-
8/7/2019 Asthma British 2009
1/132
Scottish Intercollegiate Guidelines Network
Part of NHS Quality Improvement Scotland
SIGN
British Guidelineon the Management of Asthma
A national clinical guideline
May 2008
revised June 2009
101
-
8/7/2019 Asthma British 2009
2/132
NHS Quality Improvement Scotland (NHS QIS) is committed to
equality and diversity. Thisguideline has been assessed for its
likely impact on the six equality groups dened by age,
disability,gender, race, religion/belief, and sexual
orientation.
For the full equality and diversity impact assessment report
please see the published guidelinessection of the SIGN website at
www.sign.ac.uk/guidelines/published/numlist.html. The full reportin
paper form and/or alternative format is available on request from
the NHS QIS Equality andDiversity Ofcer.
This document is produced from elemental chlorine-free material
and is sourced from sustainable forests
http://www.sign.ac.uk/guidelines/published/numlist.htmlhttp://www.sign.ac.uk/guidelines/published/numlist.html
-
8/7/2019 Asthma British 2009
3/132
The College of
Emergency Medicine
British Thoracic Societ
Scottish Intercollegiate Guidelines Network
B G Maagm Ama
A national clinical guideline
May 2008
Revised June 2009
-
8/7/2019 Asthma British 2009
4/132
British Guideline on the MAnAGeMent of AsthMA
isBn 978 1 905813 28 5
f pb 2003rv pb 2008rv pb 2009
SIGN and the BTS consent to the photocoping of this guideline
for the purpose ofimplementation in the NHS in England, Wales,
Northern Ireland and Scotland.
sc icga G nwke h, 8 -10 h Cc
ebg eh7 5eA
www.g.ac.k
B tacc scy17 dgy s,l, WC1n 2Pl
www.b-acc.g.k
-
8/7/2019 Asthma British 2009
5/132
Contents
C
1 ic 1
1.1 Statement of intent 1
2 dag 2
2.1 Diagnosis in children 2
2.2 Other investigations 8
2.3 Summar 9
2.4 Diagnosis in adults 11
2.5 Further investigations that ma beuseful in patients with an
intermediateprobabilit of asthma 16
2.6 Monitoring asthma 18
3 n-pamacgca maagm 24
3.1 Primar prophlaxis 243.2 Secondar non-pharmacological
prophlaxis 27
3.3 Other environmental factors 28
3.4 Dietar manipulation 29
3.5 Complementar and alternative medicine 31
3.6 Other complementar or alternativeapproaches 32
4 Pamacgca maagm 33
4.1 Step 1: mild intermittent asthma 34
4.2 Step 2: introduction of regular
preventer therap 34
4.3 Step 3: initial add-on therap 38
4.4 Step 4: poor control on moderatedose of inhaled steroid +
add-on therap:addition of fourth drug 40
4.5 Step 5: continuous or frequentuse of oral steroids 41
4.6 Stepping down 46
4.7 Specicmanagementissues 46
5 ia vc 48
5.1 Technique and training 48
5.2 2
agonist deliver 48
5.3 Inhaled steroids for stable asthma 49
5.4 Cfc propellant pmdi vs hfapropellant pmdi 49
5.5 Prescribing devices 50
5.6 Use and care of spacers 50
6 Maagm ac ama 51
6.1 Lessons from studies of asthmadeaths and near-fatal asthma
51
6.2 Acute asthma in adults 53
6.3 Treatment of acute asthma in adults 56
6.4 Further investigation and monitoring 60
6.5 Asthma management protocolsand proformas 60
6.6 Hospital discharge and follow up 60
6.7 Acute asthma in children agedover 2 ears 61
6.8 Initial treatment of acute asthma inchildren aged over 2
ears 63
6.9 Second line treatment of acute asthma inchildren aged over 2
ears 66
6.10 Assessment of acute asthma in childrenaged less than 2 ears
67
6.11 Treatment of acute asthma in childrenaged less than 2 ears
68
7 spca a 69
7.1 Difcultasthma 69
7.2 Factorscontributingtodifcultasthma 69
7.3 Asthma in pregnanc 71
7.4 Management of acute asthma inpregnanc 72
7.5 Drug therap in pregnanc 73
7.6 Management during labour 75
7.7 Drug therap in breastfeeding mothers 76
7.8 Occupational asthma 77
7.9 Management of occupational asthma 79
8 ogaa a vy ca,
a a 80
8.1 Routine primar care 80
8.2 Acute exacerbations 82
8.3 Audit 83
9 Pa ca a maagm 85
9.1 Self-management education andpersonalised asthma action
plans 85
9.2 Compliance and concordance 86
9.3 Implementation in practice 88
9.4 Practical advice 88
10 dvpm g 90
10.1 Introduction 90
10.2 Executive and steering groups 90
10.3 Evidence review groups 91
10.4 Dissemination group 94
10.5 Sstematic literature review 94
10.6 Consultation and peer review 95
Abbva 96A 97rc 109
Revised
2009
Revised
2009
Revised
2009
-
8/7/2019 Asthma British 2009
6/132
British Guideline on the MAnAGeMent of AsthMA
KeY to eVidenCe stAteMents And GrAdes of reCoMMendAtions
leVels of eVidenCe
1++ High qualit meta-analses, sstematic reviews of RCTs, or RCTs
with a ver low risk of bias
1+ Well conducted meta-analses, sstematic reviews, or RCTs with
a low risk of bias
1 - Meta-analses, sstematic reviews, or RCTs with a high risk of
bias
2++ High qualit sstematic reviews of case control or cohort
studies
High qualit case control or cohort studies with a ver low risk
of confounding or bias and ahigh probabilit that the relationship
is causal
2+ Well conducted case control or cohort studies with a low risk
of confounding or bias and amoderate probabilit that the
relationship is causal
2
Casecontrolorcohortstudieswithahighriskofconfoundingorbiasandasignicantriskthatthe
relationship is not causal
3 Non-analtic studies, eg case reports, case series
4 Expert opinion
GRADES OF RECOMMENDATION
Note: The grade of recommendation relates to the strength of the
evidence on which therecommendation is based. It does not reect the
clinical importance of the recommendation.
A At least one meta-analsis, sstematic review, or RCT rated as
1++,and directl applicable to the target population; or
A bod of evidence consisting principall of studies rated as
1+,directl applicable to the target population, and demonstrating
overall consistenc of results
B A bod of evidence including studies rated as 2++,
directl applicable to the target population, and demonstrating
overall consistenc of results; or
Extrapolated evidence from studies rated as 1++ or 1+
C A bod of evidence including studies rated as 2+,directl
applicable to the target population and demonstrating overall
consistenc of results; or
Extrapolated evidence from studies rated as 2++
D Evidence level 3 or 4; or
Extrapolated evidence from studies rated as 2+
GOOD PRACTICE POINTS
Recommended best practice based on the clinical experience of
the guideline developmentgroup.
Audit point
-
8/7/2019 Asthma British 2009
7/132
1
1 ic
In 1999 the British Thoracic Societ (BTS) and the Scottish
Intercollegiate Guidelines Network(SIGN) agreed to jointl produce a
comprehensive new asthma guideline, both having previouslpublished
guidance on asthma. The original BTS guideline dated back to 1990
and the SIGN
guidelines to 1996. Both organisations recognised the need to
develop the new guidelineusing explicitl evidence based methodolog.
The joint process was further strengthened bcollaboration with
Asthma UK, the Roal College of Phsicians of London, the Roal
College ofPaediatrics and Child Health, the General Practice Airwas
Group, and the British Associationof Accident and Emergenc Medicine
(now the College of Emergenc Medicine). The outcomeof these efforts
was the British Guideline on the Management of Asthma published in
2003.1
The 2003 guideline was developed using SIGN methodolog,2 adapted
for UK-wide use.Electronic literature searches extended to 1995,
although some sections required searchesback as far as 1966. The
pharmacological management section utilised the North of
EnglandAsthma guideline to address some of the ke questions on
adult management. 3 The North ofEngland guideline literature search
covered a period from 1984 to December 1997, and SIGNaugmented this
with a search from 1997 onwards.
Since 2003 sections within the guideline have been updated
annuall and posted on both theBTS (www.brit-thoracic.org.uk) and
SIGN (www.sign.ac.uk) websites. In 2004 the sections
onpharmacological management, acute asthma and patient self
management and compliancewere revised. In 2005 sections on
pharmacological management, inhaler devices, outcomesand audit and
asthma in pregnanc were updated, and occupational asthma was
rewritten withhelp from the British Occupational Health Research
Foundation.
In 2006 the pharmacological management section was again
updated. While the web-basedalterations appeared successful, it was
felt an appropriate time to consider producing a newpaper-based
version in which to consolidate the various earl updates. In
addition, since 2006,the guideline has had input from colleagues
from Australia and New Zealand.
The 2008 guideline considered literature published up to March
2007. It contains a completel
rewritten section on diagnosis for both adults and children; a
section on special situations
whichincludesoccupationalasthma,asthmainpregnancyandthenewtopicofdifcultasthma;updated
sections on pharmacological and non-pharmacological management; and
amalgamatedsections on patient education and compliance, and on
organisation of care and audit. The2009revisions include updates to
pharmacological management, the management of acute asthmaand
asthma in pregnanc. Update searches were conducted on inhaler
devices but there
wasinsufcientnewevidencetochangetheexistingrecommendations.Theannexeshavealsobeenamendedtoreectcurrentevidence.
The timescale of the literature search for each section isgiven in
Annex 1. It is hoped that this asthma guideline continues to serve
as a basis for highqualit management of both acute and chronic
asthma and a stimulus for research into areasof management for
which there is little evidence. Sections of the guideline will
continue to beupdated on the BTS and SIGN websites on an annual
basis.
1.1 stAteMent of intent
This guideline is not intended to be construed or to serve as a
standard of care. Standardsof care are determined on the basis of
all clinical data available for an individual case
andaresubjecttochangeasscienticknowledgeandtechnologyadvanceandpatternsofcareevolve.
Adherence to guideline recommendations will not ensure a successful
outcome inever case, nor should the be construed as including all
proper methods of care or excludingother acceptable methods of care
aimed at the same results. The ultimate judgement must bemade b the
appropriate healthcare professional(s) responsible for clinical
decisions regardinga particular clinical procedure or treatment
plan. This judgement should onl be arrived atfollowing discussion
of the options with the patient, covering the diagnostic and
treatmentchoicesavailable.Itisadvised,however,thatsignicantdeparturesfromthenationalguideline
or an local guidelines derived from it should be full documented
in the patients case notesat the time the relevant decision is
taken.
