Embed Size (px)
Citation preview

Original Investigation | Cardiology
Association of Sickle Cell Trait With Incidence of Coronary Heart DiseaseAmong African American IndividualsHyacinth I. Hyacinth, MD, PhD, MPH; Nora Franceschini, MD, MPH; Samantha R. Seals, PhD; Marguerite R. Irvin, PhD; Ninad Chaudhary, MBBS, MPH; Rakhi P. Naik, MD;Alvaro Alonso, MD, PhD; Cara L. Carty, PhD; Gregory L. Burke, MD, MS; Neil A. Zakai, MD, MSc; Cheryl A. Winkler, PhD; Victor A. David, MS; Jeffrey B. Kopp, MD;Suzanne E. Judd, PhD; Robert J. Adams, MD, MS; Beatrice E. Gee, MD; W. T. Longstreth Jr, MD, MPH; Leonard Egede, MD, MS; Daniel T. Lackland, DrPH;Charles S. Greenberg, MD; Herman Taylor, MD; JoAnn E. Manson, MD, DrPH; Nigel S. Key, MD; Vimal K. Derebail, MD; Abhijit V. Kshirsagar, MD; Aaron R. Folsom, MD;Suma H. Konety, MD; Virginia Howard, PhD; Matthew Allison, MD, MPH; James G. Wilson, MD; Adolfo Correa, MD, PhD; Degui Zhi, PhD; Donna K. Arnett, PhD;George Howard, DrPH; Alexander P. Reiner, MD, MS; Mary Cushman, MD, MSc; Monika M. Safford, MD, MS
Abstract
IMPORTANCE The incidence of and mortality from coronary heart disease (CHD) are substantiallyhigher among African American individuals compared with non-Hispanic White individuals, evenafter adjusting for traditional factors associated with CHD. The unexplained excess risk might be dueto genetic factors related to African ancestry that are associated with a higher risk of CHD, such asthe heterozygous state for the sickle cell variant or sickle cell trait (SCT).
OBJECTIVE To evaluate whether there is an association between SCT and the incidence ofmyocardial infarction (MI) or composite CHD outcomes in African American individuals.
DESIGN, SETTING, AND PARTICIPANTS This cohort study included 5 large, prospective,population-based cohorts of African American individuals in the Women’s Health Initiative (WHI)study, the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study, the Multi-Ethnic Study of Atherosclerosis (MESA), the Jackson Heart Study (JHS), and the Atherosclerosis Riskin Communities (ARIC) study. The follow-up periods included in this study were 1993 and 1998 to2014 for the WHI study, 2003 to 2014 for the REGARDS study, 2002 to 2016 for the MESA, 2002 to2015 for the JHS, and 1987 to 2016 for the ARIC study. Data analysis began in October 2013 and wascompleted in October 2020.
EXPOSURES Sickle cell trait status was evaluated by either direct genotyping or high-qualityimputation of rs334 (the sickle cell variant). Participants with sickle cell disease and those with ahistory of CHD were excluded from the analyses.
MAIN OUTCOMES AND MEASURES Incident MI, defined as adjudicated nonfatal or fatal MI, andincident CHD, defined as adjudicated nonfatal MI, fatal MI, coronary revascularization procedures, ordeath due to CHD. Cox proportional hazards regression models were used to estimate the hazardratio for incident MI or CHD comparing SCT carriers with noncarriers. Models were adjusted for age,sex (except for the WHI study), study site or region of residence, hypertension status or systolicblood pressure, type 1 or 2 diabetes, serum high-density lipoprotein level, total cholesterol level, andglobal ancestry (estimated from principal components analysis).
RESULTS A total of 23 197 African American men (29.8%) and women (70.2%) were included in thecombined sample, of whom 1781 had SCT (7.7% prevalence). Mean (SD) ages at baseline were 61.2(6.9) years in the WHI study (n = 5904), 64.0 (9.3) years in the REGARDS study (n = 10 714), 62.0(10.0) years in the MESA (n = 1556), 50.3 (12.0) years in the JHS (n = 2175), and 53.2 (5.8) years in theARIC study (n = 2848). There were no significant differences in the distribution of traditional factors
(continued)
Key PointsQuestion Is sickle cell trait associated
with increased risk of myocardial
infarction and coronary heart disease
among African American individuals?
Findings In this cohort study of 23 197
African American individuals in 5
cardiovascular epidemiologic studies,
sickle cell trait was not associated with
increased risk of myocardial infarction or
coronary heart disease among African
American individuals.
Meaning In this study, sickle cell trait
was not associated with increased risk of
fatal and nonfatal myocardial infarction
or coronary heart disease, suggesting
that these disorders may not be
associated with sickle cell trait–related
sudden death.
+ Supplemental content
Author affiliations and article information arelisted at the end of this article.
Open Access. This is an open access article distributed under the terms of the CC-BY License.
JAMA Network Open. 2021;4(1):e2030435. doi:10.1001/jamanetworkopen.2020.30435 (Reprinted) January 5, 2021 1/13
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 05/26/2021

Abstract (continued)
associated with cardiovascular disease by SCT status within cohorts. A combined total of 1034participants (76 with SCT) had incident MI, and 1714 (137 with SCT) had the composite CHD outcome.The meta-analyzed crude incidence rate of MI did not differ by SCT status and was 3.8 per 1000person-years (95% CI, 3.3-4.5 per 1000 person-years) among those with SCT and 3.6 per 1000person-years (95% CI, 2.7-5.1 per 1000 person-years) among those without SCT. For the compositeCHD outcome, these rates were 7.3 per 1000 person-years (95% CI, 5.5-9.7 per 1000 person-years)among those with SCT and 6.0 per 1000 person-years (95% CI, 4.9-7.4 per 1000 person-years)among those without SCT. Meta-analysis of the 5 study results showed that SCT status was notsignificantly associated with MI (hazard ratio, 1.03; 95% CI, 0.81-1.32) or the composite CHD outcome(hazard ratio, 1.16; 95% CI, 0.92-1.47).
CONCLUSIONS AND RELEVANCE In this cohort study, there was not an association between SCTand increased risk of MI or CHD in African American individuals. These disorders may not beassociated with sickle cell trait–related sudden death in this population.
JAMA Network Open. 2021;4(1):e2030435. doi:10.1001/jamanetworkopen.2020.30435
Introduction
The burden of cardiovascular disease (CVD) in general and coronary heart disease (CHD) in particularis disproportionately high among African American individuals,1,2 resulting in a substantial healthdisparity.3-5 Approximately 60% of this disparity is associated with the excess burden of classicalfactors associated with CVD among African American individuals compared with non-Hispanic Whiteindividuals.3,4,6-10 The associations of hypertension with CHD11 and of the apolipoprotein L1 (APOL1[RefSeq ID NG_023228]) risk gene variant (ie, G1 [rs73885319 and rs60910145] and/or G2[rs71785313]) with excess burden of hypertensive kidney disease among African Americanindividuals12-14 have raised the question of a possible association between genetic variation and someof the observed excess and unexplained burden of CHD among African American individualscompared with non-Hispanic White individuals. Ito et al15 reported that possession of 2 APOL1 riskalleles was associated with higher overall risk for CVD and with early age at onset among AfricanAmerican individuals. Although there have been inconsistent findings for the association betweenAPOL1 genotypes and CVD,16 there is a rationale that genetic variation is possibly associated with theobserved disparities in the incidence and prevalence of CVD in general and CHD in particular amongAfrican American individuals. Several studies have reported that in addition to the APOL1 genevariant, heterozygosity for the sickle cell variant (sickle cell trait [SCT]) was associated with theincidence and progression of chronic kidney disease (CKD) and albuminuria,17-19 a factor associatedwith CVD.20,21
Sickle cell trait results from the genetic inheritance of 1 normal and 1 sickle β-globin gene (ie, theheterozygous state for the sickle β-globin gene). Approximately 8% of African American individualsand 20% to 35% of African individuals are SCT carriers. The variant is attributable to a functionalsingle-nucleotide variant involving the substitution of GTG (valine) for GAG (glutamic acid) at thesixth amino acid position in the gene encoding β-globin. Long considered a silent or benign carrierstate, some studies have suggested a possible association between SCT and clinicalcomplications.22,23 For instance, among African American individuals with end-stage kidney disease,the prevalence of SCT was higher compared with that among those without the disease.19 Similarly,SCT is associated with a higher risk for CKD and albuminuria,17,24 kidney medullary carcinoma,25,26
venous thromboembolism in various clinical contexts,27-29 and pulmonary embolism.30
Furthermore, individuals with SCT may have a prothrombotic state characterized by higher serumlevels of C-reactive protein,31 F2.1 fragments, thrombin-antithrombin complex, and D-dimer32; thesebiomarkers have been associated with an increased risk of CHD. Thus, given the association between
JAMA Network Open | Cardiology Sickle Cell Trait and Coronary Heart Disease Among African American Individuals
JAMA Network Open. 2021;4(1):e2030435. doi:10.1001/jamanetworkopen.2020.30435 (Reprinted) January 5, 2021 2/13
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 05/26/2021

CKD and CVD20,33,34 and between SCT and CKD or end-stage kidney disease,17-19,24 we hypothesizedthat among African American individuals, the presence of SCT would be associated with a higherincidence of myocardial infarction (MI) and/or CHD. We also examined whether African Americanindividuals with SCT, compared with those without SCT, had a higher risk of MI or CHD afteradjustment for traditional factors associated with CHD.
