Embed Size (px)
Citation preview

J Neurol (2001) 248 : 676–683© Steinkopff Verlag 2001 ORIGINAL COMMUNICATION
Knut WesterDexter R. F. IrvineKenneth Hugdahl
Auditory laterality and attentional deficits after thalamic haemorrhage
JON
494
Introduction
It is well-known that thalamic lesions may cause severeneuropsychological dysfunction [14, 37]. Language andmemory disorders are most frequently reported in theliterature [1, 8, 10, 20, 24–26, 28, 31–33], but cases of inat-tention [38], neglect [15], and “thought disorder” [6]have also been reported. While language and verbal
memory deficits are commonly found after left-sided le-sions, disorders of non-verbal memory are typicallyfound after right-sided lesions (e. g. Stuss et al. [37]; seealso Ojemann [29, 30] using electrical stimulation ofthalamic nuclei). Thus, it is commonly believed thatthalamic nuclei are functionally organized in a way likethat of the left and right cortex (cf. Crosson [9]).
Many studies have reported cognitive deficits afterlesions in anterior and dorsomedial thalamic nuclei (see
Received: 27 October 2000Received in revised form: 23 January 2001Accepted: 19 February 2001
K. Wester (�)Department of NeurosurgeryHaukeland University Hospital5021 Bergen, Norway.Tel.: +47-55 97-50 00Fax: +47-55 97-56 99e-mail: [email protected]
D. R. F. IrvineDepartment of PsychologyMonash UniversityVictoria 3800, Australia
K. HugdahlDepartment of Biological and Medical PsychologyUniversity of BergenÅrstadvn 215009 Bergen, Norway
The present research was financiallysupported by a grant to Knut Wester andKenneth Hugdahl from the NorwegianResearch Council – Medical ResearchDivision.
■ Abstract Thalamic lesions havebeen shown to produce severe cog-nitive deficits involving languageand memory. A majority of thestudies have reported cognitivedeficits after lesions in the anteriorand dorsomedial thalamic nuclei.We report five case studies of ef-fects on language processing afterpostero-dorsal thalamic haemor-rhages. Four of the patients hadlesions on the right side, and onepatient had a lesion on the left side.Effects on language processingwere investigated with the dichoticlistening test with consonant-vowelsyllables. This test, in which con-flicting auditory stimuli are pre-sented simultaneously to the twoears, has been used to probe diffe-rences in language processing inthe left and right hemispheres. Thefour patients with right-sided le-sions reported almost none of thesyllables presented to the left ear,and were unable to modify thismassive right ear advantage bydirecting attention to the left or
right ear. The patient with a left-sided lesion showed a weaker leftear advantage, and was able tomodify his responses by shiftingattention, to an extent similar tothat of healthy reference individu-als. When tested with monauralstimulus presentation, the scores ofall patients rose to almost 100 %correct for each ear. The pattern ofeffects with dichotic stimuli underdifferent instructional conditionscannot be accounted for in purelystructural terms, and indicates thatlesions in the posterior part of thethalamus, including the pulvinarnucleus and medial geniculatebody, produce deficits not only inprocessing of complex auditorystimuli but also in the allocation ofattention to input from one ear orthe other.
■ Key words Attentional deficit ·Auditory pathways · Dichoticlistening · Thalamic haemorrhage ·Verbal perception

677
Stuss et al. [37]), while fewer studies have reported cog-nitive deficits after lesions affecting the posterior, par-ticularly the postero-dorsal, region of the thalamus, in-cluding the medial geniculate body (cf. Peru & Fabbro[33]; see also Fabbro & Paradis [11]). In a previous casestudy [19], we reported on a surprising “neglect” effectin a young male patient with a small circumscribed le-sion in the right pulvinar region, which is part of thepostero-dorsal thalamus. When exposed to differentacoustic stimuli, simultaneously presented in the twoears (“dichotic listening”), he failed almost completelyto report consonant-vowel syllables presented to the leftear, while his right ear performance was much betterthan normally found in intact individuals in the samesituation (cf. Hugdahl 1995 [18]). Moreover, he was un-able to modify this pronounced right ear advantage(REA) when specifically instructed to attend to the leftor right ear. His hearing was normal when tested withstandard screening audiometry, and when testedmonaurally,his left ear scores rose to above 80 % correct.We labelled this particular effect as due to “auditoryhemispatial extinction” and suggested that the pulvinarnucleus may play a critical role in gating or tuning audi-tory input to the cortex (cf. Bhatnagar et al. [3]).