1 introduCtion
-
8/7/2019 Asthma British 2009
8/132
-
8/7/2019 Asthma British 2009
9/132
2++
2++
3
Table 1: Clinical features that increase the probability of
asthma
Morethanoneofthefollowingsymptoms:wheeze,cough,difcultybreathing,chesttightness,
particularl if these smptoms:
are frequent and recurrent 10-13
are worse at night and in the earl morning 11,12,14
occur in response to, or are worse after, exercise or other
triggers, such as exposureto pets, cold or damp air, or with
emotions or laughter
occur apart from colds 10
Personal histor of atopic disorder 10,13,15
Famil histor of atopic disorder and/or asthma 10,16
Widespreadwheezeheardonauscultation
Histor of improvement in smptoms or lung function in response to
adequate therap
Table 2: Clinical features that lower the probability of
asthma
Smptoms with colds onl, with no interval smptoms10
Isolatedcoughintheabsenceofwheezeordifcultybreathing 17
Histor of moist cough 18
Prominentdizziness,light-headedness,peripheraltingling
Repeatedl normal phsical examination of chest when
smptomatic
Normalpeakexpiratoryow(PEF)orspirometrywhensymptomatic
No response to a trial of asthma therap 19
Clinical features pointing to alternative diagnosis (see Table
3)
Severalfactorsareassociatedwithahigh(orlow)riskofdevelopingpersistingwheezingorasthma
through childhood.15,20 The presence of these factors increases the
probabilit that a
child with respirator smptoms will have asthma.
These factors include:
Ag a pa
The naturalhistoryofwheeze isdependentonageatrst presentation.
Ingeneral,
theearliertheonsetofwheeze,thebettertheprognosis.Cohortstudiesshowabreakpointataround
two ears; most children who present before this age become
asmptomatic b
mid-childhood.6,8,9,21Co-existentatopyisariskfactorforpersistenceofwheezeindependentofageof
presentation.
s
Male sex is a risk factor for asthma in pre-pubertal children.
Female sex is a risk factor for the
persistence of asthma in the transition from childhood to
adulthood.22,23 Bos with asthma
aremorelikelytogrowoutoftheirasthmaduringadolescencethangirls.10,21,22,24-37
svy a qcy pv wzg p
Frequentorsevereepisodesofwheezinginchildhoodareassociatedwithrecurrentwheezethat
persists into adolescence.5,8,13,16,21,26,38,39
2 diAGnosis
-
8/7/2019 Asthma British 2009
10/132
2++
2++
3
British Guideline on the MAnAGeMent of AsthMA
4
Cc apc a
Ahistoryofotheratopicconditionssuchaseczemaandrhinitisincreasestheprobabilityofasthma.Positivetestsforatopyinawheezingchildalsoincreasethelikelihoodofasthma.AraisedspecicIgEtowheat,eggwhite,orinhalantallergenssuchashousedustmiteandcatdander,
predicts later childhood asthma.40,41
Other markers of allergic disease at presentation, such as
positive skin prick tests and a raised
blood eosinophil count, are related to the severit of current
asthma and persistence throughchildhood.
famy y apy
Afamilyhistoryofatopyisthemostclearlydenedriskfactorforatopyandasthmainchildren.The
strongest association is with maternal atop, which is an important
risk factor for the
childhoodonsetofasthmaandforrecurrentwheezingthatpersiststhroughoutchildhood.6,34,37,42,43
Abma g c
Persistent reductions in baseline airwa function and increased
airwa responsiveness duringchildhood are associated with having
asthma in adult life.23
Table 3: Clinical clues to alternative diagnoses in wheezy
children (features not commonly
found in children with asthma)
Paa a amy y Pb ag
Smptoms present from birth or perinatallung problem
Cysticbrosis;chroniclungdiseaseof prematurit; ciliar
dskinesia;developmental anomal
Famil histor of unusual chest disease
Cysticbrosis;neuromusculardisorder
Severe upper respirator tract disease Defect of host defence;
ciliar dskinesia
sympm a g
Persistent moist cough18
Cysticbrosis;bronchiectasis;protracted
bronchitis; recurrent aspiration; hostdefence disorder; ciliar
dskinesia
Excessive vomiting Gastro-oesophagealreux(aspiration)
Dsphagia Swallowingproblems(aspiration)
Breathlessness with light-headedness andperipheral tingling
Hperventilation/panic attacks
Inspirator stridor Tracheal or larngeal disorder
Abnormal voice or cr Larngeal problem
Focal signs in chest Developmental anomal;
post-infectivesndrome; bronchiectasis; tuberculosis
Finger clubbing Cysticbrosis;bronchiectasis
Failure to
thriveCysticbrosis;hostdefencedisorder;gastro-oesophagealreux
ivga
Focal or persistent radiological changes
Developmentalanomaly;cysticbrosis;post-infective disorder;
recurrentaspiration; inhaled foreign bod;bronchiectasis;
tuberculosis
-
8/7/2019 Asthma British 2009
11/132
2+
5
Case detection studies have used smptom questionnaires to screen
for asthma in school-agechildren. A small number of questions -
about current smptoms, their relation to exercise
andtheiroccurrenceatnighthasbeensufcienttodetectasthmarelativelyefciently.11,12,14,44
Theaddition of spirometr11,44 or bronchial hper-responsiveness
testing45 to these questionnairesadds little to making a diagnosis
of asthma in children.
B fc a am c pc avg ama :
pc ky a y a amaca ca aav ag.
Record the basis on which a diagnosis of asthma is
suspected.
2.1.2 ASSESSING THE PROBABLITy OF A DIAGNOSIS OF ASTHMA
Based on the initial clinical assessment it should be possible
to determine the probabilit of adiagnosis of asthma.
With a thorough histor and examination, an individual child can
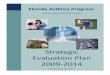
usuall be classed into oneof three groups (see Figure 1):
g pbaby diagnosisofasthmalikely
w pbaby diagnosisotherthanasthmalikely
ma pbaby diagnosisuncertain.
2.1.3 HIGH PROBABILITy OF ASTHMA
In children with a high probabilit of asthma based on the
initial assessment, move straight toa diagnostic trial of
treatment. The initial choice of treatment will be based on an
assessmentof the degree of asthma severit (see section 4).
The clinical response to treatment should be reassessed within
2-3 months. In this group,reserve more detailed investigations for
those whose response to treatment is poor or thosewith severe
disease.19
In children with a high probabilit of asthma:
start a trial of treatment
review and assess response
reserve further testing for those with a poor response.
2.1.4 LOW PROBABILITy OF ASTHMA
Where smptoms, signs or initial investigations suggest that a
diagnosis of asthma is unlikel, (seeTable 2), or the point to an
alternative diagnosis (see Table 3), consider further
investigations.This ma require referral for specialist assessment
(see Table 4).
Reconsideradiagnosisofasthmainthosewhodonotrespondtospecictreatments.
In children with a low probabilit of asthma, consider more
detailed investigation andspecialist referral.
2 diAGnosis
-
8/7/2019 Asthma British 2009
12/132
2+
2+
2+
3
2+
British Guideline on the MAnAGeMent of AsthMA
6
2.1.5 INTERMEDIATE PROBABILITy OF ASTHMA
Insomechildren,andparticularlythosebelowtheageoffourtove,thereisinsufcientevidenceattherstconsultationtomakearmdiagnosisofasthma,butnofeaturestosuggestan
alternative diagnosis. There are several possible approaches to
reaching a diagnosis
inthisgroup.Whichapproachistakenwillbeinuencedbythefrequencyandseverityofthesmptoms.
These approaches include:
Wac wag w vw
Inchildrenwithmild,intermittentwheezeandotherrespiratorysymptomswhichoccuronlywithviralupperrespiratoryinfections(colds),itisoftenreasonabletogivenospecictreatmentand
to plan a review of the child after an interval agreed with the
parents/carers.
ta am w vw
The choice of treatment (for example, inhaled bronchodilators or
corticosteroids) dependson the severit and frequenc of smptoms.
Although a trial of therap with inhaled or oralcorticosteroids is
widel used to help make a diagnosis of asthma, there is little
objectiveevidencetosupportthisapproachinchildrenwithrecurrentwheeze.
Itcanbedifculttoassesstheresponsetotreatmentasanimprovementinsymptomsorlungfunction
ma be due to spontaneous remission. If it is unclear whether a
child has improved,careful observation during a trial of
withdrawing the treatment ma clarif whether a responseto asthma
therap has occurred.
spmy a vby g
Inchildren,as in adults, tests ofairowobstruction, airway
responsivenessandairwayinammationmayprovidesupportforadiagnosisofasthma.12,44
However, normal results ontesting, especiall if performed when the
child is asmptomatic, do not exclude a diagnosis ofasthma.46
Abnormal results ma be seen in children with other respirator
diseases. Measuringlung functionin youngchildren isdifcult and
requires techniqueswhicharenotwidelyavailable.
Aboveveyearsofage,conventionallungfunctiontestingispossibleinmostchildreninmostsettings.Thisincludesmeasuresofairwayobstruction(spirometryandpeakow),reversibilitywith
bronchodilators, and airwa hper-responsiveness.
The relationship between asthma smptoms and lung function tests
including
bronchodilatorreversibilityiscomplex.Asthmaseverityclassiedbysymptomsanduseofmedicinescorrelatespoorl
with single measurements of forced expirator volume in one second
(FEV
1) and other
spirometric indices: FEV1is often normal in children with
persistent asthma.46,47 Serial measures
ofpeakowvariabilityandFEV1
show poor concordance with disease activit and do notreliabl
rule the diagnosis of asthma in or out.47 Measures of gas trapping
(residual volume andthe ratio of residual volume to total lung
capacit, RV/TLC) ma be superior to
measurementsofexpiratoryowatdetectingairwaysobstructionespeciallyinasymptomaticchildren.46,48
AsignicantincreaseinFEV1
(>12% from baseline)49 or PEF after bronchodilator
indicatesreversibleairowobstructionandsupportsthediagnosisofasthma.It
isalsopredictiveofagood response to inhaled corticosteroids.50
However, an absent response to bronchodilatorsdoes not exclude
asthma.51
Between 2-5 ears of age, man children can perform several newer
lung function tests that donot rel on their cooperation or the
abilit to perform a forced expirator manoeuvre. In general,these
tests have not been evaluated as diagnostic tests for asthma. There
is often substantialoverlap between the values in children with and
without asthma.52Ofthetestsavailable,specicairwas resistance
(sRaw), impulse oscillometr (IOS), and measurements of residual
volume(RV) appear the most promising.53 While some of these tests
have been useful in research, theirrole in clinical practice is
uncertain.48,53,54 Most have onl been used in specialist centres
and arenot widel available elsewhere. It is often not practical to
measure variable airwa obstruction
inchildrenbelowtheageofve.
