Embed Size (px)
Citation preview
Auditory-Visual Synesthesia
Sound-Induced Photisms
Lawrence Jacobs, MD; Alice Karpik, MD; Diana Bozian; Svend Gethgen, MD
• Nine patients with visual loss due tolesions of the optic nerve or chiasm expe-rienced photisms induced by sound.Descriptions of these varied from simpleflashes of white light to complicated col-orful hallucinations likened to a flame, apetal of oscillating lines, a kaleidoscope,or an ameba; they always appeared withina defective portion of the visual field asdemonstrated by perimetry. The provok-ing sounds were usually those of normaldaily life, ranged from soft to loud, andalways seemed to be heard by the earipsilateral to the eye in which the photismwas seen. Sound-induced photisms oc-curred under circumstances that wouldpromote a startle reaction to sound, andeach patient was startled when the pho-tisms occurred. Visual evoked responsesdemonstrated partial deafferentation ofthe eye in which photisms were seen inseven patients tested. The phenomenonmay occur when the patient with a partial-ly deafferent anterior visual pathway isstartled by sound.
(Arch Neural 1981;38:211-216)
Accepted for publication July 5. 1980.From the Harry M. Dent Neurologic Institute,
Millard Fillmore Hospital, Buffalo, NY (DrsJacobs and Gtrthgen and Ms Bozian), and theDepartments of Neurology (Drs Jacobs andG0thgen), Ophthalmology, and Physiology (DrJacobs), State University of New York, School ofMedicine at Buffalo. Dr Karpik was a student atthe State University of New York School ofMedicine at the time of this study; she is nowwith Rush-Presbyterian-St Luke's Hospital, Chi-cago.
Reprint requests to Harry M. Dent NeurologicInstitute, Millard Fillmore Hospital, 3 Gates Cir-cle, Buffalo, NY 14209 (Dr Jacobs).
rPhe inherent potential of the normalbrain for "cross-talk" between the
auditory and visual senses is demon-strated by rare, healthy individualswho sometimes see lights and colorswhen they hear certain sounds.' 'However, the occurrence of such audi-tory-visual synesthesias as a manifes-tation of disease of the CNS is notgenerally appreciated. We describenine patients with visual loss due tolesions of the anterior portions of thevisual pathways who experiencedsound-induced photisms, and we pre-sent data suggesting that the effectsof an acoustic startle reaction on apartially deafferent visual systemmay be important in the developmentof the phenomenon.
CLINICAL OBSERVATIONS
The cases are summarized in Table 1.The site of the lesion causing visual losswas the optic nerve in seven patients andthe optic chiasm in two patients. A definitediagnosis was made in every patientexcept in case 9. Mult iple sclerosis (MS)was diagnosed in three patients (cases 1 to3) who had clear histories of exacerbationsand remissions of disseminated neurologicdeficits prior to the onset of visual symp-toms associated with photisms. The pa-tients with^jVIS had unequivocally positivehot-bath tests" and visual evoked responses(VERs) consistent with demyelination.Each had elevated serum total protein con-tent, and two had elevations of y-globulinfraction in the CSF. Each patient with MSimproved with adrenocorticotropic hor-mone therapy. Tumors of the sella turci-ca-juxtasellar regions were diagnosed (bytomographic radiographs, angiography,
and computerized tomography [CT]) incases 4 and 5. Craniotomy revealed a tuber-culum sellae meningioma in case 5; thetumor type was unknown in patient 4, whorefused surgery. Temporal arteritis wasdiagnosed in cases 6 and 7 by elevatedESRs and examination of temporal arterybiopsy specimens. Patient 8 had beenamaurotic on the right side for 25 yearssince surgery for removal of neurofibromaat the orbital apex. Probable vascularocclusive optic neuropathy was diagnosedin patient 9, a chronically hypertensivewoman with atherosclerotic heart andperipheral arterial occlusive disease. Hercerebral angiogram revealed luminal nar-rowing and plaques of both cervical carotidarteries and right-sided intracavernouscarotid stenosis. Fluorescein angiographyrevealed narrowed retinal arterioles, butno definite arteriolar occlusion. The onsetof visual loss associated with photisms wassudden (seconds) in cases 8 and 9, over fourto seven days in cases 1 to 3, 6, and 7, andgradual (six months and two years) in cases4 and 5. The photisms were seen within oneto three days after the first symptom ofvisual loss in eight patients, the only excep-tion being patient 8, in whom photismswere first experienced three months afterthe onset of right-sided amaurosis. Thefirst photism experienced by each patientwas of the same degree of brightness assubsequent ones. There was no gradual"buildup" of photism intensity over time.Optic atrophy and Marcus Gunn pupillaryreactions were present in the eye in whichthe photisms were seen in seven patients.
