Embed Size (px)
Citation preview

CLINICAL FOCU
SVol 2 September 2010 Clinical Pharmacist 291
By Christine Clark, PhD, FRPharmS
Atopic eczema is a relapsing and remitting disease.Managing the condition focuses on reducing thenumber of relapses (also known as “flares”) and
ensuring their prompt treatment when they occur. Some aspects of management, in particular the use of
emollients, will also be relevant to the management ofother types of eczema. However, a full discussion of themanagement of other types of eczema is beyond the scopeof this article.
Principles of managementManaging atopic eczema in primary care involves:
� Identification and avoidance of trigger factors� Implementation of a stepped-care plan where
treatment is tailored to disease severity (treatment isstepped up if there is deterioration and steppeddown once a flare is under control)
� Referral for specialist care when conventionalmeasures are ineffective1
Avoidance of trigger factorsThe first step in eczema management is avoiding, as muchas possible, factors that can trigger a flare. Helping people
to identify their own or their children’s trigger factors is animportant part of supporting self-management (see Box 1).
Stepped-care planThe National Institute for Health and Clinical Excellenceguidance for atopic eczema in children1 recommends theuse of a stepped-care plan (see Figure 1, p295), similar tothat recommended for the management of asthma.Although the NICE guidance is for children, the principleof stepped care is equally applicable to adults.
EmollientsEmollients are the mainstay of eczema treatment. Theyrestore the integrity of the skin barrier and should be usedto keep the skin in good condition, even when it is clear ofeczema. If used correctly, emollients can help maintain orrestore the suppleness and pliability of the skin, reducecorticosteroid requirements and improve cosmeticappearance. Emollient products include creams,ointments, lotions, bath additives and soap substitutes.
Although there is a lack of good quality evidence tosupport the use of emollients for the treatment of eczema,there can be little doubt about their usefulness. Anemollient forms an oily layer over the skin that preventswater evaporation. The water, trapped in the stratumcorneum, passes into the corneocytes, which swell, closingintercellular gaps.
Emollients can also penetrate deep into the stratumcorneum and mimic the barrier effects of deficient lipids.
Complete emollient therapy To be effective, emollientsneed to be applied often and generously. Manydermatologists recommend “complete emollient therapy”(see Box 2, p294).2
This involves the frequent application of emollientcreams or ointments, the use of bath oil when bathing orshowering and routine use of an emollient soap substitute.Regular soaps and detergents (especially bubble baths)
The education of patients and their carers on avoiding trigger factors, using emollients effectively and adopting a stepped management plan is essential for successful treatment of eczema
Atopic eczemamanagement
Box 1: Trigger factors for atopic eczema
SUMMARYThe treatment of atopic eczema is centred around identification andavoidance of trigger factors, effective use of emollients and theimplementation of a stepped-care plan for managing flares.
The stepped-care model involves identifying the severity of a patient’seczema at any particular time and providing treatment as appropriate.Mild atopic eczema can usually be managed with emollients alone or incombination with topical corticosteroids. Moderate eczema may requirethe addition of immunotherapeutic medicines such as topical tacrolimus.Systemic immunosuppressants might be needed for severe atopic eczema.
FACTOR EXAMPLE EXPLANATION
Irritation Soaps and detergents Removal of lipids from skin andactivation of skin proteases
Abrasive clothing Direct physical irritationbecause of scratchy texture
Extremes of temperature orhumidity
Drying effect on skin
Psychologicalstress
Psychological stress causedby life events
Some people respond withhabitual scratching, whichexacerbates eczema
Foodhypersensitivity
Cow’s milk, eggs, soya,wheat, fish, nuts
Only likely to be a factor inabout 10% of children, mainlyunder three years of age
Allergens House dust mite Allergens in house dust mitefaeces
Animal dander Allergens in animal saliva
Toiletries and cosmetics Allergens include perfumes andpreservatives
Moulds and pollens Plant or mould allergens
CP, Sept, CF2, p291_Layout 1 8/24/2010 1:32 PM Page 291

CLIN
ICAL
FOC
US
294 Clinical Pharmacist September 2010 Vol 2
Lanolin is a good emollient and, contrary to popularbelief, is a weak contact sensitiser. Large studies haveshown that the true incidence of lanolin sensitivity is verylow. Modern lanolin-containing products use highlypurified, hypoallergenic lanolin that is well tolerated. Onenew product (Evolve) contains highly purified lanolin in aspray form, which may be useful for those who dislike thefeel of creams.
