Embed Size (px)
Citation preview

American Academy of Audiology • 8300 Greensboro Drive, Suite 750, McLean, VA 22102-3611
Caring for America’s Hearing
AMERICAN WARTIME MILITARY AUDIOLOGYAMERICAN WARTIME MILITARY AUDIOLOGYOn the Origins of Audiology
AUDIOLOGY TODAY • MONOGRAPH NO. 1 • JANUARY 2002WRITTEN BY MOE BERGMAN, EDD

The origin of our specialty of audiology is generally acknowledged to have evolved from therehabilitative services developed by the military during the World Wars I and II. However,we have never had a well-documented historical account to the “birth” of our profession.
This monograph on the early beginnings of audiology has been meticulously researched and writ-ten by Moe Bergman and will finally fill that void in our literature. Professor Moe Bergman, whoas a young military soldier, was present and deeply involved in the development of the militaryaural rehabilitation services in several major Army hospitals during World War II and providesfirst-hand descriptions for us of the various early military audiology programs.
Moe Bergman is an internationally noted audiologist who has received numerous honors frommany of our professional societies for his contributions to the field. Bergman holds degrees fromthe University of Illinois (A.B., 1937) and Columbia University in New York (M.A., 1939).Following his military service, he returned to Columbia University to earn a doctorate degree in1949. He taught at Hunter College of the City University of New York (1953-1976) and was the
first Program Director of the Speech and Hearing Sciences Department. During his Hunter College years, Bergman was an out-standing professor, keen researcher and active leader in audiological issues and programs. As a Professor Emeritus of HunterCollege of the City University of New York, he re-located to Tel-Aviv, Israel in 1976 to serve as a Professor in the SacklerSchool of Medicine where he was ultimately honored with a second Emeritus award in 1985. During his retirement, Bergmanhas remained active in audiology and devoted considerable time and effort to the development of this valuable monograph.
In this monograph audiologists will find a fascinating account of the development of hearing testing activities used by the mili-tary hospital centers of World Wars I and II. With little prior experience, selected military and civilian personnel found it nec-essary to develop hearing services programs based on aural rehabilitation procedures and the fitting of hearing aids to largenumbers of active duty soldiers and sailors. Many of the personnel involved in these early military programs went on to devel-op academic university audiology programs following their wartime service.
The American Academy of Audiology is proud to publish this historical account of the origins of our profession of audiology.This special monograph will undoubtedly become required reading for students of audiology and hearing sciences and no doubtserve as a useful reference document for all audiologists. We are all grateful and, indeed, indebted to Professor Moe Bergmanfor providing this legacy of our profession.
Jerry L. Northern, EditorAudiology Today
Of the many pioneers who were present during the early formative years of the professionduring and shortly after World War II, none had a better view than Moe Bergman. As ayoung recruit in the Army Medical Corps he was assigned to the Aural Rehabilitation
program at Hoff General Hospital, Santa Barbara, California. Here he rose to the rank of secondlieutenant. When the war ended, after the bombing of Hiroshima and Nagasaki, he was transferredto Borden General Hospital in Chickasha Oklahoma where he served the remainder of his armytour of duty. In 1945 Moe visited the third army installation, Deshon General Hospital, ButlerPennsylvania, on a tour to compare experiences at the three units, Hoff, Borden and Deshon. Thisexperience uniquely prepared him for his life’s work in audiology and aural rehabilitation. In hisarmy travels and assignments he encountered many of the early giants in the field; Ira Hirsh,Grant Fairbanks, Raymond Carhart, Leo Doerfler, Herbert Koepp-Baker, Mary Woods Whitehurst,Shirley Stein, William Hardy, Miriam Pauls, Harriet Haskins, Fran Sonday, Louie DiCarlo, JohnDuffy, Freeman McConnell, Frank Lassman, Elizabeth Nitchie, and many others. This unique per-spective served Moe well in his subsequent career. He went on to develop audiology programs at
Hunter college in New York City and more recently in Tel Aviv in his adopted land of Israel.
In this account of American Wartime Military Audiology Moe sketches for us not only the structural and hierarchical frame-works of the various rehabilitation units but the different philosophies brought to the common mission and the wide resourcesthe military was able to muster to help the soldiers and sailors of World War II. He captures the spirit and excitement of thoseearly years in the development of our profession.
James F. JergerDallas, Texas
ACKNOWLEDGMENT
James Jerger
Jerry Northern

Origins of Audiology World War II Programs1
It is important for every profession to document its origins.It should be of interest to today’s practitioners of audiologyto know how the American military “aural rehabilitation”
programs for hearing casualties in the 20th century world warspracticed what is now known as “audiology.” The multidisci-plinary organization of personnel and services in those pro-grams and the introduction of electronic equipment for audi-tory measurements and hearing testing in the WWII centerswas a historic landmark in the evolution of clinical audiology.
Every so often there is an allusion in published materialsto the origins of the military aural rehabilitation programs ofWorld War II, apparently based upon what the writer mayhave heard or read from others who were not directlyinvolved in those programs. Fortunately, there are still a few(very few!) of us still extant who were in one or another ofthose programs from their inception to their termination, andwho still have archival material, military records and docu-ments of our service and authorized military travel at thetime. The following account draws upon retained memorabil-ia and documents, memories of participation by the writerand other contacted survivors, and reports published by others immediately or shortly after the war.
Of the three U.S. Army programs established during WW II, the only one that was fully described by an activemember of that program was the one at Borden General Hospital at Chickasha, Oklahoma, in a report dated 1 July1946, and edited by the late Grant Fairbanks (Fairbanks, 6. 1946). I had been a member of the Borden GeneralHospital program for a short period after active duty at the Hoff General Hospital Center (at which I had beensince its inception), was then deactivated, and as a staff member I received a copy of the report which is still in mypossession. While departures from the Borden General Hospital procedures at the other centers are noted in thedetailed accounts of each center that follow, the report by Fairbanks provides a good framework description ofthe programs at all three Army centers.
Historical accounts of the aural rehabilitation programs were published at the close of that war and shortlythereafter by those who had central responsibility for them in the Surgeon General’s offices in the Pentagon(Morrissett, L.E., 1957; Canfield, N. and Morrissett, L.E. 1947), or who headed the Navy program (Lederer, F. L.,1946), or were personnel in one of the aural rehabilitation centers (Bergman, M., 1957; Scriver, H. 1944; Carhart,R. 1946 a,b,c,d; 1947 a,b), or who were otherwise knowledgeable about the program (Hillman, C.C., 1944). Inaddition, I retained an operating manual of the Hoff General Hospital Center and various written communicationsof that period, that will be cited in this monograph.
Moe Bergman, EdDTel Aviv, Israel
AUTHOR’S FOREWORD
REHABILITATION OF AMERICAN WARTIME HEARING CASUALTIES IN WORLD WARS I AND IIthe beginnings of
clinical audiology
Moe Bergman

✯✯✯✯✯THE WORLD WAR I PROGRAMThe dangerous implications of hearingloss were recognized in World War I,resulting in the activation of a hearingrehabilitation program at the Army’sGeneral Hospital No. 11 at Cape May,New Jersey. Hillman (1944) wrote that“In the first World War, 1 man in 5,000was discharged for defective hearing”,and “the average annual admission rateto Army hospitals for deafness anddefective hearing was approximately 1in 1,000 per annum.” (“Communicationfrom Statistical Division, Office of theSurgeon General, Oct. 30, 1943”).
The basic rehabilitative treatment atthe New Jersey Cape May Center wasthe teaching of lip reading by eleventeachers who were considered to beexperts in that field. ( Morrissett, 1957;Hillman 1944). Morrissett (p. 448)quotes Berry, whose summary of the pro-gram in 1942 stated that “The men weresaturated with lip reading, in an opti-mistic environment of devoted service.”There does not seem to be any report ofthe use of electric or electronic amplifi-cation in that program.
Despite predictions of thousands ofaural casualties, only 108 soldiers wereprocessed through the Cape May Centerprogram in the year of its operation, butapparently hundreds more were recognizedafter discharge from the Army. By October1943 the U.S. Veterans Administrationhad on its rolls for compensation 416“totally deaf” and 12,397 “partially deaf-ened” veterans of WW I. (Morrissett, p.447). It was suspected that a large num-ber of the soldiers treated at Cape Mayhad auditory problems before inductioninto the service, an important observationthat we made as well in World War II.
In the quarter century between theWW I program and our programs inWW II, electric (carbon microphone)hearing aids and then electronic hearingaids had been introduced. The emphasisin the rehabilitation programs for adultswith hearing impairment was still onthe development of new communica-tion skills, including lip reading, “auric-ular” (auditory) training and speechconservation and correction. In fact,many of the civilian and military per-sonnel of the Army and Navy centershad previously been engaged in thework in leagues for the hard of hearingor similar organizations. The December1943 issue of the Bulletin of the New YorkLeague for the Hard-of-Hearing reportedthat then-Major Leslie E. Morrissett,Chief of ENT at the program at theBorden General Hospital in Chickasha,Oklahoma (later to become the Chief,Otolaryngology Branch, Office of theSurgeon General), “spent long hoursobserving lip reading classes and dis-cussing the subjects of auricular training,hearing aids and recreation with mem-bers of the (NY) League Staff.” H. Davis(1947, p. 12) cites Miriam Pauls Hardy’sview of “how admirably speech readingand a hearing aid supplement eachother”, clearly equating their contribu-tions to the rehabilitation process.
This understanding of the auralrehabilitation problem, in the WorldWar II programs, was also expressedclearly in the Borden historical report oftheir program: “The early directives andoral pronouncements specified onlyhearing aids and lip reading in additionto medical treatment, and it is clearfrom these statements that the hearingaid problem was regarded almost entire-
ly as one of engineering. Experienceswiftly revealed, however, that suchtreatment did not provide total auralrehabilitation.” (Fairbanks, 1946, p. 28)
An engaging comment by Ledererand Hardy (1946), reporting on theWW II U.S. Navy program, hints at theresidual confidence of their staff in thecentrality of lip (speech) reading in therehabilitative process, rather than thehearing aid. Lederer and Hardy found itnecessary to express their view that thehearing aid should be fitted as early aspossible in the rehabilitation program,since “The gains in confidence and theease of communicative and socialadjustments more than compensate forany lag of effort to master speech read-ing.” (ibid p. 437)
THE WW II PROGRAMSIn anticipation of a large number ofaural casualties of the tremendouslyenhanced explosive arsenals and of thenoisy new war machines, such as tanksand sophisticated aircraft in WW II, theAmerican Army designated threeGeneral Hospitals as specialized centersfor hearing treatment in May 1943. Thelater chiefs of the program in Washington,D.C., Canfield and Morrissett (1947)credit otologist Dr. Walter Hughson as“the chief inspiration for the armed-service programs...” (Ibid p. 322)
The three hearing treatment centerswere placed geographically, at HoffGeneral Hospital in Santa Barbara,California; Borden General Hospital inChickasha, Oklahoma; Walter ReedGeneral Hospital in Washington, D.C.The Walter Reed Center, which was thefirst designated for the purpose in the
2Origins of Audiology World War II Programs
Many aspects of early audiology in the U.S. had been developed in the civilian leagues for the hard-of-hearing at the beginning of the 20th century. These early aspects of what is now known in general as“audiology” involved new services for adults to complement the ongoing educational programs that weredirected at hearing impaired children in previous decades. These new services were introduced mainly byadults who were themselves suffering with hearing impairment, and by teachers of hearing impaired children who were recruited by the former to teach them alternate communication skills. There was also a growing awareness of the increasing numbers of the aging population, many of them with hearing problems. In short, there was a growing realization that impaired hearing occurred not only in children,and not only in severe or profound forms, but that any noticeable hearing loss was a potential impedimentto a comfortable and productive life. Clear also, was the threat of hearing loss accompanying modern warcaused directly by its noisy machines and greatly enhanced firepower.
INTRODUCTION& Background