Photisms
The most commonly described photismswere small to large Hashes of white light inthe scotoma (Table 2). The sounds of walls"crackling" as they cooled at night, an
Arch Neurol-Vol 38, April 1981 Auditory-Visual Synesthesia—Jacobs et al 211
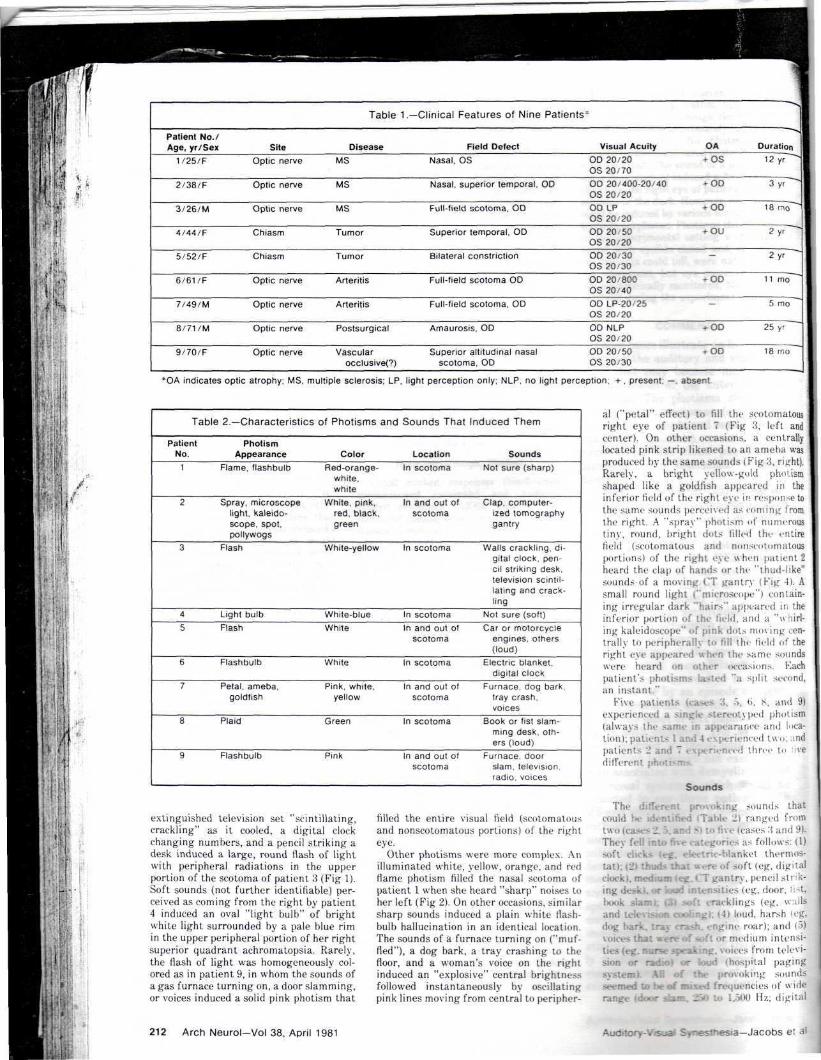
Table 1.— Clinical Features of Nine Patients* |
Patient No./Age, yr/Sex
1/25/F
2/38/F
3/26/M
4/44/F
5/52/F
6/61/F
7/49/M
8/71/M
9/70/F
SiteOptic nerve
Optic nerve
Optic nerve
Chiasm
Chiasm
Optic nerve
Optic nerve
Optic nerve
Optic nerve
DiseaseMS
MS
MS
Tumor
Tumor
Arteritis
Arteritis
Postsurgical
Vascularocclusive(?)
Field DefectNasal, OS
Nasal, superior temporal, OD
Full-field scotoma, OD
Superior temporal, OD
Bilateral constriction
Full-field scotoma OD
Full-field scotoma. OD
Amaurosis, OD
Superior altitudinal nasalscotoma, OD
Visual AcuityOD 20/20OS 20/70OD 20/400-20/40OS 20/20OD LPOS 20 20OD 20 50OS 20 20OD 20/30OS 20 30OD 20/800OS 20/40OD LP-20 25OS 20/20OD NLPOS 20/20OD 20/50OS 20/30
OA Duration-OS 12 yr
+ OD 3 yr ~
+ OD 18 rno~~~
+ OU 2 yr ~~
2 y r
-OD 11 mo""""
5 mo
f-OD 25 yr
-OD 18 mo
*OA indicates optic atrophy; MS, multiple sclerosis; LP, light perception only; NLP, no light perception; + , present; —, absent
Table 2.— Characteristics of Photisms and Sounds That Induced Them
PatientNo.
