Embed Size (px)
Citation preview
Athena SWAN Bronze department award application
Name of university: University of Oxford
Department: Cardiovascular Medicine
Date of application: 30 April 2013
Date of university Bronze and/or Silver SWAN award:
Bronze 2010
Contact for application: Prof Barbara Casadei
Email: [email protected]
Telephone: 01865 234664
Departmental website address: http://www.cardiov.ox.ac.uk/ (please note that a new website is currently under development)
Athena SWAN Bronze Department awards recognise that in addition to university-wide policies the department is working to promote gender equality and to address challenges particular to the discipline.
Not all institutions use the term ‘department’ and there are many equivalent academic groupings with different names, sizes and compositions. The definition of a ‘department’ for SWAN purposes can be found on the Athena SWAN website. If in doubt, contact the Athena SWAN Officer well in advance to check eligibility.
It is essential that the contact person for the application is based in the department.
Sections to be included
At the end of each section state the number of words used. Click here for additional guidance on completing the template.

1. Letter of endorsement from the head of department: maximum 500 words
An accompanying letter of endorsement from the head of department should explain how the SWAN action plan and activities in the department contribute to the overall department strategy and academic mission.
The letter is an opportunity for the head of department to confirm their support for the application and to endorse and commend any women and STEMM activities that have made a significant contribution to the achievement of the departmental mission.

DEPARTMENT OF CARDIOVASCULAR MEDICINE UNIVERSITY OF OXFORD Level 6, West Wing, John Radcliffe Hospital, Oxford OX3 9DU Tel: +44(0)1865 234657 Fax: +44(0)1865 234658 Email: [email protected] http://www.cardiov.ox.ac.uk/ Head of Department: Professor Hugh Watkins MD PhD FRCP FMedSci Field Marshal Alexander Professor of Cardiovascular Medicine
29th April 2013
Dear ATHENA SWAN panel
I am writing as Head of the Department of Cardiovascular Medicine (CVM), to lend my strongest support to our application for an Athena SWAN Bronze award. My department is fully committed to ensuring the career development of our women
scientists and clinicians. I wholeheartedly endorse the plans and aspirations in the application, and am committed to ensuring that the Athena SWAN principles, and our
action plan, are embedded in the culture of the department and implemented in our activities and initiatives. Doing so will benefit all members of the Department.
The department is dedicated to world class research and training in Cardiovascular
Science. We employ a broad range of staff, researchers and students from many different countries and need to draw on the widest pool of talent and ensure the
scientific development of all of our able trainees.
Through the self-assessment we have learnt much about ourselves and how the department is perceived. This provided the opportunity to reflect on both successes
and deficiencies. CVM is an informal, supportive and friendly place to work, and we have been able to engender a strong sense of identity across our four sites. But some
of what we have leant via the panel and survey has been uncomfortable, revealing areas where we must and will do better. Many of the challenges identified are
common themes across medical departments in Oxford and elsewhere, and indeed we recognise that clinical cardiology is a specialty with particular obstacles for women.
At present we have one female member of staff at professorial level (Professor
Barbara Casadei, who has led our Self Assessment Panel). Our Action Plan includes a commitment to increase the numbers of senior female staff and group leaders. We
have a large number of female scientists and students working in the department, but a discrepancy is apparent between junior grades (where genders are balanced) and higher grades and established academic positions. Nevertheless, a number of women
have recently obtained their own personal fellowships (Gehmlich, Reilly, Bissell, Stoll, Ariga) and we have a good proportion of women in post at grade 8 (senior
postdoctoral scientists).
I have been impressed by the enthusiasm and commitment of the Departmental Athena SWAN self-assessment team. They have contributed to a re-evaluation of our
activities and ethos of the department, and have made recommendations that will benefit all staff at all levels. We are committed to delivering our action plan over the

next 2-3 years and will ensure that progress on our milestones and action plan is
regularly reviewed.
Our application to Athena SWAN has come at a very opportune time in our transition
to becoming a component of the Radcliffe Department of Medicine (RDM). I am now
Head of this larger department and so will ensure continuity of our plans for CVM.
Within RDM we will provide dedicated administrative support to review and implement
the Athena SWAN action plans of all our components, learning from each other, and
under my leadership, implement best practice across the whole of RDM.
Thanks and best wishes
Yours sincerely
Hugh Watkins Professor of Cardiovascular Medicine
and Head of Department
2. The self-assessment process – maximum 1000 words
Describe the Self-Assessment Process. This should include:
A description of the self assessment team: members’ roles (both within the department and as part of the team) and their experiences of worklife balance;
The Self Assessment Team (SAT) included 13 women and 7 men, representing graduate students, postdoctoral scientists, academics, and research support staff from CVM.
1. Barbara Casadei (Chair), BHF Professor, member of the CVM and RDM Management Committee, Harassment Officer and Director of Graduate Studies (DGS) until 2012. Barbara has raised one daughter with a working partner, took maternity leave, and then worked full-time with an au pair living in.
2. Hugh Watkins, BHF Professor and CVM Head of Department; in 2012 he also became Head
of the newly formed RDM, of which CVM is a component. He has two teenage children and his wife works part-time.
3. Lynn Clee, Head of Administration for RDM, and until November 2012 for CVM. She is a
member of the CVM and RDM Management Committees. Lynn has raised one son with a working partner, working full-time throughout.
4. Priti Colbeck, current CVM Administrator. She lives in Bristol with her husband and
commutes on a weekly basis to Oxford.
5. Ruth McCaffrey, CVM Research Facilitator (previously a postdoctoral scientist) and member of the RDM Management Committee. She works part-time (60% FTE). Her husband is an academic and they have two daughters, aged 5 and 3.
6. Martin Farrall, Lecturer in Cardiovascular Genetics and member of the CVM Management
Committee. He is the current DGS and has a working partner.
7. Paul Leeson, BHF Senior Fellow and Consultant Cardiologist. He heads the Cardiovascular Clinical Research Facility and, with his wife, he is bringing up four children aged between 10 years and 18 months.
8. Stefan Neubauer, Professor, member of the CVM and RDM Management Committee,
Director of the Oxford Centre for Clinical Magnetic Resonance, and Head of the Oxford Biomedical Research Centre Cardiovascular Theme.
9. Polly Whitworth, Lead Research Nurse. Since returning from maternity leave Polly
gradually increased her hours (currently working 90% FTE).
10. Dorota Szumska, Postdoctoral Scientist in CVM for 8 years. Her partner is also a scientist.
11. Mark Crabtree, BHF CRE Intermediate Fellow. He is married with one son, who attends nursery.
12. Martina McAteer, Postdoctoral Scientist in CVM for 10.5 years. Martina has a working partner and two children (age 5 and 6). She took 2 maternity leaves, and has worked full-time since.
13. Charles Redwood, Group Leader and member of the CVM Management & Safety
Committees, joined the department in 1996 as a Postdoctoral Scientist. Charles has a 3-year old son, who he raises with his wife who works full-time.
14. Svetlana Reilly, Postdoctoral Researcher who recently completed her DPhil in CVM. She is married with two sons and took maternity leave in 2009 and 2011 for 18 months in total. She works full-time with an au pair living in. In September 2013 she will start a BHF CRE Intermediate Fellowship.
15. Sacha Bull, cardiology trainee who recently completed a DPhil in CVM as a BHF Clinical
Training Research Fellow (CTRF).
16. Malenka Bissell, BHF CTRF currently undertaking her DPhil. She is married.
17. Erica Dall’Armellina, BRC-funded Consultant Cardiologist. She recently completed her DPhil in CVM and is applying for a research fellowship. She is married.
18. Jyoti Patel, Postdoctoral Scientist. Jyoti recently completed her DPhil and was the CVM graduate student representative on the Medical Sciences Joint Consultative Committee.
19. Katja Gehmlich, Postdoctoral Scientist and project manager. In September 2013, she will
start a BHF Intermediate Fellowship. Her partner is an academic.
20. James Brown, Laboratory Manager and previously a Postdoctoral Scientist. He shares childcare duties for his two pre-school age children with his partner, an early career scientist. [598 words]
b) an account of the self assessment process: details of the self assessment team meetings, including any consultation with staff or individuals outside of the university, and how these have fed into the submission;
Establishing the core self-assessment team (SAT) and working groups (WG)
Hugh Watkins and administrative team started considering an application for a Bronze Athena SWAN award in January 2012; Barbara Casadei coordinated the process with support from Lynn Clee, Priti Colbeck and Ruth McCaffrey. They consulted the University’s central administration and other departments about the applications, downloaded material from the Athena SWAN website, and attended relevant seminars.
Members of CVM were informed in April 2012 of the intention to apply to Athena SWAN and, based on expression of interests, 16 individuals were invited to represent staff and graduate students.
All invitees agreed to serve in the SAT and the first meeting was held in May 2012. The decision
was made that the SAT should subdivide into 3 WGs focusing on:
1. Issues relating to work:family balance.
2. Early career (graduate students, CRTFs).
3. Career progression for postdoctoral scientists.
The WGs met separately to discuss their common experiences and identify problem areas. These discussions generated considerable interest, with other members of CVM expressing a desire to join in; as a result the SAT expanded and reached a final membership of 20 individuals.
Self-assessment questionnaire development
The UKRC Culture Analysis Tool (QuickCAT)
The SAT aimed to compile a Self-Assessment Questionnaire (SAQ) tailor-made for CVM.
In the interim, the opportunity arose to pilot the UKRC QuickCAT. This was launched by a joint email from the HoD and BC in July 2012 and 48 people (40% of CVM staff) responded. The SAT met again in August to review the findings and plan the CVM SAQ.
The CVM SAQ
The SAQ was issued in December 2012; 51 people (42%) responded to the survey (61% females). A summary of the results was circulated and WGs met separately to draft Actions points, which were discussed by the SAT in February 2013. Throughout this process SAT members were given articles and information on events promoting women in SET disciplines.
[320 words]
c) Plans for the future of the self-assessment team, such as how often the team will continue to meet, any reporting mechanisms and in particular how the self-assessment team intends to monitor implementation of the action plan.
Dedicated administrative support will be provided to ensure implementation of the Action Plan. The SAT has committed to meeting on at least a termly basis to monitor progress against the Action plan and report to the CVM management committee. All staff and graduate students will be informed through regular posting on the CVM website (which will have a section dedicated to Athena SWAN).
ACTION
2c Appoint an “Athena champion” who will dedicate 20-25% of their time to implementing the Action Plan.
[81 words]
Total for section=999 words
3. A picture of the department – maximum 2000 words
a) Provide a pen-picture of the department to set the context for the application, outlining in particular any significant and relevant features.
Department of Cardiovascular Medicine (CVM)
CVM is a small department employing 121 people across a range of staff groups. CVM is based on 4 sites, 3 at the John Radcliffe Hospital (JRH) and one at the Old Road Campus, approximately one mile away. CVM’s main base, together with laboratories for molecular and cellular studies, is housed in the West Wing of the JRH. Clinical research is also based at the JRH and is largely focused around the Oxford Centre for Magnetic Resonance Imaging (OCMR) and Cardiovascular Clinical Research Facility (CCRF) whereas the molecular genetics and model organism programmes are based at the Wellcome Trust Centre for Human Genetics (WTCHG) at the Old Road Campus. The department has undergone a period of sustained growth since Professor Watkins’ appointment in 1996 (see Table below). CVM has a total turnover of approximately £10.0M per annum. CVM has recently come together with a number of other departments/centres, to form the Radcliffe Department of Medicine (RDM). CVM will retain its own admin team and independence but will benefit from greater financial stability and added support in areas such as graduate recruitment, senior staff recruitment, implementation of the Athena SWAN action plan, outreach activities etc. The ECU advised that RDM should not submit a single Athena SWAN application since the department is new and has no culture of its own yet. Rather, we were advised that each department/centre should submit its own Athena SWAN Bronze application and that a single Silver application would be submitted in due course for the whole of RDM.
All CVM Staff
1996 – 19
2000 – 37 (+95% from 1996)
2004 – 58 (+57% from 2000)
2008 – 98 (+69% from 2004)
2012 – 121 (+24% from 2008)
In the 2008 RAE results CVM, together with colleagues from stroke research, received the highest quality rating of any biomedical return in the country (45% of CVM's work was rated in the highest category 4*, defined as 'world-leading’ and a further 40% was rated 3*, i.e. 'internationally excellent’).
Commitment and excellence in training and research has been recognised by the receipt of a Wellcome Trust Cardiovascular Research Initiative (2003-2009, one of two nationally), a British Heart Foundation Centre of Research Excellence (BHF CRE) Award (one of 4 nationally, 2008-2014, recently renewed 2014-2019) and also by the BHF 4 year graduate student programme, 4 students for each of four years, recently renewed for a third time 2013-2017.
CVM is regarded academically as an excellent place to work, and provides an inclusive, supportive, friendly and relaxed atmosphere for all staff. Many staff work across multiple sites, and there is extensive collaboration between groups within the department, with other departments in
Oxford, nationally and internationally. With people based at multiple sites, CVM works hard to maintain its sense of belonging and identity; this is achieved via both academic (e.g., joint lab meetings and seminars) and social gatherings, for example the annual Christmas party to which all staff, graduate students and partners are invited, and an annual Summer party, at the HoD’s home, to which all staff, graduate students, partners, and families are invited.
Cardiovascular science is a well-integrated research theme across the University covering a comprehensive spectrum of disciplines with significant activity in a number of Departments and Institutes (e.g., CVM, the Department of Physiology Anatomy and Genetics, Pharmacology, Chemistry, the WTCHG and the Weatherall Institute of Molecular Medicine, WIMM) that together form the Oxford BHF CRE.
[566 words]
b) Provide data for the past three years (where possible with clearly labelled graphical illustrations) on the following with commentary on their significance and how they have affected action planning.
Student data
(i) Numbers of males and females on access or foundation courses –
comment on the data and describe any initiatives taken to attract women to the courses.
We do not provide any of these courses.
[8 words]
(ii) Undergraduate male and female numbers – full and part-time –comment on the female:male ratio compared with the national picture for the discipline. Describe any initiatives taken to address any imbalance and the impact to date. Comment upon any plans for the future.
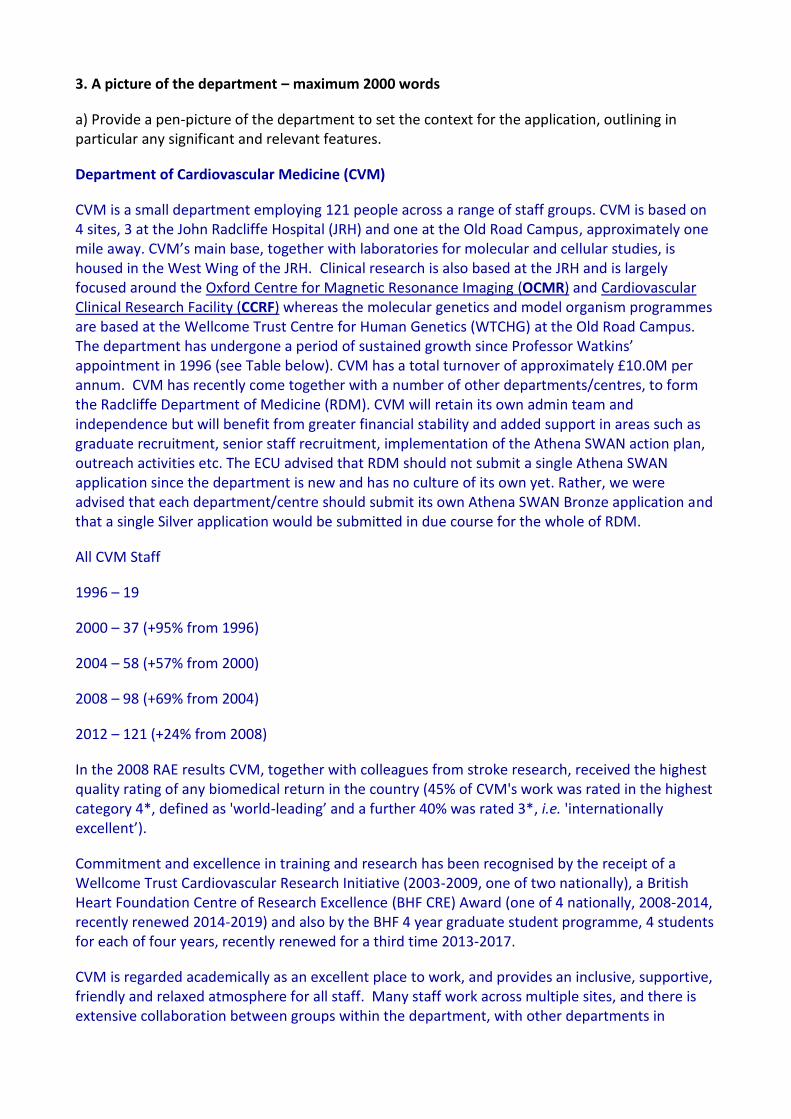
No undergraduate students are based in CVM; however, many members of staff contribute to undergraduate and graduate teaching (e.g., to the Special Study Module in Cardiology for medical students and the Cardiovascular Physiology module for the Graduate-Entry medical students). CVM contribution to teaching is consistently ranked very highly by the students (top 10-20% of lectures and modules). The numbers of students studying medicine at Oxford are shown below. Recruitment of these students is administered centrally by the Medical School.
