Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Association between statins and clinical outcomes among menwith prostate cancer: a systematic review and meta-analysisAD Raval1,2, D Thakker3, H Negi4, A Vyas5 and MW Salkini6,7
BACKGROUND: Mixed evidence exists regarding the effects of statins among men with prostate cancer. We aimed to determinethe association between statin use and clinical outcomes in prostate cancer using systematic review and meta-analysis.METHODS: Original articles published until second week of August 2015 were searched in electronic databases (Medline-Ovid,Pubmed, Scopus, The Cochrane Library, Web of Science, ProQuest) for studies on statin use in prostate cancer. The main clinicaloutcomes for the review were: biochemical recurrence (BCR), metastases, and all-cause and prostate cancer-specific mortality.Meta-analysis was performed to calculate the pooled hazard ratio (pHR) and their 95% confidence interval (95% CI). Heterogeneitybetween the studies was examined using I2 statistics. Meta-regression was performed, wherever significant heterogeneity wasfound in the meta-analyses, to find factors associated with poor outcomes, and sensitivity analyses were conducted to assess therobustness of findings. The analyses were conducted using RevMan v5.3, STATA v14, and R v3.1.1.RESULTS: Out of the 1002 retrieved citations, 34 observational cohort studies met the inclusion criteria. Statin use was associatedwith a 21% reduction in the risk of BCR among those treated with radiation therapy (pHR: 0.79, 95% CI: 0.65, 0.95, P-value = 0.01, 10studies, I2 = 54%), whereas it was not associated with the BCR among those treated with radical prostatectomy (pHR: 0.94, 95% CI:0.81, 1.09, P-value = 0.43, 15 studies, I2 = 65%). Statin use was associated with a 22% reduction in the risk of metastases (pHR: 0.78,95% CI: 0.68, 0.87, P-valueo0.001, 6 studies, I2 = 0%), and a 24% reduction in risk of both all-cause mortality (pHR: 0.76, 95% CI: 0.63,0.91, P-value = 0.004, 6 studies, I2 = 71%), and prostate cancer-specific mortality (pHR: 0.76, 95% CI: 0.64, 0.89, P-value = 0.0007, 5studies, I2 = 40%).CONCLUSIONS: Our systematic review found that statin significantly reduced the all-cause and prostate cancer-specific mortalityand improved the BCR in certain subgroup of men with prostate cancer. In future, randomized controlled trials should beconducted to establish efficacy of statins among men with prostate cancer.
Prostate Cancer and Prostatic Diseases advance online publication, 19 January 2016; doi:10.1038/pcan.2015.58
INTRODUCTIONAccording to the recent report of the World Health Organizationof 184 countries, prostate cancer is the most common non-skincancer in men with an estimated incidence of 1.1 million cases ofprostate cancer and accounts for 15% of cancer cases diagnosedin men as of 2012. Prostate cancer is the fifth leading cause ofdeath owing to cancer in men (6.6% of total death in men)worldwide with an estimated death of 307 000 in 2012.1 Men withprostate cancer usually experience a rise in the PSA levels, acondition called biochemical recurrence (BCR).2 BCR is also one ofthe strongest factors associated with development of subsequentmetastasis and death. Although radiation therapy (RT) and radicalprostatectomy (RP) are the key treatment options to reduce therisk of BCR, nearly 20–40% men treated with RP3–5 or 30–50% ofthose treated with RT develop BCR.5 Therefore, there are urgentneeds for effective treatment to improve survival and quality oflife by reducing the risk of recurrence and metastases among menwith prostate cancer.Statins aka 3-hydroxy-3-methylglutaryl coenzyme A reductase
inhibitors are usually prescribed to decrease the serum cholesterollevels and reduce the risk of cardiovascular disease.6 Recently, the
role of statins has been examined for the management of prostatecancer owing to its anticancer properties.7 Cancer cells haveincreased rates of lipid biosynthesis to improve the cellularstructure, angiogenesis and to reduce the rates of apoptosis.8
Statins inhibit lipid biosynthesis by inhibiting 3-hydroxy-3-methylglutaryl coenzyme A, leading to increase the apoptosis ofcancer cells.7–9 In addition, statins have pleiotropic effects, whichhelp in the reduction of inflammation and cellular proliferation byinhibiting Ras proteins,7,10 and inhibit other cellular pathways. Inaddition, certain lipophilic statins in high concentrations inhibitcancer cell's migration in prostate cancer cells, which may preventmetastases.11 Therefore, many clinical studies have been per-formed to investigate the clinical utility of statin among men withprostate cancer.Two prior systematic reviews of epidemiological studies
reported mixed findings on the association between statin useand clinical outcomes among men with prostate cancer.12,13 In thefirst systematic review, Scosyrev et al.13 retrieved eight cohortstudies as of May 2012 and concluded that statin use was notassociated with BCR among men treated with either RP or RT. Inthe subsequent meta-analysis, Park et al.12 retrieved 13 studies as
1Department of Pharmaceutical Systems and Policy, School of Pharmacy, West Virginia University, Morgantown, WV, USA; 2Healthcore, Inc., Wilmington, DE, USA; 3HealthOutcomes Research, Capita India, Mumbai, India; 4Department of Pharmacology, Post-Graduate Medical Education and Research Institute (PGIMER), Chandigarh, India;5Department of Epidemiology, School of Public Health, Rutgers, the State University of New Jersey, Piscataway, NJ, USA; 6Department of Hospital Medicine, Cleveland Clinic,Cleveland, OH, USA and 7Department of Urology, School of Medicine, West Virginia University, Morgantown, WV, USA. Correspondence: Dr AD Raval, HealthCore, Inc., 123Justison Street, Suite 200, Wilmington, DE 19801, USA.E-mail: [email protected] 2 September 2015; revised 11 October 2015; accepted 8 November 2015
Prostate Cancer and Prostatic Diseases (2016), 1–12© 2016 Macmillan Publishers Limited All rights reserved 1365-7852/16
www.nature.com/pcan

of August 2012 and concluded that statin use was associated witha 32% reduction in the risk of BCR among men treated with RT;however, this study did not find any association between statinuse and BCR among men treated with RP. The investigators of thisstudy also noticed a significant heterogeneity in the pooled studyestimates from the limited number of studies and suggested theneed for further research to provide conclusive evidence.12 Manystudies have been published since the date of search of thosesystematic reviews. Therefore, we have conducted this systematicreview and meta-analysis to examine the association betweenstatin use and clinical outcomes such as BCR, metastases and all-cause and prostate cancer-related mortality among men withprostate cancer.
MATERIALS AND METHODSWe followed the standard guidelines of the Preferred Reporting Itemsfor Systematic Reviews and Meta-Analyses (PRISMA) Statement14 andCochrane Collaboration guidelines15 to carry out this systematic reviewand meta-analysis.
Criteria for study selectionWe included both prospective randomized clinical trials (RCTs) (double-blinded, single-blinded or cross-over) and observational (cohort or case–control) studies examining the clinical outcomes of statins among menwith prostate cancer. We excluded animal studies and in vitro studies, quasior pseudo RCTs and studies with shorter duration (⩽6 months) of follow-up. The primary outcome of interest for our review was BCR. Secondaryoutcomes of interest were: development of metastases, all-cause mortality,and prostate cancer-specific mortality.
Data sources and searchesWe searched Medline (Ovid), Scopus and the Cochrane library (sinceinception to second week of March 2015) to identify RCTs andobservational studies assessing the effects of statins among men withprostate cancer. In addition, we also searched the Web of Science andProQuest Dissertations and Theses Full Text until March 2015 to identifygray literature related to unpublished theses or dissertations on the effectsof statins on prostate cancer. We searched these databases usingkeywords, such as ‘statins’, ‘prostate neoplasm’ and ‘prostate cancer’. Thesearch strategy for each database is reported in Supplementary AppendixS1 with keywords and the number of retrieved citations per string. We alsocreated weekly alerts for new articles for the electronic databases andincluded the new articles available until 15 August 2015. Finally, we alsoskimmed through the reference lists of identified studies to find additionalpertinent studies.
Data extraction and quality assessmentTwo authors (DT, HN) independently assessed the retrieved articlesand gray literature for inclusion of articles in the review. The inter-raterkappa statistic was calculated to assess the agreement between thetwo authors for inclusion or exclusion of the articles. Discrepancies aboutthe inclusion or exclusion were resolved by consensus of the thirdauthor (ADR).From all the eligible studies, all four authors (ADR, AV, DT, and HN)
independently extracted information from the included studies using apredefined data extraction form. In the presence of multiple publicationsof a study, we included the article with latest and comprehensiveinformation available out of those multiple publications. We designed thedata extraction form to capture information about study design, country ofparticipants, year of publication, sample size, inclusion and exclusioncriteria of individual studies, prostate cancer stage and severity relatedvariables, duration of statin use, type and other baseline characteristics. Inaddition, we also extracted data on the reported outcomes from eachstudy on BCR, metastases, all-cause mortality, and prostate cancer-specificmortality with details on statistical parameters, such as unadjusted andadjusted hazard ratios (HRs).We utilized the Newcastle–Ottawa scale (NOS) tool to examine the risk
of bias in included observational studies. The NOS allots up to nine pointsfor the least risk of bias in three domains: (1) selection of study groups(four points); (2) comparability of groups (two points); and (3)
ascertainment of exposure and outcomes (three points) for cohortstudies.16 The risk of bias or poor quality were considered as ‘high’ withone or four score total scores, ‘fair’ with a total score of 4 to 6 and ‘good’with a total score ⩾7.17
Data synthesis and analysisWe computed a pooled hazard ratio (pHR) with 95% confidence interval(CI) for all clinical outcomes reported in the included studies usingrandom-effects models in RevMan version 5.3 (The CochraneCollaboration, Copenhagen, Denmark).18 We used the Cochrane Chi-square χ2 (Cochran Q) statistic and the I2 test to analyze heterogeneityacross the included studies.18 We performed meta-regression analysiswherever we found considerable heterogeneity in the pooled analysis. Weentered parameters such as: age, follow-up duration, publication year, PSAlevel, percentage of patients in tumor stage ⩾ T2, percentage of patientswith Gleason score ⩾ 7, and ethnicity, which could be responsible for thedifferences in the outcomes observed among the studies. We processedmeta-regression analysis in STATA version 14 (STATA, College Station,TX, USA) using the metareg command.19 We also derived the polygramsbased on various predicted values of the factors that were found to besignificantly associated with the outcomes in the meta-regression analysisin R version 3.1.1 (R Foundation for Statistical Computing, Vienna, Austria).We determined the presence of publication bias in observational studiesusing Egger’s method (Kendall’s Tau)20 and using a contour-enhancedfunnel plot to determine other causes of publication bias by examining thesymmetry of the plot.21 Further, we did sensitivity analyses by status ofprimary therapy (RT or RP) for prostate cancer to assess the robustness ofpooled estimates.
