Embed Size (px)
Citation preview

Association Between Early Follow-up with a Nephrologist
and Death in Survivors of Acute Kidney Injury
By
Ziv Harel
A thesis submitted in conformity with the requirements
for the degree of Master’s of Science
Graduate Department of Health Policy Management and Evaluation
University of Toronto
© Copyright by Ziv Harel 2012

ii
Association Between Early Follow-up with a Nephrologist and
Death in Survivors of Acute Kidney Injury
Ziv Harel
Master’s of Science
Department of Health Policy, Management and Evaluation
University of Toronto
2012
Abstract
Background: Survivors of severe acute kidney injury remain at high risk of death well-after
apparent recovery from the initial event.
Methods: We conducted a cohort study of hospitalized adults in Ontario from 1996 to 2008 with
acute kidney injury who received temporary dialysis and survived for 90 days following
discharge independent from dialysis. The exposure was nephrology follow-up. We used
propensity scores to match individuals with early nephrology follow-up to those without. The
primary outcome was time to mortality.
Results : We identified 3877 patients with acute kidney injury who met the eligibility criteria. A
total of 1583 patients had nephrology follow. The incidence of all-cause mortality was lower in
those with early nephrology follow-up as compared to those without early follow-up (8.4 vs. 10.6
per 100 person-years, HR 0.76 (95% CI 0.62-0.93)).
Conclusions: Nephrology follow-up after hospitalization with acute kidney injury and temporary
dialysis was associated with improved survival.

iii
Acknowledgments
I am extremely grateful to my primary supervisor Ed Etchells, and my co-supervisors Chaim Bell
and Ron Wald for their continued guidance, inspiration, and encouragement through this process.
Their mentorship, intelligence, enthusiasm and friendship made this a truly enjoyable experience.
I would also like to thank my committee members Muhammad Mamdani and Joanne Bargman,
as well as Amit Garg, Tara Gomes, Rob Quinn, Peter Austin and Donald Redelmeier for the
knowledge and expertise they shared with me during these 2 years.
This work was supported by a Canadian Institute of Health Research Master’s Award as
well as by the Clinician Scientist Program at the University of Toronto. The funding, and
educational components provided by these programs were invaluable in allowing me to complete
this work.
Finally, I would like to profoundly thank my family for their support and encouragement
not only throughout this Master’s but my entire academic career. I would not be where I am
without them.

iv
Table of Contents
Abstract ii
Acknowledgments iii
List of Tables vi
List of Figures vii
List of Appendices viii
Introduction 1.1 Study Rationale and Study Question 1
1.2 Hypothesis 1
Background
2.1. Epidemiology of Acute Kidney Injury (AKI) 2.1.1. Definition and Classification of Acute Kidney Injury 2
2.1.2. Prevalence of AKI in Hospitalized Patients 4
2.1.3. Short-term Outcomes of AKI 4
2.1.4. Methodological Issues in Studying the Long-term Outcomes of AKI 5
2.1.5. Long-term Outcomes of AKI 7
2.2. Pathophysiology of Acute Kidney Injury
2.2.1. Renal and Non-Renal Effects of AKI and their Relationship with Mortality 12
2.3 Potential Impact of Nephrologist Follow-up After Hospitalization with Severe AKI 14
Methods 3.1 Overview of Study Design 16
3.2 Description of Data Sources and Validity
3.2.1. Canadian Institute for Health Information Discharge Abstract Database 17
3.2.2. Ontario Health Insurance Premium Database 18
3.2.3. Registered Persons Databases 18
3.2.4. Canadian Organ Replacement Registry 18
3.2.5. Canadian Census Database 19
3.2.6. Ottawa Warehouse Database 19
3.2.7. CERNER Database 19
3.3 Cohort Definition
3.3.1. Inclusion criteria 20
3.3.2. Exclusion criteria 20
3.3.3. Justification of Cohort Selection (Inclusion and Exclusion Category) 22
3.4 Covariates and Outcome Variables
3.4.1. Primary Exposure: Nephrologist Consultation Within 90 Days of Discharge 23
3.4.2. Primary Outcome: All-Cause Mortality 25
3.4.3. Secondary Outcome: Receipt of Chronic Dialysis 25
3.5 Statistical Methods
3.5.1 Propensity Score Modelling 25
3.5.1.1. Specifying the Propensity Score 26
3.5.1.2. Matching on the Propensity Score 26
3.5.1.3. Assessing Balance Between Treated and Untreated Subjects 27
3.5.1.4. Estimation of the Treatment Effect 27
3.6 Subgroup Analysis 28
3.7 Sensitivity Analyses 28
3.7.1. High Dimensional Propensity Score 29
3.8 Additional Analyses

v
3.8.1. Healthcare Utilization 30
3.8.2. Unmatched Cohort 30
Results 4.1 Description of the Cohort 31
4.2 Outcomes 35
4.3 Subgroups 38
4.4 Sensitivity Analyses
4.4.1. Patients with a Discharge Serum Creatinine Measurement 41
4.4.2. Dialysis Censored Cohort 44
4.4.3. High Dimensional Propensity Score 44
4.4.4. Test of Specificity 45
4.5 Additional Analyses
4.5.1. Healthcare Utilization 46
4.5.2. Unmatched Cohort 47
Discussion 5.1 Major Findings 49
5.2 Interpretation 50
5.3 Strengths 54
5.4 Limitations 55
5.5 Implications and Future Directions 58
Conclusion 59
References 60
Appendices 68

vi
List of Tables
Table 1: The RIFLE criteria for acute kidney injury……………………………….... 3
Table 2: The AKIN criteria for acute kidney injury……………………………….…. 4
Table 3: Comparison of Two Algorithms for Defining Nephrologist………………... 24
Table 4: Baseline Characteristics of Cohort (Pre-Match)………………….……….... 33
Table 5: Baseline Characteristics of Cohort (Post-Match)………………..…………. 34
Table 6: Risk of All-Cause Mortality and Chronic Dialysis by Group ……………… 35
Table 7: Risk of All-Cause Mortality Stratified by Subgroup………………..……..... 39
Table 8: Baseline Characteristics of Patients with Discharge Creatinine
Values………………………………………………………………..…............. 42
Table 9: Characteristics of Patients with Discharge Creatinine Values
Post-Matching......................................................................................................43
Table 10: Additional Covariates Specified by the High Dimensional Propensity
Score……………………………………………………………………….…... 45
Table 11: Risk of All-Cause Mortality and Chronic Dialysis for Tracer Exposure.….46
Table 12: Characteristics of Post-Discharge Health Services Utilization and
Procedures in the Matched Cohort…………………………………………..47
Table 13: Comparison of Matched and Unmatched Cohorts…………………………. 48

vii
List of Figures
Figure 1: Creation of the Acute Kidney Injury Survivor Cohort……………………. 21
Figure 2: Comparison of High Dimensional Versus Traditional Propensity Score
Modeling……………………………………………………………………… 30
Figure 3: Risk of All-Cause Mortality in Association with Early Nephrology
Follow-up…………………………………………………………………....... 36
Figure 4: Risk of Chronic Dialysis in Association with Early Nephrology
Follow-up…………………………………………………………………….. 37
Figure 5: Association of Nephrology Follow-up with All-Cause Mortality
Within Subgroups…………………………………………………………… 40

viii
List of Appendices
Appendix 1: Diagnostic and Procedural Codes Used to Identify the Cohort, Exposure,
Comorbidities, and Outcomes………………………………………………68
Appendix2: Covariates Used in the Development of the Propensity Score……………72

1
Chapter 1
Introduction
The purpose of this chapter is to:
Describe the study rationale and study question.
1.1 Rationale and Study Question
Acute kidney injury (AKI) is an increasingly common and serious complication in hospitalized
patients.1;2
Even after discharge, survivors of hospitalizations that are complicated by AKI are
at higher risk of dying and are more likely to develop progressive chronic kidney disease
(CKD).3-6
These complications may occur even if renal recovery is ostensibly complete at the
time of the initial discharge.7 The first 3 to 24 months following an episode of AKI represent the
time of greatest risk for the long-term complications of AKI.8 As such, specialized nephrology
care during this crucial window of time may prevent poor outcomes. However, only 40% of
patients hospitalized with an episode of AKI see a nephrologist within the first year.9 This may
represent a missed opportunity for intervention.
Despite the theoretical benefits of nephrology follow-up in survivors of AKI, little is
known about the effect that this intervention may have on the long-term complications of AKI.
Accordingly, we undertook a population-based cohort study in Ontario, Canada, to determine
whether early follow-up with a nephrologist in survivors of severe AKI is associated with
reduced mortality and progression to chronic dialysis.
1.2 Hypothesis
It is hypothesized that follow-up with a nephrologist within 90 days of discharge is associated
with a decrease in mortality within 2 years of the index date, and a decrease in the need for
chronic dialysis.

2
Chapter 2
Background
The purpose of this chapter is to:
Review the epidemiology of acute kidney injury;
Describe the pathophysiological effects of acute kidney injury;
Discuss the potential impact of nephrologist follow-up in survivors of acute kidney injury
requiring temporary dialysis.
2.1. Epidemiology of Acute Kidney Injury
2.1.1 Definition and Classification of Acute Kidney Injury
Conceptually, acute kidney injury is defined by an abrupt increase in serum creatinine resulting
from injury or insult that causes a functional or structural change in the kidney. It involves a
spectrum of injury from less severe, which may require only watchful waiting, to more
advanced, often requiring supportive therapy with dialysis.
In the past, multiple definitions for AKI have been used in clinical studies, which has
limited our understanding of the epidemiology for AKI and thereby hindered progress in the
field. In order to address this and to establish a standardized definition of AKI, a
multidisciplinary collaborative network of investigators established the Acute Dialysis Quality
Initiative (ADQI).
This group formulated two definitions for AKI: the RIFLE criteria in 2004 and the Acute
Kidney Injury Network (AKIN) criteria in 2007. (Tables 1 and 2)
The RIFLE criteria represent an acronym for three graded levels of kidney injury: RISK,
INJURY and FAILURE, based upon either the magnitude of elevation in serum creatinine or
decrease in urine output; and two outcomes: LOSS and END STAGE RENAL DISEASE

3
(ESRD). A patient may fulfill the criteria through changes in serum creatinine or glomerular
filtration rate (GFR) or changes in urine output. The RIFLE stages are included in Table 1.
Table1: The RIFLE criteria for acute kidney injury.
RISK – 1.5 fold increase in serum creatinine or GFR decrease by 25% or urine output
<0.5ml/kg per hour for six hours.
INJURY - Twofold increase in serum creatinine or GFR decrease by 50% or urine output
<0.5ml/kg per hour for twelve hours.
FAILURE - Threefold increase in serum creatinine or GFR decrease by 75% or urine
output <0.5ml/kg per hour for twenty four hours or anuria for 12 hours.
LOSS – Complete loss of kidney function for more than four weeks.
ESRD – Complete loss of kidney function for more than three months.
The RIFLE criteria is dependent on a priori knowledge of the patient’s baseline
creatinine. In cases where the baseline creatinine is unknown, the developers of the RIFLE
criteria suggest calculating a theoretical baseline based on the Modification of Diet in Renal
Disease (MDRD) formula. 10
The AKIN criteria is more commonly used in clinical studies.11;12
These criteria stratify
patients into three stages of AKI based on their severity of renal dysfunction: Stage 1, 2, and 3.
These stages are synonymous with the RISK, INJURY AND FAILURE stages of the RIFLE
criteria with slight modifications. Specifically, these modifications include: i) broadening the
RISK category of RIFLE to include an increase in serum creatinine of at least 0.3mg/dL
(26umol/L) even if this doesn’t reach the 50% threshold; ii) setting a 48 hour window on the first
documentation of any criteria; and iii) categorizing patients as FAILURE if they are treated with
renal replacement therapy (RRT) regardless of what their serum creatinine or urine output is at
the point of initiation. Furthermore, the AKIN criteria should only be applied after volume status
has been optimized and urinary tract obstruction has been ruled out if oliguria was used as the

4
sole diagnostic criterion. As with the RIFLE criteria a patient may fulfill the AKIN criteria
through changes in serum creatinine or urine output.
Table 2: The AKIN criteria for acute kidney injury.
Stage Serum creatinine criteria Urine output criteria
I Increase in serum creatinine ≥0.3 mg/dL (26.4
µmol/L) or increase to more than or equal to 150-
200% from baseline
< 0.5ml/kg/hr for > 6 hours
II Increase in serum creatinine greater than 200-
300% from baseline
< 0.5ml/kg/hr for > 12
hours
III Increase in serum creatinine greater than 300%
from baseline or serum creatinine > 4.0 mg/dL
(354 µmol/L) with an acute increase of at least
0.5 mg/dL (44 µmol/L)
<0.3ml/kg/hr for 24 hours
or anuria for 12 hours
2.1.2 Prevalence of Acute Kidney Injury in Hospitalized Patients
Acute kidney injury is one of the most common conditions affecting hospitalized patients. Using
administrative data, Waikar and colleagues showed that it affects up to 15.3% of all hospitalized
patients.13
However, estimates of the incidence of AKI in hospitalized patients vary according
to the clinical setting as well as the definition of this condition.14-18
2.1.3 Short Term Outcomes of Acute Kidney Injury
Regardless of the definition used, AKI has been found to be associated with increased short-term
mortality, length of stay and hospital costs.1;19-22
This was first demonstrated by Chertow and
colleagues who retrospectively studied a cohort of 19 982 patients admitted for various
conditions to an urban academic hospital. They confirmed that an increase in serum creatinine as

5
low as 0.3 mg/dL (26 µmol/L) from baseline was associated with an odds ratio for mortality at
30 days of 4.1 (95% CI 3.1 to 5.5).1 In fact, the greater the deviation from the baseline
creatinine, the higher the odds of mortality. This association has been subsequently confirmed
by others across a spectrum of clinical settings including post-cardiothoracic surgery, post-
contrast injection, sepsis, congestive heart failure, and in the intensive care unit. 23-26
Aside
from an increase in mortality, AKI has also been found to be associated with an extended
hospital length of stay (LOS) and increased hospital costs.1;27;28
Similar to the association found
with 30 day mortality, the severity of renal dysfunction is positively correlated with increasing
LOS.27
The financial impact of AKI has been found to be largely explained by the increased
LOS associated with this condition.1
2.1.4 Methodological Issues in Studying the Long Term Outcomes of Acute Kidney Injury
While the short term hazards of AKI have been well defined, only recently has attention been
paid to the long-term complications of AKI. This trend may partly be explained by four reasons
including: i) the lack of a standardized definition for renal recovery; ii) the short duration, and
single-centre nature of most studies; iii) issues related to the definition of AKI and baseline
creatinine; and iv) potential confounding in studies of AKI.
The lack of a standardized definition of renal recovery has hampered research into the
long-term effects of AKI. Prior to 2005, studies describing the long-term implications of AKI
were heterogeneous in their definition of renal recovery, which limited not only generalizability,
but may have biased results.29-31
The apparent reversibility of AKI as manifest by a diminution of
serum creatinine from its peak was commonly used to define renal recovery in numerous historic
studies. This notion may have propagated the fallacy of complete renal recovery, when in fact
this was not the case as has been demonstrated by recent clinical and basic science studies.
4;8;32Collectively, these recent studies have refuted the belief that recovery of AKI, be it partial or
complete, portends no future adverse consequences. Responding to the issue surrounding the
heterogeneity in defining renal recovery, the Acute Dialysis Quality Initiative (ADQI) published
a consensus definition for renal recovery in 2004.33
Complete renal recovery was defined as the
return of kidney function to pre-ARF baseline levels. Recovery would be defined as partial if a

6
persistent change from baseline remained evident, but not including the continued need for
RRT. The requirement for RRT for more than 4 weeks would be classified as persistent ARF,
whereas those remaining dependent on RRT at 3 months would be defined as having progressed
to ESRD.33
The impact of the standardization of the definition of renal recovery has led to the
design of methodologically sound studies that are increasingly generalizable .
Another issue that has hampered studying the long-term effects of AKI has been the short
follow-up and single centre design of studies. Historically, most studies focusing on the long-
term impact of AKI were less than 6 months.5;34-37
This short follow-up had likely
underestimated the true effect of AKI on long-term outcomes such as progression of renal
disease and mortality as has been demonstrated by more recent studies. Similarly, study
generalizability was also impacted by the single centre design as protocols and procedures may
vary among different centres. Again, more recent works have addressed this issue using
population-based studies from Ontario, Canada and the Veteran’s Health Administration. 3;6
Consensus definitions of AKI (AKIN and/or RIFLE) fail to account for the underlying
cause of the acute renal injury, which may confound the true relationship between AKI and long-
term outcomes. Previous studies of AKI have considered this entity to be a homogeneous
phenomenon, such that disease entities such as prerenal azotemia, acute tubular necrosis (ATN),
and acute interstitial nephritis have been considered to be one and the same.1;38;39
It seems
implausible that an acute rise in serum creatinine due to prerenal azotemia would have the same
long-term renal effect as that due to acute tubular necrosis (ATN) as these entities may impart
different degrees of renal injury which may have dissimilar risks for the development of CKD,
the acceleration of CKD, or mortality.
Defining what constitutes baseline renal function has also hindered quality of care
research on long-term outcomes of AKI. In the renal literature, there is marked heterogeneity in
the definition of baseline creatinine. For example, it has been defined as the lowest serum
creatinine observed during hospitalization, the lowest of the first three inpatient serum
creatinines, or the prehospitalization serum creatinine.1;22;40;41
While the RIFLE criteria uses the
MDRD formula to estimate a baseline serum creatinine in cases where the baseline is unknown,
this too has its limitations as the patient may have had some renal dysfunction prior to the
episode of AKI, which would be unaccounted for by this approach. Researchers have attempted

