Embed Size (px)
Citation preview

Association of Polymorphic Markers of the Catalaseand Superoxide Dismutase Genes with Type 2
Diabetes Mellitus
Maivel H. Ghattas1 and Dina M. Abo-Elmatty2
Our study aims at determining whether genetic polymorphisms of catalase (CAT 1167C/T) and superoxidedismutase (SOD + 35 A/C) could be associated with type 2 diabetes mellitus (T2DM). The study was conductedon 105 Egyptian patients with T2DM and 115 control subjects. Genotypes were done by polymerase chainreaction-restriction fragment length polymorphism methods. Homeostatic model assessment of insulin resis-tance (HOMA-IR), CAT and SOD activities, glycated hemoglobin, and insulin and lipid profiles were assessed.CAT and SOD activities were significantly decreased in T2DM compared with the control subjects. T allele ofCAT and C allele of SOD1 were significant risk factors for T2DM. No effects of CAT or SOD1 gene polymor-phisms on glycated haemoglobin or on HOMA-IR were found. With regard to the enzymes activities, only + 35A/C of SOD1 was related to SOD activity. Genetic variants C1167T of CAT gene and + 35 A/C of SOD1 genehas no role in insulin resistance in T2DM.
Introduction
Oxidative stress has been shown to be responsible, atleast in part, for the progression of type 2 diabetes
(Rosen et al., 2001). In diabetes, chronic hyperglycemia isresponsible for producing mitochondrial dysfunction withreactive oxygen species super production, which is the trig-gering factor of endothelial dysfunction (Brownlee, 2001). Avicious circle is formed in which the antioxidant defenseplays an important role, protecting against diabetes mellituscomplications (Nishikawa et al., 2000). In addition, glucosetoxicity causes b-cell dysfunction; this leads to severe im-pairment of glucose-stimulated insulin secretion, apparentdegranulation of b-cells, and a decrease in its number, re-sulting in the aggravation of insulin resistance (IR) (Songet al., 2007). However, some patients with diabetes developcomplications, but this cannot be seen in the others with thesame level of disease control (Fumeron et al., 2006). More-over, pharmacological supplementation of antioxidants hasnot been successful as a method that prevents atheroscleroticvascular diseases (Virtamo et al., 1998). One possibility couldbe variations in genetically determined endogenous protec-tion against oxidative processes (Ukkola et al., 2001).
Catalase (CAT) and copper-zinc superoxide dismutase(CuZnSOD) are well-known antioxidant enzymes. Super-oxide is dismutated to H2O2 by CuZnSOD in the cytosol(Maritim et al., 2003). H2O2 is converted to H2O and O2 byCAT in the mitochondria and the lysosomes (Yung et al.,2006).
In this study, we raised the question of whether the ge-netically determined polymorphisms of the key antioxidantenzymes, CAT and CuZnSOD, could be related to variousrisk factors of type 2 diabetes mellitus (T2DM). Specifically,we hypothesized that the allele frequencies of these poly-morphisms could be associated with IR in diabetic patients.
CuZnSOD, CAT is encoded on 21q22.1. The + 35 A/Cpolymorphism (rs 2234694) is adjacent to the splicing point(exon3/intron3) and is related to SOD1 activity with AA ge-notype having the higher activity (Flekac et al., 2008). The CATgene contains 13 exons and is located in chromosome 11p13(Goth et al., 2001). A number of single nucleotide polymor-phisms have been reported in the CAT gene. With regard todiabetes, previous reports suggested that C1167T polymor-phism in codon 389 of exon 9 (rs 769217) plays a role in thedevelopment of the disease (Schroeder and Saunders, 1987).
Therefore, the purpose of the current study is to assess thepossible association of + 35 A/C polymorphism in the SOD1gene and 1167 C/T polymorphism in the CAT gene withT2DM in Egypt.
Materials and Methods
Subjects
A total of 105 Egyptian patients with T2DM and 115 controlgroups of healthy Egyptian subjects were examined in thisstudy. Diagnosis of T2DM was based on the criteria of theAmerican Diabetes Association (American Diabetes
1Department of Medical Biochemistry, Faculty of Medicine, Suez Canal University, Ismailia, Egypt.2Department of Biochemistry, Faculty of Pharmacy, Suez Canal University, Ismailia, Egypt.
