Embed Size (px)
Citation preview
AUA Guidelines for Invasive Bladder Cancer: What’s New?”
MichaelS.Cookson,MD,MMHCProfessorandChairman
DepartmentofUrology,UniversityofOklahoma
History• 1999:AUAguidelinesPanelNon-muscleinvasivebladdercancer(AUA)–Smithetal
• 2009:UpdateAUAguidelinesPanelNon-muscleinvasivebladdercancer(AUA)– Halletal
• 2016:UpdateAUAguidelinesPanelNon-muscleinvasivebladdercancer(AUA/SUO)– Changetal
• 2017:TreatmentofNon-MetastaticMuscle-Invasive BladderCancer:AUA/ASCO/ASTRO/SUOGuideline
GuidelineReview
AHRQSYSTEMATICREVIEW• January1990- October2014
Twoinvestigatorsindependentlyassessedtheriskofbiasforallrandomizedtrialsandobservationalstudiesandassignedratingsof“high,” “medium,” or“low” riskofbias.
Methodology
• GradingofGuidelines:
A• WellconductedRCT’s• Exceptionalobservationalstudies
B• RCT’sand/orobservationalstudieswithsomeweaknesses
C• Observationalstudiesthatareinconsistent-difficulttointerpret
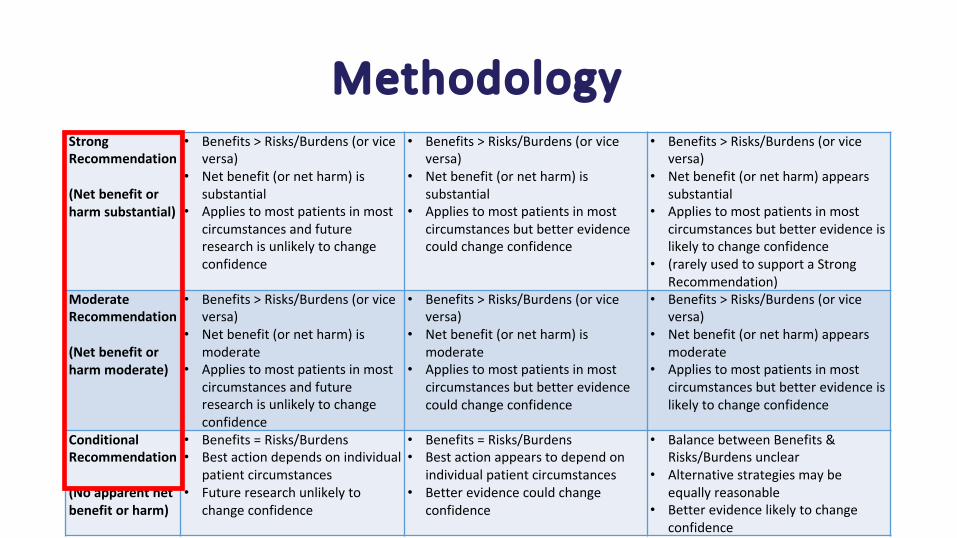
MethodologyStrongRecommendation
(Netbenefitorharmsubstantial)
• Benefits>Risks/Burdens(orviceversa)
• Netbenefit(ornetharm)issubstantial
• Appliestomostpatientsinmostcircumstancesandfutureresearchisunlikelytochangeconfidence
• Benefits>Risks/Burdens(orviceversa)
• Netbenefit(ornetharm)issubstantial
• Appliestomostpatientsinmostcircumstancesbutbetterevidencecouldchangeconfidence
• Benefits>Risks/Burdens(orviceversa)
• Netbenefit(ornetharm)appearssubstantial
• Appliestomostpatientsinmostcircumstancesbutbetterevidenceislikelytochangeconfidence
• (rarelyusedtosupportaStrongRecommendation)
ModerateRecommendation
(Netbenefitorharmmoderate)
• Benefits>Risks/Burdens(orviceversa)
• Netbenefit(ornetharm)ismoderate
• Appliestomostpatientsinmostcircumstancesandfutureresearchisunlikelytochangeconfidence
• Benefits>Risks/Burdens(orviceversa)
• Netbenefit(ornetharm)ismoderate
• Appliestomostpatientsinmostcircumstancesbutbetterevidencecouldchangeconfidence
• Benefits>Risks/Burdens(orviceversa)
• Netbenefit(ornetharm)appearsmoderate
• Appliestomostpatientsinmostcircumstancesbutbetterevidenceislikelytochangeconfidence
ConditionalRecommendation
(Noapparentnetbenefitorharm)
• Benefits=Risks/Burdens• Bestactiondependsonindividual
patientcircumstances• Futureresearchunlikelyto
changeconfidence
• Benefits=Risks/Burdens• Bestactionappearstodependon
individualpatientcircumstances• Betterevidencecouldchange
confidence
• BalancebetweenBenefits&Risks/Burdensunclear
• Alternativestrategiesmaybeequallyreasonable
• Betterevidencelikelytochangeconfidence
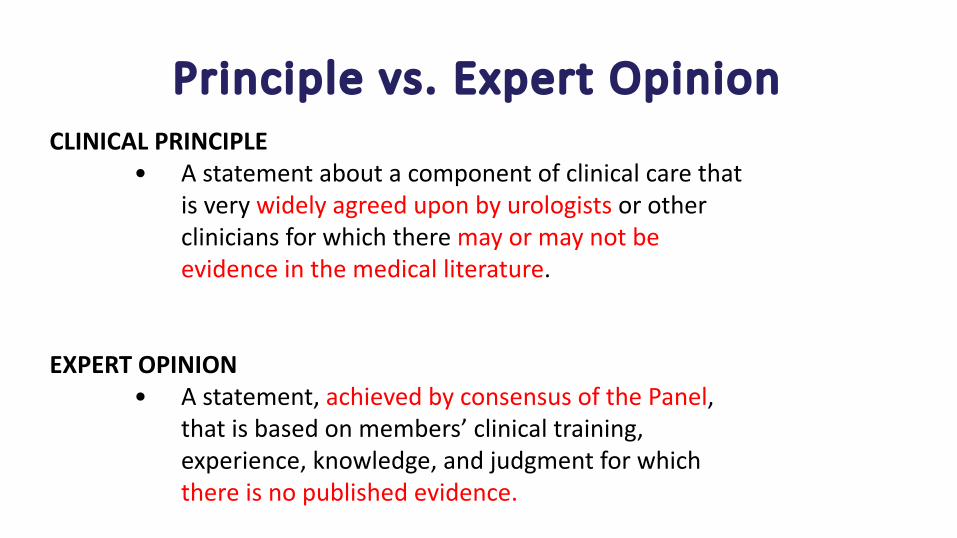
Principlevs.ExpertOpinionCLINICALPRINCIPLE
• Astatementaboutacomponentofclinicalcarethatisverywidelyagreeduponbyurologistsorothercliniciansforwhichtheremayormaynotbeevidenceinthemedicalliterature.