The aim of the present study was therefore to expandon the original findings of the previous case study. Wereport dichotic listening performance to consonant-vowel (CV)-syllables in five patients with circumscribedlesions involving the same dorsal posterior thalamic re-gion, including portions of the pulvinar and medialgeniculate nuclei. Four of the patients had a right-sidedhaemorrhage, while the fifth had a similar lesion on theleft side. The data are reported as five case studies, andcompared with dichotic listening performance in fivehealthy intact individuals within the same age range asthe patients, matched for handedness and gender.
Patients and methods
■ Patients
The patients were five males admitted to the department of neuro-surgery with a discrete lesion affecting right (4 patients) or left (1pa-tient) postero-dorsal thalamic regions, including the medial genicu-late body. In one patient the lesion was of traumatic origin. In theother four, the lesion was caused by a spontaneous intracerebralhaemorrhage. They were all right-handed, as determined from a Nor-wegian translation of the handedness questionnaire constructed byRaczkowzki et al. [35]. The questionnaire consists of 15 items of man-ual/pedal activities for which the subject has to indicate hand/footpreference. Four of the patients indicated 15/15 items as preferredwith the right hand/foot, and one patient indicated 14/15 items. Threeof the patients were tested in an acute stage (2–10 days) after a spon-taneous haemorrhage, while two patients were tested in a chronicstage (see below).All the patients gave their informed consent to par-ticipate in the study.
Case 1
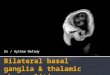
The patient was a 13-year-old boy who was admitted to the hospitalafter having experienced an acute right-sided headache.After a while,he felt a numbness in the left side of the body and face, without a mo-tor deficit. Immediate CT showed a haemorrhage in the right postero-dorsal thalamus with a diameter of 15–20 mm (Fig. 1). The lesion af-fected mainly the medial geniculate body as well as the medial andlateral subdivisions of the pulvinar nucleus [36]. Further radiologicalexamination (MRI) failed to disclose any vascular malformations. Itwas therefore assumed that the bleeding source had been a cavernoushaemangioma that was destroyed by the haemorrhage. He was fullyawake during the stay in our hospital, and was tested in the dichoticlistening test 2 days after the incident.
Case 2
The patient was a 70-year-old man who suddenly noticed weaknessin his left leg and arm, without losing consciousness. He was admit-ted to the hospital a few hours later, still with a moderate paresis inhis left extremities, and a reduced sensibility in the left side of the faceand body. CT showed a haemorrhage involving large portions of theposterior right thalamus, but also extending into more anterior por-tions of the thalamic complex (Fig. 2). The diameter was ca. 25 mm,and it apparently affected the right internal capsule in addition to thepulvinar and the dorsal thalamic nuclei [36]. His consciousness re-mained unaffected, and he was tested with dichotic listening 10 daysafter the incident.
Case 3
The patient was a 22-year-old man who was admitted to our hospital4 years after he sustained a severe head injury in a car accident. Ini-tially, he was unconscious for 10 days, and had a pronounced lefthemiparesis that gradually subsided, but was replaced by a severe in-tentional ataxia in the left arm. He was referred to our department be-cause of this ataxia, and he was later, i. e. after being tested in the di-
Fig. 1 Case 1. Axial CT scan showing an acute, discrete haemorrhagic lesion in theright posterodorsal thalamus.

678
chotic listening test, successfully treated with a thalamotomy. CT andMRI showed a small lesion in the right postero-dorsal thalamus(Fig. 3), as well as minor areas of contusion in the right frontal lobe.The thalamic lesions were confined to the pulvinar nucleus and the
medial geniculate body [36]. This patient was the one reported inHugdahl et al. [19].