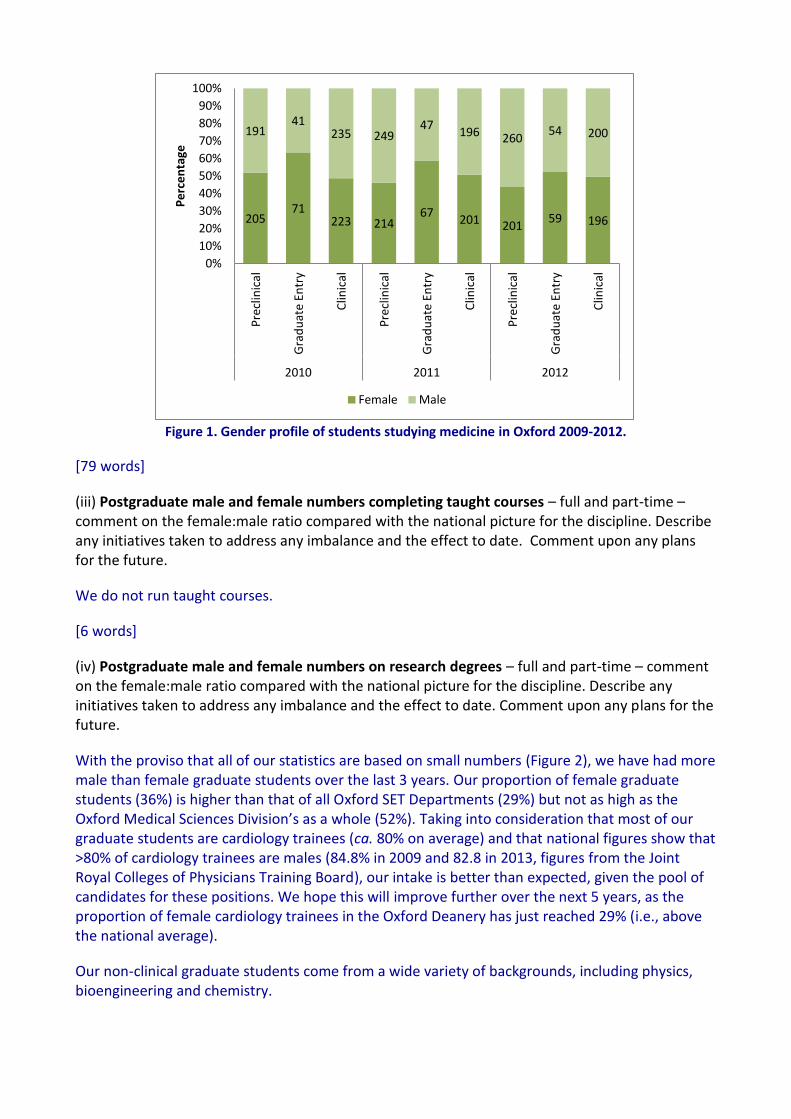
Figure 1. Gender profile of students studying medicine in Oxford 2009-2012.
[79 words]
(iii) Postgraduate male and female numbers completing taught courses – full and part-time – comment on the female:male ratio compared with the national picture for the discipline. Describe any initiatives taken to address any imbalance and the effect to date. Comment upon any plans for the future.
We do not run taught courses.
[6 words]
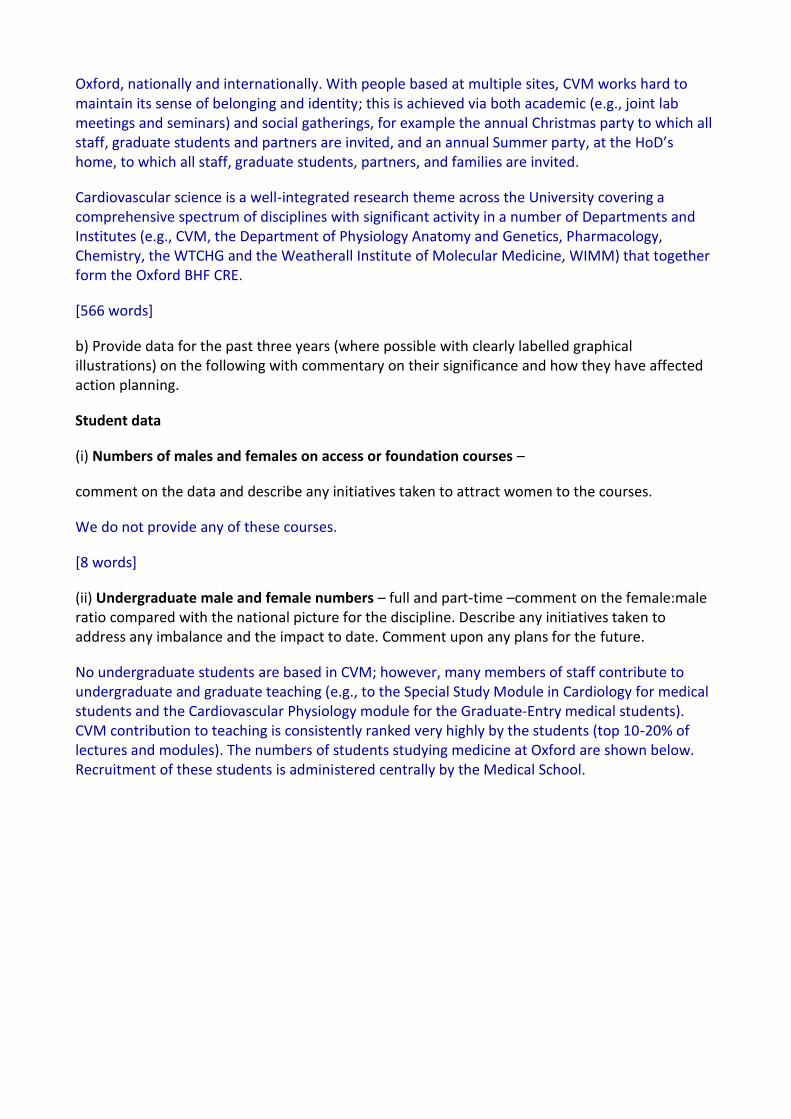
(iv) Postgraduate male and female numbers on research degrees – full and part-time – comment on the female:male ratio compared with the national picture for the discipline. Describe any initiatives taken to address any imbalance and the effect to date. Comment upon any plans for the future.
With the proviso that all of our statistics are based on small numbers (Figure 2), we have had more male than female graduate students over the last 3 years. Our proportion of female graduate students (36%) is higher than that of all Oxford SET Departments (29%) but not as high as the Oxford Medical Sciences Division’s as a whole (52%). Taking into consideration that most of our graduate students are cardiology trainees (ca. 80% on average) and that national figures show that >80% of cardiology trainees are males (84.8% in 2009 and 82.8 in 2013, figures from the Joint Royal Colleges of Physicians Training Board), our intake is better than expected, given the pool of candidates for these positions. We hope this will improve further over the next 5 years, as the proportion of female cardiology trainees in the Oxford Deanery has just reached 29% (i.e., above the national average).
Our non-clinical graduate students come from a wide variety of backgrounds, including physics, bioengineering and chemistry.
205 71
223 214 67
201 201 59 196
191 41
235 249 47
196 260 54 200
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pre
clin
ical
Gra
du
ate
Entr
y
Clin
ical
Pre
clin
ical
Gra
du
ate
Entr
y
Clin
ical
Pre
clin
ical
Gra
du
ate
Entr
y
Clin
ical
2010 2011 2012
Pe
rce
nta
ge
Female Male
Numbers of graduate students are shown below; all of our graduate students are full-time, as the Medical Sciences Division does not currently offer part-time degrees (under consultation).
Figure 2. Gender profile of CVM postgraduate students on research degrees.
[193 words]
(v) Ratio of course applications to offers and acceptances by gender for undergraduate, postgraduate taught and postgraduate research degrees – comment on the differences between male and female application and success rates and describe any initiatives taken to address any imbalance and their effect to date. Comment upon any plans for the future.
Overall, there seems to be no evidence of a gender bias in the application to offer or to acceptance ratio. In 2009/2010 the ratio of male to female applicants was uncommonly high, and this, as expected, is reflected in the application to acceptance ratio.
2008-09 2009-10 2010-11
Female Male Total Female Male Total Female Male Total
Applications 4 5 9 5 13 18 8 10 18
Offers 4 4 8 3 9 12 3 6 9
Acceptances 4 4 8 2 8 10 3 4 7
App to Offer Ratio 1.0 1.3 1.1 1.7 1.4 1.5 2.7 1.7 2.0
App to accept ratio
1.0 1.3 1.1 2.5 1.6 1.8 2.7 2.5 2.6
[44 words]
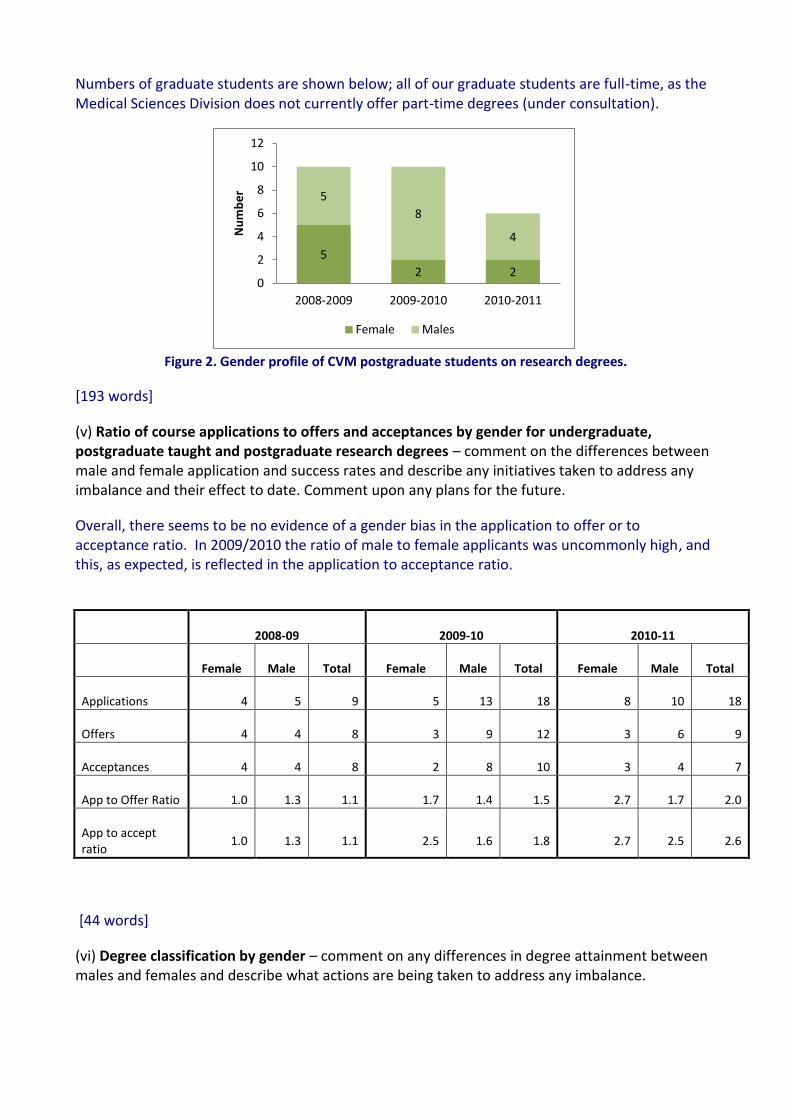
(vi) Degree classification by gender – comment on any differences in degree attainment between males and females and describe what actions are being taken to address any imbalance.
5
2 2
5
8
4
0
2
4
6
8
10
12
2008-2009 2009-2010 2010-2011
Nu
mb
er
Female Males
We only offer postgraduate degrees that are not classified. All but one of our DPhil students who started their studies over the last 5 years completed their degree in 4 years (one male student took longer). There is, therefore, no evidence for gender imbalance in degree attainment.
Our SAQ did not uncover gender bias in the quality of supervision and availability of networking/career opportunities at this stage. We will continue to monitor these data; in addition, some suggestions were made to improve the experience of graduate students, which are now part of our action plan.
ACTIONS
3.iv a. Continue to monitor applicants and admission figures and rate of degree attainment
between males and females. b. Support the Medical Sciences Division’s consultation on offering part-time research
degrees.
3.v a. Add information on Athena SWAN and family friendly policies to our DPhil prospectus and
advertisement.
3.vi a. Monitor adherence to training for first-time supervisors and refresher training for other
supervisors. b. Organise a welcome event for Graduate Students & their supervisors both as a social
occasion and as a forum to increase awareness of University and Department’s family friendly policies, training opportunities, and to discuss students and supervisors’ expectations.
c. Pilot a mentorship scheme [see 3vii(a)] d. Start monitoring student’s career choices after concluding their DPhil by the introduction
of an exit interview and questionnaire.
[223 words]
Staff data
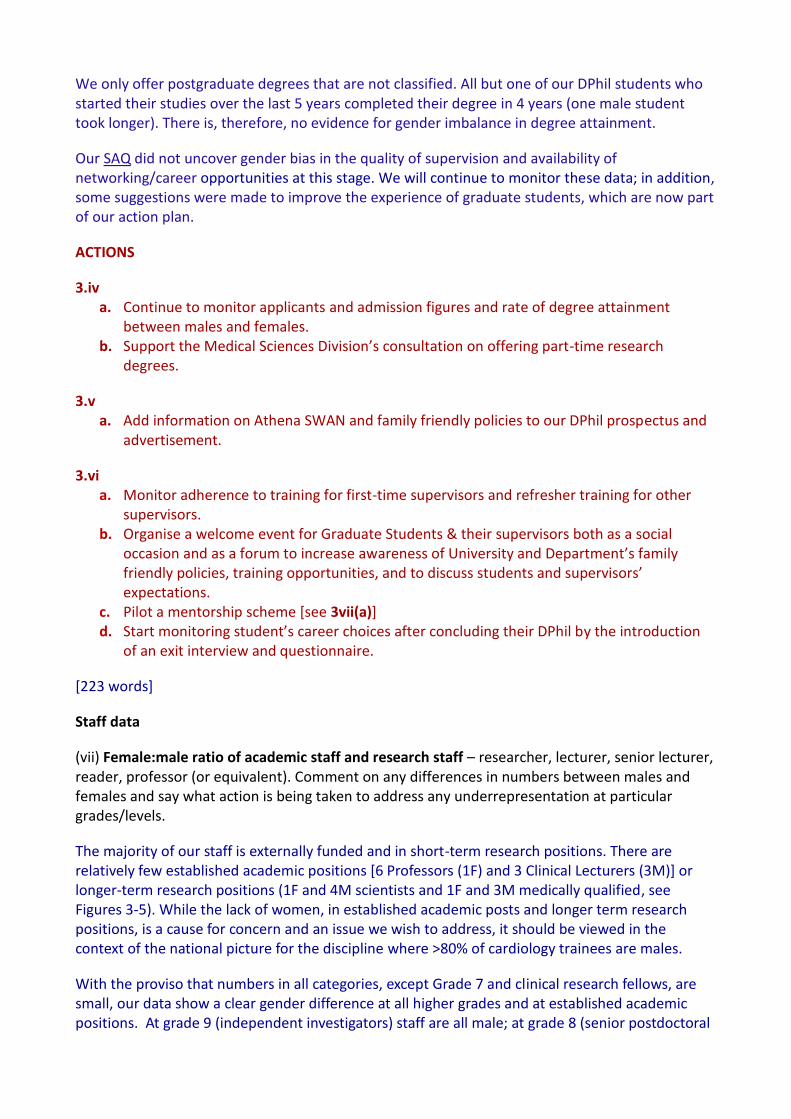
(vii) Female:male ratio of academic staff and research staff – researcher, lecturer, senior lecturer, reader, professor (or equivalent). Comment on any differences in numbers between males and females and say what action is being taken to address any underrepresentation at particular grades/levels.
The majority of our staff is externally funded and in short-term research positions. There are relatively few established academic positions [6 Professors (1F) and 3 Clinical Lecturers (3M)] or longer-term research positions (1F and 4M scientists and 1F and 3M medically qualified, see Figures 3-5). While the lack of women, in established academic posts and longer term research positions, is a cause for concern and an issue we wish to address, it should be viewed in the context of the national picture for the discipline where >80% of cardiology trainees are males.