EXPERTOPINION• Astatement,achievedbyconsensusofthePanel,
thatisbasedonmembers’ clinicaltraining,experience,knowledge,andjudgmentforwhichthereisnopublishedevidence.

Epidemiology
• 79,000newcasesin2017• 16,870deathsin2017
• 25%ofnewlydiagnosedpatientspresentwithmuscleinvasivedisease

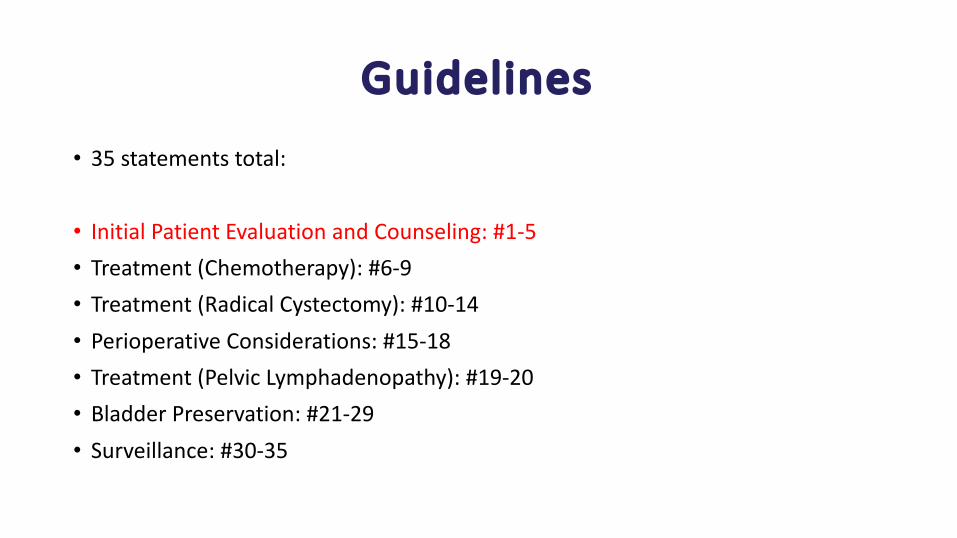
Guidelines
• 35statementstotal:
• InitialPatientEvaluationandCounseling:#1-5• Treatment(Chemotherapy):#6-9• Treatment(RadicalCystectomy):#10-14• PerioperativeConsiderations:#15-18• Treatment(PelvicLymphadenopathy):#19-20• BladderPreservation:#21-29• Surveillance:#30-35
Guidelines
• 35statementstotal:
• InitialPatientEvaluationandCounseling:#1-5• Treatment(Chemotherapy):#6-9• Treatment(RadicalCystectomy):#10-14• PerioperativeConsiderations:#15-18• Treatment(PelvicLymphadenopathy):#19-20• BladderPreservation:#21-29• Surveillance:#30-35
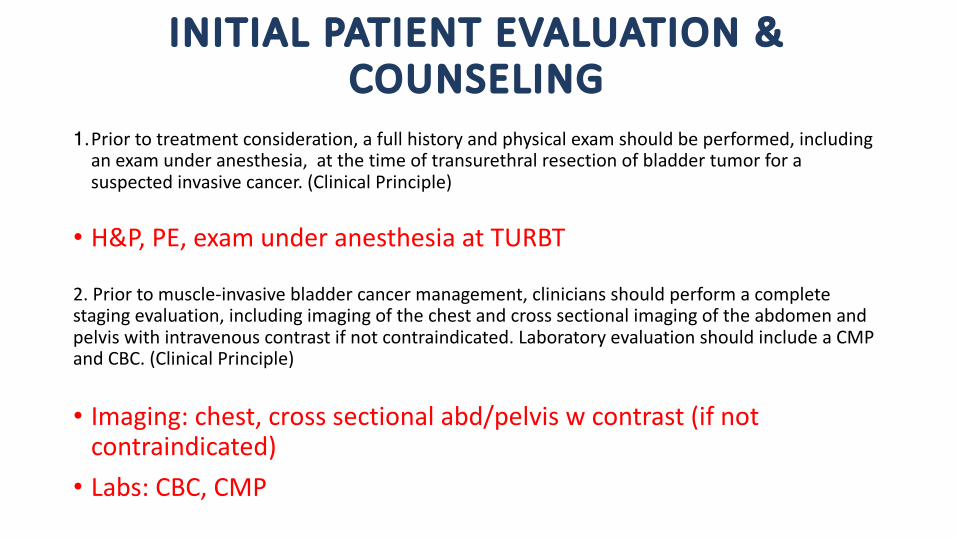
INITIALPATIENTEVALUATION&COUNSELING
1.Priortotreatmentconsideration,afullhistoryandphysicalexamshouldbeperformed,includinganexamunderanesthesia,atthetimeoftransurethralresectionofbladdertumorforasuspectedinvasivecancer.(ClinicalPrinciple)
• H&P,PE,examunderanesthesiaatTURBT
2.Priortomuscle-invasivebladdercancermanagement,cliniciansshouldperformacompletestagingevaluation,includingimagingofthechestandcrosssectionalimagingoftheabdomenandpelviswithintravenouscontrastifnotcontraindicated.LaboratoryevaluationshouldincludeaCMPandCBC.(ClinicalPrinciple)
• Imaging:chest,crosssectionalabd/pelviswcontrast(ifnotcontraindicated)• Labs:CBC,CMP
INITIALPATIENTEVALUATION&COUNSELING
3.Anexperiencedgenitourinarypathologistshouldreviewthepathologyofapatientwhenvarianthistologyissuspectedorifmuscleinvasionisequivocal(e.g.,micropapillary,nested,plasmacytoid,neuroendocrine,sarcomatoid,extensivesquamousorglandulardifferentiation).(ClinicalPrinciple)
• VariantHistologyshouldbere-viewedbyGUtrainedpathologist• Upto1/3treatmentstrategieschangedafterreviewbyGUPathologist• VariantHistologiesàMorelocallyadvancedcomparedtoUCbladder
INITIALPATIENTEVALUATION&COUNSELING
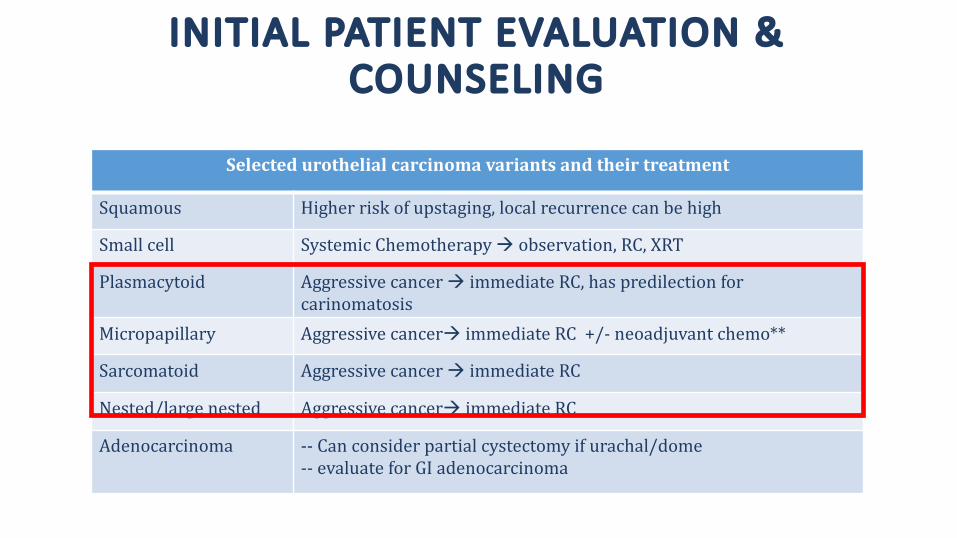
Selectedurothelialcarcinomavariantsandtheirtreatment
Squamous Higherriskofupstaging,localrecurrence canbehigh
Smallcell SystemicChemotherapyà observation,RC,XRT
Plasmacytoid Aggressivecancerà immediateRC, haspredilectionforcarinomatosis
Micropapillary Aggressivecancerà immediateRC+/- neoadjuvant chemo**
Sarcomatoid Aggressivecancerà immediateRC
