Embed Size (px)
Citation preview

Asthma
Presentation and Treatment
Symptoms of Asthma
The usual presenting features are well known
1) Wheeze
2) Dyspnoea
3) Cough (usually persistent)
4) Chest tightness
Less well known complaints
1) Difficulty in sleeping
2) Chest pain
3) Vomiting
4) Itching (in children usually on upper body)

Asthma
Asthma is a common disorder affecting
between 5-10% of the population. There is
no cure but proper management can
usually control patient’s symptoms to
maintain quality of life.

Diagnostic Algorithm For Wheezing/Airway Obstruction
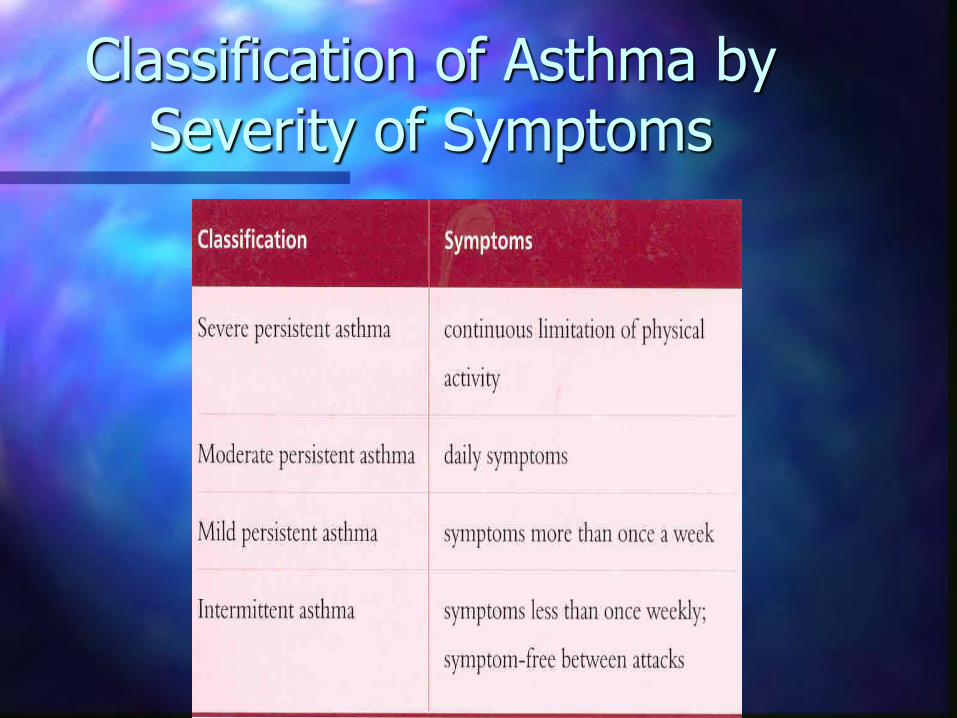
Classification of Asthma by Severity of Symptoms