7
to solve this issue by postulating that outpatient serum creatinines be used to define baseline
values of creatinine.42
While this approach has been used by some, it too may misclassify
individuals. The time lapse between the acute event and the last outpatient serum creatinine may
be excessive thereby being unable to account for interim changes in renal function. Conversely,
using outpatient values too close to the time of hospitalization may lead to the inclusion of an
already impaired serum creatinine due to the acute or subacute process that eventually leads to
hospitalization.
Associated with difficulties in determining baseline renal function is the issue of
confounding. Previous long-term studies of patients with AKI, have been unable to account for
important confounders. This may impact the determination of the relationship between AKI and
subsequent outcomes such as mortality, development of CKD, or progression of CKD as was
demonstrated in a systematic review and metaanalysis by Coca et al.5 Use of methodologically
sound techniques to account for residual confounding, such as propensity scores and matching,
have addressed some of these concerns.
2.1.5 The Epidemiology of Long Term Outcomes of Acute Kidney Injury
The long-term outcomes of AKI have recently been the focus of a number of studies.
Collectively, these have demonstrated that AKI is associated with increased mortality as well as
the progression of renal disease and ESRD.
In 2007, Coca and colleagues summarized the prevailing data on the long-term outcomes
of AKI in a systematic review and meta-analysis.5 The review focused on three outcomes: i) the
risk of mortality; ii) the risk of progression to chronic kidney disease (CKD) or dialysis; and iii)
the risk of cardiovascular events imparted by AKI. Their meta-analysis included 48 studies
which were heterogeneous in their definition of AKI, their duration of study, and their patient
populations. Nonetheless, Coca et al. were able to demonstrate an increased risk of mortality for
survivors of AKI compared to those without AKI [Risk Ratio 2.59; 95% CI 1.99-3.42]. They
also demonstrated a graded increase in risk of long-term mortality with increasing severity of
AKI. In fact, patients with severe AKI (dialysis requiring AKI) had twice the risk of mortality as

8
those with less severe AKI (not requiring dialysis) (RR 3.09; 95% CI 2.20-4.33 [severe]; RR
1.67; 95% CI 1.41-1.98 [mild]). Aside from demonstrating an increased risk for long term
mortality, Coca and colleagues also showed an increased rate of CKD at 7.8 per 100 patient
years in survivors of AKI. Due to methodological constraints imposed by the included studies,
risk ratios were unable to be calculated for the outcomes of progression to CKD as the majority
of studies did not include a comparator group without AKI.
Recent studies have overcome many of the methodological limitations of those included
in Coca’s review. They have demonstrated that AKI is associated with increased mortality and
the progression to CKD and chronic dialysis, even in patients with normal baseline renal
function. Wald and colleagues demonstrated that AKI requiring dialysis is associated with an
increased risk of progression to chronic dialysis.3 They used administrative data to study a
cohort of 3769 adult patients in Ontario, Canada with acute kidney injury who required in-
hospital dialysis and survived free of dialysis for at least 30 days after discharge. Using a
propensity score model, they demonstrated that AKI necessitating in-hospital dialysis was
associated with almost three times greater risk of chronic dialysis [adjusted hazard ratio 3.23;
95% CI 2.70 to 3.86) after a median follow up of 3 years. All-cause mortality was not increased
among patients with AKI [adjusted hazard ratio 0.95; 95% CI 0.89 to 1.02], which may have
been due to the exclusion of 7% of the exposed group with whom an appropriate match could not
be found. The unmatched individuals exhibited a higher mortality rate over time, such that the
inclusion of them in the final analysis may have altered the point estimate towards an increased
risk of all-cause mortality.
Similarly, work by Hsu and colleagues further established the association between
dialysis requiring AKI and poor long-term outcomes.43
They focused on a hospitalized cohort of
patients with underlying CKD (pre-hospitalization eGFR <45ml/min) and found that an episode
of AKI requiring dialysis increased the risk for progression to end stage renal disease (ESRD) or
death by 30% compared to those without AKI (adjusted HR 1.37; 95% CI 1.01-1.86). These
findings are clinically consistent as patients with underlying CKD already possess underlying
kidney damage. Therefore a subsequent renal ―hit‖ or ―insult‖ may unmask and/or accelerate
this injury. Subsequent work has corroborated the finding that CKD modifies the effect of AKI
on mortality and progression to CKD.44

9
While a prior history of CKD may accelerate the progression of CKD, subjects with
relatively normal renal function at baseline have also been found to be at risk of increased
mortality and the development of CKD after an episode of acute kidney injury. This has been
demonstrated by Lo et al. who used administrative data from the Kaiser Permanente Health Care
system to examine the impact of an episode of AKI requiring dialysis on the risk of progression
of renal disease and death among patients who had relatively preserved baseline renal function
(eGFR ≥45ml/min) and did not develop ESRD within 30 days of hospital discharge compared
with a matched control group.44
They demonstrated that patients experiencing AKI had a 28-
fold increased risk for the progression of CKD, which was defined as the development of stage
IV CKD or higher (95% CI 21.1 to 37.6), and an increased risk for death (adjusted HR 2.3; 95%
CI 1.8 to 3.0).
The studies by Wald, Hsu and Lo all focused on patients who developed AKI requiring
dialysis, which is the most severe form of renal injury according to validated criteria such as the
RIFLE and AKIN criteria. Hence, the need for dialysis may be the most important predictor of
not only mortality but the progression or development of subsequent CKD. This notion has been
corroborated by the work of Chawla and colleagues who used Veteran’s Administration (VA)
data to develop and validate a prediction tool for the progression to Stage IV CKD after an
episode of AKI.45
They studied a cohort of patients admitted to the VA who had normal baseline
kidney function (defined as an eGFR >60 ml/min) and developed AKI during their
hospitalization. Among the variables included in their predictive model, the requirement for
dialysis was the strongest predictor for the progression to CKD (adjusted odds ratio 53.18; 95%
CI 11.28-250.64).
Studies have also focused on the impact of less severe AKI on long-term outcomes and
have demonstrated an increased risk of mortality and progression of renal disease among
affected individuals. In their metaanalysis, Coca and colleagues examined the association
between AKI and death stratified by severity of AKI into mild, moderate and severe categories.5
Studies stratified into mild AKI enrolled patients which had a rise in serum creatinine ≥ 25%
from baseline or had a decrease in creatinine clearance ≥ 10% from baseline (3 studies).
Moderate AKI studies enrolled subjects which had a >50% rise in serum creatinine or a
creatinine concentration of > 1.7mg/dL from baseline (6 studies). Severe AKI studies enrolled

10
patients with AKI that required RRT (7 studies). Not surprisingly, Coca et al. demonstrated
that while severe AKI correlates with the greatest risk of mortality, both mild and moderate AKI
also increase the risk for long-term mortality. (mild AKI RR 1.67, 95% CI 1.41-1.98; moderate
AKI RR 2.70, 95% CI 1.77-4.12; severe AKI RR 3.09, 95% CI 2.20-4.33).
Aside from increased mortality, AKI not requiring RRT has been associated with
progression to ESRD, particularly among patients with underlying CKD. This was demonstrated
by Ishani et al. who used a random sample of Medicare beneficiaries.46
They showed that while
both patients with and without CKD had an increased risk of progression to ESRD, the risk was
substantially higher for patients with CKD (non-CKD: aHR 2.38; 95% CI 2.31-2.46; CKD: aHR
13.0; 95% CI 10.6-16.0). Despite demonstrating an important trend, Ishani et al.’s study had a
number of methodological issues particularly stemming from the use of administrative data.
Firstly, their use of administrative data may have misclassified individuals. It is well established
that administrative coding for AKI and CKD is highly specific but poorly sensitive. Therefore,
they may have misclassified some individuals with AKI and CKD as free from these conditions.
Secondly, the data set. did not include creatinine values. This did not allow for the classification
of AKI severity or the stage of CKD. Accounting for baseline CKD stage and severity of AKI
may have important prognostic significance as it is unlikely that an individual with Stage II CKD
and less severe AKI would have the same risk of subsequent poor outcomes as an individual with
Stage IV CKD and more severe AKI.
Building on the work of Ishani, LaFrance and Miller used VA administrative data to
show that patients who developed an episode of AKI while hospitalized and did not require RRT
were at increased risk for long-term mortality compared to control subjects (adjusted HR 1.41,
95% CI 1.39-1.43).6 In contrast to previous studies, they used the AKIN criteria to classify the
severity of AKI and accounted for post-discharge renal function as determined by eGFR.
Adjustment for post-discharge renal function is particularly important as CKD is an important
modifier of mortality.47;48
LaFrance also demonstrated that AKI severity, as classified by the
AKIN criteria, independently associates with a graded rise in the risk of long-term mortality
(AKIN I aHR 1.36, 95% CI 1.34-1.38; AKIN II aHR 1.46; 95% CI 1.42-1.50; AKIN III aHR
1.59; 95% CI 1.54-1.65).

11
It has also been proposed that the type of renal injury may impact long-term outcomes
of AKI. In this regard, patients with fulminant renal injury such as oligoanuric ATN may have
worse outcomes than those with less severe episodes of AKI. While this theory has biological
plausibility, there have been conflicting studies on this association. Amdur and colleagues
demonstrated that US veterans with no history of CKD who were admitted to hospital with AKI
have an increased risk of reaching the combined end-point of Stage 4 CKD, chronic dialysis or
death over a 75 month follow-up period. 49
In fact, patients with a history of ATN had a higher
hazard of this combined endpoint than their counterparts with non-ATN AKI (adjusted HR 6.64
for ATN, 4.03 non-ATN AKI). Interestingly, when studying the risk of mortality alone, there
was an increased risk of death in the non-ATN AKI group but not in the ATN group. This may
be reflective of the small sample size of the ATN group or the inability to adjust for potential
important confounders. However, studies by Chawla et al. and Liano et al. have also failed to
find an association between ATN and subsequent mortality compared to non-ATN AKI.49;50
Such a discrepancy may be a consequence of their use of administrative data to classify AKI, and
more specifically ATN, as previously discussed.
A majority of work focusing on AKI not requiring RRT has previously focused on
specialized populations such as the elderly and U.S. veterans. 6 Again, these studies have largely
corroborated the relationship between poor long-term outcomes and AKI. More recently, broad-
based population studies have expanded on literature of the long-term complications of AKI.
James and colleagues studied a cohort of patients undergoing coronary angiography who
developed AKI and were stratified according to AKIN criteria.51
They showed that over a
median of 19 months follow up, the risk of death and progression to ESRD was increased in
patients with AKI. The risk of such events was commensurate with increasing severity of AKI
[(Death: AKIN Stage I aHR 2.00; 95% CI 1.69-2.36; AKIN Stage II-III aHR3.72; 95% CI 2.92-
4.76); ESRD: AKIN Stage I aHR 4.15; 95% CI 2.32-7.42; AKIN Stage II-III 11.74; 95% CI
6.38-21.59)]. Similarly, a study by Lopes et al., focusing on patients admitted to the hospital
with infectious complications has also demonstrated that AKI is an independent predictor of
mortality at 1 and 2 years respectively. 52
Despite the convincing evidence that AKI leads to poor long-term outcomes, not all
studies have come to the same conclusion. For example, studies by Schiffl et al., Ponte et al. and

12
Liano et al. have all demonstrated opposing results.50;53;54
However, the conclusions of these
analyses are controversial. They are mostly small, single centre studies that failed to account for
residual confounding stemming from patient characteristics, the varying time periods under
study, as well as the aspect that not all patients required dialysis Therefore, the outcomes are
likely biased and reflect a selected cohort of patients who were fairly healthy prior to and during
their AKI event.
2.2 The Pathophysiology of Acute Kidney Injury
Recent epidemiological evidence demonstrating the association between AKI and poor long-term
outcomes has generated much interest in the pathophysiological mechanisms underscoring these
findings.
The majority of our current knowledge concerning the pathophysiology of AKI has been
gleaned from animal studies. Collectively, these have demonstrated that AKI primarily causes
structural changes in the kidney, which over time leads to functional changes such as proteinuria
and hypertension and ultimately a progressive decrease in GFR. However, AKI also affects
other organ systems, and perhaps the combination of the maladaptive processes affecting the
kidney and these other organs results in increased mortality demonstrated in observational
studies.
2.2.1 Renal and Non-Renal Effects of Acute Kidney Injury and their Relationship with Mortality
The kidney is the primary organ affected by AKI. Evidence from basic science studies has
shown that there exists strong biologic support for the association between AKI and subsequent
fixed renal damage.
Basile and colleagues were the first to confirm the structural-functional derangements
manifest by AKI in an elegant animal experiment.55
They took two groups of rats and subjected
one group to bilateral ischemic-reperfusion injury resulting in AKI. Each group of rats was
serially followed for changes in serum TGF-β levels, serum creatinine levels, urine protein
excretion, blood pressure and changes in renal morphology. As expected, in the AKI group,

13
there was a marked initial rise in serum creatinine which decreased to levels similar to the
control group by the end of the first week. The serum creatinine levels remained similar in both
groups for the duration of the study. However, from the outset levels of TGF-β were
significantly higher in the AKI group. Similarly, the AKI group manifested a significant rise in
urine protein excretion compared to the control group beginning at 20 week mark, along with an
increase in mean arterial pressure (MAP). Structural analysis of the renal parenchyma revealed a
decrease in microvascular density and the development of tubulointerstitial fibrosis at the 40
week mark in the AKI group.
Subsequent work by Spurgeon-Pechman and others has confirmed the findings of Basile
and elucidated the mechanism in which AKI leads to structural and functional changes in the
kidney.56-58
Initially, AKI leads to structural damage to the capillary network of the kidneys
leading to renal hypoxia. As a result, an inflammatory response ensues whereby many
proinflammatory and profibrotic cytokines such as TGF-β, interleukin-6 (IL-5) and tumour
necrosis factor α (TNFα) are elaborated. Some of these cytokines such as TGF-β mediate
tubulointerstitial fibrosis, while others promote arteriosclerosis. The arteriosclerosis that ensues
caused impairments in renal autoregulation leading to hypertension which promotes further renal
decline by way of ongoing ischemic renal injury. Moreover, the combination of interstitial
fibrosis and hypertension contribute to the development of proteinuria, which further damages an
already susceptible kidney. Accordingly, the acute renal injury results in a process leading to
further renal injury.
Aside from its effects on the kidney, it is increasingly recognized that AKI is a
multisystem disease affecting many other organs including the heart, lungs, and brain. Klein and
colleagues had demonstrated that an episode of ischemia-reperfusion renal injury in rats leads to
an ARDS-like lesion in the lungs manifest by increased vascular permeability.59
Similarly, in
rats subjected to ischemic reperfusion renal injury, cardiac myocyte function is impaired leading
to aberrant cardiac function and increased apoptosis.60
As with the renal manifestations of AKI,
the non-renal structural and functional changes are believed to be a consequence of the
elaboration of inflammatory cytokines resulting from the initial renal insult.
While the specific reason for the association between AKI and long-term mortality has
yet to be elucidated, it is highly probable that it may be mediated by the downstream effects of

14
the incident AKI. In other words, the functional changes that occur in both the kidney and other
organ systems leading to manifestations such as proteinuria, hypertension, and impaired lung
function may be the link between AKI and mortality. There is compelling evidence that
hypertension and proteinuria, both of which are cardiovascular risk factors, are associated with
increased mortality.47;61
Similarly, long-term survivors of ARDS also have also been found to
have persistent impairments in lung function and quality of life, both of which may lead to
increased morbidity and possibly mortality.62;63
2.3 The Potential Impact of Nephrologist Follow-up After Hospitalization with Severe
Acute Kidney Injury
The value of specialist follow-up after hospitalization for an array of acute conditions is well
established.64-67
Studies have shown that specialist follow-up is associated with decreased
mortality, rehospitalization, and emergency room visits.
The field of cardiology was the first specialty to demonstrate the importance of specialist
follow-up on mortality. In his seminal paper, Ayanian et al. demonstrated an almost 4%
decrease in two year mortality after admission with a myocardial infarction in patients who had
follow-up with a cardiologist after discharge compared to those who did not.64
Although
Ayanian and colleagues were unable to establish the underlying reason behind this finding, they
hypothesized that perhaps differences in quality of care among patients with and without follow-
up could account for this. Building upon Ayanian’s work, Ezekowitz et al. showed that new-
onset CHF patients who were recently discharged from Canadian hospitals had a survival
advantage at one year if they had follow-up with a cardiologist after discharge compared to those
who did not.68
More recently, two population-based studies of CHF and COPD patients had
indicated that early specialist follow-up after hospital discharge may have more immediate
benefits, specifically, fewer rehospitalizations and emergency room visits within 30 days.67;69
The benefit imparted by specialist follow-up after hospitalization may be related to
improvements in quality of care imparted by these physicians. Azaynian demonstrated that
patients who were followed-up by a cardiologist after an admission for myocardial infarction

15
were more likely to be prescribed evidence-based medications such as statins and beta-blockers
compared to those seen by a family physician or internist.70
Similarly, specialist care may also
provide for better health services utilization including access to life saving procedures such as
coronary bypass surgery and angioplasty.64
For survivors of severe acute kidney injury, nephrologist follow-up may have a number
of benefits, which may lead to improvement in morbidity and mortality. For example, follow-up
may lead to: i) testing for risk factors for future loss of renal function; ii) initiation of preventive
measures for progression of renal disease and generalized vascular disease; iii) monitoring and
management of patients with established CKD and its complications, and iv) improved access to
other health services and specialists.

16
CHAPTER 3
Methods
The purpose of this chapter is to:
Provide an overview of the study design;
Describe the data sources;
Clarify the patient selection criteria;
Define the propensity score model;
Specify the statistical approach for analysis;
Outline the subgroup and additional analyses.
3.1 Overview of Study Design
We performed a propensity-score matched cohort study of all adults in Ontario with acute kidney
injury and who received in-hospital dialysis, followed by a 90 day period of being free from
dialysis, death or rehospitalization after discharge, from 1994 to 2008. We compared those who
did versus those who did not receive follow-up care with a nephrologist within 90 days after the
index hospitalization discharge date, matched by a propensity score to receive such care. Cox
Proportional Hazards models were used to estimate the hazard ratio (HR) and 95% confidence
interval (CI).

