Embed Size (px)
Citation preview

J Am Acad Audiol 13 : 367-382 (2002)
Auditory Brainstem Response, Middle Latency Response, and Late Cortical Evoked Potentials in Children with Learning Disabilities Suzanne C. Purdy* Andrea S. Kelly,' Merren G. Davies`
Abstract
Auditory evoked potentials (AEPs) and behavioral tests were used to evaluate auditory process-ing in 10 children aged 7 to 11 years who were diagnosed as learning disabled (LID) . AEPs included auditory brainstem responses (ABRs), middle latency responses (Iv1LRs), and late cortical responses (P1, N1, P2, P3) . Late cortical responses were recorded using an active listening oddball proce-dure . Auditory processing disorders were suspected in the LID children after a psychologist found phonologic processing and auditory memory problems . A control group of 10 age- and gender-matched children with no hearing or reported learning difficulties was also tested . Teacher ratings of classroom listening and SCAN Competing Words and Staggered Spondaic Word scores were poorer in the LD children . There were minor ABR latency differences between the two groups . Wave Na of the Iv1LR was later and Nb was smaller in the LID group . The main differences in cor-tical responses were that P1 was earlier and P3 was later and smaller in the LD group .
Key Words: Auditory evoked response, auditory processing disorder, learning disability
Abbreviations : ABR = auditory brainstem response ; APD = auditory processing disorder ; CAEP = cortical auditory evoked potential ; CAPD = central auditory processing disorder ; LD = learning disabled ; Iv1LR = middle latency response ; Iv1NIN = mismatch negativity ; WISC-R = Wechsler Intelligence Scale for Children-Revised
Surnario
Se utlizaron potenciales evocados auditivos (AEP) y pruebas conductuales para evaluar el proce-samiento auditivo en 10 ninos con edades entre 7 y 11 anos, quienes fueron diagnosticados como portadores de trastornos del aprendizaje (LID) . Los AEP incluyeron respuestas auditivas de tallo cerebral (ABR), respuestas de latencia media (MLR) y respuestas corticales tardias (P1, N1, P2, P3) . Las respuestas corticales tardias fueron registradas utilizando un procedimiento inusual de escucha activa . Se sospecharon trastornos de procesamiento auditivo en los ninos LID despues de que un psicologo encontro problemas fonologicos y de memoria auditiva . Se evaluo tambien un grupo de control de 10 ninos ordenados por edad y genero, quienes no presentaban dificultades para escuchar o para apren-der . La estimacion del maestro sobre la habilidad de escuchar en clase y los resultados de la prueba de Palabras SCAN de Competencia y la prueba SSW fueron peores en los n0os con LID . Existieron diferencias menores de latencia en el ABR entre los dos grupos . La onda Na en las IVILR fue mas tardia y la Nb fue mas pequena en el grupo LID . Las principales diferencias en las respuestas corticales fueron clue la P1 aparecia mas temprano y la P3 mas tarde y mas pequena en el grupo LID .
Palabras Clave : Respuestas evocadas auditivas, trastornos de procesamiento auditivo, trastornos del aprendizaje
Abreviaturas : ABR = respuesta auditiva del tallo cerebral ; APD = trastornos de procesamiento auditivo ; CAEP = potencial evocado auditivo cortical ; CAPD = trastornos central de procesamiento auditivo ; LID = discapacidad para el aprendizaje ; MLR = respuesta de latencia media ; IVIIV1N = ne-gatividad desigual ; WISC = Escala Revisada Wechsler de Inteligencia para Ninos
*National Acoustic Laboratories, Sydney, Australia: 'Discipline of Audiology, The University of Auckland, Auckland, New Zealand, 'Cochlear Corp ., Sydney, Australia
Reprint requests : Suzanne C . Purdy, National Acoustic Laboratories, 126 Greville Street, Chatswood, NSW 2067, Australia
367

Journal of the American Academy of Audiology/Volume 13, Number 7, July/August 2002
M any studies have used electrophysio-logic measures to objectively investi-gate auditory processing . Unlike
speech and other behavioral auditory process-ing tests, auditory evoked potentials can be recorded regardless of a child's developmental age or language, motivation, or attention level. Auditory processing from the level of the eighth nerve to the auditory cortex has been investi-gated using the auditory brainstem response (ABR), middle latency response (MLR), late cor-tical, P3, and mismatch negativity (MMN) evoked responses. ABR, MLR, and the P1-N1-P2 late cortical responses are "obligatory" responses that depend on the physical properties of the stimulus . P3 and MMN are "discriminative" responses recorded using an oddball stimulus paradigm in which an infrequent, deviant stim-ulus is interspersed randomly among a fre-quently occurring standard stimulus . P3 is also referred to as "P300" or "P3b" (Stapells, 2002) and is usually recorded using an active listen-ing paradigm with the subject responding to the deviant stimulus, whereas MMN is a preat-tentive response that is usually recorded with the subject ignoring the stimuli (Schroger and Wolff, 1998).
The American Speech-Language-Hearing Association (ASHA) Task Force on Central Audi-tory Processing (1996) concluded that electro-physiologic measures are useful for the diagnosis of central auditory processing disorders (CAPDs) but acknowledged that further research is needed to establish the clinical utility of middle and late evoked potentials . More recently, the Bruton Conference held at the Callier Center in Dallas (Jerger and Musiek, 2000 ; Chermak, 2001) produced the recommendation that a min-imal test battery for the diagnosis of auditory processing disorders (APDs) in school-aged chil-dren should include ABR and MLR testing. The P3 event-related response was included in the list of optional procedures that are potentially useful for strengthening the diagnosis of APD.
ABR is well understood and is used rou-tinely for the detection of brainstem and eighth nerve lesions (ASHA, 1996). An abnormal ABR in a child thought to have APD can be indicative of neuropathology requiring medical interven-tion (e .g., Musiek et al, 1991). There are many reports in the literature dating back to the 1970s of ABR abnormalities in patients with sensory and motor neuropathies affecting the auditory system (e.g ., Satya-Murti et al, 1979). An abnor-mal ABR combined with intact otoacoustic emis-sions now leads to a diagnosis of auditory
neuropathy/dyssynchrony (Starr et al, 2000 ; Berlin, 1999). ABR abnormalities have been reported in children with learning problems (Sohmer and Student, 1978; Greenblatt et al, 1983 ; Jerger et al, 1987 ; Cunningham et al, 2001), speech and language disorders (Mason and Mellor, 1984; Milicic et al, 1998), and audi-tory processing deficits (Yencer, 1998). In con-trast, Marosi and colleagues (1990) did not see ABR latency or amplitude differences in their study of primary schoolchildren with a learning disability. Thus, there is conflicting evidence for ABR abnormalities in school-aged children with APD who do not have auditory neuropathy or any evidence of auditory neural pathology.
Some years ago, Jerger and his colleagues (1988) described MLR as potentially "the single most important auditory evoked response in terms of its ability to help us identify and under-stand CAPD ." MLR abnormalities have been found in children with learning or speech/lan-guage disabilities (Squires and Hecox, 1983 ; Mason and Mellor, 1984; Jerger and Jerger, 1985 ; Jerger et al, 1987, 1988 ; Fifer and Sierra-Irizarry, 1988 ; Arehole et al, 1995; Milicic et al, 1998). The MLR is also affected in adults with APD (Jerger et al, 1991 ; Marvel et al, 1992), cor-tical lesions (Ozdamar et al, 1982; Shehata-Dieler et al, 1991 ; Kraus and McGee, 1993 ; Musiek and Lee, 1997 ; Musiek et al, 1999; Set-zen et al, 1999 ; Akkuzu et al, 2001), and multi-ple sclerosis (Jerger and Jerger, 1985 ; Stach and Hudson, 1990; Celebisoy et al, 1996). MLR appears to be a sensitive indicator of central nervous system pathology involving the auditory system. Many of the MLR investigations in chil-dren have been case studies, however; hence, there are still relatively few data on the nature of MLR abnormalities in children with APD.
MLRs can be reliably recorded in young children and infants if appropriate stimulus and recording parameters are used (Tucker and Ruth, 1996). In younger children, the MLR typ-ically consists of a broad, late Pa, followed by a negative trough, Nb (Musiek et al, 1988 ; Suzuki and Hirabayashi, 1987). Pb is typically absent . Pa and Nb latencies approximate adult values by 8 to 11 years (Suzuki and Hirabayashi, 1987). The change in waveform morphology with age has been attributed to differential maturation of multiple MLR generators . Kraus and McGee (1993) hypothesized that the earlier-maturing mesencephalic reticular formation dominates the younger child's MLR, and adult-like MLR morphology occurs with maturation of the thal-amocortical pathways .
368