-
8/7/2019 Asthma British 2009
13/132
7
2.1.6 CHILDREN WITH AN INTERMEDIATE PROBABILITy OF ASTHMA AND
EVIDENCE OFAIRWAy OBSTRUCTION
Asthma is the b far the commonest cause of airwas obstruction on
spirometr in children.Obstruction due to other disorders, or due to
multiple causes, is much less common in childrenthan in adults.
Spirometr and other lung function tests, including tests of PEF
variabilit,47 lungvolumes and airwa responsiveness,45 are poor at
discriminating between children with asthmaand those with
obstruction due to other conditions.
In children with an intermediate probabilit of asthma who can
perform spirometr andhave evidence of airwas obstruction, assess
the change in FEV
1or PEF in response to an inhaled
bronchodilator(reversibility)and/ortheresponsetoatrialoftreatmentforaspeciedperiod:
if there issignicant reversibility,or if a treatmenttrial
isbenecial, adiagnosis
ofasthmaisprobable.Continuetotreatasasthma,butaimtondtheminimum
effective dose of therap. At a later point, consider a trial of
reduction or withdrawalof treatment.
ifthereisnosignicantreversibility,andatreatmenttrialisnotbenecial,considertests
for alternative conditions (see Table 3).
2.1.7 CHILDREN WITH AN INTERMEDIATE PROBABILITy OF ASTHMA
WITHOUT EVIDENCE OFAIRWAy OBSTRUCTION
In this group, further investigations, including assessment of
atopic status and bronchodilatorresponsiveness and if possible
tests of airwa responsiveness, should be considered (see
section2.2.1). This is particularl so if there has been a poor
response to a trial of treatment or if smptomsare severe. In these
circumstances, referral for specialist assessment is indicated.
C i c w a ma pbaby ama w ca pm pmy aav vc away bc:
c g apc a, bca vby a, pb, bcayp-pv g mac, c ma.
c pca a.
2.1.8 CHILDREN WITH AN INTERMEDIATE PROBABILITy OF ASTHMA WHO
CANNOT PERFORMSPIROMETRy
Mostchildrenunderveyearsandsomeolderchildrencannotperformspirometry.Inthesechildren,offeratrialoftreatmentforaspecicperiod.Ifthereisclearevidenceofclinicalimprovement,
the treatment should be continued and the should be regarded as
havingasthma (it ma be appropriate to consider a trial of
withdrawal of treatment at a later stage).
Ifthetreatmenttrialisnotbenecial,thenconsidertestsforalternativeconditionsandreferralfor
specialist assessment.
In children with an intermediate probabilit of asthma who cannot
perform spirometr,
offeratrialoftreatmentforaspeciedperiod:
iftreatmentisbenecial,treatasasthmaandarrangeareview
iftreatmentisnotbenecial,stopasthmatreatmentandconsidertestsforalternative
conditions and specialist referral.
2 diAGnosis
-
8/7/2019 Asthma British 2009
14/132
3
2++
2+
2++
British Guideline on the MAnAGeMent of AsthMA
8
2.2 other inVestiGAtions
2.2.1 TESTS OF AIRWAy HyPER-RESPONSIVENESS
The role of tests of airwa responsiveness (airwa hper-reactivit)
in the diagnosis of childhoodasthma is unclear.45,55 For example, a
methacholine challenge test has a much lower sensitivitthan smptoms
in diagnosing asthma in children and onl marginall increases the
diagnosticaccurac after the smptom histor is taken into account.45
However, a negative methacholinetest in children, which has a high
negative predictive value, makes a diagnosis of asthmaimprobable.55
Similarl, a negative response to an exercise challenge test is
helpful in excludingasthma in children with exercise related
breathlessness.56
2.2.2 TEST OF EOSINOPHILIC AIRWAy INFLAMMATION
Eosinophilicinammationinchildrencanbeassessednon-invasivelyusinginducedsputumdifferential
eosinophil count or exhaled nitric oxide concentrations (FENO).
Sputum induction is feasible in school age children.57,58 Higher
sputum eosinophil counts areassociated with more marked airwas
obstruction and reversibilit, greater asthma severit andatop.59 In
children with newl diagnosed mild asthma, sputum eosinophilia is
present anddeclines with inhaled steroid treatment.58 Sputum
induction is possible in approximatel 75%
of children tested, but it is technicall demanding and time
consuming and at present remainsa research tool.
It is feasible to measure FENO in unsedated children from the
age of 3-4 ears.60 A raised FENO
isneitherasensitivenoraspecicmarkerofasthmawithoverlapwithchildrenwhodonothaveasthma.61
FENO is closel linked with atopic status, age and height.62,63 In
some studies, FENOcorrelated better with atopic dermatitis and
allergic rhinitis than with asthma. It is not closellinked with
underling lung function. FENO could not differentiate between
groups once atopwas taken into account.64 Home measurements of FENO
have a highl variable relationship withother measures of disease
activit and var widel from da to da.65
Atpresent,thereisinsufcientevidencetosupportaroleformarkersofeosinophilicinammationin
the diagnosis of asthma in children. The ma have a role in
assessing severit of disease
or response to treatment.
2.2.3 TESTS OF ATOPy
Positive skin
tests,66bloodeosinophilia4%10,oraraisedspecicIgEtocat,dogormite,67,68increasetheprobabilityofasthmainachildwithwheeze,particularlyinchildrenoverveears
of age.66It
isimportanttorecognisethatnon-atopicwheezingisasfrequentasatopicwheezinginschool-agechildren.69
2.2.4 CHEST X-RAy
A stud in primar care in children age 0-6 ears concluded that a
chest X-ra (CXR), in theabsence of a clinical indication, need not
be part of the initial diagnostic work up.70
Reserve chest X-ras for children with severe disease or clinical
clues suggesting otherconditions.
-
8/7/2019 Asthma British 2009
15/132
9
2.3 suMMArY
fc a am c pc avg ama :
presence of ke features in the histor and clinical
examination
careful consideration of alternative diagnoses.
rc ba wc ag ama pc.
Using a structured questionnaire ma produce a more standardised
approach to the recordingof presenting clinical features and the
basis for a diagnosis of asthma.
1. i c w a g pbaby ama:
move straight to a trial of treatment
reserve further testing for those with a poor response.
2. i c w a w pbaby ama:
consider more detailed investigation and specialist
referral.
3. i c w a ma pbaby ama w ca pm pmya av vc away bc, a vby a/ a a
am
foraspeciedperiod:
ifthereisreversibility,oriftreatmentisbenecial,treatasasthma
ifthereisinsignicantreversibility,and/ortreatmenttrialisnotbenecial,consider
tests for alternative conditions.
4. i c w a ma pbaby ama w ca pm pmy, aav vc away bc, c g apc a,
bcavby a, pb, bca yp-pv g mac c.
5. i c w a ma pbaby ama, w ca pm pmy,
considertestingforatopicstatusandofferingatrialoftreatmentforaspeciedperiod:
iftreatmentisbenecial,treatasasthma
iftreatmentisnotbenecial,stopasthmatreatment,andconsidertestsforalternativeconditions
and specialist referral.
Table 4: Indications for specialist referral in children
Diagnosis unclear or in doubt
Smptoms present from birth or perinatal lung problem
Excessive vomiting or posseting
Severe upper respirator tract infection
Persistent wet or productive cough
Famil histor of unusual chest disease
Failure to thrive
Nasal polps
Unexpectedclinicalndingsegfocalsigns,abnormalvoiceorcry,dysphagia,
inspirator stridor
Failure to respond to conventional treatment (particularl
inhaled corticosteroids above400 mcg/da or frequent use of steroid
tablets)
Parental anxiet or need for reassurance
2 diAGnosis
-
8/7/2019 Asthma British 2009
16/132
British Guideline on the MAnAGeMent of AsthMA
10
Clinical assessment
Considerreferral
Continue
treatment andfind minimumeffective dose
Assess compliance and
inhaler technique.Consider further
investigation and/or referral
Continuetreatment
Further investigation.Consider referral
+VE -VE
HIGH PROBABILITY:diagnosis of asthma
likely
INTERMEDIATEPROBABILITY:
diagnosis uncertainor poor response to
asthma treatment
LOW PROBABILITY:other diagnosis likely
Consider tests oflung function*
and atopy
Response? Response?
Investigate/treat othercondition
Trial of asthmatreatment
Yes No No Yes
* Lung function tests include spirometry before and after
bronchodilator (test of airway reversibility) andpossible exercise
or methacholine challenge (tests of airway responsiveness).Most
children over the age of 5 years can perform lung function
tests.
Figure 1: Presentation with suspected asthma in children
-
8/7/2019 Asthma British 2009
17/132
11
2.4 diAGnosis in Adults
The diagnosis of asthma is based on the recognition of a
characteristic pattern of smptoms andsigns and the absence of an
alternative explanation for them (see Table 5). The ke is to take
acareful clinical histor. In man cases this will allow a reasonabl
certain diagnosis of asthma,or an alternative diagnosis, to be
made. If asthma does appear likel, the histor should alsoexplore
possible causes, particularl occupational.
In view of the potential requirement for treatment over man
ears, it is important even inrelativel clear cut cases, to tr to
obtain objective support for the diagnosis. Whether or notthis
should happen before starting treatment depends on the certaint of
the initial diagnosis andthe severit of presenting smptoms.
Repeated assessment and measurement ma be
necessarbeforeconrmatoryevidenceisacquired.
Conrmationhingesondemonstrationofairowobstructionvaryingovershortperiodsoftime.Spirometr,
which is now becoming more widel available, is preferable to
measurement ofpeakexpiratoryowbecauseitallowscleareridenticationof
airowobstruction,and theresults are less dependent on effort. It
should be the preferred test where available (althoughsome training
is required to obtain reliable recordings and to interpret the
results). Of note, anormal spirogram (or PEF) obtained when the
patient is not smptomatic does not exclude thediagnosis of
asthma.
Results from spirometr are also useful where the initial histor
and examination leave genuineuncertaint about the diagnosis. In
such cases, the differential diagnosis and approach
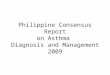
toinvestigationisdifferentinpatientswithandwithoutairowobstruction(see
Figure 2 andTable 6). In patients with a normal or near-normal
spirogram when smptomatic, potentialdifferential diagnoses are
mainl non-pulmonar; 71,72 these conditions do not respond to
inhaledcorticosteroids and bronchodilators. In contrast, in
patients with an obstructive spirogram thequestion is less whether
the will need inhaled treatment but rather exactl what form andhow
intensive this should be.