17
3.2 Data Sources
3.2.1. Canadian Institute for Health Information Discharge Abstract Database (CIHI-DAD)
The Canadian Institute for Health Information Discharge Abstract Database
(CIHI-DAD) contains data on inpatient hospital discharges across Canada, supplied to the
Canadian Institute for Health Information (CIHI) from participating hospitals in all territories
and provinces of Canada except Quebec. The DAD contains demographic, administrative and
clinical data for hospital discharges (inpatient acute, chronic, rehabilitation) and day surgeries,
which is abstracted from patient charts by trained medical staff. In addition to clinical
information, the DAD contains some nonmedical data elements related to demographic and
administrative information for each separation.
Prior to 2002, the CIHI-DAD had used the International Classification of Diseases 9th
revision (ICD-9), and later the ICD-9 Clinical Modification (ICD-9CM) for diagnostic coding.
During that time, procedures were coded in the CIHI-DAD using the Canadian Classification of
Procedures (CCP). Beginning in 2002, the CIHI-DAD began using the International
Classification of Diseases 10th
revision (ICD-10) for diagnostic coding, and the Canadian
Classification of Health Interventions (CCI) for procedural coding for the province of Ontario.
In this study, the CIHI-DAD was used to: i) identify the index hospitalization; ii) define
the AKI-RRT cohort (along with the OHIP database); iii) measure important comorbidities
(through diagnostic codes); and iv) define outcome events.
In terms of data validity, a reabstraction study of the CIHI-DAD demonstrated excellent
agreement with regard to demographic variables (~99% ) and procedural codes (77.1%). 71
Coding of the most responsible diagnosis (MRDx), defined as the one diagnosis responsible for
the greatest contribution to the length of stay, demonstrated variability in agreement (67.6%). 71
Variability in agreement was more pronounced for coding of secondary codes, such as Type 1, 2
and 3 diagnoses.

18
3.2.2. Ontario Health Insurance Plan Database (OHIP)
The Ontario Health Insurance Plan (OHIP) database contains information on physician claims
for inpatient and outpatient services. These services include: i) physician consultations and
assessments in acute care settings, office settings and long-term care facilities; ii) technical and
professional components for diagnostic and therapeutic procedures; iii) surgical procedures; and
iv) laboratory services. The OHIP database also includes information on physician identifiers
(specialty codes) and patient identifiers. This database only captures information on Ontario
physicians who practice within a fee-for-service system. It is estimated that approximately 95%
of physicians practicing in Ontario are enrolled in a fee-for-service billing schedule with the
remaining 5% covered by alternate funding plans (AFPs).
In this study, the OHIP database was used to: i) define the cohort (along with the CIHI-
DAD); ii) define the exposure; iii) measure important comorbidities; and iv) define outcome
events.
Validity of the OHIP database has been less rigorous than for the CIHI-DAD. However,
the OHIP database has been utilized as a supplement to CIHI-DAD codes in administrative
diagnostic algorithms.72;73
It has also been used in administrative algorithms.74
3.2.3 Registered Persons Database (RPDB)
The Registered Persons Database (RPD) contains demographic and vital status data for
individuals with a valid OHIP number. Specifically, the RPDB contains the following
information: i) date of birth; ii) gender; iii) postal code; iv) date of death; and iv) individual
identifier.
In this study, RPDB was used to: i) obtain demographic information for each patient; and
ii) identify deaths (mortality outcome).
3.2.4 Canadian Organ Replacement Registry (CORR)
The Canadian Organ Replacement Register (CORR) is a Canadian information system
for renal and extra-renal organ failure and transplantation. It contains information on

19
outcomes of solid organ transplantation and renal dialysis, which is collected from hospital
dialysis programs, regional transplant programs, organ procurement organizations (OPOs) and
kidney dialysis services offered at independent health facilities. It contains the locations of all
dialysis facilities within Canada. This database has recently undergone validation and
demonstrates excellent agreement with the medical record for demographic data, but poor
sensitivity for comorbid conditions.75
In this study, the CORR database was used to define the distance from a subject’s
residence to the closest dialysis centre using geospatial mapping techniques. 76
The dialysis
centre was a marker for a nephrologists’ practice address.
3.2.5 Canadian Census Data
The Canadian Census data was used to determine income quintile and rural residence status
based on the 2001 Statistics Canada Census, which assigns income quintiles to each
neighborhood community.
3.2.6 Ottawa Data Warehouse
The Ottawa Data Warehouse contains inpatient laboratory data from the Ottawa Hospital and
affiliated institutions. It was used to determine the discharge serum creatinine in a subset of
hospitalized patients. The Ottawa Data Warehouse holdings have recently been used in a study,
but no formal validation process of its data holdings has been undertaken.77
3.2.7 CERNER Database
The CERNER database contains inpatient laboratory data from 11 hospitals in Southwestern
Ontario for patients aged 40 years and older. It was used in this study to determine the discharge
serum creatinine in a subset of hospitalized patients from 2002-2008. This database has been
used in a previous study but has not undergone formal validation.78

20
3.3 Cohort Definition
3.3.1 Inclusion Criteria
The cohort consisted of all adults (age ≥ 18 years) who were hospitalized in Ontario, Canada
between April 1, 1996 and March 31, 2008, and were discharged alive following an episode of
severe acute kidney injury requiring renal replacement therapy (AKI-RRT) during
hospitalization.
AKI-RRT was defined by the combination of a diagnostic code for AKI (all diagnostic
types) and a procedure code for dialysis. We defined AKI by ICD-9 codes: 584.5-584.9, 669.3,
958.5 634.3, 635.3, 636.3, 637.3, 638.3, 639.3; and ICD-10 codes: N17.0-N17.9, O08.4, T79.5,
O90.4. Dialysis was defined by OHIP codes: R849, R850, G323, G325, G326, G330, G331,
G332, G860, G333, G083, G091, G085, G295, G082, G090, G092, G093, G094, G861, G862,
G863, G864, G865, G866, G294, G095, G096; CCP codes: 51.95, 66.98; and CCI
codes:1PZ21HQBR, 1PZ21HPD4. This definition has been used in a previous study.3
(Appendix 1)
3.3.2 Exclusion Criteria
Patients were excluded from the study based on the following criteria: < 18 years at hospital
admission, AKI in the preceding 5 years, dialysis in the preceding 5 years, kidney transplant in
the preceding 5 years, patients who died, received dialysis or were re-hospitalized during the 90
days following hospitalization discharge date and patients with invalid/missing OHIP number or
data. Patients with > 1 hospitalization with AKI-RRT had the first hospitalization counted for
creation of the original cohort.
We had excluded patients with the aforementioned characteristics as we felt their
inclusion would impart a strong selection bias leading to confounding of our results.

21
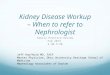
Figure 1: Creation of the Acute Kidney Injury Survivor Cohort.

22
3.3.3 Justification of Cohort Selection (Inclusion and Exclusion Criteria)
Patients with AKI-RRT were chosen as the cohort of study for multiple reasons. Firstly, we felt
this group to be of sufficiently ―high-risk‖ for subsequent deleterious outcomes. Multiple studies
have demonstrated a continuum of renal damage conditional on the severity of the acute kidney
insult. 8;38;44;79
As dialysis requiring AKI represents the most severe form of AKI, it is plausible
that this cohort would develop clinically significant renal damage which would portend an
increased risk for long-term morbidity and mortality. This construct has been corroborated by
clinical studies where individuals with AKI-RRT demonstrate inferior outcomes and a faster
decline of renal function than their non-dialysis requiring counterparts with AKI.38;44;80
As such,
we felt that this cohort, compared to others with less severe forms of AKI, would garner the most
benefit from early nephrology follow-up.
Secondly, our cohort had been validated in a previous study and demonstrated excellent
sensitivity and specificity. 81
In that study, the combination of an ICD-9 diagnostic code for AKI
and an ICD-9 procedure code for dialysis had 90% sensitivity (95% CI 85% - 94%), 94%
specificity (95% CI 89% - 97%), and 94% positive predictive value (95% CI 89% - 97%) for
capturing the combination of acute kidney injury and dialysis. This is in contrast to ICD-9 and
ICD-10 diagnostic codes for AKI which demonstrated excellent specificity (median 99%) but
poor sensitivity (median 29%), according to a recent systematic review. 81
Furthermore, the same
definition of AKI-RRT had been employed in a recent study using linked Ontario administrative
databases to assess the risk of chronic dialysis and all-cause mortality, thereby adding to its face
validity. 38
We chose to exclude patients with a diagnosis of AKI, dialysis or transplantation in the 5
years preceding the index admission as these are all important confounders. We also excluded
patients who died, received dialysis or were rehospitalized during the first 90 days post-
discharge. Studies have demonstrated that a majority of patients discharged from hospital free of
dialysis either return to dialysis, are readmitted or die within the first 90 days and including such
patients would impart selection bias as sicker patients may experience the outcome earlier
regardless of the exposure.

23
3.4 Covariates and Outcome Variables
3.4.1. Primary exposure: Nephrology Consultation within 90 days of Discharge
The primary exposure for this study was at least one outpatient nephrology consultation within
90 days of discharge from the index hospitalization defined using the OHIP database. In the
OHIP database, the specialty code for nephrology (specialty code 16) was introduced in October
2009. Prior to this, nephrologists were coded in the same category as internal medicine
(specialty code 13). Therefore, we defined a nephrologist as per an algorithm used by Wald et
al. Accordingly, a nephrologist was any physician with 10 claims using any combination of the
following OHIP codes between start of ICES data until March 31, 2008: G326, G860, G333,
G862, G863, G865, G866, G332, G861, G864.
Aside from the aforementioned study by Wald et al., a study by Jain et al. looking at the
impact of eGFR reporting on nephrology referral rates in Ontario also used OHIP data to define a
nephrologist. 38;82
In that study, a nephrologist was a physician who had billed for chronic
dialysis (i.e. one of codes G860-866 or three of codes G326 or G333) at least 10 times in the past
year and who had billed at least one A135 claim in the same year. Jain et al.’s algorithm
identified nearly similar numbers of nephrologists in Ontario when compared to the ICES
Physicians Database (IPDB), as the gold standard, for the years 1999-2005.
Despite Jain et al.’s definition being validated against the IPDB, there were multiple
reasons for us not using it to define our exposure. Firstly, the IPDB has not been independently
validated, and therefore may not accurately code a physician’s specialty. Secondly, using kappa
statistics we assessed the degree of agreement between our definition and Jain et al.’s definition
with the IPDB. Both definitions had almost identical kappas (Jain κ=0.901, 95% CI 0.887-
0.915; Wald κ=0.891, 95% CI 0.876-0.905), demonstrating that both definitions had excellent
agreement with the IPDB. (Table 3) Finally, our definition yielded a greater number of exposed
individuals compared to Jain et al.’s definition (1588 vs. 1474). We felt that a greater number of
exposed individuals would protect our statistical power as it would offset any unexpected
decrements in the effect.

24
Table 3: Comparison of Two Algorithms for Defining a Nephrologist.
Jain et al.
Nephrologist*
Yes No Total
IPDB
Nephrologist
Yes 1357 63 1420
No 117 2350 2467
Total 1474 2413 3887
*one of codes G860-866 or three of codes G326 or G333 at least 10 times in the past year and who had billed at
least one A135 claim in the same year.
‡ any physician with 10 claims using any combination of the following OHIP codes: G326, G860, G333, G862,
G863, G865, G866, G332, G861, G864
Wald et al.
Nephrologist‡
Yes No Total
IPDB
Nephrologist
Yes 1403 17 1420
No 185 2282 2467
Total 1588 2299 3887
Κ =0.901
95% CI: 0.887-0.915 95% CI: 0.887-0.915
Standard Error: 0.0072
Κ =0.891
95% CI: 0.876-0.905
Standard Error: 0.0075

25
3.4.2 Primary Outcome: All-cause Mortality
The primary outcome of this study was all cause mortality within 2 years of the index date (date
of discharge + 90 days). The RPDB was used to define this outcome.
3.4.3 Secondary Outcome: Receipt of Chronic Dialysis
Using CCI/CCP and OHIP procedural codes, we defined ESRD as the receipt of dialysis
(hemodialysis or peritoneal dialysis) for a 90 day period. (Appendix 1) We censored this
outcome at the earliest of death or 2 years from the index date. The date of first dialysis claim
was considered to be the date of initiation of chronic dialysis. Our definition of ESRD is similar
to that used in previous studies. 9;38
Despite there being no direct validation study of our
definition of chronic dialysis, it has been used in previous studies.9;38
Moreover, procedure
codes in the OHIP and DAD are very accurate.83;84
3.5 Statistical Methods
3.5.1 Propensity Score Modeling
Propensity score modeling was used for our risk analysis. This is a statistical method that is used
to reduce the impact of confounding when estimating of causal treatment effects with
nonrandomized data.85-87
The propensity score is defined as a subject’s probability of receiving a
specific treatment conditional on the observed covariates. Individuals with the same propensity
score have the same distribution of measured covariates, independent of treatment status.
However, treated and untreated subjects with the same propensity score can have different
distributions of unmeasured variables.
We used an accepted iterative process to generate our propensity model.85;88
This process
comprised 4 steps: i) specifying the propensity score model; ii) matching on the propensity
score; iii) assessing balance between treated and untreated subjects, and iv) estimation of the
treatment effect.

26
3.5.1.1 Specifying the Propensity Score Model
Using a thorough review of the literature, we derived a list of measured baseline variables
(confounders) that are likely related to the exposure (nephrology consultation within 90 days of
discharge) and outcome (death) but are not in the causal pathway. These included: age
(continuous in years), sex, and income quintile at the hospital discharge date; era of admission
(1996-2001 vs. 2002-2008), distance from dialysis centre, hospital type (teaching vs. non-
teaching), rural location (in kilometres), number of hospitalizations or health care visits to any
physician (including nephrologist) or emergency department in the 5 years preceding the
hospital discharge date, CKD in the five years preceding the hospital admission date; receipt of
coronary, carotid, or peripheral arterial revascularization, cardiac valve surgery, coronary
angiography, cardiac stress testing, echocardiography, single 12-lead or ambulatory 24-hour
electrocardiography, pacemaker insertion, carotid Doppler ultrasonography or renal biopsy in the
5 years before the hospital discharge date; diagnosed liver dysfunction, heart failure, diabetes
mellitus, cancer, cerebrovascular disease, cardiac dysrhythmias, myocardial infarction or angina,
peripheral artery disease, major infection, hypertension, proteinuria, hematuria and score on the
Charlson Comorbidity Index in the 5 years before the hospital discharge date; and sepsis, receipt
of mechanical ventilation, nonruptured aortic aneurysm repair, or cardiac surgery, all within the
index hospitalization. The receipt of mechanical ventilation was used as a surrogate for
admission to a critical care unit.89
Geospatial mapping methods were used to calculate the
distance between each patient’s residence and the practice location of the closest dialysis unit.76
(Appendix 2)
We then derived a propensity score model using logistic regression. Here, treatment
assignment (at least one outpatient nephrology consultation within 90 days of discharge) was
regressed on the baseline variables. Using this model, the likelihood of nephrology consultation
within 90 days of discharge (propensity score) was calculated for each individual patients.
3.5.1.2 Matching on the Propensity Score
We next matched treated and untreated subjects on propensity score. We employed
nearest-neighbor matching within a 0.2 caliper width. In nearest-neighbour matching, the first
randomly selected treated subject is matched to the untreated subject with the closest propensity

27
score within a 0.2 caliper width. If multiple untreated subjects are equally close to this treated
subject, then one of these untreated subjects is randomly selected for matching to the treated
subject. This process is repeated until all possible matches have been formed. A 0.2 caliper
width was used as a recent study demonstrated that matching using this width tended to have
superior performance compared with other competing methods that are used in the medical
literature. 90
We also forced an exact match on the covariate hospital type as there was an
imbalance between the pairs as demonstrated by a standardized difference >10% for this variable
(see next section).
3.5.1.3. Assessing Balance between Treated and Untreated Subjects: Standardized Difference
Statistical hypothesis testing to detect differences in baseline variables between treated and
untreated subjects is inappropriate in matched propensity based samples. It is has been proposed
that assessment of balance in such situations be assessed using standardized differences. The
standardized difference is defined as:
where treatment and control are the mean of the variable among the treated and untreated subjects,
respectively, while s2
treatment and s2
control the sample standard deviation of covariate in the treated
and untreated subjects, respectively. A standardized difference greater than 10% for a pair of
covariates indicates imbalance. 91
We used standardized differences to assess for balance between
treated and untreated subjects in our cohort before and after the matching process.
3.5.1.4. Estimation of Treatment Effect
Time-to-event analyses were performed until March 31, 2010. For the mortality end-point, an
individual was censored at the earlier of death or 2 years from the initiation of the period of
follow-up (i.e., 90 days after the index hospitalization discharge date). For the chronic dialysis
outcome, an individual was censored at the earlier of dialysis, death, or 2 years from the index
date. Incidence rates of both all-cause mortality and chronic dialysis were determined for

28
participants with and without nephrology follow-up. Hazard ratios (HRs) and 95% confidence
intervals (CIs) were derived from Cox proportional hazards models, stratified on matched sets,
with matched individuals without a nephrology follow-up being the reference group. Survival
curves for all-cause mortality and chronic dialysis were generated from the Cox models. The
proportional hazards assumption was tested using graphical methods (log 1-log plots).
3.6 Subgroup Analysis
Stratified analyses were performed in the following subgroups: age, sex, rural location, hospital
type, prior nephrologist visit, Charlson score92
and a history of myocardial infarction, diabetes
mellitus, CKD, liver disease and peripheral vascular disease. For these subgroup analyses, we
repeated the same propensity-score matching process while simultaneously forcing an exact
match on the subgroup characteristics. A z-test was used to compare whether the hazard rates
differed within subgroups.
3.7 Sensitivity Analyses
We performed several sensitivity analyses. Firstly, to account for the effect of discharge serum
creatinine on our results we repeated the primary analysis after modifying the original propensity
score to include serum creatinine (continuous variable in µmol/L) for the individuals where this
data was available. Secondly, to demonstrate that the association between follow-up and
mortality was not due to better predialysis care, we repeated our primary analysis for the
mortality endpoint and censored all patients who went on to receive chronic dialysis. Thirdly,
we undertook high dimensional propensity score modeling in an attempt to further account for
potential confounders. Finally, we assessed the specificity of effect using dermatology or
psychiatry consultation within 90 days of hospital discharge as a tracer exposure, an exposure for
which we would not expect an association with all-cause mortality. Observing an association
would raise concerns about residual confounding.

