Embed Size (px)
Citation preview
Atypical pain with positive CTA
and normal myocardial perfusion
F. Mut, M. Kapitan, A. Beltran
Nuclear Medicine Service, Italian Hospital
& CUDIM
Montevideo, Uruguay
• Woman 51 y.o.
• Heavy family history of CAD, no other known risk factors.
• Episodes of atypical chest discomfort.
• Positive exercise test.
• Submitted for CT angiography (CTA), reported as:
Severe proximal LAD stenosis.
No other lesions.
Ca score >1000.
Clinical history
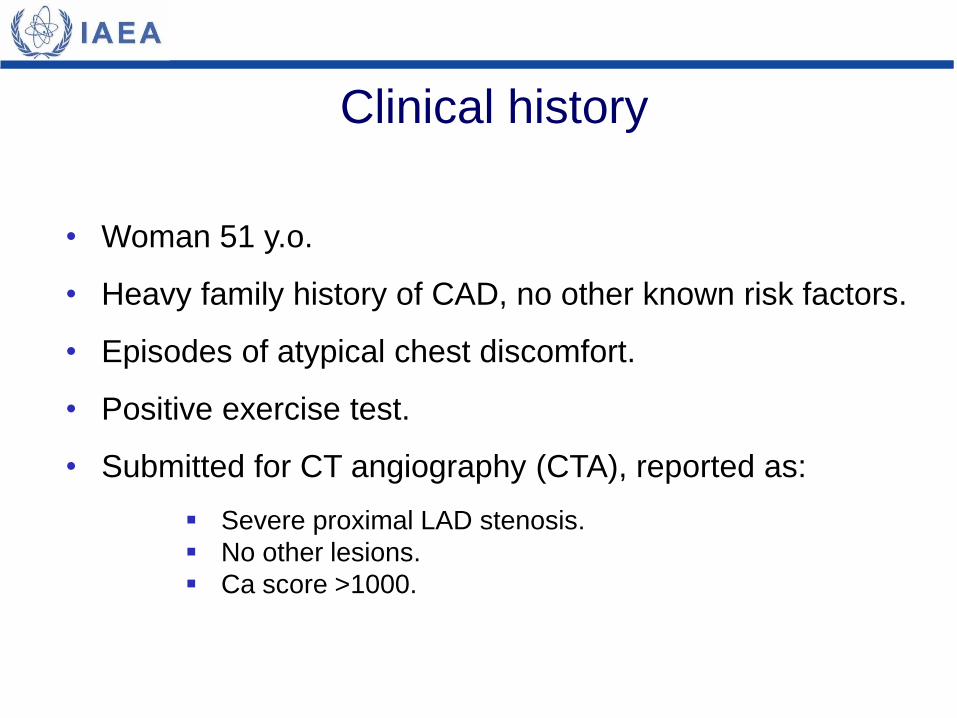
64-slice CT angiography
Cx
3D rendering
LAD lesion (arrow)
• Since Ca score was high, a myocardial perfusion study
was indicated using 99mTc-MIBI with exercise test.
• Patient achieved 101% of maximum predicted heart rate.
• She remained asymptomatic.
• There was a 1 mm ST segment depression.