DNA AND CELL BIOLOGYVolume 31, Number 11, 2012ª Mary Ann Liebert, Inc.Pp. 1598–1603DOI: 10.1089/dna.2012.1739
1598

Association, 2010). Subjects were recruited from those attend-ing the outpatient clinics at North Sinai area. The ethics com-mittee of Faculty of Pharmacy, Suez Canal University,approved the study protocol, and written informed consent toparticipate in the study was obtained from all the individuals.
All the study subjects underwent a complete medicalhistory and complete physical examinations. Anthropo-metric parameters, including weight and height as well asblood pressure, were measured, and body mass index (BMI)was calculated.
Methods
Laboratory measurements. Venous blood samples weredrawn after overnight fasting. Serum was separated and usedfor assessment of fasting blood glucose and lipid profiles[including total cholesterol (TC), triglyceride (TG), high den-sity lipoprotein cholesterol (HDL-C), and very low density li-poprotein (VLDL-C)] by automated enzymatic methods on aHitachi - 912- analyzer. Low density lipoprotein cholesterol(LDL-C) cholesterol was calculated according to Friedewaldformula (Friedewald et al., 1972). Fasting serum insulin levelwas measured by using ADVIA Centaur� XP ImmunoassaySystem (Siemens Healthcare Diagnostics); IR and b cell dys-function were assessed by using the homeostatic model as-sessment of insulin resistance (HOMA-IR) (Matthews et al.,1985). Glycated hemoglobin (HbA1C) was measured in wholeblood collecting on EDTA anticoagulant using ADVIA� 1800Chemistry System (Siemens Healthcare Diagnostics). PlasmaCAT activity and erythrocyte SOD activity were determined byspectrophotometer assay kits (Bio-Diagnostic).
Genotype analysis. Genomic DNA was extracted fromperipheral blood leucocytes obtained from 200mL EDTAanticoagulated blood samples using the wizard genomicDNA purification kit (Promega). Determination of C1167TCAT and + 35 A/C SOD1 gene polymorphisms were deter-mined by polymerase chain reaction-restriction fragmentlength polymorphism (PCR-RFLP) using the primers and therestriction enzymes shown in Table 1. PCR was carried out ina final volume of 50mL, using 300 ng of genomic DNA, 2.5 Uof Taq DNA polymerase (Bioron), 0.1 mM of each dNTP(Bioron), and 1 mmol of each of the primers (Metabion In-ternational AG). The reaction buffer contains 1.5 mM MgCl2,10 mM Tris–HCl (pH 9.0), 50 mM KCl, and nuclease-freewater to 50mL. Amplification was done by initial denatur-ation of 94�C for 5 min. followed by 35 cycles of denaturingat 94�C for 1 min., annealing 55�C or 64�C for 1 min., andextension at 72�C for 1 min. A final extension of 5 min at 72�Cwas done. For RFLP-PCR analysis, amplified products weredigested with a restriction endonuclease (SibEnzyme Ltd.).The digestion products were separated in 2% (weight/vol-ume) agarose gel along with a 100-base pair marker (Axygen
Biosciences). The products were then visualized under UVlight following staining with ethidium bromide. To assessaccuracy, 20 samples were done in duplicate, and the dis-crepancy rate was 0/20 among the single nucleotide poly-morphisms (SNPs) and samples we studied.
Statistical analysis. The genotype and allele frequencieswere determined by direct counting. Hardy–Weinberg equi-librium was evaluated using a Chi-square (w2) test. Statisticalcomparisons between healthy and diabetic populations wereperformed using w2 test, fisher exact test, and two-way stu-dent’s t-test. Associations of genotypes with CAT and SODactivity were evaluated by analysis of variance test. Backwardstepwise multiple logistic regression analysis was used to elu-cidate the association of rare allele carriage with diabetes usingSPSS version 17 program. A value of p < 0.05 was consideredstatistically significant. All data were presented as mean – SD.
