Embed Size (px)
Citation preview
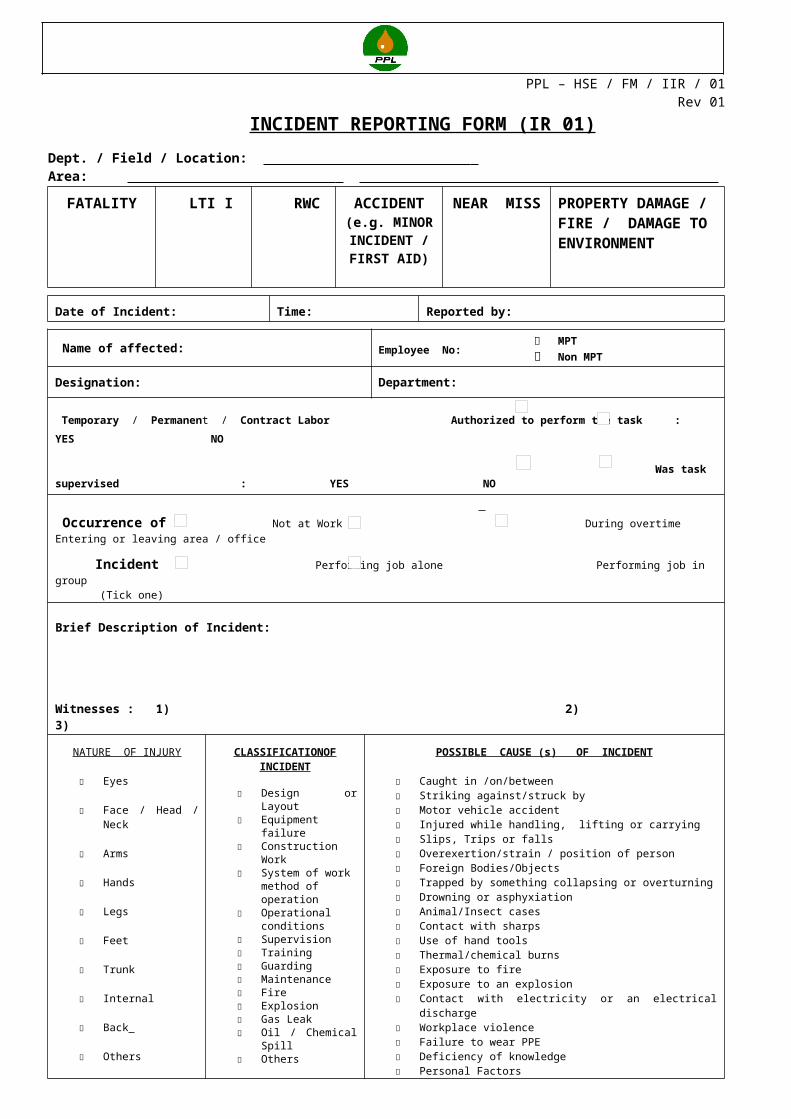
PPL – HSE / FM / IIR / 01Rev 01
INCIDENT REPORTING FORM (IR 01)Dept. / Field / Location: Area:
FATALITY LTI I RWC ACCIDENT (e.g. MINOR INCIDENT / FIRST AID)
NEAR MISS PROPERTY DAMAGE / FIRE / DAMAGE TO ENVIRONMENT
Date of Incident: Time: Reported by:
Name of affected: Employee No: MPT Non MPT
Designation: Department:
Temporary / Permanent / Contract Labor Authorized to perform the task : YES NO
Was task supervised : YES NO Occurrence of Not at Work During overtime Entering or leaving area / office
Incident Performing job alone Performing job in group (Tick one) Brief Description of Incident:
Witnesses : 1) 2) 3)
NATURE OF INJURY
Eyes
Face / Head / Neck
Arms
Hands
Legs
Feet
Trunk
Internal
Back
Others
CLASSIFICATION OF INCIDENT
Design or Layout Equipment failure Construction Work System of work
method of operation Operational
conditions Supervision Training Guarding Maintenance Fire Explosion Gas Leak Oil / Chemical Spill Others
POSSIBLE CAUSE (s) OF INCIDENT
