Embed Size (px)
Citation preview
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 1/54
Required when distributed (EMR, EMT, AEMT)
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 2/54
ObjectivesAt the completion of this educationmodule, the provider will have:
An understanding of scene safety and assuring
responder safety.An understanding of the physiological effectsof nerve agents.Will demonstrate with 100% accuracy the
procedure to auto-injection administration.
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 3/54
Why Now?Increased concern for
terrorismAvailable in old munitionsin US and elsewhere
Have been successfullymanufactured byother countries
Very lethal
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 4/54
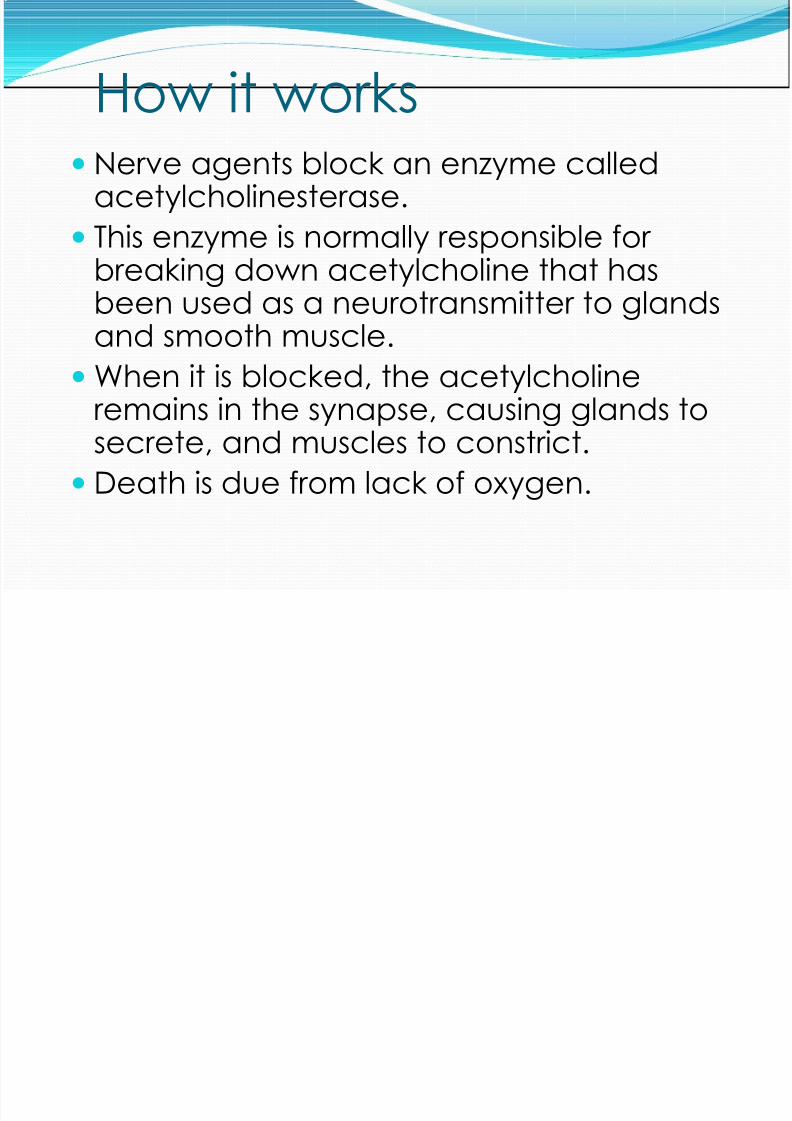
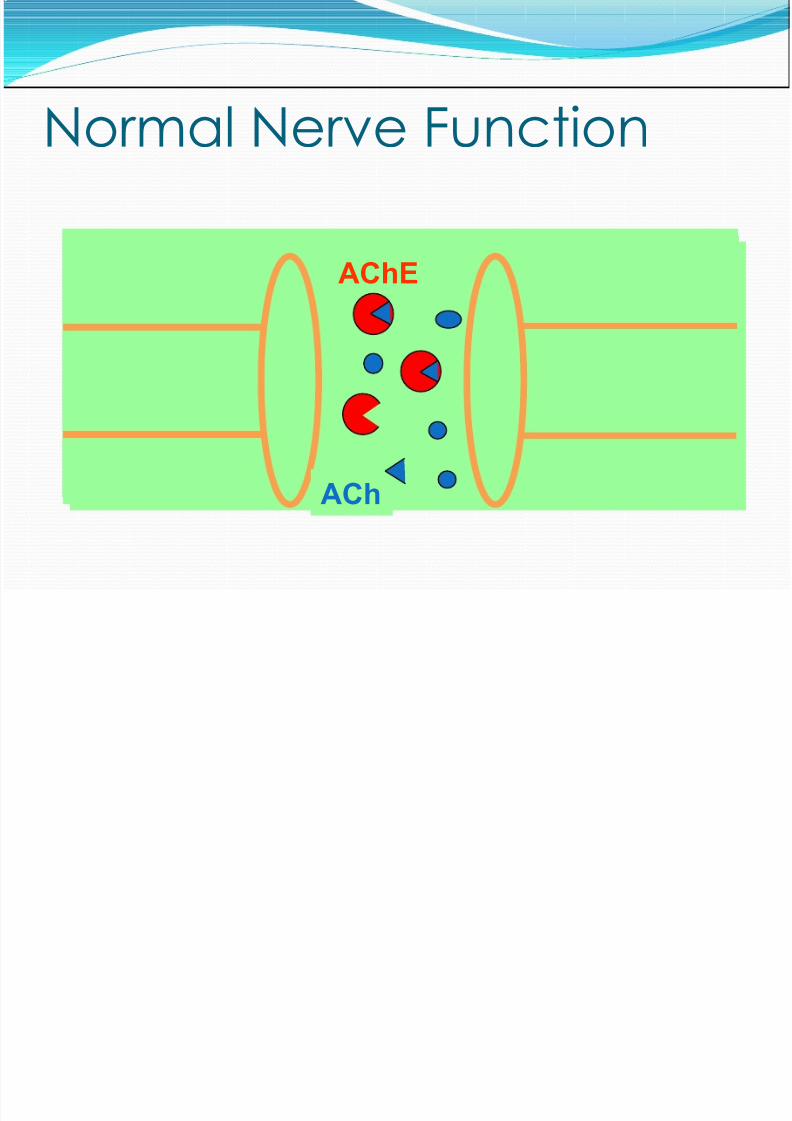
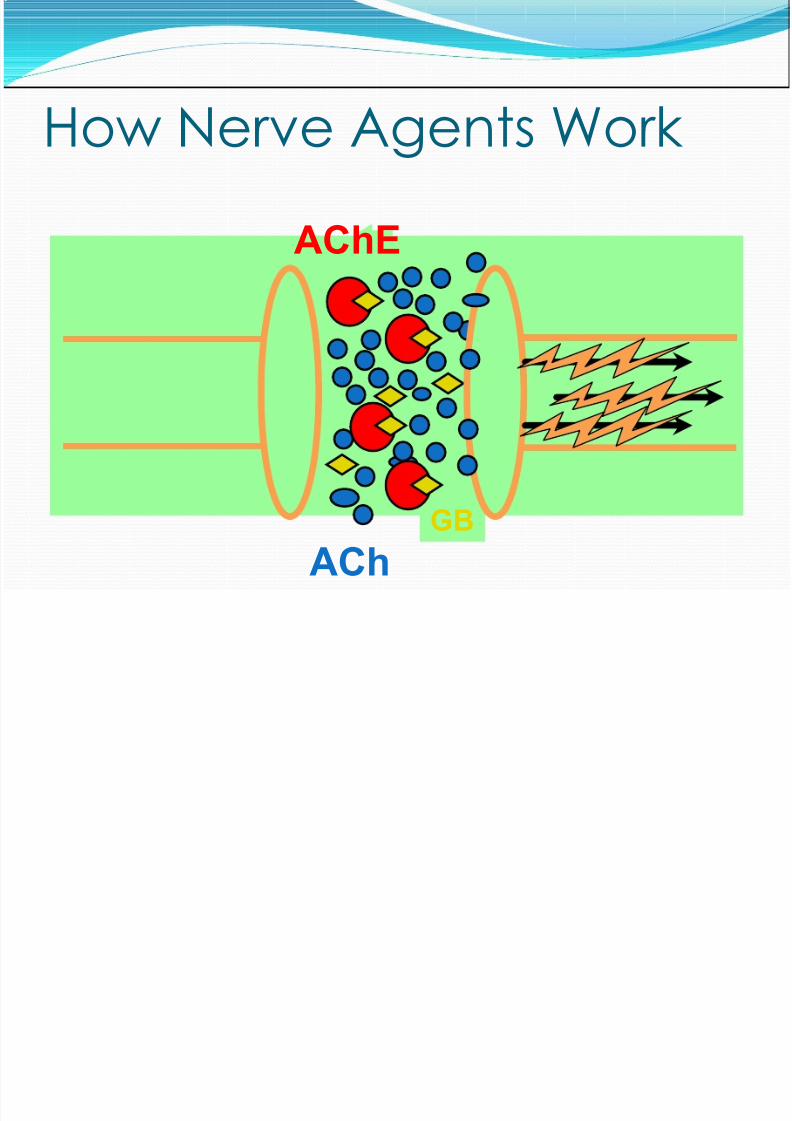
How it worksNerve agents block an enzyme calledacetylcholinesterase.This enzyme is normally responsible for
breaking down acetylcholine that hasbeen used as a neurotransmitter to glandsand smooth muscle.When it is blocked, the acetylcholine
remains in the synapse, causing glands tosecrete, and muscles to constrict.Death is due from lack of oxygen.
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 5/54
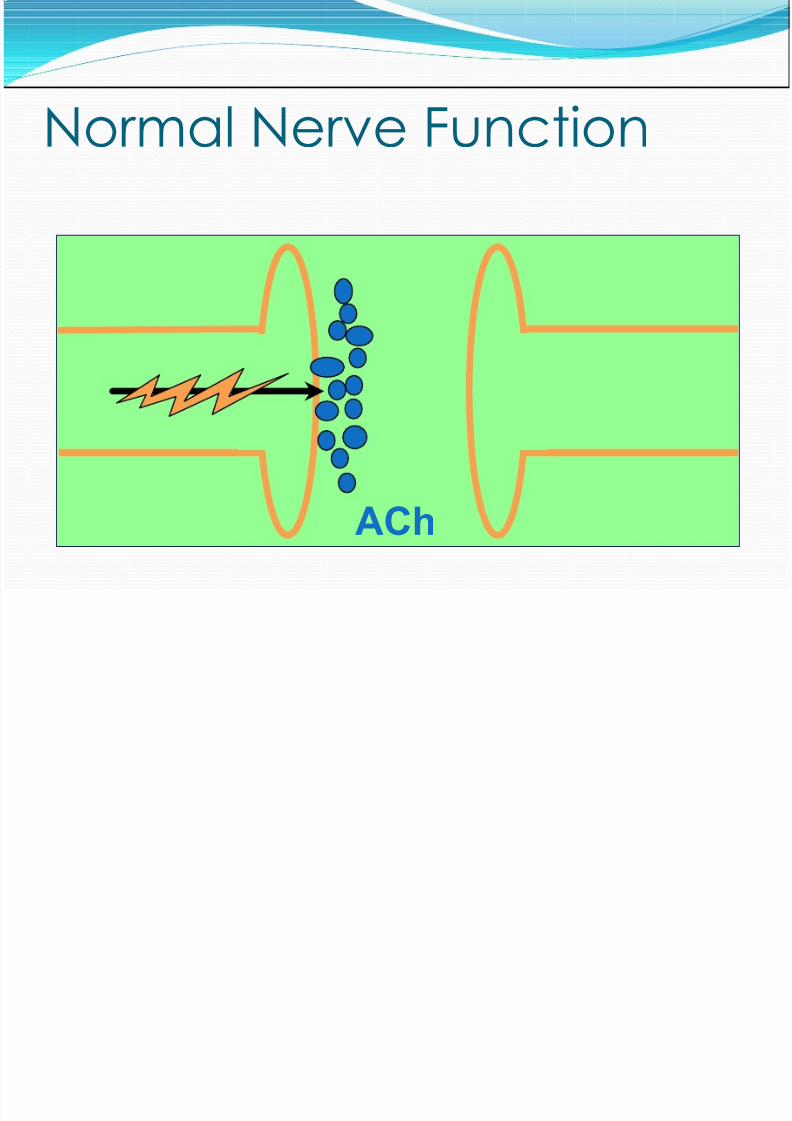
Normal Nerve Function
ACh
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 6/54
