Embed Size (px)
Citation preview

Associations Between the Four Toll-Like ReceptorPolymorphisms and the Risk of Gastric Cancer:
A Meta-Analysis
Jian Chen,1 Sheng Hu,1 Sanghua Liang,1 Qilong Chen,2 Qingqing Yang,3 Wenling Zheng,4 and Wenli Ma1
Abstract
Purpose: The association between Toll-like receptor 2 (TLR2) - 196 to - 174del polymorphism and Toll-likereceptor 4 (TLR4) polymorphisms (Asp299Gly, Thr399Ile, and 3725G > C) and gastric cancer risk are still con-flicting. For better understanding of the effects of these four polymorphisms on gastric cancer risk, a meta-analysis was performed.Methods: An extensive search was performed to identify all case–control studies investigating such associations.Odds ratios (ORs) with 95% confidence intervals (CIs) were estimated to assess the relationship.Results: A total of 21 studies (3,436 cases and 4,239 controls) were found to be eligible for meta-analysis. In theoverall analysis, a significantly increased risk was observed in TLR4 Asp299Gly polymorphism (G allele vs. Aallele: OR = 1.84, 95%CI: 1.41, 2.39; GA vs. AA: OR = 1.89, 95%CI: 1.43, 2.48; Recessive model: OR = 1.90, 95%CI:1.44, 2.49) and TLR4 Thr399Ile polymorphism (T allele vs. C allele: OR = 1.97, 95%CI: 1.22, 3.18; TC vs. CC:OR = 1.94, 95%CI: 1.19, 3.15; Recessive model: OR = 1.98, 95%CI: 1.21, 3.21), whereas no associations were foundin any genetic models of TLR2 - 196 to - 174del and TLR4 3725G > C polymorphisms. Similar results werefound in the subgroup analyses by ethnicity. However, we detected that A allele carriers of the TLR4 Asp299Glypolymorphism might have an increase risk of gastric cancer in the Helicobacter pylori-positive population (G allelevs. A allele: OR = 2.01, 95%CI: 1.22, 3.31).Conclusion: The results of this meta-analysis indicate that the TLR4 Asp299Gly and Thr399Ile polymorphismsare risk factors for gastric cancer development.
Key words: gastric cancer, meta-analysis, single-nucleotide polymorphism, Toll-like receptors
Background
While gastric cancer incidence and mortality have bothshown decreasing trends in recent decades, gastric
cancer is still one of the most devastating human cancersworldwide, ranking fourth in incidence and second in mor-tality universally.1 In 2008, an estimated 989,600 new casesand 738,000 deaths occurred, accounting for 8% of the totalcases and 10% of total deaths, respectively.2 Over two-thirdsof the cases and deaths occurred in developing countries and42% in Eastern Asia.2 Although the precise etiology of gastric
cancer is unknown, unhealthy diet, infectious agents (e.g.,Helicobacter pylori), genetic factors, and pre-existing conditions(e.g., pernicious anemia, atrophic gastritis, and intestinalpolyps) are thought to be risk factors for the development ofgastric cancer.3 On the other hand, a diet that is high in rawfruits and vegetables, citrus fruits, and fiber may lower therisk.4 However, they do not provide a complete explanation.Recently, close attention has been paid to the association be-tween genetic factors, such as single-nucleotide polymor-phisms (SNPs) of genes, and the development of gastriccancer.5
1Institute of Genetic Engineering, Southern Medical University, Guangzhou, China.2Research Center for TCM Complexity System, Shanghai University of Traditional Chinese Medicine, Shanghai, China.3School of Life Sciences, Shanghai University, Shanghai, China.4Genome Centre of Southern China, Guangzhou, China.
Address correspondence to: Wenli Ma; Institute of Genetic Engineering, Southern Medical University; North of Guangzhou Avenue,Guangzhou 510080, ChinaE-mail: [email protected]
CANCER BIOTHERAPY AND RADIOPHARMACEUTICALSVolume 28, Number 9, 2013ª Mary Ann Liebert, Inc.DOI: 10.1089/cbr.2012.1395
674

Toll-like receptors (TLRs) belong to a group of patternrecognition receptors that play an important role in theregulation of inflammatory reactions and activation of theadaptive immune response to eliminate infectious patho-gens and cancer debris.6–8 In humans, 10 different TLRshave been identified.9 TLRs are important pattern recogni-tion receptors of microorganisms. Their dysregulationsowing to SNPs may alter the ligand binding and balancebetween pro- and anti-inflammatory cytokines and maythereby modulate the risk of developing chronic inflam-matory diseases and cancers.10–12
In the past decade, there were many epidemiologicalstudies, which have studied the association between TLRgene variants and risk of gastric cancer; however, the resultsof these studies were conflicting. For example, a case–controlstudy conducted in Brazil by de Oliveira13 indicated thatTLR2 - 196 to - 174del and TLR4 + 896G may increase therisk of gastric cancer. However, other studies reported thatthere were no associations between TLR polymorphisms(e.g., TLR4 3725G > C and TLR2 - 196 to - 174del) and therisk of gastric cancer.14,15 Similarly, inconclusive results werealso reported for other polymorphisms.