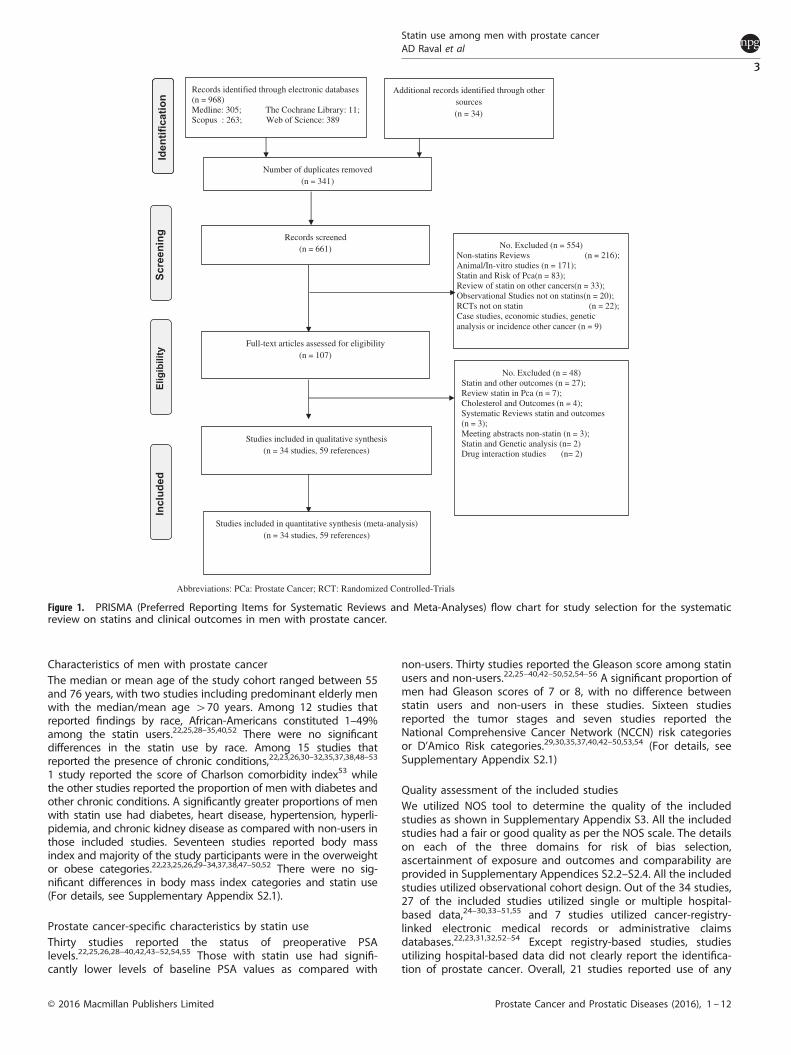
RESULTSWe retrieved a total of 1002 citations through electronic databasesand gray literature. Figure 1 depicts the study selection process asper PRISMA framework from the retrieved citations. We excludedthe following studies: studies assessing outcomes followingstatin use in animal models; in vitro studies; reviews; RCTs ofinterventions other than statins; statin use in other population;and assessing risk of prostate cancer with the use of statins.Finally, 34 studies (59 references) met the inclusion criteria for thecurrent review. Multiple references per study was mainly due tothe study published as conference presentations or comments onthe published studies.
Characteristics of included studiesCharacteristics of all the 34 studies are presented in Table 1. All thestudies were observational cohort studies published between2003 and 2015. Twenty-five studies were conducted in theUnited States,22–46 two in France,47,48 two in Korea,49,50 onein Greece,51 one in United Kingdom,52 one in Canada53 and onein Norway54 each while the last one utilized data from six centerslocated in the North America and Europe.55 The study cohort sizeranged from 247 (ref. 50) to 11 772 (ref. 52) among the includedstudies. Overall, the percentage of statin users ranged from 5.3%24
to 71.1%.27 All the included studies had at least 2 years mean ormedian follow-up. Sixteen studies restricted the study cohort tomen with prostate cancer treated with RP25–31,33–35,47–51,55 and notusing adjuvant hormone therapy and RT, whereas 13 studiesincluded men with prostate cancer treated with RT and nottreated with RP.32,36–46 The rest of the five studies included mendiagnosed with prostate cancer without restricting them to anyprimary prostate cancer treatment RP/RT.Furthermore, 12 of the included studies restricted their study
cohort to those diagnosed with localized prostate cancer andexcluded those who have metastatic or node-positive prostatecancer,22,29–32,40,44,46,47,52,53,55, whereas 11 studies excluded thosewith receipt of adjuvant hormone therapy.24,25,28,32,33,35,39,40,47,49,53
Statin use among men with prostate cancerAD Raval et al
2
Prostate Cancer and Prostatic Diseases (2016), 1 – 12 © 2016 Macmillan Publishers Limited
Characteristics of men with prostate cancerThe median or mean age of the study cohort ranged between 55and 76 years, with two studies including predominant elderly menwith the median/mean age 470 years. Among 12 studies thatreported findings by race, African-Americans constituted 1–49%among the statin users.22,25,28–35,40,52 There were no significantdifferences in the statin use by race. Among 15 studies thatreported the presence of chronic conditions,22,23,26,30–32,35,37,38,48–53
1 study reported the score of Charlson comorbidity index53 whilethe other studies reported the proportion of men with diabetes andother chronic conditions. A significantly greater proportions of menwith statin use had diabetes, heart disease, hypertension, hyperli-pidemia, and chronic kidney disease as compared with non-users inthose included studies. Seventeen studies reported body massindex and majority of the study participants were in the overweightor obese categories.22,23,25,26,29–34,37,38,47–50,52 There were no sig-nificant differences in body mass index categories and statin use(For details, see Supplementary Appendix S2.1).
Prostate cancer-specific characteristics by statin useThirty studies reported the status of preoperative PSAlevels.22,25,26,28–40,42,43–52,54,55 Those with statin use had signifi-cantly lower levels of baseline PSA values as compared with
non-users. Thirty studies reported the Gleason score among statinusers and non-users.22,25–40,42–50,52,54–56 A significant proportion ofmen had Gleason scores of 7 or 8, with no difference betweenstatin users and non-users in these studies. Sixteen studiesreported the tumor stages and seven studies reported theNational Comprehensive Cancer Network (NCCN) risk categoriesor D’Amico Risk categories.29,30,35,37,40,42–50,53,54 (For details, seeSupplementary Appendix S2.1)
Quality assessment of the included studiesWe utilized NOS tool to determine the quality of the includedstudies as shown in Supplementary Appendix S3. All the includedstudies had a fair or good quality as per the NOS scale. The detailson each of the three domains for risk of bias selection,ascertainment of exposure and outcomes and comparability areprovided in Supplementary Appendices S2.2–S2.4. All the includedstudies utilized observational cohort design. Out of the 34 studies,27 of the included studies utilized single or multiple hospital-based data,24–30,33–51,55 and 7 studies utilized cancer-registry-linked electronic medical records or administrative claimsdatabases.22,23,31,32,52–54 Except registry-based studies, studiesutilizing hospital-based data did not clearly report the identifica-tion of prostate cancer. Overall, 21 studies reported use of any
Abbreviations: PCa: Prostate Cancer; RCT: Randomized Controlled-Trials
No. Excluded (n = 48) Statin and other outcomes (n = 27); Review statin in Pca (n = 7); Cholesterol and Outcomes (n = 4); Systematic Reviews statin and outcomes (n = 3); Meeting abstracts non-statin (n = 3); Statin and Genetic analysis (n= 2) Drug interaction studies (n= 2)
No. Excluded (n = 554) Non-statins Reviews (n = 216); Animal/In-vitro studies (n = 171); Statin and Risk of Pca(n = 83); Review of statin on other cancers(n = 33); Observational Studies not on statins(n = 20); RCTs not on statin (n = 22); Case studies, economic studies, genetic analysis or incidence other cancer (n = 9)
Studies included in quantitative synthesis (meta-analysis) (n = 34 studies, 59 references)
Studies included in qualitative synthesis (n = 34 studies, 59 references)
Full-text articles assessed for eligibility (n = 107)
Records identified through electronic databases(n = 968) Medline: 305; The Cochrane Library: 11; Scopus : 263; Web of Science: 389
Scre
enin
g In
clud
ed
Elig
ibili
ty
Additional records identified through other sources (n = 34)
Records screened (n = 661)
Number of duplicates removed (n = 341)
Iden
tific
atio
n
Figure 1. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow chart for study selection for the systematicreview on statins and clinical outcomes in men with prostate cancer.
Statin use among men with prostate cancerAD Raval et al
3
© 2016 Macmillan Publishers Limited Prostate Cancer and Prostatic Diseases (2016), 1 – 12

Table1.
Characteristicsofincluded
studiesin
thesystem
atic
review
andmeta-an
alysis
Stud
yna
me
Datasou
rce
N(NOS)
Statin
users
N(%
)Follow-upmedian
(IQR),inyears
Age
(years),mean(s.d.)
ormedian(IQ
R)AA(%
)PSA(in
ngml−
1 )mean
(s.d.)or
median(IQ
R)GS
Tumor
stag
e
Radicalprostatectom
yan
d/or
radiationtherap
yKatzet
al.,2
3US
Can
ceroftheProstateStrategic
Urologic
ResearchEn
deavo
r(CaP
SURE);
7042
1824
(25.9)
4(0–16
)μ:6
4.4(7.8)
——
——
Geybelset
al.,2
2US
Seattle-Pu
get
SountSu
rveillance,E
pidem
iology,
andEn
dResultscancerregistry
1001
289(28.9)
μ:6
.1(1)μ:6
3.1(6.8)
(2)μ:6
0.9(8.1)
—(1)M:5
.7(4.4,8
.5)
(2)M:6
.3(4.7,9
.5)
(1)⩾7:
47%
(2)⩾7:
47%
(1)Lo
cal:72
%(2)Lo
cal:73
%Macleodet
al.,2
4US
University
ofWashingtonSchoolofMed
icine
1734
92(5.3)
3.9
——
——
—Grytliet
al.,5
4Norw
ayCan
cerregistryofNorw
ay;N
orw
egian
Prescriptiondatab
ase
3561
927(26.0)
3.25
(1)μ:7
1.9(7.5)
(2)μ:7
1.1(9.3)
—410
:91%
⩾7:
87.1%
⩽T2
a:15
%;T2b
-2c:
19%;⩾T3
a:67
%Yu
etal.,5
2UK
United
Kingdom
National
Can
cerReg
istry
Linkeddatab
ases
1177
234
07(28.9)
μ:4
.4(2.9)
μ:7
6.3(8.1)
(1)1.3%
(2)1.1%
(1)410
:42.7%
(2)410
:40.0%
(1)⩾7:
34.7%
(2)⩾7:
291%
—
Radicalprostatectom
yHam
iltonet
al.,2
5USa
5Ve
teransAdministrationMed
ical
Cen
ters;
Shared
Equal
AccessReg
ional
Can
cerHospital
(SEA
RCH)Datab
ase
1319
236(17.9)
μ:3
.58
(1)μ:6
2.6(5.6)
(2)μ:6
0.6(6.6)
(1)36
%(2)47
%(1)M:6
.2(4.7,9
.1)
(2)M:6
.9(4.9,1
0.5)
(1)⩾7:
50%
(2)⩾7:
38%
(1)T1
c:67
%;
T2/T3:
33%
(2)T1
c:58
%;
T2/T3:
42%
Kraneet
al.,2
6US
VattikutiUrologyInstitute
data
3828
1031
(26.9)
μ:2
.17
(1)μ:6
1.4(6.6)
(2)μ:5
9.4(7.5)
(1)36
%(2)47
%(1)M:5
.0(4.1,6
.5)
(2)M:5
.2(4.1,7
.2)
(1)⩾7:
69%
(2)⩾7:
64%
(1)T1
c:73
;T2
/T3:
27%
(2)T1
c:73
;T2
/T3:
27%
Rioja
etal.,2
7US
Mem
orial
Sloan
-KetteringCan
cerCen
ter
3748
1093
(29.0)
(1)M:6
2(57,
66)
(2)M:5
9(54,
64)
(1)36
%(2)47
%.
