Embed Size (px)
Citation preview

CARDIOVASCULAR DISEASES
Associations between overall physical activity level and cardiovascular risk factors
in an adult population
Mette Aadahl1,2, Michael Kjær3 & Torben Jørgensen11Research Centre for Prevention and Health, Glostrup University Hospital, Ndr. Ringvej 57, Building 84/85, 2600, Glostrup,
Denmark; 2Department of Medical Orthopaedics and Rehabilitation, University Hospital of Copenhagen, Rigshospitalet,
Blegdamsvej 9, 2100, Copenhagen, Denmark; 3Sports Medicine Research Unit, Bispebjerg Hospital, Bispebjerg Bakke 23,
2400, Copenhagen NV, Denmark
Accepted in revised form 19 December 2006
Abstract. Background: It is well established thatphysical activity level is inversely associated withcardiovascular morbidity and mortality, and withall-cause mortality. However, the dose–responserelationship between physical activity and other car-diovascular disease risk factors is not fully under-stood. The aim of the present study was to explorethe dose–response relationship between daily physicalactivity, as measured by a metabolic equivalent score,and BMI, waist circumference, waist hip ratio, totalcholesterol, HDL, LDL, triglycerides, systolic anddiastolic blood pressure. Methods: A total of 1693men and women, 33–64 years of age, from the 3 yearfollow-up of a population-based intervention study,were included in this cross-sectional study. Informa-tion on physical activity and other lifestyle factorswas obtained by self-report questionnaire. Associa-tions between activity level and biological variables
were explored by general linear regression. Results:Data from 835 (51%) men and 805 (49%) womenwere included. Mean age was 50.8 years (33–64). Asignificant inverse association between average 24-hour physical activity level £ 45 METs and waistcircumference (men p = 0.012, women p = 0.011),BMI (p = 0.0004), waist-hip-ratio (p = 0.002) andtriglycerides (p = 0.0001) was found as well as apositive association with HDL (p = <0.0001). Inthose with an activity level above 45 METs there wereno associations. No association was found with totalcholesterol, LDL, systolic or diastolic blood pressure.Conclusion: This study suggests a linear dose–re-sponse relationship between activity level and certainbiological cardiovascular risk factors up to a thresh-old of a daily 24 h MET-score of 45, which corre-sponds to a moderate physical activity level.
Key words: Anthropometric measures, Blood pressure, Dose–response, Physical activity, Serum lipids,Questionnaire
Abbreviations: BMI = Body mass index; BP = Blood pressure; CVD = Cardiovascular disease; HDL =Highdensity lipoprotein; IHD = Ischemic heart disease; LDL = Low density lipoprotein; MET= Metabolic equiv-alent; REE = Resting energy expenditure
Introduction
Physical activity is known to have an overallfavourable influence on obesity and other biologicalcardiovascular disease (CVD) risk factors such ashigh waist circumference, dyslipidemia and hyper-tension [1–5]. The associations between physicalactivity and CVD risk factors have been found in anumber of cross-sectional studies [6–14], and inter-vention studies have established that CVD risk fac-tors can to some extent be modified through exercise[15–17]. Physical inactivity is also an independentCVD risk factor, since prospective epidemiologicalstudies find an inverse relationship between physicalactivity level and cardiovascular as well as all causemortality [18–22]. However, in several of these studies
the measurements of physical activity are crude esti-mates that do not allow for a detailed exploration ofthe relationship between activity level and risk fac-tors. In accordance with this, the magnitude and typeof association between physical activity level andCVD risk factors differ substantially between studies.Most large scale epidemiological studies have usedself-report questionnaires for measuring physicalactivity [2 ,6, 20, 23]. A 4-way classification of activitylevel at work and in leisure time has been usedextensively [24] and has proven a valid measurementof physical activity level in population studies [2, 20,23]. Other studies, more limited in number, haveapplied objective measures of physical activity, suchas accelerometry, heart-rate measurement or stableisotopes [7, 10, 11]. However, these studies have often
European Journal of Epidemiology (2007) 22:369–378 � Springer 2007DOI 10.1007/s10654-006-9100-3

investigated a limited number of subjects only.Regardless of the type of physical activity measure-ment, all studies seem to find some significant asso-ciations between physical activity and risk ofcardiovascular disease, but neither the biologicalmechanisms behind the associations nor the rela-tionship and interactions between risk factors seemfully understood yet. In particular it is not clearwhether the dose–response relationship betweenphysical activity level and biological CVD risk factorsis linear through the entire range of physical activitylevels or if a threshold of benefits may be observed inthe association.
The aim of the present study was to explore theassociation between total physical activity level asmeasured by a self-report MET-score and biologicalcardiovascular disease risk factors in a randomsample of adult Danish men and women between 33and 63 years of age. Furthermore to study the vari-ation in biological CVD risk factors by physicalactivity level as measured by MET-score and 4-wayactivity classification, respectively.
