-
7/28/2019 Atresia Biliar ClinLiv[1].06
1/16
Pathogenesis and Treatment Opportunities for
Biliary Atresia
Claus Petersen, MDDepartment of Pediatric Surgery, Hannover
Medical School, Carl-Neuberg Strasse 1,
30625 Hannover, Germany
Biliary atresia is a devastating liver disease of the newborn
with an un-
predictable outcome occurring in about 1 in 14,000 live births.
The first clinical
symptoms of this rare disease are difficult to distinguish from
the frequent and
mostly benign neonatal (physiologic) jaundice. Therefore,
diagnosis and surgical
therapy often occur late, reducing the chance for a good
outcome. Despitesuccessful surgery, fibrosis of the liver often
becomes an ongoing process and
results in cirrhosis in the majority of patients. As a
consequence, biliary atresia is
the most frequent indication for liver transplantation in
childhood.
The long and eventful history of this disease is a story of
innovative ideas
and promising therapeutic options as well as frustrating
curative attempts against
an etiologically incomprehensible entity. Nowadays,
interdisciplinary and inter-
national initiatives enable experts to coordinate their
individual competence,
taking up the challenge to uncover the cause and to improve the
outcome of pa-
tients who have biliary atresia.
Pathogenesis
History and classification
More than 100 years ago, the observation of destruction and
obliteration of
extrahepatic bile ducts with progression to biliary cirrhosis
was first described
1089-3261/06/$ see front matterD 2006 Elsevier Inc. All rights
reserved.
doi:10.1016/j.cld.2005.10.001 liver.theclinics.com
E-mail address: [email protected]
Clin Liver Dis 10 (2006) 7388
-
7/28/2019 Atresia Biliar ClinLiv[1].06
2/16
in children undergoing autopsies [1,2]. This observation had no
impact or any
therapeutic consequences, however. In the early twentieth
century, the obstruc-
tion of the common bile duct was considered to be one reason for
prolongedneonatal jaundice and cholestasis in newborns. The disease
was named con-
genital extrahepatic biliary atresia, and for the first time a
classification strat-
egy was proposed: patients presenting with an isolated distal
and short atresia
of the common bile duct were considered surgically curable if
the proximal
ducts were still patent and wide enough to be drained by a
biliodigestive anas-
tomosis. Unfortunately, most of the patients remained surgically
not curable,
and their outcome was death within the first 2 years of life.
Another surgical
approach was developed at the end of the 1950s, when Kasai
introduced porto-
enterostomy to correct the uncorrectable [3]. Through this
innovative tech-nique, more knowledge of the diversity of changes
along the extrahepatic biliary
tree was gained. During the following years, more
classifications and sophis-
ticated subgroups were defined to improve the understanding of
biliary atresia
[4,5]. In 1972, Landing [6] theorized that biliary atresia might
be an ongoing
inflammatory process induced by an external agent such as viral
infection. From
then on, etiologic possibilities were that biliary atresia is a
congenital morpho-
genic disorder or that biliary atresia is an acquired disease.
As a consequence,
the attribute congenital was dropped, and the term extrahepatic
biliary atresia
became widely used.Despite Kasais successful procedure with
initially good bile flow, several pa-
tients presented with continuous deterioration of the liver
function. This phe-
nomenon was the turning point in realizing that biliary atresia
is an ongoing
inflammatory process of the extra- and the intrahepatic bile
ducts with an un-
predictable clinical course. Therefore the limiting factor for
the outcome in
patients who have biliary atresia is related not only to the
timely removal of atretic
extrahepatic bile ducts and the surgical restoration of bile
flow but rather is an
autonomous and probably self-limiting process of intrahepatic
inflammation. To
encompass this spectrum, the disease is usually referred to as
biliary atresia,which includes all types of destructive
obliteration along the whole bile duct
system. Hence, the challenge for the future and a potential key
for a new and
useful classification is to uncover the still unknown pathogenic
mechanisms of
biliary atresia.
Defective morphogenesis
With regard to the unknown origin, the onset of morphologic or
functional
changes in patients who have biliary atresia is of crucial
interest. Antenatal
detection of prestenotic cystic dilatation of the common bile
duct has been
reported in rare cases [7,8]. In these patients, biliary atresia
is not necessarily
combined with other anomalies, such as polysplenia, a
preduodenal portal vein,
and an interrupted inferior portal vein, which are summarized by
the term biliary
petersen74
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
7/28/2019 Atresia Biliar ClinLiv[1].06
3/16
atresiasplenic malformation [9] or various congenital laterality
defects. It is
still unclear whether these patients form a subgroup in which a
defective
embryogenesis of the biliary tree might play a causative role.
Therefore, whetherthe so-called ductal plate malformation, which is
defined as the persistence or
lack of remodeling of the embryonic ductal plate [10], relates
to the pathogenesis
of biliary atresia and several other diseases of the
intrahepatic bile ducts remains a
matter of discussion. Studies of biliary remnants in patients
who had biliary
atresia revealed morphologic similarities with the remodeling
process of the
ductal plate in fetuses with a gestational age between 11 and 13
weeks [11,12].
A recent study exploring the molecular basis for biliary atresia
found a liver
gene expression profile that differentiates patients who have
biliary atresia from
patients who have other cholestatic liver diseases [13]. A
similar specific approachwas applied to a different group of
patients and found a coordinate expression of
regulatory genes that distinguished the so-called embryonic and
perinatal forms of
biliary atresia [14]. These studies provide preliminary results
of a new and
promising research direction. Before continuing these important
basic studies,
which also focus on the morphogenetic aspect, it is necessary to
generate a better
definition for etiologically relevant terms, such as embryonic,
syndromic,
congenital, acquired, perinatal, and other forms of biliary
atresia [15].