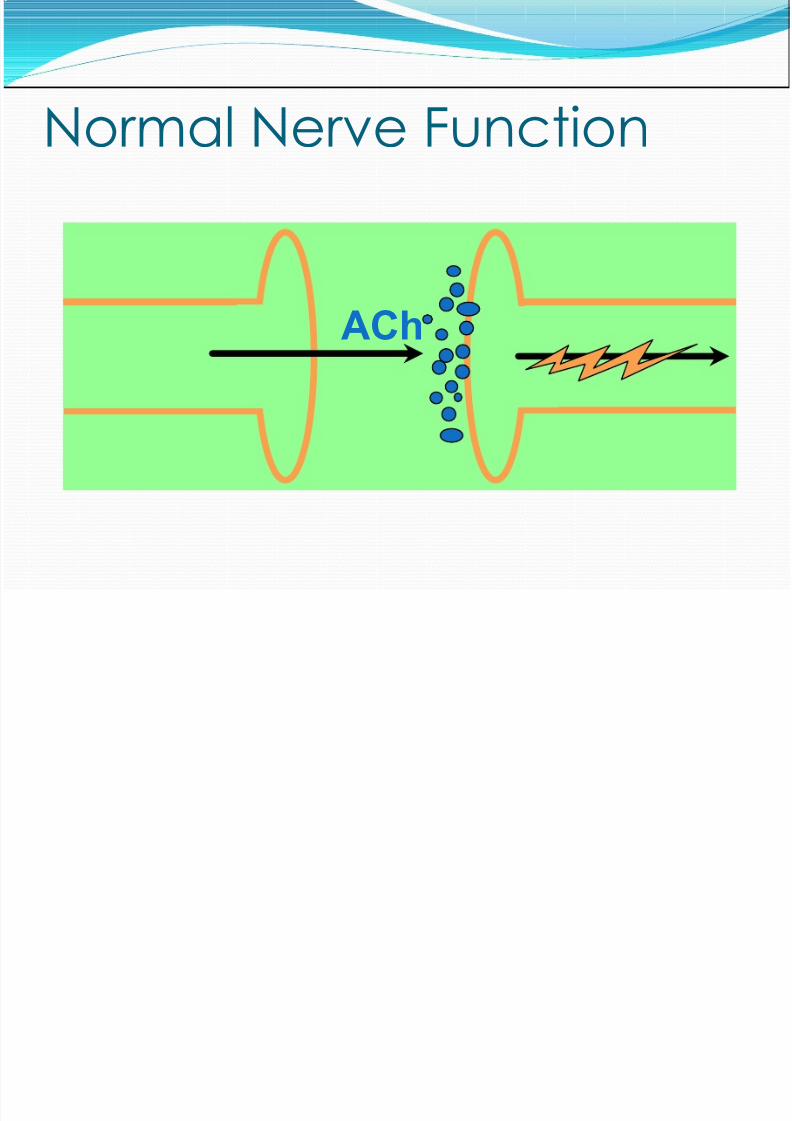
Normal Nerve Function
ACh
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 7/54
Normal Nerve Function
ACh
AChE
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 8/54
How Nerve Agents WorkAChE
AChGB
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 9/54
EffectsAcetylcholine is a transmitter in two kinds of
synapses, meaning nerve agents function in twowaysMuscarinic Receptors
Smooth muscleGlands
Nicotinic ReceptorsSkeletal musclesAutonomic ganglion
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 10/54
How it works cont.The interruption in communication causesoverstimulation of these organs or musclescausing hyperactivity
Effects are seen in the skeletal muscles andsmooth muscles (GI tract)
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 11/54
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 12/54
How it works cont.If the agent is inhaled, bronchoconstrictionoccursSudden loss of consciousness and convulsions
may follow
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 13/54
Effects: NicotinicSkeletal muscle
FasiculationsLocalizedtwitchingLeads to
flaccidityGanglion
TachycardiaHypertension
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 14/54
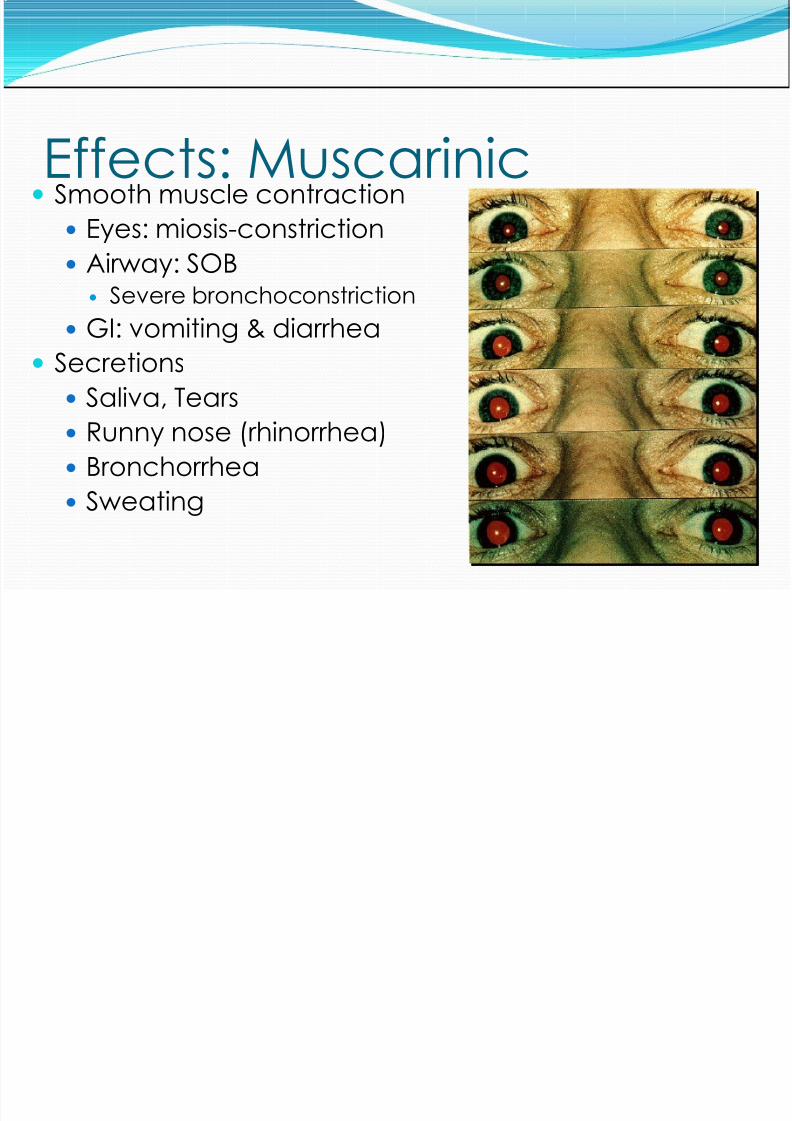
Effects: MuscarinicSmooth muscle contraction
Eyes: miosis-constriction
Airway: SOBSevere bronchoconstrictionGI: vomiting & diarrhea
