Embed Size (px)
Citation preview

©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
JOURNAL OF ASTHMA
Vol. 40, No. 7, pp. 733–739, 2003
REVIEW ARTICLE
Asthma, Body Mass Index, and C-Reactive Protein Among US Adults
Earl S. Ford, M.D., M.P.H.*
Division of Environmental Hazards and Health Effects,
National Center for Environmental Health, Centers for Disease Control and
Prevention, Atlanta, Georgia, USA
ABSTRACT
Obesity, a state that may be characterized by a low-grade inflammation, has been
associated with asthma. C-reactive protein, an acute phase reactant, is elevated in
obese people. However, little is known about how asthma affects C-reactive protein
concentrations. Using data from 14,224 participants of the Third National Health and
Nutrition Examination Survey (1988–1994), the author examined C-reactive protein
concentrations among participants with current asthma (n¼ 651), who formerly
had asthma (n¼ 303), and who never had asthma (n¼ 13,270). Compared with 21%
of participants with current asthma, 11% with former asthma (P<.001) and 15%
without asthma (P¼ .018) had C-reactive protein concentrations �85th percentile
of the sex-specific distribution. Compared with participants without asthma, the
age-adjusted odds ratios for having an elevated C-reactive protein concentration was
1.49 (95% confidence interval [CI]: 1.11, 2.00) for persons with current asthma. After
adjusting for age, sex, race or ethnicity, years of education, cotinine concentration, body
mass index, waist-hip ratio, physical activity level, aspirin use, oral corticosteroid use,
and inhaled corticosteroid use, the odds ratio decreased to 1.15 (95% CI: 0.83, 1.59).
Body mass index was the main reason for the attenuation of the odds ratio. Whether
the inflammatory activity associated with body mass index contributes to the
pathophysiology of asthma is unknown.
INTRODUCTION
The prevalences of both obesity (1,2) andasthma (3) have increased dramatically in recent
decades. The concordant increases of theseconditions has raised speculation that the two arecausally related. Prospective studies support thispossibility (4). Although the mechanisms through
*Correspondence: Earl S. Ford, M.D., M.P.H., Division of Environmental Hazards and Health Effects, National Center for
Environmental Health, Centers for Disease Control and Prevention, 1600 Clifton Road, MS E17, Atlanta, GA 30333, USA;
Fax: (404) 498-1088; E-mail: [email protected].
733
DOI: 10.1081/JAS-120023497 0277-0903 (Print); 1532-4303 (Online)
Copyright & 2003 by Marcel Dekker, Inc. www.dekker.com
J A
sthm
a D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Auc
klan
d on
11/
05/1
4Fo
r pe
rson
al u
se o
nly.

©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
which obesity is linked to asthma remain to be fullyelucidated, several possibilities could link thetwo conditions. For example, interleukin-6 (IL-6)and tumor necrosis factor-� (TNF-�), which areelevated in obese people, are thought to be impor-tant agents in the pathophysiology of asthma.Because IL-6 is a potent stimulant of hepatic C-reac-tive protein production, C-reactive protein con-centration may be regarded as a proxy for IL-6activity.
Little is known about C-reactive protein con-centrations among people with asthma. Becausepeople with asthma have a higher prevalence ofobesity than people who do not have asthma (5,6),speculation that people with asthma are more likelyto have elevated C-reactive protein concentrationsseems reasonable. To test this hypothesis, theauthor examined data from the Third NationalHealth and Nutrition Examination Survey.
METHODS
From 1988 through 1994, a representative sampleof the noninstitutionalized civilian US population,selected by using a multistage, stratified samplingdesign, was interviewed and invited for a clinicalexamination. For most participants, blood wasdrawn at the examination clinic; for some who wereunable to attend the examination because of healthreasons, a blood sample was obtained during thehome interview. Persons ages �60 years, AfricanAmericans, and Mexican Americans were over-sampled. Details about the survey and its methodshave been published (7,8).
