Embed Size (px)
Citation preview

ASTR SCIENTIFIC PAPERS
TO BE PRESENTED
1_
THE TREATMENT OF CRANIOPHARYNGIOMAS
Allen S. Lichter, M.D., William M. Wara, M.D., Glenn E. Sheline, M.D.Charles Wilson, M.D. and Jeannette Towsend, M.D.
Division of Radiation Oncology, University of California-San Francisco
The optimal treatment for craniopharyngiomas is widely disputed.Many authors recommend total surgical removal when possible. while othersadvocate decompression followed by radiation therapy. We have reviewed34 cases of craniopharyngioma seen at the University of California. SanFrancisco (UCSF) from 1956 to 1973. 18 patients were treated with surgeryplus radiotherapy and 16 with surgery alone. The results of both treatmentregimens will be compared and contrasted. Minimum follow-up time is 3years with 14 patients followed from 5 - 9 years and 8 patients followedfollowed for 10 years or more. Results of treatment and therapeuticrecommendation are discussed. It appears that radiation therapy prolongsdisease-free interval and may lead to permanent control.
2_
THE RELATIONSHIP OF TIME-DOSE FACTORS TO COMPLICATIONS IN THETREATMENT OF PITUITARY TUMORS BY IRRADIATION
Silvio Aristizabal, M.D., Division of Radiation Oncology,University of Arizona, College of Medicine
William L. Caldwell, M.D., Dept. of Human Oncology,University of Wisconsin Hospitals
The records of Radiotherapy Division of the Radiology Department ofVanderbilt University Hospital were reviewed for the years 1952-1971.During that period of time 122 patients with diagnosis of Pituitary Adenomas - 51 chromophobe, 46 basophilic, 25 eosinophilic - were treatedprimarily by external irradiation. A variety of techniqgBs (2 or 3stationar¥ fields, lBaP rotational fields) equipment (Co , 6 MeV Linac)and fractlonation schedules treating 'four, five or six days per week,doses ranging between 150 and 250 rads per fraction, were used.
Five patients developed severe complications - brain necrosis 1,blindness related to optic nerve atrophy or vascular damage 4. Fromanalysis of time-dose factors and conversion of the various treatmentregimens to equivalent NSD or TDF methods, it is evident that the riskof complications increases as the dose exceeds as NSD of 1500 rets orTDF of 76 (e.g. 4600 rads in 23 fract10ns over 30 days), as exemplifiedin Table I. Of 87 patients who received less than 1500 rets - TDF 76,none developed complications. Of 20 cases who received between 15001599 rets - TDF 77-86, 2 (10%) presented complications and 3 out of 15patients (20%) receiving more than 1600 rets - TDF 87, had radiation induced complications.
24
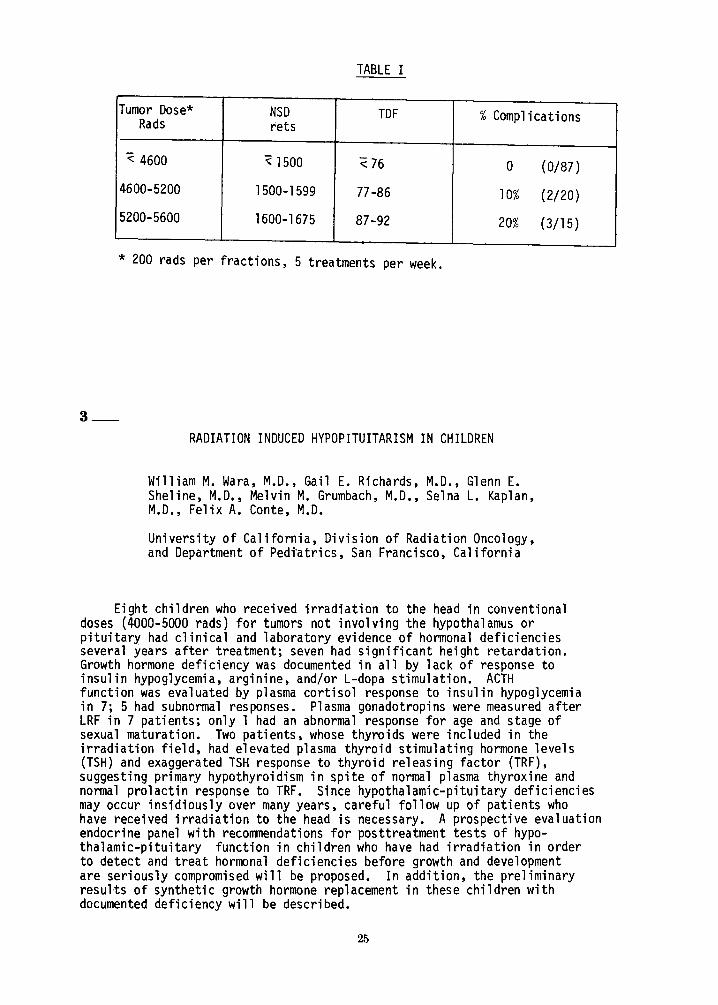
TABLE I
Tumor Dose* NSD TDF %ComplicationsRads rets
"< 4600 ~ 1500 "< 76 0 (0/87)
4600-5200 1500-1599 77-86 10% (2/20)
5200-5600 1600-1675 87-92 20% (3/15)
* 200 rads per fractions, 5 treatments per week.
3_
RADIATION INDUCED HYPOPITUITARISM IN CHILDREN
William M. Wara, M.D., Gail E. Richards, M.D., Glenn E.Sheline, M.D., Melvin M. Grumbach, M.D., Selna L. Kaplan,M.D., Felix A. Conte, M.D.
University of California, Division of Radiation Oncology,and Department of Pedi"atrics, San Francisco, California
Eight children who received irradiation to the head in conventionaldoses (4000-5000 rads) for tumors not involving the hypothalamus orpituitary had clinical and laboratory evidence of hormonal deficienciesseveral years after treatment; seven had significant height retardation.Growth hormone deficiency was documented in all by lack of response toinsulin hypoglycemia, arginine, and/or L-dopa stimulation. ACTHfunction was evaluated by plasma cortisol response to insulin hypoglycemiain 7; 5 had subnormal responses. Plasma gonadotropins were measured afterLRF in 7 patients; only 1 had an abnormal response for age and stage ofsexual maturation. Two patients, whose thyroids were included in theirradiation field, had elevated plasma thyroid stimulating hormone levels(TSH) and exaggerated TSH response to thyroid releasing factor (TRF),suggesting primary hypothyroidism in spite of normal plasma thyroxine andnormal prolactin response to TRF. Since hypothalamic-pituitary deficienciesmay occur insidiously over many years, careful follow up of patients whohave received irradiation to the head is necessary. A prospective evaluationendocrine panel with recommendations for posttreatment tests of hypothalamic-pituitary function in children who have had irradiation in orderto detect and treat hormonal deficiencies before growth and developmentare seriously compromised will be proposed. In addition, the preliminaryresults of synthetic growth hormone replacement in these children withdocumented deficiency will be described.
25
4_MEDULLOBLASTOMA : IMPROVED TREATMENT RESULTS
BY MODIFIED RADIOTHERAPY REGIMEN
Tae H. Kim, M.D., Yashoda T.R • Rao, M.D., James Ausman, M.D.,Seymour H. Levitt, M.D.
Department of Therapeutic Radiology and Neurosurgery,University of Minnesota Hospitals, Minneapolis, Minnesota
Forty-nine patients with medulloblastoma who were treated at Universityof Minnesota Hospitals between 1943 and 1975 were evaluated. Three out often patients (30%) who were irradiated to only a proportion of the CNS areliving, whereas twenty out of thirty-three patients (60%) who wereirradiated to the entire CNS are living.
Our previous review revealed that there were six proven intracranialrecurrences. All recurrences were anterior to posterior fossa.
Five of these six patients had received 3500 rads to the whole brainand spine with boosting dose of 1000 rads to 1500 rads to posterior fossa.Remaining one patient had received 4000 rads to whole brain only.
Based on this review a modification of treatment technique was madein 1971. Eleven patients including two adults have been treated with5000 rads to the whole brain and 3500 rads to the spine since then.
Of nine pediatric patients treated, eight patients are alive at rangeof 60 months and 12 months. The median survival time is 30 months. One ofthese patients had recurrence of disease at 38 months. One remainingpatient expired at 15 months because of recurrent disease in the cranium.The patient had not received adequate irradiation because of poor conditionat time of diagnosis.
Two adult patients are doing well at 41 months and 16 months.
Although numbers are small and follow up time is short, this resultseems to indicate that irradiating whole brain with 5000 rads and spine with3500 rads has improved treatment results of medulloblastoma.
This research was supported by Research Grants CA 15548 and CA 16545 from theNational Cancer Institute.
26
5_
MEDULLOBLASTOMA: A REVIEW OF THE L.D.S. HOSPITAL EXPERIENCEWITH IRRADIATION THERAPY
Richard C. Brown, M.D., Leonard L. Gunderson, M.D.,M.S.and Henry P. Plenk, M.D.,M.S.
Radiation Oncology Division, Arizona Medical Center
A review of 14 patients with an initial diagnosis of medulloblastomatreated with irradiation therapy is presented. Follow-up data is availableon all patients. When one evaluates those patients who were treated withtotal CNS irradiation, an excellent five-year survival of approximately70% is observed. The point of significance is that the dose to the spinalaxis was in the range of 2500 rads for the majority of the survivors witha boost to the posterior fossa between 4500 and 5000 rads. Only one patienthad metastatic disease, and that was a patient who had a ventricular atrialshunt placed initially for control of increased intracranial pressure. Thissurvival data adds to already published data from Hope-Stone and othersreporting excellent five-year survival with total CNS irradiation and iscontradictory to the reports of approximately 40% five year survival. Theimplications of the following review is that one can question the necessityof taking all patients with medulloblastoma to 3500 rads to the spinal column.We would suggest that included in the routine work-up would be Milliporeevaluation of the CSF, and if negative, use a low dose to the spinal columnof approximately 2500 rads. Thus, decrease the potential for spinal columnarrest in this young group of patients.
6_
CEREBELLAR ASTROCYTOMAS: PREDICTORS OF RECURRENCE
James E. Marks, M.D., A.B. Kliefoth, M.D., and James S. Nelson, M.D.
Washington University School of MedicineSt. Louis, MO
Aretrospective review of 97 cases of cerebellar astrocytoma was undertakento determine predictors of recurrence in an effort to define indicationsfor adjuvant radiation. In the group of 97 cases, 17 or 18% recurred a meaninterval of 36 months following craniotomy. A total of 20 cases or 21% werereferred for radiation; 10 of the irradiated cases later recurred and 10 did not.The decision to refer for adjuvant radiation was likely based on subtotal removal andgrade of tumor since 18 of 20 irradiated cases or 90% were subtotally removedand 46% had grade greater than one. Of the predictors studied, age, grade oftumor and subtotal removal of tumor, only subtotal removal significantlycorrelated with recurrence. Subtotal removal of tumor should, therefore, bethe prime indication for adjuvant radiation. The clinician should be awarethat radiation does not always prevent recurrence and that many cases do notrecur after long periods of observation despite subtotal removal. In thisseries q cases or 48% were subtotally removed and only 16 or 34% of these laterrecurred.
27
7_GLIOBLASTOMA MULTIFORME: DETERMINANTS OF
TIME-DOSE-VOLUME FACTORS
Omar M. Salazar, M.D., Philip Rubin, M.D.Division of Radiation Oncology, Universityof Rochester Cancer Center, 601 ElmwoodAvenue, Rochester, New York.
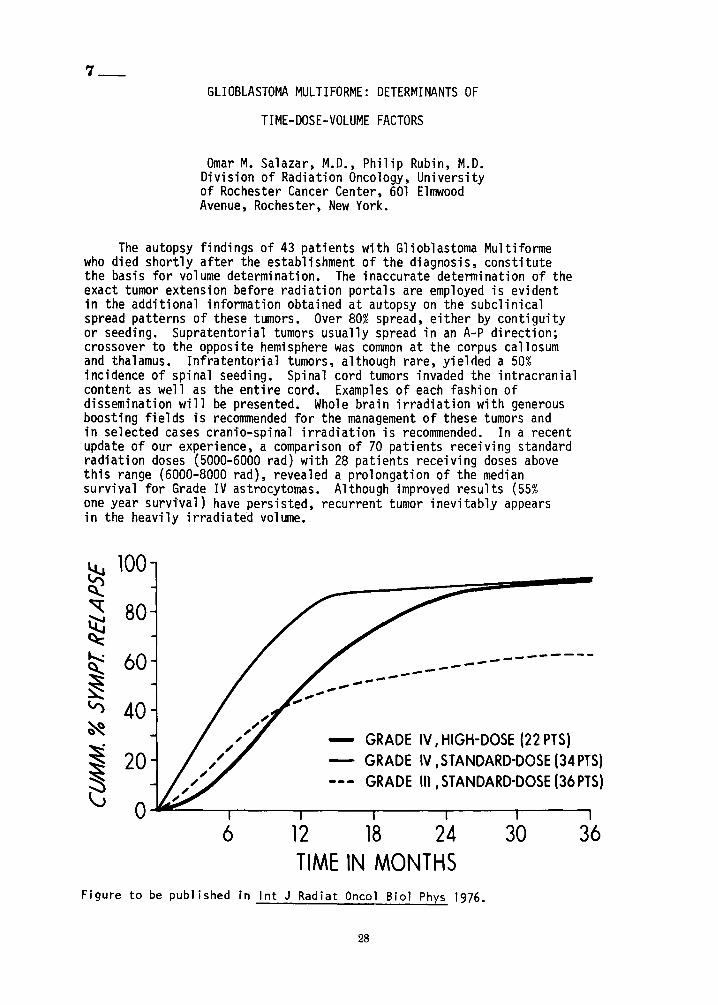
The autopsy findings of 43 patients with Glioblastoma Multiformewho died shortly after the establishment of the diagnosis, constitutethe basis for volume determination. The inaccurate determination of theexact tumor extension before radiation portals are employed is evidentin the additional information obtained at autopsy on the subclinicalspread patterns of these tumors. Over 80% spread, either by contiguityor seeding. Supratentorial tumors usually spread in an A-P direction;crossover to the opposite hemisphere was common at the corpus callosumand thalamus. Infratentorial tumors, although rare, yielded a 50%incidence of spinal seeding. Spinal cord tumors invaded the intracranialcontent as well as the entire cord. Examples of each fashion ofdissemination will be presented. Whole brain irradiation with generousboosting fields is recommended for the management of these tumors andin selected cases cranio-spinal irradiation is recommended. In a recentupdate of our experience, a comparison of 70 patients receiving standardradiation doses (5000-6000 rad) with 28 patients receiving doses abovethis range (6000-8000 rad), revealed a prolongation of the mediansurvival for Grade IV astrocytomas. Although improved results (55%one year survival) have persisted, recurrent tumor inevitably appearsin the heavily irradiated volume.
~100
~
~ 80~«<t......: 60~~V) 40~
~ 20s~ 0
-----------... ------------- GRADE IV, HIGH-DOSE (22 PTS)
GRADE IV,STANDARD-DOSE (34PTS)GRADE III ,STANDARD-DOSE (36PTS)
6 12 18 24TIME IN MONTHS
30 36
Figure to be published in Int J Radiat Oncol BioI Phys 1976.
28
8_
ANALYSIS OF LOCAL CONTROL IN THE TREATMENT OF EWING'S SARCOMABY RADIOTHERAPY AND MULTIAGENT SYSTEMIC CHEMOTHERAPY
Carlos A. Perez, M.D., Melvin Tefft, M.D., Ed Gehan, Ph.D.,Aly Razek, M.D., Mark Nesoit, M.D.
Division of Radiation Oncology, 4511 Forest Park, St. Louis,Missouri
The Intergroup Ewing 's Sarcoma study in ~rogress ~as accumulatedapproximately 200 patients in a four year per-iod, pat~:ents are treatedwith three, four drug combinations and high dose radiat10n thera~y to theentire bone (approximately 4500 rads tumor dose) ~omplemented w1th abooster dose of approximately 1500 rads to the pr1mary tumor volume.A recent preliminary analysis of treatment results in approximately 150patients show a local tumor control rate of over 90% i~ the major~ty ofanatomical locations seen, 75% in the humerus and 65% 10 the pelv1s.The factors affecting recurrences and other mechanisms of failure willbe analyzed in approximately 140 patients with complete records.
9_
EWING'S SARCOMA: PROPHYLACTIC WHOLE-LUNG IRRADIATION
Phillip C. Smith, M.D., Dempsey S. Springfield, M.D., and Rodney R. Mi l li on ,M.D.; Division of Radiation Therapy and Department of Orthopaedics,University of Florida College of Medicine, Gainesville, Florida 32610
Eighteen patients with non-metastatic Ewing's sarcoma have been treated forcure from 1966 to 1975 at the University of Florida. Prior to 1972, eightpatients received local irradiation and adjuvant chemotherapy. Of thisgroup, five have failed, four with metastatic pulmonary disease as a part oftheir first recurrence. Beginning in 1972, planned prophylactic whole lungirradiation given concomi tantly with irradiation of the primary site has beenused in all patients. Adjuvant chemotherapy has consisted of cyclophosphamide, vincristine, and actinomycin-D, and more recently Adriamycin, givenaccording to generally recommended protocols. Of the 10 patients with aminimum 12-month followup who have received prophylactic whole lung irradiation , there have been no patients with pulmonary metastases as the first siteof failure. There have been four failures and two deaths with skeletalmetastases. At the dose rate used (1500 rads in 15 fractions, uncorrectedfor lung transmission), there have been no acute or late pulmonary complications.
long-term functional results were evaluated in the 11 surviving patients.One patient treated in 1969 with a 2 Mev Van de Graaff generator has residualasymptomatic subcutaneous fibrosis. Two patients whose surgical biopsywounds were not completely healed at the start of irradiation experienceddelay in wound healing, but both eventually healed completely. A singlepatient with a proximal tibial lesion treated at the age of six yearsdeveloped a 4.4 em limb length discrepancy . One patient with a mandibularlesion has slight hypoplasia of the mandible and malocclusion. The remainingpatients maintain excellent function of irradiated sites.
29
In summary, prophylactic whole lung irradiation of 1500 rads in 15 treatmentshas markedly reduced the incidence of lung metastases from Ewing's sarcomaand is free of any complications. The incidence of skeletal metastases asthe site of failure has been unchanged in our series, despite more aggressivechemotherapy. Long-term functional results of primary sites irradiated from5500 to 6200 rads have been largely excellent.
10_
ADJUVANT CHEMOTHERAPY FOR HEAD AND NECK CANCER
Thomas C. Pomeroy, M.D.
Radiation Oncology BranchNational Cancer Institute
Bethesda, Maryland
To date, chemotherapy has had little effect on long-term survival inadvanced epidermoid cancer of the mouth and throat. However, a number ofdrugs have shown objective responses either singly or in combination.Combined with radiation therapy, there has been an increase in completeclearance rates of both the primary lesion and neck nodes as related insome recent reports. This is demonstrated in this pilot study as wellas with combined radiation and single drug (Bleomycin) or with multidrug (Bleomycin-Methotrexate) or (Bleomycin-Methotrexate-AdriamycinVincristine). Primary clearance rates have been 67% for Bleomycin-RTand 92% for multi-drug-RT in T3-T4 primary oral and pharyngeal cancers.Node clearance has been 50% and 64% respectively.
The possibility of significant increase in survival is indicatedby the current survival of 10/28 patients in this study for greater thantwo years with seven of them remaining free of disease. Of concern isthe poor tolerance of this class of patient to the chemotherapy and thesevere mucosal reactions from the simultaneous RT and chemotherapyleading to acute nutritional problems and dangerous episodes of aspirationpneumonia. However, emphasis is placed on the potential for greaterreduction of radiation dosage than realized early in the study. Completeclearance of massive primary or recurrent disease has been attained withdoses as low as 1600 rads in ten days ahd less than 4000 rads in fourcases with 2/4 with no evidence of disease more than three years aftertreatment.
This experience indicates the potential for application of thisapproach to earlier stages of disease combined with post-treatment surgeryto provide more careful evaluation of minimum radiation doses for optimumlocal cure with minimal sequelae.
30
11_
SPLIT-COURSE RADIOTHERAPY IN ADVANCED HEAD AND NECK TUMORS
M.V. Pilepich, M.D., F.G. Bloedorn, M.D., J.E. Munzenrider, M.D.,J.B. Rene, M.D., and W.S. Lowry, M.D.Department of Therapeutic Radiology'
Tufts-New England Medical CenterBoston, Massachusetts
A substantial number of patients with squamous cell carcinoma of the headand neck area present in a quite advanced stage of disease, often associatedwith a multitude of other medical problems. Conventional fractionationpatterns utilizing equal daily doses of radiation over a period of 6 to 8weeks usually produce significant morbidity due to acute reactions in agroup of patients in which the aim is primarily palliation. The main theoretical advantages of split-course irradiation include improved tolerance(reduction of acute reaction), shortened treatment time, and possibly bettertumor control.
Between 1969 and 1974, 95 patients with advanced head and neck tumors received split-course radiotherapy at the New England Medical Center Hospital.Based on radiobiological data, a specific fractionation pattern using alarge Iprimin9" dose of 800 rads was employed. The majority of patients(74 out of 95) received the following fractionation: On the first day800 rads was given, followed by 400 rads on the second day and 400 rads onthe third day. After a rest period of 2 to 3 weeks, a second course wasgiven, consisting of 2000 rads in 5 treatments. The third part of thesplit course, consisting of an additional 2000 rads in 5 treatments, wasgiven after a second rest period of 2 to 3 weeks. There were slight modifications of this scheme in 20 patients. Five patients received an implantfollowing external radiotherapy. Of 79 patients who completed radiotherapy,13% showed no evidence of disease at completion of treatment, 37% showedbetter than 50% regression of the tumor, 21% showed tumor regression of lessthan 50%, and 29% showed very little or no response. Acute reaction totreatment, usually occurring one week after each course and lasting forapproximately 4 to 6 days, was considered mild or moderate in the majorityof patients. In 11 patients the reaction was considered severe. In 4 instances severe laryngeal edema occurred 2 to 3 weeks after completion ofradiotherapy. Four patients, whose tumors were considered unresectableinitially, underwent radical surgery subsequent to a full course of radiotherapy because of residual tumor. In 3 of these patients, healing was complete, while the wound did not heal in one patient.
Four patients remain alive with no evidence of disease at 26 to 56 months.Two patients died of metastatic disease with local tumor control. Twopatients died of other causes with no evidence of tumor. Average survivalwas 7 months, with only 8% of patients surviving one year.
Meaningful palliation was achieved in the majority of patients with relatively little radiation-related morbidity. Occasional unexpected long-termcontrol was observed. Late normal tissue changes appear acceptable.
A statistically valid prospective trial comparing split-course and continuouscourse irradiation is needed.
Supported in part by Grant CA-12l78 of the National Cancer Institute,National Institutes of Health.
31
12_
A PERCUTANEOUS TRANSPTERYGOID IMPLANT FOR NASOPHARYNGEAL TUMORS
Vincent P. Collins, M.D .9200 Westheimer, Houston, Texas 77063
Tumors of the nasopharynx commonly show a degree of radiosensitivitythat encourages treatment with intent to cure. However, the locationpresents technical problems in avoiding high dose effects on bra in stem,pituitary gland, optic chiasma, parotid glands, and all the epithelialtissues of pharynx and much of oral cavity . The common problemof technicsof external therapy, particularly when there is reliance on opposing fields,is the unwanted radiation in intervening and surrounding normal tissues . Theuse of interstitial sources is one method for improving dose distribution.This paper describes the technic and dosimetry for permanent implantationof interstitial sources of Au 198, along with illustrative case histories.Thls method has been particularly useful in dealing with recurrence whentolerance has been jeopardized by prior treatment .
13_
t XTRA MEDULL ARY PLA SMAC YTOMA OF TH E UPPER RESP IRATORY PASS AG ES
ZB IGNI EW PETROVICH, M.D .BEN FIS HKIN , M.D.MAR IO ACQUAR ELLI , M.D.RICHARD BA RTON, M.D .
RAD IA T ION THE RAP Y SERVICEVA WADS WO RTH HOSPITAL CENTERLOS AN GELES, CALI FORNIA 90073
Th i s pape r is a r e v i e w of the c l in ica l exper ience wit h the P l a s macytoma of the Upper Respiratory Pa s s a ge s see n in the Departmen t ofRadiothe rapy at our institutio n from 1946 to 1976. Seven cases arediscussed .
A tumor ma s s was prese nt at d iagnos is i n a l I patients . 2/7 presentscer v i c a l l ymph a den o pa t hy . 1/7 had ce rvical ly mph a de no pa t hy 4 ye ar saf ter diagnos is, c o i ncidenta l with wid e sprea d meta st a s e s. Allpa ti e nt s were tre ated prima ri Iy wi th r a d i ati on fo l low i ng b iop s y a ndhisto log ic d iag nos is. Two pat ie nts ha d pa rt ia l exc isio ns , a nd twopati en t s r e ceiv e d c hemotherapy .
Fo llow-u p exte nds fro m 4 to 23 ye a r s . 6/7 were f ree o f disease a tl a s t eval ua t i on , and 1/7 died of d isseminated dis ease 9 yea rs a f t e ri nitial tr e atment .
32
14_
THE INCIDENCE OF NECK NODE METASTASES IN CARCINOMA OF THE MAXILLARY-ETHMOID SINUS
Edgardo M. Sayoc, M.D.; Ned B. Hornback, M.D.; Homayoon Shidn;a, M.D.;Raleigh E. Lingeman, M.D.; and Ronald Hamaker, M.D.Address: Department of Radiation Oncology and E.N.T.