Epidemiology
8-10% of children diagnosed as asthmatic and
15-20% adults experience wheeze but
probably around 5% suffer nocturnal
breathlessness or have the reversible airflow
obstruction that defines asthma. Thus a
proportion of children with asthma ‘grow out’
of the condition. Asthma costs the U.K. £500
million per year in drug costs alone.
Prevalence
Asthma is increasing in prevalence between the
early 1970’s and mid 1980’s prevalence increased
by 50%. In the same period hospital admissions for
asthma rose from 20,000 to 80,000 per year.
Currently the figure is 100,000.
Deaths from asthma peaked in the late 1980’s at 39
per million of U.K. population (2,300) and are now
around 27 per million (1,600). Since the early
1990’s hospital admissions have been fairly stable.
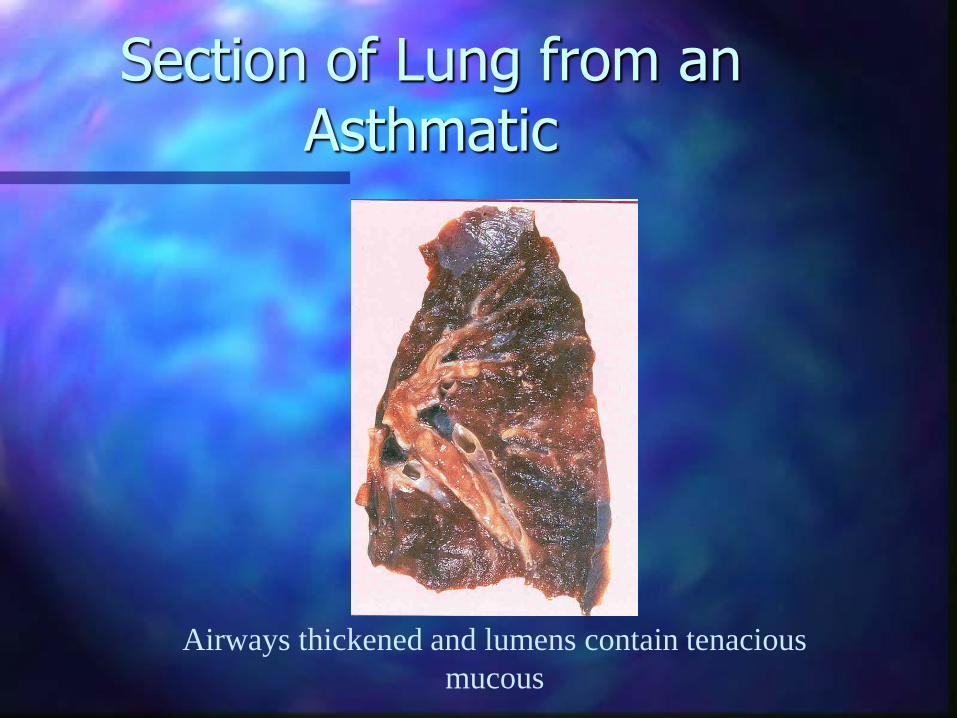
Section of Lung from an Asthmatic
Airways thickened and lumens contain tenacious
mucous
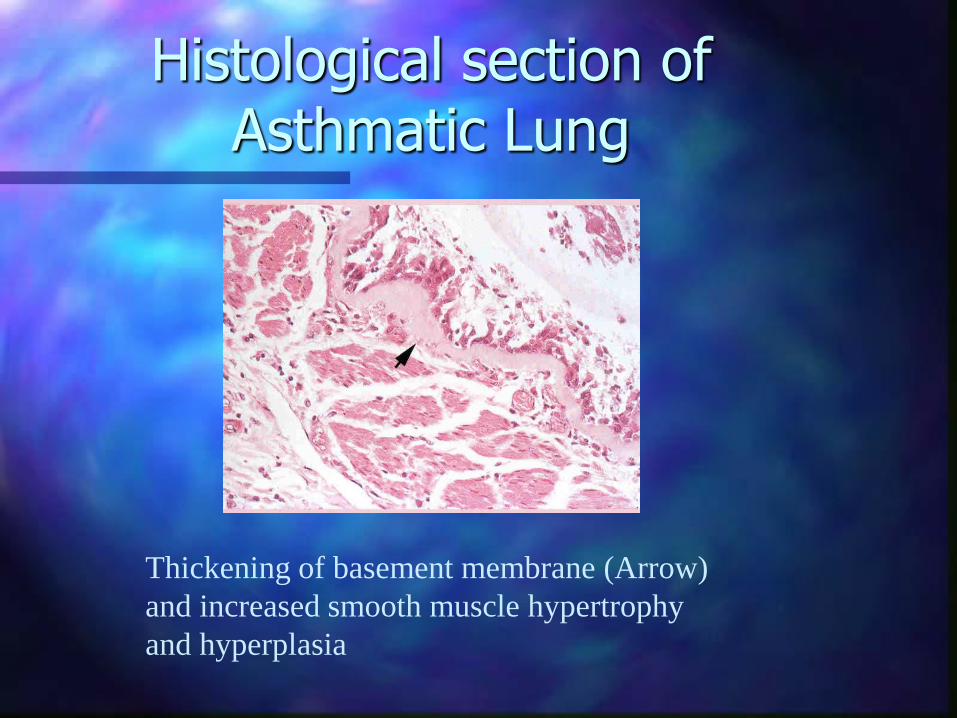
Histological section of Asthmatic Lung
Thickening of basement membrane (Arrow)
and increased smooth muscle hypertrophy
and hyperplasia