In addition to the basic ingredients, many emollientproducts also contain other therapeutically activesubstances.
Humectants attract water from the dermis into theepidermis. They can improve epidermal barrier functionand increase hydration of the stratum corneum. Emollientsthat contain humectants are particularly useful forrehydrating dry, flaky skin. Commonly used humectantsinclude urea, glycerin, polyethylene glycol and lactic acid.
Colloidal oatmeal is added to emollients (eg, Aveeno)for its soothing and antipruritic properties.Lauromacrogols, also antipruritic, are contained inproducts such as Balneum Plus and E45 Itch.
Adding antiseptics to emollients is said to be helpful incontrolling flares. Such products (eg, Oilatum Plus) do notreplace specific treatment for infected eczema.
Some emollients contain potential irritants (eg, benzylalcohol) that can exacerbate eczema; a list of sensitisingexcipients is available in the British National Formulary.
Aqueous cream is unsuitable as a leave-on emollient formany people because it contains the anionic surfactantsodium lauryl sulphate, which has well documentedirritant effects. It also contains chlorocresol orphenoxyethanol, which can contribute to the irritationfurther. Despite this, aqueous cream can be used as a wash-off product (ie, as an emollient soap substitute).3
Patients should always test a new product on a smallarea of skin before using it on large or sensitive areas.
must be avoided at all times. Educating patients and theircarers on how to use the emollients is essential.
Patient acceptability To ensure that emollients areused on a regular basis, finding a product that matches apatient’s needs and preferences is essential (children witheczema often complain that the worst aspect of the diseaseis “the creams”).
Finding the most suitable emollient is usually a matterof trial and error. In general, greasier oil-based productsare more efficacious, but they are less acceptable topatients and there is often a trade-off between efficacy andcosmetic acceptability (eg, smell or consistency).
Different emollients may be required for particularareas of the body, for example a rich emollient for dry skinon the limbs and a lighter product for the face. Patientsmay be more prepared to use a richer (greasier) emollientat night than during the day. Richer products may also beneeded in the winter to combat the drying effects of coldweather and central heating.
Patients, including children, should be encouraged totry a range of emollients to help them to find those theylike best. Some hospitals have now developed “trial kits” ofemollients specifically for this purpose.
Formulation considerations Greasier emollients areharder to spread and more occlusive than lighteremollients.
Box 2: Complete emollient therapy2
Emollient cream or ointment should be:
� Used liberally (500g per week for an adult is not unusual) � Applied gently but quickly with clean hands � Applied at least half an hour before any topical corticosteroid to
avoid dilution of the corticosteroid or its spread to unaffected areas� Warmed before use if more easy application is required (by standing
it in the airing cupboard) � Cooled before use if itch is a problem (by storing it in the fridge)� Applied frequently: after washing or bathing (to replace the natural
oils lost); and several times during the day (at least twice a day, butideally three to four times). Additional emollient should be applied inextreme weather
Emollient soap substitute should be:
� Used for washing instead of conventional soaps and wash products(which can be drying). Ordinary soap, “moisturising” soap or bubblebath should never be used
� Applied to dry skin then rinsed off with water. Although theseproducts do not lather like soap, they cleanse the skin effectively
Emollient bath oil should be:
� Used as another means of moisturising — they leave a fine film ofemollient on the skin after bathing
� Added to a warm bath (but not too hot since this exacerbates itching);15ml should be added to an adult bath and 5ml to a baby bath. Afterbathing skin should be patted dry (not rubbed, because this can alsoexacerbate itch)
CP, Sept, CF2, p291_Layout 1 8/24/2010 1:32 PM Page 294

CLINICAL FOCU
SVol 2 September 2010 Clinical Pharmacist 295
Emollients and corticosteroids Correct emollient usecan reduce a patient’s requirement for topicalcorticosteroids (ie, steroid-sparing effect).4 It can behelpful to point this out to people who are apprehensiveabout using corticosteroids. As a general rule, patientsshould use about 10 times as much emollient as topicalcorticosteroid preparation.