Methods
Study SampleThis cohort study included 5 large population-based cohort studies: the Women’s Health Initiative(WHI) study,35 the Reasons for Geographic and Racial Differences in Stroke (REGARDS) study,36 theMulti-Ethnic Study of Atherosclerosis (MESA),37 the Jackson Heart Study (JHS),38,39 and theAtherosclerosis Risk in Communities (ARIC) study.40,41 The study sample consisted of participants inthese studies who self-identified as African American. The design and methods of each study havebeen previously described35,37-42 and are summarized in the eMethods in the Supplement. Onlyparticipants without evidence of CHD at baseline either by medical history or electrocardiographywere included in the analyses. The follow-up periods for each of the cohorts included in this studywere 1993 and 1998 to 2014 for the WHI study, 2003 to 2014 for the REGARDS study, 2002 to 2016for the MESA, 2002 to 2015 for the JHS, and 1987 to 2016 for the ARIC study. The sample from theJHS excluded participants who were also in the ARIC study cohort. All participants included in thesestudies provided prior written informed consent for genetic studies, and institutional review boardapproval was obtained by each cohort at each participating institution. This study followed theStrengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Exposure AssessmentThe primary exposure for this study was presence of the rs334 single-nucleotide variant, whichcauses the variant leading to the formation of hemoglobin S or sickle hemoglobin and the amino acidsubstitution (HBB p.Glu7Val). Assessment of SCT status was done by direct custom genotyping(n = 19 814), exome sequencing (n = 1979), or imputation into the remaining sample of AfricanAmerican individuals with genome-wide single-nucleotide variant genotyping (Affymetrix 6.0;Thermo Fisher Scientific) (n = 1404) (eMethods in the Supplement). Participants who werehomozygous for rs334 (ie, had sickle cell anemia) or were compound heterozygotes (ie, inherited 1sickle cell gene and 1 hemoglobinopathy gene), including 1 participant in the ARIC study, 3 in the JHS,and 2 in the WHI study, were excluded from the analyses. After further excluding participants withmissing genotype, CHD outcomes, or relevant covariate information and after ensuring no overlap ofparticipants (between the JHS and the ARIC study), a combined total of 23 197 participants wereincluded in this study (5904 from the WHI study, 10 714 from the REGARDS study, 1556 from theMESA, 2175 from the JHS, and 2848 from the ARIC study).
Covariate AssessmentEach study (cohort) administered questionnaires, a physical examination, and physiologicalassessment at baseline. Data collected included participants’ sociodemographic information, healthbehaviors, and medical and medication history. Physical examination included blood pressure,height, and weight measurements. Physiological assessment included testing of blood samples forfasting blood glucose and lipid profiles.
Factors associated with CHD included hypertension, type 1 or 2 diabetes, cigarette smoking, andserum total cholesterol and high-density lipoprotein levels. Hypertension was defined as a baselinesystolic blood pressure of 140 mm Hg or more, a diastolic blood pressure of 90 mm Hg or more, orself-reported use of antihypertensive medication. Diabetes was defined as a baseline fasting glucoselevel of 126 mg/dL or more (to convert to millimoles per liter, multiply by 0.0555), a nonfastingglucose level of 200 mg/dL or more, self-reported physician diagnosis of diabetes, or self-reported
JAMA Network Open | Cardiology Sickle Cell Trait and Coronary Heart Disease Among African American Individuals
JAMA Network Open. 2021;4(1):e2030435. doi:10.1001/jamanetworkopen.2020.30435 (Reprinted) January 5, 2021 3/13
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 05/26/2021

use of oral hypoglycemic medication or insulin. Cigarette smoking status was defined as self-reportof being a current smoker or not except in the WHI and ARIC studies, in which smoking status wasbased on history of smoking (ie, ever smokers vs never smokers). Serum lipid levels as a covariate wasdefined using total cholesterol levels, high-density lipoprotein cholesterol levels, or both.
Other covariates included annual household income, educational level, C-reactive proteinconcentration, use of statins at baseline, use of aspirin at baseline, and baseline estimated glomerularfiltration rate. Population substructure was assessed through estimation of global ancestry usingprincipal components analysis derived from genome-wide genotyping data.43 Adjustment forpopulation substructure was done using eigenvalues derived from the principal componentsanalysis.
Assessment of CHD OutcomesAdjudicated CHD outcomes were obtained during follow-up in each cohort and, for the purpose ofour study, were grouped into 2 outcomes. The first was MI, including fatal and nonfatal MI events.The second was a composite CHD outcome including nonfatal and fatal MI, other types of fatal CHDevents, and coronary revascularization procedures. The clinical and laboratory criteria for assessingand adjudicating MI and CHD in each cohort are published elsewhere35,37,41,42,44 and summarized inthe eMethods in the Supplement. All 5 cohorts used similar criteria for MI and CHD adjudication.
Statistical AnalysisData analysis began in October 2013 and was completed in October 2020. We tabulated baselinedemographic characteristics, factors associated with CVD, and follow-up data stratified by SCT statusand reported them as either proportions or means with SDs. The crude incidence of MI or CHD wasestimated per 1000 person-years and then meta-analyzed using inverse variance weighting a prioriassuming a random-effects model owing to the small number of cohorts (5) and potentialheterogeneity among study cohorts because of differences in sampling frame and some covariateascertainment. The association of SCT carrier status with incident MI or CHD was evaluated using Coxproportional hazards regression models and expressed as hazard ratios. The first set of analysesinvestigated the association between incident MI and SCT status. The second set of analysesinvestigated the association between incident composite CHD outcome and SCT status.
We performed a stepwise analysis with 4 levels of baseline covariate adjustment, resulting in 4analytical models for each end point and for each cohort. In model 1, we adjusted for age, sex,principal components of global genetic ancestry (derived from the genome-wide array genotypingdata), and region of residence for the REGARDS study (stroke belt [the 9 Southeastern states withthe highest incidence of and mortality from stroke] vs nonstroke belt) and the ARIC study (ForsythCounty vs Jackson) only because region was a sampling variable in both cohorts. In model 2, we alsoadjusted for the components of the Framingham CHD Risk Score (hypertension, diabetes, cigarettesmoking status, and total cholesterol level, high-density lipoprotein cholesterol level, or both)45,46 inaddition to the covariates in model 1. In model 3, we adjusted for all the covariates in model 2, inaddition to adjusting for income, educational level, serum C-reactive protein level, self-reportedbaseline statin use, and self-reported baseline aspirin use. In the WHI study, we also adjusted forclinical trial or observational study participation. In model 4, we added estimated glomerular filtrationrate to all the covariates in model 3. The results from the Cox proportional hazards regression models(ie, from each of models 1, 2, 3, and 4) were each meta-analyzed using inverse variance–weightedmeta-analysis assuming a random-effects model. We also present the results of the meta-analysis ofthe fully adjusted model (model 4) in forest plots. Statistical analysis was performed with Stata,version 12 (StataCorp LLC). All P values were from 2-sided tests and results were deemed statisticallysignificant at P < .05.