29
3.7.1 High Dimensional Propensity Score
High dimensional propensity score (HDPS) modeling is a strategy, developed by the Brigham
and Women’s Division of Pharmacoepidemiology, that has been extensively used. 93;94
This
method of modeling uses an algorithm to ―mine‖ administrative databases resulting in the
definition of a large number of potential candidate covariates, which may act as ―proxies‖ for
potential confounders. These proxies are covariates that may not necessarily be included in the
traditional propensity score model by the investigator; hence they are considered to be candidate
covariates.
The creation of the HDPS involves several iterative steps which are simplistically
summarized and contrasted to the creation of the traditional PS in Figure 2. The first step
involves identifying the administrative databases or data sources in which the search for
candidate covariates will be identified. The next step involves the identification of candidate
covariates and ranking of these variables according to the degree of bias they impart. After this
step, the investigator decides which of the candidate variables to include in the propensity model
using clinical reasoning. Once the candidate variables have been selected, these are included
along with the investigator specified covariates to develop the propensity score model.

30
Comparison of HD versus conventional propensity
score models
High Dimensional Conventional
Estimate Propensity Score
CANDIDATE covariates + INVESTIGATOR SPECIFIED covariates
Algorithm identifies most prevalent codes in data sources
= CANDIDATE Covariates
Identify Administrative Data Sources
DAD
(Proc)
DAD
(Dx )
OHIP (Dx)
Estimate Propensity Score
Investigator Specified Covariates
Figure 2. Comparison of high dimensional versus traditional propensity score modeling.
3.8 Additional Analyses
3.8.1 Healthcare Utilization
We also performed a descriptive analysis of the matched primary cohort, in which we assessed
the use of health services and cardiac procedures within 2 years after the index date for patients
with and without follow-up with a nephrologist.
3.8.2 Unmatched Cohort
For unmatched patients, we also undertook descriptive analyses and calculated the
incidence of mortality and receipt of chronic dialysis within 2 years.

31
CHAPTER 4
Results
The purpose of this chapter is to:
Describe the acute kidney injury cohort and compare the baseline characteristics of
individuals with and without early post discharge nephrologist follow-up.
Determine the impact of early post-discharge nephrologist follow-up on the risk of
mortality and the receipt of chronic dialysis.
Describe the subgroup and sensitivity analyses
4.1 Description of the Cohort
During the 12 year study period 21,809 patients were hospitalized with acute kidney injury
requiring temporary renal replacement therapy. Of these patients, 4216 (19.4%) had an
exclusionary event [3982 had an exclusionary event in the 5 years preceding their admission to
hospital (2525 had a previous episode of AKI, 1454 previously received dialysis, and 3 had
kidney transplantation and 234 had a hospital stay greater than 180 days]. This left 17,593
(80.6%) patients with a first hospitalization for AKI-RRT. Of these subjects, 7176 died during
the index hospitalization and were subsequently excluded leaving 10,417 (47.7%) patients
surviving to discharge. Of the 10,417 patients, 6540 had an exclusionary event [6530 had an
exclusionary event within 90 days post-discharge (4409 received dialysis, 1851 were readmitted
to hospital, 270 died) and 10 had incomplete data]. Therefore, our final cohort included 3,877
(17.8%) who survived more than 90 days post-discharge without receiving dialysis or being re-
hospitalized. (Figure 1)
Of the 3,877 patients, 40.8% (n=1583) had follow-up with a nephrologist within 90 days
of hospital discharge. (Table 4) The mean duration between discharge and nephrologist follow-
up was 12 days (±19 days). The mean age of the participants was 61 years, approximately 40%

32
were women, and about one quarter lived in a rural setting. Most of the participants (>90%)
lived within 50 km of a dialysis unit. Access to healthcare was not substantially different
between the groups in the 5 years preceding hospital admission, except for prior nephrology
visits (median 0 (IQR 0-0) without follow-up vs. median 0 (IQR 0-2) with follow-up). There was
marked comorbid disease in both groups. Almost 45% of the cohort had a history of cardiac
disease, 40% had a history of cancer, and 42% had a history of diabetes. The mean Charlson
Comorbidity Index was 2.9 (± 2.3). A number of subjects in both groups had previous
procedures, with the majority being cardiac in nature.
Individuals who had post-discharge nephrologist follow-up differed from those who did
not undergo follow up on a number of baseline characteristics. (Table 4) Subjects with early
follow-up had a higher likelihood of having pre-existing CKD; a history of hematuria, and
hypertension; previous visits to a nephrologist, and a prior renal biopsy. They also had lower
rates of a previous history of cerebrovascular disease, liver disease, and a major respiratory tract
infection; sepsis, receipt of mechanical ventilation, cardiac surgery and admission to a teaching
hospital during their index hospitalization. The standardized differences for each covariate pair
were all less than 10% with the exception of teaching hospital.
Overall, 74.8% of individuals who underwent early follow-up with a nephrologist
(n=1184) were successfully matched to similar patients who did not. The covariate balance in
the matched cohort was considerably improved as demonstrated by smaller standardized
differences. (Table 5)

33
Table 4: Baseline characteristics of cohort (pre-match).
No. (%)a
Characteristic
No Nephrology
Follow-up
(n=2294)
Nephrology
Follow-up
(n=1583)
Standardized
Difference
Demographics Age, mean (SD), y
Female gender
60.7 (16.4)
929 (40.5)
60.8 (16.5)
633 (40.0)
0.01
0.01
Lowest income quintile
Rural residence
564 (24.6)
327 (14.3)
382 (24.1)
214 (13.5)
0.01
0.02
Distance from nearest dialysis unit (km) 0-50
51-150
151-300 >300
207 (90.1)
212 (9.2)
9 (0.4) 6 (0.3)
1454(91.9)
114 (7.2)
8 (0.5) 7 (0.4)
0.06
0.07
0.02 0.03
Hospital type Teaching hospital
Healthcare accessb Number of hospitalizations
Number of emergency visits
Number of GP visits Number of internist visits
Number of cardiology visits
Number of nephrology visits
1291 (56.3)
1 (0-2)
2 (1-5)
39 (18-68) 5 (1-16)
0 (0-2)
0 (0-0)
656 (41.4)
1(0-2)
2 (1-5)
40 (19-69) 7 (2-20)
0 (0-3)
0 (0-2)
0.3
0.05
0.05
0.03 0.1
0.05
0.39
Comorbid diseasec
Myocardial Infarction Coronary artery disease
Cardiac dysrythmias
Heart failure Cerebrovascular disease
Diabetes
Cancer Liver disease
Peripheral vascular disease
Chronic kidney diseasec
Hypertension
Hematuria Proteinuria
Major respiratory infection
Major genitourinary/gastrointestinal infection Major skin/soft tissue infection
Charlson comorbidity index, mean (SD), score
1053 (45.9) 890 (38.8)
338 (14.7)
881 (38.4) 475 (20.7)
959 (41.8)
916 (39.9) 388 (16.9)
75 (3.3)
282 (12.3)
1545 (67.3)
578 (25.2) 9 (0.4)
1561 (68.0)
614 (26.8) 686 (29.9)
2.9 (2.3)
664 (41.9) 595 (37.6)
206 (13.0)
573(36.2) 223 (14.1)
707 (44.7)
584 (36.9) 204 (12.9)
56 (3.5)
387 (24.4)
1131 (71.4)
479 (30.3) 11 (0.7)
985 (62.2)
354 (22.4) 443 (28.0)
2.9 (2.3)
0.08 0.02
0.05
0.05 0.17
0.06
0.06 0.11
0.01
0.33
0.09
0.11 0.04
0.12
0.1 0.04
0
Proceduresd Angiography
Coronary artery bypass grafting
Percutaneous coronary intervention Valvular surgery
Pacemaker
Echocardiography Electrocardiography
Holter monitor Stress test
Peripheral vascular procedures
Carotid doppler ultrasound Carotid endarderectomy
Renal biopsy
519 (22.6)
244 (10.6)
485 (21.1) 162 (7.1)
176 (7.7)
957 (41.7) 1919 (83.7)
242 (10.5) 707 (30.8)
46 (2.0)
302 (13.2) 17 (0.7)
47 (2.0)
293 (18.5)
141 (8.9)
271 (17.1) 66 (4.2)
94 (5.9)
686 (43.3) 1362 (86.0)
188 (11.9) 546 (34.5)
26 (1.6)
262 (16.6) 10 (0.6)
168 (10.6)
0.1
0.06
0.1 0.12
0.07
0.03 0.07
0.04 0.08
0.03
0.1 0.01
0.38
Procedure or condition during index hospitalization Sepsis
Cardiac surgery
Abdominal aortic aneurysm repair Mechanical ventilation
509 (22.2)
333 (14.5)
118 (5.1) 1474 (64.3)
196 (12.4)
143 (9.0)
37 (2.3) 602 (38.0)
0.26
0.17
0.14 0.54
a All data presented as No. (%) unless otherwise indicated. b In the 5 years preceding hospital admission expressed as median (IQR). c In the 5 years preceding the hospital discharge date except chronic kidney disease which had a lookback period of 5 years preceding the hospital admission date. d In the 5 years preceding hospital discharge date.

34
Table 5: Baseline characteristics of cohort (post-match).
`
No. (%)a
Characteristic
No Nephrology
Follow-up
(n=1184)
Nephrology
Follow-up
(n=1184)
Standardized
Difference
Demographics
Age, mean (SD), y
Female gender
61.4 (16.5)
474 (40.0)
61.0 (16.5)
473 (39.9)
0.03
0
Lowest income quintile Rural residence
279 (23.6) 156 (13.2)
280 (23.6) 170 (14.4)
0 0.03
Distance from nearest dialysis unit (km)
0-50 51-150
151-300
>300
1077 (91.0) 94 (7.9)
7 (0.6)
6 (0.5)
1072 (90.5) 99 (8.4)
7 (0.6)
6 (0.5)
0.01
Hospital type
Teaching hospital
Healthcare access b
Number of hospitalizations Number of emergency visits
Number of GP visits
Number of internist visits Number of cardiology visits
Number of nephrology visits
535 (45.2)
1 (0-2) 2 (1-5)
40 (19-69)
5 (1-16) 0 (0-3)
0 (0-1)
535 (45.2)
1(0-2) 2 (1-5)
39 (18-68)
6 (1-17) 0 (0-3)
0 (0-1)
0
0.05 0.02
0
0.02 0
0.04
Comorbid diseasec
Myocardial Infarction
Coronary artery disease Cardiac dysrythmias
Heart failure
Cerebrovascular disease Diabetes
Cancer
Liver disease Peripheral vascular disease
Chronic kidney disease
Hypertension Hematuria
Proteinuria Major respiratory infection
Major genitourinary/gastrointestinal infection
Major skin/soft tissue infection
Charlson comorbidity index, mean (SD), score
522 (44.1)
443 (37.4) 164 (13.9)
430 (36.3)
198 (16.7) 510 (43.1)
448 (37.8)
157 (13.3) 39 (3.3)
204 (17.2)
839 (69.5) 175 (14.8)
<5(0.4) 753 (63.6)
272 (23.0)
328 (27.7)
2.8 (2.3)
514 (43.4)
456 (38.5) 155 (13.1)
429 (36.2)
189 (16.0) 517 (43.7)
440 (37.2)
164 (13.9) 41 (3.5)
205 (17.3)
816 (68.9) 345 (29.1)
8 (0.7) 742 (62.7)
279 (23.6)
344 (29.1)
2.9 (2.2)
0.01
0.02 0.02
0
0.02 0.01
0.01
0.02 0.01
0
0.01 0.03
0.03 0.02
0.01
0.03
0.02
Procedured
Angiography Coronary artery bypass grafting
Percutaneous coronary intervention
Valvular surgery Pacemaker
Echocardiography
Electrocardiography Holter monitor
Stress test
Peripheral vascular procedures
Carotid doppler ultrasound
Carotid endarderectomy Renal biopsy
232 (19.6) 115 (9.7)
214 (18.1)
68 (5.7) 68 (5.7)
495 (41.8)
996 (84.1) 139 (11.7)
377 (31.8)
21 (1.8)
178 (15.0)
8 (0.7) 46 (3.9)
226 (19.1) 114 (9.6)
209 (17.7)
56 (4.7) 70 (5.9)
483 (40.8)
1000 (84.5) 123 (10.4)
378 (31.9)
17 (1.4)
177( 14.9)
7 (0.6) 49 (4.1)
0.01 0
0.01
0.05 0.01
0.02
0.01 0.04
0
0.03
0
0.01 0.01
Procedure or condition during index hospitalization
Sepsis Cardiac surgery
Abdominal aortic aneurysm repair
Mechanical ventilation
175 (14.8) 131 (11.1)
36 (3.0)
563 (47.6)
183 (15.5) 121 (10.4)
33 (2.8)
550 (46.5)
0.02 0.02
0.02
0.02
a All data presented as No. (%) unless otherwise indicated. b In the 5 years preceding hospital admission expressed as median (IQR). c In the 5 years preceding the hospital discharge date except chronic kidney disease which had a lookback period of 5 years preceding the hospital admission date. d In the 5 years preceding hospital discharge date.

35
4.2 Outcomes
Within the matched cohort, the frequency of all-cause mortality was 15.5% (n=184 patients)
among those with follow-up with a nephrologist after hospitalization. The mortality rate was
18.9% (n=224 patients) among those without follow-up with a nephrologist after hospitalization.
The incidence rate of all-cause mortality was 8.4 per 100 person-years and 10.6 per 100 person-
years among those with and without follow-up with a nephrologist, corresponding to a hazard
ratio of 0.76 (95% confidence interval [CI] 0.62-0.93). In contrast, the frequency of chronic
dialysis was 7.0% (83 patients) in patients with nephrologist follow-up, which was higher than
those without follow-up [2.7% (32 patients)]. The incidence rate was 7.0 per 100 person-years,
and 2.7 per 100 person-years among those with and without follow-up with a nephrologist,
corresponding to a hazard ratio of 2.71 (95% CI 1.76-4.19). (Figures 3 and 4; Table 6)
Table 6: Risk of all-cause mortality and chronic dialysis by group
Nephrology Follow-up
(n=1184)
No Nephrology Follow-up
(n=1184)
Outcome
No. of Events
(%)
Incidence
Rate Per 100
Person-
Years
No. of Events
(%)
Incidence
Rate Per 100
Person-
Years
Hazard Ratio
(95% Confidence
Interval)
All-cause
mortality
184 (15.5) 8.4 224 (18.9) 10.6 0.76 (0.62-0.93)
Chronic
Dialysis
83 (7.0) 7.0 32 (2.7) 2.7 2.71 (1.76-4.19)

36
0%
5%
10%
15%
20%
0 100 200 300 400 500 600 700 800
Cu
mu
lati
ve
Ris
k o
f A
ll-C
au
se
Mo
rta
lity
Follow-up, days
No Follow-up
Follow-up
Figure 3. Risk of All-Cause Mortality in Association with Early Nephrology Follow-up

37
Figure 4. Risk of Chronic Dialysis in Association with Early Nephrology Follow-up

38
4.3 Subgroup Analysis
Stratified analysis for all-cause mortality among subgroups demonstrated findings consistent
with our primary analysis: decreased all-cause mortality for patients with early nephrology
follow-up within 2 years. (Table 7) (Figure 5) Although the point estimate demonstrating a
decrease in mortality was consistent among all pre-specified subgroups, except those with no
history of peripheral vascular disease (aHR 1.00), it was only statistically significant in certain
subgroups. These subgroups included males (aHR 0.72, 95% CI 0.55-0.94), those less than 65
years of age (aHR 0.56, 95% CI 0.42-0.85), those with a history of diabetes (aHR 0.66, 95% CI
0.48-0.90), those with no previous nephrology visits (aHR 0.75, 95% CI 0.85-0.97) and those
with no history of liver disease (aHR 0.79, 95% CI 0.64-0.98). Within subgroups, there was only
a significant difference in the HR among those less than 65 and greater than and equal to 65
years old (p=0.00).