(see following slide for stress ECG)
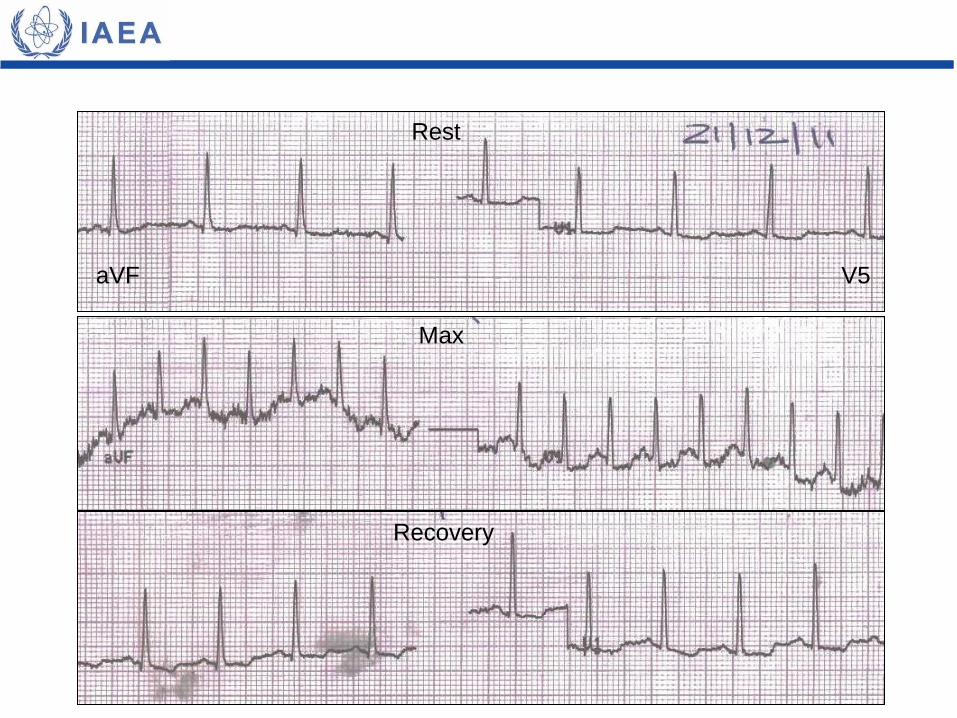
aVF V5
Rest
Recovery
Max
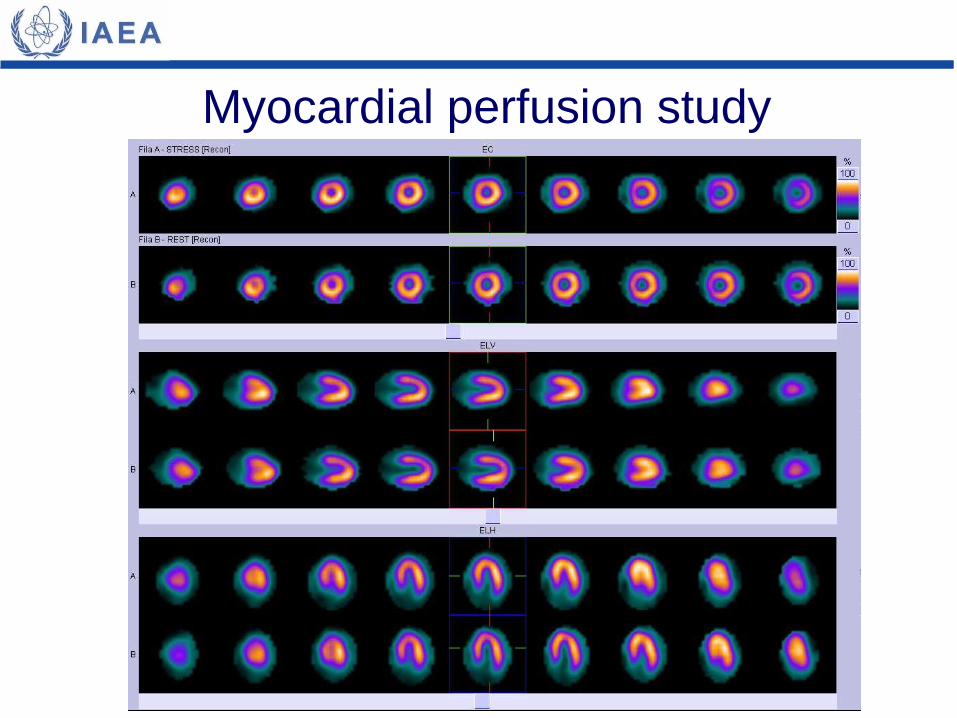
Myocardial perfusion study
The perfusion result is consistent with:
a) Small inferior myocardial infarction.
b) Mild anterior myocardial ischemia.
c) Normal.
d) Myocardial infarction + technical artifact.
The perfusion result is consistent with:
a) Small inferior myocardial infarction.
b) Mild anterior myocardial ischemia.
c) Normal.
d) Myocardial infarction + technical artifact.
• The technical quality of the study is adequate.
• No perfusion defects are observed.
What would you do now?
a) Send patient home with medication.
b) Send patient to the cath lab.
c) Indicate stress echocardiography.
d) Hospitalize patient in the coronary care unit.
What would you do now?
a) Send patient home with medication.
b) Send patient to the cath lab.
c) Indicate stress echocardiography.
d) Hospitalize patient in the coronary care unit.
• Despite a normal perfusion study, due to CTA findings and a
positive stress test in a symptomatic patient, coronary
angiography is the most logical option.