Evoked Potentials in Learning-Disabled Children/Purdy et al
In adults, Pa is largest at the vertex (Cz) and symmetrically distributed over the temporal lobes (Ozdamar and Kraus, 1983 ; Kraus and McGee, 1988 ; Cacace et al, 1990) . A trend for broader and later MLR peaks at more lateral recording sites has been seen in adults (Deiber et al, 1988) . Mason and Mellor (1984) found that differences between MLR amplitudes in chil-dren with speech and language disorders and con-trol group children were greater at hemispheric (T3, C3, C4, T4) electrode sites than at the ver-tex . The effects of neuropathology in adults may also be more evident when recordings are made over temporoparietal regions (Kileny et al, 1987) . A slight left ear Pa amplitude advantage has been reported in adults (Cacace et al, 1990), but the opposite has also been found (Deiber at al, 1988) . Kadoya and colleagues (1988) found that Pa amplitudes recorded over the hemisphere contralateral to the test ear in guinea pigs and adult humans were significantly larger than those recorded over the ipsilateral hemisphere . Ozdamar and Kraus (1983) also noted this con-tralateral advantage in their data . Marvel and colleagues (1992) found significant hemispheric asymmetry in MLR topographic brain maps in elderly listeners with suspected APD, whereas control subjects had symmetric MLR distribu-tions . Musiek and his colleagues have suggested that MLR hemispheric and ear asymmetries are more reliable indicators of APD than absolute MLR latencies or amplitudes (Musiek et al, 1994 ; Cbermak and Musiek, 1997 ; Musiek et al, 1999) . Normal maturational changes and ear and recording electrode effects on the MLR need to be better characterized to establish normative data for MLR ear and hemisphere differences in children .
The cortical P1-N1-P2 evoked potentials that occur within about 300 msec after stimu-lus onset in adults depend primarily on the physical properties of the stimulus . Discrimi-native cortical potentials elicited using an odd-ball stimulus paradigm result from either preconscious (e.g ., MMN) or conscious (e.g., P3b) perception of a change in the auditory stimulus and hence have been referred to as "process-ing-contingent potentials" (Stapells, 2002) . Both obligatory and discriminative potentials have been investigated as objective indices of central auditory function since they correlate well with perception and discrimination of auditory stim-uli (Hyde, 1997 ; Stapells, 2002) and are abnor-mal in individuals with brain lesions affecting auditory cortical regions (e.g ., Hood et al, 1994) . Cortical auditory evoked potential (CAEP) gen-
erators include primary auditory cortex, audi-tory association areas, frontal cortex, and sub-cortical regions (see reviews by Picton et al, 1999, and Stapells, 2002) . Although these responses are present in infants (Steinschneider et al, 1992), they undergo considerable matu-rational changes, and some cortical potentials may not be fully mature until close to adulthood (Ponton et al, 2002) . In infants and young chil-dren, CAEPs are dominated by P1, which becomes earlier and smaller as N1 and P2 begin to emerge in the waveform at about 8 to 10 years of age (Sharma et al, 1997 ; Ponton et al, 2002) . These maturational changes complicate the use of CAEP for diagnosis ofAPD since more extensive normative data are required than for the earlier-maturing evoked potentials . The scalp distribution of P1, N1, and P2 is normally symmetric with maximal amplitude near the vertex (Picton et al, 1999), but, as for MLR wave Pa, a contralateral hemisphere advantage (ear-lier latencies, greater amplitudes) has been reported in adults (Verkindt et al, 1995 ; Picton et al, 1999 ; Ponton et al, 2002) . The amplitude, latency, and scalp distribution of the discrimi-native cortical potential P3 depends on subject age as well as state of arousal and attention (Squires et al, 1975 ; Pearce et al, 1989 ; Johnstone et al, 1996 ; Oades et al, 1997; Stapells, 2002) .
Both obligatory and discriminative CAEPs have been investigated in children and adults thought to have APD. Researchers have found a variety of Pl-Nl-P2 and P3 abnormalities, including increased absolute and interwave latencies (Jirsa and Clontz, 1990 ; Arehole, 1995 ; Tonnquist-Uhlen, 1996a, 1996b; Bruneau et al, 1999 ; Seri et al, 1999), reduced N1 amplitude (Bruneau et al, 1999; Seri et al, 1999 ; Cun-ningham et al, 2001 ; Wioland et al, 2001), reduced P3 amplitude (Jirsa and Clontz, 1990), increased (Bernal et al, 2000) or decreased (Ton-nquist-Uhlen, 1996b) P2 and N2 amplitudes, and increased hemispheric asymmetry (Mason and Mellor, 1984 ; Jerger et al, 1991). A number of studies have shown reduced MMN ampli-tudes (and sometimes increased latencies) in adults and children with speech/language, read-ing, or learning difficulties (Kraus et al, 1993, 1996 ; Korpilahti and Lang, 1994 ; Schulte-Korne et al, 1998, 1999, 2001 ; Baldeweg et al, 1999 ; Bradlow et al, 1999). Further research is required, however, before MMN can be regarded as a clinical tool for APD assessment owing to the small amplitude and high variability of the response (Picton et al, 2000 ; Dalebout and Fox, 2001 ; McGee et al, 2001).
369

Journal of the American Academy of Audiology/Volume 13, Number 7, July/August 2002
In the present study, ABR, MLR, P1-N1-P2, and P3 responses were recorded in children with a learning disability whose phonologic process-ing and auditory memory problems led to a sus-picion of APD. Electrophysiologic responses, scores on behavioral tests of APD, and teacher assessments of classroom listening were com-pared with the results for a control group of children to determine which tests distinguished the two groups of children and the pattern of elec-trophysiologic and behavioral results for the children with a learning disability (LD) .
METHOD
Subjects
Ten children (6 boys, 4 girls) aged 7 to 11 years (mean = 9.3 years, SD = 1.5 years) were recruited with the assistance of the University ofAuckland's Learning Assessment Centre . The children had been assessed by a psychologist and had been diagnosed as having an LD and a pos-sible APD. Children with no significant atten-tion deficit whose Weschler Intelligence Scale for Children-Revised (WISC-R) scores were within normal limits were invited to participate in the research . The psychologist made a diagnosis of possible APD if the children showed difficulties with auditory blended phoneme analysis and one or more of the following tasks: (1) auditory immediate memory and/or attention, (2) auditory and visual immediate memory and/or attention, (3) auditory discrimination of speech phonemes, and (4) auditory long-term memory. These audi-tory skills were assessed using the WISC-R digit span and arithmetic subtests, the Learning Effi-ciency Test (LET) of auditory and visual imme-diate memory and auditory long-term memory (Webster, 1981), the Detroit Tests of Learning Aptitude-2 (DTLA-2) Following Oral Directions subtest (Hammill, 1985), the revised Lindamood Auditory Conceptualization (LAC) tests of speech phoneme auditory discrimination and auditory blended phoneme analysis (Lindamood and Lin-damood, 1979), and the Selective Reminding Test (Buschke and Fuld, 1974).
The control group consisted of 10 children recruited via friends and colleagues who were matched for age and gender with the experi-mental group (6 boys, 4 girls ; mean age = 9 .2 years, SD =1.6 years) whose parents reported no history of learning or hearing difficulties . Chil-dren in both groups had normal pure-tone thresh-olds (<_ 15 dB HL at octave frequencies from 500 to 8000 Hz), Type Atympanograms (Jerger, 1972),
and normal ipsilateral and contralateral acoustic reflexes (Gelfand et al, 1990). None of the chil-dren had a history of significant middle ear dis-ease or any known medical problems .
Procedure
Parents were given a questionnaire to deliver to the children's teachers to assess class-room listening behavior. The questionnaire was based on Sanger and colleagues' (1987) and Smoski and colleagues' (1992) questionnaires and contained four items requiring a response on a 7-point rating scale and six items with yes-no answers (Appendix) . The children were tested in two sessions separated by about a week . All testing were done in a double-walled sound-proofed booth. Audiometry and behavioral APD testing were performed in the first session and electrophysiologic testing was performed in the second session.
Behavioral APD tests consisted of the SCAN (Keith, 1986) and the Staggered Spondaic Word (SSW) List EC test (Katz, 1968). The SCAN test was developed as a screening tool but, despite this, is widely used by audiologists for clinical diagnosis ofAPD. The behavioral test battery was not com-prehensive owing to the time requirements for the electrophysiologic testing and hence did not include a test of temporal processing as recom-mended by ASHA (1996) and the Bruton Con-ference (Jerger and Musiek, 2000). Two W-22 phonetically balanced (PB) word lists (one list per ear) were also presented so that corrected SSW (C-SSW) scores could be calculated (Arnst and Doyle,1983). The speech items were presented at 50-dB sensation level (re 500-, 1000-, 2000-Hz pure-tone average) .
Evoked potential testing was done using a Neuroscan STIMTM system to deliver stimuli. Responses were recorded using SCAN TM soft-ware and hardware and a Grass Model 12 Neu-rodata Acquisition System . Stimuli for ABR and MLR testing were 70 dB nHL (99.7 dB peak to peak equivalent SPL) 100- isec rar-efaction clicks presented at 8.7/sec . An oddball paradigm was used for CAEP testing with the 1000-Hz frequent and the 2000-Hz deviant tones presented on 80 percent and 20 percent of trials, respectively, at 1 .1/sec . The 1000- and 2000-Hz tones had rise-fall times of 5-msec and 20-msec plateaus and were presented at 70 dB HL (70 and 73 dB SPL re HA-2 2-cc coupler, respec-tively). Stimuli were presented to left and right ears and binaurally via ER3-A insert earphones in random order for each evoked potential test .
370