Othertestsofairowobstruction,airwayresponsivenessandairwayinammationcanalsoprovide
support for the diagnosis of asthma, but to what extent the results
of the tests alter theprobabilit of a diagnosis of asthma has not
been clearl established, nor is it clear when these
tests are best performed.
2 diAGnosis
-
8/7/2019 Asthma British 2009
18/132
British Guideline on the MAnAGeMent of AsthMA
12
Table 5: Clinical features in adults that inuence the
probability that episodic respiratorysymptoms are due to asthma
fa a ca pbaby ama
Morethanoneofthefollowingsymptoms:wheeze,breathlessness,chesttightnessandcough,
particularl if:
smptoms worse at night and in the earl morning
smptoms in response to exercise, allergen exposure and cold
air
smptoms after taking aspirin or beta blockers
Histor of atopic disorder
Famil histor of asthma and/or atopic disorder
Widespreadwheezeheardonauscultationofthechest
Otherwise unexplained low FEV1
or PEF (historical or serial readings)
Otherwise unexplained peripheral blood eosinophilia
fa a w pbaby ama
Prominentdizziness,light-headedness,peripheraltingling
Chronicproductivecoughintheabsenceofwheezeorbreathlessness
Repeatedl normal phsical examination of chest when
smptomatic
Voice disturbance
Smptoms with colds onl
Signicantsmokinghistory(ie>20pack-years)
Cardiac disease
Normal PEF or spirometr when smptomatic*
* A normal spirogram/spirometr when not smptomatic does not
exclude the diagnosis of asthma. Repeated
measurements of lung function are often more informative than a
single assessment.
Baseinitialdiagnosisonacarefulassessmentofsymptomsandameasureofairowobstruction:
in patients with a high probabilit of asthma move straight to a
trial of treatment.Reserve further testing for those whose response
to a trial of treatment is poor.
in patients with a low probabilit of asthma, whose smptoms are
thought to be dueto an alternative diagnosis, investigate and
manage accordingl. Reconsider thediagnosis of asthma in those who
do not respond.
the preferred approach in patients with an intermediate
probabilit of having asthmais to carr out further investigations,
including an explicit trial of treatments for
aspeciedperiod, before conrminga diagnosis
andestablishingmaintenance
treatment.
d
Spirometryisthepreferredinitialtesttoassessthepresenceandseverityofairowbc.
-
8/7/2019 Asthma British 2009
19/132
13
2.4.1 FURTHER INVESTIGATION OF PATIENTS WITH AN INTERMEDIATE
PROBABILITy OFASTHMA
Pa w away bc
Testsofpeakexpiratoryowvariability,lungvolumes,gastransfer,airwayhyper-responsivenessandairwayinammationareoflimitedvalueindiscriminatingpatientswithestablishedairowobstructionduetoasthmafromthosewhoseairowobstructionisduetootherconditions.73-
76Patientsmayhavemorethanonecauseofairowobstruction,whichcomplicatestheinterpretation
of an test. In particular, asthma and chronic obstructive pulmonar
disease(COPD) commonl coexist.
Offer patients with airwas obstruction and intermediate
probabilit of asthma a
reversibilitytestand/oratrialoftreatmentforaspeciedperiod:
ifthereissignicantreversibility,orifatreatmenttrialisclearlybenecialtreatas
asthma
ifthereisinsignicantreversibilityanda
treatmenttrialisnotbenecial,considertests for alternative
conditions.*
Pa w away bc
In patients with a normal or near-normal spirogram it is more
useful to look for evidence
ofairwayhyper-responsivenessand/orairway inammation 71,77-79 These
tests are sensitive sonormal results provide the strongest evidence
against a diagnosis of asthma.
In patients without evidence of airwas obstruction and with an
intermediate probabilitof asthma, arrange further investigations*
before commencing treatment.
* see section 2.5 for more detailed information on further
tests
2 diAGnosis
-
8/7/2019 Asthma British 2009
20/132
British Guideline on the MAnAGeMent of AsthMA
14
Clinical assessment including spirometry
(or PEF if spirometry not available)
Continue
treatment
Assess compliance andinhaler technique.
Consider furtherinvestigation and/or referral
Continue
treatment
Further investigation.
Consider referral
HIGH PROBABILITY:
diagnosis of asthma
likely
LOW PROBABILITY:
other diagnosis likely
Response? Response?
Investigate/
treat othercondition
Trial of
treatment*
Yes No No Yes
Figure 2: Presentation with suspected asthma in adults
Presentation with suspected asthma
FEV1
/ FVC0.7
INTERMEDIATE
PROBABILITY:
diagnosis uncertain
* See section 2.5.1 See Table 6
-
8/7/2019 Asthma British 2009
21/132
15
Table 6: Differential diagnosis of asthma in adults, according
to the presence or absence ofairow obstruction (FEV
1/FVC 1 x 10 9/l)
Poor response to asthma treatment
Severe asthma exacerbation
2 diAGnosis
-
8/7/2019 Asthma British 2009
22/132
2+
2+
British Guideline on the MAnAGeMent of AsthMA
16
2.5 further inVestiGAtions thAt MAY Be useful in PAtients With
An
interMediAte ProBABilitY of AsthMA
Three studies have looked at tests to discriminate patients with
asthma from those with conditionsthat are commonl confused with
asthma.71,77,79 These studies provide a basis for evaluating
thediagnosticvalueofdifferenttests.Table7summarisesthesensitivityandspecicityofdifferentndingsoninvestigation.Asnotallstudiesincludedpatientswithuntreatedasthma,thesevalues
ma underestimate the value of the investigations in clinical
practice, where man patients willbe investigated before treatment
is started. The diagnostic value of testing ma also be greaterwhen
more than one test is done or if there are previous lung function
results available in thepatients notes. The choice of test will
depend on a number of factors including severit ofsmptoms and local
availabilit of tests.
Analternativeandpromisingapproachtotheclassicationofairwaysdiseaseistousetestswhichbest
identif patients who are going to respond to corticosteroid
therap.78,80 A raised sputumeosinophil count and an increased
exhaled nitric oxide concentration (FENO) are more closelrelated to
corticosteroid response than other tests in a variet of clinical
settings.78,81-83
Thereisalsoevidencethatmarkersofeosinophilicairwayinammationareofvalueinmonitoringthe
response to corticosteroid treatment.84-86 More experience with
these techniques and moreinformation on the long term response to
corticosteroid in patients who do not have a raised
sputum eosinophil count or FENO is needed before this approach
can be recommended.Table 7: Estimates of sensitivity and specicity
of test results in adults with suspected asthmaand normal or
near-normal spirometric values.71,77,79
t nma ag Vay
vy specicity
Methacholine PC20 >8 mg/ml High Medium
Indirect challenges* varies Medium# High
FENO
-
8/7/2019 Asthma British 2009
23/132
2+
17
A >400 ml improvement in FEV1to either
2agonists or corticosteroid treatment trials strongl
suggests underling asthma. Smaller improvements in FEV1
are less discriminator71 and adecision on continuation of
treatment should be based on objective assessment of smptomsusing
validated tools (see Table 8). Trials of treatment withdrawal ma be
helpful where thereis doubt.
C A feV1
( Pef) a/ ympm:
b a a 400 mcg a abam pa w agc cay
andairowobstructionpresentatthetimeofassessment
pa, a cmp p a abam, a a cc(200 mcg twice daily beclometasone
equivalent for6-8 weeks) a p (30 mg once daily for 14 days).
2.5.2 PEAK EXPIRATORy FLOW MONITORING
PEF should be recorded as the best of three forced expirator
blows from total lung capacitwith a maximum pause of two seconds
before blowing.88 The patient can be standing or sitting.Further
blows should be done if the largest two PEF are not within 40
l/min.88
PEFisbestusedtoprovideanestimateofvariabilityofairowfrommultiplemeasurements
made over at least two weeks. Increased variabilit ma be evident
from twice dail readings.More frequent readings will result in a
better estimate 89 but the improved precision is likel tobe
achieved at the expense of reduced patient compliance.90
PEF variabilit is best calculated as the difference between the
highest and lowest PEF expressedas a percentage of either the mean
or highest PEF.91-93
The upper limit of the normal range for the amplitude % highest
is around 20% using four ormore PEF readings per da 91,93,94 but ma
be lower using twice dail readings.95 Epidemiologicalstudies have
shown sensitivities of between 19 and 33% for identifing
phsician-diagnosedasthma. 92,96
PEF variabilit can be increased in patients with conditions
commonl confused with
asthma71,73sothespecicityofabnormalPEFvariabilityislikelytobelessinclinicalpracticethanit
is in population studies.PEF records from frequent readings
taken at work and awa from work are useful whenconsidering a
diagnosis of occupational asthma (see section 7.8). A computer
generated analsisof occupational records which provides an index of
the work effect is available.97
Peakowrecordsshouldbeinterpretedwithcautionandwithregardtotheclinicalcontext.
The are more useful in the monitoring of patients with established
asthma thanin making the initial diagnosis.
2.5.3 ASSESSMENT OF AIRWAy RESPONSIVENESS
Tests of airwa responsiveness have been useful in research but
are not et widel available ineverda clinical practice. The most
widel used method of measuring airwa responsiveness
relies on measuring response in terms of change in FEV1 a set
time after inhalation of increasingconcentrations of histamine or
methacholine. The agent can be delivered b
breath-activateddosimeter, via a nebuliser using tidal breathing,
or via a hand held atomiser.98 The response
isusuallyquantiedastheconcentration(ordose)requiredtocausea20%fallinFEV
1(PC20 or
PD20) calculated b linear interpolation of the log concentration
or dose-response curve.
Communit studies in adults have consistentl shown that airwa
responsiveness has aunimodal distribution with between 90 and 95%
of the normal population having a histamineor methacholine PC20 of
>8 mg/ml (equivalent to a PD20 of >4 micromoles).92,99,100
This valuehas a sensitivit of between 60-100% in detecting
phsician-diagnosed asthma.92,96,99,100
2 diAGnosis
-
8/7/2019 Asthma British 2009
24/132
British Guideline on the MAnAGeMent of AsthMA
18
In patients with normal or near-normal spirometric values,
assessment of airwa responsivenessis signicantlybetterthan
othertests indiscriminatingpatientswithasthma frompatientswith
conditions commonl confused with asthma (see Table 6).71,77 In
contrast, tests of
airwaresponsivenessareoflittlevalueinpatientswithestablishedairowobstructionasthespecicityis
low.73,76
Other potentiall helpful constrictor challenges include indirect
challenges such as inhaledmannitol and exercise.101 A positive
response to these indirect stimuli (ie a >15% fall in FEV
1
)isaspecicindicatorofasthmabutthetestsarelesssensitivethantestsusingmethacholineand
histamine, particularl in patients tested while on
treatment.101,102
2.5.4 TESTS OF EOSINOPHILIC AIRWAy INFLAMMATION
Eosinophilicairwayinammationcanbeassessednon-invasivelyusingtheinducedsputumdifferential
eosinophil count or the exhaled nitric oxide concentration
(FENO).103,104 A raisedsputum eosinophil count (>2%) or FENO
(>25 ppb at 50 ml/sec) is seen in 70-80% of patientswith
untreated
asthma.74,103Neitherndingisspecictoasthma:30-40%ofpatientswithchroniccough
82,105,106 and a similar proportion of patients with COPD81 have
abnormal results. There
isgrowingevidencethatmeasuresofeosinophilicairwayinammationaremorecloselylinkedto
a positive response to corticosteroids than other measures even in
patients with diagnosesother than asthma. 81,83,105
Experience with induced sputum and FENO is limited to a few
centres and more research needsto be done before an recommendations
can be made.