Respondents were asked: ‘‘Has a doctor evertold you that you had asthma?’’ and those whoresponded ‘‘yes’’ were then asked ‘‘Do you stillhave asthma?’’ Respondents with positive answersto both questions were classified as having ‘‘current’’asthma. Respondents who answered affirmatively tothe first question but negatively to the second onewere classified as having ‘‘former’’ asthma.Respondents who reported not having been toldby a physician that they had asthma were classifiedas never having had asthma.
Participants attended one of three examinationsessions: morning, afternoon, or evening. Thoseattending the morning sessions were asked to fastfor 10–16 hours. Those attending the afternoonand evening sessions were asked to fast for atleast 6 hours. C-reactive protein was measuredat the University of Washington Department of
Laboratory Medicine by using latex-enhancednephelometry (8). Details about the laboratory pro-cedures and quality control have been published (8).The lower detection limit was 3.0mg/L. Participantswith C-reactive protein concentrations below thedetection limit were assigned a value of 2.1mg/L.An elevated C-reactive protein concentration wasdefined as one at or above the 85th percentile ofthe sex-specific distribution: �4.4mg/dL for menand �7.0 for women (9).
The analyses included the following variables:age, sex, ethnicity, education, serum cotinine con-centration, body mass index, waist-to-hip-ratio, phy-sical activity, aspirin use, oral corticosteroid use, andinhaled corticosteroid use. In addition, oral contra-ceptive use and hormone-replacement therapywere included in analyses limited to women. Serumcotinine concentration was determined by usinghigh-performance liquid chromatography atmo-spheric-pressure chemical ionization tandem massspectrometry. Body mass index was calculatedfrom measured weight and height. The waist circum-ference was measured at the high point of theiliac crest at minimal respiration to the nearest0.1 cm. The hip circumference was measured atthe maximal extension of the buttocks. Four levelsof physical activity were defined: vigorously active,moderately active, lightly active, and sedentary.Aspirin use was estimated from the followingquestion: ‘‘In the past month, have you taken anyaspirin, Anacin, Bufferin, Ecotrin, Ascriptin, orMidol?’’ Participants were then asked how oftenthey used these products in the prior month. Useof oral and inhaled corticosteroids was derivedfrom drug class information for medications usedby participants. The use of oral contraceptives andhormone-replacement therapy was determined fromvarious questions on the reproductive history ques-tionnaire.
Analyses were limited to participants ages �20years who attended the mobile examination center.Pregnant women were excluded. The data wereage-adjusted to the 1980 US population age �20years using the direct method. Two sample testof proportions and t-tests were performed forproportions and means. Associations between thedichotomized C-reactive protein concentrationsand asthma status were examined by using logisticregression analysis. To account for the complexsurvey design, analyses were conducted withSUDAAN (10). Medical examination clinic sam-pling weights were used to produce weightedestimates.
734 Ford
J A
sthm
a D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Auc
klan
d on
11/
05/1
4Fo
r pe
rson
al u
se o
nly.

©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
RESULTS
After participants with missing data for thedependent and independent variables were excluded,14,224 participants remained in the analyses. Theyincluded 651 participants with current asthma, 303who formerly had asthma, and 13,270 who neverhad asthma.
The mean ages among the three groupswere similar (Table 1). Participants with currentasthma were more likely than those without asthmato be female. Cotinine concentrations, physicalactivity participation, and aspirin use did not differsignificantly among the three groups. Almost 31% ofparticipants with asthma were obese compared with22% of participants without asthma (P¼ .001).
About 35% of participants with current asthmaand 23% of participants with former asthma hada C-reactive protein concentration of >2.1mg/Lcompared with 28% of participants withoutasthma. In addition, about 21% of participantswith current asthma, 11% of participants withformer asthma, and 15% of participants withoutasthma had a C-reactive protein concentrationat or above the 85th percentile of the sex-specificdistribution.
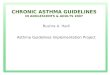
For each body mass index category, a higherpercentage of participants with asthma had anelevated C-reactive protein concentration (Fig. 1).
