Embed Size (px)
Citation preview

An Update on Diabetes in 2016
Assoc Prof Jeremy Krebs Endocrinologist
University of Otago Wellington

Outline
Pathogenesis of Type 2 DM and how this relates to treatment options
What do we want in a drug?
Incretin-based therapy
SGLT2 Inhibitors
Glucose monitoring devices

0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
45.00%
50.00%
00-04 05-09 10-14 15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85+
Rate
(B
ase=
Pra
cti
ce e
nro
lled
po
pu
lati
on
)
Age group
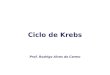
New Zealand Diabetes Prevalence Rate as of 31 Dec 2011
European/Other Mäori Pacific people Indian

Type 2 Diabetes
De Fronzo J. Diabetes 1998; 37:667–687.
Insulin Resistance
hepatic
glucose
production glucose uptake
-cell Dysfunction
impaired
insulin secretion
Genetic Susceptibility
Obesity, Sedentary Lifestyle
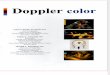
Pathogenesis of Type 2 Diabetes: Insulin Resistance and -cell dysfunction

Glucose
(mg/dl)
50 –
100 –
150 –
200 –
250 –
300 –
350 –
0 –
50 –
100 –
150 –
200 –
250 –
-10 -5 0 5 10 15 20 25 30 Years of diabetes
Adapted from Burger HG, et al. 2001. Diabetes Mellitus, Carbohydrate Metabolism, and Lipid Disorders. In Endocrinology.
4th ed. Edited by LJ DeGroot and JL Jameson. Philadelphia: W.B. Saunders Co., 2001.
Originally published in Type 2 Diabetes BASICS. International Diabetes Center, Minneapolis, 2000.
Relative
function
(%)
Fasting
glucose
Obesity IFG Diabetes Uncontrolled
hyperglycemia
Insulin resistance
Insulin resistance and -cell dysfunction are fundamental to type 2 diabetes
Postprandial
glucose
Insulin secretion Clinical
diagnosis

HbA1c
cross-sectional, median values
06
7
8
9
0 3 6 9 12 15
HbA
1c (
%)
Years from randomisation
Conventional
Intensive
6.2% upper limit of normal range

Assumptions
Obesity is bad, Diabetes is worse
Tight glycaemic control is good
– But too tight is bad
– Target HbA1c < 53mmol/mol (<7.0%)
Tight control reduces complications
– Unequivocal for microvascular
– Less clear for macrovascular!
• But becoming more convincing...
• May be variation between agents re CVD outcomes

Factors in Deciding on Choice of Agent
Efficacy
– Large reduction in HbA1c
– Sustained effect
– Preserve or improve beta cell function
– Weight loss
Adverse effects
– Easy to take (oral, daily or less, no titration)
– No hypoglycaemia
– No weight gain
Impact on Cardiovascular factors
– Reduced vascular disease and events
– Neutral or positive effect on lipids
Cost
– Cheaper the better!

Glycaemic Control Target HbA1c 48-58 mmol/mol
(6.5 - 7.5%)
Diet and Lifestyle
Oral Hypoglycaemics
Monotherapy
Combination therapy
Insulin
Management Strategy

Type 2 Diabetes Algorithm
Diet and Lifestyle
Metformin
Glitazone SU Acarbose
Insulin
Oral agent
No hypos
But GI side effects
No hypos
But weight gain, heart
failure, fractures.
?IHD risk
Oral agent
Good evidence
But weight gain,
hypos

The Therapeutic Challenge in Managing Type 2 Diabetes
We need new treatments that:
– Additive to traditional treatments
– Can be used in presence of complications (eg kidney failure, heart disease)
– Acceptable to patients
– Reduce rather than worsen complications of diabetes
– Reduce cardiovascular events
– (preferably) not increase weight
– (ideally) not cause hypos

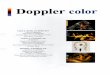
Major Targeted Sites of Diabetes Drug Classes
Buse JB et al. In: Williams Textbook of Endocrinology. 10th ed. Philadelphia: WB Saunders; 2003:1427–1483; DeFronzo RA. Ann Intern Med.
1999;131:281–303; Inzucchi SE. JAMA 2002;287:360-372; Porte D et al. Clin Invest Med. 1995;18:247–254.
DPP-4=dipeptidyl peptidase 4; TZDs=thiazolidinediones.
Glucose
absorption
Hepatic glucose
overproduction
Impaired insulin
secretion
Insulin
resistance
Pancreas
↓Glucose level
Muscle
and fat Liver
Biguanides
TZDs Biguanides
Sulfonylureas
GLP-1 mimetics
TZDs
α-Glucosidase
inhibitors
Gut
DPP-4 inhibitors
DPP-4 inhibitors
Biguanides
15
GLP-1 mimetics
SGLT2 Inhibitors
Kidney