JAMA Network Open | Cardiology Sickle Cell Trait and Coronary Heart Disease Among African American Individuals
JAMA Network Open. 2021;4(1):e2030435. doi:10.1001/jamanetworkopen.2020.30435 (Reprinted) January 5, 2021 4/13
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 05/26/2021

Results
Baseline CharacteristicsA total of 23 197 African American men (29.8%) and women (70.2%) were included in the combinedsample. The mean (SD) ages for participants at baseline were 61.2 (6.9) years in the WHI study, 64.0(9.3) years in the REGARDS study, 62.2 (10.0) years in the MESA, 50.3 (12.0) years in the JHS, and53.2 (5.8) years in the ARIC study. Of the total 23 197 participants, 1781 had SCT; the prevalence ofSCT in our study ranged from 6.4% to 9.1% across cohorts, with a mean of 7.7%, which is consistentwith the reported range of population prevalence of SCT in the US.17,47,48 There were no differencesin the distribution of traditional factors associated with CVD by SCT status within each cohort-based comparison using a univariate χ2 test. Table 1 provides a detailed within-cohort comparison ofbaseline characteristics between participants with and without SCT.35-41
Table 1. Baseline Characteristics of Participants by Study Cohort and SCT Status
Variable
Participantsa
WHI study35 (N = 5904) REGARDS study36 (N = 10 714) MESA37 (N = 1556) JHS38,39 (N = 2175) ARIC study40,41 (N = 2848)
SCT No SCT SCT No SCT SCT No SCT SCT No SCT SCT No SCTFrequency of rs334 485/5904
(8.2)5419/5904(91.8)
802/10 714(7.5)
9912/10 714(92.5)
141/1556(9.1)
1415/1556(90.9)
171/2175(7.9)
2004/2175(92.1)
182/2848(6.4)
2666/2848(93.6)
Age, mean (SD), y 61.1(7.1)
61.2(6.9)
63.5(9.4)
64.0(9.3)
61.0(10.0)
62.0(10.0)
50.9(12.4)
50.3(12.0)
53.4(5.8)
53.2(5.8)
Male 0 0 287/802(35.8)
3836/9912(38.7)
64/141(45.4)
651/1415(46.0)
75/171(43.9)
768/2004(38.3)
72/182(39.6)
1171/2848(41.1)
Systolic bloodpressure, mm Hg,mean (SD)
130.7(16.8)
131.3(17.0)
131.6(17.7)
130.9(17.4)
131.0(20.0)
132.0(22.0)
123.6(16.1)
125.5(16.7)
129.0(21.0)
128(20.0)
Type 1 or 2diabetes
67/485(13.8)
585/5419(10.8)
241/802(30.0)
2896/9912(29.2)
32/141(22.7)
241/1415(17.0)
31/171(18.1)
376/2004(18.8)
30/182(16.5)
487/2666(18.3)
Hypertension 243/485(50.1)
2796/5419(51.6)
555/802(69.2)
7090/9912(71.5)
80/141(56.7)
835/1415(59.0)
80/171(46.8)
989/2004(49.4)
100/182(55.0)
1454/2666(54.5)
Current cigarettesmoking
233/485(48.0)
2807/5419(51.8)
141/802(17.5)
1739/9912(17.6)
27/141(19.1)
269/1415(19.0)
26/171(15.2)
294/2004(14.7)
43/182(23.6)
792/2666(29.7)
Atrial fibrillationb 0 0 9/802(1.1)
67/9912(0.7)
0 0 1/171(0.6)
5/2004(0.3)
0 2/2666(0.1)
LVHc NA NA 50/802(6.2)
502/9912(5.1)
NA NA 10/171(5.9)
80/2004(4.0)
8/182(4.4)
127/2666(4.8)
History of CVD 0 0 131/802(16.3)
1510/9912(15.2)
0 0 15/171(8.8)
177/2004(8.8)
NA NA
All incident MIevents
23/485(4.7)
307/5419(5.7)
21/802(2.6)
207/9912(2.1)
9/141(6.4)
80/1415(5.7)
5/171(2.9)
47/2004(2.4)
18/182(9.9)
317/2666(11.9)
Composite CHDevents
30/485(6.2)
461/5419(8.5)
42/802(5.2)
439/9912(4.4)
17/141(12.1)
107/1415(7.6)
7/171(4.1)
70/2004(3.5)
41/182(22.5)
500/2666(18.8)
History
Aspirin use NA NA 282/802(35.2)
3814/9912(38.5)
43/141(30.5)
431/1415(30.5)
29/171(17.0)
379/2004(18.9)
45/182(24.7)
748/2666(28.1)
Statin use 36/485(7.4)
354/5419(6.5)
233/802(29.1)
2868/9912(28.9)
28/141(19.9)
194/1415(13.7)
9/171(5.3)
186/2004(9.3)
0 6/2666(0.2)
Follow-up time,median, y
13.3 13.2 8.9 9.4 13.6 13.8 11.5 11.6 25.3 26.0
Total follow-uptime, person-years
5924.8 66 331.2 14 913 192 004 1918 19 527 1681.3 20 542.6 3970 58 590
Age at event,mean (SD), y
MI 73.3(7.6)
75.8(8.9)
71.0(8.3)
71.0(9.0)
69.0(9.7)
70.0(10.0)
62.1(7.4)
61.1(11.9)
70.3(8.9)
68.6(8.7)
Any CHD 72.1(7.5)
74.5(7.9)
71.7(9.2)
71.0(9.1)
68.0(9.5)
70.0(10.0)
60.3(6.8)
63.0(12.6)
69.5(9.3)
68.3(8.2)
Abbreviations: ARIC, Atherosclerosis Risk in Communities; CHD, coronary heart disease;CVD, cardiovascular disease; JHS, Jackson Heart Study; LVH, left ventricularhypertrophy; MESA, Multi-Ethnic Study of Atherosclerosis; MI, myocardial infarction;NA, not applicable; REGARDS, Reasons for Geographic and Racial Differences in Stroke;rs334, gene variant that causes sickle cell anemia; SCT, sickle cell trait; WHI, Women’sHealth Initiative.
a Data are presented as number/total number (percentage) of participants unlessotherwise indicated.
b Atrial fibrillation was determined by self-report or electrocardiographic evidence.c Left ventricular hypertrophy was determined by 12-lead electrocardiography.
JAMA Network Open | Cardiology Sickle Cell Trait and Coronary Heart Disease Among African American Individuals
JAMA Network Open. 2021;4(1):e2030435. doi:10.1001/jamanetworkopen.2020.30435 (Reprinted) January 5, 2021 5/13
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 05/26/2021

Association of SCT With MI or CHDA combined total of 1034 participants (76 with SCT) had incident MI and 1714 (137 with SCT) had thecomposite CHD outcome. Within-cohort analysis and subsequent meta-analysis showed that thecrude incidence rates for MI among participants with SCT (3.8 per 1000 person-years; 95% CI,3.3-4.5 per 1000 person-years) compared with those without SCT (3.6 per 1000 person-years; 95%CI, 2.7-5.1 per 1000 person-years) were not significantly different (Table 2).35-41 Similarly, significantdifferences were not found in the crude incidence of the composite CHD event among participantswith SCT (7.3 per 1000 person-years; 95% CI, 5.5-9.7 per 1000 person-years) compared with thosewithout SCT (6.0 per 1000 person-years; 95% CI, 4.9-7.4 per 1000 person-years).