(1)M:5
.1(3.8,7
.0)
(2)M:5
.3(3.9,7
.5)
(1)⩾7:
75%
(2)⩾7:
71%
—
Kuet
al.,4
9Korea
SeoulNational
University
Hospital
687
87(12.7)
3.2(0.3–11
.9)
(1)μ:6
5.3(6.8)
(2)μ:6
5.2(6.7)
(1)36
%(2)47
%(1)μ:9
.6(9.3)
(2)μ:1
3.6(20.5)
(1)⩾7:
79.3%
(2)⩾7:
73%
(1)T1
:60
%;
T2–T3
:40
.2%
(2)T1
:60
%;
T2–T3
:40
.3%
Mondulet
al.,2
9US
JohnHopkinsHospital
2399
386(16.1)
7(1)μ:5
7.7
(2)μ:5
6.0
(1)36
%(2)47
%(1)μ:6
.3(2)μ:7
.1(1)⩾7:
18.9%
(2)⩾7:
18.7%
(1)T1
:73
.7%;
T2–T3
a:26
.3%
(2)T1
:67
.7%;
T2–T3
a:32
.1%
Ritch
etal.,2
8US
Columbia
University
Urologic
Onco
logydata
1261
281(22.3)
3.0
(1)μ:6
2.0
(2)μ:5
9.0
(1)36
%(2)47
%(1)M:6
.4(2)M:7
.1(1)M:7
(2)M:6
(1)T1
:92
.5%;
T2–T3
a:07
.5%
(2)T1
:86
.4%;
T2–T3
a:13
.6%
Masset
al.,3
0US
New
York
University
Med
ical
Records
1446
437(30.2)
μ:4
.75
—(1)36
%(2)47
%(1)M:5
.1(4.0,6
.8)
(2)M:5
.0(4.0,7
.0)
(1)⩾7:
42.1%
(2)⩾7:
34.6%
(1)T1
:82
.0%;
T2–T3
a:18
.0%
(2)T1
:81
.6%;
T2–T3
a:18
.4%
Chao
etal.,3
1,32US
KaiserPe
rman
ente
SouthernCalifo
rnia
(KPS
C);
SEER
Reg
istryData
1184
446(37.7)
μ:4
.3(s.d.:1.35
)(1)μ:6
1.0(6.0)
(2)μ:5
9.0(7.0)
(1)36
%(2)47
%(1)μ:6
.7(4.2)
(2)μ:7
.1(6.4)
(1)⩾7:
48%
(2)⩾7:
44%
(1)Stag
eII:
85.0%
(2)Stag
eII:
87.0%
Kontraroset
al.,5
1
Greece
Hospital
Pitie-Salpetriere
588
107(18.0)
μ:3
.4(s.d.:2.6)
(1)μ:6
5.4(5.2)
(2)μ:6
5.2(5.8)
(1)36
%(2)47
%(1)M:7
.2(5.6,9
.7)
(2)M:8
.0(6,1
0.6)
(1)⩾7:
55.1%
(2)⩾7:
46.7%
—
Rieke
net
al.,5
5
multi-countries
Cen
ters
from
US,
Can
ada,
Austriab
6842
2275
(33.3)
M:2
.08(0.67–
3.5)
(1)μ:6
1.7(6.5)
(2)μ:6
1.0(6.7)
(1)36
%(2)47
%(1)μ:7
.7(5.5)
(2)μ:7
.5(6.0)
(1)⩾7:
43.5%
(2)⩾7:
45.8%
(1)T3
:25
.3%;
N1/M1:
10.9%
(2)T3
a:25
.1%;
N1/M1:
11.4%
Allo
ttet
al.,3
3US
5Ve
teransAdministration(VA)Med
ical
Cen
ters;
Shared
Equal
AccessReg
ional
Can
cerHospital
(SEA
RCH)Datab
ase
1146
400(34.9)
6.4(4.2–8.9)
(1)μ:6
0.6(6.3)
(2)μ:6
0.7(6.5)
(1)36
%(2)47
%(1)M:5
.9(4.7,9
.1)
(2)M:7
.1(5.1,1
0.7)
(1)⩾7:
29%
(2)⩾7:
40%
(1)T1
:61
%;
T2/T3:
39%
(2)T1
:64
%;
T2/T3:
36%
Ishak-Howardet
al.,3
4
US
University
ofMichigan
ProstateCan
cerGen
etics
Project
(PCGP)
539
258(47.9)
μ:7
.9(s.d.:4.7)
(1)μ:5
8.0(7.4)
(2)μ:5
5.2(7.6)
(1)36
%(2)47
%(1)μ:1
.4(13.4)
(2)μ:2
.8(23.0)
(1)⩾7:
50.4%
(2)⩾7:
51.3%
(1)T2
:65
.9%;
T3:20
.9%
(2)T2
:70
.4%;
T3:21
.0%
Dan
ziget
al.,3
5US
Columbia
urologic
onco
logydatab
ase
767
76(9.9)
2.25
(1)M:6
5(2)M:6
3(1)36
%(2)47
%(1)M:5
.72
(2)M:6
.05
(1)⩾7:
65%
(2)⩾7:
54%
(1)T1
:74
%;
T2:24
%;T
3:2%
(2)T1
:67
%;
T2:29
%;T
3:3%
Misraiet
al.,4
8Fran
ceUnclear
377
97(25.7)
μ:2
.8(s.d.:0.83
)M:6
4(61,
70)
M:6
4(59,
60)
(1)36
%(2)47
%(1)M:6
.6(4.8,8
.1)
(2)M:6
.4(4.7,8
.6)
(1)⩾7:
72.1%
(2)⩾7:
77.1%
(1)T1
c:67
%;
T2:31
%;T
3:2%
(2)T1
c:71
%;
T2:26
%;T
3:1%
Songet
al.,5
0Koreaa
AsanMed
ical
Cen
ter
2137
241(11.3)
μ:3
.3(1)67
(63,
70)
(2)67
(63,
71)
(1)36
%(2)47
%(1)M:6
.2(4.5,9
.5)
(2)M:6
.9(4.7,1
1.2)
(1)⩾7:
61.4%
(2)⩾7:
53.7%
(1)T2
:74
.8%;T3
:24
%;N+:2
%(2)T2
:64
.5%;T3
a:32
%;N+:3
%
Statin use among men with prostate cancerAD Raval et al
4
Prostate Cancer and Prostatic Diseases (2016), 1 – 12 © 2016 Macmillan Publishers Limited

Table1.
(Continued
)
Stud
yna
me
Datasou
rce
N(NOS)
Statin
users
N(%
)Follow-upmedian
(IQR),inyears
Age
(years),mean(s.d.)
ormedian(IQ
R)AA(%
)PSA(in
ngml−
1 )mean
(s.d.)or
median(IQ
R)GS
Tumor
stag
e
Cattarinoet
al.,4
7Fran
ceHospital
Pitie-Salpetriere
591
156(26.4)
M:3
.5(2.2–5)
(1)M:6
4(50,
70)
(2)M:6
2(49,
69)
(1)36
%(2)47
%(1)M:7
.9(3.9,1
1.8)
(2)M:8
.4(4.3,1
3.7)
(1)⩾7:
40.5%
(2)⩾7:
40.7%
(1)T1
c:62
%;T
2:28
%;T
3:10
%(2)T1
c:61
%;T
2:28
%;T
3:12
%Ra
diationtherap
yKatzet
al.,3
6US
Mem
orial
Sloan
-KetteringCan
cerCen
ter
905
153(16.9)
M:3
.3(2–7.6.0)
M:6
9(45,
86)
—M:8
.2(0.6–14
2)M:7
(4–10
)T1
c:41
%;T2
:45%
;T3
:14%
Moyadet
al.,3
8US
Schiffler
Can
cerCen
ter
512
65(12.7)
5.7(2.1)
(1)66
.3(6)
(2)65
.6(7.4)
—(1)μ:6
.5(2.9)
(2)μ:7
.9(4.5).
(1)μ:6
.6(s.d.:
0.7)
(2)μ:6
.6(s.d.:
0.8)
(1)T1
b–T2
b:9
2.3%
;T2
c–T3
a:7.7%
(2)T1
b–T2
b:7
7.4%
;T2
c–T3
a:22
.6%
Moyadet
al.,3
7US
Michigen
Med
ical
Cen
tre
938
191(20.4)
5.4
(1)μ:6
6(6.4)
(2)μ:6
6(7.4)
—(1)M:6
.6(2)M:7
.1.