With the proviso that numbers in all categories, except Grade 7 and clinical research fellows, are small, our data show a clear gender difference at all higher grades and at established academic positions. At grade 9 (independent investigators) staff are all male; at grade 8 (senior postdoctoral
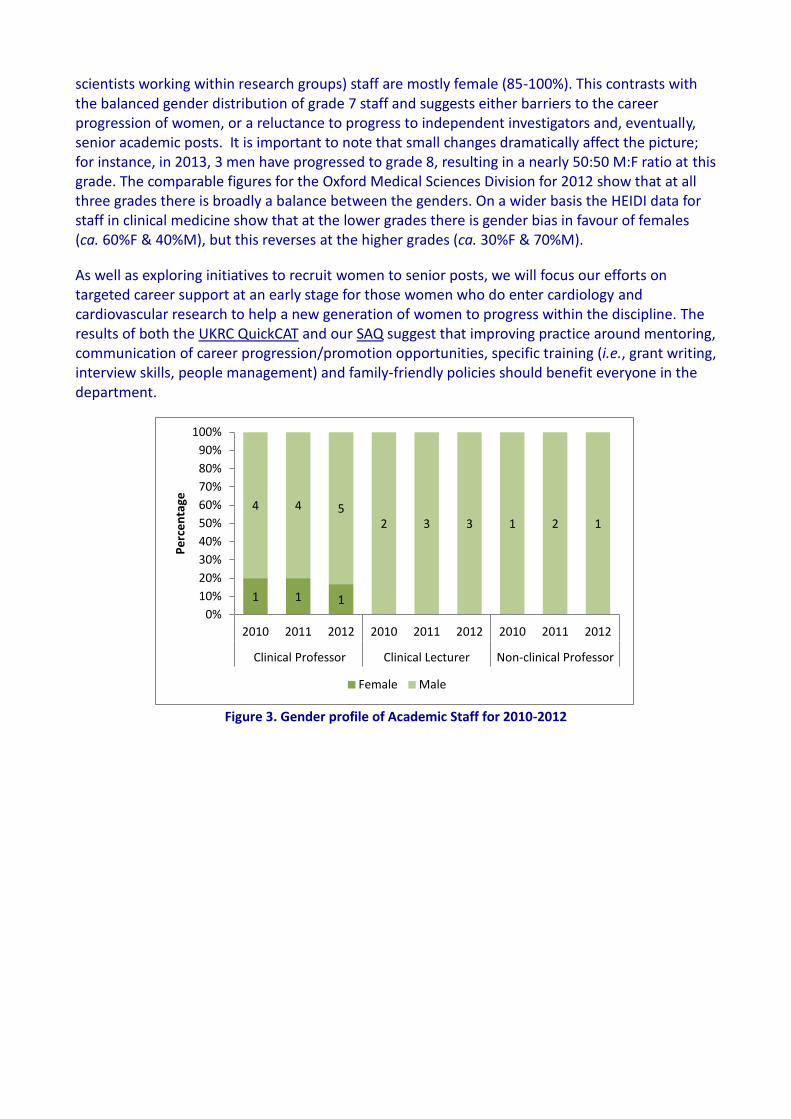
scientists working within research groups) staff are mostly female (85-100%). This contrasts with the balanced gender distribution of grade 7 staff and suggests either barriers to the career progression of women, or a reluctance to progress to independent investigators and, eventually, senior academic posts. It is important to note that small changes dramatically affect the picture; for instance, in 2013, 3 men have progressed to grade 8, resulting in a nearly 50:50 M:F ratio at this grade. The comparable figures for the Oxford Medical Sciences Division for 2012 show that at all three grades there is broadly a balance between the genders. On a wider basis the HEIDI data for staff in clinical medicine show that at the lower grades there is gender bias in favour of females (ca. 60%F & 40%M), but this reverses at the higher grades (ca. 30%F & 70%M).
As well as exploring initiatives to recruit women to senior posts, we will focus our efforts on targeted career support at an early stage for those women who do enter cardiology and cardiovascular research to help a new generation of women to progress within the discipline. The results of both the UKRC QuickCAT and our SAQ suggest that improving practice around mentoring, communication of career progression/promotion opportunities, specific training (i.e., grant writing, interview skills, people management) and family-friendly policies should benefit everyone in the department.
Figure 3. Gender profile of Academic Staff for 2010-2012
1 1 1
4 4 5 2 3 3 1 2 1
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2010 2011 2012 2010 2011 2012 2010 2011 2012
Clinical Professor Clinical Lecturer Non-clinical Professor
Pe
rce
nta
ge
Female Male
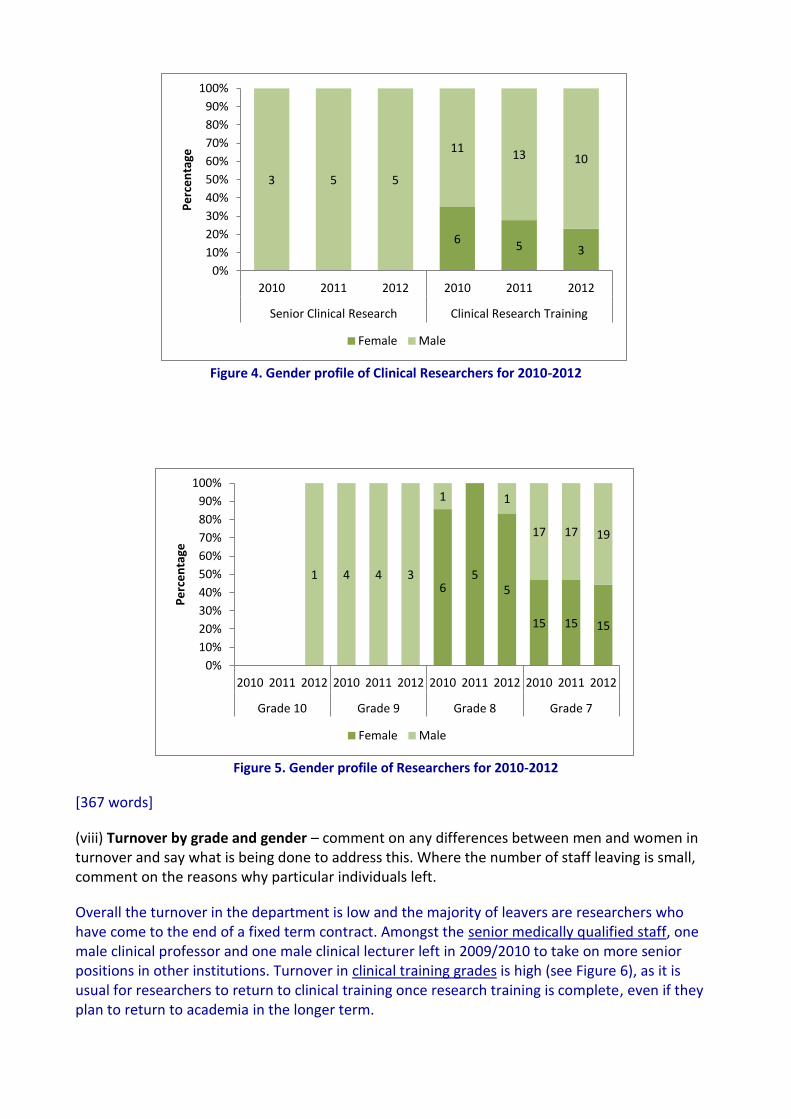
Figure 4. Gender profile of Clinical Researchers for 2010-2012
Figure 5. Gender profile of Researchers for 2010-2012
[367 words]
(viii) Turnover by grade and gender – comment on any differences between men and women in turnover and say what is being done to address this. Where the number of staff leaving is small, comment on the reasons why particular individuals left.
Overall the turnover in the department is low and the majority of leavers are researchers who have come to the end of a fixed term contract. Amongst the senior medically qualified staff, one male clinical professor and one male clinical lecturer left in 2009/2010 to take on more senior positions in other institutions. Turnover in clinical training grades is high (see Figure 6), as it is usual for researchers to return to clinical training once research training is complete, even if they plan to return to academia in the longer term.
6 5 3
3 5 5
11 13 10
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2010 2011 2012 2010 2011 2012
Senior Clinical Research Clinical Research Training
Pe
rce
nta
ge
Female Male
6 5
5
15 15 15
1 4 4 3
1 1
17 17 19
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2010 2011 2012 2010 2011 2012 2010 2011 2012 2010 2011 2012
Grade 10 Grade 9 Grade 8 Grade 7
Pe
rce
nta
ge
Female Male

The turnover of non-clinical researchers is fairly low (see Figure 7). One Grade 9 male left for a post in industry. One female Grade 8 took up an Assistant Professorship in her country of origin, and one returned to a job in industry after completing a BHF CRE fellowship. One Grade 8 male left to take up a postdoctoral position elsewhere. The Grade 7 male leavers took up jobs overseas, except one who left without a confirmed position elsewhere. Amongst the female Grade 7 leavers, one did not return after maternity due to family relocation, one took up another grade 7 post in Oxford and one took up a post in another University. Overall these data do not show a gender bias; we are not planning any action in this area but will continue to monitor these figures.
Figure 6. Turnover from fixed-term Clinical Research Training posts.
Figure 7. Turnover from Non-Clinical Research posts.
ACTIONS 3.vii - We will:
a. Pilot a mentorship scheme for all staff, drawing from staff in CVM and RDM and including both senior staff in established positions and mid-career researchers. This will meet the request of having a mentor outside CVM by some respondents, increase the availability of female mentors, and provide a wider range of age and experience. We will also refer to
4
10
6
14
5
13
1 2 2 2 2
6
0
2
4
6
8
10
12
14
16
Female Male Female Male Female Male
2010 2011 2012
Nu
mb
er
Headcount Leavers
18 20
21 22
21 21
1 2 2
3 2 2
0
5
10
15
20
25
Female Male Female Male Female Male
2010 2011 2012
Nu
mb
er
Headcount Leavers
existing mentoring schemes, such as that run by OxFest (University of Oxford Females in Engineering, Science and Technology). After discussion with the SAT, it was decided that the mentorship scheme would be provided “on demand”.
b. Organise talks by senior staff in the Department on “how to” make the next career step using the already established forum of the Departmental lunchtime seminars. Further support is outlined in Actions 4b.ii (a & b).
c. Ensure that important meetings and seminars do not take place during school half term and holiday dates, so that people with families do not miss them.
d. Communicate all funding opportunities and calls to all staff (rather than to group leaders) and include links to funding opportunities on our webpage (allowing staff to customise the alerts that are pertinent to their needs).
e. Review the wording of recruitment material and website to include information on Athena SWAN and CVM family friendly policies
f. Increase the visibility of positive female role models by including mini-biographies/testimonials of female scientists & publicise achievements, awards and fellowships in the CVM website.
g. Ensure a strong female representation on short-listing and interview panel and on search panels for all academic posts and aim to have at least one woman on the long-list of potential recruits to be considered for such posts. [513 words]
Total words for this section= 1999
Supporting and advancing women’s careers – maximum 5000 words
4. Key career transition points
(a) Provide data for the past three years (where possible with clearly labelled graphical illustrations) on the following with commentary on their significance and how they have affected action planning.
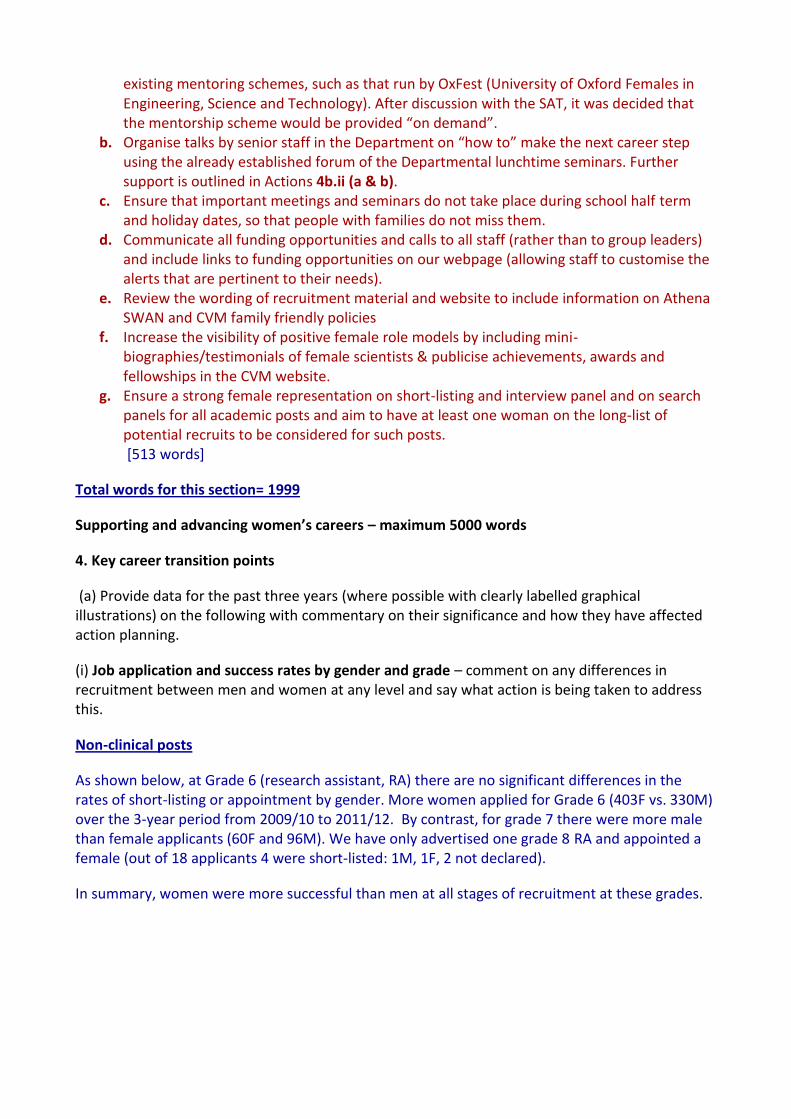
(i) Job application and success rates by gender and grade – comment on any differences in recruitment between men and women at any level and say what action is being taken to address this.
Non-clinical posts
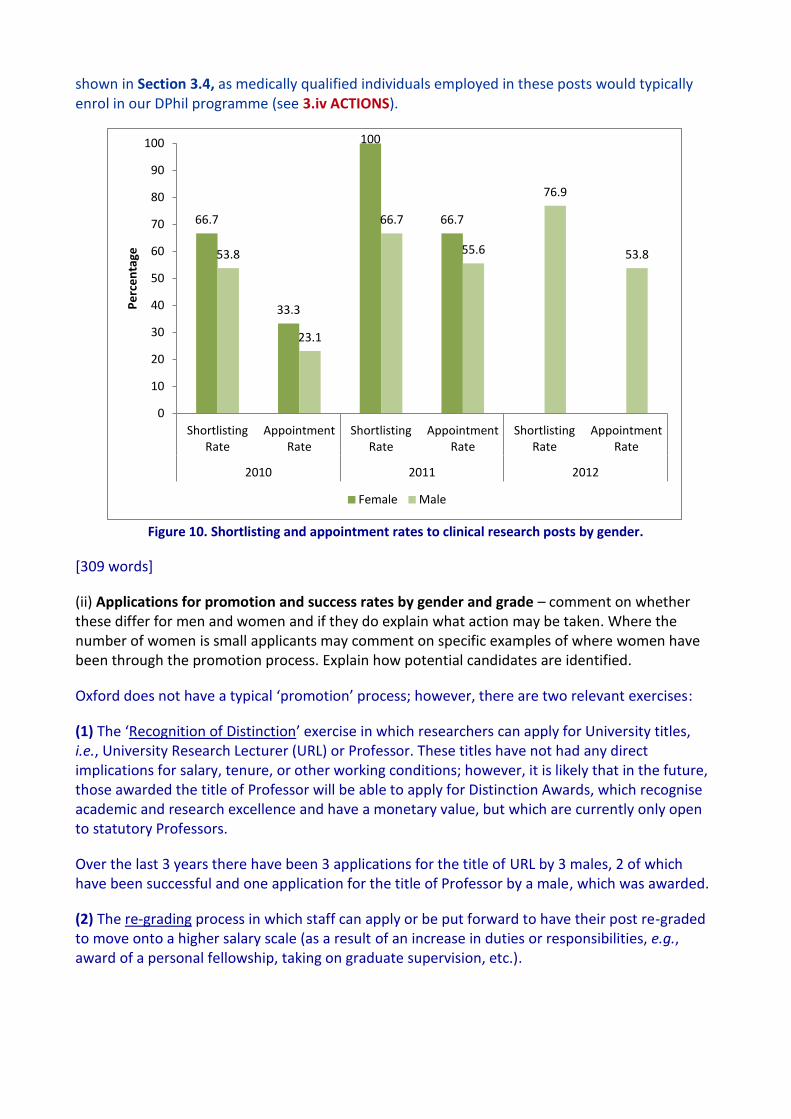
As shown below, at Grade 6 (research assistant, RA) there are no significant differences in the rates of short-listing or appointment by gender. More women applied for Grade 6 (403F vs. 330M) over the 3-year period from 2009/10 to 2011/12. By contrast, for grade 7 there were more male than female applicants (60F and 96M). We have only advertised one grade 8 RA and appointed a female (out of 18 applicants 4 were short-listed: 1M, 1F, 2 not declared).
In summary, women were more successful than men at all stages of recruitment at these grades.