Type 2 Diabetes Algorithm
Diet and Lifestyle
Metformin
GLP-1 DPPIV Glitazone SU Acarbose
Insulin
Weight loss
No hypos
But Injectable
Weight neutral
Oral agent
No hypos
Oral agent
No hypos
But GI side effects
No hypos
But weight gain, heart
failure, fractures.
?IHD risk
Oral agent
Good evidence
But weight gain,
hypos
SGLT2
Weight loss
No hypos
UTIs

Incretins based therapies

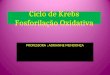
Incretin Effect After Oral Glucose: Diminished in Type 2 Diabetes
*p0.05 vs. respective value after oral load
IR=immunoreactive Adapted from Nauck M et al Diabetologia 1986;29:46–52.
Diminished incretin effect
Normal incretin effect
Oral glucose (50 g/400 ml) Isoglycemic intravenous glucose
0
–10
10
15
20
Ven
ou
s p
lasm
a g
luco
se
(mm
ol/
L) 5
60 120 180
Time (minutes)
0
40
60
80
IR i
nsu
lin
(m
U/L
)
20
Healthy controls (n=8) Type 2 diabetes (n=14)
0
10
15
20
5
Time (minutes)
0
40
60
80
IR i
nsu
lin
(m
U/L
)
20
–5 –10 60 120 180 –5
–10 60 120 180 –5 –10 60 120 180 –5
* * * * * *
* * *
*
Ven
ou
s p
lasm
a g
luco
se
(mm
ol/
L)
Oral/Intravenous Glucose Infusion Study

Adapted from Brubaker PL, Drucker DJ Endocrinology 2004;145:2653–2659; Zander M et al Lancet 2002;359:824–830; Ahrén B Curr Diab Rep 2003;3:365–372; Buse JB et al. In Williams Textbook of Endocrinology. 10th ed. Philadelphia, Saunders, 2003:1427–1483.
Incretins Regulate Glucose Homeostasis Through Effects on Islet Cell Function
Active GLP-1 and GIP
Release of incretin gut hormones
Pancreas
Blood glucose control
Glucagon
from alpha cells (GLP-1) Glucose dependent
Alpha cells
Increased insulin
and decreased
glucagon
reduce
hepatic
glucose output
Glucose dependent
Insulin
from beta cells (GLP-1 and GIP)
Beta cells
Insulin
increases
peripheral
glucose
uptake GI tract
Ingestion of food
DPP-4 enzyme
Inactive GIP
Inactive GLP-1

GLP-1 Effects in Humans: Understanding the Glucoregulatory Role of Incretins
Promotes satiety and reduces appetite
Beta cells: Enhances glucose-dependent insulin secretion
Adapted from Flint A, et al. J Clin Invest. 1998;101:515-520.; Adapted from Larsson H, et al. Acta Physiol Scand. 1997;160:413-422.; Adapted from Nauck MA, et al. Diabetologia. 1996;39:1546-1553.; Adapted from Drucker DJ. Diabetes. 1998;47:159-169.
Liver: ↓ Glucagon reduces hepatic glucose output
Alpha cells:
↓ Postprandial glucagon secretion
Stomach: Helps regulate gastric emptying
GLP-1 secreted upon
the ingestion of food

Current GLP-1–based Approaches for Improving Glycaemic Control
Drucker DJ, et al. Diabetes Care. 2003;26:2929-2940; Baggio LL, et al. Diabetes. 2004;53:2492-2500.
Agents that prolong the activity of endogenous GLP-1
• DPP-IV inhibitors
Agents that mimic the actions of GLP-1 (incretin mimetics)
– DPP-IV–resistant GLP-1 derivatives
• GLP-1 analogues
– Novel peptides that mimic the glucoregulatory actions of GLP-1
• Exenatide