The results of the fully adjusted multivariable models that also accounted for baseline kidneyfunction (model 4) for each cohort are presented in Table 3 and Table 4.35-41 Meta-analysis of resultsfrom model 4 for incident MI gave a hazard ratio of 1.03 (95% CI, 0.81-1.32), indicating no significantassociation between SCT and incidence of MI (Table 3 and Figure, A).35-41 Similarly, meta-analysis ofresults from model 4 for CHD showed that the hazard ratio for incident CHD was 1.16 (95% CI, 0.92-1.47) (Table 4 and Figure, B).35-41 A priori, we assumed a random-effects model and retained theresults of this model notwithstanding the fact that our test of heterogeneity indicated no significantheterogeneity between studies (I2 = 0.0%; P = .54 for the MI meta-analysis [Figure, A]; andI2 = 26.2%; P = .25 for the CHD meta-analysis [Figure, B]). This approach was adopted becauseheterogeneity exists between studies and the reliability of a test of heterogeneity with 5 studies isnot robust and thus not reliable.
Table 2. Crude Incidence of Myocardial Infarction and CHD Outcomes by Study Cohort and SCT Status
Outcome
Crude incidence, per 1000 person-years (95% CI)
WHI study35 REGARDS study36 MESA37 JHS38,39 ARIC study40,41 Meta-analysis
SCT No SCT SCT No SCT SCT No SCT SCT No SCT SCT No SCT SCT No SCTMyocardialinfarction
3.9(2.6-5.8)
4.6(4.1-5.1)
3.7(3.0-4.5)
2.8(2.6-3.0)
4.7(2.3-8.6)
4.1(3.3-5.1)
3.0(1.1-6.6)
2.3(1.7-3.0)
4.5(2.7-7.2)
5.4(4.8-6.0)
3.8(3.3-4.5)
3.6(2.7-5.1)
Any CHDevent
5.1(3.5-7.2)
6.9(6.3-7.6)
7.7(6.3-9.4)
6.3(5.9-6.7)
8.8(5.3-13.9)
5.5(4.5-6.6)
4.2(1.8-8.2)
3.4(2.7-4.3)
10.7(7.7-14.5)
8.7(7.9-9.5)
7.3(5.5-9.7)
6.0(4.9-7.4)
Abbreviations: ARIC, Atherosclerosis Risk in Communities; CHD, coronary heart disease;JHS, Jackson Heart Study; MESA, Multi-Ethnic Study of Atherosclerosis; REGARDS,
Reasons for Geographic and Racial Differences in Stroke; SCT, sickle cell trait; WHI,Women’s Health Initiative.
Table 3. Hazard Ratios for Myocardial Infarction Among Individuals With SCT Compared With Those Without SCT by Study Cohort
Modela
WHI study35 REGARDS study36 MESA37 JHS38,39 ARIC study40,41 Meta-analysis
HR (95% CI) P value HR (95% CI) P value HR (95% CI) P value HR (95% CI) P value HR (95% CI) P value HR (95% CI) P valueModel 1 0.94
(0.61-1.43).76 1.47
(0.83-2.61).18 1.26
(0.63-2.52).51 1.19
(0.55-2.67).66 0.82
(0.51-1.32).41 1.04
(0.82-1.33).71
Model 2 0.98(0.64-1.50)
.93 1.48(0.83-2.63)
.18 1.21(0.60-2.42)
.59 1.37(0.62-3.02)
.44 0.83(0.52-1.34)
.46 1.07(0.84-1.37)
.59
Model 3b 1.00(0.65-1.54)
.99 1.40(0.77-2.54)
.27 1.21(0.61-2.43)
.59 1.49(0.67-3.32)
.33 0.82(0.51-1.32)
.41 1.07(0.83-1.37)
.60
Model 4b 0.98(0.64-1.51)
.92 1.27(0.70-2.31)
.43 1.28(0.64-2.56)
.49 1.48(0.67-3.32)
.33 0.77(0.48-1.24)
.28 1.03(0.81-1.32)
.80
Abbreviations: ARIC, Atherosclerosis Risk in Communities; CHD, coronary heart disease;HR, hazard ratio; JHS, Jackson Heart Study; MESA, Multi-Ethnic Study of Atherosclerosis;REGARDS, Reasons for Geographic and Racial Differences in Stroke; SCT, sickle cell trait;WHI, Women’s Health Initiative.a Model 1 adjusted for age, sex, study region (REGARDS and ARIC studies only), and
principal components analysis of global genetic ancestry; model 2 adjusted forcomponents of model 1 and components of the Framingham CHD risk score(hypertension [defined as diagnosed or current use of antihypertensive medication] ora high systolic blood pressure), diabetes, cigarette smoking (current vs noncurrent
except in the WHI and ARIC studies, in which the data were ever smokers vs neversmokers), and serum total cholesterol and/or high-density lipoprotein cholesterollevels; model 3 adjusted for components of model 2 and income, educational level,serum high-sensitivity C-reactive protein level, and history of statin and aspirin use(WHI analysis also adjusted for trial group among WHI participants); and model 4adjusted for components of model 3 and glomerular filtration rate, estimated from theCKD-Epi equation.
b For models 3 and 4 in the WHI study, the total sample size was 5744, with 473individuals with SCT.
JAMA Network Open | Cardiology Sickle Cell Trait and Coronary Heart Disease Among African American Individuals
JAMA Network Open. 2021;4(1):e2030435. doi:10.1001/jamanetworkopen.2020.30435 (Reprinted) January 5, 2021 6/13
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 05/26/2021

Discussion
In this study, we sought to examine whether SCT was independently associated with an increasedincidence of MI or CHD in African American individuals. The premise is based on studies showing thatSCT was associated with putative factors (inflammation and thrombosis) associated with CHD inaddition to CKD, which is associated with atherosclerotic CVD.19,27,49,50 In this analysis of 23 197unrelated individuals from 5 different population-based cohort studies, our main finding was thatSCT was not associated with the incidence of MI or CHD in both unadjusted and fully adjusted(accounting for factors associated with CVD) models.
Furthermore, in fully adjusted models, significant associations were not present between SCTand incident MI within each cohort or after meta-analysis of all 5 studies. In addition, SCT was notindependently associated with increased risk of the composite CHD outcome. Although unadjusted
Table 4. Hazard Ratios for Combined CHD Outcomes Among Individuals With SCT Compared With Those Without SCT by Study Cohort
Modela
WHI study35 REGARDS study36 MESA37 JHS38,39 ARIC study40,41 Meta-analysis
HR (95% CI) P value HR (95% CI) P value HR (95% CI) P value HR (95% CI) P value HR (95% CI) P value HR (95% CI) P valueModel 1 0.81
(0.56-1.17).26 1.35
(0.91-1.99).13 1.87
(1.11-3.12).01 1.03
(0.24-4.40).97 1.20
(0.87-1.65).27 1.20
(0.91-1.54).12
Model 2 0.83(0.57-1.22)
.35 1.39(0.94-2.05)
.10 1.77(1.06-2.97)
.03 1.00(0.23-4.37)
.99 1.20(0.87-1.66)
.26 1.21(0.93-1.56)
.15
Model 3b 0.86(0.59-1.25)
.43 1.34(0.90-2.00)
.15 1.68(1.00-2.83)
.05 1.15(0.26-5.15)
.85 1.20(0.87-1.65)
.27 1.19(0.95-1.48)
.13
Model 4b 0.85(0.58-1.24)
.39 1.26(0.84-1.87)
.27 1.80(1.06-3.04)
.03 1.16(0.26-5.20)
.84 1.13(0.82-1.56)
.45 1.16(0.92-1.47)
.21
Abbreviations: ARIC, Atherosclerosis Risk in Communities study; CHD, coronary heartdisease; HR, hazard ratio; JHS, Jackson Heart Study; MESA, Multi-Ethnic Study ofAtherosclerosis; REGARDS, Reasons for Geographic and Racial Differences in Stroke; SCT,sickle cell trait; WHI, Women’s Health Initiative.a Model 1 adjusted for age, sex, study region (REGARDS study only), and principal
components analysis of global genetic ancestry; model 2 adjusted for components ofmodel 1 and components of the Framingham CHD risk score (hypertension [defined asdiagnosed or current use of antihypertensive medication] or a high systolic bloodpressure), diabetes, cigarette smoking (current vs noncurrent except in the WHI and
ARIC studies, in which the data were ever smokers vs never smokers), and serum totalcholesterol and/or high-density lipoprotein cholesterol levels; model 3 adjusted forcomponents of model 2 and income, educational level, serum high-sensitivityC-reactive protein level, and history of statin use (WHI analysis also adjusted for trialgroup among WHI participants); and model 4 adjusted for components of model 3 andglomerular filtration rate, estimated from the CKD-Epi equation.
b For models 3 and 4 in the WHI study, the total sample size was 5744, with 473individuals with SCT.