(1)M:7
(2)M:7
(1)T1
b–T2
b:9
4.2%
;T2
c–T3
a:5.8%
(2)T1
b–T2
b:9
0.6%
;T2
c–T3
a:9.4%
Sharmaet
al.,3
9US
FoxChaseCan
cerCen
ter
983
178(18.1)
4.8
M:6
9(43,
84)
—M:7
.4⩾7:31
%T1
–T2
:90
%;T
3–T4
:3.5%
Soto
etal.,4
0US
Michigen
Can
cerCen
tre
968
220(22.7)
3.9(0.2–16
.5)
(1)μ:6
8.0
(2)μ:6
8.2
(1)8.4%
(2)4.1%
(1)410
:23.3%
(2)4
10:4
1.9%
.(1)⩾7:
58.9%
(2)⩾7:
56.5%
(1)T1
:55
%;T
2:42
%;T
3:3%
(2)T1
:37
%;T
2:51
%;T
3:12
%Sh
ippyet
al.,4
1US
Mem
orial
Sloan
-KetteringCan
cerCen
ter
871
168(19.3)
7.1
——
——
—Kollm
eier
etal.,4
2US
Mem
orial
Sloan
-KetteringCan
cerCen
ter
1681
382(22.7)
5.9(0–14
)(1)⩾65
:284
(2)⩾65
:951
—(1)410
:27%
(2)410
:39%
(1)⩾7:
52%
(2)⩾7:
55%
(1)T1
:56
%;T
2:37
%;T
3:7%
(2)T1
:48
%;T
2:40
%;T
3:12
%Gutt
etal.,4
3US
University
ofChicag
o69
118
9(27.4)
4.2
(1)M:6
9(42,
83)
(2)M:6
8(44,
83)
(1)49
%(2)53
%(1)410
:34%
(2)410
:43%
(1)⩾7:
54%
(2)⩾7:
37%
(1)T1
–2a
:88%
;T2
b–c:9%
;T3/4:
3%(2)T1
–2a
:79%
;T2
b–c:15
%;T
3–4:
7%Zao
rsky
etal.,4
6US
FoxChaseCan
cerCen
ter,US
2051
691(33.7)
6.3(1.5–19
.9)
M:6
9(36,
86)
—410
:30%
⩾7:
26%
T1:58
%;T
2:39
%;
T3:3%
Chao
etal.,3
1,32USa
KaiserPe
rman
ente
SouthernCalifo
rnia
(KPS
C)-
SEER
Reg
istryData
774
401(51.8)
μ:4
.10(s.d.:1.4)
(1)μ:6
9.3(5.9)
(2)μ:6
7.5(8.0)
(1)19
.0%
(2)19
.0%
(1)μ:6
.2(s.d.:6.7)
(2)μ:6
.7(s.d.:7.8)
(1)⩾7:
52.1%
(2)⩾7:
49.6%
(1)Stag
eII:
97.5%;
Stag
eIII:2.5%
(2)Stag
eII:
98.7%;
Stag
eIII:1.3%
Cao
net
al.,5
3Can
ada
British
Columbia;
3851
914(23.7)
8.0
(1)μ:7
2(2)μ:7
1—
——
—
Ohet
al.,4
5US
Durham
VeteransAffairs
Med
ical
Cen
ter
247
174(70.4)
4.3(0.78–
11.7)
(1)μ:6
2.8
(2)μ:6
1.4
—(1)410
:5.7%
(2)410
:15.0%
(1)⩾7:
8.1%
(2)⩾7:
17.8%
(1)T1
–T2
a:97
%;
T2b–c:3%
;T3
–4:
0.0%
(2)T1
–T2
a:92
%;
T2b–c:7%
;T3
–4:
1%Cuaronet
al.,4
4US
Mem
orial
Sloan
KetteringCan
cerCen
ter
754
273(36.2)
4(0.08–
13)
(1)⩾65
:72%
(2)⩾65
:60%
—(1)410
:18%
(2)410
:29%
(1)⩾7:
84%
(2)⩾7:
85%
1)T1
–T2
a:79
%;
T2b–T2
c:18
%;
T3a+
:3%
(2)T1
–T2
a:75
%;
T2b–T2
c:19
%;
T3a+
:6%
Abbreviations:AA,African
-American
;GS,
Gleasonscore;IQR,interquartile
range;
M,m
ale;
NOS,
New
castle–Ottaw
ascale.
(1)Den
otesstatin
users
and(2)non-statinuser.Allthestudiesutilized
retrospective
cohortdesign.aIn
thestudybyCao
net
al.,5
3thedistributionofstatin
users
were:
atorvastatin:3
.5%;lovastatin:7
7.8%
;sim
vastatin:1
8.4%
;pravastatin:0
.2%.InthestudybyHam
iltonet
al.,2
5thedistributionof
statin
users
was:sim
vastatin
171(72%
);lovastatin
35(15%
);atorvastatin12
(5%);pravastatin
4(2%);fluvastatin
4(2%);rosuvastatin
1(o
1%);unkn
own9(4%).Th
estudybySo
nget
al.50usedthefollo
wing
statins:atorvastatin:57.2%
;sim
vastatin:19.2%
;rosuvastatin:11.4%
;pitavastatin:6.2%;p
ravastatin:3.1%;lovastatin:2.0%;fl
uvastatin:0.9%.InthestudybyIshak-Howardet
al.,3
419
6(36.4%
)werelip
ophilicstatin
users
and51
(9.5%)werehyd
rophilicstatin
users
.bTh
eau
thors
utilized
electronic
med
ical
reco
rdsofthefollo
wingsixcenters:(1)New
York
PresbyterianHospital;(2)University
ofMontreal,Can
ada;
(3)
University
ofTexas,TX
,USA
;(4)Urological
ResearchInstitute,Italy;(5)
Prostatecancercenter,Austria;
and(6)Med
ical
UnivesityofGraz,Austria.
Statin use among men with prostate cancerAD Raval et al
5
© 2016 Macmillan Publishers Limited Prostate Cancer and Prostatic Diseases (2016), 1 – 12

statins, whereas rest of 13 studies mentioned the use of specificstatins. Four studies also considered the use of cerivastatin whileidentifying the stain use.23,34,40,52 Statin exposure was measuredafter initial therapy in 17 studies,22,24,26–32,38,44,47,49–52 during orafter initial cancer therapy in 13 studies23,30,33–35,39–41,43–45,48,55
and after initial cancer therapy in 2 studies,25,36 whereas the
measurement of statin exposure was unclear in two studies.37,42
Every included studies performed multivariable regressioncontrolling for the potential confounders. Although there weredifferences in the number of controlled factors amongincluded studies, age, body mass index, comorbid conditions,prostate cancer stage, and grade were the most common
Study or Subgroup
Radiationtherapy
Chao 2013, US
Cuaron 2015, US
Gutt 2010, US
Kollmeier2009, US
Moyad 2006, US
Oh 2015, US
Sharma 2006, US
Shippy2007, US
Soto 2006, US
Zaorsky 2011, USSubtotal (95% CI)
Heterogeneity: Tau² = 0.05; Chi² = 19.47, df = 9 (P = 0.02); I² = 54%
Test for overall effect: Z = 2.45 (P = 0.01)
Radical Prostatectomy
Allott 2014, US
Chao 2013a, US
Danzig 2015,US
Hamilton 2010, US
Ishak-Howard 2014
Kontraros 2013
Krane 2010, US
Ku 2011, Korea
Mass 2012, US
Misrai 2015, France
Mondul 2011, US
Rieken 2013
Ritch 2011, US
Roija 2010, US
Song 2015 KoreaSubtotal (95% CI)
Heterogeneity: Tau² = 0.05; Chi² = 39.70, df = 14 (P = 0.0003); I² = 65%
Test for overall effect: Z = 0.79 (P = 0.43)
Radiation and/or Radical Prostatectomy
Geybels 2013, US
Macleod 2013,USSubtotal (95% CI)
Heterogeneity: Tau² = 0.00; Chi² = 0.23, df = 1 (P = 0.63); I² = 0%
Test for overall effect: Z = 0.94 (P = 0.35)
Total (95% CI)
Heterogeneity: Tau² = 0.05; Chi² = 69.13, df = 26 (P < 0.00001); I² = 62%
Test for overall effect: Z = 1.83 (P = 0.07)Test for subgroup differences: Chi² = 5.21, df= 2 (P = 0.07), I² = 61.6%
log[Hazard Ratio]
-0.0101
0.1133
-0.5621
-0.3711
0.4055
-1.2448
-0.0408
-0.462
0.0953
-0.462
-0.4463
0
0.1823
-0.3567
0.0583
0.4121
-0.0101
0.1655
0.1398
-0.7765
-0.0101
-0.1278
0.4055
0.1398
-0.6931
0.0583
0.1823
SE
0.1769
0.28
0.1936
0.1643
0.7725
0.6167
0.19
0.21
0.1625
0.1282
0.1575
0.1676
0.4467
0.1616
0.2265
0.2103
0.0899
0.2888
0.1726
0.37
0.2226
0.0748
0.2069
0.1308
0.1968
0.1834
0.1807
Weight
4.2%
2.6%
3.9%
4.4%
0.5%
0.8%
3.9%
3.6%
4.5%
5.1%33.5%
4.6%
4.4%
1.3%
4.5%
3.3%
3.6%
5.9%
2.5%
4.3%
1.8%
3.4%
6.2%
3.7%
5.1%
3.8%58.3%
4.1%
4.1%8.2%
100.0%
IV, Random, 95% CI
0.99 [0.70, 1.40]
1.12 [0.65, 1.94]
0.57 [0.39, 0.83]
0.69 [0.50, 0.95]
1.50 [0.33, 6.82]
0.29 [0.09, 0.96]
0.96 [0.66, 1.39]
0.63 [0.42, 0.95]
1.10 [0.80, 1.51]
0.63 [0.49, 0.81]0.79 [0.65, 0.95]
0.64 [0.47, 0.87]
1.00 [0.72, 1.39]
1.20 [0.50, 2.88]
0.70 [0.51, 0.96]
1.06 [0.68, 1.65]
1.51 [1.00, 2.28]
0.99 [0.83, 1.18]
1.18 [0.67, 2.08]
1.15 [0.82, 1.61]
0.46 [0.22, 0.95]
0.99 [0.64, 1.53]
0.88 [0.76, 1.02]
1.50 [1.00, 2.25]
1.15 [0.89, 1.49]
0.50 [0.34, 0.74]0.94 [0.81, 1.09]
1.06 [0.74, 1.52]
1.20 [0.84, 1.71]1.13 [0.88, 1.45]
0.90 [0.80, 1.01]
Hazard Ratio Hazard Ratio
IV, Random, 95% CI
0.1 0.2 0.5 1 2 5 10Favors Statin Favors No-statin
Figure 2. Forest plot of comparison: statin vs no statin for biochemical recurrence with subgroup analysis by primary cancer treatment:(a) radiation therapy, (b) radical prostatectomy, and (c) either radiation therapy or/and radical prostatectomy.
Statin use among men with prostate cancerAD Raval et al
6
Prostate Cancer and Prostatic Diseases (2016), 1 – 12 © 2016 Macmillan Publishers Limited
controlled variables. However, only 10 studies controlled forco-medications.22,26,29,34,35,46,52–54
Statin and BCRThe hazard of BCR was reported in 27studies.22,24–35,37,39–46,48–51,55 Figure 2 depicts the forest plots onthe statin use and BCR among the included studies. Overall, statinuse was marginally associated with reduction in risk of BCR usingrandom-effects model (pHR: 0.90, 95% CI: 0.80, 1.01, P-value = 0.07,27 studies, I2 = 62%). Overall estimates on BCR had a significantheterogeneity. We carried out subgroup analyses by primarycancer therapy to explore the possible reasons for the hetero-geneity. In a pooled analysis of 10 studies,32,37,39–46 statin use was
associated with 21% reduction in the risk of BCR among thosetreated with RT (pHR: 0.79, 95% CI: 0.65, 0.95, P-value = 0.01, 10studies, I2 = 54%). Among those treated with RP, statin use was notassociated with BCR (pHR: 0.94, 95% CI: 0.81, 1.09, P-value = 0.43,15 studies, I2 = 65%) in random-effects model, with significantheterogeneity.