Caught in /on/between Striking against/struck by Motor vehicle accident Injured while handling, lifting or carrying Slips, Trips or falls Overexertion/strain / position of person Foreign Bodies/Objects Trapped by something collapsing or overturning Drowning or asphyxiation Animal/Insect cases Contact with sharps Use of hand tools Thermal/chemical burns Exposure to fire Exposure to an explosion Contact with electricity or an electrical discharge Workplace violence Failure to wear PPE Deficiency of knowledge Personal Factors Other kind of accidents
Treatment Provided:
Sent back to work Sent to Hospital Sent Home
Referred to Site Doctor Not Applicable
Immediate Corrective actions:
Sectional Head: Name & Signature
Date:
Location Incharge: Name & Signature
Date: Comments:
All incidents must be reported to HSE at HO within 24 hrs on IR 01. Investigation report to be generated within 5 days on IR 03 from the date of incident. Near Miss incidents are not required to report on IR 03, except on directives of concerned Dept. Head / Field / Location Incharge / HSE
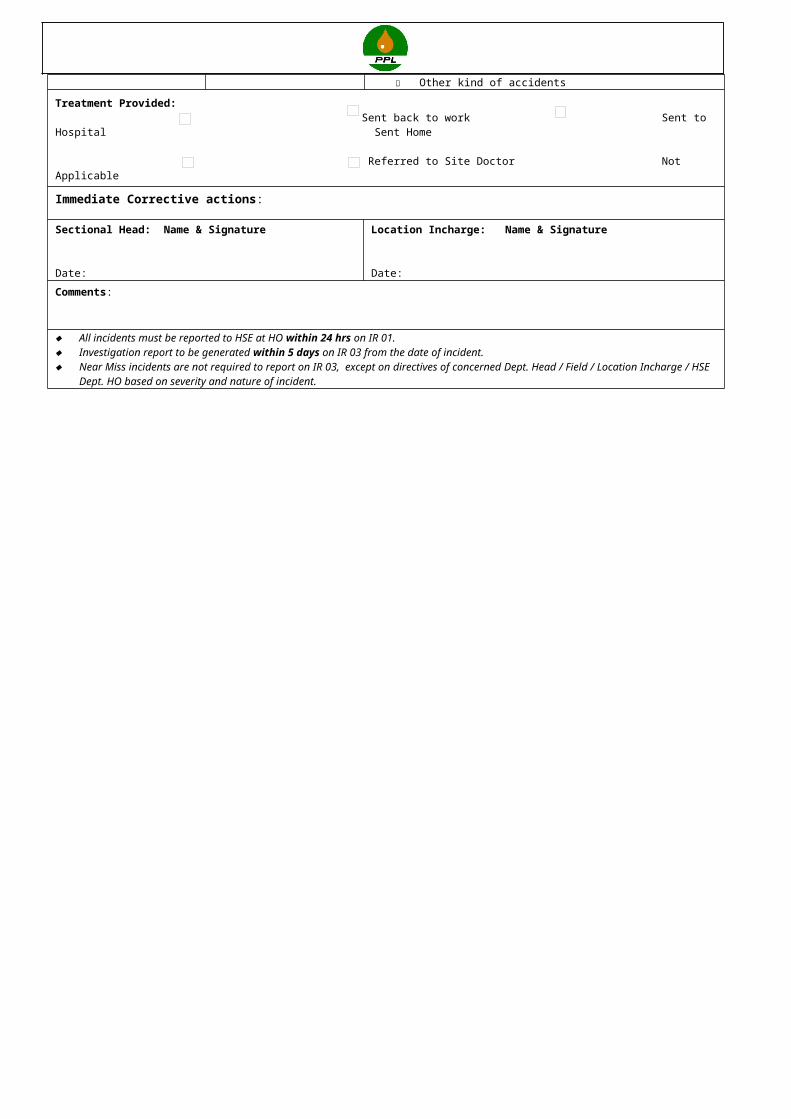
Dept. HO based on severity and nature of incident.























![**Servicing SOP 50504b [10/01/99] - Small Business Administration](https://img.pdfslide.us/doc/110x75/620631598c2f7b173005498d/servicing-sop-50504b-100199-small-business-administration.jpg)





