparison of prophylaxis andtherapy. J Exp Med 2001;194:481–9.
7. Iwai Y, Ishida M, Tanaka Y, Okazaki T, Honjo T, Minato N. Involvement ofPD-L1 on tumor cells in the escape from host immune system and tumorimmunotherapy by PD-L1 blockade. Proc Natl Acad Sci U S A 2002;99:12293–7.
8. Ribas A, Camacho LH, Lopez-Berestein G, Pavlov D, Bulanhagui CA,Millham R, et al. Antitumor activity in melanoma and anti-self responsesin a phase I trial with the anti-cytotoxic T lymphocyte-associated antigen 4monoclonal antibody CP-675,206. J Clin Oncol 2005;23:8968–77.
9. Korman A, Yellin M, Keler T. Tumor immunotherapy: preclinical andclinical activity of anti-CTLA4 antibodies. Curr Opin Investig Drugs2005;6:582–91.
10. Agarwala SS, Ribas A. Current experience with CTLA4-blocking monoclo-nal antibodies for the treatment of solid tumors. J Immunother 2010;33:557–69.
11. Ohaegbulam KC, Assal A, Lazar-Molnar E, Yao Y, Zang X. Human cancerimmunotherapy with antibodies to the PD-1 and PD-L1 pathway. TrendsMol Med 2015;21:24–33.
12. TopalianSL,Hodi FS, Brahmer JR,Gettinger SN, SmithDC,McDermottDF,et al. Safety, activity, and immune correlates of anti-PD-1 antibody incancer. N Engl J Med 2012;366:2443–54.
13. Berger R, Rotem-Yehudar R, Slama G, Landes S, Kneller A, Leiba M, et al.Phase I safety and pharmacokinetic study of CT-011, a humanized anti-body interacting with PD-1, in patients with advanced hematologic malig-nancies. Clin Cancer Res 2008;14:3044–51.
14. Ohigashi Y, Sho M, Yamada Y, Tsurui Y, Hamada K, Ikeda N, et al. Clinicalsignificance of programmed death-1 ligand-1 and programmed death-1ligand-2 expression in human esophageal cancer. ClinCancer Res 2005;11:2947–53.
15. Shi F, Shi M, Zeng Z, Qi RZ, Liu ZW, Zhang JY, et al. PD-1 and PD-L1upregulation promotes CD8(þ) T-cell apoptosis and postoperative recur-rence in hepatocellular carcinoma patients. Int J Cancer 2011;128:887–96.
16. Duraiswamy J, Kaluza KM, Freeman GJ, Coukos G. Dual blockade of PD-1and CTLA-4 combined with tumor vaccine effectively restores T-cell rejec-tion function in tumors. Cancer Res 2013;73:3591–603.
17. Intlekofer AM, Thompson CB. At the bench: preclinical rationale for CTLA-4 and PD-1 blockade as cancer immunotherapy. J Leukoc Biol 2013;94:25–39.
18. Martinon F, Mayor A, Tschopp J. The inflammasomes: guardians of thebody. Annu Rev Immunol 2009;27:229–65.
19. Sollberger G, Strittmatter GE, Garstkiewicz M, Sand J, Beer HD. Caspase-1:the inflammasome and beyond. Innate Immun 2014;20:115–25.
20. Zitvogel L, Kepp O, Galluzzi L, Kroemer G. Inflammasomes in carcino-genesis and anticancer immune responses.Nat Immunol 2012;13:343–51.
21. Kolb R, Liu GH, Janowski AM, Sutterwala FS, ZhangW. Inflammasomes incancer: a double-edged sword. Protein Cell 2014;5:12–20.
22. Palma G, Barbieri A, Bimonte S, Palla M, Zappavigna S, Caraglia M, et al.Interleukin 18: friend or foe in cancer. Biochim Biophys Acta 2013;1836:296–303.
23. Ortaldo JR, Young HA. IL18 as critical co-stimulatory molecules in mod-ulating the immune response of ITAMbearing lymphocytes. Semin Immu-nol 2006;18:193–6.
24. Hodge DL, Subleski JJ, Reynolds DA, Buschman MD, Schill WB, BurkettMW, et al. The proinflammatory cytokine interleukin-18 alters multiplesignaling pathways to inhibit natural killer cell death. J Interferon CytokineRes 2006;26:706–18.
25. Li W, Kashiwamura S, Ueda H, Sekiyama A, Okamura H. Protection ofCD8þ T cells from activation-induced cell death by IL18. J Leukoc Biol2007;82:142–51.
26. LiW,Kubo S,OkudaA, YamamotoH,UedaH, Tanaka T, et al. Effect of IL18on expansion of gammadelta T cells stimulated by zoledronate and IL-2.J Immunother 2010;33:287–96.