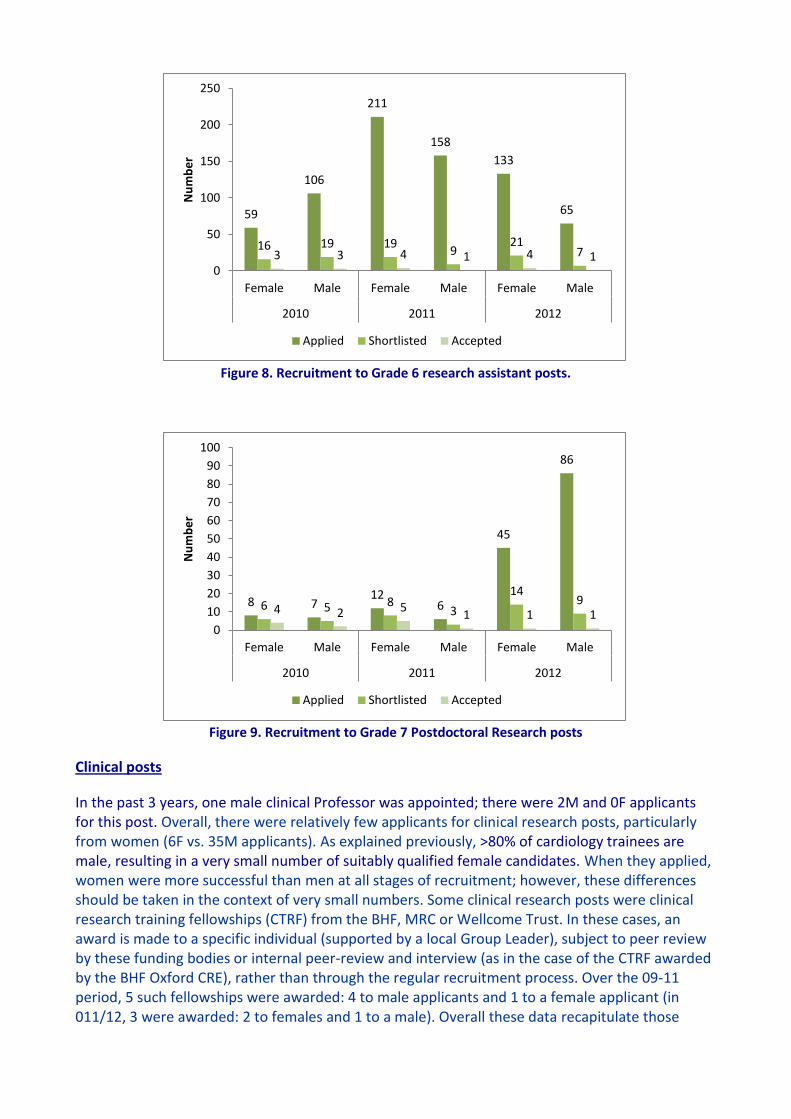
Figure 8. Recruitment to Grade 6 research assistant posts.
Figure 9. Recruitment to Grade 7 Postdoctoral Research posts
Clinical posts
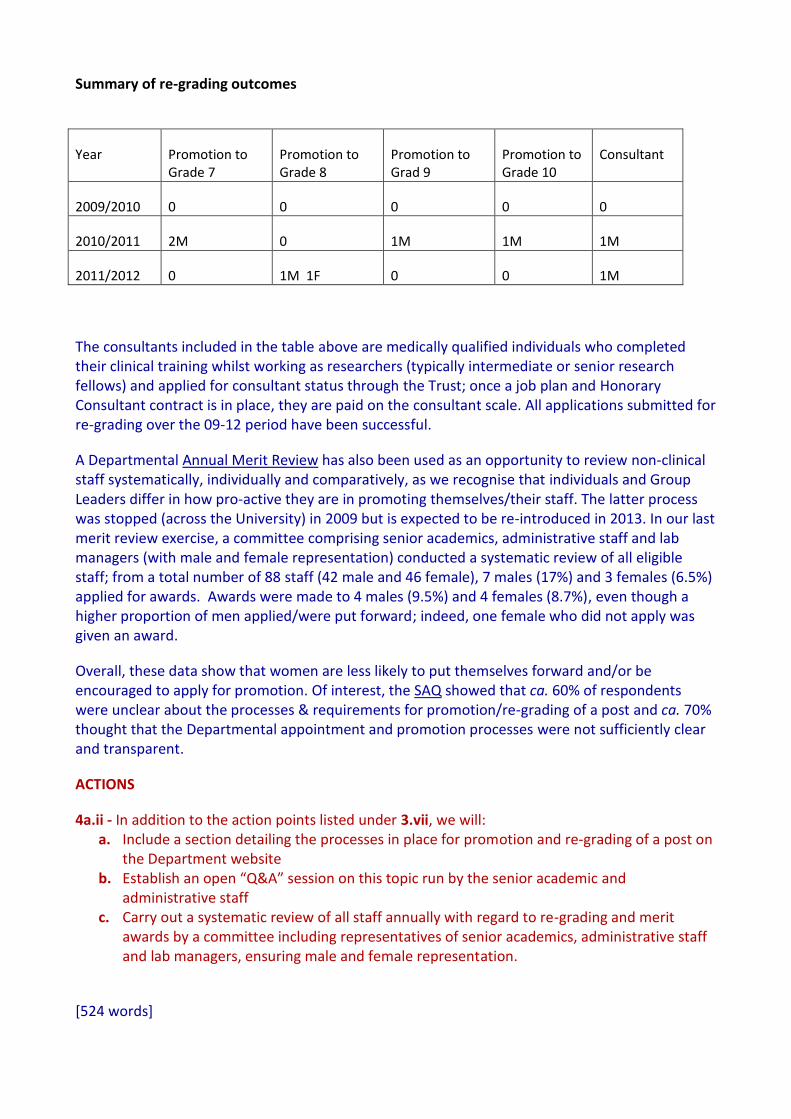
In the past 3 years, one male clinical Professor was appointed; there were 2M and 0F applicants for this post. Overall, there were relatively few applicants for clinical research posts, particularly from women (6F vs. 35M applicants). As explained previously, >80% of cardiology trainees are male, resulting in a very small number of suitably qualified female candidates. When they applied, women were more successful than men at all stages of recruitment; however, these differences should be taken in the context of very small numbers. Some clinical research posts were clinical research training fellowships (CTRF) from the BHF, MRC or Wellcome Trust. In these cases, an award is made to a specific individual (supported by a local Group Leader), subject to peer review by these funding bodies or internal peer-review and interview (as in the case of the CTRF awarded by the BHF Oxford CRE), rather than through the regular recruitment process. Over the 09-11 period, 5 such fellowships were awarded: 4 to male applicants and 1 to a female applicant (in 011/12, 3 were awarded: 2 to females and 1 to a male). Overall these data recapitulate those
59
106
211
158
133
65
16 19 19 9
21 7 3 3 4 1 4 1
0
50
100
150
200
250
Female Male Female Male Female Male
2010 2011 2012
Nu
mb
er
Applied Shortlisted Accepted
8 7 12
6
45
86
6 5 8 3
14 9
4 2 5 1 1 1
0
10
20
30
40
50
60
70
80
90
100
Female Male Female Male Female Male
2010 2011 2012
Nu
mb
er
Applied Shortlisted Accepted
shown in Section 3.4, as medically qualified individuals employed in these posts would typically enrol in our DPhil programme (see 3.iv ACTIONS).
Figure 10. Shortlisting and appointment rates to clinical research posts by gender.
[309 words]
(ii) Applications for promotion and success rates by gender and grade – comment on whether these differ for men and women and if they do explain what action may be taken. Where the number of women is small applicants may comment on specific examples of where women have been through the promotion process. Explain how potential candidates are identified.
Oxford does not have a typical ‘promotion’ process; however, there are two relevant exercises:
(1) The ‘Recognition of Distinction’ exercise in which researchers can apply for University titles, i.e., University Research Lecturer (URL) or Professor. These titles have not had any direct implications for salary, tenure, or other working conditions; however, it is likely that in the future, those awarded the title of Professor will be able to apply for Distinction Awards, which recognise academic and research excellence and have a monetary value, but which are currently only open to statutory Professors.
Over the last 3 years there have been 3 applications for the title of URL by 3 males, 2 of which have been successful and one application for the title of Professor by a male, which was awarded.
(2) The re-grading process in which staff can apply or be put forward to have their post re-graded to move onto a higher salary scale (as a result of an increase in duties or responsibilities, e.g., award of a personal fellowship, taking on graduate supervision, etc.).
66.7
33.3
100
66.7
53.8
23.1
66.7
55.6
76.9
53.8
0
10
20
30
40
50
60
70
80
90
100
Shortlisting Rate
Appointment Rate
Shortlisting Rate
Appointment Rate
Shortlisting Rate
Appointment Rate
2010 2011 2012
Pe
rce
nta
ge
Female Male
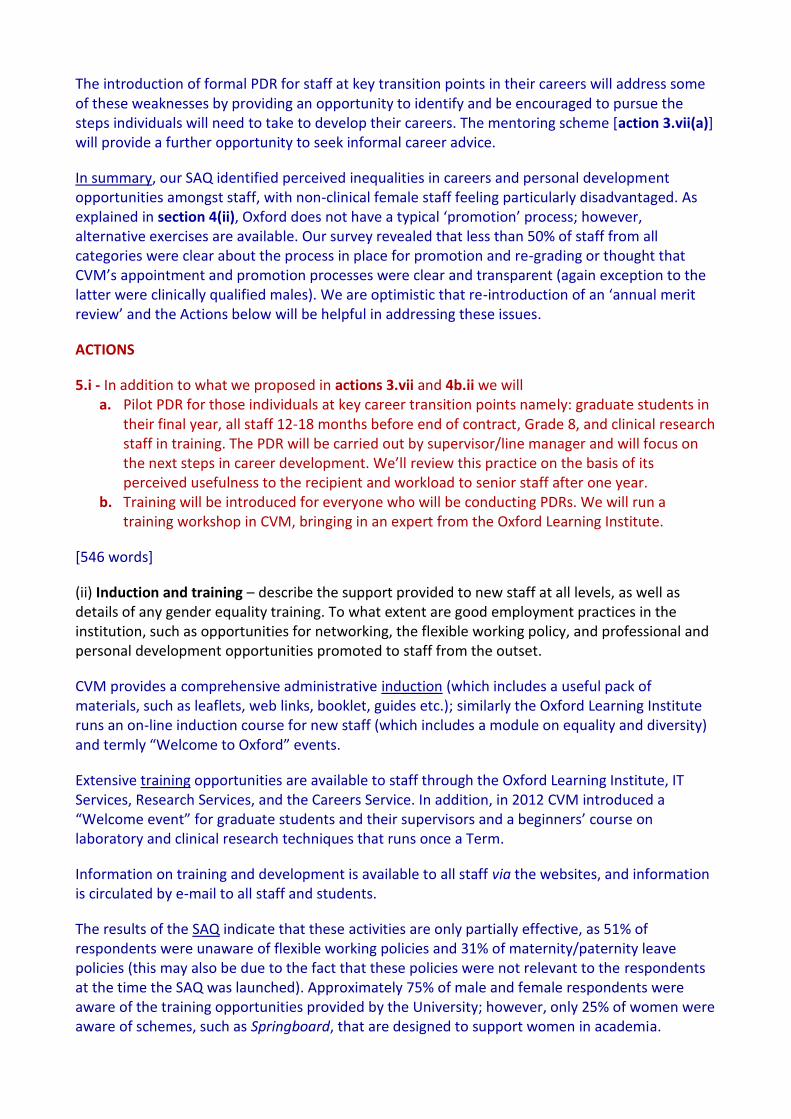
Summary of re-grading outcomes
Year Promotion to Grade 7
Promotion to Grade 8
Promotion to Grad 9
Promotion to Grade 10
Consultant
2009/2010 0 0 0 0 0
2010/2011 2M 0 1M 1M 1M
2011/2012 0 1M 1F 0 0 1M
The consultants included in the table above are medically qualified individuals who completed their clinical training whilst working as researchers (typically intermediate or senior research fellows) and applied for consultant status through the Trust; once a job plan and Honorary Consultant contract is in place, they are paid on the consultant scale. All applications submitted for re-grading over the 09-12 period have been successful.
A Departmental Annual Merit Review has also been used as an opportunity to review non-clinical staff systematically, individually and comparatively, as we recognise that individuals and Group Leaders differ in how pro-active they are in promoting themselves/their staff. The latter process was stopped (across the University) in 2009 but is expected to be re-introduced in 2013. In our last merit review exercise, a committee comprising senior academics, administrative staff and lab managers (with male and female representation) conducted a systematic review of all eligible staff; from a total number of 88 staff (42 male and 46 female), 7 males (17%) and 3 females (6.5%) applied for awards. Awards were made to 4 males (9.5%) and 4 females (8.7%), even though a higher proportion of men applied/were put forward; indeed, one female who did not apply was given an award.
Overall, these data show that women are less likely to put themselves forward and/or be encouraged to apply for promotion. Of interest, the SAQ showed that ca. 60% of respondents were unclear about the processes & requirements for promotion/re-grading of a post and ca. 70% thought that the Departmental appointment and promotion processes were not sufficiently clear and transparent.
ACTIONS
4a.ii - In addition to the action points listed under 3.vii, we will: a. Include a section detailing the processes in place for promotion and re-grading of a post on
the Department website b. Establish an open “Q&A” session on this topic run by the senior academic and
administrative staff c. Carry out a systematic review of all staff annually with regard to re-grading and merit
awards by a committee including representatives of senior academics, administrative staff and lab managers, ensuring male and female representation.
[524 words]

b) For each of the areas below, explain what the key issues are in the department, what steps have been taken to address any imbalances, what success/impact has been achieved so far and what additional steps may be needed.
(i) Recruitment of staff – comment on how the department’s recruitment processes ensure that
female candidates are attracted to apply, and how the department ensures its short listing, selection processes and criteria comply with the university’s equal opportunities policies The Department applies all the processes recommended by the University for ensuring non-discrimination in recruitment processes. All job particulars include information on maternity leave arrangements, nurseries, play-schemes and equality & opportunity. All selection and interview panels include male and female assessors and at least one representative who has taken the University’s Recruitment and Selection course (which focuses on equal opportunities and fair recruitment practices). Since 2012, there have been 18 selection panels, of which 2 were 25% women, 10 were 33-50% women and 5 were >50% women. A particular issue that we have faced is a low application rates from women for externally advertised senior clinical posts. This reflects the low proportion of women who entered training in clinical cardiology in preceding years. We are encouraged that this trend is improving, at least locally, but will continue to need to promote opportunities for women clinician scientists in the field locally and nationally.
ACTIONS
4b(i) see those listed under 3.vii.
[159 words]
(ii) Support for staff at key career transition points – having identified key areas of attrition of female staff in the department, comment on any interventions, programmes and activities that support women at the crucial stages, such as personal development training, opportunities for networking, mentoring programmes and leadership training. Identify which have been found to work best at the different career stages.
Our analysis indicates that no female postdoctoral scientist has progressed to Grade 9 or above and none of the female trainees has progressed to a Clinical Lecturer position or above (with one exception).
As mentioned in 3.vii, the results of our SAQ suggest that improving practice around mentoring, communication of career progression/promotion opportunities and family-friendly policies should help us to achieve a more balanced representation of women at all grades. Over the years, staff applying for awards and fellowships received informal mentoring and indeed the Department has achieved external recognition for success in training and career development (e.g., by being recipients of the Wellcome Trust CVRI and BHF CRE awards). However, we recognise that these ad-hoc arrangements are not sufficient and will from now put in place formal arrangements. We also recognise that supervisors/Group Leader’s knowledge and implementation of good practice are

variable and propose to invite and monitor refresher training (including Equality and Diversity training) for all supervisors and Group Leaders [action 3vi(a)].
ACTIONS
4b.ii - In addition to the actions listed under 3vi and 3.vii we will: a. Encourage research staff (e.g. grade 8), junior clinical staff, and women, in particular, to
apply for pump-priming grants from our internal funding sources (via our website, “How to” talks, and at PDR)
b. Ensure that all applications for externally funded independent fellowships are reviewed internally and that practice interviews are conducted.
[231 words]
5. Career development
a) For each of the areas below, explain what the key issues are in the department, what steps have been taken to address any imbalances, what success/impact has been achieved so far and what additional steps may be needed.
(i) Promotion and career development – comment on the appraisal and career development
process, and promotion criteria and whether these take into consideration responsibilities for teaching, research, administration, pastoral work and outreach work; is quality of work emphasised over quantity of work?
Our SAQ indicated that, whereas, male clinical staff are satisfied with the career progression and training opportunities offered by CVM, female clinical staff feel that they have fewer opportunities for career progression than their male clinical colleagues. Similarly, 70% of non-clinical female respondents perceived inequality in the access to career-enhancing opportunities and felt they missed out on such opportunities because they were not “male”, “young”, or medically qualified (i.e., “part of the club”). However, overall, all non-clinical staff (M+F) felt they had fewer opportunities for career progression within CVM than their clinical colleagues. This may be partly due to the security offered by the clinical route vs. the insecurity associated with obtaining external funding and an academic post.
Nevertheless, in all categories, male respondents were mostly clear as to the next steps they had to take to further their career (>80%) whereas females were not (50% clinical, 30% non-clinical). Similarly, all respondents agreed that they would benefit from more guidance on how to write a grant application, manage people, or interview for a job/fellowship. Only one respondent thought that family responsibility and flexible working hours were the underlying reason for missing out on career/development opportunities.