Methods
Population sample
A total of 1693 men and women between 33 and64 years of age from the 3 year follow-up of the Inter99 study were included in the present study. The Inter99 study is a population-based intervention study,initiated in 1999 [25]. The initial study populationconsisted of 61.301 men and women between 30 and60 years of age, living in Copenhagen County andobtained through the Danish Civil Registration Sys-tem. The population was pre-randomised into threegroups: a high intensity intervention group (A), a lowintensity intervention group (B) and a control group(C). Group A and B (n = 13.016) were invited for aninitial health examination and an assessment of riskof ischemic heart disease (IHD) at baseline. Risk ofIHD was assessed using the computer programme‘‘The Copenhagen Risk Score’’, which calculates the10 year absolute risk of IHD by mean of sex, age,heredity, former IHD, diabetes, height, weight,smoking habits, cholesterol and blood pressure [26].High risk was defined as the upper quintile of abso-lute risk for IHD within 10 years calculated for eachage and sex-group or at least one of the followingcharacteristics: daily smoking, systolic blood pressure‡160 mm Hg, total cholesterol ‡7.5 mmol/l, bodymass index ‡30, history of diabetes or either diabetesor impaired glucose tolerance as evaluated from anoral glucose tolerance test [25].
In both groups (A and B) those at high risk wereoffered life-style consultation at baseline and at oneand 3 year follow-up, whereas those at low risk werejust asked to fill out a questionnaire. Those at high
risk in group A were offered participation in a groupintervention in addition to the life-style consultations.Of the 13.016 people sampled, 82 individuals werenon-eligible, as they had died or could not be traced.Of the remaining 12.934 a total of 6906 (53.4%)turned up for the investigation. Of these 122 wereexcluded either due to alcoholism or drug abuse(n = 23) or because of linguistic problems (n = 99)leaving 6.784 (52.5%) participants in the study [25].
The 3 year follow-up study was conducted betweenApril 8th 2002 and April 13th 2004 and a total of 2,504high risk individuals from group A (n = 2,247) andgroup B (n = 257) showed up for the 3 year follow-upvisit at the centre. Out of these, all participants whocame after November 18th 2002 (n = 1693) where anew physical activity questionnaire [27] was applied inthe Inter 99 study, were included in the present cross-sectional study. A total of 1567 participants were fromgroup A and 126 participants were from group B.
Questionnaires
At the 3 year follow-up visit all participants an-swered a self-report questionnaire on life-style andother health aspects and were given a thoroughphysical examination. Information on physicalactivity level was obtained by a new self-reportquestionnaire measuring physical activity on anaverage weekday as a total 24 h metabolic equiva-lent (MET) score [27]. In validation studies, thequestionnaire was found to correlate well withphysical activity diaries (r = 0.74) [27], and to re-flect maximum oxygen uptake [28]. The question-naire was self-administered and respondents wereasked to describe their habitual physical activityand inactivity on an average weekday, by filling outthe amount of time spent on nine different intensitylevels of physical activity. The nine levels consistedof: sleep (0.9 METs), TV viewing and other leisuretime sedentary activity (1.0 METs), computeror desk work (1.5 METs), light standing activ-ity, cooking, washing dishes or driving a car(2.0 METs), light cleaning, walking down stairs(3 METs), brisk walking or bicycling to work or forpleasure (4.0 METs), gardening or carrying lightobjects upstairs (5.0 METs) aerobics, health clubexercise, chopping wood or shovelling snow (6.0METs) and vigorous activity, such as jogging,running, tennis etc. (>6.0 METs). The question-naire encompassed physical activity in the domains:leisure time, occupation, commuting, household andgardening all in one. The 24 h MET-score wascalculated by multiplying time spent on an activitylevel by the assigned MET-value and adding thenine MET activity levels together. Metabolicequivalents are a way of expressing intensity incomparison to resting energy expenditure (REE),with one MET equal to the standard for REE(roughly 3.5 ml of oxygen consumed per kilogram
370

of bodyweight) [29]. In addition participants werealso asked to classify themselves in one of fourgroups of leisure time activity: (1) mainly sedentary(2) light to moderate activity comprising walkingand/or riding a bicycle (3) regular sport and exer-cise or heavy gardening (4) athletic training; andlikewise in one of four (five) groups of workactivity: (1) mainly sedentary (2) predominantlywalking without heavy lifting (3) mainly walkingincluding climbing stairs or lifting heavy objects (4)heavy physical labour (5) not working [24].
Information on diet was obtained from a 48-itemfood-frequency questionnaire and participants wereclassified into three groups based on fruit, vegetable,fish and fat intake [30]. Participants with low fruit/vegetable and fish intake and high fat intake wereclassified as eating an unprudent diet, participantswith medium fruit/vegetable, fish and fat intake wereclassified as eating a moderately prudent diet andparticipants with a high fruit/vegetable and fish in-take and a low fat intake were classified as eating aprudent diet. Information on alcohol was recordedfrom self-report as units pr. week and participantswere classified as daily smokers/occasional smokers/ex-smokers and never smokers on the basis of a self-report question on smoking habits.