spring of 1943, and was headed by Lt.Col. Marion B. Mobley, was soon movedfrom that busy hospital to the DeshonGeneral Hospital in Butler, Pennsylvania.After activation of the Army centers inthe autumn of 1943, the Navy set up itscenter at the U.S. Naval Hospital inPhiladelphia in the spring of 1944.
In circular No. 81, issued Feb. 23,1944, the War Department directed that“every case in which the impairment ofhearing within the conversational range(256-2048 cycles per second) or a loss of3/16 or below to a whispered voice whenan audiometer is not available, in a caseof stationary or progressive deafness freefrom acute inflammatory aural disease, willbe transferred to a hospital designated forthe rehabilitation of the deaf at the earli-est practicable date” (Hillman, 1944).
The three Army centers processedabout 10,000 patients, while the NavalAural Rehabilitation Center admittedabout 4,000 (Canfield and Morrissett,1947; Morrissett, 1957). Many of the sol-diers seen at the centers had pre-servicehearing loss, undetected mainly to theinadequacy of the hearing tests adminis-tered to the draftees at the inductioncenters. In fact, even some men withlong-term losses were accepted. (Canfield &Morrissett, 1947). For example, dataassembled at the Hoff General HospitalCenter, and probably representative ofthe remaining military centers, revealedthat the hearing problem was of recentonset (presumably during service) inonly 15% of the patients, while 65% hadhearing loss for over 4 years and 31 % forover 12 years! (Morrissett, 1957 p. 458).
THE ARMY CENTERSMajor Leslie E. Morrissett, who
had been at the Borden General Hospitalsince January 1943, was later appoint-ed chief of the combined ENT Sectionand the program in Aural Rehabilitation inthe summer of 1943. (Fairbanks 1946,p. 3). In July of 1944 Morrissett wastransferred to the Surgeon General’sOffice in Washington, D.C. to head theentire Army hearing treatment program.
The Army programs in California,Oklahoma and Pennsylvania beganreceiving patients at about the sametime in the Fall of 1943, and after sev-eral feverish months devoted to therecruitment of both military and civil-ian staff, and the organization of hear-ing test and hearing aid selection pro-cedures, the Surgeon General’s Officearranged a conference of the medicalheads and key personnel of the three
Army Centers to meet at Hoff GeneralHospital, February 2-4, 1944 to coordi-nate their functions. Morrissett laterreferred to this meeting as a“Conference on Rehabilitation of theHard of Hearing” (Morrissett 1957; pp449-450). I recall that in addition tothe chief otologist from each Center,the nonmedical military staffs wererepresented by Francis Sonday, whohad been first at the Walter ReedCenter and then transferred to Butler,Pa., Raymond H. Hull (unrelated toour present distinguished colleague ofthe same name) of the Borden Centerand myself representing the HoffCenter. I do not have any official sum-mary of that conference, but in a briefpublished summary of the conference,written in 1945-46 (but not publisheduntil 1957), Morrissett includes amongour conference’s recommendations,“Hearing aids should be furnished toall deafened and hard of hearing in theArmy instead of, at present, only tomen with hearing impairment incurredin [the] line of duty.” (Morrissett, 1957).
There was agreement by the confer-ees that there should be a general uni-form plan for the three hearing centers,but that personnel should be free tostudy and institute new procedures.Later, after a visit to two of the centers,in June 1944, the Chief of the SurgicalConsultants Division of the SurgeonGeneral’s Office recommended thatthere be uniformity of activities andstandardization of equipment at all ofthem. This is the recommendation thatled to the appointment of Major LeslieE. Morrissett to Washington to coordi-nate the various Army programs.
As noted above, the beginning ofthe individual programs in 1943 con-tinued to resemble the WW I program,except with the addition of the puretone audiometer and the introductionof the body-worn hearing aids of theperiod. The organization chart that
would reflect one of the programs(Borden) after activation in late 1943and early 1944 would include, underthe Ear, Nose and Throat Section ofthe hospital just two sub-sections: LipReading and Audiometry and HearingAids. (Fairbanks 1946, p. 34)
Later the organization and activitiesbecame considerably broader, as we willsee in the sections on the individualcenters. As they developed, each Centerreflected the experience and creativityof its particular staff. There were contin-uing attempts to unify the proceduresafter the February meeting at HoffGeneral Hospital. For example, in June1945, Major Martin, our medical chiefat Hoff, and I traveled to the CentralInstitute for the Deaf, the DeshonGeneral Hospital and the Borden GeneralHospital to observe their programs.
THE NATIONAL DEFENSE RESEARCHCOMMITTEE ROLE IN THE WW II MILITARYAURAL REHABILITATION PROGRAMS
An important influence on theevolution of similar procedures for theselection of hearing aids, and in facton the routine of auditory testing atthe three Army centers and the Navyprogram, was a research contract withthe National Defense ResearchCommittee of the Office of ScientificResearch and Development, in whichSection 17.3 was set up with theHarvard University Cruft and Psycho-Acoustic Laboratories and the CentralInstitute for the Deaf, in St. Louis, forthe “Study and Development ofInstruments to Aid Militarily IncurredDeafened.” (NDRC 1944)
The Harvard contract was for theperiod beginning 5/25/1942, with the“Official Investigator” being S. SmithStevens, while the CID contract was tobe in effect from 10/15/1943, with S.Richard Silverman as the OfficialInvestigator. Some of the representa-tives of the Harvard labs who madevisits to our Hoff unit or who wereotherwise helpful in correspondencewith us included C.V. Hudgins (alsowith the Clarke School for the Deaf atthat time), Douglas A. Ross andClifford T. Morgan. It was after Dr.Morgan’s visit that some of us receiveddirect officer’s commissions in theArmy, but while we did not knowwhether that was related to his visit ornot, we strongly suspected a directconnection.
Today’s audiologists will be surprised
3Origins of Audiology World War II Programs
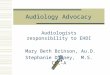
Early staff organization of the HearingProgram at Borden General Hospitallocated in Chickasha, Oklahoma.

✯✯✯✯✯
at how much of what the HarvardCruft and Psycho-AcousticLaboratories developed at that timeestablished the basis of research andclinical procedures in our field, e.g.speech audiometry, electro-acousticanalysis of hearing aids, and probe tubemeasurement.
The NDRC projects included thefollowing:
(The following descriptions arebased upon progress reports, in typedcorrespondence in 1944 and 1945,from the Cruft and PsychoacousticHarvard Laboratories to Major N.A.Martin, Chief of Aural ReconditioningUnit, Hoff General Hospital, SantaBarbara, California.)Diagnostic instruments
Central Institute for the Deaf.Measurement of the overall response of electroacoustic instruments to beused in the military hearing treatmentcenters.Evaluation of hearing aids
Harvard University, the CruftLaboratories. Then-current hearingaids were evaluated for their electro-acoustic characteristics, includingamplifier response and overload char-acteristics at various tone control set-tings, frequency response and imped-ance characteristics of hearing aidreceivers (which were physically sepa-rated by a cord at the time) and batterydrains. They developed molded eartipsto be used with small probe tubes thatcould be attached to a condensermicrophone for the measurement offrequency response characteristics.They reported that this approachexposed two differences from the meas-urements obtained with a rigid 2cccoupler, a greatly reduced low-frequen-cy response, and a broader resonancepeak, probably due to leakage aroundthe earmold in a ear, and possibly alsoto damping effects in the ear. (As with allhistory, it is sobering to realize that a rela-tively “new” technology, such as in situprobe tube measurements was conceivedso many years ago.)Speech audiometry
At the Harvard Psycho-AcousticLaboratory: “Standard deafnesses” weresimulated by selective attenuation andnoise masking. When it was demon-strated that articulation scores weresimilar to those of patients with similarhearing losses, researches were confi-dent that the articulation tests thatwere being developed in their lab forhearing aid selection procedures would
be appropriate for the purpose. Theycontinued subsequently to produce amodified word test, recorded through ahigh-pass filter for testing patients withhigh-tone losses. (Author’s note: It iscurious that now, over a half-centurylater, the possible clinical usefulness ofsuch a highpass filtered word test isapparently of little interest to audiologyclinicians.)
The NDRC project’s purposes werestated to be “to test the physical char-acteristics of various commercial hear-ing aids (Cruft Laboratory), to evaluatesuch aids using articulation procedureswith simulated deafness in normal sub-jects (Psycho-Acoustic Laboratory) andwith hard of hearing subjects (CentralInstitute for the Deaf); to develop newtests and instruments for the evaluationand fitting of hearing aids (HarvardPsycho-Acoustic and Central Institutefor the Deaf); and to validate and applythe results of such studies to individualswho have suffered hearing loss in mili-tary service (Deshon GeneralHospital). Raymond Carhart, who wasthen the Chief of the AcousticsDepartment at the Deshon Center wasapparently the main Deshon link inthe NDRC project. Measurement of the physical characteristics of hearing aids
This was carried out at the HarvardCruft Laboratory on commercial hear-ing aids of the time. In an early assess-ment of the use of rigid couplers forthe calibration of earphones, measure-ments obtained with them were com-pared with information from loudness-balancing. Development of word lists for hearingtests with and without hearing aids
Word lists were developed at theHarvard Psycho-Acoustic Laboratory fortesting the understanding of speech(“articulation testing”). The specialproperty of these lists was stated to bethat in normal ears their homogeneityresulted in “the rapid transition of theentire list from unintelligibility to intel-ligibility with a relatively small increasein loudness” (Ref. July 1, 1944, letterfrom NDRC, p. 3-49))
The lists, containing the bisyllabic“spondee” words, were designated as“Auditory Test No. 9”, in which groupsof six words were recorded at succes-sively decreasing intensity levels forarriving at a threshold for speech per-ception. The lists were also recorded atincreasing levels for the measurementof loudness tolerance (“Auditory Test
No. 10”), and through a 4000 Hz highpass filter (“Auditory Test No. 11”) as a measure of detecting high-tonehearing loss.
As reported by Egan (1948), thePB-50 word lists for tests of speech dis-crimination were also developed at theHarvard Psycho-Acoustic Laboratory atthat time. The word lists were re-recorded at the Central Institute for theDeaf and then evaluated on hearingimpaired and normal listeners for theirappropriateness as measures of speechperception and annoyance in the fittingof hearing aids. A cautionary note onthe use of these tests in the hearing aidfitting routine was published by the per-sonnel of the Harvard Laboratories,where the tests were developed. In theirarticle on the selection of hearing aids(Davis et al 1946) they concluded thathearing aid selection on the basis of testresults with such lists were inconclusiveand arbitrary. Despite such reservationson the tests they had inspired, thewartime hearing aid selection proce-dures persisted in audiological practicefor many decades.
Because of the unusual circumstanceof relatively large budgetary support andthe freedom to engage or assign a broadrange of trained personnel, the WW IIauditory and hearing programs set aremarkable example of services to adultswith hearing impairments: the first mul-tidisciplinary teams (medical, education,rehabilitation, engineering, psychology,social work, etc.); highly-structuredrehabilitation programs; the introduc-tion and development of specializedelectronic equipment for diagnosis andassessment, speech audiometry, hearingaid selection procedures; extensive andintensive counseling and training in theuse of hearing aids; and insights into“psychogenic” deafness.
It is also notable that the publica-tion of one of the first books on audiologyin the 20th century, Davis’s first editionof his Hearing and Deafness textbook (1947),was inspired by the WW II military pro-grams, with many of its illustrationstaken at the wartime hearing centers.
The trailblazing contributions ofthose centers were recognized byPresident Harry S. Truman in his WhiteHouse message on the occasion ofNational Hearing Week, Aug. 1947,when he stated that “Today, in peace-time, we are continuing the extensiveresearch in behalf of persons withimpaired hearing, initiated by the armedforces during the war” (Truman 1947).
Origins of Audiology World War II Programs4

✯✯✯✯✯✯The Hoff aural rehabilitation cen-
ter was activated on September 6,1943 at Santa Barbara, California,with the arrival of the first teacher oflip reading, Helen Scriver. (Scriver,1944). The hospital was built around anumber of Quonset barracks-like huts,which was apparently the army’s pres-sured response to the outbreak of thetwo-front war in Europe and the Pacific.
I arrived at the center early inNovember 1943 as the first soldierassigned to the Program, having beentransferred to it shortly after my basictraining and specialized instruction inradio electronics and communication.My assignment to the new Hoff pro-gram was related to my previous educa-tion and work experience with schoolspeech and hearing disorders, and wasarranged by Major Walton E. Barton, a psychiatrist who was the assistantdirector of the Reconditioning DivisionOffice of the Surgeon General of theArmy, and who was the first centraldirector of the army aural rehabilitationprograms. (Morrissett 1957, p. 449)
The Hoff program was then organi-zationally under a Col. Fuchs, who wasthe chief of the medical rehabilitationsection of the hospital. When I report-ed for duty to the Colonel he chargedme with organizing the rehabilitationprogram (I was later dubbedAdministrative Coordinator) but cau-tioned me that the soldiers would bereceiving the Zenith A-2 hearing aid,since his “father had one and it helpedhim”. Still one of the bulky “body”hearing aids, with a separate batterypack containing the heavy “A: and “B”batteries, the Zenith aid was being soldat the price-shattering cost of $40 ($50for the more advanced model), where-
as other aids were selling at the timefor about $125-150.
The medical direction of the pro-gram then proceeded from the medicalrehabilitation physician to an ophthal-mologist (Captain Herman Faier) andfinally to an otolaryngologist, MajorNorvil A. Martin, who had returnedfrom a harrowing trek as medical
officer of a U.S. army contingent thathad slogged its way over the Owen-Stanley mountains in New Guinea.Major (later Lt. Colonel) Martin
continued to head the program until it was dismantled following theHiroshima bombing.
More staff, both civilian and military were quickly added, and bythe time of the February 1944 meetingof the heads and selected staff of the three army centers at our Hoff Center we were essentially under full operation.
The delineation of responsibilityand duties in the Army required eachstaff member to have an official title,with positions in the military followingarmy protocols of rank.
For example, I arrived at Hoff as aprivate in November 1943, but inrecognition of my assigned organiza-tional tasks I was soon promoted to therank of corporal (technician 5th grade,which was about the lowest rank abovethat of private), so that I would be per-mitted to spend nights off the basewith my wife ( a privilege denied toprivates at that base). Later, however,
Origins of Audiology World War II Programs5
THE WW II HOFF GENERAL HOSPITAL HEARING PROGRAMSanta Barbara, California
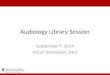
Miss Helen Scriver and a group of lip readers at Hoff Hospital
Advertisement for the $40 Zenith hearingaid of the time.
The following account is partly anecdotal, but augmented by center archives and personal army ordersthat are still in my possession. Details of the program are contained in the manual “AdministrativeRoutine and Standard Procedures for the Rehabilitation of the Deafened and Hard of Hearing”, (HoffGeneral Hospital 1945). My retained copy may be the only one that is still extant. In military organi-zational fashion, all procedures were prescribed in detail and specific forms for each procedure wererequired to be completed. Unfortunately, page numbers are irregularly entered, in my copy of the man-ual, apparently because of the inclusion of the many required forms to be completed, so the page refer-ences given in the following are only approximate.