Viral infection
In the early1970s, Landing [16] and Hays [17] proposed that a
single, probably
infective, cause induces inflammation of the intra- and
extrahepatic bile ducts or
the liver parenchyma, clinically manifesting as neonatal
hepatitis, choledochal
cyst, or biliary atresia. This hypothesis was the starting point
for several studies
searching for hepatotropic viruses in patients who had biliary
atresia. Starting in
the 1980s, different viruses were sporadically found in patients
who had biliaryatresia, but the studies were inconclusive. A few
years later, when the polymerase
chain reaction (PCR) technique became routine, larger series of
patients were
tested. Within the last 10 years, many studies have been
published focusing mainly
on four specific viruses. Compiling the results from several
studies, 34% (range,
0%50%) of 50 liver biopsies were positive for cytomegalovirus
[1821], and
14% (range, 0%55%) of 79 patients were positive for reovirus
[2225]. Rota-
virus C was detected in 50% of 18 liver biopsies [23], and human
papilloma
virus was found in 16 of 18 patients [26]. It still remains
unclear whether viruses
are an important etiologic factor for biliary atresia. The main
problems with thesestudies are threefold: first, patients who have
biliary atresia are such a hetero-
geneous group that the number of biopsies performed in each
series is too small.
Second, all studies are restricted to one or two viruses; it
would be much more
effective to test all candidate hepatotropic viruses in a large
series of liver biop-
sies. Third, the most important and overriding problem is the
time at which
samples are obtained for the PCR studies. Biopsies are taken
when the disease
biliary atresia 75
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
7/28/2019 Atresia Biliar ClinLiv[1].06
4/16
has already reached an advanced stage and the patients present
with severe clini-
cal symptoms. Therefore, it is impossible to distinguish,
whether findings are a
trace of an etiologically relevant process or simply represent
an unrelated orsecondary effect. The crucial point, and the dilemma
in most clinical research
programs addressing the viral etiology of biliary atresia, is
that investigations
begin too late in the disease course for viral causation to be
determned.
Immunologic factors
The same problems exist in immunologic investigations in
patients whohave biliary atresia, who present with well-established
disease and an ongoing
inflammatory process. First, immunologic parameters were tested
to evaluate
whether they determine the outcome after Kasais procedure. Some
factors, such
as CD68 and intracellular adhesion molecule (ICAM)-1, seem to be
related to
the postoperative course [27]. Nevertheless, it is obvious that
at the time of diag-
nosis livers of patients who have biliary atresia display a
T-cellmediated inflam-
mation [28]. Several factors of this immunologic cascade have
been described
in these patients. Antigen-presenting cells, such as Kupffers
cells, have been
reported [29], as have CD4+
cells and natural killer cells [27], which differentiateinto
T-helper 1 or T-helper 2 cells (cellular or humoral-mediated
immunity, re-
spectively) [30]. Major histocompatibility complex class I and
class II mole-
cules, which are necessary to allow T cells recognize foreign
antigens, have also
been described [31,32], although their function in biliary
atresia remains ques-
tionable [33]. Additionally, the expression of cell adhesion
molecules (ICAM-1,
vascular adhesion cell molecules, leukocyte factor antigen-1,
nerve cell adhesion
molecule), which are involved in leukocyte recruitment, is
increased in biliary
atresia [27,34]. Cytokines, such as interferon-a, tumor necrosis
factor-b, and os-
teopontin, also play an important role in the signaling pathways
of T-cell andmacrophage-mediated immune reaction and can be found
in liver biopsies of
patients who have biliary atresia [35,36].
Collectively, these data support the hypothesis that the ongoing
inflammatory
process in the liver of patients who have biliary atresia is
closely related to T-cell
activity and cytotoxicity. It remains unclear whether these
observations are the
result of any secondary effects or if the immune response is
induced by a trig-
gering agent that is etiologically relevant. Therefore, it is
necessary to search for
genomic signatures of biliary atresia. A study by Bezerra and
colleagues [37]
focusing on the inflammatory aspect revealed a predominant
cluster of genesthat regulate immunity and inflammatory processes
in the liver of patients who
have biliary atresia. The overexpression of osteopontin and
interferon-g matches
the abovementioned findings and supports the theory of an
inflammatory
pathogenesis of biliary atresia. At this point, further studies
are mandatory to
extend the knowledge about the genetic background of the ongoing
process in
biliary atresia and to trace this back process to its
origin.
petersen76
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
7/28/2019 Atresia Biliar ClinLiv[1].06
5/16
Other mechanisms
Apart from these hypothetic approaches, several other factors
may be involvedin the genesis of biliary atresia. A
population-based study from Sweden identified
several risk factors that facilitate exogenous factors to induce
the development of
biliary atresia [38], but in contrast to other studies [39],
seasonal clustering could
not be found [40]. The observation of risk factors matches the
two-hit theory
from Schreiber and Kleinman [41], who speculated that a still
unknown exoge-
nous factor meets a genetically predisposed condition of the
innate immune
system, which is restricted to the perinatal period.
Nevertheless, hereditary trans-
mission of biliary atresia or any predisposing additional factor
is not likely,
because recurrence in siblings is rare, as is concordance in
dizygotic and mono-zygotic twins [42].
Other potential pathogenetic mechanisms in biliary atresia have
also been
discussed. Ischemia-related biliary obstruction can be induced
by a vasculopathy
of the hepatic vessels, potentially associated with an
autoimmune process. It is
also possible that other nonviral agents, such as bacteria,
toxins, or environmental
factors are responsible for triggering inflammatory processes
that finally lead
to biliary atresia. No consistently evidence has been shown for
this triggering as
a mechanism of disease [43].
Animal models
If the pathogenesis of a disease cannot be elucidated in humans,
it might be
useful to simulate it in animals. In biliary atresia, numerous
attempts have been
made to occlude the extrahepatic bile ducts in different species
or by infecting
mice with reovirus. Those studies were helpful in investigating
the consequences
of artificially induced cholestasis but failed to simulate the
dynamic pattern of
developing biliary atresia [44]. In the early 1990s,
Riepenhoff-Talty and colleagues[45] reported that newborn
Balb/c-mice that were orally infected with rhesus
rotavirus developed irreversible bile duct obstruction. This
observation was the
starting point for establishing a reproducible animal model for
biliary atresia
[46]. Further studies revealed that this model is based on the
hepatotropic effect
of rhesus rotavirus, which targets the biliary system during the
immunologic gap
when the immune system of newborn Balb/c-mice is immature. The
virus seems
to trigger a T-cellmediated immune response independently from
the virus load
of the liver [47]. These observations were confirmed by an
interesting study
from Shivakumar and colleagues [48], who observed that
interferon IFN-g playsa key role in developing biliary atresia in
Balb/c-mice. Despite remarkable simi-
larities between the model and patients who have biliary
atresia, it is not possi-
ble to relate the findings in mice directly to the human
disease. Nevertheless,
the pathogenesis of developing biliary atresia in Balb/c-mice is
relatively clear.