Evoked Potentials in Learning-Disabled Children/Purdy et al
Table l Recording Parameters for the Three Electrophysiologic Tests
Electrode Averages Sampling Time Artifact Filter Response Montage x Repeats Gain Rate Window Reject (Hz) ABR Cz 1024 x 2 105 20 kHz -2 to 10 ± 22 [V 100-3000 MLR Cz, C5, C6 512 x 2 5 x 101 20 kHz -2 to 100 ±45 RV 3-300 CAEP Cz, C5, C6 300 x 2 5 x 10° 2 kHz -100 to 750 ±45 RV 1-30
For ABR and MLR testing Cz, C5, and C6 electrodes were referenced to an electrode on the neck (second cervical vertebra) . For CAEP testing, Cz C5, and C6 were referenced to linked earlobes (A1/A2) . Time windows are shown in milliseconds pre- and post-stimulus presentation .
ABR = auditory brainstem response, MLR = middle latency response, CAEP = cortical auditory evoked potential .
Test order (ABR, MLR, CAEP) was counter-balanced across children .
The children were seated in a comfortable chair and watched silent cartoon videos for ABR and MLR testing. For cortical testing, the chil-dren were asked to press the Neuroscan response button each time they heard the less frequent "higher-pitched" sound . Response accuracy for all children was greater than 90 percent . Record-ing parameters for the three electrophysiologic tests are summarized in Table 1 . Filtering was performed online by the Grass amplifiers (18 dB/octave high pass, 6 dB/octave low pass) . Because an eye-blink recording channel was not used, a strict artifact-rejection criterion of
45 l.V was used for the cortical recordings . Gold cup electrodes were placed using the Inter-national 10-20 system (Jasper, 1958) on the ver-tex (Cz), left temporal lobe region (C5), right temporal lobe region (C6), earlobes (Al/A2), neck (Cv2), and forehead (ground) . Cv2 was used as the inverting electrode for ABR and MLR recordings to maximize ABR wave V and MLR wave Pa amplitudes and to minimize postauricular muscle artifact in the MLR (Kraus and McGee, 1988 ; Hall, 1990) .
Evoked potential peaks (latencies and ampli-tudes) were identified independently by three observers, one of whom was blind to the cate-gorization of the subjects (LD versus control) . Peak identification was based on agreement between the blinded observer and at least one other observer . The latency and amplitude of ABR wave V were picked on the "shoulder" pre-ceding the negative trough after the IV/V com-plex, as is conventionally done, but other peaks were picked at the center of the positivity or neg-ativity. The latency "windows" used to identify MLR peaks were quite wide because of the pos-sibility of abnormally delayed waveforms plus the considerable intersubject MLR latency vari-ability that is seen normally. MLR wave Na was defined as the most negative replicable trough immediately preceding wave Pa occurring
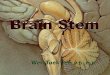
between 10 and 35 msec . Wave Pa was the max-imum vertex-positive peak immediately follow-ing Na between 20 and 55 msec . If wave Pa consisted of a single peak, the amplitude was measured at the point of the largest amplitude and latency was measured at the center of the peak . If wave Pa had multiple peaks, the largest amplitude was taken and the latency was mea-sured at the midpoint between waves Na and Nb. Wave Nb was defined as the largest vertex-neg-ative peak following Pa occurring between 30 and 85 msec . All subjects had an identifiable MLR. Latency windows used to define CAEP peaks were as follows : Pl, 40 to 200 msec ; Nl, 60 to 300 msec ; P2, 100 to 450 msec; and P3, > 200 msec . All CAEP peaks could be consistently identi-fied with the exception of P2, which was not evident in about 5 percent of waveforms . As illustrated in Figure 1, which shows the CAEP waveform of one control group subject, in gen-eral, P1, N1, and P3 could be identified as dis-tinct peaks, whereas P2 was identified as a positivity occurring after N1 and before P3, which often was on the rising shoulder of P3.
RESULTS
Teacher Questionnaire
Completed questionnaires were received back from 18 teachers (8 LD, 10 control group children) . For the four items in Section A, the con-trol group and LD children received average ratings of 0.2 (SD = 1.2) and -1.6 (SD = 1 .3), respectively. A rating of "0" in Section A indicates that the child has the same amount of difficulty and "-2" indicates that the child has more dif-ficulty than other children in the class . For Sec-tion B, which required a yes/no answer, 51 percent and 12 percent of responses were "yes" for the LD and control group children, respec-tively, indicating much greater difficulties for the LD children . Separate statistical analyses for Sections A and B using the Mann-Whitney U test
371

Journal of the American Academy of Audiology/Volume 13, Number 7, July/August 2002
Figure 1 Individual cortical auditory evoked potential waveforms for one of the control group subjects to deviant 2000-Hz (thick line) and standard 1000-Hz (thin line) stim-uli recorded using Cz-Al/A2 electrode montage and bin-aural stimulation. Peaks Pl, Nl, P2, and P3 are identified.
and Fisher's exact probability test showed that classroom listening behavior was significantly poorer for the LD children (p <_ .03) .
Speech Tests
Average SCAN (number correct) and C-SSW (percent error) scores are presented in Table 2 for the three SCAN subtests (Filtered Words, Auditory Figure Ground, Competing Words) and the four SSW test conditions (right noncompet-ing, right competing, left competing, left non-competing) . SCAN raw scores can be converted to standardized scores using Keith's (1986) nor-mative data . A standard score of 10 represents average performance for the child's age group. Standardized SCAN scores were 10.4 (SD = 2.7)
and 11.7 (SD = 2.6) for the LD and control groups, respectively, indicating that, overall, the children performed relatively well compared with the North American norms. Although SCAN scores were higher on average for the control group chil-dren for all three subtests, a combined analysis of scores for the three subtests showed no sig-nificant difference between the two groups (F = 3.28, df = 1, 18, p = .087). Table 2 shows that the greatest difference in scores occurred for the SCAN Competing Words subtest. Separate analyses of variance showed significantly poorer LD group performance for Competing Words (F = 4.91, df =1, 18, p = .040) but not for the other two SCAN subtests (p >- .235).
Mean W-22 PB word scores were high for both LD (mean = 97%, SD = 4.1) and control group children (mean = 96%, SD = 4.3) . Indi-vidual children's W-22 error scores were sub-tracted from their raw SSW error scores to produce corrected SSW scores . In some instances, this correction produced a negative error score. Table 2 shows the expected right ear advantage in both groups of children for the competing conditions (right competing errors < left com-peting errors). C-SSW scores were significantly poorer for LD children than controls (F = 7.18, df = 1, 18, p = .015).
Electrophysiologic Group Differences
A repeated-measures analysis of variance was performed to determine the effects of group, test ear, and electrode montage on the evoked potential results. All subjects had clear ABR responses with latencies that fell within the
Table 2 Means, SDs, and Ranges of SCAN Scores (Number of Correct Items) and C-SSW (SSW Error Scores Corrected Using W-22 Error Score) for the Learning-Disabled and Control Group Children
Test Group Subtest Mean SD Range
SCAN LD Filtered Words 34.9 2 .2 32 to 39 (no . correct) Figure Ground 33.8 2 .6 29 to 37
Competing Words 78.7 3 .9 74 to 84 Control Filtered Words 36 .1 2.2 33 to 39
Figure Ground 34 .1 3 .2 29 to 38 Competing Words 84.7 7 .6 75 to 100
C-SSW LD RNC 5.2 6 .5 0 to 18 (% errors) RC 12 .9 7.8 0 to 20
LC 19.4 10 .0 6 to 39 LNC 5 .1 7 .6 0 to 24
Control RNC -1 .0 3 .7 -8 to 5 RC 7.8 8 .8 -4 to 25 LC 10.0 8 .8 -4 to 23 LNC -1 .3 6 .3 -12 to 8
C-SSW = corrected Staggered Spondaic Word ; LID = learning disabled ; RNC = right noncompeting ; RC = right competing ; LC = left competing; LNC = left noncompeting .
372

