Embed Size (px)
Citation preview

Rheumatol Int (2012) 32:1069–1074
DOI 10.1007/s00296-011-1803-4SHORT COMMUNICATION
Atypical presentation of scleroderma in infancy
Navin Mishra · Devendra Shrestha · Rakesh Babu Poudyal · KC Shiva Raj
Received: 18 July 2010 / Accepted: 16 January 2011 / Published online: 16 February 2011© Springer-Verlag 2011
Abstract We present a case of a female child who haddeveloped progressive skin tightening of whole body,sclerodactyly, and severe contracture of all joints withrestricted opening of mouth with disease onset at 6 weeksof life. The child also had anemia, failure to thrive, recur-rent diarrhea, and ascites. Skin biopsy revealed characteris-tic histopathological features suggestive of scleroderma.Echocardiography revealed thrombus in the right atriumextending to inferior vena cava. Serological markers (anti-nuclear antibody, antiscl 70, anti-double-stranded DNA,anticentromere antibody) were negative. To our knowl-edge, this case of scleroderma with disease onset at 6 weeksof life could possibly be among youngest cases reported inthe literature. Also, thrombosis in inferior vena cava in achild with scleroderma is being reported for the Wrst time.
Keywords Scleroderma · Infancy · Progeria
Introduction
Juvenile systemic sclerosis (JSSc) is a chronic multi-sys-temic connective tissue disease characterized by symmetri-cal thickening and hardening of the skin, associated withWbrous changes in internal organs. Although rare in chil-dren, it represents one of the most severe rheumatic condi-tions in pediatric rheumatology practice [1]. The onset ofjuvenile systemic sclerosis in childhood is very uncommon;children under 16 years of age account for less than 5% ofall cases [2]. Recently with the joint eVort of Pediatric
Rheumatology European Society (PRES), the AmericanCollege of Rheumatology (ACR), and the European LeagueAgainst Rheumatism (EULAR), a new classiWcation crite-rion was developed to standardize the conduct of clinical,epidemiological, and outcome research for this rare pediat-ric disease [3]. Despite these valuable contributions diagno-sis of juvenile systemic sclerosis especially in infancyremains diYcult in the early stage of disease. Here, wereport the case of a child with scleroderma onset at 6 weeksof life, which was associated with inferior vena cava andright atrial thrombus.
Case report
Ten-month-old-female child presented with complaints ofprogressive skin tightening of whole body since the age of6 weeks. It started initially with mild edematous swellingover dorsum of right hand, followed by skin tightening andXexion contracture of Wngers progressing to whole body in2 months including face, trunk, and lower limbs. Skinbecame shiny, thick with Xexion contracture of bilateraltoes as well as ankle. All joint movements were restricteddue to tightening of skin, and child appeared stiV. Also,child had shiny stretched skin over face with restrictedopening of oral stoma and restricted neck movement due totight skin. Child had recurrent diarrhea since 6 months oflife managed with oral antibiotics and oral rehydration saltsolution. Child had increasing frequency of nasal regurgita-tion and occasionally vomiting mostly just after feeding forlast 3 months. The child had delay in motor developmentdue to restriction of joint movement. Social and cognitivedevelopment remained normal for age. The child was bornat term to a nonconsanguineous marriage by emergencycaesarean section for pregnancy-induced hypertension
N. Mishra (&) · D. Shrestha · R. B. Poudyal · KC Shiva RajKIST Medical College, Lalitpur, Nepale-mail: [email protected]
123

1070 Rheumatol Int (2012) 32:1069–1074
(PIH) with intrauterine growth retardation with fetal dis-tress with birth weight of 2,300 gm. Mother was diagnosedto have PIH at 28-week gestation and was controlled onNifedipine. There is no known exposure of mother to otherdrugs, toxin, and blood products during pregnancy. Therewas no family history of autoimmune disease or similar ill-ness. Child had several visits to other medical centersbefore presenting to KIST Medical College Teaching Hos-pital at 10 months of life. The parents Wrst sought medicaladvice at age of 45 days for progressive tightening of skinover Wngers associated with contracture which was diag-nosed as dactylitis and was treated with intravenous antibi-otics (Ceftriaxone, Cloxacillin, and Amikacin) for 10 days.On examination, child had failure to thrive (weight 5.5 kgand length 65.5 cm) and small head (occipitofrontalcircumference = 40 cm, <2 SD), shiny stretched skin withthin hair, and mild alopecia at fronto-parietal region withsmall oral stoma, puckered lips, thin eye lash, large anterior
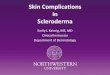