The difference was most pronounced for participantswith body mass index <25 kg/m2.
Compared with participants without asthma,the age-adjusted odds ratios for having an elevatedC-reactive protein concentration (defined as � sex-specific 85th percentile) was 1.49 (95% confidenceinterval (CI): 1.11, 2.00) for persons with currentasthma. However, after adjusting for age, sex, raceor ethnicity, years of education, cotinine con-centration, body mass index, waist-hip ratio, physicalactivity level, aspirin use, oral corticosteroid use,and inhaled corticosteroid use, the odds ratiodecreased to 1.15 (95% CI: 0.83, 1.59). Body massindex was the main reason for the attenuation of theodds ratio. In a model limited to women (n¼ 7,081),the odds ratio was 0.96 (95% CI: 0.62, 1.47) afteradditional adjustment for oral contraceptive use. Inanother model limited to women (n¼ 7,042), the oddsratio was 0.94 (95% CI: 0.61, 1.45) after additionaladjustment for use of hormone-replacement therapy.When participants with a variety of conditions wereexcluded (self-reports of arthritis, myocardial infarc-tion, congestive heart failure, stroke, cancer, bronchi-tis, emphysema, gout, lupus, and respiratoryinfections during the previous 3 weeks; presence ofrheumatoid factor; and physician’s impression of pre-sence of active infection during the examination)(n¼ 7,508; 218 participants with asthma), the oddsratio decreased to 0.76 (95% CI: 0.38, 1.54).
Table 1. Selected age-adjusted characteristics among participants age �20 years, by asthma status, national health and
nutrition examination survey III 1988–1994.
Characteristics
Current
asthma
(n¼ 651)
Former asthma
(n¼ 303)
Never asthma
(n¼ 13,270)
P current vs.
former
P current
vs. never
P former
vs. never
Age (years) 44.3 (0.7) 44.0 (1.1) 44.8 (0.5) 0.801 0.543 0.452
% Men 41.8 (2.9) 59.3 (3.1) 48.9 (0.5) 0.001 0.023 0.001
% Non-Hispanic white 80.3 (1.8) 81.1 (2.7) 76.6 (1.3) 0.780 0.078 0.109
Education (years) 12.1 (0.2) 12.7 (0.3) 12.3 (0.1) 0.057 0.091 0.241
Serum cotinine concentration
(ng/mL)
86.5 (7.5) 92.2 (14.1) 76.9 (2.7) 0.739 0.227 0.302
Body mass index (kg/m2) 27.7 (0.4) 26.5 (0.3) 26.4 (0.1) 0.032 0.004 0.815
% Body mass index �30 kg/m2 31.3 (2.8) 22.1 (3.3) 21.5 (0.7) 0.042 0.001 0.879
Waist-hip ratio 0.915 (0.005) 0.926 (0.008) 0.908 (0.001) 0.251 0.241 0.035
% Moderately or vigorously active 38.2 (3.3) 36.8 (2.9) 40.3 (1.2) 0.754 0.498 0.275
MET-frequency 108.9 (10.9) 117.6 (12.7) 111.6 (3.4) 0.638 0.806 0.668
% Aspirin use during previous
month
37.7 (3.1) 44.3 (5.2) 38.4 (1.0) 0.179 0.812 0.271
% C-reactive protein >2.1mg/L 35.2 (3.4) 23.2 (3.1) 27.7 (1.1) 0.003 0.025 0.147
% C-reactive protein �85th
percentile
20.9 (2.2) 11.3 (1.9) 15.4 (0.6) <0.001 0.018 0.050
Asthma and C-Reactive Protein 735
J A
sthm
a D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Auc
klan
d on
11/
05/1
4Fo
r pe
rson
al u
se o
nly.

©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
DISCUSSION
These results from a cross-sectional study of arepresentative sample of the US population showthat adults with asthma are more likely to havean elevated C-reactive protein concentration thanare persons who formerly had asthma or whonever had asthma. These data also show that adultswith asthma are more likely than adults withoutasthma to be obese. Because body mass index corre-lates strongly with C-reactive protein concentrations(9), much of the association between asthmastatus and C-reactive protein was accounted for bythe higher prevalence of obesity among asthmaticadults.
