Embed Size (px)
Citation preview
1560 BRIEF REPORTS
935-941. 2. Kostuk WJ, Branland DJ. Complete heart block associated with acute
myocardial infarction. Am J Cardio11970;26:380-384. 3. Biddle "rL, Ehrlich DA, Hu PN, Hodges M, Relation of heart block and left
ventricular dysfunction in acute myocardial infarction, Am J Cardiol 1977;39:961-965.
4. Strauss HW, Harrison K, Langan JK, Lebovitz E, Pitt B. Thallium-201 for myocardial imaging, Relation of thallium-201 to regional myocardial per- fusion. Circulation 1975;51:641-645.
5. Ritchie JL, Troubaugh GB, Hamilton GW, Narchase KA, Murray JA, Wil- liams DL. Myocardial imaging with thallium-201 at rest and during exercise. Circulation 1977;56:66-71.
6. Maseri A, Parodi O, Severi S, Pesola A. Transient transmural reduction of myocardial blood flow demonstrated by thallium-201 scintigraphy as a case of variant angina. Circulation 1976;54:280-288.
7. McLaughnn PR, Doherly PW, Martin RP, Goris ML, Harrison DC. Myocardial imaging in a patient with reproducible variant angina. Am J Cardio11977; 39:126-129.
Atrial Septostomy as Palliative Therapy for Refractory Primary Pulmonary Hypertension
Stuart Rich, MD Wilfred Lam, MD
Primary pulmonary hypertension (PPH) is an inexo- rably progressive illness that invariably leads to death. We describe a patient with PPH that was refractory to multiple trials with different vasodilator drugs. A right-to-left shunt using an atrial septostomy catheter was created.
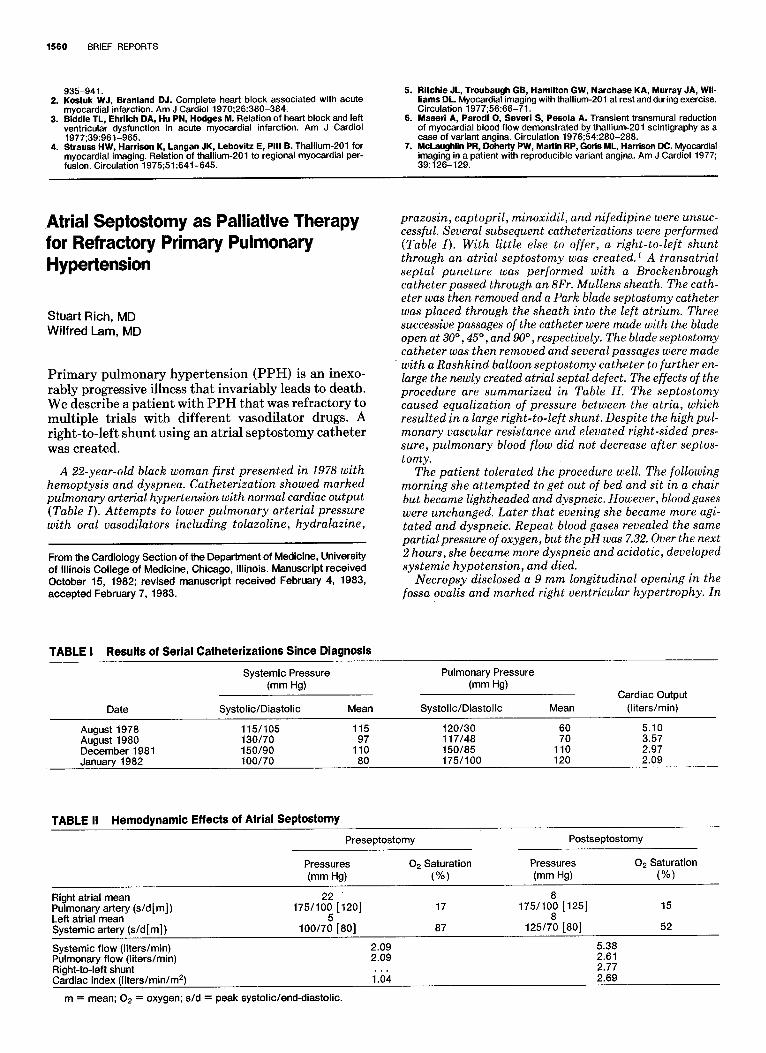
A 22-year-old black woman first presented in 1978 with hemoptysis and dyspnea. Catheterization showed marked pulmonary arterial hypertension with normal cardiac output (Table I). Attempts to lower pulmonary arterial pressure with oral vasodilators including tolazoline, hydralazine,
From the Cardiology Section of the Department of Medicine, University of Illinois College of Medicine, Chicago, Illinois. Manuscript received October 15, 1982; revised manuscript received February 4, 1983, accepted February 7, 1983.