Nested/largenested Aggressivecancerà immediateRC
Adenocarcinoma -- Canconsiderpartialcystectomyifurachal/dome-- evaluate forGIadenocarcinoma

INITIALPATIENTEVALUATION&COUNSELING
4. Forpatientswithnewlydiagnosedmuscle-invasivebladdercancer,curativetreatmentoptionsshouldbediscussedbeforedeterminingaplanoftherapythatisbasedonbothpatientcomorbidityandtumorcharacteristics.Patientevaluationshouldbecompletedusingamultidisciplinaryapproach.(ClinicalPrinciple)
• Multi-disciplinarydiscussion:• Cysectomy +/- Neoadj Chemotherapy
• Trimodal Therapy:TURBT+Chemotherapy+Radiotherapy
INITIALPATIENTEVALUATION&COUNSELING
5.Priortotreatment,cliniciansshouldcounselpatientsregardingcomplicationsandtheimplicationsoftreatmentonqualityoflife(e.g.,impactoncontinence,sexualfunction,fertility,boweldysfunction,metabolicproblems).(ClinicalPrinciple)
• ComplicationimpactonQOLdiscussion• Both:sexualandurinary• Cystectomy:• Complication:60%Grade2-5Clavien complicationrate(RecentRCT)• ReadmissionRC:10-30%• DiversionrelatedQOL:continence,metabolic
• Trimodal Therapy• EarlyandlateGU/GItoxicity• Longtermfollow-upwithcystoscopy
Guidelines
• 35statementstotal:
• InitialPatientEvaluationandCounseling:#1-5• Treatment(Chemotherapy):#6-9• Treatment(RadicalCystectomy):#10-14• PerioperativeConsiderations:#15-18• Treatment(PelvicLymphadenopathy):#19-20• BladderPreservation:#21-29• Surveillance:#30-35
TREATMENT:CHEMOTHERAPY(NAC/AC)
6.Utilizingamultidisciplinaryapproach,cliniciansshouldoffercisplatin-basedneoadjuvant chemotherapytoeligibleradicalcystectomypatientspriortocystectomy.(StrongRecommendation;EvidenceLevel:GradeB)
InternationalCollaborationofTrialists 2011
• Neoadjuvant Cisplatinbasedchemoshouldbeoffered
TREATMENT:CHEMOTHERAPY(NAC/AC)
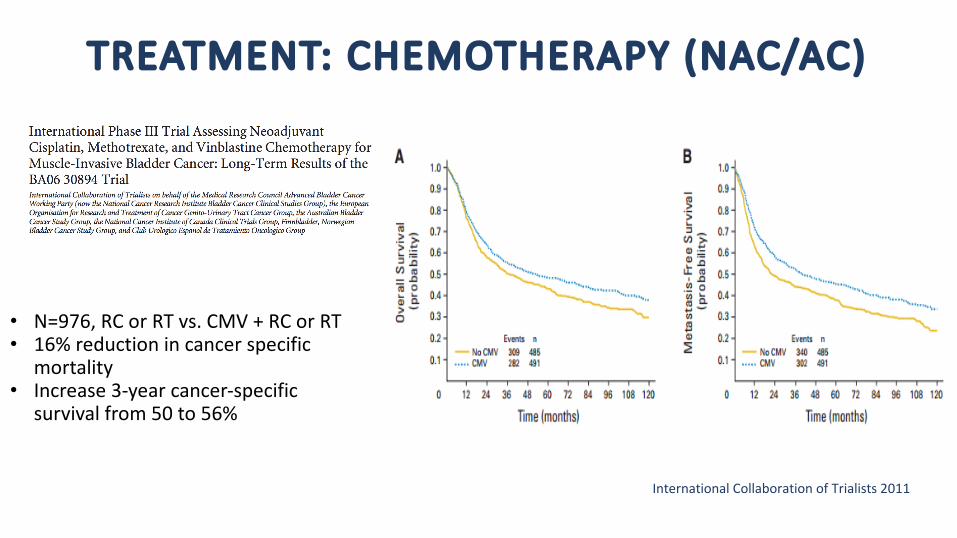
InternationalCollaborationofTrialists 2011
• N=976,RCorRTvs.CMV+RCorRT• 16%reductionincancerspecific
mortality• Increase3-yearcancer-specific
survivalfrom50to56%
TREATMENT:CHEMOTHERAPY(NAC/AC)
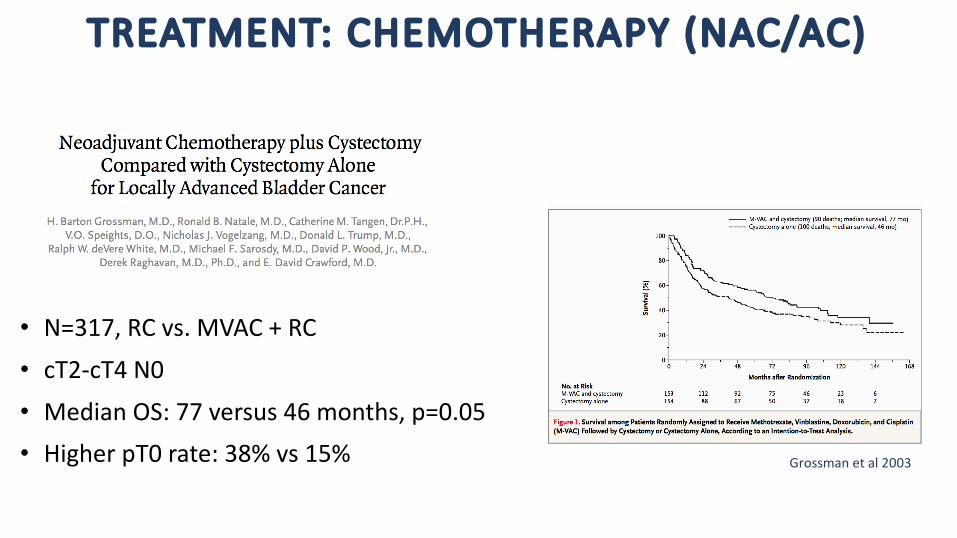
Grossmanetal2003
• N=317,RCvs.MVAC+RC
• cT2-cT4N0
• MedianOS:77versus46months,p=0.05• HigherpT0rate:38%vs15%
TREATMENT:CHEMOTHERAPY(NAC/AC)
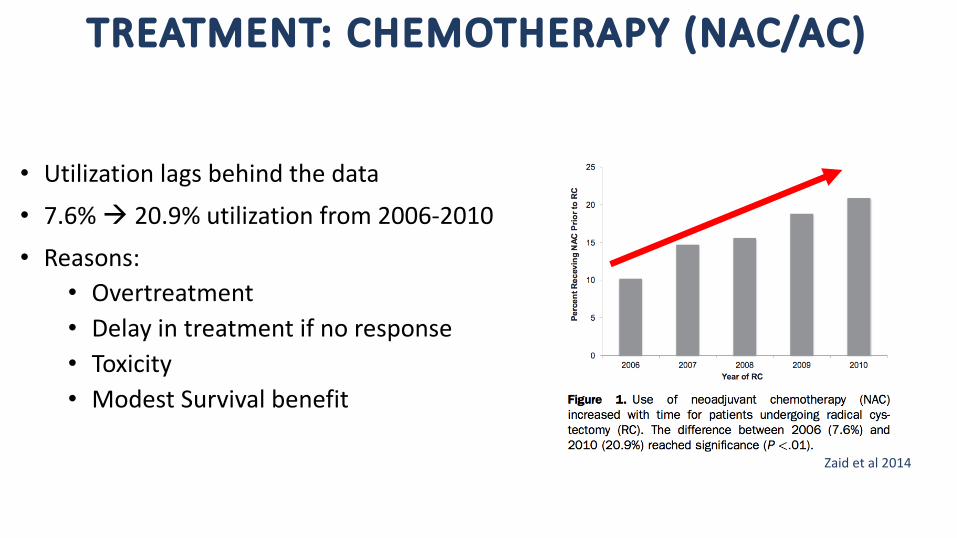
Zaidetal2014
• Utilizationlagsbehindthedata
• 7.6%à 20.9%utilizationfrom2006-2010
• Reasons:• Overtreatment• Delayintreatmentifnoresponse• Toxicity• ModestSurvivalbenefit
TREATMENT:CHEMOTHERAPY(NAC/AC)
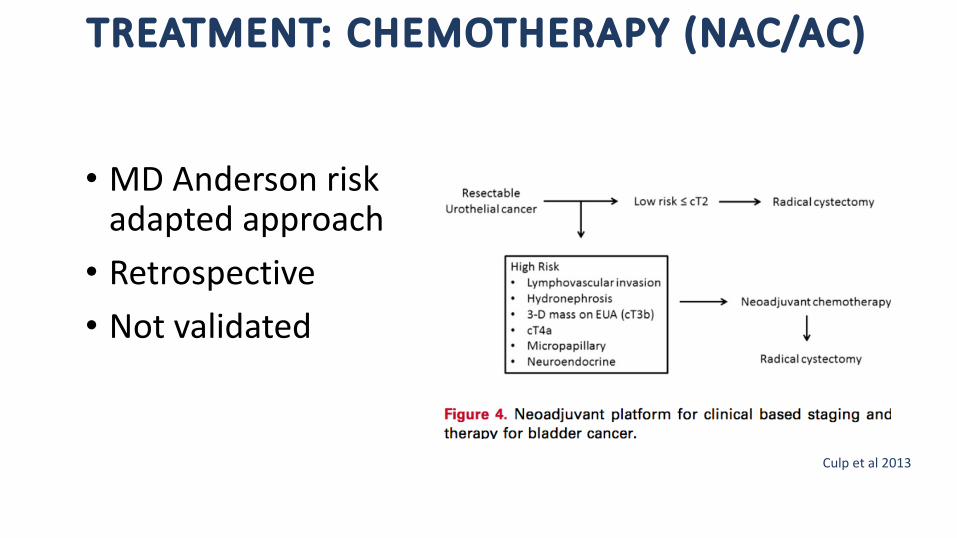