Results
The main clinical and biochemical characteristics of thediabetic subjects and controls are shown in Table 2. Age, sex,and HDL-C were not significantly different between diabetic
Table 1. Primers and Polymerase Chain Reaction Reactions
PolymorphismRestriction
enzyme PrimersAnnealing
Temp. Restriction fragments
CAT C1167T BstXI Forward: 5¢-GCCCGCCTTTTTGCCTATCCT-3¢ 64�C C allele 202 bpReverse: 5¢-TCCCGCCCATCTGCTCCAC-3¢ T allele 93 and 109 bp
SOD1 + 35A/C
HhaI Forward: 5¢-CTATCCAGAAAACACGGTGGGCC-3¢ 55�C C allele 71 and 207 bpReverse: 5¢-TCTATATTCAATCAAATGCTACAAAACC-3¢ A allele 278 bp
Table 2. General Characteristics
of the Study Population
VariablesControl
(n = 115)T2DM patients
(n = 105)
Age (year) 45.93 – 10.5 45.9 – 10.6Men, n (%) 42 (42) 40 (40)BMI (Kg/m2) 26.91 – 4.91 28.21 – 3.45a
Smoking, n (%) 30 (26.1) 85 (80.9)a
Hypertension, n (%) 3 (2.6) 78 (74.3)a
Family history, n (%) 14 (12.1) 53 (50.5)a
FBG (mg/dL) 90 – 7.2 209.6 – 61.3a
Insulin (mIU/mL) 18.75 – 2.12 10.56 – 2.37a
HbA1C (%) 4.99 – 0.71 9.68 – 1.84a
HOMA-IR 3.95 – 0.61 5.42 – 2.0 a
TAG (mg/dL) 136.25 – 46.4 217.2 – 110.54a
TC (mg/dL) 182.68 – 17.96 216.64 – 34.39a
LDL-C (mg/dL) 110.06 – 23.2 126.7 – 36.18a
HDL-C (mg/dL) 45.37 – 7.15 46.46 – 9.7CAT activity (mU/L) 103.37 – 11.14 81.1 – 11.76a
SOD activity (mU/L) 154.16 – 22.8 110.1 – 11.58a
Age and BMI, FBG, insulin, TAG, TC, HDL-C, LDL-C, and VLDL-C represented as mean – SD. Gender represented as number andpercentage of subjects.
aSignificantly different from normal control p < 0.01.BMI, body mass index; FBG, fasting blood glucose; TAG, triacylgly-
cerol; TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol;LDL-C, low-density lipoprotein cholesterol; HOMA-IR, homeostaticmodel assessment of insulin resistance; SOD, superoxide dismutase;T2DM, type 2 diabetes mellitus; CAT, catalase.
CAT AND SOD POLYMORPHISMS IN T2DM 1599

patients and control participants. Conversely, BMI, smokingstatus, hypertension, family history, blood glucose, HbA1C,serum triglycerides, total cholesterol, LDL-C, and HOMA-IRwere significantly different between the two groups. plasmaCAT activity and erythrocyte SOD activity were significantlydecreased in T2DM compared with the control subjects, bothp < 0.05.
Allele frequencies and genotypes
The genetic polymorphisms in CAT and SOD1 genes wereinvestigated, and the genotypes are shown in Figures 1 and 2.In total, two SNPs were identified in the CAT and SODgenes. Table 3 presents the name, type, allele frequencies,and location for these SNPs. All SNPs were in the Hardy–Weinberg equilibrium (Table 4). The number of patientscarrying the CAT TT genotype was determined to be 8(7.62%) among diabetic patients, whereras this was identifiedto be 2 (1.74%) among the control group. The T allele was asignificant risk factor for T2DM (odds ratio [OR] = 2.94; 95%confidence interval [CI, 1.66–5.23]) (Table 3).When thegroups were compared in terms of SOD + 35 polymorphism,the CC genotype among the patient group was 11 (10.48);whereas it was 2 (1.74%) in the control group. Con-sequentially, the C allele was a significant risk factor forT2DM (OR = 2.9; 95% CI [1.84–4.6]) (Table 3). When thegroups were compared in terms of CAT and SOD1 geno-types, statistical significance was determined ( p < 0.05).
Association of SNPs with diabetic control, IRand enzymes activities
When laboratory values were compared according to thegenotype distribution of CAT and SOD1 genes in diabeticpatients, no effect of SNP in the CAT gene on diabetes con-trol was found. Glycated haemoglobin was 9.67 – 1.7 in theCC genotype and 9.69 – 1.98 in CT + TT genotypes of the CATgene, with p > 0.05. Similar findings were made in the SOD1gene; glycated hemoglobin was 9.5 – 1.9 in AA genotypesand 9.7 – 1.7 in AC + CC genotypes with p < 0.05. Moreover,no effects of the SNPs in CAT or SOD1 genes on HOMA-IRwere found.