39
Table 7: Risk of all-cause mortality stratified by subgroup.
Subgroup Lower
Limit
Upper
Limit
Adjusted
Hazard
ratio
Log hazard
ratio
Z statistic p-value 2sided p
Age
3.451438 0 0
≥65 0.71 1.18 0.911 -9.32E-02
<65 0.42 0.85 0.595 -0.519193873
Hospital Type
Teaching Hospital 0.56 1.06 0.773 -0.25747623
Non-Teaching
Hospital
0.57 0.98 0.744 -0.295714244
0.37615 0.352 0.704
Admission Era
1996-2001 0.42 0.79 0.577 -0.549913012
2001-2008 0.69 1.17 0.9 -0.105360516 -2.60923 0.005 0.01
Gender
Male 0.55 0.94 0.72 -0.328504067
Female 0.61 1.17 0.846 -0.167235919 -1.03178 0.152 0.304
Residence
Rural 0.39 1.18 0.677 -0.390084006
Urban 0.66 1.02 0.819 -0.199671195 -0.56131 0.288 0.576
Previous Nephrology
Visit
Yes 0.64 1.25 0.889 -0.117658043
No 0.58 0.97 0.75 -0.287682072 1.119185 0.131 0.262
Charlson Score
≤2
>2
0.57
0.63
1.17
1.04
0.815
0.809
-0.204567166
-0.211956362
0.165727
0.433 0.866
History of Myocardial
Infarction
Yes
No
0.62 1.1 0.825 -0.192371893
0.60 1.05 0.791 -0.234457311 0.430481 0.334 0.668
History of Diabetes
Yes 0.48 0.90 0.656 -0.42159449
No 0.60 1.05 0.791 -0.234457311 -1.01166 0.156 0.312
History of CKD
Yes 0.64 1.44 0.958 -4.29E-02
No 0.63 1.02 0.801 -0.221894332 0.990191 0.184 0.368
History of Liver
Disease
Yes 0.32 1.14 0.6 -0.510825624
No 0.64 0.98 0.789 -0.236988958 -0.72707 0.233 0.466
History of PVD
Yes 0.66 1.00 0.813 -0.207024169
No 0.40 2.52 1 -1.477 0.074 0.148

40
Hazard Ratio and 95% CI
Hospital Type
Non-teaching Teaching Peripheral Vascular Disease Absent Present Liver Disease Absent Present Chronic Kidney Disease Absent Present Diabetes Absent Present Myocardial Infarction Absent Present Charlson Score >2 ≤2 Previous Nephrology Visit No Yes Rural Residence No Yes Sex Female Male **Age <65 ≥65
Mortality
Decreased Increased
Figure 5: Association of nephrology follow-up with all-cause mortality within subgroups
0.25 0.5 1 2 4

41
4.4 Sensitivity Analyses
4.4.1 Patients with a Discharge Serum Creatinine Measurement
Among the matched cohort, 530 patients (33%) had serum creatinine values at time of discharge
from hospital, of which 47% were in the early nephrology care visit group and 53% were in the
other group. Similar to the overall cohort there were a number of differences in baseline
characteristics between individuals that had early follow-up and those which did not. (Table 8)
Particularly, patients who had follow-up with a nephrologist after discharge were older, lived
farther away from a dialysis unit; and had a history of hypertension and chronic kidney disease.
The mean serum creatinine at time of discharge was 270 µmol/L (±147 µmol/L) for patients with
early follow-up compared to 139 µmol/L (±94 µmol/L) in those without early follow-up. Almost
75% of those with early follow-up had Stage IV/V CKD; whereas the majority of patients
without follow-up had Stage II/III CKD. Patients without early follow-up had a higher rate of
cardiovascular procedures in the preceding 5 years and had higher rates of sepsis, cardiac surgery
and ICU admission during their index hospitalization.
Of the 530 patients, 102 patients with early follow-up were matched to 102 patients
without early follow-up using the modified propensity scores (which included serum creatinine).
There was marked improvement in covariate balance in the matched cohort. (Table 9)
In keeping with the primary analysis, there was a decrease in the point estimate for all-
cause mortality (HR 0.84; 95% CI 0.43-1.64) and increased receipt chronic dialysis (HR 1.50;
95% CI 0.25-8.90) in patients who visited a nephrologist post-discharge.

42
Table 8: Baseline characteristics of patients with discharge creatinine values.
No. (%)a
Characteristic
No Nephrology
Follow-up
(n=280)
Nephrology
Follow-up
(n=250)
Standardized
Difference
Demographics
Age, mean (SD), y Female gender
60.0 (15.7) 108 (38.6)
62.4 (14.6) 109 (43.6)
0.16 0.1
Lowest income quintile
Rural residence
66 (23.6)
49 (17.5)
66 (26.4)
57 (22.8)
0.07
0.13 Distance from nearest dialysis unit (km)
0-50
51-150 151-300
249 (88.9)
29 (10.4) 2 (0.7)
207 (82.8)
43 (17.2) 0 (0)
0.18
0.2 0.12
Hospital type Teaching hospital
Healthcare accessb Number of hospitalizations
Number of emergency visits
Number of GP visits Number of internist visits
Number of cardiology visits
Number of nephrology visits
252 (90.0)
1 (0-2)
3 (1-6)
39 (22-67) 7 (2-21)
1 (0-3)
0 (0-1)
205 (82.0)
1(0-2)
3 (1-5)
40 (19-69) 9 (2-21)
0 (0-2)
0 (0-2)
0.23
0.03
0.05
0.06 0.05
0.14
0.3
Comorbid diseasec
Myocardial Infarction Coronary artery disease
Cardiac dysrythmias Heart failure
Cerebrovascular disease
Diabetes Cancer
Liver disease
Peripheral vascular disease Chronic kidney disease
Hypertension
Hematuria Proteinuria
Major respiratory infection
Major genitourinary/gastrointestinal infection Major skin/soft tissue infection
Charlson comorbidity index, mean (SD), score
115 (41.1) 90 (32.1)
37 (13.2) 95 (33.9)
53 (18.9)
127 (45.4) 124 (44.3)
61 (21.8)
7 (2.5) 38 (13.6)
186 (66.4)
83 (29.6) 1 (0.4)
183 (65.4)
67 (23.9) 96 (34.3)
3.1 (2.5)
103 (41.2) 89 (35.6)
33 (13.2) 82 (32.8)
36 (14.4)
120 (48.0) 100 (40.0)
30 (12.0)
9 (3.6) 71 (28.4)
184 (73.6)
67 (26.8) 2 (0.4)
153 (61.2)
50 (20.0) 78 (31.2)
2.9 (2.1)
0 0.07
0 0.02
0.12
0.05 0.09
0.26
0.06 0.37
0.16
0.06 0.06
0.09
0.09 0.07
0.08
Proceduresd
Angiography
Coronary artery bypass grafting
Percutaneous coronary intervention
Valvular surgery
Pacemaker Echocardiography
Electrocardiography
Holter monitor Stress test
Carotid doppler ultrasound
Renal biopsy
54 (19.3)
33 (11.8)
64 (22.9)
16 (5.7)
40 (14.3) 95 (33.9)
244 (87.1)
242 (10.5) 81 (28.9)
32 (11.4)
1 (0.4)
39 (15.6)
21 (8.4)
37 (14.8)
8 (3.2)
19 (7.6) 93 (37.2)
225 (90.0)
188 (11.9) 93 (37.2)
41 (16.4)
34 (13.6)
0.1
0.11
0.21
0.12
0.21 0.07
0.09
0.04 0.18
0.14
0.55
Procedure or condition during index hospitalization
Sepsis Cardiac surgery
Abdominal aortic aneurysm repair
Mechanical ventilation
63 (22.5) 51 (18.2)
14 (5.0)
197 (70.4)
30 (12.0) 17 (6.8)
10 (4.0)
96 (38.4)
0.28 0.35
0.05
0.68
Laboratory results
Discharge serum creatinine, mean (SD), µmol/L Chronic kidney disease stagef
Stage I
Stage II Stage III
Stage IV
Stage V
139.2 (94.3)
48 (17.1)
72 (25.7) 108 (38.6)
45 (16.1)
7 (2.5)
270.4 (147.5)
4 (1.6)
12 (4.8) 55 (22.0)
117 (46.8)
62 (24.8)
1.07
0.54
0.6 0.36
0.71
0.7 a All data presented as No. (%) unless otherwise indicated. b In the 5 years preceding hospital admission expressed as median (IQR). c In the 5 years preceding the hospital discharge date except chronic kidney disease which had a lookback period of 5 years preceding the hospital admission date. d In the 5 years preceding hospital discharge date.
eTable 1. Characteristics of hospitalized individuals by group

43
Table 9: Characteristics of patients with discharge creatinine values post-matching.
No. (%)a
Characteristic
No Nephrology
Follow-up
(n=102)
Nephrology
Follow-up
(n=102)
Standardized
Difference
Demographics
Age, mean (SD), y Female gender
65.2 (13.9) 42 (41.2)
62.0 (15.8) 39 (38.2)
0.21 0.06
Lowest income quintile
Rural residence
21 (20.6)
21 (20.6)
26 (25.5)
17 (16.7)
0.12
0.10 Distance from nearest dialysis unit (km)
0-50
51-150
87 (85.3)
15 (14.7)
90 (88.2)
12 (11.8)
0.09
0.09
Hospital type Teaching hospital
Healthcare accessb Number of hospitalizations
Number of emergency visits
Number of GP visits Number of internist visits
Number of cardiology visits
Number of nephrology visits
93 (91.2)
1 (0-2)
3 (1-6)
42 (24-71) 8 (2-17)
1 (0-3)
0 (0-1)
93 (91.2)
1 (0-2)
2 (1-5)
43 (17-75) 7 (2-20)
1 (0-3)
0 (0-1)
0
0.02
0
0.01 0.05
0.01
0.09
Comorbid diseasec
Myocardial Infarction Coronary artery disease
Cardiac dysrythmias Heart failure
Cerebrovascular disease
Diabetes Cancer
Liver disease
Peripheral vascular disease Chronic kidney diseaseb
Hypertension
Hematuria Proteinuria
Major respiratory infection
Major genitourinary/gastrointestinal infection Major skin/soft tissue infection
Charlson comorbidity index, mean (SD), score
42 (41.2) 29 (28.4)
12 (11.8) 31 (30.4)
14 (13.7)
47 (46.1) 43 (42.2)
14 (13.7)
2 (2.0) 22 (21.6)
77 (75.5)
28 (27.5) 0 (0)
67 (65.7)
24 (23.5) 38 (37.3)
2.9 (2.4)
45 (44.1) 30 (29.4)
15 (14.7) 32 (31.4)
18 (17.6)
49 (48.0) 46 (45.1)
17 (16.7)
4 (3.9) 23 (22.5)
75 (73.5)
28 (27.5) 1 (1.0)
69 (67.6)
23 (22.5) 36 (35.3)
3.1 (2.1)
0.06 0.02
0.09 0.02
0.11
0.04 0.06
0.08
0.12 0.02
0.04
0 0.14
0.04
0.02 0.04
0.11
Proceduresd
Angiography
Coronary artery bypass grafting Percutaneous coronary intervention
Valvular surgery
Pacemaker Echocardiography
Electrocardiography
Holter monitor Stress test
Carotid doppler ultrasound
Renal biopsy
14 (13.7)
6 (5.9) 13 (12.7)
5 (4.9)
8 (7.8) 39 (38.2)
94 (92.2)
7 (6.9) 33 (32.4)
15 (14.7)
1 (1.0)
15 (14.7)
10 (9.8) 15 (14.7)
4 (3.9)
10 (9.8) 38 (37.3)
92 (90.2)
7 (6.9) 35 (34.3)
16 (15.7)
4 (3.9)
0.03
0.15 0.06
0.05
0.07 0.02
0.07
0 0.04
0.03
0.19
Procedure or condition during index hospitalization
Sepsis Cardiac surgery
Abdominal aortic aneurysm repair
Mechanical ventilation
18 (17.6) 7 (6.9)
7 (6.9)
52 (51.0)
16 (15.7) 11 (10.8)
6 (5.9)
57 (55.9)
0.05 0.14
0.04
0.1
Laboratory results
Discharge serum creatinine, mean (SD), µmol/L Chronic kidney disease stagee
Stage I
Stage II Stage III
Stage IV
Stage V
188.5 (128.5)
5 (4.9)
18 (17.6) 38 (37.3)
34 (33.3)
7 (6.9)
202.4 (93.9)
3 (2.9)
10 (9.8) 35 (34.3)
47 (46.1)
7 (6.9)
0.12
0.1
0.23 0.06
0.26
0 a All data presented as No. (%) unless otherwise indicated. b In the 5 years preceding hospital admission expressed as median (IQR). c In the 5 years preceding the hospital discharge date except chronic kidney disease which had a lookback period of 5 years preceding the hospital admission date. d In the 5 years preceding hospital discharge date.
eTable 2. Characteristics of hospitalized individuals by group post-matcha

44
4.4.2 Dialysis censored cohort
Repeating the primary analysis while censoring for dialysis yielded an incidence of all-cause
mortality of 7.3 per 100-patient years in patients with follow-up compared to 10.9 per 100
patient-years in those without follow-up. The frequency of all-cause mortality within 2 years
from cohort entry was 14.1% (n=167) and 18.3% (n=217) in those with and without follow-up,
corresponding to a hazard ratio of 0.71 (95%CI 0.58-0.89). This trend was similar to that seen in
the primary analysis.
4.4.3 High Dimensional Propensity Score
The algorithm for the HDPS yielded 8 additional candidate covariates.(Table 10) These included
4 OHIP codes of which three were diagnostic codes and one was a fee/procedural code; and 3
DAD diagnostic codes of which two were fee/procedural and one was diagnostic. Of these
codes, we eliminated all but OHIP codes 531 and 519 as we felt the other candidate covariates
were not likely to be confounders. Including the OHIP diagnostic codes in our PS yielded a
total sample size of 1584 with 782 individuals in the exposed group and 782 individuals in the
unexposed group. Although the standardized differences after matching for each covariate pair
included in our PS were slightly smaller than in our traditional PS, this came at a cost of losing
782 patients (392 in each group). Despite the increased precision afforded by the HDPS, we
abandoned further analysis using this model as we felt it did not substantially add extra
information to our analysis and may have limited our statistical power to detect a difference
between the two groups.

45
Table 10: Additional covariates specified by the high dimensional propensity score.
Dimension Code
Diagnostic code – OHIP
Diagnostic code – OHIP
Diagnostic code – OHIP
Fee code – OHIP
Diagnostic Code – DAD
Fee code – DAD
Fee code – DAD
519 – Other diseases of the respiratory system
531 – Gastric ulcer with or without hemorrhage or perforation
769 – Respiratory distress syndrome
G082 – Continuous venovenous hemodiafiltration
T81 – Complications of procedure, not elsewhere classified
2GM71- Biopsy, bronchus using endoscopic per orifice approach
1OT52 – Draining, abdominal cavity
4.4.4 Test of Specificity
Our test of specificity demonstrated no association between dermatology or psychiatry
follow-up within 90 days of hospital discharge and all-cause mortality (HR 0.81; 95% CI 0.56-
1.19). Similarly there was a non-significant association for the receipt of chronic dialysis (HR
1.5; 95% CI 0.84-1.19). (Table 11)

46
Table 11: Risk of all cause mortality and chronic dialysis for tracer exposure.
Dermatology or Psychiatry Follow-
up
(n=452)
No Dermatology or Psychiatry
Follow-up
(n=452)
Outcome No. of Events (%)
Incidence
Rate Per 100
Person-Years
No. of Events (%)
Incidence
Rate Per 100
Person-Years
Hazard Ratio
(95% Confidence Interval)
All-cause
mortality
49 (10.8) 5.8 64 (14.2) 7.7 0.81 (0.56-
1.19)
Chronic
Dialysis
14 (3.1) 1.7 10 (2.2) 1.2 1.5 (0.84-
4.27)
4.5 Additional Analyses
4.5.1 Healthcare Utilization
Descriptive analysis of health services utilization and cardiac procedures among the matched
cohort failed to demonstrate marked differences in post-hospitalization care between the groups.
Individuals with early nephrologist follow-up after hospitalization did not have increased rates of
hospitalizations, emergency room visits, cardiology visits, neurologist visits, or cardiac
procedures. Notably, individuals with nephrology follow-up did have an increased number of
subsequent nephrology visits (median 2 visits versus 0 visits) and internist visits (7 visits versus
4 visits). (Table 12) The time from first nephrology consultation to initiation of dialysis was 372
days (±202) in those with early nephrology consultation versus 94 days (±166) in those without
early consultation. Every patient initiating chronic dialysis had a nephrology consultation prior
to this.

47
Table 12: Characteristics of post- discharge health services utilization and procedures in
matched cohort.
Characteristic
No Nephrology
Follow-up
(n=1184)
Nephrology
Follow-up
(n=1184)
Absolute
Standardized
Difference
Measures of healthcare access, median (IQR)
Number of hospitalizations
Number of emergency visits
Number of GP visits
Number of internist visits
Number of cardiology visits
Number of nephrology visits
0 (0-2)
1 (0-3)
20 (9-38)
4 (0-12)
0 (0-2)
0 (0-1)
0 (0-1)
1 (0-4)
18 (9-32)
7 (2-17)
0 (0-2)
2 (0-6)
0.04
0.05
0.13
0.23
0
0.3
Procedure, n (%)
Angiography
Coronary artery bypass grafting
Percutaneous coronary intervention
Valvular surgery
Pacemaker
Echocardiography
Electrocardiography
Holter monitor
Stress test
Carotid doppler ultrasound
Renal biopsy
67 (5.7)
6 (0.5)
38 (3.2)
5 (0.4)
43 (3.6)
319 (26.9)
715 (60.4)
70 (5.9)
205 (17.3)
63 (5.3)
6 (0.5)
68 (5.7)
8 (0.7)
35 (3.0)
6 (0.5)
32 (2.7)
352 (29.7)
774 (65.4)
75 (6.3)
224 (18.9)
78 (6.6)
5 (0.4)
0
0.02
0.01
0.01
0.05
0.06
0.1
0.02
0.04
0.05
0.01
4.5.2 Unmatched Cohort
There were 399 (25.2%) subjects who had early follow-up with a nephrologist and could
not be matched to a suitable control.(Table 13) The unmatched group had a much higher
proportion of patients with a history of chronic kidney disease (45.6% vs. 17.3%) and previous
nephrology visits (66.9% versus 27.2%). Their frequency of all-cause mortality and receipt of
chronic dialysis were 17.5% (70 patients) and 12.8% (51 patients) respectively, which were
higher than for the 1184 matched patients.