1
2
3
4
5
6
7
8
9
PhotismAppearance
Flame, flashbulb
Spray, microscopelight, kaleido-scope, spot,pollywogs
Flash
Light bulbFlash
Flashbulb
Petal, ameba,goldfish
Plaid
Flashbulb
ColorRed-orange-
white,white
White, pink,red, black,green
White-yellow
White-blueWhite
White
Pink, white,yellow
Green
Pink
LocationIn scotoma
In and out ofscotoma
In scotoma
In scotomaIn and out of
scotoma
In scotoma
In and out ofscotoma
In scotoma
In and out ofscotoma
SoundsNot sure (sharp)
Clap, computer-ized tomographygantry
Walls crackling, di-gital clock, pen-cil striking desk,television scintil-lating and crack-ling
Not sure (soft)Car or motorcycle
engines, others(loud)
Electric blanket,digital clock
Furnace, dog bark,tray crash,voices
Book or fist slam-ming desk, oth-ers (loud)
Furnace, doorslam, televisionradio, voices
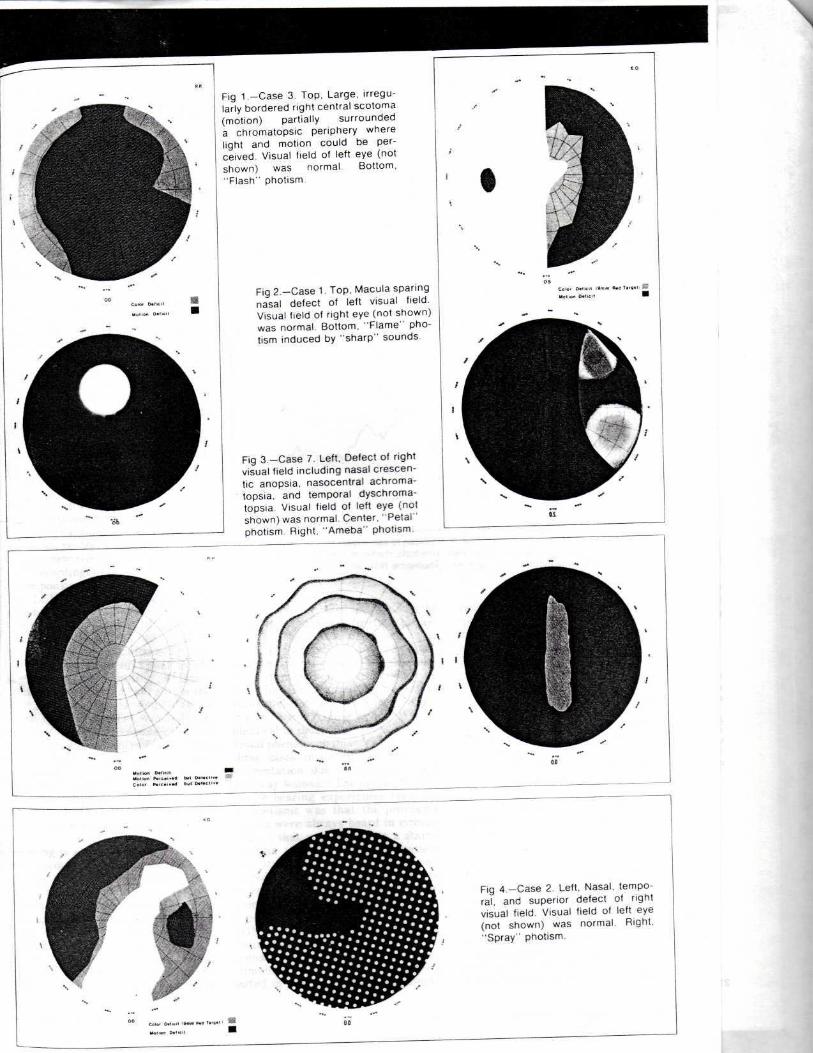
extinguished television set "scintillating,crackling" as it cooled, a digital clockchanging numbers, and a pencil striking adesk induced a large, round flash of lightwith peripheral radiations in the upperportion of the scotoma of patient 3 (Fig 1).Soft sounds (not further identifiable) per-ceived as coming from the right by patient4 induced an oval "light bulb" of brightwhite light surrounded by a pale blue rimin the upper peripheral portion of her rightsuperior quadrant achromatopsia. Rarely,the flash of light was homogeneously col-ored as in patient 9, in whom the sounds ofa gas furnace turning on, a door slamming,or voices induced a solid pink photism that
filled the entire visual field (scotomatousand nonscotomatous portions) of the righteye.
Other photisms were more complex. Anilluminated white, yellow, orange, and redflame photism filled the nasal scotoma ofpatient 1 when she heard "sharp" noises toher left (Fig 2). On other occasions, s imilarsharp sounds induced a plain whi te flash-bulb hal lucinat ion in an identical location.The sounds of a furnace turning on ("muf-fled"), a dog bark, a tray crashing to thefloor, and a woman's voice on the rightinduced an "explosive" central brightnessfollowed instantaneously by oscillatingpink lines moving from central to peripher-
al ("petal" effect) to fill the scotomatousright eye of pat ient ~ (Fig 3, l o f t andcenter). On other occasions, a centrallylocated pink strip likened to an ameba wasproduced by the same sounds (Fig 3, right).Rarely, a bright yellow-gold photismshaped l ike a goldfish appeared i n thei n f e r i o r f ield of the r ight eye in response tothe same sounds perceived as coming fromthe right. A "spray" pho t i sm of numeroust iny , round, bright dots f i l l ed the ent i refield (scotomatous and nonsrotomatousportions) of the right eye w h e n pat ient 2heard the clap of hands or the " thud- l i ke"sounds of a moving CT gantry (Fig 1). Asmall round light ("microscope") contain-ing irregular dark "hairs" appeared ir, theinferior portion of the f ie ld , and a "wii i r l -ing kaleidoscope" of pink dots nun ing cen-tral ly to per ipheral ly '.<> f i l l the f i e l d of theright eye appeared when the same soundswere heard on other occasions. Kachpatient's photisms lasted "a s p l i t second,an ins tant ."