27. Tsuda J, Li W, Yamanishi H, Yamamoto H, Okuda A, Kubo S, et al.Involvement of CD56brightCD11cþ cells in IL18-mediated expansion ofhuman gd T cells. J Immunol 2011;186:2003–12.
28. Guimont-Desrochers F, Lesage S. Revisiting the Prominent Anti-TumoralPotential of Pre-mNK Cells. Front Immunol 2013;4:446.
29. Zitvogel L, Housseau F. IKDCs or B220þNK cells are pre-mNK cells. Blood2012;119:4345–6.
30. Glockzin G, Piso P. Current status and future directions in gastriccancer with peritoneal dissemination. Surg Oncol Clin N Am 2012;21:625–33.
31. Str€ohlein MA, Lordick F, R€uttinger D, Gr€utzner KU, Schemanski OC, J€agerM, et al. Immunotherapy of peritoneal carcinomatosis with the antibodycatumaxomab in colom, gastric, or pancreatic cancer: an open-label,multicenter, phase I/II trial. Onkologie 2011;34:101–8.
32. Takiguchi S, Nishino Y, Inoue K, IkedaM, Kataoka Y,Matsusue K, et al. Thebisphosphonate incadronate inhibits intraperitoneal dissemination in anin vivo pancreatic cancer model. Oncol Rep 2012;28:111–6.
33. Kuramoto Y, Kawakami S, Zhou S, Fukuda K, Yamashita F, Hashida M.Efficient peritoneal dissemination treatment obtained by an immunosti-mulatory phosphorothioate-type CpGDNA/cationic liposome complex inmice. J Control Release 2008;126:274–80.
34. Desrichard A, Snyder A, Chan TA. Cancer neoantigens and applications forimmunotherapy. Clin Cancer Res. 2015 Oct 29 [Epub ahead of print].
35. Kroeger KM, Sullivan BM, Locksley RM. IL18 and IL-33 elicit Th2 cytokinesfrom basophils via a MyD88- and p38alpha-dependent pathway. J LeukocBiol 2009;86:769–78.
36. Chandrasekar B,Mummidi S, Valente AJ, Patel DN, Bailey SR, FreemanGL,et al. The pro-atherogenic cytokine interleukin-18 induces CXCL16 expres-sion in rat aortic smooth muscle cells via MyD88, interleukin-1 receptor-associated kinase, tumor necrosis factor receptor-associated factor 6, c-Src,phosphatidylinositol 3-kinase, Akt, c-Jun N-terminal kinase, and activatorprotein-1 signaling. J Biol Chem 2005;280:26263–77.
37. Reddy VS, Harskamp RE, van Ginkel MW, Calhoon J, Baisden CE, Kim IS,et al. Interleukin-18 stimulates fibronectin expression in primary humancardiac fibroblasts via PI3K-Akt-dependent NF-kappaB activation. J CellPhysiol 2008;215:697–707.
38. Li W, Yamamoto H, Kubo S, Okamura H. Modulation of innate immunityby IL18. J Reprod Immunol 2009;83:101–5.
39. NakanishiK, Yoshimoto T, TsutsuiH,OkamuraH. Interleukin-18 regulatesboth Th1 and Th2 responses. Annu Rev Immunol 2001;19:423–74.
40. Terme M, Ullrich E, Aymeric L, Meinhardt K, Coudert JD, Desbois M, et al.Cancer-induced immunosuppression: IL18-elicited immunoablative NKcells. Cancer Res 2012;72:2757–67.
41. TermeM, Ullrich E, Aymeric L, Meinhardt K, Desbois M, Delahaye N, et al.IL18 Induces PD-1–dependent immunosuppression in cancer. Cancer Res2011;71:5393–9.
42. Fabbi M, Carbotti G, Ferrini S. Context-dependent role of IL18 in cancerbiology and counter-regulation by IL18BP. J Leukoc Biol 2015;97:665–75.
Clin Cancer Res; 22(12) June 15, 2016 Clinical Cancer Research2980
Ma et al.
on April 12, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 11, 2016; DOI: 10.1158/1078-0432.CCR-15-1655

2016;22:2969-2980. Published OnlineFirst January 11, 2016.Clin Cancer Res Zhifeng Ma, Wen Li, Shinichi Yoshiya, et al. IL18Augmentation of Immune Checkpoint Cancer Immunotherapy with
Updated version
10.1158/1078-0432.CCR-15-1655doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2016/01/09/1078-0432.CCR-15-1655.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/22/12/2969.full#ref-list-1
This article cites 41 articles, 13 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/22/12/2969.full#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/22/12/2969To request permission to re-use all or part of this article, use this link
on April 12, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst January 11, 2016; DOI: 10.1158/1078-0432.CCR-15-1655