Topical corticosteroidsFlares of eczema should be treated with topicalcorticosteroids, which inhibit the production and action ofinflammatory mediators, reducing inflammation and itch.
The least potent corticosteroid to produce the requiredeffect should be prescribed. However, this does not meanthat treatment should be started with the weakest topicalcorticosteroid — the strength selected should matchdisease severity. In general, a short burst of treatment witha potent or moderate corticosteroid is preferable toprotracted under-treatment.
Where the skin is thin, such as on the face, genitals andflexures, a mild corticosteroid (eg, hydrocortisone) shouldbe used. Mild-to-moderate eczema in other areas of thebody can be treated for one to two weeks with a moderatecorticosteroid (eg, clobetasone butyrate). Potentcorticosteroids (eg, mometasone furoate) are required formoderate-to-severe eczema and for areas where the skin isthick (eg, scalp, palms of hand and soles of feet). Infantsyounger than one year of age should only be treated witha mild potency preparation such as hydrocortisoneointment 1%. It is important to remember that the potencyof a topical corticosteroid depends on both theformulation and the corticosteroid itself. A full list of therelative potencies of topical corticosteroid preparations isavailable in the British National Formulary.
Topical corticosteroids should be applied once or twicea day. Ointments are suitable for dry, thick or scaly lesions,whereas creams are more appropriate when the skin isoozing or infected (because the area should not beoccluded).
Community pharmacists can provide over-the-countertopical corticosteroids for eczema as described below:6
� Hydrocortisone 1% creams and ointments can beprovided to treat mild-to-moderate atopic eczema.These products are useful to treat flares, but shouldnot be used for more than one week withoutmedical advice. Patients who have not previouslybeen diagnosed with atopic eczema should bereferred to their GP, as should patients whosecondition is widespread or severe. It isinappropriate to supply topical hydrocortisone forchildren under 10 years of age or for pregnantwomen (unless it has been recommended by a GPor other doctor, who has not provided aprescription for it)
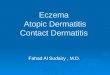
Figure 1: Model of stepped care adapted from the NICE guidance for the management of atopic eczema in children1
STEP TREATMENT UP OR DOWN ACCORDING TO ECZEMA SEVERITY
CLEAR
Emollients
MILD
Emollients
Mild potency topicalcorticosteroids (or emollients alone)
MODERATE
Emollients
Topical corticosteroidsBody: moderate potency for
seven to 14 days Face/neck: mild potency for
three to five days
Topical calcineurin inhibitorsBody: tacrolimus
Face/neck: tacrolimus or pimecrolimus
Bandages
SEVERE
Emollients
Topical corticosteroidsBody: potent for seven to 14 days Face/neck: moderate potency for
three to five days
Topical tacrolimus
Bandages
Phototherapy
Systemic therapy
�CORRECTEMOLLIENT USECAN REDUCE APATIENT’SREQUIREMENT FORTOPICALCORTICOSTEROIDS
�Sh
eila
Terry
| SP
L
CP, Sept, CF2, p291_Layout 1 8/24/2010 1:32 PM Page 295

CLIN
ICAL
FOC
US
296 Clinical Pharmacist September 2010 Vol 2
� Clobetasone butyrate 0.05% cream can beprovided over the counter for the short-termtreatment and control of small patches of atopiceczema for patients over 12 years of age
The possible local and systemic side effects ofcorticosteroids are well recognised but often exaggerated.Side effects usually only occur after using potentcorticosteroids for a long time. The incidence and severityof side effects are determined by the area treated,thickness of the skin, potency of the preparation andduration of treatment. Greater absorption occurs wherethe skin is damaged and raw.