Five patients ica.-k.-s 3. ^>, ti, 8. and 9)experienced a single stereotyped phot i sm(always the same in appearance and loca-tion); patients 1 and 4 experienced two; .indpatients 2 and 7 experienced three tn ' ived i f fe rent ph
Sounds
The different provoking sounds tha tcould U.- '. : -d iTable 2) ranged fromtwo (cases 2.5..-.- • • • (cases 3 and 9).They fell ir •trories as follows: (1)soft click? | Tic-blanket thermos-tat); (21 thuds that were uf soft (eg, digi talclock), medium (eg. CT gantry, penc i l s ink-ing desk), or loud intensities (eg, door, i^t,l>ook slam); -oft cracklings (eg. wallsand televi g -I > loud , harsh log,dog bark, tray crash, engine roar); and (o)
• lU 'd ium intensi-ties (eg. nurse lices from televi-
or loud (hospital pagingf the provoking sounds
seemed to be of mixed frequencies of widerange (door siam. 25o to 1..SOO Hz; d ig i ta l
212 Arch Neurol-Vol 38, April 1981 Auditory-Visual Synesttiesia—Jacobs e: al
N
Fig 1.—Case 3. Top, Large, irregu-larly bordered right central scotomamotion) partially surrounded
a chromatopsic periphery wherelight and motion could be per-ceived. Visual field of left eye (notshown) was normal. Bottom,'Flash" photism.
Fig 2.—Case 1. Top, Macula sparingnasal defect of left visual field.Visual field of right eye (not shown)was normal Bottom, "Flame" pho-tism induced by "sharp" sounds.
Fig 3.—Case 7. Left, Defect of rightvisual field including nasal crescen-tic anopsia, nasocentral achroma-topsia, and temporal dyschroma-topsia. Visual field of left eye (notshown) was normal. Center, "Petal"photism Right, "Ameba" photism.
Fig 4.—Case 2. Left, Nasal, tempo-ral, and superior defect of rightvisual field. Visual field of left eye(not shown) was normal. Right,"Spray" photism.
P
clock, walls or television crackling, 500 to2,000 Hz; dog bark or tray crash, 1,000 to2,000 Hz; voices, 1,000 to 3,000 Hz). Twopatients who could not identify any of theprovoking sounds described them as sharp(case 1) or soft (case 4). Patients 5 and 8,who could identify some but not all of theprovoking sounds, described those thatthey could not identify as loud.
The sounds inducing the photisms werealways reported as being heard from theside ipsilateral to the eye in which thephotism was seen. The click of an electricblanket thermostat induced a flashbulbphotism in the right eye of patient 6 onlywhen the thermostat located to her rightclicked; the same clicking from her hus-band's thermostat located to her left neverinduced the phenomenon. A petal photismwas perceived as coming from the right eyeof patient 7 when a nurse spoke into hisright ear. The photism never occurredwhen the nurse spoke into his left ear. Thefrequencies with which the photismsoccurred was from one to ten times pernight for between 1.5 and 11 months in fivepatients (cases 1, 2, 5 to 7), two times perweek for 18 months in one patient (case 3),five times during 18 months (approximate-ly once every three to four weeks) chang-ing to two to three per day during the nextsix months for patient 4, and three timesper year for 25 years for patient 8. Thephotisms disappeared in patient 7 afterfive months but have persisted in the otherpatients. In patients who saw more thanone photism, the same sound that induced agiven photism on one occasion mightinduce a different one on another occasion.The sound of a moving CT gantry mightinduce a spray photism in the right eye ofpatient 2 on one occasion and a microscopelight photism on another occasion. In allpatients, a given sound might induce aphotism on one occasion but fail to do so onnumerous other occasions.
Circumstances of the Photismsand Associated Phenomena
The conditions in which the photismsoccurred were similar in seven patients(cases 1 to 3, 5 to 7, and 9). They werealways relaxed, drowsy, or dozing in aquiet, dark or dimly i l luminated room withtheir eyes closed. The photisms occurredbetween the time they entered the darkand fell asleep; this period never exceededone hour. Photisms were not experiencedwhen they awakened later in the night.Patients 4 and 8 differed from the othersin that they experienced photisms in thelight (bright daylight, fluorescent or stan-dard room lighting) with their eyelidsopened and never experienced them in thedark. Patient 4 was relaxed (but not drow-sy) and patient 8 was "tense, anxious,concentrating" when sounds induced thephotisms.
Each patient was startled when the pho-tism occurred. Frequently, the startle wasassociated with a gross body jerk thatresulted in arousal from early sleep ordrowsiness. Patient 8 was certain that thesound had startled him. The others wereuncertain as to whether the sound or the
214 Arch Neurol-Vol 38, April 1981
photism had startled them. Each patientstated that the sound, the photism, and thestartle seemed to occur simultaneously.Patients 1, 2, 4, and 9 described the experi-ence as "seeing the sound on the inside oftheir eyelids."