Indiana University School of Medicine1100 West Michigan StreetIndianapolis, Indiana 46202
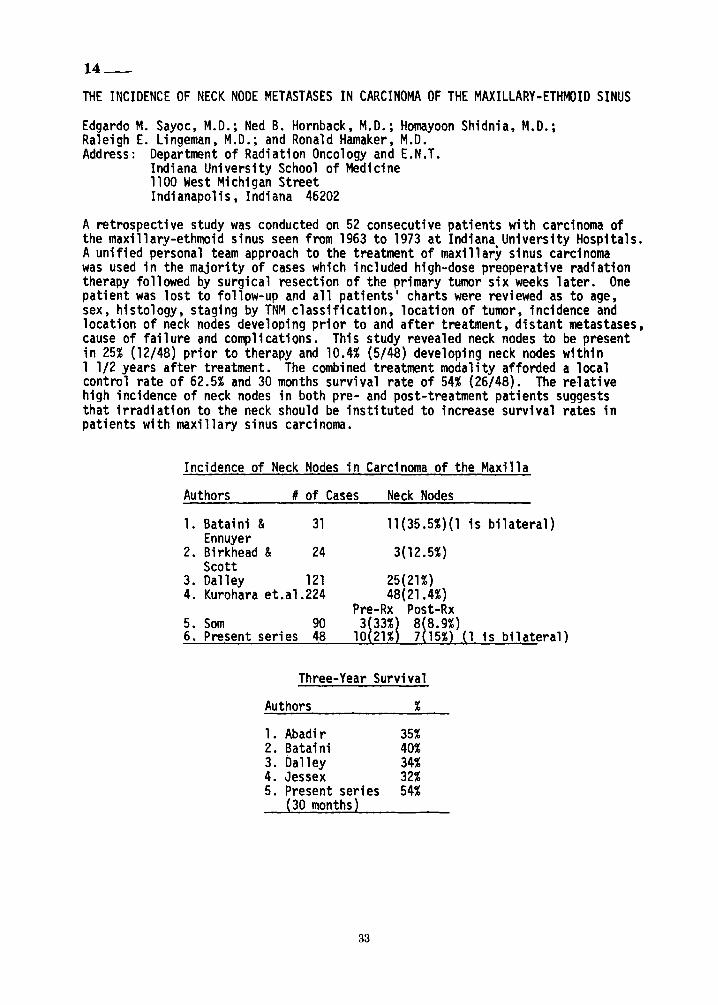
A retrospective study was conducted on 52 consecutive patients with carcinoma ofthe maxillary-ethmoid sinus seen from 1963 to 1973 at Indiana University Hospitals.Aunified personal team approach to the treatment of maxillary sinus carcinomawas used in the majority of cases which included high-dose preoperative radiationtherapy followed by surgical resection of the primary tumor six weeks later. Onepatient was lost to follow-up and all patients' charts were reviewed as to age,sex, histology, staging by TNM classification, location of tumor, incidence andlocation of neck nodes developing prior to and after treatment, distant metastases,cause of failure and complications. This study revealed neck nodes to be presentin 25% (12/48) prior to therapy and 10.4% (5/48) developing neck nodes within1 1/2 years after treatment. The combined treatment modality afforded a localcontrol rate of 62.5% and 30 months survival rate of 54% (26/48). The relativehigh incidence of neck nodes in both pre- and post-treatment patients suggeststhat irradiation to the neck should be instituted to increase survival rates inpatients with maxillary sinus carcinoma.
Incidence of Neck Nodes in Carcinoma of the Maxilla
Authors # of Cases Neck Nodes
1. Bataini & 31Ennuyer
2. Birkhead & 24Scott
3. Dalley 1214. Kurohara et.al.224
5. Som 906. Present series 48
is bilateral)
1 is bilateral)
Three-Year Survival
Authors %
1. Abadir 35%2. Bataini 40%3. Dalley 34%4. Jessex 32%5. Present series 54%
(30 months)
33
15_
MALIGNANT METASTATIC DISEASE OF THE EYES
Virendra S. Saxena. B.SC. M.D .• D.M.R.T .• F.R.C.R.• Salitha Reddy, M.D.,William Duetch, M.D. and Frank R. Hendrickson. M.D.
Department of Therapeutic Radiology, Rush-Presbyterian St. Luke's Hospital
Metastatic disease to the choroid of the eye is an infrequentoccurrance in practice of Oncology. In our department in the lastten years, we have seen 24 patients with this complication of malignancy.This paper will describe in detail the signs and symptoms when it occurs,and various characteristic appearances on fundoscopic examination beforeand after therapy. There will be discussion of its management with radiotherapy, its success, and failures and technique and dose schedules ofirradiation. The survival rates in these patients will also be discussed.It is not surprising that more than two third patients had carcinoma oftheir breast as primary disease. Other primary sets of malignancies arealso implicated though rarely including Ewing's Sarcoma. BronchogenicCarcinoma, etc. Quarter of these patients had involvement of both eyes.
16_
A CONTROLLED PROSPECTIVE STUDY OF THYROID HORMONAL CHANGESAND HYPOTHALAMIC/PITUITARY/THYROID AXIS CHANGES IN THE
FIRST THREE WEEKS OF A COURSE OF RADIATION THERAPY
M.J. Moriarty and P. SmythSaint Luke's Hospital, Rathgar, Dublin 6
and Department of Medicine, WoodviewUniversity College, Dublin, Ireland
The long term effects of external irradiation on normal thyroid functionare receiving increasing attention. The actual effects of external irradiationon normal thyroid function and on the associated Hypothalamic/Pituitary axisduring a course of external irradiation do not appear to have been thoroughlyinvestigated. This study records these effects in two groups of patientsover the first three weeks of a course of external radiotherapy.
The two groups consisted of: Group A.- This was composed of six patients withhead and neck primary tumors (4 larynx, 1 nasopharynx, 1 floor of mouth) inwhom the thyroid gland received a dose of 3000 Rover three weeks withexternal radiotherapy. Group B.- This was composed of five patients in whomthe thyroid gland received no irradiation (2 bladder tumors, 2 cervicalcancers and 1 seminoma of testis) but who did receive a minimum dose of3000 R in three weeks to the abdomen with external radiotherapy.
Investigations done included TRH stimulation test on day a and day 21of the treatment. In addition serum T4 and T3 and basal T.S.H. levels wereestimated post 1st and 2nd treatment and after 1/52 and after 2/52treatment.
34
Results: 1) Those patients who received irradiation to the thyroid glanddemonstrated significant suppression of TRH responsiveness. The group meanmaximal increment in TSH over basal levels produced by 200 UG of TRH (~ T.S.H.)fell from 5.5 ± 2.8 (S.D.) microunits per ml day 0 to 1.3 ~ 0.6 (S.D.) microunits per ml day 21. This difference is highly significant (P<O.Ol) and wasa consistent finding in all six patients. 2) In those patients who receivedno irradiation to the thyroid gland, TRH responsiveness was unchanged duringtreatment. The mean values for ~ TSH were 7.4 ± 4 (S.D.) microunits per mlon day 0 and 7.4 ± 3.8 (S.D.) microunits per ml on day 21. Values for basalTSH, serum T4 and serum T3 were not significantly altered in either groupfollowing irradiation.
Conclusion: These results indicate that thyroid function is not affectedby doses of external irradiation up to 3000 R, but pituitary responsivenessto the stimulatory effects of TRH (a hypothalamic hormone) is depressed.This suppression of pituitary function is possibly due to, as yet, unidentifiedsubstances being produced by the irradiated thyroid gland.
Acknowledgement: I wish to thank Saint Luke's Cancer Research Fund forsupporting this study.
17_
CANCER PATIENTS: KNOWLEDGE AND ATTITUDES
Glenn W. Mitchell, M.D., Rhode Island Hospital*; Arvin S. Glicksman, M.D., Dept.of Radiation Medicine, Brown University and Dept. of Radiation Oncology,Rhode Island Hospital, Providence, Rhode Island
* Now at Butler Hospital, Section of Psychiatry and Human Behavior, Brown UniversityProvidence, Rhode Island
Fifty adult patients were interviewed while undergoing radiation therapy atthe Department of Radiation Oncology of Rhode Island Hospital, Providence, Rhode Island.A loosely-directed interview technique was followed using an instrument of our owndesign. The average session required forty-five minutes to complete the requisitequestions.
The areas probed during the course of the interview included: (1) thepatient's expectations of and experience with his physicians, both referral andtherapist; (2) the patient's knowledge of his diagnosis, who first informed him,and his thoughts about the future; (3) the initial confrontation with and laterside-effects from the machines; (4) the patient's expectations of and experiencewith the technical and nursing staff; (5) the patient's attitude towards the other
35
patients with whom he has contact during therapy; (6) emotional and physical problemsand who handles them.
. It .was found that today'~ ~atient is more sophisticated in his knowledge ofdlag~osls.and treatment modalltles than previously reported. There is little knowledgeor dlrectlon, however, toward obtaining emotional support and guidance during thisstressful period.
18_
COMBINED INTRA-ARTERIAL ACTINOMYCIN-D AND RADIATION THERAPY FOR ADVANCED ANDUNRESECTABLE MALIGNANCIES: RESULTS OF TREATMENT OF 50 PATIENTS
Albert L. Wiley, M.D., Michael T. Kademian, M.D. and George W. Wirtanen, M.D.Division of Radiation Oncology, Department of Human Oncology, University ofWisconsin Center for Health Sciences, 1300 University Ave., Madison, WI. 53706
For the past 12 years we have utilized intra-arterial actinomycin-D topotentiate the effect of radiation in the treatment of 50 patients with advancedor unresectable malignancies. Approximately 90% of these tumors were soft tissueand bone sarcomas, but a few were malignant schwanoma, hypernephroma or malignantepithelial tumors.
With this combined therapy, 7/8 massive, initially unresectable tumors becameresectable. Also as either definitive therapy for unresectable sarcoma or as postsurgery therapy for residual gross sarcoma, a local control rate of better than60% has been obtained in those patients followed for longer than 2 years. Oftenwe have also found the regimen to be useful for palliation.
Over 90% of the patients were able to complete the planned course of therapy,with a low morbidity rate, probably because of our infusion technique, whichgenerally employs the transbrachial artery insertion of a small, flexible, polyethylene catheter for continuous infusion of actinomycin-D into selective tumorarteries.
The infusion catheter is also used for artergraphic tumor localization andfor the intra-arterial introduction of radiopharmaceuticals into the tumor. Suchstudies have occasionally assisted tumor boundary definition and the subsequentdesign of "boost" portals, in addition to providing a means of assessing tumorvascular response to therapy.
Partially supported by: NCl Grant #CAl45-20
36
19_
THE SIGNIFICANCE OF THE VERTEBRAL VENOUS (BATSON'S) PLEXUSIN METASTATIC SPREAD
Manuel Vider, M.D.Radiotherapy Department
Temple University HospitalPhiladelphia, PA
Yosh Maruyama, M.D.Department of Radiation Medicine
University of Kentucky Medical CenterLexington, KY
The Vertebral plexus of veins described by Batson in 1940 has beenpostulated to represent a pathway by which tumor spread can take place.The classical work of Batson was supported by the radiographic studiesof roengeno10gists and the anatomic studies of pathologists. This "thirdcirculation" bypasses the lungs and enters the systemic circulation througha valveless vertebral venous plexus system. Research studies by Comanand Delong (Cancer 4:610, 1951) showed a pattern of tumor spread in animalswhich was identical-to the roentgenographic pattern described by Batson .The advent of radioisotope bone~scanning offers a new tool to study andassess the pattern of spread of cancer through the vertebral venous plexus.Bone scan and radiographic studies will be described. We propose a dualmechanism of spread for colo-rectal carcinoma. There is a low pressureunobstructed drainage of large intra-abdominal veins to the liver andlungs. There is postulated to also be a higher pressure drainage throughBatson's plexus system mainly to the skeleton and brain. The conventionalview of colo-rectal carcinoma spread is assumed to be to the liver andlungs through the low pressure abdominal venous drainage system. We havefound and current reports suggest, a high incidence of skeletal and bonymetastases by isotopic bone scans (30-60%). This would suggest thatspread by the vertebral plexus system is much more important in colo-rectalcarcinoma than previously assumed.
20_
"TOTAL" THERAPY OF SMALL CELL LUNG CANCER
Ralph E. Johnson, M.D., C. Harry Kent, M.D. &Harmar D. Brereton, M.D.Radiation Oncology Branch, National Cancer Institute
Bethesda, Maryland
Single modality therapy for small cell cancer of the lung hasbeen disappointing and we have likewise abandoned the sequential useof radiotherapy and chemotherapy. In the past two years, 31 consecutive patients received simultaneous irradiation of bulk disease(primary and metastatic), prophylactic whole brain irradiation, andcombination chemotherapy in nearly bone marrow-ablating doses. Acomplete remission rate of 90%has been achieved with the 3-monthtreatment program to be described. Remissions of encouraging durationwithout maintenance therapy suggest curative treatment may become apotential for this almost uniformly fatal type of lung cancer.
37
21_
AN AGGRESSIVE APPROACH TO MARGINALLY RESECTABLE LilliG CANCER
David M. Sherman, M.D., Wilford Neptune, M.D., Stanley E. Order, M.D.,Anthony J. Piro, M.D., from the Joint Center for Radiation Therapy, NewEngland Deaconess Hospital, and Overholt Thoracic Clinic, and the Department of Radiation Therapy and Thoracic Surgery. Harvard Medical School,50 Binney Street, Boston, MA 02115.
Between July 1968 and December 1974, 53 patients with lung cancer wereplanned for preoperative irradiation and surgery. All patients were consideredclinically marginally resectable because of hilar, mediastinal and/or chest wallinvolvement. Most patients received 3000 to 4000 rad in 250 to 300 rad fractions4 times per week followed in two weeks by thoracotomy. Seven patients did nothave surgery because of the development of metastasis or medical contraindications.46 patients were explored and 38 were resectable. The median age was 61 years.12 patients are alive with a median follow up of 41 months; there were 2 intercurrent deaths. The cumulative 5 year survival of all resectable patients is 27%;and for 19 patients with epidermoid cancer, 31%. The common radiation toxicitywas mild esophagitits; and there was an 11% surgical morbidity and one mortalityin the resectable group. There were 3 treatment related deaths; one patient withfatal hemoptysis 2 days following radiation therapy and 2 patients died within onemonth of surgery. These data suggest that the survival of patients with marginally resectable lung cancer treated by accelerated radiotherapy followed by aggressive surgery approaches the survival experience of patients with primary resectablelung cancer and is superior to that of marginally resectable patients with radiationtherapy alone.
22_
CLINICAL REPORT ON THE TREATMENT OF LOCALLY ADVANCED LUNG CANCER
ZBIGNIEW PETROVICH, M.D.*WILLIAM MIETLOWSKI, Ph.D**MAIMU OHANIAN, M.D.**JAMES COX, M.D.**
VETERANS ADMINISTRATION LUNG CANCER STUDY GROUPTHE RADIATION THERAPY SERVICE, WADSWORTH HOSPITAL CENTERLOS ANGELES, CALIFORNIA 90073
*CHAIRMAN OF WRITING COMMITTEE**WRITING COMMITTEE
This paper discusses the results of the treatment of 345 patientsentered in the VALG Protocol 13L. The study was activated inMarch 1972, and closed for patient accession March 1975. Allpatients had a histologic diagnosis of primary lung cancer considered clinically non-resctable or inoperable.
38
Patien ts wer e e quall y r a ndomized into tw o g r o ups , ra diothera pyal one, or r a di oth era py with c he mo th e r a py .
The a na ly s is o f th e dat a in cluded : tr eatment r e gimen, radiationdo s e, initial pe rf o r manc e statu s, perf orman c e status chan ge, celltyp e, duration o f survi val, qualit y of survival, age and previoussur gery.
The s t ro nge s t influence o n median survival was the level of radiationdose. The pati e nt s t rea ted wi t h radi otherap y a nd chemoth erapys ho wed i mprovem ent in pe r fo r ma nce s t a t us mor e frequently than thepa t ie nts t rea t ed wi th ra d io t he r apy al on e. The l e ngt h of s ur v i va lf or both groups i s s i mi l a r .
Oth e r pa r ame te r s of t he an alysi s a re presen te d.
23_
WHOLE LUNG IRRADIATION IN THE PEDIATRIC AGE GROUP: LOW-DOSEVERSUS CONVENTIONAL FRACTIONATION WITH MULTI-DRUG CHEMOTHERAPY
Beryl McD. Chabora, M.D., Paul B. Lattin, D.O., M. Lois, Murphy,M.D., Departments of Radiotherapy and Pediatrics, MemorialHospital, New York, New York
Arnold Herskovic, M.D., Department of Radiotherapy, USC MedicalCenter, Los Angeles, California
Whole lung irradiation has been documented in the literature as aneffective control of pulmonary metastases in the pediatric age group. Priorto January 1975, daily fractions of 200 rad per day were used at MemorialHospital for this patient group. However, combined with the multi-drugchemotherapy protocols so often used in this group, such treatmentsresulted in a high percentage of severe complications.
Since January 1975, a radiation regimen of 100 rad per day, to atotal dose of 1400 rad, has been utilized in these cases, encompassingone or both lung fields as the cljnical situation dictated. Ten patientshave been so treated and followed for a minimum of one year. The localtumor control in this group, as well as the complication rate, has beencompared to thirteen similar cases treated prior to January 1975.Radiation factors, including time-dose relationships, and chemotherapyregimens, will be presented and discussed for both groups of patients.
39
24 ___
SPECIFIC EARLY FINE STRUCTURAL CHANGES
IN THE LUNG FOLLOWING IRRADIATION
David P. Penney. Ph.D •• Philip Rubin. M.D.University of Rochester Cancer Center, Strong Memorial Hospital,
Rochester. New York.
Irradiation of the lung has been shown to induce fibrosis,atelectasis, and edema. Since these histopathologic changes becomemanifested after considerable time has elapsed following irradiationinsult, we have attempted to determine the early responses of the alveolito irradiation. Toward this end. mouse thoraces were irradiated at asingle dosage of 1000. 2000, or 3000 R. At various post-irradiationtimes (1 hr, 1 day, 1 week, 14 weeks), the animals were sacrificed andtissue samples of the lungs were prepared for subsequent electronmicroscopic observation. Concomitant sham-control animals were processedsimultaneously. Noteworthy among early changes. detectable at alldosages by 24 hours. was a decrease in the numbers of surfactant-containing lamellated bodies in Type II alveolar cells. By 1 week, theobserved depletion of lamellated bodies was restored to approximate normalmorphology. By 14 weeks. many of the alveolar spaces contained considerableprecipitate, lipid-like material, and myelin figures, rendering athickened morphologic barrier across which functional exchange must occur.The possible association of these findings with potential atelecticdevelopment and hyaline membrane formation will be discussed. Biochemicalmeasurements of surfactant to correlate with morphologic findings arein progress.
25 ___
RADIATION DOSE RESPONSE IN LUNG
Homeira Moosavi, M.D., Philip Rubin, M.D •• Robert Cooper, Jr., M.D.,S~a~l:y McDonald, Ph.D., I. D?na~d Stuard, M.D., and David Penney, Ph.D .Dlvlslon of ~athology and Radlatlon Oncology, University of Rochester,Strong Memorlal Hospital, 601 Elmwood Avenue, Rochester, New York.
To ascertain the radiation dose response in the lungs of large animalsa systematic fine structural study of dog lungs was undertaken. Dogs '(~5 Kg) were.given 3600 rad of irrad;a~ion through the apex to one lung,wlth protectlon to the other lung. Anlmals were sacrificed at 2, 4, 6, 8.and 14 weeks. The dose distribution was reconstructed. Tissue samplesfrom subpleural and deep parenchymal sites of each dose region wereprepared for electron microscopic observation . Similar tissues from thenon-irradiated lung served as controls. The subpleural response includedseptal thickening, fibrosis, edema. and reduced alveolar lumina. The
deep parenchymal response involved perivascular hypertrophy and hyperplasiaof granular pneumocytes, increased numbers of lamellar bodies, increasedrelease of their contents, and perivascular fibrosis. No changes ofalveolar luminar size were noted. The most significant changes wereobserved in those zones exposed to greater than 3000 rad suggesting thepossibility of an identifiable dose response relationship. Early detectionof radiation pneumonitis by electron microscopy is feasible. Gradationsof injury correlating with both time and dose will be presented.
26_
''MICRCMITASTASES'' IN LEWIS LUNG CARCINmAA: 1Th10R SIZE VS CELLULAR SENSITMTITO IRRADIATION OR QfEMJIHERAPYJudith A. Stanley, B.Sc., William U. Shipley, M.D.*, G. Gordon Steel, Ph.D.,Divisions of Radiotherapy and Biophysics, Institute of Cancer Research and theRoyal Marsden Hospital, Sutton, Surrey, England, and the Department of RadiationMedicine, Massachusetts General Hospital, Boston, }~sachusetts
Tumor cell survival analysis following in situ 60coar- irradiation of pulmonaryand subcutaneous "micrometastases" of the Lewi'S'LtIDg Carcinoma showed that radiosensitivity decreased as microtumor size increased from 1 rom to 3.5 rom in diameter.For microtumors of 1 TIm, 2.2 TIm, and 3.5 TIm in diameter the fraction of tumor cellssurviving 1000 rads was 0.001, 0.01, and 0.25 respectively while the hypoxic fractionincreased from <0.005, to 0.01, to 0.04. Cellular sensitivity to BOlli and Cyclophosphamide also decreased with increasing microtumor size, e.g., following Bam(20 mg/kg) surviving fraction values ranged from 0.001 for 1-:TiiDn pulmonary microtumors to 0.50 for 10 TIm s.c. tumors.
Treatment of 2.2 nm pulmonary microtumors (hypoxic fraction = 0.01) with Bamor Cyclophosphamide (300 mgjkg) achieved a volume reduction to 1 rom in ten days andat this size radiosensitivity had increased to that of untreated 1 rnrn microtumorsand no hypoxic population was detected.
The results show that for the Lewis Lung Carcinoma: 1) tumor cell sensitivity~o radiation or chemotherapy decreased as microtumors became larger than 1 rom indiameter, and 2) pretreatment of larger micrometastases tumors> 1 rnrn with chemotherapydoes produce changes in the tumors which are associated with a return to maximnntumor cell radiation sensitivity. The data give additional experimental support tothe clinical interest in early adjuvant therapy of micrometastases and for sequentialcombined modality therapy for larger tumors.
This work is partly supported by NCI Contract No. NCI-CM-237l7.
41
27 ___
THE ROLE OF RADIATION THERAPY IN THE TREATMENT OF SOFT TISSUE SARCOMAS
Theodore L. Phillips, M.D., Allen S. Lichter, M.D.,William M. Wara, M.D., Steven A. Leibel, M.D., and Dennis R. Hill, M.D.Division of Radiation Oncology, University of California-San Francisco
In order to define the role of radiation therapy in soft tissuesarcomas, we treated 90 patients with a combination of limited resectionand irradiation between 1959 and 1974. In the patients receiving over5000 rads, local control was achieved in 88% of lesions of the extremitiesand head. Lesions of the retroperitoneum and thorax were only controlledin 20% of patients. Crude 3 year survival was 50% for all patients. Thechief cause of death was distant metastases as well as local recurrencein retroperitoneal lesions. Functional results will be correlated withhistology.
28 ___
MULTIMODALITY THERAPY FOR METASTATIC OSTEOSARCOMA
James R. Cassady, M.D., Ralph R. Weichselbaum, M.D., NormanJaffe, M.D., Robert M. Filler, M.D., Hugh Watts, M.D.
Harvard University Medical School, Boston, Massachusetts
The therapeutic efficacy of high dose methotrexate therapy withcitrovorum rescue administered every three weeks as adjuvant therapy forosteosarcoma has been demonstrated. More recently, the efficacy of thisprogram on a weekly basis has become apparent. However, patients withosteosarcoma who present with metastatic disease or develop metastasisdespite adjuvant therapy continue to pose difficult patient managementdecisions.
We describe the results of an aggressive multimodality plan forosteosarcoma patients with metastases utilizing surgery, irradiation andweekly high-dose methotrexate therapy with citrovorum rescue developedat the Joint Center for Radiation Therapy, Sidney Farber Cancer Center andChildren's Hospital Medical Center. Of 23 patients with metastasis whoreceived weekly high dose methotrexate, 12 underwent irradiation to eitherregions of completely excised tumor (group 1) or regions of known residualdisease (group 2). Five of six patients in group 1 are alive withoutdisease and six of six have disease control in the irradiated site. Fourof six patients in group 2 are without evidence of disease, and all of thesehave control in irradiated sites. These were encompassable in small volumehigh dose portals. Two of six were not encompassable with high doseportals and failed in irradiated sites. The entire group of 23 patients isanalyzed for survival and sites of failure and an optimum therapeuticregimen outlined. A radiation dose response relationship for osteosarcomarelated to tumor volume is suggested and correlated with previous knownlaboratory and clinical data.
42
29_
THE CORRELATION BE1WEEN IN-VITRO LABELLING INDICES (LIS) AND TUMORREGRESSION FOLLOWING RADIOTHERAPY.Flora T. Elequin, Ph.D. *, Franco M. Muggia, M. D. **, and Nemetallah A. Ghossein, M.D. **Radiotherapy Section- Albert Einstein College of Medicine of Yeshiva UniversityBronx, New York.** National Cancer Institute, Bethesda, Md.
The in-vitro labelling indices (LIs) of fine-needle aspirates obtainedfrom 31 cases of solid twnors were studied before, during and after radiotherapy.The fine-needle aspirates obtained from metastatic lymph nodes and subcutaneousnodules were incubated for 30 to 60 minutes at 370 centigrade in 4 - 5 ml of culturemedium (Eagle's minimum essential medium + 10% fetal calf serum) containing2 pc Iml of H3-thymidine. After incubation the tumor cells were concentratedby centrifugation in a density gradient solution (specific gravity 1.050 - 1.052),which was prepared by adding 10 volumes of 33. 9% sodium Hypaque solutionand 24 volumes of 9% Ficoll solution. The desired specific gravity was obtainedby diluting with double-distilled water. Concentrated malignant cells wererecovered from the interface of the two liquids and were spread over a smallarea (5 mm in diameter) of the slide with the Cytospin centrifuge. Fixed slides werecoated with Kodak NTB-2 emulsion and the film was exposed for three days beforeautoradiographs were developed. Eleven cases of squamous cell carcinoma werestudied. Their pre-radiotherapy LIs ranged from 0.7% to 28.6%. Their geometricmean was 3. 8%. Samples obtained during and after radiotherapy showed LIs of 0.0%to 2.6% with a geometric mean of 0.6%. Twenty cases of adenocarcinoma werestudied. The pre-radiotherapy samples had a LIs which varied between O.9% to23.7%, with a geometric mean of 4. 6%. Post-radiotherapy samples varied between0.0% to 19% with a geometric mean of 1. 8%. Lls were performed following doseswhich varied between 1000 to 5000 rads, The drop in LIs following radiation seemedto correlate with tumor regression. Favorable responses (decrease in mean diameterby 50% or more) were observed whenever post-radiotherapy Lis showed at leasttwo-thirds decrease from the pre-radiotherapy Lis. This technique may be usefulin determining the radiation response of accessible tumor nodules.