fontanel with prominent groove in frontal bone, nonpittingedematous swelling of both upper and lower limbs mainlyon dorsal surface, Xexion contracture of Wngers with sclero-dactyly and extensor contracture of toe and feet withrestriction of joint movements (Fig. 1). She also had fewsmall areas of hyperpigmentation over knuckles, atrophiedand hyperpigmented skin over back of the neck and postau-ricular region, hemorrhoids, and pressure sore over sacralarea. There were no nail fold capillary dilatation anddestruction noted by nail fold capillaroscopy. Hemody-namic parameters including blood pressure were normal forage. Abdominal examination revealed mild hepatomegalywith minimal ascites. Other systemic examination was clin-ically within normal limits. Initial work up showed mildanemia (Hemoglobin = 8.9 gm/dl) with normal leukocytecount and with ESR of 25 mm/h. Serum electrolytes(sodium, potassium, calcium, phosphate), alkaline phos-phatase, renal function test, muscle enzymes (CPK, LDH),
Fig. 1 a Shiny stretched skin over face with thin hair and mild alopecia at fronto-parietal region with small oral stoma, puckered lips, thin eye lash, large anterior fontanel with prominent groove in frontal bone. b Child has fail-ure to thrive, shiny stretched skin, Wxed Xexion contractures in upper and lower limb and neck. Abdominal distension can be noted. c Atrophied and hyper-pigmented skin over back of the neck and postauricular and pre-auricular region (salt and pepper appearance) d Flexion contrac-ture of Wngers and sclerodactyly. e Hemorrhoids seen prolapsed through anal opening
123

Rheumatol Int (2012) 32:1069–1074 1071
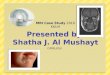
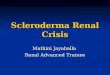
and blood sugar were within normal limits. Also antinu-clear antibody, antiscl 70, anti-double-stranded DNA, anti-centromere antibody, rheumatoid factor, and VDRL werenegative. Liver function test revealed mildly elevated liverenzyme (Total bilirubin = 1.1 mg/dl conjugated bilirubin =0.3 mg/dl, SGPT = 120 IU/l, SGOT = 96 IU/l). Ascitic taprevealed transudative type ascitic Xuid. Skin biopsyrevealed collagen bundles in dermis with sparse append-ages surrounded by sclerotic collagen along with replace-ment of subcutaneous fat by collagen suggestive ofscleroderma (Fig. 2). Muscle biopsy Wndings remainednormal. Chest X-ray showed mild haziness and some cysticspaces in bilateral middle and lower zone. Similarly,abdominal X-ray showed dilated stomach and bowel loops(Fig. 3). Though HRCT chest was planned, it could not bedone due to Wnancial constraint. Skeletal survey revealedmild generalized osteopenia. Electrocardiogram was foundnormal. However, echocardiography showed thrombus inright atrium and inferior vena cava with normal pulmonaryarterial pressure (Fig. 4). Initial ultrasonography of abdo-
men showed minimal ascites. Doppler imaging of carotidwas normal. Lipid proWle (cholesterol = 186 mg/dl, HDL =32 mg/dl, LDL = 129 mg/dl, Triglyceride = 129 mg/dl) waswithin normal limit. Coagulogram (PT = 15 s, APTT = 29 s,INR = 1) was within normal limit, and D-dimer was nega-tive. Child was also detected to have urinary tract infection(Klebsiella pneumoniae) which was treated with intrave-nous Amikacin and was put on UTI prophylaxis. Hemor-rhoids were treated conservatively, and speciWc surgicalmanagement was planned for later date. Initially, lowmolecular weight heparin was started for thrombolysis andcontinued for 3 weeks, but in follow-up, it was noted thatchild had grossly increased ascites with no signiWcantchange in size of thrombus at successive echocardiography.After conWrming the diagnosis of diVuse scleroderma, childwas started on oral Prednisolone 2 mg/kg, and at follow-upafter 2 week, no signiWcant skin changes were noted. Par-ents were counseled for the starting treatment with subcuta-neous Methotrexate and need of further prothombotic workup and CT scan Chest. But they lost to follow-up after12 months of age. On inquiring parents after 2 months oftheir last visit, it was informed that child expired just fewdays prior at the age of 14 months at home. The death was
Fig. 2 a Skin showing proliferation of Wbrocollagenous tissue withsparse skin adnexae (5£). b Entrapment of adipose tissue with prolif-eration of Wbrocollagenous tissue in the subcutis (10£)
Fig. 3 X-ray showing haziness in bilateral lung Weld and dilated stom-ach
123

1072 Rheumatol Int (2012) 32:1069–1074
preceded by profused diarrhea and poor feeding for whichno further specialized medical care was taken except for thepalliative home treatment with oral rehydration. The secondfemale child was born to the parent of index case who is inour follow-up and until the last follow-up visit at age of9 months, has remained asymptomatic.