SecretionsSaliva, TearsRunny nose (rhinorrhea)BronchorrheaSweating
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 15/54
Overall EffectsHeart Rate: tachy or bradyCan get arrhythmiasCentral Nervous System
AcuteLoss of consciousnessSeizuresApnea
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 16/54
Remember SLUDGEM
SalivationLacrimation
UrinationDefecationG astric upsetEmesisMiosis (pupil constriction), muscle twitching
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 17/54
Symptoms[4,5]
Mild Moderate
Blurred vision, miosis(excessive constriction of
the pupils)Excessive, unexplainedteary eyesExcessive, unexplainedrunny nose
Increased salivation, suchas sudden drooling
Chest tightness ordifficulty breathing
Tremors throughout thebody or musculartwitchingNausea and/or vomitingUnexplained wheezing,coughing, or increased
airway secretionsAcute onset of stomachcrampsTachycardia orbradycardia (abnormallyfast or slow heartbeat)
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 18/54
Severe Symptoms [4,5] Strange or confused behaviorSevere difficulty breathing or copioussecretions from lungs/airway
Severe muscular twitching and generalweaknessInvoluntary urination and defecationConvulsions
Loss of consciousnessRespiratory arrest (possibly leading to death)
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 19/54
No amount of atropine will stopseizures.