Histological section of a cartilaginous airway from a case of fatal asthma
Inflammation and Asthma
The role of inflammation in the pathogenesis of asthma is now known to be pre-eminent. Asthma arises from interactions between Mast cells, eosinophils, T-lymphocytes, neutrophils and epithelial cells. These interactions are triggered by inflammatory processes and modulated by mediators of inflammation. Disease control is achieved by early use of anti-inflammatory medications to retard disease progression and reduce the severity of airway hyperreactivity.
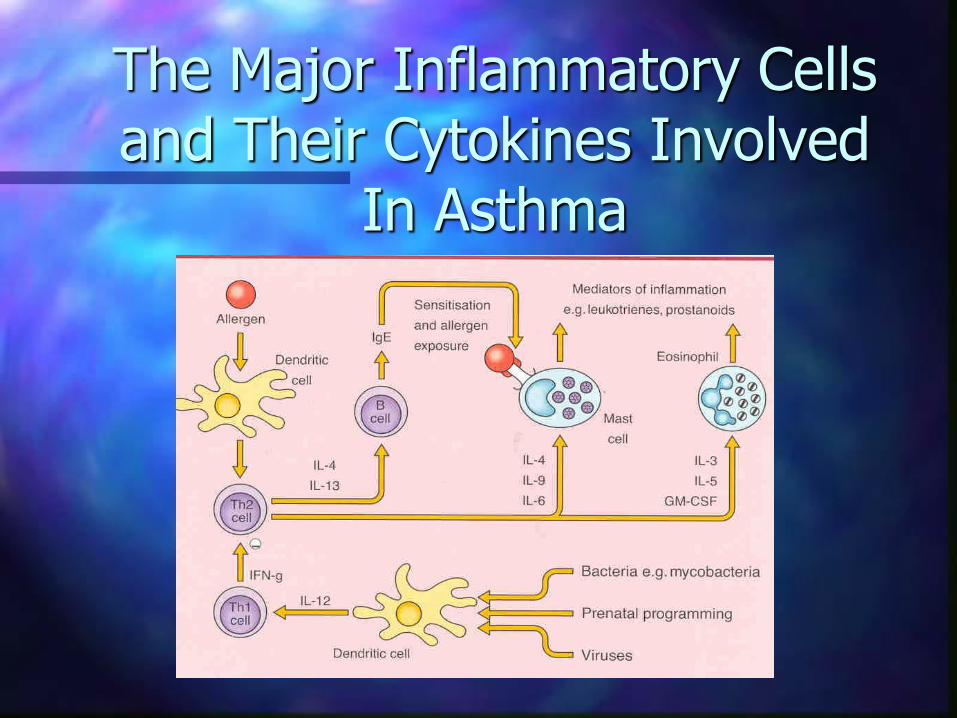
The Major Inflammatory Cells and Their Cytokines Involved
In Asthma

Cell interactions involved in monocyte/macrophage migration in Asthma
What should Asthma Therapy Do?