prazosin, captopril, minoxidil, and nifedipine were unsuc- cessful. Several subsequent catheterizations were performed (Table I). With little else to offer, a right-to-left shunt through an atrial septostomy was created. ~ A transatrial septal puncture was performed with a Brockenbrough catheter passed through an 8Fr. Mullens sheath. The cath- eter was then removed and a Park blade septostomy catheter was placed through the sheath into the left atrium. Three successive passages of the catheter were made with the blade open at 30 °, 45 °, and 90 ° , respectively. The blade septostomy catheter was then removed and several passages were made with a Rashkind balloon septostomy catheter to further en- large the newly created atrial septal defect. The effects of the procedure are summarized in Table H. The septostomy caused equalization of pressure between the atria, which resulted in a large right-to-left shunt. Despite the high pul- monary vascular resistance and elevated right-sided pres- sure, pulmonary blood flow did not decrease after septos- tomy.
The patient tolerated the procedure well. The following morning she attempted to get out of bed and sit in a chair but became lightheaded and dyspneic. However, blood gases were unchanged. Later that evening she became more agi- tated and dyspneic. Repeat blood gases revealed the same partial pressure of oxygen, but the pH was 7.32. Over the next 2 hours, she became more dyspneic and acidotic, developed systemic hypotension, and died.
Necropsy disclosed a 9 mm longitudinal opening in the fossa ovalis and marked right ventricular hypertrophy. In
TABLE I Results of Serial Catheterizations Since Diagnosis
Systemic Pressure (mm Hg)
Date Systolic/Diastolic Mean
Pulmonary Pressure (mm Hg)
Cardiac Output Systolic/Diastolic Mean (liters/min)
August1978 115/105 115 120/30 60 5.10 August1980 130/70 97 117/48 70 3.57 December1981 150/90 110 150/85 110 2.97 January 1982 100/70 80 175/100 120 2.09
TABLE II Hemodynamic Effects of Atrial Septostomy
Preseptostomy
Pressures 02 Saturation (ram Hg) (%)
Postseptostomy
Pressures (mm Hg)
02 Saturation (%)
Right atrial mean 22 Pulmonary artery (s/d[m]) 175/100 [120] Left atrial mean 5 Systemic artery (s/d [m]) 100/70 [80]
Systemic flow (liters/min) 2.09 Pulmonary flow (liters/rain) 2.09 Right-to-left shunt Cardiac index (l iters/min/m 2) 1".()4
m = mean; 02 = oxygen; s/d = peak systolic/end-diastolic.
17
87
8 175/100 [125]
8 125/70 [80]
5.38 2.61 2.77 2.69
15
52

May 15, 1983 THE AMERICAN JOURNAL OF CARDIOLOGY Volume 51 1561
addition, the left side of her heart was markedly dilated and marked pulmonary venous congestion was present.