Only 40% of respondents were aware of training/development opportunities provided by CVM or the Medical Sciences Division (vs. 78% awareness of training opportunities provided by the University). However, the majority of respondents were satisfied with the opportunities available in CVM to experience teaching (ca. 70% for both M and F), give scientific presentations (100% for both M and F) & write a scientific paper (90% for both M &F).
The introduction of formal PDR for staff at key transition points in their careers will address some of these weaknesses by providing an opportunity to identify and be encouraged to pursue the steps individuals will need to take to develop their careers. The mentoring scheme [action 3.vii(a)] will provide a further opportunity to seek informal career advice.
In summary, our SAQ identified perceived inequalities in careers and personal development opportunities amongst staff, with non-clinical female staff feeling particularly disadvantaged. As explained in section 4(ii), Oxford does not have a typical ‘promotion’ process; however, alternative exercises are available. Our survey revealed that less than 50% of staff from all categories were clear about the process in place for promotion and re-grading or thought that CVM’s appointment and promotion processes were clear and transparent (again exception to the latter were clinically qualified males). We are optimistic that re-introduction of an ‘annual merit review’ and the Actions below will be helpful in addressing these issues.
ACTIONS
5.i - In addition to what we proposed in actions 3.vii and 4b.ii we will a. Pilot PDR for those individuals at key career transition points namely: graduate students in
their final year, all staff 12-18 months before end of contract, Grade 8, and clinical research staff in training. The PDR will be carried out by supervisor/line manager and will focus on the next steps in career development. We’ll review this practice on the basis of its perceived usefulness to the recipient and workload to senior staff after one year.
b. Training will be introduced for everyone who will be conducting PDRs. We will run a training workshop in CVM, bringing in an expert from the Oxford Learning Institute.
[546 words]
(ii) Induction and training – describe the support provided to new staff at all levels, as well as details of any gender equality training. To what extent are good employment practices in the institution, such as opportunities for networking, the flexible working policy, and professional and personal development opportunities promoted to staff from the outset.
CVM provides a comprehensive administrative induction (which includes a useful pack of materials, such as leaflets, web links, booklet, guides etc.); similarly the Oxford Learning Institute runs an on-line induction course for new staff (which includes a module on equality and diversity) and termly “Welcome to Oxford” events.
Extensive training opportunities are available to staff through the Oxford Learning Institute, IT Services, Research Services, and the Careers Service. In addition, in 2012 CVM introduced a “Welcome event” for graduate students and their supervisors and a beginners’ course on laboratory and clinical research techniques that runs once a Term.
Information on training and development is available to all staff via the websites, and information is circulated by e-mail to all staff and students.
The results of the SAQ indicate that these activities are only partially effective, as 51% of respondents were unaware of flexible working policies and 31% of maternity/paternity leave policies (this may also be due to the fact that these policies were not relevant to the respondents at the time the SAQ was launched). Approximately 75% of male and female respondents were aware of the training opportunities provided by the University; however, only 25% of women were aware of schemes, such as Springboard, that are designed to support women in academia.
65% of respondents to the UKRC QuickCAT agreed or strongly agreed that CVM had made its policies in relation to gender equality clear to them, 23% disagreed, and the rest did not know. Similarly, the SAQ respondents were mostly satisfied with the training opportunities provided by CVM, as far as teaching, giving scientific presentations, and writing a scientific paper were concerned, although only 50% of females were satisfied with the training provided for managing people, writing a grant application, or interviewing for a job.
ACTIONS
5.ii a. Pilot a “buddy” system for new staff and ask all newcomers to complete the online
University induction. b. Increase awareness of training opportunities and University-led personal development
activities for all staff and particularly for women (e.g., Springboard and Ad-Feminam) both by regular emails and by adding links to our website. Training needs will be expressly discussed and monitored at PDRs.
c. As indicated in ACTION 3.vi(b) and 3.vii(b), we will relate relevant information at the students’ Welcome Event and through ‘How to’ and ‘Q&A’ sessions run by CVM’s senior academic and administrative staff [ACTION 4a.i(b)] and will ensure that group leaders, supervisors and line managers receive appropriate training on these matters [ACTION 3.vi(a)].
[412 words]
(iii) Support for female students – describe the support (formal and informal) provided for female students to enable them to make the transition to a sustainable academic career, particularly from postgraduate to researcher, such as mentoring, seminars and pastoral support and the right to request a female personal tutor. Comment on whether these activities are run by female staff and how this work is formally recognised by the department.
The Director of Graduate Studies (DGS, a female academic from 2003-2012 and a male academic since 2012) provides academic support and pastoral care to all students (though the latter mostly on demand). All graduate students and supervisors are asked to provide a progress report and feed-back on their experience on-line once a term. All postgraduate students are attached to a college as well as the department. The colleges provide students with a personal tutor and considerable pastoral care.
In addition, regular termly meetings with the academic supervisor (in addition to lab meetings), a targeted induction, and students’ networking events were considered to be particularly useful by the ‘Early career WG’.
We have no evidence of underperformance or attrition at this stage of women’s careers. However, the
‘Early career WG’ expressed the desire of graduate students to have access to a mentor (who could be junior or senior postdoctoral scientists) in addition to their supervisor(s) and college advisor for ad-hoc consultations. Finally, it was suggested that exit questionnaires should be implemented to monitor the students’ experience and the impact of our Action plan.
ACTIONS
5.iii - as in 3.vi & 3.vii(a). In addition, we will:
a. Ask the supervisors to meet their students at least once a term (outside the lab meeting) to assess progress, expectations and provide and receive informal verbal feedback
b. Organise graduate students and early career networking events jointly with RDM.
c. DGS will have an annual meeting with all graduate students to monitor their progress.
[249 words]
6. Organisation and culture
a) Provide data for the past three years (where possible with clearly labelled graphical illustrations) on the following with commentary on their significance and how they have affected action planning.
(i) Male and female representation on committees – provide a breakdown by committee and
explain any differences between male and female representation. Explain how potential members are identified.
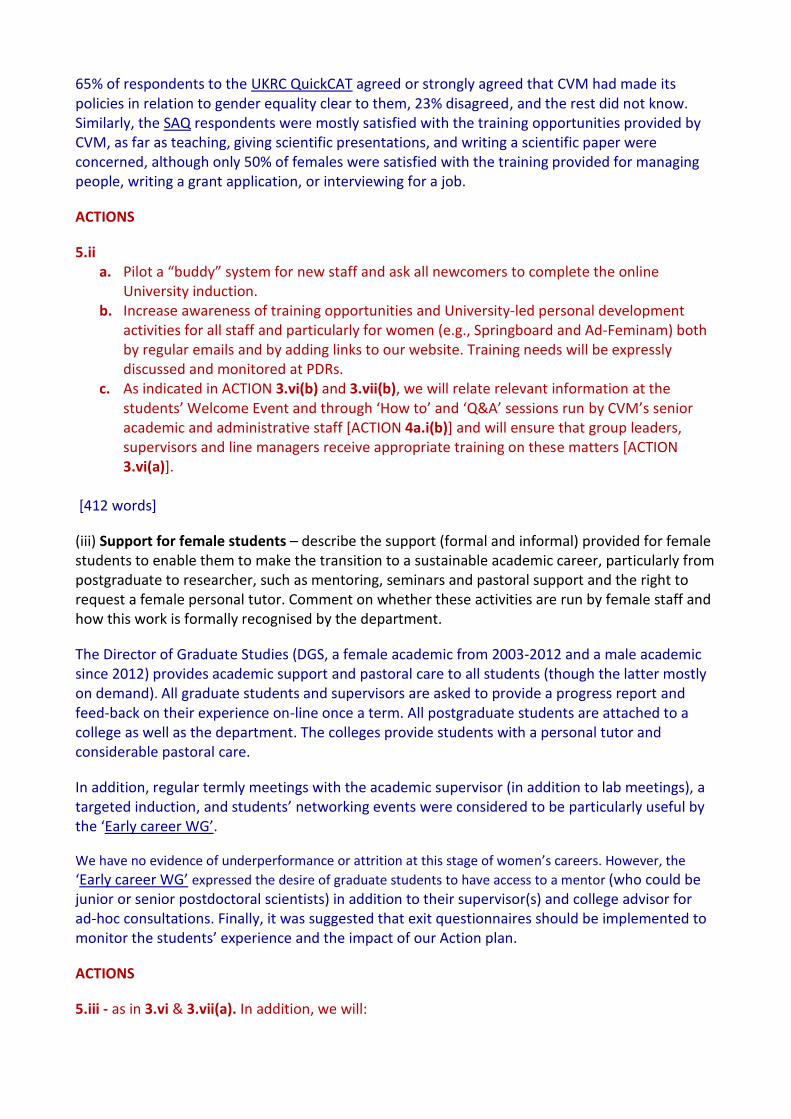
CVM does not have many Committees, but those we do have reflect the F:M ratio of staff in CVM as a whole and in its components (see graph). We only have one senior female academic (BC) who sits on both the CVM Group Leaders and the RDM management committees (both of which are chaired by Hugh Watkins) and is currently a member of the Steering Committee of the BHF Graduate Programme in Cardiovascular Science at the University of Oxford (since 2003). There have been no women representatives from CVM on the Oxford BHF CRE Steering or Executive committees (chaired by Hugh Watkins) over the last 5 years; however, BC will be part of the new BHF CRE steering committee from 2013.
Membership of the CVM Group Leaders includes all senior academic staff (8M, 1F), the administrator (F) and the lab manager (M) and is decided by consensus. Please note that the administrator is a senior role in Oxford departments.
OCMR and CCRF management committees include their core staff and are chaired by the head of the unit.
The Safety Committee is responsible for monitoring and guiding safe practice in all the departmental activities and includes 4M and 3F.
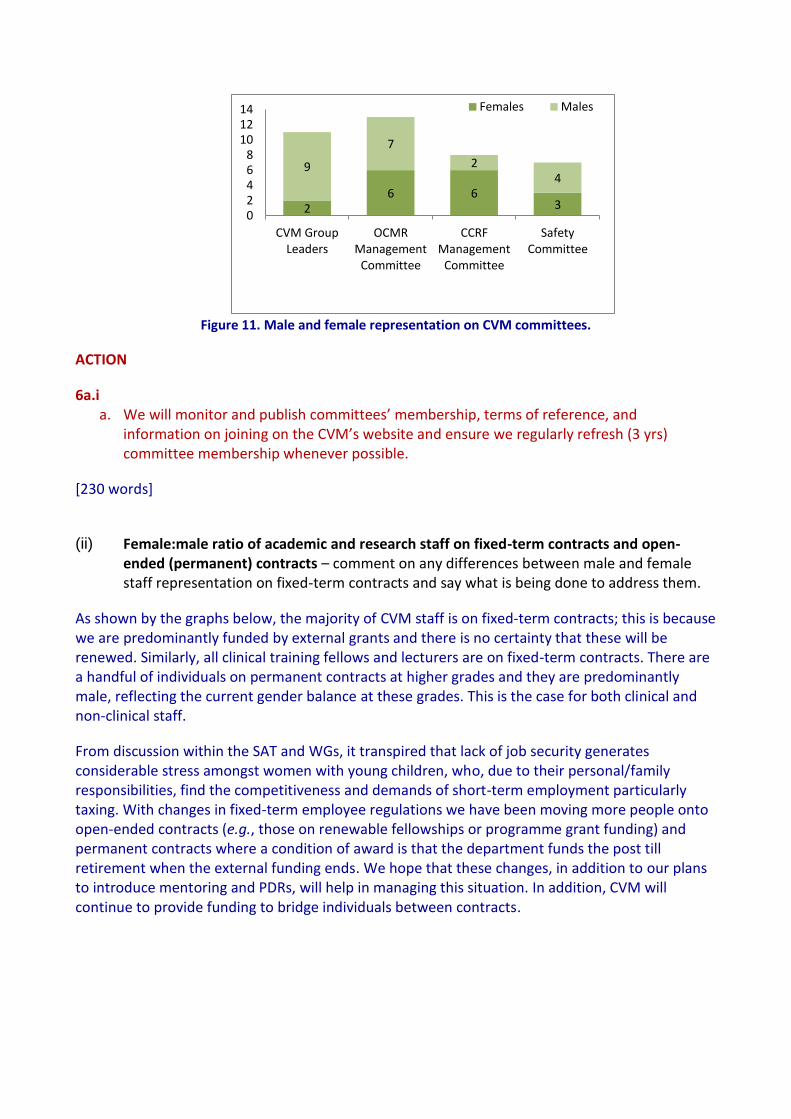
Figure 11. Male and female representation on CVM committees.
ACTION
6a.i a. We will monitor and publish committees’ membership, terms of reference, and
information on joining on the CVM’s website and ensure we regularly refresh (3 yrs) committee membership whenever possible.
[230 words]
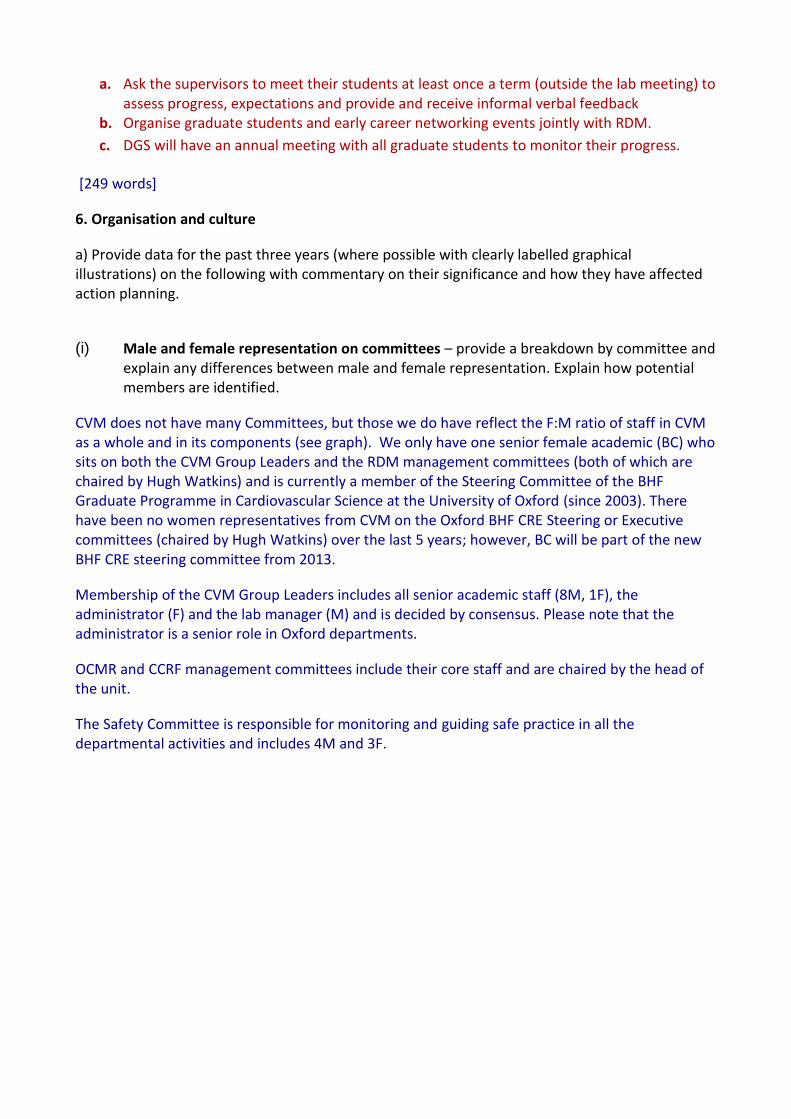
(ii) Female:male ratio of academic and research staff on fixed-term contracts and open-
ended (permanent) contracts – comment on any differences between male and female staff representation on fixed-term contracts and say what is being done to address them.
As shown by the graphs below, the majority of CVM staff is on fixed-term contracts; this is because we are predominantly funded by external grants and there is no certainty that these will be renewed. Similarly, all clinical training fellows and lecturers are on fixed-term contracts. There are a handful of individuals on permanent contracts at higher grades and they are predominantly male, reflecting the current gender balance at these grades. This is the case for both clinical and non-clinical staff.
From discussion within the SAT and WGs, it transpired that lack of job security generates considerable stress amongst women with young children, who, due to their personal/family responsibilities, find the competitiveness and demands of short-term employment particularly taxing. With changes in fixed-term employee regulations we have been moving more people onto open-ended contracts (e.g., those on renewable fellowships or programme grant funding) and permanent contracts where a condition of award is that the department funds the post till retirement when the external funding ends. We hope that these changes, in addition to our plans to introduce mentoring and PDRs, will help in managing this situation. In addition, CVM will continue to provide funding to bridge individuals between contracts.
2 6 6
3
9
7
2 4
0 2 4 6 8
10 12 14
CVM Group Leaders
OCMR Management
Committee
CCRF Management
Committee
Safety Committee
Females Males
Figure 11. Academic Staff divided by contract type and gender.
Figure 12. Clinical Researchers divided by contract type and gender.