Case 4
The patient was a 68-year-old man who, following a physical strain,suddenly noticed a numbness in the left side. Initially, he also hadslight ataxia of his left leg and arm, but his consciousness was undis-turbed. He was admitted to a local hospital after a few hours, still witha reduced sensibility in the left side of the face and body. CT showeda small haemorrhage in the right postero-dorsal thalamus with a di-ameter of approximately 10 mm, later confirmed by MRI (Fig. 4). Thethalamic lesions seemed to be confined to the pulvinar nucleus andthe medial geniculate body [36]. He was transferred to our hospital toinvestigate possible causes. A vascular malformation was not found.His consciousness remained unaffected, but the numbness in the leftside persisted when he was tested with the dichotic listening test 10days after the incident.
Case 5
The patient was a 23-year-old man who was admitted to our hospital7 months after he sustained an acute, spontaneous haemorrhage froma small vascular malformation in the pulvinar region of the left thal-amus. Fig. 5 shows the MRI appearances shortly after the haemor-rhage. The thalamic lesion was confined to the pulvinar nucleus andpossibly also the medial geniculate body [36].This patient and his re-sults in the dichotic listening test has previously been reported inHugdahl and Wester [17] as a case study.
In addition to comparing between right- and left-lesions, the pa-tients were also compared with five healthy intact subjects randomlypicked from the dichotic listening data pool (n = 692) compiled byHugdahl [18], matched for age and handedness.
■ Acoustic stimuli and apparatus
The dichotic stimuli consisted of the six stop consonants paired withthe vowel /a/ to form six consonant-vowel syllables (ba, da, ga, pa, ta,ka). The syllables were paired with each other in all possible combi-nations, thus giving 36 different syllable pairs. The 36 dichotic pairswere recorded three times on tape with three different randomisa-tions, for each attentional instruction. The tape was played from aSony Walkman WMDD-II with plug-in type mini headphones. Theoutput from the cassette player was calibrated at a level of 75 dB (A).All subjects were tested for monaural hearing acuity with standardscreening audiometry for frequencies between 500 and 6000 Hz insteps of 1000 Hz.
■ Procedure
Four patients were tested bedside in the neurosurgery or neurologydepartment where they had been admitted. The testing situation wasmade as undisturbed as possible, with the test person sitting besidethe patient as the only two persons in the room, and with the cassetteplayer on a small table beside the bed. The fifth patient was tested inan examination room in the neurosurgery department.
Each patient was first informed about the dichotic listening pro-cedure, and told that he would hear different “sounds”, like “pa”,“da”etc. He was also shown all six syllables on a sheet of paper, and askedto read them aloud, in order to familiarise him with the sounds. Thetransducers were put in place and fastened with surgical tape to theear. Each patient was given a few practice trials before the test properbegan.
There were three different dichotic listening sessions, with diffe-rent instructions on how to focus attention. In the first session, thesubjects were simply told they would be presented with a list ofCV-syllables. Thus no specific instruction regarding attention was
Fig. 2 Case 2. Axial CT scan showing the maximal extent of an acute haemorrhagiclesion in the right thalamus.
Fig. 3 Case 3. Axial CT scan 4 years after the head injury, showing a discrete areaof low attenuation in the right posterodorsal thalamus.

679
presented. This session is called the Non-Forced (NF) attention con-dition. The subject’s task was to answer with the syllable he heard oneach trial. Thus, the instruction emphasised one response for eachtrial, even though the subject may have perceived both syllables onsome trials. This was done to eliminate the risk of artificial change inear-advantages due to comparison of double-responses against singleresponse trials.During the Forced-Right (FR) attentional test, the sub-jects were told to pay close attention to only the right ear syllables,andonly to report what they heard in the right ear. During the Forced-Left(FL) attentional test, the subjects were conversely told to pay close at-tention to the left ear syllables, and only to report what they heard inthe left ear. A fourth condition involved monaural listening, with the
same CV-syllables presented to only one ear at a time for 36 ran-domised presentations.
■ Data scoring and presentation
The data were scored as number of correctly reported syllables, fromthe left and right ears, respectively, excluding the 6 homonymic pairsfrom the data analysis. The typical finding in healthy individuals isthat of more correct syllables being reported from the right ear thanfrom the left ear, i. e. a right ear advantage (REA).An opposite patternof reports is called a left ear advantage (LEA). In order to facilitatecomparisons between different studies, and laboratories, the rawscores were converted to percentage scores in the figures and tables.The data are presented for each patient separately.