48
Table 13: Characteristics of matched versus unmatched cohort.
Characteristic
Nephrology Follow-up
Unmatched
(n=399)
Nephrology Follow-up
Matched
(n=1184)
Demographics
Age, mean (SD), y
Female gender
60.4 (16.5)
160 (40.1)
61.0 (16.5)
473 (39.9)
Low income quintile
Rural residence
102 (25.6)
44 (11.0)
280 (23.6)
170 (14.4)
Distance from nearest dialysis unit (km)
0-50
51-150
151-300
>300
382 (95.7)
15 (3.8)
1 (0.3)
1 (0.3)
1072 (90.5)
99 (8.4)
7 (0.6)
6 (0.5)
Hospital type
Teaching hospital
Healthcare access in the 5 y preceding hospital admission date
Number of hospitalizations
Number of emergency visits
Number of GP visits
Number of internist visits
Number of cardiology visits
Number of patients with nephrology visits, mean
121 (30.3)
1 (0-2)
2 (1-5)
42 (23-73)
11 (3-27)
1 (0-3)
267 (66.9)
535 (45.2)
1(0-2)
2 (1-5)
39 (18-68)
6 (1-17)
0 (0-3)
322 (27.2)
Comorbid disease in the 5 y preceding hospital discharge dateb
Myocardial Infarction
Coronary artery disease
Cardiac dysrythmias
Heart failure
Cerebrovascular disease
Diabetes
Cancer
Liver disease
Peripheral vascular disease
Chronic kidney diseaseb
Hypertension
Hematuria
Proteinuria
Major respiratory infection
Major genitourinary/gastrointestinal infection
Major skin/soft tissue infection
Charlson comorbidity index, mean (SD), score
150 (37.6)
139 (38.4)
51 (12.8)
144 (36.1)
34 (8.5)
190 (47.6)
144 (36.1)
40 (10.0)
15 (3.8)
182 (45.6)
315 (78.9)
134 (33.6)
3 (0.8)
243 (60.9)
75 (18.8)
99 (24.8)
3.0 (2.3)
514 (43.4)
456 (38.5)
155 (13.1)
429 (36.2)
189 (16.0)
517 (43.7)
440 (37.2)
164 (13.9)
41 (3.5)
205 (17.3)
816 (68.9)
345 (29.1)
8 (0.7)
742 (62.7)
279 (23.6)
344 (29.1)
2.9 (2.2)
Procedures in the 5 y preceding hospital discharge date
Angiography
Coronary artery bypass grafting
Percutaneous coronary intervention
Valvular surgery
Pacemaker
Echocardiography
Electrocardiography
Holter monitor
Stress test
Peripheral vascular procedures
Carotid doppler ultrasound
Carotid endarderectomy
Renal biopsy
67 (16.8)
27 (6.8)
62 (15.5)
10 (2.5)
24 (6.0)
203 (50.9)
362 (90.7)
65 (16.3)
168 (42.1)
9 (2.3)
85 (23.1)
9 (0.8)
119 (29.8)
226 (19.1)
114 (9.6)
209 (17.7)
56 (4.7)
70 (5.9)
483 (40.8)
1000 (84.5)
123 (10.4)
378 (31.9)
17 (1.4)
177( 14.9)
7 (0.6)
49 (4.1)
Procedure or condition during index hospitalization
Sepsis
Cardiac surgery
Abdominal aortic aneurysm repair
Mechanical ventilation
13 (3.3)
20 (5.0)
4 (1.0)
52 (13.0)
183 (15.5)
121 (10.4)
33 (2.8)
550 (46.5)
a All data presented as No. (%) unless otherwise indicated.
b Chronic kidney disease lookback period of 5 years preceding the hospital admission date.

49
Chapter 5
Discussion
The purpose of this chapter is to:
Discuss the major findings of the study.
Discuss the strengths of the study.
Discuss the limitations of the study.
Discuss the implications of the study.
5.1 Major Findings
In this large population-based cohort study of survivors of acute kidney injury requiring in-
hospital dialysis, we have demonstrated that a visit with a nephrologist within 90 days of
discharge was associated with a 24% lower mortality rate at 2 years (HR 0.73; 95% CI 0.63-
0.93). This finding was consistent among all important subgroups. Follow-up was also
associated with a statistically significant increase in the rate of chronic dialysis (HR 2.71; 95%
CI 1.76-4.19) within 2 years.
Sensitivity analysis comprising 530 patients with a serum creatinine measurement at time
of discharge confirmed our primary findings of decreased mortality and increased need for
chronic dialysis among those with follow-up compared to those without follow-up, although
these results were not statistically significant [(mortality: HR 0.84; 95% CI 0.43-1.64) and
(chronic dialysis: HR 1.50; 95% CI 0.25-8.90)]. Our sensitivity analysis also demonstrated that
the mortality benefit imparted by follow-up extends beyond those patients who received chronic
dialysis.

50
5.2 Interpretation
The benefit of specialist follow-up on important clinical outcomes has been well
established for an array of acute conditions across many disciplines. However, aside from a
single case-series by Khan et al.95
, the impact of nephrologist follow-up in survivors of AKI has
not been studied. Khan described the effect of post-discharge follow up with a nephrologist in
patients who were hospitalized with AKI of varying severity at a single centre in the United
Kingdom during the period 1989-1990. Among the 310 patients with AKI studied, those
classified as ―high-risk‖ based on clinical and demographic characteristics demonstrated a
survival benefit at two years. Despite this result, Khan’s study had many limitations, including
its single centre and small sample size, arbitrary definition for AKI, and its failure to account for
potential confounders given its case series design. Furthermore, not all patients in the ―high
risk‖ subgroup had dialysis requiring AKI. As such, it was difficult to draw any meaningful
conclusions from Khan’s study.
In contrast, our study was designed to evaluate the effect of early follow-up with a
nephrologist on the long-term outcomes of AKI among survivors of AKI receiving temporary
dialysis in a large population with universal access to healthcare. Similar to previous studies of
AKI survivors,3;6;46
patients in our matched cohort possessed a large burden of comorbid illness.
Some historical reports have demonstrated that referral of such patients to a nephrologist may be
considered futile by some practitioners thereby leading to selection bias whereby healthier
patients are selectively referred.96;97
To mitigate the impact of the inevitable bias associated with
referral practices, we matched patients who received nephrology follow-up with those who did
not using a propensity score. To further reduce the possibility of survivor-treatment bias, we also
required a 90-day period following hospital discharge in which an individual survived and was
free of dialysis. We expected that this time period would appropriately exclude individuals with
a high burden of disease in whom early nephrology visit would be of little impact.
We demonstrated that follow-up with a nephrologist after an episode of severe AKI was
associated with decreased mortality within 2 years. While the mechanism underlying this
association is uncertain, a possible explanation is that follow-up may have enhanced the quality
of care of survivors by targeting the maladaptive physiological changes that ensue as a
consequence of AKI.

51
Basic science data has shown that in the kidney, ischemia-reperfusion injury causes
permanent histological changes, including interstitial fibrosis and loss of the renal vasculature,
which occur even if there is recovery of renal function.58;98;99
In time, these changes lead to
functional impairments such as proteinuria and hypertension which promote deterioration of
kidney function and cardiovascular mortality.47;56;100
The degree of structural and functional
changes in the kidney correlate with the severity of the episode of AKI, such that survivors of
AKI requiring dialysis possess the highest risk of progression to CKD, dialysis and mortality.101
Even in patients without a history of CKD, defined as an eGFR > 60 ml/min, dialysis requiring
AKI is associated with a 500 fold increased risk of progressing to Stage 4 CKD.45
Nephrologists may be uniquely positioned to attenuate these risks and manage the
complications that ensue from progressive renal decline. While internists are well versed in the
management of hypertension and hyperlipidemia in patients with renal dysfunction, the potential
value added by nephrology care is the management of the anemia, acidemia, electrolyte
disorders, malnutrition and bone disease that accompany renal decline; as well as the preparation
for ESRD. Indeed, interventions targeting these conditions have been found to reduce mortality
and preserve kidney function.102-107
Unfortunately, our study was not designed to measure these
processes of care, and therefore, the impact of these interventions is merely speculative.
Additionally, early follow-up with a nephrologist may allow for the timely initiation of
dialysis, possibly with permanent vascular access in place among select patients. In the
predialysis population, delayed nephrology care is associated with several unfavorable outcomes.
It may lead to reduced access to peritoneal dialysis (PD), which may impact on the quality of life
of patients.108
Moreover, it may also restrict access to kidney transplantation, which may
decrease patient survival and quality of life.109;110
Among patients who start hemodialysis,
delayed nephrological care is associated with increased rates of dialysis initiation through a
central venous catheters (CVCs) instead of arteriovenous fistulas (AVFs) or grafts.111;112
Initiation of dialysis with CVCs is associated with an increased risk of mortality, compared to
initiation with an AVF or graft.113;114
Patients with CKD who consult a nephrologist relatively
later or infrequently also experience a considerable excess mortality rate after starting
maintenance dialysis, especially during the first few months of dialysis initiation.115

52
In our study, individuals who had early nephrology follow-up had higher rates of
initiation of chronic dialysis, which may be attributed primarily to the timely initiation of
dialysis. As demonstrated in our sensitivity analysis patients with follow-up tended to have
higher serum creatinine levels at the time of discharge. In fact, a majority of these patients had
Stage IV and V CKD and therefore were at higher risk of having uremic symptoms,
hyperkalemia and volume overload and therefore were more likely to start dialysis in a timely
manner.
However, there are other reasons which may explain the higher rate of chronic dialysis
among survivors with nephrology follow-up. First, our inability to adjust for discharge serum
creatinine for our entire matched cohort may have led to confounding by indication whereby
patients with higher discharge creatinine values and thereby higher risk for progression to
chronic dialysis, were preferentially referred to a nephrologist. Another possibility is that
interventions undertaken by nephrologists, such as initiation of blockers of the renin-angiotensin
system or diuretics, may have hastened the decline in renal function in survivors. Patients with
CKD are at higher risk of developing AKI.116
In our study, patients with nephrology follow-up
had an increased burden of CKD, as demonstrated by our sensitivity analysis; therefore, they
were more likely to develop subsequent episodes of AKI which may have been severe enough to
require initiation of chronic dialysis. Furthermore, this group may have had greater access to
dialysis services, which may have hastened the initiation of dialysis. It has been recently shown
that between 1996 and 2006 patients aged greater than 65 had initiated dialysis with increasingly
preserved kidney function, from an estimated eGFR of 8 ml/min in 1996 to 12 ml/min in 2006.117
Although the timely initiation of dialysis may have contributed to the decreased mortality
among patients with follow-up with a nephrologist seen in our study, our sensitivity analysis
demonstrated that the survival benefit seen in those with early follow-up extended beyond those
patients initiated on chronic dialysis. This implies that the benefits conferred by nephrological
follow-up are not just related to dialysis initiation, but to other processes of care.
Moreover, patients with nephrologist follow-up may also have benefited from improved
access to specialist care for comorbid conditions such as diabetes, coronary artery disease and
COPD. Our descriptive analysis of post hospitalization healthcare utilization showed that
patients with nephrologist follow-up had more visits with internists in the ensuing two years.

53
Combined care among nephrologists, internists, and primary care practitioners may lead to
better management of common coexisting conditions such as coronary artery disease and
diabetes, as well as timely referral for lifesaving medical procedures such as coronary artery
bypass and revascularization.68;107
Indeed, the merits of combined care on survival have been
demonstrated in multiple disciplines including nephrology.64;68;118
Although we found no
difference in the receipt of cardiac medical procedures between the two groups after discharge,
the number of events was low. Moreover, there may have been other lifesaving interventions that
we did not account for in our descriptive analysis that may have impacted on the survival benefit.
On a similar note, the timing of follow-up may also be an important determinant of
patient survival. Ishani et al. recently demonstrated that the risk of adverse events related to an
episode of AKI is greatest within the first 3 to 24 months after the episode.8 This may be related
to the initiation of new medications, alterations in usual medications, or comorbid conditions,
such as cardiac disease.119
Studies in other medical specialties have also corroborated the
importance of the timing of follow-up.69;120;121
For example, in patients with congestive heart
failure, follow-up by a cardiologist within 2 weeks of hospital discharge for a heart failure
admission was associated with a significant decrease in 30-day readmission and mortality.69
As
such, our 90 day follow-up period may have allowed for the early identification of high-risk
individuals and therefore timely introduction of interventions, which may have led to our
observed survival benefit.
Finally, improvements in continuity of care in patients with follow-up may have
contributed to the survival benefit demonstrated. Continuity of care involves three inclusive
dimensions—continuity in information, continuity in management, and continuity in the patient-
physician relationship.122
It is especially important for patients with a large burden of chronic
disease as they are most likely to benefit from informed management and shared decision
making among their healthcare providers.123
There are numerous benefits to continuity of care
including: improved patient satisfaction, increased use of appropriate preventive health services,
greater medication adherence, lower hospitalization rates, and lower cost. In the field of
nephrology, continuity of care can also impart a graded survival benefit commensurate with
increasing nephrology visits, especially in patients with CKD not on dialysis. 118
Our
descriptive analysis found that patients with follow-up with a nephrologist had more nephrology

54
visits over the ensuing two years, which may have improved their quality of care and
contributed to their survival benefit.
5.3 Strengths
Our study has several strengths. First, it is a novel study that uses a population-based
design to determine the benefit of early follow-up with a nephrologist in a cohort that has the
highest risk for progression to CKD and death among AKI survivors. The use of a population-
based design allowed us to capture a large sample size of survivors of severe AKI and adequately
power our study for our primary outcome.
Second, we used rigorous propensity score methods to minimize selection bias and
undertook multiple sensitivity analyses to demonstrate our findings are robust.
We also excluded patients who were readmitted, required dialysis or died within 90 days of
discharge. Exclusion of patients who had received dialysis within 90 days of discharge was
important all these patients had seen a nephrologist for this procedure to be initiated. Including
them in the cohort would had led to reverse causality whereby the need for dialysis prompted
nephrology follow-up.
Finally, our study design protected against immortal time bias.124
Immortal time refers
to a span of time in the observation or follow-up period of a cohort during which the outcome
under study could not have occurred. It usually occurs with the passing of time before a subject
initiates a given exposure. While a subject is not truly immortal during this time span, the subject
necessarily had to remain event free until start of exposure to be classified as exposed. In our
study, all patients had to survive to 90 days post discharge and had to have follow-up with a
nephrologist prior to this time, which ensured that no immortal time bias exists.
5.4 Limitations
Our study has a number of limitations. First, as an observational study, our results demonstrate
an association but do not prove causation. While randomized control trials are best suited to
demonstrate causality, our population is of sufficiently high-risk that a randomized study design

55
would be both unfeasible and unethical. However, given that we studied a selected population
with the most severe form of AKI, our results may not be generalizable to patients with less
severe episodes of AKI. As such, similar cohort studies using different samples of patients with
varying degrees of AKI are needed to confirm our findings.
Second, despite our rigorous matching and adjustment on important variables,
confounding by indication could still occur due to unmeasured confounders. We employed
propensity score modeling as a means to adjust for a large amount of confounders. While
propensity scores are a powerful method to minimize bias in observational trials, they are subject
to bias due to unmeasured confounders. 85
Indeed, in our primary analysis we were unable to
account for potential unmeasured confounders including laboratory data of which residual
kidney function at the time of discharge was most important. As demonstrated in our sensitivity
analysis, patients with higher discharge serum creatinine, were more likely to be referred for
nephrology follow-up. This is in contrast to some studies which have demonstrated that an
inverse referral bias may exist whereby physicians would be less willing to refer some patients
with high creatinine levels to nephrologists. According to physicians following this philosophy
of care, some patients with high creatinines may not benefit from nephrological care including
dialysis as they possess a large burden of comorbid illness and referral for nephrological care
would bring undue hardship without any demonstrable benefit. While this may be plausible, our
sensitivity analysis does not confirm this practice is occurring to a large extent in our cohort.
Furthermore, our propensity score methods were able to account for a myriad of comorbid
conditions in the two groups that may have affected referral practices. As CKD is a potent risk
factor for mortality, the inability to adjust for this confounder using discharge serum creatinine
values in our primary analysis should have tended to bias the hazard ratio for mortality towards
the null hypothesis.47
However, we demonstrated a robust relationship between nephrology
follow-up and mortality, implying that the magnitude of the protective effect of early follow-up
may be even greater than demonstrated.
Furthermore, our test of specificity using a tracer exposure was able to mitigate further
concerns regarding residual confounding as demonstrated by a lack of a statistically significant
association between psychiatry or dermatology consultation and mortality. This group of
patients was fundamentally different than our matched cohort on a number of baseline

56
characteristics – they were younger, had substantially less comorbid illness (including CKD)
and procedures; and had less severe hospital admissions. Given this, one would have expected a
statistically significant decrease in mortality in this group, which was not the case.
Third, we completed our study using administrative data, and had to rely on diagnosis
and procedure codes to identify exposure, outcome and covariates. As such, there may be issues
related to the validity of our exposure, cohort and the variables included in our propensity score.
As previously mentioned, the primary exposure for this study was at least one outpatient
nephrology consultation within 90 days of discharge from the index hospitalization defined using
the OHIP database. In the OHIP database, the specialty code for nephrology (specialty code 16)
was introduced in October 2009. Prior to this, nephrologists were coded in the same category as
internal medicine (specialty code 13). This required us to use an algorithm developed by Wald et
al., which has face validity, but has not been formally validated, to define a nephrologist. 38
We
compared our results to those obtained using a different algorithm for defining a nephrologist
using OHIP data by Jain et al., which has been used in a previous study. 82
Jain et al.’s algorithm
identified nearly similar numbers of nephrologists in Ontario when compared to the ICES
Physicians Database (IPDB), as the gold standard, for the years 1999-2005. Using kappa
statistics we demonstrated a high degree of agreement between our definition of nephrologist and
Jain et al.’s definition with the IPDB. However, our definition yielded a slightly greater number
of exposed individuals compared to Jain et al.’s definition.
The use of administrative data may also misclassify individuals with AKI, as this code in
isolation has fairly low sensitivity but high specificity. However, the combination of a
diagnostic code for AKI and a procedure code for dialysis demonstrated greater than 90%
sensitivity and specificity in a recent validation study13
, which mitigates any misclassification of
our cohort.
Our secondary outcomes of chronic dialysis and AKI may have also been susceptible to
misclassification. Although we used widely accepted definition for chronic dialysis that has
been employed in many studies, we may have misclassified individuals who truly developed end
stage renal disease but died in the first 90 days after commencing chronic dialysis.3;125
Similarly,
as previously mentioned AKI has poor sensitivity (19-28%) but excellent specificity. As such,

57
patients with true AKI may be misclassified as not having this condition and thus
underrepresented in administrative databases.
Furthermore, administrative databases show poor accuracy in defining certain comorbid
conditions which we included in our propensity score. For example, a recent systematic review
of validating administrative data codes for AKI, CKD and dialysis demonstrated that chronic
kidney disease is poorly sensitive but highly specific (19-80% Sensitivity; 97-100%
Specificity).126
As with AKI, administrative databases may be underreporting the true number of
patients with this condition.
Fourth, we were unable to explain the process(es) of care leading to the mortality benefit
demonstrated in our study, despite examining the patterns of healthcare utilization between
exposed and unexposed patients. Future work is needed to elucidate the mechanism by which
nephrologist’s impact on mortality in survivors of severe AKI.
Finally, the estimated association between early nephrology follow-up and outcomes are
valid for the matched cohort but not necessarily for the unmatched cohort. Unmatched patients
who underwent follow-up had higher rates of chronic kidney disease, previous nephrology visits,
and had a higher risk of mortality and chronic dialysis than the matched cohort. These
characteristics made them difficult to match. As such, the advantage of early nephrology follow-
up may not be generalizable to the entire spectrum of patients with dialysis-requiring AKI.
5.5 Implications and Future Directions
We have demonstrated that in patients affected by the most severe form of AKI, that which
requires dialysis, there is an increased risk of mortality within 2 years that may be mitigated with
appropriate nephrology follow-up. Currently, approximately 25% of Medicare patients
hospitalized for an episode of AKI are seen by a nephrologist within 30 days of discharge. This
increases to almost 40% within 180 days after hospitalization. In the non-Medicare population,
only 25% of patients are referred to a nephrologist post hospitalization complicated by AKI. 23
This trend may be leading to missed opportunities for intervention especially among patients at
high risk of progressive renal decline and death.