1 1 1
2 4
3
5 5
6
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2010 2011 2012 2010 2011 2012
Female Male
Pe
rce
nta
ge
Fixed-term Permanent
1
3 4
6 5 3 11 13 10
2
2 1
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
100%
2010 2011 2012 2010 2011 2012 2010 2011 2012 2010 2011 2012
Female Male Female Male
Senior Clinical Research Clinical Research Training
Pe
rce
nta
ge
Fixed-term Permanent
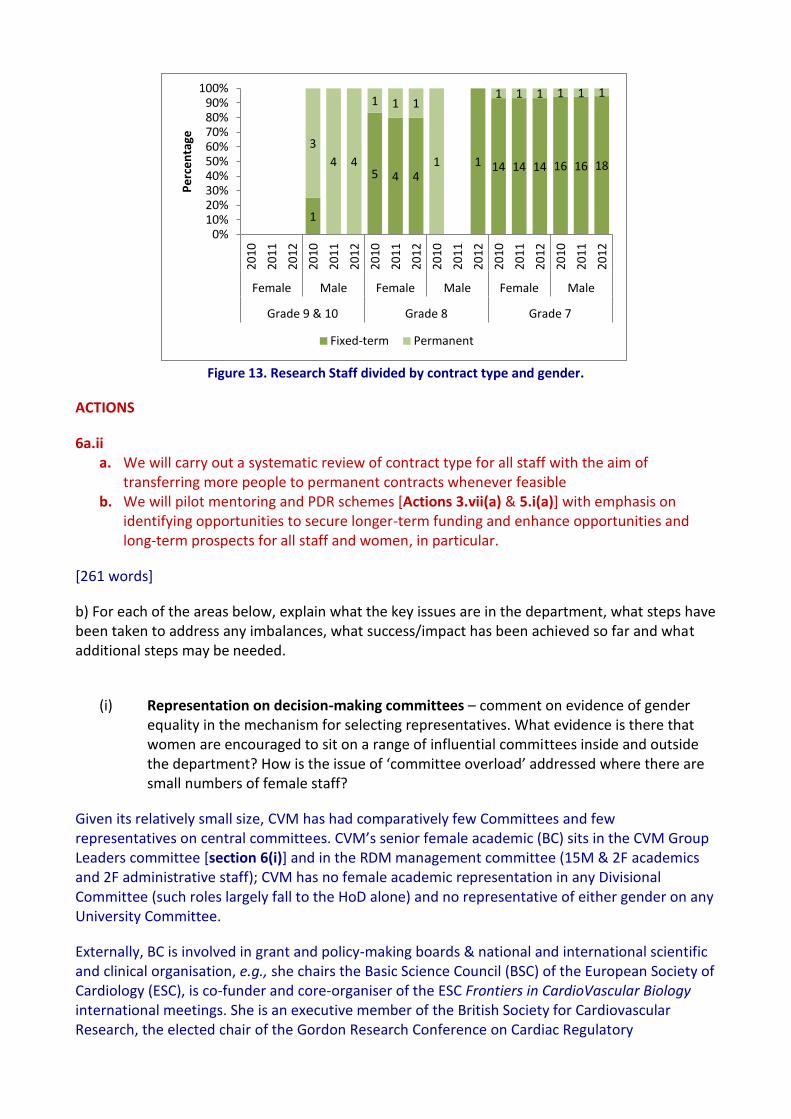
Figure 13. Research Staff divided by contract type and gender.
ACTIONS
6a.ii a. We will carry out a systematic review of contract type for all staff with the aim of
transferring more people to permanent contracts whenever feasible b. We will pilot mentoring and PDR schemes [Actions 3.vii(a) & 5.i(a)] with emphasis on
identifying opportunities to secure longer-term funding and enhance opportunities and long-term prospects for all staff and women, in particular.
[261 words]
b) For each of the areas below, explain what the key issues are in the department, what steps have been taken to address any imbalances, what success/impact has been achieved so far and what additional steps may be needed.
(i) Representation on decision-making committees – comment on evidence of gender
equality in the mechanism for selecting representatives. What evidence is there that women are encouraged to sit on a range of influential committees inside and outside the department? How is the issue of ‘committee overload’ addressed where there are small numbers of female staff?
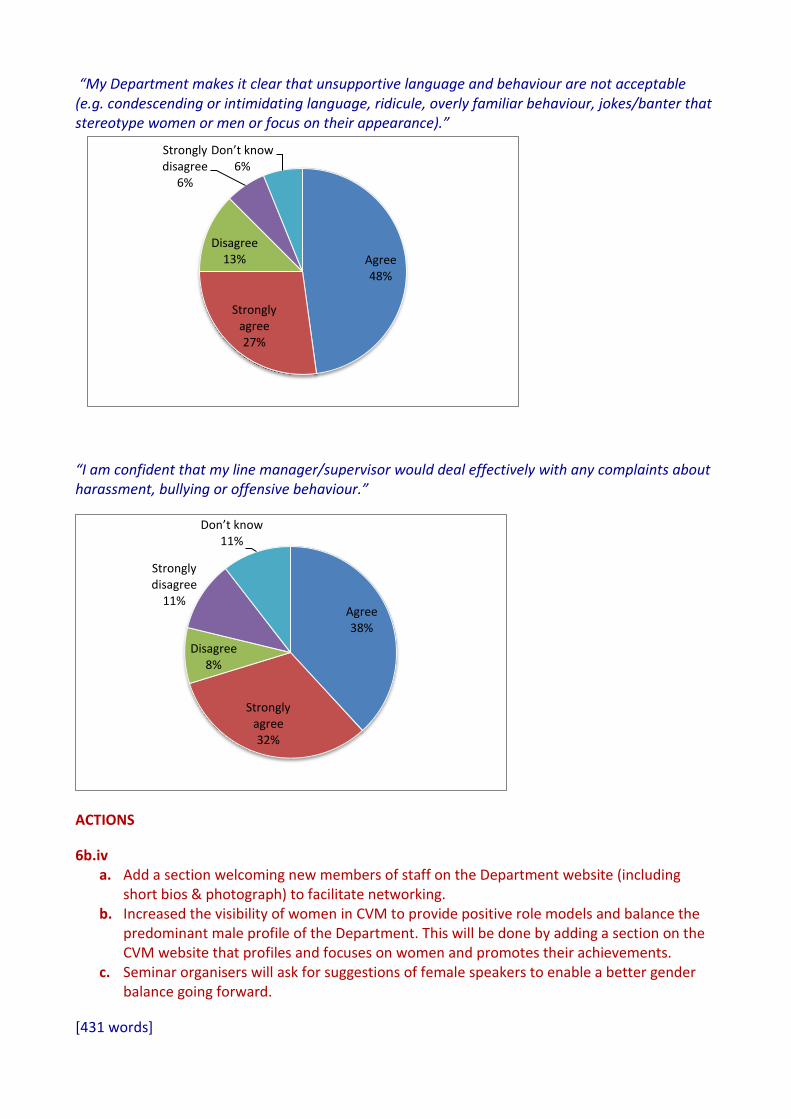
Given its relatively small size, CVM has had comparatively few Committees and few representatives on central committees. CVM’s senior female academic (BC) sits in the CVM Group Leaders committee [section 6(i)] and in the RDM management committee (15M & 2F academics and 2F administrative staff); CVM has no female academic representation in any Divisional Committee (such roles largely fall to the HoD alone) and no representative of either gender on any University Committee.
Externally, BC is involved in grant and policy-making boards & national and international scientific and clinical organisation, e.g., she chairs the Basic Science Council (BSC) of the European Society of Cardiology (ESC), is co-funder and core-organiser of the ESC Frontiers in CardioVascular Biology international meetings. She is an executive member of the British Society for Cardiovascular Research, the elected chair of the Gordon Research Conference on Cardiac Regulatory
1
5 4 4 1 14 14 14 16 16 18
3
4 4
1 1 1
1
1 1 1 1 1 1
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
100%
20
10
20
11
20
12
20
10
20
11
20
12
20
10
20
11
20
12
20
10
20
11
20
12
20
10
20
11
20
12
20
10
20
11
20
12
Female Male Female Male Female Male
Grade 9 & 10 Grade 8 Grade 7
Pe
rce
nta
ge
Fixed-term Permanent
Mechanisms (USA), served as Strategic adviser to the EU commission DG research, is an associate editor of Cardiovascular Research and member of several Scientific Advisory Boards outside the UK.
We do not currently have formal procedures in place to avoid committee overload. We are aware that encouraging greater participation of women on decision-making committees may overburden females, particularly in Departments such as ours where senior female academics are under-represented. The most desirable solution for this problem is to foster women’s careers within CVM and we are confident that over the next 5 years we will have at least 3 more female junior group leaders. In the meanwhile, we will monitor additional duties that people are performing to try and ensure female representation in decision-making committee whilst avoiding administrative overload.
[270 words]
(ii) Workload model – describe the systems in place to ensure that workload allocations, including pastoral and administrative responsibilities (including the responsibility for work on women and science) are taken into account at appraisal and in promotion criteria. Comment on the rotation of responsibilities e.g. responsibilities with a heavy workload and those that are seen as good for an individual’s career.
As there are few administrative roles within CVM (other than those carried by the administrator, lab managers and HoD) and since members of staff tend to have light teaching loads, most workloads are determined by a person’s research commitments. Therefore, we do not use formal workload models at departmental level.
We have used informal mechanisms to ensure rotation of onerous responsibilities (e.g. DGS). Until now these activities have not been monitored.
ACTION
6b.ii a. Start a record of formal administrative roles and other comparable duties performed by all
staff; this will be reviewed at the CVM Group Leaders committee on an annual basis and discussed at PDRs and rotated as appropriate.
[110 words]
(iii) Timing of departmental meetings and social gatherings – provide evidence of consideration for those with family responsibilities, for example what the department considers to be core hours and whether there is a more flexible system in place.
52% of the respondents of the UKRC QuickCAT disagreed/strongly disagreed with the assertion that “meetings in my Department are completed in core hours (e.g., 10am to 4pm) to enable those with caring responsibilities to attend”. We have been holding our seminars on Monday between 12:30 and 1:30pm and the Departmental Lab meetings on Friday at 4 pm. This was discussed at the SAT, and it was decided all CVM (internal and external) activities be held on the Monday between 12 and 2 pm, as a pilot to be reviewed after one year. Timing of committee meetings is variable but generally within core hours; e.g. OCMR at 2 pm and CCRF at 10:30 am.
ACTIONS
6b.iii a. Hold Seminars, Departmental Lab meetings, and Q&A and “How to” sessions on Mondays
between 12 and 2 pm, as a pilot and review this decision periodically. b. Alert Group Leaders of the desirability of holding lab meetings during core hours and
accommodating the schedule of part-time/flexible working staff and monitor adherence to these recommendations at the SAT meetings.
[174 words]
(iv) Culture –demonstrate how the department is female-friendly and inclusive. ‘Culture’ refers to the language, behaviours and other informal interactions that characterise the atmosphere of the department, and includes all staff and students.
In Europe and in the US Cardiovascular Medicine has been and still is a male-dominated area and, currently, only about 20% of cardiology trainees in the UK are women. This gender disparity does not apply to the non-clinical research staff; nevertheless leadership of all Cardiology/Cardiovascular Medicine departments has been largely male dominated and a female-friendly and inclusive culture within clinical academic cardiology is only just starting to develop, largely because of the opening of new areas within the specialty that have been populated by a larger proportion of women (e.g., imaging) and generated a local “critical mass”.
The results of the UKRC QuickCAT showed that 77% of respondents agreed (29%)/strongly agreed (48%) that CVM is “a great place to work” for women; [85% of respondents agreed (33%)/strongly agreed (52%) that is a great place to work for men] and 88% of females agreed that in CVM “staff are treated on their merits irrespective of their gender”.
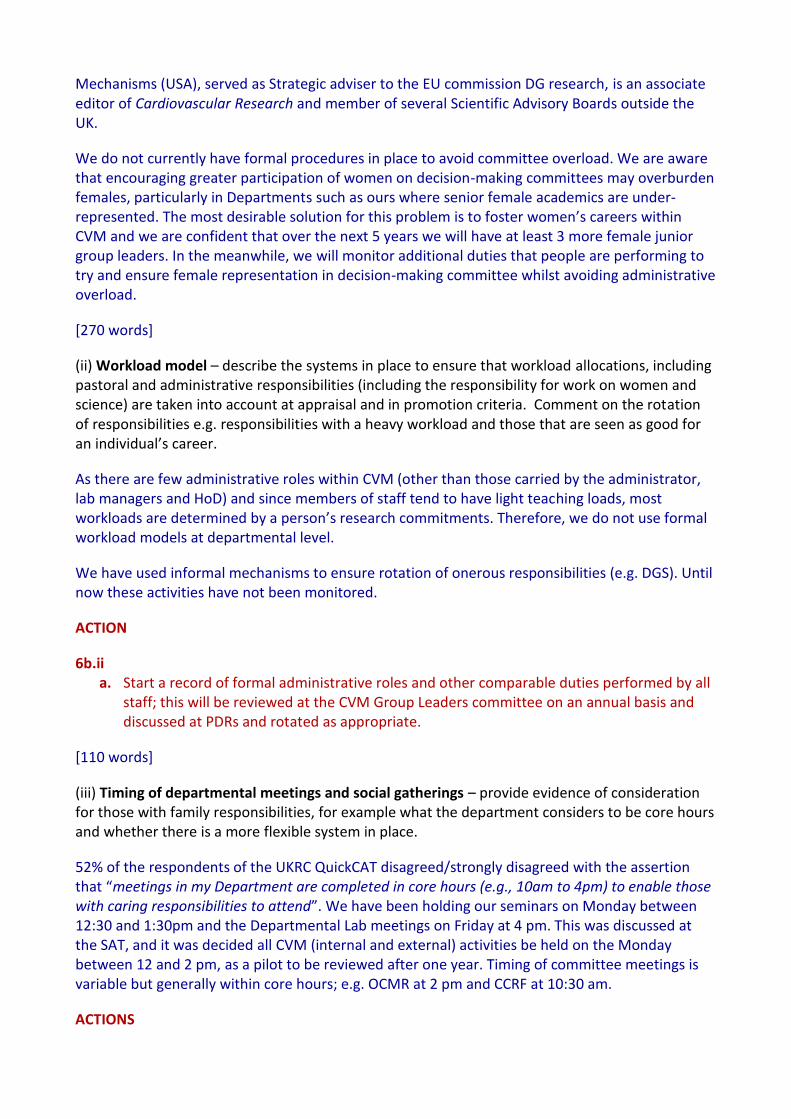
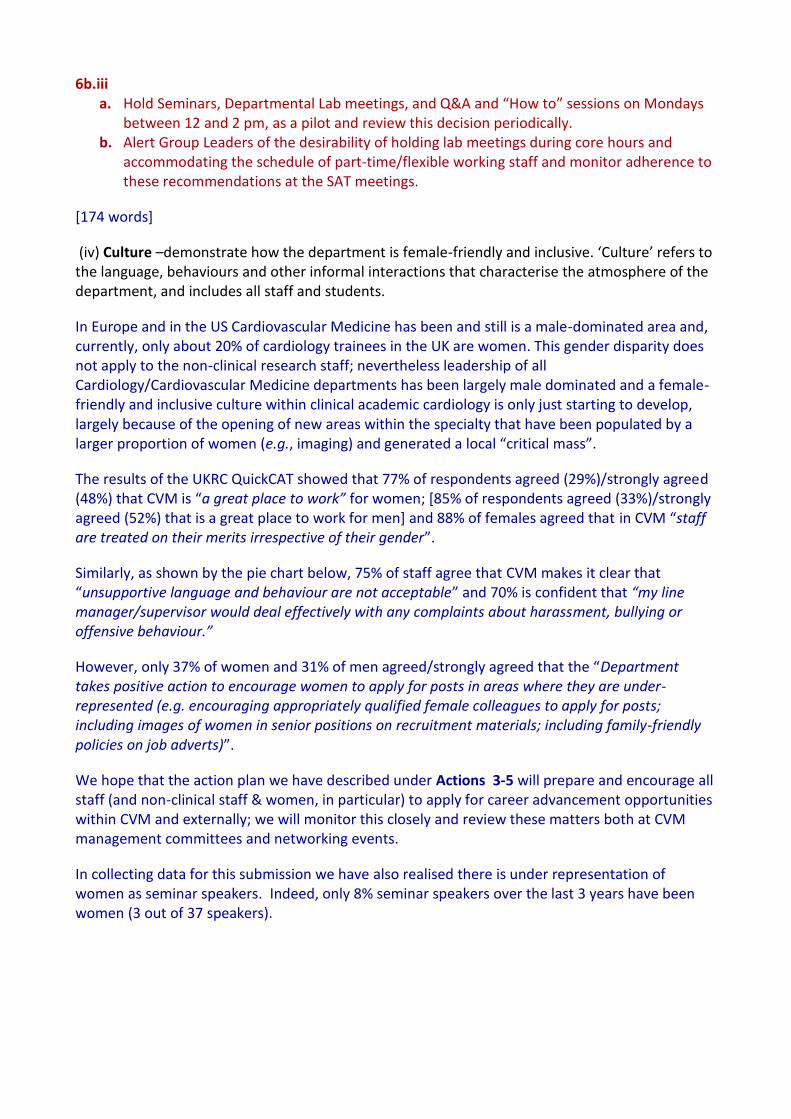
Similarly, as shown by the pie chart below, 75% of staff agree that CVM makes it clear that “unsupportive language and behaviour are not acceptable” and 70% is confident that “my line manager/supervisor would deal effectively with any complaints about harassment, bullying or offensive behaviour.”