Treatment endpoint is airwayimprovement with decreased salivation
and rhinorrhea
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 20/54
Signs and Symptoms of Vapor ExposureMild exposure
Miosis (dim vision, eye pain), rhinorrhea, slightdyspnea
Moderate exposurePronounced dyspnea, nausea, vomiting,diarrhea, weakness
Severe exposure
Immediate loss of consciousness, seizures,apnea, and flaccid paralysis
Vapor effects occur within seconds,peak within minutes; no late onset
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 21/54
Signs and Symptoms of Liquid Exposure
Mild exposure (up to 18 hours)Localized sweatingFasciculationsNo miosis
Moderate exposure ( to 18 hours)Gastrointestinal effectsMiosis uncommon
Severe exposure (<30 minutes)Sudden loss of consciousnessSeizures, apneaFlaccid paralysisDeath
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 22/54
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 23/54
Types of Nerve AgentsSarin (GB)Soman (GD)
Tabun (GA)V agent (VX)
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 24/54
Physical PropertiesGas vs. liquid4-6x denser than air
soluble in waterG agents disperse within several hoursVX will persist for weeksVX>GD>GB>GA lethality
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 25/54
PersistencyTerm used to describe how long the agent willstay on a surface before it evaporatesPersistent agents remain on a surface usuallylonger than 24 hours.
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 26/54
Volatilitythe ease with which a chemical changes from aliquid to a gas; the tendency of a chemicalagent to evaporate.
Name Code Odor Features Onset of Volatility Route of
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 27/54
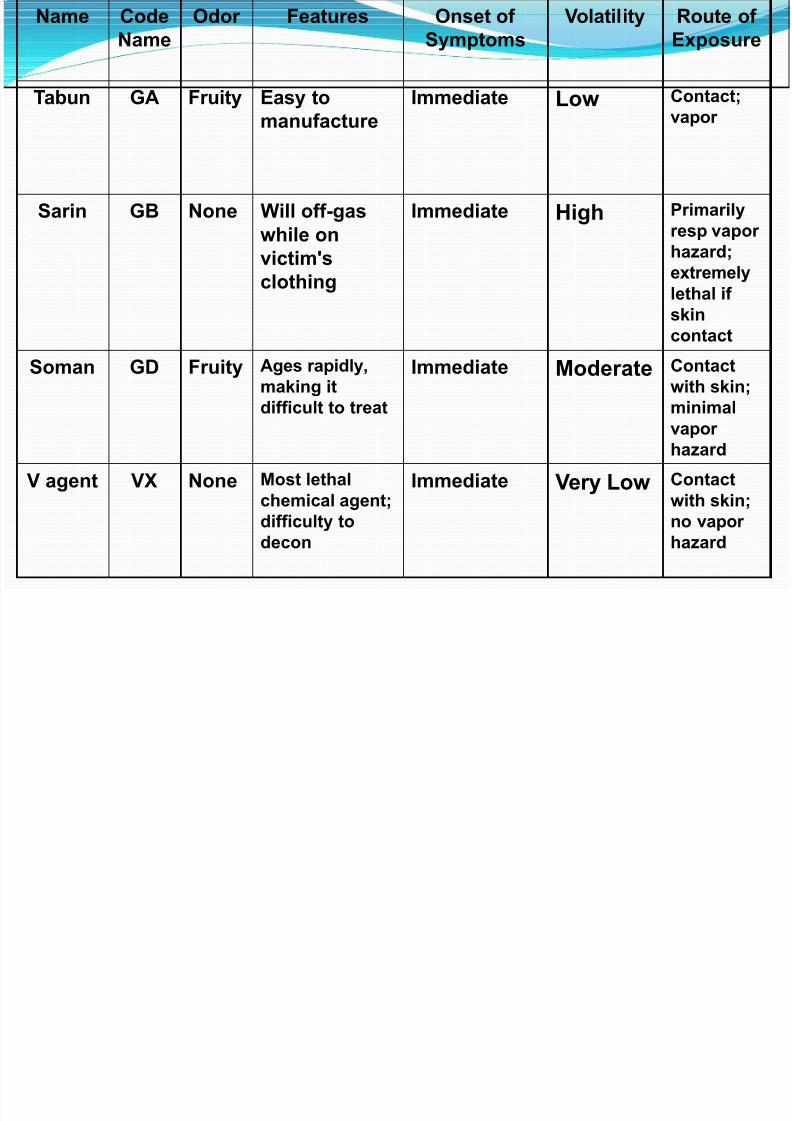
Name CodeName
Odor Features Onset ofSymptoms
Volatility Route ofExposure
Tabun GA Fruity Easy tomanufacture
Immediate Low Contact;vapor
Sarin GB None Will off-gaswhile onvictim'sclothing
Immediate High Primarilyresp vaporhazard;
extremelylethal ifskincontact
Soman GD Fruity Ages rapidly,making itdifficult to treat
Immediate Moderate Contactwith skin;minimalvaporhazard
V agent VX None Most lethalchemical agent;difficulty todecon
Immediate Very Low Contactwith skin;no vaporhazard
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 28/54
Transporting Contaminated PatientsEMS personnel must be wearing PPE.If necessary, different triage categories of
contaminated patients may betransported together.Helicopters do not transportcontaminated patients.