To further evaluate the association between TLR2 poly-morphisms (- 196 to - 174del) and TLR4 polymorphisms(Asp299Gly, Thr399Ile, and 3725G > C) and the risk of gastriccancer, a meta-analysis was conducted on all eligible pub-lished studies in the current study.
Methods
Selection of published studies
A systematic search was performed using the PubMed,Embase databases (last search: July 13, 2011) with the fol-lowing MeSH terms and keywords: TLR2, TLR4, Toll-likereceptor 2, Toll-like receptor 4, polymorphism, gastric cancer,gastric carcinoma, and stomach neoplasms. The scope ofarticle search was expanded according to the reference list ofretrieved studies. Studies included in our meta-analysis haveto meet the following criteria: (i) articles investigating theassociation between TLR2 polymorphism (- 196 to - 174del)and TLR4 polymorphisms (Asp299Gly, Thr399Ile, and3725G > C) and gastric cancer risk; (ii) case–control studies;(iii) providing available genotype frequency for computingodds ratios (ORs) with 95% confidence intervals (CIs); (iv)studies with full-text article. Major reasons for exclusion ofstudies were (i) only case population; (ii) the study did nothave the outcomes of comparison reported or it was notpossible to determine them; (iii) duplicate of previous pub-lication; (iv) benign tumors, precancerous lesions.
Data extraction
Two investigators ( Jian Chen and Sheng Hu) screenedtitles, abstracts, and full texts independently using a stan-dardized extraction form. For conflicting evaluation, anagreement was reached following consensus and discussion.For each study, the following characteristics were collected:the first author’s name, year of publication, country of origin,ethnicity, genotyping method, total number of cases andcontrols, H. pylori infection status, and genotype distribu-tions in cases and controls. We did not define any minimumnumber of patients to include in our meta-analysis.
Statistical analysis
All analyses were performed using STATA software(version 11.0; Stata Corporation, College Station, TX), and alltests were two sided with a significance level of 0.05, unlessstated otherwise. The Hardy–Weinberg equilibrium (HWE)in controls was assessed by the chi-squared test and a p < 0.05was considered as significant disequilibrium. If HWE dis-equilibrium existed ( p < 0.05), or it was impossible to evalu-ate this equilibrium, sensitivity analysis was performed. Thestrength of the association between the TLR polymorphismsand gastric cancer risk was measured by ORs with 95% CIs.The Q statistic was used to test for heterogeneity among thestudies included in the meta-analysis.16 When the Q-test p-value was no less than 0.1, the fixed effect model with theMantel–Haenszel method was used to calculate the pooledORs.17 Otherwise, a random effect model with the inversevariance method was used. To take TLR4 Asp299Gly as anexample, pooled ORs were obtained from a combination ofsingle studies by heterozygote comparison (GA vs. AA),homozygote comparison (GG vs. AA), dominant and reces-sive models (GG + GA vs. AA and GG vs. GA + AA), andallelic comparison (G vs. A). Similarly, the comparisons ofthe results of other polymorphisms were also obtained. Inaddition, we also performed stratification analyses on eth-nicity. The Begg and Mazumdar18 adjusted rank correlationtest and the Egger regression asymmetry test19 were plottedto provide a diagnosis of publication bias.
Results
Characteristics of the studies
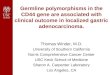
According to the search strategy of using different com-binations of key terms on PubMed, a total of 90 articles wereincluded in this meta-analysis (Fig. 1). Of the 90 studies, wereviewed the articles, abstracts, and the full texts. A total of21 case–control studies in11 articles met our inclusion crite-ria,12–15,20–26 including 3436 cases and 4550 controls. Table 1lists the characteristics of each study. Among these studies,four case–control studies, including 1294 cases and 1566
FIG. 1. Studies identified with criteria for inclusion andexclusion.
TOLL-LIKE RECEPTOR POLYMORPHISMS AND GASTRIC CANCER RISK 675

controls were investigated in the TLR2 polymorphism (- 196to - 174del); nine studies were included in the TLR4 As-p299Gly polymorphism analysis, with 1286 cases and 1215controls; the TLR4 Thr399Ile polymorphism employed 5studies, including 554 cases and 821 controls, whereas twostudies were included in the TLR4 3725G > C polymorphismanalysis, with 696 cases and 637 controls. The distribution ofgenotypes in the controls of all studies was consistent withthe HWE.