Culpetal2013
• MDAndersonriskadaptedapproach• Retrospective• Notvalidated
TREATMENT:CHEMOTHERAPY(NAC/AC)
• Therearenovalidatedpredictivefactorsorclinicalcharacteristics(includingage)associatedwithanincreasedordecreasedprobabilityofresponseandbenefit
• Thebestregimenanddurationforcisplatin-basedNACremainsundefined
• Thedecisionregardingeligibility forcisplatin-basedNACshouldbebasedoncomorbiditiesandperformancestatus,includingcardiacstatusandpresenceofperipheralneuropathy,hearingloss,andrenaldysfunction
TREATMENT:CHEMOTHERAPY(NAC/AC)
7.Cliniciansshouldnotprescribecarboplatin-basedneoadjuvantchemotherapyforclinicallyresectable stagecT2-T4aN0bladdercancer.Patientsineligibleforcisplatin-basedneoadjuvantchemotherapyshouldproceedtodefinitivelocoregional therapy.(ExpertOpinion)
• NoCarboplatin(patientswhoarecisplatinineligible)• Proceedtodefinitivetreatment
TREATMENT:CHEMOTHERAPY(NAC/AC)
8.Cliniciansshouldperformradicalcystectomyassoonaspossiblefollowingapatient’scompletionofandrecoveryfromneoadjuvantchemotherapy.(ExpertOpinion)
• TimelyCystectomyafterNeoadj chemo• ~4weeks(dependingonpatient’sfunctionalstatus,CBC)
TREATMENT:CHEMOTHERAPY(NAC/AC)
9.Eligiblepatientswhohavenotreceivedcisplatin-basedneoadjuvantchemotherapyandhavenon-organconfined(pT3/T4and/orN+)diseaseatcystectomyshouldbeofferedadjuvantcisplatin- basedchemotherapy.(ModerateRecommendation;EvidenceLevel:GradeC)
• AdjuvantCisplatinbasedchemoshouldbeoffered pT3/pT4/andorN+• Alladj chemotrialsunderpowered,terminatedearly• Meta-analyseshavedemonstratedpossiblebenefit(qualityofdatavariable)
Guidelines
• 35statementstotal:
• InitialPatientEvaluationandCounseling:#1-5• Treatment(Chemotherapy):#6-9• Treatment(RadicalCystectomy):#10-14• PerioperativeConsiderations:#15-18• Treatment(PelvicLymphadenopathy):#19-20• BladderPreservation:#21-29• Surveillance:#30-35
TREATMENT:RADICALCYSTECTOMY10.Cliniciansshouldofferradicalcystectomywithbilateralpelviclymphadenectomyforsurgicallyeligiblepatientswithresectable non-metastatic(M0)muscle-invasivebladdercancer.(StrongRecommendation;EvidenceLevel:GradeB)
• RC+BilateralPLNDshouldbeperformed11.Whenperformingastandardradicalcystectomy,cliniciansshouldremovethebladder,prostate,
andseminalvesiclesinmalesandshouldremovethebladder,uterus,fallopiantubes,ovaries,andanteriorvaginalwallinfemales.(ClinicalPrinciple)
• Removeadjacentorgansathighestriskofharboringdisease• Male:Prostate,SVs• Female:Uterus,fallopiantubes,ovaries,anteriorvaginalwall