C In patients inwhom thereisdiagnostic uncertainty andnoevidence
ofairowbc a am, away pv wv pb.
2.6 MonitorinG AsthMA
In the majorit of patients with asthma smptom-based monitoring
is adequate. Patients achievingcontrol of smptoms with treatment
have a low risk for exacerbations.107
Table 8 summarises the methodolog, measurement characteristics
and interpretation of some
of the validated tools used to assess smptoms and other aspects
of asthma. Some measuresprovide information about future risk (ie
sputum eosinophil count, airwa responsiveness andFENO) rather than
immediate clinical control. Risk reduction, eg minimising future
adverseoutcomes such as exacerbations and accelerated decline in
lung function, is also a goal ofasthma management.
Amanagementstrategythatcontrolseosinophilicairwayinammation
84-86 or airwa hper-responsiveness108 results in better control of
exacerbations than one which controls
immediateclinicalmanifestations.Thebenetsofthismoreintensiveapproacharegreaterinpatientswithsevere
asthma, when exacerbations can occur frequentl and unpredictabl.
More research isneeded to assess the relative roles of the
different measures and to address the feasibilit andcost of
incorporating them into monitoring protocols before the can be
recommended morewidel.
-
8/7/2019 Asthma British 2009
25/132
19
2.6.1 MONITORING IN PRIMARy CARE
Asthma is best monitored in primar care b routine clinical
review on at least an annual basis(see section 8.1.2).
The factors that should be monitored and recorded include:
smptomatic asthma control: best assessed using directive
questions such as the RCP 3questions,109 or the Asthma Control
Questionnaire or Asthma Control Test (see Table 8),
sincebroadnon-specicquestionsmayunderestimatesymptoms
lung function, assessed b spirometr or b PEF. Reduced lung
function compared topreviousl recorded values ma indicate current
bronchoconstriction or a long term declinein lung function and
should prompt detailed assessment
exacerbations, oral corticosteroid use and time off work or
school since last assessment
inhaler technique (see section 5)
compliance (see section 9.2)whichcanbeassessed
byreviewingprescriptionrellfrequenc
bronchodilatorreliancewhichcanbeassessedbyreviewingprescriptionrellfrequency
possession of and use of self management plan/personal action
plan (see section 9.1).
2 diAGnosis
-
8/7/2019 Asthma British 2009
26/132
British Guideline on the MAnAGeMent of AsthMA
20
Table 8: Summary of tools that can be used to assess asthma.
Mam MgyMamcaacc
Cmm
Spirometr110, 111 Widel available.
Enables cleardemonstration ofairowobstruction.
FEV1
largelindependent ofeffort and highlrepeatable.
Less applicable inacute severe asthma.Onl assesses oneaspect of
the diseasestate.
Normal rangeswidel available and
robust.
Short term (20minute) 95% rangefor repeat measureof FEV
160 l/min increasein PEF suggestedas best criteria
fordeningreversibility.
Normal range of PEFvariabilitydenedasamplitude % highest
-
8/7/2019 Asthma British 2009
27/132
21
Mam MgyMamcaacc
Cmm
Roal College ofPhsicians (RCP)3 Questions109
yes/no or gradedresponse to thefollowing threequestions:
In the last week (ormonth)
1. Have ou haddifcultysleepingbecause of ourasthma
smptoms(including cough)?
2. Have ou hadour usual asthmasmptoms during
theday(cough,wheeze,
chest tightness orbreathlessness)?
3. Has our asthmainterfered with ourusual activities
(eghousework, work/school etc)?
No to all questionsconsistent withcontrolled asthma.
Not well validated.
Simplicit isattractive for use inda to da clinical
practice.
Asthma ControlQuestionnaire113-115
Response to 7questions, 5 relatingto smptoms, 1rescue treatment
useand 1 FEV
1
.
Response usuallassessed over thepreceding week.
Shortened,vequestion smptomonl questionnaire isjust as
valid.
Well controlled0.75,inadequatelycontrolled1.5.95% range for
repeatmeasure +/- 0.36.
Minimal importantdifference 0.5.
Well validatedcomposite scoringsstem with a strongbias to
smptoms.
Could be used toassess responseto longer termtreatment
trials.
Shortenedve-pointquestionnaire isprobabl best forthose with
normal ornear normal FEV
1.
Asthma ControlTest (ACT)116, 117
Response to 5questions, 3 related
to smptoms, 1medication use and1 overall control. 5point
response score
Well controlled>19.
Within subjectintraclass correlationcoefcient0.77.
95% range forrepeat measure andminimall clinicallimportant
differencenotdened.
Could be used toassess response
to longer termtreatment trials,particularl in thosewith normal
or near-normal spirometricvalues.
95% range forrepeat measure andminimall clinicallimportant
differenceneedtobedened.
2 diAGnosis
-
8/7/2019 Asthma British 2009
28/132
British Guideline on the MAnAGeMent of AsthMA
22
Mam MgyMamcaacc
Cmm
Mini AsthmaQualit of LifeQuestionnaire(AQLQ)114, 118
Response to 15questions in 4domains (smptoms,activit
limitations,
emotional functionand environmentalstimuli).
Response usuallassessed over thepreceding week.Closel relatedto
larger 32-itemasthma qualit of lifequestionnaire.
95% range for repeatmeasure +/- 0.36.
Minimal importantdifference 0.5.
Well validatedqualit of lifequestionnaire.
Could be used to
assess responseto longer termtreatment trials.
Airwaresponsiveness98,108
Onl available inselected secondarcare facilities.
Responsive tochange (particularlindirect challengessuch as
inhaledmannitol).
Less of a ceilingeffect.
Not applicable insevere asthma or in
acute severe asthma
Normalmethacholine PC20
> 8 mg/ml.
95% range for repeatmeasure +/- 1.5-2doubling doses.
Has not been widelused to monitordisease and assesstreatment
responses.
Some evidencethat using airwaresponsiveness as anadditional
measurefor monitoringasthma results in areduction in
asthmaexacerbations andimproved airwa
patholog.
-
8/7/2019 Asthma British 2009
29/132
23
Mam MgyMamcaacc
Cmm
Exhaled nitricoxide (FENO)78, 85,103, 119, 120
Not widelavailable.
Monitors stillexpensive,
although expectthe technolog tobecome cheaper andmore
widespread.
Measurementscan be obtained inalmost all adultsand children over
5ears.
Immediate resultsare available.
Reasonabl closerelationshipbetween FENO andeosinophilic
airwainammation,whichis independentof gender, age,atop and
inhaledcorticosteroid use.
Relationship is lostin smokers.
Not closel relatedto other measures ofasthma morbidit.
Normal range 50 ppb highlpredictive ofeosinophilic
airwainammation.
50 ppb) verpredictive of apositive response to
corticosteroids.Use of FENO toguide corticosteroidtreatment has
beenshown to result inanon-signicant25% reductionin
exacerbationswith 40% lesscorticosteroid.
Low FENO (
-
8/7/2019 Asthma British 2009
30/132
-
8/7/2019 Asthma British 2009
31/132
1+
2+
1+
25
3.1.2 FOOD ALLERGEN AVOIDANCE
Sensitisation to foods, particularl eggs, frequentl precedes the
development of aeroallergand subsequent asthma.135 Food allergen
avoidance in pregnanc and postnatall has not beenshown to prevent
the later development of asthma.136 Allergen avoidance during
pregnancma adversel affect maternal, and perhaps fetal,
nutrition.137 High-dose food allergen exposureduring pregnanc ma
reduce subsequent sensitisation rates b inducing tolerance.138
B
Intheabsenceofanyevidenceofbenetandgiventhepotentialforadverseeffects,maa
ag avac g pgacy a aca cmma a agy pvg c ama.
3.1.3 BREAST FEEDING
A sstematic review of observational studies on the allerg
preventive effects of breast feedingindicates that it is effective
for all infants irrespective of allergic heredit. The preventive
effectis more pronounced in high-risk infants provided the are
breast fed for at least four
months.139However,notallstudieshavedemonstratedbenetandinalargebirthcohorttherewasnoprotective
effect against atop and asthma and mabe even an increase in
risk.140
Observational studies have the potential to be confounded b, for
example, higher rates of breast
feeding in atopic families, and taking this into account, the
weight of evidence is in favour ofbreast feeding as a preventive
strateg.
C
Breastfeedingshouldbeencouragedforitsmanybenets,andasitmayalsohaveapa
pcv c a ay ama.
3.1.4 MODIFIED INFANT MILK FORMULAE
Trialsofmodiedmilkformulaehavenotincludedsufcientlylongfollowuptoestablishwhetherthereisanyimpactonasthma.ACochranereviewidentiedinconsistenciesinndingsand
methodological concerns amongst studies, which mean that hdrolsed
formulae cannotcurrentl be recommended as part of an asthma
prevention strateg.141 A review of the use
ofsoyformulaefoundnosignicanteffectonasthmaoranyotherallergicdisease.142
Intheabsenceofanyevidenceofbenetfromtheuseofmodiedinfantmilkformulaeitis
pb cmm a a agy pvg c ama.
3.1.5 WEANING
Thereareconictingdataontheassociationbetweenearlyintroductionofallergenicfoodsintotheinfantdietandthesubsequentdevelopmentofallergyandatopiceczema.Noevidencewasidentiedinrelationtoasthma.143
In one stud late introduction of egg was associated with
anon-signicantincreaseinpre-schoolwheezing.144
i abc vc cm a ama cmma modiedweaningcanbemade.