Evoked Potentials in Learning-Disabled Children/Purdy et al
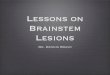
Figure 2 Grand-averaged auditory brainstem response waveforms of the control group (thick line) and learning-disabled children (thin line) recorded using Cz-Cv2 elec-trode montage and binaural stimulation .
normal range (Hall, 1990). ABR amplitudes, latencies, and interwave intervals showed two group differences . Wave V latency was shorter overall for LD (mean = 5.68 msec) than control (mean = 5.82 msec) children (F = 5 .29, df = 1, 54, p = .025) and the wave III-V interwave interval was shorter for LD (mean = 1.97) than control (mean = 2 .10 msec) children (F = 10.72, df = 1, 54, p = .002). These group latency differences are fairly subtle, as illustrated by the grand-aver-aged ABR waveforms shown in Figure 2 .
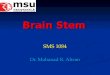
MLR group differences are illustrated in Figure 3 . Na latency was longer overall (aver-aged across test ear and electrode montage) for LD (mean = 24.99 msec) than for control (mean = 21.81 msec) children (F = 15.87, df = 1, 162, p < .001), and Nb amplitude was less negative for LD (mean = -1.56 RV) than for control (mean = -2.05 IN) children (F = 7.89, df =1,162, p = .006) . There was a trend for Pa latencies to be longer in the LD children (mean = 38.60 msec versus 36.79 in control group), but the difference was not statistically significant (p = .062) . Figure 3 shows an ear asymmetry in the MLR wave-forms of the control children that was much less pronounced in the LD group .
CAEP waveforms obtained in response to the standard 1000-Hz tone and the deviant 2000-Hz tone were analyzed separately. As shown in Figure 4, the waveforms for both the standard and the deviant contain a P3 response, suggest-ing that for the children in this study, the change back to the frequent stimuli from the deviant was causing an attention switch . The grand-aver-aged waveforms in Figure 4 show clear P1 and P3 peaks, but it is difficult to identify N1 and P2 in the average waveforms owing to the inter-subject variability of these peaks and the small
Figure 3 Grand-averaged right ear (thick line) and left ear (thin line) middle latency response waveforms recorded using Cz-Cv2 electrode montage. Responses of the learning-disabled (LD) and control children are shown at the top and bottom, respectively.
amplitude of P2 . The two groups' P1, N1, P2, and P3 results are summarized in Table 3 . F ratios and p values are also shown in Table 3 for the peak latencies and amplitudes that differed sig-nificantly between the groups . For the standard stimulus, P1 and P3 latencies and N1 and P3 amplitudes differed significantly between the two groups (p < .001). For the deviant stimulus, P1, N1, and P3 latencies and P2-N2 and P3 amplitudes differed between the two groups (p 5 .045). The earlier peaks, PI and Nl, had shorter latencies and smaller amplitudes in the LD group . P3 was later and smaller in the LD chil-dren for both standard and deviant stimuli . P2-N2 relative amplitude for the deviant stim-ulus was larger in the LD group. As shown in Table 4, P1 and N1 were 7 to 18 msec earlier on
Figure 4 Grand-averaged cortical auditory evoked poten-tial waveforms to deviant 2000-Hz (thick line) and stan-dard 1000-Hz (thin line) stimuli recorded using Cz A1/A2 electrode montage and binaural stimulation. Responses of the learning-disabled (LD and control children are shown at the top and bottom, respectively.
373

Journal of the American Academy of Audiology/Volume 13, Number 7, July/August 2002
Table 3 Means (and SDs) of CAEP Peak Latencies and Amplitudes Recorded in Response to the 1000-Hz Standard and the 2000-Hz Deviant Stimuli Using a Cz-A1/A2 Electrode Montage and
Binaural Stimulation
Wave Measure Stimulus LD Control F Value p Value
P1 Latency (msec) Standard 88.06 (23 .86) 102 .94 (18 .49) F (1, 161) = 17.48 < .001 Deviant 84.34 (41 .25) 101 .34 (26 .26) F (1, 161) = 24.54 < .001
Amplitude (wV) Standard 4.10 (2 .11) 1 .93 (2 .33) NS NS Deviant 3.85 (2 .25) 2 .36 (3 .37) NS NS
N1 Latency (msec) Standard 165.42 (62 .71) 163 .05 (39 .28) NS NS Deviant 151 .81 (50 .09) 154 .60 (37 .35) F (1, 161) = 10.68 001
Amplitude (wV) Standard -4.00 (2 .31) -5 .33 (2 .46) F (1, 158) = 20.12 < .001 Deviant -4.46 (2 .88) -6 .24 (2 .67) NS NS
N1-P2 Amplitude (~,V) Standard 3.76 (3 .33) 3 .23 (2 .84) F (1, 146) = 6.33 .013 Deviant 3.87 (2 .35) 5 .99 (3 .24) NS NS
P2 Latency (msec) Standard 208.49 (113.13) 197 .86 (59 .25) NS NS Deviant 194.73 (66 .30) 213 .43 (58 .66) NS NS
Amplitude (~LV) Standard 0.37 (2 .99) -1 .71 (2 .61) NS NS Deviant 0.13 (2 .71) -0 .25 (3 .71) NS NS
P2-N2 Amplitude (8,V) Standard 6.03 (3 .98) 3 .12 (2 .15) NS NS Deviant 4.91 (2 .54) 2 .80 (3 .11) F (1, 146) = 7.33 008
P3 Latency (msec) Standard 408.85 (100.39) 361 .92 (43 .61) F (1, 162) = 17.03 < .001 Deviant 406.41 (67 .43) 355 .81 (51 .11) F (1, 162) = 20.11 < .001
Amplitude (~LV) Standard 3.68 (1 .42) 4 .39 (1 .56) F (1, 162) = 13.85 < .001 Deviant 5.60 (4 .51) 8 .15 (2 .50) F (1, 159) = 4.07 045
F ratios, degrees of freedom, and p values are shown for the analyses of variance that showed significant group differences across conditions (test ear and electrode montage) .
CAEP = cortical auditory evoked potential ; LID = learning disabled ; NS = not significant .
average and P3 was 45 to 46 msec later in the LD group. The significant amplitude differences ranged from 0.8 to 1.5 p,V (14 to 39% of the nor-mal peak amplitudes).
Summary of Group Differences
The teacher questionnaire and SSW and Competing Word scores indicated significantly poorer auditory processing in the LD group compared with the control children . The LD and
control groups differed significantly on a num-ber of electrophysiologic measures . In LD chil-dren, (1) ABR wave V and III-V latencies were shorter; (2) MLR wave Na latency was longer and wave Nb amplitude was smaller; (3) for standard and deviant stimuli, P1 latencies were shorter, P3 latencies were longer, and P3 amplitudes were smaller; (4) for standard stim-uli, N1 amplitude was smaller and P2 was ear-lier ; and (5) for deviant stimuli, N1 was earlier and P2-N2 was smaller.
Table 4 Overall Differences in CAEP Peak Latencies and Amplitudes between the Learning-Disabled and Control Groups Averaged across Test Ear and Electrode Montage
Overall Group Difference (Learning Disabled minus Control) timulus 1 1 3 1-P2 2-N2 Latency (msec) Standard -11 .72 -7.39 44.84
Deviant -17.89 -15.74 46.06 Amplitude (8V) Standard 0.18 1 .45 -0.81 -1 .26 0.73
Deviant 0.53 0.63 -0.92 -0.22 1 .01 Latency (% of normal) Standard 11 .29 4.55 12.48
Deviant 17.47 9.86 13.07 Amplitude (% of normal) Standard 7.27 30.18 21 .11 28.40 29.16
Deviant 26.46 9.40 13.77 3.32 39.12
Differences are shown as absolute values (learning disabled minus control) or as a percentage of the mean value of the control group. Negative values indicate earlier latencies and smaller amplitudes in the learning-disabled group . Significant differences are indicated in bold . P2 differences are not listed since none of these were significant .
374