Origins of Audiology World War II Programs
I was named AdministrativeCoordinator of the program, afterreceiving a direct commission as anofficer (along with other colleagues atthe three army centers) Next, I wasthe Acoustic Officer, responsible forthe development and supervision oftesting and hearing aid fittings untilthe arrival of 2nd Lt. Ira J. Hirsh, whowas assigned to that position. My nextofficial title was Project Director of theAural Rehabilitation Program.Entering the program later was thetransferred line officer, CaptainDonald R. Caziarc, who became theranking officer in charge of theHearing Program in October 1945.
PROCESSING OF PATIENTSThe patient’s stay at the hospital
was for eight weeks. FIRST WEEK: Upon admission
to the hospital he was quartered in theactive rehabilitation ward (as distin-guished from the general sicknesswards), and a ward medical officer
took a history and dida physical examina-tion, with particularattention to eye com-plaints In addition, avisual acuity test wasrequired, evidentlyrelated to our empha-sis on lip reading inthe rehabilitation pro-gram. (As an exampleof the distinction of patients by theirmilitary rank, the AdministrativeRouting and Standard Proceduresmanual stated that all officer patientswere to be interviewed and examinedonly by the Chief of the Section.)
The soldier was then given anaudiometric test, followed on the sameafternoon or the next morning by asecond audiometric test. An impres-sion of the ear for an ear mold wasthen taken, he was interviewed by theclinical psychologist, and examined by otologists in the ENT clinic, before being assigned to the rehabilita-tion program.
He met with the Administrator,who registered him for the programand prepared the work sheets. He wasthen interviewed in turn by the super-visors of lip reading, auditory trainingand speech. Vocational or educationalcounseling might be recommended bythe Administrator to the ReconditioningDivision for such counseling and forassignments in job therapy or appren-tice training.
Another interview was with theRed Cross counselor, who arrangedpersonal and family services as needed.
Also in the first week the patientattended discussion groups conducted
6
ENT and Aural Rehabilitation staff, Hoff General Hospital. Ira Hirshis looking over the head of Don Caziarc (in light-colored uniform) whois seated in the center of the front row, next to Lt. Col. Norvil Martin(with moustache), Chief of the clinic.
Lt. Col. Norvil A. Martin, Chief of Clinic, pinning new2nd Lt. bars on Joe R. Shinpaugh, Jr. as newly commis-sioned 2nd Lt. Moe Bergman looks on (Hoff Hospital)

by members of the aural rehabilitationstaff. These discussions were on suchtopics as: a) Orientation, led by theAural Rehabilitation Officer andfocusing on the purposes, etc. of theprogram; b) Medical Aspects, by amedical officer; c) Hearing Aids, athree-hour orientation to the tests tobe conducted in the sound-isolated(test) rooms, to the types of hearingaids, their care and use, and an oppor-tunity to see and informally try severaldifferent types of the then-availableaids, and d) Lip Reading, an orienta-tion stressing its importance, with aresume of the lip reading program. Asrequired, a group hearing aid was usedfor these discussions.
At a weekly clinical conference,attended by the otologists, the psycholo-gist, the Aural Rehabilitation Officer,the Acoustic Officer and the ProjectDirector, each new patient who had beenadmitted during the week was inter-viewed, and after that group interviewdecisions were made about the patient’srehabilitation program. (A “game” weenjoyed indulging in at those confer-ences was guessing from the patient’sspeech the region of the country he camefrom. I recall becoming quite pleasedwith the skill I acquired at the game).
SECOND WEEK: The patient con-tinued receiving individual lip readinginstruction, begun during the first week,and reported to the test rooms for com-plete hearing tests, followed later in theweek by the hearing aid fittings withthe various aids. (Note: In the earlydays of the program before we receivedequipment, the “fitting” was essentiallyentirely subjective, with the patient try-ing out each model in the hospital cor-ridor, wards and recreation areas).
During this week all patients had
instruction in “speech retention”, whilethose with diagnosed speech problemsreceived individual speech/voice correc-tion. Those who were considered to bein need of group or individual auditorytraining were assigned to those classes.
In addition to the instruction just
described, the soldiers participated inthe following activities: educationaland orientation programs, physicalreconditioning, G.I (army) movies andnews reels, and group discussions relat-ing to other rehabilitation, i.e. voca-tional guidance, occupational therapy
and job therapy, such asapprentice training on andoff the post. NEXT WEEKS: The sched-ule remained the same forthe third week, but in thefourth week group lip read-ing was begun. No furtherchange occurred in the sixthand seventh week, but in theeighth and final week the sol-dier’s evaluationpapers were com-pleted and submit-ted to the Chief ofENT, where a pre-liminary disposi-
tion was decided, with fur-ther decisions being made bya Disposition Board, thatcould recommend reassign-ment to duty or separationfrom the service.
THE HEARING TESTSFor the audiometric
examination there were twotypes of audiometers avail-able, the Maico D-5 andthe Western Electric 6Bp.
Western Electric had first produced forgeneral distribution a portable version(Model 2A) of their innovative rack-mounted model 1-A audiometer, thenfollowed it with the models 6A and6Bp (portable). It had to be frequencycalibrated by the examiner by adjust-
ing a small potentiometer to extin-guish a hum when the frequency dialwas set to 0. The Hearing Loss dial wasto be set to the engraved zero referencevalue for the frequency being tested.(There was no automatic internaladjustment for the normal thresholdcurve on that model.) To move fromthe air conduction test to bone con-duction the examiner was instructed to“place the index ring #126A over theHearing Loss potentiometer” and to“read the figures on this ring for loss-es.” (Once again, the zero HL refer-ence for each test frequency was at adifferent position on the index ring.)
Today’s audiologists will be inter-ested to know the approach to masking
Origins of Audiology World War II Programs7
Corporal Bergman fitting hearing aids at Hoff Hospital
Miss Ruth Bartlett with the first class for group instruction in lip reading at Hoff Hospital
The Western Electric 6BP audiometer. The knobs on the control panel, from leftto right, are tuning adjustment, frequency selector, and intensity control (attenu-ator). The accessories in the foreground behind the power cable include thereceiver (1) (with sponge-rubber face); two accessory ring-shaped scales (2) forthe attenuator (to give readings for bone conduction); and the bone-conductionreceiver (3) with its metal head-band. The small box (4) with the push-button isthe masking attachment.

at that time, over a half-century ago.The manual’s instructions are thereforereproduced verbatim:
Masking is necessary in many casesin air conduction tests, in addition tobone conduction tests. Routine prac-tice has shown that the safe procedurein audiometry is to test the better earfirst. If the threshold for the poorer earis found to be 40 decibels or morelower (i.e. poorer) on the audiometrictest than that for the better ear, thesubject may hear the test tones withthe better ear. If this occurs, maskingshould be used while testing the poorear. When masking, provide thepatient with a headband to hold theair conduction receiver used for mask-ing the opposite ear of the patient,thus leaving the hand free so that thepatient can signal whether or not hehears the test tone. The examiner mayset the masking tone just loud enoughto effectively mask out the better ear.(Hoff General Hospital, 1945, p. 20)
In somewhat greater detail for themasking procedure with the WE 6Baudiometer, the examiner was to usethe Pilling-Witting Masker (a separatedevice) as follows: (ibid p.20)4. Attach the power cord from masker
to power outlet. 5. Turn on masker but place “Normal
- Add 50” switch at “Normal”6. Place receiver on patient’s ear not
being tested.7. Use from 70 to 80 decibels of masking
noise, depending on the degree of the patient’s loss to bone conduction.
(Note: I do not recall whether the exter-nal masker was referenced to SPL or HL.)
An interesting entry was con-cerned with tinnitus. “When thepatient says he has a head noise it willbe up to the examiner to ask the sub-ject the apparent pitch, loudness, andquality of tinnitus, by going over theentire range of the audiometer untilthe patient signals that he has the toneequal to his head noise.”
LIP READINGOf the eight weeks of the program,
the soldier received 22 to 24 lessons inthe first four weeks with the sameinstructor. This was followed by 22 to24 groups lessons, with instructorsbeing rotated weekly. The studentswere grouped according to their lip
reading ability, but age and educationalbackground were also considered. Itwas recognized that there were morethan one “school” of lip reading at thetime and the instructor was free to fol-low any method that he or shefavored, but “in the interest of unifor-mity” there was a framework builtaround groups of phoneme movements,such as:
First week: Introduction of vowel sounds ah, o, oo, a, e with
1. f,v, (ph optional)2. m,b,p3. s,z, soft c4. sh, ch, j, soft c5. review
Later, group lessons included prac-tice material related to jobs “of interestto special students in the group” and“general topical practice material,preferably related to fitting the studentfor civilian life” (ibid p. 24).
AUDITORY TRAININGWhile the detailed instructions
refer to “auricular training”, this sec-tion of the 1945 manual is headed“Auditory Training” indicating thatthe name was in the process of change.(Hoff Report 1945, p. 28)
The first aim of auditory trainingwas stated simply as “the integration ofauditory, visual, and kinesthetic stimulifor quick and accurate interpretationof sound...with emphasis on the per-ception of auditory stimuli.” (ibid p.29) Auditory stimuli were listed asspeech, everyday sounds, gross sounds,music and “other complex externalauditory stimuli.” Visual stimuli werepresented as “speech reading” (a termalso in the process of change from “lipreading”) including gestures, expres-sions, etc. and printed texts and nota-tions for both music and speech. Auditoryintolerance problems received specialtraining attention and a variety ofhuman voices and articulation patternsformed the practice material, both inisolation and over backgrounds ofnoise and competing speech.
As soon as the hearing aid was pro-vided, the patient was given a diagnos-tic test of aided speech reception bythe auditory training staff. In additionto a list of carefully selected words, thetest included sentences, phrases andproverbs, in graded difficulty. A low
performance on these tests led toassignment for individual auditorytraining instruction. Auditory trainingwas also designed for those with a lowthreshold of acoustic tolerance or largediscrepancies in inter-ear thresholds.All patients were entered into the classprogram.
Stimuli were mostly recorded onreel-to-reel tapes, including everydaysounds (e.g. birds, traffic noises, etc.),spoken phrases, parodies of proverbsand word lists, instruments of theorchestra, song recordings for practicewith such variations as soprano, alto,tenor, baritone and bass voices, record-ed stories (e.g. anecdotes and jokes),prose, poetry and drama for prolongedand intensive listening, and, of greatemphasis, selective listening of speechover competing noises and talkers. It isinteresting to note also that two tele-phones of the hospital were equippedwith amplifiers for use by our patients.
SPEECH RETENTION AND CORRECTIONEvery patient was interviewed by
the Supervisor of the SpeechDepartment. This interview includedconversation, the reading of a shortparagraph and of sentences designed toreveal articulation errors. Patientswhose speech and voice were judged tobe good were then assigned to a “speechretention” class, the objective of whichwas “to emphasize the importance ofmaintaining these.” Speech sounds thatmight be vulnerable to change becauseof hearing loss received special atten-tion and minor articulatory errors werecorrected. Voice characteristics, such asvolume, placement, resonance, breathcontrol and pitch were considered, andthis training concluded with appliedpractice through group and individualreading aloud, short talks, radio skitsand short plays.
Significant speech and voice prob-lems were addressed in individual andsmall group therapy sessions. (Even atthat time “before” and “after” record-ings were made, with the introductionof the revolutionary “Mirrophone”,which replaced the disk-cutting tech-nology with a magnetic recording on areel of metal tape.)
HEARING AID FITTINGEar canal impressions were taken
shortly after the soldier was admitted tothe hospital, and the ear mold was fabri-cated in the hospital’s dental laboratory.
Origins of Audiology World War II Programs8

Following an audiometric workup,the patient was scheduled for the testsuite where a sound field unaidedaudiogram and spondee threshold weredetermined. The spondee thresholdwas measured using the recorded ver-sion of the spondee lists (“ArticulationTest No. 9”) provided by the HarvardPsycho-Acoustic Laboratories.
Since the bulky body-worn hearingaids were then always monaural, therule for determining which ear to aidwas based on the following guidelines:
When the fabricated ear mold wasready the patient returned for compara-tive hearing aid tests with 6 or 7 differ-ent instruments, using the same fabricat-ed mold for each. (It should be recalledthat all hearing aids of the period termi-nated in a separate mini-earphone towhich the ear mold was to be attached.)The Center stocked only those models
of hearing aids that had been approvedby the Council of Physical Therapy ofthe American Medical Association. Atthat time, all hearing aids utilized twobatteries, an “A” battery (1 1/2 volts)and a “B” battery usually of 45 volts.
The gain control of each aid wasadjusted by the patient as the examinerread sentences taken from the Fletcher-Steinberg lists (developed at the BellTelephone Laboratories), from a dis-tance of 10 feet; then the patient’s aidedsound field thresholds for pure tones and
spondee words were measured asbefore. The patient was thenasked to rate the aid under test as“clear” or “blurred”, “natural” or“mechanical”, and “quiet” or“noisy”. The results of the com-parative tests were then submittedto the Acoustic Officer for selec-tion of the hearing aid to be dis-pensed. The patient was author-ized to draw batteries from the
Property Officer, was individuallyadvised in the early use of the aid andgiven a printed set of instructions on thecare of the instrument. An additionalhandout contained clear instructions tomembers of the patient’s family, such as“Do not shout at him”, “Attract hisattention first before speaking to him”,“Do not talk to him in the dark”, “Do
not say the same words to himover and over again... think ofsome other way to express thesame thought.”, etc. The patientwas then instructed to report tothe hearing aid technician severaltimes thereafter for checks on thefabricated ear insert and the oper-ation of the hearing aid. Weeklymeetings were held for newpatients during which frank dis-cussion of the problems associatedwith hearing aid use was encour-aged. Continuous follow-up andguidance were provided in theauditory training classes. Upondischarge from the hospital thepatient was given a month’s sup-ply of batteries.
OTHER SERVICESPsychologist. During the first
week of the patient’s stay at theCenter he was interviewed by theclinical psychologist. If psychosiswas suspected, he was referred to
the psychiatrist; if war neurosis or otherpsychoneurosis was noted, he was sched-uled for psychotherapy; personal problems,such as family relationships, vocational,etc. were addressed and counseling given.A battery of tests was available for use asindicated, and included measures ofintelligence (Army Basic IntelligenceTest), personality (Minnesota MultiphasicTest), vocational counseling, etc.
NON-ORGANIC DEAFNESSComplaints of non-organic deafness
by military personnel during wartimehad been identified in various combatarmies in World War I and earlier ashysterical deafness. Reports were pub-lished about the experience in theAmerican army (Loeb, 1918), in theBritish army (Hurst and Peters, 1917),and in the Russian army (Zilboorg, 1944).Interestingly, Zilboorg reported that 50percent of the cases of deafness acquiredunder combat conditions were found tobe of psychological origin. Theseauthors also cited experiences in theFrench and German armies. This historyand the related diagnostic approachesare reported in detail by Bergman (1957).
An engaging view of this problemwas reported by Lederer, a Naval otolo-gist who headed the U.S. Navy auralrehabilitation program in WW II andWilliam Hardy, also of that program(Lederer and Hardy, 1946). They describedcases of what they termed “situationaldeafness”, in which there was a true ini-tial deafness related to exposure to blastand noise, with the symptoms lastingenough to send the victim to the medicalofficer. With the passage of time thehearing problem cleared up; but by then,fearing an accusation of malingering thepatient continued to complain, becomingmore involved in the deception. Ledererand Hardy reported that an understand-ing attitude by the medical officer couldclear up the problem promptly.
NARCOSYNTHESISUntil February of 1945 the suspi-
cion of possible psychogenic deafnessor outright malingering in some of thesoldiers evoked various diagnosticattempts, with uncertain results, at theHoff Center (many of such ad libapproaches are described in the reportof the Borden Center). The Hoff
9Origins of Audiology World War II Programs
IF……a. there is approximately a
uniform, moderate loss bilaterally
b. the poorer ear is better than 70 dB loss in the speech range
c. the poorer ear has greater than 70 dB loss in the speech range
THEN FITa. the ear not used
on the telephone.
b. the poorer ear.
c. the better ear.
An example of howWWII hearing aidswere worn. Note theearphone in thepatient”s right ear,the microphone andamplifier pack on thechest, and the largebattery pack at theside, all connected by wires.