Descendants of nonimmunized mothers present postpartum with a
short immu-
nologic gap and are susceptible to a virus-triggered
T-cellmediated immune
biliary atresia 77
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
7/28/2019 Atresia Biliar ClinLiv[1].06
6/16
response, finally leading to fibrotic obstruction of the bile
ducts. The missing
link in the pathogenetic cascade is the biologic basis for the
localized atresia
within the extrahepatic, but not the intrahepatic, bile ducts.
Inflammatory reactionof the arterioles, which are potentially
mediated by interferon and autoimmunity
factors, may induce an ischemia-related fibrotic transformation
of the extra-
hepatic bile ducts. This hypothesis matches a study in patients
who had biliary
atresia, which described arteriopathy from the trunk of the
common hepatic ar-
tery to its peripheral branches supplying the entire biliary
tree [49,50].
All these observations support the hypothesis that biliary
atresia is an acquired
disease and throw a new light on Perlmutters provocative
speculation as to
whether biliary atresia is a single disease or a phenomenon of
superior patho-
genic mechanism [51]. Therefore discovering more details of the
pathogenesisof biliary atresia in the mouse model is a
priority.
Treatment opportunities
The first therapeutic opportunities were restricted to patients
who had the so-
called correctable form of biliary atresia [52]. Therefore, the
most patients
were still incurable until Kasais portoenterostomy was
introduced. This
procedure was the first breakthrough in the treatment of
patients who had biliaryatresia. The second milestone was liver
transplantation, which continues to
be perfected. Today, surgical treatment is still the only
approach, although the
outcome of patients who have biliary atresia depends on multiple
diagnostic
and therapeutic factors and close interdisciplinary
cooperation.
Diagnosis and Kasais procedure
The first hurdle with biliary atresia is to identify babies who
have pathologichyperbilirubinemia among the large number of
newborns who present with
common and uncomplicated jaundice. It is important to refer
these patients to a
pediatric hepatologist when the clinical signs of cholestasis
persist longer than
2 weeks. The second hurdle is to exclude the most frequent
diseases that also
present with direct hyperbilirubinemia by using a reasonable
diagnostic algo-
rithm. Imaging and functional methods, such as ultrasound (the
triangular cord
sign [53]), MRI cholangiography [54], and hepatobiliary
scintigraphy, are indis-
pensable tools, but they are not accurate enough to exclude the
presence of bili-
ary atresia. The same is true for liver biopsies, which are
helpful either to ruleout several other liver diseases or to be
consistent with an extrahepatic bile duct
obstruction. If the bile duct obstruction cannot definitely be
ruled out, the entire
biliary tree must be visualized, because biliary atresia is
still defined as fibrotic
obstruction of the extrahepatic bile ducts. In pediatric centers
where endoscopic
retrograde cholangiopancreatography in babies is routine, the
patency of the
common bile duct can be shown by this less-invasive method,
probably sparing
petersen78
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
7/28/2019 Atresia Biliar ClinLiv[1].06
7/16
an unnecessary laparotomy. In all other cases, an open
cholangiogram, which can
also be performed by a minimally invasive approach, is necessary
to confirm
the diagnosis.If the intraoperative cholangiogram reveals that
the extrahepatic bile duct is
partially or completely atretic, a portoenterostomy can be
performed during
the same operative procedure. The technical recommendations
originating from
Kasais first papers are still state of the art. Meticulous
preparation of the
duodenal ligament is necessary to identify the branches of the
hepatic artery and
the portal vein as well as the remnants of the hepatic ducts.
The gallbladder must
be dissected, and the remnants of the extrahepatic bile ducts
are the guide to the
fibrous cone in the porta hepatis. The original description of
the Kasai procedure
restricts the preparation of the porta hepatis to a central
area, which is surroundedby the bifurcation of the portal vein
[55]. Today, a much more extensive portal
dissection is recommended to open as many small intrahepatic
bile ducts as
possible and to make better bile flow possible [56]. This change
is the only
variation of the original technique that is accepted worldwide
as a new standard.
Numerous modifications of the original Kasai hepatic
portojejunostomy ver-
sion have been proposed, which can be summarized as total or
partial diversion
of a biliary conduit with or without intestinal valve formation.
None of these
variations proved to be beneficial, however, and most surgeons
returned to the
original procedure, using a 4- to 60-cm Roux-en-Y loop [57,58].
The porto-enteral anastomosis must be performed so that the
funnel-shaped end of the
jejunal loop overrides the completely transected porta hepatis,
so as to catch
every drop of bile. From the surgical point of view, the
preparation and the tran-
section of the porta hepatis is as important as the perfect
placement of the intes-
tinal funnel.
The postoperative management after the Kasai procedure is a
matter of
ongoing discussion. The benefit of peri-, postoperative, and
long-term antibiotic
prophylaxis is indisputable, although the drug used, its
administration, and the
duration of therapy, vary widely [57]. Long-term treatment with
cholereticagents and administration of fat-soluble vitamins are
widely used; a high-caloric
formula with medium-chain triglyceride oil is recommended [42].
Positive ef-
fects on the outcome of postoperative treatment with
corticosteroids are fre-
quently reported. The design and many details of
single-institution studies are
incongruent, however, and no recommendation can yet be made
[5961]. Hence,
a prospective multicenter study is mandatory to determine
whether corticoste-
roids are really helpful in improving the outcome of patients
who have biliary
atresia after the Kasai procedure.
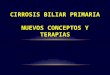
The criterion for successful portoenterostomy in patients who
have biliaryatresia is survival with their own liver. Over the
years the results have im-
proved remarkably, but the data from single-institution and
national multicenter
studies vary greatly. The rate of survival with native liver
ranges between 32%
and 60% after 5 years and between 22% and 53% after 10 years
[57,61,62].
