Ateneo de Zamboanga UniversityCollege of Nursing
NURSING SKILLS OUTPUT (NSO)Report No. 10RADIOACTIVE UPTAKE and
(1311 UPTAKE) EXCRETION TESTI. DESCRIPTION: A radioactive iodine
uptake (RAIU) test uses aradioactive tracerand a special probe to
measure how much tracer thethyroid glandabsorbs from theblood. The
test can show how much tracer is absorbed by the thyroid gland and
if it is evenly spread in the gland. This helps your doctor know if
the thyroid gland is working properly. The radioactive tracer
commonly used in this test is iodine.A radioactive iodine uptake
test is done to find problems with how the thyroid gland works,
such ashyperthyroidism. An RAIU test may be done at the same time
as a thyroid scan.
II. MATERIALS /EQUIPMENT NEEDED: radioactiveiodinein the form of
capsule or fluid, scintillation counter The dose is typically
0.150.37MBq(410Ci) of131I sodium iodide, or 3.77.4 MBq (100200 Ci)
of123I sodium iodide.
III. PROCEDURE1. Explain the test and the purpose of the test to
the patient. He will need to begin fasting at midnight the night
before the test. Explain that he will receive the radioactive
iodine in capsule or liquid form and then be scanned at the 6-hour
interval and again at a 24-hour interval. If the patient is an
inpatient, the nurse or a technician will administer the dose to
him right on the nursing unit at the specified time. Be sure to
note the exact time the dose is administered. If he is an
outpatient, the patient will usually be given the capsule to take
at home at a certain time. Be sure you instruct the patient to take
the dose at the specified time. If he misses the exact time, be
sure to have the patient write down the exact time he did take the
dose. Be sure to explain that the test is painless. Be sure to
explain that the radioactive material is very small and will not
harm him.2. Check the patient's history for IODINE EXPOSURE , which
may interfere with the test results. Note any prior radiological
tests using contrast media, nuclear medicine procedures, or current
use of iodine preparations or thyroid medications on the film
request form. Substances containing iodine, such as dyes used for
the intravenous pyelogram (IVP), gallbladder series, or
bronchograms may cause incorrect test results. Iodine
hypersensitivity (allergy) is not considered a contraindication for
this test because the amount of iodine used is similar to the
amount consumed in a normal diet.3. Radioactive iodine uptake
testing is contraindicated during pregnancy and lactation because
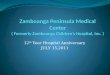
of possible teratogenic effects.4. After ingesting an oral dose of
radioactive iodine, the patient's thyroid is scanned at 6 hours and
at 24 hours by placing the anterior portion of his neck in front of
an external single counting probe.5. Instruct the patient to resume
a light diet 2 hours after taking the oral dose of radioactive
iodine. When the study is complete, the patient may resume a normal
diet.
IV. DIAGRAM/ILLUSTRATION:
V. NURSING RESPONSIBILITIES :Before procedure: Do not eat for 2
hours before the test. For an RAIU, you will swallow a dose of
radioactive iodine. Iodine can be taken as a capsule or a fluid 4
to 24 hours before the test. Iodine has little or no taste. Just
before the test, you will remove your dentures (if you wear them)
and all jewelry or metal objects from around your neck and upper
body. Before a radioactive iodine uptake (RAIU) test, you need to
sign a consent form that says you understand the risks of the test
and agree to have it done. Talk to your doctor about any concerns
you have regarding the need for the test, its risks, how it will be
done or what the results will mean. Do not take any antithyroid
medicine for 5 to 7 days before the test. Your doctor may ask you
to eat a low-iodine diet. During procedure Explain the test and the
purpose of the test to the patient. He will need to begin fasting
at midnight the night before the test. Explain that he will receive
the radioactive iodine in capsule or liquid form and then be
scanned at the 6-hour interval and again at a 24-hour interval. If
the patient is an inpatient, the nurse or a technician will
administer the dose to him right on the nursing unit at the
specified time. Radioactive iodine uptake testing is
contraindicated during pregnancy and lactation because of possible
teratogenic effects. After ingesting an oral dose of radioactive
iodine, the patient's thyroid is scanned at 6 hours and at 24 hours
by placing the anterior portion of his neck in front of an external
single counting probe. Instruct the patient to resume a light diet
2 hours after taking the oral dose of radioactive iodine. When the
study is complete, the patient may resume a normal diet. After
procedure At 6 hours, 5% to 20% of the radioactive iodine should
accumulate in the thyroid. At 24 hours, accumulation should be 15%
to 40%. The balance of the radioactive iodine is excreted in the
urine. Local variations in the normal range of iodine uptake may
occur due to regional differences in dietary iodine intake and
procedural differences among laboratories. Below-normal iodine
uptake may indicate hypothyroidism, subacute thyroiditis, or iodine
overload. Above-normal iodine uptake may indicate hyperthyroidism,
early Hashimoto's thyroiditis, hypoalbuminemia, lithium ingestion,
or iodine-deficient goiter. However, in hyperthyroidism, the rate
of turnover may be so rapid that a false normal measurement occurs
at 24 hours.