Biological variables and anthropometric measures
Biological variables were measured at the 3 yearfollow-up examination at the research centre [25].Participants were asked to be fasting from midnightprior to the examination. Blood pressure (BP) wasmeasured twice with a mercury sphygmomanometerafter 5 min of rest in lying position. Height wasmeasured without shoes to the nearest cm, weightwithout shoes and overcoat to the nearest kg andbody mass index (BMI) was calculated (kg/m2).Waist and hip circumference was measured in cm andwaist/hip ratio calculated. Waist circumference wasmeasured midway between the lower rib margin andiliac crest. Hip circumference was measured over lightclothing at the widest girth of the hip, using an un-stretched tape meter, without any pressure to bodysurface. Fasting blood samples were drawn forassessment of total cholesterol, HDL-cholesterol andtriglyceride. Total cholesterol, triglyceride and HDL-cholesterol were determined with enzymatic tech-niques (Boeringer Mannhein, Germany). LDL wascalculated by Fridewald’s equation. All participantsgave written consent before taking part in the study.The study was approved by the local ethics committee(KA 98 155) and was registered at Clinical Trials.gov(ID NCT00289237).
Quality of physical activity data
The population sample consisted of 1693 men andwomen. Out of the 1693 respondents, 84.2%
(n = 1426) had completed the questionnairedescribing their habitual physical activity and inac-tivity over 24 h exactly. A total of 12.6% (n = 214)had not managed to hit 24 h exactly, but had de-scribed their habitual physical activity in 20–23.9 h or24.1–2.8 h. These questionnaires were corrected byadding or subtracting the missing or the excess timemultiplied by the intensity factor 2.0 MET to thetotal 24 h MET score. The intensity factor 2.0 METcorresponds to the mean of self-care/walking at home(2.5 METs) and sitting, eating/transportation etc (1.5METs). Former studies have shown that the extent ofthese low-intensity activities at home is very difficultfor most respondents to assess [27, 31]. The remaining3.1% (n = 53) of the questionnaires were filled outwith less than 20 hours. These questionnaires wereexcluded, based on the assumption that respondentshad not understood the concept of describing a 24-hour weekday and their responses were thereforeconsidered invalid. The 3.1% participants (n = 53)that were excluded did not differ significantly fromthe eligible sample with respect to key variables; 55%(n = 29) of the excluded participants were men witha mean age of 50.8 and 45% (n = 24) were womenwith a mean age of 51.1.
Statistical analysis
Associations between physical activity level and thebiological response variables were explored by linearsplines and in a series of general linear regressionmodels with sex, age, diet, alcohol and smokinghabits as co-variates and with body mass index, waistcircumference, waist hip ratio, LDL, HDL, triglyce-rides, total cholesterol, and systolic and diastolicblood pressure as response variables. BMI was in-cluded as a confounder only in the analyses withwaist circumference as dependent variable, because itmay be an intermediate variable in the chronologicalpathway between physical activity and CVD bio-markers. The co-variates were included stepwise. Theindependent variable physical activity was parame-terised as a continuous MET variable with two sep-arate parameter estimates for physical activity level£ 45 METs and >45 METs respectively, since plotsand univariate as well as multivariate splines of theassociation between the physical activity MET vari-able and antropometric measures, HDL and trigly-cerides, showed that the slope of the line changedmarkedly around 45 METs. No such phenomenonwas found with LDL, total cholesterol, systolic ordiastolic blood pressure and the physical activityvariable was therefore included with a single param-eter estimate. The distribution of the outcome vari-ables was studied, before further analyses.Triglyceride was not normally distributed and wastherefore logarithm transformed, before entered inthe regression analysis. Participants on current lipidlowering medication (n = 103) were excluded from
371

the analyses with cholesterol, HDL, LDL and tri-glycerides as response variables and participants oncurrent antihypertensive medication (n = 323) wereexcluded from the analyses with systolic and diastolicblood pressure as response variables. Interactionsbetween sex and physical activity, and age andphysical activity were explored in all general linearmodels.
Akaike’s information criteria [32] was used toexplore to what degree physical activity levelexplained the variation in biological variables, whenmeasured with the continuous MET variable, a4-way classification of leisure time physical activityand a 5-way classification of leisure time/workactivity, respectively (Appendix 1). Three analyseswere performed for each biological risk factor, eachanalysis with either the 4-way classification mea-surement of physical activity in leisure time, the5-way combined leisure time and work activity
classification or the physical activity MET-score asindependent variable. Akaike’s information criterionwas calculated in each analysis. Interpretation ofAkaike’s information criteria was performed on a‘smaller-is-better’ form [32]. P-values below 0.05were considered significant. Analyses were per-formed using the SAS 9.1 statistical package withproc GLM and proc REG.
Results
Study population
A total of 51% (n = 835) of the participants weremen and 49% (n = 805) were women. Mean age inthe total sample was 50.8 (33.0–64.6), 51.3 yearsamong men and 50.3 among women. Other popula-tion characteristics are presented in Table 1.
