Embed Size (px)
Citation preview

International Psychogeriatrics (2016) 2811 1761ndash1774 Ccopy International Psychogeriatric Association 2016doi101017S1041610216000922
R E V I E W
A systematic review of the relationship between behavioraland psychological symptoms (BPSD) and caregiver well-being
Alexandra Feast1 Esme Moniz-Cook2 Charlotte Stoner3 Georgina Charlesworth3
and Martin Orrell41Division of Psychiatry University College London London UK2Faculty of Health and Social Care University of Hull Hull UK3Research Department of Clinical Educational and Health Psychology University College London London UK4Institute of Mental Health University of Nottingham Nottingham UK
ABSTRACT
Background Behavioral and psychological symptoms in dementia (BPSD) are important predictors ofinstitutionalization as well as caregiver burden and depression Previous reviews have tended to group BPSDas one category with little focus on the role of the individual symptoms This review investigates the role of theindividual symptoms of BPSD in relation to the impact on different measures of family caregiver well-being
Methods Systematic review and meta-analysis of papers published in English between 1980 and December2015 reporting which BPSD affect caregiver well-being Paper quality was appraised using the Downs andBlack Checklist (1998)
Results Forty medium and high quality quantitative papers met the inclusion criteria 16 were suitableto be included in a meta-analysis of mean distress scores Depressive behaviors were the most distressingfor caregivers followed by agitationaggression and apathy Euphoria was the least distressing Correlationcoefficients between mean total behavior scores and mean distress scores were pooled for four studiesIrritability aberrant motor behavior and delusions were the most strongly correlated to distress disinhibitionwas the least correlated
Conclusions The evidence is not conclusive as to whether some BPSD impact caregiver well-being morethan others Studies which validly examined BPSD individually were limited and the included studies usednumerous measures of BPSD and numerous measures of caregiver well-being Future research may benefitfrom a consistent measure of BPSD examining BPSD individually and by examining the causal mechanismsby which BPSD impact well-being by including caregiver variables so that interventions can be designed totarget BPSD more effectively
Key words behavioral and psychological symptoms of dementia carer dementia neuropsychiatric symptoms quality of life
Introduction
Behavioral and psychological symptoms in de-mentia (BPSD) can occur in up to 90 ofpeople with dementia and have been associatedwith the breakdown of home care increasedpsychiatric referral misuse of medication andincreased healthcare costs (Cerejeira et al 2012)BPSD are described as a major source ofdistress for the caregiver (Craig et al 2005Tan et al 2005 Bandeira et al 2007) and
Correspondence should be addressed to Alexandra Feast 6th Floor Maple House149 Tottenham Court Road London W1T 7NF UK Phone 0300 555 1200ext 64491 Email afeastuclacuk Received 4 Sep 2015 revision requested2 Nov 2015 revised version received 5 Feb 2016 accepted 25 May 2016 Firstpublished online 27 June 2016
are composed of wide-ranging symptoms suchas agitation aggression calling out repeatedlysleep disturbance wandering and apathy Themajority of past research which has investigatedthe empirical relationship between BPSD and poorcaregiver outcomes has used summative BPSDscores therefore it remains unclear as to whetherspecific individual symptoms impact caregiversdifferentially (Mohamed et al 2010 Rocca et al2010)
The limited research which has distinguishedbetween symptoms is mainly exploratory and doesnot control for the effect of multiple BPSD(Ballard et al 1995 Gonzalez-Salvador et al 1999Neundorfer et al 2001 Lim et al 2008) However
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1762 A Feast et al
Ornstein et al (2012) have advanced the field byexamining how and why symptoms clusters impactcaregiver depression Nevertheless the symptomswere clustered rather than individually representedand the systematic review did not employ a formalmethod of synthesis but instead a descriptiveanalysis was given along with tallying of symptoms
It is often the case that BPSD are presented in asummative fashion due to the nature of the outcomemeasure and how the total score is calculatedand are consequently usually operationalized as asingle construct of ldquobehavior problemrdquo thereforethe data cannot be extracted Research by Fauthand Gibbons (2014) highlighted the extensiveinconsistencies in identifying BPSD that arethe most problematic These inconsistences arepartly due to whether ldquoproblematicrdquo is definedand measured in terms of symptom prevalenceintensity distress rating or association withcaregiver outcomes such as depressive symptoms(Ornstein et al 2012) A review by Black andAlmeida (2004) has progressed our understandingof the association between BPSD as a wholeand the burden of care and caregiver depressionby performing a meta-analysis However multipletypes of behavior measures burden measuresand measures of depression were pooled in thesame meta-analysis In future meta-analyses it isimportant to combine the same outcome measuresof a particular construct such as ldquodistressrdquo in orderto ensure the statistical analysis is valid ratherthan combining multiple types of measures Thisis addressed in the current review
As recommended by Ornstein et al (2012) it isnecessary to design future systematic reviews whichcapture the complexity of unique behaviors in orderto further our understanding of their differentialimpact upon caregivers The aim of this studywas to respond to Ornsteinrsquos recommendation andto systematically review the relationship betweenindividual BPSD and caregiver well-being in orderto identify which BPSD are the most problematicfor caregivers This was achieved by distinguishingbetween psychological constructs of caregiveroutcome (distress burden strain stress) withineach meta-analysis and by distinguishing betweenhow BPSD are measured (prevalence frequencyand total score) within each meta-analysis
Methods
Identification and selection of studiesA search strategy combining medical subjectheadings and text words relating to dementiaBPSD mental disorders and behaviors behaviorselder care significant others carers family
daughters aged carer burden carer strain carerdistress and cost of illness was devised and adaptedfor five electronic databases Searches of studiespublished between 1980 and December 2015 werecarried out through PsycINFO CINAHL EBSCO(Cumulative Index to Nursing and Allied Health)MEDLINE EMBASE and Web of Science(including Science Citation Index-Expanded (SCI-EXPANDED) Conference Proceedings CitationIndex-Science (CPCI-S) Social Science CitationIndex (SSCI) Conference Proceedings CitationIndex-Social Science amp Humanities (CPCI-SSH)and reference lists of included studies Studieswere restricted to peer-reviewed original paperspublished in English and included participants whowere family caregivers of someone with dementiaused a measure of caregiver response to BPSDand a measure of BPSD and reported data forboth measures Reviews conference proceedingsconference abstracts theses supplements reportsletters and non-peer reviewed papers wereexcluded
Quality appraisalTwo reviewers (AF and CS) assessed theincluded papers for methodological quality anddisagreements were resolved by discussion The 27-item Downs and Black Checklist (1998) was usedto assess quality Quality thresholds were those usedin a previous systematic review (Crellin et al 201475 for high quality 50 to 74 for mediumquality) Agreement was measured using Cohenrsquos κweighted for closeness of scores
AnalysisSummary statistics for each comparable caregiveroutcome associated with each behavior (meansstandard deviation and sample size) were extractedfor each study and were used to calculate the pooledweighted mean and standard deviation for thatoutcome The following formulae were used
Mean for combined studiessum
i n i m isumi n i
where ni isthe sample size for study 1 and mi is the mean forstudy 1 (Price 1970) The standard deviation of thecombined studies [Σi (ni ndash 1) (sdi)2 ((Σi ni) ndash T)]where T is the number of studies (all summationsfrom 1 to T) (Cohen 1988) Standard deviationswere converted to standard errors SE = SDN
MedCalc software (Version 15 Ostend Bel-gium) was used to perform a meta-analysis ofcomparable studies where possible in order toproduce a pooled effect Studies with smallerstandard errors and larger sample sizes weregiven more weight in the calculation The I2
statistic was calculated to denote the percentage ofobserved total variation across studies that is due
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1763
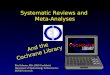
Records identified through database searching (n = 12244)
MEDLINE Ovid = 3618EMBASE Ovid = 576 PsycINFO Ovid = 1502 CINAHL EBSCO = 1056 OpenGrey = 30 Web of Science= 5454
Records after duplicates removed (n = 9485)
Records excluded following the screening of titles and abstracts
(n = 8892)
Studies included (n = 32)
Full-text articles excluded n = 553
(No data on the association between BPSD
and distress n = 425 ) (Not English n = 32)
(No dementia n = 20 ) (Not a family carer n = 22)
(Review n = 35) (Report n = 1)
(Residential care n = 17) (Thesis n = 1)
Full-text screened and articles assessed for eligibility (n = 593)
Hand searched reference lists(n = 8)
Total studies included(n = 40)
Figure 1 Study selection process
to heterogeneity A p value of gt010 determines ifheterogeneity is present consequently the summaryeffect from the random-effects model rather thanthe fixed-effects model is utilized In cases wheredata were not amenable to meta-analysis (either notcomparable or insufficient data) these studies werecompared descriptively and tabulated
Results
A total of 12244 references were identified(Figure 1) of which 11651 were excluded byscreening the title abstract and the removal ofduplicates Of the remaining 593 references fulltexts were sought and 40 met the inclusion criteriaregardless of quality Reasons for exclusion can beseen in Figure 1
The 40 included studies were quantitativemainly cross-sectional with two longitudinal studies(Berger et al 2005 Johnson et al 2013) 21 studies
were graded as high quality and 19 as mediumquality A brief summary of the demographic dataof the studies is provided in Table S1 along with adescription of the measures used quality score andthe main findings There was little consistency inthe sample populations across studies The includedstudies consisted of 10978 caregivers in total ofthese 67 were female and had a mean age of60 years Only five studies reported ethnicity Ofthose which reported dementia stage nine studiesincluded participants with mild dementia 20 withmoderate and one with severe dementia
Quality appraisal of included studiesLevel of agreement between the two independentreviewers was κ = 072 p = 0002 95 CI (073078) indicating substantial agreement (Landis andKoch 1977) The studies scoring the lowest onthe checklist were Haley et al (1987) Hishikawaet al (2012) and Savorani et al (1998) All studieslost points on questions covering external validity
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1764 A Feast et al
validity and reliability of outcome measures and thereporting of statistics
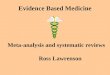
Meta-analysis of comparable studiesSixteen of the 40 studies were suitable to beincluded in a meta-analysis of mean distress scores(see Table S2 available as supplementary materialattached to the electronic version of this paper atwwwjournalscambridgeorgjid_IPG) All of thesestudies reported data on the mean and standarddeviation of distress associated with the meantotal score on the NPI for individual behaviorsEach adapted version of the NPI was reportedas valid and reliable and all were administeredby a researcher or clinician Five studies utilizedthe ten-item version of the NPI thereforedata reporting distress associated with sleep andappetiteeating change were unavailable for thesestudies Participants were recruited from clinic-based and population-based studies had a mix ofdementia participants and studies only includingthose with a diagnosis of Alzheimerrsquos diseaseParkinsonrsquos disease dementia and frontotemporaldementia (see Table S1 available as supplementarymaterial attached to the electronic version of thispaper at wwwjournalscambridgeorgjid_IPG) InTable S3 (available as supplementary materialattached to the electronic version of this paperat wwwjournalscambridgeorgjid_IPG) the meandistress reported for the total NPI symptom canbe seen for each of the 16 studies along with thepooled standard deviations for each behavior acrossthe studies There is considerable variation betweenthe studies for each of the symptoms this can beseen in Figure 2 in particular there is substantialvariation in the mean distress reported for the totalscore of irritable behavior Baiyewu et al (2003)reported 06 (between ldquonot at all distressingrdquo andldquominimally distressingrdquo) and Balieiro et al (2010)reported 36 (between ldquomoderatelyrdquo and ldquoseverelyrdquodistressing) However it is possible to concludethat euphoria was the least distressing across thestudies
As seen in Figure 3 the most distressingBPSD across the 16 studies was depressionAgitationaggression was the second most distress-ing followed by apathy Euphoria was the leastdistressing and had the smallest standard errorDelusional and euphoric behaviors were the onlytwo behaviors with a standard deviation exceedingthe mean indicating high variance between studiesfor these behaviors
Four studies reported correlation data betweenmean NPI total scores and mean NPI distress(Matsumoto et al 2007 Balieiro et al 2010Davidsdottir et al 2012 Huang et al 2012)
all of these studies were involved in the previousmeta-analysis other than Davidsdottir et al (2012)Three of these studies reported data on all 12behaviors The sample size and the correlationcoefficients were entered into MedCalc in order toproduce a pooled effect size for each behavior Thepooled effect sizes within the fixed-effect modelrandom-effects model and heterogeneity statisticsare reported in Table 1 Significant heterogeneitywas identified between studies for all behaviorsother than apathy and sleep In contrast tothe mean distress data the meta-analysis of thecorrelation data identified that irritable behaviorwas the most strongly associated with caregiverdistress followed by aberrant motor behavior andthen delusions Disinhibition had the weakestassociation with distress Depression was seento be one of the behaviors which was morestrongly associatedcorrelated with distress acrossboth meta-analyses Appetite and eating-relatedbehavior was one of the behaviors which had aweaker associationcorrelation with distress acrossboth meta-analyses
Non-comparable studiesTwenty of the 40 included studies were notsuitable for meta-analysis These studies werenot comparable in terms of BPSD measure andthe associated unit of measurement caregiverwell-being measure and the associated unit ofmeasurement It was therefore only possible tocompare these 20 studies descriptively due to theirheterogeneity
Prevalence of BPSD and the impact oncaregiver well-beingMean prevalence and mean distress were reportedon the NPI by Haley et al (2008) and deVugt et al (2006) Although these two studiesboth measure prevalence of BPSD methodsfor measuring caregiver well-being differed (seeTable S1)
Frequency of BPSD and caregiver well-beingMemory-related behaviors were reported as moststressful and problematic across three studies(Nygaard 1998 Quayhagen and Quayhagen 1998Muangpaisan et al 2010) However Robinsonet al (2001) and Fauth and Gibbons (2014) bothfound the frequency of memory-related behaviorswas associated with the least amount of reactivityDisruptive behaviors were associated with themost reactivity followed by depressive behaviors(Robinson et al 2001 Fauth and Gibbons2014) In all of the studies which measuredhallucinations caregivers reported this behavior
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1765
005
115
225
335
445
Mea
n di
stre
ss
Delusions Hallucinations AgitationAggression Depression
005
115
225
335
Mea
n di
stre
ss
Anxiety Euphoria Apathy Disinhibition
0
05
1
15
2
25
3
35
4
Mea
n di
stre
ss
Irritability Aberrant motor behaviour Sleep Appettite and eating
Figure 2 Mean distress scores across 16 studies for behaviors on the NPI (total score)
as less problematic burdensome and distressingcompared to many of the other behaviors Verbalaggression across three of the five studies wasreported as problematic and burdensome Acrosstwo of the five studies which reported sexualdisinhibition this behavior was reported as theleast problematic Reports of wandering acrossfour of the studies were not consistent since
some of the studies reported this behavior asmuch more problematic and burdensome thanothers
Across four of the five studies which reportedincontinence this was consistently reported as oneof the more burdensome stressful and problematicbehaviors Physical aggression was only measuredin three studies and only one study reported this
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1766 A Feast et al
Figure 3 Meta-analysis of mean distress for each BPSD associated with NPI total score
behavior as a common problem Both studies whichreported irritability identified this behavior to be oneof the most problematic and burdensome
Correlational data between BPSD andcaregiver well-beingSleeping- and eating-related behaviors were foundto be significantly correlated to burden and strainhowever they had a stronger association withburden (Donaldson et al 1998) With regard toadult-child caregivers four (delusions agitationdisinhibition and appetiteeating change) of theeight behaviors reported by Conde-Sala et al (2010)as being significantly associated with burden werealso found to be significantly associated with burdenby Allegri et al (2006) Apathy and irritabilitywere reported to be significantly associated withburden in the study conducted by Conde-Sala et al(2010) but no significant relationship was reportedby Allegri et al (2006) Spousal caregivers onlyfound appetiteeating change burdensome (Conde-Sala et al 2010) Apathy had a moderate significantassociation with burden in spousal and adult-child caregivers (Conde-Sala et al 2010) but thisassociation was non-significant in the data reported
by Allegri et al (2006) Delusional and irritablebehaviors were also reported as non-significantlyrelated to burden (Allegri et al 2006) but weresignificantly related to burden by Conde-Sala et al(2010) In contrast to the previous studies reportingthe weak association between euphoria and distressFuh et al (2001) reported a significant correlationbetween euphoria and burden No other behaviorson the NPI had a significant correlation with burden(Fuh et al 2001)
In agreement with the data concerning atthe association between the frequency of thebehavior within each subscale on the RMBPCand reactivity disruptive behaviors had the largestcorrelation of the three subscales with burden(Huang et al 2012) Using the BEHAVE-AD (Reisberg et al 1982) and the NOSGER(Spiegel et al 1991) mood social behaviorsand disturbing behaviors were found to havea significant moderate association with burdenbut no significant correlations with depression incaregivers Chiu et al (2014) noted that all of thebehaviors on the NPI significantly predicted sleepdisturbance in caregivers other than anxiety andaberrant motor behavior
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1767
Table 1 Meta-analysis of mean distress scores correlated with behaviors using NPI total scores
P O O L E D C O R RELATION COEFFI CIENT T EST F OR HETEROGENEITY
FI XE D-E FF E C T S RANDOM-E FF E C T S
BEHAVIOR N MODEL (95 CI) MODEL (95 CI) I2 95 CI P
Delusions 243 0557 (0462 to 0640) 0567 (0412 to 0690) 5864 000 to 8623 p = 00643Hallucinations 243 0502 (0399 to 0532) 0520 (0198 to 0791) 8771 7081 to 9482 p lt 00001AgitationAggression 243 0540 (0443 to 0625) 0537 (0299 to 0712) 7941 4517 to 9482 p = 00022Depression 243 0528 (0429 to 0615) 0564 (0360ndash0717) 7465 2949 to 9089 p = 00080Anxiety 243 0482 (0377 to 0575) 0481 (0236 to 0669) 7845 4203 to 9199 p = 00030Euphoria 243 0540 (0443 to 0625) 0480 (0147 to 0715) 8764 7061 to 9480 p lt 00001Apathy 243 0456 (0351 to 0554) 0459 (0351 to 0540) 000 000 to 8423 p = 04834Disinhibition 243 0357 (0240 to 0464) 0371 (0162 to 0548) 6574 000 to 8833 p = 00327Irritability 243 0668 (0590 to 0733) 0691 (0486 to 0823) 8281 5601 to 9329 p = 00006Aberrant motor
behavior243 0606 (0518 to 0681) 0603 (0437 to 0730) 6764 371 to 8871 p = 00280
Sleep 176 0438 (0307 to 0552) 0436 (0301 to 0554) 532 000 to 9682 p = 03478Appetite and eating 176 0405 (0271 to 0523) 0442 (0200 to 0633) 6617 000 to 9026 p = 00520
Predictive data between BPSD and well-beingConde-Sala et al (2010) Chappell and Penning(1996) Davis and Tremont (2007) and Slachevskyet al (2013) used the same burden measurebut used different measures of BPSD Apathysignificantly predicted burden across three studiesalthough it was less burdensome for adult-childcaregivers and did not predict apathy in the study byDavis and Tremont (2007) Three studies (Mouriket al 2004 Khoo et al 2013 Lee et al 2013)reported data identifying which behaviors predicteddistress as measured by the NPI Apathy wasa significant predictor across two of the threestudies Delusions and anxiety were the only othercomparable behaviors across two of the three studiesand were both significant predictors of distressCovinsky et al (2003) did not use a formal behaviorscale but identified that anger and aggressivebehaviors were stronger predictors of caregiverdepression followed by dangerous behaviors to selfand others and then behaviors which wake thecaregiver up at night
Discussion
To our knowledge this is the first review to controlfor the effect of multiple BPSD on caregiver well-being by discriminating between individual BPSDand also discriminating between caregiver outcomesof well-being Additional advantages of this reviewwere the use of a formal method of synthesis andthe decision to distinguish between how BPSD andcaregiver well-being are measured which ensuredvalid conclusions were drawn by only synthesizing
comparable data Only two meta-analyses werepossible due to limited homogeneous studiesCategories in which the relationship betweenBPSD and well-being were qualitatively examinedincluded minimal studies displaying considerablevariation therefore valid conclusions could not bedrawn The results are discussed in the context ofprevious research
Meta-analysis of mean distress scoresAs seen in Figures 2 and 3 even within one measureand one criterion (distress associated with totalscore on the NPI) variability in distress ratingsfor each symptom can be seen between the 16studies This was also evident in research conductedby Fauth and Gibbons (2014) in which a widevariation in the prevalence of NPI symptoms wasseen between studies However data regardingdistress associated with euphoria and delusionsdemonstrated high levels of variance in terms of theratio between the mean and the standard deviationresulting in considerable variability between scoresTherefore the ratio of the mean distress ratingscompared with the standard deviation associatedwith the other ten behaviors signifies that there islow variance between the 16 studies It is unclearat present why there is increased variability foreuphoric and delusional behaviors In terms of totalscore depression followed by agitationaggressionand apathy were found to be the most distressingfor caregivers across 16 studies in the meta-analysis(Figure 3) This suggests that it is mood-relatedbehaviors which are associated with increaseddistress Fauth and Gibbons (2014) examinedthe relationship between total score of BPSD
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1768 A Feast et al
and distress and found similar results howevereven with identical analysis there were noteworthydiscrepancies such as delusions being the mostdistressing but only the fourth most distressing inthe current review Consistent with the currentmeta-analysis of mean data apathy and depression-related behaviors have been reported as distressingin numerous studies (Teri 1997 deVugt et al2003 Aarsland et al 2007 Kosberg et al 2007)Similarly depression in the person with dementia isassociated with depression in the caregiver (Waiteet al 2004)
Meta-analysis of correlation dataAs seen in Table 1 there were high levels ofheterogeneity between the studies included in thesecond meta-analysis investigating which behaviorswere associated with distress Only apathy- andsleep-related behaviors displayed homogeneitybetween studies Furthermore behaviors which hadstronger correlations with distress (Table 1) didnot have strong associations in the previous meta-analysis (Figure 3) regarding distress associatedwith behaviors At present it is unclear why thisdiscrepancy exists and also why distress correlatedwith apathy- and sleep-related behaviors is more ho-mogenous between studies than the other behaviorsSince only a few studies contributed to this meta-analysis more research is needed to investigate thepooled effects Nevertheless a meta-analysis of thisnature has not been performed previously and therandom-effects model was used to report a moreconservative estimate for the heterogeneous pooledeffects in order to reduce bias
Apathy and irritable behaviors were not con-sistently significantly correlated to burden acrossmultiple studies whereas delusions agitationdisinhibition and appetiteeating change werethese associations were also reported in otherstudies (Rymer et al 2002 Rocca et al 2010) Incontrast a review by Ornstein and Gaugler (2012)reported that angeraggression and depression werethe most frequently cited BPSD associated withcaregiver burden depression was also linked tocaregiver burden in a review by Black and Almeida(2004) In addition to burden delusional behaviorwas consistently associated with distress acrossstudies with a significant correlation also beingseen with stress (Kosmala and Kloszewska 2004)Berger et al (2005) noted that behaviors whichare significantly correlated with burden are notcorrelated with depression This demonstrates theimportance of including multiple measures of well-being since the same behaviors affect caregiversdifferently which has implications for futureinterventions
Studies unamenable to quantitative synthesisOnly two studies reported the prevalence of BPSDand the impact on caregiver well-being due todifferences between studies comparisons werenot possible Although five studies reported thefrequency of BPSD each measure of caregiver well-being was different Memory-related behaviorsverbal aggression incontinence and irritabilitywere reported to affect well-being across multiplestudies These findings were also seen in previousresearch (Bruce and Paterson 2000 Farran et al2004) However Fauth and Gibbons (2014) andRobinson et al (2001) did not find that memory-related behaviors were distressing despite being themost frequent type of behavior on the RMBPCHallucinations sexual disinhibition and physicalaggression were consistently reported to affect well-being less than the other behaviors Although thisfinding is reflected in the majority of studies Haleyet al (2008) and Arango-Lasprilla et al (2010)reported contradictory results
It is noteworthy that aggressionagitation whenmeasured in terms of total score was reported asthe second most distressing across 16 of the studiesbut when measured in terms of frequency only oneof the three studies reported physical aggressionas a common problem However the frequency ofverbal aggression consistently affected well-beingIt is not possible to provide an explanation for thisdiscrepancy but it may be because of the distinctionbetween how aggressionagitation is measured (ietotal score or frequency) or that verbal and physicalaggression have been differentiated and thereforeaffect caregiver well-being differently
Predictive data were limited and heterogeneousin the present review however it was possible toconclude that apathy predicted burden and distressacross studies Anger restlessness combativenessdangerous to others and embarrassing behaviorwere found to be strong predictors of burden ina study by Gaugler et al (2011) Only one studyreported the predictors of caregiver depression
Potential explanations for variability incaregiver well-beingDifference in study quality does not appear to be anexplanation for the variation in distress rating acrossstudies since even between two medium qualitystudies there was considerable variation (Balieiroet al 2010 displaying one of the highest meandistress scores Baiyewu et al 2003 displayingone of the lowest) Two studies consistently hadthe highest mean distress rating across each of thebehavior domains Balieiro et al (2010) and Tanet al (2005) Both of these studies were clinic-basedhigher distress ratings would be expected as those
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1769
experiencing more BPSD might be more likely toattend a clinic as indeed were the majority ofstudies included in the meta-analysis It may bepossible that dementia severity is an explanationsince participants in the studies with the highestdistress scores (Tan et al 2005 Balieiro et al 2010)had moderate and severe dementia respectivelywhereas Baiyewu et al (2003) who consistentlyreported the lowest distress scores across eachof the behavior domains included participantswith mild dementia However both Aarslandet al (2007) and de Vugt et al (2006) reportedlower mean distress scores in comparison with theother included studies and they both includedparticipants with moderate dementia FurthermoreDavidsdottir et al (2012) found that there wasno significant difference between caregiver distressscores depending on dementia severity
Baiyewu et al (2003) had a much smallersample of spousal caregivers in comparison to Tanet al (2005) which might account for the lowerdistress scores This is in agreement with Almberget al (1997) who reported that spouses experiencegreater levels of burden However three studieswhich had consistently higher mean distress scoresacross all behaviors (Tan et al 2005 Balieiro et al2010 Huang et al 2012) were mainly comprisedof adult-child caregivers When comparing a studysolely comprised of spousal caregivers (deVugt et al2006) with a study (Baiyewu et al 2003) withminimal spousal caregivers (25) it was possibleto see that spousal caregivers were substantiallymore distressed with depressive apathetic andanxiety-related behaviors Although distress ratingscan be differentiated between behavior types forspousal and non-spousal caregivers both Baiyewuet al (2003) and de Vugt et al (2006) had two of thelowest distress scores across all behaviors in compar-ison to the other studies in the meta-analysis
The explanation may also be cultural sinceBaiyewu et al (2003) and Baiyewu et al (2012)(with similarly low distress scores across behaviors)were the only Africa-based studies in the meta-analysis Baiyewu et al (2003) and Baiyewu et al(2012) were also both community-based studieswhich may also be a reason for the reduceddistress ratings There is every reason to believethat BPSD are present across cultures (Shajiet al 2009) however the low levels of publicawareness of dementia have many implications(Prince 2000) One of these implications maybe the misinterpretation of BPSD as deliberateconsequently affecting the well-being of the carer(Shaji et al 2009) It is beyond the scope ofthis paper to determine why there is considerablevariation between studies reporting caregiverdistress for identical behaviors using identical
measures However it is likely that it is the caregivercharacteristics rather than the characteristics of theperson with dementia (such as dementia severity)which may underlie the explanation as to whyvariation between studies exists
Limitations
The data available for this review allowed for onlytwo meta-analyses to be conducted There wererelatively few studies which assessed the relationshipbetween individual BPSD and caregiver well-beingand which met the inclusionexclusion criteriafor the review In an attempt to be systematicbased on prior recommendation an effort wasmade to distinguish between how ldquoproblematicrdquosymptoms are measured Consequently studieswere categorized into whether BPSD weremeasured in terms of frequency or prevalence andalso categorized in terms of the statistical analysisemployed Other than data regarding mean distressassociated with NPI total score only a small amountof studies were included in each category andunfortunately it was often the case that measuresof caregiver well-being were dissimilar From the 40included studies there were 12 different measuresof behavior and 17 different measures of well-being making comparisons difficult which mayhave contributed to the inconsistent findings
The majority of included studies recruitedparticipants from clinics therefore caregiversincluded in the review were not representative ofthe population In addition the samples across theincluded studies were heterogeneous in a numberof factors therefore caution should be taken wheninterpreting the results Although beyond the scopeof this review study characteristics such as culturegender and relationship direction were not ex-amined through subgroup analyses Due to the lim-ited number of studies it was not possible to imposea quality criteria however all included studies wereeither of high or medium quality as assessed by theDowns and Back Checklist (1998) Furthermore allof the included studies relied on caregiver reportsof BPSD which may themselves be affected bycaregiver well-being unfortunately it is not possibleto determine if this was the case Nonetheless twovalid meta-analyses were completed and a numberof comments can be made about the relationshipbetween BPSD and caregiver well-being
Implications and recommendations
The vast majority of studies addressing the rela-tionship between BPSD and caregiver well-being
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1770 A Feast et al
did not examine individual BPSD Consequentlythis comparatively limited the amount of studiesincluded in the present review Therefore if we areto understand this relationship more studies needto examine individual BPSD in their research Inaddition it is more clinically relevant to examinewhich BPSD affect well-being rather than BPSDas a whole as this is essential in determiningwhere clinical staff should allocate resources mosteffectively Nevertheless there is preliminary datasuggesting it is mood-related behaviors whichare associated with increased levels of distresstherefore interventions for the management ofBPSD should target these behaviors
The lack of consistency in the measurementof BPSD (neuropsychiatric or memory problemsfrequency or prevalence) and the measurementof caregiver well-being (the use of interchangeableterminology such as stress strain and burdenmeaning the same construct) limits our ability toreach a consensus as to which BPSD result inthe most negative outcomes for caregivers Forexample Donaldson et al (1998) used GilleardrsquosStrain Scale (1984) to measure burden andthe General Health Questionnaire (Goldberg andHillier 1979) to measure distress Furthermorefour studies (see Table S1) did not have formalscales to measure the impact of BPSD on well-being and used terms such as ldquoburdensomerdquoldquoseriousrdquo and ldquodisturbingrdquo This problem impactsupon the validity and reliability of the originalstudies and consequently the review Howeverthis mainly occurred in the earlier studies Futureresearch should also include more than one measureof well-being in order to identify if individual BPSDdifferentially affect caregiver burden compared tocaregiver distress as identified in the current reviewFurthermore future research should identify whythere is reduced variability in distress ratings forcertain behaviors compared to others and whycertain behaviors are more distressing dependingon which type of statistical analysis is used
Although there are potential methodologicalreasons (limited studies inconsistent measures)for why there is substantial variability whenidentifying which BPSD affect certain types ofcaregiver well-being the most there is growingevidence that factors associated with the personwith dementia (eg BPSD frequency cognition) areonly part of the story when explaining a caregiverrsquosresponse to BPSD Caregiver characteristicshave been shown to account for twice thevariance of person with dementia characteristicswhen reporting neuropsychiatric symptoms (Sinket al 2006) and the presence of BPSD wasnot found to be a significant predictor ofburden whereas caregiver characteristics such as
confidence neuroticism and relationship qualitywere significant predictors (Campbell et al 2008)Therefore as recommended by Ornstein andGaugler (2012) future studies should focus onidentifying pathways for the association betweenindividual BPSD caregiver variables and caregiveroutcomes More research is needed to understandif and why certain BPSD affect certain caregiveroutcomes and also how much of this is attributableto caregiver variability in response to BPSD ratherthan the presence of BPSD itself More longitudinalstudies would be useful to examine how changes inindividual BPSD are associated with caregiver well-being over time A review by Black and Almeida(2004) examined the limited longitudinal studiesavailable and reported mixed findings betweenburden and BPSD and found no associationbetween BPSD and distress Although BPSDincreased significantly over a two-year periodcaregiver burden remained stable and depressionwas found to decrease (Berger et al 2005) Futureresearch needs to examine caregiver factors overtime (well-being role captivity etc) along withchanges in individual BPSD in order to have a morevalid understanding of this relationship
Caution should be exercised when creating ameasure of BPSD since Jackson et al (2014)found that the Revised Memory and BehaviorProblem Checklist (Teri et al 1992) might bemore suitable in explaining caregiver depressionthan the NPI It is important that the measureof BPSD is not biased toward explaining a moreunique association between BPSD and a measure ofcaregiver well-being such as depression As stated byGitlin and Rose (2014) item selection for measuresof BPSD is often based upon specific disciplines(eg neurology psychiatry social sciences) andthus implicitly represents different conceptual-izations of behavior A shared framework fordefining behaviors and their underlying causesmust be created in order to move on fromthe implicit assumption of most measures thatbehaviors are a direct cause of neuropathologyand to develop measures which also address thecontextual and caregiver characteristics associatedwith the behavior
Conclusions
This study has improved our understanding of theimpact of individual BPSD on caregiver well-beingin particular caregiver distress The relationshipbetween individual BPSD and caregiver well-beingwas inconsistent and varied according to behavioralsymptom Due to limited studies and heterogeneousdata the results should be interpreted with caution
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1771
but advances have been made with respect towhich behaviors are associated with distress Theinconsistencies may be partly explained by caregivervariables which were not taken into account inthe review Based on this review and previousresearch it is not possible to fully understand therelationship between BPSD and caregiver well-being without examining the influence of caregivervariables such as caregiver strategies acceptancegender relationship with person with dementiaand confidence We recommend that future studiesare designed to examine individual BPSD ratherthan BPSD as a whole use consistent measures forBPSD and well-being use consistent terminologyfor psychological constructs (eg burden) andexamine the causal mechanisms by which individualBPSD impact caregiver well-being by collectingdata on a range of caregiver factors Theseapproaches will clarify whether it is important forclinicians to focus on the frequency or prevalence ofcertain BPSD in addition to targeting the presenceof certain caregiver characteristics and addressingunmet need
Conflict of interest
None
Description of authorsrsquo roles
A Feast was responsible for developing the reviewobjectives writing the search strategies conductingthe searches designing and completing studyeligibility and data extraction forms undertakingthe quality appraisals conducting the meta-analysisand writing the paper M Orrell was responsible fordeveloping the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper C Stoner was responsible forundertaking the quality appraisals and assisting inwriting the paper G Charlesworth was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper E Moniz-Cook was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper
Acknowledgments
We would like to thank Dr Zoeuml Hoare for herstatistical advice This paper presents independentresearch funded by the National Institute for HealthResearch (NIHR) under its Programme Grants forApplied Research (RP-PG-0606-1067 and RP-PG-
060- 1083) The views expressed in this publicationare those of the author(s) and not necessarily thoseof the NHS the NIHR or the Department ofHealth
Supplementary Material
To view supplementary material for thisarticle please visit httpdxdoiorg101017S1041610216000922
References
Aarsland D et al (2007) Neuropsychiatric symptoms inpatients with Parkinsonrsquos disease and dementia frequencyprofile and associated care giver stress Journal of NeurologyNeurosurgery amp Psychiatry 78 36ndash42doihttpdxdoiorg101136jnnp2005083113
Allegri R F et al (2006) Neuropsychiatric symptoms as apredictor of caregiver burden in Alzheimerrsquos diseaseNeuropsychiatric Disease amp Treatment 2 105ndash110doi102147ndts47133
Almberg B Grafstrom M and Winblad B (1997)Major strain and coping strategies as reported by familymembers who care for aged demented relatives Journal ofAdvanced Nursing 26 683ndash691doihttpdxdoiorg101046j1365-2648199700392x
Arango-Lasprilla J C Lehan T Drew A MorenoA Deng X and Lemos M (2010) Health-relatedquality of life in caregivers of individuals with dementiafrom Colombia American Journal of Alzheimerrsquos Disease andOther Dementias 25 556ndash561doi1011771533317510382287ltbibgt
Baiyewu O et al (2003) Behavioral and caregiver reactionof dementia as measured by the neuropsychiatric inventoryin Nigerian community residents InternationalPsychogeriatrics 15 399ndash409doi101017s1041610203009645
Baiyewu O et al (2012) Behavioral symptoms incommunity-dwelling elderly Nigerians with dementia mildcognitive impairment and normal cognition InternationalJournal of Geriatric Psychiatry 27 931ndash939 doihttpdxdoiorg101002gps2804
Balieiro A P Jr Sobreira E S T Pena M C SSilva-Filho J H and Vale F A C (2010) Caregiverdistress associated with behavioral and psychologicalsymptoms in mild Alzheimerrsquos disease Dementia eNeuropsychologia 4 238ndash244
Ballard C G et al (1995) The aetiology of depression inthe carers of dementia sufferers Journal of AffectiveDisorders 35 59ndash63 doi1010160165-0327(95)00041-k
Bandeira D R Pawlowski J Goncalves T RHilgert J B Bozzetti M C and Hugo F N (2007)Psychological distress in Brazilian caregivers of relativeswith dementia Aging and Mental Health 11 14ndash19doi10108013607860600640814
Berger G Bernhardt T Weimer E Peters JKratzsch T and Frolich L (2005) Longitudinal studyon the relationship between symptomatology of dementia
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1772 A Feast et al
and levels of subjective burden and depression amongfamily caregivers in memory clinic patients Journal ofGeriatric Psychiatry and Neurology 3 119ndash128doi1011770891988704273375
Black W and Almeida O P (2004) A systematic reviewof the association between the behavioral and psychologicalsymptoms of dementia and burden of care InternationalPsychogeriatrics 16 295ndash315doi101017s1041610204000468
Bruce D G and Paterson A (2000) Barriers tocommunity support for the dementia carer a qualitativestudy International Journal of Geriatric Psychiatry 15451ndash457 doi101002(sici)1099-1166(200005)155lt451aid-gps143gt30co2-k
Campbell P et al (2008) Determinants of burden in thosewho care for someone with dementia International Journalof Geriatric Psychiatry 23 1078ndash1085doi101002gps2071
Cerejeira J Lagarto L and Mukaetova-LadinskaE B (2012) Behavioral and psychological symptoms ofdementia Frontiers in Neurology 3 1ndash23doi103389fneur201200073
Chappell N L and Penning M (1996) Behaviouralproblems and distress among caregivers of people withdementia Ageing amp Society 16 57ndash73doi101017s0144686x00003135
Chiu Y C et al (2014) Family caregiversrsquo sleepdisturbance and its associations with multilevel stressorswhen caring for patients with dementia Aging amp MentalHealth 18 92ndash101 doihttpdxdoiorg101080136078632013837141
Cohen J (1988) Statistical Power Analysis for the BehavioralSciences 2nd edn New York University New YorkLawrence Erlbaum Associatesdoi1043249780203771587
Conde-Sala J L Garre-Olmo J Turroacute-Garriga OVilalta-Franch J and Loacutepez-Pousa S (2010)Differential features of burden between spouse andadult-child caregivers of patients with Alzheimerrsquos diseasean exploratory comparative design International Journal ofNursing Studies 47 1262ndash1273doi101016jijnurstu201003001
Covinsky K E et al (2003) Patient and caregivercharacteristics associated with depression in caregivers ofpatients with dementia Journal of General Internal Medicine18 1006ndash1014 doihttpdxdoiorg101111j1525-1497200330103x
Craig D Mirakhur A Hart D J McIlroy S P andPassmore A P (2005) A cross-sectional study ofneuropsychiatric symptoms in 435 patients withAlzheimerrsquos disease American Journal of GeriatricPsychiatry 13 460ndash468 doi10109700019442-200506000-00004
Crellin N Charlesworth G and Orrell M (2014)Measuring family caregiver efficacy for managing behavioraland psychological symptoms in dementia a psychometricevaluation International Psychogeriatrics 26 93ndash103 doihttpdxdoiorg101017s1041610213001646
Davidsdottir S R Snaedal J Karlsdottir GAtladottir I and Hannesdottir K (2012) Validationof the Icelandic version of the neuropsychiatric inventorywith caregiver distress (NPI-D) Nordic Journal of
Psychiatry 66 26ndash32 doihttpdxdoiorg103109080394882011593100
Davis J D and Tremont G (2007) Impact of frontalsystems behavioral functioning in dementia on caregiverburden The Journal of Neuropsychiatry and ClinicalNeurosciences 19 43ndash49 doihttpdxdoiorg101176jnp200719143
de Vugt M E Riedijk S R Aalten P Tibben Avan Swieten J C and Verhey F R J (2006) Impactof behavioural problems on spousal caregivers acomparison between Alzheimerrsquos disease andfronto-temporal dementia Dementia and Geriatric CognitiveDisorders 22 35ndash41 doi101159000093102
de Vugt M E et al (2003) Behavioural disturbances indementia patients and quality of the marital relationshipInternational Journal of Geriatric Psychiatry 18 149ndash154doi101002gps807
Donaldson C Tarrier N and Burns A (1998)Determinants of carer stress in Alzheimerrsquos diseaseInternational Journal of Geriatric Psychiatry 13 248ndash256doi101002(sici)1099-1166(199804)134lt248aid-gps770gt30co2-0
Downs S and Black N (1998) The feasibility of creating achecklist for the assessment of the methodological qualityboth of randomised and non-randomised studies of healthcare interventions Journal of Epidemiological CommunityHealth 52 377ndash384 doi101136jech526377
Farran C J Loukissa D A Lindeman D A andMcCann J (2004) Caring for self while caring for othersthe two-track life of coping with Alzheimerrsquos diseaseJournal of Gerontological Nursing 30 38ndash45doi1039280098-9134-20040501-09
Fauth E B and Gibbons A (2014) Which behavioral andpsychological symptoms of dementia are the mostproblematic Variability by prevalence intensity distressratings and associations with carer depressive symptomsInternational Journal of Geriatric Psychiatry 29 263ndash271doi101002gps4002
Fuh J L Liu C K Mega M S Wang S J andCummings J L (2001) Behavioral disorders andcaregiversrsquo reaction in Taiwanese patients with Alzheimerrsquosdisease International Psychogeriatrics 13 121ndash128 doihttpdxdoiorg101017s1041610201007517
Gaugler J E et al (2011) Does caregiver burden mediatethe effects of behavioral disturbances on nursing homeadmission The American Journal of Geriatric Psychiatry 19497ndash506 doi101097jgp0b013e31820d92cc
Gilleard C J Belford H Gilleard E Whittick J Eand Gledhill K (1984) Emotional distress amongst thesupporters of the elderly mental infirm British Journal ofPsychiatry 145 172ndash177doihttpdxdoiorg101192bjp1452172
Gitlin L N and Rose K (2014) Factors associated withcarer readiness to use nonpharmacologic strategies tomanage dementia-related behavioral symptomsInternational Journal of Geriatric Psychiatry 29 93ndash102doihttpdxdoiorg101002gps3979
Goldberg D P and Hillier V F (1979) A scaled versionof the general health questionnaire Psychological Medicine9 139ndash145 doi101017s0033291700021644
Gonzalez-Salvador M T Arango C Lyketsos C Gand Barba A C (1999) The stress and psychological
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1773
morbidity of the Alzheimer patient caregiver InternationalJournal of Geriatric Psychiatry 14 701ndash710doi101002(sici)1099-1166(199909)149lt701aidps5gt30co2-
Haley W E Brown S and Levine E G (1987) Familycaregiver appraisals of patient behavioral disturbance insenile dementia Clinical Gerontologist The Journal of Agingand Mental Health 6 25ndash34doi101300j018v06n04_04
Haley W E Levine E G Brown S L Berry J Wand Hughes G H (2008) The psychological social andhealth consequences of caring for a relative with seniledementia Journal of the American Geriatrics Society 35405ndash411 doi101111j1532-54151987tb04661x
Hishikawa N et al (2012) Effects of turmeric onAlzheimerrsquos disease with behavioral and psychologicalsymptoms of dementia Ayu 33 499ndash504 doihttpdxdoiorg1041030974-8520110524
Huang S S Lee M C Liao Y C Wang W F andLai T J (2012) Caregiver burden associated withbehavioral and psychological symptoms of dementia(BPSD) in Taiwanese elderly Archives of Gerontology andGeriatrics 55 55ndash59 doihttpdxdoiorg101016jarchger201104009
Jackson M A Fauth E B and Geiser C (2014)Comparing the neuropsychiatric inventory and the revisedmemory and behavior problems checklist for associationswith caregiver burden and depressive symptomsInternational Psychogeriatrics 26 1021ndash1031doi101017s1041610213002421
Johnson D K Niedens M Wilson J RSwartzendruber L Yeager A and Jones K (2013)Treatment outcomes of a crisis intervention program fordementia with severe psychiatric complications the Kansasbridge project The Gerontologist 53 102ndash112 doihttpdxdoiorg101093gerontgns104
Khoo S A Chen T Y Ang Y H and Yap P (2013)The impact of neuropsychiatric symptoms on caregiverdistress and quality of life in persons with dementia in anAsian tertiary hospital memory clinic InternationalPsychogeriatrics 25 1991ndash1999 doihttpdxdoiorg101017s1041610213001518
Kosberg J I Kaufman A V Burgio L D Leeper Jand Sun F (2007) Family caregiving to those withdementia in rural Alabama racial similarities anddifferences Journal of Aging and Health 19 3ndash21 doi1011770898264306293604
Kosmala K and Kloszewska I (2004) The burden ofproviding care for Alzheimerrsquos disease patients in PolandInternational Journal of Geriatric Psychiatry 19 191ndash193doi101002gps1054
Landis J R and Koch G G (1977) The measurement ofobserver agreement for categorical data Biometrics 33159ndash174 doi 1023072529310
Lee D R McKeith I Mosimann U Ghosh-NodyalA and Thomas A J (2013) Examining carer stress indementia the role of subtype diagnosis andneuropsychiatric symptoms International Journal ofGeriatric Psychiatry 28 135ndash141 doihttpdxdoiorg101002gps3799
Lim Y M Son G R Song J A and Beattie E(2008) Factors affecting burden of family caregivers of
community-dwelling ambulatory elders with dementia inKorea Archives of Psychiatric Nursing 22 226ndash234 doi101016japnu200712005
Matsumoto N et al (2007) Caregiver burden associatedwith behavioral and psychological symptoms of dementia inelderly people in the local community Dementia andGeriatric Cognitive Disorders 23 219ndash224doi101159000099472
Mohamed S Rosenheck R Lyketsos C G andSchneider L S (2010) Caregiver burden in Alzheimerdisease cross-sectional and longitudinal patient correlatesThe American Journal of Geriatric Psychiatry 18 917ndash927doi101097jgp0b013e3181d5745d
Mourik J C Rosso S M Niermeijer M FDuivenvoorden H J Van Swieten J C and TibbenA (2004) Frontotemporal dementia behavioral symptomsand caregiver distress Dementia and Geriatric CognitiveDisorders 18 299ndash306 doihttpdxdoiorg101159000080123
Muangpaisan W et al (2010) Caregiver burden and needsof dementia caregivers in Thailand a cross-sectional studyJournal of the Medical Association of Thailand 93 601ndash607
Neundorfer M M McClendon M J Smyth K AStuckey J C Strauss M E and Patterson M B(2001) A longitudinal study of the relationship betweenlevels of depression among persons with Alzheimerrsquosdisease and levels of depression among their familycaregivers Journal of Gerontology Series B - PsychologicalSciences and Social Sciences 56 301ndash313
Nygaard H A (1998) Strain on caregivers of dementedelderly people living at home Scandinavian Journal ofPrimary Health Care 6 33ndash37doihttpdxdoiorg10310902813438809009287
Ornstein K and Gaugler J E (2012) The problem withldquoproblem behaviorsrdquoa systematic review of the associationbetween individual patient behavioral and psychologicalsymptoms and caregiver depression and burden within thedementia patientndashcaregiver dyad InternationalPsychogeriatrics 24 1536ndash1552doi101017s1041610212000737
Ornstein K Gaugler J E Devanand N S CarolynZ and Yaakov S (2012) The differential impact ofunique behavioral and psychological symptoms for thedementia caregiver how and why do patientsrsquo individualsymptom clusters impact caregiver depressive symptomsThe American Journal of Geriatric Psychiatry 12 77ndash1286doi httpdxdoiorg101016jjagp201301062
Price G R (1970) Selection and covariance Nature 227520ndash521 doi101038227520a0
Prince M (2000) Dementia in developing countries Aconsensus statement from the 1066 Dementia ResearchGroup International Journal of Geriatric Psychiatry 1514ndash20 doihttpdxdoiorg101002(sici)1099-1166(200001)151lt14aid-gps70gt30co2-8
Quayhagen M P and Quayhagen M (1998) Alzheimerrsquosstress coping with the caregiving role Gerontologist 28391ndash396 doihttpdxdoiorg101093geront283391
Reisberg B Ferris S H de Leon M J and Crook T(1982) The global deterioration scale for assessment ofprimary degenerative dementia American Journal ofPsychiatry 139 1136ndash1139 doihttpdxdoiorg101176ajp13991136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1774 A Feast et al
Robinson K M Adkisson P and Weinrich S (2001)Problem behaviour caregiver reactions and impact amongcaregivers of persons with Alzheimerrsquos disease Journal ofAdvanced Nursing 36 573ndash582 doihttpdxdoiorg101046j1365-2648200102010x
Rocca P et al (2010) Neuropsychiatric symptomsunderlying caregiver stress and insight in Alzheimerrsquosdisease Dementia and Geriatric Cognitive Disorders 3057ndash63 doi101159000315513
Rymer S Salloway S Norton L Mallow PCorreia S and Monast D (2002) Impaired awarenessbehavior disturbance and caregiver burden in Alzheimerdisease Alzheimer Disease and Associated Disorders 16248ndash253 doi 10109700002093-200210000-00006
Savorani G Vulcano V Boni S Sarti G andRavaglia G (1998) Behavioral disorders in dementiapatients and their impact on the stress of caregivingrelatives the ldquoARADrdquo questionnaire Archives ofGerontology and Geriatrics 6 481ndash485doi101016s0167-4943(98)80070-8
Shaji K S George R K Prince M J and JacobK S (2009) Behavioral symptoms and caregiver burdenin dementia Indian Journal of Psychiatry 51 45 doihttpdxdoiorg1041030019-554544905
Sink K M Covinsky K E Barnes D E NewcomerR J and Yaffe K (2006) Caregiver characteristics areassociated with neuropsychiatric symptoms of dementiaJournal of the American Geriatrics Society 54 796ndash803 doi101111j1532-5415200600697x
Slachevsky A et al (2013) The CUIDEME studydeterminants of burden in chilean primary caregivers ofpatients with dementia Journal of Alzheimerrsquos Disease 35297ndash306
Spiegel R et al (1991) A new behavioral assessment scalefor geriatric out- and in-patients the NOSGER (nursesrsquoobservation scale for geriatric patients) Journal of theAmerican Geriatric Society 39 339ndash347 doihttpdxdoiorg101111j1532-54151991tb02897x
Tan L L Wong H B and Allen H (2005) The impactof neuropsychiatric symptoms of dementia on distress infamily and professional caregivers in SingaporeInternational Psychogeriatrics 17 253ndash263 doi101017s1041610205001523