Meta-analysis
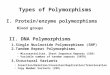
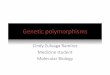
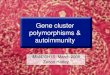
The association strength between TLR polymorphismsand the susceptibility for GC are presented in Table 2.Overall, no associations were found in any genetic models ofTLR2 (- 196 to - 174del) polymorphism (del vs. ins:OR = 1.27, 95%CI: 0.83, 1.95; insdel vs. deldel: OR = 1.12,95%CI: 0.74, 1.69; deldel vs. insins: OR = 1.61, 95%CI: 0.64,4.03; Dominant model: OR = 1.58, 95%CI: 0.70, 3.57; Re-cessive model: OR = 1.21, 95%CI: 0.75, 1.94) (Fig. 2) and TLR43725G > C (C allele vs. G allele: OR = 0.90, 95%CI: 0.75, 1.08;CG vs. GG: OR = 0.92, 95%CI: 0.72, 1.17; CC vs. GG:OR = 0.79, 95%CI: 0.51, 1.22; Dominant model: OR = 0.83,95%CI: 0.54, 1.27; Recessive model: OR = 0.89, 95%CI: 0.71,1.13), whereas a significant increased risk was observed inthe TLR4 Asp299Gly polymorphism (G allele vs. A allele:OR = 1.84, 95%CI: 1.41, 2.39; GA vs. AA: OR = 1.89, 95%CI:1.43, 2.48; Recessive model: OR = 1.90, 95%CI: 1.44, 2.49) (Fig.3) and TLR4 Thr399Ile polymorphism (T allele vs. C allele:OR = 1.97, 95%CI: 1.22, 3.18; TC vs. CC: OR = 1.94, 95%CI:1.19, 3.15; Recessive model: OR = 1.98, 95%CI: 1.21, 3.21)(Fig. 4). When stratified according to ethnicity, we found that
the TLR4 Asp299Gly polymorphism (G allele vs. A allele:OR = 1.90, 95%CI: 1.43, 2.51; GA vs. AA: OR = 1.96, 95%CI:1.46, 2.63; Recessive model: OR = 1.97, 95%CI: 1.47, 2.63) andthe TLR4 Thr399Ile polymorphism (T allele vs. C allele:OR = 2.84, 95%CI: 1.56, 5.15; TC vs. CC: OR = 2.81, 95%CI:1.53, 5.17; Recessive model: OR = 2.88, 95%CI: 1.57, 5.29) in-creased the cancer risk in Caucasians, however, no associa-tion was found in any subgroup of the TLR2 polymorphism.When stratified by the source of control, significant associa-tions between the TLR2 (- 196 to - 174del) polymorphism(del vs. ins: OR = 1.93, 95%CI: 1.18, 3.15), TLR4 Asp299Glypolymorphism (G allele vs. A allele: OR = 1.90, 95%CI: 1.43,2.51), TLR4 Thr399Ile polymorphism (T allele vs. C allele:OR = 2.84, 95%CI: 1.56, 5.15), and gastric cancer were foundin the population-based case–control subgroup (Table 2).When stratifying for H. pylori infection status (H. pylori-positive cancer patients compared with H. pylori-positivecontrols, or H. pylori-negative cancer patients compared withH. pylori-negative controls), no statistically findings wereobserved in the TLR2 (- 196 to - 174del) polymorphism andTLR4 Thr399Ile polymorphism, whereas we detected that Aallele carriers of the TLR4 Asp299Gly polymorphism mighthave an increase risk of gastric cancer in the H. pylori-positivepopulation (G allele vs. A allele: OR = 2.01, 95%CI: 1.22, 3.31).