Patients 1, 2, 4, and 7 saw spontaneous(not sound-induced) photisms in theinvolved eye as well as those induced bysound. Patient 7 began experiencing spon-taneous photisms at a time when vision inthe right eye had improved to near normaland sound-induced photisms were ceasing.They continued for one month after sound-induced photisms had ceased completely.In cases 1, 2, and 4, spontaneous photismsbegan at approximately the same time asthose induced by sounds and have contin-ued (approximately 20% as frequently asthose induced by sound). Spontaneous pho-tisms occurred under identical conditionsand were of similar characteristics as thoseinduced by sound. When spontaneous pho-tisms occurred, they were not related toeye movement, sudden lid closure, or anyother identifiable maneuver. Photismscould not be induced by tapping or applica-tion of a vibrating tuning fork to theorbital bone or globe (lids closed) or vigor-ous deviations of the eyes.
Neurophysiologic Studies
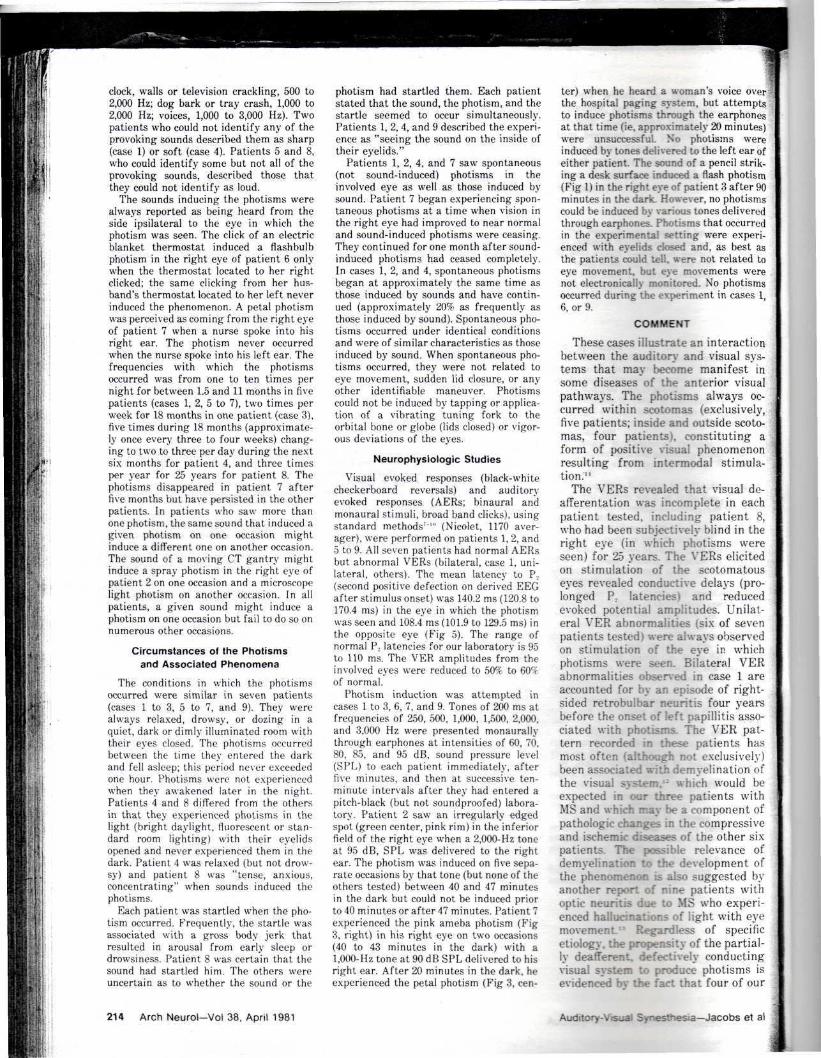
Visual evoked responses (black-whitecheckerboard reversals) and auditoryevoked responses (AERs; binaural andmonaural stimuli, broad band clicks), usingstandard methods7 '" (Nicolet, 1170 aver-ager), were performed on patients 1, 2, and5 to 9. All seven patients had normal AERsbut abnormal VERs (bilateral, case 1, uni-lateral, others). The mean latency to P,(second positive defection on derived EECafter stimulus onset) was 140.2 ms (120.8 to170.4 ms) in the eye in which the photismwas seen and 108.4 ms (101.9 to 129.5 ms) inthe opposite eye (Fig 5). The range ofnormal P, latencies for our laboratory is 95to 110 ms. The VER amplitudes from theinvolved eyes were reduced to 50% to 60%of normal.
Photism induction was attempted incases 1 to 3, 6, 7, and 9. Tones of 200 ms atfrequencies of 250, 500, 1,000, 1,500, 2,000,and 3,000 Hz were presented monaurallythrough earphones at intensities of 60, 70,80, 85, and 95 dB, sound pressure level(SPL) to each patient immediately, afterfive minutes, and then at successive ten-minute intervals after they had entered apitch-black (but not soundproofed) labora-tory. Patient 2 saw an irregularly edgedspot (green center, pink rim) in the inferiorfield of the right eye when a 2,000-Hz toneat 95 dB, SPL was delivered to the rightear. The photism was induced on five sepa-rate occasions by that tone (but none of theothers tested) between 40 and 47 minutesin the dark but could not be induced priorto 40 minutes or after 47 minutes. Patient 7experienced the pink ameba photism (Fig3, right) in his right eye on two occasions(40 to 43 minutes in the dark) with a1,000-Hz tone at 90 dB SPL delivered to hisright ear. After 20 minutes in the dark, heexperienced the petal photism (Fig 3, cen-
ter) when he heard a woman's voice over<!the hospital paging system, but attemptsto induce photisms through the earphonesat that time (ie, approximately 20 minutes)were unsuccessful. No photisms wereinduced by tones delivered to the left ear ofeither patient. The sound of a pencil strik-ing a desk surface induced a flash photism(Fig 1) in the right eye of patient 3 after 90minutes in the dark. However, no photismscould be induced by various tones deliveredthrough earphones. Photisms that occurredin the experimental setting were experi-enced with eyelids closed and, as best asthe patients could tell, were not related toeye movement, but eye movements werenot electronically monitored. No photismsoccurred during the experiment in cases 1,6, or 9.