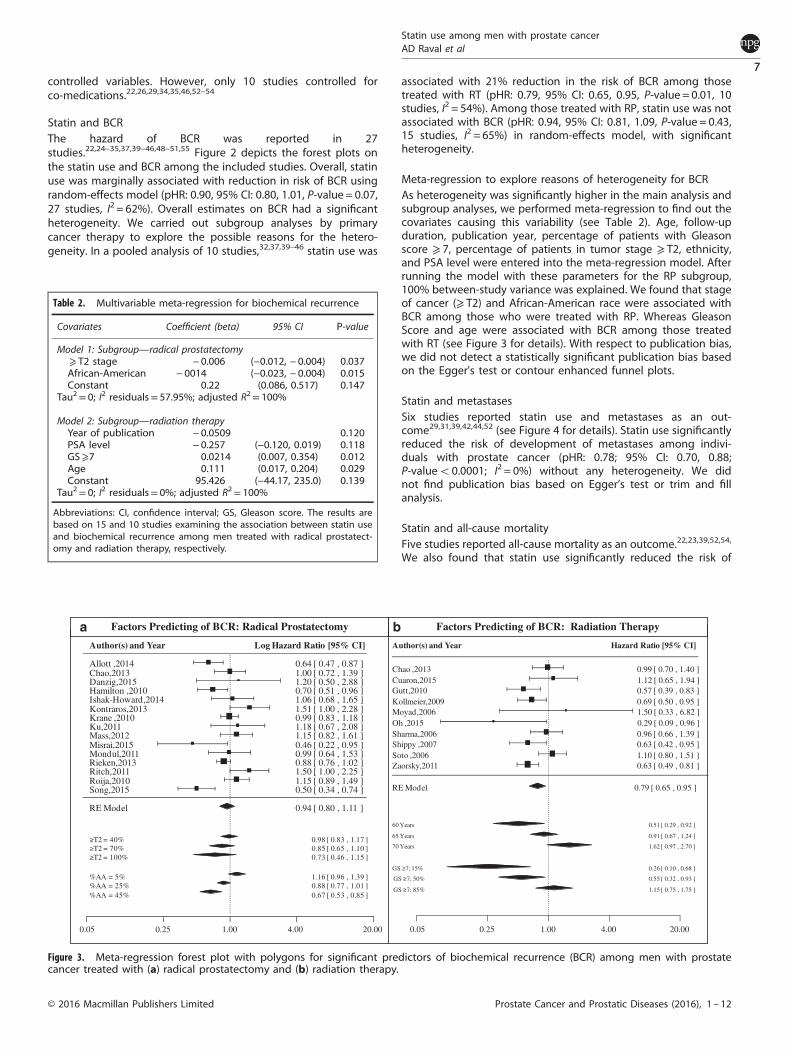
Meta-regression to explore reasons of heterogeneity for BCRAs heterogeneity was significantly higher in the main analysis andsubgroup analyses, we performed meta-regression to find out thecovariates causing this variability (see Table 2). Age, follow-upduration, publication year, percentage of patients with Gleasonscore ⩾ 7, percentage of patients in tumor stage ⩾ T2, ethnicity,and PSA level were entered into the meta-regression model. Afterrunning the model with these parameters for the RP subgroup,100% between-study variance was explained. We found that stageof cancer (⩾ T2) and African-American race were associated withBCR among those who were treated with RP. Whereas GleasonScore and age were associated with BCR among those treatedwith RT (see Figure 3 for details). With respect to publication bias,we did not detect a statistically significant publication bias basedon the Egger's test or contour enhanced funnel plots.
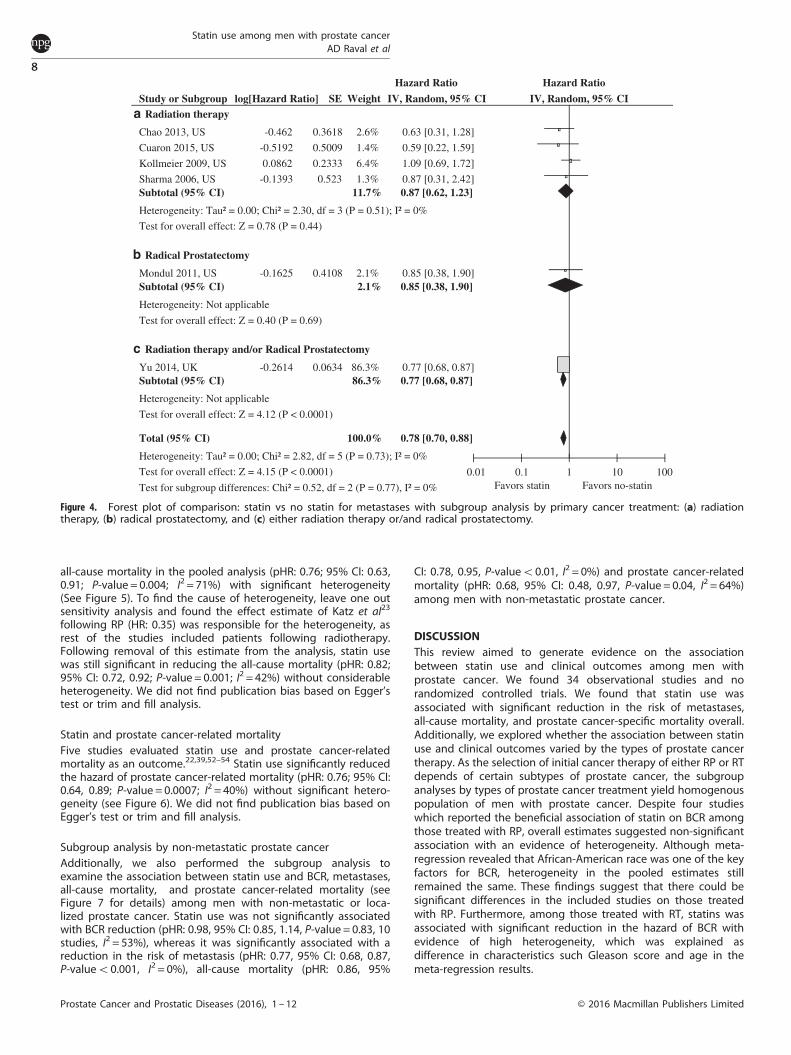
Statin and metastasesSix studies reported statin use and metastases as an out-come29,31,39,42,44,52 (see Figure 4 for details). Statin use significantlyreduced the risk of development of metastases among indivi-duals with prostate cancer (pHR: 0.78; 95% CI: 0.70, 0.88;P-valueo0.0001; I2 = 0%) without any heterogeneity. We didnot find publication bias based on Egger’s test or trim and fillanalysis.
Statin and all-cause mortalityFive studies reported all-cause mortality as an outcome.22,23,39,52,54,
We also found that statin use significantly reduced the risk of
RE Model
0.05 0.25 1.00 4.00 20.00
Song,2015Roija,2010Ritch,2011Rieken,2013Mondul,2011Misrai,2015Mass,2012Ku,2011Krane ,2010Kontraros,2013Ishak-Howard,2014Hamilton ,2010Danzig,2015Chao,2013Allott ,2014
0.50 [ 0.34 , 0.74 ]1.15 [ 0.89 , 1.49 ]1.50 [ 1.00 , 2.25 ]0.88 [ 0.76 , 1.02 ]0.99 [ 0.64 , 1.53 ]0.46 [ 0.22 , 0.95 ]1.15 [ 0.82 , 1.61 ]1.18 [ 0.67 , 2.08 ]0.99 [ 0.83 , 1.18 ]1.51 [ 1.00 , 2.28 ]1.06 [ 0.68 , 1.65 ]0.70 [ 0.51 , 0.96 ]1.20 [ 0.50 , 2.88 ]1.00 [ 0.72 , 1.39 ]0.64 [ 0.47 , 0.87 ]
0.94 [ 0.80 , 1.11 ]
0.98 [ 0.83 , 1.17 ]0.85 [ 0.65 , 1.10 ]0.73 [ 0.46 , 1.15 ]
T2 = 40%T2 = 70%T2 = 100%
1.16 [ 0.96 , 1.39 ]0.88 [ 0.77 , 1.01 ]0.67 [ 0.53 , 0.85 ]
%AA = 5%%AA = 25%%AA = 45%
Author(s) and Year Log Hazard Ratio [95% CI]
RE Model
0.05 0.25 1.00 4.00 20.00
Zaorsky,2011Soto ,2006Shippy ,2007Sharma,2006Oh ,2015Moyad,2006Kollmeier,2009Gutt,2010Cuaron,2015Chao ,2013
0.63 [ 0.49 , 0.81 ]1.10 [ 0.80 , 1.51 ]0.63 [ 0.42 , 0.95 ]0.96 [ 0.66 , 1.39 ]0.29 [ 0.09 , 0.96 ]1.50 [ 0.33 , 6.82 ]0.69 [ 0.50 , 0.95 ]0.57 [ 0.39 , 0.83 ]1.12 [ 0.65 , 1.94 ]0.99 [ 0.70 , 1.40 ]
0.79 [ 0.65 , 0.95 ]
0.51 [ 0.29 , 0.92 ]
0.91 [ 0.67 , 1.24 ]
1.62 [ 0.97 , 2.70 ]
60 Years
65 Years
70 Years
Author(s) and Year Hazard Ratio [95% CI]
0.26 [ 0.10 , 0.68 ]
0.55 [ 0.32 , 0.93 ]
1.15 [ 0.75 , 1.75 ]
GS 7; 15%
GS 7; 50%
GS 7; 85%
Factors Predicting of BCR: Radical Prostatectomy Factors Predicting of BCR: Radiation Therapy
Figure 3. Meta-regression forest plot with polygons for significant predictors of biochemical recurrence (BCR) among men with prostatecancer treated with (a) radical prostatectomy and (b) radiation therapy.
Table 2. Multivariable meta-regression for biochemical recurrence
Covariates Coefficient (beta) 95% CI P-value
Model 1: Subgroup—radical prostatectomy⩾ T2 stage − 0.006 (−0.012, − 0.004) 0.037African-American − 0014 (−0.023, − 0.004) 0.015Constant 0.22 (0.086, 0.517) 0.147
Tau2= 0; I2 residuals= 57.95%; adjusted R2= 100%
Model 2: Subgroup—radiation therapyYear of publication − 0.0509 0.120PSA level − 0.257 (−0.120, 0.019) 0.118GS⩾7 0.0214 (0.007, 0.354) 0.012Age 0.111 (0.017, 0.204) 0.029Constant 95.426 (−44.17, 235.0) 0.139
Tau2= 0; I2 residuals= 0%; adjusted R2= 100%
Abbreviations: CI, confidence interval; GS, Gleason score. The results arebased on 15 and 10 studies examining the association between statin useand biochemical recurrence among men treated with radical prostatect-omy and radiation therapy, respectively.