Sensitivity analyses and publication bias
When examining the genotype frequencies in the controls,no significant deviation from HWE was detected, indicatingthat the final results of this meta-analysis were relativelystable and reliable. Both the Begg’s and Egger’s test wereconducted to assess the publication bias of literature. For the
Table 1. Characteristics of the Studies Included in the Meta-Analysis
First author Year Country Ethnicity Design Genotyping method Case Control p of HWE
TLR2 - 196 to - 174del(Delta22)Taharaa 2007 Japan Japanese PB Allele-specific PCR 289 146 0.18Zenga 2011 China Chinese HB PCR-RFLP 248 496 0.20de Oliveira 2012 Brazil Caucasian PB PCR-RFLP 174 225 0.73Hishidaa 2010 Japan Japanese HB PCR 583 699 0.82
TLR4_896A/G(Asp299Gly, rs4986790)Trejo-de la 2008 Mexico Mexican HB PCR-sequencing 38 144 0.80de Oliveira 2012 Brazil Caucasian PB PCR-RFLP 174 225 0.70Hold 2007 US Caucasian PB PCR-RFLP 304 211 0.30Hold 2007 Poland Caucasian PB PCR-RFLP 312 419 0.65Holda 2007 Scotland Caucasian PB PCR-RFLP 149 100 0.68Santini 2008 Italy Caucasian PB Allele-specific PCR 171 151 0.64Garza-Gonzaleza 2007 Mexico Mexican HB PCR-RFLP 78 189 0.60Rigolia 2010 Italy Caucasian PB PCR-RFLP 60 87 0.70
TLR4_1196C/T(Thr399Ile, rs4986791)Trejo-de la 2008 Mexico Mexican HB PCR-sequencing 61 202 0.75de Oliveira 2012 Brazil Caucasian PB PCR-RFLP 174 225 0.84Santini 2008 Italy Caucasian PB Allele-specific PCR 171 151 0.87Garza-Gonzaleza 2007 Mexico Mexican HB PCR-RFLP 78 156 0.71Rigolia 2010 Italy Caucasian PB PCR-RFLP 70 87 0.74
TLR4_3725G/C(rs11536889)Hishida 2009 Japan Japanese HB PCR-CTPP 583 401 0.37Kupcinskas 2011 Germany Caucasian HB PCR-CTPP 113 236 0.13
aStudy data of the status of Helicobacter pylori of gastric cancer were accessible.HWE, Hardy–Weinberg equilibrium; PCR-RFLP, polymerase chain reaction-restriction fragment length polymorphism; PCR-CTPP, PCR
with confronting two-pair primers; PB, population-based case–control study; HB, hospital-based case control.
676 CHEN ET AL.

Ta
bl
e2.
Po
ol
ed
Od
dR
at
io
sa
nd
95%
Co
nfi
de
nc
eIn
te
rv
al
so
fS
tr
at
ifi
ed
Me
ta
-A
na
ly
sis
VR
alle
lev
s.W
Tal
lele
Ht
vs.
WT
Ho
VR
Ho
vs.
WT
Ho
Dom
inan
tm
odel
Rec
essi
ve
mod
el
Su
bgro
up
Var
iabl
esN
OR
(95
%C
I)I2
(%)
OR
(95
%C
I)I2
(%)
OR
(95
%C
I)I2
(%)
OR
(95
%C
I)I2
(%)
OR
(95
%C
I)I2
(%)
TL
R2
-19
6to
-17
4del
(Del
ta22
)T
ota
l4
1.27
(0.8
3,1.
95)
90.9
1.12
(0.7
4,1.
69)
82.1
1.61
(0.6
4,4.
03)
86.6
1.58
(0.7
0,3.
57)
84.2
1.21
(0.7
5,1.
94)
87.6
Eth
nic
ity
Jap
anes
e2
1.25
(0.8
8,1.
77)
75.6
1.04
(0.8
5,1.
28)
01.
95(0
.63,
6.06
)85
.21.
93(0
.80,
1.58
)86
.91.
13(0
.93,
1.37
)0
Ch
ines
e1
0.7
1(0
.56
,0
.89
)_
0.7
0(0
.51
,0
.97
)_
0.4
7(0
.27
,0
.83
)_
0.5
7(0
.33
,0
.98
)_
0.6
6(0
.48
,0.8
9)
_C
auca
sian
12
.54
(1.6
6,
3.8
9)
_2
.40
(1.4
6,
3.9
2)
_6
.52
(1.3
6,
31
.22
)_
5.3
7(1
.27
,2
5.6
3)
_2
.63
(1.6
3,
4.2
2)
_D
esig
nP
B2
1.9
3(1
.18
,3
.15
)71
.81.
53(0
.65,
3.61
)85
.74
.15
(2.0
4,
8.4
6)
03
.98
(1.9
9,
7.9
6)
01.
82(0
.91,
3.64
)79
.9H
B2
0.88
(0.5
9,1.
31)
87.6
0.88
(0.5
9,1.
30)
75.3
0.76
(0.3
2,1.
82)
88.6
0.83
(0.4
3,1.
60)
77.1
0.85
(0.5
2,1.
38)
84.7
H.
py
lori
infe
ctio
nP
osi
tiv
e3
NA
_N
A_
NA
_N
A_
0.97
(0.6
6,1.
42)
72.3
Neg
ativ
e3
NA
_N
A_
NA
_N
A_
0.98
(0.7
6,1.
26)
26.9
TL
R4_
896A
/G
(Asp
299G
ly,
rs49
8679
0)T
ota
l9
1.8
4(1
.41
,2
.39
)5.
91
.89
(1.4
3,
2.4
8)
13.8
NA
_N
A_
1.9
0(1
.44
,2
.49
)12
.6E
thn
icit
yM
exic
an2
1.40
(0.6
5,3.
04)
20.0
1.42
(0.6
5,3.
12)
22.4
NA
_N
A_
1.42
(0.6
5,3.
