Embed Size (px)
Citation preview

ASSOCIATION OF BRITISH NEUROLOGISTS
ACUTE NEUROLOGY BOOT CAMP 2020
Wednesday 17th June
Dr Aisling Carr
NHNN, London
Acute Neuromuscular Weakness

ALL THE CMT’S………..

NEUROMUSCULAR BOOTCAMP
Neuromuscular respiratory failure
Physiology
• Lungs, respiratory drive, respiratory muscles• Diaphragm: 70%• Inspiratory: SCM, intercostal, scalene• Expiratory: abdominal wall, intercostal
• Respiratory failure: 25-30% of normal
Pathophysiology• ↓functional residual capacity
• ↑work of breathing• ↓gas exchange
• More susceptible to subtle changes

NEUROMUSCULAR BOOTCAMP
Neuromuscular respiratory failure
Physiology
• Lungs, respiratory drive, respiratory muscles• Diaphragm: 70%• Inspiratory: SCM, intercostal, scalene• Expiratory: abdominal wall, intercostal
• Respiratory failure: 25-30% of normal
Pathophysiology• ↓functional residual capacity
• ↑work of breathing• ↓gas exchange
• More susceptible to subtle changes
Investigations• FVC<20ml/Kg • ↓15-20% on lying • MIP<80cm H20• SNIP <70cm H20• Peak cough flow <160-200L/min• ABG• CXR• Overnight oximetry

NEUROMUSCULAR BOOTCAMP
Acute neuromuscular respiratory failure
ICU admission: I&V
• Patient anxiety, respiratory effort and HR
• FVC<1L or <1.5ml/kg
• ↓FVC >50%• Bulbar weakness

NEUROMUSCULAR BOOTCAMP
Acute-on-chronic neuromuscular respiratory failure
NIV
• Confusion, sedation
• Hypercapnia (PaCO2 >6kPa)
• Hypoxia

NEUROMUSCULAR BOOTCAMP
Top three neuromuscular OOH scenarios
•Essential clinical assessment
•Management
•Molecular mechanisms

CASE 1
• 25yr old
• 4 days earlier lower back pain
• 3 days of tingling in feet
• Past 2 days feels weak in his legs
• Today clumsy in his hands
• Fall in the shower when washing hair

CASE 1
• 25yr old
• 4 days earlier lower back pain
• 3 days of tingling in feet
• Past 2 days feels weak in his legs
• Today clumsy in his hands
• Fall in the shower when washing hair
Normal cranial nerves
Normal speech
Grade 4 in hands
HF 4 ADF 4 b/l
Areflexia
Impaired JPS to ankle
PP : lower abdomen
Romberg positive

UMN LMN
↑tone
No wasting
↑reflexes
↑plantars
↓tone
Muscle wasting
↓reflexes
↓plantars
Brain Cord Nerve NMJ Muscle
Root Neuropathy Mononeuro
pathy
Distribution Hemi-body Symmetrical asymme
trical
Symmetrical patchy Ocular,
bulbar,
limb
girdle
Symmetric
al
Pattern of
weakness
Pyramidal
pattern
Pyramidal
pattern
Myotom
al
pattern
Length
dependent
Patchy Fatiguab
le
Limb girdle
Gait Circumductin
g gait
Spastic diplegia Foot drop/
high
steppage
asymmetric
al
Waddle
/
trendele
nberg
trendelenb
erg
Sensory
involvement
Contralateral
sensory
inattention
Truncal sensory
level
Dermat
omal
Length
dependent
Correspon
ding
No No

UMN LMN
↑tone
No wasting
↑reflexes
↑plantars
↓tone
Muscle wasting
↓reflexes
↓plantars
Brain Cord Nerve NMJ Muscle
Root Neuropathy Mononeuro
pathy
Distribution Hemi-body Symmetrical asymme
trical
Symmetrical patchy Ocular,
bulbar,
limb
girdle
Symmetric
al
Pattern of
weakness
Pyramidal
pattern
Pyramidal
pattern
Myotom
al
pattern
Length
dependent
Patchy Fatiguab
le
Limb girdle
Gait Circumductin
g gait
Spastic diplegia Foot drop/
high
steppage
asymmetric
al
Waddle
/
trendele
nberg
trendelenb
erg
Sensory
involvement
Contralateral
sensory
inattention
Truncal sensory
level
Dermat
omal
Length
dependent
Correspon
ding
No No

Case 1: Anatomical localisation?/mechanism?