Patients with P P H usually develop symptoms from reduced cardiac output, 2 and on initial presentation are often difficult to distinguish from patients with Eisen- menger's physiology from congenital heart disease. However, patients with severe pulmonary hypertension from an atrial septal defect do better than do patients with PPH, 3 possibly because the right side of the heart is able to decompress itself during periods of stress through the right-to-left shunt. 4
Some patients with P P H have a patent foramen ovale and thus are able to decompress the right side of the heart. Although it has not been clearly demonstrated that these patients do better, a recent retrospective study on patient survival with P P H suggested that this may be the case. 5 We created a right-to-left shunt in our patient because her condition was refractory to medi- cines and because it was clear that she would die soon. The procedure increased the systemic blood flow without compromising pulmonary blood flow despite the marked right-to-left shunting and the increase in left atrial pressure. That this was beneficial to the pa- tient acutely was confirmed by the fact that she survived initially without other medical support.
The cause of her sudden death is not understood. The findings of acute left ventricular volume overload at necropsy implies that the left ventricle was no longer able to handle a normal preload, as it had 3 years earlier. Although the patient had no clinical signs of left ven- tricular dysfunction, perhaps left ventricular function is compromised when right ventricular pressure over- load develops. 6
A theoretical basis exists for creating an atrial septal defect in a patient with refractory pulmonary hyper- tension. Further studies will determine if the creation of an atrial septal defect in patients with P P H will provide long-term benefit.
References
1. Park SC, Neches WH, Mullins CE, Girod DA, Olley PM, Falkowski G, Gar- ibJan VA, Mathews RA, Fricker FJ, Beerman LB, Lenox CC, Zuberbuhler JR. Blade atrial septostomy: collaborative study. Circulation 1982;66: 258-266.
2. Kanemoto N, Sasamoto H. Pulmonary hemodynamics in primary pulmonary hypertension. Jpn Heart J 1979;20:395-405.
3. Young D, Mark H. Fate of the patient with Eisenmenger syndrome. Am J Cardio11971;28:655-669.
4. Austen WG, Morrow AG, Berry WB. Experimental studies on the surgical treatment of primary pulmonary hypertension. J Thorac Cardiovasc Surg 1964;48:448-455.
5. Montanes P, Rozkovec A, Oakley CM. The natural history of primary pul- monary hypertension (abstr). Bull Eur Physiopath Resp 1982;18:87.
6. Ferllnz J. Right ventricular function in adult cardiovascular disease. Prog Cardiovasc Dis 1982;25:225-267.
Fatal Small Bowel Obstruction After Pacemaker Generator Implantation in the Abdominal Wall
Meir Mazuz, MD Natesa G. Pandian, MD Richard E. Kerber, MD
Major complications due to pacemaker implantation are unusual and most often associated with implanta- tion of an epicardial electrode by thoracotomy under general anesthesia. Fatal complications remote from the time of implantation are rare and almost always due to pacemaker malfunction. A case is reported of fatal in- testinal obstruction caused by a pacemaker generator which was implanted in the abdominal wall 7 years earlier.
A 69-year-old man was admitted because of abdominal pain, nausea, and Vomiting. Nine years earlier a transvenous ventricular demand pacemaker had been implanted because 0/2 episodes of syncope associated with left anterior hemi- block on electrocardiogram. Because of pacemaker real- function, it was replaced I year later; because of continued
intermittent capture, I year later it was replaced again, this time with an epicardial pacing electrode with the generator placed subcutaneously in the left upper quadrant of the abdominal wall. The generator was replaced a fourth time because of abdominal wall pacing thought to be due to a current leak. Thereafter, the patient's condition remained stable for 30 months, when abdominal pain prompted readmission. During his outpatient clinic visits, electrocar- diograms and 24-hour Holter monitoring always showed normal sinus rhythm with frequent ventricular premature
From the Cardiovascular Division, Department of Internal Medicine, University of Iowa Hospital, Iowa City, Iowa. This study was supported in part by Grant HL-14388 from the National Heart, Lung, and Blood Institute, Bethesda, Maryland. Manuscript received January 6, 1983; revised manuscript received January 26, 1983, accepted January 28, 1983.
FIGURE 1. Upright abdominal roentgenogram showing multiple dilated loops of small bowel with air-fluid levels. The pacemaker generator implanted in the left lower abdominal wall is visible.