Table 1. Biological and sociodemografic characteristics among respondents according to gender (n = 1640)
Biological variables Men (n = 835) Women (n = 805)
Mean (SD) Mean (SD)
Systolic blood pressure mm Hg 136 (16.83) 129 (18.53)
Diastolic blood pressure mm Hg 87 (11.35) 82 (11.21)Total cholesterol mmol/L 5.65 (1.07) 5.63 (1.03)HDL mmol/L 1.25 (0.37) 1.54 (0.40)
LDL mmol/L 3.61 (0.97) 3.44 (0.93)Triglycerides mmol/L 1.73 (1.12) 1.32 (0.68)BMI 28.26 (4.52) 27.56 (6.11)Waist circumference cm 97.01 (11.85) 85.95 (14.33)
Waist hip ratio 0.96 (0.06) 0.84 (0.07)
Lifestyle, education and medicationAlcohol : (n = 1525) units/week 13.93 (13.07) 6.28 (6.62)
Smoking status: (n = 1633) n (%) n (%)Daily smoker 333 (40) 354 (44)Occasional smoker 33 (4) 26 (3)Ex-smoker 279 (34) 184 (23)
Never smoker 187 (22) 237 (30)
Diet: (n = 1620)Low fruit/vegetables/fish and high fat 125 (15) 72 (9)Medium fruit/vegetables/fish/fat 573 (70) 511 (64)High fruit/vegetables/fish and low fat 125 (15) 214 (27)
Leisure time physical activity: (n = 1625)
Sedentary 159 (19) 154 (19)Light activity 514 (62) 551 (69)Moderate activity 143 (17) 89 (11)High activity 14 (2) 1 (<1)
Vocational training: (n = 1277)Basic ( £ 1 year) 289 (44) 209 (34)
Short (1–3 years) 172 (26) 170 (28)Medium (3 years) 120 (18) 204 (33)Academic (>3 years) 81 (12) 32 (5)
Medication:Current lipid lowering therapy 66 (8) 37 (5)
Current hypertensive therapy 171 (21) 152 (19)
372

Men and women had a mean 24 h MET score of49.7 (12.2) and 45.3 (8.9), respectively. The differencein MET-score between genders was statisticallysignificant (p = 0.0001). In Table 2 mean MET-scores for the various classes of leisure time and workactivity are presented along with the index combiningwork and leisure time activity in a 5-way classification(appendix 1) and as seen from the table there was asignificant linear trend for mean MET-scores acrossactivity groups encompassing leisure time and work(Table 2). Out of the 1640 respondents, 49 %(n = 803) had a MET score £ 45 METs and 51%(n = 837) had a MET score >45 METs. Amongmen 58% (n = 483) had an activity level >45 METsand 44% (n = 354) of the women were active above45 METs.
Associations between physical activity level andbiological variables
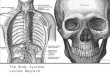
There was a strong linear association between phys-ical activity level and BMI in sedentary to moderatelyactive men and women, whereas the association wasnot seen in those with an activity level above mod-erate (>45 METs) (Figure 1). In the low activitygroup a decrease of 0.12 in BMI was seen for every1-MET-increase in activity level (Table 3). Whenco-variates sex, age, smoking, diet and alcohol wereincluded, 17% of the variation in BMI was explained.In the model with waist circumference, significant
interaction between sex and physical activity wasfound. In both men and women with an activity levelof £ 45 METs there was a significant inverse asso-ciation between physical activity and waistcircumference. In men with an activity level >45METs the association was no longer significant,whereas the association remained significant, but nowpositive in women (table 3). For both men and wo-men there was a significant association with waist hipratio in those with an activity level £ 45 METs.
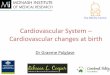
In the models with lipids as response variables,significant associations were found with HDL (Fig-ure 2) and triglycerides in those with an activity level£ 45 METs, whereas the association was not signifi-cant in those with an activity level above 45 METs.LDL and total cholesterol showed no associationswith physical activity. Finally no association wasfound between physical activity and neither systolicblood pressure, nor diastolic blood pressure(Table 3).
According to Akaike’s information criteria varia-tion in biological outcome variables was explained toan almost similar degree by the three different mea-sures of physical activity (Table 4). None of the threephysical activity measurements was systematicallysuperior to the other two in the analyses where asignificant association with physical activity wasfound (waist circumference, BMI, waist hip ratio,HDL and triglycerides).
Analyses performed with the 4- or 5-way activityclassification as independent variable and biologicalrisk factors as dependent variables, did not indicatean activity ‘threshold’ in the association (data notshown).