COMMENT
These cases illustrate an interactionbetween the auditory and visual sys-tems that may become manifest insome diseases of the anterior visualpathways. The photisms always oc-curred within scotomas (exclusively,five patients; inside and outside scoto-mas, four patients), constituting aform of positive visual phenomenonresulting from intermodal stimula-tion."
The VERs revealed that visual de-afferentation was incomplete in eachpatient tested, including patient 8,who had been subjectively blind in theright eye (in which photisms wereseen) for 25 years. The VERs elicitedon stimulation of the scotomatouseyes revealed conductive delays (pro-longed P.. latencies) and reducedevoked potential amplitudes. Unilat-eral VER abnormalities (six of sevenpatients tested) were always observedon stimulation of the eye in whichphotisms were seen. Bilateral VERabnormalities observed in case 1 areaccounted for by an episode of right-sided retrobulbar neuritis four yearsbefore the onset of left papillitis asso-ciated with photisms. The VER pat-tern recorded in these patients hasmost often (although not exclusively)been associated with demyelination ofthe visual system.1- which would beexpected in our three patients withMS and which may be a component ofpathologic changes in the compressiveand ischemic diseases of the other sixpatients. The possible relevance ofdemyelination to the development ofthe phenomenon is also suggested byanother report of nine patients withoptic neuritis due to MS who experi-enced hallucinations of light with eyemovement_:: Regardless of specificetiology, the propensity of the partial-ly deafferent, defectively conductingvisual system to produce photisms isevidenced by the fact that four of our
Auditory-Visual Synesthesia—Jacobs et al
patients (three with the demonstratedVER abnormality) experienced spon-taneous as well as sound-induced pho-tisms.
Each patient had evidence of alesion involving the presynaptic por-tions of the third-order neuron (axonsof retinal ganglion cells) of the visualpathway. Partial deafferentation atthis site might produce a heightenedstate of excitation of the fourth-orderneuron (lateral geniculate nucleus[LGN]) since impulse and chemicaltrophic influences from the third-order neuron on the LGN would stillbe partially intact (albeit reduced).The LGN supersensitivity might par-ticularly be expected in purely or pre-dominantly demyelinating lesionswith axons left intact. Supersensitivestates of postjunctional elements fol-lowing partial deafferentation havebeen demonstrated in the autonomicand peripheral nervous systems andthe CNS (including visual).14-" Partialrather than complete deafferentationhas been stressed as the necessaryelement for the development of suchpostjunctional supersensitivity."' •"'The anatomic basis of the supersensi-tivity may be sprouting of preservedelements, which has been observed inmany instances of partially deaffer-ent postsynaptic elements."'JS In suchinstances, postsynaptic elements maydevelop new receptive fields (intracel-lular recordings) that are heightenedin responsiveness to novel inputs."1
The LGN is normally responsive tosounds as well as visual stimuli. Soundstimuli elicit transient discharges thatcan be recorded from the LGN ofnormal experimental animals.27""' Par-tial deafferentation of visual inputsmight result in sprouting of intactsound-responsive elements within theLGN, heightening its sensitivity tosound to the point that sounds begininducing threshold responses for vi-sion, resulting in photisms. The reti-notopic map is near-perfectly pre-served in the LGN (l ikened' to an"internal retina").-5 "1 J Partiallydeafferent retinal axons correspond"-ing to the scotoma plotted by perime-try would be the most sensitive com-ponents (lowest thresholds for re-sponding to sound) of the LGN, whichmay account for the occurrence ofsound-induced photisms within scoto-mas. The colliculus superior (anotherfourth-order neuron for vision) mightalso become Supersensitive in thestate of partial deafferentation de-scribed. This nucleus is also normallyresponsive to sounds and has retino-topic organization, but its role in thegenesis of sound-induced photisms
1uV
0050 ms
Fig 5.—Visual evoked responses of patient 9; P. latency is prolonged (170.4 ms) followingstimulation of right eye in which photisms were seen, but normal (104.1 ms) followingstimulation of left eye. Th~fc VER amplitude from right eye is diminished due to patient'sright scotoma.
uides and fields of these discharges(pontogeniculo-occipital spikes) in-duced by startling sounds in mon-keys."' The exaggerated startling ef-fect on an already Supersensitive LGNmay be the critical element resultingin a threshold discharge for vision on asound stimulus that produces pho-tisms. The briefness of the sound-induced photisms and their tendencyto habituate (subjectively reported byall patients, experimentally demon-strated in cases 2 and 7) are featuresthat the phenomenon shares with thestartle reaction to sound." ' 7 1 S
The startle reaction also results inabrupt eyelid blinking and deviationof the eyes toward the offendingsound, both of which might inducephotisms. However, we were unable toinduce photisms by forced bl inking,eyelid closures, globe-orbit tapping, oreye movement at any time, includingthe period when photisms were beinginduced experimentally by soundsdelivered through earphones.