58
Despite the noted benefits of nephrology follow-up after an episode of AKI, one must
keep in mind the public health ramifications of such an intervention. Given the limited pool of
nephrologists in Canada, there is a strong potential to overwhelm this already scarce healthcare
resource by a significant increase in the number of post-AKI nephrology referrals. In fact, such a
trend was seen after automated laboratory reporting of estimated glomerular filtration rate
(eGFR) was introduced in Ontario and Alberta.82;127
As such, the development of a risk prediction rule for mortality and CKD progression in
AKI survivors is of paramount importance. Such a rule would accurately predict the risk of
mortality and CKD progression and thereby facilitate individualized decision making, enabling
timely and appropriate care. This rule would also help direct scare resources, costly testing and
interventions. Although predictive rules of CKD progression are in widespread use, only one has
been developed for a cohort of AKI survivors. 45;128-130
That rule, by Chawla and colleagues, was
developed using a fairly limited set of covariates in a fairly homogeneous population of United
States veterans.45
Therefore, it might not perform accurately in other settings. Furthermore,
there are currently no predictive rules in use that estimate the risk of mortality in AKI survivors.
Given these points, physicians must often make ad hoc decisions about which survivors of AKI
to refer to nephrologists for follow-up based on their personal determination of risk. This is
undoubtedly a dangerous task especially with a heterogeneous and sick patient population.
Accordingly, further studies are necessary to elucidate the factors that predict progression
to CKD, chronic dialysis and mortality among survivors of AKI and develop an integrative
prediction rule that will appropriately stratify these patients according to their level of risk. This
will not only protect scarce health resources, but should also improve patient outcomes. Once
the prediction rule is developed and validated, subsequent work can begin on identifying factors
that may ameliorate the long-term complications of AKI.
Conclusion
Survivors of acute kidney injury requiring dialysis who receive post-discharge follow-up with a
nephrologist appear to have decreased mortality but increased progression to chronic dialysis

59
within 2 years. Our findings expand on those found in other disciplines, that is, improved
continuity of care among specialists translates into improved survival after hospital discharge.

60
Reference List
(1) Chertow GM, Burdick E, Honour M, Bonventre JV, Bates DW. Acute kidney injury,
mortality, length of stay, and costs in hospitalized patients. J Am Soc Nephrol
2005;16:3365-3370.
(2) Liangos O, Wald R, O'Bell JW, Price L, Pereira BJ, Jaber BL. Epidemiology and
outcomes of acute renal failure in hospitalized patients: a national survey. Clin J Am Soc
Nephrol 2006;1:43-51.
(3) Wald R, Quinn RR, Luo J et al. Chronic dialysis and death among survivors of acute
kidney injury requiring dialysis. JAMA 2009;302:1179-1185.
(4) Lo LJ, Go AS, Chertow GM et al. Dialysis-requiring acute renal failure increases the risk
of progressive chronic kidney disease. Kidney Int 2009;76:893-899.
(5) Coca SG, Yusuf B, Shlipak MG, Garg AX, Parikh CR. Long-term risk of mortality and
other adverse outcomes after acute kidney injury: a systematic review and meta-analysis.
Am J Kidney Dis 2009;53:961-973.
(6) Lafrance JP, Miller DR. Acute kidney injury associates with increased long-term
mortality. J Am Soc Nephrol 2010;21:345-352.
(7) Bagshaw SM, Laupland KB, Doig CJ et al. Prognosis for long-term survival and renal
recovery in critically ill patients with severe acute renal failure: a population-based study.
Crit Care 2005;9:R700-R709.
(8) Ishani A, Nelson D, Clothier B et al. The magnitude of acute serum creatinine increase
after cardiac surgery and the risk of chronic kidney disease, progression of kidney
disease, and death. Arch Intern Med 2011;171:226-233.
(9) National Institutes of Health, National Institues of Diabetes and Digestive and Kidney
Diseases. U.S. Renal Data System, USRDS 2010 Annual Data Report: Atlas of Chronic
Kidney Disease and End-Stage Renal Disease in the United States. 2010. Bethesda, MD.
(10) Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to
estimate glomerular filtration rate from serum creatinine: a new prediction equation.
Modification of Diet in Renal Disease Study Group. Ann Intern Med 1999;130:461-470.
(11) Ando M, Mori J, Ohashi K et al. A comparative assessment of the RIFLE, AKIN and
conventional criteria for acute kidney injury after hematopoietic SCT. Bone Marrow
Transplant 2010;45:1427-1434.

61
(12) Cuhaci B. More data on epidemiology and outcome of acute kidney injury with AKIN
criteria: benefits of standardized definitions, AKIN and RIFLE classifications. Crit Care
Med 2009;37:2659-2661.
(13) Waikar SS, Wald R, Chertow GM et al. Validity of International Classification of
Diseases, Ninth Revision, Clinical Modification Codes for Acute Renal Failure. J Am Soc
Nephrol 2006;17:1688-1694.
(14) Bagshaw SM, George C, Bellomo R. Early acute kidney injury and sepsis: a multicentre
evaluation. Crit Care 2008;12:R47.
(15) Weisbord SD, Mor MK, Resnick AL, Hartwig KC, Palevsky PM, Fine MJ. Incidence and
outcomes of contrast-induced AKI following computed tomography. Clin J Am Soc
Nephrol 2008;3:1274-1281.
(16) Thakar CV, Kharat V, Blanck S, Leonard AC. Acute kidney injury after gastric bypass
surgery. Clin J Am Soc Nephrol 2007;2:426-430.
(17) Wald R, Waikar SS, Liangos O, Pereira BJ, Chertow GM, Jaber BL. Acute renal failure
after endovascular vs open repair of abdominal aortic aneurysm. J Vasc Surg
2006;43:460-466.
(18) Hsu CY, McCulloch CE, Fan D, Ordonez JD, Chertow GM, Go AS. Community-based
incidence of acute renal failure. Kidney Int 2007;72:208-212.
(19) Bagshaw SM, George C, Dinu I, Bellomo R. A multi-centre evaluation of the RIFLE
criteria for early acute kidney injury in critically ill patients. Nephrol Dial Transplant
2008;23:1203-1210.
(20) Kwon SH, Noh H, Jeon JS, Kim Y, Han DC. An assessment of AKIN criteria for
hospital-acquired acute kidney injury: a prospective observational cohort study. Nephron
Clin Pract 2010;116:c217-c223.
(21) Levy EM, Viscoli CM, Horwitz RI. The effect of acute renal failure on mortality. A
cohort analysis. JAMA 1996;275:1489-1494.
(22) Hou SH, Bushinsky DA, Wish JB, Cohen JJ, Harrington JT. Hospital-acquired renal
insufficiency: a prospective study. Am J Med 1983;74:243-248.
(23) Ali T, Khan I, Simpson W et al. Incidence and outcomes in acute kidney injury: a
comprehensive population-based study. J Am Soc Nephrol 2007;18:1292-1298.
(24) Lassnigg A, Schmid ER, Hiesmayr M et al. Impact of minimal increases in serum
creatinine on outcome in patients after cardiothoracic surgery: do we have to revise
current definitions of acute renal failure? Crit Care Med 2008;36:1129-1137.
(25) Hoste EA, Clermont G, Kersten A et al. RIFLE criteria for acute kidney injury are
associated with hospital mortality in critically ill patients: a cohort analysis. Crit Care
2006;10:R73.

62
(26) Iglesias JI, DePalma L, Hom D, Antoniotti M, Ayoub S, Levine JS. Predictors of
mortality in adult patients with congestive heart failure receiving nesiritide--retrospective
analysis showing a potential adverse interaction between nesiritide and acute renal
dysfunction. Nephrol Dial Transplant 2008;23:144-153.
(27) Mangano CM, Diamondstone LS, Ramsay JG, Aggarwal A, Herskowitz A, Mangano
DT. Renal dysfunction after myocardial revascularization: risk factors, adverse outcomes,
and hospital resource utilization. The Multicenter Study of Perioperative Ischemia
Research Group. Ann Intern Med 1998;128:194-203.
(28) Abelha FJ, Botelho M, Fernandes V, Barros H. Determinants of postoperative acute
kidney injury. Crit Care 2009;13:R79.
(29) Lins RL, Elseviers MM, Daelemans R. Severity scoring and mortality 1 year after acute
renal failure. Nephrol Dial Transplant 2006;21:1066-1068.
(30) Liano F, Pascual J. Epidemiology of acute renal failure: a prospective, multicenter,
community-based study. Madrid Acute Renal Failure Study Group. Kidney Int
1996;50:811-818.
(31) Morgera S, Kraft AK, Siebert G, Luft FC, Neumayer HH. Long-term outcomes in acute
renal failure patients treated with continuous renal replacement therapies. Am J Kidney
Dis 2002;40:275-279.
(32) Lafrance JP, Miller DR. Defining acute kidney injury in database studies: the effects of
varying the baseline kidney function assessment period and considering CKD status. Am
J Kidney Dis 2010;56:651-660.
(33) Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P. Acute renal failure - definition,
outcome measures, animal models, fluid therapy and information technology needs: the
Second International Consensus Conference of the Acute Dialysis Quality Initiative
(ADQI) Group. Crit Care 2004;8:R204-R212.
(34) Bagshaw SM, Laupland KB, Doig CJ et al. Prognosis for long-term survival and renal
recovery in critically ill patients with severe acute renal failure: a population-based study.
Crit Care 2005;9:R700-R709.
(35) Tolwani AJ, Campbell RC, Stofan BS, Lai KR, Oster RA, Wille KM. Standard versus
high-dose CVVHDF for ICU-related acute renal failure. J Am Soc Nephrol
2008;19:1233-1238.
(36) Uchino S, Bellomo R, Morimatsu H et al. Continuous renal replacement therapy: a
worldwide practice survey. The beginning and ending supportive therapy for the kidney
(B.E.S.T. kidney) investigators. Intensive Care Med 2007;33:1563-1570.
(37) Schiffl H. Renal recovery from acute tubular necrosis requiring renal replacement
therapy: a prospective study in critically ill patients. Nephrol Dial Transplant
2006;21:1248-1252.

63
(38) Wald R, Quinn RR, Luo J et al. Chronic dialysis and death among survivors of acute
kidney injury requiring dialysis. JAMA 2009;302:1179-1185.
(39) Bagshaw SM. Short- and long-term survival after acute kidney injury. Nephrol Dial
Transplant 2008;23:2126-2128.
(40) Thakar CV, Christianson A, Freyberg R, Almenoff P, Render ML. Incidence and
outcomes of acute kidney injury in intensive care units: a Veterans Administration study.
Crit Care Med 2009;37:2552-2558.
(41) Palevsky PM, Zhang JH, O'Connor TZ et al. Intensity of renal support in critically ill
patients with acute kidney injury. N Engl J Med 2008;359:7-20.
(42) Liu KD, Lo L, Hsu CY. Some methodological issues in studying the long-term renal
sequelae of acute kidney injury. Curr Opin Nephrol Hypertens 2009;18:241-245.
(43) Hsu CY, Chertow GM, McCulloch CE, Fan D, Ordonez JD, Go AS. Nonrecovery of
kidney function and death after acute on chronic renal failure. Clin J Am Soc Nephrol
2009;4:891-898.
(44) Lo LJ, Go AS, Chertow GM et al. Dialysis-requiring acute renal failure increases the risk
of progressive chronic kidney disease. Kidney Int 2009;76:893-899.
(45) Chawla LS, Amdur RL, Amodeo S, Kimmel PL, Palant CE. The severity of acute kidney
injury predicts progression to chronic kidney disease. Kidney Int 2011;79:1361-1369.
(46) Ishani A, Xue JL, Himmelfarb J et al. Acute kidney injury increases risk of ESRD among
elderly. J Am Soc Nephrol 2009;20:223-228.
(47) Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the
risks of death, cardiovascular events, and hospitalization. N Engl J Med 2004;351:1296-
1305.
(48) Cerda J, Lameire N, Eggers P et al. Epidemiology of acute kidney injury. Clin J Am Soc
Nephrol 2008;3:881-886.
(49) Amdur RL, Chawla LS, Amodeo S, Kimmel PL, Palant CE. Outcomes following
diagnosis of acute renal failure in U.S. veterans: focus on acute tubular necrosis. Kidney
Int 2009;76:1089-1097.
(50) Liano F, Felipe C, Tenorio MT et al. Long-term outcome of acute tubular necrosis: a
contribution to its natural history. Kidney Int 2007;71:679-686.
(51) James MT, Ghali WA, Knudtson ML et al. Associations between acute kidney injury and
cardiovascular and renal outcomes after coronary angiography. Circulation
2011;123:409-416.
(52) Lopes JA, Fernandes P, Jorge S et al. Long-term risk of mortality after acute kidney
injury in patients with sepsis: a contemporary analysis. BMC Nephrol 2010;11:9.

64
(53) Schiffl H, Fischer R. Five-year outcomes of severe acute kidney injury requiring renal
replacement therapy. Nephrol Dial Transplant 2008;23:2235-2241.
(54) Ponte B, Felipe C, Muriel A, Tenorio MT, Liano F. Long-term functional evolution after
an acute kidney injury: a 10-year study. Nephrol Dial Transplant 2008;23:3859-3866.
(55) Basile DP, Donohoe D, Roethe K, Osborn JL. Renal ischemic injury results in permanent
damage to peritubular capillaries and influences long-term function. Am J Physiol Renal
Physiol 2001;281:F887-F899.
(56) Spurgeon-Pechman KR, Donohoe DL, Mattson DL, Lund H, James L, Basile DP.
Recovery from acute renal failure predisposes hypertension and secondary renal disease
in response to elevated sodium. Am J Physiol Renal Physiol 2007;293:F269-F278.
(57) Spurgeon KR, Donohoe DL, Basile DP. Transforming growth factor-beta in acute renal
failure: receptor expression, effects on proliferation, cellularity, and vascularization after
recovery from injury. Am J Physiol Renal Physiol 2005;288:F568-F577.
(58) Venkatachalam MA, Griffin KA, Lan R, Geng H, Saikumar P, Bidani AK. Acute kidney
injury: a springboard for progression in chronic kidney disease. Am J Physiol Renal
Physiol 2010.
(59) Klein CL, Hoke TS, Fang WF, Altmann CJ, Douglas IS, Faubel S. Interleukin-6 mediates
lung injury following ischemic acute kidney injury or bilateral nephrectomy. Kidney Int
2008;74:901-909.
(60) Kelly KJ. Distant effects of experimental renal ischemia/reperfusion injury. J Am Soc
Nephrol 2003;14:1549-1558.
(61) Gerstein HC, Mann JF, Yi Q et al. Albuminuria and risk of cardiovascular events, death,
and heart failure in diabetic and nondiabetic individuals. JAMA 2001;286:421-426.
(62) Cheung AM, Tansey CM, Tomlinson G et al. Two-year outcomes, health care use, and
costs of survivors of acute respiratory distress syndrome. Am J Respir Crit Care Med
2006;174:538-544.
(63) Rothenhausler HB, Ehrentraut S, Stoll C, Schelling G, Kapfhammer HP. The relationship
between cognitive performance and employment and health status in long-term survivors
of the acute respiratory distress syndrome: results of an exploratory study. Gen Hosp
Psychiatry 2001;23:90-96.
(64) Ayanian JZ, Landrum MB, Guadagnoli E, Gaccione P. Specialty of ambulatory care
physicians and mortality among elderly patients after myocardial infarction. N Engl J
Med 2002;347:1678-1686.
(65) Hernandez AF, Greiner MA, Fonarow GC et al. Relationship between early physician
follow-up and 30-day readmission among Medicare beneficiaries hospitalized for heart
failure. JAMA 2010;303:1716-1722.

65
(66) Lin CY, Barnato AE, Degenholtz HB. Physician Follow-Up Visits After Acute Care
Hospitalization for Elderly Medicare Beneficiaries Discharged to Noninstitutional
Settings. J Am Geriatr Soc 2011.
(67) Sharma G, Kuo YF, Freeman JL, Zhang DD, Goodwin JS. Outpatient follow-up visit and
30-day emergency department visit and readmission in patients hospitalized for chronic
obstructive pulmonary disease. Arch Intern Med 2010;170:1664-1670.
(68) Ezekowitz JA, van WC, McAlister FA, Armstrong PW, Kaul P. Impact of specialist
follow-up in outpatients with congestive heart failure. CMAJ 2005;172:189-194.
(69) Hernandez AF, Greiner MA, Fonarow GC et al. Relationship between early physician
follow-up and 30-day readmission among Medicare beneficiaries hospitalized for heart
failure. JAMA 2010;303:1716-1722.
(70) Ayanian JZ, Landrum MB, McNeil BJ. Use of cholesterol-lowering therapy by elderly
adults after myocardial infarction. Arch Intern Med 2002;162:1013-1019.
(71) Juurlink D PCCRCAAPTJLA. Canadian Institute for Health Information Discharge
Abstract Database: A Validation Study. 2006. Toronto, Institute for Clinical
EvaluativeSciences.
(72) Hux JE, Ivis F, Flintoft V, Bica A. Diabetes in Ontario: determination of prevalence and
incidence using a validated administrative data algorithm. Diabetes Care 2002;25:512-
516.
(73) Scales DC, Guan J, Martin CM, Redelmeier DA. Administrative data accurately
identified intensive care unit admissions in Ontario. J Clin Epidemiol 2006;59:802-807.
(74) Jain AK, McLeod I, Huo C et al. When laboratories report estimated glomerular filtration
rates in addition to serum creatinines, nephrology consults increase. Kidney Int
2009;76:318-323.
(75) Moist LM, Richards HA, Miskulin D et al. A validation study of the Canadian Organ
Replacement Register. Clin J Am Soc Nephrol 2011;6:813-818.
(76) Tonelli M, Manns B, Culleton B et al. Association between proximity to the attending
nephrologist and mortality among patients receiving hemodialysis. CMAJ
2007;177:1039-1044.
(77) Oake N, Taljaard M, van WC, Wilson K, Roth V, Forster AJ. The effect of hospital-
acquired Clostridium difficile infection on in-hospital mortality. Arch Intern Med
2010;170:1804-1810.
(78) Molnar AO, Coca SG, Devereaux PJ et al. Statin use associates with a lower incidence of
acute kidney injury after major elective surgery. J Am Soc Nephrol 2011;22:939-946.