GUILLAIN-BARRE SYNDROME
IR=1/100,000 per year
Nadir @ 2-4 weeks
>8weeks suggests CIDP
20-25% require respiratory +/- cardiovascular support
5% mortality rate

Subacute onset, monophasic, immune-mediated polyradiculoneuropathies
Demyelinating and axonal forms
GBS PATHOGENESIS

GBS PATHOGENESIS
Molecular mimicry
Associated pathogens
C.jejuni
CMV
EBV
M.pneumoniae
H.influenzae
HEV
Zika virus
Vaccinations
Antibodies:
GM1
GD1a
GQ1b

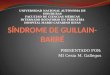
Patterns of weakness in Guillain-Barré syndrome (GBS) and
Miller Fisher syndrome and their subtypes.
Benjamin R Wakerley, and Nobuhiro Yuki Pract Neurol
2015;15:90-99
©2015 by BMJ Publishing Group Ltd

The GB Syndromes
AIDP Acute inflammatory demyelinating
polyradiculoneuropathy.
AMAN - Acute motor axonal neuropathy .
AMSAN - Acute motor and sensory axonal neuropathy .
Pharyngeal- Cervical Brachial Variant
Miller-Fisher Syndrome (Opthalmoplegia, Ataxia and Areflexia)
Bickerstaffs (CNS involvement- low GCS/brainstem)
Pure Sensory Neuropathy.
Acute Pandysautonomia.
Acute or sub acute, monophasic neuropathy.
Acute :- Peak disability by 4 weeks.
Antecedent “trigger”
Areflexia (10% can have retained or even brisk reflexes)
CSF “albuminocytologic dissociation”
Generally spontaneous recovery occurs
Commonalities…..

INVESTIGATION/ DIAGNOSIS
Clinical presentation
Neurophysiology
CSF- albuminocytological dissociation
Central Imaging if atypical presentation
In acute setting- Clinical presentation and CSF (albuminocytological dissociation)

INVESTIGATION/ DIAGNOSIS
Clinical presentation
Neurophysiology
CSF
Normal Central Imaging
Exclude mimics
Variants and Mimics of Guillain Barré SyndromeLevin, Kerry H. MDThe Neurologist: March 2004 -Volume

INVESTIGATION/ DIAGNOSIS
Neurophysiology
Delayed F-waves
Temporal dispersion
Conduction block

MANAGEMENT OF GBS
Who? Mild- mobile independently- not treated Yet at 6 months up to 38% patients may have hand function problems
When? “Time is Nerve”, probably optimal to treat early
With what IVIG and PLEX are equitable in the trails. IVIG preferred
What if they aren’t getting better? Mmmmmmm

MEGOS

The role of steroids? Early trials suggested higher mortality in GBS- yet clear benefit in SIDP, CIDP and in GBS models
Use if disability continuing beyond 4 weeks
Check Neurofascin and contactin antibodies
PLEX?
Second IVIg??......
Non-responders?

IGOS 2ND IVIG?
Walgaard et al. Second IVIg Course in Guillain-Barré Syndrome Patients with PoorPrognosis (SID-GBS) Second IVIg Dose in Guillain-Barré Syndrome;Double-blind Randomized Controlled TrialJPNS Suppl 2019.

The role of steroids?
Early trials suggested higher mortality in GBS- yet clear benefit in SIDP, CIDP and in GBS models
Use if disability continuing beyond 4 weeks
Check Neurofascin and contactin antibodies
PLEX?
Second IVIg??......
Complement inhibitors: GBS-JET phase 3 trial underway
Non-responders?

OTHER ASPECTS TO MANAGEMENT
SIADH
Thromboembolism
Labile BP- failure of autoregulation causing PRES
Cardiac Monitoring for tachy-brady- PPM insertion may be required
Gut

@12 months- over 60% independently ambulate
OUTCOME

GBS

GBS
56 yr old male
Previously fit and well
4 week history of Diplopia- horizontal Variable through the day Struggling with drinks- leaking from mouth Slurred and low volume speech
Admitted to hospital
?

CASE 2
Whilst in hospital Weakness of neck- head drop
Weakness of arms: SAD/ WE, FE)
Difficulty breathing, but CXR normal-taken to the ICU Low FVC, VC and borderline PEFR
Needed ICU as tiring, confused
Noted to using accessory muscles and accessory muscle use
Exam Ptosis
Complex ophthalmoplegia
Facial weakness
Fatiguable dysarthria
Neck flex/ext weakness
Fatiguable UL weakness
Intact reflexes
Normal sensory exam
MRI Brain normal

UMN LMN
↑tone
No wasting
↑reflexes
↑plantars
↓tone
Muscle wasting
↓reflexes
↓plantars
Brain Cord Nerve NMJ Muscle
Root Neuropathy Mononeuro
pathy
Distribution Hemi-body Symmetrical asymme
trical
Symmetrical patchy Ocular,
bulbar,
limb
girdle
Symmetric
al
Pattern of
weakness
Pyramidal
pattern
Pyramidal
pattern
Myotom
al
pattern
Length
dependent
Patchy Fatiguab
le
Limb girdle
Gait Circumductin
g gait
Spastic diplegia Foot drop/
high
steppage
asymmetric
al
Waddle
/
trendele
nberg
trendelenb
erg
Sensory
involvement
Contralateral
sensory
inattention
Truncal sensory
level
Dermat
omal
Length
dependent
Correspon
ding
No No

INVESTIGATION
NCS/EMG: Normal
RNS/SFEMG: confirms a junctionopathy
Acetylcholine receptor ab positive(MuSK if bulbar predominance)
Ct Thorax confirms a enlarged Thymus Gland
Diagnosis: Myasthenia Gravis

NMJ transmission and failure

NEUROPHYSIOLOGY
10 % decrement 1st: 5th positive• 65-80% Generalised• 50% Ocular
Repetitive nerve stimulation Single fibre EMG
Normal jitter < 35µsec.
Abnormal
94% Generalised MG.
80% Ocular MG.
Also abnormal in MND, Myopathy and Neuropathy.