Evoked Potentials in Learning-Disabled Children/Purdy et al
Table 5 Middle Latency Response Means (and SDs) for the Children in the Two Groups Recorded Using a Cz-Cv2 Electrode Montage
Ear Measure Group Na Pa Nb Na-Pa Pa-Nb
Left Latency (msec) LD 23 .20 (5 .11) 38 .21 (8 .52) 54.29 (15 .09) Control 22 .78 (5 .05) 36 .85 (4 .42) 57.14 (7 .85)
Amplitude (~LV) LD -0.82 (0 .90) 0.23 (1 .29) -1 .28 (1 .30) 1 .06 (0 .55) 1 .49 (0 .86)
Control -1 .53 (0 .55) -0.38 (0 .74) -2.15 (1 .06) 1 .19 (0 .66) 1 .80 (0 .72)
Right Latency (msec) LD 23.82 (6 .36) 38.40 (6 .87) 56.74 (12 .56) Control 21 .89 (5 .01) 36.23 (5 .13) 59 .29 (8 .24)
Amplitude (pV) LD -1 .14 (1 .01) 0.19 (1 .18) -1 .50 (1 .48) 1 .34 (0 .70) 1 .69 (0 .98)
Control -1 .37 (0 .79) -0.20 (0 .95) -2 .53 (0 .70) 1 .39 (0 .72) 2.33 (0 .66) Binaural Latency (msec) LD 25.20 (6 .82) 39.99 (10.68) 59 .64 (16 .15)
Control 22.56 (6 .37) 36.53 (4 .34) 59.35 (7 .95) Amplitude (ltV) LD -1 .36 (1 .06) 0.05 (1 .42) -1 .74 (0 .97) 1 .73(1 .11) 2 .11 (1 .12)
Control -1 .64 (1 .03) -0.30 (0 .76) -2.37 (1 .00) 1 .37 (0 .57) 2 .35 (0 .42)
The right-hand columns show relative Na-Pa and Pa-Nb amplitudes .
Ear Effects on Electrophysiologic Results
this one exception, CAEP measures were not affected by test ear.
There were no significant statistical inter-actions among ear, group, and electrode montage
for any of the electrophysiologic measures, so the
effects of test ear were consistent between groups and across electrode montage . The only signif-
icant ear effects on the ABR were attributable
to the expected binaural advantage . This
resulted in greater wave V amplitudes (F =
21 .16, df = 2, 54, p < .001) and a shorter wave
I-V interval (F = 5 .62, df = 2, 52, p = .006) for
binaural stimulation . Binaural wave V ampli-
tude was larger (mean = 1.30 iiLV) than left
(mean = 0.74 V V, p < .001) or right (mean = 0.71
~LV, p < .001) ear amplitudes . The binaural wave I-V interval was shorter (mean = 3.89 msec) than
left (mean = 4 .16 msec, p = .012) or right (mean = 4.21 msec, p = .003) ear values .
MLR latencies and absolute and relative amplitudes are shown in Table 5. These data illustrate the significant ear effects on Na-Pa (F = 7.47, df = 2,162, p = .001) and Pa-Nb (F = 3.42, df = 2, 162, p = .035) relative amplitudes . As illus-trated in Figure 3, both groups had a right ear amplitude advantage, but it was more pro-nounced in the control children. Binaural and right ear amplitudes did not differ significantly, but left ear MLR amplitudes were smaller than both right ear and binaural amplitudes (p <_
.028). There was only one minor effect of test ear
on CAEP results. P1 amplitude was smaller for left ear (mean = 1.77 j,V) than for binaural (mean = 6.73 v,V) stimulation (F = 3 .62, df = 2, 158, p = .029). This "left ear disadvantage" for P1 is consistent with the MLR results . With
Electrode Montage Effects on Electrophysiologic Results
Only one electrode montage was used for the ABR recordings, and there were no effects of elec-
trode montage (C5, Cz, C6) on MLR results. There were quite a few electrode montage effects on CAEP results, mainly owing to a vertex ampli-tude advantage for the later CAEP waves (P2, N2, P3). N2 amplitudes were larger at Cz than at C5 or C6 for both standard (F = 10.03, df = 2, 141, p < .001) and deviant (F = 3.56, df = 2, 150, p = .031) stimuli. P2-N2 and N2-P3 relative amplitudes were also larger at Cz than at C5 or C6 for both standard and deviant stimuli (p <_ .014), and P3 amplitude was larger at the vertex for the standard stimulus (p <- .013). In contrast, N1 was less negative and Nl-P2 rel-ative amplitude was smaller at the vertex for the
deviant stimulus compared with C5 and C6 (p <_ .008).
DISCUSSION
T he results of the teacher questionnaire, the SSW, and the SCAN Competing Words sub-
test support the diagnosis of probable APD that was made by the psychologists who used a vari-ety of tests of phonologic processing, auditory memory, and attention to assess the children in the LD group. The electrophysiologic results showed significant group differences on selected parameters for all of the evoked potentials inves-tigated, providing further evidence that these children had auditory processing difficulties.
375

Journal of the American Academy of Audiology/Volume 13, Number 7, July/August 2002
The children in both groups performed quite well on the SCAN test compared with the North American norms. This may reflect the selection of subjects for the study and the optimized test conditions, and the North American norms may be inappropriate for New Zealand children . In the preselection process, children with signifi-cant attention problems were excluded . The children were given frequent rest breaks with refreshments during both test sessions to ensure that they were motivated and cooperative. Sil-man and colleagues (2000) demonstrated how a high level of motivation improves scores on behavioral tests of APD.
Overall, the SCAN test showed a trend for poorer performance in the LD group, but the group differences were significant only for the Competing Words subtest, which tests binaural separation (Domitz and Schow, 2000). The LD group had significantly poorer performance on the SSW test than the control group, with the left ear showing the greatest deficit. Schow and Chermak's (1999) factor analysis of APD test results indicated that SSW and SCAN Com-peting Word scores measure similar auditory processing abilities . This is supported by the consistency between the SCAN and SSW results in the present study. A correlation analysis also showed that SCAN and SSW competing word scores were related (r = -.56, p < .001). Accord-ing to Bellis's APD classification scheme (Bellis, 1996; Bellis and Ferre, 1999), the pattern of behavioral results in the LD group suggests an integration or associative deficit, owing to dys-function involving the corpus callosum or pri-mary and associative auditory cortex . Anatomic differences in the medial geniculate nucleus in the thalamus, corpus callosum, and auditory cortex have been reported in children with lan-guage and reading difficulties (Galaburda, 1993 ; Galaburda et al, 1994 ; Green et al, 1999; Preis et al, 2000). Anatomic differences in thalamic and cortical auditory areas could be the basis for altered middle latency and cortical evoked poten-tial results in the LD children (Kraus and McGee, 1993 ; Picton et al, 1999).
Previous studies examining ABR changes in adults and children with suspected APD have shown absent peaks or abnormal morphology (Greenblatt et al, 1983 ; Jerger et al, 1987 ; Kraus et al, 1993), reduced amplitudes (Mason and Mellor, 1984), or prolonged latencies (Milicic et al, 1998 ; Yencer, 1998). These are the types of ABR changes typically associated with neu-ropathology such as multiple sclerosis or eighth nerve and brainstem tumors (Hall, 1990). In
the present study, all subjects had normal ABR waveforms, but wave V and III-V latencies were slightly reduced in the LD group. The reason for this is unclear. Subject selection criteria and stimulus and recording characteristics could account for the difference between our ABR find-ings and other studies. In general, ABR changes in children and adults with APD who do not have known neuropathology appear to be small and variable across studies. There is better agreement among studies investigating the effects of APD on later evoked potentials .
Published case studies of MLR in children with APD have shown degraded or absent wave-forms (Jerger and Jerger, 1985 ; Jerger et al, 1987, 1988 ; Musiek et al, 1991). In the latter case, the child was diagnosed as having a sub-arachnoid cyst . Other studies demonstrating more subtle changes such as MLR latency pro-longation or amplitude reductions (Mason and Mellor, 1984 ; Arehole et al, 1995 ; Milicic et al, 1998) were presumably assessing children with less severe underlying auditory pathology. In the present study, the two significant group dif-ferences were prolonged Na latencies and smaller Nb amplitudes in the LD children . The "repre-sentative" MLR waveforms reported by Arehole and colleagues (1995) showed a similar trend for Nb amplitudes to be greater in their control group than in their experimental group of chil-dren with learning difficulties . The MLR wave-forms in Figure 3 suggest other differences between the two groups (Na more negative, Pa reduced amplitude and longer latency), but these were not statistically significant. Arehole and col-leagues (1995) also found no group differences for Pa latencies using a vertex-ipsilateral ear electrode montage, but Pa latencies were sig-nificantly longer in their LD children for a ver-tex-contralateral montage . As in the present study, the average group latency differences were only in the order of 1 to 2 msec, however. Such small latency shifts make it difficult to use MLR latency criteria clinically to identify APD in children . MLR amplitudes appear to have better sensitivity to central auditory ner-vous system pathology than latencies (Musiek and Lee, 1997).
Musiek and colleagues (1999) found that the most sensitive and specific MLR measure in adults with central auditory nervous system lesions was the percentage Na-Pa amplitude difference between contralateral recordings (left ear, right hemisphere versus right ear, left hemi-sphere). The grand-averaged contralateral MLR waveforms in Figure 5 do not show any clear
376