TREATMENT:RADICALCYSTECTOMY
12. Cliniciansshoulddiscussandconsidersexualfunctionpreservingproceduresforpatientswithorgan-confineddiseaseandabsenceofbladderneck,urethra,andprostate(male)involvement.(ModerateRecommendation;EvidenceLevel:GradeC)
• Considersexualpreservation• Vaginalsparing,ovariansparing
• Periprostatic nervesparing
TREATMENT:RADICALCYSTECTOMY
13.Inpatientsundergoingradicalcystectomy,ileal conduit,continentcutaneous,andorthotopicneobladder urinarydiversionsshouldallbediscussed.(ClinicalPrinciple)
• ConsiderQOLwithdiversionchoice
TREATMENT:RADICALCYSTECTOMY
14.Inpatientsreceivinganorthotopic urinarydiversion,cliniciansmustverifyanegativeurethralmargin.(ClinicalPrinciple)
• Verifynegativeurethralmargin• Riskofcancerinretainedurethracanbebetween1%-17%• Reportedriskfactors:• tumormultifocality• papillarypattern• CIS/tumoratthebladderneck• prostaticurethralinvolvementandprostaticstromalinvasion**(shouldnotprecludeneobladderàfrozen section)
Guidelines
• 35statementstotal:
• InitialPatientEvaluationandCounseling:#1-5• Treatment(Chemotherapy):#6-9• Treatment(RadicalCystectomy):#10-14• PerioperativeConsiderations:#15-18• Treatment(PelvicLymphadenopathy):#19-20• BladderPreservation:#21-29• Surveillance:#30-35
Perioperative Management
15.Cliniciansshouldattempttooptimizepatientperformancestatusintheperioperativesetting.(ExpertOpinion)
• Optimizationofpatientperformancestatus• Nutritionalcounseling• Smokingcessation• PhysicalConditioning
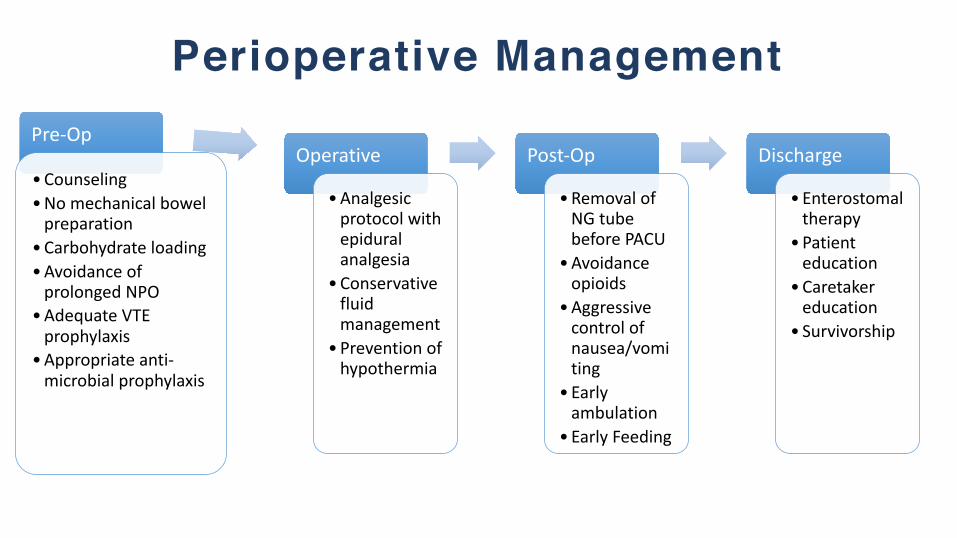
Perioperative ManagementPre-Op
•Counseling•Nomechanicalbowelpreparation
•Carbohydrateloading•Avoidance ofprolonged NPO
•AdequateVTEprophylaxis
•Appropriateanti-microbialprophylaxis
Operative
•Analgesicprotocolwithepiduralanalgesia
•Conservativefluidmanagement
•Preventionofhypothermia
Post-Op
•RemovalofNGtubebeforePACU
•Avoidanceopioids
•Aggressivecontrolofnausea/vomiting
• Earlyambulation
•EarlyFeeding
Discharge
•Enterostomaltherapy
•Patienteducation
•Caretakereducation
• Survivorship
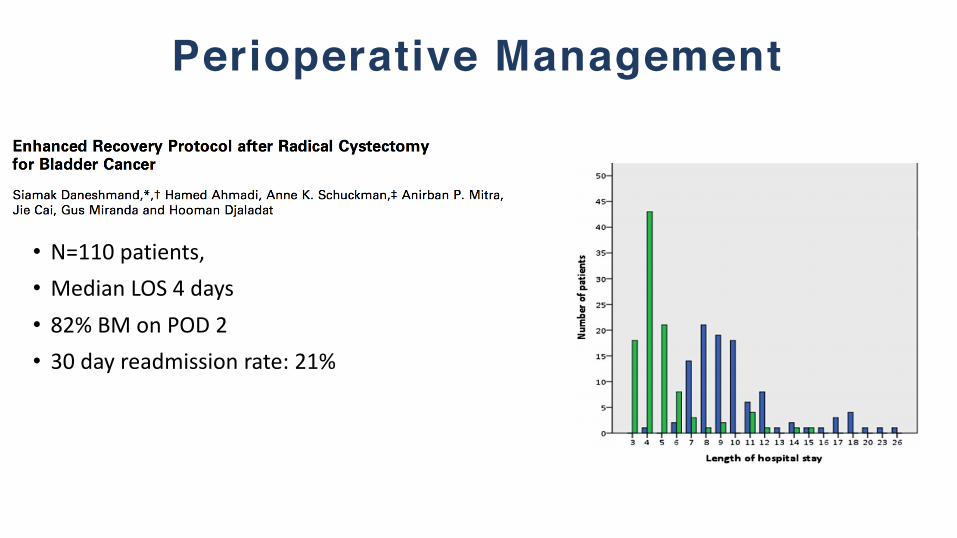
Perioperative Management
• N=110patients,• MedianLOS4days• 82%BMonPOD2• 30dayreadmissionrate:21%
PerioperativeManagement
16.Perioperativepharmacologicthromboembolicprophylaxisshouldbegiventopatientsundergoingradicalcystectomy.(StrongRecommendation;EvidenceLevel:GradeB)• VTEprophylaxis• OptimalPerioperativetiminganddurationstillundetermined• ConsiderextendedDVTproph for30dayspost-op(upto15%mayexperiencepost-opDVT)• >50%VTEoccurafterdischarge