Non Pharmacological Measures
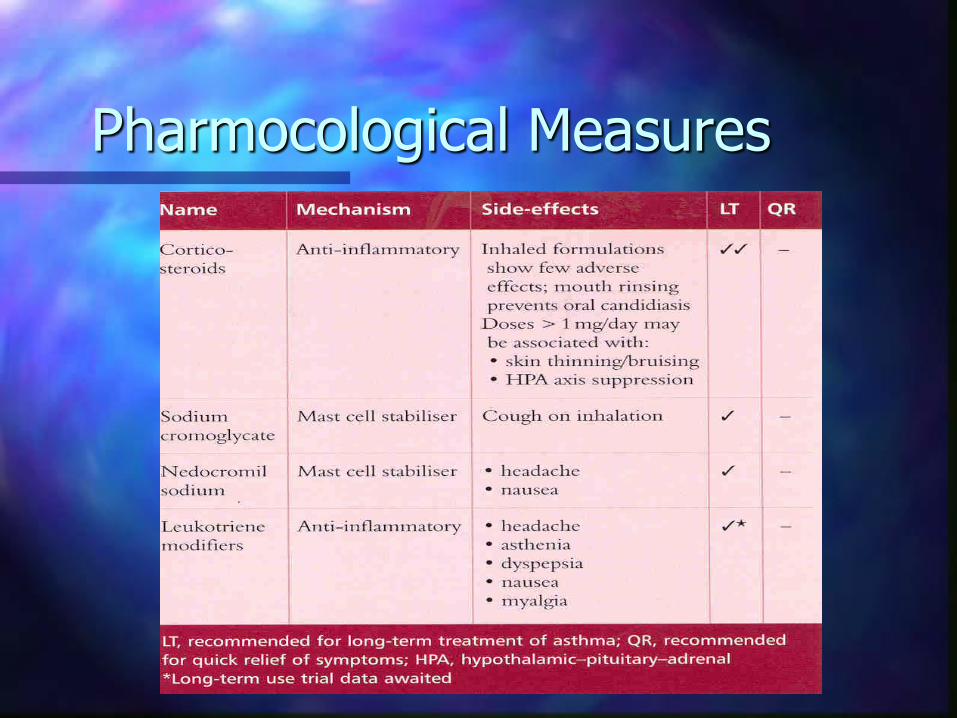
Pharmocological Measures