Initial Combination Therapy With Sitagliptin Plus
Metformin Study: Additive Decrease in HbA1c
aLeast squares mean change from baseline with adjustment for placebo.bWithin-group mean change from baseline.
qd=once a day; bid=twice a day.
Goldstein B et al. Diabetes Care. 2007;30:1979–1987.
117
–2.9b
Metformin 1000 mg bid
Sitagliptin 100 mg qd
Sitagliptin 50 mg + metformin 500 mg bid
Metformin 500 mg bid
Sitagliptin 50 mg + metformin 1000 mg bid
Hb
A1
cC
ha
ng
e F
rom
Baselin
e, %
–3.5
–3.0
–2.5
–2.0
–1.5
–1.0
–0.5
0.0
0.5
178 177 183 178175n=
–0.8a
–1.0a
–1.3a
–1.6a
–2.1a
24-Week Placebo-Adjusted Results
Mean HbA1c = 8.8%
Open-Label
Mean Change From Baseline
Mean HbA1c= 11.2%
All-Patients-Treated Population
31

DPP-IV Antagonists and HbA1c lowering
JAMA. 2007;298(2):194-206.

DPPIV Antogonists Adverse Effects
No hypoglycaemia
Weight neutral
Nausea
Nasopharyngitis
Pros Cons

Exenatide (Exendin-4)
Synthetic version of salivary protein found in the Gila monster
Approximately 50% identity with human GLP-1
– Binds to known human GLP-1 receptors on cells in vitro
– Resistant to DPP-IV inactivation
Exenatide: An Incretin Mimetic
Adapted from Nielsen LL, et al. Regulatory Peptides. 2004;117:77-88.; Fineman MS, et al. Diabetes Care. 2003;26:2370-2377. Reprinted from Regulatory Peptides, 117, Nielsen LL, et al, Pharmacology of exenatide (synthetic exendin-4): a potential therapeutic for improved glycaemic control of type 2 diabetes, 77-88, 2004, with permission from Elsevier for English use only.
Site of DPP-IV Inactivation
H G E G T F T S D L S K Q M E E E A V R L F I E W L K N G G P S S G A P P P S – NH2
H A E G T F T S D V S S Y L E G Q A A K E F I A W L V K G R – NH2
Exenatide
GLP-1
Human

JAMA. 2007;298(2):194-206.
GLP-1 Agonists and HbA1c lowering


Primary and Exploratory Outcomes.
Marso SP et al. N Engl J Med 2016;375:311-322

Primary Composite Outcomes in Various Demographic and Clinical Subgroups.
Marso SP et al. N Engl J Med 2016;375:311-322

Primary and Secondary Outcomes.
Marso SP et al. N Engl J Med 2016;375:311-322

Selected Adverse Events Reported during the Trial.
Marso SP et al. N Engl J Med 2016;375:311-322

GLP-1 Agonists Adverse Effects
No hypoglycaemia
– Unless combined with other secretagogues
Weight loss
?? Beta cell neogenesis
Nausea and vomiting
Pros Cons

Incretin Therapies and Pancreatitis / Pancreatic Cancer
Pancreatitis and pancreatic cancer more common in those with diabetes
No convincing evidence that DPPIV antagonists or GLP-1 agonists increase this

The Kidney and Normal Glucose Handling
Minimal to no glucose excretion
Proximal tubule
Majority of glucose reabsorbed
SGLT2/1
Glucose
Glucose
filtration
SGLT: sodium-glucose cotransporter
1. Wright EM, et al. J Int Med 2007;261:32–43. 2. Hummel CS. Am J Physiol Cell Physiol 2011;300:C14−21.

SGLT2 Inhibitors: Insulin-independent approach to remove excess glucose
• Selectively inhibits SGLT2 in the renal proximal tubule1
• FORXIGA 10 mg/day removes approximately 70 g of glucose/day (corresponding to 280 kcal/day) via the urine2
1. Gerich JE, Bastien A. Expert Rev Clin Pharmacol 2011;4:669−6683. 2. FORXIGA® ( dapagliflozin propanediol monohydrate) data sheet available at http://www.medsafe.govt.nz/profs/datasheet/f/forxigatab.pdf
Glucose
filtration
Reduced glucose
reabsorption
Glucose
FORXIGA
SGLT2
SGLT2
Inhibitor
Increased urinary excretion of excess glucose

SGLT-2 Inhibitors: “Flozins”
Increase renal loss of glucose
• Action is independent of insulin
• Dont cause hypoglycaemia
• Assoc weight loss and reduced BP
• Require renal function (ineffective with eGFR <45)
Side effects:
• UTIs and genital fungal infection.
• DKA (esp if used in T1DM)
Usual HbA1c reduction 6 – 16 mmol/mol (0.6-1.5%)