Teri L (1997) Behavior and caregiver burden behavioralproblems in patients with Alzheimer disease and itsassociation with caregiver distress Alzheimer Disease andAssociated Disorders 11 35ndash38
Teri L Truax P Logsdon R Uomoto J Zarit Sand Vitaliano P P (1992) Assessment of behavioralproblems in dementia the revised memory and behaviorproblems checklist Psychology and Aging 7 622 doi1010370882-797474622
Waite A Bebbington P Skelton-Robinson M andOrrell M (2004) Social factors and depression in carersof people with dementia International Journal of GeriatricPsychiatry 19 582ndash587 doihttpdxdoiorg101002gps1136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at

1762 A Feast et al
Ornstein et al (2012) have advanced the field byexamining how and why symptoms clusters impactcaregiver depression Nevertheless the symptomswere clustered rather than individually representedand the systematic review did not employ a formalmethod of synthesis but instead a descriptiveanalysis was given along with tallying of symptoms
It is often the case that BPSD are presented in asummative fashion due to the nature of the outcomemeasure and how the total score is calculatedand are consequently usually operationalized as asingle construct of ldquobehavior problemrdquo thereforethe data cannot be extracted Research by Fauthand Gibbons (2014) highlighted the extensiveinconsistencies in identifying BPSD that arethe most problematic These inconsistences arepartly due to whether ldquoproblematicrdquo is definedand measured in terms of symptom prevalenceintensity distress rating or association withcaregiver outcomes such as depressive symptoms(Ornstein et al 2012) A review by Black andAlmeida (2004) has progressed our understandingof the association between BPSD as a wholeand the burden of care and caregiver depressionby performing a meta-analysis However multipletypes of behavior measures burden measuresand measures of depression were pooled in thesame meta-analysis In future meta-analyses it isimportant to combine the same outcome measuresof a particular construct such as ldquodistressrdquo in orderto ensure the statistical analysis is valid ratherthan combining multiple types of measures Thisis addressed in the current review
As recommended by Ornstein et al (2012) it isnecessary to design future systematic reviews whichcapture the complexity of unique behaviors in orderto further our understanding of their differentialimpact upon caregivers The aim of this studywas to respond to Ornsteinrsquos recommendation andto systematically review the relationship betweenindividual BPSD and caregiver well-being in orderto identify which BPSD are the most problematicfor caregivers This was achieved by distinguishingbetween psychological constructs of caregiveroutcome (distress burden strain stress) withineach meta-analysis and by distinguishing betweenhow BPSD are measured (prevalence frequencyand total score) within each meta-analysis
Methods
Identification and selection of studiesA search strategy combining medical subjectheadings and text words relating to dementiaBPSD mental disorders and behaviors behaviorselder care significant others carers family
daughters aged carer burden carer strain carerdistress and cost of illness was devised and adaptedfor five electronic databases Searches of studiespublished between 1980 and December 2015 werecarried out through PsycINFO CINAHL EBSCO(Cumulative Index to Nursing and Allied Health)MEDLINE EMBASE and Web of Science(including Science Citation Index-Expanded (SCI-EXPANDED) Conference Proceedings CitationIndex-Science (CPCI-S) Social Science CitationIndex (SSCI) Conference Proceedings CitationIndex-Social Science amp Humanities (CPCI-SSH)and reference lists of included studies Studieswere restricted to peer-reviewed original paperspublished in English and included participants whowere family caregivers of someone with dementiaused a measure of caregiver response to BPSDand a measure of BPSD and reported data forboth measures Reviews conference proceedingsconference abstracts theses supplements reportsletters and non-peer reviewed papers wereexcluded
Quality appraisalTwo reviewers (AF and CS) assessed theincluded papers for methodological quality anddisagreements were resolved by discussion The 27-item Downs and Black Checklist (1998) was usedto assess quality Quality thresholds were those usedin a previous systematic review (Crellin et al 201475 for high quality 50 to 74 for mediumquality) Agreement was measured using Cohenrsquos κweighted for closeness of scores
AnalysisSummary statistics for each comparable caregiveroutcome associated with each behavior (meansstandard deviation and sample size) were extractedfor each study and were used to calculate the pooledweighted mean and standard deviation for thatoutcome The following formulae were used
Mean for combined studiessum
i n i m isumi n i
where ni isthe sample size for study 1 and mi is the mean forstudy 1 (Price 1970) The standard deviation of thecombined studies [Σi (ni ndash 1) (sdi)2 ((Σi ni) ndash T)]where T is the number of studies (all summationsfrom 1 to T) (Cohen 1988) Standard deviationswere converted to standard errors SE = SDN
MedCalc software (Version 15 Ostend Bel-gium) was used to perform a meta-analysis ofcomparable studies where possible in order toproduce a pooled effect Studies with smallerstandard errors and larger sample sizes weregiven more weight in the calculation The I2
statistic was calculated to denote the percentage ofobserved total variation across studies that is due
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1763
Records identified through database searching (n = 12244)
MEDLINE Ovid = 3618EMBASE Ovid = 576 PsycINFO Ovid = 1502 CINAHL EBSCO = 1056 OpenGrey = 30 Web of Science= 5454
Records after duplicates removed (n = 9485)
Records excluded following the screening of titles and abstracts
(n = 8892)
Studies included (n = 32)
Full-text articles excluded n = 553
(No data on the association between BPSD
and distress n = 425 ) (Not English n = 32)
(No dementia n = 20 ) (Not a family carer n = 22)
(Review n = 35) (Report n = 1)
(Residential care n = 17) (Thesis n = 1)
Full-text screened and articles assessed for eligibility (n = 593)
Hand searched reference lists(n = 8)
Total studies included(n = 40)
Figure 1 Study selection process
to heterogeneity A p value of gt010 determines ifheterogeneity is present consequently the summaryeffect from the random-effects model rather thanthe fixed-effects model is utilized In cases wheredata were not amenable to meta-analysis (either notcomparable or insufficient data) these studies werecompared descriptively and tabulated
Results
A total of 12244 references were identified(Figure 1) of which 11651 were excluded byscreening the title abstract and the removal ofduplicates Of the remaining 593 references fulltexts were sought and 40 met the inclusion criteriaregardless of quality Reasons for exclusion can beseen in Figure 1
The 40 included studies were quantitativemainly cross-sectional with two longitudinal studies(Berger et al 2005 Johnson et al 2013) 21 studies
were graded as high quality and 19 as mediumquality A brief summary of the demographic dataof the studies is provided in Table S1 along with adescription of the measures used quality score andthe main findings There was little consistency inthe sample populations across studies The includedstudies consisted of 10978 caregivers in total ofthese 67 were female and had a mean age of60 years Only five studies reported ethnicity Ofthose which reported dementia stage nine studiesincluded participants with mild dementia 20 withmoderate and one with severe dementia
Quality appraisal of included studiesLevel of agreement between the two independentreviewers was κ = 072 p = 0002 95 CI (073078) indicating substantial agreement (Landis andKoch 1977) The studies scoring the lowest onthe checklist were Haley et al (1987) Hishikawaet al (2012) and Savorani et al (1998) All studieslost points on questions covering external validity
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1764 A Feast et al
validity and reliability of outcome measures and thereporting of statistics
Meta-analysis of comparable studiesSixteen of the 40 studies were suitable to beincluded in a meta-analysis of mean distress scores(see Table S2 available as supplementary materialattached to the electronic version of this paper atwwwjournalscambridgeorgjid_IPG) All of thesestudies reported data on the mean and standarddeviation of distress associated with the meantotal score on the NPI for individual behaviorsEach adapted version of the NPI was reportedas valid and reliable and all were administeredby a researcher or clinician Five studies utilizedthe ten-item version of the NPI thereforedata reporting distress associated with sleep andappetiteeating change were unavailable for thesestudies Participants were recruited from clinic-based and population-based studies had a mix ofdementia participants and studies only includingthose with a diagnosis of Alzheimerrsquos diseaseParkinsonrsquos disease dementia and frontotemporaldementia (see Table S1 available as supplementarymaterial attached to the electronic version of thispaper at wwwjournalscambridgeorgjid_IPG) InTable S3 (available as supplementary materialattached to the electronic version of this paperat wwwjournalscambridgeorgjid_IPG) the meandistress reported for the total NPI symptom canbe seen for each of the 16 studies along with thepooled standard deviations for each behavior acrossthe studies There is considerable variation betweenthe studies for each of the symptoms this can beseen in Figure 2 in particular there is substantialvariation in the mean distress reported for the totalscore of irritable behavior Baiyewu et al (2003)reported 06 (between ldquonot at all distressingrdquo andldquominimally distressingrdquo) and Balieiro et al (2010)reported 36 (between ldquomoderatelyrdquo and ldquoseverelyrdquodistressing) However it is possible to concludethat euphoria was the least distressing across thestudies
As seen in Figure 3 the most distressingBPSD across the 16 studies was depressionAgitationaggression was the second most distress-ing followed by apathy Euphoria was the leastdistressing and had the smallest standard errorDelusional and euphoric behaviors were the onlytwo behaviors with a standard deviation exceedingthe mean indicating high variance between studiesfor these behaviors
Four studies reported correlation data betweenmean NPI total scores and mean NPI distress(Matsumoto et al 2007 Balieiro et al 2010Davidsdottir et al 2012 Huang et al 2012)
all of these studies were involved in the previousmeta-analysis other than Davidsdottir et al (2012)Three of these studies reported data on all 12behaviors The sample size and the correlationcoefficients were entered into MedCalc in order toproduce a pooled effect size for each behavior Thepooled effect sizes within the fixed-effect modelrandom-effects model and heterogeneity statisticsare reported in Table 1 Significant heterogeneitywas identified between studies for all behaviorsother than apathy and sleep In contrast tothe mean distress data the meta-analysis of thecorrelation data identified that irritable behaviorwas the most strongly associated with caregiverdistress followed by aberrant motor behavior andthen delusions Disinhibition had the weakestassociation with distress Depression was seento be one of the behaviors which was morestrongly associatedcorrelated with distress acrossboth meta-analyses Appetite and eating-relatedbehavior was one of the behaviors which had aweaker associationcorrelation with distress acrossboth meta-analyses
Non-comparable studiesTwenty of the 40 included studies were notsuitable for meta-analysis These studies werenot comparable in terms of BPSD measure andthe associated unit of measurement caregiverwell-being measure and the associated unit ofmeasurement It was therefore only possible tocompare these 20 studies descriptively due to theirheterogeneity
Prevalence of BPSD and the impact oncaregiver well-beingMean prevalence and mean distress were reportedon the NPI by Haley et al (2008) and deVugt et al (2006) Although these two studiesboth measure prevalence of BPSD methodsfor measuring caregiver well-being differed (seeTable S1)
Frequency of BPSD and caregiver well-beingMemory-related behaviors were reported as moststressful and problematic across three studies(Nygaard 1998 Quayhagen and Quayhagen 1998Muangpaisan et al 2010) However Robinsonet al (2001) and Fauth and Gibbons (2014) bothfound the frequency of memory-related behaviorswas associated with the least amount of reactivityDisruptive behaviors were associated with themost reactivity followed by depressive behaviors(Robinson et al 2001 Fauth and Gibbons2014) In all of the studies which measuredhallucinations caregivers reported this behavior
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1765
005
115
225
335
445
Mea
n di
stre
ss
Delusions Hallucinations AgitationAggression Depression
005
115
225
335
Mea
n di
stre
ss
Anxiety Euphoria Apathy Disinhibition
0
05
1
15
2
25
3
35
4
Mea
n di
stre
ss
Irritability Aberrant motor behaviour Sleep Appettite and eating
Figure 2 Mean distress scores across 16 studies for behaviors on the NPI (total score)
as less problematic burdensome and distressingcompared to many of the other behaviors Verbalaggression across three of the five studies wasreported as problematic and burdensome Acrosstwo of the five studies which reported sexualdisinhibition this behavior was reported as theleast problematic Reports of wandering acrossfour of the studies were not consistent since
some of the studies reported this behavior asmuch more problematic and burdensome thanothers
Across four of the five studies which reportedincontinence this was consistently reported as oneof the more burdensome stressful and problematicbehaviors Physical aggression was only measuredin three studies and only one study reported this
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1766 A Feast et al
Figure 3 Meta-analysis of mean distress for each BPSD associated with NPI total score
behavior as a common problem Both studies whichreported irritability identified this behavior to be oneof the most problematic and burdensome
Correlational data between BPSD andcaregiver well-beingSleeping- and eating-related behaviors were foundto be significantly correlated to burden and strainhowever they had a stronger association withburden (Donaldson et al 1998) With regard toadult-child caregivers four (delusions agitationdisinhibition and appetiteeating change) of theeight behaviors reported by Conde-Sala et al (2010)as being significantly associated with burden werealso found to be significantly associated with burdenby Allegri et al (2006) Apathy and irritabilitywere reported to be significantly associated withburden in the study conducted by Conde-Sala et al(2010) but no significant relationship was reportedby Allegri et al (2006) Spousal caregivers onlyfound appetiteeating change burdensome (Conde-Sala et al 2010) Apathy had a moderate significantassociation with burden in spousal and adult-child caregivers (Conde-Sala et al 2010) but thisassociation was non-significant in the data reported
by Allegri et al (2006) Delusional and irritablebehaviors were also reported as non-significantlyrelated to burden (Allegri et al 2006) but weresignificantly related to burden by Conde-Sala et al(2010) In contrast to the previous studies reportingthe weak association between euphoria and distressFuh et al (2001) reported a significant correlationbetween euphoria and burden No other behaviorson the NPI had a significant correlation with burden(Fuh et al 2001)
In agreement with the data concerning atthe association between the frequency of thebehavior within each subscale on the RMBPCand reactivity disruptive behaviors had the largestcorrelation of the three subscales with burden(Huang et al 2012) Using the BEHAVE-AD (Reisberg et al 1982) and the NOSGER(Spiegel et al 1991) mood social behaviorsand disturbing behaviors were found to havea significant moderate association with burdenbut no significant correlations with depression incaregivers Chiu et al (2014) noted that all of thebehaviors on the NPI significantly predicted sleepdisturbance in caregivers other than anxiety andaberrant motor behavior
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1767
Table 1 Meta-analysis of mean distress scores correlated with behaviors using NPI total scores
P O O L E D C O R RELATION COEFFI CIENT T EST F OR HETEROGENEITY
FI XE D-E FF E C T S RANDOM-E FF E C T S
BEHAVIOR N MODEL (95 CI) MODEL (95 CI) I2 95 CI P
Delusions 243 0557 (0462 to 0640) 0567 (0412 to 0690) 5864 000 to 8623 p = 00643Hallucinations 243 0502 (0399 to 0532) 0520 (0198 to 0791) 8771 7081 to 9482 p lt 00001AgitationAggression 243 0540 (0443 to 0625) 0537 (0299 to 0712) 7941 4517 to 9482 p = 00022Depression 243 0528 (0429 to 0615) 0564 (0360ndash0717) 7465 2949 to 9089 p = 00080Anxiety 243 0482 (0377 to 0575) 0481 (0236 to 0669) 7845 4203 to 9199 p = 00030Euphoria 243 0540 (0443 to 0625) 0480 (0147 to 0715) 8764 7061 to 9480 p lt 00001Apathy 243 0456 (0351 to 0554) 0459 (0351 to 0540) 000 000 to 8423 p = 04834Disinhibition 243 0357 (0240 to 0464) 0371 (0162 to 0548) 6574 000 to 8833 p = 00327Irritability 243 0668 (0590 to 0733) 0691 (0486 to 0823) 8281 5601 to 9329 p = 00006Aberrant motor
behavior243 0606 (0518 to 0681) 0603 (0437 to 0730) 6764 371 to 8871 p = 00280
Sleep 176 0438 (0307 to 0552) 0436 (0301 to 0554) 532 000 to 9682 p = 03478Appetite and eating 176 0405 (0271 to 0523) 0442 (0200 to 0633) 6617 000 to 9026 p = 00520
Predictive data between BPSD and well-beingConde-Sala et al (2010) Chappell and Penning(1996) Davis and Tremont (2007) and Slachevskyet al (2013) used the same burden measurebut used different measures of BPSD Apathysignificantly predicted burden across three studiesalthough it was less burdensome for adult-childcaregivers and did not predict apathy in the study byDavis and Tremont (2007) Three studies (Mouriket al 2004 Khoo et al 2013 Lee et al 2013)reported data identifying which behaviors predicteddistress as measured by the NPI Apathy wasa significant predictor across two of the threestudies Delusions and anxiety were the only othercomparable behaviors across two of the three studiesand were both significant predictors of distressCovinsky et al (2003) did not use a formal behaviorscale but identified that anger and aggressivebehaviors were stronger predictors of caregiverdepression followed by dangerous behaviors to selfand others and then behaviors which wake thecaregiver up at night
Discussion
To our knowledge this is the first review to controlfor the effect of multiple BPSD on caregiver well-being by discriminating between individual BPSDand also discriminating between caregiver outcomesof well-being Additional advantages of this reviewwere the use of a formal method of synthesis andthe decision to distinguish between how BPSD andcaregiver well-being are measured which ensuredvalid conclusions were drawn by only synthesizing
comparable data Only two meta-analyses werepossible due to limited homogeneous studiesCategories in which the relationship betweenBPSD and well-being were qualitatively examinedincluded minimal studies displaying considerablevariation therefore valid conclusions could not bedrawn The results are discussed in the context ofprevious research
Meta-analysis of mean distress scoresAs seen in Figures 2 and 3 even within one measureand one criterion (distress associated with totalscore on the NPI) variability in distress ratingsfor each symptom can be seen between the 16studies This was also evident in research conductedby Fauth and Gibbons (2014) in which a widevariation in the prevalence of NPI symptoms wasseen between studies However data regardingdistress associated with euphoria and delusionsdemonstrated high levels of variance in terms of theratio between the mean and the standard deviationresulting in considerable variability between scoresTherefore the ratio of the mean distress ratingscompared with the standard deviation associatedwith the other ten behaviors signifies that there islow variance between the 16 studies It is unclearat present why there is increased variability foreuphoric and delusional behaviors In terms of totalscore depression followed by agitationaggressionand apathy were found to be the most distressingfor caregivers across 16 studies in the meta-analysis(Figure 3) This suggests that it is mood-relatedbehaviors which are associated with increaseddistress Fauth and Gibbons (2014) examinedthe relationship between total score of BPSD
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1768 A Feast et al
and distress and found similar results howevereven with identical analysis there were noteworthydiscrepancies such as delusions being the mostdistressing but only the fourth most distressing inthe current review Consistent with the currentmeta-analysis of mean data apathy and depression-related behaviors have been reported as distressingin numerous studies (Teri 1997 deVugt et al2003 Aarsland et al 2007 Kosberg et al 2007)Similarly depression in the person with dementia isassociated with depression in the caregiver (Waiteet al 2004)
Meta-analysis of correlation dataAs seen in Table 1 there were high levels ofheterogeneity between the studies included in thesecond meta-analysis investigating which behaviorswere associated with distress Only apathy- andsleep-related behaviors displayed homogeneitybetween studies Furthermore behaviors which hadstronger correlations with distress (Table 1) didnot have strong associations in the previous meta-analysis (Figure 3) regarding distress associatedwith behaviors At present it is unclear why thisdiscrepancy exists and also why distress correlatedwith apathy- and sleep-related behaviors is more ho-mogenous between studies than the other behaviorsSince only a few studies contributed to this meta-analysis more research is needed to investigate thepooled effects Nevertheless a meta-analysis of thisnature has not been performed previously and therandom-effects model was used to report a moreconservative estimate for the heterogeneous pooledeffects in order to reduce bias
Apathy and irritable behaviors were not con-sistently significantly correlated to burden acrossmultiple studies whereas delusions agitationdisinhibition and appetiteeating change werethese associations were also reported in otherstudies (Rymer et al 2002 Rocca et al 2010) Incontrast a review by Ornstein and Gaugler (2012)reported that angeraggression and depression werethe most frequently cited BPSD associated withcaregiver burden depression was also linked tocaregiver burden in a review by Black and Almeida(2004) In addition to burden delusional behaviorwas consistently associated with distress acrossstudies with a significant correlation also beingseen with stress (Kosmala and Kloszewska 2004)Berger et al (2005) noted that behaviors whichare significantly correlated with burden are notcorrelated with depression This demonstrates theimportance of including multiple measures of well-being since the same behaviors affect caregiversdifferently which has implications for futureinterventions
Studies unamenable to quantitative synthesisOnly two studies reported the prevalence of BPSDand the impact on caregiver well-being due todifferences between studies comparisons werenot possible Although five studies reported thefrequency of BPSD each measure of caregiver well-being was different Memory-related behaviorsverbal aggression incontinence and irritabilitywere reported to affect well-being across multiplestudies These findings were also seen in previousresearch (Bruce and Paterson 2000 Farran et al2004) However Fauth and Gibbons (2014) andRobinson et al (2001) did not find that memory-related behaviors were distressing despite being themost frequent type of behavior on the RMBPCHallucinations sexual disinhibition and physicalaggression were consistently reported to affect well-being less than the other behaviors Although thisfinding is reflected in the majority of studies Haleyet al (2008) and Arango-Lasprilla et al (2010)reported contradictory results
It is noteworthy that aggressionagitation whenmeasured in terms of total score was reported asthe second most distressing across 16 of the studiesbut when measured in terms of frequency only oneof the three studies reported physical aggressionas a common problem However the frequency ofverbal aggression consistently affected well-beingIt is not possible to provide an explanation for thisdiscrepancy but it may be because of the distinctionbetween how aggressionagitation is measured (ietotal score or frequency) or that verbal and physicalaggression have been differentiated and thereforeaffect caregiver well-being differently
Predictive data were limited and heterogeneousin the present review however it was possible toconclude that apathy predicted burden and distressacross studies Anger restlessness combativenessdangerous to others and embarrassing behaviorwere found to be strong predictors of burden ina study by Gaugler et al (2011) Only one studyreported the predictors of caregiver depression
Potential explanations for variability incaregiver well-beingDifference in study quality does not appear to be anexplanation for the variation in distress rating acrossstudies since even between two medium qualitystudies there was considerable variation (Balieiroet al 2010 displaying one of the highest meandistress scores Baiyewu et al 2003 displayingone of the lowest) Two studies consistently hadthe highest mean distress rating across each of thebehavior domains Balieiro et al (2010) and Tanet al (2005) Both of these studies were clinic-basedhigher distress ratings would be expected as those
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1769
experiencing more BPSD might be more likely toattend a clinic as indeed were the majority ofstudies included in the meta-analysis It may bepossible that dementia severity is an explanationsince participants in the studies with the highestdistress scores (Tan et al 2005 Balieiro et al 2010)had moderate and severe dementia respectivelywhereas Baiyewu et al (2003) who consistentlyreported the lowest distress scores across eachof the behavior domains included participantswith mild dementia However both Aarslandet al (2007) and de Vugt et al (2006) reportedlower mean distress scores in comparison with theother included studies and they both includedparticipants with moderate dementia FurthermoreDavidsdottir et al (2012) found that there wasno significant difference between caregiver distressscores depending on dementia severity
Baiyewu et al (2003) had a much smallersample of spousal caregivers in comparison to Tanet al (2005) which might account for the lowerdistress scores This is in agreement with Almberget al (1997) who reported that spouses experiencegreater levels of burden However three studieswhich had consistently higher mean distress scoresacross all behaviors (Tan et al 2005 Balieiro et al2010 Huang et al 2012) were mainly comprisedof adult-child caregivers When comparing a studysolely comprised of spousal caregivers (deVugt et al2006) with a study (Baiyewu et al 2003) withminimal spousal caregivers (25) it was possibleto see that spousal caregivers were substantiallymore distressed with depressive apathetic andanxiety-related behaviors Although distress ratingscan be differentiated between behavior types forspousal and non-spousal caregivers both Baiyewuet al (2003) and de Vugt et al (2006) had two of thelowest distress scores across all behaviors in compar-ison to the other studies in the meta-analysis
The explanation may also be cultural sinceBaiyewu et al (2003) and Baiyewu et al (2012)(with similarly low distress scores across behaviors)were the only Africa-based studies in the meta-analysis Baiyewu et al (2003) and Baiyewu et al(2012) were also both community-based studieswhich may also be a reason for the reduceddistress ratings There is every reason to believethat BPSD are present across cultures (Shajiet al 2009) however the low levels of publicawareness of dementia have many implications(Prince 2000) One of these implications maybe the misinterpretation of BPSD as deliberateconsequently affecting the well-being of the carer(Shaji et al 2009) It is beyond the scope ofthis paper to determine why there is considerablevariation between studies reporting caregiverdistress for identical behaviors using identical
measures However it is likely that it is the caregivercharacteristics rather than the characteristics of theperson with dementia (such as dementia severity)which may underlie the explanation as to whyvariation between studies exists
Limitations
The data available for this review allowed for onlytwo meta-analyses to be conducted There wererelatively few studies which assessed the relationshipbetween individual BPSD and caregiver well-beingand which met the inclusionexclusion criteriafor the review In an attempt to be systematicbased on prior recommendation an effort wasmade to distinguish between how ldquoproblematicrdquosymptoms are measured Consequently studieswere categorized into whether BPSD weremeasured in terms of frequency or prevalence andalso categorized in terms of the statistical analysisemployed Other than data regarding mean distressassociated with NPI total score only a small amountof studies were included in each category andunfortunately it was often the case that measuresof caregiver well-being were dissimilar From the 40included studies there were 12 different measuresof behavior and 17 different measures of well-being making comparisons difficult which mayhave contributed to the inconsistent findings
The majority of included studies recruitedparticipants from clinics therefore caregiversincluded in the review were not representative ofthe population In addition the samples across theincluded studies were heterogeneous in a numberof factors therefore caution should be taken wheninterpreting the results Although beyond the scopeof this review study characteristics such as culturegender and relationship direction were not ex-amined through subgroup analyses Due to the lim-ited number of studies it was not possible to imposea quality criteria however all included studies wereeither of high or medium quality as assessed by theDowns and Back Checklist (1998) Furthermore allof the included studies relied on caregiver reportsof BPSD which may themselves be affected bycaregiver well-being unfortunately it is not possibleto determine if this was the case Nonetheless twovalid meta-analyses were completed and a numberof comments can be made about the relationshipbetween BPSD and caregiver well-being
Implications and recommendations
The vast majority of studies addressing the rela-tionship between BPSD and caregiver well-being
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1770 A Feast et al
did not examine individual BPSD Consequentlythis comparatively limited the amount of studiesincluded in the present review Therefore if we areto understand this relationship more studies needto examine individual BPSD in their research Inaddition it is more clinically relevant to examinewhich BPSD affect well-being rather than BPSDas a whole as this is essential in determiningwhere clinical staff should allocate resources mosteffectively Nevertheless there is preliminary datasuggesting it is mood-related behaviors whichare associated with increased levels of distresstherefore interventions for the management ofBPSD should target these behaviors
The lack of consistency in the measurementof BPSD (neuropsychiatric or memory problemsfrequency or prevalence) and the measurementof caregiver well-being (the use of interchangeableterminology such as stress strain and burdenmeaning the same construct) limits our ability toreach a consensus as to which BPSD result inthe most negative outcomes for caregivers Forexample Donaldson et al (1998) used GilleardrsquosStrain Scale (1984) to measure burden andthe General Health Questionnaire (Goldberg andHillier 1979) to measure distress Furthermorefour studies (see Table S1) did not have formalscales to measure the impact of BPSD on well-being and used terms such as ldquoburdensomerdquoldquoseriousrdquo and ldquodisturbingrdquo This problem impactsupon the validity and reliability of the originalstudies and consequently the review Howeverthis mainly occurred in the earlier studies Futureresearch should also include more than one measureof well-being in order to identify if individual BPSDdifferentially affect caregiver burden compared tocaregiver distress as identified in the current reviewFurthermore future research should identify whythere is reduced variability in distress ratings forcertain behaviors compared to others and whycertain behaviors are more distressing dependingon which type of statistical analysis is used
Although there are potential methodologicalreasons (limited studies inconsistent measures)for why there is substantial variability whenidentifying which BPSD affect certain types ofcaregiver well-being the most there is growingevidence that factors associated with the personwith dementia (eg BPSD frequency cognition) areonly part of the story when explaining a caregiverrsquosresponse to BPSD Caregiver characteristicshave been shown to account for twice thevariance of person with dementia characteristicswhen reporting neuropsychiatric symptoms (Sinket al 2006) and the presence of BPSD wasnot found to be a significant predictor ofburden whereas caregiver characteristics such as
confidence neuroticism and relationship qualitywere significant predictors (Campbell et al 2008)Therefore as recommended by Ornstein andGaugler (2012) future studies should focus onidentifying pathways for the association betweenindividual BPSD caregiver variables and caregiveroutcomes More research is needed to understandif and why certain BPSD affect certain caregiveroutcomes and also how much of this is attributableto caregiver variability in response to BPSD ratherthan the presence of BPSD itself More longitudinalstudies would be useful to examine how changes inindividual BPSD are associated with caregiver well-being over time A review by Black and Almeida(2004) examined the limited longitudinal studiesavailable and reported mixed findings betweenburden and BPSD and found no associationbetween BPSD and distress Although BPSDincreased significantly over a two-year periodcaregiver burden remained stable and depressionwas found to decrease (Berger et al 2005) Futureresearch needs to examine caregiver factors overtime (well-being role captivity etc) along withchanges in individual BPSD in order to have a morevalid understanding of this relationship
Caution should be exercised when creating ameasure of BPSD since Jackson et al (2014)found that the Revised Memory and BehaviorProblem Checklist (Teri et al 1992) might bemore suitable in explaining caregiver depressionthan the NPI It is important that the measureof BPSD is not biased toward explaining a moreunique association between BPSD and a measure ofcaregiver well-being such as depression As stated byGitlin and Rose (2014) item selection for measuresof BPSD is often based upon specific disciplines(eg neurology psychiatry social sciences) andthus implicitly represents different conceptual-izations of behavior A shared framework fordefining behaviors and their underlying causesmust be created in order to move on fromthe implicit assumption of most measures thatbehaviors are a direct cause of neuropathologyand to develop measures which also address thecontextual and caregiver characteristics associatedwith the behavior
Conclusions
This study has improved our understanding of theimpact of individual BPSD on caregiver well-beingin particular caregiver distress The relationshipbetween individual BPSD and caregiver well-beingwas inconsistent and varied according to behavioralsymptom Due to limited studies and heterogeneousdata the results should be interpreted with caution
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1771
but advances have been made with respect towhich behaviors are associated with distress Theinconsistencies may be partly explained by caregivervariables which were not taken into account inthe review Based on this review and previousresearch it is not possible to fully understand therelationship between BPSD and caregiver well-being without examining the influence of caregivervariables such as caregiver strategies acceptancegender relationship with person with dementiaand confidence We recommend that future studiesare designed to examine individual BPSD ratherthan BPSD as a whole use consistent measures forBPSD and well-being use consistent terminologyfor psychological constructs (eg burden) andexamine the causal mechanisms by which individualBPSD impact caregiver well-being by collectingdata on a range of caregiver factors Theseapproaches will clarify whether it is important forclinicians to focus on the frequency or prevalence ofcertain BPSD in addition to targeting the presenceof certain caregiver characteristics and addressingunmet need
Conflict of interest
None
Description of authorsrsquo roles
A Feast was responsible for developing the reviewobjectives writing the search strategies conductingthe searches designing and completing studyeligibility and data extraction forms undertakingthe quality appraisals conducting the meta-analysisand writing the paper M Orrell was responsible fordeveloping the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper C Stoner was responsible forundertaking the quality appraisals and assisting inwriting the paper G Charlesworth was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper E Moniz-Cook was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper
Acknowledgments
We would like to thank Dr Zoeuml Hoare for herstatistical advice This paper presents independentresearch funded by the National Institute for HealthResearch (NIHR) under its Programme Grants forApplied Research (RP-PG-0606-1067 and RP-PG-
060- 1083) The views expressed in this publicationare those of the author(s) and not necessarily thoseof the NHS the NIHR or the Department ofHealth
Supplementary Material
To view supplementary material for thisarticle please visit httpdxdoiorg101017S1041610216000922
References
Aarsland D et al (2007) Neuropsychiatric symptoms inpatients with Parkinsonrsquos disease and dementia frequencyprofile and associated care giver stress Journal of NeurologyNeurosurgery amp Psychiatry 78 36ndash42doihttpdxdoiorg101136jnnp2005083113
Allegri R F et al (2006) Neuropsychiatric symptoms as apredictor of caregiver burden in Alzheimerrsquos diseaseNeuropsychiatric Disease amp Treatment 2 105ndash110doi102147ndts47133
Almberg B Grafstrom M and Winblad B (1997)Major strain and coping strategies as reported by familymembers who care for aged demented relatives Journal ofAdvanced Nursing 26 683ndash691doihttpdxdoiorg101046j1365-2648199700392x
Arango-Lasprilla J C Lehan T Drew A MorenoA Deng X and Lemos M (2010) Health-relatedquality of life in caregivers of individuals with dementiafrom Colombia American Journal of Alzheimerrsquos Disease andOther Dementias 25 556ndash561doi1011771533317510382287ltbibgt
Baiyewu O et al (2003) Behavioral and caregiver reactionof dementia as measured by the neuropsychiatric inventoryin Nigerian community residents InternationalPsychogeriatrics 15 399ndash409doi101017s1041610203009645
Baiyewu O et al (2012) Behavioral symptoms incommunity-dwelling elderly Nigerians with dementia mildcognitive impairment and normal cognition InternationalJournal of Geriatric Psychiatry 27 931ndash939 doihttpdxdoiorg101002gps2804
Balieiro A P Jr Sobreira E S T Pena M C SSilva-Filho J H and Vale F A C (2010) Caregiverdistress associated with behavioral and psychologicalsymptoms in mild Alzheimerrsquos disease Dementia eNeuropsychologia 4 238ndash244
Ballard C G et al (1995) The aetiology of depression inthe carers of dementia sufferers Journal of AffectiveDisorders 35 59ndash63 doi1010160165-0327(95)00041-k
Bandeira D R Pawlowski J Goncalves T RHilgert J B Bozzetti M C and Hugo F N (2007)Psychological distress in Brazilian caregivers of relativeswith dementia Aging and Mental Health 11 14ndash19doi10108013607860600640814
Berger G Bernhardt T Weimer E Peters JKratzsch T and Frolich L (2005) Longitudinal studyon the relationship between symptomatology of dementia
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1772 A Feast et al
and levels of subjective burden and depression amongfamily caregivers in memory clinic patients Journal ofGeriatric Psychiatry and Neurology 3 119ndash128doi1011770891988704273375
Black W and Almeida O P (2004) A systematic reviewof the association between the behavioral and psychologicalsymptoms of dementia and burden of care InternationalPsychogeriatrics 16 295ndash315doi101017s1041610204000468
Bruce D G and Paterson A (2000) Barriers tocommunity support for the dementia carer a qualitativestudy International Journal of Geriatric Psychiatry 15451ndash457 doi101002(sici)1099-1166(200005)155lt451aid-gps143gt30co2-k
Campbell P et al (2008) Determinants of burden in thosewho care for someone with dementia International Journalof Geriatric Psychiatry 23 1078ndash1085doi101002gps2071
Cerejeira J Lagarto L and Mukaetova-LadinskaE B (2012) Behavioral and psychological symptoms ofdementia Frontiers in Neurology 3 1ndash23doi103389fneur201200073
Chappell N L and Penning M (1996) Behaviouralproblems and distress among caregivers of people withdementia Ageing amp Society 16 57ndash73doi101017s0144686x00003135
Chiu Y C et al (2014) Family caregiversrsquo sleepdisturbance and its associations with multilevel stressorswhen caring for patients with dementia Aging amp MentalHealth 18 92ndash101 doihttpdxdoiorg101080136078632013837141
Cohen J (1988) Statistical Power Analysis for the BehavioralSciences 2nd edn New York University New YorkLawrence Erlbaum Associatesdoi1043249780203771587
Conde-Sala J L Garre-Olmo J Turroacute-Garriga OVilalta-Franch J and Loacutepez-Pousa S (2010)Differential features of burden between spouse andadult-child caregivers of patients with Alzheimerrsquos diseasean exploratory comparative design International Journal ofNursing Studies 47 1262ndash1273doi101016jijnurstu201003001
Covinsky K E et al (2003) Patient and caregivercharacteristics associated with depression in caregivers ofpatients with dementia Journal of General Internal Medicine18 1006ndash1014 doihttpdxdoiorg101111j1525-1497200330103x
Craig D Mirakhur A Hart D J McIlroy S P andPassmore A P (2005) A cross-sectional study ofneuropsychiatric symptoms in 435 patients withAlzheimerrsquos disease American Journal of GeriatricPsychiatry 13 460ndash468 doi10109700019442-200506000-00004
Crellin N Charlesworth G and Orrell M (2014)Measuring family caregiver efficacy for managing behavioraland psychological symptoms in dementia a psychometricevaluation International Psychogeriatrics 26 93ndash103 doihttpdxdoiorg101017s1041610213001646
Davidsdottir S R Snaedal J Karlsdottir GAtladottir I and Hannesdottir K (2012) Validationof the Icelandic version of the neuropsychiatric inventorywith caregiver distress (NPI-D) Nordic Journal of
Psychiatry 66 26ndash32 doihttpdxdoiorg103109080394882011593100
Davis J D and Tremont G (2007) Impact of frontalsystems behavioral functioning in dementia on caregiverburden The Journal of Neuropsychiatry and ClinicalNeurosciences 19 43ndash49 doihttpdxdoiorg101176jnp200719143
de Vugt M E Riedijk S R Aalten P Tibben Avan Swieten J C and Verhey F R J (2006) Impactof behavioural problems on spousal caregivers acomparison between Alzheimerrsquos disease andfronto-temporal dementia Dementia and Geriatric CognitiveDisorders 22 35ndash41 doi101159000093102
de Vugt M E et al (2003) Behavioural disturbances indementia patients and quality of the marital relationshipInternational Journal of Geriatric Psychiatry 18 149ndash154doi101002gps807
Donaldson C Tarrier N and Burns A (1998)Determinants of carer stress in Alzheimerrsquos diseaseInternational Journal of Geriatric Psychiatry 13 248ndash256doi101002(sici)1099-1166(199804)134lt248aid-gps770gt30co2-0
Downs S and Black N (1998) The feasibility of creating achecklist for the assessment of the methodological qualityboth of randomised and non-randomised studies of healthcare interventions Journal of Epidemiological CommunityHealth 52 377ndash384 doi101136jech526377
Farran C J Loukissa D A Lindeman D A andMcCann J (2004) Caring for self while caring for othersthe two-track life of coping with Alzheimerrsquos diseaseJournal of Gerontological Nursing 30 38ndash45doi1039280098-9134-20040501-09
Fauth E B and Gibbons A (2014) Which behavioral andpsychological symptoms of dementia are the mostproblematic Variability by prevalence intensity distressratings and associations with carer depressive symptomsInternational Journal of Geriatric Psychiatry 29 263ndash271doi101002gps4002
Fuh J L Liu C K Mega M S Wang S J andCummings J L (2001) Behavioral disorders andcaregiversrsquo reaction in Taiwanese patients with Alzheimerrsquosdisease International Psychogeriatrics 13 121ndash128 doihttpdxdoiorg101017s1041610201007517
Gaugler J E et al (2011) Does caregiver burden mediatethe effects of behavioral disturbances on nursing homeadmission The American Journal of Geriatric Psychiatry 19497ndash506 doi101097jgp0b013e31820d92cc
Gilleard C J Belford H Gilleard E Whittick J Eand Gledhill K (1984) Emotional distress amongst thesupporters of the elderly mental infirm British Journal ofPsychiatry 145 172ndash177doihttpdxdoiorg101192bjp1452172
Gitlin L N and Rose K (2014) Factors associated withcarer readiness to use nonpharmacologic strategies tomanage dementia-related behavioral symptomsInternational Journal of Geriatric Psychiatry 29 93ndash102doihttpdxdoiorg101002gps3979
Goldberg D P and Hillier V F (1979) A scaled versionof the general health questionnaire Psychological Medicine9 139ndash145 doi101017s0033291700021644
Gonzalez-Salvador M T Arango C Lyketsos C Gand Barba A C (1999) The stress and psychological
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1773
morbidity of the Alzheimer patient caregiver InternationalJournal of Geriatric Psychiatry 14 701ndash710doi101002(sici)1099-1166(199909)149lt701aidps5gt30co2-
Haley W E Brown S and Levine E G (1987) Familycaregiver appraisals of patient behavioral disturbance insenile dementia Clinical Gerontologist The Journal of Agingand Mental Health 6 25ndash34doi101300j018v06n04_04
Haley W E Levine E G Brown S L Berry J Wand Hughes G H (2008) The psychological social andhealth consequences of caring for a relative with seniledementia Journal of the American Geriatrics Society 35405ndash411 doi101111j1532-54151987tb04661x
Hishikawa N et al (2012) Effects of turmeric onAlzheimerrsquos disease with behavioral and psychologicalsymptoms of dementia Ayu 33 499ndash504 doihttpdxdoiorg1041030974-8520110524
Huang S S Lee M C Liao Y C Wang W F andLai T J (2012) Caregiver burden associated withbehavioral and psychological symptoms of dementia(BPSD) in Taiwanese elderly Archives of Gerontology andGeriatrics 55 55ndash59 doihttpdxdoiorg101016jarchger201104009
Jackson M A Fauth E B and Geiser C (2014)Comparing the neuropsychiatric inventory and the revisedmemory and behavior problems checklist for associationswith caregiver burden and depressive symptomsInternational Psychogeriatrics 26 1021ndash1031doi101017s1041610213002421
Johnson D K Niedens M Wilson J RSwartzendruber L Yeager A and Jones K (2013)Treatment outcomes of a crisis intervention program fordementia with severe psychiatric complications the Kansasbridge project The Gerontologist 53 102ndash112 doihttpdxdoiorg101093gerontgns104
Khoo S A Chen T Y Ang Y H and Yap P (2013)The impact of neuropsychiatric symptoms on caregiverdistress and quality of life in persons with dementia in anAsian tertiary hospital memory clinic InternationalPsychogeriatrics 25 1991ndash1999 doihttpdxdoiorg101017s1041610213001518
Kosberg J I Kaufman A V Burgio L D Leeper Jand Sun F (2007) Family caregiving to those withdementia in rural Alabama racial similarities anddifferences Journal of Aging and Health 19 3ndash21 doi1011770898264306293604
Kosmala K and Kloszewska I (2004) The burden ofproviding care for Alzheimerrsquos disease patients in PolandInternational Journal of Geriatric Psychiatry 19 191ndash193doi101002gps1054
Landis J R and Koch G G (1977) The measurement ofobserver agreement for categorical data Biometrics 33159ndash174 doi 1023072529310
Lee D R McKeith I Mosimann U Ghosh-NodyalA and Thomas A J (2013) Examining carer stress indementia the role of subtype diagnosis andneuropsychiatric symptoms International Journal ofGeriatric Psychiatry 28 135ndash141 doihttpdxdoiorg101002gps3799
Lim Y M Son G R Song J A and Beattie E(2008) Factors affecting burden of family caregivers of
community-dwelling ambulatory elders with dementia inKorea Archives of Psychiatric Nursing 22 226ndash234 doi101016japnu200712005
Matsumoto N et al (2007) Caregiver burden associatedwith behavioral and psychological symptoms of dementia inelderly people in the local community Dementia andGeriatric Cognitive Disorders 23 219ndash224doi101159000099472
Mohamed S Rosenheck R Lyketsos C G andSchneider L S (2010) Caregiver burden in Alzheimerdisease cross-sectional and longitudinal patient correlatesThe American Journal of Geriatric Psychiatry 18 917ndash927doi101097jgp0b013e3181d5745d
Mourik J C Rosso S M Niermeijer M FDuivenvoorden H J Van Swieten J C and TibbenA (2004) Frontotemporal dementia behavioral symptomsand caregiver distress Dementia and Geriatric CognitiveDisorders 18 299ndash306 doihttpdxdoiorg101159000080123
Muangpaisan W et al (2010) Caregiver burden and needsof dementia caregivers in Thailand a cross-sectional studyJournal of the Medical Association of Thailand 93 601ndash607
Neundorfer M M McClendon M J Smyth K AStuckey J C Strauss M E and Patterson M B(2001) A longitudinal study of the relationship betweenlevels of depression among persons with Alzheimerrsquosdisease and levels of depression among their familycaregivers Journal of Gerontology Series B - PsychologicalSciences and Social Sciences 56 301ndash313
Nygaard H A (1998) Strain on caregivers of dementedelderly people living at home Scandinavian Journal ofPrimary Health Care 6 33ndash37doihttpdxdoiorg10310902813438809009287
Ornstein K and Gaugler J E (2012) The problem withldquoproblem behaviorsrdquoa systematic review of the associationbetween individual patient behavioral and psychologicalsymptoms and caregiver depression and burden within thedementia patientndashcaregiver dyad InternationalPsychogeriatrics 24 1536ndash1552doi101017s1041610212000737
Ornstein K Gaugler J E Devanand N S CarolynZ and Yaakov S (2012) The differential impact ofunique behavioral and psychological symptoms for thedementia caregiver how and why do patientsrsquo individualsymptom clusters impact caregiver depressive symptomsThe American Journal of Geriatric Psychiatry 12 77ndash1286doi httpdxdoiorg101016jjagp201301062
Price G R (1970) Selection and covariance Nature 227520ndash521 doi101038227520a0
Prince M (2000) Dementia in developing countries Aconsensus statement from the 1066 Dementia ResearchGroup International Journal of Geriatric Psychiatry 1514ndash20 doihttpdxdoiorg101002(sici)1099-1166(200001)151lt14aid-gps70gt30co2-8
Quayhagen M P and Quayhagen M (1998) Alzheimerrsquosstress coping with the caregiving role Gerontologist 28391ndash396 doihttpdxdoiorg101093geront283391
Reisberg B Ferris S H de Leon M J and Crook T(1982) The global deterioration scale for assessment ofprimary degenerative dementia American Journal ofPsychiatry 139 1136ndash1139 doihttpdxdoiorg101176ajp13991136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1774 A Feast et al
Robinson K M Adkisson P and Weinrich S (2001)Problem behaviour caregiver reactions and impact amongcaregivers of persons with Alzheimerrsquos disease Journal ofAdvanced Nursing 36 573ndash582 doihttpdxdoiorg101046j1365-2648200102010x
Rocca P et al (2010) Neuropsychiatric symptomsunderlying caregiver stress and insight in Alzheimerrsquosdisease Dementia and Geriatric Cognitive Disorders 3057ndash63 doi101159000315513
Rymer S Salloway S Norton L Mallow PCorreia S and Monast D (2002) Impaired awarenessbehavior disturbance and caregiver burden in Alzheimerdisease Alzheimer Disease and Associated Disorders 16248ndash253 doi 10109700002093-200210000-00006
Savorani G Vulcano V Boni S Sarti G andRavaglia G (1998) Behavioral disorders in dementiapatients and their impact on the stress of caregivingrelatives the ldquoARADrdquo questionnaire Archives ofGerontology and Geriatrics 6 481ndash485doi101016s0167-4943(98)80070-8
Shaji K S George R K Prince M J and JacobK S (2009) Behavioral symptoms and caregiver burdenin dementia Indian Journal of Psychiatry 51 45 doihttpdxdoiorg1041030019-554544905
Sink K M Covinsky K E Barnes D E NewcomerR J and Yaffe K (2006) Caregiver characteristics areassociated with neuropsychiatric symptoms of dementiaJournal of the American Geriatrics Society 54 796ndash803 doi101111j1532-5415200600697x
Slachevsky A et al (2013) The CUIDEME studydeterminants of burden in chilean primary caregivers ofpatients with dementia Journal of Alzheimerrsquos Disease 35297ndash306
Spiegel R et al (1991) A new behavioral assessment scalefor geriatric out- and in-patients the NOSGER (nursesrsquoobservation scale for geriatric patients) Journal of theAmerican Geriatric Society 39 339ndash347 doihttpdxdoiorg101111j1532-54151991tb02897x
Tan L L Wong H B and Allen H (2005) The impactof neuropsychiatric symptoms of dementia on distress infamily and professional caregivers in SingaporeInternational Psychogeriatrics 17 253ndash263 doi101017s1041610205001523
Teri L (1997) Behavior and caregiver burden behavioralproblems in patients with Alzheimer disease and itsassociation with caregiver distress Alzheimer Disease andAssociated Disorders 11 35ndash38
Teri L Truax P Logsdon R Uomoto J Zarit Sand Vitaliano P P (1992) Assessment of behavioralproblems in dementia the revised memory and behaviorproblems checklist Psychology and Aging 7 622 doi1010370882-797474622
Waite A Bebbington P Skelton-Robinson M andOrrell M (2004) Social factors and depression in carersof people with dementia International Journal of GeriatricPsychiatry 19 582ndash587 doihttpdxdoiorg101002gps1136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at

Individual BPSD and caregiver well-being 1763
Records identified through database searching (n = 12244)
MEDLINE Ovid = 3618EMBASE Ovid = 576 PsycINFO Ovid = 1502 CINAHL EBSCO = 1056 OpenGrey = 30 Web of Science= 5454
Records after duplicates removed (n = 9485)
Records excluded following the screening of titles and abstracts
(n = 8892)
Studies included (n = 32)
Full-text articles excluded n = 553
(No data on the association between BPSD
and distress n = 425 ) (Not English n = 32)
(No dementia n = 20 ) (Not a family carer n = 22)
(Review n = 35) (Report n = 1)
(Residential care n = 17) (Thesis n = 1)
Full-text screened and articles assessed for eligibility (n = 593)
Hand searched reference lists(n = 8)
Total studies included(n = 40)
Figure 1 Study selection process
to heterogeneity A p value of gt010 determines ifheterogeneity is present consequently the summaryeffect from the random-effects model rather thanthe fixed-effects model is utilized In cases wheredata were not amenable to meta-analysis (either notcomparable or insufficient data) these studies werecompared descriptively and tabulated
Results
A total of 12244 references were identified(Figure 1) of which 11651 were excluded byscreening the title abstract and the removal ofduplicates Of the remaining 593 references fulltexts were sought and 40 met the inclusion criteriaregardless of quality Reasons for exclusion can beseen in Figure 1
The 40 included studies were quantitativemainly cross-sectional with two longitudinal studies(Berger et al 2005 Johnson et al 2013) 21 studies
were graded as high quality and 19 as mediumquality A brief summary of the demographic dataof the studies is provided in Table S1 along with adescription of the measures used quality score andthe main findings There was little consistency inthe sample populations across studies The includedstudies consisted of 10978 caregivers in total ofthese 67 were female and had a mean age of60 years Only five studies reported ethnicity Ofthose which reported dementia stage nine studiesincluded participants with mild dementia 20 withmoderate and one with severe dementia
Quality appraisal of included studiesLevel of agreement between the two independentreviewers was κ = 072 p = 0002 95 CI (073078) indicating substantial agreement (Landis andKoch 1977) The studies scoring the lowest onthe checklist were Haley et al (1987) Hishikawaet al (2012) and Savorani et al (1998) All studieslost points on questions covering external validity
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1764 A Feast et al