With regard to the enzyme activities, no effect of SNPin CAT gene on CAT activity was found. Conversely, + 35A/C of SOD1 was related to SOD activity. Higher activitieswere found in AA than in CC genotypes of diabetic patients(Table 5).
Discussion
Oxidative stress is a single mechanism that is related to allmajor pathways responsible for diabetic damage and can beconsidered a hallmark of microvascular and macrovasculardisorders (Makuc and Petrovi�c, 2011, Cilensek et al., 2012,Fukumoto et al., 2012, Santl Letonja et al., 2012). Several
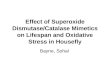
FIG. 1. CAT C1167T polymerase chain reaction (PCR) ge-notype of type 2 diabetic patients on 2% Agarose gel. M: 100base pair (bp) marker, Lanes 1, 2, 3 4, 5, 6, 8, 9,10, and 11 areCC genotypes and Lane 7 is TT genotypes for type 2 diabeticpatients.
FIG. 2. SOD1 + 35 A/C PCR genotype type 2 diabetic pa-tients on 2% Agarose gel. M: 50 bp marker, Lanes 1, 2, 3 and4 are AA genotypes and Lanes 5, 6, 7, 8, 9, 10, and 11 are ACgenotypes for type 2 diabetic patients.
Table 3. Allele Frequencies and Genotypes Distribution of CAT 1167 C/T and SOD + 35 A/CPolymorphism in Control and Type 2 Diabetes Mellitus Patients
Marker Allele/genotype n (%) Control n = 115 Diabetics n = 105 w2 p OR (95% CI)
CAT 1167 C/T Allele C 211 (91.74) 166 (79.05)Allele T 19 (8.26) 44 (20.95) 14.41 0.001a 2.94 (1.66–5.23)Genotype CC 98 (85.22) 69 (65.71)Genotype CT 15 (13.04) 28 (26.67) 7.79 0.005b 2.65 (1.32–5.33)Genotype TT 2 (1.74) 8 (7.62) 0.022c 5.68 (1.17–27.58)CT + TT 17 (14.78) 36 (34.29) 11.42 0.0007d 3 (1.56–5.78)
SOD + 35 A/C Allele A 195 (84.78) 138 (65.71)Allele C 35 (15.22) 72 (34.29) 21.68 0.0001e 2.9 (1.84–4.6)Genotype AA 82 (71.3) 44 (41.9)Genotype AC 31 (26.96) 50 (47.62) 14.29 0.0002f 3 (1.69–5.36)Genotype CC 2 (1.74) 11 (10.48) 0.0007g 10.25 (2.17–48.32)AC + CC 33 (28.7) 61 (58.1) 19.38 0.0001h 3.44 (1.97–6.03)
aT versus C; bCT versus CC; cTT versus CC; dCT + TT versus CC; eC versus A; fAC versus AA; gCC versus AA; hAC + CC versus AA.Comparisons were performed by w2 and Fisher’s exact tests. p < 0.05 is statistically significant.w2, Chi square test; CAT, catalase; CI, confidence interval; OR, odds ratio.
1600 GHATTAS AND ABO-ELMATTY

genome-wide association studies (GWAS) on susceptibil-ity to type 2 diabetes have now been published (Ahlqvistet al., 2011), and none report association with genes relatedto oxidative stress. Nevertheless, only *15% of diabetesheritability has been explained up to now by the GWAS thathas involved mainly individuals of European origin; so,studies on candidate genes and other ethnic groups maystill be of value. The current study found an evidence ofassociation between both CAT 1167C/T and SOD + 35 A/Cgene polymorphisms and T2DM in an Egyptian populationsample.
An association between diabetes susceptibility and aC1167T of the CAT gene was earlier reported in ethnicRussians (Chistyakov et al., 2000). Our results also suggestthat the CAT gene C1167T polymorphism is associated withdiabetes susceptibility with the heterozygote CT genotypebeing significantly more frequent among diabetic patientsthan healthy controls. Moreover, we observed a significantincrease in the frequency of the T allele in diabetic patientsthan healthy individuals. With regard to the + 35 A/C SOD1gene polymorphism, our study has indicated that the rarehomozygote CC genotype has increased diabetes risk com-pared with the wild-type AA, and the minor C allele carriersappeared to be susceptible to T2DM. Our study does notcontradict the results of Panduru et al. (2010) or Flekac et al.(2008), but some differences of susceptibility may exist thatare dependent on the studied population and the presence ofdiabetic complications, facts that are encountered in otherstudies.