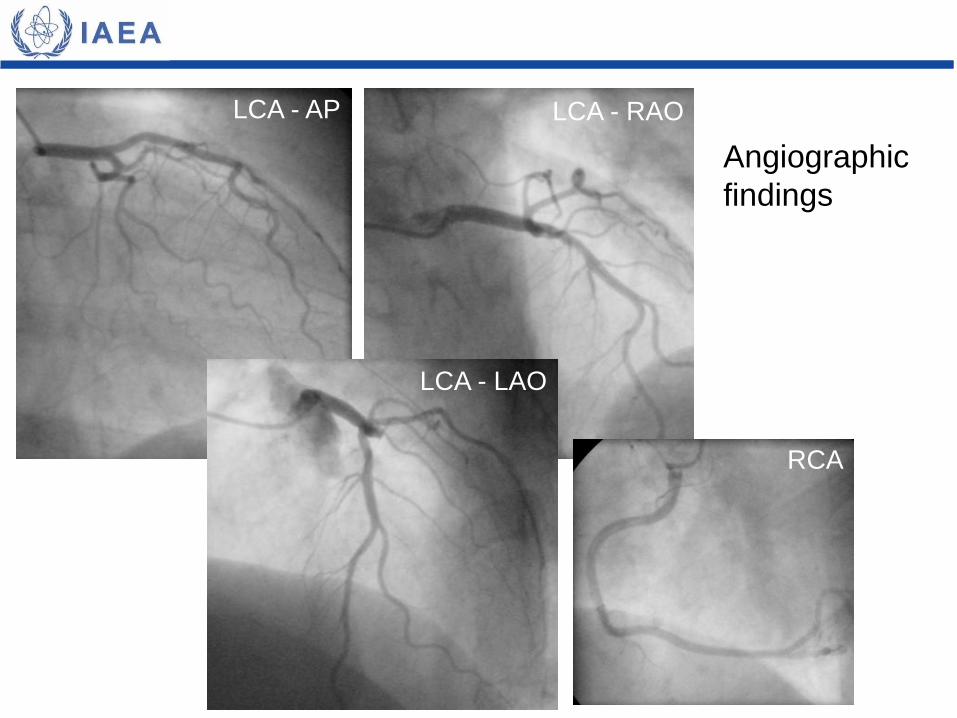
LCA - AP LCA - RAO
LCA - LAO
RCA
Angiographic
findings
a) Normal coronary arteries.
b) Multivessel disease.
c) Moderate Cx stenosis.
d) Minimal LAD stenosis.
Coronary angiography shows:
a) Normal coronary arteries.
b) Multivessel disease.
c) Moderate Cx stenosis.
d) Minimal LAD stenosis.
(see next slide)
Coronary angiography shows:
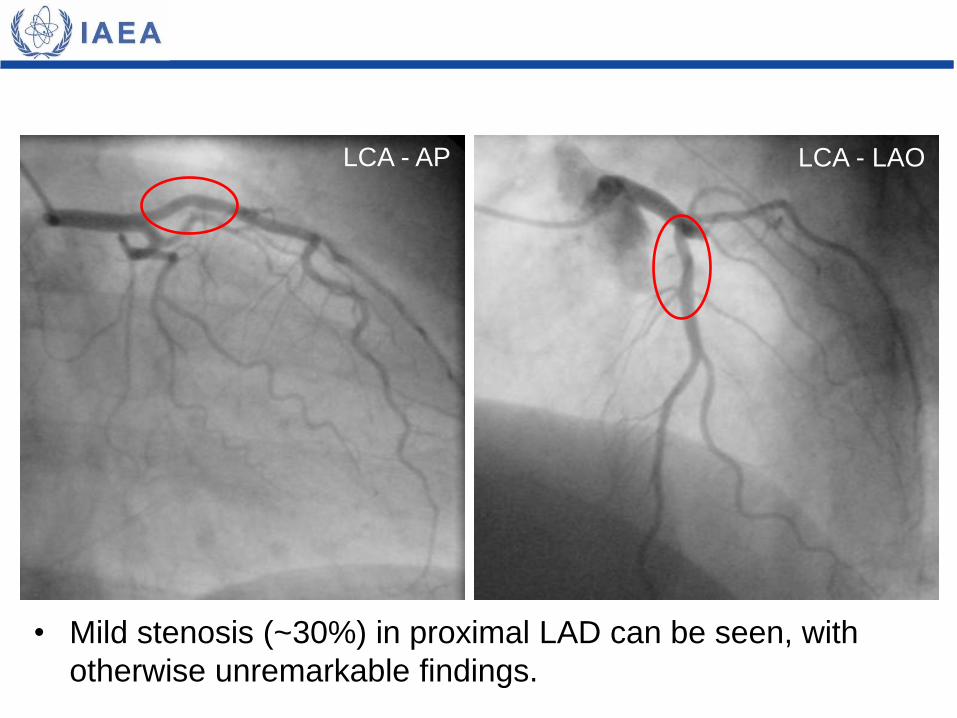
• Mild stenosis (~30%) in proximal LAD can be seen, with
otherwise unremarkable findings.