PerioperativeManagement
17.Inpatientsundergoingradicalcystectomyµ-opioidantagonisttherapyshouldbeusedtoaccelerategastrointestinalrecovery,unlesscontraindicated.(StrongRecommendation;EvidenceLevel:GradeB)
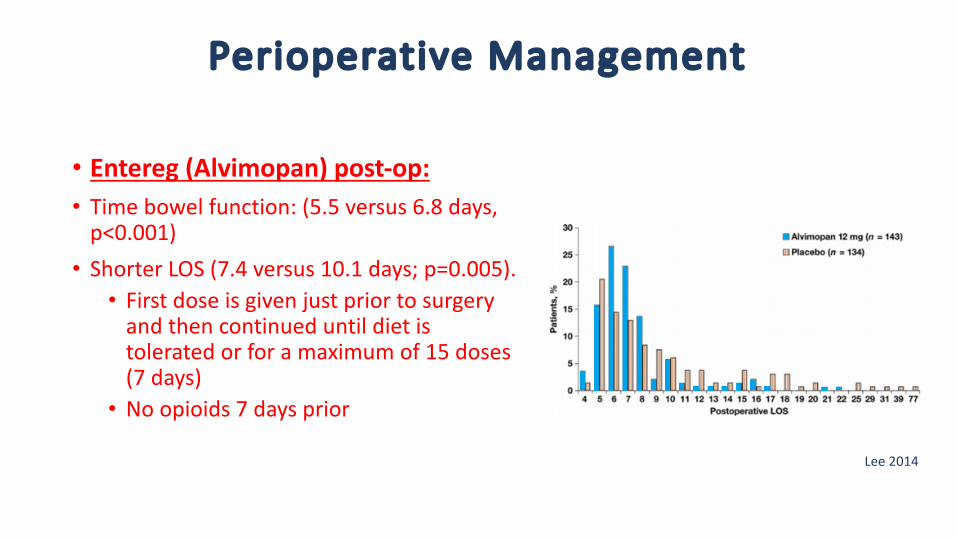
• Entereg (Alvimopan)post-op:
Lee2014
PerioperativeManagement
• Entereg (Alvimopan)post-op:• Timebowelfunction:(5.5versus6.8days,p<0.001)• ShorterLOS(7.4versus10.1days;p=0.005).• Firstdoseisgivenjustpriortosurgeryandthencontinueduntildietistoleratedorforamaximumof15doses(7days)
• Noopioids7daysprior
Lee2014
PerioperativeManagement
18.Patientsshouldreceivedetailedteachingregardingcareofurinarydiversionpriortodischargefromthehospital.(ClinicalPrinciple)
• UrinaryDiversionPatientEducationisParamount• Ostomyteaching
• Continentdiversionteaching
• Homehealthassistancepost-op
Guidelines
• 35statementstotal:
• InitialPatientEvaluationandCounseling:#1-5• Treatment(Chemotherapy):#6-9• Treatment(RadicalCystectomy):#10-14• PerioperativeConsiderations:#15-18• Treatment(PelvicLymphadenopathy):#19-20• BladderPreservation:#21-29• Surveillance:#30-35
Treatment:PelvicLymphadenectomy
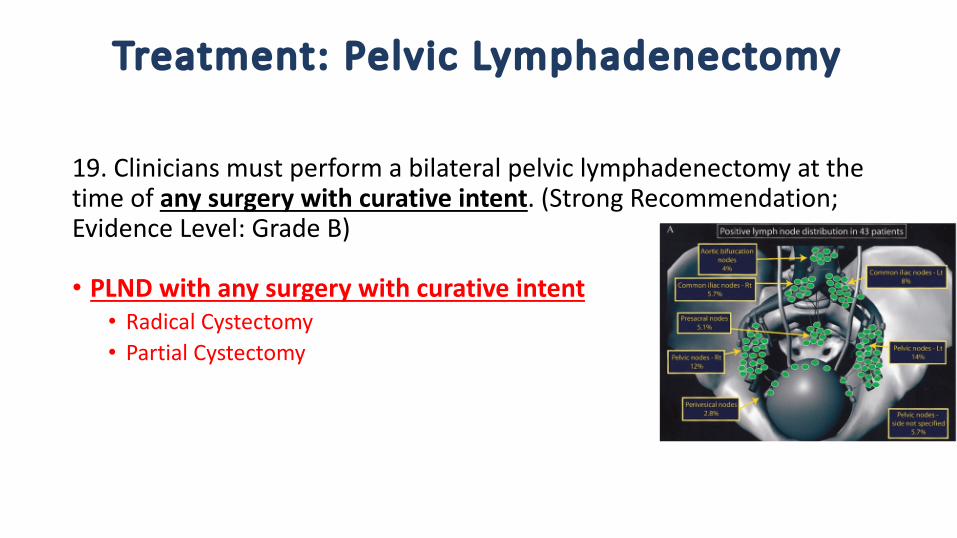
19.Cliniciansmustperformabilateralpelviclymphadenectomyatthetimeofanysurgerywithcurativeintent.(StrongRecommendation;EvidenceLevel:GradeB)
• PLNDwithanysurgerywithcurativeintent• RadicalCystectomy• PartialCystectomy
Treatment:PelvicLymphadenectomy
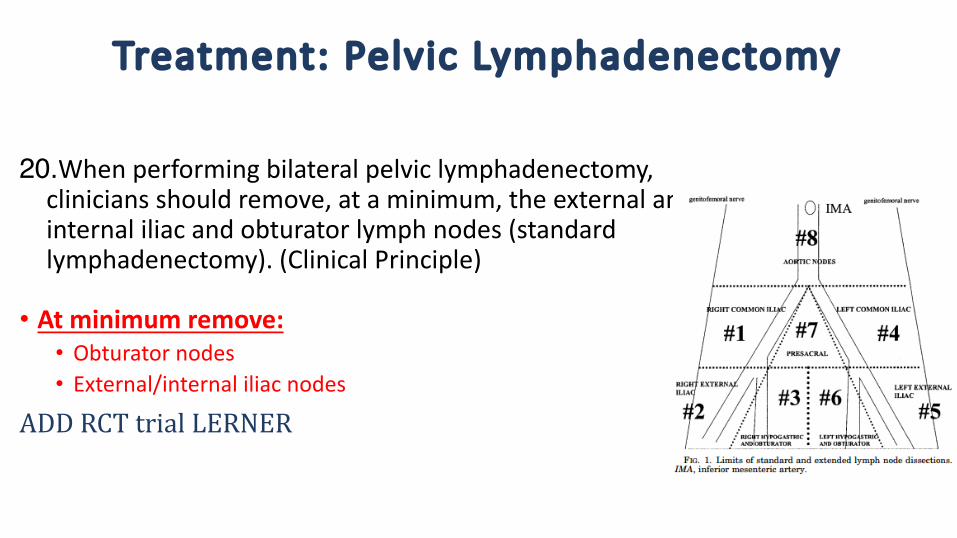
20.Whenperformingbilateralpelviclymphadenectomy,cliniciansshouldremove,ataminimum,theexternalandinternaliliacandobturatorlymphnodes(standardlymphadenectomy).(ClinicalPrinciple)
• Atminimumremove:• Obturatornodes• External/internaliliacnodes
ADDRCTtrialLERNER
Guidelines
• 35statementstotal:
• InitialPatientEvaluationandCounseling:#1-5• Treatment(Chemotherapy):#6-9• Treatment(RadicalCystectomy):#10-14• PerioperativeConsiderations:#15-18• Treatment(PelvicLymphadenopathy):#19-20• BladderPreservation:#21-29• Surveillance:#30-35
BLADDERPRESERVATION:PATIENTSELECTION
21.Forpatientswithnewlydiagnosednon-metastaticmuscle-invasivebladdercancerwhodesiretoretaintheirbladder,andforthosewithsignificantcomorbiditiesforwhomradicalcystectomyisnotatreatmentoption,cliniciansshouldofferbladderpreservingtherapywhenclinicallyappropriate.(Clinicalprinciple)