validity and reliability of outcome measures and thereporting of statistics
Meta-analysis of comparable studiesSixteen of the 40 studies were suitable to beincluded in a meta-analysis of mean distress scores(see Table S2 available as supplementary materialattached to the electronic version of this paper atwwwjournalscambridgeorgjid_IPG) All of thesestudies reported data on the mean and standarddeviation of distress associated with the meantotal score on the NPI for individual behaviorsEach adapted version of the NPI was reportedas valid and reliable and all were administeredby a researcher or clinician Five studies utilizedthe ten-item version of the NPI thereforedata reporting distress associated with sleep andappetiteeating change were unavailable for thesestudies Participants were recruited from clinic-based and population-based studies had a mix ofdementia participants and studies only includingthose with a diagnosis of Alzheimerrsquos diseaseParkinsonrsquos disease dementia and frontotemporaldementia (see Table S1 available as supplementarymaterial attached to the electronic version of thispaper at wwwjournalscambridgeorgjid_IPG) InTable S3 (available as supplementary materialattached to the electronic version of this paperat wwwjournalscambridgeorgjid_IPG) the meandistress reported for the total NPI symptom canbe seen for each of the 16 studies along with thepooled standard deviations for each behavior acrossthe studies There is considerable variation betweenthe studies for each of the symptoms this can beseen in Figure 2 in particular there is substantialvariation in the mean distress reported for the totalscore of irritable behavior Baiyewu et al (2003)reported 06 (between ldquonot at all distressingrdquo andldquominimally distressingrdquo) and Balieiro et al (2010)reported 36 (between ldquomoderatelyrdquo and ldquoseverelyrdquodistressing) However it is possible to concludethat euphoria was the least distressing across thestudies
As seen in Figure 3 the most distressingBPSD across the 16 studies was depressionAgitationaggression was the second most distress-ing followed by apathy Euphoria was the leastdistressing and had the smallest standard errorDelusional and euphoric behaviors were the onlytwo behaviors with a standard deviation exceedingthe mean indicating high variance between studiesfor these behaviors
Four studies reported correlation data betweenmean NPI total scores and mean NPI distress(Matsumoto et al 2007 Balieiro et al 2010Davidsdottir et al 2012 Huang et al 2012)
all of these studies were involved in the previousmeta-analysis other than Davidsdottir et al (2012)Three of these studies reported data on all 12behaviors The sample size and the correlationcoefficients were entered into MedCalc in order toproduce a pooled effect size for each behavior Thepooled effect sizes within the fixed-effect modelrandom-effects model and heterogeneity statisticsare reported in Table 1 Significant heterogeneitywas identified between studies for all behaviorsother than apathy and sleep In contrast tothe mean distress data the meta-analysis of thecorrelation data identified that irritable behaviorwas the most strongly associated with caregiverdistress followed by aberrant motor behavior andthen delusions Disinhibition had the weakestassociation with distress Depression was seento be one of the behaviors which was morestrongly associatedcorrelated with distress acrossboth meta-analyses Appetite and eating-relatedbehavior was one of the behaviors which had aweaker associationcorrelation with distress acrossboth meta-analyses
Non-comparable studiesTwenty of the 40 included studies were notsuitable for meta-analysis These studies werenot comparable in terms of BPSD measure andthe associated unit of measurement caregiverwell-being measure and the associated unit ofmeasurement It was therefore only possible tocompare these 20 studies descriptively due to theirheterogeneity
Prevalence of BPSD and the impact oncaregiver well-beingMean prevalence and mean distress were reportedon the NPI by Haley et al (2008) and deVugt et al (2006) Although these two studiesboth measure prevalence of BPSD methodsfor measuring caregiver well-being differed (seeTable S1)
Frequency of BPSD and caregiver well-beingMemory-related behaviors were reported as moststressful and problematic across three studies(Nygaard 1998 Quayhagen and Quayhagen 1998Muangpaisan et al 2010) However Robinsonet al (2001) and Fauth and Gibbons (2014) bothfound the frequency of memory-related behaviorswas associated with the least amount of reactivityDisruptive behaviors were associated with themost reactivity followed by depressive behaviors(Robinson et al 2001 Fauth and Gibbons2014) In all of the studies which measuredhallucinations caregivers reported this behavior
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1765
005
115
225
335
445
Mea
n di
stre
ss
Delusions Hallucinations AgitationAggression Depression
005
115
225
335
Mea
n di
stre
ss
Anxiety Euphoria Apathy Disinhibition
0
05
1
15
2
25
3
35
4
Mea
n di
stre
ss
Irritability Aberrant motor behaviour Sleep Appettite and eating
Figure 2 Mean distress scores across 16 studies for behaviors on the NPI (total score)
as less problematic burdensome and distressingcompared to many of the other behaviors Verbalaggression across three of the five studies wasreported as problematic and burdensome Acrosstwo of the five studies which reported sexualdisinhibition this behavior was reported as theleast problematic Reports of wandering acrossfour of the studies were not consistent since
some of the studies reported this behavior asmuch more problematic and burdensome thanothers
Across four of the five studies which reportedincontinence this was consistently reported as oneof the more burdensome stressful and problematicbehaviors Physical aggression was only measuredin three studies and only one study reported this
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1766 A Feast et al
Figure 3 Meta-analysis of mean distress for each BPSD associated with NPI total score
behavior as a common problem Both studies whichreported irritability identified this behavior to be oneof the most problematic and burdensome
Correlational data between BPSD andcaregiver well-beingSleeping- and eating-related behaviors were foundto be significantly correlated to burden and strainhowever they had a stronger association withburden (Donaldson et al 1998) With regard toadult-child caregivers four (delusions agitationdisinhibition and appetiteeating change) of theeight behaviors reported by Conde-Sala et al (2010)as being significantly associated with burden werealso found to be significantly associated with burdenby Allegri et al (2006) Apathy and irritabilitywere reported to be significantly associated withburden in the study conducted by Conde-Sala et al(2010) but no significant relationship was reportedby Allegri et al (2006) Spousal caregivers onlyfound appetiteeating change burdensome (Conde-Sala et al 2010) Apathy had a moderate significantassociation with burden in spousal and adult-child caregivers (Conde-Sala et al 2010) but thisassociation was non-significant in the data reported
by Allegri et al (2006) Delusional and irritablebehaviors were also reported as non-significantlyrelated to burden (Allegri et al 2006) but weresignificantly related to burden by Conde-Sala et al(2010) In contrast to the previous studies reportingthe weak association between euphoria and distressFuh et al (2001) reported a significant correlationbetween euphoria and burden No other behaviorson the NPI had a significant correlation with burden(Fuh et al 2001)
In agreement with the data concerning atthe association between the frequency of thebehavior within each subscale on the RMBPCand reactivity disruptive behaviors had the largestcorrelation of the three subscales with burden(Huang et al 2012) Using the BEHAVE-AD (Reisberg et al 1982) and the NOSGER(Spiegel et al 1991) mood social behaviorsand disturbing behaviors were found to havea significant moderate association with burdenbut no significant correlations with depression incaregivers Chiu et al (2014) noted that all of thebehaviors on the NPI significantly predicted sleepdisturbance in caregivers other than anxiety andaberrant motor behavior
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1767
Table 1 Meta-analysis of mean distress scores correlated with behaviors using NPI total scores
P O O L E D C O R RELATION COEFFI CIENT T EST F OR HETEROGENEITY
FI XE D-E FF E C T S RANDOM-E FF E C T S
BEHAVIOR N MODEL (95 CI) MODEL (95 CI) I2 95 CI P
Delusions 243 0557 (0462 to 0640) 0567 (0412 to 0690) 5864 000 to 8623 p = 00643Hallucinations 243 0502 (0399 to 0532) 0520 (0198 to 0791) 8771 7081 to 9482 p lt 00001AgitationAggression 243 0540 (0443 to 0625) 0537 (0299 to 0712) 7941 4517 to 9482 p = 00022Depression 243 0528 (0429 to 0615) 0564 (0360ndash0717) 7465 2949 to 9089 p = 00080Anxiety 243 0482 (0377 to 0575) 0481 (0236 to 0669) 7845 4203 to 9199 p = 00030Euphoria 243 0540 (0443 to 0625) 0480 (0147 to 0715) 8764 7061 to 9480 p lt 00001Apathy 243 0456 (0351 to 0554) 0459 (0351 to 0540) 000 000 to 8423 p = 04834Disinhibition 243 0357 (0240 to 0464) 0371 (0162 to 0548) 6574 000 to 8833 p = 00327Irritability 243 0668 (0590 to 0733) 0691 (0486 to 0823) 8281 5601 to 9329 p = 00006Aberrant motor
behavior243 0606 (0518 to 0681) 0603 (0437 to 0730) 6764 371 to 8871 p = 00280
Sleep 176 0438 (0307 to 0552) 0436 (0301 to 0554) 532 000 to 9682 p = 03478Appetite and eating 176 0405 (0271 to 0523) 0442 (0200 to 0633) 6617 000 to 9026 p = 00520
Predictive data between BPSD and well-beingConde-Sala et al (2010) Chappell and Penning(1996) Davis and Tremont (2007) and Slachevskyet al (2013) used the same burden measurebut used different measures of BPSD Apathysignificantly predicted burden across three studiesalthough it was less burdensome for adult-childcaregivers and did not predict apathy in the study byDavis and Tremont (2007) Three studies (Mouriket al 2004 Khoo et al 2013 Lee et al 2013)reported data identifying which behaviors predicteddistress as measured by the NPI Apathy wasa significant predictor across two of the threestudies Delusions and anxiety were the only othercomparable behaviors across two of the three studiesand were both significant predictors of distressCovinsky et al (2003) did not use a formal behaviorscale but identified that anger and aggressivebehaviors were stronger predictors of caregiverdepression followed by dangerous behaviors to selfand others and then behaviors which wake thecaregiver up at night
Discussion
To our knowledge this is the first review to controlfor the effect of multiple BPSD on caregiver well-being by discriminating between individual BPSDand also discriminating between caregiver outcomesof well-being Additional advantages of this reviewwere the use of a formal method of synthesis andthe decision to distinguish between how BPSD andcaregiver well-being are measured which ensuredvalid conclusions were drawn by only synthesizing
comparable data Only two meta-analyses werepossible due to limited homogeneous studiesCategories in which the relationship betweenBPSD and well-being were qualitatively examinedincluded minimal studies displaying considerablevariation therefore valid conclusions could not bedrawn The results are discussed in the context ofprevious research
Meta-analysis of mean distress scoresAs seen in Figures 2 and 3 even within one measureand one criterion (distress associated with totalscore on the NPI) variability in distress ratingsfor each symptom can be seen between the 16studies This was also evident in research conductedby Fauth and Gibbons (2014) in which a widevariation in the prevalence of NPI symptoms wasseen between studies However data regardingdistress associated with euphoria and delusionsdemonstrated high levels of variance in terms of theratio between the mean and the standard deviationresulting in considerable variability between scoresTherefore the ratio of the mean distress ratingscompared with the standard deviation associatedwith the other ten behaviors signifies that there islow variance between the 16 studies It is unclearat present why there is increased variability foreuphoric and delusional behaviors In terms of totalscore depression followed by agitationaggressionand apathy were found to be the most distressingfor caregivers across 16 studies in the meta-analysis(Figure 3) This suggests that it is mood-relatedbehaviors which are associated with increaseddistress Fauth and Gibbons (2014) examinedthe relationship between total score of BPSD
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1768 A Feast et al
and distress and found similar results howevereven with identical analysis there were noteworthydiscrepancies such as delusions being the mostdistressing but only the fourth most distressing inthe current review Consistent with the currentmeta-analysis of mean data apathy and depression-related behaviors have been reported as distressingin numerous studies (Teri 1997 deVugt et al2003 Aarsland et al 2007 Kosberg et al 2007)Similarly depression in the person with dementia isassociated with depression in the caregiver (Waiteet al 2004)
Meta-analysis of correlation dataAs seen in Table 1 there were high levels ofheterogeneity between the studies included in thesecond meta-analysis investigating which behaviorswere associated with distress Only apathy- andsleep-related behaviors displayed homogeneitybetween studies Furthermore behaviors which hadstronger correlations with distress (Table 1) didnot have strong associations in the previous meta-analysis (Figure 3) regarding distress associatedwith behaviors At present it is unclear why thisdiscrepancy exists and also why distress correlatedwith apathy- and sleep-related behaviors is more ho-mogenous between studies than the other behaviorsSince only a few studies contributed to this meta-analysis more research is needed to investigate thepooled effects Nevertheless a meta-analysis of thisnature has not been performed previously and therandom-effects model was used to report a moreconservative estimate for the heterogeneous pooledeffects in order to reduce bias
Apathy and irritable behaviors were not con-sistently significantly correlated to burden acrossmultiple studies whereas delusions agitationdisinhibition and appetiteeating change werethese associations were also reported in otherstudies (Rymer et al 2002 Rocca et al 2010) Incontrast a review by Ornstein and Gaugler (2012)reported that angeraggression and depression werethe most frequently cited BPSD associated withcaregiver burden depression was also linked tocaregiver burden in a review by Black and Almeida(2004) In addition to burden delusional behaviorwas consistently associated with distress acrossstudies with a significant correlation also beingseen with stress (Kosmala and Kloszewska 2004)Berger et al (2005) noted that behaviors whichare significantly correlated with burden are notcorrelated with depression This demonstrates theimportance of including multiple measures of well-being since the same behaviors affect caregiversdifferently which has implications for futureinterventions
Studies unamenable to quantitative synthesisOnly two studies reported the prevalence of BPSDand the impact on caregiver well-being due todifferences between studies comparisons werenot possible Although five studies reported thefrequency of BPSD each measure of caregiver well-being was different Memory-related behaviorsverbal aggression incontinence and irritabilitywere reported to affect well-being across multiplestudies These findings were also seen in previousresearch (Bruce and Paterson 2000 Farran et al2004) However Fauth and Gibbons (2014) andRobinson et al (2001) did not find that memory-related behaviors were distressing despite being themost frequent type of behavior on the RMBPCHallucinations sexual disinhibition and physicalaggression were consistently reported to affect well-being less than the other behaviors Although thisfinding is reflected in the majority of studies Haleyet al (2008) and Arango-Lasprilla et al (2010)reported contradictory results
It is noteworthy that aggressionagitation whenmeasured in terms of total score was reported asthe second most distressing across 16 of the studiesbut when measured in terms of frequency only oneof the three studies reported physical aggressionas a common problem However the frequency ofverbal aggression consistently affected well-beingIt is not possible to provide an explanation for thisdiscrepancy but it may be because of the distinctionbetween how aggressionagitation is measured (ietotal score or frequency) or that verbal and physicalaggression have been differentiated and thereforeaffect caregiver well-being differently
Predictive data were limited and heterogeneousin the present review however it was possible toconclude that apathy predicted burden and distressacross studies Anger restlessness combativenessdangerous to others and embarrassing behaviorwere found to be strong predictors of burden ina study by Gaugler et al (2011) Only one studyreported the predictors of caregiver depression
Potential explanations for variability incaregiver well-beingDifference in study quality does not appear to be anexplanation for the variation in distress rating acrossstudies since even between two medium qualitystudies there was considerable variation (Balieiroet al 2010 displaying one of the highest meandistress scores Baiyewu et al 2003 displayingone of the lowest) Two studies consistently hadthe highest mean distress rating across each of thebehavior domains Balieiro et al (2010) and Tanet al (2005) Both of these studies were clinic-basedhigher distress ratings would be expected as those
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1769
experiencing more BPSD might be more likely toattend a clinic as indeed were the majority ofstudies included in the meta-analysis It may bepossible that dementia severity is an explanationsince participants in the studies with the highestdistress scores (Tan et al 2005 Balieiro et al 2010)had moderate and severe dementia respectivelywhereas Baiyewu et al (2003) who consistentlyreported the lowest distress scores across eachof the behavior domains included participantswith mild dementia However both Aarslandet al (2007) and de Vugt et al (2006) reportedlower mean distress scores in comparison with theother included studies and they both includedparticipants with moderate dementia FurthermoreDavidsdottir et al (2012) found that there wasno significant difference between caregiver distressscores depending on dementia severity
Baiyewu et al (2003) had a much smallersample of spousal caregivers in comparison to Tanet al (2005) which might account for the lowerdistress scores This is in agreement with Almberget al (1997) who reported that spouses experiencegreater levels of burden However three studieswhich had consistently higher mean distress scoresacross all behaviors (Tan et al 2005 Balieiro et al2010 Huang et al 2012) were mainly comprisedof adult-child caregivers When comparing a studysolely comprised of spousal caregivers (deVugt et al2006) with a study (Baiyewu et al 2003) withminimal spousal caregivers (25) it was possibleto see that spousal caregivers were substantiallymore distressed with depressive apathetic andanxiety-related behaviors Although distress ratingscan be differentiated between behavior types forspousal and non-spousal caregivers both Baiyewuet al (2003) and de Vugt et al (2006) had two of thelowest distress scores across all behaviors in compar-ison to the other studies in the meta-analysis
The explanation may also be cultural sinceBaiyewu et al (2003) and Baiyewu et al (2012)(with similarly low distress scores across behaviors)were the only Africa-based studies in the meta-analysis Baiyewu et al (2003) and Baiyewu et al(2012) were also both community-based studieswhich may also be a reason for the reduceddistress ratings There is every reason to believethat BPSD are present across cultures (Shajiet al 2009) however the low levels of publicawareness of dementia have many implications(Prince 2000) One of these implications maybe the misinterpretation of BPSD as deliberateconsequently affecting the well-being of the carer(Shaji et al 2009) It is beyond the scope ofthis paper to determine why there is considerablevariation between studies reporting caregiverdistress for identical behaviors using identical
measures However it is likely that it is the caregivercharacteristics rather than the characteristics of theperson with dementia (such as dementia severity)which may underlie the explanation as to whyvariation between studies exists
Limitations
The data available for this review allowed for onlytwo meta-analyses to be conducted There wererelatively few studies which assessed the relationshipbetween individual BPSD and caregiver well-beingand which met the inclusionexclusion criteriafor the review In an attempt to be systematicbased on prior recommendation an effort wasmade to distinguish between how ldquoproblematicrdquosymptoms are measured Consequently studieswere categorized into whether BPSD weremeasured in terms of frequency or prevalence andalso categorized in terms of the statistical analysisemployed Other than data regarding mean distressassociated with NPI total score only a small amountof studies were included in each category andunfortunately it was often the case that measuresof caregiver well-being were dissimilar From the 40included studies there were 12 different measuresof behavior and 17 different measures of well-being making comparisons difficult which mayhave contributed to the inconsistent findings
The majority of included studies recruitedparticipants from clinics therefore caregiversincluded in the review were not representative ofthe population In addition the samples across theincluded studies were heterogeneous in a numberof factors therefore caution should be taken wheninterpreting the results Although beyond the scopeof this review study characteristics such as culturegender and relationship direction were not ex-amined through subgroup analyses Due to the lim-ited number of studies it was not possible to imposea quality criteria however all included studies wereeither of high or medium quality as assessed by theDowns and Back Checklist (1998) Furthermore allof the included studies relied on caregiver reportsof BPSD which may themselves be affected bycaregiver well-being unfortunately it is not possibleto determine if this was the case Nonetheless twovalid meta-analyses were completed and a numberof comments can be made about the relationshipbetween BPSD and caregiver well-being
Implications and recommendations
The vast majority of studies addressing the rela-tionship between BPSD and caregiver well-being
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1770 A Feast et al
did not examine individual BPSD Consequentlythis comparatively limited the amount of studiesincluded in the present review Therefore if we areto understand this relationship more studies needto examine individual BPSD in their research Inaddition it is more clinically relevant to examinewhich BPSD affect well-being rather than BPSDas a whole as this is essential in determiningwhere clinical staff should allocate resources mosteffectively Nevertheless there is preliminary datasuggesting it is mood-related behaviors whichare associated with increased levels of distresstherefore interventions for the management ofBPSD should target these behaviors
The lack of consistency in the measurementof BPSD (neuropsychiatric or memory problemsfrequency or prevalence) and the measurementof caregiver well-being (the use of interchangeableterminology such as stress strain and burdenmeaning the same construct) limits our ability toreach a consensus as to which BPSD result inthe most negative outcomes for caregivers Forexample Donaldson et al (1998) used GilleardrsquosStrain Scale (1984) to measure burden andthe General Health Questionnaire (Goldberg andHillier 1979) to measure distress Furthermorefour studies (see Table S1) did not have formalscales to measure the impact of BPSD on well-being and used terms such as ldquoburdensomerdquoldquoseriousrdquo and ldquodisturbingrdquo This problem impactsupon the validity and reliability of the originalstudies and consequently the review Howeverthis mainly occurred in the earlier studies Futureresearch should also include more than one measureof well-being in order to identify if individual BPSDdifferentially affect caregiver burden compared tocaregiver distress as identified in the current reviewFurthermore future research should identify whythere is reduced variability in distress ratings forcertain behaviors compared to others and whycertain behaviors are more distressing dependingon which type of statistical analysis is used
Although there are potential methodologicalreasons (limited studies inconsistent measures)for why there is substantial variability whenidentifying which BPSD affect certain types ofcaregiver well-being the most there is growingevidence that factors associated with the personwith dementia (eg BPSD frequency cognition) areonly part of the story when explaining a caregiverrsquosresponse to BPSD Caregiver characteristicshave been shown to account for twice thevariance of person with dementia characteristicswhen reporting neuropsychiatric symptoms (Sinket al 2006) and the presence of BPSD wasnot found to be a significant predictor ofburden whereas caregiver characteristics such as
confidence neuroticism and relationship qualitywere significant predictors (Campbell et al 2008)Therefore as recommended by Ornstein andGaugler (2012) future studies should focus onidentifying pathways for the association betweenindividual BPSD caregiver variables and caregiveroutcomes More research is needed to understandif and why certain BPSD affect certain caregiveroutcomes and also how much of this is attributableto caregiver variability in response to BPSD ratherthan the presence of BPSD itself More longitudinalstudies would be useful to examine how changes inindividual BPSD are associated with caregiver well-being over time A review by Black and Almeida(2004) examined the limited longitudinal studiesavailable and reported mixed findings betweenburden and BPSD and found no associationbetween BPSD and distress Although BPSDincreased significantly over a two-year periodcaregiver burden remained stable and depressionwas found to decrease (Berger et al 2005) Futureresearch needs to examine caregiver factors overtime (well-being role captivity etc) along withchanges in individual BPSD in order to have a morevalid understanding of this relationship
Caution should be exercised when creating ameasure of BPSD since Jackson et al (2014)found that the Revised Memory and BehaviorProblem Checklist (Teri et al 1992) might bemore suitable in explaining caregiver depressionthan the NPI It is important that the measureof BPSD is not biased toward explaining a moreunique association between BPSD and a measure ofcaregiver well-being such as depression As stated byGitlin and Rose (2014) item selection for measuresof BPSD is often based upon specific disciplines(eg neurology psychiatry social sciences) andthus implicitly represents different conceptual-izations of behavior A shared framework fordefining behaviors and their underlying causesmust be created in order to move on fromthe implicit assumption of most measures thatbehaviors are a direct cause of neuropathologyand to develop measures which also address thecontextual and caregiver characteristics associatedwith the behavior
Conclusions
This study has improved our understanding of theimpact of individual BPSD on caregiver well-beingin particular caregiver distress The relationshipbetween individual BPSD and caregiver well-beingwas inconsistent and varied according to behavioralsymptom Due to limited studies and heterogeneousdata the results should be interpreted with caution
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1771
but advances have been made with respect towhich behaviors are associated with distress Theinconsistencies may be partly explained by caregivervariables which were not taken into account inthe review Based on this review and previousresearch it is not possible to fully understand therelationship between BPSD and caregiver well-being without examining the influence of caregivervariables such as caregiver strategies acceptancegender relationship with person with dementiaand confidence We recommend that future studiesare designed to examine individual BPSD ratherthan BPSD as a whole use consistent measures forBPSD and well-being use consistent terminologyfor psychological constructs (eg burden) andexamine the causal mechanisms by which individualBPSD impact caregiver well-being by collectingdata on a range of caregiver factors Theseapproaches will clarify whether it is important forclinicians to focus on the frequency or prevalence ofcertain BPSD in addition to targeting the presenceof certain caregiver characteristics and addressingunmet need
Conflict of interest
None
Description of authorsrsquo roles
A Feast was responsible for developing the reviewobjectives writing the search strategies conductingthe searches designing and completing studyeligibility and data extraction forms undertakingthe quality appraisals conducting the meta-analysisand writing the paper M Orrell was responsible fordeveloping the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper C Stoner was responsible forundertaking the quality appraisals and assisting inwriting the paper G Charlesworth was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper E Moniz-Cook was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper
Acknowledgments
We would like to thank Dr Zoeuml Hoare for herstatistical advice This paper presents independentresearch funded by the National Institute for HealthResearch (NIHR) under its Programme Grants forApplied Research (RP-PG-0606-1067 and RP-PG-
060- 1083) The views expressed in this publicationare those of the author(s) and not necessarily thoseof the NHS the NIHR or the Department ofHealth
Supplementary Material
To view supplementary material for thisarticle please visit httpdxdoiorg101017S1041610216000922
References
Aarsland D et al (2007) Neuropsychiatric symptoms inpatients with Parkinsonrsquos disease and dementia frequencyprofile and associated care giver stress Journal of NeurologyNeurosurgery amp Psychiatry 78 36ndash42doihttpdxdoiorg101136jnnp2005083113
Allegri R F et al (2006) Neuropsychiatric symptoms as apredictor of caregiver burden in Alzheimerrsquos diseaseNeuropsychiatric Disease amp Treatment 2 105ndash110doi102147ndts47133
Almberg B Grafstrom M and Winblad B (1997)Major strain and coping strategies as reported by familymembers who care for aged demented relatives Journal ofAdvanced Nursing 26 683ndash691doihttpdxdoiorg101046j1365-2648199700392x
Arango-Lasprilla J C Lehan T Drew A MorenoA Deng X and Lemos M (2010) Health-relatedquality of life in caregivers of individuals with dementiafrom Colombia American Journal of Alzheimerrsquos Disease andOther Dementias 25 556ndash561doi1011771533317510382287ltbibgt
Baiyewu O et al (2003) Behavioral and caregiver reactionof dementia as measured by the neuropsychiatric inventoryin Nigerian community residents InternationalPsychogeriatrics 15 399ndash409doi101017s1041610203009645
Baiyewu O et al (2012) Behavioral symptoms incommunity-dwelling elderly Nigerians with dementia mildcognitive impairment and normal cognition InternationalJournal of Geriatric Psychiatry 27 931ndash939 doihttpdxdoiorg101002gps2804
Balieiro A P Jr Sobreira E S T Pena M C SSilva-Filho J H and Vale F A C (2010) Caregiverdistress associated with behavioral and psychologicalsymptoms in mild Alzheimerrsquos disease Dementia eNeuropsychologia 4 238ndash244
Ballard C G et al (1995) The aetiology of depression inthe carers of dementia sufferers Journal of AffectiveDisorders 35 59ndash63 doi1010160165-0327(95)00041-k
Bandeira D R Pawlowski J Goncalves T RHilgert J B Bozzetti M C and Hugo F N (2007)Psychological distress in Brazilian caregivers of relativeswith dementia Aging and Mental Health 11 14ndash19doi10108013607860600640814
Berger G Bernhardt T Weimer E Peters JKratzsch T and Frolich L (2005) Longitudinal studyon the relationship between symptomatology of dementia
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1772 A Feast et al
and levels of subjective burden and depression amongfamily caregivers in memory clinic patients Journal ofGeriatric Psychiatry and Neurology 3 119ndash128doi1011770891988704273375
Black W and Almeida O P (2004) A systematic reviewof the association between the behavioral and psychologicalsymptoms of dementia and burden of care InternationalPsychogeriatrics 16 295ndash315doi101017s1041610204000468
Bruce D G and Paterson A (2000) Barriers tocommunity support for the dementia carer a qualitativestudy International Journal of Geriatric Psychiatry 15451ndash457 doi101002(sici)1099-1166(200005)155lt451aid-gps143gt30co2-k
Campbell P et al (2008) Determinants of burden in thosewho care for someone with dementia International Journalof Geriatric Psychiatry 23 1078ndash1085doi101002gps2071
Cerejeira J Lagarto L and Mukaetova-LadinskaE B (2012) Behavioral and psychological symptoms ofdementia Frontiers in Neurology 3 1ndash23doi103389fneur201200073
Chappell N L and Penning M (1996) Behaviouralproblems and distress among caregivers of people withdementia Ageing amp Society 16 57ndash73doi101017s0144686x00003135
Chiu Y C et al (2014) Family caregiversrsquo sleepdisturbance and its associations with multilevel stressorswhen caring for patients with dementia Aging amp MentalHealth 18 92ndash101 doihttpdxdoiorg101080136078632013837141
Cohen J (1988) Statistical Power Analysis for the BehavioralSciences 2nd edn New York University New YorkLawrence Erlbaum Associatesdoi1043249780203771587
Conde-Sala J L Garre-Olmo J Turroacute-Garriga OVilalta-Franch J and Loacutepez-Pousa S (2010)Differential features of burden between spouse andadult-child caregivers of patients with Alzheimerrsquos diseasean exploratory comparative design International Journal ofNursing Studies 47 1262ndash1273doi101016jijnurstu201003001
Covinsky K E et al (2003) Patient and caregivercharacteristics associated with depression in caregivers ofpatients with dementia Journal of General Internal Medicine18 1006ndash1014 doihttpdxdoiorg101111j1525-1497200330103x
Craig D Mirakhur A Hart D J McIlroy S P andPassmore A P (2005) A cross-sectional study ofneuropsychiatric symptoms in 435 patients withAlzheimerrsquos disease American Journal of GeriatricPsychiatry 13 460ndash468 doi10109700019442-200506000-00004
Crellin N Charlesworth G and Orrell M (2014)Measuring family caregiver efficacy for managing behavioraland psychological symptoms in dementia a psychometricevaluation International Psychogeriatrics 26 93ndash103 doihttpdxdoiorg101017s1041610213001646
Davidsdottir S R Snaedal J Karlsdottir GAtladottir I and Hannesdottir K (2012) Validationof the Icelandic version of the neuropsychiatric inventorywith caregiver distress (NPI-D) Nordic Journal of
Psychiatry 66 26ndash32 doihttpdxdoiorg103109080394882011593100
Davis J D and Tremont G (2007) Impact of frontalsystems behavioral functioning in dementia on caregiverburden The Journal of Neuropsychiatry and ClinicalNeurosciences 19 43ndash49 doihttpdxdoiorg101176jnp200719143
de Vugt M E Riedijk S R Aalten P Tibben Avan Swieten J C and Verhey F R J (2006) Impactof behavioural problems on spousal caregivers acomparison between Alzheimerrsquos disease andfronto-temporal dementia Dementia and Geriatric CognitiveDisorders 22 35ndash41 doi101159000093102
de Vugt M E et al (2003) Behavioural disturbances indementia patients and quality of the marital relationshipInternational Journal of Geriatric Psychiatry 18 149ndash154doi101002gps807
Donaldson C Tarrier N and Burns A (1998)Determinants of carer stress in Alzheimerrsquos diseaseInternational Journal of Geriatric Psychiatry 13 248ndash256doi101002(sici)1099-1166(199804)134lt248aid-gps770gt30co2-0
Downs S and Black N (1998) The feasibility of creating achecklist for the assessment of the methodological qualityboth of randomised and non-randomised studies of healthcare interventions Journal of Epidemiological CommunityHealth 52 377ndash384 doi101136jech526377
Farran C J Loukissa D A Lindeman D A andMcCann J (2004) Caring for self while caring for othersthe two-track life of coping with Alzheimerrsquos diseaseJournal of Gerontological Nursing 30 38ndash45doi1039280098-9134-20040501-09
Fauth E B and Gibbons A (2014) Which behavioral andpsychological symptoms of dementia are the mostproblematic Variability by prevalence intensity distressratings and associations with carer depressive symptomsInternational Journal of Geriatric Psychiatry 29 263ndash271doi101002gps4002
Fuh J L Liu C K Mega M S Wang S J andCummings J L (2001) Behavioral disorders andcaregiversrsquo reaction in Taiwanese patients with Alzheimerrsquosdisease International Psychogeriatrics 13 121ndash128 doihttpdxdoiorg101017s1041610201007517
Gaugler J E et al (2011) Does caregiver burden mediatethe effects of behavioral disturbances on nursing homeadmission The American Journal of Geriatric Psychiatry 19497ndash506 doi101097jgp0b013e31820d92cc
Gilleard C J Belford H Gilleard E Whittick J Eand Gledhill K (1984) Emotional distress amongst thesupporters of the elderly mental infirm British Journal ofPsychiatry 145 172ndash177doihttpdxdoiorg101192bjp1452172
Gitlin L N and Rose K (2014) Factors associated withcarer readiness to use nonpharmacologic strategies tomanage dementia-related behavioral symptomsInternational Journal of Geriatric Psychiatry 29 93ndash102doihttpdxdoiorg101002gps3979
Goldberg D P and Hillier V F (1979) A scaled versionof the general health questionnaire Psychological Medicine9 139ndash145 doi101017s0033291700021644
Gonzalez-Salvador M T Arango C Lyketsos C Gand Barba A C (1999) The stress and psychological
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1773
morbidity of the Alzheimer patient caregiver InternationalJournal of Geriatric Psychiatry 14 701ndash710doi101002(sici)1099-1166(199909)149lt701aidps5gt30co2-
Haley W E Brown S and Levine E G (1987) Familycaregiver appraisals of patient behavioral disturbance insenile dementia Clinical Gerontologist The Journal of Agingand Mental Health 6 25ndash34doi101300j018v06n04_04
Haley W E Levine E G Brown S L Berry J Wand Hughes G H (2008) The psychological social andhealth consequences of caring for a relative with seniledementia Journal of the American Geriatrics Society 35405ndash411 doi101111j1532-54151987tb04661x
Hishikawa N et al (2012) Effects of turmeric onAlzheimerrsquos disease with behavioral and psychologicalsymptoms of dementia Ayu 33 499ndash504 doihttpdxdoiorg1041030974-8520110524
Huang S S Lee M C Liao Y C Wang W F andLai T J (2012) Caregiver burden associated withbehavioral and psychological symptoms of dementia(BPSD) in Taiwanese elderly Archives of Gerontology andGeriatrics 55 55ndash59 doihttpdxdoiorg101016jarchger201104009
Jackson M A Fauth E B and Geiser C (2014)Comparing the neuropsychiatric inventory and the revisedmemory and behavior problems checklist for associationswith caregiver burden and depressive symptomsInternational Psychogeriatrics 26 1021ndash1031doi101017s1041610213002421
Johnson D K Niedens M Wilson J RSwartzendruber L Yeager A and Jones K (2013)Treatment outcomes of a crisis intervention program fordementia with severe psychiatric complications the Kansasbridge project The Gerontologist 53 102ndash112 doihttpdxdoiorg101093gerontgns104
Khoo S A Chen T Y Ang Y H and Yap P (2013)The impact of neuropsychiatric symptoms on caregiverdistress and quality of life in persons with dementia in anAsian tertiary hospital memory clinic InternationalPsychogeriatrics 25 1991ndash1999 doihttpdxdoiorg101017s1041610213001518
Kosberg J I Kaufman A V Burgio L D Leeper Jand Sun F (2007) Family caregiving to those withdementia in rural Alabama racial similarities anddifferences Journal of Aging and Health 19 3ndash21 doi1011770898264306293604
Kosmala K and Kloszewska I (2004) The burden ofproviding care for Alzheimerrsquos disease patients in PolandInternational Journal of Geriatric Psychiatry 19 191ndash193doi101002gps1054
Landis J R and Koch G G (1977) The measurement ofobserver agreement for categorical data Biometrics 33159ndash174 doi 1023072529310
Lee D R McKeith I Mosimann U Ghosh-NodyalA and Thomas A J (2013) Examining carer stress indementia the role of subtype diagnosis andneuropsychiatric symptoms International Journal ofGeriatric Psychiatry 28 135ndash141 doihttpdxdoiorg101002gps3799
Lim Y M Son G R Song J A and Beattie E(2008) Factors affecting burden of family caregivers of
community-dwelling ambulatory elders with dementia inKorea Archives of Psychiatric Nursing 22 226ndash234 doi101016japnu200712005
Matsumoto N et al (2007) Caregiver burden associatedwith behavioral and psychological symptoms of dementia inelderly people in the local community Dementia andGeriatric Cognitive Disorders 23 219ndash224doi101159000099472
Mohamed S Rosenheck R Lyketsos C G andSchneider L S (2010) Caregiver burden in Alzheimerdisease cross-sectional and longitudinal patient correlatesThe American Journal of Geriatric Psychiatry 18 917ndash927doi101097jgp0b013e3181d5745d
Mourik J C Rosso S M Niermeijer M FDuivenvoorden H J Van Swieten J C and TibbenA (2004) Frontotemporal dementia behavioral symptomsand caregiver distress Dementia and Geriatric CognitiveDisorders 18 299ndash306 doihttpdxdoiorg101159000080123
Muangpaisan W et al (2010) Caregiver burden and needsof dementia caregivers in Thailand a cross-sectional studyJournal of the Medical Association of Thailand 93 601ndash607
Neundorfer M M McClendon M J Smyth K AStuckey J C Strauss M E and Patterson M B(2001) A longitudinal study of the relationship betweenlevels of depression among persons with Alzheimerrsquosdisease and levels of depression among their familycaregivers Journal of Gerontology Series B - PsychologicalSciences and Social Sciences 56 301ndash313
Nygaard H A (1998) Strain on caregivers of dementedelderly people living at home Scandinavian Journal ofPrimary Health Care 6 33ndash37doihttpdxdoiorg10310902813438809009287
Ornstein K and Gaugler J E (2012) The problem withldquoproblem behaviorsrdquoa systematic review of the associationbetween individual patient behavioral and psychologicalsymptoms and caregiver depression and burden within thedementia patientndashcaregiver dyad InternationalPsychogeriatrics 24 1536ndash1552doi101017s1041610212000737
Ornstein K Gaugler J E Devanand N S CarolynZ and Yaakov S (2012) The differential impact ofunique behavioral and psychological symptoms for thedementia caregiver how and why do patientsrsquo individualsymptom clusters impact caregiver depressive symptomsThe American Journal of Geriatric Psychiatry 12 77ndash1286doi httpdxdoiorg101016jjagp201301062
Price G R (1970) Selection and covariance Nature 227520ndash521 doi101038227520a0
Prince M (2000) Dementia in developing countries Aconsensus statement from the 1066 Dementia ResearchGroup International Journal of Geriatric Psychiatry 1514ndash20 doihttpdxdoiorg101002(sici)1099-1166(200001)151lt14aid-gps70gt30co2-8
Quayhagen M P and Quayhagen M (1998) Alzheimerrsquosstress coping with the caregiving role Gerontologist 28391ndash396 doihttpdxdoiorg101093geront283391
Reisberg B Ferris S H de Leon M J and Crook T(1982) The global deterioration scale for assessment ofprimary degenerative dementia American Journal ofPsychiatry 139 1136ndash1139 doihttpdxdoiorg101176ajp13991136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1774 A Feast et al
Robinson K M Adkisson P and Weinrich S (2001)Problem behaviour caregiver reactions and impact amongcaregivers of persons with Alzheimerrsquos disease Journal ofAdvanced Nursing 36 573ndash582 doihttpdxdoiorg101046j1365-2648200102010x
Rocca P et al (2010) Neuropsychiatric symptomsunderlying caregiver stress and insight in Alzheimerrsquosdisease Dementia and Geriatric Cognitive Disorders 3057ndash63 doi101159000315513
Rymer S Salloway S Norton L Mallow PCorreia S and Monast D (2002) Impaired awarenessbehavior disturbance and caregiver burden in Alzheimerdisease Alzheimer Disease and Associated Disorders 16248ndash253 doi 10109700002093-200210000-00006
Savorani G Vulcano V Boni S Sarti G andRavaglia G (1998) Behavioral disorders in dementiapatients and their impact on the stress of caregivingrelatives the ldquoARADrdquo questionnaire Archives ofGerontology and Geriatrics 6 481ndash485doi101016s0167-4943(98)80070-8
Shaji K S George R K Prince M J and JacobK S (2009) Behavioral symptoms and caregiver burdenin dementia Indian Journal of Psychiatry 51 45 doihttpdxdoiorg1041030019-554544905
Sink K M Covinsky K E Barnes D E NewcomerR J and Yaffe K (2006) Caregiver characteristics areassociated with neuropsychiatric symptoms of dementiaJournal of the American Geriatrics Society 54 796ndash803 doi101111j1532-5415200600697x
Slachevsky A et al (2013) The CUIDEME studydeterminants of burden in chilean primary caregivers ofpatients with dementia Journal of Alzheimerrsquos Disease 35297ndash306
Spiegel R et al (1991) A new behavioral assessment scalefor geriatric out- and in-patients the NOSGER (nursesrsquoobservation scale for geriatric patients) Journal of theAmerican Geriatric Society 39 339ndash347 doihttpdxdoiorg101111j1532-54151991tb02897x
Tan L L Wong H B and Allen H (2005) The impactof neuropsychiatric symptoms of dementia on distress infamily and professional caregivers in SingaporeInternational Psychogeriatrics 17 253ndash263 doi101017s1041610205001523
Teri L (1997) Behavior and caregiver burden behavioralproblems in patients with Alzheimer disease and itsassociation with caregiver distress Alzheimer Disease andAssociated Disorders 11 35ndash38
Teri L Truax P Logsdon R Uomoto J Zarit Sand Vitaliano P P (1992) Assessment of behavioralproblems in dementia the revised memory and behaviorproblems checklist Psychology and Aging 7 622 doi1010370882-797474622
Waite A Bebbington P Skelton-Robinson M andOrrell M (2004) Social factors and depression in carersof people with dementia International Journal of GeriatricPsychiatry 19 582ndash587 doihttpdxdoiorg101002gps1136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at

1764 A Feast et al
validity and reliability of outcome measures and thereporting of statistics
Meta-analysis of comparable studiesSixteen of the 40 studies were suitable to beincluded in a meta-analysis of mean distress scores(see Table S2 available as supplementary materialattached to the electronic version of this paper atwwwjournalscambridgeorgjid_IPG) All of thesestudies reported data on the mean and standarddeviation of distress associated with the meantotal score on the NPI for individual behaviorsEach adapted version of the NPI was reportedas valid and reliable and all were administeredby a researcher or clinician Five studies utilizedthe ten-item version of the NPI thereforedata reporting distress associated with sleep andappetiteeating change were unavailable for thesestudies Participants were recruited from clinic-based and population-based studies had a mix ofdementia participants and studies only includingthose with a diagnosis of Alzheimerrsquos diseaseParkinsonrsquos disease dementia and frontotemporaldementia (see Table S1 available as supplementarymaterial attached to the electronic version of thispaper at wwwjournalscambridgeorgjid_IPG) InTable S3 (available as supplementary materialattached to the electronic version of this paperat wwwjournalscambridgeorgjid_IPG) the meandistress reported for the total NPI symptom canbe seen for each of the 16 studies along with thepooled standard deviations for each behavior acrossthe studies There is considerable variation betweenthe studies for each of the symptoms this can beseen in Figure 2 in particular there is substantialvariation in the mean distress reported for the totalscore of irritable behavior Baiyewu et al (2003)reported 06 (between ldquonot at all distressingrdquo andldquominimally distressingrdquo) and Balieiro et al (2010)reported 36 (between ldquomoderatelyrdquo and ldquoseverelyrdquodistressing) However it is possible to concludethat euphoria was the least distressing across thestudies
As seen in Figure 3 the most distressingBPSD across the 16 studies was depressionAgitationaggression was the second most distress-ing followed by apathy Euphoria was the leastdistressing and had the smallest standard errorDelusional and euphoric behaviors were the onlytwo behaviors with a standard deviation exceedingthe mean indicating high variance between studiesfor these behaviors
Four studies reported correlation data betweenmean NPI total scores and mean NPI distress(Matsumoto et al 2007 Balieiro et al 2010Davidsdottir et al 2012 Huang et al 2012)
all of these studies were involved in the previousmeta-analysis other than Davidsdottir et al (2012)Three of these studies reported data on all 12behaviors The sample size and the correlationcoefficients were entered into MedCalc in order toproduce a pooled effect size for each behavior Thepooled effect sizes within the fixed-effect modelrandom-effects model and heterogeneity statisticsare reported in Table 1 Significant heterogeneitywas identified between studies for all behaviorsother than apathy and sleep In contrast tothe mean distress data the meta-analysis of thecorrelation data identified that irritable behaviorwas the most strongly associated with caregiverdistress followed by aberrant motor behavior andthen delusions Disinhibition had the weakestassociation with distress Depression was seento be one of the behaviors which was morestrongly associatedcorrelated with distress acrossboth meta-analyses Appetite and eating-relatedbehavior was one of the behaviors which had aweaker associationcorrelation with distress acrossboth meta-analyses
Non-comparable studiesTwenty of the 40 included studies were notsuitable for meta-analysis These studies werenot comparable in terms of BPSD measure andthe associated unit of measurement caregiverwell-being measure and the associated unit ofmeasurement It was therefore only possible tocompare these 20 studies descriptively due to theirheterogeneity
Prevalence of BPSD and the impact oncaregiver well-beingMean prevalence and mean distress were reportedon the NPI by Haley et al (2008) and deVugt et al (2006) Although these two studiesboth measure prevalence of BPSD methodsfor measuring caregiver well-being differed (seeTable S1)
Frequency of BPSD and caregiver well-beingMemory-related behaviors were reported as moststressful and problematic across three studies(Nygaard 1998 Quayhagen and Quayhagen 1998Muangpaisan et al 2010) However Robinsonet al (2001) and Fauth and Gibbons (2014) bothfound the frequency of memory-related behaviorswas associated with the least amount of reactivityDisruptive behaviors were associated with themost reactivity followed by depressive behaviors(Robinson et al 2001 Fauth and Gibbons2014) In all of the studies which measuredhallucinations caregivers reported this behavior
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1765
005
115
225
335
445
Mea
n di
stre
ss
Delusions Hallucinations AgitationAggression Depression
005
115
225
335
Mea
n di
stre
ss
Anxiety Euphoria Apathy Disinhibition
0
05
1
15
2
25
3
35
4
Mea
n di
stre
ss
Irritability Aberrant motor behaviour Sleep Appettite and eating
Figure 2 Mean distress scores across 16 studies for behaviors on the NPI (total score)
as less problematic burdensome and distressingcompared to many of the other behaviors Verbalaggression across three of the five studies wasreported as problematic and burdensome Acrosstwo of the five studies which reported sexualdisinhibition this behavior was reported as theleast problematic Reports of wandering acrossfour of the studies were not consistent since
some of the studies reported this behavior asmuch more problematic and burdensome thanothers
Across four of the five studies which reportedincontinence this was consistently reported as oneof the more burdensome stressful and problematicbehaviors Physical aggression was only measuredin three studies and only one study reported this
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1766 A Feast et al
Figure 3 Meta-analysis of mean distress for each BPSD associated with NPI total score
behavior as a common problem Both studies whichreported irritability identified this behavior to be oneof the most problematic and burdensome
Correlational data between BPSD andcaregiver well-beingSleeping- and eating-related behaviors were foundto be significantly correlated to burden and strainhowever they had a stronger association withburden (Donaldson et al 1998) With regard toadult-child caregivers four (delusions agitationdisinhibition and appetiteeating change) of theeight behaviors reported by Conde-Sala et al (2010)as being significantly associated with burden werealso found to be significantly associated with burdenby Allegri et al (2006) Apathy and irritabilitywere reported to be significantly associated withburden in the study conducted by Conde-Sala et al(2010) but no significant relationship was reportedby Allegri et al (2006) Spousal caregivers onlyfound appetiteeating change burdensome (Conde-Sala et al 2010) Apathy had a moderate significantassociation with burden in spousal and adult-child caregivers (Conde-Sala et al 2010) but thisassociation was non-significant in the data reported
by Allegri et al (2006) Delusional and irritablebehaviors were also reported as non-significantlyrelated to burden (Allegri et al 2006) but weresignificantly related to burden by Conde-Sala et al(2010) In contrast to the previous studies reportingthe weak association between euphoria and distressFuh et al (2001) reported a significant correlationbetween euphoria and burden No other behaviorson the NPI had a significant correlation with burden(Fuh et al 2001)
In agreement with the data concerning atthe association between the frequency of thebehavior within each subscale on the RMBPCand reactivity disruptive behaviors had the largestcorrelation of the three subscales with burden(Huang et al 2012) Using the BEHAVE-AD (Reisberg et al 1982) and the NOSGER(Spiegel et al 1991) mood social behaviorsand disturbing behaviors were found to havea significant moderate association with burdenbut no significant correlations with depression incaregivers Chiu et al (2014) noted that all of thebehaviors on the NPI significantly predicted sleepdisturbance in caregivers other than anxiety andaberrant motor behavior
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1767
Table 1 Meta-analysis of mean distress scores correlated with behaviors using NPI total scores
P O O L E D C O R RELATION COEFFI CIENT T EST F OR HETEROGENEITY
FI XE D-E FF E C T S RANDOM-E FF E C T S
BEHAVIOR N MODEL (95 CI) MODEL (95 CI) I2 95 CI P
Delusions 243 0557 (0462 to 0640) 0567 (0412 to 0690) 5864 000 to 8623 p = 00643Hallucinations 243 0502 (0399 to 0532) 0520 (0198 to 0791) 8771 7081 to 9482 p lt 00001AgitationAggression 243 0540 (0443 to 0625) 0537 (0299 to 0712) 7941 4517 to 9482 p = 00022Depression 243 0528 (0429 to 0615) 0564 (0360ndash0717) 7465 2949 to 9089 p = 00080Anxiety 243 0482 (0377 to 0575) 0481 (0236 to 0669) 7845 4203 to 9199 p = 00030Euphoria 243 0540 (0443 to 0625) 0480 (0147 to 0715) 8764 7061 to 9480 p lt 00001Apathy 243 0456 (0351 to 0554) 0459 (0351 to 0540) 000 000 to 8423 p = 04834Disinhibition 243 0357 (0240 to 0464) 0371 (0162 to 0548) 6574 000 to 8833 p = 00327Irritability 243 0668 (0590 to 0733) 0691 (0486 to 0823) 8281 5601 to 9329 p = 00006Aberrant motor
behavior243 0606 (0518 to 0681) 0603 (0437 to 0730) 6764 371 to 8871 p = 00280
Sleep 176 0438 (0307 to 0552) 0436 (0301 to 0554) 532 000 to 9682 p = 03478Appetite and eating 176 0405 (0271 to 0523) 0442 (0200 to 0633) 6617 000 to 9026 p = 00520
Predictive data between BPSD and well-beingConde-Sala et al (2010) Chappell and Penning(1996) Davis and Tremont (2007) and Slachevskyet al (2013) used the same burden measurebut used different measures of BPSD Apathysignificantly predicted burden across three studiesalthough it was less burdensome for adult-childcaregivers and did not predict apathy in the study byDavis and Tremont (2007) Three studies (Mouriket al 2004 Khoo et al 2013 Lee et al 2013)reported data identifying which behaviors predicteddistress as measured by the NPI Apathy wasa significant predictor across two of the threestudies Delusions and anxiety were the only othercomparable behaviors across two of the three studiesand were both significant predictors of distressCovinsky et al (2003) did not use a formal behaviorscale but identified that anger and aggressivebehaviors were stronger predictors of caregiverdepression followed by dangerous behaviors to selfand others and then behaviors which wake thecaregiver up at night
Discussion