Discussion
In this cross sectional population-based study ofadult Danish men and women, we found a significant
Table 2. Physical activity classification. The crude 4/5 classquestions on physical activity in leisure time and at work
respectively, were combined in a matrix that categorizedparticipants in five activity classes encompassing both workand leisure time activity
Leisure time physical activity (4 class )
Activity level Mean MET score n
Sedentary 41.8 313Light 47.8 1065Moderate 53.1 232High 55.1 15
Work related physical activity (5 class)
Activity level Mean MET score nSedentary 40.8 473Light 47.5 576Moderate 56.7 224
High 65.0 67Not working 47.1 285
Work/leisure time physical activity (5 class)*Activity level Mean MET score (SD) n1 Sedentary 40.7 (6.9) 572
2 Light 47.8 (9.2) 6633 Moderate 54.2 (9.7) 2844 High 62.3 (12.6) 95
5 Very high 68.7 (7.8) 16
*p for trend = <0.0001.
Figure 1. General linear regression model with dependentvariable BMI. Final model adjusted for sex, age, smoking
status, diet and alcohol. Based on parameter estimates forindependent variable physical activity level as measured bythe continuous MET-score.
373

linear association between overall physical activitylevel up to 45 METs as measured by a self-reportMET-score and BMI, waist circumference, waist hipratio, HDL and triglycerides after adjustment forsignificant co-variates. The linear association did not
exist in those with an activity level above 45 METsand no associations were found between physicalactivity level and total cholesterol, LDL, systolic ordiastolic blood pressure. These findings suggest apossible threshold of benefits in the association
Table 3. General linear regression models: effect of physical activity level (total MET-score) on biological variables. Finaladjusted models. Separate parameter estimates for MET- score £ 45 and>45 in models with antropometric measures,
HDL and triglycerides
Response variable Parameter estimatesTotal MET-score
p-value Total MET-score R2
£ 45 METs >45 METs £ 45 METs >45 METs
Antropometric measures (n = 1640)
Waist circumferenceMen )0.14 )0.04 0.012* 0.06 0.86Women )0.15 0.14 0.011* 0.0003*
Waist hip ratio )0.0014 0.0003 0.002* 0.27 0.51Body mass index )0.12 )0.004 0.0004* 0.8 0.17
Serum lipids (n = 1503)HDL 0.011 0.001 <0.0001* 0.48 0.23Triglycerides (logarithm) )0.015 0.014 0.0001* 0.77 0.08
Total cholesterol 0.0013 0.61 0.06LDL 0.0002 0.93 0.04
Blood pressure(n = 1640)Systolic blood pressure 0.042 0.28 0.21Diastolic blood pressure )0.03 0.25 0.21
All models adjusted for sex, age, smoking status, diet and alcohol intake.
Model with waist circumference additionally adjusted for BMI.In models with serum lipids participants on self-reported statin medication excluded. In models with blood pressureparticipants on self-reported antihypertension medication excluded as well as participants with systolic blood pressure >
170 mm hg.*Significant estimates.
Figure 2. General linear regression model with dependent variable HDL. Final model adjusted for sex, age, smoking status,diet and alcohol. Based on parameter estimates for independent variable physical activity level as measured by the con-tinuous MET-score.
374

between physical activity and important cardiovas-cular biomarkers.
Several cross sectional population-based studies ofadult men and women have found significantassociations between physical activity level andanthropometric measures (BMI, waist circumferenceand waist hip ratio) in both genders and across age-group [6, 9–12, 14], but to our knowledge a physicalactivity threshold value as the one observed in thisstudy has not been reported previously. There was anunexpected finding, however. In women with anactivity level above 45 METs we found a positiveassociation between physical activity MET-score andwaist circumference, also before adjustment for BMI.There is no obvious explanation for this finding, butit may be confounded by e.g. hormonal changes inrelation to menopause, which may affect body com-position [11]. It could also be caused by women withhigh waist circumference overreporting their physicalactivity level or in fact being more physically activebecause of life-style counselling in the Inter 99 inter-vention.
Reported findings on physical activity and serumlipids seem inconsistent and the type of lipoproteinsubfraction measured differs between studies. An in-verse association with HDL is reported in themajority of cross sectional studies, regardless of thetype of physical activity measurement applied [6, 9,14]. One study included men only [33], another foundthe association in women only [13]. In relation totriglycerides, our finding of an association betweenphysical activity and triglycerides in both genderscorresponds with the findings of Jakes et al [9] andKronenberg et al [6], but other studies have not foundthis association [8, 13, 33]. An association with LDLhas been reported in men [8, 9] and women [6, 9], andwith total cholesterol in men [8, 9] and women [6, 9].Some studies have not found an association with
LDL and total cholesterol [13, 33], which correspondto the findings in the present study. The associationwith HDL and triglycerides was only significant up toan activity level threshold 45 METs, a phenomenonthat deserves some attention. It seems biologicallyplausible that the association between physicalactivity level and other CVD risk factors should bemore pronounced at lower activity levels and that athreshold for benefits of physical activity exists. Areview of major studies on physical activity havereported a similar finding in the association betweenphysical activity and CVD and all cause mortality[21]. The mortality risk seem to decrease markedlyfrom low to moderate levels of physical activity,whereas the risk reduction is limited or non-existentat increasing activity levels from moderate to high.We found no indication of a threshold in the analyseswith the four or five class physical activity variable.This may be explained by the uneven distributionacross the crude activity groups. There were very fewindividuals in the high activity groups and accordingto the leisure time activity classification 2/3 of theentire population (n = 1065) was in the light activitygroup.