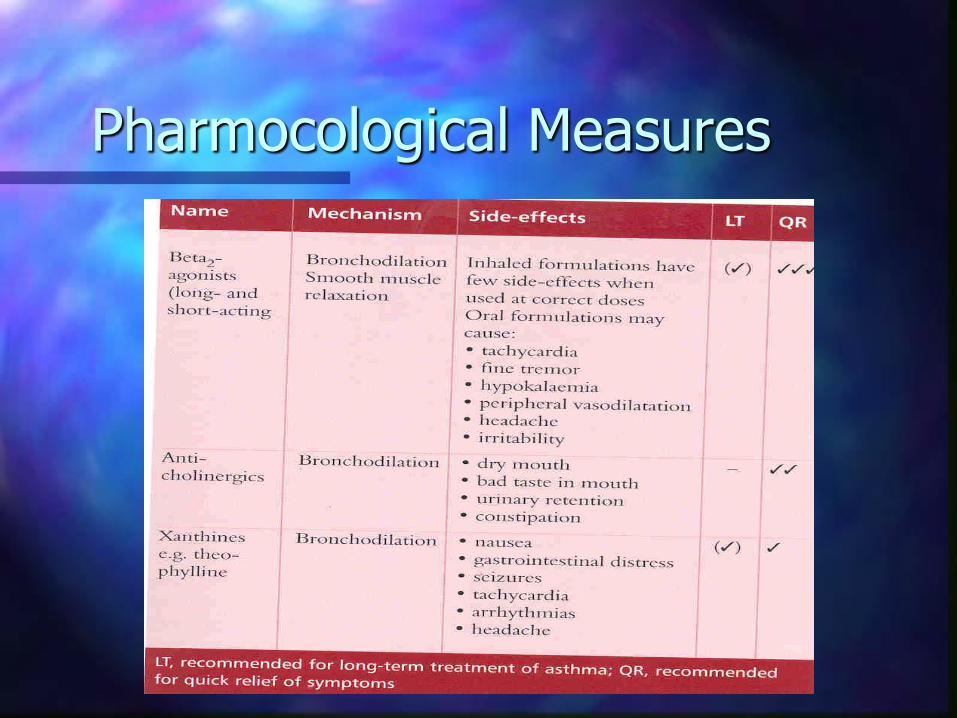
Pharmocological Measures
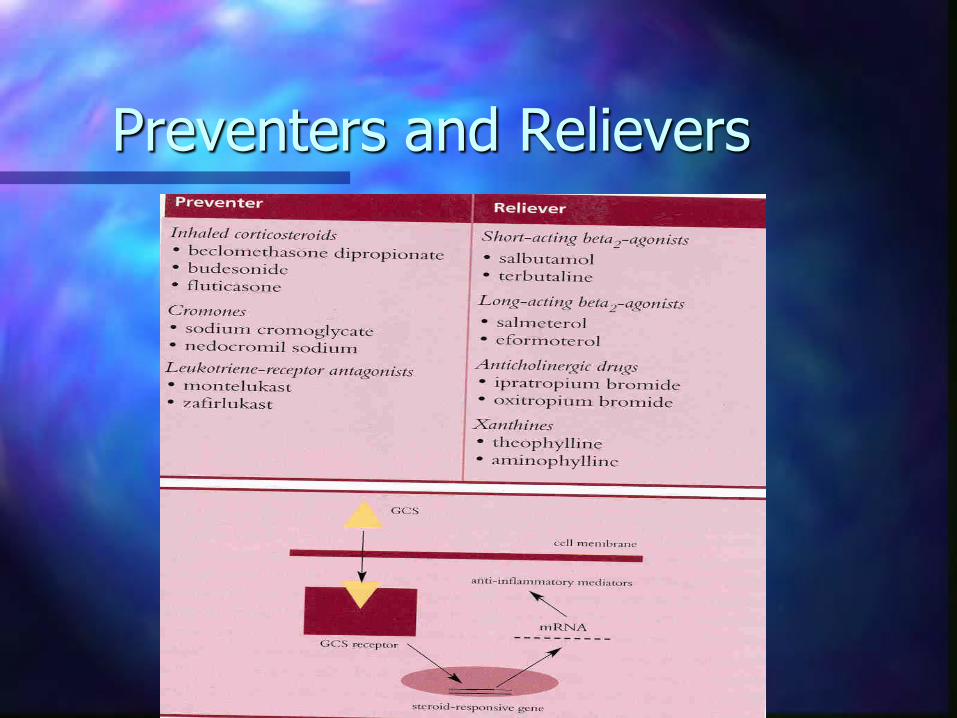
Preventers and Relievers