However, only 37% of women and 31% of men agreed/strongly agreed that the “Department takes positive action to encourage women to apply for posts in areas where they are under-represented (e.g. encouraging appropriately qualified female colleagues to apply for posts; including images of women in senior positions on recruitment materials; including family-friendly policies on job adverts)”.
We hope that the action plan we have described under Actions 3-5 will prepare and encourage all staff (and non-clinical staff & women, in particular) to apply for career advancement opportunities within CVM and externally; we will monitor this closely and review these matters both at CVM management committees and networking events.
In collecting data for this submission we have also realised there is under representation of women as seminar speakers. Indeed, only 8% seminar speakers over the last 3 years have been women (3 out of 37 speakers).
“My Department makes it clear that unsupportive language and behaviour are not acceptable (e.g. condescending or intimidating language, ridicule, overly familiar behaviour, jokes/banter that stereotype women or men or focus on their appearance).”
“I am confident that my line manager/supervisor would deal effectively with any complaints about harassment, bullying or offensive behaviour.”
ACTIONS
6b.iv a. Add a section welcoming new members of staff on the Department website (including
short bios & photograph) to facilitate networking. b. Increased the visibility of women in CVM to provide positive role models and balance the
predominant male profile of the Department. This will be done by adding a section on the CVM website that profiles and focuses on women and promotes their achievements.
c. Seminar organisers will ask for suggestions of female speakers to enable a better gender balance going forward.
[431 words]
Agree 38%
Strongly agree 32%
Disagree 8%
Strongly disagree
11%
Don’t know 11%
Agree 48%
Strongly agree 27%
Disagree 13%
Strongly disagree
6%
Don’t know 6%
(v) Outreach activities – comment on the level of participation by female and male staff in outreach activities with schools and colleges and other centres. Describe who the programmes are aimed at, and how this activity is formally recognised as part of the workload model and in appraisal and promotion processes.
CVM is involved in a number of outreach activities that involve all staff. For instance, we contributed to/hosted BBC Bang Goes the Theory, Oxford University Press training videos, and NHS Innovation/ISIS videos and provided a base for Public-Patient Involvement Groups in collaboration with NIHR Research Design Service. We run stands at the Oxford BRC Open Days and will be holding an Open Day in support of International Clinical Trials Day/UKCRF and have produced a patient information video with Oxford Sparks. In addition, our Staff work closely with the BHF (our main funder) helping them with outreach activities and public engagement events.
As outreach activities will be a priority for RDM, we envisage that this programme will expand further. In particular, we plan to put in place activities that would encourage female graduates to consider cardiovascular medicine as a career option, both at the non-clinical and clinical level.
ACTIONS
6b.v a. Start central co-ordination and support for public engagement activities, e.g., database of
people willing to get involved.
[167 words]
7. Flexibility and managing career breaks
a) Provide data for the past three years (where possible with clearly labelled graphical
illustrations) on the following with commentary on their significance and how they have affected action planning.
(i) Maternity return rate – comment on whether maternity return rate in the department has improved or deteriorated and any plans for further improvement. If the department is unable to provide a maternity return rate, please explain why.
The University offers one of the most generous maternity leave schemes in the HEI sector. Academic and research staff is entitled to 52 weeks’ leave: 26 on full pay, 13 on SMP, and 13 unpaid. Nine women took maternity leave over the past 3 years; of those all but one returned to work. The one who didn’t return to work in CVM following maternity leave did so because of her husband’s relocation.
[72 words]
(ii) Paternity, adoption and parental leave uptake – comment on the uptake of paternity leave by grade and parental and adoption leave by gender and grade. Has this improved or deteriorated and what plans are there to improve further.
Uptake of Statutory Paternity leave is increasing (e.g., 2008/09: none; 2009/10: 3; 2010/11:1; 2011/12: 4). Numbers are actually higher than those reported as some individuals have taken
advantage of informal arrangements to take time out for such responsibilities. In one case, although not eligible for the University scheme (due to recently taking up his post), one postdoctoral fellow was granted two weeks paternity/compassionate leave.
[64 words]
(iii) Numbers of applications and success rates for flexible working by gender and grade – comment on any disparities. Where the number of women in the department is small, applicants may wish to comment on specific examples.
CVM has always been flexible in terms of distribution of hours worked by all staff and has approved all three formal requests for flexible working, as outlined below.
[28 words]
b) For each of the areas below, explain what the key issues are in the department, what steps have been taken to address any imbalances, what success/impact has been achieved so far and what additional steps may be needed.
(i) Flexible working – comment on the numbers of staff working flexibly and their grades
and gender, whether there is a formal or informal system, the support and training provided for managers in promoting and managing flexible working arrangements, and how the department raises awareness of the options available.
While only a minority of staff work part-time, 79% of SAQ respondents agreed that CVM accommodates flexible working arrangements. All of our clinical academics, non-clinical academics and clinical researchers work full time (and have done so for the past 3 years). We currently have three formal flexible working agreements in place (all female, non-clinical, two grade 7 and one grade 8). For example, one member of staff reduced her working hours to 70% FTE, 3 days one week and 4 the next, upon return from her third maternity leave.
We have several other informal agreements for flexible working – e.g., changing working hours as needs change (nursery to school), plus two staff who work from home some of the time.
Many of our non-academic staff have very flexible working patters; for example:
(1) one grade 3 female works 54% FTE as she is a foster carer;
(2) our Research Facilitator initially worked 60% FTE (mon – wed, 9 am-5 pm), as she had a young child. This subsequently changed to 8 am-4 pm upon returning from her second maternity. When her eldest child started school, she requested changing her working hours to 4 shorter days, finishing at 2.30 pm to facilitate school pickup;
(3) our Research Genetics Counsellor, employed on a 30 hrs contract in 2008, asked whether she could work partly from home and the department agreed a 50: 50 split. In 2011 due to change in responsibilities, she requested an increase in hours and currently works 3 days on site + 2 days from home.
(4) our lead Research Nurse member changed her working pattern to 90% overall, but working less in school holidays, again to accommodate childcare.

These examples help illustrate the flexible nature of CVM when it comes to working practises. Flexible working arrangements are discussed at induction; however, from now on we will also bring this and other options up during the ‘Q&A’ session [ACTION 4a.i(b)].
[319 words] (ii) Cover for maternity and adoption leave and support on return – explain what the
department does, beyond the university maternity policy package, to support female staff before they go on maternity leave, arrangements for covering work during absence, and to help them achieve a suitable work-life balance on their return.
The University has good childcare provision, including subsidised places at nurseries, holiday schemes, and au pair services. Many members of staff make use of this provision.
CVM has endeavoured to provide cover during maternity leave where this is needed operationally and where a grant funder pays maternity, leaving the department to pay the cover. For example, employing a research assistant (RA) to help progress the work of postdoctoral researchers on maternity leave.
CVM operates a flexible return to work scheme, where requests to return part-time and build up gradually to hours worked before maternity, or to agree a flexible working arrangement are supported. Indeed some employees never return to full time work [examples in Section 7b(i)]. Some employees return from maternity leave to a full-time position but make use of annual leave accrued during maternity leave to work only 3 days per week for the first 8 to 9 weeks.
[150 words]
Total Words for this section=4706
8. Any other comments – maximum 500 words
Please comment here on any other elements which are relevant to the application, e.g. other SET-specific initiatives of special interest that have not been covered in the previous sections. Include any other relevant data (e.g. results from staff surveys), provide a commentary on it and indicate how it is planned to address any gender disparities identified.
An important part of preparing the Athena Swan application has been the opportunity to receive systematic feedback from staff on how policies and activities in CVM actually operate, and the degree to which they are understood by staff and graduate students. Although we think (and feedback confirms) that CVM is a supportive and friendly Department in which to work, the WGs and questionnaire responses have been useful in identifying areas where we could, and should do better. In particular, CVM needs to improve lines of communication, so that policies are presented clearly, transparently, regularly and accessibly to all staff.
We must improve the information and advice on our web pages, and the links to central University policies, in terms of information regarding training and support, promotion and re-grading, and the flexibility that is already available to cater for people’s needs and circumstances.
Lack of mentoring and appraisal of non-clinical staff has left several of them feel disenfranchised and without obvious milestones and career structure. On the other hand, the demands of clinical training and its rigid structure have been perceived by medically-qualified females undertaking a DPhil as stifling their research and academic career progression. We must pay particular attention to the training and career development of non-clinical staff and support the transition of medically-qualified women from graduate studies to clinical training and academic career paths within the context of the ACTION Points we have already planned.
In addition, our experience suggests that not every postdoc (whether male or female) wants to become an independent researcher with their own research group, and so we will commit to supporting everyone to fulfill their career ambitions at whatever level they wish to progress to; for example, this could include being an applicant, or co-applicant, on a grant in order to give greater ownership of their research.
ACTION
8 a. Introduce a termly seminar with a female researcher talking about their research and their
career path. This would be held over lunch and the attendees could arrange one to one meetings with the speaker afterwards to gain advice relating to their own career paths. This would be coordinated by RDM.
[356 words]
9. Action plan
Provide an action plan as an appendix. An action plan template is available on the Athena SWAN website.

Abbreviations (alphabetical): AC=Athena champion; BHF CRE=British Heart Foundation Centre of Research Excellence; BRC=Oxford Biomedical Research Centre; CCRF= Cardiovascular Clinical Research Facility; CTRF=clinical research training fellowship; CVM=Department of Cardiovascular Medicine; RDM=Radcliffe Department of Medicine; DA=Department administrator; DGS=Director of Graduate Studies; GSA=graduate studies administrator; HoD=Head of Department; JRH=John Radcliffe Hospital; OCMR=Oxford Centre for Clinical Magnetic Resonance; PO=personnel officer; QuickCAT=UKRC (now WISE) Culture Analysis Tool; RA=recruitment administrator; RF=research facilitator; SAQ= self-assessment questionnaire; SAT=Self-Assessment Team; SO=seminar organiser; WG=working group; WTCHG=Wellcome Trust Centre for Human Genetics.
Ac
tio
n
Description of action Action taken already and outcome at March 2013
Further action planned at April 2013
Progress Log
Responsibility Timescale Start date Success Measure
2 Self-assessment/Plan for the future
2c Appoint an “Athena champion” who will dedicate 20-25% of their time to implementing the Action Plan.
Agreed with HoD
DA/PO On-going November 2013
Person in place by next Term.
3 Student Data
3.iv(a) Monitor applicants, admission figures and the rate of degree attainment between males and females for medically qualified and science graduate students
Adjust database
Populate database with information
DGS/GSA On-going November 2013
Statistics more readily available and results displayed in the Department’s website.
3.iv(b) Support the Medical Science Division’s consultation on offering part-time research degrees.
Discussed by the SAT and WGs and approved by HoD
Divisional consultation launched 22.4.13
DGS/GSA On-going On-going Impact on the Division’s decision.
3.v(a) Add information on Athena SWAN and family friendly policies to our DPhil and CTRF prospectus and advertisement.
Review our current wording
Revise wording for the next call
RF/GSA Next recruitment call
November 2013
Attract more female applicants.
3.vi(a) Monitor adherence to training for first-time supervisors and refresher training for other supervisors.
Discussed by the SAT and WGs and agreed by HoD and DA
Write to staff and start collecting the information
DGS/HoD/GSA On-going From now on
Relevant staff would have completed the training within the next 2 years.
xxxvi
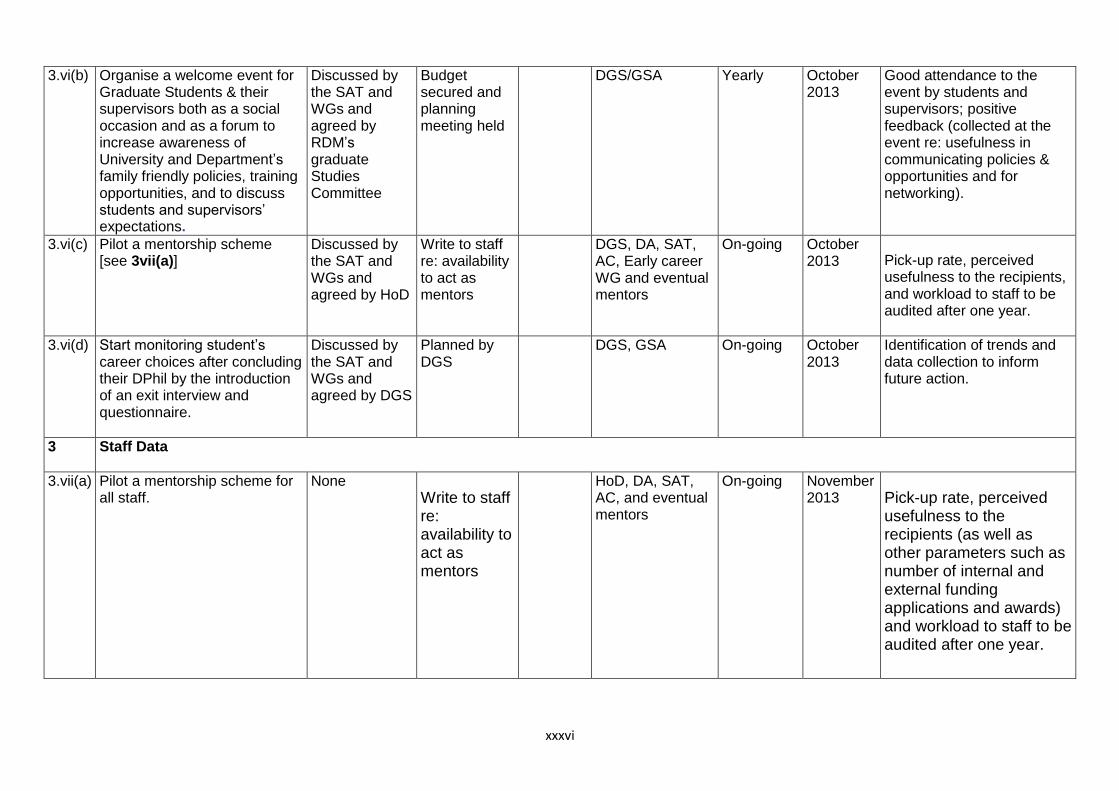
3.vi(b) Organise a welcome event for Graduate Students & their supervisors both as a social occasion and as a forum to increase awareness of University and Department’s family friendly policies, training opportunities, and to discuss students and supervisors’ expectations.
Discussed by the SAT and WGs and agreed by RDM’s graduate Studies Committee
Budget secured and planning meeting held
DGS/GSA Yearly October 2013
Good attendance to the event by students and supervisors; positive feedback (collected at the event re: usefulness in communicating policies & opportunities and for networking).
3.vi(c) Pilot a mentorship scheme [see 3vii(a)]
Discussed by the SAT and WGs and agreed by HoD
Write to staff re: availability to act as mentors
DGS, DA, SAT, AC, Early career WG and eventual mentors
On-going October 2013 Pick-up rate, perceived
usefulness to the recipients, and workload to staff to be audited after one year.
3.vi(d) Start monitoring student’s career choices after concluding their DPhil by the introduction of an exit interview and questionnaire.
Discussed by the SAT and WGs and agreed by DGS
Planned by DGS
DGS, GSA On-going October 2013
Identification of trends and data collection to inform future action.
3 Staff Data
3.vii(a) Pilot a mentorship scheme for all staff.
None Write to staff re: availability to act as mentors
HoD, DA, SAT, AC, and eventual mentors
On-going November 2013 Pick-up rate, perceived
usefulness to the recipients (as well as other parameters such as number of internal and external funding applications and awards) and workload to staff to be audited after one year.
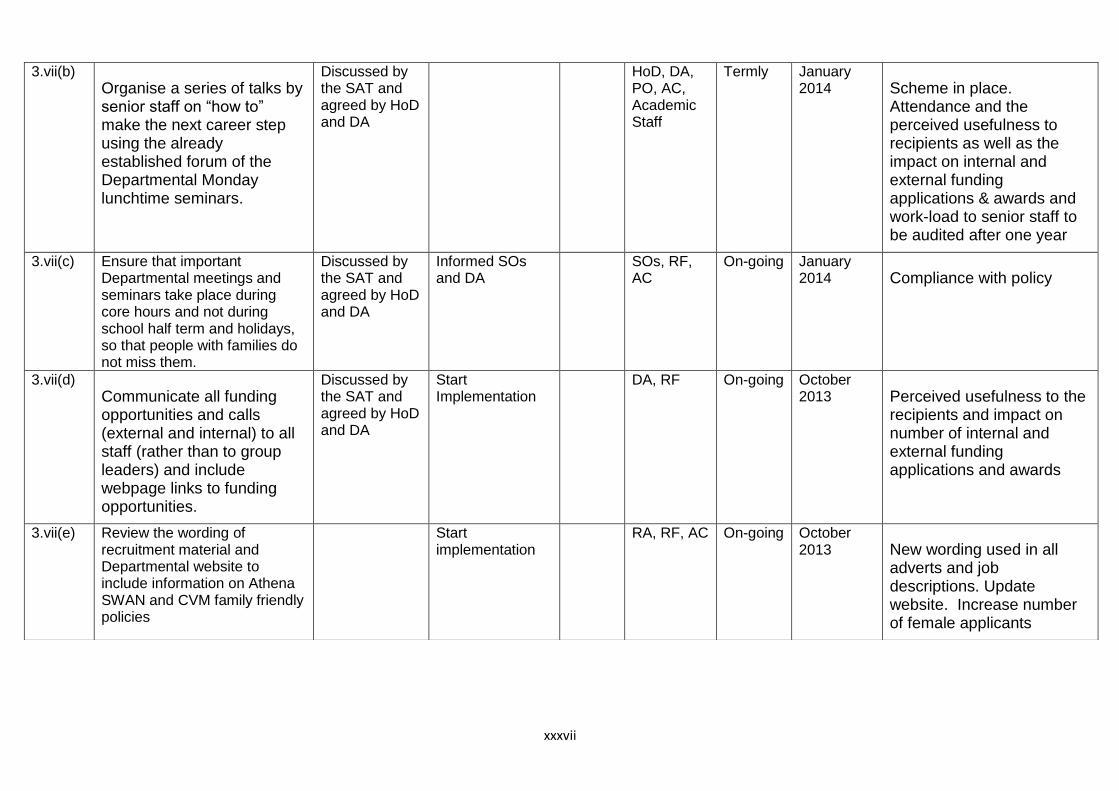
xxxvii
3.vii(b) Organise a series of talks by senior staff on “how to” make the next career step using the already established forum of the Departmental Monday lunchtime seminars.