Evoked Potentials in Learning-Disabled Children/Purdy et al
Figure 5 Grand-averaged contralateral middle latency
response waveforms. Right ear/left hemisphere (thick
line) and left ear/right hemisphere (thin line) responses are shown. Left and right hemisphere recordings were
made using C5-Cv2 and C6-Cv2 electrode montages,
respectively. LD = learning disabled .
group asymmetries in the LD children's results. To investigate MLR asymmetry in individual subjects, contralateral Na-Pa amplitude dif-ferences were calculated (bigger-smaller ampli-
tude, divided by smaller amplitude) as recommended by Musiek and colleagues (1999) . Musiek and colleagues suggested that criteria of > 20 to > 50 percent differences in contralat-eral MLR amplitudes might be clinically useful .
In support of Musiek and colleagues' recom-mendations, all children in the LD group had
contralateral differences greater than 20 percent (mean = 60%, range = 23-103%) . Although five children in the control group had small con-tralateral differences (mean = 12%, range = 9-14%), one of the control group children had a
contralateral difference of 21 percent and the remaining four control subjects had substan-tial contralateral differences (55-478%). Thus, for this group of subjects, MLR NaPa con-tralateral differences had good sensitivity but poor specificity.
Musiek (1999) suggested that ear asym-metry may also be an abnormal characteristic of the MLR in APD but stated that electrode
effects are more diagnostic than ear effects. In the present study, ear differences were evident
in the MLR waveforms for the control group in
the region of Nb (see Fig. 3) and were much less
evident in the LD group . Thus, ear asymmetry appears to be a normal characteristic of the MLR in our children . Figure 6 may offer some explanation for the discrepancy between our results and Musiek's . The grand average wave-forms at the top, which shown no ear asymme-try, have been high pass filtered using the same
Figure 6 Right ear grand-averaged MLR waveforms
recorded in control (thick line) and learning-disabled
(thin line) children at the Cz-Cv2 electrode montage.
The top traces, which show no group differences, have
been digitally high pass filtered (12 dB/octave) at 20 Hz .
The bottom traces are the original middle latency response
waveforms that were recorded with 3- to 300-Hz online
filtering .
filter settings as Musiek and colleagues (1999) .
The bottom waveforms that do show the right
ear group difference were recorded using a
wider filter setting. Although MLR ear asym-metry looks promising as an index of abnormal auditory processing in these children, there was considerable individual variability in the
degree of asymmetry, and two of the control group children showed the opposite result, with
a left ear Nb amplitude advantage . Thus, more work is needed to investigate both hemisphere and ear asymmetries in children's MLRs before
such criteria can be applied clinically for the diagnosis of APD.
P3 amplitude was reduced and latency was
prolonged for both deviant and standard stim-uli in the LD children, consistent with Jirsa and Clontz's results (1990) . Jirsa and Clontz only reported P3 results for their deviant stim-
uli. P3 can be elicited by a deviant stimulus in
both active and passive paradigms (Zenker and Barajas, 1999). A P3 response to the standard stimulus in an oddball paradigm is not nor-
mally reported but was evident in the results from both groups of children in the present
study. A "Ma" peak can be recorded when sub-
jects are ignoring the stimuli in an oddball par-
adigm. Ma is thought to reflect an attention
switch owing to the stimulus being noticed (Stapells, 2002) . Since the children were instructed not to attend to the standard stimu-lus, the P3 elicited by the standard is presum-ably a "P3a-like" response . As shown in Figure 4, on average, there was little difference in the
377

Journal of the American Academy of Audiology/Volume 13, Number 7, July/August 2002
cortical responses to the standard and deviant stimuli in the P3 latency region in the LD group. The finding of group differences for P3 elicited by both standard and deviant stimuli suggests that both passively and actively elicited P3 may be useful diagnostic tools for investigating audi-tory processing .
P1 latencies were shorter in the LD children for both the standard and deviant stimuli. Changes in P1 latency have not been reported previously in LD children, but most studies have focused on N1 and P2 rather than P1 . The latency of MLR wave Pb, which is regarded as equivalent to Pl, is altered in stutterers (Diet-rich et al, 1995) and adults with autism (Buch-wald et al, 1992). Dietrich and colleagues (1995) found shorter Pb latencies in adult stutterers compared with age-matched control subjects . Researchers have suggested that abnormal metabolism and/or neurotransmitter function in the thalamic reticular activating system may underlie Pb/P1 abnormalities in autism, stut-terers, schizophrenia, and Alzheimer's disease (Dietrich et al, 1995).
The reduction in N1 amplitudes in the LD children is consistent with other studies (Ton-nquist-Uhlen, 1996b ; Bruneau et al, 1999 ; Seri et al, 1999 ; Cunningham et al, 2001; Wioland et al, 2001). P2-N2 amplitudes were larger in the LD children, consistent with Bernal and col-leagues (2000), who also used an oddball para-digm and found larger N2 and P2 peaks in children with suspected APD who were poor readers. The CAEP results indicate that changes in cortical processing account for, at least in part, the auditory processing difficulties expe-rienced by the LD children .
Quite a number of studies have now demon-strated abnormal CAEP in adults and children with APD. More research effort is required, how-ever, to establish the normative data that are needed clinically to use CAEP recordings to diagnose APD in children . There are consider-able maturational and aging effects on Pl, Nl, P2, and P3 latencies, amplitudes, and scalp dis-tribution (Pearce et al, 1989 ; Johnstone et al, 1996 ; Oades et al, 1997). CAEPs with very abnor-mal morphology or absent responses could be used clinically to assist diagnosis of APD. Although all of the LD children had obligatory CAEP responses, not all (only 40%) had a P3 to the deviant stimuli that was different from the response to the standard stimuli.
The recent Bruton Conference (Jerger and Musiek, 2000) on APD concluded that electro-physiologic testing can assist in the differen-
tial diagnosis ofAPD in school-aged children. The Bruton Conference recommended the use of ABR and MLR. ABR did not appear to be a use-ful diagnostic tool for the group of LD subjects with suspected APD investigated here but would play an important role in diagnosis of auditory neuropathy/dyssynchrony disorders (Berlin, 1999). In the present study, both MLR and cor-tical evoked potentials were sensitive to the suspected APD in the children with learning difficulties . This was based on an analysis of group data, however, and relatively few indi-vidual children in the LD group showed extremely abnormal results. Thus, further work is required to establish validated clinical crite-ria for identifying evoked potential abnormali-ties in individual children with suspected APD.
Acknowledgment . This work was supported by a grant from the New Zealand Lottery Grants Board Health Research Committee . We thank Professor Ivan Beale and Dr. Sue Beechey for their assistance in recruitment of subjects for this research .
Part of this study was presented at the Midwinter Meeting of the Association for Research in Otolaryngol-ogy, St. Petersburg's Beach, FL, February 1995 .
REFERENCES
Akkuzu B, Fisiloglu AG, Ozluoglu L, Can U. (2001) . Sudden cortical hearing loss for speech : a case report . Ear Hear 22:14-17 .
American Speech-Language-Hearing Association (ASHA) Task Force on Central Auditory Processing Development. (1996) . Central auditory processing : current status of research and implications for clinical practice . Am J Audiol 5:41-54.
Arehole S. (1995). A preliminary study of the relation-ship between long latency response and learning disorder. Br JAudiol 29:295-298 .
Arehole S, Augustine LE, Simhadri R. (1995) . Middle latency response in children with learning disabilities : preliminary findings . J Commun Disord 28:21-38 .
Arnst DJ, Doyle PC . (1983). Verification of the corrected Staggered Spondaic Word (SSW) score in adults with cochlear hearing loss . Ear Hear 4:243-246 .
Baldeweg T, Richardson A, Watkins S, et al . (1999) . Impaired auditory frequency discrimination in dyslexia detected with mismatch evoked potentials . Ann Neurol 45:495-503 .
Bellis TJ. (1996) . Central Auditory Processing Disorders. San Diego: Singular.
Bellis TJ, Ferre JM . (1999) . Multidimensional approach to the differential diagnosis of central auditory process-ing disorders in children . JAm Acad Audiol 10:319-328 .
Berlin CI . (1999) . Auditory neuropathy. Using OAEs and ABRs from screening to management . Semin Hear 20:307-313 .
378