Once an ambulance has been used tomove contaminated patients, it may onlybe used for contaminated patients untildecontamination is verified.
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 29/54
• Request specific staging information.• Maintain safe location upwind and uphill.• Pay strict attention to hot, warm and coldzones.• Activate ICS.
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 30/54
TriageImmediate : 2 or more body systems involved-airway, convulsing, decreased consciousness, nospontaneous respirationsDelayed : no immediate life threat, patientwithout symptoms OR has been given >4mgAtropine and is recovering… observe at least 18hours
Minimal: walking and talking, may only have dimvision, pinpoint pupils… observe 18 hours Expectant : inadequate resources, completearrest
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 31/54
Treatment
Airway supportAntidotes
Atropine2-PamChloride(pralidoxime Chloride)Diazepam (valium)
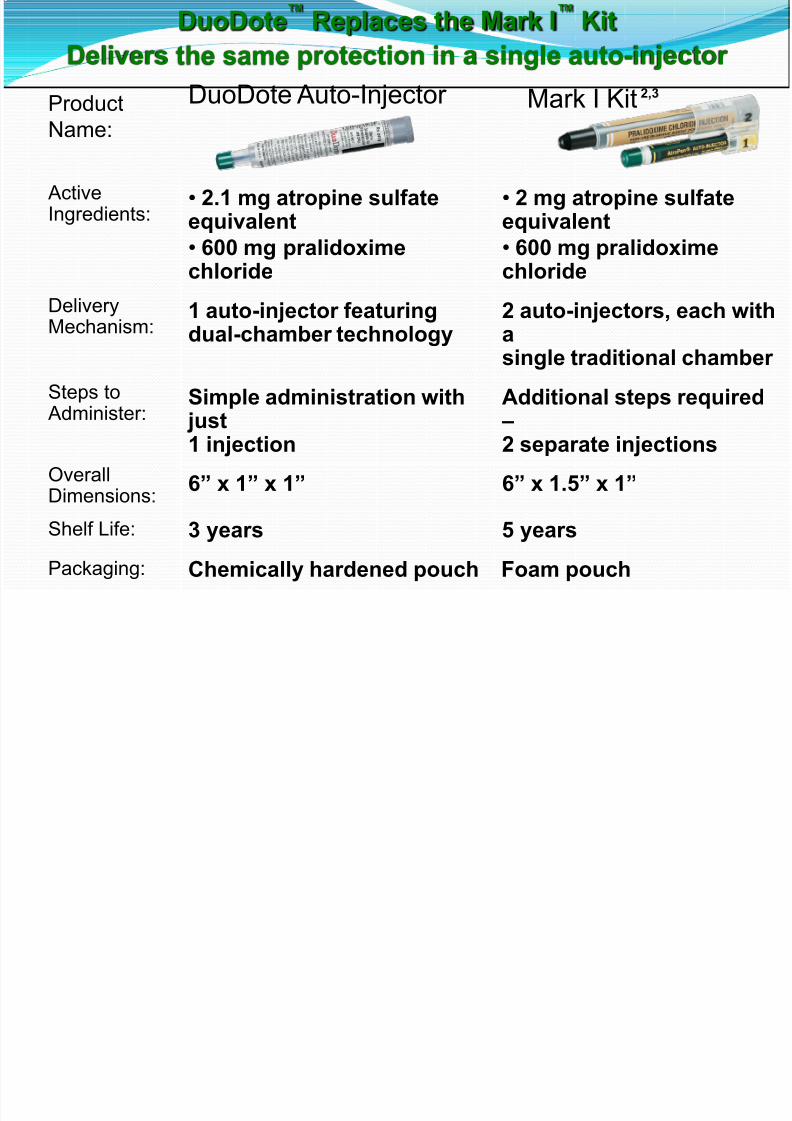
DuoDote ™ Has one auto-injector2mg Atropine and600mg 2-PamCl
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 32/54
AtropineWorks on muscarinic effectsDose until airway sx resolve, and secretions aredryingDo not rely on heart rate or pupil size
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 33/54
Pralidoxime (2PAM)Works like a “crowbar” byremoving nerve agent from
acetylcholinesteraseMore effective if given early, assome of the nerve agents bond“ages” to permanent in under 2minutes
AChE 2-PAMCl
Nerve Agent
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 34/54