Statin use among men with prostate cancerAD Raval et al
7
© 2016 Macmillan Publishers Limited Prostate Cancer and Prostatic Diseases (2016), 1 – 12
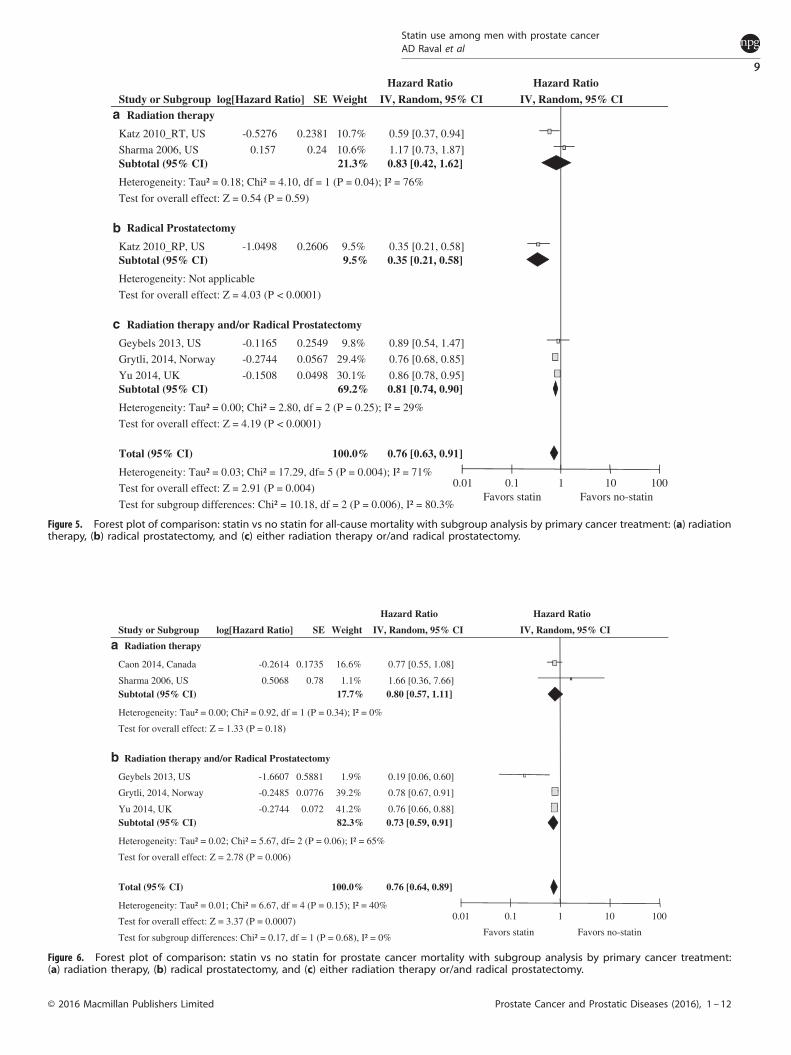
all-cause mortality in the pooled analysis (pHR: 0.76; 95% CI: 0.63,0.91; P-value = 0.004; I2 = 71%) with significant heterogeneity(See Figure 5). To find the cause of heterogeneity, leave one outsensitivity analysis and found the effect estimate of Katz et al23
following RP (HR: 0.35) was responsible for the heterogeneity, asrest of the studies included patients following radiotherapy.Following removal of this estimate from the analysis, statin usewas still significant in reducing the all-cause mortality (pHR: 0.82;95% CI: 0.72, 0.92; P-value = 0.001; I2 = 42%) without considerableheterogeneity. We did not find publication bias based on Egger’stest or trim and fill analysis.
Statin and prostate cancer-related mortalityFive studies evaluated statin use and prostate cancer-relatedmortality as an outcome.22,39,52–54 Statin use significantly reducedthe hazard of prostate cancer-related mortality (pHR: 0.76; 95% CI:0.64, 0.89; P-value = 0.0007; I2 = 40%) without significant hetero-geneity (see Figure 6). We did not find publication bias based onEgger’s test or trim and fill analysis.
Subgroup analysis by non-metastatic prostate cancerAdditionally, we also performed the subgroup analysis toexamine the association between statin use and BCR, metastases,all-cause mortality, and prostate cancer-related mortality (seeFigure 7 for details) among men with non-metastatic or loca-lized prostate cancer. Statin use was not significantly associatedwith BCR reduction (pHR: 0.98, 95% CI: 0.85, 1.14, P-value = 0.83, 10studies, I2 = 53%), whereas it was significantly associated with areduction in the risk of metastasis (pHR: 0.77, 95% CI: 0.68, 0.87,P-valueo0.001, I2 = 0%), all-cause mortality (pHR: 0.86, 95%
CI: 0.78, 0.95, P-valueo0.01, I2 = 0%) and prostate cancer-relatedmortality (pHR: 0.68, 95% CI: 0.48, 0.97, P-value = 0.04, I2 = 64%)among men with non-metastatic prostate cancer.
DISCUSSIONThis review aimed to generate evidence on the associationbetween statin use and clinical outcomes among men withprostate cancer. We found 34 observational studies and norandomized controlled trials. We found that statin use wasassociated with significant reduction in the risk of metastases,all-cause mortality, and prostate cancer-specific mortality overall.Additionally, we explored whether the association between statinuse and clinical outcomes varied by the types of prostate cancertherapy. As the selection of initial cancer therapy of either RP or RTdepends of certain subtypes of prostate cancer, the subgroupanalyses by types of prostate cancer treatment yield homogenouspopulation of men with prostate cancer. Despite four studieswhich reported the beneficial association of statin on BCR amongthose treated with RP, overall estimates suggested non-significantassociation with an evidence of heterogeneity. Although meta-regression revealed that African-American race was one of the keyfactors for BCR, heterogeneity in the pooled estimates stillremained the same. These findings suggest that there could besignificant differences in the included studies on those treatedwith RP. Furthermore, among those treated with RT, statins wasassociated with significant reduction in the hazard of BCR withevidence of high heterogeneity, which was explained asdifference in characteristics such Gleason score and age in themeta-regression results.
Study or SubgroupRadiation therapy
Chao 2013, US
Cuaron 2015, US
Kollmeier 2009, US
Sharma 2006, USSubtotal (95% CI)
Heterogeneity: Tau² = 0.00; Chi² = 2.30, df = 3 (P = 0.51); I² = 0%
Test for overall effect: Z = 0.78 (P = 0.44)
Radical Prostatectomy
Mondul 2011, USSubtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 0.40 (P = 0.69)
Radiation therapy and/or Radical Prostatectomy
Yu 2014, UKSubtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 4.12 (P < 0.0001)
Total (95% CI)
Heterogeneity: Tau² = 0.00; Chi² = 2.82, df = 5 (P = 0.73); I² = 0%
Test for overall effect: Z = 4.15 (P < 0.0001)
Test for subgroup differences: Chi² = 0.52, df = 2 (P = 0.77), I² = 0%
log[Hazard Ratio]
-0.462
-0.5192
0.0862
-0.1393
-0.1625
-0.2614
SE
0.3618
0.5009
0.2333
0.523
0.4108
0.0634
Weight
2.6%
1.4%
6.4%
1.3%11.7%
2.1%2.1%
86.3%86.3%
100.0%
IV, Random, 95% CI
0.63 [0.31, 1.28]
0.59 [0.22, 1.59]
1.09 [0.69, 1.72]
0.87 [0.31, 2.42]0.87 [0.62, 1.23]
0.85 [0.38, 1.90]0.85 [0.38, 1.90]
0.77 [0.68, 0.87]0.77 [0.68, 0.87]
0.78 [0.70, 0.88]
Hazard Ratio Hazard Ratio
IV, Random, 95% CI
0.01 0.1 1 10 100Favors statin Favors no-statin
Figure 4. Forest plot of comparison: statin vs no statin for metastases with subgroup analysis by primary cancer treatment: (a) radiationtherapy, (b) radical prostatectomy, and (c) either radiation therapy or/and radical prostatectomy.
Statin use among men with prostate cancerAD Raval et al
8
Prostate Cancer and Prostatic Diseases (2016), 1 – 12 © 2016 Macmillan Publishers Limited
Study or SubgroupRadiation therapy
Katz 2010_RT, US
Sharma 2006, USSubtotal (95% CI)
Heterogeneity: Tau² = 0.18; Chi² = 4.10, df = 1 (P = 0.04); I² = 76%
Test for overall effect: Z = 0.54 (P = 0.59)
Radical Prostatectomy
Katz 2010_RP, USSubtotal (95% CI)
Heterogeneity: Not applicable
Test for overall effect: Z = 4.03 (P < 0.0001)
Radiation therapy and/or Radical Prostatectomy
Geybels 2013, US
Grytli, 2014, Norway
Yu 2014, UKSubtotal (95% CI)
Heterogeneity: Tau² = 0.00; Chi² = 2.80, df = 2 (P = 0.25); I² = 29%
Test for overall effect: Z = 4.19 (P < 0.0001)
Total (95% CI)
Heterogeneity: Tau² = 0.03; Chi² = 17.29, df= 5 (P = 0.004); I² = 71%
Test for overall effect: Z = 2.91 (P = 0.004)
Test for subgroup differences: Chi² = 10.18, df = 2 (P = 0.006), I² = 80.3%
log[Hazard Ratio]
-0.5276
0.157
-1.0498
-0.1165
-0.2744
-0.1508
SE
0.2381
0.24
0.2606
0.2549
0.0567
0.0498
Weight
10.7%
10.6%21.3%
9.5%9.5%
9.8%
29.4%
30.1%69.2%
100.0%
IV, Random, 95% CI
0.59 [0.37, 0.94]
1.17 [0.73, 1.87]0.83 [0.42, 1.62]
0.35 [0.21, 0.58]0.35 [0.21, 0.58]
0.89 [0.54, 1.47]
0.76 [0.68, 0.85]
0.86 [0.78, 0.95]0.81 [0.74, 0.90]
0.76 [0.63, 0.91]
Hazard Ratio Hazard Ratio
IV, Random, 95% CI
0.01 0.1 1 10 100Favors statin Favors no-statin
Figure 5. Forest plot of comparison: statin vs no statin for all-cause mortality with subgroup analysis by primary cancer treatment: (a) radiationtherapy, (b) radical prostatectomy, and (c) either radiation therapy or/and radical prostatectomy.
Study or Subgroup
Radiation therapy
Caon 2014, Canada
Sharma 2006, USSubtotal (95% CI)
Heterogeneity: Tau² = 0.00; Chi² = 0.92, df = 1 (P = 0.34); I² = 0%
Test for overall effect: Z = 1.33 (P = 0.18)
Radiation therapy and/or Radical Prostatectomy
Geybels 2013, US
Grytli, 2014, Norway
Yu 2014, UKSubtotal (95% CI)
Heterogeneity: Tau² = 0.02; Chi² = 5.67, df= 2 (P = 0.06); I² = 65%
Test for overall effect: Z = 2.78 (P = 0.006)
Total (95% CI)
Heterogeneity: Tau² = 0.01; Chi² = 6.67, df = 4 (P = 0.15); I² = 40%
Test for overall effect: Z = 3.37 (P = 0.0007)
Test for subgroup differences: Chi² = 0.17, df = 1 (P = 0.68), I² = 0%
log[Hazard Ratio]
-0.2614
0.5068
-1.6607
-0.2485
-0.2744
SE
0.1735
0.78
0.5881
0.0776
0.072
Weight
16.6%
1.1%17.7%
1.9%
39.2%
41.2%82.3%
100.0%
IV, Random, 95% CI
0.77 [0.55, 1.08]
1.66 [0.36, 7.66]0.80 [0.57, 1.11]
0.19 [0.06, 0.60]
0.78 [0.67, 0.91]
0.76 [0.66, 0.88]0.73 [0.59, 0.91]
0.76 [0.64, 0.89]
Hazard Ratio Hazard Ratio
IV, Random, 95% CI
0.01 0.1 1 10 100
Favors statin Favors no-statin
Figure 6. Forest plot of comparison: statin vs no statin for prostate cancer mortality with subgroup analysis by primary cancer treatment:(a) radiation therapy, (b) radical prostatectomy, and (c) either radiation therapy or/and radical prostatectomy.