The 45 MET threshold is difficult to interpret interms of absolute activity level. The physical activityquestionnaire was found to overestimate MET-scorescompared to physical activity diaries in the initialvalidation study [27], and the high average MET-scores observed in this study, 49.7 METs in men and45.3 METs in women, also indicate that the physicalactivity questionnaire overestimates activity level,when expressed as a total MET-score. Finally, otherstudies have found somewhat lower total MET-scoresof 40.6 [12] and 40.8 [31] in men and 38.8 in women[12], which support the fact that the MET-scores inour study are overestimated. Approximately half ofthe participants in this study had an activity levelbelow 45 METs, (49%, n = 803), and according tothe activity classification all sedentary individuals hadan average MET-score of approximately 40 METs(Table 2). An average daily MET-score of 45 METsis therefore likely to correspond to a moderateactivity level, but a more precise definition of thethreshold is not possible.
In this study we failed to detect an associationbetween self-reported physical activity level andblood pressure, as do several other studies [6, 8, 23].Barengo et al found an association between physicalactivity and diastolic BP only in both sexes [14],whereas Jakes et al found significant associationsbetween leisure-time physical activity and systolicand diastolic BP both in a very large population-based study of 14 189 adult men and women [9].Likewise a significant association has been found instudies with objective measurement of physicalactivity [7, 10]. The lack of association with BP in ourstudy may be attributed to the self-report measure-ment of physical activity or to the fact that our study
Table 4. Akaike’s information criteria for the three types ofphysical activity measurement: the MET-score, the 4-wayleisure time activity classification and the 5 class index
combining physical activity at work and in leisure time(appendix 1), in relation to each biological outcome vari-able
Biological variable MET-score
Continuousvariable
Leisure
timeactivity4 class
Leisure
time/Work5 class index
Waist circumference 5004 5008 5006Body mass index 4705 4682 4707
Waist hip ratio )8238 )8255 )8229HDL )3003 )3001 )2997LDL )143 )143 )138Triglyceride )180 )191 )178Total cholesterol 110 112 117Systolic BP 8186 8185 8184
Diastolic BP 6978 6974 6969
375

population was a high risk population with relativelyhigh levels of systolic and diastolic blood pressures.The variation in blood pressures may not have beensufficient to detect an association. Confounding byother factors that were not measured and thereforenot adjusted for, e.g. stress, may also explain the lackof association between physical activity and BP.
Furthermore we found that the physical activityMET-score described the variation in biological CVDrisk factors to a similar degree as the well-validatedand frequently used 4-way classification of leisuretime and work physical activity [24]. The size ofAkaike’s information criteria varied so little inabsolute numbers, in most cases <10, that definiteconclusions about detectable differences in types ofmeasurement cannot be drawn [32]. In addition tothis the MET-score has some advantages over theactivity classification. Statistically the continuousMET-variable permits the use of ‘genuine’ linearregression analyses that in this study led to observa-tion of the 45-MET ‘threshold’ in the associationbetween physical activity level and biological CVDrisk factors. Also, the MET-score comprises physicalactivity in multiple domains: leisure-time, occupa-tion, commuting, household and gardening. How-ever, the concept of physical activity on an averageweekday, which respondents are required to describewhen answering the questionnaire, involves a risk ofinformation bias, especially in relation to leisure-timephysical activity. Leisure-time sports and exercise istypically performed weekly, i.e. once or twice perweek and can therefore not be measured accuratelyby a questionnaire that assesses physical activity onan average weekday. Also, some respondents may byphysically active primarily on weekends, but will beclassified as inactive by a questionnaire that measuresphysical activity on an average weekday. These lim-itations in the physical activity measurement can haveled to misclassification. Finally the linear associationbetween physical activity and anthropometric mea-sures, HDL and triglycerides was found at loweractivity levels only. We cannot rule out the possibilitythat this is an artefact as a result of inaccuracy in thephysical activity measurement by the MET-score. Itcould be a reflection of the fact that physical activitylevel is measured more accurately at lower activitylevels. However, the fact that the MET-score corre-sponds well with the physical activity classification inleisure time and at work contradicts this.
The studied population was part of an on-goingprospective intervention study focussing on life style,which means that participants have recently beeninformed about the health benefits of physical activ-ity. This may generally have led to an overestimationof self-reported physical activity level, the so called‘social desirability bias’, in which case associationsmay have been underestimated. Moreover partici-pants may have received different levels of life-styleintervention in group A and B, which involves a risk
of additional bias and misclassification. However,both groups were offered individual life-style coun-selling at baseline and at 1 year follow-up and thedegree of possible adherence to guidelines and sub-sequent change in life-style is no doubt multi-factorialand not solely attributable to an offer of life-styleintervention.