What is DuoDote™? Developed by Meridian Medical Technologies as astreamlined, easy-to-use replacement for the Mark IKitFDA-approved for emergency medical services (EMS)use in the treatment of organophosphorus nerveagent and organophosphorus insecticide poisoning
Contains 2 antidotes in 1 auto-injector:2.1 mg of atropine in a 0.7-mL solution600 mg of pralidoxime chloride in a 2-mL solution
Features next-generation BinaJect™
delivery technology2 antidotes delivered sequentiallyinto separate areas of the muscleEasy to use: only 1 injection
with 1 needle
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 35/54
Where Does DuoDote
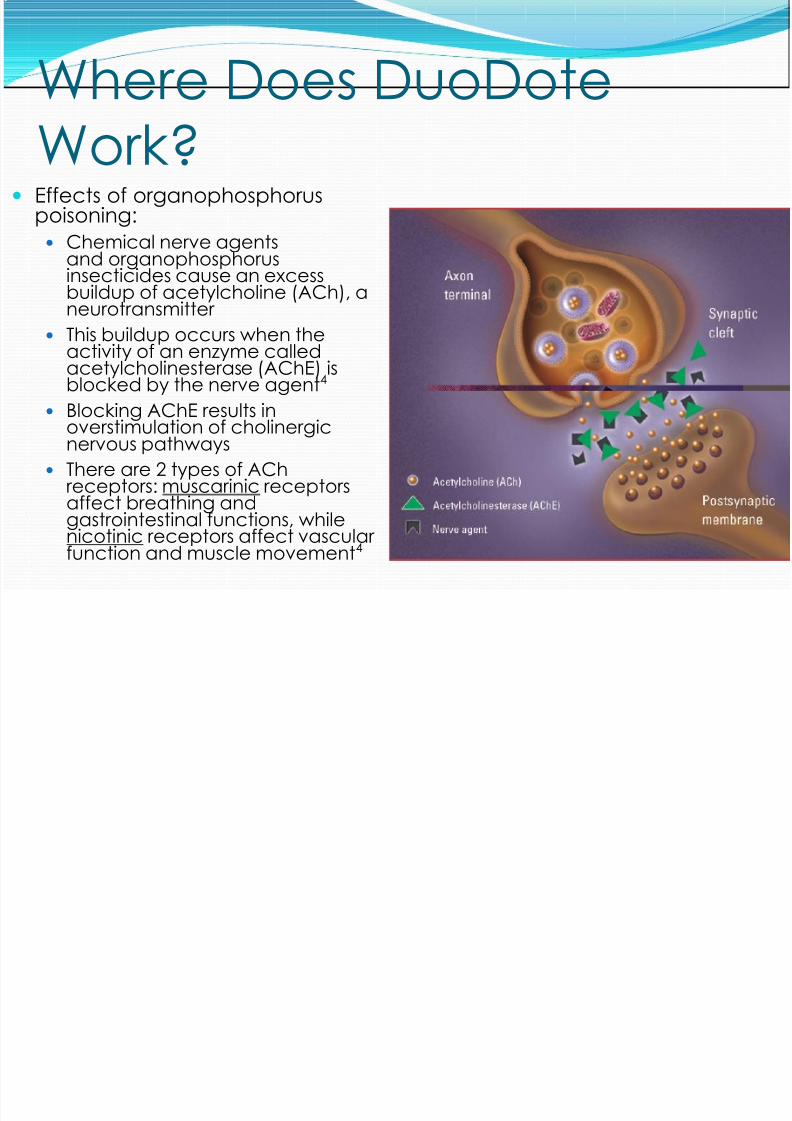
Work? Effects of organophosphoruspoisoning:
Chemical nerve agentsand organophosphorus
insecticides cause an excessbuildup of acetylcholine (ACh), aneurotransmitterThis buildup occurs when theactivity of an enzyme calledacetylcholinesterase (AChE) isblocked by the nerve agent 4
Blocking AChE results inoverstimulation of cholinergicnervous pathways
There are 2 types of AChreceptors: muscarinic receptorsaffect breathing andgastrointestinal functions, whilenicotinic receptors affect vascular
function and muscle movement4
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 36/54
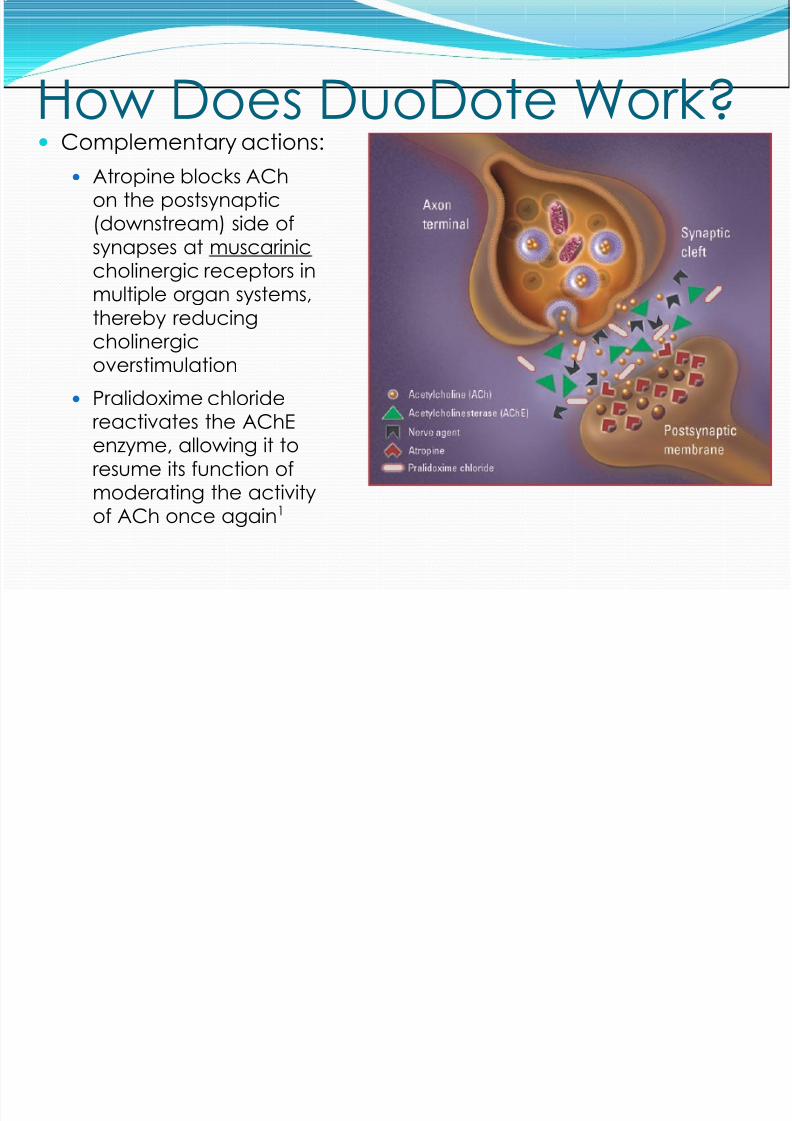
How Does DuoDote Work? Complementary actions:
Atropine blocks AChon the postsynaptic(downstream) side ofsynapses at muscariniccholinergic receptors inmultiple organ systems,thereby reducingcholinergicoverstimulation
Pralidoxime chloridereactivates the AChEenzyme, allowing it toresume its function ofmoderating the activityof ACh once again 1
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 37/54
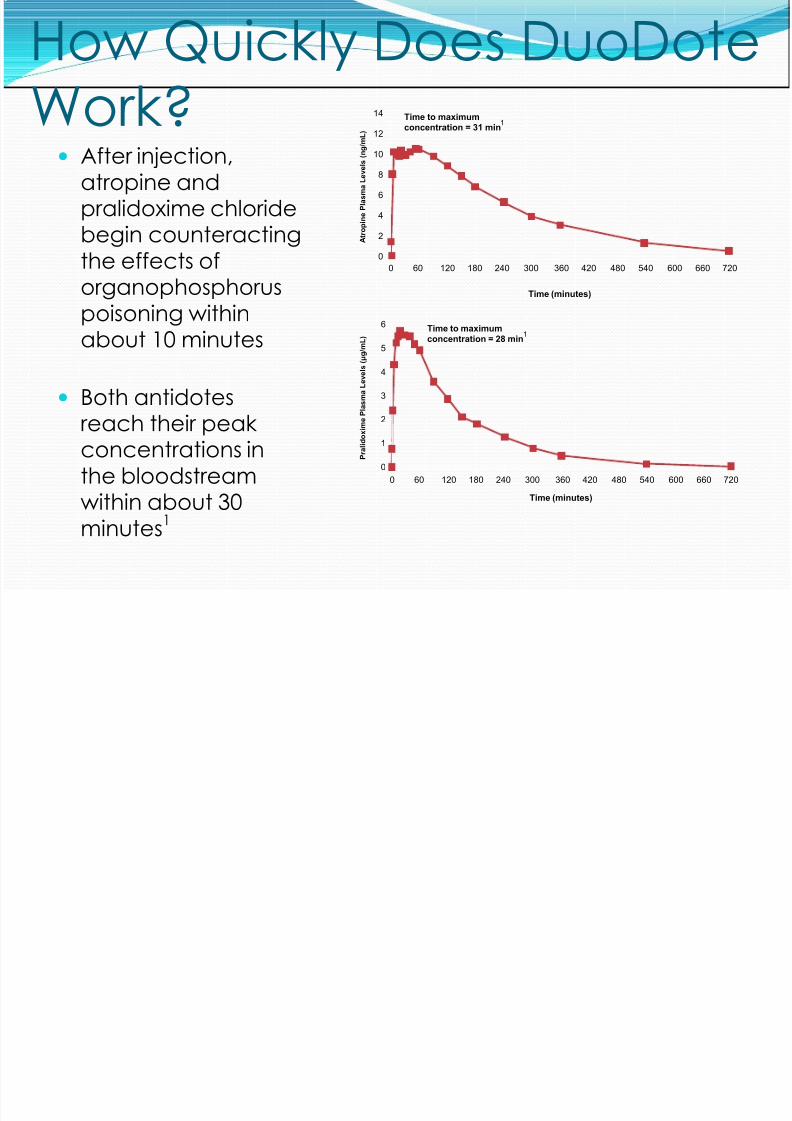
How Quickly Does DuoDoteWork?