Statin use among men with prostate cancerAD Raval et al
9
© 2016 Macmillan Publishers Limited Prostate Cancer and Prostatic Diseases (2016), 1 – 12

Collectively, our study findings on statin use and BCR in prostatecancer could be explained by the study population-specificeffect and additive effects of statins. First, the use of RP is thepreferred treatment option for men with localized prostate cancer,which has been considered a slow-progressive stage. Previousmeta-analyses also suspected the similar reasons. Our subgroupanalyses by stage of cancer confirmed that statin use was notassociated with BCR among those with localized prostate cancer.The use of RT alone or along with hormone therapy is thepreferred treatment option for those with locally advanced ormetastatic stage of prostate cancer. In our review, we also
observed that, among those receiving RT, a greater proportion ofmen had high NCCN risk categories or D’Amico Risk score ascompared with those with RP at baseline. Therefore, statins mayhave role in the prevention of BCR in men with aggressive cancer,such as locally advanced cancer as compared with localizedprostate cancer. In addition, statins may augment the effect ofRT on cancer cells owing to its radiation-sensitizing properties.56
Our findings confirm the previous findings and explained theuncertainties remained in the previous two meta-analyses12,30
with additional 21 studies since publications of those meta-analyses.
Study or Subgroup
Biochemical recurrence
Chao 2013, US
Chao 2013a, US
Cuaron 2015, US
Geybels 2013, US
Kontraros 2013
Mass 2012, US
Mondul 2011, US
Rieken 2013
Soto 2006, US
Zaorsky 2011, USSubtotal (95% CI)
Heterogeneity: Tau² = 0.03; Chi² = 18.99, df = 9 (P = 0.03); I² = 53%
Test for overall effect: Z = 0.21 (P = 0.83)
Metastasis
Cuaron 2015, US
Mondul 2011, US
Yu 2014, UKSubtotal (95% CI)
Heterogeneity: Tau² = 0.00; Chi² = 0.32, df = 2 (P = 0.85); I² = 0%
Test for overall effect: Z = 4.23 (P < 0.0001)
All-cause mortality
Geybels 2013, US
Yu 2014, UKSubtotal (95% CI)
Heterogeneity: Tau² = 0.00; Chi² = 0.02, df = 1 (P = 0.89); I² = 0%
Test for overall effect: Z = 3.06 (P = 0.002)
Prostate cancer specific mortality
Caon 2014, Canada
Geybels 2013, US
Yu 2014, UKSubtotal (95% CI)
Heterogeneity: Tau² = 0.06; Chi² = 5.51, df = 2 (P = 0.06); I² = 64%
Test for overall effect: Z = 2.11 (P = 0.04)
log[Hazard Ratio]
-0.0101
0
0.1133
0.0583
0.4121
0.1398
-0.0101
-0.1278
0.0953
-0.462
-0.5192
-0.1625
-0.2614
-0.1165
-0.1508
-0.2614
-1.6607
-0.2744
SE
0.1769
0.1676
0.28
0.1834
0.2103
0.1726
0.2226
0.0748
0.1625
0.1282
0.5009
0.4108
0.0634
0.2549
0.0498
0.1735
0.5881
0.072
Weight
9.6%
10.2%
5.3%
9.2%
7.9%
9.9%
7.3%
17.2%
10.5%
12.9%100.0%
1.5%
2.3%
96.2%100.0%
3.7%
96.3%100.0%
38.2%
8.2%
53.5%100.0%
IV, Random, 95% CI
0.99 [0.70, 1.40]
1.00 [0.72, 1.39]
1.12 [0.65, 1.94]
1.06 [0.74, 1.52]
1.51 [1.00, 2.28]
1.15 [0.82, 1.61]
0.99 [0.64, 1.53]
0.88 [0.76, 1.02]
1.10 [0.80, 1.51]
0.63 [0.49, 0.81]0.98 [0.85, 1.14]
0.59 [0.22, 1.59]
0.85 [0.38, 1.90]
0.77 [0.68, 0.87]0.77 [0.68, 0.87]
0.89 [0.54, 1.47]
0.86 [0.78, 0.95]0.86 [0.78, 0.95]
0.77 [0.55, 1.08]
0.19 [0.06, 0.60]
0.76 [0.66, 0.88]0.68 [0.48, 0.97]
Hazard Ratio Hazard Ratio
IV, Random, 95% CI
0.2 0.5 1 2 5Favors statin Favors no-statin
Figure 7. Forest plot of comparison: statin vs no statin for (a) biochemical recurrence, (b) metastases, (c) all-cause mortality and (d) prostatecancer-specific mortality among those with non-metastatic prostate cancer.
Statin use among men with prostate cancerAD Raval et al
10
Prostate Cancer and Prostatic Diseases (2016), 1 – 12 © 2016 Macmillan Publishers Limited

Additionally, we found a beneficial association between statinuse and metastases and all-cause and prostate cancer-specificmortality among men with prostate cancer in the pooled analysiswith no heterogeneity among the included studies even amongthose with non-metastatic prostate cancer. Although prostatecancer is the second leading cause of cancer death in the UnitedStates,57 only 16% of men with prostate cancer died owing toprostate cancer, while others died owing to non-cancer-relatedconditions. Cardiovascular disease is one of the major reasons ofdeaths among men with prostate cancer.58 Statins have shownbeneficial effects of reduction in the risk of cardiovascularevents.59 Our systematic review found the potential of statins inthe reduction in prostate cancer-related mortality, thereforestatins could serve as a therapeutic agent among men withprostate cancer.However, the findings should be carefully interpreted in the
light of limitations of meta-analytical techniques. First, there maybe potential bias of statin use by indication, that is, a greaterproportion of men receiving statins had preexisting cardiovasculardiabetes and/or diabetes. Therefore, studies examining the role ofstatins in the prostate cancer outcomes often have a different setof characteristics as compared with those with prostate cancerand not having diabetes and/or cardiovascular diseases. Second,there would be potential misclassification bias as some of thestudies included the use of the banned and potentially harmfulcerivastatin to define statin use. The inclusion of statins may havea negative impact on the clinical outcomes. Third, the timing ofstatin use among included studies varied in the included studies.Additionally, a very few of the included studies examined theduration and dose of statins. The differences in the time, dose andduration of statins among included studies could be a potentialreason for the heterogeneity in the pooled study estimates. Inaddition, none of the studies rationalized the timing of initiatingstatin therapy among those with prostate cancer. Often men withprostate cancer had a change in the adherence to non-cancermedications as evident from the real-world studies.60 Timing andduration of statin use could be considered as potentialconfounders while examining the relationship between statinuse and clinical outcomes in men with prostate cancer.Strengths and limitations of our study findings suggest a scope
for future clinical trials to examine the effects of statins amongmen with advanced stage or grade of prostate cancer treated withRT. As statins are relatively cheaper as compared with newer-generation chemotherapy (ranged from $14 839 to $93 000),61
finding beneficial effects of statins will provide a cost-effectivesolution to manage prostate cancer. In addition, the futureobservational studies should have robust measures to control fortreatment selection bias, such as use of inverse-probabilityweighting, propensity-score matching or instrumental variableanalysis techniques.62
CONCLUSIONSWe believe ours is the most comprehensive systematic review tofind that statin significantly reduced the all-cause and prostatecancer-specific mortality and improved BCR in certain subgroup ofmen with prostate cancer. In future, randomized controlled trialsshould be conducted to establish efficacy of statins among menwith prostate cancer.
CONFLICT OF INTERESTThe authors declare no conflict of interest.
REFERENCES1 Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C et al. GLOBOCAN
2012 v1.0. Cancer Incidence and Mortality Worldwide: IARC Cancer Base No. 11.
International Agency for Research on Cancer: Lyon, France, 2013. Available from:http://globocan.iarc.fr (accessed on 13 June 2015).
2 Paller CJ, Antonarakis ES. Management of biochemically recurrent prostate cancerafter local therapy: evolving standards of care and new directions. Clin AdvHematol Oncol 2013; 11: 14–23.
3 Roehl KA, Han M, Ramos CG, Antenor JA, Catalona WJ. Cancer progression andsurvival rates following anatomical radical retropubic prostatectomy in 3478consecutive patients: long-term results. J Urol 2004; 172: 910–914.
4 Freedland SJ, Humphreys EB, Mangold LA, Eisenberger M, Dorey FJ, Walsh PCet al. Risk of prostate cancer-specific mortality following biochemical recurrenceafter radical prostatectomy. JAMA 2005; 294: 433–439.
5 Kupelian PA, Mahadevan A, Reddy CA, Reuther AM, Klein EA. Use of differentdefinitions of biochemical failure after external beam radiotherapy changes con-clusions about relative treatment efficacy for localized prostate cancer. Urology2006; 68: 593–598.
6 Taylor F, Huffman MD, Macedo AF, Moore TH, Burke M, Davey Smith G et al.Statins for the primary prevention of cardiovascular disease. Cochrane DatabaseSyst Rev 2013; 1: CD004816.
7 Papadopoulos G, Delakas D, Nakopoulou L, Kassimatis T. Statins and prostatecancer: molecular and clinical aspects. Eur J Cancer 2011; 47: 819–830.
8 Munoz-Pinedo C, El Mjiyad N, Ricci JE. Cancer metabolism: current perspectivesand future directions. Cell Death Dis 2012; 3: e248.
9 Zhuang L, Kim J, Adam RM, Solomon KR, Freeman MR. Cholesterol targeting alterslipid raft composition and cell survival in prostate cancer cells and xenografts.J Clin Invest 2005; 115: 959–968.
10 Cho KJ, Hill MM, Chigurupati S, Du G, Parton RG, Hancock JF. Therapeutic levels ofthe hydroxmethylglutaryl-coenzyme A reductase inhibitor lovastatin activate rassignaling via phospholipase D2. Mol Cell Biol 2011; 31: 1110–1120.
11 Brown M, Hart C, Tawadros T, Ramani V, Sangar V, Lau M et al. The differentialeffects of statins on the metastatic behaviour of prostate cancer. Br J Cancer 2012;106: 1689–1696.
12 Park HS, Schoenfeld JD, Mailhot RB, Shive M, Hartman RI, Ogembo R et al. Statinsand prostate cancer recurrence following radical prostatectomy or radiotherapy: asystematic review and meta-analysis. Ann Oncol 2013; 24: 1427–1434.
13 Scosyrev E, Tobis S, Donsky H, Wu G, Joseph J, Rashid H et al. Statin use and therisk of biochemical recurrence of prostate cancer after definitive local therapy: ameta-analysis of eight cohort studies. BJU Int 2013; 111 (Pt B): E71–E77.
14 Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematicreviews and meta-analyses: the PRISMA statement. Int J Surg 2009 2014/07; 8:336–341.
15 Higgins JPT, Green S (eds). Cochrane Handbook for Systematic Reviews ofInterventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration,2011. Available from (http://www.cochrane-handbook.org.).
16 Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa Health Research Institute: Ottawa (ON); 1999. Available from(http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp); (accessed on10 October 2015).
17 McPheeters ML, Kripalani S, Peterson NB, Idowu RT, Jerome RN, Potter SA et al.Quality improvement interventions to address health disparities. closing the qualitygap: revisiting the state of the science. Agency for Healthcare Research and Quality:Rockville, MD, USA, 2012. Evidence Report No. 208. (Prepared by the VanderbiltUniversity Evidence-based Practice Center under Contract No. 290-2007-10065.)AHRQ Publication No. 12-E009-EF (http://www.effectivehealthcare.ahrq.gov/reports/final.cfm.).