Important counselling points for topical corticosteroidsinclude:
� The importance of not using topical corticosteroidpreparations as emollients
� The difference between potency and concentration� The amount of topical corticosteroid to apply. To
cover an area twice the size of the flat of thepatient’s hand, the patient should be instructed touse one “fingertip unit” (that is the amount ofcream that covers from the tip of the index fingerto the first crease of the finger when squeezed fromthe tube)
Pharmacists should always take care not to confuseclobetasol (very potent) with clobetasone (moderate).Mix-ups with these products can also arise on computer-generated prescriptions.
Anti-infective agentsPrompt treatment of infected eczema is important whenmanaging flares. Moderate-to-severe bacterial infectionwith Staphylococcus aureus (identified by weeping or brokenskin) should be treated using oral antibiotics such asflucloxacillin or erythromycin. Oral antibiotics shouldonly be used for a short period (about seven days) tominimise the risk of resistance and sensitisation.
There is no evidence that topical antibiotic andcorticosteroid combination products are any more
effective than topical corticosteroids alone and, given therisk of bacterial resistance developing, they are notrecommended.
Sedating antihistaminesSedating antihistamines can be helpful for some patients.They are taken at night and are reported to provide benefitby reducing itching and allowing the patient to have agood night’s sleep.
Neither promethazine nor alimemazine is licensed foruse in children under two years of age. However,hydroxyzine is licensed for use for babies of six months ofage and older.
Severe atopic eczemaPeople with atopic eczema that fails to respond toemollients, topical steroids and avoidance of triggerfactors should be referred to a specialist for ongoingmanagement.
Topical immunomodulators In recent years, topicalimmunomodulators (tacrolimus and pimecrolimus) havebeen used for the treatment of atopic eczema. Thesemedicines can be helpful when there is a risk of seriousside effects with topical corticosteroids or when eczema isnot controlled with topical corticosteroids. Topicalpimecrolimus is used to treat mild-to-moderate atopiceczema, whereas topical tacrolimus is used for thetreatment of moderate-to-severe atopic eczema.
Tacrolimus and pimecrolimus are both inhibitors ofcalcineurin phosphatase, a key enzyme in the activation ofT cells and propagation of the inflammatory response.
NICE guidance suggests that tacrolimus may be usedin three situations:6
� As an alternative to potent corticosteroids that wouldbe inappropriate on sensitive areas such as the face
� When potent corticosteroids would otherwise beneeded most of the time
� When there is evidence of corticosteroid-inducedskin damage
Tacrolimus is also approved for maintenance treatment(applied twice a week) for up to 12 months to prevent flares.
The main side effect of tacrolimus and pimecrolimus isa burning sensation in the skin. Patients should be advisedto persevere with treatment because this effect usuallyonly lasts a few days.
Systemic immunosuppression For the treatment of severe atopic eczema, ciclosporin, azathioprine,methotrexate and systemic corticosteroids can be used.Most published data relate to ciclosporin.
In general, the doses used are lower than those usedafter organ transplantation and, for this reason, it issometimes described as immunomodulatory treatment(rather than immunosuppression). Patients receiving thesetreatments must be closely supervised and monitored byspecialists. Before starting treatment with azathioprine, apatient’s thiopurine methyltransferase enzyme activityshould be measured (deficiency increases the risk ofmyelosuppression).
Emollient baths can help to tackle atopic eczema
�THERE IS NOEVIDENCE THATTOPICAL ANTIBIOTICANDCORTICOSTEROIDCOMBINATIONPRODUCTS ARE ANYMORE EFFECTIVETHAN TOPICALCORTICOSTEROIDSALONE
�
Gust
oim
ages
| SP
L
CP, Sept, CF2, p291_Layout 1 8/24/2010 1:32 PM Page 296

CLINICAL FOCUS
298 Clinical Pharmacist September 2010 Vol 2
Phototherapy Phototherapy involves controlledexposure to ultraviolet (UV) light; UVA or UVB can beused. Because UVA alone has little effect, it is alwaysadministered in combination with a psoralenphotosensitiser. The mechanism of action forphototherapy is not fully understood but it is believed toinvolve immunosuppression. Long-term UV exposure isassociated with an increased risk of skin cancer and so thistype of treatment is reserved for the most severelyaffected patients and should be given by specialists withclose supervision and monitoring. Tanning beds cannotprovide the same controlled exposure and are not suitablefor treatment of severe eczema.