The links between obesity and asthma have notbeen adequately explained. Summarizing a numberof studies, Camargo and colleagues suggested thatobesity causes histological changes in the lungs ofobese rats, reduction in airway caliber, and increasedbronchial hyperreactivity (4). Furthermore, theysuggested that obese people may be more sedentary,thus, spending more time indoors with continuedexposure to potential allergens; are more likelyto have gastroesophageal reflux, which has beenassociated with asthma; and may have diets that aremore likely to lead to asthma. Finally, they speculatethat effects of obesity on hormonal patterns could berelated to the risk of developing asthma.
Several additional possibilities merit mention.Obesity affects immune function (11,12). Becausethe immune system is critically involved in thepathophysiology of asthma, some of these immunealterations may be linked to asthma. For example,leptin, which is elevated in obese persons, canaffect the immune response (13). In addition to
producing hormones such as leptin, adipose tissueis an important source of cytokines, such as TNF-�,IL-1, and IL-6 (14–16). Both TNF-� and IL-1affect numerous processes that may be importantin asthma. These cytokines increase adhesion ofeosinophils to epithelial cells (17), cause releaseof eotaxin, a potent chemotactic agent for eosinophils,from lung fibroblasts (18) and epithelial cells (19,20),cause release of IL-9 from eosinophils (21), upregulateIL-8 production by alveolar macrophages (22),increase IL-8m RNA of bronchial epithelial cells(23), damage bronchial epithelial cells (24), activateendothelial cells (25), increase cyclooxygenase-2(COX-2) activity (26), and cause bronchoconstriction(27). Furthermore, TNF-� or IL-1 may upregulate theexpression and release of various interleukins, such asIL-1, IL-6, IL-8, IL-11, and IL-15, some of whichaffect asthma activity. IL-6, which stimulates humoralimmunity, and prostaglandin E2, a product of theCOX-2 pathway that stimulates humoral immunityand promotes various cytokine responses that havebeen implicated in asthma pathophysiology, may belinked to asthma (28). Although it remains unclearwhether IL-6 is an important mediator in asthma,IL-6 concentrations were higher in bronchial lavagefluid from patients with status asthmaticus than fromcontrol subjects (29). However, whether TNF-�, IL-1,and IL-6 produced by adipocytes are biologicallyactive in lung tissues remains uncertain.
Whether elevated C-reactive protein concentra-tions among overweight and obese adults withasthma potentially affect the course of their diseaseis unclear. Research thus far has not implicatedC-reactive protein as a factor in asthma severityor prognosis. However, C-reactive protein cantrigger the complement cascade through activation
Figure 1. Age-adjusted percentages of US adults age �20 years with a C-reactive protein concentration �85th percentile, by
self-reported asthma status and body mass index, National Health and Nutrition Examination Survey III, 1988–1994.
736 Ford
J A
sthm
a D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Auc
klan
d on
11/
05/1
4Fo
r pe
rson
al u
se o
nly.

©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
of the classical pathway. Although the role ofthe complement system in asthma remains to befully worked out, researchers have suggested thatit may be involved in the pathophysiology of asthma(30–32). Furthermore, recent research suggeststhat C-reactive protein can affect endothelial function(33,34).
If high C-reactive protein concentrations inadults with asthma are not biologically inert andif the source of some of the C-reactive protein con-centration is excess weight, weight control amongoverweight and obese adults with asthma is clearlydesirable. Weight loss among obese patients withasthma results in improvements in clinical measuresand quality of life (35–40).