To elucidate the underlying effect mediating the oxidativestress-induced outcome in T2DM, especially IR and b-cellfunction, we evaluate the influence of CAT and SOD1 genepolymorphisms on HOMA-IR in diabetic patients. Althoughthere were significant differences between genotypes of the
CAT and SOD1 between the diabetic patients and the controlsubjects, our data suggest that the C1167T CAT and + 35 A/C SOD1 gene polymorphisms have no effect on HOMA-IR.Moreover, no impact of these polymorphisms on lipid pro-file, glycemic control, or other risk factors for T2DM wasdetected.
It is widely postulated that the etiology of T2DM has astrong association with oxidative stress, originating fromincreased oxidative stress and impaired antioxidant defensesystems (Rahimi et al., 2005). Our data revealed that plasmaCAT and erythrocyte SOD activities were significantly de-creased in diabetic patients compared with control subjects.Our findings are in agreement with previous observations ofother authors (Goth et al., 2001) and (Smaoui et al., 2004).Low CAT and SOD activities and its consequence on highH2O2 level could contribute to the oxidative destruction ofpancreatic b cells and decreased insulin effectiveness in di-abetic patients (Flekac et al., 2008).
The low activity of antioxidant enzymes in diabetes isaccountable by genotype background or by the enzymeglycation effect of hyperglycemia (Flekac et al., 2008). Inter-estingly, the current study found no association betweenCAT activity and genotypes of the CAT C1167T polymor-phism in diabetics or control subjects. This finding was inaccordance with Zovota et al. (2004). The reason behind lackof association was related to the fact that this variation re-sults in a silent substitution of aspartate residue at codon 389;hence, it is unlikely to directly affect CAT activity. On thecontrary, other reports approved the association between theCAT polymorphisms and low CAT in vitiligo (Gavalas et al.,2006), hypertension ( Jiang et al., 2001), Alzheimer’s disease(Capurso et al., 2008), and diabetes mellitus (Tarnai et al.,2007). They explained the association by the possibility thatthe CAT C1167T polymorphism may be linked to other CAT
Table 4. Hardy–Weinberg Equilibrium of CAT 1167 C/T and SOD + 35 A/C Genotypes
Control T2DM
Marker Genotype Expected Observed p Expected Observed p
CAT 1167 CC 96.78 98 NS 65.61 69 NSCT 17.43 15 34.78 28TT 0.78 2 4.61 8
SOD + 35 AA 82.66 82 NS 45.34 44 NSAC 29.67 31 47.31 50CC 2.66 2 12.34 11
Comparisons were performed by w2 test.NS, nonsignificant differences.
Table 5. Glycemic Control, Insulin Resistance, CAT, and SOD1 Activities According to Genotype
Distribution of CAT and SOD1 Genes in Type 2 Diabetes Mellitus Patients
CAT SOD1
Variable CC (n = 69) CT + TT (n = 36) AA (n = 44) AC + CC (n = 61)
HbA1C (%) 9.67 – 1.7 9.69 – 1.98 9.5 – 1.9 9.7 – 1.7HOMA-IR 5.27 – 1.6 5.7 – 2.5 5.39 – 1.86 5.44 – 2.1Enzyme activity 80.8 – 14 81.28 – 5.1 119.0 – 2.3 103.6 – 11.3a
Values are presented as mean – SD.ap < 0.05, statistically significant.
CAT AND SOD POLYMORPHISMS IN T2DM 1601

polymorphisms that are deleterious to the expression of thegene or the activity of CAT (Gavalas et al., 2006). Contrary tothe lack of association between the CAT C1167T polymor-phism and the enzyme activity, our results are indicative ofthe potential effect of + 35 A/C in the SOD1 gene on enzymeactivity. Higher activities were found in AA than in CC ge-notypes of diabetic patients. Though a previous report byFlekac et al. (2008) found some evidence for an associationbetween the AA genotype and higher SOD activity, signifi-cance was borderline and was only achieved by combiningdata from diabetic and healthy subjects. Deficiency in SOD1activity can lead to increased levels of vascular superoxideand impaired endothelial dependent relaxation in both largearteries and microvessels, which results in diabetic vascularcomplications (Rolo and Palmeira, 2006).