Discussion
DiVuse scleroderma in infancy—the manifestation of vari-ous systemic diseases has been reported in very less num-bers [4–6]. Hence, it is liable to be misdiagnosed in earlierstage as in this case.
In this child, the dermal changes were obvious and hadevolved starting aurally and gradually involving face, arms,neck, trunk and had passed through all three classicalphases of dermal changes (edematous phase, indurativephase and atrophic phase) in scleroderma [7]. The general-ized sclerosis of skin with puckered lips, edematous limbs,small oral stoma, areas of hyperpigmentation, atrophied
skin, and hair loss which were seen in this child are the typ-ical skin lesions found in systemic sclerosis. Also, the childhad gastro-esophageal reXux, recurrent diarrhea, dilatedstomach, dilated bowel loops, failure to thrive, and hemor-rhoids, which are common gastrointestinal manifestation ofscleroderma [8–10]. The chest X-ray showed bilateral hazi-ness, which could be feature of lung Wbrosis. Besides these,the child had progressive right heart failure secondary tothrombus in inferior vena cava and right atrium. Thus, thechild had generalized scleroderma, typical facial features,sclerodactyly, gastrointestinal manifestation, right heartfailure, and radiological features supportive of lung Wbro-sis, fulWlling the ClassiWcation Criteria for Juvenile sys-temic sclerosis developed in 2007 [3]. It has been foundthat during the overall course of the systemic sclerosis,Raynaud phenomenon and skin induration are far the mostfrequent symptoms (84%), followed by involvement of therespiratory (42%) and gastrointestinal (GI) systems (30%),arthritis (27%), and cardiac involvement (15%) [1]. How-ever, this child did not show obvious Raynaud phenome-non. The tests for various autoantibodies performed in thiscase were negative. However, diVerent studies haveshowed varying results on positivity of these autoantibodiesin scleroderma. Antinuclear antibody has been detected invaried number of cases of scleroderma with an incidence aslow as 23% to as high as 95% [11–14]. Similarly, antitopo-isomerase I autoantibodies were present in 28–34% ofpatients with juvenile systemic sclerosis, while the prevalenceof anticentromere antibodies was only 7–8% [2, 15, 16].
Besides the very early age of manifestation of the dis-ease, the child also had uncommon association of diVusescleroderma with thrombus in right atrium and inferiorvena cava. Very few cases of thrombotic events in childrenwith scleroderma are reported, but no reports of such eventsare published in infants [17, 18]. Axillary vein thrombosiswas reported in 1990 by Leak et al. in a 14-year-old girlwith scleroderma with prolonged euglobulin clot lysis time,antiendothelial cell antibodies, and raised von Willebrandfactor antigen [17]. The thrombotic event in systemicscleroderma may be attributed to antiendothelial cell anti-body, which is detected in 22–85% of patients [19–21].Also, prevalence of anticardiolipin antibodies (aCL) andantibeta2-glycoprotein-I antibodies of 0–40% has beenreported in systemic scleroderma [22–27]. In our patient,due to Wnancial constraints we were not able to performprothrombotic work up, hence it cannot be said whetherthrombosis was because of primary disease-related processor due to an associated prothrombotic disorder.
The diVerential diagnosis would be Hutchinson–GilfordProgeria, which is a rare genetic disorder resulting frommutations in the LMNA gene [28]. Infants with sclero-derma should be followed closely for the development ofprogeria [5, 29]. However, our child lacked other clinical
Fig. 4 Echocardiography shows thrombus can in right atrium andinferior vena cava
123

Rheumatol Int (2012) 32:1069–1074 1073
features of progeria till her demise. Also, stiV skin syn-drome is a hereditary scleroderma-like disease that involvesareas with abundant fascia such as thighs and buttockscausing symmetrical joint contractures and motion limita-tion of knees and hips. However, there is sparing of facewith characteristic histological Wnding of thick fascia instiV skin syndrome [30, 31].