12)
22.4
Cau
casi
an5
1.9
0(1
.43
,2
.51
)15
.41
.96
(1.4
6,
2.6
3)
23.7
NA
_N
A_
1.9
7(1
.47
,2
.63
)22
.0D
esig
nP
B5
1.9
0(1
.43
,2
.51
)15
.41
.96
(1.4
6,
2.6
3)
23.7
NA
_N
A_
1.9
7(1
.47
,2
.63
)22
.0H
B2
1.40
(0.6
5,3.
04)
20.0
1.42
(0.6
5,3.
12)
22.4
NA
_N
A_
1.42
(0.6
5,3.
12)
22.4
H.
py
lori
infe
ctio
nP
osi
tiv
e3
2.0
1(1
.22
,3
.31
)61
.32.
07(0
.81,
5.27
)66
.0N
AN
A2.
07(0
.81,
5.27
)66
.0N
egat
ive
11.
09(0
.32,
3.72
)_
1.10
(0.3
1,3.
84)
_N
A_
NA
_1.
10(0
.31,
3.84
)_
TL
R4_
1196
C/
T(T
hr3
99Il
e,rs
4986
791)
To
tal
51
.97
(1.2
2,
3.1
8)
36.2
1.9
4(1
.19
,3
.15
)34
.3N
A_
NA
_1
.98
(1.2
1,
3.2
1)
36.6
Eth
nic
ity
Mex
ican
20.
75(0
.28,
2.01
)59
.20.
75(0
.28,
2.02
)60
.0N
AN
A_
0.75
(0.2
8,2.
02)
60.0
Cau
casi
an3
2.8
4(1
.56
,5
.15
)0
2.8
1(1
.53
,5
.17
)0
NA
_N
A_
2.8
8(1
.57
,5
.29
)0
Des
ign
PB
32
.84
(1.5
6,
5.1
5)
02
.81
(1.5
3,
5.1
7)
0N
A_
NA
_2
.88
(1.5
7,
5.2
9)
0H
B2
0.75
(0.2
8,2.
01)
59.2
0.75
(0.2
8,2.
02)
60.0
NA
_N
A_
0.75
(0.2
8,2.
02)
60.0
H.
py
lori
infe
ctio
nP
osi
tiv
e2
0.98
(0.0
9,10
.93)
77.8
1.00
(0.0
8,12
.22)
79.0
NA
_N
A_
1.00
(0.0
8,12
.22)
79.0
Neg
ativ
e0
NA
_N
A_
NA
_N
A_
NA
_
TL
R4_
3725
G/
C(r
s115
3688
9)T
ota
l2
0.90
(0.7
5,1.
08)
00.
92(0
.72,
1.17
)0
0.79
(0.5
1,1.
22)
00.
83(0
.54,
1.27
)0
0.89
(0.7
1,1.
13)
0E
thn
icit
yA
sian
10.
88(0
.72,
1.07
)_
0.88
(0.6
8,1.
16)
_0.
79(0
.50,
1.24
)_
0.83
(0.5
3,1.
28)
_0.
86(0
.67,
1.11
)_
Cau
casi
an1
1.03
(0.6
2,1.
70)
_1.
08(0
.60,
1.94
)_
0.84
(0.1
6,4.
44)
_0.
83(0
.16,
4.36
)_
1.06
(0.6
0,1.
85)
_D
esig
nH
B2
0.90
(0.7
5,1.
08)
00.
92(0
.72,
1.17
)0
0.79
(0.5
1,1.
22)
00.
83(0
.54,
1.27
)0
0.89
(0.7
1,1.
13)
0H
.p
ylo
riin
fect
ion
0N
A_
NA
_N
A_
NA
_N
A_
Ran
do
mm
od
elw
asch
ose
nfo
rd
ata
po
oli
ng
wh
enp-
val
ue
<0.
10an
d/
or
I2>
50%
;o
ther
wis
efi
xed
mo
del
was
use
d.
Th
en
um
ber
sin
bo
ldin
dic
ated
stat
isti
call
ysi
gn
ifica
nt
val
ues
.N
,in
vo
lved
stu
die
s’n
um
ber
;OR
,o
dd
sra
tio
;CI,
con
fid
ence
inte
rval
s;V
R,
var
ian
t;W
T,w
ild
-ty
pe;
Ht,
het
ero
zyg
ote
;V
RH
o,
var
ian
th
om
ozy
go
te;
WT
Ho
,w
ide-
typ
eh
om
ozy
go
te;N
A,
no
tap
pli
cab
le.
677

FIG. 2. Forest plot of odd ratios (ORs) of TLR2 - 196 to - 174del polymorphism (del allele vs. ins allele) associated withcancer stratified by ethnicity.