Several limitations of the data deserve comment.The presence of asthma was self-reported by partici-pants. However, self-reported asthma is commonlyused in epidemiologic studies. Compared withmedical records and other data sources, self-reportedasthma has demonstrated acceptable validityand reliability (41–43). Among NHANES IIIparticipants with asthma, 19.2% had low lungfunction, 13.9% reported cough, 11.1% reportedphlegm production, 66.7% reported wheezing,and 44.5% reported shortness of breath (44). Thetest to use C-reactive protein concentration hada high lower detection limit than current tests.Residual confounding is a possibility. Adding bodymass index and waist-hip-ratio to logistic regressionmodels may not have accounted for the full effectof excess adipose tissue on C-reactive proteinconcentrations. Furthermore, imperfect measurementof other confounders could have resulted inincomplete adjustment.
In conclusion, adults with asthma are morelikely to have elevated C-reactive protein con-centration than are persons who formerly hadasthma or who never had asthma. However, muchof this elevation is accounted for by the highprevalence of obesity among adults with asthma.The implications, if any, of elevated C-reactiveprotein concentrations in adults with asthma isunknown.
REFERENCES
1. Flegal KM, Carroll MD, Kuczmarski RJ,JohnsonCL.Overweight and obesity in theUnitedStates: prevalence and trends, 1960–1994. Int JObes Relat Metab Disord 1998; 22(1):39–47.
2. Mokdad AH, Bowman BA, Ford ES, Vinicor F,Marks JS, Koplan JP. The continuing epidemicsof obesity and diabetes in the United States.JAMA. 2001; 286(10):1195–1200.
3. CDC. Surveillance for asthma—United States,1960–1995. MMWR. 1998; 47(No. SS-1).
4. Camargo CA Jr, Weiss ST, Zhang S, WillettWC, Speizer FE. Prospective study of bodymass index, weight change, and risk of adult-onset asthma in women. Arch Intern Med1999; 159(21):2582–2588.
5. Chen Y, Dales R, Krewski D, Breithaupt K.Increased effects of smoking and obesity onasthma among female Canadians: the NationalPopulation Health Survey, 1994–1995. Am JEpidemiol 1999; 150(3):255–262.
6. Young SY, Gunzenhauser JD, Malone KE,McTiernan A. Body mass index and asthma inthe military population of the northwesternUnited States. Arch Intern Med 2001;161(13):1605–1611.
7. Centers for Disease Control and Prevention.Plan and operation of the Third NationalHealth and Nutrition Examination Survey,1988–94. Bethesda, MD: National Centerfor Health Statistics. Vital Health Stat 1994;1(32).
8. Centers for disease control and prevention. TheThird National Health and NutritionExamination Survey (NHANES III 1988–94)Reference Manuals and Reports. Bethesda,MD: National Center for Health Statistics;1996 (CD-ROM).
9. Ford ES. Body mass index, diabetes, andC-reactive protein among U.S. adults. DiabetesCare 1999; 22(12):1971–1977.
10. Shah BV, Barnwell BG, Bieler GS. SUDAANUser’s Manual, Version 7.5. Research TrianglePark, NC: Research Triangle Institute, 1997.
11. Cousin B, Munoz O, Andre M, Fontanilles AM,Dani C, Cousin JL, Laharrague P, Casteilla L,Penicaud L. A role for preadipocytes as macro-phage-like cells. FASEB J 1999; 13(2):305–312.
12. Nieman DC, Henson DA, Nehlsen-CannarellaSL, Ekkens M, Utter AC, Butterworth DE,Fagoaga OR. Influence of obesity on immunefunction. J Am Diet Assoc 1999; 99(3):294–299.
13. Zarkesh-Esfahani H, Pockley G, Metcalfe RA,Bidlingmaier M, Wu Z, Ajami A, Weetman AP,Strasburger CJ, Ross RJ. High-dose leptinactivates human leukocytes via receptorexpression on monocytes. J Immunol 2001;167(8):4593–4599.
Asthma and C-Reactive Protein 737
J A
sthm
a D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Auc
klan
d on
11/
05/1
4Fo
r pe
rson
al u
se o
nly.

©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
14. Hotamisligil GS, Shargill NS, Spiegelman BM.Adipose expression of tumor necrosis factor-alpha: direct role in obesity-linked insulinresistance. Science 1993; 259(5091):87–91.