(This investigation was supported by Grant # CA 14770, awarded by theNational Cancer Institute, DHEW )
43
30_
WITHDRAWN
31_
UNUSUAL RADIATION RESPONSE OF HUMAN OSTEOGENIC SARCOMA CELLS IN VITRO----Ralph R. Weichselbaum, M.D. and John B. Little, M.D., Harvard MedicalSchool, Joint Center for Radiation Therapy, and Harvard School ofPublic Health, Department of Physiology.
We have established three human tumor lines of varying radiocurability intissue culture: osteosarcoma, medulloblastoma and glioblastoma. We havedetermined their X-ray and UV survival parameters in vitro. Sublethal damagerepair was examined by split dose experiments in all lines. The osteosarcomacells appeared unusually sensitive to UV light irradiation when compared to humandiploid fibroblast strains and we will describe the effects of "UV-like" drugson their in vitro cellular survival.
The capacity to repair potentially lethal X-ray damage (PLD) was measuredby irradiating the tumor cells in the plateau phase of growth and delayingsubculture for 0 to 24 hrs. The duration of PLD repair in the osteosarcoma cellswas longer and the degree of the enhancement of survival was greater than has beenseen in a number of aneuploid cell lines. Significant repair was observed followingdoses of 200 rads. We conclude that the efficient repair of potentially lethaldamage may be an important factor in the radiation response of human malignanttumors.
44
32 ___
RADIATION INDUCED OSTEOGENIC SARCOMA OF C3H MOUSE: NATURAL HISTORY, TCD50ASSAY AND INFLUENCES OF WBI AND CORYNEBACTERIUM PARVUM ON THESE PARAMETERSChan H. Choi, M.D., M.S., D.M.R.T., F.R.C.P.; Robert Sedlacek, B.S., M.S.;Herman Suit, M.D., D.Phil.Edwin L. Steele Laboratory of Radiation Biology, Department of RadiationMedicine, Massachusetts General Hospital, Boston, Mass.
A radiation induced osteogenic sarcoma of C3H mouse was studied for itsgrowth, pattern of spread, immunogenicity, and response to local irradiationin mice with tumor isotransplanted to the right flank (s.c.). 60 mice wererandomized into 3 groups: Control, WBI (600 rads 24 hours prior to tumortransplantation) and C parvum (350 mcg. I.V. 96 hours after tumor transplantation). Median survivals were 126 days, 118 days and 151 days forControl, WBI and C parvum group respectively. Tumor appeared in the flankof 100% of Control and WBI group, and 17 of 20 mice in C parvum group.Pulmonary metastases were found in 85%, 100% and 70% of Control, WBI andC parvum groups respectively. Lungs were the only site of metastases in50 of 51 mice with metastases. 3 TCD50 assays were performed with tumortransplanted by trocar s.c. to the right hind leg (155 mice): Normalhosts (55), WBI (40), and a C parvum group (60 mice, 350 mcg. given I.V .at time tumor was 5mm); in all 3 assays, the local irradiation of tumorwas performed at tumor size of 8mm. Results of these studies will bepresented and compared with results obtained from related experimentsusing a fibrosarcoma and a squamous cell carcinoma.
This investigation was supported in part by Grant Number 2 ROI CA133ll,awarded by the National Cancer Institute, DHEW.
33 ___
EFFECT OF CALCIUM DEPRIVATION ON REPAIR OF POTENTIALLYLETHAL AND SUBLETHAL IRRADIATION DAMAGE IN HeLa CELLS
Bozidar Djordjevic and Giny Dymbort
Biophysics Laboratory, Memorial Sloan-KetteringCancer Center, New York, New York
Repair of sublethal damage in x- or gamma-irradiated HeLa cells isaffected by calcium in the nutrient medium, both in surface attached andfn suspended cells. A significantly lower recovery is obtained incalcium-free. than in complete Eagle's medium. This effect ispotentiated in a HeLa subline displaying a pronounced shoulder in thedose-response curve.
In cells irradiated in suspension, concurrent with repair of sublethaldamage, repair of potentially lethal damage takes place, as evidencedby an increased survival with time of plating after a single dose ofirradiation. Such cells display an increased slope and a reducedshoulder in dose-response curves, which is more pronounced when cells aresuspended in calcium-free medium. While the two repair processes are to
45
some extent complementary, they can be distinguished by appropriateplating techniques.
Our findings indicate that following irradiation cells are susceptibleto additional injury, and that this susceptibility wanes with time andmay be influenced by cultural conditions. This situation may have bearingto combined radio- and chemo-therapy of tumors, where the final outcomemay depend on the time scale of individual treatments.
34 ___
TUMOR REGRESSION PATTERN AND HOST CELL INFILTRATE IN FIBROSARCOMA GROWINGIN NORMAL AND IMMUNOSUPPRESSED C3H MICE.Oscar Mendiondo, M.D.; Herman D. Suit, M.D., D.Phil.; and Arul K. Bahn, M.D.Edwin L. Steele Laboratory of Radiation Biology , Department of RadiationMedicine, Massachusetts General Hospital, Boston, Mass.
The methyl cholanthrene induced fibrosarcoma is an immunogenic tumor asshown by a decrease in the TD50 and increase in the TCD50 in immunosuppressedhosts. When transplanted into the muscle of syngeneic C3H mice, the tumoris infiltrated by host cells and 10 days after transplant (>7mm in diameter),phagocytic mono-nuclear cel l s compose 25%+ 5%of the tumor cell population.Tumor regression patterns were studied after radiation doses which willinduce a local control rate of 50% and 90%. A slower regression rate anda decrease in the incidence of complete regression were found in the wholebody irradiated group . This was accompanied by a decrease in the proportionof tumor macrophages in the immuno-suppressed mice, as evaluated by incubationof tumor cell suspensions with colloidal carbon and rosette forming assays incell suspensions and in frozen sections. The importance of the host celli nf i l t r at e and its role in modifying the tumor control probability and regression patterns are discussed.
This investigation was supported in part by Grant Number 2 ROI CA133ll,awarded by the National Cancer Institue, DHEW.
35 ___
RADIATION NECROSIS OF THE RECTUM SURGICALLY CORRECTED BY THECOMBINED ABDOMINOTRANSSACRAL TECHNIQUE
Gerald Marks, M.D.Jefferson Medical CollegeThomas Jefferson UniversityPhiladelphia, Pennsylvania
A method of rectal reconstruction by combined abdominotranssacralproctocolectomy and proctocolostomy is reported as an alternative to thetime-honored surgical conservatism in managing the radiation-injuredrectum. This presentation deals with the technique as it has beenemployed since 1960 as a method of sphincter preservation in thetreatment of benign and malignant lesions of the rectum. Its more recent
46
application and modification permitting an anastomosis with as small acuf f as 1 em are outlined in the treatment of nine patients with radiationinjuries of the rectum. Eight of the nine patients with radiationinjured rectums are now enjoying full and satisfactory reconstitutionof rectal function although it was necessary to perform the proceduretwice on two patients before the desired result was achieved. Thismethod has proven effective in providing normal rectal function in casesof radiation injuries so severe that a surgical technique employingan abdominal approach alone would not permit a low enough anastomosisand would require abandonment of the rectum. These results suggest thatreinspection of the traditional approach to the radiation-injured rectumis warranted now that safe and physiologically effective reconstitutioncan be accomplished by the combined abdomino~ranssacral technique, aprocedure that permits direct anastomosis under clear vision to a rectalstump of as little as 1 em.
36 ___
LOCAL CONTROL OF MALIGNANT MELANOMA BY RADIATION
Allan H. Rappaport, M.D. and Theodore L. Phillips, M.D.,Oivision ofRadiation Oncology, University of California San Francisco,Calif. 94143
Between 1959 and 1973 60 patients were treated for metastatic orrecurrent malignant melanoma at the University of California i n SanFrancisco. Of this ·g r ou p 41 patients completed a planned course ofexternal radiation to a total of 50 sites of disease. The largestnumber of sites treated were lymph nodes (21), skin (11), bone (8),and brain (5). Local control was evaluable for a minimum of 6 monthsin 27 sites. Permanent local control until death was obtained in8/27 sites, partial regression in 15/27 sites, and no response in4/27 sites. Those sites receiving less than 4500 rads tumor dosewere not controlled permanently. Radiation is found to have a definite role in the palliation of malignant melanoma, particularly inlymph nodes, brain, and skin, with application of moderately highdoses.
37 ___
NEUROBLASTOMA - RECOMMENDATIONS FOR THE ROLE OF RADIATION THERAPY IN ITS MANAGEMENT
Raymundo R. Calaguan, M.D.; Ned B. Hornback, M.D. ; Homayoon Shidnia, M.D.; andEdgardo Sayoc, M.D.Address: Department of Radiation Therapy
Indiana University School of Medicine1100 West Michigan StreetIndianapolis, Indiana 46202
From 1962-1975 40 consecutive cases of histologically proven neuroblastomas weretreated by the Department of Radiation Therapy at Indiana University Hospitals.All cases were analyzed at age of diagnosis. sex, primary presenting site. stage,
47
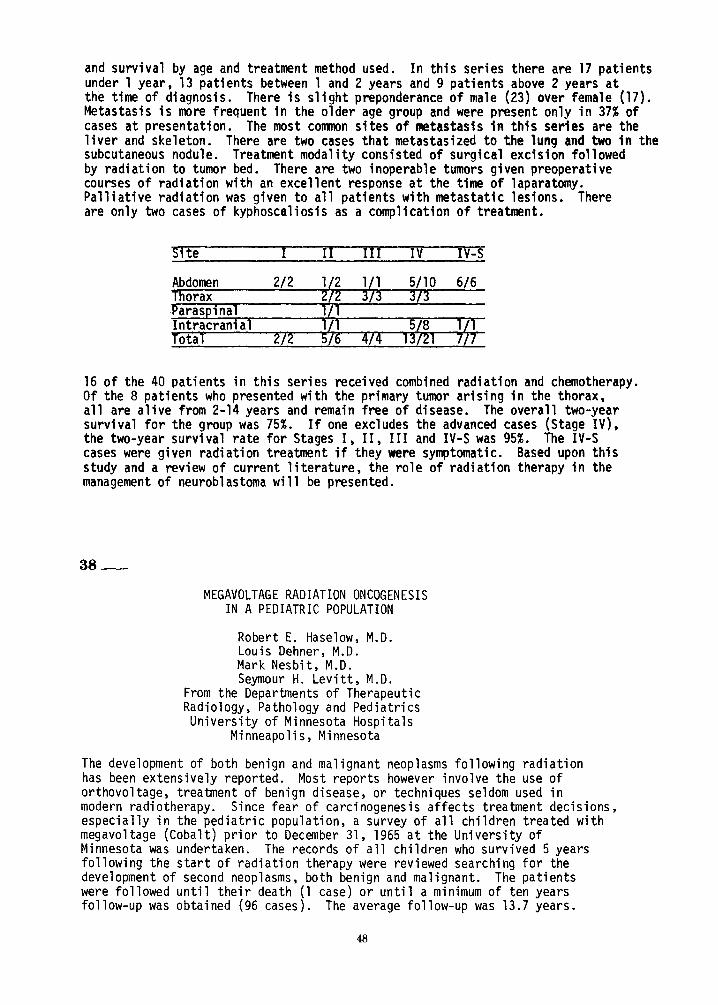
and survival by age and treatment method used. In this series there are 17 patientsunder 1 year, 13 patients between 1 and 2 years and 9 patients above 2 years atthe time of diagnosis. There is slight preponderance of male (23) over female (17).Metastasis is more frequent in the older age group and were present only in 37% ofcases at presentation. The most common sites of metastasis in this series are theliver and skeleton. There are two cases that metastasized to the lung and two in thesubcutaneous nodule. Treatment modality consisted of surgical excision followedby radiation to tumor bed. There are two inoperable tumors given preoperativecourses of radiation with an excellent response at the time of laparatomy.Palliative radiation was given to all patients with metastatic lesions. Thereare only two cases of kyphoscaliosis as a complication of treatment.
Site I II III IV IV-S
16 of the 40 patients in this series received combined radiation and chemotherapy.Of the 8 patients who presented with the primary tumor arising in the thorax,all are alive from 2-14 years and remain free of disease. The overall two-yearsurvival for the group was 75%. If one excludes the advanced cases (Stage IV),the two-year survival rate for Stages I, II, III and IV-S was 95%. The IV-Scases were given radiation treatment if they were symptomatic. Based upon thisstudy and a review of current literature, the role of radiation therapy in themanagement of neuroblastoma will be presented.
38 ___
MEGAVOLTAGE RADIATION ONCOGENESISIN A PEDIATRIC POPULATION
Robert E. Haselow, M.D.Louis Dehner, M.D.Mark Nesbit, M.D.Seymour H. Levitt, M.D.
From the Departments of TherapeuticRadiology, Pathology and PediatricsUniversity of Minnesota Hospitals
Minneapolis, Minnesota
The development of both benign and malignant neoplasms following radiationhas been extensively reported. Most reports however involve the use oforthovoltage, treatment of benign disease, or techniques seldom used inmodern radiotherapy. Since fear of carcinogenesis affects treatment decisions,especially in the pediatric population, a survey of all children treated withmegavoltage (Cobalt) prior to December 31, 1965 at the University ofMinnesota was undertaken. The records of all children who survived 5 yearsfollowing the start of radiation therapy were reviewed searching for thedevelopment of second neoplasms, both benign and malignant. The patientswere followed until their death (1 case) or until a minimum of ten yearsfollow-up was obtained (96 cases). The average follow-up was 13.7 years.
In a total of over 1300 patient-years, 8 neoplasms were discovered, six benign andtwo malignant. One malignant neoplasm was a neurofibrosarcoma developing near orat the edge of a low dose radiation field in a patient with neurofibromatosis.The other malignancy was a carcinoma in situ of the cervix developing nine yearsafter radiation to the right frontal lobe for an astrocytoma. Of the six benignneoplasms, four were unquestionably outside the prior radiation field. One ofthe benign radiation-unrelated neoplasms hemorrhaged, causing the only death dueto development of a second neoplasm in this study. One benign neoplasm was at ornear the margin and one was in the exit dose of a prior radiation field. Thesetwo benign neoplasms related to prior radiation were both asymptomatic and discovered incidental to radiographic examinations following up the primary tumoror its treatment sequelae. Neither would have been discovered had they been indifferent anatomic locations. Of 8 second neoplasms discovered, 5 were definitelynot related to prior radiation. The data of this retrospective review suggeststhat
1) the incidence of radiation induced neoplasia is less with megavoltagethan would be expected with orthovoltage,
2) children who survive one malignancy are much more susceptible to secondneoplasms than is the general population, regardless of prior radiationtherapy.
Supported by NCI grant CA-15548 and ACS grant CF 3557
39 ___
SIMILARITY OF SURVIVAL FOR IF AND EF RADIOTHERAPY AND
DECREASING FAVORABILITY OF NS HISTOLOGY
IN CHILDREN IN THE NATIONAL STUDY ON HODGKIN'S DISEASE
Arvin S. Glicksman, M.D., Melvin Tefft, M.D., Dept. of Radiation Medicine, BrownUniversity and Dept. of Radiation Oncology, Rhode Island Hospital; Lillian M.Fuller, M.D., Margaret Sullivan, M.D., Dept. of Radiotherapy and Dept. of Pediatrics, M.D. Anderson Hospital and Tumor Institute
Seventy one children between the ages of 10 and 18 were among the subjects ofthe National Study on Hodgkin's Disease Stages I and II and form the basis of thisreport. All the children had biopsy proven Hodgkin's disease, the pathologiesbeing reviewed by a central panel under the direction of Henry Rappaport. Stagingwas according to the Rye classification and required chest x-ray, bone marrow, andlymphangiogram as a minimum. Halfway through the study, laparotomies were more regularly performed and approximately half of the children in this study were subjectedto this procedure which included splenectomy, liver biopsies, and random sample of
49
periaortic nodes. The protocol randomized the patients to either involved fieldradiation (IF) or extended field radiation (EF) .
Only nine of the 71 children had mixed cellular lymphocyte depleted or anunclassifiable type of Hodgkin's disease. In the overall study (520 patients) 35%of the patients were found to have this pathology. Overall survival for both the IFand the EF treated patients is ident i cal at 90%. All 6 deaths occurred in patientswith nodular sclerosing Hodgkin's disease; only 4 of the so-called poor histologypatients have had an extension of their disease and all of these are in the nonlaparotomized patients. The full data on these 71 children will be discussed andthe implications for further studies presented.
40 ___
lIB &IIIB HODGKIN'S DISEASE : RESULTS OF COMBINED MODALITY TREATMENT
Robert Goodman, M.D., Peter Mauch, M.D., Anthony J. Piro, M.D.David Rosenthal, M.D., Samuel Hellman, M.D., Joint Center forRadiation Therapy, Peter Bent Brigham Hospital, and the Departments of Radiation Therapy and Medicine, Harvard Medical School,Boston, MA
Between April, 1969 and December, 1974,23 lIB &26 IIIB surgically stagedpatients with Hodgkin's disease were treated at the Joint Center for RadiationTherapy and affiliated hospitals. Stage lIB patients received either mantle andpara-aortic, total nodal irradiation (TNI) alone, or irradiation and MOPP chemotherapy if bulky disease was present. Relapse rate is similar for the two groups.Relapse-free survival is 84%and overall survival is 91 %with a median follow-upof 28 months. All three relapses were extensions; one is currently alive withoutdisease.
Of 26 IIIB patients, 6 received TNI alone with 4 relapses and 20 were treatedwith TNI and MOPP with 2 relapses. The relapse rates are significantly different(p= .05). Patients treated with the combined modalities have a relapse-free survival of 80% and overall survival of 90%with a median follow-up of 47 months.Patients over 40 years old have a statistically poorer prognosis and subdiaphragmatic nodal disease added to splenic involvement appears to confer a worse prognosis than just splenic involvement alone. There were 4 true recurrences, 2 extranodal relapses, and 2 disease related deaths. Four patients are presently al ivewithout disease.
These data suggest that radiation therapy alone may be sufficient treatmentfor those stage lIB patients with less extensive disease . The combination of TNIand MOPP is superior to TNI alone for stage IIIB disease. Tne survival of patientstreated with high dose TNI and MOPP suggests that this treatment allows relapse-freesurvival similar to early stage patients without systemic symptoms.
50
41 ___
HODGKIN'S DISEASE STAGE I AND II: A COMPARISON BETWEENTWO DIFFERENT IRRADIATION TREATMENT POLICIES
Thomas J. STOFFEL, M.D. (Walter Reed Army Medical Center)
and
James D. Cox, M.D. (Medical College of Wisconsin)
A retrospective analysis was performed on 145 patients with StageI &II Hodgkin's disease treated over a ten yeer period. Eighty-threepatients (Group A) received radiotherapy according to the present policy:all Stage I-B and II-B and all mixed cellularity and lymphocytic depletiontypes received total nodal irradiation while Stage I-A and II-A nodularsclerosing and lymphocytic predominance cases received irradiation to amantle field and to the para-aortic lymph nodes. Sixty-two patients(Group B) received a mantle field without systematic irradiation of thepara-aortic lymph nodes. Sixty-two patients (Group B) received a mantlefield without systematic irradiation of the para-aortic lymph nodes chains.The characteristics of the two groups were roughly comparable in age range,sex, staging, histopathologic subtypes and total irradiation doses. Allpatients had lymphangiograms although not all underwent staging laparotomies.The staging laparotomy did not appear to have an influence within eachgroup. The extent of irradiation did affect both the incidence of furthermanifestation of disease as well as survival rates. The incidence oflymph node extension, organ extension and local recurrence was 4%, 6%, and~% for Group A patients while for Group B i t was 24%, 14%and 3%, respectively. Especially notable was the pelvic nodal extension in 6 of 27 patientswith mixed cellularity in the Group B patients who did not receive pelvicirradiation. With an average follow-up of 3.75 years, 83%of Group Apatients are relapse-free with an over-all survival rate of 95%. Withan average follow-up of 4.75 years, 58%of Group B patients are relapsefree with an over-all survival rate of 63%.
42 ___
PREGNANCY FOLLOIVING OOPHOROPEXY AND TOTAL NODALIRRADIATION IN WOMEN WITH HODGKIN'S DISEASE
BY
Olivier Le Floch, M.D.Sarah S. Donaldson, M.D.Henry S. Kaplan, M.D.
From the Department of Radiology, Division of Radiation Therapy, StanfordUniversity School of Medicine, Stanford, Cal ifornia 94305
During the past decade at Stanford University Medical Center, oophoropexyhas been performed at the time of surgical staging in an attempt to protect
51
ovarian function in young female patients irradiated for Hodgkin's disease.When pelvic irradiation is administered, a 10 cm. thick lead block is usedto shield the ovaries in the midline. The dose under the center of the ovarianshield is 8% of the shielded dose, of which 0.5% is due to primary transmissionand the remainder to scattered radiation. With this technique, 2/3 of femaleshave retained ovarian function, and 9 women who underwent oophoropexy priorto high-dose pelvic irradiation have become pregnant. Six patients have givenbirth to 8 babies. An additional 2 patients have had therapeutic abortionsand 1 a spontaneous abortion. Five of the 9 patients received MOPP chemotherapyin addition to total nodal irradiation. The minimum radiation dose to the ovarieswas 350 - 400 rads in 39 - 46 days. No abnormalities have been observed inthe children; no ectopic pregnancies have occurred. There has been no instanceof recurrent Hodgkin's disease occurring in a pelvic lymph node under the pelvicmidline block.
Supported in part by grant CA-05838 from the National Cancer Institute,National Institutes of Health.
43_
COMPLICATIONS OF TREATMENT OF HODGKIN'S DISEASE
Hipolito Poussin-Rossilo, M.D., Lourdes Z. Nisce, M.D.,&Burton J. Lee, M.D .
Memorial Sloan-Kettering Cancer CenterNew York, New York
The use of wide field irradiation for the management of Hodgkin'sdisease and the common sites of involvement by disease make' it necessaryto include many normal structures within the treatment volume.Complications have been previously described by several authors. Thepurpose of this study is to analyze the complications of the use ofthe "3 &2" technique in regard to cardiac, pulmonary, and thyroiddiseases induced by this approach. In addition, the incidence ofHerpes Zoster in relation to sequential irradiation and chemotherapy, andthe influence of splenectomy will be reviewed. Since 1969, the managementof Stage III patients at Memorial Hospital has been total nodal irradiation employing split-course and sequential irradiation techniques,the so-called "3 &. 2" techni que. A dose of 3500 to 4000 rads isdelivered in 2 phases in an overall period of 11 to 12 weeks. Of the131 patients treated between 1969-1974, 2 developed pericarditis (1.5%),6 pneumonitis (4.6%), 5 hypothyroidism (3.8%). The incidence of HerpesZoster in patients receiving total nodal irradiation following asplenectomy is 91%and the onset is 5 to 10 months following treatment.The lower incidence of pericarditis and pneumonitis as compared toother series, is primarily the result of the ability to shrink fieldsafter the first phase of treatment.
52
44 ___
EPITHELIOID GRANULOMAS ASSOCIATED WITH HODGKIN'S DISEASE - CLINICAL CORRELATIONS
BY
E.L. Sacks, M.D.S.S. Donaldson, M.D.J. Gordon, M.D.R.F. Dorfman, M.D.
From the Department of Radiology and Pathology, Stanford University MedicalCenter, Stanford, California, 94305
Records of 512 consecutive patients with biopsy proven Hodgkin's disease initiallystaged and treated at Stanford University Medical Center between 1968 and 1973were examined. Forty-five of these patients (8.7%) with histologically verifiednon-caseating epithelioid granulomas in addition to Hodgkin's disease wereanalyzed separately from the non-granuloma group. The two groups were equivalentwith regards to age, sex, stage and histological subclassification. Survivaland relapse-free survival data with follow-up from two to seven years are 93.6%and 68.1% for the granuloma group and 75.7% and 61.9% for the non-granulomagroup. Survival is significantly improved for the granuloma group (p=O.03).Analysis of histological subcategories reveals significant improvement of bothsurvival (p=0.02) and relapse-free survival (p=O.03) when granulomas are associatedwith the nodular sclerosing Hodgkin's disease subgroup. Concomitant granulomasand Hodgkin's disease were found in 2/22 liver biopsies and 9/36 spleens. Ofthose 10/45 patients with granulomas who suffered a relapse after initialtherapy, two extended to areas previously involved with granulomas. Elevenpatients demonstrating hepatic granulomas without concomitant Hodgkin'sdisease at initial staging did not receive prophylactic hepatic therapy. Fiveof these eleven relapsed, but none primarily in the liver. We conclude that:1) epithelioid granulomas found in patients with Hodgkin's disease may b~
associated with increased overall survival 2) the presence of granulomas inan organ does not herald involvement with nor subsequent extension of Hodgkin'sdisease into that organ.
Supported in part by grant CA-05838 from the National Cancer Institute, NationalInstitutes of Health.
45 ___
EARLY NODAL AND EXTRA-NODAL NON-HODGKIN'S LYMPHOMAS
Salitha Reddy, M.D., Virendra S. Saxena, M.D. and Frank R. Hendrickson, M.D.Department of Therapeutic Radiology, Rush-Presbyterian St. Luke's Hospital
Chicago, Illinois
There were 53 Stage I and 38 Stage II non-Hodgkin's lymphomastreated with curative radiotherapy through the years 1964 to 1974. Theactuarial 5-year survival rates of Stage I and II were 88% and 49%respectively. Their recurrence-free survival rates were found to be57% for Stage I and 28% for Stage II at the end of five years. Thesites of first recurrence were also evaluated; 14 out of 22 Stage.Iand 18 out of 27 Stage II patients recurred in nodal areas as thelr
53
first site of recurrence. In 40%. this was in contiguous nodal areasonly. The influence of this on proposed management will be discussed.Extra-nodal non-Hodgkin's lymphomas. survival and recurrence-freesurvival rates at 5 years were 92%and 82%for Stage I and 47%and28%for Stage II. The survival and recurrence-free survival rateswere evaluated according to the histology.