FIG. 3. Forest plot of ORs of TLR4 Asp299Gly polymorphism (G allele vs. A allele) associated with cancer stratified byethnicity.
678 CHEN ET AL.

Begg’s test, no evidence of publication bias was observed inall comparison models in this meta-analysis, whereas theEgger’s test revealed statistical significance for publicationbias in all comparison models except one study12 (Table 3).When this study was deleted, I2 decreased from 34.3%(P = 0.192) to 0% (P = 0.663). While the summary OR for allelecontrast (T vs. C) remained significant (OR = 2.45, 95%CI:
1.46, 4.12), this result was similar to pooled OR withoutdeletion of any study (OR = 1.97, 95%CI: 1.22, 3.18).
Discussion
TLRs are a central part of the innate immune defenseagainst microorganisms. TLRs are evolutionarily conservedreceptors first described in Drosophila27 and contain threedomains: (i) leucine-rich repeat motif in the ectodomain; (ii)the single transmembrane domain; and (iii) cytoplasmicsignaling domains known as Toll IL-receptor domains.28 Theprotein function of TLRs may be impaired by SNPs withinTLR genes, causing an altered susceptibility to cancer. Theimportance of TLR polymorphisms’ influence on gastriccancer has been recognized in recent years, however, theexisting data are contradictory. Therefore, we provided acomprehensive analysis on the association of the TLR poly-morphisms with gastric cancer risk. To the best of ourknowledge, this is the first meta-analysis associating TLRpolymorphisms with gastric cancer risk.
For the past decades, the causal link between H. pylori andGC has been confirmed.29 TLR2 mediates immune responseagainst HP infection30 and Noguchi31 found that the del al-lele of the Delta22 SNP decreased the transcriptional activityof the TLR2 gene and may therefore increase the risk of H.pylori infection and lead to severe H. pylori-related disease,such as gastric cancer.30 However, our meta-analysis indi-cated that the TLR2 gene polymorphism (- 196 to - 174del,Delta22) may not be associated with gastric cancer. In thestratified analysis by ethnicity, no significant associationswere found. Possible explanations may include the follow-ing: (i) lack of case–control studies limited our evaluation onthe association between Delta22 and gastric cancer risk; (ii)
FIG. 4. Forest plot of ORs of TLR4 Thr399Ile (T allele vs. C allele) associated with cancer stratified by ethnicity.
Table 3. The Results of Begg’s and Egger’s
Test for Publication Bias
Begg’s test Egger’s test
Comparison type z p t p
TLR2 - 196 to - 174del(Delta22)Del/ins 1.02 0.308 1.15 0.370Deldel/insins 0.34 0.734 0.88 0.470Delins/insins 0.34 0.734 0.74 0.538Dominant model 0.34 0.734 0.99 0.427Recessive model 1.02 0.308 0.90 0.463
TLR4_896A/G (Asp299Gly, rs4986790)G/A 0.00 1.000 - 0.94 0.375GA/AA 0.36 0.721 - 0.88 0.407GG/AA 0.34 0.734 - 1.84 0.208Dominant model 0.34 0.734 - 1.69 0.234Recessive model 0.36 0.721 - 0.88 0.406
TLR4_1196C/T(Thr399Ile, rs4986791)T/C 1.22 0.221 - 3.23 0.048TC/CC 1.22 0.221 - 3.58 0.037Recessive model 1.22 0.221 - 3.36 0.044
The numbers in bold indicated no statistically significant values.
TOLL-LIKE RECEPTOR POLYMORPHISMS AND GASTRIC CANCER RISK 679

Mbulaiteye32 and Cavaleiro-Pinto33 showed a stronger as-sociation between noncardia gastric cancer and H. pylori in-fection than cardia gastric cancers, so no evidence of Delta22on gastric cancer was found because of the different casesthey recruited; and (iii) ethnic differences in the geneticbackground and the environment the population lived inmay contribute to different cancer susceptibility. For exam-ple, Zeng21 and de Oliveira13 found that individuals withTLR2 del allele could reduce cancer susceptibility in Chinese(del vs. ins: OR = 0.71, 95%CI: 0.56, 0.89), but increase cancersusceptibility in Caucasians (del vs. ins: OR = 2.54, 95%CI:1.66, 3.89), for the reason that the former subjects were fromthe northern Chinese and the latter Caucasian populationwere from Brazil (a country of high incidence of gastriccancer), suggesting that gastric cancer is a complex diseasewith many associated factors, such as the dietary habits andlife-style factors. However, detailed large-sample studiesshould be employed.