To our knowledge this is the first review to controlfor the effect of multiple BPSD on caregiver well-being by discriminating between individual BPSDand also discriminating between caregiver outcomesof well-being Additional advantages of this reviewwere the use of a formal method of synthesis andthe decision to distinguish between how BPSD andcaregiver well-being are measured which ensuredvalid conclusions were drawn by only synthesizing
comparable data Only two meta-analyses werepossible due to limited homogeneous studiesCategories in which the relationship betweenBPSD and well-being were qualitatively examinedincluded minimal studies displaying considerablevariation therefore valid conclusions could not bedrawn The results are discussed in the context ofprevious research
Meta-analysis of mean distress scoresAs seen in Figures 2 and 3 even within one measureand one criterion (distress associated with totalscore on the NPI) variability in distress ratingsfor each symptom can be seen between the 16studies This was also evident in research conductedby Fauth and Gibbons (2014) in which a widevariation in the prevalence of NPI symptoms wasseen between studies However data regardingdistress associated with euphoria and delusionsdemonstrated high levels of variance in terms of theratio between the mean and the standard deviationresulting in considerable variability between scoresTherefore the ratio of the mean distress ratingscompared with the standard deviation associatedwith the other ten behaviors signifies that there islow variance between the 16 studies It is unclearat present why there is increased variability foreuphoric and delusional behaviors In terms of totalscore depression followed by agitationaggressionand apathy were found to be the most distressingfor caregivers across 16 studies in the meta-analysis(Figure 3) This suggests that it is mood-relatedbehaviors which are associated with increaseddistress Fauth and Gibbons (2014) examinedthe relationship between total score of BPSD
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1768 A Feast et al
and distress and found similar results howevereven with identical analysis there were noteworthydiscrepancies such as delusions being the mostdistressing but only the fourth most distressing inthe current review Consistent with the currentmeta-analysis of mean data apathy and depression-related behaviors have been reported as distressingin numerous studies (Teri 1997 deVugt et al2003 Aarsland et al 2007 Kosberg et al 2007)Similarly depression in the person with dementia isassociated with depression in the caregiver (Waiteet al 2004)
Meta-analysis of correlation dataAs seen in Table 1 there were high levels ofheterogeneity between the studies included in thesecond meta-analysis investigating which behaviorswere associated with distress Only apathy- andsleep-related behaviors displayed homogeneitybetween studies Furthermore behaviors which hadstronger correlations with distress (Table 1) didnot have strong associations in the previous meta-analysis (Figure 3) regarding distress associatedwith behaviors At present it is unclear why thisdiscrepancy exists and also why distress correlatedwith apathy- and sleep-related behaviors is more ho-mogenous between studies than the other behaviorsSince only a few studies contributed to this meta-analysis more research is needed to investigate thepooled effects Nevertheless a meta-analysis of thisnature has not been performed previously and therandom-effects model was used to report a moreconservative estimate for the heterogeneous pooledeffects in order to reduce bias
Apathy and irritable behaviors were not con-sistently significantly correlated to burden acrossmultiple studies whereas delusions agitationdisinhibition and appetiteeating change werethese associations were also reported in otherstudies (Rymer et al 2002 Rocca et al 2010) Incontrast a review by Ornstein and Gaugler (2012)reported that angeraggression and depression werethe most frequently cited BPSD associated withcaregiver burden depression was also linked tocaregiver burden in a review by Black and Almeida(2004) In addition to burden delusional behaviorwas consistently associated with distress acrossstudies with a significant correlation also beingseen with stress (Kosmala and Kloszewska 2004)Berger et al (2005) noted that behaviors whichare significantly correlated with burden are notcorrelated with depression This demonstrates theimportance of including multiple measures of well-being since the same behaviors affect caregiversdifferently which has implications for futureinterventions
Studies unamenable to quantitative synthesisOnly two studies reported the prevalence of BPSDand the impact on caregiver well-being due todifferences between studies comparisons werenot possible Although five studies reported thefrequency of BPSD each measure of caregiver well-being was different Memory-related behaviorsverbal aggression incontinence and irritabilitywere reported to affect well-being across multiplestudies These findings were also seen in previousresearch (Bruce and Paterson 2000 Farran et al2004) However Fauth and Gibbons (2014) andRobinson et al (2001) did not find that memory-related behaviors were distressing despite being themost frequent type of behavior on the RMBPCHallucinations sexual disinhibition and physicalaggression were consistently reported to affect well-being less than the other behaviors Although thisfinding is reflected in the majority of studies Haleyet al (2008) and Arango-Lasprilla et al (2010)reported contradictory results
It is noteworthy that aggressionagitation whenmeasured in terms of total score was reported asthe second most distressing across 16 of the studiesbut when measured in terms of frequency only oneof the three studies reported physical aggressionas a common problem However the frequency ofverbal aggression consistently affected well-beingIt is not possible to provide an explanation for thisdiscrepancy but it may be because of the distinctionbetween how aggressionagitation is measured (ietotal score or frequency) or that verbal and physicalaggression have been differentiated and thereforeaffect caregiver well-being differently
Predictive data were limited and heterogeneousin the present review however it was possible toconclude that apathy predicted burden and distressacross studies Anger restlessness combativenessdangerous to others and embarrassing behaviorwere found to be strong predictors of burden ina study by Gaugler et al (2011) Only one studyreported the predictors of caregiver depression
Potential explanations for variability incaregiver well-beingDifference in study quality does not appear to be anexplanation for the variation in distress rating acrossstudies since even between two medium qualitystudies there was considerable variation (Balieiroet al 2010 displaying one of the highest meandistress scores Baiyewu et al 2003 displayingone of the lowest) Two studies consistently hadthe highest mean distress rating across each of thebehavior domains Balieiro et al (2010) and Tanet al (2005) Both of these studies were clinic-basedhigher distress ratings would be expected as those
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1769
experiencing more BPSD might be more likely toattend a clinic as indeed were the majority ofstudies included in the meta-analysis It may bepossible that dementia severity is an explanationsince participants in the studies with the highestdistress scores (Tan et al 2005 Balieiro et al 2010)had moderate and severe dementia respectivelywhereas Baiyewu et al (2003) who consistentlyreported the lowest distress scores across eachof the behavior domains included participantswith mild dementia However both Aarslandet al (2007) and de Vugt et al (2006) reportedlower mean distress scores in comparison with theother included studies and they both includedparticipants with moderate dementia FurthermoreDavidsdottir et al (2012) found that there wasno significant difference between caregiver distressscores depending on dementia severity
Baiyewu et al (2003) had a much smallersample of spousal caregivers in comparison to Tanet al (2005) which might account for the lowerdistress scores This is in agreement with Almberget al (1997) who reported that spouses experiencegreater levels of burden However three studieswhich had consistently higher mean distress scoresacross all behaviors (Tan et al 2005 Balieiro et al2010 Huang et al 2012) were mainly comprisedof adult-child caregivers When comparing a studysolely comprised of spousal caregivers (deVugt et al2006) with a study (Baiyewu et al 2003) withminimal spousal caregivers (25) it was possibleto see that spousal caregivers were substantiallymore distressed with depressive apathetic andanxiety-related behaviors Although distress ratingscan be differentiated between behavior types forspousal and non-spousal caregivers both Baiyewuet al (2003) and de Vugt et al (2006) had two of thelowest distress scores across all behaviors in compar-ison to the other studies in the meta-analysis
The explanation may also be cultural sinceBaiyewu et al (2003) and Baiyewu et al (2012)(with similarly low distress scores across behaviors)were the only Africa-based studies in the meta-analysis Baiyewu et al (2003) and Baiyewu et al(2012) were also both community-based studieswhich may also be a reason for the reduceddistress ratings There is every reason to believethat BPSD are present across cultures (Shajiet al 2009) however the low levels of publicawareness of dementia have many implications(Prince 2000) One of these implications maybe the misinterpretation of BPSD as deliberateconsequently affecting the well-being of the carer(Shaji et al 2009) It is beyond the scope ofthis paper to determine why there is considerablevariation between studies reporting caregiverdistress for identical behaviors using identical
measures However it is likely that it is the caregivercharacteristics rather than the characteristics of theperson with dementia (such as dementia severity)which may underlie the explanation as to whyvariation between studies exists
Limitations
The data available for this review allowed for onlytwo meta-analyses to be conducted There wererelatively few studies which assessed the relationshipbetween individual BPSD and caregiver well-beingand which met the inclusionexclusion criteriafor the review In an attempt to be systematicbased on prior recommendation an effort wasmade to distinguish between how ldquoproblematicrdquosymptoms are measured Consequently studieswere categorized into whether BPSD weremeasured in terms of frequency or prevalence andalso categorized in terms of the statistical analysisemployed Other than data regarding mean distressassociated with NPI total score only a small amountof studies were included in each category andunfortunately it was often the case that measuresof caregiver well-being were dissimilar From the 40included studies there were 12 different measuresof behavior and 17 different measures of well-being making comparisons difficult which mayhave contributed to the inconsistent findings
The majority of included studies recruitedparticipants from clinics therefore caregiversincluded in the review were not representative ofthe population In addition the samples across theincluded studies were heterogeneous in a numberof factors therefore caution should be taken wheninterpreting the results Although beyond the scopeof this review study characteristics such as culturegender and relationship direction were not ex-amined through subgroup analyses Due to the lim-ited number of studies it was not possible to imposea quality criteria however all included studies wereeither of high or medium quality as assessed by theDowns and Back Checklist (1998) Furthermore allof the included studies relied on caregiver reportsof BPSD which may themselves be affected bycaregiver well-being unfortunately it is not possibleto determine if this was the case Nonetheless twovalid meta-analyses were completed and a numberof comments can be made about the relationshipbetween BPSD and caregiver well-being
Implications and recommendations
The vast majority of studies addressing the rela-tionship between BPSD and caregiver well-being
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1770 A Feast et al
did not examine individual BPSD Consequentlythis comparatively limited the amount of studiesincluded in the present review Therefore if we areto understand this relationship more studies needto examine individual BPSD in their research Inaddition it is more clinically relevant to examinewhich BPSD affect well-being rather than BPSDas a whole as this is essential in determiningwhere clinical staff should allocate resources mosteffectively Nevertheless there is preliminary datasuggesting it is mood-related behaviors whichare associated with increased levels of distresstherefore interventions for the management ofBPSD should target these behaviors
The lack of consistency in the measurementof BPSD (neuropsychiatric or memory problemsfrequency or prevalence) and the measurementof caregiver well-being (the use of interchangeableterminology such as stress strain and burdenmeaning the same construct) limits our ability toreach a consensus as to which BPSD result inthe most negative outcomes for caregivers Forexample Donaldson et al (1998) used GilleardrsquosStrain Scale (1984) to measure burden andthe General Health Questionnaire (Goldberg andHillier 1979) to measure distress Furthermorefour studies (see Table S1) did not have formalscales to measure the impact of BPSD on well-being and used terms such as ldquoburdensomerdquoldquoseriousrdquo and ldquodisturbingrdquo This problem impactsupon the validity and reliability of the originalstudies and consequently the review Howeverthis mainly occurred in the earlier studies Futureresearch should also include more than one measureof well-being in order to identify if individual BPSDdifferentially affect caregiver burden compared tocaregiver distress as identified in the current reviewFurthermore future research should identify whythere is reduced variability in distress ratings forcertain behaviors compared to others and whycertain behaviors are more distressing dependingon which type of statistical analysis is used
Although there are potential methodologicalreasons (limited studies inconsistent measures)for why there is substantial variability whenidentifying which BPSD affect certain types ofcaregiver well-being the most there is growingevidence that factors associated with the personwith dementia (eg BPSD frequency cognition) areonly part of the story when explaining a caregiverrsquosresponse to BPSD Caregiver characteristicshave been shown to account for twice thevariance of person with dementia characteristicswhen reporting neuropsychiatric symptoms (Sinket al 2006) and the presence of BPSD wasnot found to be a significant predictor ofburden whereas caregiver characteristics such as
confidence neuroticism and relationship qualitywere significant predictors (Campbell et al 2008)Therefore as recommended by Ornstein andGaugler (2012) future studies should focus onidentifying pathways for the association betweenindividual BPSD caregiver variables and caregiveroutcomes More research is needed to understandif and why certain BPSD affect certain caregiveroutcomes and also how much of this is attributableto caregiver variability in response to BPSD ratherthan the presence of BPSD itself More longitudinalstudies would be useful to examine how changes inindividual BPSD are associated with caregiver well-being over time A review by Black and Almeida(2004) examined the limited longitudinal studiesavailable and reported mixed findings betweenburden and BPSD and found no associationbetween BPSD and distress Although BPSDincreased significantly over a two-year periodcaregiver burden remained stable and depressionwas found to decrease (Berger et al 2005) Futureresearch needs to examine caregiver factors overtime (well-being role captivity etc) along withchanges in individual BPSD in order to have a morevalid understanding of this relationship
Caution should be exercised when creating ameasure of BPSD since Jackson et al (2014)found that the Revised Memory and BehaviorProblem Checklist (Teri et al 1992) might bemore suitable in explaining caregiver depressionthan the NPI It is important that the measureof BPSD is not biased toward explaining a moreunique association between BPSD and a measure ofcaregiver well-being such as depression As stated byGitlin and Rose (2014) item selection for measuresof BPSD is often based upon specific disciplines(eg neurology psychiatry social sciences) andthus implicitly represents different conceptual-izations of behavior A shared framework fordefining behaviors and their underlying causesmust be created in order to move on fromthe implicit assumption of most measures thatbehaviors are a direct cause of neuropathologyand to develop measures which also address thecontextual and caregiver characteristics associatedwith the behavior
Conclusions
This study has improved our understanding of theimpact of individual BPSD on caregiver well-beingin particular caregiver distress The relationshipbetween individual BPSD and caregiver well-beingwas inconsistent and varied according to behavioralsymptom Due to limited studies and heterogeneousdata the results should be interpreted with caution
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1771
but advances have been made with respect towhich behaviors are associated with distress Theinconsistencies may be partly explained by caregivervariables which were not taken into account inthe review Based on this review and previousresearch it is not possible to fully understand therelationship between BPSD and caregiver well-being without examining the influence of caregivervariables such as caregiver strategies acceptancegender relationship with person with dementiaand confidence We recommend that future studiesare designed to examine individual BPSD ratherthan BPSD as a whole use consistent measures forBPSD and well-being use consistent terminologyfor psychological constructs (eg burden) andexamine the causal mechanisms by which individualBPSD impact caregiver well-being by collectingdata on a range of caregiver factors Theseapproaches will clarify whether it is important forclinicians to focus on the frequency or prevalence ofcertain BPSD in addition to targeting the presenceof certain caregiver characteristics and addressingunmet need
Conflict of interest
None
Description of authorsrsquo roles
A Feast was responsible for developing the reviewobjectives writing the search strategies conductingthe searches designing and completing studyeligibility and data extraction forms undertakingthe quality appraisals conducting the meta-analysisand writing the paper M Orrell was responsible fordeveloping the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper C Stoner was responsible forundertaking the quality appraisals and assisting inwriting the paper G Charlesworth was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper E Moniz-Cook was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper
Acknowledgments
We would like to thank Dr Zoeuml Hoare for herstatistical advice This paper presents independentresearch funded by the National Institute for HealthResearch (NIHR) under its Programme Grants forApplied Research (RP-PG-0606-1067 and RP-PG-
060- 1083) The views expressed in this publicationare those of the author(s) and not necessarily thoseof the NHS the NIHR or the Department ofHealth
Supplementary Material
To view supplementary material for thisarticle please visit httpdxdoiorg101017S1041610216000922
References
Aarsland D et al (2007) Neuropsychiatric symptoms inpatients with Parkinsonrsquos disease and dementia frequencyprofile and associated care giver stress Journal of NeurologyNeurosurgery amp Psychiatry 78 36ndash42doihttpdxdoiorg101136jnnp2005083113
Allegri R F et al (2006) Neuropsychiatric symptoms as apredictor of caregiver burden in Alzheimerrsquos diseaseNeuropsychiatric Disease amp Treatment 2 105ndash110doi102147ndts47133
Almberg B Grafstrom M and Winblad B (1997)Major strain and coping strategies as reported by familymembers who care for aged demented relatives Journal ofAdvanced Nursing 26 683ndash691doihttpdxdoiorg101046j1365-2648199700392x
Arango-Lasprilla J C Lehan T Drew A MorenoA Deng X and Lemos M (2010) Health-relatedquality of life in caregivers of individuals with dementiafrom Colombia American Journal of Alzheimerrsquos Disease andOther Dementias 25 556ndash561doi1011771533317510382287ltbibgt
Baiyewu O et al (2003) Behavioral and caregiver reactionof dementia as measured by the neuropsychiatric inventoryin Nigerian community residents InternationalPsychogeriatrics 15 399ndash409doi101017s1041610203009645
Baiyewu O et al (2012) Behavioral symptoms incommunity-dwelling elderly Nigerians with dementia mildcognitive impairment and normal cognition InternationalJournal of Geriatric Psychiatry 27 931ndash939 doihttpdxdoiorg101002gps2804
Balieiro A P Jr Sobreira E S T Pena M C SSilva-Filho J H and Vale F A C (2010) Caregiverdistress associated with behavioral and psychologicalsymptoms in mild Alzheimerrsquos disease Dementia eNeuropsychologia 4 238ndash244
Ballard C G et al (1995) The aetiology of depression inthe carers of dementia sufferers Journal of AffectiveDisorders 35 59ndash63 doi1010160165-0327(95)00041-k
Bandeira D R Pawlowski J Goncalves T RHilgert J B Bozzetti M C and Hugo F N (2007)Psychological distress in Brazilian caregivers of relativeswith dementia Aging and Mental Health 11 14ndash19doi10108013607860600640814
Berger G Bernhardt T Weimer E Peters JKratzsch T and Frolich L (2005) Longitudinal studyon the relationship between symptomatology of dementia
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1772 A Feast et al
and levels of subjective burden and depression amongfamily caregivers in memory clinic patients Journal ofGeriatric Psychiatry and Neurology 3 119ndash128doi1011770891988704273375
Black W and Almeida O P (2004) A systematic reviewof the association between the behavioral and psychologicalsymptoms of dementia and burden of care InternationalPsychogeriatrics 16 295ndash315doi101017s1041610204000468
Bruce D G and Paterson A (2000) Barriers tocommunity support for the dementia carer a qualitativestudy International Journal of Geriatric Psychiatry 15451ndash457 doi101002(sici)1099-1166(200005)155lt451aid-gps143gt30co2-k
Campbell P et al (2008) Determinants of burden in thosewho care for someone with dementia International Journalof Geriatric Psychiatry 23 1078ndash1085doi101002gps2071
Cerejeira J Lagarto L and Mukaetova-LadinskaE B (2012) Behavioral and psychological symptoms ofdementia Frontiers in Neurology 3 1ndash23doi103389fneur201200073
Chappell N L and Penning M (1996) Behaviouralproblems and distress among caregivers of people withdementia Ageing amp Society 16 57ndash73doi101017s0144686x00003135
Chiu Y C et al (2014) Family caregiversrsquo sleepdisturbance and its associations with multilevel stressorswhen caring for patients with dementia Aging amp MentalHealth 18 92ndash101 doihttpdxdoiorg101080136078632013837141
Cohen J (1988) Statistical Power Analysis for the BehavioralSciences 2nd edn New York University New YorkLawrence Erlbaum Associatesdoi1043249780203771587
Conde-Sala J L Garre-Olmo J Turroacute-Garriga OVilalta-Franch J and Loacutepez-Pousa S (2010)Differential features of burden between spouse andadult-child caregivers of patients with Alzheimerrsquos diseasean exploratory comparative design International Journal ofNursing Studies 47 1262ndash1273doi101016jijnurstu201003001
Covinsky K E et al (2003) Patient and caregivercharacteristics associated with depression in caregivers ofpatients with dementia Journal of General Internal Medicine18 1006ndash1014 doihttpdxdoiorg101111j1525-1497200330103x
Craig D Mirakhur A Hart D J McIlroy S P andPassmore A P (2005) A cross-sectional study ofneuropsychiatric symptoms in 435 patients withAlzheimerrsquos disease American Journal of GeriatricPsychiatry 13 460ndash468 doi10109700019442-200506000-00004
Crellin N Charlesworth G and Orrell M (2014)Measuring family caregiver efficacy for managing behavioraland psychological symptoms in dementia a psychometricevaluation International Psychogeriatrics 26 93ndash103 doihttpdxdoiorg101017s1041610213001646
Davidsdottir S R Snaedal J Karlsdottir GAtladottir I and Hannesdottir K (2012) Validationof the Icelandic version of the neuropsychiatric inventorywith caregiver distress (NPI-D) Nordic Journal of
Psychiatry 66 26ndash32 doihttpdxdoiorg103109080394882011593100
Davis J D and Tremont G (2007) Impact of frontalsystems behavioral functioning in dementia on caregiverburden The Journal of Neuropsychiatry and ClinicalNeurosciences 19 43ndash49 doihttpdxdoiorg101176jnp200719143
de Vugt M E Riedijk S R Aalten P Tibben Avan Swieten J C and Verhey F R J (2006) Impactof behavioural problems on spousal caregivers acomparison between Alzheimerrsquos disease andfronto-temporal dementia Dementia and Geriatric CognitiveDisorders 22 35ndash41 doi101159000093102
de Vugt M E et al (2003) Behavioural disturbances indementia patients and quality of the marital relationshipInternational Journal of Geriatric Psychiatry 18 149ndash154doi101002gps807
Donaldson C Tarrier N and Burns A (1998)Determinants of carer stress in Alzheimerrsquos diseaseInternational Journal of Geriatric Psychiatry 13 248ndash256doi101002(sici)1099-1166(199804)134lt248aid-gps770gt30co2-0
Downs S and Black N (1998) The feasibility of creating achecklist for the assessment of the methodological qualityboth of randomised and non-randomised studies of healthcare interventions Journal of Epidemiological CommunityHealth 52 377ndash384 doi101136jech526377
Farran C J Loukissa D A Lindeman D A andMcCann J (2004) Caring for self while caring for othersthe two-track life of coping with Alzheimerrsquos diseaseJournal of Gerontological Nursing 30 38ndash45doi1039280098-9134-20040501-09
Fauth E B and Gibbons A (2014) Which behavioral andpsychological symptoms of dementia are the mostproblematic Variability by prevalence intensity distressratings and associations with carer depressive symptomsInternational Journal of Geriatric Psychiatry 29 263ndash271doi101002gps4002
Fuh J L Liu C K Mega M S Wang S J andCummings J L (2001) Behavioral disorders andcaregiversrsquo reaction in Taiwanese patients with Alzheimerrsquosdisease International Psychogeriatrics 13 121ndash128 doihttpdxdoiorg101017s1041610201007517
Gaugler J E et al (2011) Does caregiver burden mediatethe effects of behavioral disturbances on nursing homeadmission The American Journal of Geriatric Psychiatry 19497ndash506 doi101097jgp0b013e31820d92cc
Gilleard C J Belford H Gilleard E Whittick J Eand Gledhill K (1984) Emotional distress amongst thesupporters of the elderly mental infirm British Journal ofPsychiatry 145 172ndash177doihttpdxdoiorg101192bjp1452172
Gitlin L N and Rose K (2014) Factors associated withcarer readiness to use nonpharmacologic strategies tomanage dementia-related behavioral symptomsInternational Journal of Geriatric Psychiatry 29 93ndash102doihttpdxdoiorg101002gps3979
Goldberg D P and Hillier V F (1979) A scaled versionof the general health questionnaire Psychological Medicine9 139ndash145 doi101017s0033291700021644
Gonzalez-Salvador M T Arango C Lyketsos C Gand Barba A C (1999) The stress and psychological
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1773
morbidity of the Alzheimer patient caregiver InternationalJournal of Geriatric Psychiatry 14 701ndash710doi101002(sici)1099-1166(199909)149lt701aidps5gt30co2-
Haley W E Brown S and Levine E G (1987) Familycaregiver appraisals of patient behavioral disturbance insenile dementia Clinical Gerontologist The Journal of Agingand Mental Health 6 25ndash34doi101300j018v06n04_04
Haley W E Levine E G Brown S L Berry J Wand Hughes G H (2008) The psychological social andhealth consequences of caring for a relative with seniledementia Journal of the American Geriatrics Society 35405ndash411 doi101111j1532-54151987tb04661x
Hishikawa N et al (2012) Effects of turmeric onAlzheimerrsquos disease with behavioral and psychologicalsymptoms of dementia Ayu 33 499ndash504 doihttpdxdoiorg1041030974-8520110524
Huang S S Lee M C Liao Y C Wang W F andLai T J (2012) Caregiver burden associated withbehavioral and psychological symptoms of dementia(BPSD) in Taiwanese elderly Archives of Gerontology andGeriatrics 55 55ndash59 doihttpdxdoiorg101016jarchger201104009
Jackson M A Fauth E B and Geiser C (2014)Comparing the neuropsychiatric inventory and the revisedmemory and behavior problems checklist for associationswith caregiver burden and depressive symptomsInternational Psychogeriatrics 26 1021ndash1031doi101017s1041610213002421
Johnson D K Niedens M Wilson J RSwartzendruber L Yeager A and Jones K (2013)Treatment outcomes of a crisis intervention program fordementia with severe psychiatric complications the Kansasbridge project The Gerontologist 53 102ndash112 doihttpdxdoiorg101093gerontgns104
Khoo S A Chen T Y Ang Y H and Yap P (2013)The impact of neuropsychiatric symptoms on caregiverdistress and quality of life in persons with dementia in anAsian tertiary hospital memory clinic InternationalPsychogeriatrics 25 1991ndash1999 doihttpdxdoiorg101017s1041610213001518
Kosberg J I Kaufman A V Burgio L D Leeper Jand Sun F (2007) Family caregiving to those withdementia in rural Alabama racial similarities anddifferences Journal of Aging and Health 19 3ndash21 doi1011770898264306293604
Kosmala K and Kloszewska I (2004) The burden ofproviding care for Alzheimerrsquos disease patients in PolandInternational Journal of Geriatric Psychiatry 19 191ndash193doi101002gps1054
Landis J R and Koch G G (1977) The measurement ofobserver agreement for categorical data Biometrics 33159ndash174 doi 1023072529310
Lee D R McKeith I Mosimann U Ghosh-NodyalA and Thomas A J (2013) Examining carer stress indementia the role of subtype diagnosis andneuropsychiatric symptoms International Journal ofGeriatric Psychiatry 28 135ndash141 doihttpdxdoiorg101002gps3799
Lim Y M Son G R Song J A and Beattie E(2008) Factors affecting burden of family caregivers of
community-dwelling ambulatory elders with dementia inKorea Archives of Psychiatric Nursing 22 226ndash234 doi101016japnu200712005
Matsumoto N et al (2007) Caregiver burden associatedwith behavioral and psychological symptoms of dementia inelderly people in the local community Dementia andGeriatric Cognitive Disorders 23 219ndash224doi101159000099472
Mohamed S Rosenheck R Lyketsos C G andSchneider L S (2010) Caregiver burden in Alzheimerdisease cross-sectional and longitudinal patient correlatesThe American Journal of Geriatric Psychiatry 18 917ndash927doi101097jgp0b013e3181d5745d
Mourik J C Rosso S M Niermeijer M FDuivenvoorden H J Van Swieten J C and TibbenA (2004) Frontotemporal dementia behavioral symptomsand caregiver distress Dementia and Geriatric CognitiveDisorders 18 299ndash306 doihttpdxdoiorg101159000080123
Muangpaisan W et al (2010) Caregiver burden and needsof dementia caregivers in Thailand a cross-sectional studyJournal of the Medical Association of Thailand 93 601ndash607
Neundorfer M M McClendon M J Smyth K AStuckey J C Strauss M E and Patterson M B(2001) A longitudinal study of the relationship betweenlevels of depression among persons with Alzheimerrsquosdisease and levels of depression among their familycaregivers Journal of Gerontology Series B - PsychologicalSciences and Social Sciences 56 301ndash313
Nygaard H A (1998) Strain on caregivers of dementedelderly people living at home Scandinavian Journal ofPrimary Health Care 6 33ndash37doihttpdxdoiorg10310902813438809009287
Ornstein K and Gaugler J E (2012) The problem withldquoproblem behaviorsrdquoa systematic review of the associationbetween individual patient behavioral and psychologicalsymptoms and caregiver depression and burden within thedementia patientndashcaregiver dyad InternationalPsychogeriatrics 24 1536ndash1552doi101017s1041610212000737
Ornstein K Gaugler J E Devanand N S CarolynZ and Yaakov S (2012) The differential impact ofunique behavioral and psychological symptoms for thedementia caregiver how and why do patientsrsquo individualsymptom clusters impact caregiver depressive symptomsThe American Journal of Geriatric Psychiatry 12 77ndash1286doi httpdxdoiorg101016jjagp201301062
Price G R (1970) Selection and covariance Nature 227520ndash521 doi101038227520a0
Prince M (2000) Dementia in developing countries Aconsensus statement from the 1066 Dementia ResearchGroup International Journal of Geriatric Psychiatry 1514ndash20 doihttpdxdoiorg101002(sici)1099-1166(200001)151lt14aid-gps70gt30co2-8
Quayhagen M P and Quayhagen M (1998) Alzheimerrsquosstress coping with the caregiving role Gerontologist 28391ndash396 doihttpdxdoiorg101093geront283391
Reisberg B Ferris S H de Leon M J and Crook T(1982) The global deterioration scale for assessment ofprimary degenerative dementia American Journal ofPsychiatry 139 1136ndash1139 doihttpdxdoiorg101176ajp13991136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1774 A Feast et al
Robinson K M Adkisson P and Weinrich S (2001)Problem behaviour caregiver reactions and impact amongcaregivers of persons with Alzheimerrsquos disease Journal ofAdvanced Nursing 36 573ndash582 doihttpdxdoiorg101046j1365-2648200102010x
Rocca P et al (2010) Neuropsychiatric symptomsunderlying caregiver stress and insight in Alzheimerrsquosdisease Dementia and Geriatric Cognitive Disorders 3057ndash63 doi101159000315513
Rymer S Salloway S Norton L Mallow PCorreia S and Monast D (2002) Impaired awarenessbehavior disturbance and caregiver burden in Alzheimerdisease Alzheimer Disease and Associated Disorders 16248ndash253 doi 10109700002093-200210000-00006
Savorani G Vulcano V Boni S Sarti G andRavaglia G (1998) Behavioral disorders in dementiapatients and their impact on the stress of caregivingrelatives the ldquoARADrdquo questionnaire Archives ofGerontology and Geriatrics 6 481ndash485doi101016s0167-4943(98)80070-8
Shaji K S George R K Prince M J and JacobK S (2009) Behavioral symptoms and caregiver burdenin dementia Indian Journal of Psychiatry 51 45 doihttpdxdoiorg1041030019-554544905
Sink K M Covinsky K E Barnes D E NewcomerR J and Yaffe K (2006) Caregiver characteristics areassociated with neuropsychiatric symptoms of dementiaJournal of the American Geriatrics Society 54 796ndash803 doi101111j1532-5415200600697x
Slachevsky A et al (2013) The CUIDEME studydeterminants of burden in chilean primary caregivers ofpatients with dementia Journal of Alzheimerrsquos Disease 35297ndash306
Spiegel R et al (1991) A new behavioral assessment scalefor geriatric out- and in-patients the NOSGER (nursesrsquoobservation scale for geriatric patients) Journal of theAmerican Geriatric Society 39 339ndash347 doihttpdxdoiorg101111j1532-54151991tb02897x
Tan L L Wong H B and Allen H (2005) The impactof neuropsychiatric symptoms of dementia on distress infamily and professional caregivers in SingaporeInternational Psychogeriatrics 17 253ndash263 doi101017s1041610205001523
Teri L (1997) Behavior and caregiver burden behavioralproblems in patients with Alzheimer disease and itsassociation with caregiver distress Alzheimer Disease andAssociated Disorders 11 35ndash38
Teri L Truax P Logsdon R Uomoto J Zarit Sand Vitaliano P P (1992) Assessment of behavioralproblems in dementia the revised memory and behaviorproblems checklist Psychology and Aging 7 622 doi1010370882-797474622
Waite A Bebbington P Skelton-Robinson M andOrrell M (2004) Social factors and depression in carersof people with dementia International Journal of GeriatricPsychiatry 19 582ndash587 doihttpdxdoiorg101002gps1136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at

Individual BPSD and caregiver well-being 1765
005
115
225
335
445
Mea
n di
stre
ss
Delusions Hallucinations AgitationAggression Depression
005
115
225
335
Mea
n di
stre
ss
Anxiety Euphoria Apathy Disinhibition
0
05
1
15
2
25
3
35
4
Mea
n di
stre
ss
Irritability Aberrant motor behaviour Sleep Appettite and eating
Figure 2 Mean distress scores across 16 studies for behaviors on the NPI (total score)
as less problematic burdensome and distressingcompared to many of the other behaviors Verbalaggression across three of the five studies wasreported as problematic and burdensome Acrosstwo of the five studies which reported sexualdisinhibition this behavior was reported as theleast problematic Reports of wandering acrossfour of the studies were not consistent since
some of the studies reported this behavior asmuch more problematic and burdensome thanothers
Across four of the five studies which reportedincontinence this was consistently reported as oneof the more burdensome stressful and problematicbehaviors Physical aggression was only measuredin three studies and only one study reported this
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1766 A Feast et al
Figure 3 Meta-analysis of mean distress for each BPSD associated with NPI total score
behavior as a common problem Both studies whichreported irritability identified this behavior to be oneof the most problematic and burdensome
Correlational data between BPSD andcaregiver well-beingSleeping- and eating-related behaviors were foundto be significantly correlated to burden and strainhowever they had a stronger association withburden (Donaldson et al 1998) With regard toadult-child caregivers four (delusions agitationdisinhibition and appetiteeating change) of theeight behaviors reported by Conde-Sala et al (2010)as being significantly associated with burden werealso found to be significantly associated with burdenby Allegri et al (2006) Apathy and irritabilitywere reported to be significantly associated withburden in the study conducted by Conde-Sala et al(2010) but no significant relationship was reportedby Allegri et al (2006) Spousal caregivers onlyfound appetiteeating change burdensome (Conde-Sala et al 2010) Apathy had a moderate significantassociation with burden in spousal and adult-child caregivers (Conde-Sala et al 2010) but thisassociation was non-significant in the data reported
by Allegri et al (2006) Delusional and irritablebehaviors were also reported as non-significantlyrelated to burden (Allegri et al 2006) but weresignificantly related to burden by Conde-Sala et al(2010) In contrast to the previous studies reportingthe weak association between euphoria and distressFuh et al (2001) reported a significant correlationbetween euphoria and burden No other behaviorson the NPI had a significant correlation with burden(Fuh et al 2001)
In agreement with the data concerning atthe association between the frequency of thebehavior within each subscale on the RMBPCand reactivity disruptive behaviors had the largestcorrelation of the three subscales with burden(Huang et al 2012) Using the BEHAVE-AD (Reisberg et al 1982) and the NOSGER(Spiegel et al 1991) mood social behaviorsand disturbing behaviors were found to havea significant moderate association with burdenbut no significant correlations with depression incaregivers Chiu et al (2014) noted that all of thebehaviors on the NPI significantly predicted sleepdisturbance in caregivers other than anxiety andaberrant motor behavior
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1767
Table 1 Meta-analysis of mean distress scores correlated with behaviors using NPI total scores
P O O L E D C O R RELATION COEFFI CIENT T EST F OR HETEROGENEITY
FI XE D-E FF E C T S RANDOM-E FF E C T S
BEHAVIOR N MODEL (95 CI) MODEL (95 CI) I2 95 CI P
Delusions 243 0557 (0462 to 0640) 0567 (0412 to 0690) 5864 000 to 8623 p = 00643Hallucinations 243 0502 (0399 to 0532) 0520 (0198 to 0791) 8771 7081 to 9482 p lt 00001AgitationAggression 243 0540 (0443 to 0625) 0537 (0299 to 0712) 7941 4517 to 9482 p = 00022Depression 243 0528 (0429 to 0615) 0564 (0360ndash0717) 7465 2949 to 9089 p = 00080Anxiety 243 0482 (0377 to 0575) 0481 (0236 to 0669) 7845 4203 to 9199 p = 00030Euphoria 243 0540 (0443 to 0625) 0480 (0147 to 0715) 8764 7061 to 9480 p lt 00001Apathy 243 0456 (0351 to 0554) 0459 (0351 to 0540) 000 000 to 8423 p = 04834Disinhibition 243 0357 (0240 to 0464) 0371 (0162 to 0548) 6574 000 to 8833 p = 00327Irritability 243 0668 (0590 to 0733) 0691 (0486 to 0823) 8281 5601 to 9329 p = 00006Aberrant motor
behavior243 0606 (0518 to 0681) 0603 (0437 to 0730) 6764 371 to 8871 p = 00280
Sleep 176 0438 (0307 to 0552) 0436 (0301 to 0554) 532 000 to 9682 p = 03478Appetite and eating 176 0405 (0271 to 0523) 0442 (0200 to 0633) 6617 000 to 9026 p = 00520
Predictive data between BPSD and well-beingConde-Sala et al (2010) Chappell and Penning(1996) Davis and Tremont (2007) and Slachevskyet al (2013) used the same burden measurebut used different measures of BPSD Apathysignificantly predicted burden across three studiesalthough it was less burdensome for adult-childcaregivers and did not predict apathy in the study byDavis and Tremont (2007) Three studies (Mouriket al 2004 Khoo et al 2013 Lee et al 2013)reported data identifying which behaviors predicteddistress as measured by the NPI Apathy wasa significant predictor across two of the threestudies Delusions and anxiety were the only othercomparable behaviors across two of the three studiesand were both significant predictors of distressCovinsky et al (2003) did not use a formal behaviorscale but identified that anger and aggressivebehaviors were stronger predictors of caregiverdepression followed by dangerous behaviors to selfand others and then behaviors which wake thecaregiver up at night
Discussion
To our knowledge this is the first review to controlfor the effect of multiple BPSD on caregiver well-being by discriminating between individual BPSDand also discriminating between caregiver outcomesof well-being Additional advantages of this reviewwere the use of a formal method of synthesis andthe decision to distinguish between how BPSD andcaregiver well-being are measured which ensuredvalid conclusions were drawn by only synthesizing
comparable data Only two meta-analyses werepossible due to limited homogeneous studiesCategories in which the relationship betweenBPSD and well-being were qualitatively examinedincluded minimal studies displaying considerablevariation therefore valid conclusions could not bedrawn The results are discussed in the context ofprevious research
Meta-analysis of mean distress scoresAs seen in Figures 2 and 3 even within one measureand one criterion (distress associated with totalscore on the NPI) variability in distress ratingsfor each symptom can be seen between the 16studies This was also evident in research conductedby Fauth and Gibbons (2014) in which a widevariation in the prevalence of NPI symptoms wasseen between studies However data regardingdistress associated with euphoria and delusionsdemonstrated high levels of variance in terms of theratio between the mean and the standard deviationresulting in considerable variability between scoresTherefore the ratio of the mean distress ratingscompared with the standard deviation associatedwith the other ten behaviors signifies that there islow variance between the 16 studies It is unclearat present why there is increased variability foreuphoric and delusional behaviors In terms of totalscore depression followed by agitationaggressionand apathy were found to be the most distressingfor caregivers across 16 studies in the meta-analysis(Figure 3) This suggests that it is mood-relatedbehaviors which are associated with increaseddistress Fauth and Gibbons (2014) examinedthe relationship between total score of BPSD
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1768 A Feast et al
and distress and found similar results howevereven with identical analysis there were noteworthydiscrepancies such as delusions being the mostdistressing but only the fourth most distressing inthe current review Consistent with the currentmeta-analysis of mean data apathy and depression-related behaviors have been reported as distressingin numerous studies (Teri 1997 deVugt et al2003 Aarsland et al 2007 Kosberg et al 2007)Similarly depression in the person with dementia isassociated with depression in the caregiver (Waiteet al 2004)
Meta-analysis of correlation dataAs seen in Table 1 there were high levels ofheterogeneity between the studies included in thesecond meta-analysis investigating which behaviorswere associated with distress Only apathy- andsleep-related behaviors displayed homogeneitybetween studies Furthermore behaviors which hadstronger correlations with distress (Table 1) didnot have strong associations in the previous meta-analysis (Figure 3) regarding distress associatedwith behaviors At present it is unclear why thisdiscrepancy exists and also why distress correlatedwith apathy- and sleep-related behaviors is more ho-mogenous between studies than the other behaviorsSince only a few studies contributed to this meta-analysis more research is needed to investigate thepooled effects Nevertheless a meta-analysis of thisnature has not been performed previously and therandom-effects model was used to report a moreconservative estimate for the heterogeneous pooledeffects in order to reduce bias
Apathy and irritable behaviors were not con-sistently significantly correlated to burden acrossmultiple studies whereas delusions agitationdisinhibition and appetiteeating change werethese associations were also reported in otherstudies (Rymer et al 2002 Rocca et al 2010) Incontrast a review by Ornstein and Gaugler (2012)reported that angeraggression and depression werethe most frequently cited BPSD associated withcaregiver burden depression was also linked tocaregiver burden in a review by Black and Almeida(2004) In addition to burden delusional behaviorwas consistently associated with distress acrossstudies with a significant correlation also beingseen with stress (Kosmala and Kloszewska 2004)Berger et al (2005) noted that behaviors whichare significantly correlated with burden are notcorrelated with depression This demonstrates theimportance of including multiple measures of well-being since the same behaviors affect caregiversdifferently which has implications for futureinterventions
Studies unamenable to quantitative synthesisOnly two studies reported the prevalence of BPSDand the impact on caregiver well-being due todifferences between studies comparisons werenot possible Although five studies reported thefrequency of BPSD each measure of caregiver well-being was different Memory-related behaviorsverbal aggression incontinence and irritabilitywere reported to affect well-being across multiplestudies These findings were also seen in previousresearch (Bruce and Paterson 2000 Farran et al2004) However Fauth and Gibbons (2014) andRobinson et al (2001) did not find that memory-related behaviors were distressing despite being themost frequent type of behavior on the RMBPCHallucinations sexual disinhibition and physicalaggression were consistently reported to affect well-being less than the other behaviors Although thisfinding is reflected in the majority of studies Haleyet al (2008) and Arango-Lasprilla et al (2010)reported contradictory results
It is noteworthy that aggressionagitation whenmeasured in terms of total score was reported asthe second most distressing across 16 of the studiesbut when measured in terms of frequency only oneof the three studies reported physical aggressionas a common problem However the frequency ofverbal aggression consistently affected well-beingIt is not possible to provide an explanation for thisdiscrepancy but it may be because of the distinctionbetween how aggressionagitation is measured (ietotal score or frequency) or that verbal and physicalaggression have been differentiated and thereforeaffect caregiver well-being differently
Predictive data were limited and heterogeneousin the present review however it was possible toconclude that apathy predicted burden and distressacross studies Anger restlessness combativenessdangerous to others and embarrassing behaviorwere found to be strong predictors of burden ina study by Gaugler et al (2011) Only one studyreported the predictors of caregiver depression
Potential explanations for variability incaregiver well-beingDifference in study quality does not appear to be anexplanation for the variation in distress rating acrossstudies since even between two medium qualitystudies there was considerable variation (Balieiroet al 2010 displaying one of the highest meandistress scores Baiyewu et al 2003 displayingone of the lowest) Two studies consistently hadthe highest mean distress rating across each of thebehavior domains Balieiro et al (2010) and Tanet al (2005) Both of these studies were clinic-basedhigher distress ratings would be expected as those
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1769
experiencing more BPSD might be more likely toattend a clinic as indeed were the majority ofstudies included in the meta-analysis It may bepossible that dementia severity is an explanationsince participants in the studies with the highestdistress scores (Tan et al 2005 Balieiro et al 2010)had moderate and severe dementia respectivelywhereas Baiyewu et al (2003) who consistentlyreported the lowest distress scores across eachof the behavior domains included participantswith mild dementia However both Aarslandet al (2007) and de Vugt et al (2006) reportedlower mean distress scores in comparison with theother included studies and they both includedparticipants with moderate dementia FurthermoreDavidsdottir et al (2012) found that there wasno significant difference between caregiver distressscores depending on dementia severity
Baiyewu et al (2003) had a much smallersample of spousal caregivers in comparison to Tanet al (2005) which might account for the lowerdistress scores This is in agreement with Almberget al (1997) who reported that spouses experiencegreater levels of burden However three studieswhich had consistently higher mean distress scoresacross all behaviors (Tan et al 2005 Balieiro et al2010 Huang et al 2012) were mainly comprisedof adult-child caregivers When comparing a studysolely comprised of spousal caregivers (deVugt et al2006) with a study (Baiyewu et al 2003) withminimal spousal caregivers (25) it was possibleto see that spousal caregivers were substantiallymore distressed with depressive apathetic andanxiety-related behaviors Although distress ratingscan be differentiated between behavior types forspousal and non-spousal caregivers both Baiyewuet al (2003) and de Vugt et al (2006) had two of thelowest distress scores across all behaviors in compar-ison to the other studies in the meta-analysis
The explanation may also be cultural sinceBaiyewu et al (2003) and Baiyewu et al (2012)(with similarly low distress scores across behaviors)were the only Africa-based studies in the meta-analysis Baiyewu et al (2003) and Baiyewu et al(2012) were also both community-based studieswhich may also be a reason for the reduceddistress ratings There is every reason to believethat BPSD are present across cultures (Shajiet al 2009) however the low levels of publicawareness of dementia have many implications(Prince 2000) One of these implications maybe the misinterpretation of BPSD as deliberateconsequently affecting the well-being of the carer(Shaji et al 2009) It is beyond the scope ofthis paper to determine why there is considerablevariation between studies reporting caregiverdistress for identical behaviors using identical
measures However it is likely that it is the caregivercharacteristics rather than the characteristics of theperson with dementia (such as dementia severity)which may underlie the explanation as to whyvariation between studies exists
Limitations
The data available for this review allowed for onlytwo meta-analyses to be conducted There wererelatively few studies which assessed the relationshipbetween individual BPSD and caregiver well-beingand which met the inclusionexclusion criteriafor the review In an attempt to be systematicbased on prior recommendation an effort wasmade to distinguish between how ldquoproblematicrdquosymptoms are measured Consequently studieswere categorized into whether BPSD weremeasured in terms of frequency or prevalence andalso categorized in terms of the statistical analysisemployed Other than data regarding mean distressassociated with NPI total score only a small amountof studies were included in each category andunfortunately it was often the case that measuresof caregiver well-being were dissimilar From the 40included studies there were 12 different measuresof behavior and 17 different measures of well-being making comparisons difficult which mayhave contributed to the inconsistent findings
The majority of included studies recruitedparticipants from clinics therefore caregiversincluded in the review were not representative ofthe population In addition the samples across theincluded studies were heterogeneous in a numberof factors therefore caution should be taken wheninterpreting the results Although beyond the scopeof this review study characteristics such as culturegender and relationship direction were not ex-amined through subgroup analyses Due to the lim-ited number of studies it was not possible to imposea quality criteria however all included studies wereeither of high or medium quality as assessed by theDowns and Back Checklist (1998) Furthermore allof the included studies relied on caregiver reportsof BPSD which may themselves be affected bycaregiver well-being unfortunately it is not possibleto determine if this was the case Nonetheless twovalid meta-analyses were completed and a numberof comments can be made about the relationshipbetween BPSD and caregiver well-being
Implications and recommendations
The vast majority of studies addressing the rela-tionship between BPSD and caregiver well-being
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1770 A Feast et al
did not examine individual BPSD Consequentlythis comparatively limited the amount of studiesincluded in the present review Therefore if we areto understand this relationship more studies needto examine individual BPSD in their research Inaddition it is more clinically relevant to examinewhich BPSD affect well-being rather than BPSDas a whole as this is essential in determiningwhere clinical staff should allocate resources mosteffectively Nevertheless there is preliminary datasuggesting it is mood-related behaviors whichare associated with increased levels of distresstherefore interventions for the management ofBPSD should target these behaviors
The lack of consistency in the measurementof BPSD (neuropsychiatric or memory problemsfrequency or prevalence) and the measurementof caregiver well-being (the use of interchangeableterminology such as stress strain and burdenmeaning the same construct) limits our ability toreach a consensus as to which BPSD result inthe most negative outcomes for caregivers Forexample Donaldson et al (1998) used GilleardrsquosStrain Scale (1984) to measure burden andthe General Health Questionnaire (Goldberg andHillier 1979) to measure distress Furthermorefour studies (see Table S1) did not have formalscales to measure the impact of BPSD on well-being and used terms such as ldquoburdensomerdquoldquoseriousrdquo and ldquodisturbingrdquo This problem impactsupon the validity and reliability of the originalstudies and consequently the review Howeverthis mainly occurred in the earlier studies Futureresearch should also include more than one measureof well-being in order to identify if individual BPSDdifferentially affect caregiver burden compared tocaregiver distress as identified in the current reviewFurthermore future research should identify whythere is reduced variability in distress ratings forcertain behaviors compared to others and whycertain behaviors are more distressing dependingon which type of statistical analysis is used
Although there are potential methodologicalreasons (limited studies inconsistent measures)for why there is substantial variability whenidentifying which BPSD affect certain types ofcaregiver well-being the most there is growingevidence that factors associated with the personwith dementia (eg BPSD frequency cognition) areonly part of the story when explaining a caregiverrsquosresponse to BPSD Caregiver characteristicshave been shown to account for twice thevariance of person with dementia characteristicswhen reporting neuropsychiatric symptoms (Sinket al 2006) and the presence of BPSD wasnot found to be a significant predictor ofburden whereas caregiver characteristics such as
confidence neuroticism and relationship qualitywere significant predictors (Campbell et al 2008)Therefore as recommended by Ornstein andGaugler (2012) future studies should focus onidentifying pathways for the association betweenindividual BPSD caregiver variables and caregiveroutcomes More research is needed to understandif and why certain BPSD affect certain caregiveroutcomes and also how much of this is attributableto caregiver variability in response to BPSD ratherthan the presence of BPSD itself More longitudinalstudies would be useful to examine how changes inindividual BPSD are associated with caregiver well-being over time A review by Black and Almeida(2004) examined the limited longitudinal studiesavailable and reported mixed findings betweenburden and BPSD and found no associationbetween BPSD and distress Although BPSDincreased significantly over a two-year periodcaregiver burden remained stable and depressionwas found to decrease (Berger et al 2005) Futureresearch needs to examine caregiver factors overtime (well-being role captivity etc) along withchanges in individual BPSD in order to have a morevalid understanding of this relationship