DIFFERENTIAL DIAGNOSIS
Brainstem Pupils Bulbar vs pseudobulbar/cerebellar Bladder/Bowel
Peripheral Nerve (GBS etc) Areflexia Pupils Wasting
Anterior Horn Eyes not involved Fascics/Wasting
Muscle CK Ocular /Facial not involved
All lack fatiguability and diurnal variation

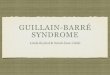
MG EPIDEMIOLOGY
IR: 14/million per year
PR: 150/million0-9 10-19 20-29 30-39 40-49 50-59 60-69 70-79 >80
0
25
50
75 Thymoma MG
Non-thymoma MG
age groups (years)
nu
mb
er
of
ca
se
s
00
50
100
150
Male
Female
0-9 10-19 20-29 30-39 40-49 50-59 60-69 70-79 >80
EOMG LOMG
age group (years)
IR (
cases p
er
mil
lio
n p
ers
on
-years
)
AS Carr. Actual world epidemiology of Myasthenia Gravis (Chapter
2). In Mineo TC, editor. Novel Challenges in Myasthenia Gravis.
Nova Science Publishers, Inc.: 2015;

MG EPIDEMIOLOGY
IR: 14/million per year
PR: 150/million0-9 10-19 20-29 30-39 40-49 50-59 60-69 70-79 >80
0
25
50
75 Thymoma MG
Non-thymoma MG
age groups (years)
nu
mb
er
of
ca
se
s
00
50
100
150
Male
Female
0-9 10-19 20-29 30-39 40-49 50-59 60-69 70-79 >80
EOMG LOMG
age group (years)
IR (
cases p
er
mil
lio
n p
ers
on
-years
)

MANAGEMENT
A patient should be managed in hospital for significant bulbar symptoms, low vital capacity, respiratory symptoms or progressive deterioration.
Assessment by speech and language therapist to advise on swallowing is mandatory.
Regular assessment of vital capacity is mandatory.
•IVIg (2g/kg/3-5 days) or PLEX
•Commence oral steroids
•Pyridostigmine
Sussman J,Farrugia ME, Maddison P,et al. Pract Neurol 2015;15:199–206.

MANAGEMENT
A patient should be managed in hospital for significant bulbar symptoms, low vital capacity, respiratory symptoms or progressive deterioration.
Assessment by speech and language therapist to advise on swallowing is mandatory.
Regular assessment of vital capacity is mandatory.
•IVIg (1g/kg/3-5 days) or PLEX
•Commence oral steroids
•Pyridostigmine
•RCT: Rozanolixizumab
Sussman J,Farrugia ME, Maddison P,et al. Pract Neurol 2015;15:199–206.

MANAGEMENT
A patient should be managed in hospital for significant bulbar symptoms, low vital capacity, respiratory symptoms or progressive deterioration.
Assessment by speech and language therapist to advise on swallowing is mandatory.
Regular assessment of vital capacity is mandatory.
•IVIg (2g/kg/3-5 days) or PLEX
•Commence oral steroids
•Pyridostigmine
•RCT: Rozanolixizumab
Sussman J,Farrugia ME, Maddison P,et al. Pract Neurol 2015;15:199–206.

GBS
MG

GBS
MG Acute on Chronic

GBS
MG Acute on Chronic
De novo NMRF:
• MND
• MG
• Adult onset acid maltase deficiency (Pompe’s)
• Mitochondrial myopathy
• Sporadic late-onset nemaline myopathy
• colchicine myopathy

CHRONIC NMRF

CHRONIC NMRF
• Cardiorespiratory surveillance• Emergency care plan• End of life discussion

ASSOCIATION OF BRITISH NEUROLOGISTSACUTE NEUROLOGY BOOT CAMP 2020
Week 2
15 June 7 – 8 pm Stroke - Dr Akram Hosseini, Nottingham
16 June 7 – 8 pm The Dizzy Patient - Dr Diego Kaski, London
17 June 7 – 8 pmAcute neuromuscular weakness - Dr Aisling Carr,
London
18 June 7 – 8 pmSurviving your first year as registrar - Dr Alex Foulkes,
London
Association of British Neurologists, Ormond House, 27 Boswell Street, London WC1N 3JZ
Email: [email protected]. Telephone: 02074054060







![Guillain-Barré Syndrome 28 and Related DisordersGuillain-Barré syndrome (GBS), also known as Landry-Guillain-Barré-Strohl syndrome, was described in 1916 [ 1, 2 ] . GBS is usually](https://img.pdfslide.us/doc/110x75/5f334ccc3207631439633ebc/guillain-barr-syndrome-28-and-related-disorders-guillain-barr-syndrome-gbs.jpg)