15. Vgontzas AN, Papanicolaou DA, Bixler EO,Kales A, Tyson K, Chrousos GP. Elevationof plasma cytokines in disorders of excessivedaytime sleepiness: role of sleep disturbanceand obesity. J Clin Endocrinol Metab 1997;82(5):1313–1316.
16. Zhang HH, Kumar S, Barnett AH, Eggo MC.Dexamethasone inhibits tumor necrosis factor-alpha-induced apoptosis and interleukin-1beta release in human subcutaneous adipocytesand preadipocytes. J Clin Endocrinol Metab2001; 86(6):2817–2825.
17. Godding V, Stark JM, Sedgwick JB, Busse WW.Adhesion of activated eosinophils to respi-ratory epithelial cells is enhanced by tumornecrosis factor-alpha and interleukin-1 beta.Am J Respir Cell Mol Biol 1995; 13(5):555–562.
18. Sato E, Nelson DK, Koyama S, Hoyt JC,Robbins RA. Inflammatory cytokines modulateeotaxin release by human lung fibroblast cellline. Exp Lung Res 2001; 27(2):173–183.
19. Lilly CM, Nakamura H, Kesselman H, Nagler-Anderson C, Asano K, Garcia-Zepeda EA,Rothenberg ME, Drazen JM, Luster AD.Expression of eotaxin by human lung epithelialcells: induction by cytokines and inhibitionby glucocorticoids. J Clin Invest 1997; 99(7):1767–1773.
20. Koyama S, Sato E, Masubuchi T, TakamizawaA, Kubo K, Nagai S, Isumi T. Procaterolinhibits IL-1beta- and TNF-alpha-mediatedepithelial cell eosinophil chemotactic activity.Eur Respir J 1999; 14(4):767–775.
21. Gounni AS, Nutku E, Koussih L, Aris F,Louahed J, Levitt RC, Nicolaides NC, HamidQ. IL-9 expression by human eosinophils:regulation by IL-1beta and TNF-alpha. JAllergy Clin Immunol 2000; 106(3):460–466.
22. Mazzarella G, Grella E, D’Auria D, PacioccoG, Perna F, Petillo O, Peluso G. Phenotypicfeatures of alveolar monocytes/macrophagesand IL-8 gene activation by IL-1 andTNF-alpha in asthmatic patients. Allergy 2000;55(Suppl 61):36–41.
23. Cromwell O, Hamid Q, Corrigan CJ, Barkans J,Meng Q, Collins PD, Kay AB. Expressionand generation of interleukin-8, IL-6 and gran-ulocyte-macrophage colony-stimulating factorby bronchial epithelial cells and enhancement
by IL-1 beta and tumour necrosis factor-alpha.Immunology 1992; 77(3):330–337.
24. Kampf C, Relova AJ, Sandler S, Roomans GM.Effects of TNF-alpha IFN-gamma and IL-betaon normal human bronchial epithelial cells. EurRespir J 1999; 14(1):84–91.
25. Bjornsdottir US, Cypcar DM. Asthma: aninflammatory mediator soup. Allergy 1999; 54(Suppl 49):55–61.
26. Belvisi MG, Saunders MA, Haddad el-B, HirstSJ, Yacoub MH, Barnes PJ, Mitchell JA.Induction of cyclo-oxygenase-2 by cytokines inhuman cultured airway smooth muscle cells:novel inflammatory role of this cell type. Br JPharmacol 1997; 120(5):910–916.
27. Martin C, Wohlsen A, Uhlig S. Changes inairway resistance by simultaneous exposure toTNF-alpha and IL-1beta in perfused rat lungs.Am J Physiol Lung Cell Mol Physiol 2001;280(4):L595–L601.
28. Varner AE. An immunologic mechanism forthe association between obesity and asthma.Arch Intern Med 2000; 160(15):2395–2396.