The requirement for the sound to beheard by the ear ipsilateral to the eyein which photisms were seen (subjec-
seems unlikely because, unlike theLGN, it has no direct cortical projec-tions in the primate." '-'
There was nothing unusual aboutthe sounds that induced the photisms;most were sounds that are encoun-tered in daily l i fe , and some (electric-blanket click, dog bark, furnace turn-ing on, house cooling at night) wereidentical to those that induced similarvisual phenomena in another report ofthree cases involving unilateral de-afferentation due to anterior visualpathway lesions.1' The unique featureof the hearing experiences resultingin photisms was that the provokingsounds were always heard in circum-stances that would promote a startlereaction to sound, and each patientwas startled when the photism oc-curred. The startle reaction may beextremely important in the genesis ofsound-induced photisms, since it pro-duces a sudden, brief discharge in theLGN as well as other portions of thevisual system that are normally re-sponsive to sound as well as visualstimuli.14-''1 Visual deafferentation re-sulted in dramatic increase in ampli-
Arch Neurol-Vol 38, April 1981 Auditory-Visual Synesthesia—Jacobs et al 215
;*"n
tively reported by all patients, experi-mentally demonstrated in cases 2 and6) cannot be adequately explained.Responsiveness to auditory stimulifrom either side would be expectedbecause nasal retinal fibers from oneeye (involved in scotomas of sevenpatients) are represented in the con-tralateral LGN, and auditory inputsare bilaterally represented in thebrainstem reticular formation.
The physiologic basis of sound-induced photisms experienced in otherpathologic states (eg, congenitallyblind, drug intoxication) may beentirely different from that sug-
gested for unilateral partial deaffer-entation of the anterior visual path-way. The numerous regions of thebrain where visual and auditory path-ways lay in close anatomic proximityand on which postsynaptic fibers fromthe two systems converge might serveas substrates for the synesthesia inthose cases."
Sound-induced photisms do not ap-pear to be unusually rare in patientswith lesions of the anterior visualpathways. The phenomenon was expe-rienced by the last seven of 20patients with optic nerve lesions andtwo of nine patients with optic chiasm
lesions whom we have examined.However, such patients must be spe-cifically questioned about the symp-tom because, like patients with cer-tain other forms of auditory andvisual positive phenomena/""" theyoften do not spontaneously report thesymptom.
This research was supported by grants fromthe Delaware North Corporation and the HarryM. Dent Family Foundation. Buffalo, NY.
Werner Noeli, MD. PhD. of the State Universi-ty of New York at Buffalo, reviewed the manu-script and provided valuable constructive criti-cism.
References
IK;
1. Colman WS: Further remarks on 'colourhearing.' Lancet 1898;l:22-24.
2. Ortman 0: Theories of synesthesia in thelight of a case of color-hearing. Hum Bio!1933;5:155-211.
3. Dudycha GJ, Dudycha MM: A case of synes-thesia: Visual-pain and visual-audit ion. -/ Ab-norm Sot Psychol 1935;30:57-69.
4. Duke-Elder S, Scott GI: Neuro-ophthalmoio-gy. vol 12, in Duke-Elder S (ed): System of Oph-thalmology. St Louis, CV Mosby Co, 1971, pp571-573.
5. Critchley M: Ecstatic and synaesthetic expe-riences during musical perception, in CritchleyM, Henson RA (eds): Music and the BrainSpringfield, 111, Charles C Thomas Publisher,1977, pp 217-232.
6. Davis FA: The hot bath test in the diagnosisof mul t ip le sclerosis, in Bender MB, Feldman M(eds}: The Approach to Diagnosis in ModernNeurology. New York. Grune & Stratton Inc,1967, pp 80-82.
7. Starr A, Anchor LJ: Auditory brain stemresponses in neurological disease. Arch Neural1975:32:761-768.
8. Operating Manual for Ca-1000 ClinicalAverager System in Audiometry and Neurologi-cal Applications. Madison, Wis, Nicolet Instru-ment Corp, 1977.
9. Operating Manual for Ca-1000 ClinicalAverager System in Visual Evoked ResponseApplication. Madison, Wis, Nicolet InstrumentCorp, 1978.
10. Hall iday AM, McDonald WI, M u s k i n J:Visual evoked response in multiple sclerosis. BrMeil J 1973;4:661-664.
11. Taylor J (ed): Selected Writings of JohnHuyhlings Jac!:son. New York, Basic Books Inc,1958, vol 2, pp 16-27.
12. Halliday AM, McDonald WI, M u s k i n J:Visual evoked potentials in patients with demye-iinating disease, in Desmedt JE (ed): VisualEvoked Potentials in Man: New Developments.Oxford, England, Clarendon Press, 1977, pp 438-449.
13. Davis FA, Bergen D, Schauf C, et al:Movement phosphenes in optic neuritis: A newclinical sign. Neurology 1976;26:1100-1104.