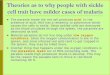
Figure. Random-Effects Meta-Analysis of the Fully Adjusted Cox Proportional Hazards Regression Model
0.30 3.321.00
HR (95% CI)
Weight, %HR (95% CI)Study
Incident MIA
33.27WHI35
Overall(I2 = 0.0%, P = .54)
0.98 (0.64-1.51)17.20REGARDS36 1.27 (0.70-2.31)12.75MESA37 1.28 (0.64-2.56)9.57JHS38,39 1.48 (0.67-3.32)27.21ARIC40,41 0.77 (0.48-1.24)
1.03 (0.81-1.32) 100.00
0.192 5.21.00
HR (95% CI)
Weight, %HR (95% CI)Study
Incident CHDB
25.79WHI35
Overall(I2 = 26.2%, P = .25)
0.85 (0.58-1.24)24.04REGARDS36 1.26 (0.84-1.87)15.97MESA37 1.80 (1.06-3.04)2.41JHS38,39 1.16 (0.26-5.20)31.80ARIC40,41 1.13 (0.82-1.56)
1.16 (0.92-1.47) 100.00
Protectsfrom MI
Favors development of MI
Protectsfrom CHD
Favors development of CHD
A, Association of sickle cell trait with incidentmyocardial infarction (MI). B, Association of sickle celltrait with incidence of any coronary heart disease(CHD). The follow-up periods were 1993 and 1998 to2014 for the Women’s Health Initiative (WHI) study,2003 to 2014 for the Reasons for Geographic andRacial Differences in Stroke (REGARDS) study, 2002 to2016 for the Multi-Ethnic Study of Atherosclerosis(MESA), 2002 to 2015 for the Jackson Heart Study(JHS), and 1987 to 2016 for Atherosclerosis Risk inCommunities (ARIC) study. Squares represent means,with horizontal lines representing 95% CIs. Diamondsrepresent the pooled means with the points of thediamonds representing the 95% CIs of the pooledmeans. The dotted vertical lines indicate thedirectionality of the overall effect. The sizes of the datamarkers indicate the individual weight for each study.HR indicates hazard ratio.
JAMA Network Open | Cardiology Sickle Cell Trait and Coronary Heart Disease Among African American Individuals
JAMA Network Open. 2021;4(1):e2030435. doi:10.1001/jamanetworkopen.2020.30435 (Reprinted) January 5, 2021 7/13
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 05/26/2021

meta-analyzed incidence rates for CHD were higher among SCT carriers than among non-SCTcarriers, the fully adjusted meta-analyzed hazard ratio for the composite CHD outcome was notsignificant. Both SCT risk estimates for MI and the composite CHD outcome were not statisticallysignificant in the meta-analyses.
An examination of the results in each cohort indicated that, among participants with SCT in theREGARDS study, the MESA, and the JHS, the risk of MI was slightly higher compared with that amongparticipants without SCT, although the difference was not statistically significant. Also, the broad95% CIs indicate a less-robust estimate of risk within each of these cohorts. However, estimates inthe MESA cohort revealed that SCT was independently associated with a significantly higher risk ofthe composite CHD outcome. As was the case in the MI analysis, the risk of CHD was slightly higheramong participants with SCT in the REGARDS study, JHS, and ARIC study cohorts than among thosewithout SCT, but the difference was not statistically significant. The reasons for these differences inthe association of SCT with CHD in the MESA and the other cohorts is not known but might be relatedto the higher proportion of male participants in the MESA cohort (46%) compared with the othercohorts (approximately 8% excluding the WHI study), differences in age, and/or the prevalence ofother factors associated with CHD. This point is supported by 2 studies.51,52 One showed that SCTwas associated with a higher risk of retinopathy among men, but not women, with diabetes,51 andthe second showed that SCT was associated with coronary artery disease among men, but notwomen, with CKD.52 Despite having a higher proportion of men with SCT than men without SCT, theJHS cohort did not show a significant association between SCT and CHD, which could be owing tothe small number of CHD events in this cohort. However, sex likely did not have a significant effect onour results because our analysis was adjusted for sex and we expect this adjustment to haveaddressed any differential effect of sex. Future studies could explore this factor because the cohortsanalyzed in this study were not well powered to perform a sex-stratified analysis.
Our study is, to our knowledge, the largest to examine the association between SCT andincidence of MI and CHD and, as such, adds to the current literature. The findings may provide usefulinformation leading to a closer examination and a more thorough workup for a patient with SCT whopresents with CHD symptoms.
LimitationsThis study has limitations. We were unable to account for the modifying effect of other geneticfactors, such as alpha-thalassemia, which is a modifier of the effect of the sickle β-globin variant,53,54
although this variant has not been associated with CHD. We were also unable to stratify our analysisby sex owing to the limited number of events within sex strata; thus, we could not confirm the sexdifferences described in an earlier study.52 Future studies with larger samples will be needed toproperly address the question of whether SCT is associated with MI or CHD alone or whether theassociation varies by sex and other factors. In addition, we were not able to stratify our analysis bythe different CHD components, for instance, by examining individuals who underwent procedures(coronary artery bypass grafting or percutaneous transluminal coronary angioplasty) for CHD.
Conclusions
In this cohort study of 5 prospective studies, there was not a significant association between SCT andan increased risk of MI or CHD in African American individuals. Although prior studies showed thatSCT is associated with sudden death,55,56 our findings suggest that these disorders may not beassociated with SCT-related sudden death.
JAMA Network Open | Cardiology Sickle Cell Trait and Coronary Heart Disease Among African American Individuals
JAMA Network Open. 2021;4(1):e2030435. doi:10.1001/jamanetworkopen.2020.30435 (Reprinted) January 5, 2021 8/13
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 05/26/2021

ARTICLE INFORMATIONAccepted for Publication: October 21, 2020.
Published: January 5, 2021. doi:10.1001/jamanetworkopen.2020.30435
Open Access: This is an open access article distributed under the terms of the CC-BY License. © 2021 Hyacinth HIet al. JAMA Network Open.
Corresponding Author: Hyacinth I. Hyacinth, MD, PhD, MPH, Aflac Cancer and Blood Disorder Center,Department of Pediatrics, Emory University School of Medicine, 2015 Uppergate Dr, Atlanta, GA 30322 ([email protected]).