In the overall Asp299Gly and Thr399Ile analysis, weshowed that the presence of minor alleles significantly in-creased the risk of gastric cancer when compared to majoralleles, indicating that the two genetic variants in TLR4 maycrucially modify the susceptibility of GC. In the subgroup ofethnicity, we found significant associations between the twopolymorphisms and increased risks of GC in Caucasians, butnot in Mexicans. The inconsistency between the two ethni-cities may be explained by the different life styles and en-vironment factors of the different ethnic groups. A formermeta-analysis reported insignificant associations betweenAsp299Gly and GC because of fewer included studies.34
When stratified by H. pylori infection status for Asp299Glypolymorphism, we only found that patients with H. pyloriinfection (compared with H. pylori-positive controls) had asignificantly higher frequency of A allele carriers, however,these results should be considered with care because of thelimited studies. TLR4 is one of the best-studied TLRs.9 Ge-netic variants of the two polymorphisms may disrupt thenormal structure of the extracellular region of the TLR4 andare therefore thought to disturb TLR signaling and affect theproduction of inflammatory cytokines and the maturationand apoptosis of immune cells, which play a critical role inthe development of carcinogenesis.35 In conclusion, the twopolymorphisms should be paid more attention as the mostsignificant TLR4 polymorphisms.
In the overall TLR4 3725G > C analysis, our results did notshow any statistical significance. However, new and large-scale case–control studies are required to ascertain the ac-curate effect of the polymorphism on gastric cancer risk.
In interpreting the present results, some limitations shouldbe addressed. First, lack of the original data of the reviewedstudies limited our evaluation on the potential both gene–geneand gene–environment interactions. Second, the controls werenot uniformly defined. Some studies employed a healthypopulation as the reference group, whereas others used hos-pital patients without gastric cancer as the reference group.Thus, the controls may not always truly represent the under-lying source populations. Third, all case–control studies werefrom Asia, Europe, the United States, and Mexico. Therefore,these results may be applicable only to these ethnicities.
In summary, this meta-analysis indicated that Delta22,Asp299Gly, and Thr399Ile may increase the susceptibility ofgastric cancer in Caucasians, whereas Delta22 may decrease
the susceptibility of gastric cancer in Chinese. However, it isnecessary to employ detailed large-sample studies, contain-ing detailed individual data, standardized unbiased geno-typing methods, homogeneous gastric cancer patients, andwell-matched controls, to lead to a better, in-depth under-standing of the association between these polymorphismsand gastric cancer risk.
Acknowledgments
We thank all the people who helped in this study. Thisresearch was supported by the Guangdong Foundation forLeading Talented Scientists (C1030925).
Disclosure Statement
All authors have declared that no competing interestsexist.
References
1. Parkin DM, Bray F, Ferlay J, et al. Global cancer statistics,2002. CA Cancer J Clin 2005;55:74.
2. Jemal A, Bray F, Center MM, et al. Global cancer statistics.CA Cancer J Clin 2011;61:69.
3. Lee SG, Kim B, Choi J, et al. Genetic polymorphisms ofXRCC1 and risk of gastric cancer. Cancer Lett 2002;187:53.
4. Palli D. Epidemiology of gastric cancer: An evaluation ofavailable evidence. J Gastroenterol 2000;35 Suppl 12:84.
5. El-Omar EM, Chow WH, Rabkin CS. Gastric cancer and H.pylori: Host genetics open the way. Gastroenterology 2001;121:1002.
6. Akira S, Takeda K, Kaisho T. Toll-like receptors: Criticalproteins linking innate and acquired immunity. Nat Im-munol 2001;2:675.
7. Krieg AM, Vollmer J. Toll-like receptors 7, 8, and 9: Linkinginnate immunity to autoimmunity. Immunol Rev 2007;220:251.
8. Wang RF, Miyahara Y, Wang HY. Toll-like receptors andimmune regulation: Implications for cancer therapy. Onco-gene 2008;27:181.
9. Akira S, Takeda K. Toll-like receptor signalling. Nat RevImmunol 2004;4:499.
10. Achyut BR, Ghoshal UC, Moorchung N, et al. Association ofToll-like receptor 4 (Asp299Gly and Thr399Ileu) gene poly-morphisms with gastritis and precancerous lesions. HumImmunol 2007;68:901.
11. Lawrence T. Inflammation and cancer: A failure of resolu-tion? Trends Pharmacol Sci 2007;28:162.
12. Garza-Gonzalez E, Bosques-Padilla FJ, Mendoza-Ibarra SI,et al. Assessment of the Toll-like receptor 4 Asp299Gly,Thr399Ile and interleukin-8–251 polymorphisms in the riskfor the development of distal gastric cancer. BMC Cancer2007;7:70.
13. de Oliveira JG, Silva AE. Polymorphisms of the TLR2 andTLR4 genes are associated with risk of gastric cancer in aBrazilian population. World J Gastroenterol 2012;18:1235.