Wet-wrappingWet-wrapping is an approach that is usedfor extensive and severe eczema in young children. Itinvolves the application of a generous layer of emollient ormild topical corticosteroid cream, which is then coveredwith a wet cotton tubular bandage. This bandage is thenover-wrapped with a dry bandage. The bandages can beapplied over the whole body, apart from the scalp, and canbe left in place overnight. Close supervision is requiredwhen a topical corticosteroid is used because theocclusion increases the likelihood of absorption and therisk of systemic adverse effects.
Behavioural therapy Behavioural therapy using avariety of techniques (including hypnotherapy, cognitivebehavioural therapy and autogenic training) has also beenused as an adjunct to conventional treatment for eczema,often with good results.7
Patient educationNICE guidance1 recommends that all healthcareprofessionals should spend time educating people withatopic eczema (and children’s parents or carers) about thecondition and its treatment. The information should bereinforced at each consultation, especially addressingfactors that affect adherence.
To ensure prompt and appropriate treatment of flares,education must contain information about:
� How to recognise a flare (increased skin dryness,itching, redness, swelling and, for infants, generalirritability)
� How to manage a flare according to the stepped-care plan
� The importance of starting treatment for flares assoon as signs and symptoms appear and the need tocontinue treatment for approximately 48 hoursafter symptoms subside
Pharmacists can help to educate patients and theircarers about atopic eczema and how it is treated. Details ofpatient support groups can also be provided whereappropriate (see Box 3).
References1 National Institute for Health and Clinical Excellence. Atopic eczema in
children: Management of atopic eczema in children from birth up to theage of 12 years. December 2007. www.nice.org.uk/cg57 (accessed 13July 2010).
2 Cork MJ. Complete emollient therapy. In: Official Yearbook 1998; National Association of Fund Holding Practices Annual Review, London: Scorpio Publishing; 1998. pp159–68.
3 Cork MJ, Timmins J, Holden C, et al. An audit of adverse drug reactionsto aqueous cream in children with atopic eczema. The PharmaceuticalJournal 2003;271:747–8.
4 Mahrle G, Wemmer U, Matthies C. Optimised interval treatment ofeczema with fluprednidene. A multicenter double-blind study. Zeitschriftfür Hautkrankheiten 1989;64:766–8,773–4.
5 Joint Formulary Committee. British National Formulary. 59 ed. London:British Medical Association and Royal Pharmaceutical Society of GreatBritain; 2010.
6 National Institute for Health and Clinical Excellence. Tacrolimus andpimecrolimus for atopic eczema. August 2004.www.guidance.nice.org.uk/ta82 (accessed 13 July 2010).
7 Hampel P, Rudolph H, Petermann F, et al. Stress management trainingfor children and adolescents with atopic dermatitis during inpatientrehabilitation. Dermatology and Psychosomatics 2001;2:116–22.
Christine Clark is a freelance journalist and chairmanof the Skin Care Campaign, a UK organisationrepresenting the interests of people with skin diseases. E: [email protected]
Box 3: Pharmacy checklist
Pharmacists should consider providing all patients with eczema written andverbal information on the following:
� Choice of emollients� The use of emollients for moisturising and bathing� Application technique for topical treatments� Appropriate use of treatments (ie, how much, how often and when to
step up and step down)� Identification and management of eczema flares� Identification and management of trigger factors� Recognising infected atopic eczema� Details of patient support groups (eg, for the National Eczema Society)
Topical corticosteroid products should be labelled with a description oftheir potency. Children and carers may require separate (small) original packs for
school or nursery use.
Dani
ela
Spyr
opou
lou
| Dre
amst
ime.
com
CP, Sept, CF2, p291_Layout 1 8/24/2010 1:32 PM Page 298