Author Affiliations: Aflac Cancer and Blood Disorder Center, Department of Pediatrics, Emory University Schoolof Medicine, Atlanta, Georgia (Hyacinth, Gee); Department of Epidemiology, University of North Carolina, ChapelHill (Franceschini); Department of Mathematics and Statistics, University of West Florida, Pensacola (Seals); Schoolof Public Health, University of Alabama at Birmingham, Birmingham (Irvin, Chaudhary, Judd); Division ofHematology, Department of Medicine, The Johns Hopkins University, Baltimore, Maryland (Naik); Department ofEpidemiology, Rollins School of Public Health, Emory University, Atlanta, Georgia (Alonso); Fred HutchinsonCancer Research Center, Seattle, Washington (Carty); Department of Public Health Sciences, Wake ForestUniversity, Winston-Salem, North Carolina (Burke); Department of Medicine and Pathology and LaboratoryMedicine, University of Vermont, Burlington (Zakai, Cushman); Basic Science Laboratory, National Cancer Instituteand Frederick National Laboratory, Leidos Biomedical Research, Frederick, Maryland (Winkler, David); NationalInstitute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, Maryland (Kopp);Stroke Center, Department of Neurology, Medical University of South Carolina, Charleston (Adams, Lackland);Department of Neurology, University of Washington, Seattle (Longstreth); Department of Epidemiology,University of Washington, Seattle (Longstreth); Division of General Internal Medicine, Medical College ofWisconsin, Milwaukee (Egede); Division of Hematology-Oncology, Medical University of South Carolina,Charleston (Greenberg); Cardiovascular Research Institute, Morehouse School of Medicine, Atlanta, Georgia(Taylor); Department of Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston,Massachusetts (Manson); Division of Hematology/Oncology, University of North Carolina at Chapel Hill, Chapel Hill(Key); University of North Carolina Kidney Center, University of North Carolina at Chapel Hill, Chapel Hill (Derebail,Kshirsagar); Division of Epidemiology and Community Health, University of Minnesota School of Public Health,Minneapolis (Folsom); Division of Cardiology, University of Minnesota Medical Center, Minneapolis (Konety);Department of Epidemiology, School of Public Health, University of Alabama at Birmingham, Birmingham(V. Howard); Department of Family Medicine and Public Health, University of California San Diego, San Diego(Allison); Department of Physiology and Biophysics, University of Mississippi Medical Center, Jackson (Wilson);Jackson Heart Study, University of Mississippi Medical Center, Jackson (Correa); Department of Biostatistics,School of Public Health, University of Alabama at Birmingham, Birmingham (Zhi); College of Public Health,University of Kentucky, Lexington (Arnett); Department of Biostatistics, School of Public Health, University ofAlabama at Birmingham, Birmingham (G. Howard); University of Washington Fred Hutchinson Cancer ResearchCenter, Seattle (Reiner); Division of General Internal Medicine, Weill Cornell Medicine, New York, NewYork (Safford).
Author Contributions: Dr Hyacinth had full access to all of the data in the study and takes responsibility for theintegrity of the data and the accuracy of the data analysis.
Concept and design: Hyacinth, Naik, Adams, Longstreth, Egede, Greenberg, Manson, Key, Kshirsagar, Arnett,Reiner, Cushman, Safford.
Acquisition, analysis, or interpretation of data: Hyacinth, Franceschini, Seals, Irvin, Chaudhary, Naik, Alonso, Carty,Burke, Zakai, Winkler, David, Kopp, Judd, Gee, Lackland, Taylor, Manson, Derebail, Folsom, Konety, V. Howard,Allison, Wilson, Correa, Zhi, G. Howard, Reiner, Cushman, Safford.
Drafting of the manuscript: Hyacinth.
Critical revision of the manuscript for important intellectual content: All authors.
Statistical analysis: Hyacinth, Franceschini, Seals, Chaudhary, Alonso, Carty.
Obtained funding: Naik, Burke, Judd, Taylor, V. Howard, Correa, G. Howard, Cushman, Safford.
Administrative, technical, or material support: Hyacinth, Burke, David, Judd, Gee, Greenberg, Manson, Folsom, V.Howard, Wilson, Correa, Arnett, G. Howard, Reiner, Cushman, Safford.
Supervision: Hyacinth, Irvin, Zakai, Adams, Egede, Manson, Kshirsagar, Allison, Arnett, G. Howard, Safford.
Conflict of Interest Disclosures: Dr Naik reported receiving grants from the National Heart, Lung, and BloodInstitute (NHLBI), National Institutes of Health (NIH) during the conduct of the study and receiving researchfunding from Rigel and serving as a consultant for Elsevier outside the submitted work. Dr Winkler reportedreceiving grants from the National Cancer Institute, NIH during the conduct of the study. Dr Judd reported
JAMA Network Open | Cardiology Sickle Cell Trait and Coronary Heart Disease Among African American Individuals
JAMA Network Open. 2021;4(1):e2030435. doi:10.1001/jamanetworkopen.2020.30435 (Reprinted) January 5, 2021 9/13
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 05/26/2021

receiving grants from the NIH during the conduct of the study. Dr Taylor reported receiving personal fees fromNovartis and Pfizer and grants from United Health Group outside the submitted work. Dr Manson reportedreceiving grants from the NIH during the conduct of the study. Dr Derebail reported receiving personal fees fromNovartis, Retrophin, and UpToDate outside the submitted work. Dr Folsom reported receiving grants from theNHLBI, NIH during the conduct of the study. Dr V. Howard reported receiving grants from the National Institute ofNeurological Disorders and Stroke NINDS), NIH during the conduct of the study. Dr Wilson reported receivinggrants from the NHLBI, NIH during the conduct of the study. Dr Safford reported receiving grants from Amgenoutside the submitted work. No other disclosures were reported.
Funding/Support: The Multi-Ethnic Study of Atherosclerosis (MESA) and the MESA SHARe project are conductedand supported by the NHLBI in collaboration with MESA investigators. Support for MESA is provided by contractsHHSN268201500003I, N01-HC-95159, N01-HC-95160, N01-HC-95161, N01-HC-95162, N01-HC-95163, N01-HC-95164, N01-HC-95165, N01-HC-95166, N01-HC-95167, N01-HC-95168, N01-HC-95169, UL1-TR-001079, UL1-TR-000040, and DK063491. Funding for SHARe genotyping was provided by NHLBI contract N02-HL-64278.Genotyping was performed at Affymetrix (Santa Clara, California) and the Broad Institute of Harvard and MIT(Boston, Massachusetts) using the Affymetrix Genome-Wide Human SNP Array 6.0. The Jackson Heart Study issupported and conducted in collaboration with Jackson State University (HHSN268201800013I), TougalooCollege (HHSN268201800014I), the Mississippi State Department of Health (HHSN268201800015I), and theUniversity of Mississippi Medical Center (HHSN268201800010I, HHSN268201800011I, andHHSN268201800012I) contracts from the NHLBI and the National Institute on Minority Health and HealthDisparities. The Women’s Health Initiative program is funded by the NHLBI, NIH, US Department of Health andHuman Services, through contracts HHSN268201100046C, HHSN268201100001C, HHSN268201100002C,HHSN268201100003C, HHSN268201100004C, and HHSN271201100004C. The Reasons for Geographic andRacial Differences in Stroke study is co-funded by the NINDS and the NIA. This research project is supported bycooperative agreement U01NS041588 co-funded by the NINDS and the NIA, NIH, US Department of Health andHuman Services. The Atherosclerosis Risk in Communities study has been funded in whole or in part with federalfunds from the NHLBI, NIH, US Department of Health and Human Services (contract numbersHHSN268201700001I, HHSN268201700002I, HHSN268201700003I, HHSN268201700004I, andHHSN268201700005I), R01HL087641, and R01HL086694; National Human Genome Research Institutecontract U01HG004402; and NIH contract HHSN268200625226C. Infrastructure was partly supported by grantnumber UL1RR025005, a component of the NIH and NIH Roadmap for Medical Research. This study wassupported in part by grant R01HL080477 from the NHLBI, NIH (Dr Safford); grants 3U01HL117721, R01HL138423,and R01HL156024 from the NHLBI, NIH (Dr Hyacinth); grant 1K08HL125100 from the NHLBI, NIH (Dr Naik); grantK08HL096841 from the NHLBI, NIH (Dr Zakai); grants R01HL136574, R01HL132947, and R01HL130733 from theNHLBI, NIH (Dr Reiner); grants R56 DK104806 and R21HL123677 from the NHLBI, NIH (Dr Franceschini); and grantK24HL148521 (Dr Alonso) from the NHLBI, NIH and grant 00051285 (Dr Hyacinth) from the Emory PediatricsChildren's Heart Research and Outcomes Center. The project has been supported in part by the NIH and theNational Cancer Institute Intramural Research Program (Dr Winkler) and under contract HHSN26120080001E.
Role of the Funder/Sponsor: The funding sources had no role in the design and conduct of the study; collection,management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; anddecision to submit the manuscript for publication.