Caution should be exercised when creating ameasure of BPSD since Jackson et al (2014)found that the Revised Memory and BehaviorProblem Checklist (Teri et al 1992) might bemore suitable in explaining caregiver depressionthan the NPI It is important that the measureof BPSD is not biased toward explaining a moreunique association between BPSD and a measure ofcaregiver well-being such as depression As stated byGitlin and Rose (2014) item selection for measuresof BPSD is often based upon specific disciplines(eg neurology psychiatry social sciences) andthus implicitly represents different conceptual-izations of behavior A shared framework fordefining behaviors and their underlying causesmust be created in order to move on fromthe implicit assumption of most measures thatbehaviors are a direct cause of neuropathologyand to develop measures which also address thecontextual and caregiver characteristics associatedwith the behavior
Conclusions
This study has improved our understanding of theimpact of individual BPSD on caregiver well-beingin particular caregiver distress The relationshipbetween individual BPSD and caregiver well-beingwas inconsistent and varied according to behavioralsymptom Due to limited studies and heterogeneousdata the results should be interpreted with caution
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1771
but advances have been made with respect towhich behaviors are associated with distress Theinconsistencies may be partly explained by caregivervariables which were not taken into account inthe review Based on this review and previousresearch it is not possible to fully understand therelationship between BPSD and caregiver well-being without examining the influence of caregivervariables such as caregiver strategies acceptancegender relationship with person with dementiaand confidence We recommend that future studiesare designed to examine individual BPSD ratherthan BPSD as a whole use consistent measures forBPSD and well-being use consistent terminologyfor psychological constructs (eg burden) andexamine the causal mechanisms by which individualBPSD impact caregiver well-being by collectingdata on a range of caregiver factors Theseapproaches will clarify whether it is important forclinicians to focus on the frequency or prevalence ofcertain BPSD in addition to targeting the presenceof certain caregiver characteristics and addressingunmet need
Conflict of interest
None
Description of authorsrsquo roles
A Feast was responsible for developing the reviewobjectives writing the search strategies conductingthe searches designing and completing studyeligibility and data extraction forms undertakingthe quality appraisals conducting the meta-analysisand writing the paper M Orrell was responsible fordeveloping the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper C Stoner was responsible forundertaking the quality appraisals and assisting inwriting the paper G Charlesworth was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper E Moniz-Cook was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper
Acknowledgments
We would like to thank Dr Zoeuml Hoare for herstatistical advice This paper presents independentresearch funded by the National Institute for HealthResearch (NIHR) under its Programme Grants forApplied Research (RP-PG-0606-1067 and RP-PG-
060- 1083) The views expressed in this publicationare those of the author(s) and not necessarily thoseof the NHS the NIHR or the Department ofHealth
Supplementary Material
To view supplementary material for thisarticle please visit httpdxdoiorg101017S1041610216000922
References
Aarsland D et al (2007) Neuropsychiatric symptoms inpatients with Parkinsonrsquos disease and dementia frequencyprofile and associated care giver stress Journal of NeurologyNeurosurgery amp Psychiatry 78 36ndash42doihttpdxdoiorg101136jnnp2005083113
Allegri R F et al (2006) Neuropsychiatric symptoms as apredictor of caregiver burden in Alzheimerrsquos diseaseNeuropsychiatric Disease amp Treatment 2 105ndash110doi102147ndts47133
Almberg B Grafstrom M and Winblad B (1997)Major strain and coping strategies as reported by familymembers who care for aged demented relatives Journal ofAdvanced Nursing 26 683ndash691doihttpdxdoiorg101046j1365-2648199700392x
Arango-Lasprilla J C Lehan T Drew A MorenoA Deng X and Lemos M (2010) Health-relatedquality of life in caregivers of individuals with dementiafrom Colombia American Journal of Alzheimerrsquos Disease andOther Dementias 25 556ndash561doi1011771533317510382287ltbibgt
Baiyewu O et al (2003) Behavioral and caregiver reactionof dementia as measured by the neuropsychiatric inventoryin Nigerian community residents InternationalPsychogeriatrics 15 399ndash409doi101017s1041610203009645
Baiyewu O et al (2012) Behavioral symptoms incommunity-dwelling elderly Nigerians with dementia mildcognitive impairment and normal cognition InternationalJournal of Geriatric Psychiatry 27 931ndash939 doihttpdxdoiorg101002gps2804
Balieiro A P Jr Sobreira E S T Pena M C SSilva-Filho J H and Vale F A C (2010) Caregiverdistress associated with behavioral and psychologicalsymptoms in mild Alzheimerrsquos disease Dementia eNeuropsychologia 4 238ndash244
Ballard C G et al (1995) The aetiology of depression inthe carers of dementia sufferers Journal of AffectiveDisorders 35 59ndash63 doi1010160165-0327(95)00041-k
Bandeira D R Pawlowski J Goncalves T RHilgert J B Bozzetti M C and Hugo F N (2007)Psychological distress in Brazilian caregivers of relativeswith dementia Aging and Mental Health 11 14ndash19doi10108013607860600640814
Berger G Bernhardt T Weimer E Peters JKratzsch T and Frolich L (2005) Longitudinal studyon the relationship between symptomatology of dementia
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1772 A Feast et al
and levels of subjective burden and depression amongfamily caregivers in memory clinic patients Journal ofGeriatric Psychiatry and Neurology 3 119ndash128doi1011770891988704273375
Black W and Almeida O P (2004) A systematic reviewof the association between the behavioral and psychologicalsymptoms of dementia and burden of care InternationalPsychogeriatrics 16 295ndash315doi101017s1041610204000468
Bruce D G and Paterson A (2000) Barriers tocommunity support for the dementia carer a qualitativestudy International Journal of Geriatric Psychiatry 15451ndash457 doi101002(sici)1099-1166(200005)155lt451aid-gps143gt30co2-k
Campbell P et al (2008) Determinants of burden in thosewho care for someone with dementia International Journalof Geriatric Psychiatry 23 1078ndash1085doi101002gps2071
Cerejeira J Lagarto L and Mukaetova-LadinskaE B (2012) Behavioral and psychological symptoms ofdementia Frontiers in Neurology 3 1ndash23doi103389fneur201200073
Chappell N L and Penning M (1996) Behaviouralproblems and distress among caregivers of people withdementia Ageing amp Society 16 57ndash73doi101017s0144686x00003135
Chiu Y C et al (2014) Family caregiversrsquo sleepdisturbance and its associations with multilevel stressorswhen caring for patients with dementia Aging amp MentalHealth 18 92ndash101 doihttpdxdoiorg101080136078632013837141
Cohen J (1988) Statistical Power Analysis for the BehavioralSciences 2nd edn New York University New YorkLawrence Erlbaum Associatesdoi1043249780203771587
Conde-Sala J L Garre-Olmo J Turroacute-Garriga OVilalta-Franch J and Loacutepez-Pousa S (2010)Differential features of burden between spouse andadult-child caregivers of patients with Alzheimerrsquos diseasean exploratory comparative design International Journal ofNursing Studies 47 1262ndash1273doi101016jijnurstu201003001
Covinsky K E et al (2003) Patient and caregivercharacteristics associated with depression in caregivers ofpatients with dementia Journal of General Internal Medicine18 1006ndash1014 doihttpdxdoiorg101111j1525-1497200330103x
Craig D Mirakhur A Hart D J McIlroy S P andPassmore A P (2005) A cross-sectional study ofneuropsychiatric symptoms in 435 patients withAlzheimerrsquos disease American Journal of GeriatricPsychiatry 13 460ndash468 doi10109700019442-200506000-00004
Crellin N Charlesworth G and Orrell M (2014)Measuring family caregiver efficacy for managing behavioraland psychological symptoms in dementia a psychometricevaluation International Psychogeriatrics 26 93ndash103 doihttpdxdoiorg101017s1041610213001646
Davidsdottir S R Snaedal J Karlsdottir GAtladottir I and Hannesdottir K (2012) Validationof the Icelandic version of the neuropsychiatric inventorywith caregiver distress (NPI-D) Nordic Journal of
Psychiatry 66 26ndash32 doihttpdxdoiorg103109080394882011593100
Davis J D and Tremont G (2007) Impact of frontalsystems behavioral functioning in dementia on caregiverburden The Journal of Neuropsychiatry and ClinicalNeurosciences 19 43ndash49 doihttpdxdoiorg101176jnp200719143
de Vugt M E Riedijk S R Aalten P Tibben Avan Swieten J C and Verhey F R J (2006) Impactof behavioural problems on spousal caregivers acomparison between Alzheimerrsquos disease andfronto-temporal dementia Dementia and Geriatric CognitiveDisorders 22 35ndash41 doi101159000093102
de Vugt M E et al (2003) Behavioural disturbances indementia patients and quality of the marital relationshipInternational Journal of Geriatric Psychiatry 18 149ndash154doi101002gps807
Donaldson C Tarrier N and Burns A (1998)Determinants of carer stress in Alzheimerrsquos diseaseInternational Journal of Geriatric Psychiatry 13 248ndash256doi101002(sici)1099-1166(199804)134lt248aid-gps770gt30co2-0
Downs S and Black N (1998) The feasibility of creating achecklist for the assessment of the methodological qualityboth of randomised and non-randomised studies of healthcare interventions Journal of Epidemiological CommunityHealth 52 377ndash384 doi101136jech526377
Farran C J Loukissa D A Lindeman D A andMcCann J (2004) Caring for self while caring for othersthe two-track life of coping with Alzheimerrsquos diseaseJournal of Gerontological Nursing 30 38ndash45doi1039280098-9134-20040501-09
Fauth E B and Gibbons A (2014) Which behavioral andpsychological symptoms of dementia are the mostproblematic Variability by prevalence intensity distressratings and associations with carer depressive symptomsInternational Journal of Geriatric Psychiatry 29 263ndash271doi101002gps4002
Fuh J L Liu C K Mega M S Wang S J andCummings J L (2001) Behavioral disorders andcaregiversrsquo reaction in Taiwanese patients with Alzheimerrsquosdisease International Psychogeriatrics 13 121ndash128 doihttpdxdoiorg101017s1041610201007517
Gaugler J E et al (2011) Does caregiver burden mediatethe effects of behavioral disturbances on nursing homeadmission The American Journal of Geriatric Psychiatry 19497ndash506 doi101097jgp0b013e31820d92cc
Gilleard C J Belford H Gilleard E Whittick J Eand Gledhill K (1984) Emotional distress amongst thesupporters of the elderly mental infirm British Journal ofPsychiatry 145 172ndash177doihttpdxdoiorg101192bjp1452172
Gitlin L N and Rose K (2014) Factors associated withcarer readiness to use nonpharmacologic strategies tomanage dementia-related behavioral symptomsInternational Journal of Geriatric Psychiatry 29 93ndash102doihttpdxdoiorg101002gps3979
Goldberg D P and Hillier V F (1979) A scaled versionof the general health questionnaire Psychological Medicine9 139ndash145 doi101017s0033291700021644
Gonzalez-Salvador M T Arango C Lyketsos C Gand Barba A C (1999) The stress and psychological
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1773
morbidity of the Alzheimer patient caregiver InternationalJournal of Geriatric Psychiatry 14 701ndash710doi101002(sici)1099-1166(199909)149lt701aidps5gt30co2-
Haley W E Brown S and Levine E G (1987) Familycaregiver appraisals of patient behavioral disturbance insenile dementia Clinical Gerontologist The Journal of Agingand Mental Health 6 25ndash34doi101300j018v06n04_04
Haley W E Levine E G Brown S L Berry J Wand Hughes G H (2008) The psychological social andhealth consequences of caring for a relative with seniledementia Journal of the American Geriatrics Society 35405ndash411 doi101111j1532-54151987tb04661x
Hishikawa N et al (2012) Effects of turmeric onAlzheimerrsquos disease with behavioral and psychologicalsymptoms of dementia Ayu 33 499ndash504 doihttpdxdoiorg1041030974-8520110524
Huang S S Lee M C Liao Y C Wang W F andLai T J (2012) Caregiver burden associated withbehavioral and psychological symptoms of dementia(BPSD) in Taiwanese elderly Archives of Gerontology andGeriatrics 55 55ndash59 doihttpdxdoiorg101016jarchger201104009
Jackson M A Fauth E B and Geiser C (2014)Comparing the neuropsychiatric inventory and the revisedmemory and behavior problems checklist for associationswith caregiver burden and depressive symptomsInternational Psychogeriatrics 26 1021ndash1031doi101017s1041610213002421
Johnson D K Niedens M Wilson J RSwartzendruber L Yeager A and Jones K (2013)Treatment outcomes of a crisis intervention program fordementia with severe psychiatric complications the Kansasbridge project The Gerontologist 53 102ndash112 doihttpdxdoiorg101093gerontgns104
Khoo S A Chen T Y Ang Y H and Yap P (2013)The impact of neuropsychiatric symptoms on caregiverdistress and quality of life in persons with dementia in anAsian tertiary hospital memory clinic InternationalPsychogeriatrics 25 1991ndash1999 doihttpdxdoiorg101017s1041610213001518
Kosberg J I Kaufman A V Burgio L D Leeper Jand Sun F (2007) Family caregiving to those withdementia in rural Alabama racial similarities anddifferences Journal of Aging and Health 19 3ndash21 doi1011770898264306293604
Kosmala K and Kloszewska I (2004) The burden ofproviding care for Alzheimerrsquos disease patients in PolandInternational Journal of Geriatric Psychiatry 19 191ndash193doi101002gps1054
Landis J R and Koch G G (1977) The measurement ofobserver agreement for categorical data Biometrics 33159ndash174 doi 1023072529310
Lee D R McKeith I Mosimann U Ghosh-NodyalA and Thomas A J (2013) Examining carer stress indementia the role of subtype diagnosis andneuropsychiatric symptoms International Journal ofGeriatric Psychiatry 28 135ndash141 doihttpdxdoiorg101002gps3799
Lim Y M Son G R Song J A and Beattie E(2008) Factors affecting burden of family caregivers of
community-dwelling ambulatory elders with dementia inKorea Archives of Psychiatric Nursing 22 226ndash234 doi101016japnu200712005
Matsumoto N et al (2007) Caregiver burden associatedwith behavioral and psychological symptoms of dementia inelderly people in the local community Dementia andGeriatric Cognitive Disorders 23 219ndash224doi101159000099472
Mohamed S Rosenheck R Lyketsos C G andSchneider L S (2010) Caregiver burden in Alzheimerdisease cross-sectional and longitudinal patient correlatesThe American Journal of Geriatric Psychiatry 18 917ndash927doi101097jgp0b013e3181d5745d
Mourik J C Rosso S M Niermeijer M FDuivenvoorden H J Van Swieten J C and TibbenA (2004) Frontotemporal dementia behavioral symptomsand caregiver distress Dementia and Geriatric CognitiveDisorders 18 299ndash306 doihttpdxdoiorg101159000080123
Muangpaisan W et al (2010) Caregiver burden and needsof dementia caregivers in Thailand a cross-sectional studyJournal of the Medical Association of Thailand 93 601ndash607
Neundorfer M M McClendon M J Smyth K AStuckey J C Strauss M E and Patterson M B(2001) A longitudinal study of the relationship betweenlevels of depression among persons with Alzheimerrsquosdisease and levels of depression among their familycaregivers Journal of Gerontology Series B - PsychologicalSciences and Social Sciences 56 301ndash313
Nygaard H A (1998) Strain on caregivers of dementedelderly people living at home Scandinavian Journal ofPrimary Health Care 6 33ndash37doihttpdxdoiorg10310902813438809009287
Ornstein K and Gaugler J E (2012) The problem withldquoproblem behaviorsrdquoa systematic review of the associationbetween individual patient behavioral and psychologicalsymptoms and caregiver depression and burden within thedementia patientndashcaregiver dyad InternationalPsychogeriatrics 24 1536ndash1552doi101017s1041610212000737
Ornstein K Gaugler J E Devanand N S CarolynZ and Yaakov S (2012) The differential impact ofunique behavioral and psychological symptoms for thedementia caregiver how and why do patientsrsquo individualsymptom clusters impact caregiver depressive symptomsThe American Journal of Geriatric Psychiatry 12 77ndash1286doi httpdxdoiorg101016jjagp201301062
Price G R (1970) Selection and covariance Nature 227520ndash521 doi101038227520a0
Prince M (2000) Dementia in developing countries Aconsensus statement from the 1066 Dementia ResearchGroup International Journal of Geriatric Psychiatry 1514ndash20 doihttpdxdoiorg101002(sici)1099-1166(200001)151lt14aid-gps70gt30co2-8
Quayhagen M P and Quayhagen M (1998) Alzheimerrsquosstress coping with the caregiving role Gerontologist 28391ndash396 doihttpdxdoiorg101093geront283391
Reisberg B Ferris S H de Leon M J and Crook T(1982) The global deterioration scale for assessment ofprimary degenerative dementia American Journal ofPsychiatry 139 1136ndash1139 doihttpdxdoiorg101176ajp13991136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1774 A Feast et al
Robinson K M Adkisson P and Weinrich S (2001)Problem behaviour caregiver reactions and impact amongcaregivers of persons with Alzheimerrsquos disease Journal ofAdvanced Nursing 36 573ndash582 doihttpdxdoiorg101046j1365-2648200102010x
Rocca P et al (2010) Neuropsychiatric symptomsunderlying caregiver stress and insight in Alzheimerrsquosdisease Dementia and Geriatric Cognitive Disorders 3057ndash63 doi101159000315513
Rymer S Salloway S Norton L Mallow PCorreia S and Monast D (2002) Impaired awarenessbehavior disturbance and caregiver burden in Alzheimerdisease Alzheimer Disease and Associated Disorders 16248ndash253 doi 10109700002093-200210000-00006
Savorani G Vulcano V Boni S Sarti G andRavaglia G (1998) Behavioral disorders in dementiapatients and their impact on the stress of caregivingrelatives the ldquoARADrdquo questionnaire Archives ofGerontology and Geriatrics 6 481ndash485doi101016s0167-4943(98)80070-8
Shaji K S George R K Prince M J and JacobK S (2009) Behavioral symptoms and caregiver burdenin dementia Indian Journal of Psychiatry 51 45 doihttpdxdoiorg1041030019-554544905
Sink K M Covinsky K E Barnes D E NewcomerR J and Yaffe K (2006) Caregiver characteristics areassociated with neuropsychiatric symptoms of dementiaJournal of the American Geriatrics Society 54 796ndash803 doi101111j1532-5415200600697x
Slachevsky A et al (2013) The CUIDEME studydeterminants of burden in chilean primary caregivers ofpatients with dementia Journal of Alzheimerrsquos Disease 35297ndash306
Spiegel R et al (1991) A new behavioral assessment scalefor geriatric out- and in-patients the NOSGER (nursesrsquoobservation scale for geriatric patients) Journal of theAmerican Geriatric Society 39 339ndash347 doihttpdxdoiorg101111j1532-54151991tb02897x
Tan L L Wong H B and Allen H (2005) The impactof neuropsychiatric symptoms of dementia on distress infamily and professional caregivers in SingaporeInternational Psychogeriatrics 17 253ndash263 doi101017s1041610205001523
Teri L (1997) Behavior and caregiver burden behavioralproblems in patients with Alzheimer disease and itsassociation with caregiver distress Alzheimer Disease andAssociated Disorders 11 35ndash38
Teri L Truax P Logsdon R Uomoto J Zarit Sand Vitaliano P P (1992) Assessment of behavioralproblems in dementia the revised memory and behaviorproblems checklist Psychology and Aging 7 622 doi1010370882-797474622
Waite A Bebbington P Skelton-Robinson M andOrrell M (2004) Social factors and depression in carersof people with dementia International Journal of GeriatricPsychiatry 19 582ndash587 doihttpdxdoiorg101002gps1136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at

1766 A Feast et al
Figure 3 Meta-analysis of mean distress for each BPSD associated with NPI total score
behavior as a common problem Both studies whichreported irritability identified this behavior to be oneof the most problematic and burdensome
Correlational data between BPSD andcaregiver well-beingSleeping- and eating-related behaviors were foundto be significantly correlated to burden and strainhowever they had a stronger association withburden (Donaldson et al 1998) With regard toadult-child caregivers four (delusions agitationdisinhibition and appetiteeating change) of theeight behaviors reported by Conde-Sala et al (2010)as being significantly associated with burden werealso found to be significantly associated with burdenby Allegri et al (2006) Apathy and irritabilitywere reported to be significantly associated withburden in the study conducted by Conde-Sala et al(2010) but no significant relationship was reportedby Allegri et al (2006) Spousal caregivers onlyfound appetiteeating change burdensome (Conde-Sala et al 2010) Apathy had a moderate significantassociation with burden in spousal and adult-child caregivers (Conde-Sala et al 2010) but thisassociation was non-significant in the data reported
by Allegri et al (2006) Delusional and irritablebehaviors were also reported as non-significantlyrelated to burden (Allegri et al 2006) but weresignificantly related to burden by Conde-Sala et al(2010) In contrast to the previous studies reportingthe weak association between euphoria and distressFuh et al (2001) reported a significant correlationbetween euphoria and burden No other behaviorson the NPI had a significant correlation with burden(Fuh et al 2001)
In agreement with the data concerning atthe association between the frequency of thebehavior within each subscale on the RMBPCand reactivity disruptive behaviors had the largestcorrelation of the three subscales with burden(Huang et al 2012) Using the BEHAVE-AD (Reisberg et al 1982) and the NOSGER(Spiegel et al 1991) mood social behaviorsand disturbing behaviors were found to havea significant moderate association with burdenbut no significant correlations with depression incaregivers Chiu et al (2014) noted that all of thebehaviors on the NPI significantly predicted sleepdisturbance in caregivers other than anxiety andaberrant motor behavior
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1767
Table 1 Meta-analysis of mean distress scores correlated with behaviors using NPI total scores
P O O L E D C O R RELATION COEFFI CIENT T EST F OR HETEROGENEITY
FI XE D-E FF E C T S RANDOM-E FF E C T S
BEHAVIOR N MODEL (95 CI) MODEL (95 CI) I2 95 CI P
Delusions 243 0557 (0462 to 0640) 0567 (0412 to 0690) 5864 000 to 8623 p = 00643Hallucinations 243 0502 (0399 to 0532) 0520 (0198 to 0791) 8771 7081 to 9482 p lt 00001AgitationAggression 243 0540 (0443 to 0625) 0537 (0299 to 0712) 7941 4517 to 9482 p = 00022Depression 243 0528 (0429 to 0615) 0564 (0360ndash0717) 7465 2949 to 9089 p = 00080Anxiety 243 0482 (0377 to 0575) 0481 (0236 to 0669) 7845 4203 to 9199 p = 00030Euphoria 243 0540 (0443 to 0625) 0480 (0147 to 0715) 8764 7061 to 9480 p lt 00001Apathy 243 0456 (0351 to 0554) 0459 (0351 to 0540) 000 000 to 8423 p = 04834Disinhibition 243 0357 (0240 to 0464) 0371 (0162 to 0548) 6574 000 to 8833 p = 00327Irritability 243 0668 (0590 to 0733) 0691 (0486 to 0823) 8281 5601 to 9329 p = 00006Aberrant motor
behavior243 0606 (0518 to 0681) 0603 (0437 to 0730) 6764 371 to 8871 p = 00280
Sleep 176 0438 (0307 to 0552) 0436 (0301 to 0554) 532 000 to 9682 p = 03478Appetite and eating 176 0405 (0271 to 0523) 0442 (0200 to 0633) 6617 000 to 9026 p = 00520
Predictive data between BPSD and well-beingConde-Sala et al (2010) Chappell and Penning(1996) Davis and Tremont (2007) and Slachevskyet al (2013) used the same burden measurebut used different measures of BPSD Apathysignificantly predicted burden across three studiesalthough it was less burdensome for adult-childcaregivers and did not predict apathy in the study byDavis and Tremont (2007) Three studies (Mouriket al 2004 Khoo et al 2013 Lee et al 2013)reported data identifying which behaviors predicteddistress as measured by the NPI Apathy wasa significant predictor across two of the threestudies Delusions and anxiety were the only othercomparable behaviors across two of the three studiesand were both significant predictors of distressCovinsky et al (2003) did not use a formal behaviorscale but identified that anger and aggressivebehaviors were stronger predictors of caregiverdepression followed by dangerous behaviors to selfand others and then behaviors which wake thecaregiver up at night
Discussion
To our knowledge this is the first review to controlfor the effect of multiple BPSD on caregiver well-being by discriminating between individual BPSDand also discriminating between caregiver outcomesof well-being Additional advantages of this reviewwere the use of a formal method of synthesis andthe decision to distinguish between how BPSD andcaregiver well-being are measured which ensuredvalid conclusions were drawn by only synthesizing
comparable data Only two meta-analyses werepossible due to limited homogeneous studiesCategories in which the relationship betweenBPSD and well-being were qualitatively examinedincluded minimal studies displaying considerablevariation therefore valid conclusions could not bedrawn The results are discussed in the context ofprevious research
Meta-analysis of mean distress scoresAs seen in Figures 2 and 3 even within one measureand one criterion (distress associated with totalscore on the NPI) variability in distress ratingsfor each symptom can be seen between the 16studies This was also evident in research conductedby Fauth and Gibbons (2014) in which a widevariation in the prevalence of NPI symptoms wasseen between studies However data regardingdistress associated with euphoria and delusionsdemonstrated high levels of variance in terms of theratio between the mean and the standard deviationresulting in considerable variability between scoresTherefore the ratio of the mean distress ratingscompared with the standard deviation associatedwith the other ten behaviors signifies that there islow variance between the 16 studies It is unclearat present why there is increased variability foreuphoric and delusional behaviors In terms of totalscore depression followed by agitationaggressionand apathy were found to be the most distressingfor caregivers across 16 studies in the meta-analysis(Figure 3) This suggests that it is mood-relatedbehaviors which are associated with increaseddistress Fauth and Gibbons (2014) examinedthe relationship between total score of BPSD
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1768 A Feast et al
and distress and found similar results howevereven with identical analysis there were noteworthydiscrepancies such as delusions being the mostdistressing but only the fourth most distressing inthe current review Consistent with the currentmeta-analysis of mean data apathy and depression-related behaviors have been reported as distressingin numerous studies (Teri 1997 deVugt et al2003 Aarsland et al 2007 Kosberg et al 2007)Similarly depression in the person with dementia isassociated with depression in the caregiver (Waiteet al 2004)
Meta-analysis of correlation dataAs seen in Table 1 there were high levels ofheterogeneity between the studies included in thesecond meta-analysis investigating which behaviorswere associated with distress Only apathy- andsleep-related behaviors displayed homogeneitybetween studies Furthermore behaviors which hadstronger correlations with distress (Table 1) didnot have strong associations in the previous meta-analysis (Figure 3) regarding distress associatedwith behaviors At present it is unclear why thisdiscrepancy exists and also why distress correlatedwith apathy- and sleep-related behaviors is more ho-mogenous between studies than the other behaviorsSince only a few studies contributed to this meta-analysis more research is needed to investigate thepooled effects Nevertheless a meta-analysis of thisnature has not been performed previously and therandom-effects model was used to report a moreconservative estimate for the heterogeneous pooledeffects in order to reduce bias
Apathy and irritable behaviors were not con-sistently significantly correlated to burden acrossmultiple studies whereas delusions agitationdisinhibition and appetiteeating change werethese associations were also reported in otherstudies (Rymer et al 2002 Rocca et al 2010) Incontrast a review by Ornstein and Gaugler (2012)reported that angeraggression and depression werethe most frequently cited BPSD associated withcaregiver burden depression was also linked tocaregiver burden in a review by Black and Almeida(2004) In addition to burden delusional behaviorwas consistently associated with distress acrossstudies with a significant correlation also beingseen with stress (Kosmala and Kloszewska 2004)Berger et al (2005) noted that behaviors whichare significantly correlated with burden are notcorrelated with depression This demonstrates theimportance of including multiple measures of well-being since the same behaviors affect caregiversdifferently which has implications for futureinterventions
Studies unamenable to quantitative synthesisOnly two studies reported the prevalence of BPSDand the impact on caregiver well-being due todifferences between studies comparisons werenot possible Although five studies reported thefrequency of BPSD each measure of caregiver well-being was different Memory-related behaviorsverbal aggression incontinence and irritabilitywere reported to affect well-being across multiplestudies These findings were also seen in previousresearch (Bruce and Paterson 2000 Farran et al2004) However Fauth and Gibbons (2014) andRobinson et al (2001) did not find that memory-related behaviors were distressing despite being themost frequent type of behavior on the RMBPCHallucinations sexual disinhibition and physicalaggression were consistently reported to affect well-being less than the other behaviors Although thisfinding is reflected in the majority of studies Haleyet al (2008) and Arango-Lasprilla et al (2010)reported contradictory results
It is noteworthy that aggressionagitation whenmeasured in terms of total score was reported asthe second most distressing across 16 of the studiesbut when measured in terms of frequency only oneof the three studies reported physical aggressionas a common problem However the frequency ofverbal aggression consistently affected well-beingIt is not possible to provide an explanation for thisdiscrepancy but it may be because of the distinctionbetween how aggressionagitation is measured (ietotal score or frequency) or that verbal and physicalaggression have been differentiated and thereforeaffect caregiver well-being differently
Predictive data were limited and heterogeneousin the present review however it was possible toconclude that apathy predicted burden and distressacross studies Anger restlessness combativenessdangerous to others and embarrassing behaviorwere found to be strong predictors of burden ina study by Gaugler et al (2011) Only one studyreported the predictors of caregiver depression
Potential explanations for variability incaregiver well-beingDifference in study quality does not appear to be anexplanation for the variation in distress rating acrossstudies since even between two medium qualitystudies there was considerable variation (Balieiroet al 2010 displaying one of the highest meandistress scores Baiyewu et al 2003 displayingone of the lowest) Two studies consistently hadthe highest mean distress rating across each of thebehavior domains Balieiro et al (2010) and Tanet al (2005) Both of these studies were clinic-basedhigher distress ratings would be expected as those
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1769
experiencing more BPSD might be more likely toattend a clinic as indeed were the majority ofstudies included in the meta-analysis It may bepossible that dementia severity is an explanationsince participants in the studies with the highestdistress scores (Tan et al 2005 Balieiro et al 2010)had moderate and severe dementia respectivelywhereas Baiyewu et al (2003) who consistentlyreported the lowest distress scores across eachof the behavior domains included participantswith mild dementia However both Aarslandet al (2007) and de Vugt et al (2006) reportedlower mean distress scores in comparison with theother included studies and they both includedparticipants with moderate dementia FurthermoreDavidsdottir et al (2012) found that there wasno significant difference between caregiver distressscores depending on dementia severity
Baiyewu et al (2003) had a much smallersample of spousal caregivers in comparison to Tanet al (2005) which might account for the lowerdistress scores This is in agreement with Almberget al (1997) who reported that spouses experiencegreater levels of burden However three studieswhich had consistently higher mean distress scoresacross all behaviors (Tan et al 2005 Balieiro et al2010 Huang et al 2012) were mainly comprisedof adult-child caregivers When comparing a studysolely comprised of spousal caregivers (deVugt et al2006) with a study (Baiyewu et al 2003) withminimal spousal caregivers (25) it was possibleto see that spousal caregivers were substantiallymore distressed with depressive apathetic andanxiety-related behaviors Although distress ratingscan be differentiated between behavior types forspousal and non-spousal caregivers both Baiyewuet al (2003) and de Vugt et al (2006) had two of thelowest distress scores across all behaviors in compar-ison to the other studies in the meta-analysis
The explanation may also be cultural sinceBaiyewu et al (2003) and Baiyewu et al (2012)(with similarly low distress scores across behaviors)were the only Africa-based studies in the meta-analysis Baiyewu et al (2003) and Baiyewu et al(2012) were also both community-based studieswhich may also be a reason for the reduceddistress ratings There is every reason to believethat BPSD are present across cultures (Shajiet al 2009) however the low levels of publicawareness of dementia have many implications(Prince 2000) One of these implications maybe the misinterpretation of BPSD as deliberateconsequently affecting the well-being of the carer(Shaji et al 2009) It is beyond the scope ofthis paper to determine why there is considerablevariation between studies reporting caregiverdistress for identical behaviors using identical
measures However it is likely that it is the caregivercharacteristics rather than the characteristics of theperson with dementia (such as dementia severity)which may underlie the explanation as to whyvariation between studies exists
Limitations
The data available for this review allowed for onlytwo meta-analyses to be conducted There wererelatively few studies which assessed the relationshipbetween individual BPSD and caregiver well-beingand which met the inclusionexclusion criteriafor the review In an attempt to be systematicbased on prior recommendation an effort wasmade to distinguish between how ldquoproblematicrdquosymptoms are measured Consequently studieswere categorized into whether BPSD weremeasured in terms of frequency or prevalence andalso categorized in terms of the statistical analysisemployed Other than data regarding mean distressassociated with NPI total score only a small amountof studies were included in each category andunfortunately it was often the case that measuresof caregiver well-being were dissimilar From the 40included studies there were 12 different measuresof behavior and 17 different measures of well-being making comparisons difficult which mayhave contributed to the inconsistent findings
The majority of included studies recruitedparticipants from clinics therefore caregiversincluded in the review were not representative ofthe population In addition the samples across theincluded studies were heterogeneous in a numberof factors therefore caution should be taken wheninterpreting the results Although beyond the scopeof this review study characteristics such as culturegender and relationship direction were not ex-amined through subgroup analyses Due to the lim-ited number of studies it was not possible to imposea quality criteria however all included studies wereeither of high or medium quality as assessed by theDowns and Back Checklist (1998) Furthermore allof the included studies relied on caregiver reportsof BPSD which may themselves be affected bycaregiver well-being unfortunately it is not possibleto determine if this was the case Nonetheless twovalid meta-analyses were completed and a numberof comments can be made about the relationshipbetween BPSD and caregiver well-being
Implications and recommendations
The vast majority of studies addressing the rela-tionship between BPSD and caregiver well-being
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1770 A Feast et al
did not examine individual BPSD Consequentlythis comparatively limited the amount of studiesincluded in the present review Therefore if we areto understand this relationship more studies needto examine individual BPSD in their research Inaddition it is more clinically relevant to examinewhich BPSD affect well-being rather than BPSDas a whole as this is essential in determiningwhere clinical staff should allocate resources mosteffectively Nevertheless there is preliminary datasuggesting it is mood-related behaviors whichare associated with increased levels of distresstherefore interventions for the management ofBPSD should target these behaviors
The lack of consistency in the measurementof BPSD (neuropsychiatric or memory problemsfrequency or prevalence) and the measurementof caregiver well-being (the use of interchangeableterminology such as stress strain and burdenmeaning the same construct) limits our ability toreach a consensus as to which BPSD result inthe most negative outcomes for caregivers Forexample Donaldson et al (1998) used GilleardrsquosStrain Scale (1984) to measure burden andthe General Health Questionnaire (Goldberg andHillier 1979) to measure distress Furthermorefour studies (see Table S1) did not have formalscales to measure the impact of BPSD on well-being and used terms such as ldquoburdensomerdquoldquoseriousrdquo and ldquodisturbingrdquo This problem impactsupon the validity and reliability of the originalstudies and consequently the review Howeverthis mainly occurred in the earlier studies Futureresearch should also include more than one measureof well-being in order to identify if individual BPSDdifferentially affect caregiver burden compared tocaregiver distress as identified in the current reviewFurthermore future research should identify whythere is reduced variability in distress ratings forcertain behaviors compared to others and whycertain behaviors are more distressing dependingon which type of statistical analysis is used
Although there are potential methodologicalreasons (limited studies inconsistent measures)for why there is substantial variability whenidentifying which BPSD affect certain types ofcaregiver well-being the most there is growingevidence that factors associated with the personwith dementia (eg BPSD frequency cognition) areonly part of the story when explaining a caregiverrsquosresponse to BPSD Caregiver characteristicshave been shown to account for twice thevariance of person with dementia characteristicswhen reporting neuropsychiatric symptoms (Sinket al 2006) and the presence of BPSD wasnot found to be a significant predictor ofburden whereas caregiver characteristics such as
confidence neuroticism and relationship qualitywere significant predictors (Campbell et al 2008)Therefore as recommended by Ornstein andGaugler (2012) future studies should focus onidentifying pathways for the association betweenindividual BPSD caregiver variables and caregiveroutcomes More research is needed to understandif and why certain BPSD affect certain caregiveroutcomes and also how much of this is attributableto caregiver variability in response to BPSD ratherthan the presence of BPSD itself More longitudinalstudies would be useful to examine how changes inindividual BPSD are associated with caregiver well-being over time A review by Black and Almeida(2004) examined the limited longitudinal studiesavailable and reported mixed findings betweenburden and BPSD and found no associationbetween BPSD and distress Although BPSDincreased significantly over a two-year periodcaregiver burden remained stable and depressionwas found to decrease (Berger et al 2005) Futureresearch needs to examine caregiver factors overtime (well-being role captivity etc) along withchanges in individual BPSD in order to have a morevalid understanding of this relationship
Caution should be exercised when creating ameasure of BPSD since Jackson et al (2014)found that the Revised Memory and BehaviorProblem Checklist (Teri et al 1992) might bemore suitable in explaining caregiver depressionthan the NPI It is important that the measureof BPSD is not biased toward explaining a moreunique association between BPSD and a measure ofcaregiver well-being such as depression As stated byGitlin and Rose (2014) item selection for measuresof BPSD is often based upon specific disciplines(eg neurology psychiatry social sciences) andthus implicitly represents different conceptual-izations of behavior A shared framework fordefining behaviors and their underlying causesmust be created in order to move on fromthe implicit assumption of most measures thatbehaviors are a direct cause of neuropathologyand to develop measures which also address thecontextual and caregiver characteristics associatedwith the behavior
Conclusions
This study has improved our understanding of theimpact of individual BPSD on caregiver well-beingin particular caregiver distress The relationshipbetween individual BPSD and caregiver well-beingwas inconsistent and varied according to behavioralsymptom Due to limited studies and heterogeneousdata the results should be interpreted with caution
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1771
but advances have been made with respect towhich behaviors are associated with distress Theinconsistencies may be partly explained by caregivervariables which were not taken into account inthe review Based on this review and previousresearch it is not possible to fully understand therelationship between BPSD and caregiver well-being without examining the influence of caregivervariables such as caregiver strategies acceptancegender relationship with person with dementiaand confidence We recommend that future studiesare designed to examine individual BPSD ratherthan BPSD as a whole use consistent measures forBPSD and well-being use consistent terminologyfor psychological constructs (eg burden) andexamine the causal mechanisms by which individualBPSD impact caregiver well-being by collectingdata on a range of caregiver factors Theseapproaches will clarify whether it is important forclinicians to focus on the frequency or prevalence ofcertain BPSD in addition to targeting the presenceof certain caregiver characteristics and addressingunmet need
Conflict of interest
None
Description of authorsrsquo roles
A Feast was responsible for developing the reviewobjectives writing the search strategies conductingthe searches designing and completing studyeligibility and data extraction forms undertakingthe quality appraisals conducting the meta-analysisand writing the paper M Orrell was responsible fordeveloping the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper C Stoner was responsible forundertaking the quality appraisals and assisting inwriting the paper G Charlesworth was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper E Moniz-Cook was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper
Acknowledgments
We would like to thank Dr Zoeuml Hoare for herstatistical advice This paper presents independentresearch funded by the National Institute for HealthResearch (NIHR) under its Programme Grants forApplied Research (RP-PG-0606-1067 and RP-PG-
060- 1083) The views expressed in this publicationare those of the author(s) and not necessarily thoseof the NHS the NIHR or the Department ofHealth
Supplementary Material
To view supplementary material for thisarticle please visit httpdxdoiorg101017S1041610216000922
References
Aarsland D et al (2007) Neuropsychiatric symptoms inpatients with Parkinsonrsquos disease and dementia frequencyprofile and associated care giver stress Journal of NeurologyNeurosurgery amp Psychiatry 78 36ndash42doihttpdxdoiorg101136jnnp2005083113
Allegri R F et al (2006) Neuropsychiatric symptoms as apredictor of caregiver burden in Alzheimerrsquos diseaseNeuropsychiatric Disease amp Treatment 2 105ndash110doi102147ndts47133
Almberg B Grafstrom M and Winblad B (1997)Major strain and coping strategies as reported by familymembers who care for aged demented relatives Journal ofAdvanced Nursing 26 683ndash691doihttpdxdoiorg101046j1365-2648199700392x
Arango-Lasprilla J C Lehan T Drew A MorenoA Deng X and Lemos M (2010) Health-relatedquality of life in caregivers of individuals with dementiafrom Colombia American Journal of Alzheimerrsquos Disease andOther Dementias 25 556ndash561doi1011771533317510382287ltbibgt
Baiyewu O et al (2003) Behavioral and caregiver reactionof dementia as measured by the neuropsychiatric inventoryin Nigerian community residents InternationalPsychogeriatrics 15 399ndash409doi101017s1041610203009645
Baiyewu O et al (2012) Behavioral symptoms incommunity-dwelling elderly Nigerians with dementia mildcognitive impairment and normal cognition InternationalJournal of Geriatric Psychiatry 27 931ndash939 doihttpdxdoiorg101002gps2804
Balieiro A P Jr Sobreira E S T Pena M C SSilva-Filho J H and Vale F A C (2010) Caregiverdistress associated with behavioral and psychologicalsymptoms in mild Alzheimerrsquos disease Dementia eNeuropsychologia 4 238ndash244
Ballard C G et al (1995) The aetiology of depression inthe carers of dementia sufferers Journal of AffectiveDisorders 35 59ndash63 doi1010160165-0327(95)00041-k
Bandeira D R Pawlowski J Goncalves T RHilgert J B Bozzetti M C and Hugo F N (2007)Psychological distress in Brazilian caregivers of relativeswith dementia Aging and Mental Health 11 14ndash19doi10108013607860600640814
Berger G Bernhardt T Weimer E Peters JKratzsch T and Frolich L (2005) Longitudinal studyon the relationship between symptomatology of dementia
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1772 A Feast et al
and levels of subjective burden and depression amongfamily caregivers in memory clinic patients Journal ofGeriatric Psychiatry and Neurology 3 119ndash128doi1011770891988704273375
Black W and Almeida O P (2004) A systematic reviewof the association between the behavioral and psychologicalsymptoms of dementia and burden of care InternationalPsychogeriatrics 16 295ndash315doi101017s1041610204000468
Bruce D G and Paterson A (2000) Barriers tocommunity support for the dementia carer a qualitativestudy International Journal of Geriatric Psychiatry 15451ndash457 doi101002(sici)1099-1166(200005)155lt451aid-gps143gt30co2-k
Campbell P et al (2008) Determinants of burden in thosewho care for someone with dementia International Journalof Geriatric Psychiatry 23 1078ndash1085doi101002gps2071
Cerejeira J Lagarto L and Mukaetova-LadinskaE B (2012) Behavioral and psychological symptoms ofdementia Frontiers in Neurology 3 1ndash23doi103389fneur201200073
Chappell N L and Penning M (1996) Behaviouralproblems and distress among caregivers of people withdementia Ageing amp Society 16 57ndash73doi101017s0144686x00003135
Chiu Y C et al (2014) Family caregiversrsquo sleepdisturbance and its associations with multilevel stressorswhen caring for patients with dementia Aging amp MentalHealth 18 92ndash101 doihttpdxdoiorg101080136078632013837141
Cohen J (1988) Statistical Power Analysis for the BehavioralSciences 2nd edn New York University New YorkLawrence Erlbaum Associatesdoi1043249780203771587
Conde-Sala J L Garre-Olmo J Turroacute-Garriga OVilalta-Franch J and Loacutepez-Pousa S (2010)Differential features of burden between spouse andadult-child caregivers of patients with Alzheimerrsquos diseasean exploratory comparative design International Journal ofNursing Studies 47 1262ndash1273doi101016jijnurstu201003001
Covinsky K E et al (2003) Patient and caregivercharacteristics associated with depression in caregivers ofpatients with dementia Journal of General Internal Medicine18 1006ndash1014 doihttpdxdoiorg101111j1525-1497200330103x
Craig D Mirakhur A Hart D J McIlroy S P andPassmore A P (2005) A cross-sectional study ofneuropsychiatric symptoms in 435 patients withAlzheimerrsquos disease American Journal of GeriatricPsychiatry 13 460ndash468 doi10109700019442-200506000-00004
Crellin N Charlesworth G and Orrell M (2014)Measuring family caregiver efficacy for managing behavioraland psychological symptoms in dementia a psychometricevaluation International Psychogeriatrics 26 93ndash103 doihttpdxdoiorg101017s1041610213001646
Davidsdottir S R Snaedal J Karlsdottir GAtladottir I and Hannesdottir K (2012) Validationof the Icelandic version of the neuropsychiatric inventorywith caregiver distress (NPI-D) Nordic Journal of
Psychiatry 66 26ndash32 doihttpdxdoiorg103109080394882011593100
Davis J D and Tremont G (2007) Impact of frontalsystems behavioral functioning in dementia on caregiverburden The Journal of Neuropsychiatry and ClinicalNeurosciences 19 43ndash49 doihttpdxdoiorg101176jnp200719143
de Vugt M E Riedijk S R Aalten P Tibben Avan Swieten J C and Verhey F R J (2006) Impactof behavioural problems on spousal caregivers acomparison between Alzheimerrsquos disease andfronto-temporal dementia Dementia and Geriatric CognitiveDisorders 22 35ndash41 doi101159000093102
de Vugt M E et al (2003) Behavioural disturbances indementia patients and quality of the marital relationshipInternational Journal of Geriatric Psychiatry 18 149ndash154doi101002gps807
Donaldson C Tarrier N and Burns A (1998)Determinants of carer stress in Alzheimerrsquos diseaseInternational Journal of Geriatric Psychiatry 13 248ndash256doi101002(sici)1099-1166(199804)134lt248aid-gps770gt30co2-0
Downs S and Black N (1998) The feasibility of creating achecklist for the assessment of the methodological qualityboth of randomised and non-randomised studies of healthcare interventions Journal of Epidemiological CommunityHealth 52 377ndash384 doi101136jech526377
Farran C J Loukissa D A Lindeman D A andMcCann J (2004) Caring for self while caring for othersthe two-track life of coping with Alzheimerrsquos diseaseJournal of Gerontological Nursing 30 38ndash45doi1039280098-9134-20040501-09
Fauth E B and Gibbons A (2014) Which behavioral andpsychological symptoms of dementia are the mostproblematic Variability by prevalence intensity distressratings and associations with carer depressive symptomsInternational Journal of Geriatric Psychiatry 29 263ndash271doi101002gps4002
Fuh J L Liu C K Mega M S Wang S J andCummings J L (2001) Behavioral disorders andcaregiversrsquo reaction in Taiwanese patients with Alzheimerrsquosdisease International Psychogeriatrics 13 121ndash128 doihttpdxdoiorg101017s1041610201007517
Gaugler J E et al (2011) Does caregiver burden mediatethe effects of behavioral disturbances on nursing homeadmission The American Journal of Geriatric Psychiatry 19497ndash506 doi101097jgp0b013e31820d92cc
Gilleard C J Belford H Gilleard E Whittick J Eand Gledhill K (1984) Emotional distress amongst thesupporters of the elderly mental infirm British Journal ofPsychiatry 145 172ndash177doihttpdxdoiorg101192bjp1452172
Gitlin L N and Rose K (2014) Factors associated withcarer readiness to use nonpharmacologic strategies tomanage dementia-related behavioral symptomsInternational Journal of Geriatric Psychiatry 29 93ndash102doihttpdxdoiorg101002gps3979
Goldberg D P and Hillier V F (1979) A scaled versionof the general health questionnaire Psychological Medicine9 139ndash145 doi101017s0033291700021644
Gonzalez-Salvador M T Arango C Lyketsos C Gand Barba A C (1999) The stress and psychological
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1773
morbidity of the Alzheimer patient caregiver InternationalJournal of Geriatric Psychiatry 14 701ndash710doi101002(sici)1099-1166(199909)149lt701aidps5gt30co2-
Haley W E Brown S and Levine E G (1987) Familycaregiver appraisals of patient behavioral disturbance insenile dementia Clinical Gerontologist The Journal of Agingand Mental Health 6 25ndash34doi101300j018v06n04_04
Haley W E Levine E G Brown S L Berry J Wand Hughes G H (2008) The psychological social andhealth consequences of caring for a relative with seniledementia Journal of the American Geriatrics Society 35405ndash411 doi101111j1532-54151987tb04661x
Hishikawa N et al (2012) Effects of turmeric onAlzheimerrsquos disease with behavioral and psychologicalsymptoms of dementia Ayu 33 499ndash504 doihttpdxdoiorg1041030974-8520110524
Huang S S Lee M C Liao Y C Wang W F andLai T J (2012) Caregiver burden associated withbehavioral and psychological symptoms of dementia(BPSD) in Taiwanese elderly Archives of Gerontology andGeriatrics 55 55ndash59 doihttpdxdoiorg101016jarchger201104009
Jackson M A Fauth E B and Geiser C (2014)Comparing the neuropsychiatric inventory and the revisedmemory and behavior problems checklist for associationswith caregiver burden and depressive symptomsInternational Psychogeriatrics 26 1021ndash1031doi101017s1041610213002421
Johnson D K Niedens M Wilson J RSwartzendruber L Yeager A and Jones K (2013)Treatment outcomes of a crisis intervention program fordementia with severe psychiatric complications the Kansasbridge project The Gerontologist 53 102ndash112 doihttpdxdoiorg101093gerontgns104
Khoo S A Chen T Y Ang Y H and Yap P (2013)The impact of neuropsychiatric symptoms on caregiverdistress and quality of life in persons with dementia in anAsian tertiary hospital memory clinic InternationalPsychogeriatrics 25 1991ndash1999 doihttpdxdoiorg101017s1041610213001518
Kosberg J I Kaufman A V Burgio L D Leeper Jand Sun F (2007) Family caregiving to those withdementia in rural Alabama racial similarities anddifferences Journal of Aging and Health 19 3ndash21 doi1011770898264306293604
Kosmala K and Kloszewska I (2004) The burden ofproviding care for Alzheimerrsquos disease patients in PolandInternational Journal of Geriatric Psychiatry 19 191ndash193doi101002gps1054
Landis J R and Koch G G (1977) The measurement ofobserver agreement for categorical data Biometrics 33159ndash174 doi 1023072529310
Lee D R McKeith I Mosimann U Ghosh-NodyalA and Thomas A J (2013) Examining carer stress indementia the role of subtype diagnosis andneuropsychiatric symptoms International Journal ofGeriatric Psychiatry 28 135ndash141 doihttpdxdoiorg101002gps3799
Lim Y M Son G R Song J A and Beattie E(2008) Factors affecting burden of family caregivers of
community-dwelling ambulatory elders with dementia inKorea Archives of Psychiatric Nursing 22 226ndash234 doi101016japnu200712005
Matsumoto N et al (2007) Caregiver burden associatedwith behavioral and psychological symptoms of dementia inelderly people in the local community Dementia andGeriatric Cognitive Disorders 23 219ndash224doi101159000099472
Mohamed S Rosenheck R Lyketsos C G andSchneider L S (2010) Caregiver burden in Alzheimerdisease cross-sectional and longitudinal patient correlatesThe American Journal of Geriatric Psychiatry 18 917ndash927doi101097jgp0b013e3181d5745d
Mourik J C Rosso S M Niermeijer M FDuivenvoorden H J Van Swieten J C and TibbenA (2004) Frontotemporal dementia behavioral symptomsand caregiver distress Dementia and Geriatric CognitiveDisorders 18 299ndash306 doihttpdxdoiorg101159000080123
Muangpaisan W et al (2010) Caregiver burden and needsof dementia caregivers in Thailand a cross-sectional studyJournal of the Medical Association of Thailand 93 601ndash607
Neundorfer M M McClendon M J Smyth K AStuckey J C Strauss M E and Patterson M B(2001) A longitudinal study of the relationship betweenlevels of depression among persons with Alzheimerrsquosdisease and levels of depression among their familycaregivers Journal of Gerontology Series B - PsychologicalSciences and Social Sciences 56 301ndash313
Nygaard H A (1998) Strain on caregivers of dementedelderly people living at home Scandinavian Journal ofPrimary Health Care 6 33ndash37doihttpdxdoiorg10310902813438809009287
Ornstein K and Gaugler J E (2012) The problem withldquoproblem behaviorsrdquoa systematic review of the associationbetween individual patient behavioral and psychologicalsymptoms and caregiver depression and burden within thedementia patientndashcaregiver dyad InternationalPsychogeriatrics 24 1536ndash1552doi101017s1041610212000737
Ornstein K Gaugler J E Devanand N S CarolynZ and Yaakov S (2012) The differential impact ofunique behavioral and psychological symptoms for thedementia caregiver how and why do patientsrsquo individualsymptom clusters impact caregiver depressive symptomsThe American Journal of Geriatric Psychiatry 12 77ndash1286doi httpdxdoiorg101016jjagp201301062
Price G R (1970) Selection and covariance Nature 227520ndash521 doi101038227520a0
Prince M (2000) Dementia in developing countries Aconsensus statement from the 1066 Dementia ResearchGroup International Journal of Geriatric Psychiatry 1514ndash20 doihttpdxdoiorg101002(sici)1099-1166(200001)151lt14aid-gps70gt30co2-8
Quayhagen M P and Quayhagen M (1998) Alzheimerrsquosstress coping with the caregiving role Gerontologist 28391ndash396 doihttpdxdoiorg101093geront283391
Reisberg B Ferris S H de Leon M J and Crook T(1982) The global deterioration scale for assessment ofprimary degenerative dementia American Journal ofPsychiatry 139 1136ndash1139 doihttpdxdoiorg101176ajp13991136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1774 A Feast et al
Robinson K M Adkisson P and Weinrich S (2001)Problem behaviour caregiver reactions and impact amongcaregivers of persons with Alzheimerrsquos disease Journal ofAdvanced Nursing 36 573ndash582 doihttpdxdoiorg101046j1365-2648200102010x
Rocca P et al (2010) Neuropsychiatric symptomsunderlying caregiver stress and insight in Alzheimerrsquosdisease Dementia and Geriatric Cognitive Disorders 3057ndash63 doi101159000315513
Rymer S Salloway S Norton L Mallow PCorreia S and Monast D (2002) Impaired awarenessbehavior disturbance and caregiver burden in Alzheimerdisease Alzheimer Disease and Associated Disorders 16248ndash253 doi 10109700002093-200210000-00006
Savorani G Vulcano V Boni S Sarti G andRavaglia G (1998) Behavioral disorders in dementiapatients and their impact on the stress of caregivingrelatives the ldquoARADrdquo questionnaire Archives ofGerontology and Geriatrics 6 481ndash485doi101016s0167-4943(98)80070-8
Shaji K S George R K Prince M J and JacobK S (2009) Behavioral symptoms and caregiver burdenin dementia Indian Journal of Psychiatry 51 45 doihttpdxdoiorg1041030019-554544905
Sink K M Covinsky K E Barnes D E NewcomerR J and Yaffe K (2006) Caregiver characteristics areassociated with neuropsychiatric symptoms of dementiaJournal of the American Geriatrics Society 54 796ndash803 doi101111j1532-5415200600697x
Slachevsky A et al (2013) The CUIDEME studydeterminants of burden in chilean primary caregivers ofpatients with dementia Journal of Alzheimerrsquos Disease 35297ndash306
Spiegel R et al (1991) A new behavioral assessment scalefor geriatric out- and in-patients the NOSGER (nursesrsquoobservation scale for geriatric patients) Journal of theAmerican Geriatric Society 39 339ndash347 doihttpdxdoiorg101111j1532-54151991tb02897x
Tan L L Wong H B and Allen H (2005) The impactof neuropsychiatric symptoms of dementia on distress infamily and professional caregivers in SingaporeInternational Psychogeriatrics 17 253ndash263 doi101017s1041610205001523
Teri L (1997) Behavior and caregiver burden behavioralproblems in patients with Alzheimer disease and itsassociation with caregiver distress Alzheimer Disease andAssociated Disorders 11 35ndash38
Teri L Truax P Logsdon R Uomoto J Zarit Sand Vitaliano P P (1992) Assessment of behavioralproblems in dementia the revised memory and behaviorproblems checklist Psychology and Aging 7 622 doi1010370882-797474622
Waite A Bebbington P Skelton-Robinson M andOrrell M (2004) Social factors and depression in carersof people with dementia International Journal of GeriatricPsychiatry 19 582ndash587 doihttpdxdoiorg101002gps1136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at

Individual BPSD and caregiver well-being 1767
Table 1 Meta-analysis of mean distress scores correlated with behaviors using NPI total scores
P O O L E D C O R RELATION COEFFI CIENT T EST F OR HETEROGENEITY
FI XE D-E FF E C T S RANDOM-E FF E C T S
BEHAVIOR N MODEL (95 CI) MODEL (95 CI) I2 95 CI P
Delusions 243 0557 (0462 to 0640) 0567 (0412 to 0690) 5864 000 to 8623 p = 00643Hallucinations 243 0502 (0399 to 0532) 0520 (0198 to 0791) 8771 7081 to 9482 p lt 00001AgitationAggression 243 0540 (0443 to 0625) 0537 (0299 to 0712) 7941 4517 to 9482 p = 00022Depression 243 0528 (0429 to 0615) 0564 (0360ndash0717) 7465 2949 to 9089 p = 00080Anxiety 243 0482 (0377 to 0575) 0481 (0236 to 0669) 7845 4203 to 9199 p = 00030Euphoria 243 0540 (0443 to 0625) 0480 (0147 to 0715) 8764 7061 to 9480 p lt 00001Apathy 243 0456 (0351 to 0554) 0459 (0351 to 0540) 000 000 to 8423 p = 04834Disinhibition 243 0357 (0240 to 0464) 0371 (0162 to 0548) 6574 000 to 8833 p = 00327Irritability 243 0668 (0590 to 0733) 0691 (0486 to 0823) 8281 5601 to 9329 p = 00006Aberrant motor
behavior243 0606 (0518 to 0681) 0603 (0437 to 0730) 6764 371 to 8871 p = 00280
Sleep 176 0438 (0307 to 0552) 0436 (0301 to 0554) 532 000 to 9682 p = 03478Appetite and eating 176 0405 (0271 to 0523) 0442 (0200 to 0633) 6617 000 to 9026 p = 00520
Predictive data between BPSD and well-beingConde-Sala et al (2010) Chappell and Penning(1996) Davis and Tremont (2007) and Slachevskyet al (2013) used the same burden measurebut used different measures of BPSD Apathysignificantly predicted burden across three studiesalthough it was less burdensome for adult-childcaregivers and did not predict apathy in the study byDavis and Tremont (2007) Three studies (Mouriket al 2004 Khoo et al 2013 Lee et al 2013)reported data identifying which behaviors predicteddistress as measured by the NPI Apathy wasa significant predictor across two of the threestudies Delusions and anxiety were the only othercomparable behaviors across two of the three studiesand were both significant predictors of distressCovinsky et al (2003) did not use a formal behaviorscale but identified that anger and aggressivebehaviors were stronger predictors of caregiverdepression followed by dangerous behaviors to selfand others and then behaviors which wake thecaregiver up at night
Discussion
To our knowledge this is the first review to controlfor the effect of multiple BPSD on caregiver well-being by discriminating between individual BPSDand also discriminating between caregiver outcomesof well-being Additional advantages of this reviewwere the use of a formal method of synthesis andthe decision to distinguish between how BPSD andcaregiver well-being are measured which ensuredvalid conclusions were drawn by only synthesizing
comparable data Only two meta-analyses werepossible due to limited homogeneous studiesCategories in which the relationship betweenBPSD and well-being were qualitatively examinedincluded minimal studies displaying considerablevariation therefore valid conclusions could not bedrawn The results are discussed in the context ofprevious research
Meta-analysis of mean distress scoresAs seen in Figures 2 and 3 even within one measureand one criterion (distress associated with totalscore on the NPI) variability in distress ratingsfor each symptom can be seen between the 16studies This was also evident in research conductedby Fauth and Gibbons (2014) in which a widevariation in the prevalence of NPI symptoms wasseen between studies However data regardingdistress associated with euphoria and delusionsdemonstrated high levels of variance in terms of theratio between the mean and the standard deviationresulting in considerable variability between scoresTherefore the ratio of the mean distress ratingscompared with the standard deviation associatedwith the other ten behaviors signifies that there islow variance between the 16 studies It is unclearat present why there is increased variability foreuphoric and delusional behaviors In terms of totalscore depression followed by agitationaggressionand apathy were found to be the most distressingfor caregivers across 16 studies in the meta-analysis(Figure 3) This suggests that it is mood-relatedbehaviors which are associated with increaseddistress Fauth and Gibbons (2014) examinedthe relationship between total score of BPSD
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1768 A Feast et al
and distress and found similar results howevereven with identical analysis there were noteworthydiscrepancies such as delusions being the mostdistressing but only the fourth most distressing inthe current review Consistent with the currentmeta-analysis of mean data apathy and depression-related behaviors have been reported as distressingin numerous studies (Teri 1997 deVugt et al2003 Aarsland et al 2007 Kosberg et al 2007)Similarly depression in the person with dementia isassociated with depression in the caregiver (Waiteet al 2004)
Meta-analysis of correlation dataAs seen in Table 1 there were high levels ofheterogeneity between the studies included in thesecond meta-analysis investigating which behaviorswere associated with distress Only apathy- andsleep-related behaviors displayed homogeneitybetween studies Furthermore behaviors which hadstronger correlations with distress (Table 1) didnot have strong associations in the previous meta-analysis (Figure 3) regarding distress associatedwith behaviors At present it is unclear why thisdiscrepancy exists and also why distress correlatedwith apathy- and sleep-related behaviors is more ho-mogenous between studies than the other behaviorsSince only a few studies contributed to this meta-analysis more research is needed to investigate thepooled effects Nevertheless a meta-analysis of thisnature has not been performed previously and therandom-effects model was used to report a moreconservative estimate for the heterogeneous pooledeffects in order to reduce bias
Apathy and irritable behaviors were not con-sistently significantly correlated to burden acrossmultiple studies whereas delusions agitationdisinhibition and appetiteeating change werethese associations were also reported in otherstudies (Rymer et al 2002 Rocca et al 2010) Incontrast a review by Ornstein and Gaugler (2012)reported that angeraggression and depression werethe most frequently cited BPSD associated withcaregiver burden depression was also linked tocaregiver burden in a review by Black and Almeida(2004) In addition to burden delusional behaviorwas consistently associated with distress acrossstudies with a significant correlation also beingseen with stress (Kosmala and Kloszewska 2004)Berger et al (2005) noted that behaviors whichare significantly correlated with burden are notcorrelated with depression This demonstrates theimportance of including multiple measures of well-being since the same behaviors affect caregiversdifferently which has implications for futureinterventions
Studies unamenable to quantitative synthesisOnly two studies reported the prevalence of BPSDand the impact on caregiver well-being due todifferences between studies comparisons werenot possible Although five studies reported thefrequency of BPSD each measure of caregiver well-being was different Memory-related behaviorsverbal aggression incontinence and irritabilitywere reported to affect well-being across multiplestudies These findings were also seen in previousresearch (Bruce and Paterson 2000 Farran et al2004) However Fauth and Gibbons (2014) andRobinson et al (2001) did not find that memory-related behaviors were distressing despite being themost frequent type of behavior on the RMBPCHallucinations sexual disinhibition and physicalaggression were consistently reported to affect well-being less than the other behaviors Although thisfinding is reflected in the majority of studies Haleyet al (2008) and Arango-Lasprilla et al (2010)reported contradictory results
It is noteworthy that aggressionagitation whenmeasured in terms of total score was reported asthe second most distressing across 16 of the studiesbut when measured in terms of frequency only oneof the three studies reported physical aggressionas a common problem However the frequency ofverbal aggression consistently affected well-beingIt is not possible to provide an explanation for thisdiscrepancy but it may be because of the distinctionbetween how aggressionagitation is measured (ietotal score or frequency) or that verbal and physicalaggression have been differentiated and thereforeaffect caregiver well-being differently
Predictive data were limited and heterogeneousin the present review however it was possible toconclude that apathy predicted burden and distressacross studies Anger restlessness combativenessdangerous to others and embarrassing behaviorwere found to be strong predictors of burden ina study by Gaugler et al (2011) Only one studyreported the predictors of caregiver depression
Potential explanations for variability incaregiver well-beingDifference in study quality does not appear to be anexplanation for the variation in distress rating acrossstudies since even between two medium qualitystudies there was considerable variation (Balieiroet al 2010 displaying one of the highest meandistress scores Baiyewu et al 2003 displayingone of the lowest) Two studies consistently hadthe highest mean distress rating across each of thebehavior domains Balieiro et al (2010) and Tanet al (2005) Both of these studies were clinic-basedhigher distress ratings would be expected as those
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1769
experiencing more BPSD might be more likely toattend a clinic as indeed were the majority ofstudies included in the meta-analysis It may bepossible that dementia severity is an explanationsince participants in the studies with the highestdistress scores (Tan et al 2005 Balieiro et al 2010)had moderate and severe dementia respectivelywhereas Baiyewu et al (2003) who consistentlyreported the lowest distress scores across eachof the behavior domains included participantswith mild dementia However both Aarslandet al (2007) and de Vugt et al (2006) reportedlower mean distress scores in comparison with theother included studies and they both includedparticipants with moderate dementia FurthermoreDavidsdottir et al (2012) found that there wasno significant difference between caregiver distressscores depending on dementia severity
Baiyewu et al (2003) had a much smallersample of spousal caregivers in comparison to Tanet al (2005) which might account for the lowerdistress scores This is in agreement with Almberget al (1997) who reported that spouses experiencegreater levels of burden However three studieswhich had consistently higher mean distress scoresacross all behaviors (Tan et al 2005 Balieiro et al2010 Huang et al 2012) were mainly comprisedof adult-child caregivers When comparing a studysolely comprised of spousal caregivers (deVugt et al2006) with a study (Baiyewu et al 2003) withminimal spousal caregivers (25) it was possibleto see that spousal caregivers were substantiallymore distressed with depressive apathetic andanxiety-related behaviors Although distress ratingscan be differentiated between behavior types forspousal and non-spousal caregivers both Baiyewuet al (2003) and de Vugt et al (2006) had two of thelowest distress scores across all behaviors in compar-ison to the other studies in the meta-analysis
The explanation may also be cultural sinceBaiyewu et al (2003) and Baiyewu et al (2012)(with similarly low distress scores across behaviors)were the only Africa-based studies in the meta-analysis Baiyewu et al (2003) and Baiyewu et al(2012) were also both community-based studieswhich may also be a reason for the reduceddistress ratings There is every reason to believethat BPSD are present across cultures (Shajiet al 2009) however the low levels of publicawareness of dementia have many implications(Prince 2000) One of these implications maybe the misinterpretation of BPSD as deliberateconsequently affecting the well-being of the carer(Shaji et al 2009) It is beyond the scope ofthis paper to determine why there is considerablevariation between studies reporting caregiverdistress for identical behaviors using identical
measures However it is likely that it is the caregivercharacteristics rather than the characteristics of theperson with dementia (such as dementia severity)which may underlie the explanation as to whyvariation between studies exists
Limitations
The data available for this review allowed for onlytwo meta-analyses to be conducted There wererelatively few studies which assessed the relationshipbetween individual BPSD and caregiver well-beingand which met the inclusionexclusion criteriafor the review In an attempt to be systematicbased on prior recommendation an effort wasmade to distinguish between how ldquoproblematicrdquosymptoms are measured Consequently studieswere categorized into whether BPSD weremeasured in terms of frequency or prevalence andalso categorized in terms of the statistical analysisemployed Other than data regarding mean distressassociated with NPI total score only a small amountof studies were included in each category andunfortunately it was often the case that measuresof caregiver well-being were dissimilar From the 40included studies there were 12 different measuresof behavior and 17 different measures of well-being making comparisons difficult which mayhave contributed to the inconsistent findings
The majority of included studies recruitedparticipants from clinics therefore caregiversincluded in the review were not representative ofthe population In addition the samples across theincluded studies were heterogeneous in a numberof factors therefore caution should be taken wheninterpreting the results Although beyond the scopeof this review study characteristics such as culturegender and relationship direction were not ex-amined through subgroup analyses Due to the lim-ited number of studies it was not possible to imposea quality criteria however all included studies wereeither of high or medium quality as assessed by theDowns and Back Checklist (1998) Furthermore allof the included studies relied on caregiver reportsof BPSD which may themselves be affected bycaregiver well-being unfortunately it is not possibleto determine if this was the case Nonetheless twovalid meta-analyses were completed and a numberof comments can be made about the relationshipbetween BPSD and caregiver well-being
Implications and recommendations
The vast majority of studies addressing the rela-tionship between BPSD and caregiver well-being
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1770 A Feast et al
did not examine individual BPSD Consequentlythis comparatively limited the amount of studiesincluded in the present review Therefore if we areto understand this relationship more studies needto examine individual BPSD in their research Inaddition it is more clinically relevant to examinewhich BPSD affect well-being rather than BPSDas a whole as this is essential in determiningwhere clinical staff should allocate resources mosteffectively Nevertheless there is preliminary datasuggesting it is mood-related behaviors whichare associated with increased levels of distresstherefore interventions for the management ofBPSD should target these behaviors
The lack of consistency in the measurementof BPSD (neuropsychiatric or memory problemsfrequency or prevalence) and the measurementof caregiver well-being (the use of interchangeableterminology such as stress strain and burdenmeaning the same construct) limits our ability toreach a consensus as to which BPSD result inthe most negative outcomes for caregivers Forexample Donaldson et al (1998) used GilleardrsquosStrain Scale (1984) to measure burden andthe General Health Questionnaire (Goldberg andHillier 1979) to measure distress Furthermorefour studies (see Table S1) did not have formalscales to measure the impact of BPSD on well-being and used terms such as ldquoburdensomerdquoldquoseriousrdquo and ldquodisturbingrdquo This problem impactsupon the validity and reliability of the originalstudies and consequently the review Howeverthis mainly occurred in the earlier studies Futureresearch should also include more than one measureof well-being in order to identify if individual BPSDdifferentially affect caregiver burden compared tocaregiver distress as identified in the current reviewFurthermore future research should identify whythere is reduced variability in distress ratings forcertain behaviors compared to others and whycertain behaviors are more distressing dependingon which type of statistical analysis is used
Although there are potential methodologicalreasons (limited studies inconsistent measures)for why there is substantial variability whenidentifying which BPSD affect certain types ofcaregiver well-being the most there is growingevidence that factors associated with the personwith dementia (eg BPSD frequency cognition) areonly part of the story when explaining a caregiverrsquosresponse to BPSD Caregiver characteristicshave been shown to account for twice thevariance of person with dementia characteristicswhen reporting neuropsychiatric symptoms (Sinket al 2006) and the presence of BPSD wasnot found to be a significant predictor ofburden whereas caregiver characteristics such as
confidence neuroticism and relationship qualitywere significant predictors (Campbell et al 2008)Therefore as recommended by Ornstein andGaugler (2012) future studies should focus onidentifying pathways for the association betweenindividual BPSD caregiver variables and caregiveroutcomes More research is needed to understandif and why certain BPSD affect certain caregiveroutcomes and also how much of this is attributableto caregiver variability in response to BPSD ratherthan the presence of BPSD itself More longitudinalstudies would be useful to examine how changes inindividual BPSD are associated with caregiver well-being over time A review by Black and Almeida(2004) examined the limited longitudinal studiesavailable and reported mixed findings betweenburden and BPSD and found no associationbetween BPSD and distress Although BPSDincreased significantly over a two-year periodcaregiver burden remained stable and depressionwas found to decrease (Berger et al 2005) Futureresearch needs to examine caregiver factors overtime (well-being role captivity etc) along withchanges in individual BPSD in order to have a morevalid understanding of this relationship
Caution should be exercised when creating ameasure of BPSD since Jackson et al (2014)found that the Revised Memory and BehaviorProblem Checklist (Teri et al 1992) might bemore suitable in explaining caregiver depressionthan the NPI It is important that the measureof BPSD is not biased toward explaining a moreunique association between BPSD and a measure ofcaregiver well-being such as depression As stated byGitlin and Rose (2014) item selection for measuresof BPSD is often based upon specific disciplines(eg neurology psychiatry social sciences) andthus implicitly represents different conceptual-izations of behavior A shared framework fordefining behaviors and their underlying causesmust be created in order to move on fromthe implicit assumption of most measures thatbehaviors are a direct cause of neuropathologyand to develop measures which also address thecontextual and caregiver characteristics associatedwith the behavior
Conclusions
This study has improved our understanding of theimpact of individual BPSD on caregiver well-beingin particular caregiver distress The relationshipbetween individual BPSD and caregiver well-beingwas inconsistent and varied according to behavioralsymptom Due to limited studies and heterogeneousdata the results should be interpreted with caution
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1771
but advances have been made with respect towhich behaviors are associated with distress Theinconsistencies may be partly explained by caregivervariables which were not taken into account inthe review Based on this review and previousresearch it is not possible to fully understand therelationship between BPSD and caregiver well-being without examining the influence of caregivervariables such as caregiver strategies acceptancegender relationship with person with dementiaand confidence We recommend that future studiesare designed to examine individual BPSD ratherthan BPSD as a whole use consistent measures forBPSD and well-being use consistent terminologyfor psychological constructs (eg burden) andexamine the causal mechanisms by which individualBPSD impact caregiver well-being by collectingdata on a range of caregiver factors Theseapproaches will clarify whether it is important forclinicians to focus on the frequency or prevalence ofcertain BPSD in addition to targeting the presenceof certain caregiver characteristics and addressingunmet need
Conflict of interest
None
Description of authorsrsquo roles
A Feast was responsible for developing the reviewobjectives writing the search strategies conductingthe searches designing and completing studyeligibility and data extraction forms undertakingthe quality appraisals conducting the meta-analysisand writing the paper M Orrell was responsible fordeveloping the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper C Stoner was responsible forundertaking the quality appraisals and assisting inwriting the paper G Charlesworth was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper E Moniz-Cook was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper
Acknowledgments
We would like to thank Dr Zoeuml Hoare for herstatistical advice This paper presents independentresearch funded by the National Institute for HealthResearch (NIHR) under its Programme Grants forApplied Research (RP-PG-0606-1067 and RP-PG-
060- 1083) The views expressed in this publicationare those of the author(s) and not necessarily thoseof the NHS the NIHR or the Department ofHealth
Supplementary Material
To view supplementary material for thisarticle please visit httpdxdoiorg101017S1041610216000922
References
Aarsland D et al (2007) Neuropsychiatric symptoms inpatients with Parkinsonrsquos disease and dementia frequencyprofile and associated care giver stress Journal of NeurologyNeurosurgery amp Psychiatry 78 36ndash42doihttpdxdoiorg101136jnnp2005083113
Allegri R F et al (2006) Neuropsychiatric symptoms as apredictor of caregiver burden in Alzheimerrsquos diseaseNeuropsychiatric Disease amp Treatment 2 105ndash110doi102147ndts47133
Almberg B Grafstrom M and Winblad B (1997)Major strain and coping strategies as reported by familymembers who care for aged demented relatives Journal ofAdvanced Nursing 26 683ndash691doihttpdxdoiorg101046j1365-2648199700392x
Arango-Lasprilla J C Lehan T Drew A MorenoA Deng X and Lemos M (2010) Health-relatedquality of life in caregivers of individuals with dementiafrom Colombia American Journal of Alzheimerrsquos Disease andOther Dementias 25 556ndash561doi1011771533317510382287ltbibgt
Baiyewu O et al (2003) Behavioral and caregiver reactionof dementia as measured by the neuropsychiatric inventoryin Nigerian community residents InternationalPsychogeriatrics 15 399ndash409doi101017s1041610203009645
Baiyewu O et al (2012) Behavioral symptoms incommunity-dwelling elderly Nigerians with dementia mildcognitive impairment and normal cognition InternationalJournal of Geriatric Psychiatry 27 931ndash939 doihttpdxdoiorg101002gps2804
Balieiro A P Jr Sobreira E S T Pena M C SSilva-Filho J H and Vale F A C (2010) Caregiverdistress associated with behavioral and psychologicalsymptoms in mild Alzheimerrsquos disease Dementia eNeuropsychologia 4 238ndash244
Ballard C G et al (1995) The aetiology of depression inthe carers of dementia sufferers Journal of AffectiveDisorders 35 59ndash63 doi1010160165-0327(95)00041-k
Bandeira D R Pawlowski J Goncalves T RHilgert J B Bozzetti M C and Hugo F N (2007)Psychological distress in Brazilian caregivers of relativeswith dementia Aging and Mental Health 11 14ndash19doi10108013607860600640814
Berger G Bernhardt T Weimer E Peters JKratzsch T and Frolich L (2005) Longitudinal studyon the relationship between symptomatology of dementia
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1772 A Feast et al
and levels of subjective burden and depression amongfamily caregivers in memory clinic patients Journal ofGeriatric Psychiatry and Neurology 3 119ndash128doi1011770891988704273375
Black W and Almeida O P (2004) A systematic reviewof the association between the behavioral and psychologicalsymptoms of dementia and burden of care InternationalPsychogeriatrics 16 295ndash315doi101017s1041610204000468
Bruce D G and Paterson A (2000) Barriers tocommunity support for the dementia carer a qualitativestudy International Journal of Geriatric Psychiatry 15451ndash457 doi101002(sici)1099-1166(200005)155lt451aid-gps143gt30co2-k
Campbell P et al (2008) Determinants of burden in thosewho care for someone with dementia International Journalof Geriatric Psychiatry 23 1078ndash1085doi101002gps2071
Cerejeira J Lagarto L and Mukaetova-LadinskaE B (2012) Behavioral and psychological symptoms ofdementia Frontiers in Neurology 3 1ndash23doi103389fneur201200073
Chappell N L and Penning M (1996) Behaviouralproblems and distress among caregivers of people withdementia Ageing amp Society 16 57ndash73doi101017s0144686x00003135
Chiu Y C et al (2014) Family caregiversrsquo sleepdisturbance and its associations with multilevel stressorswhen caring for patients with dementia Aging amp MentalHealth 18 92ndash101 doihttpdxdoiorg101080136078632013837141
Cohen J (1988) Statistical Power Analysis for the BehavioralSciences 2nd edn New York University New YorkLawrence Erlbaum Associatesdoi1043249780203771587
Conde-Sala J L Garre-Olmo J Turroacute-Garriga OVilalta-Franch J and Loacutepez-Pousa S (2010)Differential features of burden between spouse andadult-child caregivers of patients with Alzheimerrsquos diseasean exploratory comparative design International Journal ofNursing Studies 47 1262ndash1273doi101016jijnurstu201003001
Covinsky K E et al (2003) Patient and caregivercharacteristics associated with depression in caregivers ofpatients with dementia Journal of General Internal Medicine18 1006ndash1014 doihttpdxdoiorg101111j1525-1497200330103x
Craig D Mirakhur A Hart D J McIlroy S P andPassmore A P (2005) A cross-sectional study ofneuropsychiatric symptoms in 435 patients withAlzheimerrsquos disease American Journal of GeriatricPsychiatry 13 460ndash468 doi10109700019442-200506000-00004
Crellin N Charlesworth G and Orrell M (2014)Measuring family caregiver efficacy for managing behavioraland psychological symptoms in dementia a psychometricevaluation International Psychogeriatrics 26 93ndash103 doihttpdxdoiorg101017s1041610213001646
Davidsdottir S R Snaedal J Karlsdottir GAtladottir I and Hannesdottir K (2012) Validationof the Icelandic version of the neuropsychiatric inventorywith caregiver distress (NPI-D) Nordic Journal of
Psychiatry 66 26ndash32 doihttpdxdoiorg103109080394882011593100
Davis J D and Tremont G (2007) Impact of frontalsystems behavioral functioning in dementia on caregiverburden The Journal of Neuropsychiatry and ClinicalNeurosciences 19 43ndash49 doihttpdxdoiorg101176jnp200719143
de Vugt M E Riedijk S R Aalten P Tibben Avan Swieten J C and Verhey F R J (2006) Impactof behavioural problems on spousal caregivers acomparison between Alzheimerrsquos disease andfronto-temporal dementia Dementia and Geriatric CognitiveDisorders 22 35ndash41 doi101159000093102
de Vugt M E et al (2003) Behavioural disturbances indementia patients and quality of the marital relationshipInternational Journal of Geriatric Psychiatry 18 149ndash154doi101002gps807
Donaldson C Tarrier N and Burns A (1998)Determinants of carer stress in Alzheimerrsquos diseaseInternational Journal of Geriatric Psychiatry 13 248ndash256doi101002(sici)1099-1166(199804)134lt248aid-gps770gt30co2-0
Downs S and Black N (1998) The feasibility of creating achecklist for the assessment of the methodological qualityboth of randomised and non-randomised studies of healthcare interventions Journal of Epidemiological CommunityHealth 52 377ndash384 doi101136jech526377
Farran C J Loukissa D A Lindeman D A andMcCann J (2004) Caring for self while caring for othersthe two-track life of coping with Alzheimerrsquos diseaseJournal of Gerontological Nursing 30 38ndash45doi1039280098-9134-20040501-09
Fauth E B and Gibbons A (2014) Which behavioral andpsychological symptoms of dementia are the mostproblematic Variability by prevalence intensity distressratings and associations with carer depressive symptomsInternational Journal of Geriatric Psychiatry 29 263ndash271doi101002gps4002
Fuh J L Liu C K Mega M S Wang S J andCummings J L (2001) Behavioral disorders andcaregiversrsquo reaction in Taiwanese patients with Alzheimerrsquosdisease International Psychogeriatrics 13 121ndash128 doihttpdxdoiorg101017s1041610201007517
Gaugler J E et al (2011) Does caregiver burden mediatethe effects of behavioral disturbances on nursing homeadmission The American Journal of Geriatric Psychiatry 19497ndash506 doi101097jgp0b013e31820d92cc
Gilleard C J Belford H Gilleard E Whittick J Eand Gledhill K (1984) Emotional distress amongst thesupporters of the elderly mental infirm British Journal ofPsychiatry 145 172ndash177doihttpdxdoiorg101192bjp1452172
Gitlin L N and Rose K (2014) Factors associated withcarer readiness to use nonpharmacologic strategies tomanage dementia-related behavioral symptomsInternational Journal of Geriatric Psychiatry 29 93ndash102doihttpdxdoiorg101002gps3979
Goldberg D P and Hillier V F (1979) A scaled versionof the general health questionnaire Psychological Medicine9 139ndash145 doi101017s0033291700021644
Gonzalez-Salvador M T Arango C Lyketsos C Gand Barba A C (1999) The stress and psychological
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1773
morbidity of the Alzheimer patient caregiver InternationalJournal of Geriatric Psychiatry 14 701ndash710doi101002(sici)1099-1166(199909)149lt701aidps5gt30co2-
Haley W E Brown S and Levine E G (1987) Familycaregiver appraisals of patient behavioral disturbance insenile dementia Clinical Gerontologist The Journal of Agingand Mental Health 6 25ndash34doi101300j018v06n04_04
Haley W E Levine E G Brown S L Berry J Wand Hughes G H (2008) The psychological social andhealth consequences of caring for a relative with seniledementia Journal of the American Geriatrics Society 35405ndash411 doi101111j1532-54151987tb04661x
Hishikawa N et al (2012) Effects of turmeric onAlzheimerrsquos disease with behavioral and psychologicalsymptoms of dementia Ayu 33 499ndash504 doihttpdxdoiorg1041030974-8520110524
Huang S S Lee M C Liao Y C Wang W F andLai T J (2012) Caregiver burden associated withbehavioral and psychological symptoms of dementia(BPSD) in Taiwanese elderly Archives of Gerontology andGeriatrics 55 55ndash59 doihttpdxdoiorg101016jarchger201104009
Jackson M A Fauth E B and Geiser C (2014)Comparing the neuropsychiatric inventory and the revisedmemory and behavior problems checklist for associationswith caregiver burden and depressive symptomsInternational Psychogeriatrics 26 1021ndash1031doi101017s1041610213002421
Johnson D K Niedens M Wilson J RSwartzendruber L Yeager A and Jones K (2013)Treatment outcomes of a crisis intervention program fordementia with severe psychiatric complications the Kansasbridge project The Gerontologist 53 102ndash112 doihttpdxdoiorg101093gerontgns104
Khoo S A Chen T Y Ang Y H and Yap P (2013)The impact of neuropsychiatric symptoms on caregiverdistress and quality of life in persons with dementia in anAsian tertiary hospital memory clinic InternationalPsychogeriatrics 25 1991ndash1999 doihttpdxdoiorg101017s1041610213001518
Kosberg J I Kaufman A V Burgio L D Leeper Jand Sun F (2007) Family caregiving to those withdementia in rural Alabama racial similarities anddifferences Journal of Aging and Health 19 3ndash21 doi1011770898264306293604
Kosmala K and Kloszewska I (2004) The burden ofproviding care for Alzheimerrsquos disease patients in PolandInternational Journal of Geriatric Psychiatry 19 191ndash193doi101002gps1054
Landis J R and Koch G G (1977) The measurement ofobserver agreement for categorical data Biometrics 33159ndash174 doi 1023072529310
Lee D R McKeith I Mosimann U Ghosh-NodyalA and Thomas A J (2013) Examining carer stress indementia the role of subtype diagnosis andneuropsychiatric symptoms International Journal ofGeriatric Psychiatry 28 135ndash141 doihttpdxdoiorg101002gps3799
Lim Y M Son G R Song J A and Beattie E(2008) Factors affecting burden of family caregivers of
community-dwelling ambulatory elders with dementia inKorea Archives of Psychiatric Nursing 22 226ndash234 doi101016japnu200712005
Matsumoto N et al (2007) Caregiver burden associatedwith behavioral and psychological symptoms of dementia inelderly people in the local community Dementia andGeriatric Cognitive Disorders 23 219ndash224doi101159000099472
Mohamed S Rosenheck R Lyketsos C G andSchneider L S (2010) Caregiver burden in Alzheimerdisease cross-sectional and longitudinal patient correlatesThe American Journal of Geriatric Psychiatry 18 917ndash927doi101097jgp0b013e3181d5745d
Mourik J C Rosso S M Niermeijer M FDuivenvoorden H J Van Swieten J C and TibbenA (2004) Frontotemporal dementia behavioral symptomsand caregiver distress Dementia and Geriatric CognitiveDisorders 18 299ndash306 doihttpdxdoiorg101159000080123
Muangpaisan W et al (2010) Caregiver burden and needsof dementia caregivers in Thailand a cross-sectional studyJournal of the Medical Association of Thailand 93 601ndash607
Neundorfer M M McClendon M J Smyth K AStuckey J C Strauss M E and Patterson M B(2001) A longitudinal study of the relationship betweenlevels of depression among persons with Alzheimerrsquosdisease and levels of depression among their familycaregivers Journal of Gerontology Series B - PsychologicalSciences and Social Sciences 56 301ndash313
Nygaard H A (1998) Strain on caregivers of dementedelderly people living at home Scandinavian Journal ofPrimary Health Care 6 33ndash37doihttpdxdoiorg10310902813438809009287
Ornstein K and Gaugler J E (2012) The problem withldquoproblem behaviorsrdquoa systematic review of the associationbetween individual patient behavioral and psychologicalsymptoms and caregiver depression and burden within thedementia patientndashcaregiver dyad InternationalPsychogeriatrics 24 1536ndash1552doi101017s1041610212000737
Ornstein K Gaugler J E Devanand N S CarolynZ and Yaakov S (2012) The differential impact ofunique behavioral and psychological symptoms for thedementia caregiver how and why do patientsrsquo individualsymptom clusters impact caregiver depressive symptomsThe American Journal of Geriatric Psychiatry 12 77ndash1286doi httpdxdoiorg101016jjagp201301062
Price G R (1970) Selection and covariance Nature 227520ndash521 doi101038227520a0
Prince M (2000) Dementia in developing countries Aconsensus statement from the 1066 Dementia ResearchGroup International Journal of Geriatric Psychiatry 1514ndash20 doihttpdxdoiorg101002(sici)1099-1166(200001)151lt14aid-gps70gt30co2-8
Quayhagen M P and Quayhagen M (1998) Alzheimerrsquosstress coping with the caregiving role Gerontologist 28391ndash396 doihttpdxdoiorg101093geront283391
Reisberg B Ferris S H de Leon M J and Crook T(1982) The global deterioration scale for assessment ofprimary degenerative dementia American Journal ofPsychiatry 139 1136ndash1139 doihttpdxdoiorg101176ajp13991136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1774 A Feast et al
Robinson K M Adkisson P and Weinrich S (2001)Problem behaviour caregiver reactions and impact amongcaregivers of persons with Alzheimerrsquos disease Journal ofAdvanced Nursing 36 573ndash582 doihttpdxdoiorg101046j1365-2648200102010x
Rocca P et al (2010) Neuropsychiatric symptomsunderlying caregiver stress and insight in Alzheimerrsquosdisease Dementia and Geriatric Cognitive Disorders 3057ndash63 doi101159000315513
Rymer S Salloway S Norton L Mallow PCorreia S and Monast D (2002) Impaired awarenessbehavior disturbance and caregiver burden in Alzheimerdisease Alzheimer Disease and Associated Disorders 16248ndash253 doi 10109700002093-200210000-00006
Savorani G Vulcano V Boni S Sarti G andRavaglia G (1998) Behavioral disorders in dementiapatients and their impact on the stress of caregivingrelatives the ldquoARADrdquo questionnaire Archives ofGerontology and Geriatrics 6 481ndash485doi101016s0167-4943(98)80070-8
Shaji K S George R K Prince M J and JacobK S (2009) Behavioral symptoms and caregiver burdenin dementia Indian Journal of Psychiatry 51 45 doihttpdxdoiorg1041030019-554544905
Sink K M Covinsky K E Barnes D E NewcomerR J and Yaffe K (2006) Caregiver characteristics areassociated with neuropsychiatric symptoms of dementiaJournal of the American Geriatrics Society 54 796ndash803 doi101111j1532-5415200600697x
Slachevsky A et al (2013) The CUIDEME studydeterminants of burden in chilean primary caregivers ofpatients with dementia Journal of Alzheimerrsquos Disease 35297ndash306
Spiegel R et al (1991) A new behavioral assessment scalefor geriatric out- and in-patients the NOSGER (nursesrsquoobservation scale for geriatric patients) Journal of theAmerican Geriatric Society 39 339ndash347 doihttpdxdoiorg101111j1532-54151991tb02897x
Tan L L Wong H B and Allen H (2005) The impactof neuropsychiatric symptoms of dementia on distress infamily and professional caregivers in SingaporeInternational Psychogeriatrics 17 253ndash263 doi101017s1041610205001523
Teri L (1997) Behavior and caregiver burden behavioralproblems in patients with Alzheimer disease and itsassociation with caregiver distress Alzheimer Disease andAssociated Disorders 11 35ndash38
Teri L Truax P Logsdon R Uomoto J Zarit Sand Vitaliano P P (1992) Assessment of behavioralproblems in dementia the revised memory and behaviorproblems checklist Psychology and Aging 7 622 doi1010370882-797474622
Waite A Bebbington P Skelton-Robinson M andOrrell M (2004) Social factors and depression in carersof people with dementia International Journal of GeriatricPsychiatry 19 582ndash587 doihttpdxdoiorg101002gps1136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at

1768 A Feast et al
and distress and found similar results howevereven with identical analysis there were noteworthydiscrepancies such as delusions being the mostdistressing but only the fourth most distressing inthe current review Consistent with the currentmeta-analysis of mean data apathy and depression-related behaviors have been reported as distressingin numerous studies (Teri 1997 deVugt et al2003 Aarsland et al 2007 Kosberg et al 2007)Similarly depression in the person with dementia isassociated with depression in the caregiver (Waiteet al 2004)
Meta-analysis of correlation dataAs seen in Table 1 there were high levels ofheterogeneity between the studies included in thesecond meta-analysis investigating which behaviorswere associated with distress Only apathy- andsleep-related behaviors displayed homogeneitybetween studies Furthermore behaviors which hadstronger correlations with distress (Table 1) didnot have strong associations in the previous meta-analysis (Figure 3) regarding distress associatedwith behaviors At present it is unclear why thisdiscrepancy exists and also why distress correlatedwith apathy- and sleep-related behaviors is more ho-mogenous between studies than the other behaviorsSince only a few studies contributed to this meta-analysis more research is needed to investigate thepooled effects Nevertheless a meta-analysis of thisnature has not been performed previously and therandom-effects model was used to report a moreconservative estimate for the heterogeneous pooledeffects in order to reduce bias
Apathy and irritable behaviors were not con-sistently significantly correlated to burden acrossmultiple studies whereas delusions agitationdisinhibition and appetiteeating change werethese associations were also reported in otherstudies (Rymer et al 2002 Rocca et al 2010) Incontrast a review by Ornstein and Gaugler (2012)reported that angeraggression and depression werethe most frequently cited BPSD associated withcaregiver burden depression was also linked tocaregiver burden in a review by Black and Almeida(2004) In addition to burden delusional behaviorwas consistently associated with distress acrossstudies with a significant correlation also beingseen with stress (Kosmala and Kloszewska 2004)Berger et al (2005) noted that behaviors whichare significantly correlated with burden are notcorrelated with depression This demonstrates theimportance of including multiple measures of well-being since the same behaviors affect caregiversdifferently which has implications for futureinterventions
Studies unamenable to quantitative synthesisOnly two studies reported the prevalence of BPSDand the impact on caregiver well-being due todifferences between studies comparisons werenot possible Although five studies reported thefrequency of BPSD each measure of caregiver well-being was different Memory-related behaviorsverbal aggression incontinence and irritabilitywere reported to affect well-being across multiplestudies These findings were also seen in previousresearch (Bruce and Paterson 2000 Farran et al2004) However Fauth and Gibbons (2014) andRobinson et al (2001) did not find that memory-related behaviors were distressing despite being themost frequent type of behavior on the RMBPCHallucinations sexual disinhibition and physicalaggression were consistently reported to affect well-being less than the other behaviors Although thisfinding is reflected in the majority of studies Haleyet al (2008) and Arango-Lasprilla et al (2010)reported contradictory results
It is noteworthy that aggressionagitation whenmeasured in terms of total score was reported asthe second most distressing across 16 of the studiesbut when measured in terms of frequency only oneof the three studies reported physical aggressionas a common problem However the frequency ofverbal aggression consistently affected well-beingIt is not possible to provide an explanation for thisdiscrepancy but it may be because of the distinctionbetween how aggressionagitation is measured (ietotal score or frequency) or that verbal and physicalaggression have been differentiated and thereforeaffect caregiver well-being differently
Predictive data were limited and heterogeneousin the present review however it was possible toconclude that apathy predicted burden and distressacross studies Anger restlessness combativenessdangerous to others and embarrassing behaviorwere found to be strong predictors of burden ina study by Gaugler et al (2011) Only one studyreported the predictors of caregiver depression
Potential explanations for variability incaregiver well-beingDifference in study quality does not appear to be anexplanation for the variation in distress rating acrossstudies since even between two medium qualitystudies there was considerable variation (Balieiroet al 2010 displaying one of the highest meandistress scores Baiyewu et al 2003 displayingone of the lowest) Two studies consistently hadthe highest mean distress rating across each of thebehavior domains Balieiro et al (2010) and Tanet al (2005) Both of these studies were clinic-basedhigher distress ratings would be expected as those
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1769
experiencing more BPSD might be more likely toattend a clinic as indeed were the majority ofstudies included in the meta-analysis It may bepossible that dementia severity is an explanationsince participants in the studies with the highestdistress scores (Tan et al 2005 Balieiro et al 2010)had moderate and severe dementia respectivelywhereas Baiyewu et al (2003) who consistentlyreported the lowest distress scores across eachof the behavior domains included participantswith mild dementia However both Aarslandet al (2007) and de Vugt et al (2006) reportedlower mean distress scores in comparison with theother included studies and they both includedparticipants with moderate dementia FurthermoreDavidsdottir et al (2012) found that there wasno significant difference between caregiver distressscores depending on dementia severity
Baiyewu et al (2003) had a much smallersample of spousal caregivers in comparison to Tanet al (2005) which might account for the lowerdistress scores This is in agreement with Almberget al (1997) who reported that spouses experiencegreater levels of burden However three studieswhich had consistently higher mean distress scoresacross all behaviors (Tan et al 2005 Balieiro et al2010 Huang et al 2012) were mainly comprisedof adult-child caregivers When comparing a studysolely comprised of spousal caregivers (deVugt et al2006) with a study (Baiyewu et al 2003) withminimal spousal caregivers (25) it was possibleto see that spousal caregivers were substantiallymore distressed with depressive apathetic andanxiety-related behaviors Although distress ratingscan be differentiated between behavior types forspousal and non-spousal caregivers both Baiyewuet al (2003) and de Vugt et al (2006) had two of thelowest distress scores across all behaviors in compar-ison to the other studies in the meta-analysis
The explanation may also be cultural sinceBaiyewu et al (2003) and Baiyewu et al (2012)(with similarly low distress scores across behaviors)were the only Africa-based studies in the meta-analysis Baiyewu et al (2003) and Baiyewu et al(2012) were also both community-based studieswhich may also be a reason for the reduceddistress ratings There is every reason to believethat BPSD are present across cultures (Shajiet al 2009) however the low levels of publicawareness of dementia have many implications(Prince 2000) One of these implications maybe the misinterpretation of BPSD as deliberateconsequently affecting the well-being of the carer(Shaji et al 2009) It is beyond the scope ofthis paper to determine why there is considerablevariation between studies reporting caregiverdistress for identical behaviors using identical
measures However it is likely that it is the caregivercharacteristics rather than the characteristics of theperson with dementia (such as dementia severity)which may underlie the explanation as to whyvariation between studies exists
Limitations
The data available for this review allowed for onlytwo meta-analyses to be conducted There wererelatively few studies which assessed the relationshipbetween individual BPSD and caregiver well-beingand which met the inclusionexclusion criteriafor the review In an attempt to be systematicbased on prior recommendation an effort wasmade to distinguish between how ldquoproblematicrdquosymptoms are measured Consequently studieswere categorized into whether BPSD weremeasured in terms of frequency or prevalence andalso categorized in terms of the statistical analysisemployed Other than data regarding mean distressassociated with NPI total score only a small amountof studies were included in each category andunfortunately it was often the case that measuresof caregiver well-being were dissimilar From the 40included studies there were 12 different measuresof behavior and 17 different measures of well-being making comparisons difficult which mayhave contributed to the inconsistent findings
The majority of included studies recruitedparticipants from clinics therefore caregiversincluded in the review were not representative ofthe population In addition the samples across theincluded studies were heterogeneous in a numberof factors therefore caution should be taken wheninterpreting the results Although beyond the scopeof this review study characteristics such as culturegender and relationship direction were not ex-amined through subgroup analyses Due to the lim-ited number of studies it was not possible to imposea quality criteria however all included studies wereeither of high or medium quality as assessed by theDowns and Back Checklist (1998) Furthermore allof the included studies relied on caregiver reportsof BPSD which may themselves be affected bycaregiver well-being unfortunately it is not possibleto determine if this was the case Nonetheless twovalid meta-analyses were completed and a numberof comments can be made about the relationshipbetween BPSD and caregiver well-being
Implications and recommendations
The vast majority of studies addressing the rela-tionship between BPSD and caregiver well-being
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1770 A Feast et al
did not examine individual BPSD Consequentlythis comparatively limited the amount of studiesincluded in the present review Therefore if we areto understand this relationship more studies needto examine individual BPSD in their research Inaddition it is more clinically relevant to examinewhich BPSD affect well-being rather than BPSDas a whole as this is essential in determiningwhere clinical staff should allocate resources mosteffectively Nevertheless there is preliminary datasuggesting it is mood-related behaviors whichare associated with increased levels of distresstherefore interventions for the management ofBPSD should target these behaviors
The lack of consistency in the measurementof BPSD (neuropsychiatric or memory problemsfrequency or prevalence) and the measurementof caregiver well-being (the use of interchangeableterminology such as stress strain and burdenmeaning the same construct) limits our ability toreach a consensus as to which BPSD result inthe most negative outcomes for caregivers Forexample Donaldson et al (1998) used GilleardrsquosStrain Scale (1984) to measure burden andthe General Health Questionnaire (Goldberg andHillier 1979) to measure distress Furthermorefour studies (see Table S1) did not have formalscales to measure the impact of BPSD on well-being and used terms such as ldquoburdensomerdquoldquoseriousrdquo and ldquodisturbingrdquo This problem impactsupon the validity and reliability of the originalstudies and consequently the review Howeverthis mainly occurred in the earlier studies Futureresearch should also include more than one measureof well-being in order to identify if individual BPSDdifferentially affect caregiver burden compared tocaregiver distress as identified in the current reviewFurthermore future research should identify whythere is reduced variability in distress ratings forcertain behaviors compared to others and whycertain behaviors are more distressing dependingon which type of statistical analysis is used
Although there are potential methodologicalreasons (limited studies inconsistent measures)for why there is substantial variability whenidentifying which BPSD affect certain types ofcaregiver well-being the most there is growingevidence that factors associated with the personwith dementia (eg BPSD frequency cognition) areonly part of the story when explaining a caregiverrsquosresponse to BPSD Caregiver characteristicshave been shown to account for twice thevariance of person with dementia characteristicswhen reporting neuropsychiatric symptoms (Sinket al 2006) and the presence of BPSD wasnot found to be a significant predictor ofburden whereas caregiver characteristics such as
confidence neuroticism and relationship qualitywere significant predictors (Campbell et al 2008)Therefore as recommended by Ornstein andGaugler (2012) future studies should focus onidentifying pathways for the association betweenindividual BPSD caregiver variables and caregiveroutcomes More research is needed to understandif and why certain BPSD affect certain caregiveroutcomes and also how much of this is attributableto caregiver variability in response to BPSD ratherthan the presence of BPSD itself More longitudinalstudies would be useful to examine how changes inindividual BPSD are associated with caregiver well-being over time A review by Black and Almeida(2004) examined the limited longitudinal studiesavailable and reported mixed findings betweenburden and BPSD and found no associationbetween BPSD and distress Although BPSDincreased significantly over a two-year periodcaregiver burden remained stable and depressionwas found to decrease (Berger et al 2005) Futureresearch needs to examine caregiver factors overtime (well-being role captivity etc) along withchanges in individual BPSD in order to have a morevalid understanding of this relationship
Caution should be exercised when creating ameasure of BPSD since Jackson et al (2014)found that the Revised Memory and BehaviorProblem Checklist (Teri et al 1992) might bemore suitable in explaining caregiver depressionthan the NPI It is important that the measureof BPSD is not biased toward explaining a moreunique association between BPSD and a measure ofcaregiver well-being such as depression As stated byGitlin and Rose (2014) item selection for measuresof BPSD is often based upon specific disciplines(eg neurology psychiatry social sciences) andthus implicitly represents different conceptual-izations of behavior A shared framework fordefining behaviors and their underlying causesmust be created in order to move on fromthe implicit assumption of most measures thatbehaviors are a direct cause of neuropathologyand to develop measures which also address thecontextual and caregiver characteristics associatedwith the behavior
Conclusions
This study has improved our understanding of theimpact of individual BPSD on caregiver well-beingin particular caregiver distress The relationshipbetween individual BPSD and caregiver well-beingwas inconsistent and varied according to behavioralsymptom Due to limited studies and heterogeneousdata the results should be interpreted with caution
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1771
but advances have been made with respect towhich behaviors are associated with distress Theinconsistencies may be partly explained by caregivervariables which were not taken into account inthe review Based on this review and previousresearch it is not possible to fully understand therelationship between BPSD and caregiver well-being without examining the influence of caregivervariables such as caregiver strategies acceptancegender relationship with person with dementiaand confidence We recommend that future studiesare designed to examine individual BPSD ratherthan BPSD as a whole use consistent measures forBPSD and well-being use consistent terminologyfor psychological constructs (eg burden) andexamine the causal mechanisms by which individualBPSD impact caregiver well-being by collectingdata on a range of caregiver factors Theseapproaches will clarify whether it is important forclinicians to focus on the frequency or prevalence ofcertain BPSD in addition to targeting the presenceof certain caregiver characteristics and addressingunmet need
Conflict of interest
None
Description of authorsrsquo roles
A Feast was responsible for developing the reviewobjectives writing the search strategies conductingthe searches designing and completing studyeligibility and data extraction forms undertakingthe quality appraisals conducting the meta-analysisand writing the paper M Orrell was responsible fordeveloping the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper C Stoner was responsible forundertaking the quality appraisals and assisting inwriting the paper G Charlesworth was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper E Moniz-Cook was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper
Acknowledgments
We would like to thank Dr Zoeuml Hoare for herstatistical advice This paper presents independentresearch funded by the National Institute for HealthResearch (NIHR) under its Programme Grants forApplied Research (RP-PG-0606-1067 and RP-PG-
060- 1083) The views expressed in this publicationare those of the author(s) and not necessarily thoseof the NHS the NIHR or the Department ofHealth
Supplementary Material
To view supplementary material for thisarticle please visit httpdxdoiorg101017S1041610216000922
References
Aarsland D et al (2007) Neuropsychiatric symptoms inpatients with Parkinsonrsquos disease and dementia frequencyprofile and associated care giver stress Journal of NeurologyNeurosurgery amp Psychiatry 78 36ndash42doihttpdxdoiorg101136jnnp2005083113
Allegri R F et al (2006) Neuropsychiatric symptoms as apredictor of caregiver burden in Alzheimerrsquos diseaseNeuropsychiatric Disease amp Treatment 2 105ndash110doi102147ndts47133
Almberg B Grafstrom M and Winblad B (1997)Major strain and coping strategies as reported by familymembers who care for aged demented relatives Journal ofAdvanced Nursing 26 683ndash691doihttpdxdoiorg101046j1365-2648199700392x
Arango-Lasprilla J C Lehan T Drew A MorenoA Deng X and Lemos M (2010) Health-relatedquality of life in caregivers of individuals with dementiafrom Colombia American Journal of Alzheimerrsquos Disease andOther Dementias 25 556ndash561doi1011771533317510382287ltbibgt
Baiyewu O et al (2003) Behavioral and caregiver reactionof dementia as measured by the neuropsychiatric inventoryin Nigerian community residents InternationalPsychogeriatrics 15 399ndash409doi101017s1041610203009645
Baiyewu O et al (2012) Behavioral symptoms incommunity-dwelling elderly Nigerians with dementia mildcognitive impairment and normal cognition InternationalJournal of Geriatric Psychiatry 27 931ndash939 doihttpdxdoiorg101002gps2804
Balieiro A P Jr Sobreira E S T Pena M C SSilva-Filho J H and Vale F A C (2010) Caregiverdistress associated with behavioral and psychologicalsymptoms in mild Alzheimerrsquos disease Dementia eNeuropsychologia 4 238ndash244
Ballard C G et al (1995) The aetiology of depression inthe carers of dementia sufferers Journal of AffectiveDisorders 35 59ndash63 doi1010160165-0327(95)00041-k
Bandeira D R Pawlowski J Goncalves T RHilgert J B Bozzetti M C and Hugo F N (2007)Psychological distress in Brazilian caregivers of relativeswith dementia Aging and Mental Health 11 14ndash19doi10108013607860600640814
Berger G Bernhardt T Weimer E Peters JKratzsch T and Frolich L (2005) Longitudinal studyon the relationship between symptomatology of dementia
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1772 A Feast et al
and levels of subjective burden and depression amongfamily caregivers in memory clinic patients Journal ofGeriatric Psychiatry and Neurology 3 119ndash128doi1011770891988704273375
Black W and Almeida O P (2004) A systematic reviewof the association between the behavioral and psychologicalsymptoms of dementia and burden of care InternationalPsychogeriatrics 16 295ndash315doi101017s1041610204000468
Bruce D G and Paterson A (2000) Barriers tocommunity support for the dementia carer a qualitativestudy International Journal of Geriatric Psychiatry 15451ndash457 doi101002(sici)1099-1166(200005)155lt451aid-gps143gt30co2-k
Campbell P et al (2008) Determinants of burden in thosewho care for someone with dementia International Journalof Geriatric Psychiatry 23 1078ndash1085doi101002gps2071
Cerejeira J Lagarto L and Mukaetova-LadinskaE B (2012) Behavioral and psychological symptoms ofdementia Frontiers in Neurology 3 1ndash23doi103389fneur201200073
Chappell N L and Penning M (1996) Behaviouralproblems and distress among caregivers of people withdementia Ageing amp Society 16 57ndash73doi101017s0144686x00003135
Chiu Y C et al (2014) Family caregiversrsquo sleepdisturbance and its associations with multilevel stressorswhen caring for patients with dementia Aging amp MentalHealth 18 92ndash101 doihttpdxdoiorg101080136078632013837141
Cohen J (1988) Statistical Power Analysis for the BehavioralSciences 2nd edn New York University New YorkLawrence Erlbaum Associatesdoi1043249780203771587
Conde-Sala J L Garre-Olmo J Turroacute-Garriga OVilalta-Franch J and Loacutepez-Pousa S (2010)Differential features of burden between spouse andadult-child caregivers of patients with Alzheimerrsquos diseasean exploratory comparative design International Journal ofNursing Studies 47 1262ndash1273doi101016jijnurstu201003001
Covinsky K E et al (2003) Patient and caregivercharacteristics associated with depression in caregivers ofpatients with dementia Journal of General Internal Medicine18 1006ndash1014 doihttpdxdoiorg101111j1525-1497200330103x
Craig D Mirakhur A Hart D J McIlroy S P andPassmore A P (2005) A cross-sectional study ofneuropsychiatric symptoms in 435 patients withAlzheimerrsquos disease American Journal of GeriatricPsychiatry 13 460ndash468 doi10109700019442-200506000-00004
Crellin N Charlesworth G and Orrell M (2014)Measuring family caregiver efficacy for managing behavioraland psychological symptoms in dementia a psychometricevaluation International Psychogeriatrics 26 93ndash103 doihttpdxdoiorg101017s1041610213001646
Davidsdottir S R Snaedal J Karlsdottir GAtladottir I and Hannesdottir K (2012) Validationof the Icelandic version of the neuropsychiatric inventorywith caregiver distress (NPI-D) Nordic Journal of
Psychiatry 66 26ndash32 doihttpdxdoiorg103109080394882011593100
Davis J D and Tremont G (2007) Impact of frontalsystems behavioral functioning in dementia on caregiverburden The Journal of Neuropsychiatry and ClinicalNeurosciences 19 43ndash49 doihttpdxdoiorg101176jnp200719143
de Vugt M E Riedijk S R Aalten P Tibben Avan Swieten J C and Verhey F R J (2006) Impactof behavioural problems on spousal caregivers acomparison between Alzheimerrsquos disease andfronto-temporal dementia Dementia and Geriatric CognitiveDisorders 22 35ndash41 doi101159000093102
de Vugt M E et al (2003) Behavioural disturbances indementia patients and quality of the marital relationshipInternational Journal of Geriatric Psychiatry 18 149ndash154doi101002gps807
Donaldson C Tarrier N and Burns A (1998)Determinants of carer stress in Alzheimerrsquos diseaseInternational Journal of Geriatric Psychiatry 13 248ndash256doi101002(sici)1099-1166(199804)134lt248aid-gps770gt30co2-0
Downs S and Black N (1998) The feasibility of creating achecklist for the assessment of the methodological qualityboth of randomised and non-randomised studies of healthcare interventions Journal of Epidemiological CommunityHealth 52 377ndash384 doi101136jech526377
Farran C J Loukissa D A Lindeman D A andMcCann J (2004) Caring for self while caring for othersthe two-track life of coping with Alzheimerrsquos diseaseJournal of Gerontological Nursing 30 38ndash45doi1039280098-9134-20040501-09
Fauth E B and Gibbons A (2014) Which behavioral andpsychological symptoms of dementia are the mostproblematic Variability by prevalence intensity distressratings and associations with carer depressive symptomsInternational Journal of Geriatric Psychiatry 29 263ndash271doi101002gps4002
Fuh J L Liu C K Mega M S Wang S J andCummings J L (2001) Behavioral disorders andcaregiversrsquo reaction in Taiwanese patients with Alzheimerrsquosdisease International Psychogeriatrics 13 121ndash128 doihttpdxdoiorg101017s1041610201007517
Gaugler J E et al (2011) Does caregiver burden mediatethe effects of behavioral disturbances on nursing homeadmission The American Journal of Geriatric Psychiatry 19497ndash506 doi101097jgp0b013e31820d92cc
Gilleard C J Belford H Gilleard E Whittick J Eand Gledhill K (1984) Emotional distress amongst thesupporters of the elderly mental infirm British Journal ofPsychiatry 145 172ndash177doihttpdxdoiorg101192bjp1452172
Gitlin L N and Rose K (2014) Factors associated withcarer readiness to use nonpharmacologic strategies tomanage dementia-related behavioral symptomsInternational Journal of Geriatric Psychiatry 29 93ndash102doihttpdxdoiorg101002gps3979
Goldberg D P and Hillier V F (1979) A scaled versionof the general health questionnaire Psychological Medicine9 139ndash145 doi101017s0033291700021644
Gonzalez-Salvador M T Arango C Lyketsos C Gand Barba A C (1999) The stress and psychological
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1773
morbidity of the Alzheimer patient caregiver InternationalJournal of Geriatric Psychiatry 14 701ndash710doi101002(sici)1099-1166(199909)149lt701aidps5gt30co2-
Haley W E Brown S and Levine E G (1987) Familycaregiver appraisals of patient behavioral disturbance insenile dementia Clinical Gerontologist The Journal of Agingand Mental Health 6 25ndash34doi101300j018v06n04_04
Haley W E Levine E G Brown S L Berry J Wand Hughes G H (2008) The psychological social andhealth consequences of caring for a relative with seniledementia Journal of the American Geriatrics Society 35405ndash411 doi101111j1532-54151987tb04661x
Hishikawa N et al (2012) Effects of turmeric onAlzheimerrsquos disease with behavioral and psychologicalsymptoms of dementia Ayu 33 499ndash504 doihttpdxdoiorg1041030974-8520110524
Huang S S Lee M C Liao Y C Wang W F andLai T J (2012) Caregiver burden associated withbehavioral and psychological symptoms of dementia(BPSD) in Taiwanese elderly Archives of Gerontology andGeriatrics 55 55ndash59 doihttpdxdoiorg101016jarchger201104009
Jackson M A Fauth E B and Geiser C (2014)Comparing the neuropsychiatric inventory and the revisedmemory and behavior problems checklist for associationswith caregiver burden and depressive symptomsInternational Psychogeriatrics 26 1021ndash1031doi101017s1041610213002421
Johnson D K Niedens M Wilson J RSwartzendruber L Yeager A and Jones K (2013)Treatment outcomes of a crisis intervention program fordementia with severe psychiatric complications the Kansasbridge project The Gerontologist 53 102ndash112 doihttpdxdoiorg101093gerontgns104
Khoo S A Chen T Y Ang Y H and Yap P (2013)The impact of neuropsychiatric symptoms on caregiverdistress and quality of life in persons with dementia in anAsian tertiary hospital memory clinic InternationalPsychogeriatrics 25 1991ndash1999 doihttpdxdoiorg101017s1041610213001518
Kosberg J I Kaufman A V Burgio L D Leeper Jand Sun F (2007) Family caregiving to those withdementia in rural Alabama racial similarities anddifferences Journal of Aging and Health 19 3ndash21 doi1011770898264306293604
Kosmala K and Kloszewska I (2004) The burden ofproviding care for Alzheimerrsquos disease patients in PolandInternational Journal of Geriatric Psychiatry 19 191ndash193doi101002gps1054
Landis J R and Koch G G (1977) The measurement ofobserver agreement for categorical data Biometrics 33159ndash174 doi 1023072529310
Lee D R McKeith I Mosimann U Ghosh-NodyalA and Thomas A J (2013) Examining carer stress indementia the role of subtype diagnosis andneuropsychiatric symptoms International Journal ofGeriatric Psychiatry 28 135ndash141 doihttpdxdoiorg101002gps3799
Lim Y M Son G R Song J A and Beattie E(2008) Factors affecting burden of family caregivers of
community-dwelling ambulatory elders with dementia inKorea Archives of Psychiatric Nursing 22 226ndash234 doi101016japnu200712005
Matsumoto N et al (2007) Caregiver burden associatedwith behavioral and psychological symptoms of dementia inelderly people in the local community Dementia andGeriatric Cognitive Disorders 23 219ndash224doi101159000099472
Mohamed S Rosenheck R Lyketsos C G andSchneider L S (2010) Caregiver burden in Alzheimerdisease cross-sectional and longitudinal patient correlatesThe American Journal of Geriatric Psychiatry 18 917ndash927doi101097jgp0b013e3181d5745d
Mourik J C Rosso S M Niermeijer M FDuivenvoorden H J Van Swieten J C and TibbenA (2004) Frontotemporal dementia behavioral symptomsand caregiver distress Dementia and Geriatric CognitiveDisorders 18 299ndash306 doihttpdxdoiorg101159000080123
Muangpaisan W et al (2010) Caregiver burden and needsof dementia caregivers in Thailand a cross-sectional studyJournal of the Medical Association of Thailand 93 601ndash607
Neundorfer M M McClendon M J Smyth K AStuckey J C Strauss M E and Patterson M B(2001) A longitudinal study of the relationship betweenlevels of depression among persons with Alzheimerrsquosdisease and levels of depression among their familycaregivers Journal of Gerontology Series B - PsychologicalSciences and Social Sciences 56 301ndash313
Nygaard H A (1998) Strain on caregivers of dementedelderly people living at home Scandinavian Journal ofPrimary Health Care 6 33ndash37doihttpdxdoiorg10310902813438809009287
Ornstein K and Gaugler J E (2012) The problem withldquoproblem behaviorsrdquoa systematic review of the associationbetween individual patient behavioral and psychologicalsymptoms and caregiver depression and burden within thedementia patientndashcaregiver dyad InternationalPsychogeriatrics 24 1536ndash1552doi101017s1041610212000737
Ornstein K Gaugler J E Devanand N S CarolynZ and Yaakov S (2012) The differential impact ofunique behavioral and psychological symptoms for thedementia caregiver how and why do patientsrsquo individualsymptom clusters impact caregiver depressive symptomsThe American Journal of Geriatric Psychiatry 12 77ndash1286doi httpdxdoiorg101016jjagp201301062
Price G R (1970) Selection and covariance Nature 227520ndash521 doi101038227520a0
Prince M (2000) Dementia in developing countries Aconsensus statement from the 1066 Dementia ResearchGroup International Journal of Geriatric Psychiatry 1514ndash20 doihttpdxdoiorg101002(sici)1099-1166(200001)151lt14aid-gps70gt30co2-8
Quayhagen M P and Quayhagen M (1998) Alzheimerrsquosstress coping with the caregiving role Gerontologist 28391ndash396 doihttpdxdoiorg101093geront283391
Reisberg B Ferris S H de Leon M J and Crook T(1982) The global deterioration scale for assessment ofprimary degenerative dementia American Journal ofPsychiatry 139 1136ndash1139 doihttpdxdoiorg101176ajp13991136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1774 A Feast et al
Robinson K M Adkisson P and Weinrich S (2001)Problem behaviour caregiver reactions and impact amongcaregivers of persons with Alzheimerrsquos disease Journal ofAdvanced Nursing 36 573ndash582 doihttpdxdoiorg101046j1365-2648200102010x
Rocca P et al (2010) Neuropsychiatric symptomsunderlying caregiver stress and insight in Alzheimerrsquosdisease Dementia and Geriatric Cognitive Disorders 3057ndash63 doi101159000315513
Rymer S Salloway S Norton L Mallow PCorreia S and Monast D (2002) Impaired awarenessbehavior disturbance and caregiver burden in Alzheimerdisease Alzheimer Disease and Associated Disorders 16248ndash253 doi 10109700002093-200210000-00006
Savorani G Vulcano V Boni S Sarti G andRavaglia G (1998) Behavioral disorders in dementiapatients and their impact on the stress of caregivingrelatives the ldquoARADrdquo questionnaire Archives ofGerontology and Geriatrics 6 481ndash485doi101016s0167-4943(98)80070-8
Shaji K S George R K Prince M J and JacobK S (2009) Behavioral symptoms and caregiver burdenin dementia Indian Journal of Psychiatry 51 45 doihttpdxdoiorg1041030019-554544905
Sink K M Covinsky K E Barnes D E NewcomerR J and Yaffe K (2006) Caregiver characteristics areassociated with neuropsychiatric symptoms of dementiaJournal of the American Geriatrics Society 54 796ndash803 doi101111j1532-5415200600697x
Slachevsky A et al (2013) The CUIDEME studydeterminants of burden in chilean primary caregivers ofpatients with dementia Journal of Alzheimerrsquos Disease 35297ndash306
Spiegel R et al (1991) A new behavioral assessment scalefor geriatric out- and in-patients the NOSGER (nursesrsquoobservation scale for geriatric patients) Journal of theAmerican Geriatric Society 39 339ndash347 doihttpdxdoiorg101111j1532-54151991tb02897x
Tan L L Wong H B and Allen H (2005) The impactof neuropsychiatric symptoms of dementia on distress infamily and professional caregivers in SingaporeInternational Psychogeriatrics 17 253ndash263 doi101017s1041610205001523
Teri L (1997) Behavior and caregiver burden behavioralproblems in patients with Alzheimer disease and itsassociation with caregiver distress Alzheimer Disease andAssociated Disorders 11 35ndash38
Teri L Truax P Logsdon R Uomoto J Zarit Sand Vitaliano P P (1992) Assessment of behavioralproblems in dementia the revised memory and behaviorproblems checklist Psychology and Aging 7 622 doi1010370882-797474622
Waite A Bebbington P Skelton-Robinson M andOrrell M (2004) Social factors and depression in carersof people with dementia International Journal of GeriatricPsychiatry 19 582ndash587 doihttpdxdoiorg101002gps1136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at

Individual BPSD and caregiver well-being 1769
experiencing more BPSD might be more likely toattend a clinic as indeed were the majority ofstudies included in the meta-analysis It may bepossible that dementia severity is an explanationsince participants in the studies with the highestdistress scores (Tan et al 2005 Balieiro et al 2010)had moderate and severe dementia respectivelywhereas Baiyewu et al (2003) who consistentlyreported the lowest distress scores across eachof the behavior domains included participantswith mild dementia However both Aarslandet al (2007) and de Vugt et al (2006) reportedlower mean distress scores in comparison with theother included studies and they both includedparticipants with moderate dementia FurthermoreDavidsdottir et al (2012) found that there wasno significant difference between caregiver distressscores depending on dementia severity
Baiyewu et al (2003) had a much smallersample of spousal caregivers in comparison to Tanet al (2005) which might account for the lowerdistress scores This is in agreement with Almberget al (1997) who reported that spouses experiencegreater levels of burden However three studieswhich had consistently higher mean distress scoresacross all behaviors (Tan et al 2005 Balieiro et al2010 Huang et al 2012) were mainly comprisedof adult-child caregivers When comparing a studysolely comprised of spousal caregivers (deVugt et al2006) with a study (Baiyewu et al 2003) withminimal spousal caregivers (25) it was possibleto see that spousal caregivers were substantiallymore distressed with depressive apathetic andanxiety-related behaviors Although distress ratingscan be differentiated between behavior types forspousal and non-spousal caregivers both Baiyewuet al (2003) and de Vugt et al (2006) had two of thelowest distress scores across all behaviors in compar-ison to the other studies in the meta-analysis
The explanation may also be cultural sinceBaiyewu et al (2003) and Baiyewu et al (2012)(with similarly low distress scores across behaviors)were the only Africa-based studies in the meta-analysis Baiyewu et al (2003) and Baiyewu et al(2012) were also both community-based studieswhich may also be a reason for the reduceddistress ratings There is every reason to believethat BPSD are present across cultures (Shajiet al 2009) however the low levels of publicawareness of dementia have many implications(Prince 2000) One of these implications maybe the misinterpretation of BPSD as deliberateconsequently affecting the well-being of the carer(Shaji et al 2009) It is beyond the scope ofthis paper to determine why there is considerablevariation between studies reporting caregiverdistress for identical behaviors using identical
measures However it is likely that it is the caregivercharacteristics rather than the characteristics of theperson with dementia (such as dementia severity)which may underlie the explanation as to whyvariation between studies exists
Limitations
The data available for this review allowed for onlytwo meta-analyses to be conducted There wererelatively few studies which assessed the relationshipbetween individual BPSD and caregiver well-beingand which met the inclusionexclusion criteriafor the review In an attempt to be systematicbased on prior recommendation an effort wasmade to distinguish between how ldquoproblematicrdquosymptoms are measured Consequently studieswere categorized into whether BPSD weremeasured in terms of frequency or prevalence andalso categorized in terms of the statistical analysisemployed Other than data regarding mean distressassociated with NPI total score only a small amountof studies were included in each category andunfortunately it was often the case that measuresof caregiver well-being were dissimilar From the 40included studies there were 12 different measuresof behavior and 17 different measures of well-being making comparisons difficult which mayhave contributed to the inconsistent findings
The majority of included studies recruitedparticipants from clinics therefore caregiversincluded in the review were not representative ofthe population In addition the samples across theincluded studies were heterogeneous in a numberof factors therefore caution should be taken wheninterpreting the results Although beyond the scopeof this review study characteristics such as culturegender and relationship direction were not ex-amined through subgroup analyses Due to the lim-ited number of studies it was not possible to imposea quality criteria however all included studies wereeither of high or medium quality as assessed by theDowns and Back Checklist (1998) Furthermore allof the included studies relied on caregiver reportsof BPSD which may themselves be affected bycaregiver well-being unfortunately it is not possibleto determine if this was the case Nonetheless twovalid meta-analyses were completed and a numberof comments can be made about the relationshipbetween BPSD and caregiver well-being
Implications and recommendations
The vast majority of studies addressing the rela-tionship between BPSD and caregiver well-being
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1770 A Feast et al
did not examine individual BPSD Consequentlythis comparatively limited the amount of studiesincluded in the present review Therefore if we areto understand this relationship more studies needto examine individual BPSD in their research Inaddition it is more clinically relevant to examinewhich BPSD affect well-being rather than BPSDas a whole as this is essential in determiningwhere clinical staff should allocate resources mosteffectively Nevertheless there is preliminary datasuggesting it is mood-related behaviors whichare associated with increased levels of distresstherefore interventions for the management ofBPSD should target these behaviors
The lack of consistency in the measurementof BPSD (neuropsychiatric or memory problemsfrequency or prevalence) and the measurementof caregiver well-being (the use of interchangeableterminology such as stress strain and burdenmeaning the same construct) limits our ability toreach a consensus as to which BPSD result inthe most negative outcomes for caregivers Forexample Donaldson et al (1998) used GilleardrsquosStrain Scale (1984) to measure burden andthe General Health Questionnaire (Goldberg andHillier 1979) to measure distress Furthermorefour studies (see Table S1) did not have formalscales to measure the impact of BPSD on well-being and used terms such as ldquoburdensomerdquoldquoseriousrdquo and ldquodisturbingrdquo This problem impactsupon the validity and reliability of the originalstudies and consequently the review Howeverthis mainly occurred in the earlier studies Futureresearch should also include more than one measureof well-being in order to identify if individual BPSDdifferentially affect caregiver burden compared tocaregiver distress as identified in the current reviewFurthermore future research should identify whythere is reduced variability in distress ratings forcertain behaviors compared to others and whycertain behaviors are more distressing dependingon which type of statistical analysis is used
Although there are potential methodologicalreasons (limited studies inconsistent measures)for why there is substantial variability whenidentifying which BPSD affect certain types ofcaregiver well-being the most there is growingevidence that factors associated with the personwith dementia (eg BPSD frequency cognition) areonly part of the story when explaining a caregiverrsquosresponse to BPSD Caregiver characteristicshave been shown to account for twice thevariance of person with dementia characteristicswhen reporting neuropsychiatric symptoms (Sinket al 2006) and the presence of BPSD wasnot found to be a significant predictor ofburden whereas caregiver characteristics such as
confidence neuroticism and relationship qualitywere significant predictors (Campbell et al 2008)Therefore as recommended by Ornstein andGaugler (2012) future studies should focus onidentifying pathways for the association betweenindividual BPSD caregiver variables and caregiveroutcomes More research is needed to understandif and why certain BPSD affect certain caregiveroutcomes and also how much of this is attributableto caregiver variability in response to BPSD ratherthan the presence of BPSD itself More longitudinalstudies would be useful to examine how changes inindividual BPSD are associated with caregiver well-being over time A review by Black and Almeida(2004) examined the limited longitudinal studiesavailable and reported mixed findings betweenburden and BPSD and found no associationbetween BPSD and distress Although BPSDincreased significantly over a two-year periodcaregiver burden remained stable and depressionwas found to decrease (Berger et al 2005) Futureresearch needs to examine caregiver factors overtime (well-being role captivity etc) along withchanges in individual BPSD in order to have a morevalid understanding of this relationship
Caution should be exercised when creating ameasure of BPSD since Jackson et al (2014)found that the Revised Memory and BehaviorProblem Checklist (Teri et al 1992) might bemore suitable in explaining caregiver depressionthan the NPI It is important that the measureof BPSD is not biased toward explaining a moreunique association between BPSD and a measure ofcaregiver well-being such as depression As stated byGitlin and Rose (2014) item selection for measuresof BPSD is often based upon specific disciplines(eg neurology psychiatry social sciences) andthus implicitly represents different conceptual-izations of behavior A shared framework fordefining behaviors and their underlying causesmust be created in order to move on fromthe implicit assumption of most measures thatbehaviors are a direct cause of neuropathologyand to develop measures which also address thecontextual and caregiver characteristics associatedwith the behavior
Conclusions
This study has improved our understanding of theimpact of individual BPSD on caregiver well-beingin particular caregiver distress The relationshipbetween individual BPSD and caregiver well-beingwas inconsistent and varied according to behavioralsymptom Due to limited studies and heterogeneousdata the results should be interpreted with caution
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1771
but advances have been made with respect towhich behaviors are associated with distress Theinconsistencies may be partly explained by caregivervariables which were not taken into account inthe review Based on this review and previousresearch it is not possible to fully understand therelationship between BPSD and caregiver well-being without examining the influence of caregivervariables such as caregiver strategies acceptancegender relationship with person with dementiaand confidence We recommend that future studiesare designed to examine individual BPSD ratherthan BPSD as a whole use consistent measures forBPSD and well-being use consistent terminologyfor psychological constructs (eg burden) andexamine the causal mechanisms by which individualBPSD impact caregiver well-being by collectingdata on a range of caregiver factors Theseapproaches will clarify whether it is important forclinicians to focus on the frequency or prevalence ofcertain BPSD in addition to targeting the presenceof certain caregiver characteristics and addressingunmet need
Conflict of interest
None
Description of authorsrsquo roles
A Feast was responsible for developing the reviewobjectives writing the search strategies conductingthe searches designing and completing studyeligibility and data extraction forms undertakingthe quality appraisals conducting the meta-analysisand writing the paper M Orrell was responsible fordeveloping the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper C Stoner was responsible forundertaking the quality appraisals and assisting inwriting the paper G Charlesworth was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper E Moniz-Cook was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper
Acknowledgments
We would like to thank Dr Zoeuml Hoare for herstatistical advice This paper presents independentresearch funded by the National Institute for HealthResearch (NIHR) under its Programme Grants forApplied Research (RP-PG-0606-1067 and RP-PG-
060- 1083) The views expressed in this publicationare those of the author(s) and not necessarily thoseof the NHS the NIHR or the Department ofHealth
Supplementary Material
To view supplementary material for thisarticle please visit httpdxdoiorg101017S1041610216000922
References
Aarsland D et al (2007) Neuropsychiatric symptoms inpatients with Parkinsonrsquos disease and dementia frequencyprofile and associated care giver stress Journal of NeurologyNeurosurgery amp Psychiatry 78 36ndash42doihttpdxdoiorg101136jnnp2005083113
Allegri R F et al (2006) Neuropsychiatric symptoms as apredictor of caregiver burden in Alzheimerrsquos diseaseNeuropsychiatric Disease amp Treatment 2 105ndash110doi102147ndts47133
Almberg B Grafstrom M and Winblad B (1997)Major strain and coping strategies as reported by familymembers who care for aged demented relatives Journal ofAdvanced Nursing 26 683ndash691doihttpdxdoiorg101046j1365-2648199700392x
Arango-Lasprilla J C Lehan T Drew A MorenoA Deng X and Lemos M (2010) Health-relatedquality of life in caregivers of individuals with dementiafrom Colombia American Journal of Alzheimerrsquos Disease andOther Dementias 25 556ndash561doi1011771533317510382287ltbibgt
Baiyewu O et al (2003) Behavioral and caregiver reactionof dementia as measured by the neuropsychiatric inventoryin Nigerian community residents InternationalPsychogeriatrics 15 399ndash409doi101017s1041610203009645
Baiyewu O et al (2012) Behavioral symptoms incommunity-dwelling elderly Nigerians with dementia mildcognitive impairment and normal cognition InternationalJournal of Geriatric Psychiatry 27 931ndash939 doihttpdxdoiorg101002gps2804
Balieiro A P Jr Sobreira E S T Pena M C SSilva-Filho J H and Vale F A C (2010) Caregiverdistress associated with behavioral and psychologicalsymptoms in mild Alzheimerrsquos disease Dementia eNeuropsychologia 4 238ndash244
Ballard C G et al (1995) The aetiology of depression inthe carers of dementia sufferers Journal of AffectiveDisorders 35 59ndash63 doi1010160165-0327(95)00041-k
Bandeira D R Pawlowski J Goncalves T RHilgert J B Bozzetti M C and Hugo F N (2007)Psychological distress in Brazilian caregivers of relativeswith dementia Aging and Mental Health 11 14ndash19doi10108013607860600640814
Berger G Bernhardt T Weimer E Peters JKratzsch T and Frolich L (2005) Longitudinal studyon the relationship between symptomatology of dementia
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1772 A Feast et al
and levels of subjective burden and depression amongfamily caregivers in memory clinic patients Journal ofGeriatric Psychiatry and Neurology 3 119ndash128doi1011770891988704273375
Black W and Almeida O P (2004) A systematic reviewof the association between the behavioral and psychologicalsymptoms of dementia and burden of care InternationalPsychogeriatrics 16 295ndash315doi101017s1041610204000468
Bruce D G and Paterson A (2000) Barriers tocommunity support for the dementia carer a qualitativestudy International Journal of Geriatric Psychiatry 15451ndash457 doi101002(sici)1099-1166(200005)155lt451aid-gps143gt30co2-k
Campbell P et al (2008) Determinants of burden in thosewho care for someone with dementia International Journalof Geriatric Psychiatry 23 1078ndash1085doi101002gps2071
Cerejeira J Lagarto L and Mukaetova-LadinskaE B (2012) Behavioral and psychological symptoms ofdementia Frontiers in Neurology 3 1ndash23doi103389fneur201200073
Chappell N L and Penning M (1996) Behaviouralproblems and distress among caregivers of people withdementia Ageing amp Society 16 57ndash73doi101017s0144686x00003135
Chiu Y C et al (2014) Family caregiversrsquo sleepdisturbance and its associations with multilevel stressorswhen caring for patients with dementia Aging amp MentalHealth 18 92ndash101 doihttpdxdoiorg101080136078632013837141
Cohen J (1988) Statistical Power Analysis for the BehavioralSciences 2nd edn New York University New YorkLawrence Erlbaum Associatesdoi1043249780203771587
Conde-Sala J L Garre-Olmo J Turroacute-Garriga OVilalta-Franch J and Loacutepez-Pousa S (2010)Differential features of burden between spouse andadult-child caregivers of patients with Alzheimerrsquos diseasean exploratory comparative design International Journal ofNursing Studies 47 1262ndash1273doi101016jijnurstu201003001
Covinsky K E et al (2003) Patient and caregivercharacteristics associated with depression in caregivers ofpatients with dementia Journal of General Internal Medicine18 1006ndash1014 doihttpdxdoiorg101111j1525-1497200330103x
Craig D Mirakhur A Hart D J McIlroy S P andPassmore A P (2005) A cross-sectional study ofneuropsychiatric symptoms in 435 patients withAlzheimerrsquos disease American Journal of GeriatricPsychiatry 13 460ndash468 doi10109700019442-200506000-00004
Crellin N Charlesworth G and Orrell M (2014)Measuring family caregiver efficacy for managing behavioraland psychological symptoms in dementia a psychometricevaluation International Psychogeriatrics 26 93ndash103 doihttpdxdoiorg101017s1041610213001646
Davidsdottir S R Snaedal J Karlsdottir GAtladottir I and Hannesdottir K (2012) Validationof the Icelandic version of the neuropsychiatric inventorywith caregiver distress (NPI-D) Nordic Journal of
Psychiatry 66 26ndash32 doihttpdxdoiorg103109080394882011593100
Davis J D and Tremont G (2007) Impact of frontalsystems behavioral functioning in dementia on caregiverburden The Journal of Neuropsychiatry and ClinicalNeurosciences 19 43ndash49 doihttpdxdoiorg101176jnp200719143
de Vugt M E Riedijk S R Aalten P Tibben Avan Swieten J C and Verhey F R J (2006) Impactof behavioural problems on spousal caregivers acomparison between Alzheimerrsquos disease andfronto-temporal dementia Dementia and Geriatric CognitiveDisorders 22 35ndash41 doi101159000093102
de Vugt M E et al (2003) Behavioural disturbances indementia patients and quality of the marital relationshipInternational Journal of Geriatric Psychiatry 18 149ndash154doi101002gps807
Donaldson C Tarrier N and Burns A (1998)Determinants of carer stress in Alzheimerrsquos diseaseInternational Journal of Geriatric Psychiatry 13 248ndash256doi101002(sici)1099-1166(199804)134lt248aid-gps770gt30co2-0
Downs S and Black N (1998) The feasibility of creating achecklist for the assessment of the methodological qualityboth of randomised and non-randomised studies of healthcare interventions Journal of Epidemiological CommunityHealth 52 377ndash384 doi101136jech526377
Farran C J Loukissa D A Lindeman D A andMcCann J (2004) Caring for self while caring for othersthe two-track life of coping with Alzheimerrsquos diseaseJournal of Gerontological Nursing 30 38ndash45doi1039280098-9134-20040501-09
Fauth E B and Gibbons A (2014) Which behavioral andpsychological symptoms of dementia are the mostproblematic Variability by prevalence intensity distressratings and associations with carer depressive symptomsInternational Journal of Geriatric Psychiatry 29 263ndash271doi101002gps4002
Fuh J L Liu C K Mega M S Wang S J andCummings J L (2001) Behavioral disorders andcaregiversrsquo reaction in Taiwanese patients with Alzheimerrsquosdisease International Psychogeriatrics 13 121ndash128 doihttpdxdoiorg101017s1041610201007517
Gaugler J E et al (2011) Does caregiver burden mediatethe effects of behavioral disturbances on nursing homeadmission The American Journal of Geriatric Psychiatry 19497ndash506 doi101097jgp0b013e31820d92cc
Gilleard C J Belford H Gilleard E Whittick J Eand Gledhill K (1984) Emotional distress amongst thesupporters of the elderly mental infirm British Journal ofPsychiatry 145 172ndash177doihttpdxdoiorg101192bjp1452172
Gitlin L N and Rose K (2014) Factors associated withcarer readiness to use nonpharmacologic strategies tomanage dementia-related behavioral symptomsInternational Journal of Geriatric Psychiatry 29 93ndash102doihttpdxdoiorg101002gps3979
Goldberg D P and Hillier V F (1979) A scaled versionof the general health questionnaire Psychological Medicine9 139ndash145 doi101017s0033291700021644
Gonzalez-Salvador M T Arango C Lyketsos C Gand Barba A C (1999) The stress and psychological
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1773
morbidity of the Alzheimer patient caregiver InternationalJournal of Geriatric Psychiatry 14 701ndash710doi101002(sici)1099-1166(199909)149lt701aidps5gt30co2-
Haley W E Brown S and Levine E G (1987) Familycaregiver appraisals of patient behavioral disturbance insenile dementia Clinical Gerontologist The Journal of Agingand Mental Health 6 25ndash34doi101300j018v06n04_04
Haley W E Levine E G Brown S L Berry J Wand Hughes G H (2008) The psychological social andhealth consequences of caring for a relative with seniledementia Journal of the American Geriatrics Society 35405ndash411 doi101111j1532-54151987tb04661x
Hishikawa N et al (2012) Effects of turmeric onAlzheimerrsquos disease with behavioral and psychologicalsymptoms of dementia Ayu 33 499ndash504 doihttpdxdoiorg1041030974-8520110524
Huang S S Lee M C Liao Y C Wang W F andLai T J (2012) Caregiver burden associated withbehavioral and psychological symptoms of dementia(BPSD) in Taiwanese elderly Archives of Gerontology andGeriatrics 55 55ndash59 doihttpdxdoiorg101016jarchger201104009
Jackson M A Fauth E B and Geiser C (2014)Comparing the neuropsychiatric inventory and the revisedmemory and behavior problems checklist for associationswith caregiver burden and depressive symptomsInternational Psychogeriatrics 26 1021ndash1031doi101017s1041610213002421
Johnson D K Niedens M Wilson J RSwartzendruber L Yeager A and Jones K (2013)Treatment outcomes of a crisis intervention program fordementia with severe psychiatric complications the Kansasbridge project The Gerontologist 53 102ndash112 doihttpdxdoiorg101093gerontgns104
Khoo S A Chen T Y Ang Y H and Yap P (2013)The impact of neuropsychiatric symptoms on caregiverdistress and quality of life in persons with dementia in anAsian tertiary hospital memory clinic InternationalPsychogeriatrics 25 1991ndash1999 doihttpdxdoiorg101017s1041610213001518
Kosberg J I Kaufman A V Burgio L D Leeper Jand Sun F (2007) Family caregiving to those withdementia in rural Alabama racial similarities anddifferences Journal of Aging and Health 19 3ndash21 doi1011770898264306293604
Kosmala K and Kloszewska I (2004) The burden ofproviding care for Alzheimerrsquos disease patients in PolandInternational Journal of Geriatric Psychiatry 19 191ndash193doi101002gps1054
Landis J R and Koch G G (1977) The measurement ofobserver agreement for categorical data Biometrics 33159ndash174 doi 1023072529310
Lee D R McKeith I Mosimann U Ghosh-NodyalA and Thomas A J (2013) Examining carer stress indementia the role of subtype diagnosis andneuropsychiatric symptoms International Journal ofGeriatric Psychiatry 28 135ndash141 doihttpdxdoiorg101002gps3799
Lim Y M Son G R Song J A and Beattie E(2008) Factors affecting burden of family caregivers of
community-dwelling ambulatory elders with dementia inKorea Archives of Psychiatric Nursing 22 226ndash234 doi101016japnu200712005
Matsumoto N et al (2007) Caregiver burden associatedwith behavioral and psychological symptoms of dementia inelderly people in the local community Dementia andGeriatric Cognitive Disorders 23 219ndash224doi101159000099472
Mohamed S Rosenheck R Lyketsos C G andSchneider L S (2010) Caregiver burden in Alzheimerdisease cross-sectional and longitudinal patient correlatesThe American Journal of Geriatric Psychiatry 18 917ndash927doi101097jgp0b013e3181d5745d
Mourik J C Rosso S M Niermeijer M FDuivenvoorden H J Van Swieten J C and TibbenA (2004) Frontotemporal dementia behavioral symptomsand caregiver distress Dementia and Geriatric CognitiveDisorders 18 299ndash306 doihttpdxdoiorg101159000080123
Muangpaisan W et al (2010) Caregiver burden and needsof dementia caregivers in Thailand a cross-sectional studyJournal of the Medical Association of Thailand 93 601ndash607
Neundorfer M M McClendon M J Smyth K AStuckey J C Strauss M E and Patterson M B(2001) A longitudinal study of the relationship betweenlevels of depression among persons with Alzheimerrsquosdisease and levels of depression among their familycaregivers Journal of Gerontology Series B - PsychologicalSciences and Social Sciences 56 301ndash313
Nygaard H A (1998) Strain on caregivers of dementedelderly people living at home Scandinavian Journal ofPrimary Health Care 6 33ndash37doihttpdxdoiorg10310902813438809009287
Ornstein K and Gaugler J E (2012) The problem withldquoproblem behaviorsrdquoa systematic review of the associationbetween individual patient behavioral and psychologicalsymptoms and caregiver depression and burden within thedementia patientndashcaregiver dyad InternationalPsychogeriatrics 24 1536ndash1552doi101017s1041610212000737
Ornstein K Gaugler J E Devanand N S CarolynZ and Yaakov S (2012) The differential impact ofunique behavioral and psychological symptoms for thedementia caregiver how and why do patientsrsquo individualsymptom clusters impact caregiver depressive symptomsThe American Journal of Geriatric Psychiatry 12 77ndash1286doi httpdxdoiorg101016jjagp201301062
Price G R (1970) Selection and covariance Nature 227520ndash521 doi101038227520a0
Prince M (2000) Dementia in developing countries Aconsensus statement from the 1066 Dementia ResearchGroup International Journal of Geriatric Psychiatry 1514ndash20 doihttpdxdoiorg101002(sici)1099-1166(200001)151lt14aid-gps70gt30co2-8
Quayhagen M P and Quayhagen M (1998) Alzheimerrsquosstress coping with the caregiving role Gerontologist 28391ndash396 doihttpdxdoiorg101093geront283391
Reisberg B Ferris S H de Leon M J and Crook T(1982) The global deterioration scale for assessment ofprimary degenerative dementia American Journal ofPsychiatry 139 1136ndash1139 doihttpdxdoiorg101176ajp13991136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1774 A Feast et al
Robinson K M Adkisson P and Weinrich S (2001)Problem behaviour caregiver reactions and impact amongcaregivers of persons with Alzheimerrsquos disease Journal ofAdvanced Nursing 36 573ndash582 doihttpdxdoiorg101046j1365-2648200102010x
Rocca P et al (2010) Neuropsychiatric symptomsunderlying caregiver stress and insight in Alzheimerrsquosdisease Dementia and Geriatric Cognitive Disorders 3057ndash63 doi101159000315513
Rymer S Salloway S Norton L Mallow PCorreia S and Monast D (2002) Impaired awarenessbehavior disturbance and caregiver burden in Alzheimerdisease Alzheimer Disease and Associated Disorders 16248ndash253 doi 10109700002093-200210000-00006
Savorani G Vulcano V Boni S Sarti G andRavaglia G (1998) Behavioral disorders in dementiapatients and their impact on the stress of caregivingrelatives the ldquoARADrdquo questionnaire Archives ofGerontology and Geriatrics 6 481ndash485doi101016s0167-4943(98)80070-8
Shaji K S George R K Prince M J and JacobK S (2009) Behavioral symptoms and caregiver burdenin dementia Indian Journal of Psychiatry 51 45 doihttpdxdoiorg1041030019-554544905
Sink K M Covinsky K E Barnes D E NewcomerR J and Yaffe K (2006) Caregiver characteristics areassociated with neuropsychiatric symptoms of dementiaJournal of the American Geriatrics Society 54 796ndash803 doi101111j1532-5415200600697x
Slachevsky A et al (2013) The CUIDEME studydeterminants of burden in chilean primary caregivers ofpatients with dementia Journal of Alzheimerrsquos Disease 35297ndash306
Spiegel R et al (1991) A new behavioral assessment scalefor geriatric out- and in-patients the NOSGER (nursesrsquoobservation scale for geriatric patients) Journal of theAmerican Geriatric Society 39 339ndash347 doihttpdxdoiorg101111j1532-54151991tb02897x
Tan L L Wong H B and Allen H (2005) The impactof neuropsychiatric symptoms of dementia on distress infamily and professional caregivers in SingaporeInternational Psychogeriatrics 17 253ndash263 doi101017s1041610205001523
Teri L (1997) Behavior and caregiver burden behavioralproblems in patients with Alzheimer disease and itsassociation with caregiver distress Alzheimer Disease andAssociated Disorders 11 35ndash38
Teri L Truax P Logsdon R Uomoto J Zarit Sand Vitaliano P P (1992) Assessment of behavioralproblems in dementia the revised memory and behaviorproblems checklist Psychology and Aging 7 622 doi1010370882-797474622
Waite A Bebbington P Skelton-Robinson M andOrrell M (2004) Social factors and depression in carersof people with dementia International Journal of GeriatricPsychiatry 19 582ndash587 doihttpdxdoiorg101002gps1136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at

1770 A Feast et al
did not examine individual BPSD Consequentlythis comparatively limited the amount of studiesincluded in the present review Therefore if we areto understand this relationship more studies needto examine individual BPSD in their research Inaddition it is more clinically relevant to examinewhich BPSD affect well-being rather than BPSDas a whole as this is essential in determiningwhere clinical staff should allocate resources mosteffectively Nevertheless there is preliminary datasuggesting it is mood-related behaviors whichare associated with increased levels of distresstherefore interventions for the management ofBPSD should target these behaviors
The lack of consistency in the measurementof BPSD (neuropsychiatric or memory problemsfrequency or prevalence) and the measurementof caregiver well-being (the use of interchangeableterminology such as stress strain and burdenmeaning the same construct) limits our ability toreach a consensus as to which BPSD result inthe most negative outcomes for caregivers Forexample Donaldson et al (1998) used GilleardrsquosStrain Scale (1984) to measure burden andthe General Health Questionnaire (Goldberg andHillier 1979) to measure distress Furthermorefour studies (see Table S1) did not have formalscales to measure the impact of BPSD on well-being and used terms such as ldquoburdensomerdquoldquoseriousrdquo and ldquodisturbingrdquo This problem impactsupon the validity and reliability of the originalstudies and consequently the review Howeverthis mainly occurred in the earlier studies Futureresearch should also include more than one measureof well-being in order to identify if individual BPSDdifferentially affect caregiver burden compared tocaregiver distress as identified in the current reviewFurthermore future research should identify whythere is reduced variability in distress ratings forcertain behaviors compared to others and whycertain behaviors are more distressing dependingon which type of statistical analysis is used
Although there are potential methodologicalreasons (limited studies inconsistent measures)for why there is substantial variability whenidentifying which BPSD affect certain types ofcaregiver well-being the most there is growingevidence that factors associated with the personwith dementia (eg BPSD frequency cognition) areonly part of the story when explaining a caregiverrsquosresponse to BPSD Caregiver characteristicshave been shown to account for twice thevariance of person with dementia characteristicswhen reporting neuropsychiatric symptoms (Sinket al 2006) and the presence of BPSD wasnot found to be a significant predictor ofburden whereas caregiver characteristics such as
confidence neuroticism and relationship qualitywere significant predictors (Campbell et al 2008)Therefore as recommended by Ornstein andGaugler (2012) future studies should focus onidentifying pathways for the association betweenindividual BPSD caregiver variables and caregiveroutcomes More research is needed to understandif and why certain BPSD affect certain caregiveroutcomes and also how much of this is attributableto caregiver variability in response to BPSD ratherthan the presence of BPSD itself More longitudinalstudies would be useful to examine how changes inindividual BPSD are associated with caregiver well-being over time A review by Black and Almeida(2004) examined the limited longitudinal studiesavailable and reported mixed findings betweenburden and BPSD and found no associationbetween BPSD and distress Although BPSDincreased significantly over a two-year periodcaregiver burden remained stable and depressionwas found to decrease (Berger et al 2005) Futureresearch needs to examine caregiver factors overtime (well-being role captivity etc) along withchanges in individual BPSD in order to have a morevalid understanding of this relationship
Caution should be exercised when creating ameasure of BPSD since Jackson et al (2014)found that the Revised Memory and BehaviorProblem Checklist (Teri et al 1992) might bemore suitable in explaining caregiver depressionthan the NPI It is important that the measureof BPSD is not biased toward explaining a moreunique association between BPSD and a measure ofcaregiver well-being such as depression As stated byGitlin and Rose (2014) item selection for measuresof BPSD is often based upon specific disciplines(eg neurology psychiatry social sciences) andthus implicitly represents different conceptual-izations of behavior A shared framework fordefining behaviors and their underlying causesmust be created in order to move on fromthe implicit assumption of most measures thatbehaviors are a direct cause of neuropathologyand to develop measures which also address thecontextual and caregiver characteristics associatedwith the behavior
Conclusions
This study has improved our understanding of theimpact of individual BPSD on caregiver well-beingin particular caregiver distress The relationshipbetween individual BPSD and caregiver well-beingwas inconsistent and varied according to behavioralsymptom Due to limited studies and heterogeneousdata the results should be interpreted with caution
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1771
but advances have been made with respect towhich behaviors are associated with distress Theinconsistencies may be partly explained by caregivervariables which were not taken into account inthe review Based on this review and previousresearch it is not possible to fully understand therelationship between BPSD and caregiver well-being without examining the influence of caregivervariables such as caregiver strategies acceptancegender relationship with person with dementiaand confidence We recommend that future studiesare designed to examine individual BPSD ratherthan BPSD as a whole use consistent measures forBPSD and well-being use consistent terminologyfor psychological constructs (eg burden) andexamine the causal mechanisms by which individualBPSD impact caregiver well-being by collectingdata on a range of caregiver factors Theseapproaches will clarify whether it is important forclinicians to focus on the frequency or prevalence ofcertain BPSD in addition to targeting the presenceof certain caregiver characteristics and addressingunmet need
Conflict of interest
None
Description of authorsrsquo roles
A Feast was responsible for developing the reviewobjectives writing the search strategies conductingthe searches designing and completing studyeligibility and data extraction forms undertakingthe quality appraisals conducting the meta-analysisand writing the paper M Orrell was responsible fordeveloping the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper C Stoner was responsible forundertaking the quality appraisals and assisting inwriting the paper G Charlesworth was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper E Moniz-Cook was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper
Acknowledgments
We would like to thank Dr Zoeuml Hoare for herstatistical advice This paper presents independentresearch funded by the National Institute for HealthResearch (NIHR) under its Programme Grants forApplied Research (RP-PG-0606-1067 and RP-PG-
060- 1083) The views expressed in this publicationare those of the author(s) and not necessarily thoseof the NHS the NIHR or the Department ofHealth
Supplementary Material
To view supplementary material for thisarticle please visit httpdxdoiorg101017S1041610216000922
References
Aarsland D et al (2007) Neuropsychiatric symptoms inpatients with Parkinsonrsquos disease and dementia frequencyprofile and associated care giver stress Journal of NeurologyNeurosurgery amp Psychiatry 78 36ndash42doihttpdxdoiorg101136jnnp2005083113
Allegri R F et al (2006) Neuropsychiatric symptoms as apredictor of caregiver burden in Alzheimerrsquos diseaseNeuropsychiatric Disease amp Treatment 2 105ndash110doi102147ndts47133
Almberg B Grafstrom M and Winblad B (1997)Major strain and coping strategies as reported by familymembers who care for aged demented relatives Journal ofAdvanced Nursing 26 683ndash691doihttpdxdoiorg101046j1365-2648199700392x
Arango-Lasprilla J C Lehan T Drew A MorenoA Deng X and Lemos M (2010) Health-relatedquality of life in caregivers of individuals with dementiafrom Colombia American Journal of Alzheimerrsquos Disease andOther Dementias 25 556ndash561doi1011771533317510382287ltbibgt
Baiyewu O et al (2003) Behavioral and caregiver reactionof dementia as measured by the neuropsychiatric inventoryin Nigerian community residents InternationalPsychogeriatrics 15 399ndash409doi101017s1041610203009645
Baiyewu O et al (2012) Behavioral symptoms incommunity-dwelling elderly Nigerians with dementia mildcognitive impairment and normal cognition InternationalJournal of Geriatric Psychiatry 27 931ndash939 doihttpdxdoiorg101002gps2804
Balieiro A P Jr Sobreira E S T Pena M C SSilva-Filho J H and Vale F A C (2010) Caregiverdistress associated with behavioral and psychologicalsymptoms in mild Alzheimerrsquos disease Dementia eNeuropsychologia 4 238ndash244
Ballard C G et al (1995) The aetiology of depression inthe carers of dementia sufferers Journal of AffectiveDisorders 35 59ndash63 doi1010160165-0327(95)00041-k
Bandeira D R Pawlowski J Goncalves T RHilgert J B Bozzetti M C and Hugo F N (2007)Psychological distress in Brazilian caregivers of relativeswith dementia Aging and Mental Health 11 14ndash19doi10108013607860600640814
Berger G Bernhardt T Weimer E Peters JKratzsch T and Frolich L (2005) Longitudinal studyon the relationship between symptomatology of dementia
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1772 A Feast et al
and levels of subjective burden and depression amongfamily caregivers in memory clinic patients Journal ofGeriatric Psychiatry and Neurology 3 119ndash128doi1011770891988704273375
Black W and Almeida O P (2004) A systematic reviewof the association between the behavioral and psychologicalsymptoms of dementia and burden of care InternationalPsychogeriatrics 16 295ndash315doi101017s1041610204000468
Bruce D G and Paterson A (2000) Barriers tocommunity support for the dementia carer a qualitativestudy International Journal of Geriatric Psychiatry 15451ndash457 doi101002(sici)1099-1166(200005)155lt451aid-gps143gt30co2-k
Campbell P et al (2008) Determinants of burden in thosewho care for someone with dementia International Journalof Geriatric Psychiatry 23 1078ndash1085doi101002gps2071
Cerejeira J Lagarto L and Mukaetova-LadinskaE B (2012) Behavioral and psychological symptoms ofdementia Frontiers in Neurology 3 1ndash23doi103389fneur201200073
Chappell N L and Penning M (1996) Behaviouralproblems and distress among caregivers of people withdementia Ageing amp Society 16 57ndash73doi101017s0144686x00003135
Chiu Y C et al (2014) Family caregiversrsquo sleepdisturbance and its associations with multilevel stressorswhen caring for patients with dementia Aging amp MentalHealth 18 92ndash101 doihttpdxdoiorg101080136078632013837141
Cohen J (1988) Statistical Power Analysis for the BehavioralSciences 2nd edn New York University New YorkLawrence Erlbaum Associatesdoi1043249780203771587
Conde-Sala J L Garre-Olmo J Turroacute-Garriga OVilalta-Franch J and Loacutepez-Pousa S (2010)Differential features of burden between spouse andadult-child caregivers of patients with Alzheimerrsquos diseasean exploratory comparative design International Journal ofNursing Studies 47 1262ndash1273doi101016jijnurstu201003001
Covinsky K E et al (2003) Patient and caregivercharacteristics associated with depression in caregivers ofpatients with dementia Journal of General Internal Medicine18 1006ndash1014 doihttpdxdoiorg101111j1525-1497200330103x
Craig D Mirakhur A Hart D J McIlroy S P andPassmore A P (2005) A cross-sectional study ofneuropsychiatric symptoms in 435 patients withAlzheimerrsquos disease American Journal of GeriatricPsychiatry 13 460ndash468 doi10109700019442-200506000-00004
Crellin N Charlesworth G and Orrell M (2014)Measuring family caregiver efficacy for managing behavioraland psychological symptoms in dementia a psychometricevaluation International Psychogeriatrics 26 93ndash103 doihttpdxdoiorg101017s1041610213001646
Davidsdottir S R Snaedal J Karlsdottir GAtladottir I and Hannesdottir K (2012) Validationof the Icelandic version of the neuropsychiatric inventorywith caregiver distress (NPI-D) Nordic Journal of
Psychiatry 66 26ndash32 doihttpdxdoiorg103109080394882011593100
Davis J D and Tremont G (2007) Impact of frontalsystems behavioral functioning in dementia on caregiverburden The Journal of Neuropsychiatry and ClinicalNeurosciences 19 43ndash49 doihttpdxdoiorg101176jnp200719143
de Vugt M E Riedijk S R Aalten P Tibben Avan Swieten J C and Verhey F R J (2006) Impactof behavioural problems on spousal caregivers acomparison between Alzheimerrsquos disease andfronto-temporal dementia Dementia and Geriatric CognitiveDisorders 22 35ndash41 doi101159000093102
de Vugt M E et al (2003) Behavioural disturbances indementia patients and quality of the marital relationshipInternational Journal of Geriatric Psychiatry 18 149ndash154doi101002gps807
Donaldson C Tarrier N and Burns A (1998)Determinants of carer stress in Alzheimerrsquos diseaseInternational Journal of Geriatric Psychiatry 13 248ndash256doi101002(sici)1099-1166(199804)134lt248aid-gps770gt30co2-0
Downs S and Black N (1998) The feasibility of creating achecklist for the assessment of the methodological qualityboth of randomised and non-randomised studies of healthcare interventions Journal of Epidemiological CommunityHealth 52 377ndash384 doi101136jech526377
Farran C J Loukissa D A Lindeman D A andMcCann J (2004) Caring for self while caring for othersthe two-track life of coping with Alzheimerrsquos diseaseJournal of Gerontological Nursing 30 38ndash45doi1039280098-9134-20040501-09
Fauth E B and Gibbons A (2014) Which behavioral andpsychological symptoms of dementia are the mostproblematic Variability by prevalence intensity distressratings and associations with carer depressive symptomsInternational Journal of Geriatric Psychiatry 29 263ndash271doi101002gps4002
Fuh J L Liu C K Mega M S Wang S J andCummings J L (2001) Behavioral disorders andcaregiversrsquo reaction in Taiwanese patients with Alzheimerrsquosdisease International Psychogeriatrics 13 121ndash128 doihttpdxdoiorg101017s1041610201007517
Gaugler J E et al (2011) Does caregiver burden mediatethe effects of behavioral disturbances on nursing homeadmission The American Journal of Geriatric Psychiatry 19497ndash506 doi101097jgp0b013e31820d92cc
Gilleard C J Belford H Gilleard E Whittick J Eand Gledhill K (1984) Emotional distress amongst thesupporters of the elderly mental infirm British Journal ofPsychiatry 145 172ndash177doihttpdxdoiorg101192bjp1452172
Gitlin L N and Rose K (2014) Factors associated withcarer readiness to use nonpharmacologic strategies tomanage dementia-related behavioral symptomsInternational Journal of Geriatric Psychiatry 29 93ndash102doihttpdxdoiorg101002gps3979
Goldberg D P and Hillier V F (1979) A scaled versionof the general health questionnaire Psychological Medicine9 139ndash145 doi101017s0033291700021644
Gonzalez-Salvador M T Arango C Lyketsos C Gand Barba A C (1999) The stress and psychological
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1773
morbidity of the Alzheimer patient caregiver InternationalJournal of Geriatric Psychiatry 14 701ndash710doi101002(sici)1099-1166(199909)149lt701aidps5gt30co2-
Haley W E Brown S and Levine E G (1987) Familycaregiver appraisals of patient behavioral disturbance insenile dementia Clinical Gerontologist The Journal of Agingand Mental Health 6 25ndash34doi101300j018v06n04_04
Haley W E Levine E G Brown S L Berry J Wand Hughes G H (2008) The psychological social andhealth consequences of caring for a relative with seniledementia Journal of the American Geriatrics Society 35405ndash411 doi101111j1532-54151987tb04661x
Hishikawa N et al (2012) Effects of turmeric onAlzheimerrsquos disease with behavioral and psychologicalsymptoms of dementia Ayu 33 499ndash504 doihttpdxdoiorg1041030974-8520110524
Huang S S Lee M C Liao Y C Wang W F andLai T J (2012) Caregiver burden associated withbehavioral and psychological symptoms of dementia(BPSD) in Taiwanese elderly Archives of Gerontology andGeriatrics 55 55ndash59 doihttpdxdoiorg101016jarchger201104009
Jackson M A Fauth E B and Geiser C (2014)Comparing the neuropsychiatric inventory and the revisedmemory and behavior problems checklist for associationswith caregiver burden and depressive symptomsInternational Psychogeriatrics 26 1021ndash1031doi101017s1041610213002421
Johnson D K Niedens M Wilson J RSwartzendruber L Yeager A and Jones K (2013)Treatment outcomes of a crisis intervention program fordementia with severe psychiatric complications the Kansasbridge project The Gerontologist 53 102ndash112 doihttpdxdoiorg101093gerontgns104
Khoo S A Chen T Y Ang Y H and Yap P (2013)The impact of neuropsychiatric symptoms on caregiverdistress and quality of life in persons with dementia in anAsian tertiary hospital memory clinic InternationalPsychogeriatrics 25 1991ndash1999 doihttpdxdoiorg101017s1041610213001518
Kosberg J I Kaufman A V Burgio L D Leeper Jand Sun F (2007) Family caregiving to those withdementia in rural Alabama racial similarities anddifferences Journal of Aging and Health 19 3ndash21 doi1011770898264306293604
Kosmala K and Kloszewska I (2004) The burden ofproviding care for Alzheimerrsquos disease patients in PolandInternational Journal of Geriatric Psychiatry 19 191ndash193doi101002gps1054
Landis J R and Koch G G (1977) The measurement ofobserver agreement for categorical data Biometrics 33159ndash174 doi 1023072529310
Lee D R McKeith I Mosimann U Ghosh-NodyalA and Thomas A J (2013) Examining carer stress indementia the role of subtype diagnosis andneuropsychiatric symptoms International Journal ofGeriatric Psychiatry 28 135ndash141 doihttpdxdoiorg101002gps3799
Lim Y M Son G R Song J A and Beattie E(2008) Factors affecting burden of family caregivers of
community-dwelling ambulatory elders with dementia inKorea Archives of Psychiatric Nursing 22 226ndash234 doi101016japnu200712005
Matsumoto N et al (2007) Caregiver burden associatedwith behavioral and psychological symptoms of dementia inelderly people in the local community Dementia andGeriatric Cognitive Disorders 23 219ndash224doi101159000099472
Mohamed S Rosenheck R Lyketsos C G andSchneider L S (2010) Caregiver burden in Alzheimerdisease cross-sectional and longitudinal patient correlatesThe American Journal of Geriatric Psychiatry 18 917ndash927doi101097jgp0b013e3181d5745d
Mourik J C Rosso S M Niermeijer M FDuivenvoorden H J Van Swieten J C and TibbenA (2004) Frontotemporal dementia behavioral symptomsand caregiver distress Dementia and Geriatric CognitiveDisorders 18 299ndash306 doihttpdxdoiorg101159000080123
Muangpaisan W et al (2010) Caregiver burden and needsof dementia caregivers in Thailand a cross-sectional studyJournal of the Medical Association of Thailand 93 601ndash607
Neundorfer M M McClendon M J Smyth K AStuckey J C Strauss M E and Patterson M B(2001) A longitudinal study of the relationship betweenlevels of depression among persons with Alzheimerrsquosdisease and levels of depression among their familycaregivers Journal of Gerontology Series B - PsychologicalSciences and Social Sciences 56 301ndash313
Nygaard H A (1998) Strain on caregivers of dementedelderly people living at home Scandinavian Journal ofPrimary Health Care 6 33ndash37doihttpdxdoiorg10310902813438809009287
Ornstein K and Gaugler J E (2012) The problem withldquoproblem behaviorsrdquoa systematic review of the associationbetween individual patient behavioral and psychologicalsymptoms and caregiver depression and burden within thedementia patientndashcaregiver dyad InternationalPsychogeriatrics 24 1536ndash1552doi101017s1041610212000737
Ornstein K Gaugler J E Devanand N S CarolynZ and Yaakov S (2012) The differential impact ofunique behavioral and psychological symptoms for thedementia caregiver how and why do patientsrsquo individualsymptom clusters impact caregiver depressive symptomsThe American Journal of Geriatric Psychiatry 12 77ndash1286doi httpdxdoiorg101016jjagp201301062
Price G R (1970) Selection and covariance Nature 227520ndash521 doi101038227520a0
Prince M (2000) Dementia in developing countries Aconsensus statement from the 1066 Dementia ResearchGroup International Journal of Geriatric Psychiatry 1514ndash20 doihttpdxdoiorg101002(sici)1099-1166(200001)151lt14aid-gps70gt30co2-8
Quayhagen M P and Quayhagen M (1998) Alzheimerrsquosstress coping with the caregiving role Gerontologist 28391ndash396 doihttpdxdoiorg101093geront283391
Reisberg B Ferris S H de Leon M J and Crook T(1982) The global deterioration scale for assessment ofprimary degenerative dementia American Journal ofPsychiatry 139 1136ndash1139 doihttpdxdoiorg101176ajp13991136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1774 A Feast et al
Robinson K M Adkisson P and Weinrich S (2001)Problem behaviour caregiver reactions and impact amongcaregivers of persons with Alzheimerrsquos disease Journal ofAdvanced Nursing 36 573ndash582 doihttpdxdoiorg101046j1365-2648200102010x
Rocca P et al (2010) Neuropsychiatric symptomsunderlying caregiver stress and insight in Alzheimerrsquosdisease Dementia and Geriatric Cognitive Disorders 3057ndash63 doi101159000315513
Rymer S Salloway S Norton L Mallow PCorreia S and Monast D (2002) Impaired awarenessbehavior disturbance and caregiver burden in Alzheimerdisease Alzheimer Disease and Associated Disorders 16248ndash253 doi 10109700002093-200210000-00006
Savorani G Vulcano V Boni S Sarti G andRavaglia G (1998) Behavioral disorders in dementiapatients and their impact on the stress of caregivingrelatives the ldquoARADrdquo questionnaire Archives ofGerontology and Geriatrics 6 481ndash485doi101016s0167-4943(98)80070-8
Shaji K S George R K Prince M J and JacobK S (2009) Behavioral symptoms and caregiver burdenin dementia Indian Journal of Psychiatry 51 45 doihttpdxdoiorg1041030019-554544905
Sink K M Covinsky K E Barnes D E NewcomerR J and Yaffe K (2006) Caregiver characteristics areassociated with neuropsychiatric symptoms of dementiaJournal of the American Geriatrics Society 54 796ndash803 doi101111j1532-5415200600697x
Slachevsky A et al (2013) The CUIDEME studydeterminants of burden in chilean primary caregivers ofpatients with dementia Journal of Alzheimerrsquos Disease 35297ndash306
Spiegel R et al (1991) A new behavioral assessment scalefor geriatric out- and in-patients the NOSGER (nursesrsquoobservation scale for geriatric patients) Journal of theAmerican Geriatric Society 39 339ndash347 doihttpdxdoiorg101111j1532-54151991tb02897x
Tan L L Wong H B and Allen H (2005) The impactof neuropsychiatric symptoms of dementia on distress infamily and professional caregivers in SingaporeInternational Psychogeriatrics 17 253ndash263 doi101017s1041610205001523
Teri L (1997) Behavior and caregiver burden behavioralproblems in patients with Alzheimer disease and itsassociation with caregiver distress Alzheimer Disease andAssociated Disorders 11 35ndash38
Teri L Truax P Logsdon R Uomoto J Zarit Sand Vitaliano P P (1992) Assessment of behavioralproblems in dementia the revised memory and behaviorproblems checklist Psychology and Aging 7 622 doi1010370882-797474622
Waite A Bebbington P Skelton-Robinson M andOrrell M (2004) Social factors and depression in carersof people with dementia International Journal of GeriatricPsychiatry 19 582ndash587 doihttpdxdoiorg101002gps1136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at

Individual BPSD and caregiver well-being 1771
but advances have been made with respect towhich behaviors are associated with distress Theinconsistencies may be partly explained by caregivervariables which were not taken into account inthe review Based on this review and previousresearch it is not possible to fully understand therelationship between BPSD and caregiver well-being without examining the influence of caregivervariables such as caregiver strategies acceptancegender relationship with person with dementiaand confidence We recommend that future studiesare designed to examine individual BPSD ratherthan BPSD as a whole use consistent measures forBPSD and well-being use consistent terminologyfor psychological constructs (eg burden) andexamine the causal mechanisms by which individualBPSD impact caregiver well-being by collectingdata on a range of caregiver factors Theseapproaches will clarify whether it is important forclinicians to focus on the frequency or prevalence ofcertain BPSD in addition to targeting the presenceof certain caregiver characteristics and addressingunmet need
Conflict of interest
None
Description of authorsrsquo roles
A Feast was responsible for developing the reviewobjectives writing the search strategies conductingthe searches designing and completing studyeligibility and data extraction forms undertakingthe quality appraisals conducting the meta-analysisand writing the paper M Orrell was responsible fordeveloping the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper C Stoner was responsible forundertaking the quality appraisals and assisting inwriting the paper G Charlesworth was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper E Moniz-Cook was responsiblefor developing the review objectives advising on thereview methodology meta-analysis and assisting inwriting the paper
Acknowledgments
We would like to thank Dr Zoeuml Hoare for herstatistical advice This paper presents independentresearch funded by the National Institute for HealthResearch (NIHR) under its Programme Grants forApplied Research (RP-PG-0606-1067 and RP-PG-
060- 1083) The views expressed in this publicationare those of the author(s) and not necessarily thoseof the NHS the NIHR or the Department ofHealth
Supplementary Material
To view supplementary material for thisarticle please visit httpdxdoiorg101017S1041610216000922
References
Aarsland D et al (2007) Neuropsychiatric symptoms inpatients with Parkinsonrsquos disease and dementia frequencyprofile and associated care giver stress Journal of NeurologyNeurosurgery amp Psychiatry 78 36ndash42doihttpdxdoiorg101136jnnp2005083113
Allegri R F et al (2006) Neuropsychiatric symptoms as apredictor of caregiver burden in Alzheimerrsquos diseaseNeuropsychiatric Disease amp Treatment 2 105ndash110doi102147ndts47133
Almberg B Grafstrom M and Winblad B (1997)Major strain and coping strategies as reported by familymembers who care for aged demented relatives Journal ofAdvanced Nursing 26 683ndash691doihttpdxdoiorg101046j1365-2648199700392x
Arango-Lasprilla J C Lehan T Drew A MorenoA Deng X and Lemos M (2010) Health-relatedquality of life in caregivers of individuals with dementiafrom Colombia American Journal of Alzheimerrsquos Disease andOther Dementias 25 556ndash561doi1011771533317510382287ltbibgt
Baiyewu O et al (2003) Behavioral and caregiver reactionof dementia as measured by the neuropsychiatric inventoryin Nigerian community residents InternationalPsychogeriatrics 15 399ndash409doi101017s1041610203009645
Baiyewu O et al (2012) Behavioral symptoms incommunity-dwelling elderly Nigerians with dementia mildcognitive impairment and normal cognition InternationalJournal of Geriatric Psychiatry 27 931ndash939 doihttpdxdoiorg101002gps2804
Balieiro A P Jr Sobreira E S T Pena M C SSilva-Filho J H and Vale F A C (2010) Caregiverdistress associated with behavioral and psychologicalsymptoms in mild Alzheimerrsquos disease Dementia eNeuropsychologia 4 238ndash244
Ballard C G et al (1995) The aetiology of depression inthe carers of dementia sufferers Journal of AffectiveDisorders 35 59ndash63 doi1010160165-0327(95)00041-k
Bandeira D R Pawlowski J Goncalves T RHilgert J B Bozzetti M C and Hugo F N (2007)Psychological distress in Brazilian caregivers of relativeswith dementia Aging and Mental Health 11 14ndash19doi10108013607860600640814
Berger G Bernhardt T Weimer E Peters JKratzsch T and Frolich L (2005) Longitudinal studyon the relationship between symptomatology of dementia
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1772 A Feast et al
and levels of subjective burden and depression amongfamily caregivers in memory clinic patients Journal ofGeriatric Psychiatry and Neurology 3 119ndash128doi1011770891988704273375
Black W and Almeida O P (2004) A systematic reviewof the association between the behavioral and psychologicalsymptoms of dementia and burden of care InternationalPsychogeriatrics 16 295ndash315doi101017s1041610204000468
Bruce D G and Paterson A (2000) Barriers tocommunity support for the dementia carer a qualitativestudy International Journal of Geriatric Psychiatry 15451ndash457 doi101002(sici)1099-1166(200005)155lt451aid-gps143gt30co2-k
Campbell P et al (2008) Determinants of burden in thosewho care for someone with dementia International Journalof Geriatric Psychiatry 23 1078ndash1085doi101002gps2071
Cerejeira J Lagarto L and Mukaetova-LadinskaE B (2012) Behavioral and psychological symptoms ofdementia Frontiers in Neurology 3 1ndash23doi103389fneur201200073
Chappell N L and Penning M (1996) Behaviouralproblems and distress among caregivers of people withdementia Ageing amp Society 16 57ndash73doi101017s0144686x00003135
Chiu Y C et al (2014) Family caregiversrsquo sleepdisturbance and its associations with multilevel stressorswhen caring for patients with dementia Aging amp MentalHealth 18 92ndash101 doihttpdxdoiorg101080136078632013837141
Cohen J (1988) Statistical Power Analysis for the BehavioralSciences 2nd edn New York University New YorkLawrence Erlbaum Associatesdoi1043249780203771587
Conde-Sala J L Garre-Olmo J Turroacute-Garriga OVilalta-Franch J and Loacutepez-Pousa S (2010)Differential features of burden between spouse andadult-child caregivers of patients with Alzheimerrsquos diseasean exploratory comparative design International Journal ofNursing Studies 47 1262ndash1273doi101016jijnurstu201003001
Covinsky K E et al (2003) Patient and caregivercharacteristics associated with depression in caregivers ofpatients with dementia Journal of General Internal Medicine18 1006ndash1014 doihttpdxdoiorg101111j1525-1497200330103x
Craig D Mirakhur A Hart D J McIlroy S P andPassmore A P (2005) A cross-sectional study ofneuropsychiatric symptoms in 435 patients withAlzheimerrsquos disease American Journal of GeriatricPsychiatry 13 460ndash468 doi10109700019442-200506000-00004
Crellin N Charlesworth G and Orrell M (2014)Measuring family caregiver efficacy for managing behavioraland psychological symptoms in dementia a psychometricevaluation International Psychogeriatrics 26 93ndash103 doihttpdxdoiorg101017s1041610213001646
Davidsdottir S R Snaedal J Karlsdottir GAtladottir I and Hannesdottir K (2012) Validationof the Icelandic version of the neuropsychiatric inventorywith caregiver distress (NPI-D) Nordic Journal of
Psychiatry 66 26ndash32 doihttpdxdoiorg103109080394882011593100
Davis J D and Tremont G (2007) Impact of frontalsystems behavioral functioning in dementia on caregiverburden The Journal of Neuropsychiatry and ClinicalNeurosciences 19 43ndash49 doihttpdxdoiorg101176jnp200719143
de Vugt M E Riedijk S R Aalten P Tibben Avan Swieten J C and Verhey F R J (2006) Impactof behavioural problems on spousal caregivers acomparison between Alzheimerrsquos disease andfronto-temporal dementia Dementia and Geriatric CognitiveDisorders 22 35ndash41 doi101159000093102
de Vugt M E et al (2003) Behavioural disturbances indementia patients and quality of the marital relationshipInternational Journal of Geriatric Psychiatry 18 149ndash154doi101002gps807
Donaldson C Tarrier N and Burns A (1998)Determinants of carer stress in Alzheimerrsquos diseaseInternational Journal of Geriatric Psychiatry 13 248ndash256doi101002(sici)1099-1166(199804)134lt248aid-gps770gt30co2-0
Downs S and Black N (1998) The feasibility of creating achecklist for the assessment of the methodological qualityboth of randomised and non-randomised studies of healthcare interventions Journal of Epidemiological CommunityHealth 52 377ndash384 doi101136jech526377
Farran C J Loukissa D A Lindeman D A andMcCann J (2004) Caring for self while caring for othersthe two-track life of coping with Alzheimerrsquos diseaseJournal of Gerontological Nursing 30 38ndash45doi1039280098-9134-20040501-09
Fauth E B and Gibbons A (2014) Which behavioral andpsychological symptoms of dementia are the mostproblematic Variability by prevalence intensity distressratings and associations with carer depressive symptomsInternational Journal of Geriatric Psychiatry 29 263ndash271doi101002gps4002
Fuh J L Liu C K Mega M S Wang S J andCummings J L (2001) Behavioral disorders andcaregiversrsquo reaction in Taiwanese patients with Alzheimerrsquosdisease International Psychogeriatrics 13 121ndash128 doihttpdxdoiorg101017s1041610201007517
Gaugler J E et al (2011) Does caregiver burden mediatethe effects of behavioral disturbances on nursing homeadmission The American Journal of Geriatric Psychiatry 19497ndash506 doi101097jgp0b013e31820d92cc
Gilleard C J Belford H Gilleard E Whittick J Eand Gledhill K (1984) Emotional distress amongst thesupporters of the elderly mental infirm British Journal ofPsychiatry 145 172ndash177doihttpdxdoiorg101192bjp1452172
Gitlin L N and Rose K (2014) Factors associated withcarer readiness to use nonpharmacologic strategies tomanage dementia-related behavioral symptomsInternational Journal of Geriatric Psychiatry 29 93ndash102doihttpdxdoiorg101002gps3979
Goldberg D P and Hillier V F (1979) A scaled versionof the general health questionnaire Psychological Medicine9 139ndash145 doi101017s0033291700021644
Gonzalez-Salvador M T Arango C Lyketsos C Gand Barba A C (1999) The stress and psychological
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1773
morbidity of the Alzheimer patient caregiver InternationalJournal of Geriatric Psychiatry 14 701ndash710doi101002(sici)1099-1166(199909)149lt701aidps5gt30co2-
Haley W E Brown S and Levine E G (1987) Familycaregiver appraisals of patient behavioral disturbance insenile dementia Clinical Gerontologist The Journal of Agingand Mental Health 6 25ndash34doi101300j018v06n04_04
Haley W E Levine E G Brown S L Berry J Wand Hughes G H (2008) The psychological social andhealth consequences of caring for a relative with seniledementia Journal of the American Geriatrics Society 35405ndash411 doi101111j1532-54151987tb04661x
Hishikawa N et al (2012) Effects of turmeric onAlzheimerrsquos disease with behavioral and psychologicalsymptoms of dementia Ayu 33 499ndash504 doihttpdxdoiorg1041030974-8520110524
Huang S S Lee M C Liao Y C Wang W F andLai T J (2012) Caregiver burden associated withbehavioral and psychological symptoms of dementia(BPSD) in Taiwanese elderly Archives of Gerontology andGeriatrics 55 55ndash59 doihttpdxdoiorg101016jarchger201104009
Jackson M A Fauth E B and Geiser C (2014)Comparing the neuropsychiatric inventory and the revisedmemory and behavior problems checklist for associationswith caregiver burden and depressive symptomsInternational Psychogeriatrics 26 1021ndash1031doi101017s1041610213002421
Johnson D K Niedens M Wilson J RSwartzendruber L Yeager A and Jones K (2013)Treatment outcomes of a crisis intervention program fordementia with severe psychiatric complications the Kansasbridge project The Gerontologist 53 102ndash112 doihttpdxdoiorg101093gerontgns104
Khoo S A Chen T Y Ang Y H and Yap P (2013)The impact of neuropsychiatric symptoms on caregiverdistress and quality of life in persons with dementia in anAsian tertiary hospital memory clinic InternationalPsychogeriatrics 25 1991ndash1999 doihttpdxdoiorg101017s1041610213001518
Kosberg J I Kaufman A V Burgio L D Leeper Jand Sun F (2007) Family caregiving to those withdementia in rural Alabama racial similarities anddifferences Journal of Aging and Health 19 3ndash21 doi1011770898264306293604
Kosmala K and Kloszewska I (2004) The burden ofproviding care for Alzheimerrsquos disease patients in PolandInternational Journal of Geriatric Psychiatry 19 191ndash193doi101002gps1054
Landis J R and Koch G G (1977) The measurement ofobserver agreement for categorical data Biometrics 33159ndash174 doi 1023072529310
Lee D R McKeith I Mosimann U Ghosh-NodyalA and Thomas A J (2013) Examining carer stress indementia the role of subtype diagnosis andneuropsychiatric symptoms International Journal ofGeriatric Psychiatry 28 135ndash141 doihttpdxdoiorg101002gps3799
Lim Y M Son G R Song J A and Beattie E(2008) Factors affecting burden of family caregivers of
community-dwelling ambulatory elders with dementia inKorea Archives of Psychiatric Nursing 22 226ndash234 doi101016japnu200712005
Matsumoto N et al (2007) Caregiver burden associatedwith behavioral and psychological symptoms of dementia inelderly people in the local community Dementia andGeriatric Cognitive Disorders 23 219ndash224doi101159000099472
Mohamed S Rosenheck R Lyketsos C G andSchneider L S (2010) Caregiver burden in Alzheimerdisease cross-sectional and longitudinal patient correlatesThe American Journal of Geriatric Psychiatry 18 917ndash927doi101097jgp0b013e3181d5745d
Mourik J C Rosso S M Niermeijer M FDuivenvoorden H J Van Swieten J C and TibbenA (2004) Frontotemporal dementia behavioral symptomsand caregiver distress Dementia and Geriatric CognitiveDisorders 18 299ndash306 doihttpdxdoiorg101159000080123
Muangpaisan W et al (2010) Caregiver burden and needsof dementia caregivers in Thailand a cross-sectional studyJournal of the Medical Association of Thailand 93 601ndash607
Neundorfer M M McClendon M J Smyth K AStuckey J C Strauss M E and Patterson M B(2001) A longitudinal study of the relationship betweenlevels of depression among persons with Alzheimerrsquosdisease and levels of depression among their familycaregivers Journal of Gerontology Series B - PsychologicalSciences and Social Sciences 56 301ndash313
Nygaard H A (1998) Strain on caregivers of dementedelderly people living at home Scandinavian Journal ofPrimary Health Care 6 33ndash37doihttpdxdoiorg10310902813438809009287
Ornstein K and Gaugler J E (2012) The problem withldquoproblem behaviorsrdquoa systematic review of the associationbetween individual patient behavioral and psychologicalsymptoms and caregiver depression and burden within thedementia patientndashcaregiver dyad InternationalPsychogeriatrics 24 1536ndash1552doi101017s1041610212000737
Ornstein K Gaugler J E Devanand N S CarolynZ and Yaakov S (2012) The differential impact ofunique behavioral and psychological symptoms for thedementia caregiver how and why do patientsrsquo individualsymptom clusters impact caregiver depressive symptomsThe American Journal of Geriatric Psychiatry 12 77ndash1286doi httpdxdoiorg101016jjagp201301062
Price G R (1970) Selection and covariance Nature 227520ndash521 doi101038227520a0
Prince M (2000) Dementia in developing countries Aconsensus statement from the 1066 Dementia ResearchGroup International Journal of Geriatric Psychiatry 1514ndash20 doihttpdxdoiorg101002(sici)1099-1166(200001)151lt14aid-gps70gt30co2-8
Quayhagen M P and Quayhagen M (1998) Alzheimerrsquosstress coping with the caregiving role Gerontologist 28391ndash396 doihttpdxdoiorg101093geront283391
Reisberg B Ferris S H de Leon M J and Crook T(1982) The global deterioration scale for assessment ofprimary degenerative dementia American Journal ofPsychiatry 139 1136ndash1139 doihttpdxdoiorg101176ajp13991136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1774 A Feast et al
Robinson K M Adkisson P and Weinrich S (2001)Problem behaviour caregiver reactions and impact amongcaregivers of persons with Alzheimerrsquos disease Journal ofAdvanced Nursing 36 573ndash582 doihttpdxdoiorg101046j1365-2648200102010x
Rocca P et al (2010) Neuropsychiatric symptomsunderlying caregiver stress and insight in Alzheimerrsquosdisease Dementia and Geriatric Cognitive Disorders 3057ndash63 doi101159000315513
Rymer S Salloway S Norton L Mallow PCorreia S and Monast D (2002) Impaired awarenessbehavior disturbance and caregiver burden in Alzheimerdisease Alzheimer Disease and Associated Disorders 16248ndash253 doi 10109700002093-200210000-00006
Savorani G Vulcano V Boni S Sarti G andRavaglia G (1998) Behavioral disorders in dementiapatients and their impact on the stress of caregivingrelatives the ldquoARADrdquo questionnaire Archives ofGerontology and Geriatrics 6 481ndash485doi101016s0167-4943(98)80070-8
Shaji K S George R K Prince M J and JacobK S (2009) Behavioral symptoms and caregiver burdenin dementia Indian Journal of Psychiatry 51 45 doihttpdxdoiorg1041030019-554544905
Sink K M Covinsky K E Barnes D E NewcomerR J and Yaffe K (2006) Caregiver characteristics areassociated with neuropsychiatric symptoms of dementiaJournal of the American Geriatrics Society 54 796ndash803 doi101111j1532-5415200600697x
Slachevsky A et al (2013) The CUIDEME studydeterminants of burden in chilean primary caregivers ofpatients with dementia Journal of Alzheimerrsquos Disease 35297ndash306
Spiegel R et al (1991) A new behavioral assessment scalefor geriatric out- and in-patients the NOSGER (nursesrsquoobservation scale for geriatric patients) Journal of theAmerican Geriatric Society 39 339ndash347 doihttpdxdoiorg101111j1532-54151991tb02897x
Tan L L Wong H B and Allen H (2005) The impactof neuropsychiatric symptoms of dementia on distress infamily and professional caregivers in SingaporeInternational Psychogeriatrics 17 253ndash263 doi101017s1041610205001523
Teri L (1997) Behavior and caregiver burden behavioralproblems in patients with Alzheimer disease and itsassociation with caregiver distress Alzheimer Disease andAssociated Disorders 11 35ndash38
Teri L Truax P Logsdon R Uomoto J Zarit Sand Vitaliano P P (1992) Assessment of behavioralproblems in dementia the revised memory and behaviorproblems checklist Psychology and Aging 7 622 doi1010370882-797474622
Waite A Bebbington P Skelton-Robinson M andOrrell M (2004) Social factors and depression in carersof people with dementia International Journal of GeriatricPsychiatry 19 582ndash587 doihttpdxdoiorg101002gps1136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at

1772 A Feast et al
and levels of subjective burden and depression amongfamily caregivers in memory clinic patients Journal ofGeriatric Psychiatry and Neurology 3 119ndash128doi1011770891988704273375
Black W and Almeida O P (2004) A systematic reviewof the association between the behavioral and psychologicalsymptoms of dementia and burden of care InternationalPsychogeriatrics 16 295ndash315doi101017s1041610204000468
Bruce D G and Paterson A (2000) Barriers tocommunity support for the dementia carer a qualitativestudy International Journal of Geriatric Psychiatry 15451ndash457 doi101002(sici)1099-1166(200005)155lt451aid-gps143gt30co2-k
Campbell P et al (2008) Determinants of burden in thosewho care for someone with dementia International Journalof Geriatric Psychiatry 23 1078ndash1085doi101002gps2071
Cerejeira J Lagarto L and Mukaetova-LadinskaE B (2012) Behavioral and psychological symptoms ofdementia Frontiers in Neurology 3 1ndash23doi103389fneur201200073
Chappell N L and Penning M (1996) Behaviouralproblems and distress among caregivers of people withdementia Ageing amp Society 16 57ndash73doi101017s0144686x00003135
Chiu Y C et al (2014) Family caregiversrsquo sleepdisturbance and its associations with multilevel stressorswhen caring for patients with dementia Aging amp MentalHealth 18 92ndash101 doihttpdxdoiorg101080136078632013837141
Cohen J (1988) Statistical Power Analysis for the BehavioralSciences 2nd edn New York University New YorkLawrence Erlbaum Associatesdoi1043249780203771587
Conde-Sala J L Garre-Olmo J Turroacute-Garriga OVilalta-Franch J and Loacutepez-Pousa S (2010)Differential features of burden between spouse andadult-child caregivers of patients with Alzheimerrsquos diseasean exploratory comparative design International Journal ofNursing Studies 47 1262ndash1273doi101016jijnurstu201003001
Covinsky K E et al (2003) Patient and caregivercharacteristics associated with depression in caregivers ofpatients with dementia Journal of General Internal Medicine18 1006ndash1014 doihttpdxdoiorg101111j1525-1497200330103x
Craig D Mirakhur A Hart D J McIlroy S P andPassmore A P (2005) A cross-sectional study ofneuropsychiatric symptoms in 435 patients withAlzheimerrsquos disease American Journal of GeriatricPsychiatry 13 460ndash468 doi10109700019442-200506000-00004
Crellin N Charlesworth G and Orrell M (2014)Measuring family caregiver efficacy for managing behavioraland psychological symptoms in dementia a psychometricevaluation International Psychogeriatrics 26 93ndash103 doihttpdxdoiorg101017s1041610213001646
Davidsdottir S R Snaedal J Karlsdottir GAtladottir I and Hannesdottir K (2012) Validationof the Icelandic version of the neuropsychiatric inventorywith caregiver distress (NPI-D) Nordic Journal of
Psychiatry 66 26ndash32 doihttpdxdoiorg103109080394882011593100
Davis J D and Tremont G (2007) Impact of frontalsystems behavioral functioning in dementia on caregiverburden The Journal of Neuropsychiatry and ClinicalNeurosciences 19 43ndash49 doihttpdxdoiorg101176jnp200719143
de Vugt M E Riedijk S R Aalten P Tibben Avan Swieten J C and Verhey F R J (2006) Impactof behavioural problems on spousal caregivers acomparison between Alzheimerrsquos disease andfronto-temporal dementia Dementia and Geriatric CognitiveDisorders 22 35ndash41 doi101159000093102
de Vugt M E et al (2003) Behavioural disturbances indementia patients and quality of the marital relationshipInternational Journal of Geriatric Psychiatry 18 149ndash154doi101002gps807
Donaldson C Tarrier N and Burns A (1998)Determinants of carer stress in Alzheimerrsquos diseaseInternational Journal of Geriatric Psychiatry 13 248ndash256doi101002(sici)1099-1166(199804)134lt248aid-gps770gt30co2-0
Downs S and Black N (1998) The feasibility of creating achecklist for the assessment of the methodological qualityboth of randomised and non-randomised studies of healthcare interventions Journal of Epidemiological CommunityHealth 52 377ndash384 doi101136jech526377
Farran C J Loukissa D A Lindeman D A andMcCann J (2004) Caring for self while caring for othersthe two-track life of coping with Alzheimerrsquos diseaseJournal of Gerontological Nursing 30 38ndash45doi1039280098-9134-20040501-09
Fauth E B and Gibbons A (2014) Which behavioral andpsychological symptoms of dementia are the mostproblematic Variability by prevalence intensity distressratings and associations with carer depressive symptomsInternational Journal of Geriatric Psychiatry 29 263ndash271doi101002gps4002
Fuh J L Liu C K Mega M S Wang S J andCummings J L (2001) Behavioral disorders andcaregiversrsquo reaction in Taiwanese patients with Alzheimerrsquosdisease International Psychogeriatrics 13 121ndash128 doihttpdxdoiorg101017s1041610201007517
Gaugler J E et al (2011) Does caregiver burden mediatethe effects of behavioral disturbances on nursing homeadmission The American Journal of Geriatric Psychiatry 19497ndash506 doi101097jgp0b013e31820d92cc
Gilleard C J Belford H Gilleard E Whittick J Eand Gledhill K (1984) Emotional distress amongst thesupporters of the elderly mental infirm British Journal ofPsychiatry 145 172ndash177doihttpdxdoiorg101192bjp1452172
Gitlin L N and Rose K (2014) Factors associated withcarer readiness to use nonpharmacologic strategies tomanage dementia-related behavioral symptomsInternational Journal of Geriatric Psychiatry 29 93ndash102doihttpdxdoiorg101002gps3979
Goldberg D P and Hillier V F (1979) A scaled versionof the general health questionnaire Psychological Medicine9 139ndash145 doi101017s0033291700021644
Gonzalez-Salvador M T Arango C Lyketsos C Gand Barba A C (1999) The stress and psychological
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
Individual BPSD and caregiver well-being 1773
morbidity of the Alzheimer patient caregiver InternationalJournal of Geriatric Psychiatry 14 701ndash710doi101002(sici)1099-1166(199909)149lt701aidps5gt30co2-
Haley W E Brown S and Levine E G (1987) Familycaregiver appraisals of patient behavioral disturbance insenile dementia Clinical Gerontologist The Journal of Agingand Mental Health 6 25ndash34doi101300j018v06n04_04
Haley W E Levine E G Brown S L Berry J Wand Hughes G H (2008) The psychological social andhealth consequences of caring for a relative with seniledementia Journal of the American Geriatrics Society 35405ndash411 doi101111j1532-54151987tb04661x
Hishikawa N et al (2012) Effects of turmeric onAlzheimerrsquos disease with behavioral and psychologicalsymptoms of dementia Ayu 33 499ndash504 doihttpdxdoiorg1041030974-8520110524
Huang S S Lee M C Liao Y C Wang W F andLai T J (2012) Caregiver burden associated withbehavioral and psychological symptoms of dementia(BPSD) in Taiwanese elderly Archives of Gerontology andGeriatrics 55 55ndash59 doihttpdxdoiorg101016jarchger201104009
Jackson M A Fauth E B and Geiser C (2014)Comparing the neuropsychiatric inventory and the revisedmemory and behavior problems checklist for associationswith caregiver burden and depressive symptomsInternational Psychogeriatrics 26 1021ndash1031doi101017s1041610213002421
Johnson D K Niedens M Wilson J RSwartzendruber L Yeager A and Jones K (2013)Treatment outcomes of a crisis intervention program fordementia with severe psychiatric complications the Kansasbridge project The Gerontologist 53 102ndash112 doihttpdxdoiorg101093gerontgns104
Khoo S A Chen T Y Ang Y H and Yap P (2013)The impact of neuropsychiatric symptoms on caregiverdistress and quality of life in persons with dementia in anAsian tertiary hospital memory clinic InternationalPsychogeriatrics 25 1991ndash1999 doihttpdxdoiorg101017s1041610213001518
Kosberg J I Kaufman A V Burgio L D Leeper Jand Sun F (2007) Family caregiving to those withdementia in rural Alabama racial similarities anddifferences Journal of Aging and Health 19 3ndash21 doi1011770898264306293604
Kosmala K and Kloszewska I (2004) The burden ofproviding care for Alzheimerrsquos disease patients in PolandInternational Journal of Geriatric Psychiatry 19 191ndash193doi101002gps1054
Landis J R and Koch G G (1977) The measurement ofobserver agreement for categorical data Biometrics 33159ndash174 doi 1023072529310
Lee D R McKeith I Mosimann U Ghosh-NodyalA and Thomas A J (2013) Examining carer stress indementia the role of subtype diagnosis andneuropsychiatric symptoms International Journal ofGeriatric Psychiatry 28 135ndash141 doihttpdxdoiorg101002gps3799
Lim Y M Son G R Song J A and Beattie E(2008) Factors affecting burden of family caregivers of
community-dwelling ambulatory elders with dementia inKorea Archives of Psychiatric Nursing 22 226ndash234 doi101016japnu200712005
Matsumoto N et al (2007) Caregiver burden associatedwith behavioral and psychological symptoms of dementia inelderly people in the local community Dementia andGeriatric Cognitive Disorders 23 219ndash224doi101159000099472
Mohamed S Rosenheck R Lyketsos C G andSchneider L S (2010) Caregiver burden in Alzheimerdisease cross-sectional and longitudinal patient correlatesThe American Journal of Geriatric Psychiatry 18 917ndash927doi101097jgp0b013e3181d5745d
Mourik J C Rosso S M Niermeijer M FDuivenvoorden H J Van Swieten J C and TibbenA (2004) Frontotemporal dementia behavioral symptomsand caregiver distress Dementia and Geriatric CognitiveDisorders 18 299ndash306 doihttpdxdoiorg101159000080123
Muangpaisan W et al (2010) Caregiver burden and needsof dementia caregivers in Thailand a cross-sectional studyJournal of the Medical Association of Thailand 93 601ndash607
Neundorfer M M McClendon M J Smyth K AStuckey J C Strauss M E and Patterson M B(2001) A longitudinal study of the relationship betweenlevels of depression among persons with Alzheimerrsquosdisease and levels of depression among their familycaregivers Journal of Gerontology Series B - PsychologicalSciences and Social Sciences 56 301ndash313
Nygaard H A (1998) Strain on caregivers of dementedelderly people living at home Scandinavian Journal ofPrimary Health Care 6 33ndash37doihttpdxdoiorg10310902813438809009287
Ornstein K and Gaugler J E (2012) The problem withldquoproblem behaviorsrdquoa systematic review of the associationbetween individual patient behavioral and psychologicalsymptoms and caregiver depression and burden within thedementia patientndashcaregiver dyad InternationalPsychogeriatrics 24 1536ndash1552doi101017s1041610212000737
Ornstein K Gaugler J E Devanand N S CarolynZ and Yaakov S (2012) The differential impact ofunique behavioral and psychological symptoms for thedementia caregiver how and why do patientsrsquo individualsymptom clusters impact caregiver depressive symptomsThe American Journal of Geriatric Psychiatry 12 77ndash1286doi httpdxdoiorg101016jjagp201301062
Price G R (1970) Selection and covariance Nature 227520ndash521 doi101038227520a0
Prince M (2000) Dementia in developing countries Aconsensus statement from the 1066 Dementia ResearchGroup International Journal of Geriatric Psychiatry 1514ndash20 doihttpdxdoiorg101002(sici)1099-1166(200001)151lt14aid-gps70gt30co2-8
Quayhagen M P and Quayhagen M (1998) Alzheimerrsquosstress coping with the caregiving role Gerontologist 28391ndash396 doihttpdxdoiorg101093geront283391
Reisberg B Ferris S H de Leon M J and Crook T(1982) The global deterioration scale for assessment ofprimary degenerative dementia American Journal ofPsychiatry 139 1136ndash1139 doihttpdxdoiorg101176ajp13991136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1774 A Feast et al
Robinson K M Adkisson P and Weinrich S (2001)Problem behaviour caregiver reactions and impact amongcaregivers of persons with Alzheimerrsquos disease Journal ofAdvanced Nursing 36 573ndash582 doihttpdxdoiorg101046j1365-2648200102010x
Rocca P et al (2010) Neuropsychiatric symptomsunderlying caregiver stress and insight in Alzheimerrsquosdisease Dementia and Geriatric Cognitive Disorders 3057ndash63 doi101159000315513
Rymer S Salloway S Norton L Mallow PCorreia S and Monast D (2002) Impaired awarenessbehavior disturbance and caregiver burden in Alzheimerdisease Alzheimer Disease and Associated Disorders 16248ndash253 doi 10109700002093-200210000-00006
Savorani G Vulcano V Boni S Sarti G andRavaglia G (1998) Behavioral disorders in dementiapatients and their impact on the stress of caregivingrelatives the ldquoARADrdquo questionnaire Archives ofGerontology and Geriatrics 6 481ndash485doi101016s0167-4943(98)80070-8
Shaji K S George R K Prince M J and JacobK S (2009) Behavioral symptoms and caregiver burdenin dementia Indian Journal of Psychiatry 51 45 doihttpdxdoiorg1041030019-554544905
Sink K M Covinsky K E Barnes D E NewcomerR J and Yaffe K (2006) Caregiver characteristics areassociated with neuropsychiatric symptoms of dementiaJournal of the American Geriatrics Society 54 796ndash803 doi101111j1532-5415200600697x
Slachevsky A et al (2013) The CUIDEME studydeterminants of burden in chilean primary caregivers ofpatients with dementia Journal of Alzheimerrsquos Disease 35297ndash306
Spiegel R et al (1991) A new behavioral assessment scalefor geriatric out- and in-patients the NOSGER (nursesrsquoobservation scale for geriatric patients) Journal of theAmerican Geriatric Society 39 339ndash347 doihttpdxdoiorg101111j1532-54151991tb02897x
Tan L L Wong H B and Allen H (2005) The impactof neuropsychiatric symptoms of dementia on distress infamily and professional caregivers in SingaporeInternational Psychogeriatrics 17 253ndash263 doi101017s1041610205001523
Teri L (1997) Behavior and caregiver burden behavioralproblems in patients with Alzheimer disease and itsassociation with caregiver distress Alzheimer Disease andAssociated Disorders 11 35ndash38
Teri L Truax P Logsdon R Uomoto J Zarit Sand Vitaliano P P (1992) Assessment of behavioralproblems in dementia the revised memory and behaviorproblems checklist Psychology and Aging 7 622 doi1010370882-797474622
Waite A Bebbington P Skelton-Robinson M andOrrell M (2004) Social factors and depression in carersof people with dementia International Journal of GeriatricPsychiatry 19 582ndash587 doihttpdxdoiorg101002gps1136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at

Individual BPSD and caregiver well-being 1773
morbidity of the Alzheimer patient caregiver InternationalJournal of Geriatric Psychiatry 14 701ndash710doi101002(sici)1099-1166(199909)149lt701aidps5gt30co2-
Haley W E Brown S and Levine E G (1987) Familycaregiver appraisals of patient behavioral disturbance insenile dementia Clinical Gerontologist The Journal of Agingand Mental Health 6 25ndash34doi101300j018v06n04_04
Haley W E Levine E G Brown S L Berry J Wand Hughes G H (2008) The psychological social andhealth consequences of caring for a relative with seniledementia Journal of the American Geriatrics Society 35405ndash411 doi101111j1532-54151987tb04661x
Hishikawa N et al (2012) Effects of turmeric onAlzheimerrsquos disease with behavioral and psychologicalsymptoms of dementia Ayu 33 499ndash504 doihttpdxdoiorg1041030974-8520110524
Huang S S Lee M C Liao Y C Wang W F andLai T J (2012) Caregiver burden associated withbehavioral and psychological symptoms of dementia(BPSD) in Taiwanese elderly Archives of Gerontology andGeriatrics 55 55ndash59 doihttpdxdoiorg101016jarchger201104009
Jackson M A Fauth E B and Geiser C (2014)Comparing the neuropsychiatric inventory and the revisedmemory and behavior problems checklist for associationswith caregiver burden and depressive symptomsInternational Psychogeriatrics 26 1021ndash1031doi101017s1041610213002421
Johnson D K Niedens M Wilson J RSwartzendruber L Yeager A and Jones K (2013)Treatment outcomes of a crisis intervention program fordementia with severe psychiatric complications the Kansasbridge project The Gerontologist 53 102ndash112 doihttpdxdoiorg101093gerontgns104
Khoo S A Chen T Y Ang Y H and Yap P (2013)The impact of neuropsychiatric symptoms on caregiverdistress and quality of life in persons with dementia in anAsian tertiary hospital memory clinic InternationalPsychogeriatrics 25 1991ndash1999 doihttpdxdoiorg101017s1041610213001518
Kosberg J I Kaufman A V Burgio L D Leeper Jand Sun F (2007) Family caregiving to those withdementia in rural Alabama racial similarities anddifferences Journal of Aging and Health 19 3ndash21 doi1011770898264306293604
Kosmala K and Kloszewska I (2004) The burden ofproviding care for Alzheimerrsquos disease patients in PolandInternational Journal of Geriatric Psychiatry 19 191ndash193doi101002gps1054
Landis J R and Koch G G (1977) The measurement ofobserver agreement for categorical data Biometrics 33159ndash174 doi 1023072529310
Lee D R McKeith I Mosimann U Ghosh-NodyalA and Thomas A J (2013) Examining carer stress indementia the role of subtype diagnosis andneuropsychiatric symptoms International Journal ofGeriatric Psychiatry 28 135ndash141 doihttpdxdoiorg101002gps3799
Lim Y M Son G R Song J A and Beattie E(2008) Factors affecting burden of family caregivers of
community-dwelling ambulatory elders with dementia inKorea Archives of Psychiatric Nursing 22 226ndash234 doi101016japnu200712005
Matsumoto N et al (2007) Caregiver burden associatedwith behavioral and psychological symptoms of dementia inelderly people in the local community Dementia andGeriatric Cognitive Disorders 23 219ndash224doi101159000099472
Mohamed S Rosenheck R Lyketsos C G andSchneider L S (2010) Caregiver burden in Alzheimerdisease cross-sectional and longitudinal patient correlatesThe American Journal of Geriatric Psychiatry 18 917ndash927doi101097jgp0b013e3181d5745d
Mourik J C Rosso S M Niermeijer M FDuivenvoorden H J Van Swieten J C and TibbenA (2004) Frontotemporal dementia behavioral symptomsand caregiver distress Dementia and Geriatric CognitiveDisorders 18 299ndash306 doihttpdxdoiorg101159000080123
Muangpaisan W et al (2010) Caregiver burden and needsof dementia caregivers in Thailand a cross-sectional studyJournal of the Medical Association of Thailand 93 601ndash607
Neundorfer M M McClendon M J Smyth K AStuckey J C Strauss M E and Patterson M B(2001) A longitudinal study of the relationship betweenlevels of depression among persons with Alzheimerrsquosdisease and levels of depression among their familycaregivers Journal of Gerontology Series B - PsychologicalSciences and Social Sciences 56 301ndash313
Nygaard H A (1998) Strain on caregivers of dementedelderly people living at home Scandinavian Journal ofPrimary Health Care 6 33ndash37doihttpdxdoiorg10310902813438809009287
Ornstein K and Gaugler J E (2012) The problem withldquoproblem behaviorsrdquoa systematic review of the associationbetween individual patient behavioral and psychologicalsymptoms and caregiver depression and burden within thedementia patientndashcaregiver dyad InternationalPsychogeriatrics 24 1536ndash1552doi101017s1041610212000737
Ornstein K Gaugler J E Devanand N S CarolynZ and Yaakov S (2012) The differential impact ofunique behavioral and psychological symptoms for thedementia caregiver how and why do patientsrsquo individualsymptom clusters impact caregiver depressive symptomsThe American Journal of Geriatric Psychiatry 12 77ndash1286doi httpdxdoiorg101016jjagp201301062
Price G R (1970) Selection and covariance Nature 227520ndash521 doi101038227520a0
Prince M (2000) Dementia in developing countries Aconsensus statement from the 1066 Dementia ResearchGroup International Journal of Geriatric Psychiatry 1514ndash20 doihttpdxdoiorg101002(sici)1099-1166(200001)151lt14aid-gps70gt30co2-8
Quayhagen M P and Quayhagen M (1998) Alzheimerrsquosstress coping with the caregiving role Gerontologist 28391ndash396 doihttpdxdoiorg101093geront283391
Reisberg B Ferris S H de Leon M J and Crook T(1982) The global deterioration scale for assessment ofprimary degenerative dementia American Journal ofPsychiatry 139 1136ndash1139 doihttpdxdoiorg101176ajp13991136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at
1774 A Feast et al
Robinson K M Adkisson P and Weinrich S (2001)Problem behaviour caregiver reactions and impact amongcaregivers of persons with Alzheimerrsquos disease Journal ofAdvanced Nursing 36 573ndash582 doihttpdxdoiorg101046j1365-2648200102010x
Rocca P et al (2010) Neuropsychiatric symptomsunderlying caregiver stress and insight in Alzheimerrsquosdisease Dementia and Geriatric Cognitive Disorders 3057ndash63 doi101159000315513
Rymer S Salloway S Norton L Mallow PCorreia S and Monast D (2002) Impaired awarenessbehavior disturbance and caregiver burden in Alzheimerdisease Alzheimer Disease and Associated Disorders 16248ndash253 doi 10109700002093-200210000-00006
Savorani G Vulcano V Boni S Sarti G andRavaglia G (1998) Behavioral disorders in dementiapatients and their impact on the stress of caregivingrelatives the ldquoARADrdquo questionnaire Archives ofGerontology and Geriatrics 6 481ndash485doi101016s0167-4943(98)80070-8
Shaji K S George R K Prince M J and JacobK S (2009) Behavioral symptoms and caregiver burdenin dementia Indian Journal of Psychiatry 51 45 doihttpdxdoiorg1041030019-554544905
Sink K M Covinsky K E Barnes D E NewcomerR J and Yaffe K (2006) Caregiver characteristics areassociated with neuropsychiatric symptoms of dementiaJournal of the American Geriatrics Society 54 796ndash803 doi101111j1532-5415200600697x
Slachevsky A et al (2013) The CUIDEME studydeterminants of burden in chilean primary caregivers ofpatients with dementia Journal of Alzheimerrsquos Disease 35297ndash306
Spiegel R et al (1991) A new behavioral assessment scalefor geriatric out- and in-patients the NOSGER (nursesrsquoobservation scale for geriatric patients) Journal of theAmerican Geriatric Society 39 339ndash347 doihttpdxdoiorg101111j1532-54151991tb02897x
Tan L L Wong H B and Allen H (2005) The impactof neuropsychiatric symptoms of dementia on distress infamily and professional caregivers in SingaporeInternational Psychogeriatrics 17 253ndash263 doi101017s1041610205001523
Teri L (1997) Behavior and caregiver burden behavioralproblems in patients with Alzheimer disease and itsassociation with caregiver distress Alzheimer Disease andAssociated Disorders 11 35ndash38
Teri L Truax P Logsdon R Uomoto J Zarit Sand Vitaliano P P (1992) Assessment of behavioralproblems in dementia the revised memory and behaviorproblems checklist Psychology and Aging 7 622 doi1010370882-797474622
Waite A Bebbington P Skelton-Robinson M andOrrell M (2004) Social factors and depression in carersof people with dementia International Journal of GeriatricPsychiatry 19 582ndash587 doihttpdxdoiorg101002gps1136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at

1774 A Feast et al
Robinson K M Adkisson P and Weinrich S (2001)Problem behaviour caregiver reactions and impact amongcaregivers of persons with Alzheimerrsquos disease Journal ofAdvanced Nursing 36 573ndash582 doihttpdxdoiorg101046j1365-2648200102010x
Rocca P et al (2010) Neuropsychiatric symptomsunderlying caregiver stress and insight in Alzheimerrsquosdisease Dementia and Geriatric Cognitive Disorders 3057ndash63 doi101159000315513
Rymer S Salloway S Norton L Mallow PCorreia S and Monast D (2002) Impaired awarenessbehavior disturbance and caregiver burden in Alzheimerdisease Alzheimer Disease and Associated Disorders 16248ndash253 doi 10109700002093-200210000-00006
Savorani G Vulcano V Boni S Sarti G andRavaglia G (1998) Behavioral disorders in dementiapatients and their impact on the stress of caregivingrelatives the ldquoARADrdquo questionnaire Archives ofGerontology and Geriatrics 6 481ndash485doi101016s0167-4943(98)80070-8
Shaji K S George R K Prince M J and JacobK S (2009) Behavioral symptoms and caregiver burdenin dementia Indian Journal of Psychiatry 51 45 doihttpdxdoiorg1041030019-554544905
Sink K M Covinsky K E Barnes D E NewcomerR J and Yaffe K (2006) Caregiver characteristics areassociated with neuropsychiatric symptoms of dementiaJournal of the American Geriatrics Society 54 796ndash803 doi101111j1532-5415200600697x
Slachevsky A et al (2013) The CUIDEME studydeterminants of burden in chilean primary caregivers ofpatients with dementia Journal of Alzheimerrsquos Disease 35297ndash306
Spiegel R et al (1991) A new behavioral assessment scalefor geriatric out- and in-patients the NOSGER (nursesrsquoobservation scale for geriatric patients) Journal of theAmerican Geriatric Society 39 339ndash347 doihttpdxdoiorg101111j1532-54151991tb02897x
Tan L L Wong H B and Allen H (2005) The impactof neuropsychiatric symptoms of dementia on distress infamily and professional caregivers in SingaporeInternational Psychogeriatrics 17 253ndash263 doi101017s1041610205001523
Teri L (1997) Behavior and caregiver burden behavioralproblems in patients with Alzheimer disease and itsassociation with caregiver distress Alzheimer Disease andAssociated Disorders 11 35ndash38
Teri L Truax P Logsdon R Uomoto J Zarit Sand Vitaliano P P (1992) Assessment of behavioralproblems in dementia the revised memory and behaviorproblems checklist Psychology and Aging 7 622 doi1010370882-797474622
Waite A Bebbington P Skelton-Robinson M andOrrell M (2004) Social factors and depression in carersof people with dementia International Journal of GeriatricPsychiatry 19 582ndash587 doihttpdxdoiorg101002gps1136
httpswwwcambridgeorgcoreterms httpsdoiorg101017S1041610216000922Downloaded from httpswwwcambridgeorgcore IP address 5439106173 on 01 Sep 2020 at 113558 subject to the Cambridge Core terms of use available at