3 non-PhArMAColoGiCAl MAnAGeMent
-
8/7/2019 Asthma British 2009
32/132
1+
2+
British Guideline on the MAnAGeMent of AsthMA
26
3.1.6 NUTRITIONAL SUPPLEMENTATION - FISH OILS
Fish oils have a high level of omega-3 polunsaturated fatt acids
(n-3PUFAs). Western dietshave a low intake of n-3 PUFAs with a
corresponding increase in intake of n-6 PUFAs. Thischange has been
associated with increasing rates of allergic disease and asthma.
143
Tworandomisedcontrolledstudieshaveinvestigatedearlylifeshoildietarysupplementationinrelation
to asthma outcomes in children at high risk of atopic disease (at
least one parent orsibling had atop with or without asthma). In a
stud, powered onl to detect differences
incordblood,maternaldietaryshoilsupplementationduringpregnancywasassociatedwithreduced
ctokine release from allergen stimulated cord blood mononuclear
cells.
However,effectsonclinicaloutcomesatoneyear,inrelationtoatopiceczema,wheezeandcough,weremarginal.145Inasecondstudy,shoilsupplementationcommencinginearlyinfancywithorwithoutadditionalhousedustmiteavoidance,wasassociatedwithasignicantreductioninwheezeat18monthsofage.Byveyearsofageshoilsupplementationwasnotassociatedwith
effects on asthma or other atopic diseases.146
Intheabsenceofanyevidenceofbenetfromtheuseofshoilsupplementationinpregnancy
pb cmm a a agy pvg c ama.
3.1.7 OTHER NUTRIENTS
A number of observational studies have suggested an increased
risk of subsequent asthmafollowing reduced (maternal) intakes of
selenium (based on umbilical cord levels),147or vitaminE based on
maternal pregnanc intake.148 No intervention studies in relation to
selenium
orvitaminEhaveyetbeenconductedandoverallthereisinsufcientevidencetomakeanyrecommendations
on maternal dietar supplementation as an asthma prevention
strateg.143Observational studies suggest that intervention trials
are warranted.
3.1.8 MICROBIAL EXPOSURE
Thehygienehypothesissuggestedthatearlyexposuretomicrobialproductswouldswitchoff
allergic responses thereb preventing allergic diseases such as
asthma. The hpothesis issupported b some epidemiological studies
comparing large populations who have or havenot had such
exposure.149,150
Theconceptissometimesdescribedasthemicrobialexposurehypothesis.Adoubleblindplacebo
controlled trial of the probiotic lactobacillus GG given to mothers
resulted in a
reducedincidenceofatopiceczemaintheirchildrenbuthadnoeffectonIgEantibodyorallergicskintestresponses.Thesmallsamplesizeandshortfollowupinthisstudylimititsinterpretation.151Othertrialsofarangeofprobioticsandprebioticsarenowinprogress.Thereremainsinsufcientunderstandingoftheecologyofgutoraininfancyinrelationtooutcomes.Bido-bacteriamaybe
more important than lactobacilli in reducing susceptibilit to
allergic disease.152
Thereisinsufcientevidencetoindicatethattheuseofdietaryprobioticsinpregnancyc
cc c ama.
This is a ke area for further work with longer follow up to
establish outcomes in relation toasthma.
3.1.9 AVOIDANCE OF TOBACCO SMOKE AND OTHER AIR POLLUTANTS
No evidence has been found to support a link between exposure to
environmental tobaccosmoke (ETS) or other air pollutants and the
induction of allerg.
Thereisanincreasedriskofinfantwheezingassociatedwithmaternalsmokingduringpregnancywhich
adversel affects infant lung function.153-156 Evidence suggests
that earl life ETS exposure isassociated with later persistent
asthma157,158 with a strong interaction with genetic
polmorphismswhich affect antioxidant activit.159
B Pa a pa--b b av may av c wc mkg a c cg ca wzg acy a ca k
pama.
-
8/7/2019 Asthma British 2009
33/132
34
2+
1++
2+
27
The limited data on antenatal or earl life exposure to other
pollutants suggest similar
effectstothoseforETS,namelyincreasedinfantwheezing,enhancedbyadditionalETSexposureand
antioxidant gene variations.160-162 There is one small stud
suggesting that vitamin Csupplementation will modif the combined
effects of genetic polmorphisms and pollution onlung function in
children with asthma.163 Further research is required before
recommendationsfor practice can be made.
3.1.10 IMMUNOTHERAPy
Three observational studies with contemporaneous untreated
controls in over 8,000 patientshave shown that allergen
immunotherap in individuals with a single allerg reduces thenumbers
subsequentl developing new allergic sensitisation over a three to
four ear followup.164-166 One trial compared pollen allergen
immunotherap in children with allergic rhinitiswith contemporaneous
untreated controls and showed a lower rate of onset of asthma
duringthree ears of treatment.167 This effect was sustained for two
ears after stopping the therap.168More studies are required to
establish whether immunotherap might have a role in
primarprophlaxis.
3.1.11 IMMUNISATION
Inkeepingwiththemicrobialexposurehypothesissomestudieshavesuggestedanassociationbetween
tuberculin responsiveness and subsequent reduced prevalence of
allerg, impling aprotective effect of BCG. At present, it is not
possible to disentangle whether poor tuberculinresponsiveness
represents an underling defect which increases the risk of allerg
and asthmaor whether the immunisation itself has a protective
effect.169
Investigation of the effects of an other childhood immunisation
suggests that at worst
thereisnoinuenceonsubsequentallergicdiseaseandmaybesomeprotectiveeffectagainstthedevelopment
of asthma.170
C A c mma pc may a vc aav c cc ama.
3.2 seCondArY non-PhArMAColoGiCAl ProPhYlAxis
3.2.1 HOUSE DUST MITE AVOIDANCE
Increased allergen exposure in sensitised individuals is
associated with an increase in asthmasmptoms, bronchial
hper-responsiveness and deterioration in lung function.127,171,172
However,evidence that reducing allergen exposure can reduce
morbidit and/or mortalit in asthma
istenuous.Inuncontrolledstudies,childrenandadultshavederivedbenetfromremovaltoalowallergenenvironmentsuchasoccursathighaltitude,althoughthebenetsseenarenotnecessaril
attributable to allergen avoidance alone.173
Cochrane reviews on house dust mite control measures in a normal
domestic environmenthave concluded that chemical and phsical
methods aimed at reducing exposure to housedust mite allergens
cannot be recommended.174 Subsequent studies involving large
numbersof patients tend to support this conclusion.175,176
Heterogeneit between studies with regardto the intervention and
monitoring of outcomes makes interpretation of the sstematic
reviewdifcult.
Studiesofmattressbarrier systemshavesuggestedthat benets in
relation to treatmentrequirements for asthma and lung function can
occur.177,178 Larger and more carefull conductedcontrolled studies
emploing combinations of house dust mite reduction strategies are
required.At present house dust mite control measures do not appear
to be a cost-effective method
ofachievingbenet,althoughitisrecognisedthatmanyfamiliesareverycommittedtoattemptsto
reduce exposure to triggers.
3 non-PhArMAColoGiCAl MAnAGeMent
-
8/7/2019 Asthma British 2009
34/132
2+
3
British Guideline on the MAnAGeMent of AsthMA
28
Measures to decrease house dust mites have been shown to reduce
numbers of house dustmites, but have not been shown to have an
effect on asthma severit.
Families with evidence of house dust mite allerg and who wish to
tr mite avoidancemight consider the following:
complete barrier bed-covering sstems
removal of carpets
removal of soft tos from bedhigh temperature washing of bed
linen
acaricides to soft furnishings
goodventilationwithorwithoutdehumidication.
3.2.2 OTHER ALLERGENS
Animal allergens, particularl from cat and dog, are potent
provokers of asthma
smptoms.Thereportedeffectsofremovalofpetsfromhomesareparadoxical,witheithernobenetfor
asthma179,180 or a potential for continued high exposure to induce
a degree of
tolerance.181Inhomeswherethereisnocatbutstilldetectablecatallergen,theremaybeabenetfromintroducingadditionalavoidancemeasures
suchasairltersand highefciencyvacuum
cleaners for cat allergic patients.182,183
Although fungal exposure has been strongl associated with
hospitalisation and
increasedmortalityinasthma,nocontrolledtrialshaveaddressedtheefcacyofreductionoffungalexposure
in relation to control of asthma. Cockroach allerg is not a common
problem in the
UKandstudiesofattemptstoavoidthisallergenelsewherehaveproducedconictingresults.184
Studies of individual aeroallergen avoidance strategies show
that single interventions
havelimitedornobenet.Amultifacetedapproachismorelikelytobeeffectiveifitaddressesallthe
indoor asthma triggers. Such approaches ma even be cost
effective.185 A strateg with apotential impact on mites, mould
allergens and indoor pollutants is the use of a
mechanicalventilation sstem to reduce humidit and increase indoor
air exchange. The onl trial
thathasassessedthisinacontrolledfashionfailedtodemonstrateanysignicanteffects,butthenumbers
involved were small.120 A sstematic review of this topic concluded
that more research
is required.186
3.3 other enVironMentAl fACtors
3.3.1 SMOKING
Direct or passive exposure to cigarette smoke adversel affects
qualit of life, lung function,need for rescue medications for acute
episodes of asthma and long term control with
inhaledsteroids.187-190
There are ver few trials which have assessed smoking cessation
in relation to asthma control.Two studies have demonstrated
decreases in childhood asthma severit when parents wereable to stop
smoking.191,192 One stud in adults with asthma suggested that
smoking cessation
improvedasthma-specicqualityoflife,symptomsanddrugrequirements.
193 Intervention toreduce smoking has had disappointing
outcomes.194,195 It is likel that more intensive interventionwill
be required to achieve meaningful outcomes.196
Uptake of smoking in teenagers increases the risks of persisting
asthma. One stud showeda doubling of risk for the development of
asthma over six ears in 14 ear old children whostarted to
smoke197(see section 4.2.4 for effect of smoking on treatment).
C Pa w ama b av ab ag mkg mva c w ama a apppa pp p mkg.
-
8/7/2019 Asthma British 2009
35/132
1++
2+
3
1++
29
3.3.2 AIR POLLUTION
Challenge studies demonstrate that various pollutants can
enhance the response of patients withasthma to allergen
inhalation.198,199 Time-series studies suggest that air pollution
ma provokeacute asthma attacks or aggravate existing chronic asthma
although the effects are ver muchless than those with infection or
allergen exposure.200,201 While it might seem likel that movingfrom
a highl polluted environment might help, in the UK, asthma is more
prevalent in 12-14ear olds in non-metropolitan rather than
metropolitan areas.202 Much less attention has beenfocused on
indoor pollutants in relation to asthma and more work is
required.203,204
3.3.3 IMMUNOTHERAPy
sbca mmapy
Trialsof allergenspecic immunotherapyby subcutaneousinjectionof
increasingdosesofallergenextractshaveconsistentlydemonstratedbenecialeffectscomparedwithplacebointhemanagement
of allergic asthma. Allergens included house dust mite, grass
pollen, tree pollen, catand dog allergen and moulds. Cochrane
reviews have concluded that immunotherap reducesasthma smptoms, the
use of asthma medications and improves bronchial hper-reactivit.