Discussed by the SAT and agreed by HoD and DA
HoD, DA, PO, AC, Academic Staff
Termly January 2014 Scheme in place.
Attendance and the perceived usefulness to recipients as well as the impact on internal and external funding applications & awards and work-load to senior staff to be audited after one year
3.vii(c) Ensure that important Departmental meetings and seminars take place during core hours and not during school half term and holidays, so that people with families do not miss them.
Discussed by the SAT and agreed by HoD and DA
Informed SOs and DA
SOs, RF, AC
On-going January 2014 Compliance with policy
3.vii(d) Communicate all funding opportunities and calls (external and internal) to all staff (rather than to group leaders) and include webpage links to funding opportunities.
Discussed by the SAT and agreed by HoD and DA
Start Implementation
DA, RF On-going October 2013 Perceived usefulness to the
recipients and impact on number of internal and external funding applications and awards
3.vii(e) Review the wording of recruitment material and Departmental website to include information on Athena SWAN and CVM family friendly policies
Start implementation
RA, RF, AC On-going October 2013 New wording used in all
adverts and job descriptions. Update website. Increase number of female applicants

xxxviii
3.vii(f) Increase the visibility of positive female role models by including mini-biographies/testimonials of female scientists & publicise achievements, awards, and fellowships in the CVM website.
Start implementation
RF, AC On-going October 2013
Positive feed-back in future surveys – increased number of female applicants to internal and external career opportunities
3.vii(g) Ensure a strong female representation on short-listing and interview panels and on search panels for all academic posts and aim to have at least one woman on the long-list of potential recruits to be considered for such posts.
Identify suitable female representatives from CVM and RDM
HoD, DA, PO
On-going From now on
Scheme in place. Increase number of female applicants and female appointments.
4 Key Career Transition Points, Appointments and Promotions
4a.ii(a) Include a section detailing the processes in place for merit awards, promotion and re-grading on the Department website and induction material.
Start implementation
DA, PO, AC
On-going October 2013
Update website and positive feedback from future staff surveys
4a.ii(b) Establish an open Q&A session on merit awards, promotion, re-grading & family friendly policies.
DA, PO, AC
Yearly October 2013
Improved understanding and transparency on these matters as assessed by future staff surveys
4a.ii(c) Carry out a systematic review of all staff annually with regard to promotion, re-grading and merit awards.
HoD, DA, PO, eventual committee members
Yearly October 2013
Better gender balance in promotion and re-grading exercises

xxxix
4b.ii(a) Encourage research staff (e.g. grade 8), junior clinical staff, and women, in particular, to apply for pump-priming grants from our internal funding sources (via our website, “How to” talks, and at PDR).
HoD, DA, RF, SAT
On-going October 2013
Increased number of applications and attainment of these awards by female research staff
4b.ii(b) Ensure that all applications for externally funded independent fellowships are reviewed internally and that practise interviews are conducted.
Start full implementation
HoD, Senior Academic Staff
On-going From now on
Increased number of applications and attainment of these awards by all research staff and females, in particular
5 Career Advice and Support
5.i(a) Pilot PDR for those individuals at key career transition points namely: graduate students in their final year, all staff 12-18 months before end of contract/fellowship, Grade 8, and clinical research staff in training.
Identify training requirements for senior staff carrying out PDRs
HoD, Senior Academic Staff
On-going November 2013
Scheme in place. Pick-up and perceived usefulness to recipients, impact on internal and external funding applications & awards, and work-load to senior staff to be audited after one year
5.i(b) Introduce training for everyone who will be conducting PDRs. We will run a training workshop in CVM, bringing in an expert from the Oxford Learning Institute.
DA, AC Yearly November 2013
Scheme in place – All relevant staff trained in the next 2 years.
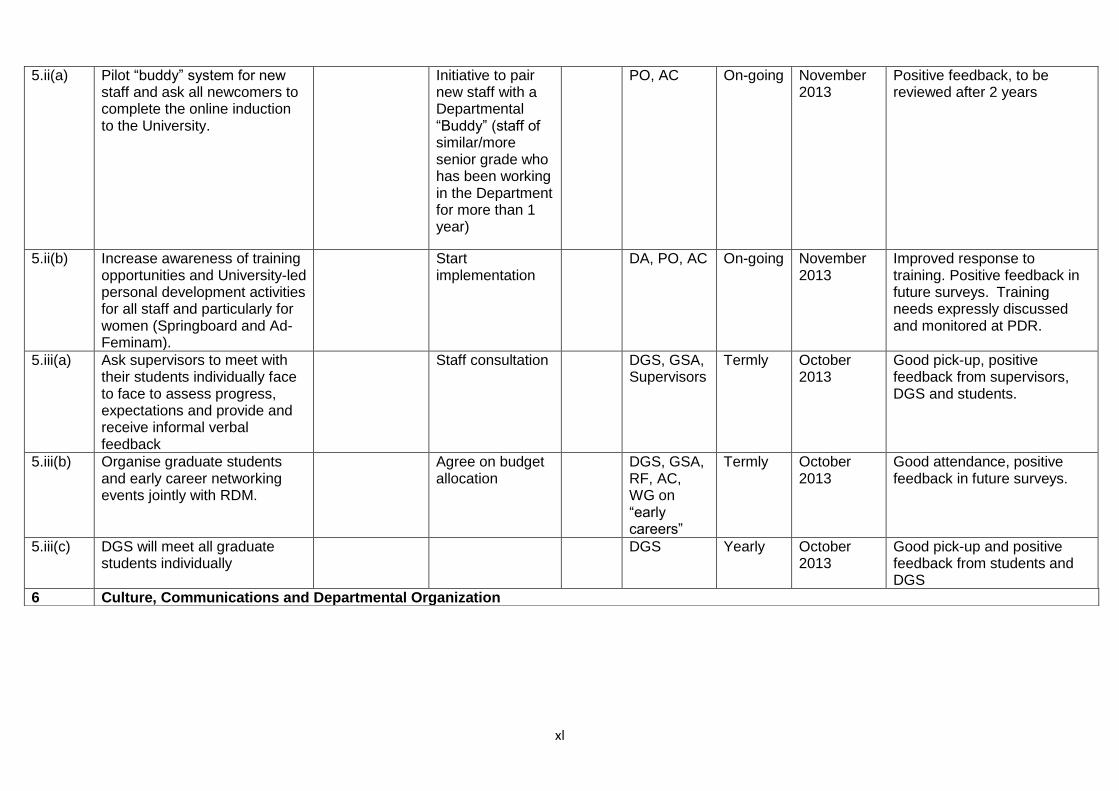
xl
5.ii(a) Pilot “buddy” system for new staff and ask all newcomers to complete the online induction to the University.
Initiative to pair new staff with a Departmental “Buddy” (staff of similar/more senior grade who has been working in the Department for more than 1 year)
PO, AC On-going November 2013
Positive feedback, to be reviewed after 2 years
5.ii(b) Increase awareness of training opportunities and University-led personal development activities for all staff and particularly for women (Springboard and Ad-Feminam).
Start implementation
DA, PO, AC On-going November 2013
Improved response to training. Positive feedback in future surveys. Training needs expressly discussed and monitored at PDR.
5.iii(a) Ask supervisors to meet with their students individually face to face to assess progress, expectations and provide and receive informal verbal feedback
Staff consultation DGS, GSA, Supervisors
Termly October 2013
Good pick-up, positive feedback from supervisors, DGS and students.
5.iii(b) Organise graduate students and early career networking events jointly with RDM.
Agree on budget allocation
DGS, GSA, RF, AC, WG on “early careers”
Termly October 2013
Good attendance, positive feedback in future surveys.
5.iii(c) DGS will meet all graduate students individually
DGS Yearly October 2013
Good pick-up and positive feedback from students and DGS
6 Culture, Communications and Departmental Organization
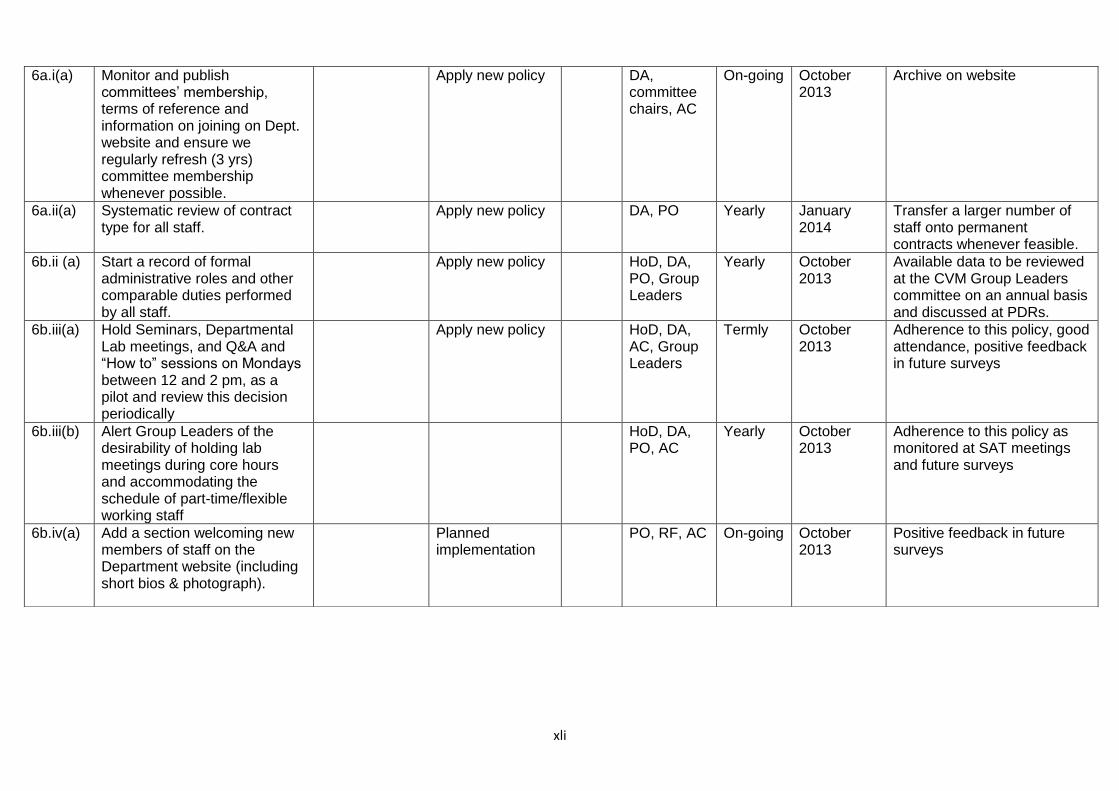
xli
6a.i(a) Monitor and publish committees’ membership, terms of reference and information on joining on Dept. website and ensure we regularly refresh (3 yrs) committee membership whenever possible.
Apply new policy DA, committee chairs, AC
On-going October 2013
Archive on website
6a.ii(a) Systematic review of contract type for all staff.
Apply new policy DA, PO Yearly January 2014
Transfer a larger number of staff onto permanent contracts whenever feasible.
6b.ii (a) Start a record of formal administrative roles and other comparable duties performed by all staff.
Apply new policy HoD, DA, PO, Group Leaders
Yearly October 2013
Available data to be reviewed at the CVM Group Leaders committee on an annual basis and discussed at PDRs.
6b.iii(a) Hold Seminars, Departmental Lab meetings, and Q&A and “How to” sessions on Mondays between 12 and 2 pm, as a pilot and review this decision periodically
Apply new policy HoD, DA, AC, Group Leaders
Termly October 2013
Adherence to this policy, good attendance, positive feedback in future surveys
6b.iii(b) Alert Group Leaders of the desirability of holding lab meetings during core hours and accommodating the schedule of part-time/flexible working staff
HoD, DA, PO, AC
Yearly October 2013
Adherence to this policy as monitored at SAT meetings and future surveys
6b.iv(a)
Add a section welcoming new members of staff on the Department website (including short bios & photograph).
Planned implementation
PO, RF, AC On-going October 2013
Positive feedback in future surveys
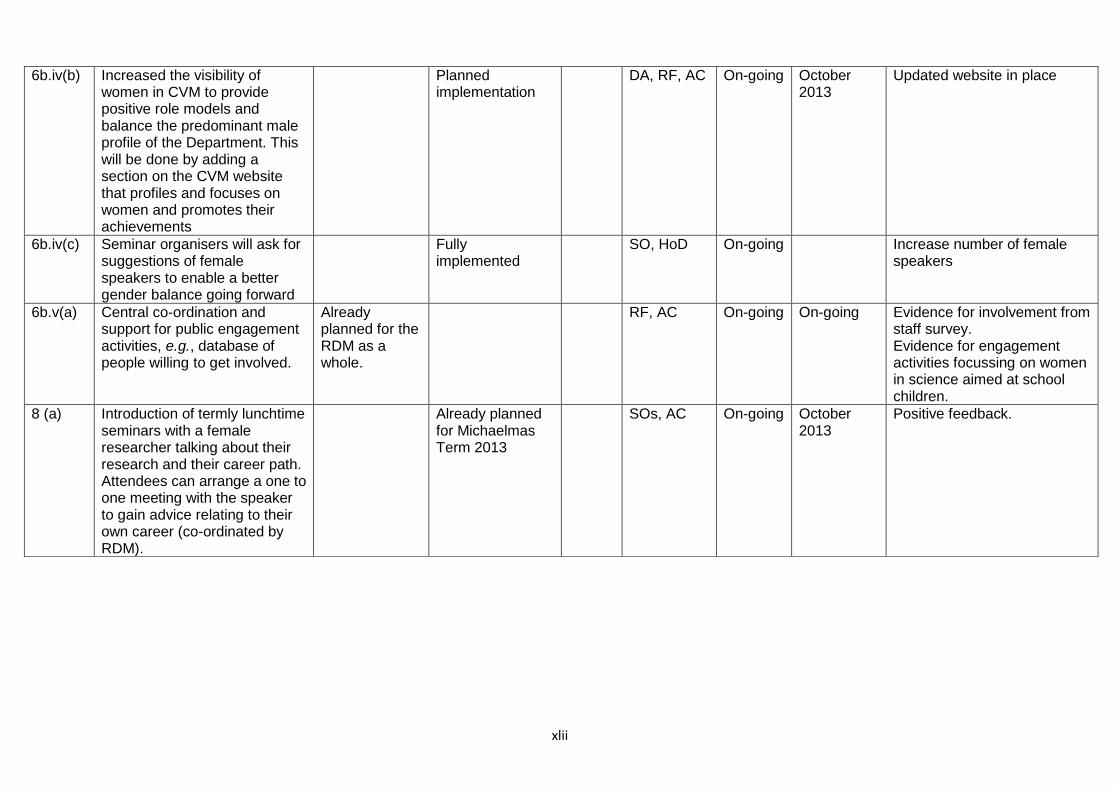
xlii
6b.iv(b)
Increased the visibility of women in CVM to provide positive role models and balance the predominant male profile of the Department. This will be done by adding a section on the CVM website that profiles and focuses on women and promotes their achievements
Planned implementation
DA, RF, AC On-going October 2013
Updated website in place
6b.iv(c)
Seminar organisers will ask for suggestions of female speakers to enable a better gender balance going forward
Fully implemented
SO, HoD On-going Increase number of female speakers
6b.v(a) Central co-ordination and support for public engagement activities, e.g., database of people willing to get involved.
Already planned for the RDM as a whole.
RF, AC On-going On-going Evidence for involvement from staff survey. Evidence for engagement activities focussing on women in science aimed at school children.
8 (a) Introduction of termly lunchtime seminars with a female researcher talking about their research and their career path. Attendees can arrange a one to one meeting with the speaker to gain advice relating to their own career (co-ordinated by RDM).
Already planned for Michaelmas Term 2013
SOs, AC On-going October 2013
Positive feedback.





