In conclusion, the results of our study point to the role ofgene polymorphisms of CAT and superoxide dismutase indecreasing the ability of antioxidant defense system in dia-betes. Furthermore, it is highly unlikely that genetic variantsC1167T of the CAT gene and + 35 A/C of SOD1 gene play arole in IR in T2DM.
Disclosure Statement
No competing financial interests exist.
References
Ahlqvist, E., Ahluwalia, T.S., and Groop, L. (2011). Genetics oftype 2 diabetes. Clin Chem 57, 2241–2254.
American Diabetes Association. (2010). Diagnosis and classifi-cation of diabetes mellitus. position statement. Diabetes Care33, S62–S69.
Brownlee, M. (2001). Biochemistry and molecular cell biology ofdiabetic complications. Nature 414, 813–820.
Capurso, C., Solfrizzi, V., D’Introno, A., Colacicco, A.M., Ca-purso, S.A., Bifaro, L., et al. (2008). Short arm of chromosome11 and sporadic Alzheimer’s disease: catalase and cathepsin Dgene polymorphisms. Neurosci Lett 432, 237–242.
Chistyakov, D.A., Savost’yanov, K.V., Turakulov, R.I., Scherba-cheva, L.N., Mamaeva, G.G., Balabolkin, M.I., et al. (2000). TheCl167T Polymorphism of the catalase gene and polymorphicmarkers DllS907 and DllS2008 located in its vicinity are as-sociated with diabetes mellitus Type 2. Mol Biol 34, 733–736.
Cilensek, I., Manko�c, S., Petrovi�c, M.G., and Petrovi�c, D. (2012).GSTT1 null genotype is a risk factor for diabetic retinopathy inCaucasians with type 2 diabetes, whereas GSTM1 null geno-type might confer protection against retinopathy. Dis Markers32, 93–99.
Flekac, M., Skrha, J., Hilgertova, J., Lacinova, Z., and Jar-olimkova, M. (2008). Gene polymorphisms of superoxidedismutases and catalase in diabetes mellitus. BMC Med Genet9, 30.
Friedewald, W.T., Levy, R.I., and Fredrickson, D.S. (1972). Esti-mation of the concentration of lowdensity lipoprotein choles-terol in plasma, without use of the preparative ultracentrifuge.Clin Chem 18, 499–502.
Fukumoto, M., Nakaizumi, A., Zhang, T., Lentz, S.I., Shibata,M., and Puro, D.G. (2012). Vulnerability of the retinal micro-vasculature to oxidative stress: ion channel-dependent mech-anisms. Am J Physiol Cell Physiol 302, C1413– C1420.
Fumeron, F., Reis, A.F., and Velho, G. (2006). Genetics ofmacrovascular complications in diabetes. Curr Diab Rep 6,
162–168.
Gavalas, N.G., Akhtar, S., Gawkrodger, D.J., Watson, P.F.,Weetman, A.P., and Kemp, E.H. (2006). Analysis of allelicvariants in the catalase gene in patients with the skin de-pigmenting disorder vitiligo. BBRC 345, 1586–1591.
Goth, L., Rass, P., and Madarasi, I. (2001). A novel catalasemutation detected by polymerase chain reaction-single strandconfirmation polymorphism, nucleotide sequencing andWestern blot analysis is responsible for the type C of Hun-garian acatalasemia. Electrophoresis 22, 49–51.
Jiang, Z., Akey, J.M., Shi, J., Xiong, M., Wang, Y., Shen, Y., et al.(2001). A polymorphism in the promoter region of catalase isassociated with blood pressure levels. Hum Genet 109, 95–98.
Makuc, J., and Petrovi�c, D. (2011). A review of oxidative stressrelated genes and new antioxidant therapy in diabeticnephropathy. Cardiovasc Hematol Agents Med Chem 9,
253–261.Maritim, A.C., Sanders, R.A., and Watkins, J.B. (2003). Oxidative
stress, antioxidants and diabetes: a review. J Biochem MolToxicol 17, 24–38.
Matthews, D.R., Hosker, J.R., Rudenski, A.S., Naylor, B.A.,Treacher, D.F., and Turner, R.C. (1985). Homeostasis modelassessment: insulin resistance and B-cell function from fastingplasma glucose and insulin concentrations in man. Diabeto-logia 28, 412–419.