The results for jaundice-free survival are significantly worse,
and after 20 years
nearly all patients are expected to suffer from liver cirrhosis
(Table 1) [63,64].
biliary atresia 79
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
7/28/2019 Atresia Biliar ClinLiv[1].06
8/16
Determination of variables that might influence the outcome of
portoenter-ostomy reveals that age at operation is a crucial
factor. The highest rate of bile
flow restoration can be achieved in patients who are operated on
before they are
60 days old, and the success rate decreases dramatically beyond
the 90-day limit
[57]. Denomination of these limits should not exclude patients
from a surgical
approach, however, because a successful clinical course can also
be seen in pa-
tients who were older than 3 months when the Kasai procedure was
performed
[65,66]. There is agreement that, apart from exceptional cases,
portoenterostomy
should be performed in all patients who have biliary atresia, at
least to bridge
the time between diagnosis and liver transplantation. Achieving
long-term,jaundice-free survival is an important goal for every
patient who has biliary atre-
sia, but prolonged survival with the native liver is always
desirable. Another im-
portant factor influencing the outcome is the experience of the
center [67,68].
Although it could be shown that the surgical outcome is related
to the frequency
of operations, successful treatment of patients who have biliary
atresia depends
both on the professional skills of the surgeon and on the
interlocking coopera-
tion of pediatric surgeons, pediatric gastrologists and
hepatologists, and trans-
plant surgeons.
Early complications that may influence the postoperative
prognosis are as-cending bacterial cholangitis and mechanical
obstruction of the Roux-en-Y loop.
Early diagnosis and adequate treatment of the cholangitis are
essential to pre-
vent deterioration of the intrahepatic bile flow [69]. Primary
or secondary con-
struction of antirefluxive intestinal valves has not been
beneficial and is not
recommended. On the other hand, recurrent episodes of ascending
cholangitis
can be induced by mechanically impaired bile flow along the
biliodigestive
conduit and should be verified by hepatobiliary scintigraphy. In
these cases, and
after acute cessation of initial good bile flow, a surgical
revision of the situs
would be useful (eg, correction of a secondary kinking of the
Roux-en-Y-loop).Debridement or revision of the porta hepatis has
been advocated mainly by
Japanese centers and should be left for specific cases [70].
Because of the unpredictable outcome of patients who have
biliary atresia,
several attempts were made to identify prognostic parameters
facilitating the
postoperative management and a potential marker for an
indication for liver
transplantation. Most of the studies focused on fibrosis markers
or on clinical,
Table 1
Five- and 10-year survival results in patients who have biliary
atresia
Study
5-year survival 10-year survival
Overall
With native
liver Overall
With native
liver
Davenport et al 1997 [89] 68% 60% 43% 22%
Chardot et al 1999 [67] 70% 32% 68% 27%
Ohi 2000 [57] 70% 60% 68% 53%
Nio et al 2003 [99]
petersen80
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
7/28/2019 Atresia Biliar ClinLiv[1].06
9/16
morphologic, and immunologic parameters, but none of the
criteria proved to be
valuable for predicting the individual prognosis [29,7175]. The
only outcome-
related classification can be made by assessing the parameters
of liver functionwithin the first 6 months after the Kasai
procedure. Patients who have normal
bilirubin levels and no signs of portal hypertension seem to
have a relatively
favorable outcome [7678]. As long as the ongoing postoperative
destructive
process of the liver in biliary atresia is not understood, these
investigations
overlap with programs studying the etiology of biliary
atresia.
In conclusion, surgery in biliary atresia is a symptomatic
approach to an
enigmatic and self-limiting process of the liver, which
manifests along the intra-
and extrahepatic biliary tree. Despite the limited therapeutic
options, every effort
must be made to reinforce early detection, timely diagnosis,
perfectly performedKasai procedure, and optimal postoperative care
of patients who have biliary
atresia. These measures will help increase the jaundice-free
survival with the
native liver and decrease the number of liver transplantations
in children who
have biliary atresia.
Liver transplantation
The replacement of the affected organ signifies the beginning of
a newchapter that carries no specific holdovers from the first
disease. The introduction
and rapid development of liver transplantation have been highly
beneficial for
patients who have biliary atresia, because the overall survival
exceeds 80%,
and the outcome of liver transplantation in these patients is
not different from
that in patients who have other end-stage liver diseases [7982].
Technical inno-
vations, such as split-graft or living related-donor liver
transplantation, continu-
ously improve the long-term results [83], and liver
transplantation in children
younger than 1 year has already become routine in highly
specialized centers
[8486]. Pediatric liver transplantation is reviewed elsewhere in
this issue byTiao and Ryckman.
In most patients, biliary atresia is an ongoing process, with
progressive portal
hypertension and deterioration of the liver function sooner or
later requiring liver
transplantation. The question has been raised as to whether
primary liver trans-
plantation should be recommended. In the light of continuously
improving re-
sults of liver transplantation, especially in infants, advocates
argued that primary
liver transplantation would spare the risks of the Kasai
procedure and its post-
operative complications; also, an untouched situs offers better
conditions for the
transplantation and decreases peritransplantation complications
[87]. On theother hand, more than 50% of the patients who have
biliary atresia are jaundice
free after the Kasai procedure, and most of them have a
realistic chance of
surviving with their native liver for more than 10 years.
Therefore, portoenter-
ostomy still remains a curative option for a minority of
patients who have biliary
atresia and for all others is an important bridge to the
expected liver transplan-
tation. Given these arguments, sequential surgical therapy must
be recommended
biliary atresia 81
http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
7/28/2019 Atresia Biliar ClinLiv[1].06
10/16
in all cases of biliary atresia. It is obvious that a correctly
performed Kasai
procedure does not interfere with the transplantation, although
multiple opera-
tions should be avoided [8891]. In some specific cases, however,
determiningthe right procedure is difficult. Late referrals of
patients who have biliary atre-
sia, presenting with complete liver cirrhosis and clinical signs
of portal hyper-
tension, do not necessarily profit from the Kasai procedure. In
these rare cases,
the optimal treatment for each individual must be found by
mutual consent be-
tween all participating disciplines.
A crucial problem of the sequential surgical therapy of patients
who have
biliary atresia is the optimal timing for liver transplantation.
There are no
available parameters that reliably monitor the ongoing
intrahepatic process of
the disease. Therefore, the clinical sequelae of portal
hypertension and impairedphysical development are the only criteria
for timing of liver transplantation.
Close cooperation within the interdisciplinary team is also
mandatory because
any therapeutic decision depends on the physical condition of
the recipient
[92,93].