Only a sub-sample of high-risk individuals from theInter 99 study population was included in the presentstudy, since the new physical activity questionnairewas not applied till midway through the 3 year follow-up of the Inter 99. However, the questionnaire wasanswered by all 3 year participants from a certain date,and the sub- sample is therefore representative of theentire three-year follow-up population.
Finally, the cross sectional design of the study doesnot allow for conclusions about causality in thechronological pathway between physical activity andCVD risk factors. In a public health perspective,however, the findings support the physical activityrecommendation that prescribes at least 30 min ofdaily physical activity of at least moderate intensity,since important biological CVD risk factors seeminversely associated to physical activity level in sed-entary to moderately active individuals. In conclusionthe present study also indicates that the greatesthealth benefit in relation to CVD risk factors:anthropometric measures, HDL and triglycerides,may be achieved by an increase in activity level froma low to a moderate level, i.e. up to a daily 24 h METscore of 45 METs, whereas limited gain seems to beachieved by an increase in physical activity from amoderate to a high level.
Acknowledgements
The Inter 99 Steering Committee: Torben Jørgensen(PI), Knut Borch-Johnsen (co-PI), Hans Ibsen,Charlotta Pisinger, Charlotte Glumer and Troels F.Thomsen. The study was supported by researchgrants from the Copenhagen Hospital Corporationand the Danish Physical Therapy Association.
Electronic supplementary material
The online version of this article (doi:10.1007/s10654-006-
9100-3) contains supplementary material, which is available
to authorized users.
Reference
1. Hu G, Tuomilehto J, Silventoinen K, Barengo N,Jousilahti P. Joint effects of physical activity, bodymass index, waist circumference and waist-to-hipratio with the risk of cardiovascular disease among
376

middle-aged Finnish men and women. Eur Heart J2004; 25: 2212–19.
2. Thune I, Njolstad I, Lochen ML, Forde OH. Physicalactivity improves the metabolic risk profiles in men andwomen: the Tromso Study. Arch Intern Med 1998; 158:1633–40.
3. Pereira MA, Folsom AR, McGovern PG, CarpenterM, Arnett DK, Liao D, et al. Physical activity andincident hypertension in black and white adults: the
Atherosclerosis Risk in Communities Study. Prev Med1999; 28: 304–12.
4. Hu FB, Li TY, Colditz GA, Willett WC, Manson JE.
Television watching and other sedentary behaviors inrelation to risk of obesity and type 2 diabetes mellitusin women. JAMA 2003; 289: 1785–91.
5. Hu G, Qiao Q, Silventoinen K, Eriksson JG, JousilahtiP, Lindstrom J, et al. Occupational, commuting, andleisure-time physical activity in relation to risk for Type2 diabetes in middle-aged Finnish men and women.
Diabetologia 2003; 46: 322–29.6. Kronenberg F, Pereira MA, Schmitz MK, Arnett DK,
Evenson KR, Crapo RO, et al. Influence of leisure time
physical activity and television watching on athero-sclerosis risk factors in the NHLBI Family HeartStudy. Atherosclerosis 2000; 153: 433–43.
7. Luke A, Kramer H, Adeyemo A, Forrester T, Wilks R,Schoeller D, et al. Relationship between blood pressureand physical activity assessed with stable isotopes.J Hum Hypertens 2005; 19: 127–32.
8. O’donovan G, Owen A, Kearney EM, Jones DW,Nevill AM, Woolf-May K, et al. Cardiovascular dis-ease risk factors in habitual exercisers, lean sedentary
men and abdominally obese sedentary men. Int J ObesRelat Metab Disord 2005.
9. Jakes RW, Day NE, Khaw KT, Luben R, Oakes S,
Welch A, et al. Television viewing and low participa-tion in vigorous recreation are independently associ-ated with obesity and markers of cardiovascular disease
risk: EPIC-Norfolk population-based study. Eur J ClinNutr 2003; 57: 1089–96.
10. Wareham NJ, Wong MY, Hennings S, Mitchell J,Rennie K, Cruickshank K, et al. Quantifying the
association between habitual energy expenditure andblood pressure. Int J Epidemiol 2000; 29: 655–60.
11. Sternfeld B, Bhat AK, Wang H, Sharp T, Quesenberry
CP Jr. Menopause, physical activity, and body com-position/fat distribution in midlife women. Med SciSports Exerc 2005; 37: 1195–202.
12. Schaller N, Seiler H, Himmerich S, Karg G, Gedrich K,Wolfram G, et al. Estimated physical activity in Ba-varia, Germany, and its implications for obesity risk:results from the BVS-II Study. Int J Behav Nutr Phys
Act 2005; 2: 6.13. Panagiotakos DB, Pitsavos C, Chrysohoou C,
Skoumas J, Zeimbekis A, Papaioannou I, et al.
Effect of leisure time physical activity on blood lipidlevels: the ATTICA study. Coron Artery Dis 2003;14: 533–39.