Conclusion
Scleroderma in infants is an uncommon entity and is liableto be misdiagnosed as in our case. Early diagnosis of thedisease is important for timely medical intervention of thisfatal disease.
References
1. Zulian F (2008) Systemic Sclerosis and Localized Scleroderma inChildhood. Rheum Dis Clin North Am 34(1):239–255
2. Scalapino K, Arkachaisri T, Lucas M, Fertig N, Helfrich DJ, Lon-dino AV Jr, Steen VD, Medsger TA Jr (2006) Childhood onsetsystemic sclerosis: classiWcation, clinical and serologic features,and survival in comparison with adult onset disease. J Rheumatol33(5):1004–1013
3. Zulian F, Woo P, Athreya BH, Laxer RM, Medsger TA Jr, LehmanTJ, Cerinic MM, Martini G, Ravelli A, Russo R, Cuttica R, de Oli-veira SK, Denton CP, Cozzi F, Foeldvari I, Ruperto N (2007) ThePediatric Rheumatology European Society/American College ofRheumatology/European League against Rheumatism provisionalclassiWcation criteria for juvenile systemic sclerosis. ArthritisRheum 57(2):203–212
4. Sato S, Ishida W, Takehara K (2003) A case of juvenile systemicsclerosis with disease onset at six months old. Clin Rheumatol22(2):162–163
5. Jansen T, Romiti R (2000) Progeria infantum (Hutchinson-Gilfordsyndrome) associated with scleroderma-like lesions and acro-osteolysis: a case report and brief review of the literature. PediatrDermatol 17(4):282–285
6. Sevenants L, Wouters C, De Sandre-Giovannoli A, Devlieger H,Devriendt K, van den Oord JJ, Marien K, Lévy N, Morren MA(2005) Tight skin and limited joint movements as early presenta-tion of Hutchinson-Gilford progeria in a 7-week-old infant. EurJ Pediatr 164(5):283–286
7. Silver RM (1991) Clinical aspects of systemic sclerosis (sclero-derma). Ann Rheum Dis 50:846–853
8. Cohen S (1980) The gastrointestinal manifestations of sclero-derma: pathogenesis and management (clinical conference).Gastroenterology 79:155–166
9. Cobden I, Axon AT, Ghoneim AT, McGoldrick J, Rowell NR(1980) Small intestinal bacterial growth in systemic sclerosis. ClinExp Dermatol 5:37–42
10. Young MA, Rose S, Reynolds JC (1996) Gastrointestinal manifes-tation of scleroderma. Rheum Dis Clin North Am 22:797–823
11. Morel Z, Benadón E, Faugier E, Maldonado MR (2009) Clinicalcharacteristics of children with scleroderma in a referral hospital.Reumatol Clin 5(3):158–162
12. Fennell RHJ, Rodnan GP, Vazquez JJ (1962) Variability of tissue-localizing properties of serum from patients with diVerent diseasestates. Lab Invest 11:24–31
13. Beck JS, Anderson JR, Gray KG, Rowell NR (1963) Antinuclearand precipitating autoantibodies in progressive systemic sclerosis.Lancet 2(7319):1188–1190
14. Solomon DH, Kavanaugh AJ, Schur PH (2002) The AmericanCollege of Rheumatology Ad Hoc Committee on ImmunologicTesting Guidelines. Evidence-based guidelines for the use ofimmunologic tests: antinuclear antibody testing. Arthritis Rheum47(4):434–444
15. Martini G, Foeldvari I, Russo R, Cuttica R, Eberhard A, Ravelli A,Lehman TJ, de Oliveira SK, Susic G, Lyskina G, Nemcova D,Sundel R, Falcini F, Girschick H, Lotito AP, Buoncompagni A,Sztajnbok F, Al-Mayouf SM, Orbàn I, Ferri C, Athreya BH, WooP, Zulian F (2006) Systemic sclerosis in childhood: clinical andimmunologic features of 153 patients in an international database.Arthritis Rheum 54(12):3971–3978