46 ___
WHOLE BODY SURFACE ELECTRON IRRADIATION FOR GENERALIZED LYMPHOMA CUTIS
Theodore C.M. Lo. M.D .• Ferdinand A. Salzman. M.D .•E. Laurie Tolman. M.D. &Kenneth A. Wright. M.S.
Lahey Clinic FoundationBoston, Massachusetts
Two hundred patients with generalized Lymphoma Cutis treated withwhole body surface electron irradiation were reviewed and analysed.All patients were treated in the department of Radiotherapy of the LaheyClinic at the Massachusetts Institute of Technology. Three million-volt electrons generated with a Van de Graaff accelerator were employed.Type of generalized skin lesions. stage of the disease, duration ofinitial remission and frequency of recurrence were found to be themost significant prognostic signs. Survival rates were evaluatedrelative to these factors. as well as to radiation dose and fractionationschemes.
The techniques in treating the entire body surface with lowmegavoltage electrons, particularly with respect to the difficultiesin obtaining a homogeneous dose distribution and obtaining an accuratetotal dose calculation. are discussed. We have improved our treatmentmethod by changing the original four-field technique to a six-field,and most recently to an eight-field technique. Emphasis is placedon supplementary irradiation to certain cutaneous areas which could beunderdosed during whole body surface irradiation. A new formula isproposed to standardize methods in reporting doses.
47 ___
SPLENIC IRRADIATION FOR PAINFUL SPLENOMEGALY IN MYELOID METAPLASIA: A PRACTICALALTERNATIVE TO SPLENECTOMYJoel S. Greenberger, M.D., John T. Chaffey, M.D., David S. Rosenthal, M.D .• andWilliam C. Moloney. M.D. Joint Center for Radiation Therapy. Harvard MedicalSchool, and Division of Hematology. Department of Medicine, Peter Bent BrighamHospital, Boston, Mass. 02115.
In 240 patients with myeloid metaplasia (MM) (210 agnogenic and 30converting from polycythemia vera) seen over 8 years, 25 required treatment forpainful splenomegaly. Splenectomy was often contraindicated for several reasons.Radiation therapy to the spleen was compared to splenectomy as the initial
54
management modality in a series of 25 patients treated over an 8 year period.Fourteen patients received 21 courses of megavoltage splenic irradiation indoses ranging from 40 rad in 3 fractions over 5 days to 1028 rad in 16 fractionsover 28 days. The dose required for long-term palliative effect was usually low:Median dose 600 rads in 9 fractions. Patients received initial low fractions of10-25 rads to the entire spleen with daily slow increase in fraction size. Dailywhite blood cell and platelet counts were performed prior to each treatment tomonitor for the marrow suppressive effect. Spleen enlargement prior to treatmentranged from 6 cm to 25 cm below the left costal margin and in 6 patientssplenomegaly filled over half the abdomen . All 21 treatments produced palliationof abdominal and left shoulder pain and 20 (95%) resulted in reduction of spleensize: with 6 complete (28%) and 14 partial (67%) responses. Response durationranged from 1 to over 73 months with 4 patients over 24 months. Five patientssubsequently underwent splenectomy and 5 chemotherapy. One developed acutemyelogenous leukemia.
In contrast, eleven other patients were treated initially with splenectomyfor painful splenomegaly and clinical status similar to the radiation therapygroup. Three suffered complications of splenectomy in this disease including:severe thrombocytosis requiring chemotherapy in 2 patients, and left pleuralsepsis in one. Five patients are asymptomatic from 20 to 34 months aftersplenectomy. Two developed acute myelogenous leukemia. It is concluded that,while splenic irradiation in MM has been considered hazardous and nontherapeutic,our experience demonstrates that cautious irradiation of painful splenomegaly inselected patients is a safe and useful therapeutic alternative.
This work supported by Grant CA-12662 from the U.S. Public Health Service.
48_
COMBINED THERAPY IN CHILDHOOD NEUROBLASTOMA
Aly Razek, M.D .• Carlos Perez. M.O .• John Aufderheide. M.D.,Fred Askin. M.D.• Vita Land. M.D .• and Teresa Vietti. M.D.
Washington University School of Medicine. St. Louis. Missouri
During the past 25 years. 66 children with neuroblastoma and seven withgang1ioneurob1astoma have been treated with combined therapy at Ma11inckrodtInstitute of Radiology and St. Louis Children's Hospital. All werefollowed for at least three years. Complete resection was performed whenpossible. Adjunctive definitive radiation therapy invo1~8d tumor doses of3000 to 4000 rads in three or four weeks delivered with Co or 4 MeVx-rays. Prior to 1969, a few patients were irradiated with 250 Kvp x-rays.Beginning in 1964. cyclophosphamide, alone or combined with vincristine.was added; the course of chemotherapy varied from 6 months to two years.depending on the age of the child. stage, tolerance to therapy and response.Three year disease free survival was 100%for Stage I, 80%for Stage II.50%for Stage III. 8%for Stage IV. and 86%for Stage IV-S. Overallsurvival was 29%among children with neuroblastoma and 73%among those withganglioneuroblastoma. Tumors in the nasopharynx and posterior mediastinumwere more responsive than those in the lumbar or pelvic sympathetic chain.while adrenal tumors had the poorest prognosis. Eight children survivingmore than five years developed scoliosis. with four severely affected;three developed liver fibrosis and portal hypertension after liver irradiationand chemotherapy. There were single occurrences of necrosis of ribs.osteochondroma. and chondrosarcoma.
55
49 ___
ROUND CELL TUMORS OF BONE: RESULTS OF TREATMENTWITH PRIMARY IRRADIATION AND MULTIAGENT CHEMOTHERAPY
Leslie Botnick, M.D., Hugh Watts, M.D., Norman Jaffe, M.B.,B.Ch., Dip. Paed., J. Robert Cassady, M.D.
Joint Center for Radiation Therapy, Boston, Massachusetts
Fifteen previously untreated patients with localized Ewing's Sarcoma(11) or Reticulum Cell Sarcoma (4) were evaluated for disease extentbetween October, 1970 and September, 1974. Diagnosis was established byincisional biopsy. Ten patients had disease confined to the extremitiesand 5 to the axial skeleton. Median follow up is 37 months (13-69).Patients received 4000-4600 rad to large fields and an additional 10001400 was given to a cone down portal. Extremities were treated by sparinga vertical strip of normal tissue. Thirteen of 15 patients receivedmultiagent chemotherapy which was begun concomitantly and was continuedfor 18-24 months. All patients with extremity lesions have undergonegrowth study analysis and all have maintained adequate function in thepreserved limb. Three patients have had corrective surgical procedures,internal fixation (2) and contralateral epiphysiodesis(l). Eight of 10patients with extremity lesions (80%) remain free of disease and nonerecurred locally. Of the 5 patients with axial tumors, one remains freeof disease (20%) while the others have failed distantly (4) and locally(1) •
Thus, with primary irradiation and multiagent chemotherapy functionis preserved in the intact extremity. Axial lesions seem to have a worseprognosis despite multiagent chemotherapy. Ewing's Sarcoma and ReticulumCell Sarcoma requires similar treatment philosophy.
50 ___
STAGE I ENDOMETRIAL CARCINOMA: PRE-OP INTRACAVITARYIRRADIATION FOLLOWED BY IMMEDIATE HYSTERECTOMY
David A. Deer, M.D., Charles Votava, Jr., M.D., Henrv P. Plenk, M.D.Thomas Roland, M.D. &Richard C. Brown: M.D.
Radiation Therapy Center, Sacramento, California
One hundred thirty-nine unselected cases with Stage I endometrialcarcinoma have been treated with pre-op intracavitary irradiation followed by immediate hysterectomy. Intracavitary irradition to the uterusand upper vagina (Fletcher-Suit applicators) is given over approximately72 hours to deliver 4000-4500 rads to Pt. A (5000 mg. hours). Surgeryfollows within two to five days. Surgical pathologic findings of cervixinvolvement, deep myometrial invasion, or extra-uterine extensiondetermines the need for further external irradiation. There have been
56
no post-operative deaths (less than one month) in those patients whohave followed the protocol. Morbidity has been minimal, and the average hospital stay was14 days. Of 115 patients with well-differentiatedtumors, 5 have developed recurrent disease of which 4 had deep myometrialinvasion. Of 23 patients with poorly-differentiated tumor, all failureshave been in patients with deep myometrial invasion. There has beenonly 1 local recurrence and uncorrected actuarial survival is 82%.The advantages of this technique are discussed.
51_
TREATMENT OF STAGE III CARCINOMA OF THE CERVIX
Edward E. Rogoff, M.D., Gustavo S. Montana, M.D. &Wesley C. Fowler, M.D.Division of Radiation Therapy, University of North Carolina
Chapel Hill, North Carolina
One hundred previously untreated patients with Stage III invasivesquamous cell carcinoma of the cervix treated from April 1969 throughJuly 1973 at North Carolina Memorial Hospital were reviewed. Themajority of patients received 5000 rads of external beam radiation tothe whole pelvis with a 25 MeV photon beam through anterior and posterior fields. If a oatient was a suitable candidate for intracavitarytherapy a single dose of 3000-4000 mg hours radium equivalent cesiumwas used. If intracavitary therapy was not possible an additional 1500rads delivered in 1~ weeks time of external beam therapy were given,using reduced lateral opposed portals. An overall, uncorrected, threeyear survival rate of 45 percent was obtained in this group of patients.Various factors such as bulk, distribution and differentiation of thetumor as well as the presence of urinary obstruction and the use ofintracavitary radiation are discussed and analysed in relationshipto local tumor control and prognosis.
52_
SEGMENTAL ABDOMINAL IRRADIATION (STRIP TECHNIQUE)IN THE MANAGEMENT OF CARCINOMA OF THE OVARY
Carlos A. Perez, M.D., Alvin Korba, M.D. &Peter Jacobson, medical studentDivision of Radiation Oncology, 4511 Forest Park, St. Louis
St. Louis, Missouri
The role of radiation therapy in the management of carcinoma of theovary has not been definitely established. The present study willevaluate the results in 38 patients with carcinoma of the ovarytreated with Cobalt 50 strip technique to the whole abdomen (3000 rads)and pelvic irradiation (2800 rads with 22 mv photons). The sites ofrecurrence and complications will be evaluated. Preliminary analysisin 30 patients show no pelvic or abdominal failures in four patientswith stage 1. In stage 2 the incidence of failure in the pelvis is
57
15% and in the abdomen 28%. In stage 3 the incidence of failureis 45%and in the abdomen 65%. Major complications have been noted insix patients (20%). The dosimetric considerations for the striptechnique in the light of recently acquired information related todiaphragmatic or lymph node spread of "carci noma of the ovary willbe reviewed. The complications will be analyzed according to thedose of radiation given. The results will be correlated accordingto the degree of differentiation of the tumor, which is known to bea significant prognostic factor.
53_
OVARIAN DYSGERMINOMA AND RADIATION THERAPY
John W. Karrow, M.D. and Ned B. Hornback, M.D.Department of Radiation Therapy, Indiana University School of Medicine
Indianapolis, Indiana
The case histories of fifteen patients with Ovarian Dysgerminomaswho were treated at the Indiana University Hospitals between 1962 and1974 are reviewed . These data are analyzed with respect to patient age,parity and stage of disease. Subsequent surgical and radiat~on therapyare evaluated in terms of tumor control and patient survival . Tumor controlby irradiation is correlated with the volume treated and the dose-timefract ionation. Data from this survey are compared with similar reportsfrom the literature which deal with Ovarian Dysgerminoma. Recommendationsfor managing this neoplasm are summarized .
54_PALLIATIVE SINGLE DOSE IRRADIATION OF 1000 RAD FOR
ADVANCED GYNECOLOGIC CANCER
Raleigh J. Boulware, M.D., Jess B. Cadero, M.D.,Luis Delclos, M.D., J. Taylor Wharton, M.D. and Lester J. Peters, M.D.
Department of Radiotherapy, M.D. Anderson HospitalHouston, Texas
Between 1967 and 1975, 118 patients with late stage gynecologic cancer(uterine cervix-82, cervical stump-4, endometrium-13, vagina-6, and ovary-13)were treated palliatively with single dose, 46 were treated with two singledoses, and 23 with three single doses. The single doses for the lattertwo groups were given 3 to 4 weeks apart . This modality of treatment wasgiven mainly to patients with far-advanced disease that could not bepossibly treated and benefit from conventional radiotherapy techniques.Some already had distant metastases and a few others were too old or weremedically unable to tolerate a prolonged course of radiation treatment.
A description of the radiation technique, analysis of signs andsymptoms palliated, tumor regression and local control within theirradiated area, survival, and some radiobiologic considerations in the useof large single doses will be presented .
58
55 ___
A RADIOTHERAPY SIMULATOR OF NOVEL DESIGN
Douglas Jones, B. Sc.
Douglas Schumacher, B.S.
Northwest Medical Physics CenterUniv. of Wash., RC-08, Seattle, Washington 98195
The high cost of present-day, commercially available radiotherapy simulatorsis a significant deterrent to the department considering the addition of thisvaluable tool to its armamentarium. The function of a simulator in theradiotherapy sequence has been analyzed and a machine constructed whichsatisfies the purpose so defined. An emphasis has been placed upon simplicityof design without sacrificing accuracy requirements. A gantry supportingstandard diagnostic X-Ray components is isocentrically-mounted with a fixedfocus-to-isocenter distance of 90 cm. At the opposite end of the gantry,means are provided to support a film cassette centered to the central axisof the beam. The couch, which is of unique design, consists of a lucitetop which is held off a central support allowing for unobstructed views overa broad arc. Other features of the macAine, such as patient contour plottingand fiduciary marking, are described and their use illustrated by examples.The machine is designed for radiographic use only and by employing standardcomponents wherever feasible it has been possible to produce a completesystem for less than $50,000.00.
56 ___
LARGE FIELD IMAGERY FOR DOSE DISTRIBUTION
William J. Root, M.M.Sc.; Alan Simons, M.S.; Arthur B. Kirchner, M.D.Division of Radiation Therapy, Emory University Scnool of Medicine, Grady MemorialHospital, 80 Butler St., S.E., Atlanta, Ga. 30303.
Fluoroscopic Imaging for therapy simulation has associated with It severalinherent factors which limit both Its quality and utility. Among these are relativelysmall input Phosphorus making it necessary to utilize scanning mechanisms for planninglarge fields and large Target to Screen distances making It necessary to use high m Atechniques. The authors have designed an imaging system using the Practical Applicationof Flbroptics Technology. The system features a 34 cm. square Input phospher makingit possible to visualize the large field techniques without scanning the field. Thesystem also incorporates a disk recorder to allow for prolonged study of a simulatedport without further exposure to the patient, and a video tape unit to allow playbackof previous simulations. Both of these features enhance the unit's value as a teachingaid.
Picture quality is good and exposure techniques are qui,te low. Systems performances data and design considerations will be discussed.
59
57 ___
ROLE OF ULTRASOUND IN THE TREATMENT PLANNING
OF PATIENTS WITH BREAST CANCER
by
C. M. Mansfield, M.D.K. Strubler, M.S.
N. Suntharalingam, Ph.D.
Thomas Jefferson University HospitalPhiladelphia, Pennsylvania 19107
For approximately three years, ultrasound techniques havebeen used in our institution to help outline the treatmentvolume in patients with breast cancer. The ultrasound procedureshave made it possible to obtain accurate surface contours,locate normal structures such as the lung and determine chestwall thickness. This information has been used to choose thevolume for which an optimal treatment plan can be developed.The ultrasound determination of surface contours was found tobe as accurate as conventional techniques of contour taking,such as flexible wires, casts, etc. In the determination ofchest wall thickness, the accuracy of ultrasound was as goodas methods that use the simulator or portal films. Ultrasoundexamination of the thickness of phantom and cadaver specimenshave shown it to be accurate to within 2-4 Mm.
In most instances, the use of ultrasound in the A, B orGray mode was quicker, less complicated and helped to improvethe initial patient set·up for treatment. Ultrasound is nowroutinely used as part of the radiation treatment planning inpatients with breast cancer.
Supported by the Public Health Service Research GrantNo. CA-08888 from the National Cancer Institute
60
58_
TESTICULAR SHIELDING OF PATIENTS RECEIVING INVERTED-Y IRRADIATION
Richard J. Carmel. M.D •• Bernice B. Palos. B.A •• C.R.P •• James P.Duggan. C.R.T •• Malcolm A. Bagshaw. M.D.
Stanford University School of Medicine, Radiation Therapy Division.Department of Radiology, Stanford, California
The testes dosage from the inverted-Y treatment field for 6 MVirradiation has been investigated using computer-aided densitometry andthermoluminescent and ionization dosimetry. The dosage to the testes isclosely related to the position of the testes relative to the inferiorborder of the inverted-Y field and ranges from 10%of the midplane tumordose at a position beneath the conventional 10 cm lead midline shieldingtray blocks to 3%of the midplane tumor dose when the testes are locatedbeyond the inferior border of the field.
In order to further reduce the testes dosage from transmitted andscattered radiation, a lead testes shield was fabricated and its effectiveness evaluated in real and phantom patients. The testes shield was foundto reduce the dosage to the testes by as much as 75%and was most effectivewhere the testes were in a position distal to the inferior border of thefield. At this location. the testes shield reduces the testes dose toapproximately 33 rads for a full inverted-Y tumor dose of 4400 rads. Theunshielded testes dose would be 132 rads. This degree of reduction intotal dose to the testes may be a critical factor in preserving fertility .
59-
THE OPTIMIZATION OF EXTERNAL BEAM RADIATION THERAPY
Stanley McDonald. Ph.D .• Philip Rubin. M.D.Division of Radiation Oncology. University of RochesterCancer Center, 601 Elmwood Avenue, Rochester. New York.
An algorithm and its computerized implementation is presented bywhich optimal external beam treatment plans may be realized. A novelapproach is taken to solve the quadratic optimization problem by whichthe optimum beam configuration yields a dose distribution which provtdesthe best "least squares" fit to a prescribed tumor contour. subject todose constraints at neighboring vulnerable sites. The variables in thisproblem are per beam exposure. orientation on a plane, field size, andPb wedge angle. In this program, a maximum of 72 separate beams may beaccommodated with .up to four different field sizes at 18 positionsdirected at a common axis. An assortment of optimum treatment plansfor various anatomical sites are presented. The hardware interfacebetween computer and therapy unit necessary for routine implementat ion ofthis program i s described and is presented as the first method bywhich optimal dynamic external beam therapy may be realized.
61
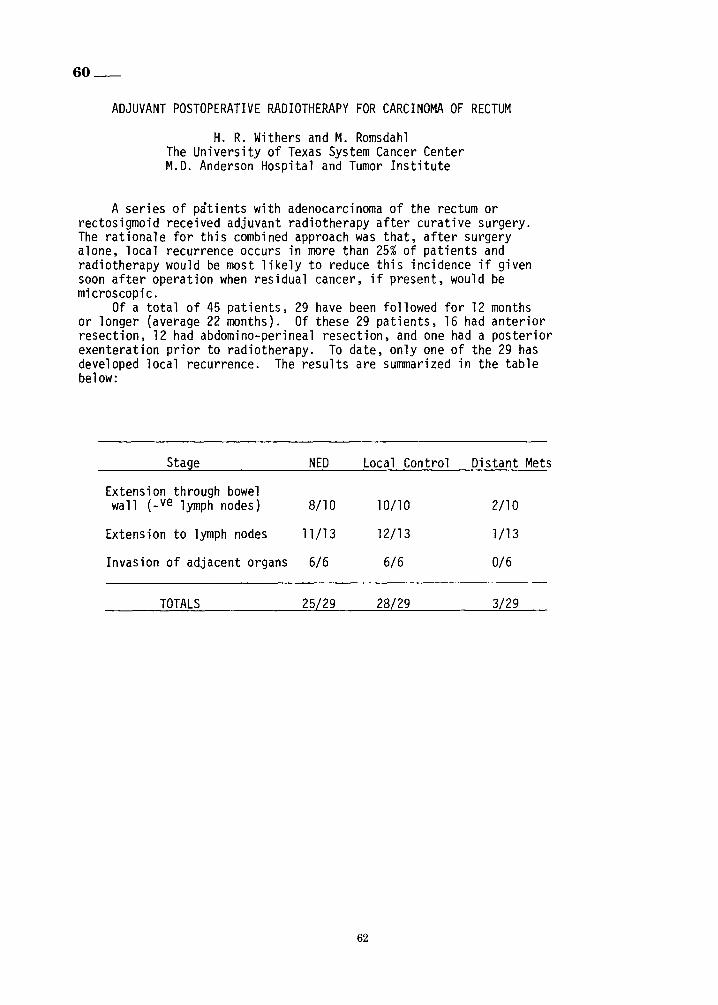
60_
ADJUVANT POSTOPERATIVE RADIOTHERAPY FOR CARCINOMA OF RECTUM
H. R. Withers and M. RomsdahlThe University of Texas System Cancer CenterM.D. Anderson Hospital and Tumor Institute
A series of patients with adenocarcinoma of the rectum orrectosigmoid received adjuvant radiotherapy after curative surgery.The rationale for this combined approach was that, after surgeryalone, local recurrence occurs in more than 25% of patients andradiotherapy would be most likely to reduce this incidence if givensoon after operation when residual cancer, if present, would bemicroscopic.
Of a total of 45 patients, 29 have been followed for 12 monthsor longer (average 22 months). Of these 29 patients, 16 had anteriorresection, 12 had abdomino-perineal resection, and one had a posteriorexenteration prior to radiotherapy. To date, only one of the 29 hasdeveloped local recurrence. The results are summarized in the tablebelow:
Stage NED Local Control Distant Mets
Extension through bowelwall (_ve lymph nodes) 8/10 10110 2/10
Extension to lymph nodes 1.1/13 12/13 1/13
Invasion of adjacent organs 6/6 6/6 0/6
TOTALS 25/29 28/29 3/29
62
61_
ANTERIOR RESECTION AND PRIMARY ANASTOMOSIS FOLLOWING HIGH DOSEPREOPERATIVE IRRADIATION FOR ADENOCARCINOMA OF THE RECTO-SIGMOID
K.R. Stevens, Jr.,M.D., W.S. Fletcher, M.D., and C.V. Allen,M.D.University of Oregon Health Sciences Center, Portland, Oregon
It is generally assumed by many surgeons and radiation therapists thatan anterior resection and primary anastomosis of the recto-sigmoid cannot be safely performed after high dose irradiation for adenocarcinomaof the recto-sigmoid. Our experience does not confirm this pessimisticview.
During the past 16 years we have had 12 patients whose surgery consistedof an anterior resection with primary anastomosis, following 5000 rads foradenocarcinoma of the recto-sigmoid. Treatment was given with 2MEV Van deGraaff or Cobalt 60 via opposed anterior and posterior pelvic fields, onefield treated daily. Treatment fields were small and ranged from 9 X 10to 11 X 11 cm in size. Midplane pelvic doses ranged from 4965 to 5050 radsand were given at a rate of 160 rads per day, 5 days per week. The loweredge of the treatment field ranged from 3 cm above the top of the pubicbone to 5 cm below the top of the pubic bone.
Anterior resection and primary anastomosis was performed 4 to 8 weeksfollowing the completion of irradiation. The highest tumor was 19 cmfrom the anal verge and the lowest tumor was 12 cm from the anal verge.An attempt was made to use non-irradiated bowel to form the anastomosis,but the demarcation line between irradiated and non-irradiated bowel wasnot always distinct. A protective colostomy was used in some patients whenit was felt that irradiated bowel may have formed part of the anastomosis.
Two patients had a temporary "protective" colostomy formed at the time of theresection and anastomosis, which was closed a few weeks later. One patienthad a colostomy because of obstruction prior to irradi &ion. This was closed6 weeks following the resection and primary anastomosis. One patient developed a post-resection sinus tract from the anastomosis to the pre-sacralhollow. This healed with only a temporary colostomy. One patient developedan anastomotic narrowing and para-anastomotic abscess draining into thebowel lumen after the resection. A permanent colostomy was formed one monthafter the resection.
Thus, of the 12 patients, 4 patients had a temporary colostomy, 1 patient hada permanent colostomy, and 7 patients required no colostomy. Six patientsare alive without tumor, 5 patients have died without evidence of rectaltumor, 1 patient died with liver metastasis and no evidence of pelvic tumor.
Anterior resection and primary anastomosis of the bowel can be safely performed in selected patients with adenocarcinoma of the recto-sigmoid following 5000 rads. We stress that if irradiated bowel is considered for formingthe anastomosis, a temporary "protective" colostomy should be formed.
Supported in part by NIH Grant #CA 05739
63
62 ___
COLORECTAL CARCINOMA:COMBINED TREATMENT WITH SURGERY AND POST-OPERATIVE RADIATION
LOS HOSPITAL EXPERIENCE
Leonard Gunderson, M.D., M.S., Charles Votava, M.D.,Richard C. Brown, M.D. and Henry P. Plenk, M.D.
Radiation Center, Latter Day Saints HospitalSalt Lake City,Utah
Fifty patients with colorectal carcinoma have been treated withpost-operative radiation with an 8-Mev linear accelerator at LOS Hospitalsince April 1971. Forty were irradiated after the initial operationrevealed gross pathologic extension outside the bowel wall and/orinvolved nodes, and ten after operations for recurrence.
Radiation factors were individualized by type of operative procedure, area and extent of tumor and radiographic position and mobilityof small intestine. Doses to the major field were usually 4500 rad/25fr/5wks or 5100 rad/30fr/6 wks. Boost fields were occasionallyutilized.
In January 1976, the 1st 44 patients were evaluated. In theprimary treatment group, a component of failure had occurred in thetreatment field (LF) in only 1/31 patients (3.2%) with. curativeresection vs 2/5 (40%) with known residual (1/4 and 2/4 in respectiverecurrent sub-groups). Distant failures (OF) were found as a newmanifestation in 23.5% of the primary and 42.9% of the recurrent groups.The incidence of severe complications in the group with primary treatmentnecessitating either an interruption in radiation (acute) or operativeintervention (chronic) was low (2/36 acute; 1/36 chronic).