Center program’s staff psychologistlearned of the successful resultachieved in the treatment of wartimeneuroses in the Eighth Air force inNorth Africa (Grinker and Spiegel,1944) and suggested the use of thatapproach for uncovering the deafnessversion.
Ninety-three patients of the HoffCenter aural rehabilitation programwere then studied under narcosynthesis,with marked “improvement” of theirhearing, while such “improvement”occurred spontaneously in 17 otherswho knew of the “treatment”. By theend of the program in 1945, it was esti-mated that 126 (9% of the total admis-sions of 1,375 patients in the program)had presented questionable complaintsof deafness.
The term “narcosynthesis” wascoined by Grinker and Spiegel becauseunder narcosis the patient “actuallysynthesizes the emotions and memo-ries connected with his experience,putting together what has lain frag-mented between consciousness andunconsciousness into a completewhole, which corresponds in almostevery detail with the original experi-ence”, and under the influence of the drug the ego, freed from therepressed emotions “can approach thetraumatic situation and, to someextent, deal with it” (Grinker andSpiegel, 1944).
Briefly, the narcosynthesis sessionproceeded as follows: In the 3-4 dayspreceding the narcosynthesis sessionthe patient was given strong suggestionthat he would hear normally after it. Ifit was thought that the hearing prob-lem was entirely non-organic thepatient was introduced, both individu-ally and in group sessions, to otherpatients who had “recovered” com-pletely after the “treatment.”
In the narcosynthesis session theanesthetist administered a light dosageof thiopental sodium (between 0.25and 0.8 gm. in a 2.5 to 5% solution),and as it was being delivered at therate of 0.1 gm per minute he wasinstructed to count aloud backwardfrom 100 to 1. Generally he becameincoherent by the time he counteddown to 50, and the anesthetist con-trolled the rate of injection so that thepatient was kept at the desired light
state. Meanwhile the patient was askedsimple questions and assured repeated-ly that he would recover his hearing,while simultaneously ethyl chloridewas sprayed at the external ear, pro-ducing local temperature changes andthe assurance of restoration of hearingwas repeated. Additional questionsconcerned the patient’s traumatic orother military experiences, his familyand other matters deemed of possibleconcern to him. The suggestive procedure was then repeated for thesecond ear.
As the patient became fully con-scious, he was repeatedly assured thathis hearing had returned to normal.Immediately he was tested by audiome-try and whisper and live voice andrecorded speech perception tests. Thetesting was repeated in the followingdays, and emotional or other symptomsthat had emerged during the pen-totherapy were addressed psychologi-cally. Occasionally a patient appearedto revert to his deafness when he real-ized that he was responding normally.Willful simulation was suspected insuch cases.
An interesting result was seen inthree patients, whose test results andhistory indicated a true long-term sen-sorineural hearing loss, and who hadasked to undergo the “treatment” inthe hopes of improvement. They wereaccepted, in order to note the effect of the suggestion. Following the nar-cotherapy all reported that they heard “much better” in such situationsas the movies, listening to radio andother difficult situations. Testingrevealed no change in their actualhearing.
During one period of data collec-tion, 42 of 76 patients who wererevealed to have functional hearingloss in these sessions had a history ofpre-induction hearing loss, over halffor more than 10 years. It may be thatin some of these a functional compo-nent was overlaid on an organic base.Only 12 patients of the 76 had actuallybeen in overseas combat.
Twenty soldiers who had beenadmitted to the program after blastconcussion and whose hearing hadreturned after narcosynthesis hadreported complete loss of hearing afterthe blast, followed a few days later by
partial recovery, then complete lossagain after a few more days. These mayhave included cases of Lederer andHardy’s “situational deafness.”
A final comment about psychologi-cal (or “psychogenic”) deafness whichcan easily be overlooked if the clini-cian is not alert to it. After the appli-cation of the narcosynthesis procedureat the Hoff Center, the staffs at theArmy Center at Deshon and the NavyCenter in Philadelphia, where fewcases of psychogenic deafness had pre-viously been noted, began to reportincreasing prevalences, until by theend of 1946 their numbers were“in close agreement” with those of Hoff (Canfield and Morrissett, 1947,p. 335).
ADDITIONAL SERVICESOther supportive and therapeutic
services were furnished by the RedCross worker, occupational therapists,psychiatrist, physiotherapist, and thephysical reconditioning program, andcounseling was available from anEducational Officer, a hospital-basedrepresentative of the VeteransAdministration and the Classificationand Separation Officer, who cooperat-ed with the psychologist in determin-ing whether to return the soldier toactive duty or to recommend separa-tion from the service.
FOLLOW-UPIn an attempt at self-evaluation of
the program’s effectiveness, the Chiefof the Aural Rehabilitation Program atHoff sent out a questionnaire to thesoldiers who had been discharged fromthe service after leaving our program,asking for such information as voca-tional adjustment, success in using thehearing aid, the usefulness of their lipreading skill, and their evaluation ofthe army rehabilitation program.
I could find no record of the repliesor their analysis, although Canfieldand Morrissett reported that “In boththe Army and the Navy units, ninety-four per cent of those who replied (to aquestionnaire) stated that they hadbeen benefited by the course and werestill wearing the hearing aids whichwere supplied.” (Canfield andMorrissett, 1947, p. 321)
Origins of Audiology World War II Programs10

APPENDIX 1: HOFF GENERALHOSPITAL HEARING PROGRAM STAFFThe personnel of the Hoff General HospitalHearing Center as of September 1945:
MEDICAL STAFF(NOTE: MC: Medical Corps; MAC:Medical Administrative Corps; S/Sgt: StaffSergeant)
Lt. Colonel Norvil A. Martin, MC, Chief, EENT Section and Aural Rehabilitation Program
Major S.N. Palevsky, MC, Assistant Chief, EENT Section
1st Lt. Arthur C. Jones, Jr., MC, Ward officer1st Lt. Legrande J. Audion, MC, Ward
officer1st Lt. Willard Parker, MC, Ward officer
AURAL REHABILITATION STAFFCapt. Donald R. Caziarc, MAC, Aural
Rehabilitation OfficerCapt. James H. Moore, Clinical Psychologist2d Lt. Moe Bergman, MAC, Project DirectorTec 4th grade Jacques P. Penn, AdministratorS/Sgt Franklin A. Buck, Jr., Assistant
Administrator
TECHNICAL STAFF(Responsible for audiometrics and hearingaid selection; ear molds, instrumentationand equipment maintenance.)2d Lt. Ira J. Hirsh, Acoustic OfficerTec 3d Grade Ransom I. Bovee,
Instrumentation and MaintenanceSgt. Russel Wilson, Ear molds, audiometricianCpl. Francis S. Dunning, Hearing aid
selection Tec 5th Grade Walter E. Riefler, Hearing
aid selectionTec 5th Grade Vesta T. Nelson, Audiometrician
EDUCATIONAL STAFFLip Reading Instructors (NOTE: It isapparent from the following that, as in theWW I program at Cape May, New Jersey,the most numerous staff in the WW II cen-ters was for lip reading.)Helen Scriver, Supervisor, Lip Reading
Department
Lip Reading Department, Civilians:Echo F. AllenMarian J. AndersonOrville ArmstrongRuth M. BartlettVirginia BaughmanCecilia Boslett
Franc(i,e ?)s E. DavidsonDale GayFrances H. DownesMargaret ManningMildred KinnierNatalie NelsonAlice StubbinsAlthea Woodruff
Lip Reading Department, Military2d Lt. Joe R. Shinpaugh, Jr.2d Lt. Emily E. LintnerTec. 4th Grade Helen A. DemaraisTec 4th Grade Gertrude Kibler
Other sectionsAgnes C. Riley - Supervisor, Speech
DepartmentMary H. Crumbling, Speech CorrectionistAlice Johnston, Speech CorrectionistOcea H. McMurry, Speech CorrectionistDorothy W. Scolton, Speech CorrectionistMartha Turner, Speech CorrectionistMary W. Whitehurst, Supervisor, Auditory
Training DepartmentDorothy Y. Lawrence, Auditory Training
Instructor1st Lt. Selma L. Larsson, Auditory Training
InstructorJacqueline Genthon, Assistant PsychologistWilma Kelly, Diversional ActivitiesJocelyn Siem, Red Cross Social Worker
11Origins of Audiology World War II Programs
REFERENCESBergman, M. (1957). Narcosynthesis in the
management of functional deafness. In:Surgery in World War II, Ophthalmologyand Otolaryngology. Office of the Surgeon General, Department of the Army, Wash., D.C.,pp. 473-487. [NOTE: This report was written in 1945-46, but was not published by the army until 1957.]
Canfield, N. and Morrissett, L.E. (1947). Military aural rehabilitation. In Davis, H., Hearing and Deafness. Rinehart Books, Inc. New York. Chapter 12.
Davis, H., Hudgins, C.V., Marquis, R,J., Nichols, R.H.Jr., Peterson, G.E., Ross, D.A., and Stevens, S.S. (1946) The selection of hearing aids. Part II. Laryngoscope 56:135-163.
Davis, H. (1947). Hearing and Deafness. Rinehart Books, Inc. New York
Egan, J. P. (1948). Articulation testing methods. Laryngoscope, 58, No. 9,
955-991Fairbanks, G. (ed) (1946) (July) History of
the Hearing Program at Borden GeneralHospital, Chickasha, Oklahoma.
Grinker, R. and Spiegel, J.R. (1944). Narcosynthesis; Psychotherapeuticmethod for acute war neuroses. Air
Surgeon’s Bulletin 1:1-5, February 1944.Hillman, C.C. (1944). The army rehabili-
tation program for the blind and the deafened. Journ. Amer. Med. Assoc. 125(5): June 1944, 321-323.
Hoff General Hospital.(1945) (Sept.). Administrative Routine and StandardProcedures for the Rehabilitation ofthe Deafened and Hard of Hearing.Hoff General Hospital, Santa Barbara,California.
Hurst, A.F.,and Peters, E.A. (1917). A reporton the pathology, diagnosis and treat-ment of absolute hysterical deafness in soldiers. Lancet 2:517-519.
Lederer, F. L. (1946). Hearing and speech rehabilitation. Hearing loss in the Navy and Marine Corps: incidence , etiology, and statistical analysis. U.S. Navy Medical Bulletin (supplement) March 1946, pp. 194-201.
Lederer, F. L. and Hardy, W.B. (1946). Treatment and training of the hard of hearing: A program of physical and psychosocial therapy. Archives of Otolaryngology 43: 429-461.
Loeb, H.W. (1918). Military Surgery of the Ear, Nose and Throat. Medical War Manual No. 8, Lea & Febiger. Philadelphia and New York.
Morrissett, L.E. (1957). The aural-rehabili-
tation program for the deafened and hard of hearing. In: Surgery in World War II, Ophthalmology and Otolaryngology. Office of the Surgeon General, Department of the Army, Wash., D.C., pp. 447-471. [NOTE thatmuch of this report was written in 1945-46, but was not published until 1957]
NDRC (1944) Report of Division 17, Section 17.3, July 1, 1944 This was included in a communication from Clifford T. Morgan, Technical Aide, NDRC 17.3 to Major N. A. Martin, Chief of the Aural Reconditioning Unit, Hoff General Hospital, Santa Barbara, California, dated August 31, 1944. Copy of this is in the possession of M. Bergman.
Scriver, H. (1944). Hoff hospital hearing aides. The Volta Review, April, 1944, p. 217.
Truman, President Harry S. (1947) (Letter to Dr. C. Stewart Nash, President,
American Hearing Society, Washington, D.C. Aug. 4, 1947, /s/ Harry S. Truman)
Zilboorg, G. 1944. Some aspects of psychiatry in the U.S.S.R. Am. Rev, Soviet Med. 1:562-575.

PERSONNELThe first of the aural rehabilitation
staff arrived in November 1943, andincluded 2d Lt. Raymond H. Hull andPrivate Edward L. Scouten of the military,and civilians John A. Morris and SaraLaurenzi. From that initial staff of four thenumber of personnel grew rapidly, untilit peaked at 81 members in September1945. The staff was augmented consider-ably by the transfer of some of the Hoffprogram’s staff after Hiroshima.
In the course of the program, fromthe end of 1943 through 1946, 118 per-sons were members of the staff, of whom93 had a Bachelor’s degree, 40 of themwith the additional M.A. degree and 6with a Ph.D. degrees. (The graduatetraining had not been in audiology,since there were no university-degreeprograms in audiology until after the war.)
PROCESSING OF THE PATIENTAfter admission to the hospital andthen to the Aural Rehabilitation pro-gram each soldier underwent a medicalwork-up by the ward officer and in the
ENT clinic. Recommendations weremade for the non-medical phases of theprogram. Concurrently the patient wasprocessed in the Aural RehabilitationSection, where the program wasexplained, questions answered andappointments made for examinations.The patient was given an orientationbooklet to the program.
ASSESSMENT OF HEARING ANDCOMMUNICATION PROBLEMS
The initial workup included, inaddition to the hearing tests describedbelow, tests of visual identification ofspeech to determine lip reading ability,speech sound inventory and voicecheck, psychological appraisal, and aninterview by a representative of theConvalescent Reconditioning Service.Tentative recommendations were thenmade about a hearing aid, lip reading,auditory training, speech instructionand counseling. (Fairbanks, 1946 pp11-12) If a hearing aid was recom-mended, the patient was referred tothe Dental Clinic for the fabrication ofan ear mold, and a temporary loanerhearing aid was provided.
AUDIOMETRY AND HEARING TESTSHearing tests consisted of pure
tone air and bone conduction thresh-olds and the required “tests of the dis-tances to which standardized spokenand whispered voice were recognized,the latter being expressed as fractionsof 20 feet and 15 feet, respectively.”(ibid p. 46). At first there were noacoustically designed rooms availablefor the audiometry tests, but later con-struction provided isolated chambers.
The tests of spoken and whisperedvoice recognition, however, “were car-ried on in one or other of two quietrooms 30 feet long and untreatedacoustically (since) it was felt that aslong as this comparatively primitivemethod of testing was used by regula-tion, elaboration of the facilities wouldnot improve the tests sufficiently towarrant the expenditure.” (ibid p. 47)Despite their reservations, however,efforts were made to standardize thewhisper-voice testing by having just onemale tester, speaking “short factualquestions, five or six words in length, ofsimple thought and unrelated one tothe other (e.g. Who was the first president? What color is an apple? How many eyes do you have?)” Theyfound the test-retest reliability with thesame tester voice to be “very high” (ibid p. 48).
The report stated that “the mosteasily standardized, most reliable andvalid tests of speech perception arethose secured under conditions of elec-trical stimulation with ‘canned’ speechor metered ‘live voice’ as a stimulusand with the results expressed in deci-bels above the normal threshold.” Butsuch measurements were made only forhearing aid selection (ibid p. 47).
Audiometer calibration appearedto be a problem. The report states thatthe audiometer of issue (the Maico D-5) seemed to be satisfactory for airconduction measurements but poor forbone conduction, where “the main dif-ficulties were unreliability and lack ofsufficient power.” A borrowedSonotone Model B audiometer wasjudged to have a satisfactory bone con-duction system, so measurements were
12Origins of Audiology World War II Programs
BORDEN GENERAL HOSPITAL AURAL REHABILITATION PROGRAMChickasha, Oklahoma
✯✯✯✯✯✯The following account is based on a final report prepared by Captain Grant Fairbanks and the staffof the Center (Fairbanks 1946). In addition, after the bombing of Hiroshima brought the war in the Pacific to an end, the Hoff Center program was closed, and I and others of its personnel were reassigned to the Borden Center. Some of the following, therefore, also includes personal recollections of that program. The Borden Hospital was designated as a Hearing Center in May,1943, and the Chief of the Ear, Nose and Throat Service, Major Leslie E. Morrissett, was laterappointed also the Director of Aural Rehabilitation.
Final staff organization of the HearingProgram, Borden General Hospital,Chickasha, Oklahoma.

done on the Maico for air thresholdsand on the Sonotone for bone conduc-tion. “These instruments were re-cali-brated on normal ears and correctionfactors applied to the manufacturer’scalibrations.” (ibid p. 47). By late1945, two more advanced Sonotone(Model 20) audiometers became avail-able and both air and bone conditionmeasurements were made on them.
It was recognized that the need formasking was “of considerable impor-tance”, but “no satisfactory commercialmasking devices were available orknown.” Toward the end of 1945,“thermal noise generators were devisedand constructed locally for this pur-pose” (ibid p.48). No guidelines formasking procedure are included in the reports.
The percentage of hearing loss wasdetermined through computing theaverage of the loss at “512, 1024, and2048 cycles (and) multiplying themean hearing loss for air conductionby 0.80 according to the prescribedmethod.” (ibid p.48) (Note: As Irecall, this was based on the fact thatthe maximum hearing level on theaudiometers was 120 dB, so a HearingLevel threshold of 120 dB would con-stitute a 100% loss.)
The problem of malingering andpsychogenic deafness, an area of con-cern at each of the military programs,was approached at Borden GeneralHospital by a method they labeled the“dark room treatment”, in which thetest room was darkened and “the spo-ken and whispered voices were deter-mined for the ear in question. Thetechnician, by shuffling his feet,attempted to mislead the patient tobelieve that he was approaching orreceding, but kept his voice at thesame level all of the time.” Anothermethod involved slipping a secondtechnician into the darkened room towalk audibly toward the patient as thestimuli were given from the originaldistance. Other techniques involvedattempting to obtain an audiometricshadow curve in claimed unilateral deaf-ness, and variations of the Stenger testusing two audiometers (no 2-channelaudiometers were available at the time).
The account of the Hoff Centerprogram contained reference to the useof narcosynthesis with the assistance of
the controlled injection of sodiumpentothal in cases of suspected malin-gering or “hysterical” deafness. Thisprocedure was later applied at Bordenby the program’s psychologist in thehospital’s Neuropsychiatric Section.
THE INDIVIDUAL AURALREHABILITATION PROGRAM
Each patient was assigned to one ofthe following programs: a. Standard full program, which con-
sisted of the dispensing of a hearingaid, 4 weeks of auditory training, 8 weeks of lip reading instruction, speech instruction and psychologicalcounseling, if indicated.
b. Abbreviated program, which included the same, except that the instruction was only for 4 weeks or longer, determined upon the durationof the hearing loss, previous experience with a hearing aid and “superior lip reading ability.”
SELECTION OF HEARING AIDSSince it was considered important to
equip the soldier patient with a meansof communication as quicklyas possible, hearing aid selec-tion was performed within thefirst two weeks following thepatient’s admission. In case ofdelay, a stock hearing aid(Zenith A3A) was loanedwith stock ear molds as soonas it was determined that hewas to receive an aid. In addi-tion to restoring communica-tion speedily, this was foundto raise morale and to preparefor the hearing aid fitting pro-cedure. Of the almost 2400hearing aids issued at Borden,200 (8%) of the aids werebone conduction heavy loss(mostly Sonotone).
As at the Hoff Center,early experience with com-mercial laboratories for fabri-cating ear mold inserts was unsatisfacto-ry, so arrangements were made with thehospital dental clinic to make them outof standard dental acrylic. This was avery successful alternative, with a mini-mum delay for delivery, and permittedrapid adjustments and re-fabricationwhen necessary.
From the outset, the hearing aid selec-
tion procedure was independent of com-mercial vendors, although some of thestaff had been commercial hearing aiddispensers and had useful knowledge to apply.
In late 1943, hearing aids wereevaluated in a conventional hospitaloffice, with informal tests using spo-ken voice at various distances. Testingequipment was later constructed at theCentral Institute for the Deaf follow-ing design cooperation between thetechnical staff of the Borden Centerand CID and with the assistance ofpersonnel of the Psycho-AcousticLaboratory of Harvard University. Thiswas made possible by the army’s con-tract with the National DefenseResearch Committee (NDRC). Thenew equipment was installed at theBorden Center in July 1944, “afterwhich time selection proceduresbecame more uniform and more objec-tive” (ibid p. 53). The equipment wasrack-mounted, and included an ampli-fier, volume indicator, oscillator andtalk-back amplifier. Pure tones weredelivered by a Maico D-5 audiometerand speech recognition was by micro-
phone (“live voice”) or recordings froma turntable. Additional microphones andloudspeakers were installed in bothcontrol and test rooms.
By October of 1945, new equip-ment added a static noise generator, athermal noise generator, and a two-channel amplifier, with associated pre-and power amplifiers, all topped with a
Origins of Audiology World War II Programs13
First Lt. Raymond H. “Woody” Hull calibrating the rack-mounted equipment used for two-room audiometry duringthe early days of the Borden program.

control console that permitted mixingof signals as desired.
Various types of speech materialswere used, but the staff favored testtranscriptions provided by the Psycho-Acoustic Laboratory of HarvardUniversity. The Borden report statesthat the use of those transcriptions “willnot be described in this report, becauseof their complexity and the variation intheir use” (ibid p.53). (For details onthese PAL tests, e.g. Auditory Test No.9, see the previous section on the HoffCenter.)
The updated equipment and two-room test suite permitted hearing aidcomparisons as follows: After an unaid-ed binaural sound field pure tone audio-gram was taken (“with careful standard-ization of the patient’s head position”),the following tests were run usingspeech materials expressed as dB “abovethe normal detection threshold”:a. Speech detection level;b. Identification level: level in dB at
which the test words could be repeated;c. Preference level: level in dB which
the patient’s preferred level for listening to the words; and
d. Tolerance level: the tolerable max-imum level in dB for speech before discomfort.Then the first trial hearing aid was
fitted on the patient and the gain con-trol adjusted as the patient signaled hispreferred level for listening to speech ata distance of six feet. The four speechtests described above were then admin-istered, plus one test for identificationin noise in which the speech signal wasaccompanied by a mixture of thermaland static noise, “approximately 40decibels above the normal threshold.”For those hearing aids that provided theexpected gain, additional tests includedthe aided sound field pure tone thresh-old audiogram, with the gain control atthe established setting, and the identifi-cation threshold, with the gain controlat maximum.
Subsequent trial hearing aids weresubjected to the same routine, withtheir gain controls set as follows: Testwords were introduced through theloudspeaker at the detection level ofthe first aid, and the control of each ofthe following aids was set to equate tothe same detection threshold.
If a review of the test results failed to
differentiate the trial hearing aids, thepatient’s opinion was solicited withregard to each aid’s clarity, freedom fromnoise, naturalness of sound, etc. Since allhearing aids at that time were body-wornand could be easily identified by looks,they were kept out of the sight of thepatient as far as was possible, “to preventbias because of such factors as size, beau-ty, reputation, etc.” (ibid p. 56)
After the early months of the pro-gram, the Army Medical PurchasingOffice arranged the acquisition of aquantity of hearing aids under contractwith five different hearing aid manufac-turers, so the hearing aid issued to thesoldier after the hearing aid selectionprocedure was the one that had beenused in the tests. In addition, the staffhad found several additional usefulmodels, e.g. for bone conduction andcertain high gain and power instru-ments, a small supply of those aids wasstocked in the center.
AUDITORY TRAINING ANDHEARING AID FOLLOW-UP
As the hearing services programevolved, some members of the auditorytraining staff were assigned to hearingaid supervision and worked closely withthe hearing aid selection staff and withthe psychologist. They provided basicinstruction and counseling in the use ofthe aid and distributed general and spe-cific product literature for guidance. Aweek after the aid was issued the patientwas recalled for follow-up and additionalinterviews were arranged as necessary.
Upon discharge from the hospital
the soldier was seen again, given a sup-ply of batteries and replacement receivercords and instructed about the VeteransAdministration services or, if returnedto duty, given a letter of instruction tohis new service station.
Both group and individual auditorytraining were given to improve listen-ing ability with the hearing aid.Stimuli included recordings of every-day sounds, such as those of automo-biles, restaurants, crowds, etc., many ofwhich were obtained from a companyspecializing in recordings for radiobroadcast. Much of the recordedmaterial was acquired also directlyfrom advertising agencies and broad-cast stations. These provided a varietyof voices and sound effects. Telephoneuse was a featured part of the auditorytraining program, and special practicerooms were set up, including a meansfor two-way telephone conversationsto be listened to by the entire class foranalysis.
Although only monaural hearingaids were then in use, practice in audi-tory localization was attempted, with
Origins of Audiology World War II Programs14
Master Sgt. Louis M. DiCarlo conducting anindividual auditory training session at BordenGeneral Hospital using a desk model hearing aid.
Group auditory training with a group hearing aid at Borden Hospital. The instructor at thefar left is John K. Duffy.

selectable loudspeakers placed at thefour 90 degree positions.
Listening Laboratory. In addition tothe group sessions the patients had theopportunity of spending hours in thelistening laboratory, in a comfortableand pleasant environment, and inwhich recorded materials, graded indifficulty, were available for listeningpractice.
The Fairbanks report contains avery detailed summary of the auditorytraining procedures and materials,emphatically endorsing the positivecontributions of the auditory trainingprogram to the continued successfuluse of the hearing aid.
LIP READING INSTRUCTIONAs in the hearing rehabilitation
program in WW I, the major staffcommitment in the WW II programswas to lip reading instruction. Thiswas clearly a carry-over of the patternin the civilian leagues for the hard-of-hearing at the time.
The teachers’ instruction plans atBorden changed over the years from1943 to 1946 from exclusively individ-ual lessons to group instruction in whichthe use of voice was permitted for theinstructors, and finally to “Sight-Hearing,”in which the patients used their hearingaids, while motion pictures were employed,and recorded background noises wereintroduced as background competition. While the lessons were organized aroundindividual phonemes the practice materi-al involved continuous speech, such assentences, games, stories, etc.
During the first weeks the instruc-tion was given under favorable condi-tions of light and distance, but theadvanced instruction was designed toincrease the complexity and difficultyof the spoken material and includedvariations in the environmental condi-tions. In a typical lesson the instructorgave a short talk or read a story, fol-lowing which the class members wereencouraged to enter the discussion,with emphasis on quick shifts of atten-tion from one face to another. Thisprovided added opportunity of readingspeech from different angles. Furtherdifficulties were introduced by chang-ing the available light and with theinstructor obstructing part of the face.
SPEECH CORRECTION AND CONSERVATIONAll new patients were checked for
voice and speech defects and thosewith problems were assigned to indi-vidual training or, for mild defects togroup instruction. Many patients wereassigned to both. A feature of thespeech correction program was the useof “a phonograph recorder” and thenewly-introduced magnetic taperecorder. These provided a record ofbefore and after progress.
As at the Hoff Center, speech con-servation (originally called speech“insurance”) instruction was given “toprevent speech defects before theyexist.” (ibid p.72) The purpose was todevelop awareness of speech, particu-larly anticipating the possible effects ofhearing loss on speech production, anddrew heavily on the use of publicaddress systems, recordings, musicalinstruments, etc. Details of the speech conservation instruction,although from the viewpoint of anothercenter (Deshon), were provided byCarhart (1947).
The Borden center received a lim-ited number of patients who did nothave hearing problems but who werein need of help for speech and voiceproblems, such as stuttering, laryngec-tomy, aphonia and dysphonia due toparalysis, articulatory defects related tomaxillo-facial wounds, etc.
PSYCHOLOGICAL AND VOCATIONAL COUNSELINGIt was evident that the entire Aural
Rehabilitation Program, centered as itwas on the quick restoration of effectivecommunication, provided the mostimmediate psychological support for ourpatients. An initial psychologicalassessment of each patient was made asa guide in his rehabilitation. This ledto the development of a HearingAttitude Scale (ibid p 76), which wasintended to uncover such problems asinaccurate self-appraisal, depression,over-optimism, emotional tension, jobworry, sensitivity, tendency to cover-up,and social withdrawal. The scale wasscored for each patient and changes dia-grammed over the period of the pro-gram. The results were used to decidewhether the patient required individualhelp beyond the group counseling ofthe program, or special educational or
vocational counseling, or had such sig-nificant emotional problems that refer-ral to the Neuropsychiatric Section ofthe hospital was indicated.[Unfortunately, although the Bordenreport (p 75) refers the reader to itsAppendix I, apparently for a copy ofthe Scale, my copy did not include it.]This scale, devised by the psychologicalteam of the Borden program, may havebeen one of the first, if not the first, ofthe hearing handicap scales that weresubsequently developed in our field. Atthe end of the program the HearingAttitude Scale was re-administered toall patients.
Other standard psychological measures were employed, if indicated,and an original word association testand a sentence completion test weredeveloped as supplementary assessmentinstruments.
Group psychological counselingincluded “situational practice”, inwhich, for example, a patient appearedat a party of his “friends” for the firsttime wearing a hearing aid, or wasapplying for a job. The emphasis, insuch sessions, was on facing the problems of withdrawal from socialactivities, sensitivity about using thehearing aid, etc.
PROGRAM FOR PATIENTS WITH MILD LOSSESA feature of the wartime programs
was the attention to those in whommild hearing losses and unilateral lossesreceived aural rehabilitation serviceseven though hearing aids were not indi-cated. At the Borden Center a specialtwo-week program was devised, withinstruction given three hours each day,five days a week, and additional individ-ual instruction or counseling as required.This program included lip reading, audi-tory training, and sight-hearing lessons,with emphasis on listening underadverse environmental conditions,localization problems, etc.
RESEARCHA staff member was designated to
head this activity, which consisted ofboth tabulative and experimental proj-ects, and focused on such activities asaudiometric testing, hearing aid fit-tings, testing lip reading ability, patientflow data, etc.
15Origins of Audiology World War II Programs

✯✯✯✯✯
The testing of voice and whisperrecognition as a function of distance,required by army regulations, continuedto be evaluated for validity and reliabil-ity. There was almost constant studyand evaluation of the procedures forthe selection of hearing aids as thesemethods were repeatedly altered andimproved.
I am grateful to Grant Fairbanks forthis very detailed report on the BordenHospital program. The night before hisuntimely death in an airplane heading
to a meeting, some years after the war,my wife and I enjoyed dinner with himat a restaurant in White Plains, NewYork, reminiscing about the war-timeexperiences we shared. Grant had beena recognized child prodigy, who appliedhis brilliance and creativity to the fieldof communication and its disorders. Hiscontributions at Borden General Hospitalduring the war and to our field, particu-larly during his many years of research atIowa University, made it a privilege tohave been associated with him.
REFERENCESCarhart, R. 1947. Conservation of
speech. In Davis, H., Hearing and Deafness. Rinehart Books, Inc. New York. Chap. 11.
Fairbanks, G. (ed) (1946) (July) History of the Hearing Program at Borden General Hospital, Chickasha, Oklahoma.
16Origins of Audiology World War II Programs
APPENDIX 2: BORDEN GENERALHOSPITAL HEARING PROGRAM STAFFBorden General Hospital aural rehabilitationstaff from activation through deactivation (inthe order in which they joined the program)MILITARY1. 1st Lt Raymond H. Hull2. T/3 Edward L Scouten3. 1st Lt Robert T. Baughman4. 2nd Lt Elizabeth Benson5. M/Sgt Louis M. DiCarlo6. T/4 John Kester7. T/3 Glenn Beaty8. T/3 Ben Straus9. Capt Grant Fairbanks10. 2nd Lt Kenneth W. Braly11. 2nd Lt Urie Bronfenbrenner12. Sgt Eugene Morrill13. Maj Luther G. Ramer14. T/4 Freeman McConnell15. T/5 Mary Mills16. 2nd Lt Robert D. Boyd17. Sgt Cyril Radcliffe18. Pvt Richard Weaver19. T/4 Grover McMillan20. 1st Lt Roger Bardsley21. 1st Lt William E. Miller22. Pvt Howard Burns23. T/4 Robert F. Suczek24. 1st Lt Windell Fewell25. 2nd Lt Kenneth Beighley26. Capt Donald R. Caziarc27. T/4 Gertrude Kibler28. 2nd Lt Joe R. Shinpaugh29. 2nd Lt Moe Bergman30. Capt James H. Moore31. 2nd Lt Mary Emily Lintner32. Pfc Victor A. Johnson33. T/3 Helen DaMarais34. Cpl Francis Dunning35. T/3 R.I.Bovee
CIVILIANS1. John A. Morris2. Sara Laurenzi3. Lois Jean Weida4. Mary L. VanBebber5. Anne Purdy6. Isabelle Demarest7. M. Evaline Rae8. Virginia K. Fletcher9. Morton Offett10. Mary Elizabeth Steen11. Dorothy K. Topping12. Doris Thiesen13. Mary Jane Ambrose14. Fern E. Haggen15. John K. Duffy16. Margaret V. Eckhart17. Marjorie M. Nerenberg18. Josephine Walker19. Armin D. Turechek20. Robert Harrington21. Gwendolyn Cline22. Lois Silver23. Helen Harris24. Jacqueline Keaster25. Douglas Wheeler26. Mary Jane Bope27. Faye Ola Bush28. Bettie J. McClelland29. Marguerite Schmelter30. Dorothy Ayers31. Barbara Smith32. Sue Scott33. Elaine Szymoniak34. Katherine Kelley35. Chester M. Shaffer36. Lois Laverne Carson37. Harry Wise38. Dorothy Nielsen39. Dorothy Downey40. Mildred Jones41. Nestor A. Wickman42. Mamie Dickerson
43. Mary Jane Sloan44. Glenn J. Taylor45. Yvonne Gowan46. Agnes Cota47. Edward Shulman48. Kay Shepherd49. Lola McMullen50. Mary Leonard51. Juliane Peterson52. Susanna Baltzer53. Waring J. Fitch54. Clayton T. Knowles55. Nora Jeanson56. Jessie Lillard57. Delwin B. Dusenbery58. Dorothy Dennis59. Georgia Barger60. Lucille Ford61. Avah Compton62. Louise Winter63. Jeanne Baker64. Betty Shepherd65. Jean Kelley66. Janet F. Watson67. Jacqueline Giles68. Ruth Doering69. Mary Hindman70. Sylvia Dossey71. Betty Black72. Nancy Ann Morse73. Patricianne Baldridge74. Anne Gormley75. Ruth Zucker76. Billie Holderman77. Bobby L. Nabors78. John H. Wiley79. Frank M. Lassman80. Everett T. Curry81. Maurice Whitlock82. Colleen Christian83. Betty B. Wallace

17Origins of Audiology World War II Programs
In the staff organization of the non-medical services, the Director over-saw a Supervisor of Speech and
Hearing Re-education, who in turnwas responsible for the auditory train-ing and speech reading instructors andthe speech correctionists. The ChiefAcoustic Technician had a staff con-sisting of other acoustic techniciansand an Electronic Technician, and theClinical Psychologists had responsibil-ity for psychometrists and articulatedwith the Red Cross worker, while theliaison with outside organizations forpost-service follow-up, such as theVeterans Administration, was theresponsibility of the Educational andVocational Counselors.
The structure of the program wasbased upon the premise that “the reha-bilitation of the person with a hearingdisability is primarily a non-medicaloperation” (ibid, p.431).
Referral to the Navy program wasbased upon the audiometer thresholdof 30 dB HL or more in the better ear“within the conversational range”(ibid p. 431), although there were notmany pure tone audiometers availablein the field at the time, and the “con-versational” voice and the whisperedvoice tests of hearing were still beingwidely used in pre-induction examina-tions, as discussed below. It is not sur-prising, therefore, that about 40% ofthe patients referred to this treatmentcenter had hearing losses before theyentered the service, a reality that wasrecognized in each of the militaryaural rehabilitation units.
INTAKE PROCESSINGOn entry the patient received a
general physical examination, followedby an otological examination and histo-ry-taking. If otosclerosis was diagnosed
the patient would be sent to the U.S.Naval Hospital in Bethesda, Maryland,which was the designated center for theaccepted surgery for that pathology,Lempert’s “fenestration nov-ovalis.”
Following the medical work-up abattery of hearing tests was adminis-tered, including the conversational andwhispered voice tests, the tuning forkWeber and Rinne tests (“to clarify theproblems of accurate diagnosis”) (ibid p.434), and audiometric and speechreception tests. The authors state flatlythat “the conversational voice test is sovariable as to be essentially meaning-less”, but they offer a defense of thewhispered voice test, conducted “withthe use of residualair” as being seeming-ly valid for measuringhigh frequency loss.(ibid p. 434) In casesof suspected simulat-ed hearing loss theLombard and Stenger tests were employed.
The Navy centerintroduced the con-cept of “situationaldeafness”, by whichwas meant thesequence of eventsfollowing thepatient’s complaintof loss of hearingwhile exposed togunfire or otherexplosions. Although his complaintwas verified by examination and hear-ing tests in the field and at the variousprocessing facilities before he reachedthe aural rehabilitation unit, the hear-ing loss may have lasted only a shorttime, during which he became increas-ingly committed to it as the examina-tions accumulated. By then, fear ofcensure or suspicion of malingering
entered as an enmeshing factor. Whilethe Lederer/Hardy report insists thatthis occurred only seldom, it does pro-vide one possible interpretation offunctional (“non-organic”) deafness.
In addition to pure tone audiome-try, speech reception was measured in afree field with a “hearing evaluator”, atwo-channel instrument developedthrough the assistance of the NationalDefense Research Committee, whoserole in the military aural rehabilitationunits is described elsewhere in thisreport of the WW II programs.
In addition to the medical andaudiologic examinations the patientmet with the Red cross worker and the
specialist in educational services andprevocational training, and then witha departmental psychologist.
An impression for an ear mold wastaken if the use of a hearing aid wasindicated. As a start in the commu-nicative re-training the sailor wasinterviewed by a speech readinginstructor, who graded his natural abil-ity in that skill. Finally, the newly-
✯✯✯✯✯US NAVY HEARING SERVICES PROGRAM
US Naval Hospital, Philadelphia, Pennsylvania
The World War II aural rehabilitation program at the U.S. Naval Hospital in Philadelphia servedmembers of the Navy, the Marine Corps and the Coast Guard. It was organized by Captain FrancisL. Lederer (MC), an otolaryngologist, and supervised by Lt. Commander Herbert Koepp-Baker, Ph.D.,as director of non-medical services. (Lederer and Hardy, 1946)
Hearing aid ear inserts were fabricated in the dental labs of thehospitals in which the aural rehabilitation clinics were located.

18Origins of Audiology World War II Programs
admitted patients met as a group for alecture by the Director of non-medicalservices on the psychology of deafnessand problems of mental hygiene.
THE AURAL REHABILITATION PROGRAMPatients remained in the program
for 5-6 weeks, during which theyreceived instruction in speech reading,auditory training and speech production.They spent five hours each week inthese activities, in sessionsdesigned separately for those with“marginal”, “moderately severe” or“profound” hearing losses. Theteaching sessions were conductedin classrooms, each of which wasequipped with a group hearing aidand a built-in glass booth for speechreading instruction with full voice.
THE SPEECH READING PROGRAMThe “speech reading”, or “lip
reading” methodology employed inthe Navy program was differentfrom that employed in the Armyprograms. This difference reflectedthe variations of methodologiesthat were current at the time.
During the early and middleperiods of the 20th century therewere passionate debates over the“true method” for teaching thisskill. The more widely practicedmethods were variants of theHamburg, Germany Muller-Walle“analytic” approach, based mainlyon syllable drill and introduced tothe U.S. at the turn of the century byMartha Bruhn. The later, “synthetic”technique, was introduced by EdwardBartlett Nitchie, the independent-thinking pupil of the Bruhn method’spopularizer, Lillie Eginton Warren, andthe father of the leagues for the hard-of-hearing. These methods were the basisof the lip reading instruction practicedby the teachers in the WW I programand continued in the three Army cen-ters in WW II.
A newer method was introduced atthe Michigan State Normal College atYpsilanti, Michigan, which departedfrom the purely visual approach to lipreading. Having originated in the cityof Jena, Germany it became known asthe Jena Method. It argued that themost effective approach to becomingskilful in the process of understanding
speech, by hearing impaired persons,was to involve the kinesthetic sense,that is, to “feel” the movements of thetalker one is watching.
This Jena method of speech reading(a term used as early as 1906 byAlexander G. Bell) was the favoredapproach in the Navy program (ibid p.437), apparently by the supervisor ofreeducation, Lt.(jg) Miriam D. Pauls.
AUDITORY TRAININGThis activity was
headed by Lt.(jg) HarrietL. Haskins. An inter-esting view expressedin the Lederer/Hardyreport as an explana-tion of the need forauditory training wasthat “We are con-vinced ...that a personcould not achieve theoptimum use of a hear-ing aid without some-thing more than a fewkindly words of advice” (ibid p. 440).This view is still advocated today, if notwidely honored in practice.
Because the dispensing of binauralhearing aids was not considered feasible
at the time, owing at least partly to thebulkiness of the available models, theauditory training instruction utilized asingle earphone, “in a fashion consonantwith the effect they will get from theirown individual aids.” (ibid p. 441) The Lederer/Hardy report provides avery detailed description of the audito-ry training course, with the focus being“a complete reeducation of the person’shearing habits.” (p. 443)
SPEECH TRAINING AND CORRECTIONAs in the army centers, the Navy
program included a belief in the desir-ability of instruction in speech produc-tion for hearing-impaired persons,
A lip reading skit being performed by staff at the Naval Hospital in Philadelphia. The animat-ed actor in the center is Lt.(jg) Miriam Pauls, Supervisor of Re-education of the program.
Practice in using the telephone with hearing aids worn onthe chest. The telephone is inverted so that the receiver facesthe hearing aid’s microphone. (Naval Hospital, Philadelphia)

19Origins of Audiology World War II Programs
✯✯✯✯✯✯✯✯✯✯✯✯
even for those without evidence ofrelated speech or voice changes, tomaintain their normal speech patterns.This “speech insurance” trainingstressed the relationship betweenspeech and hearing and included drillsin producing good, intelligible speechas a means of avoiding the undesirablechanges in speech and voice that
might be expected to accompany hear-ing loss.
Speech correction was available forthose with noted speech and or voicedeviations, often associated with pre-induction hearing losses. In apparentcoordination with the instructors ofspeech reading, the speech correction-ists emphasized the kinesthetics ofspeech, which would be cues to speechreading as well.
AUDIOMETRY AND HEARING AID FITTINGSThese activities were headed by Lt.
(jg) Eva A. Thompson, who was knownto old-timers in this field as the knowl-edgeable associate, on hearing problems,of the famous Dr. Walter Hughson.
In addition to pure-tone air and
bone conduction audiometry the hear-ing tests included measurement of thethreshold of hearing for speech in atwo-room arrangement for loudspeakerpresentation via live voice. The limitbefore overload of the equipment thatwas custom-assembled for the purposewas 80 dB, although the reference wasnot stated (p. 445)
The Navy program received thetechnical data on the performance ofthe current hearing aids that was pro-vided to the military clinics by theNational Defense ResearchCommittee, which was also involvedin the assembling of test equipment forthe speech reception testing.
The fitting of hearing aids consist-ed of several steps. First, the patienttried 3-4 different hearing aids underusual listening conditions, duringwhich he might reject those judged tobe annoying or to have poor quality.NOTE: My own recollection of patientreactions to specific hearing aids, atthat time, and continuing for someyears after the war, was that the physi-cal appearances of the available models
were sufficiently disparate, particularlyin size, that this factor could signifi-cantly influence the patient’s compara-tive judgment.
The final choice of a specific hear-ing aid was based upon the speechreception tests in the sound-treateddouble room.
As in the army centers, ear moldswere fabricated in thecenter’s own hospitalfacilities, with theadvantages of speed ofavailability and “fine-tuning” fit and comfort.
Comment: To appre-ciate the remarkableevolution of the hearingaid in the second half ofthe 20th century oneneed only read the con-stricted proposals, inthe Lederer/Hardy 1946report, for more“advanced” hearing aidsthan the bulky, two-pack models of that day.(pp.454-5) The thrustof their proposals canbe gleaned from theirrecommendation thatsuch a hearing aid“would include a com-bination battery pack,sufficiently adjustable sothat it might be pack-
aged with the transmitter[i.e. the microphone-
amplifier unit] or worn as a separateunit”. (p. 455) Will we be more pre-scient in foretelling the future evolu-tion in acoustic management of hear-ing problems in the next half century?
REFERENCESLederer, F. L. 1946. Hearing and speech
rehabilitation. Hearing loss in the Navy and Marine Corps: incidence, etiology, and statistical analysis. U.S. Navy Medical Bulletin (sup-
plement) March 1946, pp. 194-201.
Lederer, F. L. and Hardy, W.B. 1946. Treatment and training of the hard of hearing: A program of physical and psychosocial therapy. Archives of Otolaryngology 43:429-461.
A speech correction session at the U.S. Naval Hospital. Each patient’s speech was recorded for playbackon the revolutionary recording device that used a metal magnetic tape on a reel.

20Origins of Audiology World War II Programs
BEGINNINGSThe Deshon Hearing Services Programactually began at the Walter ReedGeneral Hospital in Washington, D.C.with one lip reading teacher, VirginiaHarbour. (The Service Club, 1944)Harbour was joined at the beginning ofAugust 1943 by lip reading teachersShirley Stein, Lorraine Amos, FrancesDownes and Elizabeth Helm Nitchie.Sgt. Francis Sonday, the one enlistedsoldier on the staff, constituted theAcoustic Section, responsible for hear-ing tests, hearing aid selection, etc.(Personal correspondence with ShirleyStein by telephone 16 July 2000.) Sondaylater represented the non-medical sec-tions of the Deshon Center program atthe planning meeting of the heads ofthe three army aural rehabilitation cen-ters at the Hoff center in February, 1944.
The Walter Reed Hospital was evi-dently too busy to handle the auralrehabilitation program, and it was relo-cated in November of 1943 to theDeshon General Hospital in Butler,Pennsylvania. Along with Sonday thepersonnel that moved included Steinand Nitchie, who became the head ofthe lip reading section. Sonday wassoon followed by Private First ClassHugo Schunhoff as a lip readingteacher, then Pfc Lee Doerfler and PfcAlbert Douglas as Technicians in theAcoustic Department. (Personal corre-spondence with Lee Doerfler by tele-phone 15 August 1998)
Initially the Deshon Center Programwas headed by Lt. Col. Marion R.Mobley, who was followed as Chief ofService by Edward Truex, Jr.
Raymond Carhart joined theDeshon program in mid-April 1944 asthe Chief of the Acoustic Department,first on a civil service appointment,beginning on April 14, 1944. FromNovember 27, 1944 he continued as acommissioned officer (Captain) untilApril 20, 1946. (Personal correspon-dence from Kevin B. Leonard, UniversityArchives, Northwestern UniversityLibrary, Evanston, Ill. Sept. 3, 1999)
The staff of the Deshon unit onJanuary 1, 1944 consisted of seven lipreading teachers, 2 acoustic techniciansand one medical officer. The title“acoustic technician” indicated thosewho tested hearing and were responsi-ble for authorizing the issuance of hear-ing aids to patients. By December ofthat year the staff had grown to include3 medical officers, 1 acoustic physicist(Carhart), 5 acoustic “experts”, 4acoustic “clinicians”, 1 auricular thera-pist, 3 auricular therapy instructors, 23lip reading teachers, 2 speech correc-tionists, 1 psychologist, 2 psychome-trists and a clerical staff.
As noted at the other military units,despite an anticipated inflow of patientssuffering from war-incurred trauma, alarge percentage of the patients hadbrought their hearing deficits with theminto service. Thus, the 1944 Deshonreport indicates that 53% of theirpatients had histories of pre-inductionhearing loss that had been recorded by theinduction examiners as normal hearing.
The 1944 report emphasizes therapid advances in the activities of theAcoustic Section, evidently related tothe addition of Carhart as chief of thesection in mid-April. This period saw
the installation of sound-isolated hear-ing test chambers, sound treated roomsand specialized electronic equipment,all after June 1, 1944.
Before that date hearing aid “fit-tings” were made by representatives ofhearing aid companies and the selectionof the one hearing aid issued was basedupon the patient’s report of which wasfound “most pleasing” after he usedeach trial aid around the hospital.
By July, however, the clinic staff didthe “fittings”, drawing on a library ofmakes and models as loaners, and a “lis-tening hour” in which the patient lis-tened with each aid to a variety of envi-ronmental sounds. Final selection wasmade from the 3-4 “best” aids, on thebasis of sensitivity (including speechreception) tests, tests of “upper limits”and performance in noise. The selectedinstrument was then issued to the patient.The commercial hearing aid companiesrepresented at the Deshon unit at thetime included: Acousticon, Audiphone,Aurex, Beltone, Maico, Otarion,Radioear, Sonotone, Telex, Vacoliteand Zenith.
HEARING AID SELECTIONDetailed accounts of the Deshon pro-
gram’s philosophy and procedures are foundin the series of articles published by Carhartin 1946-7, (Carhart, 1946 a,b,c,d:Carhart, 1947 a and b). The following isbased on those publications, as well as onthe other sources for this report.
The hearing aid program at Deshonbegan with a thorough work-up by theCenter’s multidisciplinary team of med-ical and non-medical personnel. By thetime the Center had its full staff and
✯✯✯✯✯✯DESHON GENERAL HOSPITAL AURAL REHABILITATION CENTER
Butler, Pennsylvania
The following discussion of the Deshon General Hospital is based on the annual reports of theHospital for the years 1942-1946 (Annual Reports, 1942-1944, 1945, 1946), and also on discussions with the few survivors I could locate and communicate with, some published material, as noted, and a few reprints of such items that were supplied to me by surviving colleagues. MajorMartin and I visited the Deshon unit on June 11-14, 1945 as part of our authorized travel to theArmy units to compare experiences.
* I am deeply grateful to Professor Sandra Gordon-Salant for devoting considerable time and effort to gathering and dispatching to me pertinent material fromthe U.S. National Archives at College Park, Maryland.

21Origins of Audiology World War II Programs
specially designed and fabricated equip-ment the hearing examination includ-ed pure tone audiometer tests, both airand bone conduction and the newly-introduced speech perception tests,including the “phonetically bal-anced” (PB) word lists providedby the Harvard PsychoacousticLaboratories.
The technique for findingthe pure tone thresholds, at theDeshon Center, “followed rigor-ously” the procedures devised byHughson and Westlake, as con-tained in a manual prepared bythem for the Committee onConservation of Hearing(Hughson and Westlake, 1944).
The hearing loss for speechwas deter- mined through head-phones in a two-room testingsetup as at present, using “equated wordlists” or if necessary, just simple ques-tions about Army experiences, againusing the Hughson-Westlake techniquefor obtaining the level of 50% correctresponses as the threshold. (Carhart 1946b,pp3-4) (It is of interest the the term“spondee” is not mentioned in the article.)
Today’s audiologists will be sur-prised at Carhart’s spirited advocacy ofthe usefulness of the measure of hear-ing loss for speech, as he writes, partlyin italics for emphasis, “Further, experi-ence and experimentation have led thegroup at Deshon General Hospital tothe firm conviction that loss in abilityto hear speech is an essential datumwhich must be obtained with everyaudiometric test” (ibid p. 5). Carhartdiscusses the general agreement of thethreshold of hearing for speech and theaverage loss at the pure tone frequen-cies 512-2048 cycles per second asnoted earlier by Hughson andThompson (1942), but argues that sig-nificant discrepancies in a particularcase can have clinical importance.
The next step in the work-up pre-ceding the evaluation with trial hearingaids included a test of speech discrimi-nation. The test material is not clearlystated in this article (Carhart 1946b),other than the statement that “It is onedevised at this hospital to give a generalpicture of discriminative ability and alsoto isolate the speech sounds causing thepatient’s particular difficulty.”Interestingly, Carhart notes that such
information can indicate the need for“special training procedures ..to increaseefficient use of an instrument” (ibid p.6). In tests with trial aids, however, the“phonetically balanced” (PB) word lists
developed at the Harvard Psychoacousticlaboratory were included.
A characteristic of the Deshontesting was the use of “live voice”, inwhich the test material is spoken bythe tester through a microphone, withmonitoring of the level via an intensi-ty meter, in contrast to the preferenceat the Hoff Center, for example, forthe recordings prepared by the Harvardand CID laboratories. (See discussionon NDRC of this report.)
An attractive feature, at theDeshon center, was the inclusionof “listening hours”, before andafter the introduction of hearingaids. Here a group of patients lis-tened through a group hearingaid to a variety of recorded noisesand sounds, such as instrumentalmusic and speech, as a structuredpreparation in the rating systemto be used later with the trialhearing aids.
After the fabrication in thehospital’s own laboratories of thepatient’s ear insert, as in theother military centers, thepatient used a pre-selection of varioushearing aids and their combinations(e.g. of different receivers) for one dayeach. In addition to his rating the per-formance of each in use around the hos-pital and at instructional sessions in lipreading and others, he again attendedthe “listening hours”, where he rated theinstrument he had been wearing for thepast day. Carhart believed that these
experiences with the various aids consti-tuted “preliminary auricular training” inwhich the patient “develops awarenessof auditory differences and lays the foun-dation for more rigorous training” when
the patient finally received hisown hearing aid (ibid p. 10).
COMPARATIVE EVALUATION OF HEARING AIDSFollowing the weaning out ofless acceptable hearing aids theremaining 3 or 4 hearing aidswere then included in the for-mal comparative hearing aidevaluation, in which four testswere conducted.
As the forerunner of such test-ing in audiology clinics eversince, hearing aid selection inthe fully organized stages of the
WW II military clinics took place withthe patient seated in the sound isolatedtest room facing a loudspeaker, adjacentto the “control” room, where the testeroperated the test equipment andwatched the patient through a smallwindow.. Carhart’s illustrative exampleat Deshon was similar to those at theother centers.
The hearing aid under test was placedon a baffle above and behind the seatedpatient, with the receiver cord runningdown to the receiver which was snapped
onto the fabricatedear insert in his ear.
Four measureswere employed at theDeshon Aural Reha-bilitation Center: a. Sensitivity, or effective gainb. Tolerance limit
Schema for hearing aid fitting (Deshon General Hospital).
Early hearing aidevaluation

22Origins of Audiology World War II Programs
c. Effective speech-to-noise ratiod. Discrimination. In Carhart’s (1946c)
article he stated that this was a measure of “the efficiency with which the patient could distinguishsmall sound differences” (ibid pp 780-781), but in application it was a test ofword discrimination.
Before beginning the test, thepatient was asked to adjust the gaincontrol of the first hearing aid so that itwould be comfortable for speech com-ing from the loudspeaker at 40 dBabove normal threshold. (Carhart 1946c,p. 782) (Note that all levels here are interms of dB above normal threshold.Post-war measurements with soundlevel meters found normal speechreception thresholds for spondee wordsto be about 22 dB SPL, which meantthat the 40dB test level was actuallyabout 60-62 dB SPL.)
The effective gain of the aid, setthus for the “40 dB comfort level”, wastaken as the difference between theunaided sensitivity, or speech receptionthreshold (SRT) and that obtainedwith the hearing aid.
Next the tolerance level, with thesame gain setting, was determined byraising the signal level gradually untilthe patient indicated that it was nolonger tolerable or 85 dB was reached.
The two tests were then repeatedwith the gain control set at the hearingaid’s maximum.
With the input signal raised to 50dB the signal-to-noise (S/N) ratio wasdetermined as “the limit of efficiency ofthe instrument in background noise.”(Carhart 1946b, p. 16), In another arti-cle Carhart suggests that the test noisemight be either “a combination of ther-mal hiss and static pulses or sawtoothwaves with a basic frequency of 120cps”. (Carhart 1946c)
After rechecking the SRT with theaid set once again for the 40 dB levelthe patient was tested for speech dis-crimination of words presented at 25 dBabove that SRT. A difference of 8% ormore was used in selecting the aids. It isinteresting that Carhart considered theprobable usefulness of what was latercalled the “intensity-performance” func-tion “to ascertain the sharpness of dis-crimination for different input levels ofspeech” (ibid p. 788), but cautionedthat the procedure needed the accumu-lation of more data.
The head of the Acoustic Clinicthen conferred with the patient toselect the “best” instrument, mainly butnot exclusively, on the basis of the
results of the four tests. When the per-formance results were essentially equiv-alent on more than one instrument “selection was based on auxiliary factorsof convenience, weight and estheticpreferences” (ibid p. 790).
COOPERATION WITH NDRCAlong with the other army centers
and the Navy Center, the Deshon unitwas involved in 1944 in the hearing aidstudies of Project 17.3, a contractualarrangement between the Office ofScientific Research and Development ofthe National Defense ResearchCommittee and the U.S. Army andNavy. According to a bimonthlyprogress report of Division 17, Section17.3 of the National Defense ResearchCommittee, dated July 1, 1944, on theSubject: Study and Development ofInstruments to Aid Militarily IncurredDeafness, the role of the Deshon Centerwas to validate and apply the results ofstudies at the Harvard UniversityPsycho- Acoustic Laboratory and theCentral Institute for the Deaf on thedevelopment of new tests and instru-ments for the evaluation and fitting ofhearing aids.
LIP READINGThis activity was similar to those at
the other military centers in which thelargest staff allocation was for the teach-ing of lip reading, the original service withwhich the program had begun. At first,all lessons were individual, with one les-son each day. By April 1944 group prac-tice sessions were added and eachpatient attended one individual and atleast one practice class daily. These weretaught by a rotating roster of teachers, toprovide “different accents, inflectionsand pronunciations.” (Annual Reports,1942-44, p 13) There was an attempt toinclude moving picture films for lipreading practice, but the staff were notsatisfied with the quality or content ofthe available films.
SPEECH CORRECTIONAbout thirty per cent of the hearing
impaired patients at Deshon, in 1944,were found to have “speech abnormali-ties”, and in 8 % these were thought tohave resulted directly from the hearingproblem. The summary of the patientspeech problems, in 1944, follows:
Dyslalia 49.6 %Dysphonia 44.5 %Dysphemia 4.6 %Dysphasia 0.8 %Dysarthria 0.6 %
SUMMARY OF THE DESHON PROGRAMBy the end of 1945 the staff of the
Deshon Center had grown to number52, in a year that saw their peak patientload and the issuing of 1,584 hearingaids. It was also a year in which, as atthe other military units, the prevalenceof “functional” hearing loss or func-tional exaggeration of a previous hear-ing problem was recognized, in 8% oftheir patients.
The Deshon program closed at theend of April 1946 after the end of thewar, having processed a total of 3, 663patients and having issued 2,792 hear-ing aids.
The Deshon program was another ofthe military’s historic examples of amultidisciplinary approach to the prob-lem of hearing impairment amongadults, with the introduction of newtechnology and materials and the emer-gence of creative thinkers, such asCarhart, who laid the basis of the newprofession of audiology.
REFERENCESAnnual Reports, 1942-1944, 1945,
1946. Deshon General Hospital. Modern Military Records, National Archives at College Park, College Park, Maryland
Carhart, R. (1946a) A practical approach to the selection of hearingaids. Trans. Amer. Acad. Ophthal. Otolaryng. 50:123-131.
Carhart, R. (1946b) Selection of hear-ing aids. Arch. Otolaryng. 44:1-18
Carhart, R. (1946c) Tests for selection ofhearing aids. Laryngoscope. 56:780-794.
Carhart, R. (1946d) Volume control adjustment in hearing aid selection. Laryngoscope. 56:510-526.
Carhart, R. (1947a) Auditory training. In Davis, H., Hearing and Deafness.
Rinehart Books, Inc. New York. Pp. 276-299.
Carhart, R. 1947b. Conservation of speech. In Davis, H., Hearing and Deafness. Rinehart Books, Inc. New
York. Pp. 300-317.The Service Club, The Volta Review
August 1944, pp. 457-8Hughson, W., and Thompson, E.,
(1942) Correlation of hearing acuity for speech with discrete frequency audiograms. Arch. Otolaryng. 3:526-540.
Hughson, W. and Westlake, H. (1944) Manual for Program Outline for Rehabilitation of Aural Casualties, both Military and Civilian. Supp. Am.Academy of Ophth., and Otolaryng.Douglas Printing Co., Omaha, Neb.

APPENDIX 3: DESHON GENERALHOSPITAL HEARING PROGRAM STAFFAS OF JULY 7, 1944:Chief of Service
Lt. Col. Marion R. MobleyActing Chief of Service
Major Edward H. Truex, Jr. Otologists
Captain Henry C. BarnabyCaptain Robert A. Schein
Acoustic DepartmentRaymond Carhart, (later Capt.), ChiefPfc Lee DoerflerPfc Albert DouglasPfc Wayne JeansSgt. Francis H. SondayMary Schmitz
Clinical Psychologist Donald A. Ramsdell
Speech Correction Department Verna AilshouseFlorence Henderson
Auricular Training Department Laila Larsen
LIP READING DEPARTMENTElisabeth H. Nitchie, PrincipalMina AveryKathryn BeckerAlice M. BurtnettMargaret DunnMae T. FisherAgnes FrazierEmily HarrisMary G. HeartyEmma D. KesslerHelen S. LowryMary MacCracken
Cpl Helen MeyerKate MorphyFlorence MurrinJosephine PrallGertrude RussellPfc Hugo SchunhoffShirley P. SteinVirginia TerryMargaret ThompsonGertrude TorreyMary K. Van WykEsther VonderheitFlorence Wooley
RED CROSSSarah BombergJoan BonnerRhoda KapelmanPhyllis McCalmontMinala Seibel
23Origins of Audiology World War II Programs
ConclusionThe “aural rehabilitation” programs
that were set up in the Americanarmed services in World Wars I and
II can be seen as the true beginnings of“clinical audiology,” and in fact the inspi-ration of the new term “audiology” itself.
The basic concept was to bring tobear on its hearing casualties a multidis-ciplinary array of personnel and servicesand the latest technical equipment formeasurements, testing and management,all facilitated by the unique circum-stances of the liberal wartime allocationof resources.
The units that were set up in 1943 inthe U.S. Army and in 1944 in the Navybrought together a concentration of mil-itary and civilian medical, rehabilitation,psychological, social work and technicalpersonnel, who focused their specializedknowledge and skills on young adultswho suffered from mild to profound lossof hearing. A significant contribution tothe maturation of the new professionalfield was the development, calibrations,and validation of sophisticated hearingtest equipment and stimuli by theHarvard University Cruft and Psycho-Acoustic laboratories and the CentralInstitute for the Deaf, under the aegis ofthe National Defense ResearchCommittee (NDRC) of the Office ofScientific Research and Development.
Whereas the WW I unit lasted justone year and serviced only 108 soldiersof the nearly 13,000 who later claimedhearing losses through the VeteransAdministration, the WW II centers
processed about 14,000 between late1943 and 1946.
The beginnings of the WW II pro-grams were based essentially on a contin-uation of the WW I reliance on theteaching of lip reading, but as the staffsgrew to include university trained speechscientists like Grant Fairbanks of theUniversity of Iowa and RaymondCarhart of Northwestern University andothers who were graduates in speech cor-rection and teaching of the deaf, alongwith the technical input sponsored bythe NDRC, the focus changed quickly toexploit the scientific and technical ori-entation of this personnel infusion.
The relatively crude but effectivenew electronic hearing aids that resultedfrom the competitive interest of themanufacturers in this attractive newmarket encouraged these staff membersto exploit the emerging technology asfully as possible in the management ofhearing impairment.
There was a price to pay. As theavailability of new technology piquedthe curiosity and desire for more “sci-ence” in our new profession, the concen-tration, before and during the militaryprograms, on a total approach to restor-ing effective communication ability andconcern for the psychological, social andvocational needs of each hearingimpaired adult would soon becomediminished in the emerging “audiology.”
Fortunately for the patients of theWW II programs, the transition actuallyprovided them with the best of the the
two eras. The organization of the reha-bilitation programs at all four centerscontained the full rehabilitation focuswhile eagerly introducing the new tech-nology.
The new interest in the validation ofprocedures, such as the testing of hear-ing, undoubtedly helped to end suchmisleading practices as the uncontrolledwhisper and speech tests which weremandated in the induction and assign-ment of military personnel.
But above all the opportunities todevelop new knowledge and skills thatwere provided by the well funded andgenerously staffed military programs ledlogically to the fashioning of a new serv-ice profession. As they returned from thewar to civilian life a number of thosewho had developed new insights whilemembers of the staffs of these unitsbecame leaders in the establishment oftraining programs in the nation’s univer-sities and in the staffing of such units asthe Veterans Administration. Theirefforts following WW II and those of thecolleagues and students with whom theyinteracted produced new professionalworkers for the field, generated expandingresearch, engaged in a flow of related scientific and professional literature, and promoted the activation of nationaland international scientific and profes-sional meetings and public informationactivities that have brought about theuniversal recognition of audiology andclinical audiology.
✯✯✯✯✯✯✯✯✯

Origins of Audiology World War II Programs24
✯✯✯✯✯✯✯✯✯✯✯✯
Post-war diagnostic audiology “narcosynthesis” evaluation.
Post-war hearing evaluations often required Galvanic skin response conditioningwith mild shock reinforcement to confirm hearing thresholds.
Military audiology facilities provided early research inhearing evaluation methods and procedures.
Special attention was given toaural-speech training.
An early wartime aural rehabilitation class.

This monograph presented by theAMERICAN ACADEMY OF AUDIOLOGY
THE VOICE OF AUDIOLOGYOver 28 million Americans suffer from hearing loss, making it one of the most prevalent chronic health condi-tions in this country. Left untreated, hearing loss has been linked to speech and language delays in children andisolation and depression in seniors. The American Academy of Audiology is the voice of the profession of audi-ology.... And a well respected source of hearing information for medical professionals, government agencies,public interest groups, consumers and press.
CARING FOR AMERICA’S HEARINGThe American Academy of Audiology is the largest professional association for, by, and composed solely of audiologists. Committed to providing quality hearing care to the public, The Academy represents over 7,000audiologists and students throughout the United States, Canada, and the world.
The Academy provides a vibrant, interactive forum for members to exchange ideas and discuss common pro-fessional issues involving new technology, continuing education, certification and licensure, regulatory and leg-islative developments, and more. The Academy serves as a liaison between the profession, the government, andthe public, and exercises an authoritative voice on hearing issues great and small. Most important, our membersconsider The Academy a true partner in their business, adding vision to their professional and academic lives.
HOW’S YOUR HEARING? ASK AN AUDIOLOGIST! The Academy is a comprehensive source of hearing information for all hearing healthcare professionals and forthe public. Armed with Academy insight and information on the diagnosis and management of persons withhearing loss, evaluation of hearing aids and amplification technologies, cochlear implants, infant and pediatrichearing screenings, diagnostic evaluations and more. Interested individuals can explore a multitude of optionswith knowledge and confidence through our publications, electronic communications, and our website atwww.audiology.org.
The American Academy of Audiology is a professional organization of individuals dedicated to providing quality hearing care to the public. We enhance the ability of our members to achieve career and practice
objectives through professional development, education, research, andincreased public awareness of hearing disorders and audiologic services.
For more information about the American Academy of Audiology visit our website at www.audiology.org