18 van Houwelingen HC, Arends LR, Stijnen T. Advanced methods in meta-analysis:multivariate approach and meta-regression. Stat Med 2002; 21: 589–624.
19 Harbord RM, Higgins JPT. Meta-regression in Stata. Stata J 2008; 8: 493–519.20 Deeks JJ, Macaskill P, Irwig L. The performance of tests of publication bias and
other sample size effects in systematic reviews of diagnostic test accuracy wasassessed. J Clin Epidemiol 2005; 58: 882–893.
21 Peters JL, Sutton AJ, Jones DR, Abrams KR, Rushton L. Contour-enhanced meta-analysis funnel plots help distinguish publication bias from other causes ofasymmetry. J Clin Epidemiol 2008; 61: 991–996.
22 Geybels MS, Wright JL, Holt SK, Kolb S, Feng Z, Stanford JL. Statin use in relation toprostate cancer outcomes in a population-based patient cohort study. Prostate2013; 73: 1214–1222.
23 Katz MS, Carroll PR, Cowan JE, Chan JM, D'Amico AV. Association of statin andnonsteroidal anti-inflammatory drug use with prostate cancer outcomes: resultsfrom CaPSURE. BJU Int 2010; 106: 627–632.
24 Macleod LC, Chery LJ, Hu EYC, Lin DW, Zeliadt S, Wright JL. Low density lipo-protine (LDL) level but not statin use is associated with recurrence of prostatecancer after primary treatment. J Urol 2013; 189: E141–E142.
25 Hamilton RJ, Banez LL, Aronson WJ, Terris MK, Platz EA, Kane CJ et al. Statinmedication use and the risk of biochemical recurrence after radical
Statin use among men with prostate cancerAD Raval et al
11
© 2016 Macmillan Publishers Limited Prostate Cancer and Prostatic Diseases (2016), 1 – 12
prostatectomy: results from the Shared Equal Access Regional Cancer Hospital(SEARCH) Database. Cancer 2010; 116: 3389–3398.
26 Krane LS, Kaul SA, Stricker HJ, Peabody JO, Menon M, Agarwal PK. Men presentingfor radical prostatectomy on preoperative statin therapy have reduced serumprostate specific antigen. J Urol 2010; 183: 118–124.
27 Rioja J, Pinochet R, Savage CJ, Guillonneau BD, Scardino PT, Eastham JA et al.Impact of statin use on pathologic features in men treated with radical prosta-tectomy. J Urol 2010; 183(4): e51.
28 Ritch CR, Hruby G, Badani KK, Benson MC, McKiernan JM. Effect of statin use onbiochemical outcome following radical prostatectomy. BJU Int 2011; 108: E211–E216.
29 Mondul AM, Han M, Humphreys EB, Meinhold CL, Walsh PC, Platz EA. Associationof statin use with pathological tumor characteristics and prostate cancer recur-rence after surgery. J Urol 2011; 185: 1268–1273.
30 Mass AY, Agalliu I, Laze J, Lepor H. Preoperative statin therapy is not associatedwith biochemical recurrence after radical prostatectomy: our experience andmeta-analysis. J Urol 2012; 188: 786–791.
31 Chao C, Jacobsen SJ, Xu L, Wallner LP, Porter KR, Williams SG. Use of statins andprostate cancer recurrence among patients treated with radical prostatectomy.BJU Int 2013; 111: 954–962.
32 Chao C, Williams SG, Xu L, Chen J, Wallner LP, Porter KR et al. Statin therapy is notassociated with prostate cancer recurrence among patients who underwentradiation therapy. Cancer Lett 2013; 335: 214–218.
33 Allott EH, Howard LE, Cooperberg MR, Kane CJ, Aronson WJ, Terris MK et al.Postoperative statin use and risk of biochemical recurrence following radicalprostatectomy: results from the Shared Equal Access Regional Cancer Hospital(SEARCH) database. BJU Int 2014; 114: 661–666.
34 Ishak-Howard MB, Okoth LA, Cooney KA. Statin use and the risk of recurrenceafter radical prostatectomy in a cohort of men with inherited and/or early-onsetforms of prostate cancer. Urology 2014; 83: 1356–1361.
35 Danzig MR, Kotamarti S, Ghandour RA, Rothberg MB, Dubow BP, Benson MC et al.Synergism between metformin and statins in modifying the risk of biochemicalrecurrence following radical prostatectomy in men with diabetes. Prostate CancerProstatic Dis 2015; 18: 63–68.
36 Katz MO, Zelefsky MJ, Marion C, Yamada Y, Kattan MW, Leibel SA. Statin use isassociated with improved biochemical outcome after high-dose radiotherapy forclinically localized prostate cancer. Int J Radiat Oncol Biol Phys 2003; 57: S271.
37 Moyad MA, Merrick GS, Butler WM, Wallner KE, Galbreath RW, Butler EG et al.Statins, especially atorvastatin, may improve survival following brachytherapy forclinically localized prostate cancer. Urol Nurs 2006; 26: 298–303.
38 Moyad MA, Merrick GS, Butler WM, Wallner KE, Galbreath RW, Kurko B et al.Statins, especially atorvastatin, may favorably influence clinical presentation andbiochemical progression-free survival after brachytherapy for clinically localizedprostate cancer. Urology 2005; 66: 1150–1154.
39 Sharma NK, Ruth K, Horwitz E, Buyyounouski M, Pollack A. Statin use prior toradiation therapy for prostate cancer does not improve outcome: the Fox Chaseexperience. Int J Radiat Oncol Biol Phys 2006; 66: S366.
40 Soto DE, Daignault S, Sandler HM, Ray ME. No effect of statins on biochemicaloutcomes after radiotherapy for localized prostate cancer. Urology 2009; 73:158–162.
41 Shippy AM, Katz MS, Yamada Y, Feder DJ, Zelefsky MJ. Statin use and clinicaloutcomes after high dose radiotherapy for prostate cancer. Int J Radiat Oncol BiolPhys 2007; 69: S113.
42 Kollmeier MA, Katz MS, Mak K, Yamada Y, Feder DJ, Zhang Z et al. Improvedbiochemical outcomes with statin use in patients with high-risk localized prostatecancer treated with radiotherapy. Int J Radiat Oncol Biol Phys 2011; 79: 713–718.
43 Gutt R, Tonlaar N, Kunnavakkam R, Karrison T, Weichselbaum RR, Liauw SL. Statinuse and risk of prostate cancer recurrence in men treated with radiation therapy.J Clin Oncol 2010; 28: 2653–2659.
44 Cuaron J, Pei X, Cohen GN, Cox BW, Yamada Y, Zelefsky MJ et al. Statin use notassociated with improved outcomes in patients treated with brachytherapy forprostate cancer. Brachytherapy 2015; 14: 179–184.
45 Oh DS, Koontz B, Freedland SJ, Gerber L, Patel P, Lewis S et al. Statin use isassociated with decreased prostate cancer recurrence in men treated withbrachytherapy. World J Urol 2015; 33: 93–97.
46 Zaorsky NG, Buyyounouski MK, Li T, Horwitz EM. Aspirin and statin nonuseassociated with early biochemical failure after prostate radiation therapy. Int JRadiat Oncol Biol Phys 2012; 84: e13–e17.
47 Cattarino S, Seisen T, Drouin SJ, Renard-Penna R, Leon P, Comperat E et al.Influence of statin use on clinicopathological characteristics of localized prostatecancer and outcomes obtained after radical prostatectomy: a single center study.Can J Urol 2015; 22: 7703–7708.
48 Misrai V, Do C, Lhez JM, Elman B, Latorzeff I, Portalez D et al. Is statin useassociated with D'Amico risk groups and biochemical recurrence after radicalprostatectomy? Prog Urol 2012; 22: 273–278.
49 Ku JH, Jeong CW, Park YH, Cho MC, Kwak C, Kim HH. Relationship of statins toclinical presentation and biochemical outcomes after radical prostatectomy inKorean patients. Prostate Cancer Prostatic Dis 2011; 14: 63–68.
50 Song C, Park S, Park J, Shim M, Kim A, Jeong IG et al. Statin use after radicalprostatectomy reduces biochemical recurrence in men with prostate cancer.Prostate 2015; 75: 211–217.
51 Kontraros M, Varkarakis I, Ntoumas K, Deliveliotis C. Pathological characteristics,biochemical recurrence and functional outcome in radical prostatectomy patientson statin therapy. Urol Int 2013; 90: 263–269.
52 Yu O, Eberg M, Benayoun S, Aprikian A, Batist G, Suissa S et al. Use of statins andthe risk of death in patients with prostate cancer. J Clin Oncol 2014; 32: 5–11.
53 Caon J, Paquette M, Hamm J, Pickles T. Does statin or ASA affect survival whenprostate cancer is treated with external beam radiation therapy? Prostate Cancer2014; 2014: 184297.
54 Grytli HH, Fagerland MW, Fossa SD, Tasken KA. Association between use of beta-blockers and prostate cancer-specific survival: a cohort study of 3561 prostatecancer patients with high-risk or metastatic disease. Eur Urol 2014; 65: 635–641.
55 Rieken M, Kluth LA, Xylinas E, Seitz C, Fajkovic H, Karakiewicz PI et al. Impact ofstatin use on biochemical recurrence in patients treated with radical prosta-tectomy. Prostate Cancer Prostatic Dis 2013; 16: 367–371.
56 Liauw SL, Connell PP, Weichselbaum RR. New paradigms and future challenges inradiation oncology: an update of biological targets and technology. Sci Transl Med2013; 5: 173sr2.
57 American Cancer Society. Cancer Facts & Figures 2015. American Cancer Society:Atlanta, GA, USA, 2015.
58 Epstein MM, Edgren G, Rider JR, Mucci LA, Adami HO. Temporal trends in cause ofdeath among Swedish and US men with prostate cancer. J Natl Cancer Inst 2012;104: 1335–1342.
59 Taylor F, Huffman MD, Macedo AF, Moore THM, Burke M, Davey Smith G et al.Statins for the primary prevention of cardiovascular disease. Cochrane Database ofSystematic Reviews 2013, Issue 1. Art. No.: CD004816. DOI: 10.1002/14651858.CD004816.pub5.
60 Stuart BC, Davidoff AJ, Erten MZ. Changes in medication management after adiagnosis of cancer among medicare beneficiaries with diabetes. J Oncol Pract2015; 11: 429–434.
61 Chustecka Z. Comparing costs of new drugs in prostate cancer [Internet]. 2015.Available from: http://www.medscape.com/viewarticle/779717.
62 Jacob BJ, Sutradhar R, Moineddin R, Baxter NN, Urbach DR. Methodologicalapproaches to population based research of screening procedures in the presenceof selection bias and exposure measurement error: colonoscopy and colorectalcancer outcomes in Ontario. BMC Med Res Methodol 2013; 13: 59,2288–13-59.
Supplementary Information accompanies the paper on the Prostate Cancer and Prostatic Diseases website (http://www.nature.com/pcan)
Statin use among men with prostate cancerAD Raval et al
12
Prostate Cancer and Prostatic Diseases (2016), 1 – 12 © 2016 Macmillan Publishers Limited





