After injection,atropine andpralidoxime chloridebegin counteractingthe effects oforganophosphoruspoisoning withinabout 10 minutes
Both antidotesreach their peakconcentrations inthe bloodstreamwithin about 30minutes 1
14
12
10
8
6
4
2
00 60 120 180 240 300 360 420 480 540 600 660 720
A t r o p
i n e
P l a s m a
L e v e
l s ( n g / m
L )
Time (minutes)
Time to maximumconcentration = 31 min
1
6
5
4
3
2
1
0 P r a
l i d o x
i m e
P l a s m a
L e v e
l s ( μ g
/ m L )
0 60 120 180 240 300 360 420 480 540 600 660 720
Time (minutes)
Time to maximumconcentration = 28 min
1
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 38/54
What Happened toMARK-1?
Mark-1 kits are no longer available for use.DuoDote has replaced themHere is a slide that compares them side by side
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 39/54
D D t I j ti
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 40/54
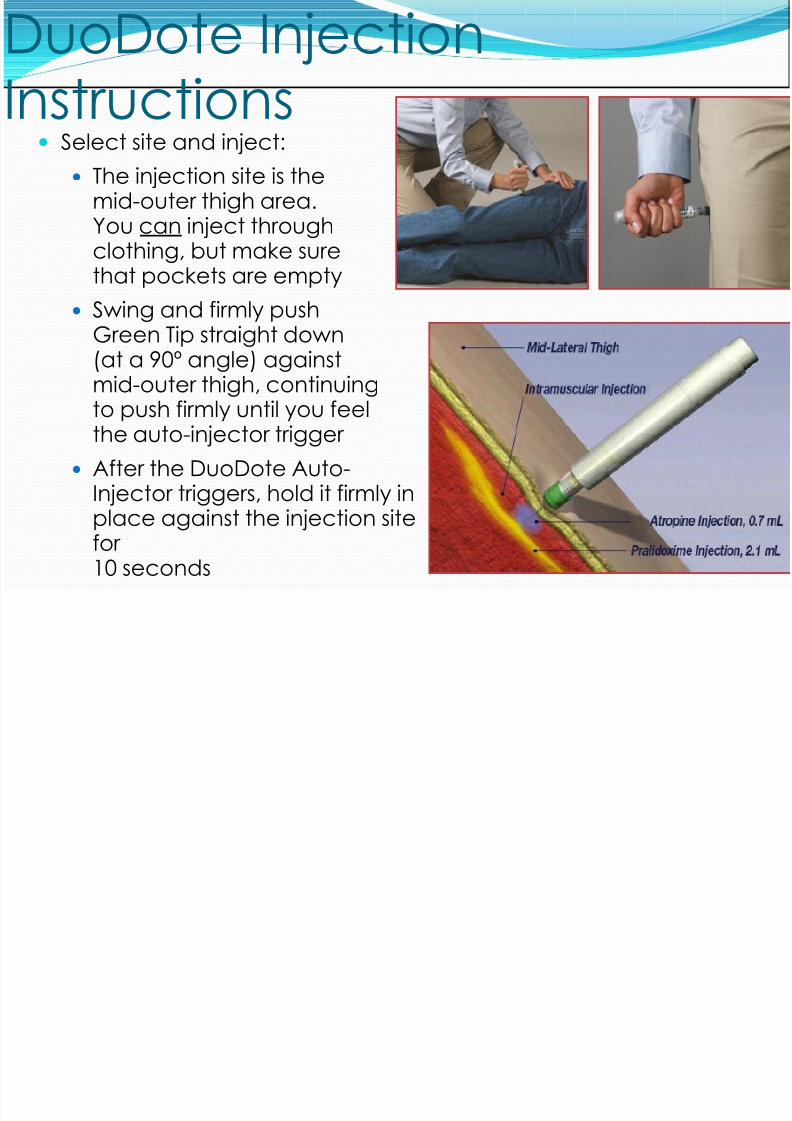
DuoDote InjectionInstructions
Select site and inject:The injection site is themid-outer thigh area.You can inject throughclothing, but make sure
that pockets are emptySwing and firmly pushGreen Tip straight down(at a 90º angle) againstmid-outer thigh, continuing
to push firmly until you feelthe auto-injector trigger
After the DuoDote Auto-Injector triggers, hold it firmly inplace against the injection sitefor10 seconds

8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 41/54
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 42/54

8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 43/54
Self TreatmentDo not place finger
over either end!Upper outerquadrant ofbuttocks is best spotHold in place for 10seconds
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 44/54
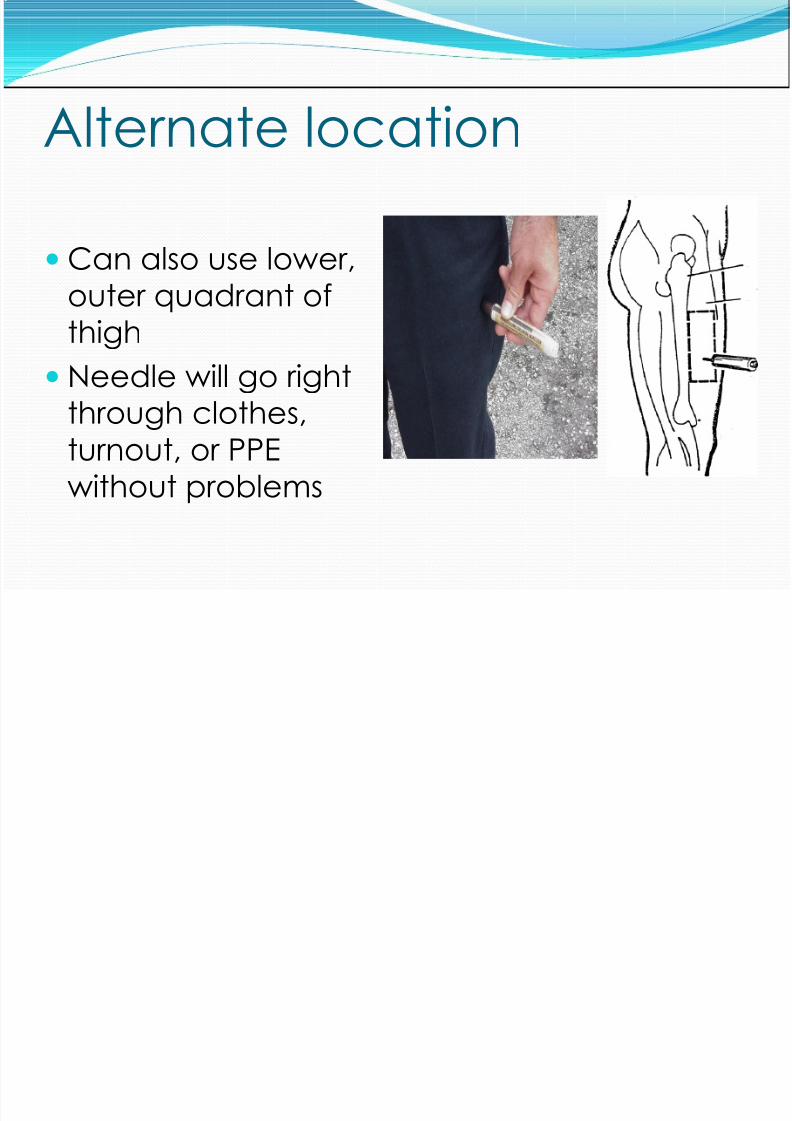
Alternate locationCan also use lower,outer quadrant ofthighNeedle will go right
through clothes,turnout, or PPEwithout problems
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 45/54
Basic/Advanced Standing OrdersRoutine patient care: Assess for SLUDGEM(salivation, lacrimation, urination,defecation, gastric upset, emesis,miosis/muscle twitching)
Remove to cold zone afterdecontamination and monitor forsymptomsTreatment using DuoDote ™ autoinjectors
self and peer onlyTreatment using DuoDote ™ autoinjectorsto public in emergency stockpile releaseonly
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 46/54
Basic Standing OrdersAntidotal therapy should be started as soon assymptoms appear.
All injections must be given IMTreatment using DuoDote ™ autoinjectors selfand peer onlyTreatment using DuoDote ™ autoinjectors topublic in emergency stockpile release only
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 47/54
Adolescent/Adult Basic
Standing Orders2 or more minor symptoms
One DuoDote ™ kit Reassess: if more severe symptoms appear within10 minutes administerTwo additional DuoDote ™ kits