• Selection:unfitforcystectomyordesirebladderpreservation• Panelpreferredapproach:à TURBT,systemicchemotherapy,radiationtherapy,andongoingcystoscopytoevaluateresponse
BLADDERPRESERVATION:PATIENTSELECTION
22.Inpatientsunderconsiderationforbladderpreservingtherapy,maximaldebulking transurethralresectionofbladdertumorandassessmentofmultifocaldisease/carcinomainsitushouldbeperformed.(StrongRecommendation;EvidenceStrength:GradeC)
• TURBTconsiderationforbladderpreservationtherapy:• MaximalResection• AssessmentofMultifocaldisease• CISassessment• Tumorsize
BLADDERPRESERVATION:MAXIMALTURBTANDPARTIALCYSTECTOMY
23.Patientswithmuscle-invasivebladdercancerwhoaremedicallyfitandconsenttoradicalcystectomyshouldnotundergopartialcystectomyormaximaltransurethralresectionofbladdertumorasprimarycurativetherapy.(ModerateRecommendation;EvidenceLevel:GradeC)
• Theidealpatientsforpartialcystectomyhavea,nohydronephrosis,solitary,initialtumorwithoutconcomitantCISinthebladderorprostaticurethrathatisamenabletoresectionwitha2cmsurgicalmargin.
• Literaturereviewindicatesthatonly5%ofpatientswithinvasivebladdercancermeetthesecriteria
BLADDERPRESERVATION:PRIMARYRADIOTHERAPY
24.Forpatientswithmuscle-invasivebladdercancer,cliniciansshouldnotofferradiationtherapyaloneasacurativetreatment.(StrongRecommendation;EvidenceLevel:GradeC)
• Donotofferradiationtherapyalone:• Highratesofpelvicfailure• Fiveyearlocalcontrolratesof31-50%• Likelyanunderestimateasthosewhodevelopmetastaticdiseasearelesslikelytoundergocontinuedbladdersurveillance
MULTIMODALBLADDERPRESERVATIONTHERAPY
25.Forpatientswithmuscle-invasivebladdercancerwhohaveelectedmulti-modalbladderpreservingtherapy,cliniciansshouldoffermaximaltransurethralresectionofbladdertumor,chemotherapycombinedwithexternalbeamradiationtherapy,andplannedcystoscopic re-evaluation.(StrongRecommendation;EvidenceLevel:GradeB)
• MaximalTURBT+chemo+radiation• Chemoàsensitizes tumorcellstoradiationandcontrolofoccultmetastases
• ConsiderCystoscopic re-evaluationwithbiopsy(advocatedduringmiddleofRT)
MULTIMODALBLADDERPRESERVATIONTHERAPY
• MaximalTURBT+chemo+radiation
• Idealcandidate• 1)unifocal tumor<3cm• 2)nocarcinomainsitu(CIS),• 3)noevidenceofhydronephrosis,and• 4)atumorthatcanbecompletelytransurethrally resected
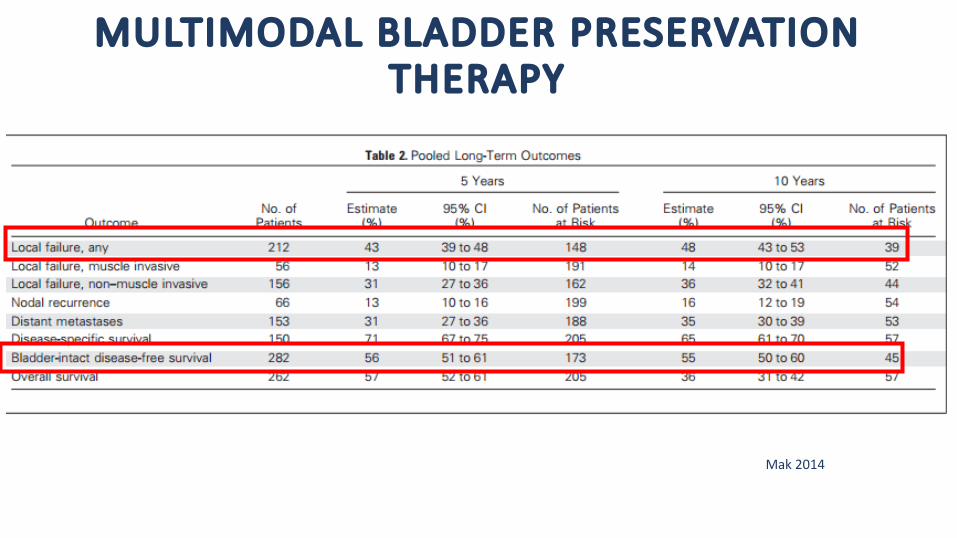
MULTIMODALBLADDERPRESERVATIONTHERAPY
Mak2014
MULTIMODALBLADDERPRESERVATIONTHERAPY
• Itisunclearwhatproportionofpatientswho,havinginitiallychosenbladderpreservation,ultimatelyrequirecystectomyinanon-studysetting.