14. Kupcinskas J, Wex T, Bornschein J, et al. Lack of associationbetween gene polymorphisms of Angiotensin convertingenzyme, Nod-like receptor 1, Toll-like receptor 4, FAS/FASLand the presence of Helicobacter pylori-induced premalignantgastric lesions and gastric cancer in Caucasians. BMC MedGenet 2011;12:112.
15. Hishida A, Matsuo K, Goto Y, et al. No associations of Toll-like receptor 2 (TLR2) - 196 to - 174del polymorphism with
680 CHEN ET AL.

the risk of Helicobacter pylori seropositivity, gastric atrophy,and gastric cancer in Japanese. Gastric Cancer 2010;13:251.
16. Higgins JP, Thompson SG, Deeks JJ, et al. Measuring in-consistency in meta-analyses. BMJ 2003;327:557.
17. Petitti DB. Meta-analysis, decision analysis, and cost-effectiveness analysis: Methods for quantitative synthesis inmedicine. New York: Oxford University Press, 2000.
18. Begg CB, Mazumdar M. Operating characteristics of a rankcorrelation test for publication bias. Biometrics 1994;50:1088.
19. Egger M, Davey Smith G, Schneider M, et al. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315:629.
20. Tahara T, Arisawa T, Wang F, et al. Toll-like receptor 2–196to 174del polymorphism influences the susceptibility ofJapanese people to gastric cancer. Cancer Sci 2007;98:1790.
21. Zeng HM, Pan KF, Zhang Y, et al. Genetic variants of toll-like receptor 2 and 5, Helicobacter pylori infection, and risk ofgastric cancer and its precursors in a Chinese population.Cancer Epidemiol Biomarkers Prev 2011;20:2594.
22. Trejo-de la OA, Torres J, Perez-Rodriguez M, et al. TLR4single-nucleotide polymorphisms alter mucosal cytokineand chemokine patterns in Mexican patients with Helico-bacter pylori-associated gastroduodenal diseases. Clin Im-munol 2008;129:333.
23. Hishida A, Matsuo K, Goto Y, et al. Toll-like receptor 4+ 3725 G/C polymorphism, Helicobacter pylori seropositivity,and the risk of gastric atrophy and gastric cancer in Japa-nese. Helicobacter 2009;14:47.
24. Hold GL, Rabkin CS, Chow WH, et al. A functional poly-morphism of Toll-like receptor 4 gene increases risk of gas-tric carcinoma and its precursors. Gastroenterology 2007;132:905.
25. Santini D, Angeletti S, Ruzzo A, et al. Toll-like receptor 4Asp299Gly and Thr399Ile polymorphisms in gastric cancer
of intestinal and diffuse histotypes. Clin Exp Immunol2008;154:360.
26. Rigoli L, Di Bella C, Fedele F, et al. TLR4 and NOD2/CARD15 genetic polymorphisms and their possible role ingastric carcinogenesis. Anticancer Res 2010;30:513.
27. Hashimoto C, Hudson KL, Anderson KV. The Toll gene ofDrosophila, required for dorsal-ventral embryonic polarity,appears to encode a transmembrane protein. Cell 1988;52:269.
28. Huyton T, Rossjohn J, Wilce M. Toll-like receptors: Struc-tural pieces of a curve-shaped puzzle. Immunol Cell Biol2007;85:406.
29. Suzuki H, Iwasaki E, Hibi T. Helicobacter pylori and gastriccancer. Gastric Cancer 2009;12:79.
30. Smith MF, Jr., Mitchell A, Li G, et al. Toll-like receptor (TLR)2 and TLR5, but not TLR4, are required for Helicobacterpylori-induced NF-kappa B activation and chemokine ex-pression by epithelial cells. J Biol Chem 2003;278:32552.
31. Noguchi E, Nishimura F, Fukai H, et al. An associationstudy of asthma and total serum immunoglobin E levels forToll-like receptor polymorphisms in a Japanese population.Clin Exp Allergy 2004;34:177.
32. Mbulaiteye SM, Hisada M, El-Omar EM. Helicobacter pyloriassociated global gastric cancer burden. Front Biosci2009;14:1490.
33. Cavaleiro-Pinto M, Peleteiro B, Lunet N, et al. Helicobacterpylori infection and gastric cardia cancer: Systematic reviewand meta-analysis. Cancer Causes Control 2011;22:375.
34. Jing JJ, Li M, Yuan Y. Toll-like receptor 4 Asp299Gly andThr399Ile polymorphisms in cancer: A meta-analysis. Gene2012;499:237.
35. Chen R, Alvero AB, Silasi DA, et al. Inflammation, cancerand chemoresistance: Taking advantage of the Toll-like re-ceptor signaling pathway. Am J Reprod Immunol 2007;57:93.
TOLL-LIKE RECEPTOR POLYMORPHISMS AND GASTRIC CANCER RISK 681