Reference: Medical -Surgical Nursing by Lewis Dirksen
http://www.netplaces.com/thyroid-disease/hyperthyroidism/radioactive-iodine-uptake-raiu-and-scan.htm
September 29, 2014 MS. CHARLITA F. AHMAD RN MN Date Clinical
Instructors Initials
CAMILLE JADE DE JESUSBSN III-C
Ateneo de Zamboanga UniversityCollege of Nursing
NURSING SKILLS OUTPUT (NSO)Report No.11TRH SIMULATION TESTI.
DESCRIPTION: Prior to the availability of sensitive TSH assays,
thyrotropin releasing hormone (TRH) stimulation tests were relied
upon for confirming and assessing the degree of suppression in
suspected hyperthyroidism. Typically, this stimulation test
involves determining basal TSH levels and levels 15 to 30 minutes
after an intravenous bolus of TRH. Normally, TSH would rise into
the concentration range measurable with less sensitive TSH assays.
Third generation TSH assays do not have this limitation and thus
TRH stimulation is generally not required when third generation TSH
assays are used to assess degree of suppression.TRH-stimulation
testing however continues to be useful for the differential
diagnosis of secondary (pituitary disorder)and tertiary
(hypothalamic disorder) hypothyroidism. Patients with these
conditions appear to have physiologically inactive TSH in their
circulation that is recognized by TSH assays to a degree such that
they may yield misleading, "euthyroid" TSH results.Use and
Interpretation: Helpful in diagnosis in patients with confusing
TFTs. In primary hyperthyroidism TSH are low and TRH administration
induces little or no change in TSH levels In hypothyroidism due to
end organ failure, administration of TRH produces a prompt increase
in TSH In hypothyroidism due to pituitary disease (secondary
hypothyroidism)administration of TRH does not produce an increase
in TSH In hypothyroidism due to hypothalamic disease (tertiary
hypothyroidism), administration of TRH produces a delayed (60-120
minutes, rather than 15-30 minutes) increase in TSH
II. MATERIALS /EQUIPMENT NEEDED:3 serum tubesTRH 200 microgm
(adults). The dose for children is 7 microgm/kg to a max 200
microgm.
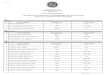
III. PROCEDURE1. The TRH Stimulation Test, however, is a much
more sensitive test because it evaluates how well the hypothalamus,
pituitary and thyroid glands are functioning and communicating
together at the same time, and in in real time2. Begins by baseline
thyroid and pituitary hormone levels being drawn.3. Then you are
given an injection of a tiny amount of thyrotropin releasing
hormone, which stimulates the pituitary to release TSH, a hormone
which signals the thyroid to release thyroxine, the main thyroid
hormone.4. A second blood sample is drawn 20 to 30 minutes later,
and the TSH level is retested. Low thyroidconditionswill result in
an exaggerated response, and excessive thyroid function and
pituitary insufficiency states will result in a depressed
response.
IV. DIAGRAM/ILLUSTRATION:
V. NURSING RESPONSIBILITIES :Before procedure: Patient must
discontinue thyroid medications 3-4 weeks before the test. During
procedure Begins by baseline thyroid and pituitary hormone levels
being drawn. Then you are given an injection of a tiny amount of
thyrotropin releasing hormone, which stimulates the pituitary to
release TSH, a hormone which signals the thyroid to release
thyroxine, the main thyroid hormone. A second blood sample is drawn
20 to 30 minutes later, and the TSH level is retested. Low
thyroidconditionswill result in an exaggerated response, and
excessive thyroid function and pituitary insufficiency states will
result in a depressed response.
After procedure Normal basal values of TSH should be 0.2-6
IU/mL. The normal increment in TSH at 20 min should be 5-30 (mean
15) IU/mL with a slight diminution at 60 min. Exaggerated TSH
response is seen in primary hypothyroidism. A flat response is seen
in primary hyperthyroidism; but also in some apparently euthyroid
patients with ophthalmic Graves disease or multinodular goitre. A
delayed response with the TSH concentration lower at 20 than 60 min
may be seen in hypothalamic dysfunction. Various drugs can modify
the TSH response: it is reduced by glucocorticoids, DOPA agonists
eg L-DOPA, bromocryptine and fluoxetine; and enhanced by DOPA
antagonists eg metoclopramide, oestrogens and theophylline and
sertraline (but ? only in thyroxine treated subjects). In neonates,
peak TSH responses < 35mU/L are not associated with subsequent
hypothyroidism, whereas responses > 35 mU/L are associated with
a rate of subsequent hypothyroidism of 35%. The TSH response is
flat in most cases of TSHoma whereas in thyroid hormone resistance
the TSH response is brisk.
Reference: Medical -Surgical Nursing by Lewis Dirksen
http://www.pathology.leedsth.nhs.uk/dnn_bilm/Investigationprotocols/Pituitaryprotocols/TRHTest.aspx
September 29, 2014 MS. CHARLITA F. AHMAD RN MN Date Clinical
Instructors Initials
CAMILLE JADE DE JESUSBSN III-C