No fundamental breakthrough in surgery for biliary atresia seems
to be in
sight. In series from experienced centers, outcomes after the
Kasai procedure are
comparable, and over the years the rate of bile flow restoration
remains un-
changed. It cannot be expected that further development of the
Kasai procedure
will improve the survival with native liver of patients who have
biliary atresia.Nevertheless, technical innovations, such as
minimally invasive surgery or ro-
botically assisted procedures, are feasible and might be
beneficial in relieving
the perioperative stress of the patients [94,95]. Because the
surgical approach to
biliary atresia addresses only the symptoms of the disease, it
will never address
its cause. Until there is an origin-related therapeutic
approach, every effort must
be made to optimize the results of the Kasai
portoenterostomy.
Future prospects
In the face of so many unsolved problems in biliary atresia, the
challenges
for the near future are clear. The first is that health care
providers should refer
every baby with neonatal jaundice lasting more than 14 days.
Screening pro-
grams are feasible [96] and essential, but in most countries,
they are not available
for economic reasons. Therefore, the second condition becomes
more evident:
every neonate thought to be suffering from biliary atresia must
immediately be
referred to a center with expertise in pediatric hepatobiliary
disorders. There a
modern management strategy will be available to rule out other
diseases, andthe Kasai portoenterostomy is a familiar procedure for
the team. In addition to
early diagnosis and adequate surgical therapy, long-term
postoperative care is
indispensable to improving the overall outcome. Unfortunately,
despite optimal
treatment modalities, the deterioration of the liver is an
ongoing process in
most patients who have biliary atresia; the tools to slow the
process are limited,
and there is no way to stop it. Hence, the third challenge has
the highest prior-
petersen82
http://-/?-http://-/?-http://-/?-http://-/?-
-
7/28/2019 Atresia Biliar ClinLiv[1].06
11/16
ity: to develop curative treatment strategies, every effort must
be made to un-
cover the cause of biliary atresia. This discovery is the only
way to understand
the pathogenesis, to guide the treatment opportunities
effectively toward the keypathogenetic mechanisms of disease, or,
optimally, to prevent newborns from
developing biliary atresia [62,97,98].
During the several last years, more and more working groups have
accepted
this challenge, and several activities have been initiated or
intensified. Existing
biliary atresia registries in Japan and France and
treatment-optimization
programs in the United Kingdom stimulated the community of
researchers in
biliary atresia to coordinate their activities and increase
their effectiveness
[67,68,99]. In the United States, the new Biliary Atresia
Research Consortium
(www.med.umich.edu/borc/barc/sites.htm) is a network of 10
clinical centersthat serves as a clinical database and a
coordinating center for clinical and basic
research studies [100]. In Europe, the Biliary Atresia Registry
(www.biliary-
atresia.com) was founded to coordinate the data from the
participating countries
[101], and the new European Foundation for Biliary Atresia
Research (www.
orpha.net) uses the existing infrastructure to sponsor
multicenter research studies.
Intensive and close cooperation among these initiatives helps
improve the in-
terim results and achieve the definite objective: uncovering the
etiology and
pathogenesis of biliary atresia and finding a cure.
Summary
Biliary atresia is a cholestatic disease affecting the intra-
and the extrahe-
patic bile ducts of the newborn; with unpredictable outcome, it
is the main indi-
cation for pediatric liver transplantation. The cause of this
rare entity still remains
unclear, hypothetically ranging from defective morphogenesis to
viral infection
or an immunologic defect. Although most patients finally need
liver transplan-tation, the interim objective is to optimize
patients survival with their native
liver. Early diagnosis, timely and perfectly performed
portoenterostomy, and op-
timal postoperative care are indispensable to reduce the
frequency of liver trans-
plantation for biliary atresia. The sequential surgical approach
to biliary atresia
(obligatory Kasai procedure and optional liver transplantation)
improves the
symptoms of the disease but does not address its cause.
Therefore, clinical and
basic research is mandatory to elucidate the origin of biliary
atresia. To compen-
sate for the infrequency of biliary atresia, international
multicenter studies
should focus on clinical and on etiologic aspects.
Unfortunately, basic researchin biliary atresia is retrospective,
because it always starts when the disease has
already reached an advanced stage. Using animal models, the
dynamic pattern of
biliary atresia can be simulated, and with a coordinated
research program the
pathogenesis of the disease can be better understood. Intensive
and close inter-
disciplinary cooperation will be beneficial for the patients and
will help solve
the riddle of biliary atresia.
biliary atresia 83
http://%20http//www.med.umich.edu/borc/barc/sites.htmhttp://%20http//www.biliary-atresia.comhttp://-/?-http://%20http//www.orpha.nethttp://-/?-http://%20http//www.orpha.nethttp://%20http//www.biliary-atresia.comhttp://%20http//www.med.umich.edu/borc/barc/sites.htmhttp://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-http://-/?-
-
7/28/2019 Atresia Biliar ClinLiv[1].06
12/16
References
[1] Thomson J. On congenital obliteration of the bile ducts.
Edinburgh Med J 1891;37:523 31.[2] Lomer R. Uber einen Fall von
congenitaler partieller Obstruktion der Galleng7nge. Virchows
Arch Path Anat Physiol 1885;99:1309.
[3] Reuben A. The sensei of Sendai: correcting the
uncorrectable. Hepatology 2003;37:952 5.
[4] Miyano T, Suruga K, Tsuchiya H, et al. A histopathological
study of the remnant of ex-
trahepatic bile duct in so-called uncorrectable biliary atresia.
J Pediatr Surg 1977;12(1):19 25.
[5] Yamagiwa I. Histopathologic study of the extrahepatic
biliary system in uncorrectable
cocongenital biliary atresia: its pathogenesis and type of
atresia. Nippon Geka Gakkai Zasshi
1985;86(5):587601.
[6] Landing BH. Considerations of the pathogenesis of neonatal
hepatitis, biliary atresia and
choledochal cystthe concept of infantile obstructive
cholangiopathy. Prog Pediatr Surg
1974;6:11339.[7] Tsuchida Y, Kawarasaki H, Iwanaka T, et al.
Antenatal diagnosis of biliary atresia (type I cyst)
at 19 weeks gestation: differential diagnosis and etiologic
implications. J Pediatr Surg 1995;
30(5):6979.