Add-on to metformin: Impact on HbA1c
Phase III, multicentre, randomised, double-blind, placebo (PBO)-controlled, parallel-group, 24-week clinical study to evaluate the efficacy and safety of FORXIGA 10 mg + MET (≥1500 mg/day) vs. PBO + MET (≥1500 mg/day) in adult patients with T2DM who had inadequate glycaemic control (HbA1c ≥7% and ≤10%) on MET alone. Primary endpoint: HbA1c reduction at 24 weeks. Values for 24 weeks are last observation (excluding data after rescue) carried forward and represent adjusted mean change from baseline. Values for the 78-week extension represent adjusted mean change from baseline (excluding data after rescue) based on a longitudinal repeated measures model.
Bailey CJ, et al. Lancet 2010;375:2223−2233. Bailey CJ, et al. BMC Medicine 2013;11:43.

Add-on to metformin: Effect on Body Weight
Bailey CJ, et al. Lancet 2010;375:2223−2233. Bailey CJ, et al. BMC Medicine 2013;11:43.
Phase III, multicentre, randomised, double-blind, placebo (PBO)-controlled, parallel-group, 24-week clinical study to evaluate the efficacy and safety of FORXIGA 10 mg + MET (≥1500 mg/day) vs. PBO + MET (≥1500 mg/day) in adult patients with T2DM who had inadequate glycaemic control (HbA1c ≥7% and ≤10%) on MET alone. Primary endpoint: HbA1c reduction at 24 weeks. Values for 24 weeks are last observation (excluding data after rescue) carried forward and represent adjusted mean change from baseline. Values for the 78-week extension represent adjusted mean change from baseline (excluding data after rescue) based on a longitudinal repeated measures model.

Ann Intern Med. 2013;159(4):262-274.
SGLT2 Inhibitors and HbA1c

SGLT2 Inhibitors Adverse Effects
Effect independent of Insulin
No hypoglycaemia
– Unless combined with secretagogues
Weight loss
BP lowering
Urinary Tract and Genital Infections
Bladder and Breast Cancer?
Pros Cons

SGLT-2 Inhibitors:
Dapagliflozin 5mg, 10mg (Forxiga)
Canagliflozin 100mg, 300mg (Invokana)
Empagliflozin 10mg, 25mg (Jardiance)


Cardiovascular Outcomes and Death from Any Cause.
Zinman B et al. N Engl J Med 2015;373:2117-2128

Subgroup Analyses for the Primary Outcome and Death from Cardiovascular Causes.
Zinman B et al. N Engl J Med 2015;373:2117-2128

Glycated Hemoglobin Levels.
Zinman B et al. N Engl J Med 2015;373:2117-2128

Primary and Secondary Cardiovascular Outcomes.
Zinman B et al. N Engl J Med 2015;373:2117-2128

Adverse Events.
Zinman B et al. N Engl J Med 2015;373:2117-2128

Cost (NZ$)
Metformin 1g BD $1.94/month
Glipizide 15mg OD $3.15/month
Acarbose 50mg TDS $16.50/month
Pioglitazone 30mg OD $5.23/month
Sitagliptin 100mg OD $110.00/month
Exenatide 10ug BD $220.00/month
Dapaglaflozin 10mg OD $90/month
NPH insulin 30u OD $59.72/month
Does not consider monitoring costs for agents causing hypoglycaemia

Summary
New agents have similar glucose lowering efficacy as older agents
Some advantages
• Weight
• Hypoglycaemia
• Use in renal failure (DPPIV)
• ? Β cell neogenesis (GLP-1 )
• Effect not dependent on insulin (SGLT2)
• CVD event reduction for SGLT2 inhibitors and GLP-1 agonists
Unknown longterm effects
Cancer
Cost

Insulin therapies in diabetes:
Short acting
– Humalog
– Novorapid
– Apidra
Longer short acting
– Actrapid
– Humulin R
Intermediate acting
– Protophane
– Humulin NPH
Long acting
– Lantus
– Levemir (not funded in NZ)
Mix insulins:
– Penmix 30
– Humulin 30/70
– Humalog Mix 25
– Humalog Mix 50
– Novo mix 30

Monitoring Glucose

FreeStyle Libre

Abbott Australia
– Order online
• AU $95 for wand
• AU $95 for sensors (2 weeks)
• Must be delivered to Australian address

Dexcom 5 Continuous Glucose Monitor

NZ Medical and Scientific
– Order online
• Dexcom receiver $999.00
• Dexcom sensors $550.00 (pack of 4)
– Each sensor lasts 7days (Officially)