Results
Fig. 6 shows the number of correctly reported syllablesfrom the right and left ear, respectively, for each patient.
As can be seen in Fig. 6, the four patients with lesionsin the right thalamus (Case #1–4) showed a marked rightear advantage (REA) for all three attentional conditions.The percentage of correctly reported syllables from theright ear was on the average around 80 %, which is wellabove the right ear score for the healthy controls (Fig. 7).The corresponding figure for the left ear syllables wasabnormally low, around 10 %. Thus, all four patientsshowed a huge REA of the order of 60–70 %. As can alsobe seen in Fig. 6, the four patients with right-sided le-sions were unable to modify their ear scores as a resultof shifting attention to either ear, i. e. the REA remainedat the same magnitude for all three attentional condi-tions.
The results for the four patients with lesions in theright thalamus are clearly different from those of thesingle patient with a left-sided lesion (case 5). As can be
Fig. 4 Case 4. Axial and sagittal MRI scans showing an acute, discrete haemorrhagic lesion in the right thalamus, just rostral to the meso-diencephalic junction.
Fig. 5 Case 5. Axial MRI scan 3 weeks after the acute intrathalamic haemorrhage,showing a discrete haemorrhagic lesion in the left pulvinar region.

680
seen in Fig. 6 (lower panel), this patient showed a left earadvantage (LEA) during the NF attention condition,which changed to a slight REA during the FR attentioncondition, and reverted to a large LEA during the FL at-tention condition. Unlike the patients with right-sidedlesions, he was able to use attention to modify his per-formance.
The performance of the patients was compared withthe performance of five healthy intact subjects matchedfor handedness, gender and age (Fig. 7). The healthysubjects showed an expected REA during the NF and FRattention conditions, and a similarly expected LEA dur-ing the FL attention condition (see Hugdahl [18] fornorms). Comparing the results for the five healthy sub-jects with the patients revealed that the patients showedmore correct reports for the ear ipsilateral to the dam-aged side (the ipsilesional ear) than with the same sidefor the reference subjects. This was particularly evidentfor the four patients with right-sided lesions, who had aREA several times larger than the REA in the referencegroup,a difference that was significant for the NF and FL
Fig. 6 Dichotic listening performance (% correct reports) in the five patients. NF =Non-forced attention, FR = Forced right attention, FL = Forced left attention.

681
conditions when comparing the ear difference betweenthe groups (F(2,14) = 6.035, p < 0.02).
A final comparison involved only monaural stimuluspresentations, with the left or right transducer removed,but with the same CV-syllables (Figures 6 and 7, far rightbars). In this monaural test, all subjects had between 85and 100 % correct responses from both ears, and therewas little difference between the patients and the refer-ence group, or between the patients with lesions in theright or the left thalamus. It is interesting to note theslight ear asymmetry also for the monaural input,favouring the right ear both in the patients and the con-trol individuals.
Discussion
When presented with conflicting dichotic auditorystimuli, the four patients with right thalamic lesionsidentified correctly almost all the auditory stimuli pre-sented to the right (ipsilesional) ear, but not those pre-sented to the left (contralesional) ear. However, the pa-tients showed a near-perfect identification from bothears when the stimuli were presented monaurally.Unlikenormal individuals, these patients were unable to mod-ify their extreme REA by shifting attention to the left earwhen instructed to do so. The results for the single pa-tient with a lesion in the left thalamus were less clear. Healso exhibited near-perfect performance with syllablespresented monaurally to either ear, but he was clearlyable to identify auditory stimuli from both ears whenstimulated dichotically. However, he showed a consider-ably weaker ipsilesional ear advantage than the patientswith right thalamic lesions. Unlike the patients with
right lesions, but similar to healthy subjects, he was alsoable to modify his responses by directing attention toone ear or the other.