[8] Hinds R, Davenport M, Mieli-Vergani G, et al. Antenatal
presentation of biliary atresia. J Pediatr
2004;144(1):43 6.
[9] Davenport M, Savage M, Mowat AP, et al. Biliary atresia
splenic malformation syndrome:
an etiologic and prognostic subgroup. Surgery
1993;113(6):6628.
[10] Desmet VJ. Congenital diseases of intrahepatic bile ducts:
variations on the theme ductal plate
malformation. Hepatology 1992;16(4):1069 83.
[11] Tan CE, Driver M, Howard ER, et al. Extrahepatic biliary
atresia: a first-trimester event?
Clues from light microscopy and immunohistochemistry. J Pediatr
Surg 1994;29(6):80812.[12] Vijayan V, El Tan C. Computer-generated
three-dimensional morphology of the hepatic hilar
bile ducts in biliary atresia. J Pediatr Surg 2000;35(8):1230
5.
[13] Chen L, Goryachev A, Sun J, et al. Altered expression of
genes involved in hepatic morpho-
genesis and fibrogenesis are identified by cDNA microarray
analysis in biliary atresia. Hepato-
logy 2003;38(3):567 76.
[14] Zhang DY, Sabla G, Shivakumar P, et al. Coordinate
expression of regulatory genes dif-
ferentiates embryonic and perinatal forms of biliary atresia.
Hepatology 2004;39(4):95462.
[15] Davenport M. A challenge on the use of the words embryonic
and perinatal in the context of
biliary atresia. Hepatology 2005;41(2):403 4 [author reply:
4045].
[16] Landing BH. Considerations of the pathogenesis of neonatal
hepatitis, biliary atresia and
choledochal cystthe concept of infantile obstructive
cholangiopathy. Prog Pediatr Surg 1974;
6:11339.
[17] Hays DM. Biliary atresia: the current state of confusion.
Surg Clin North Am 1973;53:
125773.
[18] Tarr PI, Haas JE, Christie DL. Biliary atresia,
cytomegalovirus, and age at referral. Pediatrics
1996;97:82831.
[19] Fischler B, Ehrnst A, Forsgren M, et al. The viral
association of neonatal cholestasis in Sweden:
a possible link between cytomegalovirus infection and
extrahepatic biliary atresia. J Pediatr
Gastroenterol Nutr 1998;27(1):57 64.
[20] Jevon GP, Dimmick JE. Biliary atresia and cytomegalovirus
infection: a DNA study. Pediatr
Dev Pathol 1999;2(1):114.
[21] Fjaer RB, Bruu AL, Nordbo SA. Extrahepatic bile duct
atresia and viral involvement. Pediatr
Transplant 2005;9(1):6873.
[22] Steele MI, Marshall CM, Lloyd RE, et al. Reovirus 3 not
detected by reverse transcriptase-
mediated polymerase chain reaction analysis of preserved tissue
from infants with cholestatic
liver disease. Hepatology 1995;21(3):697702.
[23] Riepenhoff-Talty M, Gouvea V, Evans MJ, et al. Detection of
group C rotavirus in infants with
extrahepatic biliary atresia. J Infect Dis 1996;174(1):815.
petersen84
-
7/28/2019 Atresia Biliar ClinLiv[1].06
13/16
[24] Tyler KL, Sokol RJ, Oberhaus SM, et al. Detection of
reovirus RNA in hepatobiliary tissues
from patients with extrahepatic biliary atresia and choledochal
cysts. Hepatology 1998;
27(6):147582.
[25] Saito T, Shinozaki K, Matsunaga T, et al. Lack of evidence
for reovirus infection in tissues
from patients with biliary atresia and congenital dilatation of
the bile duct. J Hepatol 2004;
40(2):20311.
[26] Drut R, Drut RM, Gomez MA, et al. Presence of human
papillomavirus in extrahepatic biliary
atresia. J Pediatr Gastroenterol Nutr 1998;27(5):530 5.
[27] Davenport M, Gonde C, Redkar R, et al. Immunohistochemistry
of the liver and biliary tree
in extrahepatic biliary atresia. J Pediatr Surg
2001;36(7):101725.
[28] Mack CL, Sokol RJ. Unraveling the pathogenesis and etiology
of biliary atresia. Pediatr Res
2005;57:87R94R.
[29] Urushihara N, Iwagaki H, Yagi T, et al. Elevation of serum
interleukin-18 levels and activation
of Kupffer cells in biliary atresia. J Pediatr Surg
2000;35(3):4469.
[30] Mack CL, Tucker RM, Sokol RJ, et al. Armed CD4(+) Th1
effector cells and activated
macrophages participate in bile duct injury in murine biliary
atresia. Clin Immunol 2005;
115(2):2009.
[31] Yuasa T, Tsuji H, Kimura S, et al. Human leukocyte antigens
in Japanese patients with biliary
atresia: retrospective analysis of patients who underwent living
donor liver transplantation.
Hum Immunol 2005;66(3):295300.
[32] Feng J, Li M, Gu W, et al. The aberrant expression of
HLA-DR in intrahepatic bile ducts in
patients with biliary atresia: an immunohistochemistry and
immune electron microscopy study.
J Pediatr Surg 2004;39(11):165862.
[33] Donaldson PT, Clare M, Constantini PK, et al. HLA and
cytokine gene polymorphisms in
biliary atresia. Liver 2002;22(3):213 9.[34] Torbenson M, Wang
J, Abraham S, et al. Bile ducts and ductules are positive for
CD56
(N-CAM) in most cases of extrahepatic biliary atresia. Am J Surg
Pathol 2003;27(11):
14547.
[35] Whitington PF, Malladi P, Melin-Aldana H, et al. Expression
of osteopontin correlates with
portal biliary proliferation and fibrosis in biliary atresia.
Pediatr Res 2005;57(6):837 44.
[36] Kobayashi H, Yamataka A, Lane GJ, et al. Levels of
circulating antiinflammatory cytokine
interleukin-1 receptor antagonist and proinflammatory cytokines
at different stages of biliary
atresia. J Pediatr Surg 2002;37(7):103841.
[37] Bezerra JA, Tiao G, Ryckman FC, et al. Genetic induction of
proinflammatory immunity in
children with biliary atresia. Lancet 2002;360(9346):16539.
