Embed Size (px)
Citation preview

Why bother with attachment theory?
What is attachment theory?
how to apply it to the treatment and management of sex offenders

Why bother?
Higher risk sex offenders are more likely to be personality disordered.
PD is strongly linked to Increase risk of sexual/violent re-offending Increased likelihood of failure/drop out/non-
compliance

Personality disorder is an interpersonal dysfunction - emerging from the interplay between temperament, early environmental influences, and subsequent trauma - leading to the development of attachment difficulties
The underlying premise - 1

Why bother?
Sex offenders with attachment problems are more likely to Be hypervigilent to ‘shaming’ (problems with
disclosure) Say one thing and do another (failure of mentalising) Display antagonism towards authority Engage in excessive or irrational lying and
disclosures Be rule breakers (paradoxical response to heavy
handed licence conditions) Fare badly in standard treatment programmes

Why bother?
Understanding attachment theory improves our understanding of the sexual offending
Underlying Premise 2
Sexual and violent offending contains within it a relationship between the perpetrator and victim – real, symbolic, enduring, fleeting – which mirrors the underlying attachment problems for the offender

Why bother?
The evidence base for treatment models (PD) contains attachment theory at its core Mentalisation based therapy Schema therapy Transference focussed psychotherapy Dialectical behaviour therapy

What is attachment theory?
A biopsychosocial model of human development
Rooted in evolutionary psychology
Transcending individual theoretical models
Incorporating a growing evidence base from both psychology and neurosciences

Key features
Role of primary carer in establishing secure or insecure relating to important others
Development of sense of self in relation to others leading to habitual patterns of relating, particularly in relation to understanding the thoughts and emotions of others
Development of capacity to self-sooth, and thereby manage emotional states, stress and behaviour
Influences the capacity to process and resolve later trauma

Video

Implications for treatment & management
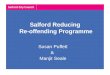
Attachment triangle
Primary carer
Adolescent experiences
Adult patterns of relating
‘transference triangle’
Primary carer
Group or supervisor
Other relationships

Management
MAPPA is a particular type of parent: High levels of over control Low levels of nurturing/affection Highly conditional approval Unwittingly duplicitous (‘confide in me’) Emphasises ‘shaming’ methods (disclosure)

A psychoanalytic perspective
“The view is taken that professionals who deal with offenders are not free agents but potential actors who have been assigned roles in the individual offender’s own re-enactment of their internal world drama. The professionals have the choice not to perform but they can only make this choice when they have a good idea of what the role is they are trying to avoid. Until they can work this out they are likely to be drawn into the plan..” (Davies)

Treatment implications
Shifts the focus of treatment Reduced emphasis on the acquisition of
‘appropriate’ cognitions & mutually agreed insight Increased emphasis on treatment as a small part of
a wider psychological informed management plan Recognising the likelihood that what someone says
and what they do are entirely different things

The framework (3)
Offending occurs as a result of
URGE ACTION
in which emotional arousal leads to a failure in thinking. Treatment aims to
i. identify the urgeii. Acknowledge the actioniii. Control the level of emotional arousaliv. Increase the capacity to thinkv. Thereby increasing choice

Treatment content
Development of a personal narrative with a beginning (development), middle (problems in adult life) and end (the index offence)
Using the attachment triangle for a relationships module
Emphasising self as victim more than offence victim
Focus on doing rather than saying the right thing (less discussion/homework, more on perspective taking skills

Treatment process
Difficulties with theory of mind means the therapists MUST explicitly demonstrate their thinking in the group
Dysfunctional/habitual thoughts and feelings are encouraged in the group (bring the pathology into the room) and worked with, using the group
It’s not what you say, it’s what you do Helping with benefits/travel expenses Letter writing to recalled members Follow up and aftercare

Case examples
The cup cake problem A child molester in a probation group places cup
cakes on the facilitators chairs every week. He generally causes considerable problems, with
arrogance, taking the therapist role, blocking direct interventions etc
In childhood, placed into care by mum and visited by her. Other kids fostered, but he was promised a return home which never materialised

Implications for treatment & management
Attachment triangle
Primary carer
Adolescent experiences
Adult patterns of relating
‘transference triangle’
Primary carer
Group or supervisor
Other relationships

Case example
When letters aren’t enough Jeff is a high risk rapist, who started the group after
30 years of refusing treatment and was then recalled for drinking
Letter writing spiraled out of control, increasingly menacing responses on a daily basis
Most striking aspect of childhood was his mother’s disapproval of him leading to her silence over many years
Rejected MH team aggressively and case closed Prison visit, and subsequent representations to
Parole Board