The basic question raised by this pattern of results iswhether they reflect lesion-produced changes solely ineither attentional or in complex auditory/speech pro-cessing mechanisms, or in some combination of the two.If dichotic listening phenomena in general reflect dif-ferential allocation of attention to input from one or theother ear when these inputs are different, a simple inter-pretation of the pattern of effects in healthy right-handed subjects would be that normally (i. e., in the NF-attention condition) there is a right-ear bias, in thatgreater attention is allocated to input from the right ear,but that the relative allocation of attentional resourcescan be partially modulated (e. g., in response to instruc-tions, as in the FR and FL attention conditions). On thisview, the fact that the REA of all four right-lesion pa-tients in the NF condition was substantially (and signif-icantly) greater than that of healthy subjects, and wasnot affected by instructions to focus attention on eitherear,could be interpreted as indicating that the lesion hadresulted in a massive reduction in the ability to allocateor shift attentional resources to the left (contralesional)ear. That the patients simply were unable to follow in-structions, is not very likely, as all the patients were alertand followed all other instructions well.
The observed pattern of effects therefore suggeststhat the nuclei in the postero-dorsal thalamus affectedby the lesions (or the regions to which they project) playa critical role in allowing attention to be differentially al-located between the two ears. Given the known connec-tions between the pulvinar and the parietal lobe [2, 27],it would seem likely that the pulvinar is the relevantstructure here, but the possibility that the magnocellu-lar or other divisions of the medial geniculate bodymight be involved cannot be excluded.
This argument cannot, however, be applied so readilyto the results for the single patient with a left thalamic le-sion.Although the LEA exhibited by this patient could re-flect a reduced ability to direct attention to the contrale-sional (right) ear, this bias was much less extreme thanthe REA of the right-lesion patients. Contrary to the pa-tients with right thalamic lesions, this patient retained anear-normal ability to modulate the relative allocation ofattention to the two ears. Interpretation of this differentpattern of effects is, however, qualified by the fact thatonly one left lesion patient was studied. The differencebetween the right- and left-lesioned patients could re-flect a true laterality difference, and would then implythat the right postero-dorsal thalamus plays a much moreimportant role in the differential allocation of attentionto input from the two ears than does the left.However,thedifference might also simply be attributable to diffe-rences in the extent and/or location of lesions in theright-lesion patients and in the single left-lesion patient.
Fig. 7 Dichotic listening performance in five healthy intact subjects who wereage-, and handedness matched to the five patients. The intact reference subjectswere drawn at random from the pool of subjects (n = 692) studied by Hugdahl(1995).

682
Alternatively, it is possible that the differences be-tween the effects of left and right thalamic lesions mightreflect different sensory processing deficits. Tradition-ally, the REA exhibited by healthy right-handed subjectshas been attributed to specialisation of the left hemi-sphere for the processing of verbal (or, more generally,complex acoustic) stimuli and some form of preferentialaccess of right ear input to the left hemisphere (see, e. g.,Geffen and Quinn [12] and Bryden [5] for reviews). Thenature of this preferential access remains unclear.Kimura’s [22] original structural model in terms ofstronger contralateral projections to the auditory cortexin a given hemisphere and suppression of ipsilateralpathways is not compatible with more recent neuro-physiological data (see e. g., Phillips and Gates [34] andGeffen and Quinn [12] for discussion). Auditory cortexin a given hemisphere does, however, contain a strongerexcitatory representation of input from the contralateralear and, as a consequence of binaural interactions, a rep-resentation predominantly of contralateral auditoryspatial locations (e. g., Brugge and Reale [4]; Clarey et al.[7]).These asymmetries are set up in the brain stem,andthus are also present at the level of the midbrain andthalamus (see e. g., Glendenning et al. [13]; Irvine [21];Clarey et al. [7]). Furthermore, recent electrophysiolog-ical evidence has also indicated an asymmetry in the re-sponses of the MGB to complex acoustic stimuli, includ-ing speech sounds, in animals [23].The pattern of effectsexhibited by right- and left-lesion patients in the NF at-tention condition is basically the same as that seen aftertemporal lobe lesions in right-handed patients, i. e.,right damage leads to a deficit on the left ear, resultingin an exaggerated REA, while left damage leads to a
deficit on the right ear, which yields an overall LEA (seeBryden [5] for review).