Nishikawa, T., Edelstein, D., Du, X.L., Yamagishi, S., Matsu-mura, T., Kaneda, Y., et al. (2000). Normalizing mitochondrialsuperoxide production blocks three pathways of hyperglyce-mic damage. Nature 404, 787–790.
Panduru, N.M., Cimponeriu, D., Cruce, M., Ion, D.A., Mota, E.,Mota, M., et al. (2010). Association of + 35A/C (intron3/exon3) polymorphism in SOD1-gene in type 1 diabetes. Rom JMorphol Embryol 51, 37–41.
Rahimi, R., Nikfar, S., Larijani, B., and Abdollahi, M. (2005).A review on the role of antioxidants in the management ofdiabetes and its complications. Biomed Pharmacother 59,
365–373.Rolo, A.P., and Palmeira, C.M. (2006). Diabetes and mitochon-
drial function: role of hyperglycemia and oxidative stress.Toxicol Appl Pharmacol 212, 167–178.
Rosen, P., Nawroth, P.P., King, G., Moller, W., Tritschler, H.J.,and Packer, L. (2001). The role of oxidative stress in the onsetand progression of diabetes and its complications: a summaryof a Congress Series sponsored by UNESCO-MCBN, theAmerican Diabetes Association and the German Diabetes So-ciety. Diabetes Metab Res Rev 17, 189–212.
Santl Letonja, M., Letonja, M., Ikolajevic-Starcevic, J.N., andPetrovic, D. (2012). Association of manganese superoxidedismutase and glutathione S-transferases genotypes with ca-rotid atherosclerosis in patients with diabetes mellitus type 2.Int Angiol 31, 33–41.
Schroeder, W.T., and Saunders, G.E. (1987). Localization of thehuman catalase and apolipoprotein A-I genes to chromosome11. Cytogenet Cell Genet 44, 231–233.
Smaoui, M., Hammami, S., Chaaba, R., Attia, N., Hamda, K.B.,Masmoudi, A.S., et al. (2004). Lipids and lipoprotein (a) con-centrations in Tunisian type 2 diabetic patients: Relationshipto glycemic control and coronary heart disease. J DiabetesComplications 18, 258–263.
Song, F., Jia, W., Yao, Y., Hu, Y., Lei, L., Lin, J., et al. (2007).Oxidative stress, antioxidant status and DNA damage in pa-tients with impaired glucose regulation and newly diagnosedtype 2 diabetes. Clin Sci (Lond) 112, 599–606.
Tarnai, I., Csordas, M., Sukei, E., Shemirani, A.H., Kaplar, M.,and Goth, L. (2007). Effect of C111T polymorphism in exon 9
1602 GHATTAS AND ABO-ELMATTY

of the catalase gene on blood catalase activity in differenttypes of diabetes mellitus. Free Radic Res 41, 806–811.
Ukkola, O., Erkkila, P.H., Savolainen, M.J., and Kesaniemi, Y.A.(2001). Lack of association between polymorphisms of cata-lase, copper-zinc superoxide dismutase (SOD), extracellularSOD and endothelial nitric oxide synthase genes and macro-angiopathy in patients with type 2 diabetes mellitus. J InternMed 249, 451–459.
Virtamo, J., Rapola, J.M., Ripatti, S., Heinonen, O.P., Taylor, P.,Albanes, D., et al. (1998). Effect of vitamin E and beta caroteneon the incidence of primary nonfatal myocardial infarction andfatal coronary heart disease. Arch Intern Med 158, 668–675.
Yung, L.M., Leung, F.P., Yao, X., Chen, Z.Y., and Huang, Y.(2006). Reactive oxygen species in vascular wall. CardiovascHematol Disord Drug Targets 6, 1–19.
Zotova, E.V., Savost’ianov, K.V., Chistiakov, D.A., Bursa, T.R.,Galeev, I.V., and Strokov, I.A. (2004). Search for the associa-
tion of polymorphic markers for genes coding for antioxidantdefense enzymes, with development of diabetic poly-neuropathies in patients with type 1 diabetes mellitus. MolBiol (Mosk) 38, 244–249.
Address correspondence to:Dina M. Abo-Elmatty, Ph.D.
Department of BiochemistryFaculty of Pharmacy
Suez Canal University41522 Ismailia
Egypt
E-mail: [email protected]
Received for publication April 24, 2012; received in revisedform July 21, 2012; accepted July 31, 2012.
CAT AND SOD POLYMORPHISMS IN T2DM 1603