14. Barengo NC, Kastarinen M, Lakka T, Nissinen A,Tuomilehto J. Different forms of physical activity andcardiovascular risk factors among 24–64-year-old men
and women in Finland. Eur J Cardiovasc Prev Rehabil2006; 13: 51–59.
15. Slentz CA, Aiken LB, Houmard JA, Bales CW,Johnson JL, Tanner CJ, et al. Inactivity, exercise and
visceral fat. STRRIDE: a randomized, controlledstudy of exercise intensity and amount. J ApplPhysiol 2005; 99(4): 1613–8.
16. Kraus WE, Houmard JA, Duscha BD, Knetzger KJ,
Wharton MB, McCartney JS, et al. Effects of theamount and intensity of exercise on plasma lipopro-teins. N Engl J Med 2002; 347: 1483–92.
17. Ross R, Janssen I. Physical activity, total and regionalobesity: dose-response considerations. Med Sci SportsExerc 2001; 33: S521–S527.
18. Hu G, Tuomilehto J, Silventoinen K, Barengo NC,Peltonen M, Jousilahti P. The effects of physicalactivity and body mass index on cardiovascular, cancer
and all-cause mortality among 47 212 middle-agedFinnish men and women. Int J Obes Relat MetabDisord 2005; 29: 894–902.
19. Richardson CR, Kriska AM, Lantz PM, Hayward RA.
Physical activity and mortality across cardiovasculardisease risk groups. Med Sci Sports Exerc 2004; 36:1923–29.
20. Andersen LB, Schnohr P, Schroll M, Hein HO. All-cause mortality associated with physical activity duringleisure time, work, sports, and cycling to work. Arch
Intern Med 2000; 160: 1621–28.21. Blair SN, Cheng Y, Holder JS. Is physical activity or
physical fitness more important in defining healthbenefits?. Med Sci Sports Exerc 2001; 33: S379–S399.
22. Wannamethee SG, Shaper AG. Physical activity in theprevention of cardiovascular disease: an epidemiologi-cal perspective. Sports Med 2001; 31: 101–14.
23. Aires N, Selmer R, Thelle D. The validity of self-re-ported leisure time physical activity, and its relation-ship to serum cholesterol, blood pressure and body
mass index. A population based study of 332,182 menand women aged 40–42 years. Eur J Epidemiol 2003;18: 479–85.
24. Saltin B, Grimby G. Physiological analysis of middle-aged and old former athletes. Comparison with stillactive athletes of the same ages. Circulation 1968; 38:1104–15.
25. Jorgensen T, Borch-Johnsen K, Thomsen TF, Ibsen H,Glumer C, Pisinger C. A randomized non-pharmaco-logical intervention study for prevention of ischaemic
heart disease: baseline results Inter99. Eur J CardiovascPrev Rehabil 2003; 10: 377–86.
26. Thomsen TF, Davidsen M, Ibsen H, Jorgensen T,
Jensen G, Borch-Johnsen K. A new method for CHDprediction and prevention based on regional risk scoresand randomized clinical trials; PRECARD and theCopenhagen Risk Score. J Cardiovasc Risk 2001; 8:
291–97.27. Aadahl M, Jorgensen T. Validation of a new self-report
instrument for measuring physical activity. Med Sci
Sports Exerc 2003; 35: 1196–202.28. Aadahl M, Kjær M, Kristensen JH, Mollerup B,
Jørgensen T. Self-reported physical activity compared
with maximal oxygen uptake in adults. Eur J Cardio-vasc Prev Rehabil 2006; In press.
29. Ainsworth BE, Haskell WL, Leon AS, Jacobs DR Jr,
Montoye HJ, Sallis JF, et al. Compendium of physicalactivities: classification of energy costs of human
377

physical activities. Med Sci Sports Exerc 1993; 25:71–80.
30. Toft U, Kristoffersen LH, Lau C, Borch-Johnsen K,Jorgensen T. The Dietary Quality Score: validation andassociation with cardiovascular risk factors: the Inter99study. Eur J Clin Nutr 2006; In press.
31. Norman A, Bellocco R, Bergstrom A, Wolk A. Validityand reproducibility of self-reported total physicalactivity–differences by relative weight. Int J Obes Relat
Metab Disord 2001; 25: 682–88.32. Harrell FE Jr. Further use of the Log Likelihood. In:
With Applications to Linear Models, Logistic Regres-
sion, and Survival Analysis. New York: Springer, 2001.
33. Fung TT, Hu FB, Yu J, Chu NF, Spiegelman D, ToflerGH, et al. Leisure-time physical activity, television
watching, and plasma biomarkers of obesity andcardiovascular disease risk. Am J Epidemiol 2000; 152:1171–78.
Address for correspondence:Mette Aadahl, Research Centrefor Prevention and Health, Glostrup University Hospital,
Ndr. Ringvej 57, Building 84/85, 2600, Glostrup, DenmarkPhone: +45-432-32197; Fax: +45-432-33977E-mail: [email protected]
378