14. Echiin FA, McDonald J: The supersensitiv-ity of chronically isolated and partially isolatedcerebral cortex as a mechanism in focal cortical
epilepsy. Trans Am Neural Assoc 1954;79:75-79.15. Burke W, Haylow WR: Disuse in the lateral
geniculate nucleus of the cat. J Physiol 1968;194:495-519.
16. Sharpless SK: Isolated and deafferentedneurons: Disuse supersensitivity, in Jasper HH,Ward AA, Pope A (eds): Basic Mechanisms of theEpilepsies. Boston, Little Brown & Co, 1969, pp329-348.
17. Ward AA: The epileptic neuron: Chronicfoci in animals and man, in Jasper HH, Ward AA,Pope A (ed): Basic Mechanisms of the Epilepsies.Boston, Little Brown & Co, 1969, pp 263-288.
18. Roper S, Ko CP: Synaptic remodeling inthe partially denervated ganglion in the heart ofthe frog, in Cotman CW (ed): Neuronal Plastici-ty. New York, Raven Press, 1978, pp 1-23.
19. Merril EG, Wall PD: Plasticity of connec-tion in the adult nervous system, in Cotman CW(ed): Neuronal Plasticity. New York, RavenPress, 1978, pp 97-111.
20. Stavarsky G: Supersensitirity FollowingLesions of the Nervous System. Toronto, Univer-sity of Toronto Press, 1961.
21. Weisel TN, Hubel DH: Single cell responsesin the striate cortex of kittens deprived of visionin one eye. J Neruophysiol 1963;26:1003-1017.
22. Liu CN, Chambers WW: Intraspinalsprouting of dorsal root axons: Development ofnew collaterals and preterminals" following par-tial denervation of the spinal cord in the cat.Arch Neural 1958;79:46-61.
23. Cunningham TJ: Sprouting of the opticprojections after cortical lesions. Auat Rec1972;172:298.
24. Goodman DG, Horel JA: Sprouting of theoptic tract projections in the brain stem of therat. ./ Comp Neural 1966;127:71-83.
25. Nakamura Y, Mizunn N, Koneski A:Synaptic reorganization of the red nucleus afterchronic deafferentation from cerebellorubralfibers. Brain Res 1974;82:293-301.
26. Edds MV Jr: Collateral nerve regeneration.Q Rev Biol 1953:28:260-276.
27. Arden GB, Soderberg U: The relationshipof lateral geniculate activity to the electrocortico-gram in the presence or absence of the optic tractinput . Enperientia 1959:15:163-164.
28. Duke-Elder S, Weale RA: The Physiology ofthe Eye and of Vision, vol 4, in Duke-Elder S (ed):System of Ophthalmology. St Louis, CV Mosby Co,
1968, pp 516-534.29. Cohen B, Feldman M: Relationship of elec-
trical activity in pontine reticular formation andlateral geniculate body to rapid eye movements.J Neurophysiol 1968;3"l:806-817.
30. Feldman M, Cohen B: Electrical activity inthe lateral geniculate body of the alert monkeyassociated with eye movements. J Neurophysiol1968:31:455-466.
31. Singer W: Control of thalamic transmis-sion by corticofugal and ascending reticular path-ways in the visual system. Physiol Rev 1977:57:386-420.
32. Duke-Elder S. Wybar KC: The Anatomy ufthe Visual System, vol 2, in Duke-Elder S (ed):System of Ophthalmology. St Louis, CV Mosby Co,1968, pp 698-701.
33. Lassell S, Cohen MM: Phosphenes inducedby sound. Neurology 1979:29:1524-1527.
34. Bizzi E, Brooks DC: Functional connectionsbetween pontine reticular formation and lateralgeniculate nucleus during sleep. Arch Hal fiiol1963;101:666-680.
35. Gogan P: The startle and orienting reac-tions in man: A study of their characterise ics andhabituation. Braid Res 1970:18:117-135.
36. Sem-Jacobsen CW: Sudden alarming noisieffect on brain func t ions and EEC changes. At -InOtorhinularyngol Belg 197125:218-220.
37. Groves PM, Wilson CH, Boyle RD: Brain-stem pathways, cortical modulation, and hab i tua -tion of the acoustic startle response. Behnr B/ol1974:10:391-418.
38. Bowker RM. Morrison AR: The startlereflex and PGO spikes. Brain Res 1976:102:185-190.
39. Feidman M. Cohen B: Eye movementresponses in the calcarine cortex after re t inalablation. Physiologist 1967:10:168.
40. Bender MB. Feldman M. Sobin AJ: Pahnopsia. Brain 196851:321-338.
41. Jacobs L, Feldman M. Bender MB: P a l i n a -eousis or persistent auditory sensations. TrimsAm Neurol Asa, 1971:96:123-126.
42. Jacobs L. Feldman M. Bender Mt i : Thepersistence of visual and auditory percepts assymptoms of irritative lesions of the cerebrum ofman. Z Ncurnl 1972:1 l-l
43. Jacobs L. Feldman M. Diamond SP, et al:Palinacousis: Persistent or recurring auditorysensations. Cortti 19735:275-287.
216 Arch Neurol—Vol 38, April 1981 Auditory-Visual Synesthesia—Jacobs et al