Themost recent review included 36 trials with house dust mite, 20
with pollen, 10 with animalallergens, two with cladosporium mould,
one with latex and six with multiple allergens.205
Evidence comparing the roles of immunotherap and pharmacotherap
in the management ofasthma is lacking. One stud directl compared
allergen immunotherap with inhaled steroidsand found that smptoms
and lung function improved more rapidl in the group on
inhaledsteroids.206 Further comparative studies are required.
Immunotherap for allergic rhinitis has been shown to have a carr
over effect after theraphas stopped.207
B
Immunotherapycanbeconsideredinpatientswithasthmawhereaclinicallysignicantag
ca b av. t pa v agc ac apym b y c w pa.
sbga mmapy
There has been increasing interest in the use of sublingual
immunotherap, which is associatedwith far fewer adverse reactions
than subcutaneous immunotherap. A sstematic
reviewsuggestedthereweresomebenetsforasthmacontrolbutthemagnitudeoftheeffectwassmall.208
Further randomised controlled trials are required.
B sbga mmapy ca cy b cmm am ama pacc.
3.4 dietArY MAniPulAtion
3.4.1 ELECTROLyTES
Increasing dietar sodium has been implicated in the geographical
variations in asthma mortalit209and high sodium intake is
associated with increased bronchial hper-responsiveness.210,211
Asystematicreviewofinterventionstudiesreducingsaltintakeidentiedonlyminimaleffectsand
concluded that dietar salt reduction could not be recommended in
the management ofasthma.212 Low magnesium intakes have been
associated with a higher prevalence of asthmawith increasing intake
resulting in reduced bronchial hper-responsiveness and higher
lungfunction.213Magnesiumplaysabenecialroleinthetreatmentofasthmathroughbronchialsmooth
muscle relaxation, leading to the use of intravenous or inhaled
preparations ofmagnesium sulphate for acute exacerbations of
asthma.214 Studies of oral supplementation arelimited and more
trials are required.215-217
3 non-PhArMAColoGiCAl MAnAGeMent
-
8/7/2019 Asthma British 2009
36/132
31+
1+
2+
1++
British Guideline on the MAnAGeMent of AsthMA
30
3.4.2 FISH OILS/LIPIDS
In vitro studies suggest that supplementing the diet with omega
n-3 fatt acids, which are
mostcommonlyfoundinshoils,mightreducetheinammationassociatedwithasthma.
218,219 Resultsfrom observational studies are inconsistent and a
Cochrane review of nine randomised
controlledtrialsconcludedthattherewasinsufcientevidencetorecommendshoilsupplementationfor
the treatment of asthma.220
3.4.3 ANTIOXIDANTS
Observational studies have reported that low vitamin C, vitamin
E and selenium intakes areassociated with a higher prevalence of
asthma.143 Intervention studies suggest that
neithersupplementationwithvitaminC,vitaminEorseleniumisassociatedwithclinicalbenetsinpeople
with asthma.221-223 Observational studies in both adults and
children have also consistentlshown that a high intake of fresh
fruit and vegetable is associated with less asthma and
betterpulmonar function.224-230 No intervention studies evaluating
the intake of fruit or vegetablesand their effects on asthma have
been reported.
3.4.4 WEIGHT REDUCTION IN OBESE PATIENTS WITH ASTHMA
Several studies have reported an association between increasing
bod mass index and smptoms
of asthma.231-234 One randomised parallel group stud has shown
improved asthma controlfollowing weight reduction in obese patients
with asthma.235
C Wg c cmm b pa w ama pm gaa a mpv ama c.
3.4.5 PROBIOTICS
Studieshavesuggestedthatanimbalanceingutoraisassociatedwithahigherriskofdevelopment
of allerg.236 Trials have investigated the use of probiotics in the
treatment ofestablished allergic disease with variable
results.237,238 Onl one stud focused on
asthma,ndingadecreaseineosinophiliabutnoeffectonclinicalparameters.239
Intheabsenceofevidenceofbenet,itisnotpossibletorecommendtheuseofprobiotics
maagm ama.
3.4.6 IMMUNISATIONS
Anumberoflargestudieshaveconcludedthathighvaccinationcoveragehasnosignicantimpact
on an allergic outcome or asthma. There is a suggestion that the
higher the vaccinecoverage the greater the possibilit that there is
a degree of protection against the
developmentofallergyintherstyearsoflife.240-243
There is some discussion about whether BCG immunisation ma
confer protection againstallerg and asthma. Research has focused on
primar prophlaxis, though there are some studiesinvestigating the
use of BCG, with or without allergen, as a means to switch off
allergic
immuneresponses.Therearesomeobservationssuggestingthatbenetmightoccur,244
but results of
trials have been disappointing.245,246 This is an area that
requires further investigation.
Therehas beenconcern thatinuenzavaccinationmightaggravate
respiratorysymptoms,thoughanysucheffectwouldbeoutweighedbythebenetsofthevaccination.
247 Studies inchildren have suggested that immunisation with the
vaccine does not exacerbate asthma248
buthasasmallbenecialeffectonqualityoflifeinchildrenwithasthma. 249
The immune responseto the immunisation ma be adversel affected b
high-dose inhaled corticosteroid therap andthis requires further
investigation.250 A Cochrane review of pneumococcal vaccine found
verlimitedevidencetosupportitsusespecicallyinindividualswithasthma.251
B imma b am p ay ca a ama. rp vacc may b aa by g- a .
-
8/7/2019 Asthma British 2009
37/132
1+
1++
1+
1++
1+
1+
1+
31
3.5 CoMPleMentArY And AlternAtiVe MediCine
Successive reviews have concluded that the evidence to support
an recommendations oncomplementar or alternative medicine is
lacking.252 It is recognised that a lack of evidencedoes not
necessaril mean that treatment is ineffective and high qualit
research, conducted inthe same rigorous and objective fashion as
that for conventional therap, is required.
3.5.1 ACUPUNCTURE
A Cochrane review of 21 trials highlighted man methodological
problems with the studiesreviewed. Onl seven of the trials in 174
patients emploed randomisation to active
(recognisedintraditionalChinesemedicinetobeofbenetinasthma)orshamacupuncturepoints(withno
recognised activit) for the treatment of persistent or chronic
asthma. Blinding was a majorproblem in the assessment of the
results and there were considerable inconsistencies
inmethodology.Thereviewconcludedthattherewasnoevidenceforaclinicallyvaluablebenetforacupunctureandnosignicantbenetsinrelationtolungfunction.253
A later sstematicreview and meta-analsis of 11 randomised
controlled trials found no evidence of an effectin reducing asthma
severit but a suggestion that where broncho-constriction was
induced
toestablishefcacyofacupuncturetherewasabenecialeffect.Concernwasexpressedaboutpotential
preferential publication in favour of positive outcome studies.254
Two other trials of
acupuncture in relation to induced asthma were also
negative.
255,256
3.5.2 AIR IONISERS
Ionisershavebeenwidelypromotedasbeingofbenetforpatientswithasthma.ACochranereviewofvestudiesusingnegativeiongeneratorsandonewithapositiveiongeneratorfoundnoevidenceofbenetinreducingsymptomsinpatientswithasthma.
257 One stud
demonstratedanincreaseinnight-timecoughtoalevelwhichapproachedstatisticalsignicance.258
A A a cmm am ama.
3.5.3 BREATHING EXERCISES INCLUDING yOGA AND THE BUTEyKO
BREATHINGTECHNIQUE
The principle of oga and Buteko breathing technique is to
control hperventilation b loweringrespirator frequenc. A Cochrane
review of breathing exercises found no change in routinemeasures of
lung function.259 One stud showed a small reduction in airwa
responsiveness tohistamine utilising pranaama, a form of oga
breathing exercise.260
TheButeykobreathingtechniquespecicallyfocusesoncontrolofhyperventilationandanyensuinghypocapnia.Fourclinicaltrialssuggestbenetsintermsofreducedsymptomsandbronchodilator
usage but no effect on lung function.261-264
B Byk bag cq may b c p pa c ympm ama.
3.5.4 HERBAL AND TRADITIONAL CHINESE MEDICINE
ACochranereviewidentied17trials,nineofwhichreportedsomeimprovementinlungfunction
but it was not clear that the results would be generalisable.265 A
more recent double blindplacebo controlled trial of a Chinese herb
decoction (Ding Chuan Tang) showed improvementin airwa
hper-responsiveness in children with stable
asthma.266Itisdifculttodisentanglethe effects of multiple
ingredients; Ding Chuan Tang for example contains nine
components.Inasecondstudy,100childrenwithasthmafoundthatave-herbmixturegavesomebenetsin
relation to lung function and smptoms compared with placebo.267
The conclusions of these trials of Chinese herbal therap are not
generalisable due to variationsin the herbal mixtures and stud
designs. There are likel to be pharmacologicall activeingredients
in the mixtures and further investigations are warranted. There is
a need for largeappropriatel powered placebo controlled
studies.
3 non-PhArMAColoGiCAl MAnAGeMent
-
8/7/2019 Asthma British 2009
38/132
1++
1+
1++
British Guideline on the MAnAGeMent of AsthMA
32
3.5.5 HOMEOPATHy
ACochranereviewidentiedonlythreemethodologicallysoundrandomisedcontrolledtrials,two
of which reported some positive effects. A criticism of the studies
was that the did notemplo individualised homeopath, which is the
essence of this approach to treatment. 268
A more recent trial of individualised homeopath in childhood
asthma, which was
placebocontrolledandappropriatelypowered,failedtoshowanyevidenceofbenetoverconventionaltreatment
in primar care.269
3.5.6 HyPNOSIS AND RELAXATION THERAPIES
Asystematicreviewofrelaxationtherapies,includinghypnotherapy,identiedvecontrolledtrials,twoofwhichshowedsomebenets.Overallthemethodologyofthestudieswaspoorandthereviewconcludedthattherewasalackofevidenceofefcacybutthatmusclerelaxationcouldconceivablybenetlungfunctioninpatientswithasthma.270
3.6 other CoMPleMentArY or AlternAtiVe APProAChes
3.6.1 MANUAL THERAPy INCLUDING MASSAGE AND SPINAL
MANIPULATION
ACochranereviewidentiedfourrelevantRCTs.271 The two trials of
chiropractic suggest thatthere is no place for this modalit of
treatment in the management of asthma. No conclusionscan be drawn
on massage therap.