Evoked Potentials in Learning-Disabled Children/Purdy et al
Bernal J, Harmony T, Rodriguez M, et al. (2000) . Auditory event-related potentials in poor readers . Int J Psychophysiol 36:11-23 .
Bradlow AR, Kraus N, Nicol TG, et al . (1999) . Effects of lengthened formant transition duration on discrimina-tion and neural representation of synthetic CV syllables by normal and learning-disabled children . JAcoust Soc Am 106:2086-2096 .
Bruneau N, Roux S, Adrien JL, Barthelemy C. (1999) . Auditory associative cortex dysfunction in children with autism : evidence from late auditory evoked potentials (N I wave-T complex) . Clin Neurophysiol 110:1927-1934 .
Gelfand SA, Schwander T, Silman S. (1990) . Acoustic reflex thresholds in normal and cochlear-impaired ears : effects of no-response rates on 90th percentiles in a large sample . J Speech Hear Disord 55:198-205.
Green RL, Hutsler JJ, Loftus WC, et al . (1999). The caudal infrasylvian surface in dyslexia : novel magnetic reso-nance imaging-based findings . Neurology 53:974-981 .
Greenblatt ER, Bar A, Zappulla RA . (1983) . Learning disability assessed through audiologic and physiologic measures : a case study. J Commun Disord 16:309-313 .
Hall JW III . (1990) . Handbook of Auditory Evoked Responses . Boston : Allyn and Bacon.
Buchwald JS, Erwin R, Van Lancker D, et al . (1992) . Midlatency auditory evoked responses: PI abnormalities in adult autistic subjects . Electroencephalogr Clin Neurophysiol 84 :164-171 .
Buschke H, Fuld PA. (1974) . Evaluating storage, reten-tion, and retrieval in disordered memory and learning . Neurology 24:1019-1025 .
Cacace AT, Satya-Murti S, Wolpaw JR. (1990) . Human middle-latency auditory evoked potentials : vertex and temporal components . Electroencephalogr Clin Neurophysiol 77:6-1.8 .
Celebisoy N, Aydogdu 1, Ekmekci O, Akurekli O. (1996) . Middle latency auditory evoked potentials (MLAEPs) in (MS) . Acta Neurol Scand 93 :318-321 .
Chermak GD. (2001) . Auditory processing disorder: an overview for the clinician. Hear J 54:10, 12, 16, 18-22, 25 .
Chermak GD, Musiek FE . (1997) . Central Auditory Processing Disorders . San Diego : Singular.
Cunningham J, Nicol T, Zecker SG, et al . (2001) . Neurobiologic responses to speech in noise in children with learning problems : deficits and strategies for improvement. Clin Neurophysiol 112:758-767 .
Dalebout SD, Fox LG. (2001) . Reliability of the mismatch negativity in the responses of individual listeners. JAm Acad Audiol 12:245-253 .
Deiber MP, Ibanez V, Fischer C, et al . (1988) . Sequential mapping favours the hypothesis of distinct generators for Na and Pa middle latency auditory evoked potentials . Electroencephalogr Clin Neurophysiol 71:187-197 .
Dietrich S, Barry SJ, Parker DE . (1995) . Middle latency auditory responses in males who stutter. J Speech Hear
Res 38:5-17.
Domitz DM, Schow RL . (2000) . A new CAPD battery-multiple auditory processing assessment : factor analysis and comparisons with SCAN . Am JAudiol 9:101-111 .
Fifer RC, Sierra-Irizarry B . (1988). Clinical applications of the auditory middle latency response . Am J Otol
9(Suppl) :47-56 .
Galaburda AM. (1993) . Neurology of developmental dyslexia . Curr Opin Neurobiol 3:237-242 .
GalaburdaAM, Menard MT, Rosen GD . (1994) . Evidence for aberrant auditory anatomy in developmental dyslexia . Proc Nall Acad Sci U S A 91:8010-8013 .
Hammill DD . (1985) . DTLA-2 Detroit Tests of Learning Aptitude . Austin, TX : Pro-Ed .
Hood LJ, Berlin CI, Allen P. (1994) . Cortical deafness : a longitudinal study. J Am Acad Audiol 5 :330-342 .
Hyde M. (1977) . The NI response and its applications . Audiol Neurotol 2:281-307 .
Jasper HH. (1958) . The ten-twenty system of the inter-national federation. Electroencephalogr Clin Neurophysiol 10:371-375 .
Jerger J, Musiek F. (2000) . Report of the Consensus Conference on the Diagnosis of Auditory Processing Disorders in School-Aged Children . J Am Acad Audiol 11:467-474 .
Jerger J, Oliver T, Chimel R. (1988) . Auditory middle latency response : a perspective. Semin Hear 9:75-86 .
Jerger J, Johnson K, Jerger S, et al . (1991) . Central audi-tory processing disorder : a case study. JAm Acad Audiol 2:36-54 .
Jerger JF . (1972) . Suggested nomenclature for imped-ance audiometry. Arch Otolaryngol 96:1-3 .
Jerger S, Jerger J. (1985). Audiologic applications of early, middle, and late auditory evoked potentials . Hear J 38:31-36 .
Jerger S, Martin RC, Jerger J. (1987) . Specific auditory perceptual dysfunction in a learning disabled child. Ear Hear 8:78-86 .
Jirsa RE, Clontz KB . (1990) . Long latency auditory event-related potentials from children with auditory processing disorders. Ear Hear 11:222-232 .
Johnstone SJ, Barry RJ, Anderson JW, Coyle SF. (1996). Age-related changes in child and adolescent event-related potential component morphology, amplitude and latency to standard and target stimuli in an auditory oddball task. Int J Psychophysiol 24:223-238 .
Kadoya C, Wada S, Matsuoka S. (1988) . Clinico-experi-mental studies on auditory evoked middle latency response (AEMLR) with specific reference to generation
and auditory dominaney. J Univ Occup Environ Health Jpn 10:11-30 .
Katz J. (1968) . The SSW test : an interim report . J Speech Hear Disord 33:132-146 .
Keith RW. (1986) . SCAN: A Screening Test for Auditory Processing Disorders. Harcourt Brace Jovanovich .
379

Journal of the American Academy of Audiology/Volume 13, Number 7, July/August 2002
Kileny P, Paccioretti D, Wilson AF. (1987). Effects of cor-tical lesions on middle-latency auditory evoked responses (MLR). Electroencephalogr Clin Neurophysiol 66:108-120 .
Korpilahti P, Lang HA . (1994) . Auditory ERP components and mismatch negativity in dysphasic children . Electroencephalogr Clin Neurophysiol 91:256-264 .
Oades RD, Dittmann-BalcarA, Zerbin D. (1997) . Development and topography of auditory event-related potentials (ERPs) : mismatch and processing negativity in individuals 8-22 years of age. Psychophysiology 34:677-693 .
Ozdamar O, Kraus N. (1983). Auditory middle-latency responses in humans . Audiology 22:34-49 .
Kraus N, McGee T. (1988) . Color imaging of the human middle latency response . Ear Hear 9:159-167 .
Kraus N, McGee T. (1993) . Clinical implications of pri-mary and nonprimary pathway contributions to the middle latency response generating system. Ear Hear 14:36-48.
Kraus N, McGee T, Ferre J, et al . (1993) . Mismatch neg-ativity in the neurophysiologic/behavioral evaluation of auditory processing deficits : a case study. Ear Hear 14:223-234 .
Kraus N, McGee TJ, Carrell TD, et al . (1996) . Auditory neurophysiologic responses and discrimination deficits in children with learning problems . Science 273:971-973 .
Lindamood C, Lindamood P. (1979) . Lindamood Auditory Conceptualization Test . Austin, TX: Pro-Ed .
Marosi E, Harmony T, Becker J. (1990) . Brainstem evoked potentials in learning disabled children . Int J Neurosci 50:233-242 .
Marvel JB, Jerger JF, Lew HL . (1992) . Asymmetries in topographic brain maps of auditory evoked potentials in the elderly. J Am Acad Audiol 3:361-368.
Mason SM, Mellor DH. (1984) . Brain-stem, middle latency and late cortical evoked potentials in children with speech and language disorders . Electroencephalogr Clin Neurophysiol 59:297-309 .
McGee TJ, King C Tremblay K, et al . (2001) . Long-term habituation of the speech-elicited mismatch negativity. Psychophysiology 38:653-658 .
Milicic D, Alcada MN, Pais Clemente L, et al. (1998) . A study of auditory afferent organization in children with dyslalia. Int J Pediatr Otorhinolaryngol 46:43-56 .
Musiek F, Charette L, Kelly T, et al . (1999). Hit and false-positive rates for the middle latency response in patients with central nervous system involvement . J Am Acad Audiol 10:124-132 .
Musiek FE . (1999) . Central auditory tests . Scand Audiol Suppl 51:33-46 .
Musiek FE, Lee WW (1997) . Conventional and maxi-mum length sequences: middle latency response in patients with central nervous system lesions. JAm Acad Audiol 8:173-180 .
Musiek FE, Verkest SB, Gollegly KM . (1988) . Effects of neuro-maturation in auditory-evoked potentials . Semin Hear 9:1-13 .
Musiek FE, Lenz S, Gollegly KM. (1991) . Neuroaudiologic correlates to anatomical changes of the brain . Am JAudiol 1 :19-24 .
Musiek FE, Baran JA, Pinheiro ML. (1994) . Neuroaudiology Case Studies . San Diego : Singular.
Ozdamar 0, Kraus N, Curry F. (1982) . Auditory brain stem and middle latency responses in a patient with cor-tical deafness . Electroencephalogr Clin Neurophysiol 53:224-230 .
Pearce JW, Crowell DH, TokiokaA, Pacheco GP. (1989) . Childhood developmental changes in the auditory P300 . J Child Neurol 4:100-106 .
Picton TW, Alain C, Woods DL, et al . (1999) . Intracerebral sources of human auditory-evoked potentials . Audiol Neurootol 4:64-79 .
Picton TW Alain C, Otten L, et al . (2000). Mismatch neg-ativity : different water in the same river. Audiol Neurootol 5:111-139.
Ponton C, Eggermont JJ, Khasla, et al . (2002) . Maturation of human central auditory activity : separating auditory evoked potentials by dipole source modeling. Clin Neurophysiol 112:319-323.
Preis S, Steinmetz H, Knorr U, Jancke L. (2000) . Corpus callosum size in children with developmental language disorder. Brain Res Cogn Brain Res 10:37-44 .
Sanger DD, Keith RW Maher BA . (1987) . An assessment technique for children with auditory-language process-ing problems . J Commun Disord 20 :265-279 .
Satya-Murti S, CacaceAT, Hanson PA. (1979) . Abnormal auditory evoked potentials in hereditary motor-sensory neuropathy. Ann Neurol 5:445-448 .
Schow RL, Chermak G. (1999) . Implications from factor analysis for central auditory processing disorders. Am J Audiol 8:137-142 .
Schroger E, Wolff C. (1998) . Attentional orienting and reorienting is indicated by human event-related brain potentials . Neuroreport 9:3355-3358 .
Schulte-Korne G, Deimel W Bartling J, Remschmidt H. (1998) . Auditory processing and dyslexia : evidence for a specific speech processing deficit . Neuroreport 9: 337-340.
Schulte-Korne G, Deimel W, Bartling J, Remschmidt H. (1999) . Pre-attentive processing of auditory patterns in dyslexic human subjects . Neurosci Lett 276:41-44 .
Schulte-Korne G, Deimel W Bartling J, Remschmidt H. (2001) . Speech perception deficit in dyslexic adults as measured by mismatch negativity (MMN). Int J Psychophysiol 40:77-87 .
Seri S, Cerquiglini A, Pisani F, Curatolo P (1999). Autism in tuberous sclerosis: evoked potential evidence for a deficit in auditory sensory processing . Clin Neurophysiol 110:1825-1830 .
Setzen G, CacaceAT, Eames F, et al . (1999) . Central deaf-ness in a young child with moyamoya disease : paternal