16. Della Rossa A, Valentini G, Bombardieri S, Bencivelli W, SilmanAJ, D’Angelo S, Cerinic MM, Belch JF, Black CM, Becvar R,Bruhlman P, Cozzi F, Czirják L, Drosos AA, Dziankowska B,Ferri C, Gabrielli A, Giacomelli R, Hayem G, Inanc M, McHughNJ, Nielsen H, Scorza R, Tirri E, van den Hoogen FH, Vlachoy-iannopoulos PG (2001) European multicentre study to deWnedisease activity criteria for systemic sclerosis. I. Clinical and epi-demiological features of 290 patients from 19 centres. Ann RheumDis 60:585–591
17. Leak A, Patel KJ, Tuddenham EG, Pearson JD, Woo P (1990)Axillary vein thrombosis in adolescent onset systemic sclerosis.Ann Rheum Dis 49(7):557–559
18. Bonam SR (2006) Isolated renal thrombotic microangiopathy asan initial presentation of scleroderma without other systemic man-ifestations of the disease. Available on URL:http://www.kidney.org/news/meetings/clinical/pdf/2006SCM-AbstractsTopicList.pdf.Accessed 28 June 2010
19. Hebbar M, Lassalle P, Delneste Y, Hatron PY, Devulder B, TonnelAB, Janin A (1997) Assessment of anti-endothelial cell antibodiesin systemic sclerosis and Sjogren’s syndrome. Ann Rheum Dis56:230–234
20. Ihn H, Sato S, Fujimoto M, Igarashi A, Yazawa N, Kubo M,Kikuchi K, Takehara K, Tamaki K (2000) Characterization of auto-antibodies to endothelial cells in systemic sclerosis (SSc): associa-tion with pulmonary Wbrosis. Clin Exp Immunol 119:203–209
21. Renaudineau Y, Revelen R, Levy Y, Salojin K, Gilburg B,Shoenfeld Y, Youinou P (1999) Anti-endothelial cell antibodies insystemic sclerosis. Clin Diagn Lab Immunol 6(2):156–160
22. Assous N, Allanore Y, Batteux F, Meune C, Toulon P, Weill B,Kahan A (2005) Prevalence of antiphospholipid antibodies in sys-temic sclerosis and association with primitive pulmonary arterialhypertension and endothelial injury. Clin Exp Rheumatol23(2):199–204
23. Pope JE, Thompson A (2000) The frequency and signiWcance ofanticardiolipin antibodies in scleroderma. J Rheumatol 27:1450–1452
24. Merkel PA, Chang Y, Pierangeli SS, Convery K, Harris EN,Polisson RP (1996) The prevalence and clinical associations ofanticardiolipin antibodies in a large inception cohort of patientswith connective tissue diseases. Am J Med 101(6):576–583
25. Ihn H, Sato S, Fujimoto M, Kikuchi K, Igarashi A, Soma Y,Tamaki K, Takehara K (1996) Measurement of anticardiolipinantibodies by ELISA using beta 2-glycoprotein I (beta 2-GPI) insystemic sclerosis. Clin Exp Immunol 105(3):475–479
26. Herrick AL, Heaney M, Hollis S, Jayson MI (1994) Anticardio-lipin, anticentromere and anti-Scl-70 antibodies in patients withsystemic sclerosis and severe digital ischaemia. Ann Rheum Dis53:540–542
27. Lima J, Fonollosa V, Fernández-Cortijo J, Ordi J, Cuenca R,Khamashta MA, Vilardell M, Simeón CP, Picó M (1991) Plateletactivation, endothelial cell dysfunction in the absence of
123

1074 Rheumatol Int (2012) 32:1069–1074
anticardiolipin antibodies in systemic sclerosis. J Rheumatol18(12):1833–1836
28. Madej-Pilarczyk A, Rosiska-Borkowska D, Rkawek J, MarchelM, Szalus E, Jablonska S, Hausmanowa-Petrusewicz I (2009)Progeroid syndrome with scleroderma-like skin changes associ-ated with homozygous R435C LMNA mutation. Am J Genet149(11):2387–2392
29. Hennekam RC (2006) Hutchinson-Gilford progeria syndrome:review of the phenotype. Am J Med Genet A 140(23):2603–2624
30. Esterly NB, McKusick VA (1971) StiV skin syndrome. Pediatrics47:360–369
31. Jablonska S, Blaszczyk M (2004) StiV skin syndrome is highlyheterogeneous, and congenital fascial dystrophy is its distinct sub-set. Pediatr Dermatol 21:508–510
123