[38] Fischler B, Haglund B, Hjern A. A population-based study on
the incidence and possible pre-and perinatal etiologic risk factors
of biliary atresia. J Pediatr 2002;141(2):21722.
[39] Caton AR, Druschel CM, McNutt LA. The epidemiology of
extrahepatic biliary atresia in
New York State, 198398. Paediatr Perinat Epidemiol 2004;18(2):97
105.
[40] Ayas MF, Hillemeier AC, Olson AD. Lack of evidence for
seasonal variation in extrahepatic
biliary atresia during infancy. J Clin Gastroenterol
1996;22(4):292 4.
[41] Schreiber RA, Kleinman RE. Genetics, immunology, and
biliary atresia: an opening or a
diversion? J Pediatr Gastroenterol Nutr 1993;16(2):111 3.
[42] Balistreri WF, Bove KE, Ryckman FC. Biliary atresia and
other disorders of the extrahe-
patic bile ducts. In: Suchy FJ, Sokol RJ, Balistreri WF,
editors. Liver diseases in children.
2nd edition. Philadelphia7 Lippincott Williams & Wilkins;
2001. p. 25374.
[43] Sokol RJ, Mack C, Narkewicz MR, Karrer FM. Pathogenesis and
outcome of biliary atresia:current concepts. J Pediatr
Gastroenterol Nutr 2003;37(1):4 21.
[44] Chang KS, Chang JHT. Animal models of pediatric surgical
diseases. Pediatr Surg Int 1994;
9:30722.
[45] Riepenhoff-Talty M, Schaekel K, Clark HF, et al. Group A
rotaviruses produce extrahepatic
biliary obstruction in orally inoculated newborn mice. Pediatr
Res 1993;33(4):394 9.
[46] Petersen C, Biermanns D, Kuske M, et al. New aspects in a
murine model for extrahepatic
biliary atresia. J Pediatr Surg 1997;32(8):1190 5.
biliary atresia 85
-
7/28/2019 Atresia Biliar ClinLiv[1].06
14/16
[47] Czech-Schmidt G, Verhagen W, Szavay P, et al. Immunological
gap in the infectious animal
model for biliary atresia. J Surg Res 2001;101(1):627.
[48] Shivakumar P, Campbell KM, Sabla GE, et al. Obstruction of
extrahepatic bile ducts by
lymphocytes is regulated by IFN-gamma in experimental biliary
atresia. J Clin Invest 2004;
114(3):3229.
[49] Ho CW, Shioda K, Shirasaki K, et al. The pathogenesis of
biliary atresia: a morphological
study of the hepatobiliary system and the hepatic artery. J
Pediatr Gastroenterol Nutr 1993;
16(1):5360.
[50] dos Santos JL, da Silveira TR, da Silva VD, et al. Medial
thickening of hepatic artery branches
in biliary atresia. A morphometric study. J Pediatr Surg
2005;40(4):63751.
[51] Perlmutter DH, Shepherd RW. Extrahepatic biliary atresia: a
disease or a phenotype?
Hepatology 2002;35(6):1297 304.
[52] Ladd WE. Congenital atresia and stenosis of the ducts. JAMA
1928;91:1082.
[53] Kotb MA, Kotb A, Sheba MF, et al. Evaluation of the
triangular cord sign in the diagnosis
of biliary atresia. Pediatrics 2001;108(2):416 20.
[54] Ryeom HK, Choe BH, Kim JY, et al. Biliary atresia:
feasibility of mangafodipir trisodium-
enhanced MR cholangiography for evaluation. Radiology
2005;235(1):2508.
[55] Kasai M, Kimura S, Asakura S. Surgical treatment of biliary
atresia. J Pediatr Surg 1968;3:
66575.
[56] Ando H. A new operation for noncorrectable biliary atresia.
Nagoya J Med Sci 1999;62(34):
10714.
[57] Ohi R. Biliary atresia. A surgical perspective. Clin Liver
Dis 2000;4(4):779 804.
[58] Maksoud JG, Fauza DO, Silva MM, et al. Management of
biliary atresia in the liver trans-
plantation era: a 15-year, single-center experience. J Pediatr
Surg 1998;33(1):115 8.
[59] Muraji T, Nio M, Ohhama Y, et al. Postoperative
corticosteroid therapy for bile drainage inbiliary atresiaa
nationwide survey. J Pediatr Surg 2004;39(12):1803 5.
[60] Kobayashi H, Yamataka A, Koga H, et al. Optimum
prednisolone usage in patients with biliary
atresia postportoenterostomy. J Pediatr Surg 2005;40(2):327
30.
[61] Davenport M. Biliary atresia. Semin Pediatr Surg
2005;14(1):42 8.
[62] Petersen C. Surgery in biliary atresiafutile or futuristic?
Eur J Pediatr Surg 2004;14(4):
2269.
[63] Lykavieris P, Chardot C, Sokhn M, et al. Outcome in
adulthood of biliary atresia: a study of
63 patients who survived for over 20 years with their native
liver. Hepatology 2005;41(2):
36671.
[64] Howard ER, MacLean G, Nio M, et al. Survival patterns in
biliary atresia and comparison
of quality of life of long-term survivors in Japan and England.
J Pediatr Surg 2001;36(6):8927.
[65] Chardot C, Carton M, Spire-Bendelac N, et al. Is the Kasai
operation still indicated in children
older than 3 months diagnosed with biliary atresia? J Pediatr
2001;138(2):2248.
[66] Davenport M, Puricelli V, Farrant P, et al. The outcome of
the older (100 days) infant
with biliary atresia. J Pediatr Surg 2004;39(4):57581.
[67] Chardot C, Carton M, Spire-Bendelac N, et al. Prognosis of
biliary atresia in the era of liver
transplantation: French national study from 1986 to 1996.
Hepatology 1999;30(3):60611.
[68] Davenport M, De Ville de Goyet J, Stringer MD, et al.
Seamless management of biliary atresia
in England and Wales (19992002). Lancet 2004;363(9418):1354
7.
[69] Lunzmann K, Schweizer P. The influence of cholangitis on
the prognosis of extrahepatic
biliary atresia. Eur J Pediatr Surg 1999;9(1):19 23.[70] Ohi R,
Hanamatsu M, Mochizuki I, et al. Reoperation in patients with
biliary atresia. J Pediatr
Surg 1985;20(3):2569.