Disclaimer: The views expressed in this manuscript are those of the authors and do not necessarily represent theviews of the NHLBI, NIA, and NINDS of the NIH or the US Department of Health and Human Services.
Additional Contributions: We thank the other investigators, the staff, and the participants of the MESA, theJackson Heart Study, the Women’s Health Initiative study, the Reasons for Geographic and Racial Differences inStroke study, and the Atherosclerosis Risk in Communities study.
REFERENCES1. Carter JS, Pugh JA, Monterrosa A. Non–insulin-dependent diabetes mellitus in minorities in the United States.Ann Intern Med. 1996;125(3):221-232. doi:10.7326/0003-4819-125-3-199608010-00011
2. Go AS, Mozaffarian D, Roger VL, et al; American Heart Association Statistics Committee and Stroke StatisticsSubcommittee. Heart disease and stroke statistics—2013 update: a report from the American Heart Association.Circulation. 2013;127(1):e6-e245. doi:10.1161/CIR.0b013e31828124ad
3. Howard G, Prineas R, Moy C, et al. Racial and geographic differences in awareness, treatment, and control ofhypertension: the Reasons for Geographic and Racial Differences in Stroke study. Stroke. 2006;37(5):1171-1178.doi:10.1161/01.STR.0000217222.09978.ce
4. Jamerson KA. The disproportionate impact of hypertensive cardiovascular disease in African Americans:getting to the heart of the issue. J Clin Hypertens (Greenwich). 2004;6(4)(suppl 1):4-10. doi:10.1111/j.1524-6175.2004.03563.x
JAMA Network Open | Cardiology Sickle Cell Trait and Coronary Heart Disease Among African American Individuals
JAMA Network Open. 2021;4(1):e2030435. doi:10.1001/jamanetworkopen.2020.30435 (Reprinted) January 5, 2021 10/13
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 05/26/2021

5. Kleindorfer DO, Khoury J, Moomaw CJ, et al. Stroke incidence is decreasing in Whites but not in Blacks:a population-based estimate of temporal trends in stroke incidence from the Greater Cincinnati/NorthernKentucky Stroke Study. Stroke. 2010;41(7):1326-1331. doi:10.1161/STROKEAHA.109.575043
6. Baruth M, Wilcox S, Egan BM, Dowda M, Laken M, Warren TY. Cardiovascular disease risk factor clusteringamong African American adults. Ethn Dis. 2011;21(2):129-134.
7. Kurian AK, Cardarelli KM. Racial and ethnic differences in cardiovascular disease risk factors: a systematicreview. Ethn Dis. 2007;17(1):143-152.
8. Lloyd-Jones D, Adams RJ, Brown TM, et al; Writing Group Members; American Heart Association StatisticsCommittee and Stroke Statistics Subcommittee. Heart disease and stroke statistics—2010 update: a report fromthe American Heart Association. Circulation. 2010;121(7):e46-e215.
9. Matthews KA, Sowers MF, Derby CA, et al. Ethnic differences in cardiovascular risk factor burden amongmiddle-aged women: Study of Women’s Health Across the Nation (SWAN). Am Heart J. 2005;149(6):1066-1073.doi:10.1016/j.ahj.2004.08.027
10. Sundquist J, Winkleby MA, Pudaric S. Cardiovascular disease risk factors among older Black, Mexican-American, and White women and men: an analysis of NHANES III, 1988-1994: Third National Health and NutritionExamination Survey. J Am Geriatr Soc. 2001;49(2):109-116. doi:10.1046/j.1532-5415.2001.49030.x
11. Benjamin EJ, Blaha MJ, Chiuve SE, et al; American Heart Association Statistics Committee and Stroke StatisticsSubcommittee. Heart disease and stroke statistics—2017 update: a report from the American Heart Association.Circulation. 2017;135(10):e146-e603. doi:10.1161/CIR.0000000000000485
12. Parsa A, Kao WH, Xie D, et al; AASK Study Investigators; CRIC Study Investigators. APOL1 risk variants, race, andprogression of chronic kidney disease. N Engl J Med. 2013;369(23):2183-2196. doi:10.1056/NEJMoa1310345
13. Foster MC, Coresh J, Fornage M, et al. APOL1 variants associate with increased risk of CKD among AfricanAmericans. J Am Soc Nephrol. 2013;24(9):1484-1491. doi:10.1681/ASN.2013010113
14. Genovese G, Friedman DJ, Ross MD, et al. Association of trypanolytic ApoL1 variants with kidney disease inAfrican Americans. Science. 2010;329(5993):841-845. doi:10.1126/science.1193032
15. Ito K, Bick AG, Flannick J, et al. Increased burden of cardiovascular disease in carriers of APOL1 genetic variants.Circ Res. 2014;114(5):845-850. doi:10.1161/CIRCRESAHA.114.302347
16. Franceschini N, Kopp JB, Barac A, et al. Association of APOL1 with heart failure with preserved ejection fractionin postmenopausal African American women. JAMA Cardiol. 2018;3(8):712-720. doi:10.1001/jamacardio.2018.1827
17. Naik RP, Derebail VK, Grams ME, et al. Association of sickle cell trait with chronic kidney disease andalbuminuria in African Americans. JAMA. 2014;312(20):2115-2125. doi:10.1001/jama.2014.15063
18. Derebail VK, Lacson EK Jr, Kshirsagar AV, et al. Sickle trait in African-American hemodialysis patients andhigher erythropoiesis-stimulating agent dose. J Am Soc Nephrol. 2014;25(4):819-826. doi:10.1681/ASN.2013060575
19. Derebail VK, Nachman PH, Key NS, Ansede H, Falk RJ, Kshirsagar AV. High prevalence of sickle cell trait inAfrican Americans with ESRD. J Am Soc Nephrol. 2010;21(3):413-417. doi:10.1681/ASN.2009070705
20. Lash JP, Ricardo AC, Roy J, et al; CRIC Study Investigators. Race/ethnicity and cardiovascular outcomes inadults with CKD: findings from the CRIC (Chronic Renal Insufficiency Cohort) and Hispanic CRIC Studies. Am JKidney Dis. 2016;68(4):545-553. doi:10.1053/j.ajkd.2016.03.429
21. Agarwal S, Shlipak MG, Kramer H, Jain A, Herrington DM. The association of chronic kidney disease andmetabolic syndrome with incident cardiovascular events: multiethnic study of atherosclerosis. Cardiol Res Pract.2012;2012:806102. doi:10.1155/2012/806102
22. Ajayi AAL. Should the sickle cell trait be reclassified as a disease state? Eur J Intern Med. 2005;16(6):463. doi:10.1016/j.ejim.2005.02.010
23. Tsaras G, Owusu-Ansah A, Boateng FO, Amoateng-Adjepong Y. Complications associated with sickle cell trait:a brief narrative review. Am J Med. 2009;122(6):507-512. doi:10.1016/j.amjmed.2008.12.020
24. Naik RP, Irvin MR, Judd S, et al. Sickle cell trait and the risk of ESRD in Blacks. J Am Soc Nephrol. 2017;28(7):2180-2187. doi:10.1681/ASN.2016101086
25. Davis CJ Jr, Mostofi FK, Sesterhenn IA. Renal medullary carcinoma: the seventh sickle cell nephropathy. Am JSurg Pathol. 1995;19(1):1-11. doi:10.1097/00000478-199501000-00001
26. Watanabe IC, Billis A, Guimarães MS, et al. Renal medullary carcinoma: report of seven cases from Brazil. ModPathol. 2007;20(9):914-920. doi:10.1038/modpathol.3800934
JAMA Network Open | Cardiology Sickle Cell Trait and Coronary Heart Disease Among African American Individuals
JAMA Network Open. 2021;4(1):e2030435. doi:10.1001/jamanetworkopen.2020.30435 (Reprinted) January 5, 2021 11/13
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 05/26/2021