Leukotrienes in Asthma
Corticosteroids
These act in a number of ways
1. Reduce the number and activity of mast cells, eosinophils and neutrophils
2. Reduce inflammatory reactions such as oedema and mucous secretion.
3. Upregulation of beta-adrenergic receptor numbers and sensitivity
4. Producing phospholipase A2 inhibitors
5. Suppressing late phase inflammatory reaction

Corticosteroids
Wherever possible inhaled corticosteroid administration is always preferred to oral administration. This is due to the much lower frequency of systemic side effects Inhaled corticosteroids are now universally recognised as an essential component of asthma therapy. They are a preventer medication i.e. prophylactic and are not indicated for use in acute asthma.

Cromones
Sodium chromoglycate and nedocromil sodium stabilise mast cells and other inflammatory cells by inhibiting the release of histamine and leukotrienes. They are well tolerated, with a low level of adverse systemic effects, but are less effective in treating adult asthma than inhaled corticosteroids. Cromones tend to be most effective in mild atopic asthma, especially in children. Compliance may be a problem as they are short acting and need to be taken at least 4 times daily.
Leukotriene modifying agents
These are of 2 types 1 Leukotriene synthesis inhibitors 2. Cysteinyl leukotriene-receptor agonists such as montelukast and zafirlukast Both types block the brochoconstrictor and proinflammatory activity of cysteinyl leukotrienes within the asthmatic airway.

Leukotriene Modifying Agents
The cysteinyl leukotrienes (LTC4, LTD4 and LTE4) are metabolites of arachidonic acid and are almost exclusively produced by inflammatory leukocytes. They cause smooth muscle constriction and proliferation and mediate the pathophysiology of the inflammatory process. Thus the inhibition of their synthesis or the blocking of their receptors can improve baseline lung function and reduce bronchial hyperresponsiveness. They are suggested as additive therapy in severe asthma as their systemic effects are less pronounced as those of corticosteroids.

Beta2-Agonists
Drugs such as Salbutamol and Terbutaline are first line agents for the acute relief of asthma symptoms and are indicated for use on an ‘as required’ basis. The drugs competitively activate beta2-adrenergic receptors and increase (cAMP) levels in bronchial smooth muscle. This provides energy for compartmental shifts in calcium resulting in bronchial smooth muscle relaxation. Inhaled beta2-agonists are effective when used shortly before exercise or exposure to known allergens. The need to increase use of the agents indicates an activated inflammatory cascade and thus the need to increase the dose of inhaled corticosteroid.

Long Acting Beta2-agonists
These include Salmeterol and eformeterol they are not intended for symptom relief, nor as replacement for prophylactic therapy. They are indicated as an add in therapy for patients receiving moderate to high doses of inhaled corticosteroid. Eformoterol is more potent and has a faster onset of action than Salmeterol.
Their mode of action is as for the short acting beta2 agonists. Like these continued use down regulates expression of beta2-adrenergic receptors. Because of their duration of action they have effects on receptors in other tissues such as vascular endothelium, mast cells and sympathetic nervous tissue.

Anticholinergic Drugs
Sometimes called antimuscarinic these drugs include Itrapropium bromide and Oxitropium bromide. These are muscarinic receptor agonists that relax smooth muscle preventing and relieving bronchospasm in asthma. Their onset of action is slow (30-60 mins) but duration of action is up to 8 hours. Regular inhalation of an anticholinergic is indicated where control is inadequate in patients receiving maximal anti-inflammatory therapy and a short acting beta2-agonist as required

Xanthine Bronchodilators (Theophyllines)
Theophylline has a narrow therapeutic index and many patients have adverse effects within the therapeutic range.Sustained release formulations can be useful in nocturnal asthma. Theophylline has anti-inflammatory effects and is used for patients with severe persistent asthma requiring multiple drugs for symptom control. The anti-inflammatory effects occur at doses lower than that required for symptom control. Serum levels must be monitored to optimise dosing. Long term use at high doses should be avoided.

Optimal Asthma Therapy
It is now increasingly recognised that optimal control of asthma is achieved by combining inhaled corticosteroid and a long acting beta2-agonist. The advantages are that it reduces the number of inhaler therapies thus improving compliance, this is further enhanced since the beta2-agonist will give fairly rapid symptom relief. The corticosteroid element provides good anti-inflammatory effects and enhances the effects of the beta2-agonist by negating the reduction in beta2-adrenergic receptors these agents induce.





![Urinary leukotriene E in bronchial asthma · increase nonspecific bronchial hyperresponsiveness (5-8], and are potent bronchoconstrictor agents [1, 9, 10]. They have the potential](https://img.pdfslide.us/doc/110x75/5ebaf313bd7a1d5b70025536/urinary-leukotriene-e-in-bronchial-asthma-increase-nonspecific-bronchial-hyperresponsiveness.jpg)






