3.6.2 PHySICAL EXERCISE TRAINING
A Cochrane review 259 has shown no effect of phsical training on
PEF, FEV1, FVC or VEmax.
However, oxgen consumption, maximum heart rate, and work capacit
all
increasedsignicantly.Moststudiesdiscussedthepotentialproblemsofexerciseinducedasthma,butnone
made an observations on this phenomenon. As phsical training
improves indices
ofcardiopulmonaryefciency,itshouldbeseenaspartofageneralapproachtoimprovinglifestyleand
rehabilitation in asthma, with appropriate precautions advised
about exercise inducedasthma (see section 4.7.2).
3.6.3 FAMILy THERAPy
ACochranereview identied two trials, in55 children, showing that
familytherapymaybe a useful adjunct to medication in children with
asthma.272Smallstudysizelimitstherecommendations.
Indifcultchildhoodasthma,theremaybearoleforfamilytherapyasanadjuncttopharmacotherap.
-
8/7/2019 Asthma British 2009
39/132
33
4 Pamacgca maagm
Theaimofasthmamanagementiscontrolofthedisease.Controlofasthmaisdenedas:
no datime smptoms
no night-time awakening due to asthma
no need for rescue medication
no exacerbations
no limitations on activit including exercise
normal lung function (in practical terms FEV1
and/or PEF>80% predicted or best) withminimal side
effects.
In clinical practice patients ma have different goals and ma
wish to balance the aims ofasthma management against the potential
side effects or inconvenience of taking medicationnecessar to
achieve perfect control.
Lung function measurements cannot be reliabl used to guide
asthma management inchildren under five ears of age.
Astepwiseapproachaimstoabolishsymptomsassoonaspossibleandtooptimisepeakowb
starting treatment at the level most likel to achieve this.
Patients should start treatment at thestep most appropriate to the
initial severit of their asthma. The aim is to achieve earl
controland to maintain b stepping up treatment as necessar and
stepping down when control is good(see gures 4, 5 and 6 for
summaries of stepwise management in adults and children).
Before initiating a new drug therap practitioners should check
compliance with existingtherapies (see section 9.2), inhaler
technique (see section 5) and eliminate trigger factors(see section
3).
Until Ma 2009 all doses of inhaled steroids in this section have
been referenced againstbeclometasone (BDP) given via CFC-MDIs
(metered dose inhaler). As BDP CFC is phased out,the reference
inhaled steroid will be the BDP-HFA equivalent, which can be used
at the samedosage. Adjustments to doses will have to be made for
other devices and other corticosteroidmolecules (see section
4.2).
In this and the following section, each recommendation has been
graded and the supportingevidence assessed for adults (>12 ears
old), children 5-12 ears, and children under 5 ears.The evidence is
less clear in children under two and the threshold for seeking an
expert opinionshould be lowest in these children.
1 2 3 1 A2 C ag 5-12 ya3 C 5 ya
rcmma appy ag gp.
4 PhArMAColoGiCAl MAnAGeMent
Revised
2009
-
8/7/2019 Asthma British 2009
40/132
5-12ears
>12ears
12ears
10-12 puffs per da is a marker of poorl
controlled asthma that puts patients at risk of fatal or
near-fatal asthma.
Patients with a high usage of inhaled short-acting 2
agonists should have their asthmamanagement reviewed.
4.2 steP 2: introduCtion of reGulAr PreVenter therAPY
For steps 2, 3, and 4, treatments have been judged on their
abilit to improve smptoms,improve lung function, and prevent
exacerbations, with an acceptable safet profile.Improvement of
qualit of life, while important, is the subject of too few studies
to be used to
make recommendations at present.
4.2.1 COMPARISON OF INHALED STEROIDS
Man studies comparing different inhaled steroids are of
inadequate design and have beenomitted from further assessment. In
view of the clear differences between normal volunteersand asthma
patients in the absorption of inhaled steroids, data from normal
volunteers havenot been taken into account. Onl studies in which
more than one dose of at least one of
theinhaledsteroidsorbothsafetyandefcacyhadbeenstudiedtogetherinthesametrialwereevaluated.
Non-blinded studies also had to be considered because of the
problems of obtainingcompetitors deliver devices. A series of
Cochrane reviews comparing different inhaled steroidsusing a
different methodolog have come to the same conclusion.
BDP and budesonide are approximatel equivalent in clinical
practice, although there ma bevariations with different deliver
devices. There is limited evidence from two open studies ofless
than ideal design that budesonide via the turbohaler is more
clinicall effective.295 However,at present a 1:1 ratio should be
assumed when changing between BDP and budesonide.
Fluticasone provides equal clinical activit to BDP and
budesonide at half the dosage. Theevidence that it causes fewer
side effects at doses with equal clinical effect is limited.
Mometasone appears to provide equal clinical activit to BDP and
budesonide at half thedosage.296 The relative safet of mometasone
is not full established.
-
8/7/2019 Asthma British 2009
41/132
35
Table 8b: Equivalent doses of inhaled steroids relative to BDP
and current licensed ageindications
These dosage equivalents are approximate and will depend on
other factors such as inhalertechnique.
uK cc cv
s eqva >12
ya
5 12
ya
-
8/7/2019 Asthma British 2009
42/132
5-12ears
>12ears
12ears
12ears
12ears
-
8/7/2019 Asthma British 2009
43/132
37
4.2.3 SAFETy OF INHALED STEROIDS
Thesafetyofinhaledsteroidsisofcrucialimportanceandabalancebetweenbenetsandrisks
for each individual needs to be assessed. Account should be taken
of other topical steroidtherap when assessing sstemic risk. It has
been suggested that steroid warning cards should
beissuedtopatientsonhigherdoseinhaledsteroids,butthebenetsandpossibledisadvantages,particularlywithregardtocompliance,ofsuchapolicyremaintobedened.
Adults
There is little evidence that doses below 800 mcg BDP per da
cause an short term detrimentaleffects apart from the local side
effects of dsphonia and oral candidiasis. However, the possibilitof
long term effects on bone has been raised. One sstematic review
reported no effect onbone densit at doses up to 1,000 mcg BDP per
da.291Thesignicanceofsmallbiochemicalchanges in adrenocortical
function is unknown.
Titrate the dose of inhaled steroid to the lowest dose at which
effective control of asthmais maintained.
Children
Administration of inhaled steroids at or above 400 mcg BDP a da
or equivalent ma be associated
with sstemic side effects.292 These ma include growth failure
and adrenal suppression. Isolatedgrowth failure is not a reliable
indicator of adrenal suppression and monitoring growth cannotbe
used as a screening test of adrenal function.290,293
Clinicaladrenalinsufciencyhasbeenidentiedinasmallnumberofchildrenwhohavebecome
acutel unwell at the time of intercurrent illness. Most of these
children had beentreated with high doses of inhaled
corticosteroids. The dose or duration of inhaled
steroidtreatmentrequiredtoplaceachildatriskofclinicaladrenalinsufciencyisunknownbutislikelytooccurat800mcgBDPperdayorequivalent.Thelow-doseACTHtestisconsideredto
provide a phsiological stimulation of adrenal responsiveness but it
is not known how
usefulsuchasensitivetestisatpredictingclinicallyrelevantadrenalinsufciency.
59,294 In addition,it is unknown how frequentl tests of adrenal
function would need to be repeated if a childremained on high-dose
inhaled corticosteroid. At higher doses, add-on agents, for
example,
long-acting 2 agonists, should be activel considered.
While the use of inhaled corticosteroids ma be associated with
adverse effects (including thepotential to reduced bone mineral
densit) with careful inhaled steroid dose adjustment thisrisk is
likel to be outweighed b their abilit to reduce the need for
multiple bursts of oralcorticosteroids.771
Monitor height of children on high doses of inhaled steroids on
a regular basis.
The lowest dose of inhaled steroids compatible with maintaining
disease control shouldbe used.
Forchildrentreatedwith800mcgBDPperdayorequivalent:
Specific written advice about steroid replacement (eg Steroid
Alert Card) in the event ofa severe intercurrent illness or surger
should be part of the management plan.
The child should be under the care of a specialist paediatrician
for the duration of thetreatment.
Considerthepossibilityofadrenalinsufciencyinanychildmaintainedoninhaledsteroidspresenting
with shock or a decreased level of consciousness; serum biochemistr
and bloodglucose levels should be checked urgentl. Consider whether
intramuscular (IM) hdrocortisoneis required.
4 PhArMAColoGiCAl MAnAGeMent
-
8/7/2019 Asthma British 2009
44/132
5-12ears
>12ears
12ears
12ears
5- 306,307
Thereisnoclearevidenceofbenetwithsodiumcromoglicateinchildrenaged-
-
8/7/2019 Asthma British 2009
45/132
-
8/7/2019 Asthma British 2009
46/132
5-12ears
>12ears
-
8/7/2019 Asthma British 2009
47/132
5-12ears
>12ears
12ears
-
8/7/2019 Asthma British 2009
48/132
1-
5-12ears
>12ears
-
8/7/2019 Asthma British 2009
49/132
43
Figure 4: Summary of stepwise management in adults
Inhaledshort-acting
2
agonistasrequired
STEP1
Mildintermittentasthma
Addinhaledsteroid200-800
mcg/day*
400mcgisanappropriate
startingdoseformanypatients
Startatdoseofinhaled
steroidappropriateto
severityofdisease.
STEP2
Regularpreventertherapy
1.A
ddinhaledlong-acting
1.A
ddinhaledlong-acting
2agonist(LABA)
2.A
ssesscontrolofasthma:
goodresponseto
LABA-continueLABA
benefitfromLABAbut
controlstillinadequate
-continueLABAand
increaseinhaledsteroid
doseto800mcg/day*(if
notalreadyonthisdose)
noresponsetoLABA
-stopLABAandincrease
inhaledsteroidto800
mcg/day.*Ifcontrol
stillinadequate,institute
trialofothertherapies,
leukotrienereceptor
antagonistorSR
theophylline
1.A
ddinhaledlong-acting
STEP3
Initialadd-ontherapy
Considertrialsof:
increasinginhaledsteroid
upto20
00mcg/day*
addition
ofafourthdrug
e.g.leukotrienereceptor
antagon
ist,SRtheophylline,
2agonisttablet
S
TEP4
Persiste
ntpoorcontrol
Usedailysteroidtablet
inlowestdosep
roviding
adequatecontro
l
Maintainhighdoseinhaled
steroidat2000mcg/day*
Considerothert
reatmentsto
minimisetheuseofsteroid
tablets
Referpatientforspecialistcare
STEP
5
Continuouso
rf