Preliminary findings will be updated. The potential of lymphangiography, special small bowel studies and serial CEA and implications formodification of treatment policy will be discussed.
63 ___
ELECTIVE POSTOPERATIVE RADIOTHERAPY FOR LOCALLY ADVANCED COLORECTAL CANCER
Sophie S. Turner, M.D., Elio F. Vieira, M.D.Phyllis J. Ager, M.D., Nemetallah A. Ghossein, M.D.
Radiotherapy Section, Hospital of the Albert Einstein College of MedicineBronx, New York
The advantage of elective postoperative radiotherapy in colorectalcarcinoma are: (1) Adequate staging. Only cases at high risk of localrecurrence are irradiated. (2) No delay in performing the surgicalresection.
From October 1972 to December 1975, 40 patients at high risk forlocal recurrence (advanced Dukes' B &Dukes' C) received elective postoperative radiotherapy. Those with lesions that were located in the
64
rectum, rectosigmoid and low sigmoid colon were given 4600 rads in4 1/2 weeks through an inverted T-shaped field which encompassed the pelvicand paraortic nodes. Those with tumor located above mid-sigmoid regionwere treated to the entire abdominal cavity by the moving strip technique.
Of the group of 19 patients with rectal and rectosigmoid lesions,14 (74%) are alive N.E.D. (average follow up 16 months ± 2.5 months).Only two (11%) had local recurrence in the treated area.
Those with tumor above the mid-sigmoid have failed locally in ahigher proportion: 4 of 21 (19%). The technique, results and complications will be discussed.
64_
ADENOCARCINOMA OF THE COLON -- AREAS OF FAILURE IN A RE-OPERATION SERIES
Leonard L. Gunderson, M.D., M.S. &Henry Sosin, M.D. Ph.D.Department of Radiation Medicine, Massachusetts General Hospital
Boston, Massachusetts
Most data concerning areas of failure for carcinoma of the colonhave been derived from clinical or autopsy information. Both sourcescan be misleading.
In 1948 the University of Minnesota began utilizing plannedre-operations in patients at high risk for recurrent or metastaticdisease (failure) in spite of initial "curative" operative procedures.The main objective was to locate failures early and attempt operativeexicision and cure. Valuable information was obtained regardingincidence and areas of failure that has not been previously analyzedin detail.
Single or multiple re-operations were performed in 165 patientswith extra-colonic involvement and/or positive nodes at the initialoperation. Recurrence and/or metastasis was found in 105 at reoperation or subsequent follow-up.
Areas of failure were correlated with initial operative andpathologic information. This information will be compared withsimilar data from a rectal re-operation series published by the authorsand a colorecta1 series presented at the ASTR in 1975 by Cass, Million&Pfaff. Preliminary analysis of 50 patients with failure suggestedthat patterns of failure may differ by area of colon involvedbased on degree of anatomic mobility. Subgroups at major risk after"curative" operative procedures will be identified and implicationfor adjuvant therapy will be discussed.
65
65_
RADIATION MANAGEMENT OF PRIMARY CARCINOMA OF THE VAGINA
by Thongbliew Prempree, M. D., Ph. D. ; Thavinsakdi Viravathana, M. D.;Robert G. Slawson, M.D.; Morris J. Wizenberg, M.D.* , and CarloA.Cuccia, M.D. **
From Division of Radiotherapy, University of Maryland Hospital, 22 S. GreeneStreet, Baltimore, Maryland 21201
* Professor of Radiology, Department of Radiological Sciences, Universityof Oklahoma Health Sciences Center, P.O . Box 26901, Oklahoma City,Oklahoma 73190
** Director of Radiotherapy, Wilmington Medical Center, Chestnut &Broom Streets, Wilmington General Hospital, Wilmington, Delaware
This 15 year retrospective study includes 72 patients with diagnosis of primarycarcinoma of the vagina treated at University of Maryland Hospital, Radiation Therapysection from 1957 to the early part of 1971. The lesions were staged according to thesystem advocated by International Federation of Gynecology and Obstetrics (FIGO)with a minor modification (Perez et. cl , 1974) with the exception of Stage 0, histologicdiagnosis was 92.5% (60/65 ) invasive squamous cell carcinoma; 6.0% (4/65) - adenocarcinoma and 1.5% (1/65) malignant melanoma. Of 72 cases who are eligible for aminimum 5 year follow-up , the absolute 5-year cure rate for various clinical stagesis as follows :
Stoge 0Stage IStage IIAStage liBStage IIIStage IV
100%832%
62%63.5%
40%0010
(717)(5/6)(13 /21)(7I II)(8/20)(017)
The overall absolute 5-year cure-rate for all stages combined was 55.5% (40172 ).A comparable result and even better result in some stages (II and III) as compared toseveral previous reports a re thought to be due to the proper integrated irradiationcombining interstitial and intracavitary radium with external supervoltage beam.Furthermore, an aggressive radium implant to the vagina, paracolpium, and specificallyto parametrium and pelvic wall in Stage II and III appears to be one of the keys toour good results. The technique of treatment, stage by stage, will be fully discussedalong with a few complications and failures.
66
66 ___
DOSIMETRIC CONSIDERATIONS IN RADIATION THERAPYOF CARCINOMA OF THE VAGINA
Carlos A. Perez, M.D., Alvin Korba, M.D., James A. Purdy, Ph.D., andAxel N. Arneson, M.D.
Division of Radiation Oncology, Mallinckrodt Institute of RadiologySt. Louis, Missouri
Radiation therapy has been shown to be highly effective in thetre~tment of patients with stage 1 and 2 carcinoma of the vagina.However, it is important to determine the optimal dose of radiationrequired to irradicate the tumor and the minimal volume that should betreated, since an important consideration in the treatment of thesepatients is the functional results. The present study will evaluate theresults in the treatment of approximately 105 patients with epidermoidcarcinoma of the vagina treated with radiation therapy alone. Theminimal doses to the tumor will be individually computed and a correlation will be made between the stage and size of the tumor and controlwith radiation as a function of dose. If enough points are availablean attempt will be made to establish a dose time relationship for thevarious stages of carcinoma of the vagina. The volume to be treatedto a critical dose for each tumor stage will be determined. Preliminarydata shows that in patients with carcinoma in situ and stage 1 the sameresult can be obtained with interstitial an~intracavitary radium alone(90%control) or with intracavitary radium combined with external beamtherapy (92%). In stage 2 the results obtained with the combination ofintracavitary-interstitial and external beam therapy are better incomparison with brachy therapy alone.
67 ___
ADENOSQUAMOUS (AS) CARCINOMA OF THE ENDOMETRIUM:
AN ENTITY WITH AN INHERENT POOR PROGNOSIS?
Philip Rubin, M.D., Omar M. Salazar, M.D.,Elise DePapp, M.D., Thomas Bonfiglio, M.D.
University of Rochester Cancer Center,Strong Memorial Hospital. 601 Elmwood Avenue,Rochester, New York 14642.
Previous reports in the literature have considered this pathologicalentity to be more aggressive than pure adenocarcinoma of the endometrium,with a 5-year survival reported as low as 20%. The records and pathological materials from 1959 to 1974 at Strong Memorial Hospital yieldedover 400 uterine tumors. After exclusions, 375 cases of endometrialcarcinoma were an~lyzed . There were 259 pure adenocarcinomas, 29 adenocanthomas, and 87 adenosquamous carcinomas. After standardization
67
according to treatment employed, patients with pure adenocarcinoma ofthe endometrium treated with a combination of radiation and surgery werecompared with a similarly treated group of patients with AS carcinoma.Comparisons were done for incidence, age at diagnosis, the pathologicalgrade for the adeno-component, clinical stage, depth of myometrialinvasion, tumor sterilization, survival and patterns of failure.Although AS carcinomas tend to be of higher grade and a deeper depth ofmyometrial invasion, 5-year survival figures for both groups of patientstreated with the combined approach do not seem to be different. Theoverall end results of treating endometrial cancer with pre-operativeirradiation followed by surgery continues to be a highly curable disease.
68_
TREATMENT FAILURE SITES ACCORDING TO IRRADIATIONTECHNIQUE AND HISTOLOGY IN PATIENTS WITH
ENDOMETRIAL CANCER
Robert C. Landgren, M. D., Gilbert H. Fletcher, M. D.,H. Stephen Gallager, M. D., Luis Delclos, M. D.,
and J. Taylor Wharton, M. D.The University of Texas System Cancer Center
M. D. Anderson Hospital and Tumor InstituteHouston, Texas 77030
Pathology material from 372 patients with endometrialcancer treated from 1948 through 1969 and having completefollowup was reviewed by one pathologist. All patientscompleted definitive therapy with preoperative·irradiationand surgery or irradiation alone and have been separatedinto two main groups: (1) those treated with irradiationby radium alone or (2) those treated with external irradiation plus diminished amounts of radium. Treatment byradium alone led to fewer pelvic failures than did externalirradiation plus diminished amounts of radium, when evaluated by stage, grade, and specific histology. Both irradiation modalities led to about the same incidence of failures due to distant metastasis only.
Acknowledgement:
This investigation was supported in part by grants CA-06294and CA-05654 from the National Cancer Institute, DHEW.
68
69 ___
DEVELOPMENT OF ADRIAMYCIN RESISTANCEIN MAMMALIAN CELLS IN CULTURE
James A. Belli. M.D •• Stephen Saletan. A.B.
The Joint Center for Radiation Therapy andDepartment of Radiation Therapy. HarvardMedical School. Boston. Massachusetts
Chinese hamster lung fibroblasts (V79) in culture rapidly developresistance to Adriamycin (ADRM) when grown in the presence of low drugconcentrations. This resistance persists in cells removed from drug andgrown in drug-free medium; reversion to wild-type ADRM response did notoccur through 35 weeks. There is cross resistance to actinomycin-D.but the radiation respons·e is similar to wild-type V79. Resistanceappears to be cell membrane mediated. but is not reversed by treatmentwith Amphotericin-B. an anti-fungal agent which modifies the cellmembrane. Studies will be described on the radiation response ofresistant cells and their response to other chemotherapeutic agents.
(Supported by NCI. NIH)
69
70 ___
RADIATION-DRUG INTERACTIONS: SKIN TOLERANCE IN PATIENTS TREATEDPOSTOPERATIVELY FOR CARCINOMA OF THE BREAST
A.L. Schlichtemeier, M.D., R.C. Miller, M.D., S. Aristizabal, M.D. andM.L.M. Boone, M.D., Ph.D.
Arizona Medical CenterRadiation Oncology Division
Tucson, Arizona 85724
The enhancement of radiation effects in normal tissues by anticancer drugs is a matter of considerable current i nt erest . To date,most knowledge of this interaction has come from retrospective observations of adverse reactions.
In the past 10 months at the University of Arizona Medical Center,we have systematically observed the interaction of radiation withdoxorubicin (Adriamycin)-cyclophosphamide (Cytoxan) chemotherapy ina series of 22 patients treated postoperatively for breast cancer'
2All
patients have received at least two cyc1 2s of doxorubicin (40 mg/m IVon day 1) and cyclophosphamide (200 mg/m p.o. on days 3-6) as adjuvanttreatment. This is followed, after a two week rest period, by 4400 radsminimum tissue dose in 22 fractions to the chest wall and 4400 radsgiven dose in 22 fractions to the regional nodes. After an additionaltwo week rest period, adjuvant doxorubicin-cyclophosphamide chemotherapyis resumed for an additional six cycles. In evaluation of patients, skinreactions have been graded and clinical photographs taken. When comparedwith a radiotherapy only regimen of 5000 rads minimum tissue dose in 25fraction to the chest wall and 5000 rads given dose in 25 fractions tothe regional nodes, there is no significant difference in either the skinreaction during radiotherapy or the healing time following completion oftreatment. In contrast, in 6 patients treated with concommitant chemotherapy and radiotherapy or with a one week or less rest period beforeresuming chemotherapy, 3 patients developed significantly enhanced skinreactions over the treated fields.
While these results reflect only short-term observations, theysuggest that synergism between radiation and doxorubicin-cyclophosphamideis dependent upon time intervals between modes and that the synergisticeffects with regard to skin reactions can be minimized by appropriatesequencing as opposed to concommitant administration of radiation andanti-cancer drugs.
70
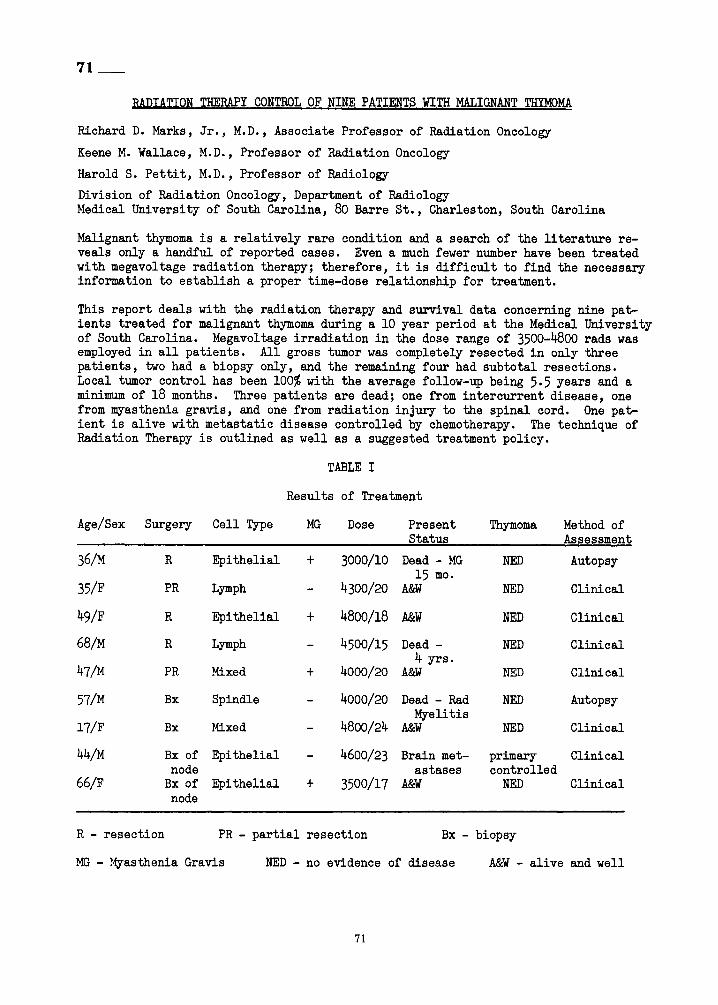
71_
RADIATION THERAPY CONTROL OF NINE PATIENTS WITH MALIGNANT THYMOMA
Richard D. Marks, Jr., M.D., Associate Professor of Radiation Oncology
Keene M. Wallace, M.D., Professor of Radiation Oncology
Harold S. Pettit, M.D., Professor of Radiology
Division of Radiation Oncology, Department of RadiologyHedical University of South Carolina, 80 Barre St., Charleston, South Carolina
Malignant thymoma is a relatively rare condition and a search of the literature reveals only a handful of reported cases. Even a much fewer number have been treatedwith megavoltage radiation therapy; therefore, it is difficult to find the necessaryinformation to establish a proper time-dose relationship for treatment.
This report deals with the radiation therapy and survival data concerning nine patients treated for malignant thymoma during a 10 year period at the Medical Universityof South Carolina. Megavoltage irradiation in the dose range of 3500-4800 rads wasemployed in all patients. All gross tumor was completely resected in only threepatients, two had a biopsy only, and the remaining four had subtotal resections.Local tumor control has been 100% with the average follow-up being 5.5 years and aminimum of 18 months. Three patients are dead; one from intercurrent disease, onefrom myasthenia gravis, and one from radiation injury to the spinal cord. One patient is alive with metastatic disease controlled by chemotherapy. The technique ofRadiation Therapy is outlined as well as a suggested treatment policy.
TABLE I
Results of Treatment
Age/Sex Surgery Cell Type MG
36/M
35/F
49/F
68/M
47/M
57/M
l7/F
44/M
66/F
R Epithelial
PR Lymph
R Epithelial
R Lymph
PR Mixed
Bx Spindle
Bx ?lixed
Bx of Epithelialnode
Bx of Epithelialnode
+
+
+
+
Dose Present ThYmoma Method ofStatus Assessment
3000/10 Dead - MG NED Autopsy15 mo.
4300/20 A&W NED Clinical
4800/18 A&W NED Clinical
4500/15 Dead - NED Clinical4 yrs.
4000/20 A&W NED Clinical
4000/20 Dead - Rad NED AutopsyMyelitis
4800/24 A&W NED Clinical
4600/23 Brain met- primary Clinicalastases controlled
3500/17 Am NED Clinical
R - resection PR - partial resection Bx - biopsy
MG - !.fyasthenia Gravis NED - no evidence of disease
71
A&W - alive and well
72 ___
EMPIRICAL TREATMENT OF MYASTHENIA GRAVIS WITHOUT THYMOMAS
by
Arnold Herskovic, M.D. James Lipsett, M.D., Frederick W.George III, M.D.
Radiation Medicine Unit, Department of Radiology, LosAngeles County/University of Southern California MedicalCenter. 1200 North State Street, Los Angeles, 90033 CA.
From 1964 to 1967 seven patients with Myasthenia gravis in poormedical control were empirically treated in the radiation medicineunit of the LAC/USC Medical Center. All of these patients hadnormal chest radiographs. Mediastinal tomography was not performed.A definite good clinical response with subjective improvement inthe symptomatology and decrease in medication dosage was describedin four patients. Some improvement was seen in one patient and noimprovement in the remaining patient. The seventh patient, who hadprior radiation to the same area, developed a cholinergic crisisfrom which she recovered.Each patient received about two thousand rads to the thymic area,delivered with a single anterior orthovoltage field. Two patientssubsequently had thymectomies at a time when one patient had improved from radiation and no subsequent improvement was noted fromthe thymectomy. The other patient had notbegun to improve untilseveral months after both the radiation and the thymectomy. Atsurgery both patients had minimal thymic tissue remaining.
72
73 ___
THE VALUE OF SUPRACLAVICULAR AREA TREATMENT INRADIOTHERAPEUTIC MANAGEMENT OF LUNG CANCER
Bahman Emami, M.D., Ding-Jen Lee, M.D., Ph.D., John E. Munzenrider, M.O.Department of Therapeutic Radiology, New England Medical Center Hospital,
Boston, Massachusetts
Between January 1, 1970 and December 30, 1974, 250 patients have beenirradiated for carcinoma of the lung at the Department of Radiotherapy atNEMCH. All patients whether inoperable or with post·op residual diseasehad histological verification of malignancy. 20% had supraclavicularinvolvement at initial presentation. Of these, no regrowth was observedin the supraclavicular area in all patients who received a minimum dose of4000 rads in 22 treatments. Approximately 40% of patients with initiallynegative supraclavicular area (clinically or biopsy) were treatedprophylactically to one or both supraclavicular areas. Over 95% ofthe group receiving supraclavicular irradiation did not develop involvementof this region during the remaining course of their disease. 20% of thepatient who did not receive prophylactic treatment to supraclavicularregion subsequently developed supraclavicular involvement. This is aretrospective study. Prophylactic treatment has been given to patientsconsidered at higher risk for supraclavicular metastasis. Therefore, themarkedly lower rate of involvement in the higher risk patients would appearto be significant, and due to the irradiation given this group.
The value of prophylactic treatment to the supraclavicular region inlung cancer patients relative to survival and incidence of distantmetastasis will be presented.
73
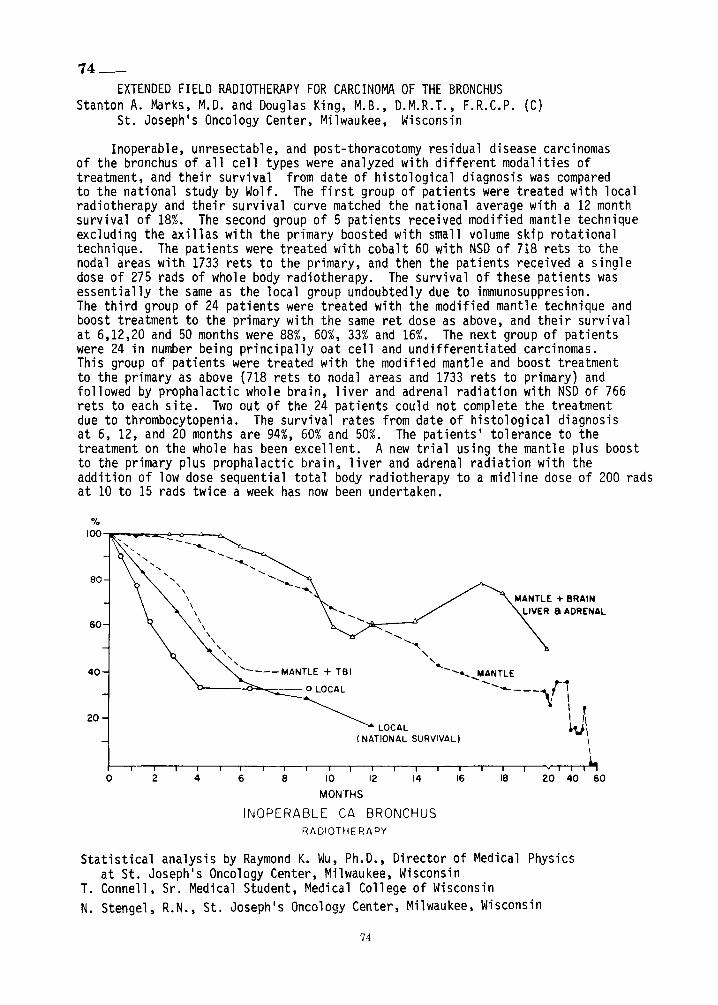
74_
EXTENDED FIELD RADIOTHERAPY FOR CARCINOMA OF THE BRONCHUSStanton A. Marks, M.D. and Douglas King, M.B., D.M.R.T., F.R.C.P. (C)
St. Joseph's Oncology Center, Milwaukee, Wisconsin
Inoperable, unresectable, and post-thoracotomy residual disease carcinomasof the bronchus of all cell types were analyzed with different modalities oftreatment, and their survival from date of histological diagnosis was comparedto the national study by Wolf. The first group of patients were treated with localradiotherapy and their survival curve matched the national average with a 12 monthsurvival of 18%. The second group of 5 patients received modified mantle techniqueexcluding the axillas with the primary boosted with small volume skip rotationaltechnique. The patients were treated with cobalt 60 with NSD of 718 rets to thenodal areas with 1733 rets to the primary, and then the patients received a singledose of 275 rads of whole body radiotherapy. The survival of these patients wasessentially the same as the local group undoubtedly due to immunosuppresion.The third group of 24 patients were treated with the modified mantle technique andboost treatment to the primary with the same ret dose as above, and their survivalat 6,12,20 and 50 months were 88%, 60%, 33% and 16%. The next group of patientswere 24 in number being principally oat cell and undifferentiated carcinomas.This group of patients were treated with the modified mantle and boost treatmentto the primary as above (718 rets to nodal areas and 1733 rets to primary) andfollowed by prophalactic whole brain, liver and adrenal radiation with NSD of 766rets to each site. Two out of the 24 patients could not complete the treatmentdue to thrombocytopenia. The survival rates from date of histological diagnosisat 6, 12, and 20 months are 94%, 60% and 50%. The patients' tolerance to thetreatment on the whole has been excellent. A new trial using the mantle plus boostto the primary plus prophalactic brain, liver and adrenal radiation with theaddition of low dose sequential total body radiotherapy to a midline dose of 200 radsat 10 to 15 rads twice a week has now been undertaken.
MANTLE + BRAINLIVER 8 ADRENAL
.................
.....,-,
"' ..... ........... MANTLE--........... r"_____.... : I
l: I
\ ~~\
I\
LOCAL(NATIONAL SURVIVAL)
-.............-- ................
<, ..... .............,
60
80
20
40
%I00 --.:"'-..-..~---o---:;..--n...
o 2 4 6 8 10 12 14 16
MONTHS
INOPERABLE CA BRONCHUSRADIOTHERAPY
18 20 40 60
Statistical analysis by Raymond K. Wu, Ph.D., Director of Medical Physicsat St. Joseph's Oncology Center, Milwaukee, Wisconsin
T. Connell, Sr. Medical Student, Medical College of WisconsinN. Stengel, R.N., St. Joseph1s Oncology Center, Milwaukee, Wisconsin
74
75 ___
ADRIAMYCIN, BLEOMYCIN & EXTERNAL IRRADIATION IN THE TREATMENT OFUNRESECTABLE BRONCHOGENIC CARCINOMA - A PILOT STUDY.
Paul Chan,M.D.*, John E. Byfield, M. D.+, Elmore Aronstam, M. D.**Edward Oppenheimer, M. D.o, Herman Nussbaum, M. D.*, Harvey A. Gilbert, M. D.*and A. Robert Kagan, M. D.*. from the departments of *Radiation Therapy,**Surgery and °Internal Medicine, Southern California Permanente MedicalGroup, Los Angeles, California and Department of+Radiation Therapy,University of San Diego, San Diego, California.
40 patients with unresectable bronchogenic carcinoma of various celltypes were treated by combination therapy of Adriamycin (ADR), Bleomycin (BLM),and megavoltage external irradiation (XRT). XRT was short-course treatment(4000 rads in 5 weeks). ADR was given with XRT on day 1 and then every 3
weeks. The dosage of ADR was 40 mg/M2 I.V. with radiotherapy and 50 mg/M2after radiotherapy to a total cumulative dose not to exceed 450 mg/M2•15 mg. of bleomycin was given twice weekly during radiotherapy, otherwisewas given simultaneous with ADR. This combination regimen was welltolerated. There was no fatal pulmonary or cardiotoxic complications.Of the 40 patients with lung cancer, 19 had squamous cell, 7 large cell,7 small cell and 7 adenocarcinoma. Based on partial (~50%) and completeregression, overall response was 23/40 (57%), including 8/40 (20%) completeregression. The response of small cell ca. was 71% (2 PR, 3 CR), squamouscell 58% (9 PR, 2C), large cell 57% (2 PR, 2 CR) and adenocarcinoma 42.8%(2 PR, 1 CR). During 6 to 15 months study period, 27 (&7%) patients arestill alive. Responders, particularly of a high initial (KarnofskyT s)performance status seemed to have significant survival advantage.Development of multi-agent combined therapy for unresectable lung cancerwill be discussed.
75
76 ___
CELLULAR IMMUNITY IN PATIENTS UNDERGOING RADIOTHERAPY
*S. Yang, PH.D. *S. Rafla, M.D., Ph.D. *
Recent studies indicate that the functional statusof immune systems may play a decisive role in the clinicalresponse of cancer patients to their disease and the treatment. The present report attempts to evaluate; (It cellularimmune competence of· patients scheduled to receive radiationtherapy; (2) possible correlation between the tumourbulk and the cellular immunocompetence~ (3) the possibleeffects of therapeutic radiation on their immune statusespecially when the thymus region was irradiated heavily.
One hundred twenty-five patients were studied.Malignancies represented included cancer of the breast,lung, head and neck and bladder. Healthy volunteers wereused as controls. We determined mainly PHA reactivity andspontaneous rosette formation, both before and aftercompletion of radiation therapy.
We have also examined the role of spontaneous invivo blastogenesis. Lymphocytes were isolated from-Peripheral blood by the Ficoll-Hapaque gradient method.
The in vitro findings and their relationship with theclinical course of the disease will be presented.
* Chief of Radiobiology, Radiation Therapy Dep't, TheMethodist Hospital, 506 6th St., Brooklyn, N.Y. 11215
** Director of Radiation Therapy, The Methodist Hospital,506 6th St., Brooklyn, N.Y. 11215
76
77 ___
IMMUNOTHERAPY OF PATIENTS WITH MYCOSIS FUNGOIDESFOLLOWING ELECTRON BEAM RADIATION *
J . R. McLaren, M.D.Z. L. Olkowski, M.D., Sc.D.F. S. Bilek, M.D.Laboratory of Tumor Biology and Clinical ImmunologyRobert Winship Memorial Clinic for Neoplastic Diseases'Emory University School of Medicine
Recent evidence suggests that Levamisole increases host resistance to avariety of infections and tumors. In vitro experiments indicate thatstimulation of cell mediated immunity may account for the effects of thisdrug. This stimulation as well as increased levels of cyclic adenosinemonophosphate were observed in lymphocytes of patients with solid tumorsfollowing immunotherapy with Levamisole (Wilkins and Olkowski, 1976).
Since most patients with mycosis fungoides show impaired cellular immunitythey qualify for adjunctive therapy with Levamisole. The objective of thisstudy was to stimulate the immunity of these patients following the completionof radiation therapy in conjunction with Levamisole and to determine whetherincreased immunocompetence correlates with clinical improvement defined asan increase in disease-free intervals.
This double blind, randomized study consisted of the administration ofLevamisole (2.5 mg/kg body weight, p.o., twice weekly) or Placebo to 12patients beginning the first week following the completion of radiationtherapy. T-lymphocyte levels, immunoglobul ins A, G, M, D, and E levels,cyclic AMP levels in lymphocytes isolated from peripheral blood, and skintests for recall antigens were used to monitor immunotherapy. A group ofhealthy individuals served as controls with the same parameters of immunitybeing evaluated.
We have found differences in circulating T-lymphocyte levels, cyclic AMPlevels, and immunoglobulin levels between patients receiving Levamisole andthose receiving Placebo . Significance of these findings and evaluation ofthe efficacy and safety of Levamisole will be discussed.
* Supported by a Grant from the Robert Winship Memorial Clinic for NeoplasticDiseases, Emory University School of Medicine
77
78_
BCG AND RADIOTHERAPY IN BRONCHOGENIC CARCINOMA: PRELIMINARY REPORT
S. Stefani and R. Kerman, Therapeutic Radiology and ResearchServices, VA Hospital, Hines, IL 60141
In a r~ndomized study we compared the effects of radiation therapy (RT) aloneor in combination with BCG on 24 patients with inoperable, locally advanced,bronchogenic carcinoma. Patient immunocompetence was evaluated before RTand at monthly intervals thereafter by the patient's reaction to five microbial skin test antigens and to dinitrochlorobenzene (DNCB) and by determining the amount of their thymus-derived (T) rosette-forming cells (RFC).Before therapy patients showed depressed response to skin test antigens andto DNCB and had decreased T-RFC. BCG treated patients exhibited more positiveresponses to skin test antigens and DNCB and higher response to in-vitrolymphocyte stimulation with PHA after RT than the patients exposed to RTalone: BCG treated patients converted to positive skin test responses afterRT more often than patients treated by RT alone. Based on life table analysis of survival rates the mean survival of BCG treated patients was at8.8 months compared to 6.3 months for patients treated by RT alone. Whilethese results are encouraging, they are not yet statistically significant.We did not observe any adverse side effects of BCG administration using themultiple puncture procedure.
Supported by the Medical Research Service of the Veterans Administration
79_
ORGAN-SPECIFIC DELETION IMMUNOTHERAPY - MODEL SYSTEMSAND PRELIMINARY STUDIES ON RADIATION RESISTANCE
John E. Byfield, Eric W. Fonkalsrud, Raque1 Zerubave1
Radiation Therapy Division, University of California,San Diego, California
Approximately one-third of human tumors are derived from organs whichare not intrinsically required for life maintenance or can be effectivelyremoved and the patient maintained by hormone administration. In theorycomplete removal of bulk disease by radiation therapy or surgery followedby active immunotherapy may be effective in prolonging the remission-free interval or increasing the cure rate. Amodel system for evaluatingthis (mouse neuroblastoma) has shown that specific antisera directed againstsurface antigens can be used to eliminate tumor cell burdens which arecompletely resistant to conventional therapies, and can reach tumor cellkilling in vivo greater by at least 4 logs than that capable of killingthe host animals. The effector cells in this reaction are highly radioresistant but appear limited in their capacity to migrate into tumors.Where appropriate anatomic prerequisites are met this approach which wehave termed "organ-specific deletion immunotherapy" may be quite useful.Preliminary experiments in ovarian cancer are in progress.
78
80_
A COMPARISON OF TIlE ANTITUMOR EFFECT OF CORYNEBACTERIUM PARVUM AND GLUCANIN MICEVlatko Silobrcic, M.D., Ph.D.; Arthur Elman, M.D.; Herman D. Suit, M.D., D.Phil.Edwin L. Steele Laboratory of Radiation Biology, Department of RadiationMedicine, Massachusetts General Hospital, Boston, Mass.
Glucan is a simple polyglucose molecule, minimally toxic and readily synthesized, that stimulates the RES system and has an antitumor effect. C parvumis a known stimulator of the RES system with a pronounced antitumor effect,and an appreciable toxicity. In this study, we compared the efficacy ofglucan to induce regression of 5mm fibrosarcoma growing as isotransplantsin the mouse leg to the well-documented antitumor effect of C parvum in thesame animal-tumor model system. An I.V. injection of 350 meg of C parvumcauses complete and permanent regression of 30-50% of such tumors. Glucanwas administered intravenously in doses of 200, 350, and 1000 meg. on day5, or as three injections of the same dose on days 5, 10, and 15 followingtumor transplantation. Single doses of 200 and 350 meg. cured no mice, buta single injection of 1000 meg. of glucan cured 3 of 15 mice, and 5 of 15tumor hosts were cured by 3 x 1000 meg. No instance of enhancement oftumor growth was observed. Therefore, in this system, glucan, when appliedin 1000 meg. doses, can be as effective as C parvum. Current studiesinclude : (1) increasing doses of glucan, and (2) effectiveness of combiningglucan with local radiation therapy in a highly radiation resistant squamouscell carcinoma.
This investigation was supported in part by Grant Number 2 ROI CA133ll,awarded by the National Cancer Institute, DHEW.
79
81 ___
STAGING OF CANCER IN HEAD AND NECK CANCERS
Harvey W. Baker, M.D.
No abstract available
82 ___
RESULTS OF INTEGRATED MANAGEMENT
OF SUPRAGLOTTIC CARCINdMA
Karen K. Fu, M.D., L. Eisenberg, M.D., Herbert H. Dedo, M.D.and Theodore L. Phillips, M.D., University of CaliforniaMedical Center, San Francisco, California 94143
Between January 1957 and June 1974, 177 patients withcarcinoma of the supraglottic larynx were treated by an integrated approach at the University of California in SanFrancisco. The policy was to use radiotherapy alone for earlycases, radiotherapy combined with either supraglottic laryngectomyor total laryngectomy for moderately advanced cases and radiotherapy alone for very advanced, inoperable cases. Controlof the primary lesion was achieved in 90% of Stage I, 92% ofStage II, 71% of Stage III, and 47% of Stage IV cases. Failuresafter radiotherapy alone in early cases were usually salvagedby subsequent surgery, whereas failures after surgery alonewere rarely salvaged by radiotherapy. Radiation alone controlled90% of patients with Stage I disease, locally, and preoperativeirradiation and supraglottic laryngectomy controlled more than90% of patients with late Stage I and early Stage III lesions.The treatment policy outlined above appears to have been highlysuccessful in yielding an excellent local control rate withpreservation of a functioning vocal apparatus.
80
83 ___
VOCAL CORD CARCINOMA : THE RELATIONSHIP BETWEEN POST-RADIOTHERAPYLARYNGEAL EDEMA AND LOCAL RECURRENCE
Carol Milligan. M.D .• Don R. Goffinet. M.D .• Willard Fee. M.D. andMalcolm A. Bagshaw. M.D.
Division of Radiation Therapy. Stanford University Medical CenterStanford. California
The records of 206 patients with vocal cord carcinomas treated atStanford with 4.8 &6 MV 1inacs between 1957 and 1975 were reviewedspecifically for the presence or absence of persistent post-irradiationedema. Moderate to severe laryngeal edema (either requiring the use ofcorticosteriods. tracheostomy or hospitalization or edema which wasrapidly progressive) occurred in 46 or 22% of the 206 patients. Thepercentage of patients with persistent edema ranged from 18% of thosewith T1A vocal cord cancers to 64% in those with T3 lesions. Over 80%of patients with edema had repeat laryngeal biopsies. A significantlyhigher incidence of recurrences was noted in patients with persistentlaryngeal edema (23 of 46 or 50%) compared to those in whom postirradiation edema did not occur (20 of 160 or 12.5%). p < 0.01. Localcontrol rates at 5 years. combining patients with stage T1A &T1Bglottic cancers were 92%for 116 patients without edema and 7% for 16with persistent edema. For the 44 patients with T2 lesions. thecorresponding values were 89%&21 %. respective and 66%&17%for 30patients with T3 carcinomas. Relapse free and actuarial survival at10 years (88%T1A. 50%T3- 4 disease free) and an analysis of time-dosefactors and their relationship to the subsequent development of edemawill also be presented. The paper will be illustrated by 35 mm photographs taken with the Hopkins rod direct vision laryngoscope.
84 ___
TIME. DOSE, AND TUMOR VOLUME RELATIONSHIPS IN MEGAVOLTAGEIRRADIATION OF SQUAMOUS CELL CARCINOMAS OF THE RETROMOLAR
TRIGONE AND ANTERIOR TONSILLAR PILLAR
Jerry L. Barker, M.D. and Gilbert H. Fletcher, M.D.The University of Texas System Cancer Center
M. D. Anderson Hospital and Tumor InstituteHouston. Texas 77030
Two-hundred and four patients with squamous cell carcinomasof the retromolar trigone and anterior tonsillar pillar weretreated with conventional definitive megavo1tage radiotherapy withconventional time schedules from March. 1954 to August. 1973. Thedata was analyzed with time-dose scattergrams in order to correlate the probability of control of the primary lesion with dose.total treatment time, and tumor volume (stage). For early lesions(T ). 6,000 to 6.500 rad tumor dose given in 6 to 6 ~ weeks isad~quate for a control rate of approximately 90%. For more advanced disease (T2-T3) a control rate in excess of 90% should beobtained when 7,000 rad tumor dose is delivered in 7 weeks. The
81
use of the high-energy electron and photon beam is often desirablein these patients but specific details of technique must be utilized because of the isodose curve contriction that is inherentwith these beams.
Surgical salvage in patients treated definitively with radiotherapy and who later fail at the primary site is high resultingin a combined ultimate failure rate in all stages of only 6%.
Complications were correlated with respect to dose andvolume of tissue irradiated. Eleven per cent of the patientsdeveloped spontaneous bone necrosis with one-half of thesere'quiring mandibu1ectomy after failing to heal with conservativemanagement. Elective dental extractions should only be performedwhen teeth are unsa1vageab1e, otherwise the necrosis rate willincrease.
Acknowledgement:
This investigation was supported in part by grants CA-06294and CA-05099 from the National Cancer Institute, DHEW.
85 ___
LOCAL CONTROLOF SQUAMOUS CARCINOMA OF ORAL CAVITY AND OROPHARYNX
WITH 3 VS. 5 TREATMENT FRACTIONS PER WEEK
Roger W. Byhardt, M.D.James D. Cox, M.D.
Radiation Therapy Section, MedicalCollege of Wisconsin, Milwaukee, Wisconsin
To compare the 18 month local control rates of 3 vs. 5 fractions perweek, the records of 94 patients at the Medical College of Wisconsinaffiliated hospitals, receiving external beam irradiation alone with curative intent, were selected for review out of 248 cases of squamous carcinomaof the oral cavity and oropharynx. Excluded were 154 cases: 45 preoperativeirradiation, 38 dead before 18 months of intercurrent or metastatic diseasewith local control, 33 postoperative irradiation, 25 interstitial implant, and13 consult only. With 3 fractions per week, the total tumor dose was calculated by the Ellis formula, and was taken as that dose associated with theupper limits of connective tissue tolerance (1800 ret), usually 5400 rads in6 weeks given as 300 rad 3 days per week. Those treated with 5 fractionsper week were taken to 6000-6600 rads in 6-7 weeks (1760-1860 ret). Withrelatively equal distribution of patients in each fractionation scheme bystage and site of primary, local control of the primary in those eligible for18 month fo110wup, was found to be significantly lower (P less than .05)with 3 fractions per week. While 37/63 (59%) patients achieved local controlat 5 fractions per week, only 5/31 (16%) did so for 3 fractions per week,all stages and sites combined. A similar trend was observed for each stageand site evaluated separately. The authors emphasize that caution should beused in applying the Ellis formula, which is based on radiation tolerance ofnormal connective tissue, to predictions of tumor lethal dose, especiallywhen using unusual fractionation schemes.
82
86 ___
MALIGNANT MAJOR AND MINOR SALIVARY GLAND TUMORS:TREATMENT RESULTS, SITES AND CAUSES OF FAILURE
Steven A. Leibel, M.D., Karen K. Fu, M.D., Lawrence M. Friedlander, M.D.Roger Boles, M.D. and Theodore L. Phillips, M.D.
Division of Radiation Oncology, University of California-San Francisco
We have reviewed the records of 160 patients with malignant majorand minor salivary gland tumors treated with surgery alone (50%), surgeryplus radiotherapy (36%) or radiotherapy alone (14%) at the Universityof California at San Francisco, Medical Center, between 1956 and June,1973. Extent of disease was retrospectively staged using a modificationof the clinical staging system for carcinoma of the parotid proposed bySpiro, Huvos and Strong (American J of Surg 130:452-459, 1975). Thepathology was reviewed and reclassified according to the World HealthOrganization system. The results and sites and causes of failure wereanalysed according to stage, histology and treatment modalities. Specialattention was paid to the influence of tumor size and histology on thelocal control rate with radiotherapy. Local control rate was directlyre~ated to the extent of the tumor. Postoperative radiotherapy enhancedlocal control in those patients with high-grade malignancy, as well asknown residual disease following surgery. The influence of histologicdiagnosis on local control by surgery and/or radiotherapy will bediscussed.
87 ___MALIGNANT PAROTID TUMOURS
*S. Rafla, M.D., Ph.D.
Sixty-five cases of histologically proven malignantparotid tumours are presented. Forty percent of the tumourswere differentiated adenocarcinoma, while malignant mixedtumours (or pleomorphic adenocarcinomas) formed 18%. Theremaining types of malignant salivary tumours are alsorepresented in the series.
The natural history and spread of these tumours arestudied in detail, with lymph-node metastasis occuring in 25% of thecases and distant metastasis in 20% . Malignant tumoursinvolve largely in the retromandibular portion of the parotidgland in over 40% of the cases and the preauricular portion inabout one fifth of the cases. Bmth regions are affected in afurther fifth of the cases.
83
A combination of surgery and radiotherapy was the methodemployed for curative therapy with radiotherapy alone reservedmainly for palliation. While the overall five-year survival was42% late recurrences constitute a serious problem with eventualdemise of about half of these patients. Various factorsaffecting the prognosis, including histological type of tumour,method of treatment and response to radiotherapy~e discussed.
* Director, Radiation Therapy Dep't, The Methodist Hospital,506 6th St. Brooklyn, N.Y. 11215
88 ___
CARCINOMA OF THE MAXILLARY SINUS
A Study of 91 Cases with Emphasis on the CombinedTherapy of Radical Surgery Followed by Irradiation
Tah Yee Chen, M.D.
Department of Radiation MedicineRoswell Park Memorial Institute
Buffalo, New York
Ninety-one cases of carcinoma of the maxillary sinus treated at theRoswell Park Memorial Institute from 1950 to 1970 were analyzed. Ninetyone per cent of the cases had advanced disease and were classified ashaving T3 or T4 lesion according to the staging system proposed bySisson et al. Ten per cent of the patients had cervical metastasesand five per cent had distant metastases. Second primary occurred infour per cent of the patients. The treatment methods consisted ofeither radical surgery (14 patients), irradiation (28 patients) or combinedradical surgery and irradiation (49 patients). For the combined treatment,pre-operative irradiation was used in all but 2 patients. The overallfive year survival rates (determinate cases) were ten per cent forradical surgery alone, twenty-three per cent for irradiation alone andthirty-four per cent for combined radical surgery and irradiation.Generally, the patients tolerated the treatment reasonably well includingthose treated with the combined method. The study suggested that thecombined procedure of radical surgery and irradiation is feasible andis the treatment of choice for the advanced cases of carcinoma of themaxillary sinus. Pre-operati"ve versus post-operative irradiation willbe discussed.
84
89 ___
TREATMENT OF CANCER OF THE BASE OF TONGUE
Carlos V. Rozenbom, M.D., Stanley Thawley, M.D., John Rollo, M.D.Alvin Korba, M.D., Donald Ragan, Ph.D., Joseph Ogura, M.D.
Carlos A. Perez, M.D. and William E. Powers, M.D.Division of Radiation Oncology, Mallinckrodt Institute of Radiology
St. Louis, Missouri
Between 1960 and 1974, 111 primarily treated patients with carcinomaof the base of tongue were seen at the Mallinckrodt Institute of Radiology.
The therapeutic intent was curative in 105 patients. Of these, 73were treated with preoperative radiation therapy to 3000 or 5000 radsmidplane dose. Radical radiation therapy with doses in excess of 6000rads was delivered to 36 patients. Three patients were treated postoperatively.
The five year actuarial survival rate for the 111 patients was 39%.The five year actuarial survival rate for patients treated with combinedradiation and surgery was 44%.
The recurrences at the primary site and each neck will be analyzedand correlated with method of treatment and doses of irradiation.
The preoperative surgical specimens will be evaluated and a correlationof pathological findings and control of tumor and survival will be made.
90 ___
AN ANALYSIS OF DISTANT METASTASIS FROM SQUAMOUS CELLCARCINOMA OF THE UPPER RESPIRATORY AND DIGESTIVE TRACT
Orlando Merino. M.D •• Robert D. Lindberg. M.D .• Gilbert H. Fletcher. M.D.
M. D. Anderson Hospital. Department of Radiotherapy. Houston. Texas
The charts of 5.168 previously untreated patients with squamous cellcarcinoma of the upper respiratory and digestive tract treated for cure
from January 1948 through August 1973 were reviewed. These patients hadno evidence of distant metastasis when initially treated. Five hundredand fifty-five patients developed clinical evidence of distant metastasis.
The incidence of distant metastasis will be presented according to:1) the anatomical site of the primary tumor. 2) the treatment of the primarytumor and. 3) the T and Nstage of the primary tumor. The time and locationof the first clinical evidence of distant metastasis will also be presented.
85

91_
EPSTEIN-BARR vmus (EBV) ANTIBODY IN PATIENTS TREATED BYRADICAL RADIOTHERAPY FOR A HEAD AND NECK CANCER.Marlene R. Hali1i, M.D. (Fellow, A.C.S.),* Ilya Splgland, M.D.**,Nan Foster, R.N.*, Nemetallah A, Ghossein, M.D.** Department of Radiology, section of Radiotherapy, Albert Einstein Collegeof Medicine , Bronx, N. Y.** Department of Pathology, Division of Virology, Montefiore Hospital Medical Ctr,Bronx, New York and Albert Einstein College of Medicine, Bronx, N. Y.
Elevation of antibody titer against Epstein-Barr Virus (EBV) caps ids (VCA) has beendocumented in patients with African Burkitt's lymphoma and with nasopharyngealcancer. It has also been demonstrated that drop in antibody titer occurs followingsuccessful radiotherapy treatment of nasopharyngeal tumors (followup periodbetween two to six years). We cause for the elevated titers in these tumors isnot clear. It has been suggested that there is a causal relation between theexistence of the viral genome and malignancy. Another hypothesis is that theviral genome which is normally present is reactivated in patients with malignanciesbecause of depressed cell mediated immunity. Determination of antibody titersagainst EBV in head and neck malignancies, other than nasopharyngeal cancer,and the effect of treatment on these titers has not been studied. Twenty-sevenpatients who received radical radiotherapy for head and neck cancers had antibodytiters measured before and at completion of treatment. All patients had asquamous cell carcinoma of the head and neck except for five patients, one had aWegener granuloma, two patients had malignant lymphoma, one patient hadglomus j.ugulare and one had an anaplastic mixed tumor of the salivary gland.Tumors were arbitrarily classsified as early (TI-2 NO Nl) or locally advanced(T3-4 N2 N3). There were eight patients with early disease and nineteen patientswith advanced cancer. Titers less than 1:20 were considered low. Titers 1:20 andabove were considered elevated. Seventeen of the 27 patients (63%) had a low titerand 10 of 27 (37% ) had a high titer. Only one of 8 (13%) of the early cases had a hightiter but 10 of 19 (53%) of advanced cases had an elevated titer. Immediately followingradiotherapy the titer was not significantly altered, compared to the pre-treatment levels.Seventeen patients were skin tested with DNCB. There is no significant correlation,as yet, between positive skin reactivity and EBV antibody. These preliminary resultsindicate that antibodies against EBV are present in a significant number of head andneck cancers other than nasopharyngeal. These titers are higher in advanced disease.Immediately followlng radiotherapy, there is no significant alteration in antlbody jdters,Correlation between cell mediated immunity, antibody level and short term prognosisis being determined. Our data does not clarify as yet the causal relationship betweencellular immunity, EBV reactivity and malignancy.
Wis investigation was supported in part by Grant # CA 13806, awarded by theNational Cancer Institute, DREW.
86
92 ___
CARCINOMA OF THE PINNA
Jose Avila, M.D., Department of Radiation MedicineUniversity of Kentucky
Antonio Bosch, M.D., Department of RadiologyUniversity of Wisconsin
Silvio Aristizabal, M.D., Division of Radiation OncologyUniversity of Arizona
Zenaida Frias, M.P.H. and Victor Marcial, M.D.Puerto Rico Nuclear Center
Over the years the concept that the proximity of a tumor tocartilaginous structures constitutes a contraindication to roentgentherapy has pervaded the literature. Carcinoma of the pinna is agood example of this clinical situation. Several authors claim thatirradiation can be used successfully in contrast to others who feelexcision should be the perferred treatment.
The records on 95 consecutive patients with carcinoma of thepinna were reviewed. Fifty-six of the tumors were basal cell andthirty-nine squamous cell carcinoma. Fifty patients were surgicallytreated and forty-five irradiated. Small and/or peripheral lesionswere excised and the large and/or centrally located referred forirradiation. Analysis of the results shows that the difference intumor control rate is not statistically significant, and the complication rate is also comparable with both modalities. Althoughchondritis is most commonly seen after irradiation, it can also occurafter excision.
In our opinion neither modality should be used with totalexclusion of the other. Initial resection would seem preferable insmall lesions in which primary closure is possible and in extensivelesions where a good cosmetic result is precluded by the destructionof normal tissue. Roentgentherapy would seem of value in those lesionsin which resection would result in objectionable cosmetic defect.
87
93 ___
RADIATION INDUCED CRANIAL NERVE PALSY
Paul S. Berger, M.D., (Department of Radiology).Albert Einstein College of Medicine, Bronx. NewYork. and J. P. Bataini, M.D .• (Department ofRadiotherapy, Foundation Curie. Paris. France)
Twenty-five patients with 35 cranial nerve palsies were seen atthe Foundation Curie during follow up after r-adica1 radiotherapy forhead and neck tumors. The twelfth nerve was involved in 19 cases, thetenth in 9. and the eleventh in 5; the fifth and second nerves wereinvolved once each and in the same patient. The twelfth nerve wasinvolved alone in 16 patients and the tenth nerve alone in 3, withmultiple nerves involved in the remaining 6 patients. The palsy wasnoted from 12 to 145 months after diagnosis of the tumor. The latencyperiod could be correlated with dose so that the least square fitequation representing NSD versus delay is NSD = 2598-De1ay (in months)x 4.6. with a correlation coefficient of -0.58. The distinction betweentumor recurrence and radiation induced nerve palsy is critical. It canoften be inferred from the latency period but must be confirmed byobservation over a period of time.
94 ___
THE SIGNIFICANCE OF NEEDLE BIOPSY AFTER IRRADIATION
FOR STAGE C ADENOCARCINOMA OF THE PROSTATE
James D. Cox, M.D ., and Thomas J. Stoffe1,M.D.The Medical College of Wisconsin, Milwaukee, Wisconsin
The presence or absence of adenocarcinoma in biopsies followingirradiation has been used to criticize or defend this treatment. AtWalter Reed Medical Center, 38 consecutive patients with Stage Cadenocarcinoma underwent definitive irradiation between August 1970and March 1973. The median dose to the pelvis was 7000 rad in 31fractions in 43 days (2030 ret). Their post treatment examinationsincluded palpation of the prostate and transperinea1 biopsy of themost suspicious area. Gradual disappearance of the palpable tumoroccurred in all patients. Two men have had palpable re-growth ofprostatic cancer. Thirty-three patients have had 1 to 7 biopsieseach for a total of 135, an average of 4 per patient. There were48 positive and 87 negative biopsies. Positive biopsy rate correlatedonly with the interval after irradiation -- 60%at 6 months, 37%atone year, 30%at 18 months, and approximately 20%after two years.There was no correlation with pre-irradiation estrogen or orchiectomy,with time-dose-fractionation relationships. or with prognosis. Thesebiopsies provide interesting data about the regression rate ofprostatic adenocarcinoma. but they have no significance for theindividual patient. They have. therefore, been eliminated from followup studies.
95_
MEGAVOLTAGE RADIATION THERAPY FOR CARCINOMAOF THE PROSTATE
By
Wm. J. Neglia, M.D. and David H. Hussey, M.D.Department of Radiotherapy
M. D. Anderson Hospital and Tumor InstituteHouston, Texas 77030
Between July 1966 and December 1972, 154 patients with Stage Ccancer of the prostate were treated with megavo1tage radiationtherapy at The University of Texas System Cancer Center, M. D. Anderson Hospital and Tumor Institute. The objectives of the studywere: 1) to determine the effectiveness of adjunctive hormonalmanipulation, 2) to corre1~te dose levels with control of thedisease within the pelvis, and 3) to correlate field size withcontrol of the cancer in the regional lymphatics.
The majority of patients were treated with 22 MV x-rays througha four-field portal arrangement using 10x10 cm anterior and posteriorportals and 10x8 cm lateral portals. No attempt was made to coverthe common iliac or periaortic lymph nodes with extended fields.The tumor dose ranged from 6000 rads in 6 weeks to 7000 rads in7 weeks.
Of the total population treated with radiation therapy, 86.4 %(133/154) of the patients had local control of their disease, 68 .2 %.(105/154) were alive and 58.4 % (90/154) were alive with no evidenceof disease (mean follow-up time = 4 years, 7 months). The majorityof treatment failures were due to hematogenous metastases.
There was no improvement in the local control or survival rateswith adjunctive hormonal therapy. Fifty-six of 76 patients (73.6 %)treated with radiation therapy alone were alive at the time ofanalysis as compared to 45 of 74 patients (60.8 %) treated withradiation therapy plus hormones.
To evaluate dose relationships, the material was divided into:1) patients receiving 6500 ± 250 rads, and 2) those receiving7000 ± 250 rads. Although there was no difference in the localcontrol and survival rates between the two groups, there was asignificantly greater incidence of major complications with higherdoses. Only one of 44 patients (2.3 %) treated with 6500 radsdeveloped major complications as compared to 11 of 110 patients(10 %) treated with doses of 7000 rads.
Because lymphadenectomy studies indicate that the incidenceof pelvic node metastases in Stage C prostatic carcinoma rangesfrom 38 to 55%, the data were analyzed to show whether recurrenceswere developing at the regional level. A significant failure ratein the regional nodes was not observed, since only three of 154patients (1.9 %) were scored as having failure at the regionallevel with central control.
89
96 ___
BEHAVIORAL PATTERNS OF PROSTATIC .ADENOCARCINOMAFOLLOWING IODINE-125 IMPLANTATION AND PELVIC NODE DISSECTION
Basil S. Hi1aris, M.D., Willet Whitmore, M.D., Mostafa A. Batata, M.D.and Winston E. Barzel1, M.D.
Department of Radiation Therapy, Memorial Sloan-Kettering Cancer CenterNew York, New York
This study is based on 200 patients with adenocarcinoma of theprostate, who were treated between February 1970 and May 1976 with acombined technique of retropubic bilateral pelvic lymphadenectomy andinterstitial implantation of the prostate with Iodine-125 sources. Thepatients were analyzed for clinico-pathological behavioral patternsaccording to age, tumor extent, size, location, and grade. Thesevariables were also correlated with mode of initial nodal involvement,subsequent recurrence, and corresponding survival patterns. Allpatients were classified according to the A.J.C. (American Joint Committee)and the UICC (International Union Against Cancer) clinical staging. Therelative value of each sta~ing system in the management and prognosis ofprostatic cancer will be discussed.
97 ___
RADIATION THERAPY TECHNIQUES IN THE TREATMENT OFPROSTATIC CARCINOMA: EVALUATION OF CHRONIC
SIDE EFFECTS AND AN IMPROVED METHOD FORTREATMENT
Thomas A. Roland, M.D., Richard C. Brown, M.D., and Henry P. Plenk, M.D.L.D.S. Radiation Center - Salt Lake City, Utah
Numerous radiotherapy techniques have been employed during the pastten years in an attempt to cure localized prostatic carcinoma. Four mostcommonly used techniques are analyzed and the morbidity associated witheach is compared. Chi-square and independent variable analysis areutilized for statistical comparisons among the treatment groups. Adetailed outline of degree of side effects, as well as pictorialrepresentation of treatment techniques, are given.
Eighty-six patients treated between 1965 and 1975 are evaluated interms of chronic bowel and bladder symptoms and symptomatic subcutaneousfibrosis. Major radiation sequelae were noted in particular patients,while others treated during the same period were essentially free fromany chronic side effects. Changes in morbidity with alterations in dosefractionation, volume and field distributions are outlined .
Techniques analyzed include: a three-field design with anterior andtwo posterior obliques; shaped anterior and posterior pelvic fieldswith prostate boost treated with two separate fractionation schemes; afour-field technique utilizing lateral prostate boosts.
90
Reduction in complications obtained with use of the recently employedfour-field technique is shown to be significant. The boost techniqueemployed and time-dose fractionation schemes appear the most significantfactors in overall morbidity. A longer follow up period for the presentlyused technique is needed for final analysis.
98 ___
RADIATION-RELATED TOXICITIES IN NATIONAL WILMS' TUMOR STUDY #1
Melvin Tefft, M. D. for the National Wilms' Tumor Study Committee
Three hundred fifty-nine patients have been randomized intothe National Wilms' Tumor Study No.1; 276 received radiationtherapy (RT). Patients with evidence of pneumonitis, carditis,hepatitis and nephritis were evaluated, to define the incidenceof such occurrences in irradiated children and the possible.relation to the combined chemo- and radiotherapy. The antineoplasticagents used were Actinomycin-D (AMD), Vincristine (VCR) or both.
Ten patients died as a consequence of therapy. Three of the10 had pulmonary metastases at diagnosis, and 5 had previouslyrelapsed in one or more sites. Of the 10, one patient given VCRand flank RT died of sepsis 19 days after surgery. The relationof RT to this complication is indefinite. Another child, giventotal abdominal RT and AMD succumbed to abdominal infection andjaundice in 74 days.
Five deaths were from pneumonitis, pneumonia or ~neumocystis
following radiation to the chest, one was from cardiac toxicityrelated to Adriamycin and possibly to RT, another was related toActinomycin-D combined with RT, and the last involved radiationnephritis in a patient who relapsed in the contralateral kidney.Of the 10 deaths, therefore, 7 can be ascribed to RT complications,aggravated by concomitant chemotherapy in patients with metastaticdisease or relapse after primary care.
A scan of patient records for significant lung and livertoxicity turned up 16 cases of radiation hepatitis, all in patientswho were also receiving Actinomycin-D, 10 in children receivingwide field RT. There was a near fatal case of pneumonitis ina patient given pulmonary RT and several others had pneumoniaand/or abnormal markings in chest films secondary to lung irradiation.
Supported by: Grant No. R01-CA-11722
91
99_
VARIOUS RADIATION REGIMENS AND CYSTECTOMYVERSUS CYSTECTOMY ALONE IN BLADDER CANCER
W.F. Whitmore, Jr., M.D., M.A. Batata, M.D.,B.S. Hilaris, M.D., A. Unal, M.D., and M. Ghoneim, M.D.
Department of Radiation Therapy, Memorial Sloan-Kettering Cancer CenterNew York, New York
Between 1948 and 1970, 420 patients with bladder cancer were treatedat Memorial Sloan-Kettering Cancer Center. Radical cystectomy was carried?ut w~th?ut prior irradiatio~ i~ 130 patients, and subsequent to megavoltagelrradlatlon to the true pelvls ln 290 patients. Subsequent radical cystectomywas done because of tumor recurrence or urinary complications within a yearor more after delivering 6000 rads in seven wee ks in 85 patients; and as aplanned procedure either within two months following 4000 rads in fourweeks in 119 patients, or within one week after 2000 rads in one week in86 patients. The patterns of survival, recurrence and complications inthe cystectomy alone group versus the three radiation groups will bediscussed.
100_
THE EFFECTIVE RADIATION DOSE FOR LOCALCONTROL OF ADVANCED BREAST CANCER
Henry M. Keys, M.D, Philip Rubin, M.D.Division of Radiation Oncology, University of Rochester
Cancer Center, Rochester, New York
A series of 50 patients with locally advanced breast carcinoma managedby radiation only as the primary form of treatment has been studied.Analysis of our patients and review of the literature demonstrates thatradiation can be effective in obtaining local control of the cancer in75-80%when tumor doses of 7000 rad or more are delivered. By contrast,doses below 7000 rad resulted in local ablation of disease in less than40%of patients so treated. As survival is determined by metastaticdisease, the combination of effective local treatment and "elective"adjuvant multi-agent chemotherapy may hold promise for improving the poorsurvival seen in this group of patients. The need for the reduction ofthe radiation dose locally when combined with chemotherapy will bediscussed.
This report will detail the treatment techniques used, includinginterstitial Iridium 192 implants in a number of patients, the patternsof failure and recommendations for future study in this advanced stageof breast cancer.
92
101_
THE MANAGEMENT OF INFLAMMATORY BREAST CARCINOMA
A. R. Kagan, M.D., H. Nussbaum, M.D., H. Gilbert, M.D.,and P. Chan, M.D.
Southern California Permanente Medical Group, Los Anqeles,California
A review of 54 patients with inflammatory breast carcinoma willbe presented. Emphasis will be placed on the clinical diagnosis, suchas findings of redness of the skin involving more than one third of the~reast, enlargement and generalized induration of the breast, withaxillary metastases. The finding of subdermal lymphatic invasion onskin biopsy will be evaluated.
Inflammatory breast carcinoma is a systemic disease from onset,and patients develop clinical evidence of disseminated disease withinone year, and die within two years . In our review of 54 patients, 52are dead. The remaining two are alive with disease for 5 years atpresent.
All treatment, from the standpoint of cure, is ineffective and onlytemporarily suppressive. Mastectomy is contraindicated. With radiotherapy, and a dose of 7000 rads, it is common to see tumor extensionoutside the irradiation fields even with wide fields.
The goal of treatment should be palliative, and the plan of treatmentsequential. The most effective initial treatment is multiple chemotherapy.Hormonal ablation procedures may yield good palliation and should be usedafter chemotherapy failure. Radiation therapy is effective local treatmentfor palliation of the primary lesion or metastatic disease. The naturalhistory of the disease is as yet only slightly affected by presenttreatment methods.
93
102_
DOSIMETRY FINDINGS FROM CLINICAL RADIOTHERAPY TRIALSWITH RECOMMENDATIONS FOR QUALITY ASSURANCE
R. J. Shalek, Ph.D., P. Kennedy, B.A., M. Stovall, B.S.,J. H. Cundiff, B.S., W. F. Gagnon, Ph.D., W. Grant III,Ph.D., and W. F. Hanson, Ph.D.
The University of Texas System Cancer Center, M. D.Anderson Hospital and Tumor Institute, Physics DepartmentHouston, Texas.
Recommendations regarding quality control in physics relating toradiation therapy are derived from experience with the Radiological PhysicsCenter which is a national review program, and the Texas Regional MedicalPhysicists, which is a regional consultation activity. Three recommendationson quality control, supported by the data and findings reported in thispaper are:
1. One person should review and take responsibility for all steps fromradiation measurement to fulfillment of dose prescription.
2. Routine review of the accumulating radiation absorbed dose topatients under treatment can reduce random errors.
3. Review of dosimetry systems by outside individuals is important.These reviews may be informal.
This work was supported in part by Grant No. CA 10953 from the NationalCancer Institute.
103_
1251 SEED(l) DOSIMETRY BY Si(Li) SCINTILLATION COUNTING:
EVIDENCE FOR UNUSUAL DOSE INHOMOGENEITY IN TUMOR IMPLANTS
Ching Clifton Ling, Ph.D. and William U. Shipley, M.D., Departmentof Radiation Medicine, Massachusetts General Hospital, HarvardMedical School, Boston, Massachusetts 02114
1251 seeds(l) are being used with increasing frequency and enthusiasmin interstitial implants of several types of solid tumors. Due to the lowenergy of the characteristic radiation emitted and the source encapsulationdesign, the isodose distribution around the 1251 seed is not expected to beisotropic, although until now isotropy has been assumed in all dosimetriccalibration and calculations for lack of quantitative data on theseriousness of the anisotropy. A new approach employing an Si(Li) solid
94
state detector, which distinctly resolves the 27.5 keV, 31.4 keV and 35.5keV photons of 1251, has been used to measure the photon fluence distributionas a function of angle around the seed. The photon angular distributionobtained shows significant anisotropy such that the fluence at the end ofthe seed is approximately 15%of that at the middle. Composite isodosecurves of idealized planar patterns of seed arrangement of 1 cm separationindicate that regions between the ends of seeds receive only a 60%dosecompared to that delivered to areas between the middle of seeds. Further,neither random nor systematic angling of seeds is effective in correctingthe dose non-uniformity. This implies either that cold spots exist inimplants, or that a portion of the implanted volume is brought to anunnecessarily high dose. Although seed movement within the implant dueto tissue shrinkage may partly alleviate the inhomogeneity, the extentof it is uncertain. Seed encapsulation redesign to achieve a morehomogeneous dose distribution may be warranted in view of these findings.
(l)From Lawrence Soft Ray, Inc., Mountain View, California.
104_
AN EXAMINATION OF CONSISTENCIES BETWEENCOMPUTERIZED RADIUM DOSIMETRY SYSTEMS
Donald D. Tolbert, Ph.D.
Radiotherapy Physics Section of the WisconsinClinical Cancer Center, Madison, Wisconsin
Test cases relevant to radium interstitial/intracavitary dosimetrywere mailed to representatives of (known) commercial vendors of computerizedradiotherapy treatment planning systems. These test cases includecalculations for individual needles and radium source configurationsappropriate to radiation treatment of the female pelvis. Calculations forthese test cases have also been done with computer programs used byMallinckrodt Institute of Radiology (St. Louis, Mo), M.D. Anderson Hospital(Houston, TX), Memorial Hospital (New York, NY), and Ontario CancerInstitute (Ontario, Canada) . The purpose of this effort is to examine theconsistencies in the prediction of dose (rate) values pertinent to radiumdosimetry and compare these predictions to experimental measurements wherepossible. A presentation of results from this study will be made.
95
105_
Possible Dose Error from Variation in Electron Beam CollimatorSetting--Clinac 18 Linear Accelerator
By Ann E. Wright, Ph.D.; Laurence Thomson, M.S.;Marvin H. Olson, M.D.; and Pranab Ray, M.D.
The University of Texas Medical Branch, Galveston, Texas
The Varian Corporation Clinac-18 linear accelerator produces fivedifferent electron beam energies ranging from 6 MeV to 18 MeV.Six applicators are provided which define square fields at theisocenter 4, 6, 8, 10, 15, or 25 cm on the side. Complete collimation of the electron beam is accomplished by a system which includesthe fixed primary collimator, the variable collimators, an adaptor,and one applicator. When an applicator is used, it is necessaryto manually set the variable collimators; the manufacturer recommends an opening 5 cm greater than the applicator size. To assessthe possible error in dose to the patient from failure to properlyset the collimators, measurements were made in a phantom using the10xlO sq. cm applicator and varying the collimator openings from10xlO sq. cm to 35x35 sq. cm. The variation in output was significant, and differed for different energies. For 6 MeV electrons,the possible error in dose ranged from -25% to +15%. For 15 MeVelectrons, the error ranged from -10% to +3%.
The collimator setting also had a significant effect on the isodosedistribution. For 9 MeV electrons, a collimator opening of 10xlOsq. cm decreased the dose near the outer edges of the field,contracting the 80% isodose line by 6 mm. Opening the collimatorsto 20x20 sq. cm increased the dose laterally, expanding the 80%isodose line. The depth of maximum dose was shifted upward from2.0 cm to 1.5 cm, and the 100% isodose line was considerably wider.The surface dose was increased by about 5%.
The foregoing data indicate the importance of proper care in adjustingthe variable collimator opening when using the Clinac-18 electronbeam applicators.
106_
THE DEVELOPMENT OF A SYSTEM TO AUTOMATE THE RADIOTHERAPY RECORD
Douglas Jones, B.Sc.Richard Seymour B.Sc.John Washington M.S.
Northwest Medical Physics CenterUniv. of Wash., RC-08, Seattle, Washington 98195
The Northwest Medical Physics Center provides physics support to 29 institutionsin Washington, Oregon, Alaska and Montana at which some 8,000 patients aretreated by radiotherapy annually. The system described here is intended
96
primarily to obviate the need for independently checking radiotherapy chartsfor errors in dose computation, a task that has been difficult to accomplishwith the large patient load described.
The remarkable reduction in the cost of minicomputers in recent years allowsthe possibility for each therapy machine to be coupled to a minicomputer. ADigital Equipment Corporation Classic System is used which contains a PDP-8Acomputer, dual floppy disc drives, CRT display with hard copy output andkeyboard. A digital clock controller has been developed to supplement theelectromechanical timer employed on Cobalt-60 machines. The software developedhas many components which are summarized below.
Schedule: To schedule patients on the therapy machine.Calculate: Output and depth dose data are stored to enable the calcula~ion
of the machine setting required in simple field.Plan: At the beginning of treatment the complete course is planned in
detai l.Treat: With information in the planned treatment, the computer will monitor
the machine setting employed and prompt the technician in the eventof errors.
Monitor: The patients progress is monitored by the therapy technician andflags set automatically in the event of adverse reactions.
Analysis: The body of data stored in the computer allows for analysis ofmany variables. The feasibility of linking the minicomputers ina network to a larger computer to produce a region wide patientsystem is currently under review.
107_
RADIATION THERAPY IN COMBINATION WITH LOCAL
HYPERTHERMIA: PRELIMINARY RESULTS
Jae Ho Kim, M.D., Ph.D., Eric W. Hahn, Ph.D.,N. Tokita, M.D., and Lourdes Z. Nisce, M.D.Memorial Sloan-Kettering Cancer Center, NewYork, New York.
Radiobiological studies by us and others have shown that hyperthermiaselectively enhances the response of tumor cells in vivo and in vitro.One of the aims of this report is to evaluate the response of normal tissuesincluding skin in patients with various cutaneous malignant lesions.Twenty-four patients with multiple malignant cutaneous lesions, (mycosisfungoides, lymphoma cutis and Kaposi's sarcoma) have been studied. Theyhave been treated with radiation alone and radiation immediately followedby hyperthermia. Varying degrees of hyperthermia were achieved byimmersing the extremities into the temperature regulated water bath.Various dose fractionation regimens in combination with hyperthermia havebeen investigated. Rates of tumor regression, maximum improvementobtained, disease-free interval and normal tissue reactions have beenused as means of assessment. The normal tissue effects with radiationand hyperthermia following either single or fractionated course ofcombined treatment do not appear to be greater than those treated with
97
radiation alone• . :h~ follow up period varies from one month to 15 months.In genera~, the ~nl~lal tumor regression rates were faster in patientstreated wlth radlatlon plus hyperthermia than in radiation aloneparticularly in patients with Kaposi's sarcoma. Details of the ;elationshipbetwe~n temperatura an~ durati on of hyperthermi a on the normal ti ssuereactlons as well as dlsease-free interval will be presented.
108_
THE EFFECT OF POST-RADIATION HYPERTHERMIAON HUMAN SKIN AND TUMOR RESPONSE
Richard Johnson, M.B., B.S., D.M.R.T., K. S. Dosi, M.D.,D.M.R.T., D.M.R.E., S. Y. Song, M.D., T. S. Sandhu, Ph.D.,D. Boyl e.
Roswell Park Memorial Institute, Buffalo, New York.
In vitro laboratory data from Elkind and Joshi demonstrated thathyperthermia (4l-420C) for 2 hours post radiation caused a significantincrease in radiation damage. Prior hyperthermia did not alter theradiation response.
Ten melanoma patients with multiple superficial metastases have beentreated with orthovoltage x-rays using 3-6 fractions in 2-3 weeks.Regional heat was applied immediately after radiation for 2 hours at4l-420C using a 2450 megahertz microwave generator.
Multiple control lesions were treated with identical field size andfractionation but varying total doses.
Surface thermistors and intra-tumor 30 gauge needle thermocouples wereused for thermometry together with a liquid crystal fibro optic unitsupplied by the Office of Naval Research to monitor operating surfacetemperature.
The skin responses were scored and the tumor responses recorded for40 separate tumors.
No skin reaction occurred in the heat alone areas exposed to 4l-42oCto a depth of 1 em. The skin radiation reaction was significantlyincreased in the heated lesions . Data on the tumor response and therapeuticratios will be presented.
98
******
109_
COMBINATION RADIATION THERAPY AND LOCALIZED CURRENT FIELD HYPERTHERMIAOF SPONTANEOUS MALIGNANT NEOPLASMS OF ANIMALS. A PRECLINICAL STUDY.Phillip W. Day, D.V.M.*; Charles J. Sternhagen, M.D., A.S.T.R.**;James D. Doss, M.S.E.E.***; Sterling Edwards, M.D.*
University of New Mexico, School of MedicineUniversity of New Mexico, Cancer Research and Treatment CenterLos Alamos Scientific Laboratory
One cat and 2 dogs, with spontaneous malignant neoplasms weretreated by combination radiaition therapy and localized current field(LCF) hyperthermia (Doss &McCabe, MED. INSTRUM., 10:16-21, 1976).
The three animals were treated by a non-invasive LCF technique.The neoplastic area was covered by a copper pad surface electrode. Thesecond, large electrode was placed on the bottom of a saline water bathwith a electrical resistivity of 500 ohms·centimeter. The animal wasthen placed in the saline water bath until 25%of its surface was immersedwith no direct contact of the second electrode.
Dog #57 had a fibrosarcoma located on the right antero-lateralnasopharynx. The tumor and surrounding area received 5 LCF treatmentsat 430C for 30 minutes and 750 rads within 10 minutes of terminatinghyperthermia. The animal shows no evidence of disease 3 months posttrea tment.
Cat #62 had a squamous cell carcinoma of long standing located inthe medial canthus of the right eye. The tumor area received 4 LCFtreatments at 43°C and 700 rads within 10 minutes of terminating hyperthermia. The tumor exhibited regression for 12 weeks with granulationtype healing in the treatment area.
Dog #63 had a fibrosarcoma located in the left postero-lateral hardpalate involving the left molar teeth . The tumor area and surroundingtissues received 4 LCF treatments at 43°C for 30 minutes and 750 radswithin 10 minutes of the terminating hyperthermia. The tumor areaexhibited continuing regression for 8 weeks when the owner euthanizedthe animal.
Previous to the combination hyperthermia and radiation study, 14animals with spontaneous neoplasms were treated with LCF alone. Thirtythree per cent of the cases have no recurrence of disease for 1 to 3years following treatment. Forty-five per cent of the tumors showedregression with the animal returning to normal function.
Research supported by USPH Grant No. HEW 1 ROI CA15833A
99
110_
THE DEVELOPMENT OF HYPERTHERMIAMICROWAVE GENERATORS AND THERMOMETRY
T.S. Sandhu, Ph.D., H. Kowal, B.S., R.J. Johnson, M.B., B.S.
Roswell Park Memorial Institute, Buffalo, New York 14263
Phase I hyperthermia studies require the development ofregional hyperthermia and thermometry in order to study the normaltissue and tumor response of superficial human tumors.
Initial animal and clinical studies were performed with a2450 MHz microwave source using the intermediate field of a cornerreflector type C applicator and foil collimation for localization.Thermometry showed that the tumor at 1 em depth could be heated to41-42oC with an exposed skin temperature of 4l-42oC.
A 915 MHz microwave generator which theoretically will almosttriple the energy penetration has been designed and built usinga direct contact applicator separated from the skin by liquiddielectric in a bag. The liquid dielectric is circulated througha heat transfer unit to keep the skin at constant temperature.The steady flow rate and the temperature of incoming and outgoingliquid through the bag are recorded to measure the energy lost tothe liquid.
Thermometry has been developed using intra-tumor 30 gaugethermocouples, surface thermistors and surface liquid crystalfibro optic units. The latter can be used to monitor the operatingtemperature and regulate the microwave output.
Isotherms have been determined in phantoms and in pigs usingthe 915 MHz generator.
100
******
111_
PRELIMINARY RESULTS USING LOCALIZED CURRENT FIELD HYPERTHERMIA IN ORALCAVITY CARCINOMAS
Charles J. Sternhagen, M.D.*; James D. Doss, M.S.E.E.**;Phillip W. Day, D.V.M.*; W. Sterling Edwards, M.D.*;Raymond C. Doberneck, M.D.*; Fred S. Herzon, M.D.*;Terry D. Powell, M.D.*; Gregory F. O'Brien, M.D.***.
Cancer Research and Treatment Center - University of New Mexico,Albuquerque, New MexicoLos Alamos Scientific Laboratories, Los Alamos, New MexicoLovelace-Bataan Medical Center, Albuquerque, New Mexico
After preclinical testing a clinical trial was instituted usinglocalized current field (LCF) hyperthermia (Doss &McCabe, MED. INSTRUM.,10:16-21, 1976) to treat accessible malignancies uncontrolled by conventional methods. Three previously irradiated patients have beentreated using both noninvasive and invasive techniques. Radiofrequencycurrent (500 kHz) was used in four treatments. Thermistors strateqicallyplaced within the tumor treatment volumes controlled and monitored thetemperature.
Two patients presented with far-advanced persistent squamous cellcarcinollla of the base of tongue. Each received a single non-invasiveLCF treatment with electrode plates. Prior to hyperthermia the firstpatient had massive obstructing local disease with widespread metastases.This patient became ambulatory with tumor shrinkage, good pain palliation,and improvement in airway. She expired after a cardiopulmonary arreston the sixth post-hyperthermia day. The second patient, debilitatedwith advanced local disease prior to LCF, obtained excellent temporarytumor regression and pain palliation. The tumor decreased initially,stabilized for four weeks, and then increased in size. Methotrexate, 20mg I.V., was started and given weekly. Pain, inanition and tumor growthincreased. At 11 weeks the methotrexate was stopped. The patient expiredwith progressive disease 15 weeks post-hyperthermia.
The third patient, a debilitated alcoholic, presented with a rapidlyregrowing 3 cm mass in the floor of the mouth, the second local recurrence.Two courses of hyperthermia were given. Tumor regression occurred onlyafter the second course at a higher temperature (440C). Pain diminishedrapidly the first week. The patient gained 19 pounds, and is currentlyalive and well over four months post-hyperthermia.
Complications from these four treatments ranged from mild erythemaand mucositis, which cleared in one week, to vesicle formation, chronicmucositis, and ulceration in the tumor bed. Complications were relatedto temperature and duration of treatments.
This work was supported in part by Grant CA-16127 to Cancer Research andTreatment Center, University of New Mexico from National Cancer InstituteDivision of Research Resources and Centers, and National Institutes ofHealth 5401-CA-15833-02.
101
112_
SINGLE DOSE X-IRRADIATION AND CONCOMITANT HYPERTHERMIAON A RADIORESISTANT FIBROSARCOMA IN THE MOUSE
Eric W. Hahn, Ph.D., Alan A. Alfieri, B.S., Jae Ho Kim, M.D., Ph.D .
Memorial Sloan-Kettering Cancer Center, New York, New York
The objectives of this study were to examine the effects of local tumorhyperthermia (LTH) and concomitant x-irradiation (RAD) on a relativelyradioresistant mouse sarcoma, to compare its response to a radiosensitivetumor also used in our laboratory and to establish it as a model systemfor combined modality studies.
1.0 cm3 Meth-A fibrosarcomas grown in the thigh muscle of Balb/Cmale mice were exposed to single doses of RAD ranging from 1.0 to 3.6 kradalone or 0.6 to 2.25 krad in combination wtih LTH (water bath at 43.0 ±O.loC for 15 min) applied immediately after irradiation. T~mor measurementswere taken routinely at the initiation of and after treatment.
LTH significantly enhanced the action of radiation as measured by tumorvolume analysis, mean survival time and cures. The ratio of radiation dosesvs. RAD + LTH required to produce an equivalent response ranged from 1.5to 1.7 depending upon the endpoint used and is consistent with previouslyreported values from our laboratory with single dose studies on the radiosensitive Ridgway osteogenic sarcoma.
Supported in part by NCI Grant CA 17410.
113_
PRELIMINARY CLINICAL RESULTS OF 433 MEGAHERTZ MICROWAVE THERAPYAND RADIATION THERAPY ON PATIENTS WITH ADVANCED CANCER
Ned B. Hornback, M.D., Robert Shupe, Ph.D., Homayoon Shidnia, M.D .Beng Tek Joe, M.D., Edgardo M. Sayoc, M.D.
Department of Radiation Therapy, Indiana University School ofMedicine, 1100 West Michigan Street, Indianapolis, Indiana
Because of recent interest in the literature regarding the enhancingeffects of radiation therapy with hyperthermia, several patients withadvanced cancers who failed to respond to standard medical treatment withsurgery, radiation and/or chemotherapy were treated with hyperthermia and
102
low dose radiation therapy. Each daily dose of 100 to 200 rads tolocalized fields was preceded by 10 to 20 minutes of hyperthermia using a433 Megahertz RF generator . Total dose varied from 2000 to 5000 rads,depending upon response and condition of the oatient. Early treatmentresults confirmed the previously described synergism between thermal radiationand ionizing radiation as manifested by subjective and objective improvementsof patients. The patients tolerated the course of treatments withoutdifficulty. This study, as well as previously reported studies in theliterature, forms a basis of an ongoing randomized study using untreatedfar-advanced head and neck and gynecological patients.
114_
FURTHER EXPERIENCE WITH HALF BODY RADIOTHERAPY
Peter J. Fitzpatrick, M.B., B.S., F:R.C.P., F.R.C.R., Walter D.Rider, M.B., Ch.B., F.R.C.P., F.R.C.R., Cyril E. Danjoux, M.D.
Princess Margaret Hospital, 500 Sherbourne Street, Toronto, Ontario.
Since 1971,245 patients with advanced cancer were treated with 355half body radiation treatments: 99 patients received total body irradiationin two halves. Most patients 'had failed to respond to conventionaltreatment. Because of the success in achieving palliation severe clinical:adiological, physiological and pathological parameters have been measured'1n order to understand the technique and decide which patients it maybenefi t ,
115_
USE OF BODY SCAtlNER IN RADIOTHERAPY TREATMENT PLAriNING
J.E. Munzenrider, M.D., M. Pilep ich, M.D., J.B. Rene-Ferrero, M.D .,I Tchakarova, M.D .• B. Carter, M.D.; New En91and Medical Center Hospital, Boston, Massachusetts
Body section computer-assisted tomography has been employedin radiotherapy treatment planning since August, 1975, when an OhioNuclear Delta Scanner became available at Tufts-New England MedicalCenter. During the first 9 months of operation, a total of 170 bodyscans were performed, with 64 (38%) being done on patients with knownmalignancy.
103
In fifty patients the scans were available during treatmentplanning for radiotherapy. Treatment volume, as determined by usualmeans, including physical exam, operative notes, isotope scans, radiographic procedures (IVP, Barium enema, arteriography, etc.) and ultrasound techniques has been compared with the determined from the bodyscan.
Amethod for recording skin portal marks on the scan has beendeveloped. Techniques are also described for magnification of the scanto accurately portray patient countour in the treatment position. Useof these contours with the Artronix 12 treatment planning system hasallowed optimization of dose distribution in the volume of interest,and minimization of radiation dosage to normal structures to a degreenot possible with other methods.
116_
CALIFORNIUM-252 FOR INTERSTITIAL IMPLANTATIONA CLINICAL STUDY AT MEMORIAL ~OSPITAL
Alvaro Vallejo, M.D., Basil S. Hilaris, M.D.and Lowell L. Anderson, Ph.D.
Memorial Sloan-Kettering Cancer Center, New York, New York
The unusual potential of 252Cf as a neutron source and the recognized theoretical advantage of neutrons in cancer therapy have prompted investigations at MSKCC into the planning and execution of clinicaltrials and radiation dosimetry of 252CF as a treatment modality.
A Phase I clinical study, using 252Cf sources in temporary implants began in January 1974. The improved 252CF source design utilized in these implants is patterned after the 192Ir seeds containedin nylon ribbons and is adopted for afterloading. This source assemblyprovides greater flexibility, facilitates the loading and unloadingprocedure and reduces the radiation exposure to hospital personnel.
An attempt was made to deliver the same effective dose with 252Cfas that delivered with 192Ir imglants (6000 rads in 6 days); the corresponding six-day dose from 252CF radiation consists of a neutron doseof 840 rads and a beta-gamma dose of 740 rads, using RBE's of 6.4 and0.86 respectively. Today a total of 10 implants have been performedin previously untreated metastatic regional nodes from squamous cellcarcinoma. Local control has been obtained in 8 of the 10 patientsimplanted (80%). No unusual normal tissue effects have been observedup to 2 year~ after implantation. The only observed disadvantage ofthe use of 252Cf sources is due to the necessity of increased radiationprecautions required to protect the hospital personnel.
Supported in part by Grant #DT-7 of the American Cancer Society.
104
117_
MEDICAL LIABILITY IN THE PRACTICE OF THERAPEUTIC RADIOLOGY
Bernard Roswit, M.D., F.A.C.R., and Francis Bensel, LL.B.
37 Roxbury Drive, Yonkers, New York
. The frequen~y a~d th~ cost of claims and lawsuits for allegedmed1cal malpract1ce 1n th1S country are sky-rocketing, as well as thecha~ges for protection. The practice of therapeutic radiology, as in allmedlcalpractice, involves the risk of patient injury in return for rescuefrom a life-threatening disease.
The authors of this communication, a radiation oncologist and amalpractice attorney, believe that the best way to avoid a malpracticesuit is "never to deserve one". To this end they have joined forcesto offer gU~delines.in,effective prophylaxis against lawsuits charging1) unau~h~rlze~ radlat10n therapy, 2) negligence in the excercise ofgo?d cll~lcal Judgement and expert treatment technology, 3) failure toga1n an lnformed consent, which must include a review of possibleradiation complication, as well as alternatives to radiation treatment.4) breach of warrant, involving a promise or guarantee of a given result,and 5 violation of the radiologist's legal duties to the patient.
A manual or syllabus on malpractice prophylaxis will be madeavailable to all participants.
118_
THE EFFECT OF RADIOTHERAPY IN COMBINATION WITH IMMUNOTHERAPY ON TUMORCURE AND MACROPHAGE LYMPHOCYTE INFILTRATION *Carleton C. Stewart, Ph.D., Carlos A. Perez, M.D. and Barbara W. Hente, B.A.Section of Cancer Biology, Division of Radiation Oncology, MallinckrodtInstitute of Radiology, Washington University School of Medicine,St. Louis, Mo. 63110.
The potential usefulness of immunotherapy combined with radiationtherapy is being tested in animal models. Local tumor radiotherapywas given at subcurative doses, followed twice weekly by doses of BCG,C. Parvum, or levamisole comparable to those used in humans. The regimenswere evaluated for curative ability and effects on infiltration of lymphocytes and macrophages into the tumor. Cytotoxicity was observed directlythrough time-lapse cinemicrography of tumor cells in culture.
In the EMT6 tumor system, which has high immunogenicity, 3000 rads cured40% of the mice. Addition of BCG raised the rate to 50%, of C. Parvum to70% and of levamisole to 80%. Duration of survival in uncured animals wasthe same with all four regimens. In the 6C3HED lymphosarcoma, 3000 rads cured30%, and addition of levamisole of C. Parvum had no effect on that rate oron the duration of remission. Addition of BCG raised the cure rate to 70%and lengthened clinical remissions markedly. The KHT fibrosarcoma, whichhas low immunogenicity, was unresponsive to radiation alone or combinedwith any of the agents.
All tumors were infiltrated with macrophages and lymphocytes. Timelapse movies of the KHT and EMT6 tumors in culture show that tumor celllysis is caused by macrophages.Supported by USPH Grant lP02CA13053
105
119_
TUMOR REGRESSION PATTERNS AND TUMOR CONTROL PROBABILITY. DEPENDENCE UPONTUMOR IMMUNOGENICITY AND IMMUNOCOMPETENCE OF THE HOST.Herman Suit, M.D., D.Phil; Oscar Mendiondo, M.D.; and Robert Sedlacek, M.S.Edwin L. Steele Laboratory of Radiation Biology, Department of RadiationMedicine, Massachusetts General Hospital, Boston, Mass.
We have examined for correlations between regression pattern followingsingle or fractionated irradiation (10 equal doses, ti = 48 hr) and localcontrol frequency using 3 murine tumor systems. These were: an immunogenicfibrosarcoma (FSa), weakly immunogenic squamous cell carcinoma (SCCIV),and an essentially non-immunogenic mammary carcinoma (MCa); the tumors weregrowing as early generation isotransplants in the leg; treatment was givento 8 mm tumors. Studies were made of tumors in normal, immune suppressed(600 rad WBI or adUlt thymectomy plus anti-lymphocyte sera), and immunepotentiation. For FSa growing in normal' hosts the rate of regression wascorrelated with TCP only over the range of TCP of 0.05 ~0.3, at higherdose levels, regression was constant. However, there was a markedly slowerregression of FSa in immune suppressed hosts (TCP was also less at anyonedose level). Immunopotentiation did not affect regression times for FSatreated successfully to doses ~800 rads. Studies have also been made ofeffect of block of macrophage function. These various results will bepresented and discussed.
This investigation was supported in part by Grant Number 2 ROI CA133ll,awarded by the National Cancer Institute, DHEW.
120_
T CELL DEPLETION AND TUMOR METASTASISL.J. Peters, M.D., W.H. McBride, Ph.D. and K.A. Mason, M.Sc., Section ofExperimental Radiotherapy, The University of Texas System Cancer CenterM.D. Anderson Hospital and Tumor Institute, Houston, Texas 77030.
Depletion of circulating T lymphocytes foll'owing localized radiotherapy for breast cancer has been claimed to facilitate the developmentof tumor metastases. The following experimental evidence does not substantiate this. Mice receiving 1000 rads in a single dose to the wholebody except thorax developed no more lung colonies than unirradiatedcontrols following intravenous injection of syngeneic fibrosarcoma cells,in spite of profound lymphopenia. Although whole body irradiation significantly increased lung colony forming efficiency, mice renderedchronically T cell deficient by thymectomy, whole body irradiation andsyngeneic bone marrow reconstitution (TIR) showed only a marginal increase in lung colony counts two months after irradiation compared withanimals which were not thymectomized prior to whole body irradiation,thus allowing recovery of T cell function. Further, reconstitution ofTIR mice with 5 x 107 thymocytes plus a thymic graft failed to increasetheir resistance to tumor growth. It is concluded that the enhancementof artificial lung metastases by high doses of whole body irradiationis largely independent of T cell depletion.
This research was supported in part by NIH Research grant numbersCA-11138, CA-06294 and CA-17769 from the National Cancer Institute.
106

121_
EFFECT OF WIDE FIELD IRRADIATION ONUNIRRADIATED TUMORS IN THE SAME HOST
Jay S. Cooper. M.D •• Robert S. Bart, M.D .• AlfredW. Kopf, M.D •• and Joseph Newall. M.D.
New York University Medical Center. Division ofRadiation Oncology, New York, New York
Ionizing radiation has an immunosuppressive potential and the immunesystem is believed to influence tumor growth. However. investigatorshave come to conflicting conclusions regarding the effect of localizedradiation therapy on both the immune system and on distant tumor growth.
This report describes a murine model. B-16 melanoma was implantedinto the left groin one week before implanting melanoma into the rightaxilla in order to immunize the mouse against the subsequently implantedaxillary tumor. Six-hundred rad caudal hemibody irradiation was givenin a single fraction by a 4 MeV linear accelerator. Significantdiminuation of the growth rate of irradiated groin tumors occurred.Unirradiated axillary tumors did not demonstrate an increased growth rate.
We conclude that, at least in this model, high dose. wide-fieldirradiation does not augment the growth of unirradiated tumors in the samehost.
122_
DEPENDENCE OF EFFICACY OF C PARVUM ON TUMOR TRANSPLANT SITERita M. Linggood, M.B. B.S .; Vlatko Silobrcic, M.D., Ph.D.; Joel Busse, M.D.;Robert Sedlacek, M.S.; and Herman Suit, M.D ., D.Phil.Edwin L. Steele Laboratory of Radiation Biology. Department of RadiationMedicine, Massachusetts General Hospital, Boston. Mass.
Barlier work indicated that the effectiveness of host immune reactionagainst tumor may be dependent, in part, on tumor site . As part of ourprogram to study efficacy of C parvum potentiated reaction against tumor,the success of C parvum treated has been assessed for tumor growing atvarious anatomic sties. For this investigation, a fibrosarcoma (methylcholanthrene induced) was transplatned into adult syngenic C3Hf/Sed mice.This tumor is immunogenic in these hosts. Transplantation was made intothe following anatomic sites ; sk in, subcutaneous tissue, muscle, liver(via portal vein) , cerebrum, urinary bladder wall, large bowel wall, leftkidney (via renal artery injection), and uterus (lung has been studiedextensively previously). Following transplantation, the mice were randomized to receive saline or C parvum. The later was administered as asingle i.v. dose of 3S0~g. Analysis of results as of this writing showthat C parvum is of greatest effect against intracutaneous tumor; verypoor results have been obtained for tumor growing in urinary bladder wa l land in the cerebrum. Complete analysis of these data will be presented.
This investigation was supported in part by Grant Number 2 ROI CA13311,awarded by the National Cancer Institute, DHEW.
107
123_
CORYNEBACTERIUM PARVUM & RADIATION INDUCED CYCLINGACTIVITY OF HEMOPOIETIC CELLS
Yosh Maruyama. M.D •• Clara Magura. B.S •• Jose Feola. Ph.D.Department of Radiation Medicine
University of Kentucky. Medical CenterLexington. KY 40506
Spleen colony forming cells (CFU-S) proliferate after irradiation of hostmice to form visible splenic nodules in mice. 10 days later. EndogenousCFU-S are a means of tracing the responses of a hemopoietic stemcell following administration of a variety of stimuli to animals.Corynebacterium Parvum Vaccine was tested to study the inter-relationbetween the hematopoietic and immuno-hematopoietic systems in C57BLmice.
C. Parvum in a dose of 0.05 ml was found to increase two-fold thenumber of surviving CFU-S when given 4-72 hours before irradiation.This increase in survivorships of the CFU-S and altered radiosensitivity was found to be sensitive to in vivo or in vitro "suicide"assay using high specific activity H3TdR (So Ci/mMol~(HSATT). Thatis. the increase in CFU-S survival caused by C. Parvum was reduced tocontrol levels by HSATT. This indicates that stem cells had beenstimulated into cell cycling activity and that a cohort of cells inS phase had been increased. The CFU-S observed after C. Parvum wasgiven 4-6 hours before and HSATT 1 hour before total body irradiationwere shown to have been stimulated into DNA-S phase. The data wereconsistent with a Gl resting CFU population positioned close to DNA-S.and a parasynchronous progression of the stem cells into S phaseshortly after C. Parvum stimulation. Syngeneic mouse lymphoma cellshad no effect on spleen CFU.
These results show that C. Parvum promptly and strongly stimulatedthe hemopoietic system. Since C. Parvum also represents a non-specificimmune stimulant there may be some inter-relation between the twosystems at the stem cell level. Response to syngeneic tumor was.however. not detectable in these experiments and therefore indicatesthat such tumors are not strong stimulants at the same level of stemcell.
108
124_
PRtCISION HIGH DOSE RADIATION THERAPY IN
THE TREATMENT OF CARCINOMA OF THE PANCREAS
R.R. Dobe1bower, Jr., M.D., Ph.D., B.B. Borgelt, M.D., Ph.D.,N. Sunthara1ingam, Ph.D. and K.A. Strub1er, M.S., Departmentof Radiation Therapy and Nuclear Medicine, Thomas JeffersonUniversity Hospital, Philadelphia, Pennsylvania.
Eighteen patients with localized adenocarcinoma of the pancreas weretreated with precision high dose radiation therapy over a 24 monthperiod. All patients had biopsy proven cancer with placement of radioopaque clips at laparotomy to define gross tumor extent. No patientswith metastatic disease (exclusive of regional nodal involvement orcontiguous involvement of adjacent structures) were treated. Externalbeam radiation was delivered using the 45 MV Betatron. The target volumeincluded the clipped tumor volume plus a 1 to 2 cm margin. Thirteenpatients were treated by a 3 field technique designed to minimize the doseto the kidneys and spinal cord. This technique consisted of opposed lateral45 MV photon beams and an anterior "mixed beam" of 50% 45 MV photons and 50%15 to 35 MeV electrons. (Dobe1bower et a1, Int. J Radiat Onco1 Bio1 Phys 1:141, 1976). Five patients were treated with a 4 field "box" techniquewith 45 MV photon beams. Minimum dose to the target volume was 6300 to6700 rad delivered in 180 rad fractions treating two or three fields dailyover 7 to 9 weeks. Post radiation follow up ranges from 6 to 24 months.Eleven patients have died, nine with local and/or metastatic disease andtwo of intercurrent disease. Seven patients are living, one with clinicalevidence of local disease and six with no evidence of disease at 10 to24 months. Treatment has been surprisingly well tolerated and there havebeen no serious radiation complications. Our preliminary experienceindicates that this therapeutic modality is capable of producing improvedpalliation if not definitive radiotherapeutic management of localizedunresectable pancreatic cancer.
This work is supported in part by a grant (CA 11602-07) from the Divisionof Cancer Research Resources and Centers, the National Cancer Institute,U.S. Department of Health, Education and Welfare.
109
125_
ON THE Hl~AN CLONOGENIC CANCER CELL: THE RADIORESISTANT FRACTION ANDITS IMPLICATIONS FOR RADIOTHERAPY
J. Robert Andrews and Kenneth L. Mossman
The Georgetown University School of Medicine and the WashingtonVeterans Administration Hospital
The local control of solid cancers by treatment with ionizing radiationsis contingent upon the destruction by these radiations of a minimumnumber of clonogenic cancer cells. Included in this minimum numberwill be the most radioresistant co~ponent of the cancer cell population.It is shown that the slope of a curve developed from clinicalradiotherapy cancer control data conforms with the negatLve slope ofthe radiation dose, cell survival curve of this most radioresistantcomponent. The reciprocal, the DB dose, of this negative slope isfound to have a value of about 40 , in terms of the Roentgen, rad, orret. By the application of the Poisson distribution it is shownthat, in small human solid cancers, this minimum number of resistantclonogenic cancer cells is, by absolute standards, small. By relativestandards this number is large and perhaps large enough to minimizethe clinical usefulness of high LET radiations.
126_
RESPONSE OF CAPILLARY ENDOTHELIAL CELLS AFTERBETA, X, GAMMA AND NEUTRON IRRADIATION
John R. Fike, M.S. and Edward L. Gillette, D.V.M., Ph. D.State University, Fort Collins, Colorado
Colorado
Induced neovascularization in the dogs' cornea was used as ameans to study the radiation response of capillary endothelial cells.Central lamellar keratectomies were used to stimulate capillary proliferation either before or after irradiation, and after seven days,corneal tissue containing the capillaries was excised, prepared histologically, and evaluated using a modified Chaukley's technique forquantitative tissue analysis. Irradiation included gOy beta particles,120 kVp x rays, 60Co gamma rays and cyclotron produced neutrons withan average energy of 9.3 meV.
Induction of capillary proliferation after irradiation provideda method to study the response of a virtually nonproliferating cellpopulation. Post irradiation induction, on the other hand, reflectedthe response of proliferating endothelial cells. Single-dose responsecurves had a Do of 381 rads if induction was stimulated 48 hours afterbeta radiation, while Do = 238 rads if irradiation was immediatelypost induction, and Do = 261 rads six hours post induction. Split-dosestudies for beta irradiation provided a D2 - 01 value of 500 rads if
110
the first dose was delivered immediately post induction and the secondsix hours later.
X-ray and 60Co gamma-ray data showed similar Do values on theorder of 380 rads if given 48 hours prior to surgery. Neutron irradiation 48 hours pre induction gave a Do value of 217 rads.
Supported by the National Cancer Institute Grant No. 2 ROlCA 13899-04.
127_
EMOTIONAL REACTIONS TO RADIATION TREATMENT
By
Arthur Peck, M.D. and John Boland, M.D.Department of Radiotherapy, Mount Sinai Medi cal Center
New York, New York
Radiation treatment has been omitted from public health information about cancer.Very little effort has been made to assess the cancer patient's own concepts ofradiation treatment. When patients arrive for radiation, have they been preparedfor what they will undergo?
Fifty patients starting a radical course of treatment for cancer at the RadiotherapyService of the Mount Sinai Medical Center of New York City were interviewed bya psychiatrist. The focus of the initial interview was what they were told when referredfor radiation. Although 60% were told by their doctors that they had cancer, all arrivedat the treatment center unprepared for the frequency, number, and procedure of treatment and for the efficacy of treatment by radiation.
Patients believed that requiring radiation was very bad news. It meant definitelyhaving cancer and that surgery had not extirpated it. Radiation was feared as inherentlydamaging and quite possibly carcinogenic. Few expected it to be curative.
Interviews after completing treatment revealed an incidence of depression and anxietyeven greater than in the pre-treatment interviews, indicating that radiation treatmentis stressful in itself. Fewer than one-third judged themselves improved by radiation.More than one-third felt worse and judged treatment to have been ineffective, notrealizing their new distress resulted from side effects of radiation.
Patients suffer irrational fears of damage and death because of erroneous preconceptionsof radiation which doctors fail to correct. Ironically, the lay and medical conceptsof the dismal manifestations and futility of radiation treatment are entirely false.In this series, only one patient suffered damage due to radiation. Sixty percent werefree of signs of cancer at follow-up 18-36 months later.
111
128_
CORYNEBACTERIUM PARVUM THERAPY IN COMBINATION
WITH RADIOTHERAPY IN EXPERIMENTAL TUMORS
C.K. Kim-Lee, M.D., C.W. Song, PH.D., A.L. Tsui Collins, Ph.D., S.H. Levitt, M.D.Dept. of Therapeutic Radiology, Medical School, University of Minnesota
The effectiveness of immunotherapy using C. parvum and the effectiveness of combined immunotherapy and radiotherapy was studied. Thetumor used was Ependymoblastoma growing subcutaneously in the hind legof C57BL mice. A single intralesional injection of 116 ug of C. parvumto 6-7 mm tumor did not cause any complete regression of tumors, butsignificantly suppressed the tumor growth and prolonged the survivingtime of the hosts. The therapeutic effect was more pronounced when tumors of 3-4 mm in diameter were treated. Out of 15 tumors treated, 5tumors completely regressed. The remaining tumors grew slowly as compared with the saline-injected control tumors, as shown in the table.The surviving time of the remaining animals was significantly longerthan that of the saline-injected control animals; while all control animals died 20-35 days after the saline injection, the C. parvum-treatedanimals died 40-80 days after the treatment. In the study of combinedtreatment, 6-7 mm diameter tumors received a single intralesional injection of 116 ug C. parvum and a single exposure of 2000 rads of X-rays24 hours later. Although the surviving time of the animals receivingthe combined treatment was longer than that of the animals receiving theradiotherapy alone, there was no significant difference in the cure rate.Further studies are in progress to determine the effect of various variables, such as the dose and the route of C. parvum administration, thedose of X-rays and the sequence of the treatments . (supported by NIHgrant CA 15548 and American Cancer Society grant PDT-17).
Diameter of Tumor in mm.
Days 0 3 7 10 14 17 21 24*
Saline 3.7 6.0 8.3 9.7 12.5 16.2 17.8 20.1
C. parvum 3.6 6.3 7.3 7.7 7.8 8.9 8.0 9.3
*Control animals started to die 24 days after treatment.
112