Evoked Potentials in Learning-Disabled Children/Purdy et al
linkage in a Caucasian family : two case reports and a review of the literature . Int J Pediatr Otorhinolaryngol 48 :53-76 .
Starr A, Sininger YS, Pratt H. (2000) . The varieties of auditory neuropathy. J Basic Clin Physiol Pharmacol 11:215-230 .
Sharma A, Kraus N, McGee TJ, Nicol TG . (1997) . Developmental changes in Pl and N1 central auditory responses elicited by consonant-vowel syllables . Electroencephalogr Clin Neurophysiol 104:540-545 .
Shehata-Dieler W Shimizu H, Soliman SM, Tusa RJ . (1991) . Middle latency auditory evoked potentials in tem-poral lobe disorders. Ear Hear 12:377-388 .
Silman S, Silverman CA, Emmer MB. (2000) . Central auditory processing disorders and reduced motivation : three case studies. J Am Acad Audiol 11 :57-63 .
Schroer H, Student M. (1978) . Auditory nerve and brain-stem evoked responses in normal, autistic, minimal brain dysfunction and psychomotor retarded children . Electroencephalogr Clin Neurophysiol 44:380-388 .
Smoski WJ, Brunt MA, Tannahill JC . (1992) . Listening characteristics of children with central auditory pro-cessing disorders. Lang Speech Hear Serv Sch 23:145-152 .
Squires KC Hecox KE . (1983) . Electrophysiological eval-uation of higher level auditory processing . Semin Hear 4:415-433 .
Squires NK, Squires KC Hillyard SA . (1975) . Two vari-eties of long-latency positive waves evoked by unpredictable auditory stimuli in man. Electroencephalogr Clin Neurophysiol 38:387-401 .
Stach B, Hudson M. (1990) . Middle and late auditory evoked potentials in multiple sclerosis. Semin Hear 11:265-275 .
Stapells DR . (2002) . Cortical event-related potentials to auditory stimuli. In : Katz J, ed . Handbook of Clinical Audiology. 5th Ed . Philadelphia : Lippincott Williams & Wilkins, 378-406.
Starr A, Picton TW Sininger Y, et al . (1996) . Auditory neuropathy. Brain 119(Pt 3) :741-753 .
Steinschneider M, Kurztberg D, Vaughan HG. (1992) . Event-related potentials in developmental neuropsy-chology. In : Rapin I, Segalowitz SJ, eds. Handbook of Neuropsychology. Vol. 6. Child Neuropsyehology. Amsterdam: Elsevier, 239-298.
Suzuki T, Hirabayashi M. (1987) . Age-related morpho-logical changes in auditory middle-latency response . Audiology 26:312-320 .
Tonnquist-Uhlen 1 . (1996a). Topography of auditory evoked cortical potentials in children with severe lan-guage impairment . Scand Audiol Suppl 44:1-40.
Tonnquist-Uhlen I . (1996b). Topography of auditory evoked long-latency potentials in children with severe language impairment : the P2 and N2 components . Ear Hear 17:314-326 .
Tucker DA, Ruth RA . (1996) . Effects of age, signal level, and signal rate on the auditory middle latency response . J Am Acad Audiol 7 :83-91 .
Verkindt C, Bertrand O, Perrin F, et al . (1995) . Tonotopic organization of the human auditory cortex : N100 topography and multiple dipole model analysis . Electro-encephalogr Clin Neurophysiol 96:143-156 .
Webster RE . (1981) . Learning Efficiency Test Manual. Novato, CA : Academic Therapy Publications.
Yencer KA . (1998) . The effects of auditory integration training for children with central auditory processing disorders. Am JAudiol 7 :1-13 .
Wioland N, Rudolf G, Metz-Lutz MN. (2001) . Electrophysiological evidence of persisting unilateral auditory cortex dysfunction in the late outcome of Landau and Kleffner syndrome . Clin Neurophysiol 112:319-323 .
Zenker F, Barajas JJ . (1999) . Auditory P300 development from an active, passive and single-tone paradigms . Int J Psychophysiol 33 :99-111 .

Journal of the American Academy of Audiology/Volume 13, Number 7, July/August 2002
APPENDIX
Teacher Evaluation of Classroom Listening Skills
Please rate this child's behavior compared to other children of similar age and background .
SECTION A. RESPONSE CHOICES: less difficulty . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . +1 same amount of difficulty . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0 slightly more difficulty . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . -1 more difficulty . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . -2 considerably more difficulty . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . -3 significantly more difficulty . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . -4 cannot function at all . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . -5
1 . If listening in a room where there is background noise such as others talking, children playing etc., this child has difficulty hearing and understanding . . . . . +1 0 -1 -2 -3 -4 -5
2. If listening in a quiet room (others may be present but are being quiet), this child has difficulty hearing and understanding . . . . . . . . . . . . . . . . . . . . . . . . . . . .+1 0 -1 -2 -3 -4 -5
3. When listening in ideal conditions (quiet room, no distractions, face to face, good eye contact), this child has difficulty hearing and understanding . . . . . . . . . +1 0 -1 -2 -3 -4 -5
4. This child has difficulty following multistage oral instructions . .+1 0 -1 -2 -3 -4 -5
SECTION B. RESPONSE CHOICES (Please circle YES or NO) 1. This child appears to have trouble picking up new spoken information and may require several
repetitions in order to understand the material . . . . . . . . . . . . . . . . . . . . . . . . YES NO 2. This child frequently requires visual cues to help understand the curricula, in addition to
auditory information . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . YES NO 3. This child has difficulty recalling auditory information compared with other
children . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .YES NO 4. The child displays difficulty formulating or generating expressive language and/or displays
inappropriate use of language . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . YES NO If YES, please explain:
5. The child displays language problems (evidenced in the use of inappropriate "wh" questions, pro-nouns, word order, possessiveness, verb tenses) . . . . . . . . . . . . . . . . . . . . . . . YES NO
If YES, please explain:
6. The child displays problems with articulation (phonology) consisting of substitutions, distortions, or omissions of sounds in words (especially when producing words that are similar auditorily) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .YES NO
If YES, please explain: