Embed Size (px)
Citation preview

DIABETES
TYPE 1
DIABETES
TYPE 2
DIABETES
monogenic diabetes
idiopathic type 1
complex genetic disorders
pancreatic diseases
endocrinopathies
iatrogenic diabetes
autoantibodies
[DNA]
[insulitis]
world epidemysecond diabetes
epidemy
DNA
hormones
insulin secretion
pancreatic imaging
O
T
H
E
R
S absence of positive
diagnostic parameter
heterogeneity
T2D DIAGNOSIS
from physiology to disease
po
pu
lati
on
%
physiology
dia
gn
ostic
thre
sh
old
common
disease
multiple genes
multifactorial
chronicunknown cause
environment
genesmonogenic
diabetes
Psammomys obesus

NATURAL HISTORY OF TYPE 2 DIABETES
a highly chronic process
adapted from Weyer C et al. J Clin Invest 1999
insulin resistance + b cell compensation
DIABETES
insulin resistance + early b cell deficit
bcell f
un
cti
on
insulin sensitivity
normoglycemia
glucose intolerancediabetes
Diabetes Audit and Research Tayside study .
DIABETES

b CELL DEFECTS IN TYPE 2 DIABETES
N
O
R
M
A
L
glucose 500mg iv
+ 20mg/min 60min
Nesher & Cerasi Diabetes 2001
APOPTOSISOXYDATIVE STRESS
markers
nitrotyrosine
8-OH-2’-deoxyguanosine
Sakuraba et al, Diabetologia, 2002
nucleus staining
DNA damage DEDIFFERENCIATIONTalchai C et al. Cell 2012
D
I
A
B
E
T
E
S
reduced first phase insulin response
to i.v. glucose
FUNCTIONAL DEFECT GLUT1/2, Glucokinase
glucose oxydation
AMPK activation
insulin
MGAT4A glycosyl trase
foxo-1, PDX-1
TYPE 2
DIABETES
glucagon
insulin
DIABETES: GENES
T2D
λs ~ 3
DZ twin concordance ~ 20%
MZ twin concordance ~ 70%
Number of genes multiple
Dominant gene none
Proportion of heritability
explained< 10%
Predicted heritability > 50%

1
1.5
TYPE 2 DIABETES: MORE THAN 40 GENES
PT
PR
D
KC
NQ
1
TC
F7
L2
SR
R
DU
SP
9
CD
KN
2A
-2B
IRS
1
UB
E2
E2
FT
O
HH
EX
-ID
E
SL
C30
A8
CD
KA
L1
IGF
BP
2
TH
AD
A
PP
AR
G
CE
NT
D2
KC
NJ11
NO
TC
H2
C2C
D4A
/B
WF
S1
AD
CY
5
CH
CH
D9
CD
C12
3/C
AM
K1d
HM
GA
2
HN
F1
B
JA
ZF
1
RB
MS
1
TS
PA
N8
/LG
R5
MT
NR
1B
AD
AM
TS
9
ZB
ED
3
DU
SP
8
BC
L11
A
DG
KB
ZF
AN
D6
PR
OX
1
KL
F1
4
GC
K
TP
53
INP
1
HN
F1
A
GC
KR
PR
C1
PPARG, ENPP1,
ADIPOQ, SREBF1,
PPARGC1A, AHSG,
SHBG, IRS1, FTO
insulin resistance
KCNJ11, HNF1B
FOXO1, SLC30A8
HHEX, CDKAL1, WFS1
IGF2BP2, CDKN2A/B
SGK1, JAZF1, KCNQ1,
TCF7L2
ADAMTS9
CAPN10 CDC123/CAMK1D, THADA
TSPAN8/LGR5, MTNR1B
ISLET GENES
Schäfer et al. 2011
Travers ME et al. 2011* GWAS
2377 participants
255 T2D
[Framingham Offspring Study]
Sex
Family history
Age
BMI
Fasting plasma glucose
Systolic blood pressure
HDL-Cholesterol
Fasting triglycerides
Meiggs JB et al. N Engl J Med 2008
Sex-adjusted
reclassification by genotype score 4.1%
11.9% < 50
0.47 > 50
sex-adjusted OR
for T2D 1.12
GENETIC DIVERSITY

TYPE 1 DIABETES MELLITUS
• insulitis
Gepts W 1965, Diabetes
Gianani R 2010, Diabetologia
b cell selectivity
an autoimmune disease
• islet cell autoantibodies
Bottazzo & Doniach 1974, Lancet
anti-GAD
anti-IA2
anti-insulin
anti-ZnT8
others
aAc threshold Specificity Sensitivity
IAA ≥50 nU/ml 99% 64%
GAD/IA-21 ≥4 UI/ml 98% 96%
GAD ≥ 5 UI/ml 98% 92%
IA-2 ≥ 7.5 UI/ml 100% 64%
ZnT8 ≥15 UI/ml 99% 68%
TYPE 1 DIABETES: A CHRONIC DISEASE
ß c
ell m
ass
diabetes
hyperglycemia
Bingley et al. Diabetologia 2006
patientduration of
diabetes
diabetes
recurrenceInsulitis ICA
1 22 years 60 days CD8+ T cells -
2 17 years 44 days CD8+ T cells -
3 27 years 92 days CD8+ T cells +

THE EFFECTOR versus REGULATORY BALANCE
Regulation
• Regulatory T cells (IL-10, TGF-β)
• Regulatory B cells (IL-10)
• NK T cells
• Regulatory dendritic cells (IDO)
Immunity
• Pathogenic CD4 & CD8 T cells
• Pathogenic B cells
• Activating dendritic cells
(iNOS, IL-12)
Innate immunity
• IFNγ
• Class I
• CXCL10
• neutrophils
incidence: > 65/105/year in Finland
3-4%/year,
earlier age at onset, milder HLA susceptibility
0
20
40
60
1921 50s 1972 1992
inc
ide
nc
e [
10
5/y
ea
r]
VIRUSES
congenital rubella
coxsackie virus B
varicella-zoster
mumps
cytomegalovirus
Epstein-Barr
OTHER
SUN EXPOSURE
vitamin D
NUTRITIONAL
FACTORS
cow milk proteins
absence of a unique environmental factorgenesenvironment
monogenic
T1DAIRE
FoxP3
SIRT1
congenital
rubella
fulminant
type 1 ?
common forms
numerous
numerous
TYPE 1 DIABETES MELLITUS
immune genesvirus-response genes
β-genes
λs 15
sibling incidence 5-6%
child of diabetic mother 2-3%
child of diabetic father 6%
ls 15
dizygotic twin
concordance0-13%
monozygotic twin
concordance21-70%
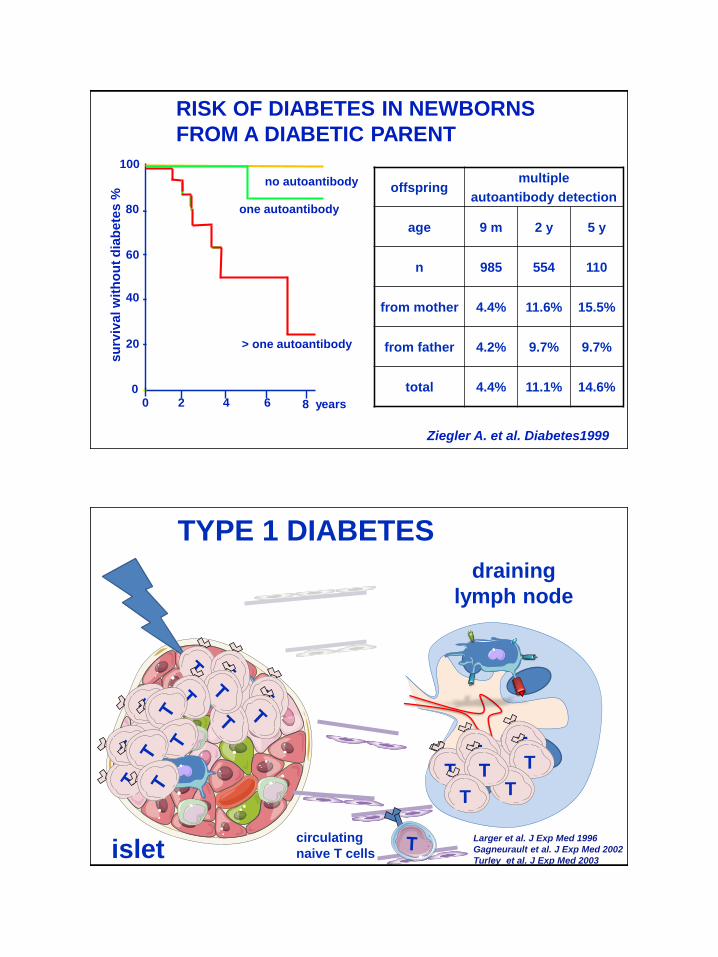
offspringmultiple
autoantibody detection
age 9 m 2 y 5 y
n 985 554 110
from mother 4.4% 11.6% 15.5%
from father 4.2% 9.7% 9.7%
total 4.4% 11.1% 14.6%
RISK OF DIABETES IN NEWBORNS
FROM A DIABETIC PARENT
Ziegler A. et al. Diabetes1999
no autoantibody
one autoantibody
su
rviv
al w
ith
ou
t d
iab
ete
s %
0
20
40
60
80
100
0 8 years42 6
> one autoantibody
TTT
T
TTT
T
TYPE 1 DIABETES
isletcirculating
naive T cells
TTT
TT
TT
T
draining
lymph node
Larger et al. J Exp Med 1996
Gagneurault et al. J Exp Med 2002
Turley et al. J Exp Med 2003

MONOCLONAL TREATMENTS OF T1D
Keymeulen B et al. 2005, N Engl J Med
anti-CD3
Ludvigsson et al, N Engl J Med, 2008
GAD-alum
n = 35
n = 34
n = 40
n = 40
4-doses n = 111
2-doses n = 108
Placebo n = 115
Ludvigsson et al, N Engl J Med, 2012Sherry N et al. Lancet 2011
anti-CD3 n = 417
placebo n = 99
all patients
primary composite outcomeInsulin < 0.5 U/kg& HbA1c < 6.5% 14d fd 19.8%
14d ld 13.7%
6d fd 20.8%
placebo 20.4%children
Allegheny County
childhood-onset (< 18) T1D registry
diagnosed 1965-79
Secrest et al. Diabetes 2010
acute
renal
cardio
vascular
infections
cancer
n = 1075
age Controls
mortality rate
/10 3 person-yrs
Standardized
Mortality Rate
♂ 0-4 1.4880 2.0
5-9 0.1511 3.7
19-14 0.2218 4.6
15-19 0.7166 3.3
20-24 0.8752 2.3
25-29 0.9381 4.5
30-34 1.1388 6.3
35-39 1.4270 3.3
♀ 0-4 1.2640 0.0
5-9 0.1550 0.0
19-14 0.1289 4.6
15-19 0.2802 5.8
20-24 0.2927 3.2
25-29 0.3477 4.6
30-34 0.5285 5.1
35-39 0.7086 2.7
3.9
4.0
Skrivarhaug et al. Diabetologia 2006 [Norway]
T1D MORTALITY
excess mortality compared to
the general population
intermediate disease compared to
high risk autoimmune diseases
normal life expectancy
In absence of nephropathy

T CD4TNF-a, IFN-g…
b cell
TYPE 1 DIABETES
FROM T CELLS TO DIABETES PREVENTION
Insulin
new preclinical
models
Towards trials
APC
MHC-resticted
peptides
β-cell proteasesproteasome
class IER
T CD8
IMMUNE IMAGE OF β-CELLSautoantigen peptides insertion in class I MHC molecules

Toma et al, PNAS2005; Toma et al. Diabetes 2009; Luce Diabetes 2011
CD8+ T CELL RESPONSE TO A*0201-RESTRICTED
PREPROINSULIN PEPTIDES [ELISPOTassay]
$ Val42, L14, L16, A23 & A24 were identified as C-terminal residues
generated by proteasome digestion in vitro.
2-11
6-14
15-24
30-39
33-42
34-42
42-51
101-109
PDHase 208-16
Nef 83-91
MATA2 58-66
hu
man
pre
pro
insu
lin
candidate peptide C-termini
proteasome digestion $
anchoring residues
A*0201: C,L,V in 2
in vitro binding to
soluble A*0201
T1D patients
P22P01
basal
P04
16.1 8.9 19.2
Insulin
B18-27
14.4
controlpositive
168.978.3
+++ +++
145.5
+++
33.3 161.1
++++
peptide CD8+ IFNγ response
long
standing
recent
onset
total
34-42* 2/4 4/10 6/14
6-14* 7/13 1/4 8/17
6-16* 5/15 2/4 7/19
14-23* 7/13 0/4 7/17
15-24* 7/13 1/4 8/17
class I preproinsulin peptide
A2.1 2-11
A2.1 6-14
A2.1 15-24
A2.1 30-39
A2.1 33-42
A2.1 34-42
A2.1 42-51
A2.1 101-109
controls PDHase 2008-216 MATA2 58-66 Nef 83-91
b cells
TCD8+
TCD8+
TETRAMER RECOGNITION OF BLOOD CD8+ T CELLS
class I
peptide
biotin
streptavidin
100
101
102
103
104
100
101
102
103
104
Dt1A5 TTM A2 PPIh_Dt1A5 TTM A2 33-42.fcsÉCD3+ CD8+
PerCP-A: CD8 PerCP-A
PE
-A:
TT
M P
E-A
0.810 0.79
99.20
100
101
102
103
104
100
101
102
103
104
Dt1A5 TTM A2 PPIh_Dt1A5 TTM A2 6-14.fcsÉCD3+ CD8+
PerCP-A: CD8 PerCP-A
PE
-A:
TT
M P
E-A
0.0370 0.037
1000
100
101
102
103
104
100
101
102
103
104
25-01-08_D124D 6-14.fcsÉCD3+ CD8+
PerCP-A: CD8 PerCP-A
PE
-A:
TT
M P
E-A
0.60 0.54
99.60
Sandrine Luce
CD8+ T cell expansions in peripheral blood

Recent-onset: leader sequence peptides
TETRAMER RECOGNITION OF BLOOD CD8+ T CELLS
A2.1-restricted peptides
Luce et al. Diabetes 2011
2-11
6-14
15-24
30-39
33-42
34-42
42-51
101-109
PDHase 208-16
Nef 83-91
MATA2 58-66
hu
man
pre
pro
insu
lin
Long-standing: B chain peptides
single cell PCR Insulin-specific CD8: central memory
CMV-specific: effector memrory
Control CD8: 33% IL-10
mouse
MHC HLAIAg7
HLADQ8HLADQ8
insulin/A2.1/DQ8 mice
YES
Insulin
A2.1
DQ8 genes
OUF
A2/DQ8 Tg Human insulin
x
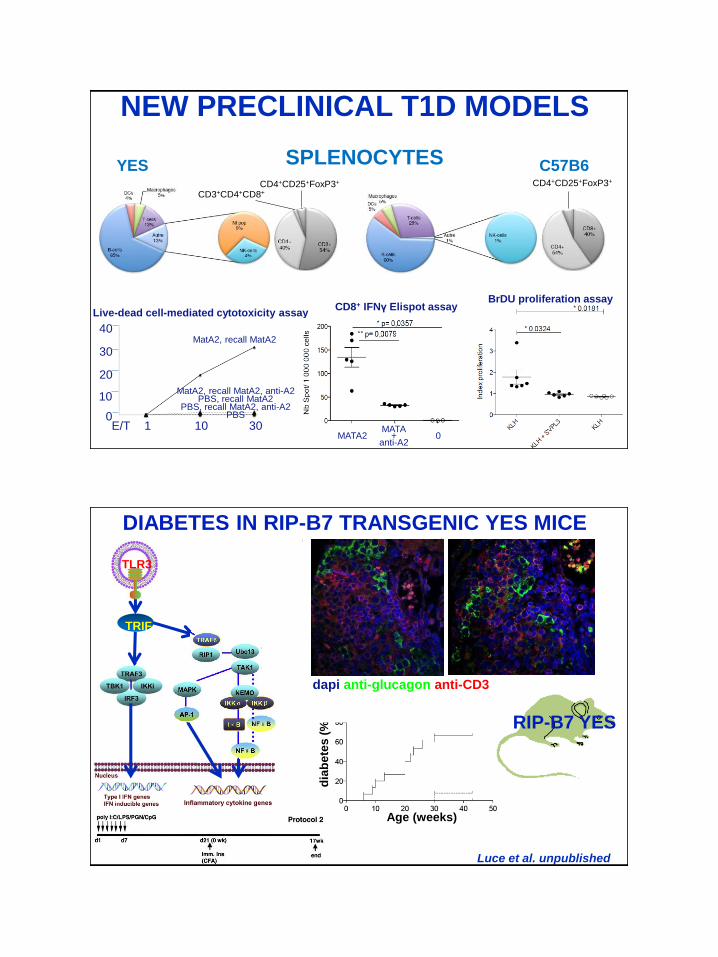
NEW PRECLINICAL T1D MODELS
♂ ♂ ♀ ♀
YES
YESCol
Col
Intraperitoneal glucose tolerance test
AU
C m
g.h
/dL
beta cell mass
mg
0
10
20
30
40
E/T 1 10 30
Live-dead cell-mediated cytotoxicity assay
MatA2, recall MatA2
MatA2, recall MatA2, anti-A2PBS, recall MatA2
PBS, recall MatA2, anti-A2PBS
BrDU proliferation assay
NEW PRECLINICAL T1D MODELS
CD8+ IFNγ Elispot assay
MATA2MATA
+anti-A2
0
SPLENOCYTES C57B6CD4+CD25+FoxP3+
YESCD4+CD25+FoxP3+
CD3+CD4+CD8+
DIABETES IN RIP-B7 TRANSGENIC YES MICE
B7.2
CD28
CD4
MHC
TCR
T cell
Luce et al. unpublished
Age (weeks)
dia
be
tes
(%
)
% t
ota
l is
lets
non diabetic diabetic
CD4
CD
8
CD11b
CD
11c
CD19
TC
Rβ
dapi anti-glucagon anti-CD3
RIP-B7 YES
TLR3
TRIF

DIABETES IN RIP-B7 TRANSGENIC YES MICE
CD8+ TMr+ expansion assay
CD4+ T cell proliferation
FROM PALLIATIVE TREATMENT TO PREVENTION OF TYPE 1 DIABETES
T CD4
APC
T CD8
NKTNK
T reg
B
damaged
islet of Langerhans
AUTHORS FROM RESEARCH TO CLINIC
YES mice
insulin
Luce S et al. Diabetes 2011
“We always overestimate the change that will occur in the next
two years and underestimate the change that will occur in the
next ten. Don’t let yourself be lulled into inaction.” Bill Gates
Carlier et al. PloSOne 2012
Immunotherapy
EU FP7 exalt project
HLApeptideautoantigen
T

M1IFNg+
Th1
M1
M1
M1
M1
Th17
CD8+
CytokinesIL1βTNFa
IFNgIL6MCP-1
FFA
insulin
resistance
insulin
resistance
insulin
resistance
insulinsecretion
A T2D/T1D CONNECTION ?
CRP, SAA
islet inflammation
β cell debris β cell
dysfuntion
T2Dsystemicinflammation
T1D?
local inflammation
T2D β-cell genesT1D
β-cell& immune genes
TLR4, TLR2TLR3, TLR7, TLR9, RIG-1
Département Hospitalo-Universitaire AUToimmune and HORmonal diseaseS
Uth rs
DHU
DIABETES
ADRENAL DISEASES
VASCULITIDES
Andrea Toma
Claire Briet
Isabelle Tardivel
Chantal Bécourt
Sandrine Luce
Etienne Larger
Ute Rogner
Roberto Mallone
François Lemonnier
Agnès Lehuen
MINISTRY OF RESEARCH (ANR)
NOVO/JDRF/EFSD joint program
« Contradiction is not a sign of falsity, nor the lack of
contradiction a sign of truth. »
Blaise Pascal
« Ni la contradiction n'est marque
de fausseté, ni l'incontradiction
n'est marque de vérité. »





