27. Austin H, Key NS, Benson JM, et al. Sickle cell trait and the risk of venous thromboembolism among blacks.Blood. 2007;110(3):908-912. doi:10.1182/blood-2006-11-057604
28. Austin H, Lally C, Benson JM, Whitsett C, Hooper WC, Key NS. Hormonal contraception, sickle cell trait, andrisk for venous thromboembolism among African American women. Am J Obstet Gynecol. 2009;200(6):620.e1-620.e3. doi:10.1016/j.ajog.2009.01.038
29. James AH, Jamison MG, Brancazio LR, Myers ER. Venous thromboembolism during pregnancy and thepostpartum period: incidence, risk factors, and mortality. Am J Obstet Gynecol. 2006;194(5):1311-1315. doi:10.1016/j.ajog.2005.11.008
30. Stein PD, Beemath A, Meyers FA, Skaf E, Olson RE. Deep venous thrombosis and pulmonary embolism inhospitalized patients with sickle cell disease. Am J Med. 2006;119(10):897.e7-897.e11. doi:10.1016/j.amjmed.2006.08.015
31. Pradhan RK, Mishra R, Nag C. Diurnal variations of C-reactive protein in trait and sickle cell disease patients.Biological Rhythm Res. 2013;44(2):277-285. doi:10.1080/09291016.2012.681846
32. Westerman MP, Green D, Gilman-Sachs A, et al. Coagulation changes in individuals with sickle cell trait. Am JHematol. 2002;69(2):89-94. doi:10.1002/ajh.10021
33. Grunwald JE, Ying GS, Maguire M, et al; Chronic Renal Insufficiency Cohort (CRIC) Study Group. Associationbetween retinopathy and cardiovascular disease in patients with chronic kidney disease (from the Chronic RenalInsufficiency Cohort [CRIC] Study). Am J Cardiol. 2012;110(2):246-253. doi:10.1016/j.amjcard.2012.03.014
34. Rahman M, Xie D, Feldman HI, et al; CRIC Study Investigators. Association between chronic kidney diseaseprogression and cardiovascular disease: results from the CRIC Study. Am J Nephrol. 2014;40(5):399-407. doi:10.1159/000368915
35. The Women’s Health Initiative Study Group. Design of the Women’s Health Initiative clinical trial andobservational study. Control Clin Trials. 1998;19(1):61-109. doi:10.1016/S0197-2456(97)00078-0
36. Howard VJ, Cushman M, Pulley L, et al. The reasons for geographic and racial differences in stroke study:objectives and design. Neuroepidemiology. 2005;25(3):135-143. doi:10.1159/000086678
37. Bild DE, Bluemke DA, Burke GL, et al. Multi-Ethnic Study of Atherosclerosis: objectives and design. Am JEpidemiol. 2002;156(9):871-881. doi:10.1093/aje/kwf113
38. Taylor HA Jr, Wilson JG, Jones DW, et al. Toward resolution of cardiovascular health disparities in AfricanAmericans: design and methods of the Jackson Heart Study. Ethn Dis. 2005;15(4)(suppl 6):S6-S4, 17.
39. Wilson JG, Rotimi CN, Ekunwe L, et al. Study design for genetic analysis in the Jackson Heart Study. Ethn Dis.2005;15(4)(suppl 6):S6-S30, 37.
40. The ARIC Investigators. The Atherosclerosis Risk in Community (ARIC) Study: design and objectives. AmericanJournal of Epidemiology. 1989;129(4):687-702. doi:10.1093/oxfordjournals.aje.a115184
41. Rosamond WD, Chambless LE, Heiss G, et al. Twenty-two–year trends in incidence of myocardial infarction,coronary heart disease mortality, and case fatality in 4 US communities, 1987-2008. Circulation. 2012;125(15):1848-1857. doi:10.1161/CIRCULATIONAHA.111.047480
42. Bluemke DA, Kronmal RA, Lima JA, et al. The relationship of left ventricular mass and geometry to incidentcardiovascular events: the MESA (Multi-Ethnic Study of Atherosclerosis) study. J Am Coll Cardiol. 2008;52(25):2148-2155. doi:10.1016/j.jacc.2008.09.014
43. Alexander DH, Novembre J, Lange K. Fast model-based estimation of ancestry in unrelated individuals.Genome Res. 2009;19(9):1655-1664. doi:10.1101/gr.094052.109
44. Keku E, Rosamond W, Taylor HA Jr, et al. Cardiovascular disease event classification in the Jackson HeartStudy: methods and procedures. Ethn Dis. 2005;15(4)(suppl 6):S6-S62, 70.
45. Wilson PWF, D’Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coronary heartdisease using risk factor categories. Circulation. 1998;97(18):1837-1847. doi:10.1161/01.CIR.97.18.1837
46. D’Agostino RB, Russell MW, Huse DM, et al. Primary and subsequent coronary risk appraisal: new results fromthe Framingham Study. Am Heart J. 2000;139(2, pt 1):272-281. doi:10.1016/S0002-8703(00)90236-9
47. Ojodu J, Hulihan MM, Pope SN, Grant AM; Centers for Disease Control and Prevention (CDC). Incidence ofsickle cell trait—United States, 2010. MMWR Morb Mortal Wkly Rep. 2014;63(49):1155-1158.
48. Hyacinth HI, Carty CL, Seals SR, et al. Association of sickle cell trait with ischemic stroke among AfricanAmericans: a meta-analysis. JAMA Neurol. 2018;75(7):802-807. doi:10.1001/jamaneurol.2018.0571
49. Diaw M, Pialoux V, Martin C, et al. Sickle cell trait worsens oxidative stress, abnormal blood rheology, andvascular dysfunction in type 2 diabetes. Diabetes Care. 2015;38(11):2120-2127. doi:10.2337/dc15-0699
JAMA Network Open | Cardiology Sickle Cell Trait and Coronary Heart Disease Among African American Individuals
JAMA Network Open. 2021;4(1):e2030435. doi:10.1001/jamanetworkopen.2020.30435 (Reprinted) January 5, 2021 12/13
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 05/26/2021

50. Folsom AR, Tang W, Roetker NS, et al. Prospective study of sickle cell trait and venous thromboembolismincidence. J Thromb Haemost. 2015;13(1):2-9. doi:10.1111/jth.12787
51. Ajayi AA, Kolawole BA. Sickle cell trait and gender influence type 2 diabetic complications in African patients.Eur J Intern Med. 2004;15(5):312-315. doi:10.1016/j.ejim.2004.06.003
52. Olaniran KO, Eneanya ND, Allegretti AS, Zhao SH, Achebe MM, Thadhani RI. Cardiovascular outcomes inAfrican Americans with sickle cell trait and chronic kidney disease. Am J Nephrol. 2019;49(2):93-102. doi:10.1159/000496058
53. Rumaney MB, Ngo Bitoungui VJ, Vorster AA, et al. The co-inheritance of alpha-thalassemia and sickle cellanemia is associated with better hematological indices and lower consultations rate in Cameroonian patients andcould improve their survival. PLoS One. 2014;9(6):e100516. doi:10.1371/journal.pone.0100516
54. Adams RJ, Kutlar A, McKie V, et al. Alpha thalassemia and stroke risk in sickle cell anemia. Am J Hematol. 1994;45(4):279-282. doi:10.1002/ajh.2830450402
55. Harmon KG, Drezner JA, Klossner D, Asif IM. Sickle cell trait associated with a RR of death of 37 times inNational Collegiate Athletic Association football athletes: a database with 2 million athlete-years as thedenominator. Br J Sports Med. 2012;46(5):325-330. doi:10.1136/bjsports-2011-090896
56. Kark JA, Posey DM, Schumacher HR, Ruehle CJ. Sickle-cell trait as a risk factor for sudden death in physicaltraining. N Engl J Med. 1987;317(13):781-787. doi:10.1056/NEJM198709243171301
SUPPLEMENT.eMethods.
JAMA Network Open | Cardiology Sickle Cell Trait and Coronary Heart Disease Among African American Individuals
JAMA Network Open. 2021;4(1):e2030435. doi:10.1001/jamanetworkopen.2020.30435 (Reprinted) January 5, 2021 13/13
Downloaded From: https://jamanetwork.com/ by a Non-Human Traffic (NHT) User on 05/26/2021