However, while a purely structural model could ac-count for the difference between right- and left-lesioneffects in the NF attention condition, a modified struc-tural account incorporating the effects of directed atten-tion would be necessary to account for the modulationof the left-lesion patient’s performance in the forced at-tention conditions (FR and FL), a modulation that wasof similar magnitude to that seen in healthy subjects.Even this modified model does not explain why the REAin the right lesion cases remained unmodulated by at-tention (i. e., in the FR and FL attention conditions). Aswith the purely attentional account developed earlier,this difference seems to require the conclusion that right(but not left) postero-dorsal thalamic lesions interferewith the mechanisms that allow attention to be allocatedto input from one ear to another. Although our findingsrelate to the auditory modality, they appear similar to re-sults obtained in the study of visual neglect [16, 27]. Forthe visual modality, the right hemisphere seems capableof directing attention to both half-fields, whereas the lefthemisphere only can direct attention to the contralateralspace.
As noted previously, it remains unclear whether thedifferences between left and right lesions reflect a truelaterality effect or only differences in the extent and/orlocation of the lesions. Although patients with such dis-crete postero-dorsal thalamic lesions are rare, we hopein the future to encounter more patients with left thala-mic lesions, to resolve this issue. Another interestingcontinuation would be to test whether the present find-ings are valid also for non-linguistic stimuli.
References
1. Aggleton JP, Mishkin M (1983) Mem-ory impairment following restrictedmedial thalamic lesions in monkeys.Exp Brain Res 52:199–209
2. Baleydir C, Mauguirère F (1987) Net-work organization of the connectivitybetween parietal area 7, posterior cin-gulate cortex and medial pulvinar nu-cleus: a double fluorescent tracer studyin monkey. Exp Brain Res 66:385–393
3. Bhatnagar SC, Andy OJ, Korabic EW,Tikofsky R.S, Saxena VK, Hellman RS,Collier BD, Krohn LD (1989) The effectof thalamic stimulation in processingof verbal stimuli in dichotic listeningtasks: A case study. Brain Lang36:236–251
4. Brugge JF, Reale RA (1985) Auditorycortex. In A. Peters & E. G. Jones (Eds.),Cerebral cortex. Vol. 4 New York:Plenum Publishing: 229–271
5. Bryden MP (1988) An overview of thedichotic listening procedure and its re-
lation to cerebral organization. In K.Hugdahl (Ed.), Handbook of DichoticListening: Theory, methods, and re-search (pp. 1–44). Chichester, UK: Wi-ley & Sons
6. Chatterje A, Yapundich R, MennemeierM, Mountz JM, Inampudi C, Pan JW,Mitchell GW (1997) Thalamic thoughtdisorder: On being “a bit addled”. Cor-tex 33:419–40
7. Clarey JC., Barone P, Imig TJ (1992)Physiology of thalamus and cortex. InA. N. Popper and R. R. Fay (Eds.), Themammalian auditory pathway: Neuro-physiology (pp. 232–334). New York:Springer-Verlag
8. Cohen JA, Gelfer CE, Sweet RD (1980)Thalamic infarction producing apha-sia. Mount Sinai J Med 47:395–404
9. Crosson B (1984) Role of dominantthalamus in language: A review. Psy-chol Bull 96:491–517
10. Della Sala S, Spinnler H, Venneri A
(1997) Persistent global amnesia fol-lowing right thalamic stroke: An 11-year longitudinal study. Neuropsychol-ogy 11:90–103
11. Fabbro F, Paradis M (1995) Differentialimpairments in four multilingual pa-tients with subcortical lesions. In M.Paradis (Ed.). Aspects of bilingualaphasia (pp. 139–176). London: Perga-mon Press
12. Geffen G, Quinn K (1984) Hemisphericspecialization and ear advantages inprocessing speech. Psychol Bull96:273–291
13. Glendenning KK, Baker BN, HutsonKA Masterton RB (1992) Acoustic chi-asm V: inhibition and excitation in theipsilateral and contralateral projec-tions of LSO. J Comp Neurol319:100–122
14. Graff-Radford NR, Tranel D, Van Hoe-sen GW, Brandt JP (1990) Diencephalicamnesia. Brain 113:1–25

683
15. Graveleau P, Viader F, Masson M, Cam-bier J (1986) Négligence thalamique.Rev Neurol (Paris) 142:425–430
16. Heilman KM, van den Abell T (1980)Right hemisphere dominance for at-tention: the mechanisms underlyinghemispheric asymmetries of inatten-tion (neglect). Neurology 30:327–330.