66
(79) Hsu CY, Chertow GM, McCulloch CE, Fan D, Ordonez JD, Go AS. Nonrecovery of
kidney function and death after acute on chronic renal failure. Clin J Am Soc Nephrol
2009;4:891-898.
(80) Landoni G, Zangrillo A, Franco A et al. Long-term outcome of patients who require renal
replacement therapy after cardiac surgery. Eur J Anaesthesiol 2006;23:17-22.
(81) Waikar SS, Wald R, Chertow GM et al. Validity of International Classification of
Diseases, Ninth Revision, Clinical Modification Codes for Acute Renal Failure. J Am Soc
Nephrol 2006;17:1688-1694.
(82) Jain AK, McLeod I, Huo C et al. When laboratories report estimated glomerular filtration
rates in addition to serum creatinines, nephrology consults increase. Kidney Int
2009;76:318-323.
(83) Clement FM, James MT, Chin R et al. Validation of a case definition to define chronic
dialysis using outpatient administrative data. BMC Med Res Methodol 2011;11:25.
(84) Quan H, Parsons GA, Ghali WA. Validity of procedure codes in International
Classification of Diseases, 9th revision, clinical modification administrative data. Med
Care 2004;42:801-809.
(85) Rubin DB. The design versus the analysis of observational studies for causal effects:
parallels with the design of randomized trials. Stat Med 2007;26:20-36.
(86) Austin PC. Propensity-score matching in the cardiovascular surgery literature from 2004
to 2006: a systematic review and suggestions for improvement. J Thorac Cardiovasc
Surg 2007;134:1128-1135.
(87) Winkelmayer WC, Kurth T. Propensity scores: help or hype? Nephrol Dial Transplant
2004;19:1671-1673.
(88) Austin PC. An Introduction to Propensity Score Methods for Reducing the Effects of
Confounding in Observational Studies. Multivariate Behav Res 2011;46:399-424.
(89) Scales DC, Guan J, Martin CM, Redelmeier DA. Administrative data accurately
identified intensive care unit admissions in Ontario. J Clin Epidemiol 2006;59:802-807.
(90) Austin PC. Optimal caliper widths for propensity-score matching when estimating
differences in means and differences in proportions in observational studies. Pharm Stat
2010.
(91) Austin PC. Assessing balance in measured baseline covariates when using many-to-one
matching on the propensity-score. Pharmacoepidemiol Drug Saf 2008;17:1218-1225.
(92) Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity
index. J Clin Epidemiol 1994;47:1245-1251.

67
(93) Schneeweiss S, Rassen J. Re: Confounding adjustment via a semi-automated high-
dimensional propensity score algorithm: an application to electronic medical records.
Pharmacoepidemiol Drug Saf 2011;20:1110-1111.
(94) Schneeweiss S, Rassen JA, Glynn RJ, Avorn J, Mogun H, Brookhart MA. High-
dimensional propensity score adjustment in studies of treatment effects using health care
claims data. Epidemiology 2009;20:512-522.
(95) Khan IH, Catto GR, Edward N, Macleod AM. Acute renal failure: factors influencing
nephrology referral and outcome. QJM 1997;90:781-785.
(96) Smith C, Da Silva-Gane M, Chandna S, Warwicker P, Greenwood R, Farrington K.
Choosing not to dialyse: evaluation of planned non-dialytic management in a cohort of
patients with end-stage renal failure. Nephron Clin Pract 2003;95:c40-c46.
(97) Sekkarie MA, Moss AH. Withholding and withdrawing dialysis: the role of physician
specialty and education and patient functional status. Am J Kidney Dis 1998;31:464-472.
(98) Basile DP, Friedrich JL, Spahic J et al. Impaired endothelial proliferation and
mesenchymal transition contribute to vascular rarefaction following acute kidney injury.
Am J Physiol Renal Physiol 2011;300:F721-F733.
(99) Basile DP. Rarefaction of peritubular capillaries following ischemic acute renal failure: a
potential factor predisposing to progressive nephropathy. Curr Opin Nephrol Hypertens
2004;13:1-7.
(100) Sagie A, Larson MG, Levy D. The natural history of borderline isolated systolic
hypertension. N Engl J Med 1993;329:1912-1917.
(101) Golestaneh L, Melamed ML, Hostetter TH. Uremic memory: the role of acute kidney
injury in long-term outcomes. Kidney Int 2009;76:813-814.
(102) de ZD, Lewis EJ, Remuzzi G, Brenner BM, Cooper ME. Renoprotective effects of renin-
angiotensin-system inhibitors. Lancet 2006;367:899-900.
(103) Tonelli M, Isles C, Curhan GC et al. Effect of pravastatin on cardiovascular events in
people with chronic kidney disease. Circulation 2004;110:1557-1563.
(104) Halbesma N, Bakker SJ, Jansen DF et al. High protein intake associates with
cardiovascular events but not with loss of renal function. J Am Soc Nephrol
2009;20:1797-1804.
(105) Einhorn LM, Zhan M, Hsu VD et al. The frequency of hyperkalemia and its significance
in chronic kidney disease. Arch Intern Med 2009;169:1156-1162.
(106) de Brito-Ashurst I, Varagunam M, Raftery MJ, Yaqoob MM. Bicarbonate
supplementation slows progression of CKD and improves nutritional status. J Am Soc
Nephrol 2009;20:2075-2084.

68
(107) Avorn J, Bohn RL, Levy E et al. Nephrologist care and mortality in patients with
chronic renal insufficiency. Arch Intern Med 2002;162:2002-2006.
(108) Stack AG. Determinants of modality selection among incident US dialysis patients:
results from a national study. J Am Soc Nephrol 2002;13:1279-1287.
(109) Winkelmayer WC, Glynn RJ, Levin R, Mittleman MA, Pliskin JS, Avorn J. Late
nephrologist referral and access to renal transplantation. Transplantation 2002;73:1918-
1923.
(110) Boehm M, Winkelmayer WC, Arbeiter K, Mueller T, Aufricht C. Late referral to
paediatric renal failure service impairs access to pre-emptive kidney transplantation in
children. Arch Dis Child 2010;95:634-638.
(111) Avorn J, Winkelmayer WC, Bohn RL et al. Delayed nephrologist referral and inadequate
vascular access in patients with advanced chronic kidney failure. J Clin Epidemiol
2002;55:711-716.
(112) Astor BC, Eustace JA, Powe NR et al. Timing of nephrologist referral and arteriovenous
access use: the CHOICE Study. Am J Kidney Dis 2001;38:494-501.
(113) Perl J, Wald R, McFarlane P et al. Hemodialysis vascular access modifies the association
between dialysis modality and survival. J Am Soc Nephrol 2011;22:1113-1121.
(114) Moist LM, Trpeski L, Na Y, Lok CE. Increased hemodialysis catheter use in Canada and
associated mortality risk: data from the Canadian Organ Replacement Registry 2001-
2004. Clin J Am Soc Nephrol 2008;3:1726-1732.
(115) Winkelmayer WC, Owen WF, Jr., Levin R, Avorn J. A propensity analysis of late versus
early nephrologist referral and mortality on dialysis. J Am Soc Nephrol 2003;14:486-492.
(116) Lafrance JP, Djurdjev O, Levin A. Incidence and outcomes of acute kidney injury in a
referred chronic kidney disease cohort. Nephrol Dial Transplant 2010;25:2203-2209.
(117) Winkelmayer WC, Liu J, Chertow GM, Tamura MK. Predialysis nephrology care of
older patients approaching end-stage renal disease. Arch Intern Med 2011;171:1371-
1378.
(118) Tseng CL, Kern EF, Miller DR et al. Survival benefit of nephrologic care in patients with
diabetes mellitus and chronic kidney disease. Arch Intern Med 2008;168:55-62.
(119) Leendertse AJ, de Koning FH, Goudswaard AN et al. Preventing hospital admissions by
reviewing medication (PHARM) in primary care: design of the cluster randomised,
controlled, multi-centre PHARM-study. BMC Health Serv Res 2011;11:4.
(120) Sharma G, Kuo YF, Freeman JL, Zhang DD, Goodwin JS. Outpatient follow-up visit and
30-day emergency department visit and readmission in patients hospitalized for chronic
obstructive pulmonary disease. Arch Intern Med 2010;170:1664-1670.

69
(121) van WC, Taljaard M, Etchells E et al. The independent association of provider and
information continuity on outcomes after hospital discharge: implications for hospitalists.
J Hosp Med 2010;5:398-405.
(122) Sharma G, Fletcher KE, Zhang D, Kuo YF, Freeman JL, Goodwin JS. Continuity of
outpatient and inpatient care by primary care physicians for hospitalized older adults.
JAMA 2009;301:1671-1680.
(123) Ettner SL. The relationship between continuity of care and the health behaviors of
patients: does having a usual physician make a difference? Med Care 1999;37:547-555.
(124) Shariff SZ, Cuerden MS, Jain AK, Garg AX. The secret of immortal time bias in
epidemiologic studies. J Am Soc Nephrol 2008;19:841-843.
(125) Quinn RR, Laupacis A, Hux JE, Moineddin R, Paterson M, Oliver MJ. Forecasting the
need for dialysis services in ontario, Canada to 2011. Healthc Policy 2009;4:e151-e161.
(126) Vlasschaert ME, Bejaimal SA, Hackam DG et al. Validity of administrative database
coding for kidney disease: a systematic review. Am J Kidney Dis 2011;57:29-43.
(127) Hemmelgarn BR, Zhang J, Manns BJ et al. Nephrology visits and health care resource
use before and after reporting estimated glomerular filtration rate. JAMA 2010;303:1151-
1158.
(128) Tangri N, Stevens LA, Griffith J et al. A predictive model for progression of chronic
kidney disease to kidney failure. JAMA 2011;305:1553-1559.
(129) Conway B, Webster A, Ramsay G et al. Predicting mortality and uptake of renal
replacement therapy in patients with stage 4 chronic kidney disease. Nephrol Dial
Transplant 2009;24:1930-1937.
(130) Levin A. Identification of patients and risk factors in chronic kidney disease--evaluating
risk factors and therapeutic strategies. Nephrol Dial Transplant 2001;16 Suppl 7:57-60.

70
Appendix
APPENDIX 1: DIAGNOSTIC CODES FOR DISEASES/CONDITIONS PERTINENT TO THE STUDY
Condition/Disease ICD-9 ICD-10 Diagnostic type
Procedure Codes
OHIP, CCI, CCP
AK
I R
RT
su
rviv
ors
co
ho
rt
Age ≥ 18 years
No codes for AKI or any form of dialysis in preceding five yrs
Hospital admission with AKI
Dialysis during hospitalization
alive at 90 days post-discharge
no dialysis during the 90-day period after discharge
no rehospitalization for 90 days following discharge
584.5-584.9
669.3, 958.5 634.3, 635.3,
636.3, 637.3
638.3, 639.3
N17.0-N17.9, O08.4, T79.5, O90.4
all R849, R850, G323, G325, G326, G330, G331, G332, G860, G333, G083, G091, G085, G295, G082, G090, G092, G093, G094, G861, G862, G863, G864, G865, G866, G294, G095, G096
CCP: 51.95, 66.98
CCI:
1PZ21HQBR, 1PZ21HPD4
Kid
ney
Tra
nsp
lan
t
exclusion from cohort if received a kidney transplant during the 5 years prior to the index admission
CCP: 6759
CCI: 1PC85LAXXJ
1PC85LAXXK

71
A
ny d
ialy
sis
exclusion from cohort if received any form of dialysis during the 5 years prior to the index admission
R849, R850, G323, G325, G326, G330, G331, G332, G860, G333, G083, G091, G085, G295, G082, G090, G092, G093, G094, G861, G862, G863, G864, G865, G866, G294, G095, G096
CCP: 51.95, 66.98
CCI:
1PZ21HQBR, 1PZ21HPD4
Mech
an
ical
Ven
tila
tio
n
describing a patient’s receipt of mechanical ventilation on an admission of interest (used for matching of cohorts to non-exposed individuals)
G557, G558, G559, G405, G406, G407
Ch
ron
ic K
idn
ey D
isea
se
the presence of this condition for any inpatient or outpatient encounter in 5 years preceding date of admission for index hospitalization
016.0x, 095.4, 250.4x,
274.1x, 403.xx,
404.xx, 405.01,
405.11, 405.91, 440.1,
446.21, 581.xx,
582.xx, 583.xx, 585.x,
586, 587.x, 588.0,
588.8x, 588.9, 589.x,
590.0x, 593.7x, 791.0,
794.4
A18.1, N29.0, E10.20,
E10.21, E11.20, E11.21,
M10.39, I12.0, I12.9,
I13.0, I13.1, I13.2, I13.9,
I15.0, I70.1, M31.0,
N03.x, N04.x, N05.x,
N06.x, N07.x, N08.x,
N11.x, N12, N13.7,
N13.8, N13.9, N14.x,
N15.x, N16.x, N18.0,
N18.8, N18.9x, N18.90,
N18.91, N19, N25.0,
N25.8, N25.9, N26,
N27.x, R80, R94.4
all 403, 581, 582, 585, 586

72
C
ard
iac s
urg
ery
includes all cardiac surgery except percutaneous insertions, pacemakers, ICDs
for subcategorization of patients with AKI-RRT on index admission
E646-647 E650-652, E656, E658, E660-661, E670-671 E682, M134,M137, R700, R709-714, R715-718, R720-730, R722-738, R741-743, R746-749, R755, R758-759, R762, R768-774, R870, R874, R920-930, R863, R876
Ao
rtic
an
eu
rysm
(no
n-
rup
ture
d)
surgical procedures for unruptured aortic (thoracic and abdominal) aneurysms
for subcategorization of patients with AKI-RRT on index admission
R799-803, R816-817, R875 (EVAR)
Sep
sis
for subcategorization of patients with AKI-RRT on index admission (based on criteria of Martin et. al. NEJM)
003·1, 036·2 and 038·00–038·90
A082.1, A39.4, A40.3, A40.9, A41.2, A41.3, A41.4, A41.51, A41.52, A41.58, A41.8, A41.9
all
Pro
pen
sit
y
sco
re
to be used for matching
variable list and associated codes attached below
Nep
hro
log
ist
Any physician with 10 claims using any
of the OHIP codes on the right anytime
between start of ICES data until March
31, 2007 (a person may have any
combination of these codes but as long
as 10 are claimed, they are considered
a nephrologist) – yellow highlighted
codes
G326, G860, G333, G862, G863, G865, G866, G332, G861, G864

Condition/Disease ICD-9 ICD-10 Diagnostic type
OHIP
Death
(in RPDB)
------- ------- ----- ----- -----
Acute Kidney Injury
-------- 584.5-584.9
669.3, 958.5 634.3, 635.3,
636.3, 637.3638.3, 639.3
N17.0-N17.9, O08.4, T79.5, O90.4
all -----
End-stage renal disease-Definition B
Receipt of dialysis for a 90-day period after 90 days post-discharge
Comment: If any of the listed codes is detected, count forward 90 days. One of the listed codes has to appear after the 90-day mark but within 60 days after the 90-day mark. The date of the initial code is considered the “date of ESRD”.
R849, R850, G323, G325, G326, G330, G331, G332, G860, G333, G083, G091, G085, G295, G082, G090, G092, G093, G094, G861, G862, G863, G864, G865, G866, G294, G095, G096
CCP: 51.95, 66.98
CCI:
1PZ21HQBR, 1PZ21HPD4

eAppendix2: Covariates used in the development of the propensity score.
Characteristic
Demographics
Age, mean (SD), y
Female gender
Lowest income quintile
Rural residence
Distance from nearest dialysis unit (km)a
0-50
51-150
151-300
>300
Admission Era
1995-2001
2002-2008
Proceduresc
Angiography
Coronary artery bypass grafting
Percutaneous coronary intervention
Valvular surgery
Pacemaker
Echocardiography
Electrocardiography
Holter monitor
Stress test
Peripheral vascular procedures
Carotid doppler ultrasound
Carotid endarderectomy
Renal biopsy
Hospital type
Teaching hospital
Healthcare accessb
Number of hospitalizations
Number of emergency visits
Number of GP visits
Number of internist visits
Number of cardiology visits
Number of nephrology visits
Procedure or condition during index hospitalization
Sepsis
Cardiac surgery
Abdominal aortic aneurysm repair
Mechanical ventilation d
Comorbid disease c
Myocardial Infarction
Coronary artery disease
Cardiac dysrythmias
Heart failure
Cerebrovascular disease
Diabetes
Cancer
Liver disease
Peripheral vascular disease
Chronic kidney diseasec
Hypertension
Hematuria
Proteinuria
Major respiratory infection
Major genitourinary/gastrointestinal infection
Major skin/soft tissue infection
Charlson comorbidity index, mean (SD), score
aGeospatial mapping methods were used to calculate the distance between each patient’s residence and the practice
location of the closest dialysis unit.1
b In the 5 years preceding the hospital discharge date except chronic kidney disease which had a lookback period of
5 years preceding the hospital admission date. c In the 5 years preceding hospital discharge date.
d The receipt of mechanical ventilation was used as a surrogate for admission to a critical care unit.2