LCA - AP LCA - LAO
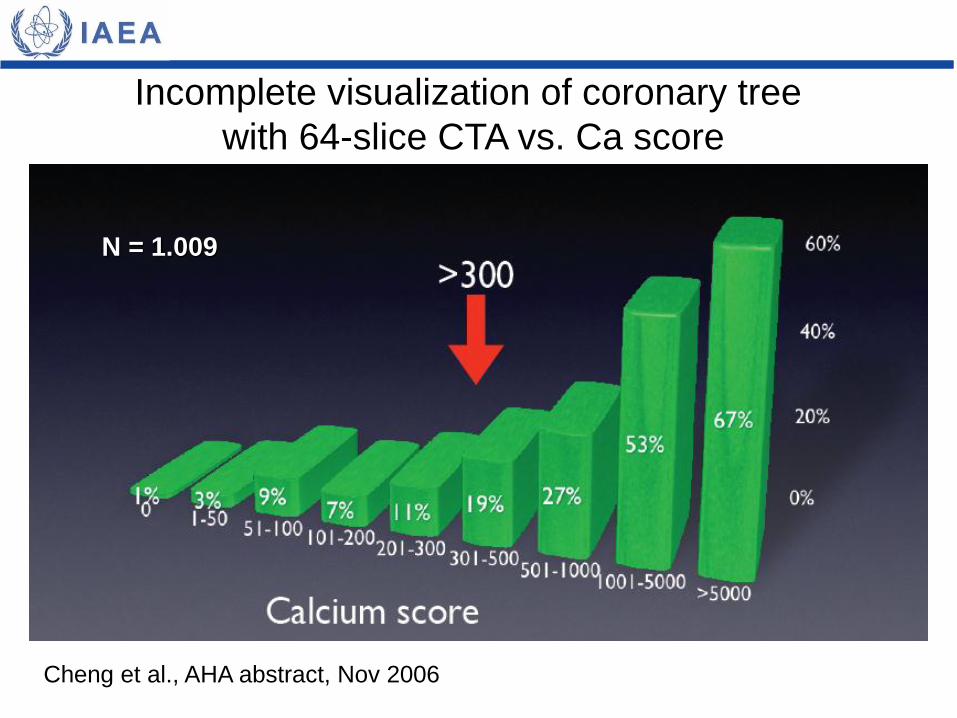
Incomplete visualization of coronary tree
with 64-slice CTA vs. Ca score
N = 1.009
Cheng et al., AHA abstract, Nov 2006
• CTA is sensitive for detecting CAD, however the
technique has limited value in predicting the degree of
stenosis.
• Especially in the presence of arterial calcifications, it is
sometimes difficult to assess the characteristics of a
coronary lesion by CTA.
• Calcium score >300 is associated with poor accuracy of
CTA results (incomplete evaluation of coronary tree).
• Myocardial perfusion has powerful prognostic value and
is not affected by calcium score.
Teaching points
• Zhang S, Levin DC, Halpern EJ, Fischman D, Savage M, Walinsky P.
Accuracy of MDCT in assessing the degree of stenosis caused by
calcified coronary artery plaques. Am J Roentgenol 2008; 191:1676-83.
• Bekkers E, Roos J. Coronary CTA: stenosis classification and
quantification, including automated measures. J Cardiovasc Comput
Tomogr 2009; 3 (Suppl 2):S109-15.
• Halpern EJ, Halpern DJ. Diagnosis of coronary stenosis with CT
angiography comparison of automated computer diagnosis with expert
readings. Acad Radiol 2011; 18:324-33.
• Li JM, Li T, Shi RF, Zhang LR. Comparative analysis between SPECT
myocardial perfusion imaging and CT coronary angiography for
diagnosis of coronary artery disease. Int J Mol Imaging 2012;
2012:253475.
Bibliography