17. Hugdahl K, Wester K (1994) Auditoryneglect and the ear extinction effect indichotic listening: A reply to Beatonand McCarthy (1993). Brain Lang46:166–173
18. Hugdahl K (1995) Dichotic listening:Probing temporal lobe functional in-tegrity. In R. J. Davidson & K. Hugdahl(Eds.), Brain asymmetry (pp. 123–156).Cambridge MA: MIT Press
19. Hugdahl K, Wester K, Asbjørnsen A(1991) Auditory neglect after frontallobe and pulvinar thalamic lesions.Brain Lang 41:465–473
20. Hugdahl K, Wester K, Asbjørnsen A(1990) The role of the left and rightthalamus in language asymmetry: Di-chotic listening in Parkinson-patientsundergoing stereotactic thalamotomy.Brain Lang 39:1–13
21. Irvine D (1986) The auditory brain-stem. A review of the structure andfunction of auditory brainstem pro-cessing mechanisms. Progress in Sen-sory Physiology, 7, Berlin: Springer-Verlag 279pp
22. Kimura D (1967) Functional asymme-try of the brain in dichotic listening.Cortex 3:163–168
23. King C, Nicol T, McGee T, Kraus N(1999) Thalamic asymmetry is relatedto acoustic signal complexity. Neuro-science Letters 267:89–92
24. Kirshner HS, Kistler KH (1982) Apha-sia after right thalamic haemorrhage.Arch Neurol 39:667–669
25. Malamut BL, Graff-Radford N,Chawluk J, Grossman RI, Gur RC(1992) Memory in a case of bilateralthalamic infarction. Neurology42:163–169
26. McFarling D, Rothi LJ, Heilman KM.(1982) Transcortical aphasia from is-chemic infarcts of the thalamus: A re-port of two cases. J Neurol NeurosurgPsychiatry 45:107–112
27. Mesulam MM (1981) A cortical net-work for directed attention and unilat-eral neglect. Ann Neurol 10:309–325
28. Mohr JP, Watters WC, Duncan GW(1975) Thalamic haemorrhage andaphasia. Brain Lang 2:3–17
29. Ojemann GA (1977) Asymmetric func-tion of the thalamus in man. Ann NewYork Acad Sci 299:380–396
30. Ojemann GA (1985) Enhancement ofmemory with human ventrolateralthalamic stimulation. Effects evidentin a dichotic listening task. Appl Neu-rophysiol 48:212–215
31. Parkin AJ, Leng RC (1993) Neuropsy-chology of the amnesic syndrome.Hove/London: Erlbaum Publishers
32. Parkin AJ, Rees JE, Hunkin NM, RosePE (1994) Impairment of memory fol-lowing discrete thalamic infarction.Neuropsychologia 32:39–51
33. Peru A, Fabbro F (1997) Thalamic am-nesia following venous infarction: Evi-dence from a single case study. BrainCogn 33:278–294
34. Phillips DP, Gates G R (1982) Repre-sentation of the two ears in the audi-tory cortex: A re-examination. Intern JNeurosci 16:41–46
35. Raczkowski D, Kalat JW, Nebes RD(1974) Reliability and validity of somehandedness questionnaire items. Neu-ropsychologia 12:43–47
36. Schaltenbrand G, Wahren W (1977) At-las for stereotaxy of the human brain.Stuttgart: Georg Thieme
37. Stuss DT, Guberman A, Nelson R,Larochelle S (1988) The neuropsychol-ogy of paramedian thalamic infarc-tion. Brain Cogn 8:348–378
38. Vilkki J (1984) Visual hemi-inattentionafter ventrolateral thalamotomy. Neu-ropsychologia 22:399–408