29. Tillie-Leblond I, Pugin J, Marquette CH,Lamblin C, Saulnier F, Brichet A, Wallaert B,Tonnel AB, Gosset P. Balance between pro-inflammatory cytokines and their inhibitors inbronchial lavage from patients with status asth-maticus. Am J Respir Crit Care Med 1999;159(2):487–494.
30. Regal JF. Role of the complement system inpulmonary disorders. Immunopharmacology1997; 38(1–2):17–25.
31. Michel O, Sergysels R, Duchateau J. Asthme etcomplement Rev Mal Respir 1988; 5(1):37–41.
32. Karp CL, Wills-Karp M. Complement and IL-12: yin and yang. Microbes Infect 2001;3(2):109–119.
33. Pasceri V, Willerson JT, Yeh ET. Direct pro-inflammatory effect of C-reactive protein onhuman endothelial cells. Circulation 2000;102(18):2165–2168.
34. Schalkwijk CG, PolandDC, vanDijkW, KokA,Emeis JJ, Drager AM, Doni A, van HinsberghVW, Stehouwer CD. Plasma concentration of C-reactive protein is increased in type I diabeticpatients without clinical macroangiopathy andcorrelates with markers of endothelial dysfunc-tion: evidence for chronic inflammation.Diabetologia 1999; 42(3):351–357.
35. Macgregor AM, Greenberg RA. Effect ofsurgically induced weight loss on asthma inthe morbidly obese. Obes Surg 1993; 3(1):15–21.
738 Ford
J A
sthm
a D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Auc
klan
d on
11/
05/1
4Fo
r pe
rson
al u
se o
nly.

©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
36. Murr MM, Siadati MR, Sarr MG. Resultsof Bariatric Surgery for morbid obesity inpatients older than 50 years. Obes Surg 1995;5(4):399–402.
37. Dixon JB, Chapman L, O’Brien P. Markedimprovement in asthma after lap-bandsurgery for morbid obesity. Obes Surg 1999;9(4):385–389.
38. Dhabuwala A, Cannan RJ, Stubbs RS.Improvement in co-morbidities following weightloss from gastric bypass surgery. Obes Surg2000; 10(5):428–435.
39. Hakala K, Stenius-Aarniala B, Sovijarvi A.Effects of weight loss on peak flow variability,airways obstruction, and lung volumes inobese patients with asthma. Chest 2000;118(5):1315–1321.
40. Stenius-Aarniala B, Poussa T, Kvarnstrom J,Gronlund EL, Ylikahri M, Mustajoki P.Immediate and long term effects of weightreduction in obese people with asthma:
randomised controlled study. BMJ 2000;320(7238):827–832.
41. Harlow SD, Linet MS. Agreement betweenquestionnaire data and medical records. The evi-dence for accuracy of recall. Am J Epidemiol1989; 129(2):233–248.
42. Linet MS, Harlow SD, McLaughlin JK,McCaffrey LD. A comparison of interviewdata and medical records for previous medicalconditions and surgery. J Clin Epidemiol 1989;42(12):1207–1213.
43. Toren K, Brisman J, Jarvholm B. Asthma andasthma-like symptoms in adults assessed byquestionnaires. A literature review. Chest 1993;104(2):600–608.
44. Mannino DM, Gagnon RC, Petty TL, LydickE. Obstructive lung disease and low lungfunction in adults in the United States: datafrom the National Health and NutritionExamination Survey, 1988–1994. Arch InternMed 2000; 160(11):1683–1689.
Asthma and C-Reactive Protein 739
J A
sthm
a D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Auc
klan
d on
11/
05/1
4Fo
r pe
rson
al u
se o
nly.

©2003 Marcel Dekker, Inc. All rights reserved. This material may not be used or reproduced in any form without the express written permission of Marcel Dekker, Inc.
MARCEL DEKKER, INC. • 270 MADISON AVENUE • NEW YORK, NY 10016
J A
sthm
a D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Auc
klan
d on
11/
05/1
4Fo
r pe
rson
al u
se o
nly.