Initial Moderate SymptomsTwo DuoDote ™ kits
Initial Severe SymptomsGive Three DuoDote kits ANDOne autoinjector of Diazepam 10 mg
May repeat DuoDote ™ kit every hour for threehours
Basic Standing Orders:
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 48/54
Basic Standing Orders:PEDIATRIC
DuoDote ™ may be used for pedi patientsin life threatening situation w/ exposuresymptomsChild 13-25kg (29 - 55lb) – One DuoDoteChild 26-50kg (56 - 110lb) – Up to TwoDuoDote kits based on progression ofsymptomsChild over 51kg (>110lb) – Up to ThreeDuoDote kits based on progression andseverity of symptoms
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 49/54
Paramedic Standing Orders:PEDIATRIC
Children <12 kg (26 lbs):Use of DuoDote kit is not recommendedIf no other source available after 90 min mayconsider using one DuoDote kit.
If child is seizing and >26 (> 57lbs)kgMay use one Adult Diazepam injector
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 50/54
Provider ProtectionIf a first responder display symptoms:Notify dispatch immediatelyEvacuate areaDo not reenter until cleared by HazmatRemove clothing and decontaminateTreatment basic and paramedic same as formass casualty
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 51/54
Provider TreatmentUse only if nerve agent symptoms are present.DuoDote ™ kits offer no prophylactic protectionand use prior to appearance of symptoms maybe harmful. All injections must be given IM.
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 52/54
Accidental ODIf First Responder accidentally gives Mark 1 kit tothemselves without being exposed to nerveagent
HotRedUnable to sweat (dry)
ConfusionNeed to be kept in cool, controlled environmentuntil wears off
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 53/54
References[1] Watson WA, Litovitz TL, Klein-Schwartz W, et al. 2003 AnnualReport of the American Association of Poison Control CentersToxic Exposure Surveillance System. Am J Emerg Med.2004;22:335-404
[2]Department of Health and Human Services. Centers for DiseaseControl and Prevention. Third National Report on HumanExposure to Environmental Chemicals . Atlanta, GA: NationalCenter for Environmental Health; 2005 NCEH Pub. No. 05-0570.[3]Olson KB. Aum Shinrikyo: once and future threat? Emerg InfectDis. 1999;5:512-516.[4]Cannard K. The acute treatment of nerve agent exposure. JNeurol Sci , 2006;249:86-94[5]Department of Health and Human Services. Centers forDisease Control and Prevention. Third National Report on HumanExposure to Environmental Chemicals . Atlanta, GA: National
Center for Environmental Health; 2005;NCEH Pub No. 05-0570
8/11/2019 ATPM Slides
http://slidepdf.com/reader/full/atpm-slides 54/54



















![Apha slides tfah sanyal slides[1]](https://img.pdfslide.us/doc/110x75/557c653ad8b42a855d8b46d1/apha-slides-tfah-sanyal-slides1.jpg)