[71] Davenport M, Gonde C, Redkar R, et al. Immunohistochemistry
of the liver and biliary tree
in extrahepatic biliary atresia. J Pediatr Surg
2001;36(7):101725.
[72] Kobayashi H, Puri P, OBriain DS, et al. Hepatic
overexpression of MHC class II antigens and
macrophage-associated antigens (CD68) in patients with biliary
atresia of poor prognosis.
J Pediatr Surg 1997;32(4):5903.
petersen86
-
7/28/2019 Atresia Biliar ClinLiv[1].06
15/16
[73] Tan CE, Davenport M, Driver M, et al. Does the morphology
of the extrahepatic biliary
remnants in biliary atresia influence survival? A review of 205
cases. J Pediatr Surg 1994;
29(11):145964.
[74] Uchida K, Urata H, Suzuki H, et al. Predicting factor of
quality of life in long-term jaundice-
free survivors after the Kasai operation. J Pediatr Surg
2004;39(7):10404.
[75] Chongsrisawat V, Kongtawelert P, Tongsoongnoen W, et al.
Serum hyaluronan as a marker
reflecting the severity of cirrhosis and portal hypertension in
postoperative biliary atresia.
Pediatr Surg Int 2004;20(10):7737.
[76] Endo M, Masuyama H, Watanabe K, et al. Calculation of
biliary atresia prognostic index
using a multivariate linear model. J Pediatr Surg
1995;30(11):15759.
[77] Subramaniam R, Doig CM, Bowen J, et al. Initial response to
portoenterostomy determines
long-term outcome in patients with biliary atresia. J Pediatr
Surg 2000;35(4):5937.
[78] Ohhama Y, Shinkai M, Fujita S, et al. Early prediction of
long-term survival and the timing
of liver transplantation after the Kasai operation. J Pediatr
Surg 2000;35(7):1031 4.
[79] Fouquet V, Alves A, Branchereau S, et al. Long-term outcome
of pediatric liver trans-
plantation for biliary atresia: a 10-year follow-up in a single
center. Liver Transpl 2005;11(2):
15260.
[80] Migliazza L, Lopez Santamaria M, Murcia J, et al. Long-term
survival expectancy after
liver transplantation in children. J Pediatr Surg
2000;35(1):57.
[81] Diem HV, Evrard V, Vinh HT, et al. Pediatric liver
transplantation for biliary atresia: results of
primary grafts in 328 recipients. Transplantation
2003;75(10):1692 7.
[82] Peeters PM, Sieders E, De Jong KP, et al. Comparison of
outcome after pediatric liver
transplantation for metabolic diseases and biliary atresia. Eur
J Pediatr Surg 2001;11(1):28 35.
[83] Otte JB. History of pediatric liver transplantation. Where
are we coming from? Where do we
stand? Pediatr Transplant 2002;6(5):37887.[84] Noujaim HM, Mayer
DA, Buckles JA, et al. Techniques for and outcome of liver
trans-
plantation in neonates and infants weighing up to 5 kilograms. J
Pediatr Surg 2002;37(2):
15964.
[85] Grabhorn E, Schulz A, Helmke K, et al. Short- and long-term
results of liver transplantation in
infants aged less than 6 months. Transplantation
2004;78(2):23541.
[86] Tiao GM, Alonso M, Bezerra J, et al. Liver transplantation
in children younger than 1 year
the Cincinnati experience. J Pediatr Surg 2005;40(1):268 73.
[87] Sandler AD, Azarow KS, Superina RA. The impact of a
previous Kasai procedure on liver
transplantation for biliary atresia. J Pediatr Surg
1997;32(3):416 9.
[88] Valayer J. Conventional treatment of biliary atresia:
long-term results. J Pediatr Surg 1996;
31(11):154651.[89] Davenport M, Kerkar N, Mieli-Vergani G, et
al. Biliary atresia: the Kings College Hospital
experience (19741995). J Pediatr Surg 1997;32(3):479 85.
[90] Visser BC, Suh I, Hirose S, et al. The influence of
portoenterostomy on transplantation for
biliary atresia. Liver Transpl 2004;10(10):1279 86.
[91] Sugawara Y, Makuuchi M, Kaneko J, et al. Impact of previous
multiple portoenterostomies
on living donor liver transplantation for biliary atresia.
Hepatogastroenterology 2004;51(55):
1924.
[92] Okazaki T, Kobayashi H, Yamataka A, et al. Long-term
postsurgical outcome of biliary atresia.
J Pediatr Surg 1999;34(2):3125.
[93] Kimura T, Hasegawa T, Sasaki T, et al. Optimal timing for
living-related liver transplantation
in children. Clin Transplant 2004;18(5):497501.[94] Esteves E,
Clemente Neto E, Ottaiano Neto M, et al. Laparoscopic Kasai
portoenterostomy for
biliary atresia. Pediatr Surg Int 2002;18(8):737 40.
[95] Lorincz A, Knight CG, Langenburg SE, et al. Robot-assisted
minimally invasive Kasai
portoenterostomy: a survival porcine study. Surg Endosc
2004;18(7):1136 9.
[96] Matsui A, Dodoriki M. Screening for biliary atresia. Lancet
1995;345(8958):1181.
[97] Rudolph JA, Balistreri WF. Optimal treatment of biliary
atresiahalfway there! Hepatology
1999;30(3):80810.
biliary atresia 87
-
7/28/2019 Atresia Biliar ClinLiv[1].06
16/16
[98] Chardot C. Treatment for biliary atresia in 2003. J Pediatr
Gastroenterol Nutr 2003;37(4):
4078.
[99] Nio M, Ohi R, Miyano T, et al. Japanese Biliary Atresia
Registry. Five- and 10-year survival
rates after surgery for biliary atresia: a report from the
Japanese Biliary Atresia Registry.
J Pediatr Surg 2003;38(7):9971000.
[100] Sokol RJ. New North American research network focuses on
biliary atresia and neonatal liver
disease. J Pediatr Gastroenterol Nutr 2003;36(1):1.
[101] Petersen C, Melter M, Leonhardt J, et al. Biliary atresia
research is crossing national and
interdisciplinary borderlines. Acta Pediatrica 2005;94:5267.
petersen88