• Thereportedbladderpreservationratesmaybedependentuponthedegreeofinitialpatientevaluationandselection
Mak2014
MULTIMODALBLADDERPRESERVATIONTHERAPY
26. Radiationsensitizingchemotherapyregimensshouldincludecisplatinor5-fluorouracilandmitomycin C.(StrongRecommendation;EvidenceLevel:GradeB)
• Radiationsenistizers:• 5FU+MMC• Cisplatin
MULTIMODALBLADDERPRESERVATIONTHERAPY
27.Followingcompletionofbladderpreservingtherapy,cliniciansshouldperformregularsurveillancewithCTscans,cystoscopy,andurinecytology.(StrongRecommendation;EvidenceLevel:GradeC)
• SurveillanceStrategy:• Publishedprotocolsrecommendevery3monthcystoscopyduringthefirstyear,every4-6monthsinthesecond,andevery6-12monthsthereafter.• Cross-sectionalimagingoftheabdomenandpelvisandchestimagingeverysixmonthsforthefirsttwoyears
MULTIMODALBLADDERPRESERVATIONTHERAPY
28.Inpatientswhoaremedicallyfitandhaveresidualorrecurrentmuscle-invasivediseasefollowingbladderpreservingtherapy,cliniciansshouldofferradicalcystectomywithbilateralpelviclymphadenectomy.(StrongRecommendation;EvidenceLevel:GradeC)
• Ifmultimodaltherapyfailsà Radicalcystectomy:• Upto30%ofpatientswillhaveaninvasiverecurrence
MULTIMODALBLADDERPRESERVATIONTHERAPY
29.Inpatientswhohaveanon-muscleinvasiverecurrenceafterbladderpreservingtherapy,cliniciansmayoffereitherlocalmeasures,suchastransurethralresectionofbladdertumorwithintravesical therapy,orradicalcystectomywithbilateralpelviclymphadenectomy.(ModerateRecommendation;EvidenceLevel:GradeC)
• Non-muscleinvasiverecurrenceà TURBT,intravesical therapy,orRC:• CaseseriesshowthatNMIBCrecurrencesfollowingbladdersparingtherapymaystillbemanagedbystandardlocalmeasuressimilartodenovo NMIBC
Guidelines
• 35statementstotal:
• InitialPatientEvaluationandCounseling:#1-5• Treatment(Chemotherapy):#6-9• Treatment(RadicalCystectomy):#10-14• PerioperativeConsiderations:#15-18• Treatment(PelvicLymphadenopathy):#19-20• BladderPreservation:#21-29• Surveillance:#30-35
PATIENTSURVEILLANCE
30.CliniciansshouldobtainchestimagingandcrosssectionalimagingoftheabdomenandpelviswithCTorMRIat6-12monthintervalsfor2-3yearsandthenmaycontinueannually.(ExpertOpinion)
• Radiographicevaluationoftheabdomenandpelvis:• Detectionofuppertractcancer• Diseasedetectioninthemostcommonsitesofrecurrence,progression,andmetastasis
• Urinarydiversionconcerns
PATIENTSURVEILLANCE
31.Followingtherapyformuscle-invasivebladdercancer,patientsshouldundergolaboratoryassessmentatthreetosixmonthintervalsfortwotothreeyearsandthenannuallythereafter.(ExpertOpinion)
• Labevaluation:Electrolyteimbalances,B12deficiency,acidosis
31.Followingradicalcystectomyinpatientswitharetainedurethra,cliniciansshouldmonitortheurethralremnantforrecurrence.(ExpertOpinion)
• Monitorurethraforrecurrence:• 4-14%riskofrecurrenceinurethra• UrethralCytologycanbelowyield(nospecificrecommendation)• Considerinhigherriskpatients(painorurethralbleedingattimeofdx)
PATIENTSURVEILLANCE33.Cliniciansshoulddiscusswithpatientshowtheyarecopingwiththeirbladdercancerdiagnosisandtreatmentandshouldrecommendthatpatientsconsiderparticipatinginacancersupportgrouporconsiderreceivingindividualcounseling.(ExpertOpinion)
34.Cliniciansshouldencouragebladdercancerpatientstoadopthealthylifestylehabits,includingsmokingcessation,exercise,andahealthydiet,toimprovelong-termhealthandqualityoflife.(ExpertOpinion)• Survivorship:
bcan.orgcancersupportcommunity.orgcancercare.org
bladdercancersupport.orgcancer.orgurologyhealth.org
PATIENTSURVEILLANCE
35.Inpatientsdiagnosedwithvarianthistology,cliniciansshouldconsideruniqueclinicalcharacteristicsthatmayrequiredivergencefromstandardevaluationandmanagementforurothelial carcinoma.(ExpertOpinion)
• Modifystandardevaluationforvarianthistology:
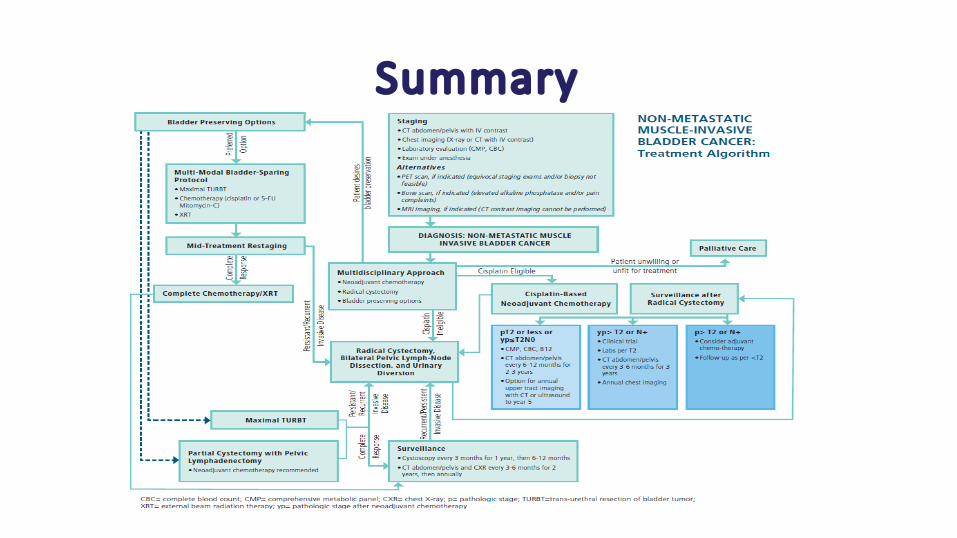
Summary







![Cancer Care Ontario Bladder Cancer Guideline: An ... · (AUA) “Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ ASCO/ ASTRO/ SUO Guideline” [1]. TARGET POPULATION](https://img.pdfslide.us/doc/110x75/5f02dfc67e708231d406703f/cancer-care-ontario-bladder-cancer-guideline-an-aua-aoetreatment-of-non-metastatic.jpg)







![Muscle-invasive and Metastatic Bladder Cancer · muscle-invasive bladder cancer (Ta,T1 and carcinoma in situ) [2], and primary urethral carcinomas [3]. 1.2 Panel Composition The EAU](https://img.pdfslide.us/doc/110x75/5e558374ee435e2e4f1b6d29/muscle-invasive-and-metastatic-bladder-cancer-muscle-invasive-bladder-cancer-tat1.jpg)






![Muscle invasive bladder Cancer [Dr.Edmond Wong]](https://img.pdfslide.us/doc/110x75/554af03bb4c90559058b477d/muscle-invasive-bladder-cancer-dredmond-wong.jpg)



