Embed Size (px)
Citation preview

ASSISTING PATIENTS with QUITTING
Released June 2000
Sponsored by the AHRQ (Agency for Healthcare Research and Quality) of the USPHS (US Public Heath Service) with:
CDC (Centers for Disease Control) NCI (National Cancer Institute) NIDA (National Institute for Drug
Addiction) NHLBI (National Heart Lung & Blood
Institute) RWJF (Robert Wood Johnson Foundation)
http://www.surgeongeneral.gov/tobacco/
CLINICAL PRACTICE GUIDELINE for TREATING TOBACCO USE and DEPENDENCE

EFFECTS OF CLINICIAN INTERVENTIONS
Fiore et al. Treating Tobacco Use and Dependence. Clinical Practice Guideline. Rockville, MD: USDHHS, PHS, 2000.
0
10
20
30
No clinician Self-helpmaterial
Nonphysicianclinician
Physicianclinician
Type of Clinician
Est
imate
d a
bst
inence
at
5+
month
s
1.0 1.1(0.9,1.3)
1.7(1.3,2.1)
2.2(1.5,3.2)
n = 29 studies

ASK
ADVISE
ASSESS
ASSIST
ARRANGE
The 5 A’s

The 5 A’s (cont’d)
Ask about tobacco use “Do you ever smoke or use any type of tobacco?”
“I take time to ask all of my patients about tobacco use—because it’s important.”
ASK

The 5 A’s (cont’d)
tobacco users to quit (clear, strong, personalized, sensitive) “It’s important that you quit as soon as possible,
and I can help you.”
“I realize that quitting is difficult. It is the most important thing you can do to protect your health now and in the future. I have training to help my patients quit, and when you are ready, I will work with you to design a specialized treatment plan.”
ADVISE
The 5 A’s (cont’d)
Assess readiness to make a quit attemptASSESS
Assist with the quit attemptASSIST

Arrange follow-up careARRANGE
The 5 A’s (cont’d)
Number of sessions
Estimated quit rate*
0 to 1 12.4%
2 to 3 16.3%
4 to 8 20.9%
More than 8 24.7%* 5 months (or more)
postcessation
Fiore et al. Treating Tobacco Use and Dependence. Clinical Practice Guideline. Rockville, MD: USDHHS, PHS, 2000.
PROVIDE ASSISTANCE THROUGHOUT THE QUIT PROVIDE ASSISTANCE THROUGHOUT THE QUIT ATTEMPTATTEMPT

5 A’s: REVIEW
ASK about tobacco USE
ADVISE tobacco users to QUIT
ASSESS readiness to make a QUIT attempt
ASSIST with the QUIT ATTEMPT
ARRANGE FOLLOW-UP care

Faced with change, most people are not ready to act.
Change is not a single step, but a process.
Typically, it takes multiple attempts.
HOW CAN I LIVE WITHOUT
TOBACCO?
The (DIFFICULT) DECISION to QUIT

HELPING SMOKERS QUIT IS a CLINICIAN’S RESPONSIBILITY
Clinicians have a professional obligation to help their patients quit using tobacco.
THE DECISION TO QUIT LIES IN THE HANDS OF EACH PATIENT.

PATIENTS DIFFER IN THEIR READINESS TO COMMIT TO QUITTING
PATIENTS DIFFER IN THEIR READINESS TO COMMIT TO QUITTING
TAILORING the INTERVENTION to MEET the PATIENT’S NEEDS
Persons NOT READY TO QUIT (in the next 30 days): Motivational interventions
Persons READY TO QUIT (in next 30 days): Behavioral counseling Pharmacotherapy
Persons who RECENTLY QUIT (in past 6 months): Relapse prevention interventions

IS a PATIENT READY to QUIT?Does the patient now use tobacco?
Is the patient now ready to quit?
Provide treatment
The 5 A’s
Promote motivation
Yes
YesNo
Did the patient once use tobacco?
Prevent relapse*
Encourage continued abstinence
Yes
No
No
*Relapse prevention interventions not necessary if patient has not used tobacco for many years and is not at risk for re-initiation.
Fiore et al. Treating Tobacco Use and Dependence. Clinical Practice Guideline. Rockville, MD: USDHHS, PHS, 2000.

FIVE STAGES THAT DESCRIBE a PERSON’S READINESS to CHANGE
STAGE 1: Not thinking about changing anytime soon
STAGE 2: Considering changing, but not yet
STAGE 3: Getting ready to change soon
STAGE 4: In the process of changing
STAGE 5: Changed a while ago

FIVE STAGES THAT DESCRIBE a PERSON’S READINESS to CHANGE
STAGE 1: Precontemplation
STAGE 2: Contemplation
STAGE 3: Preparation
STAGE 4: Action
STAGE 5: Maintenance

STAGES of CHANGE:A LINEAR VIEW
Precontemplation ActionContemplation Maintenance
Quit date
Preparation
- 30 days- 6 months + 6 months
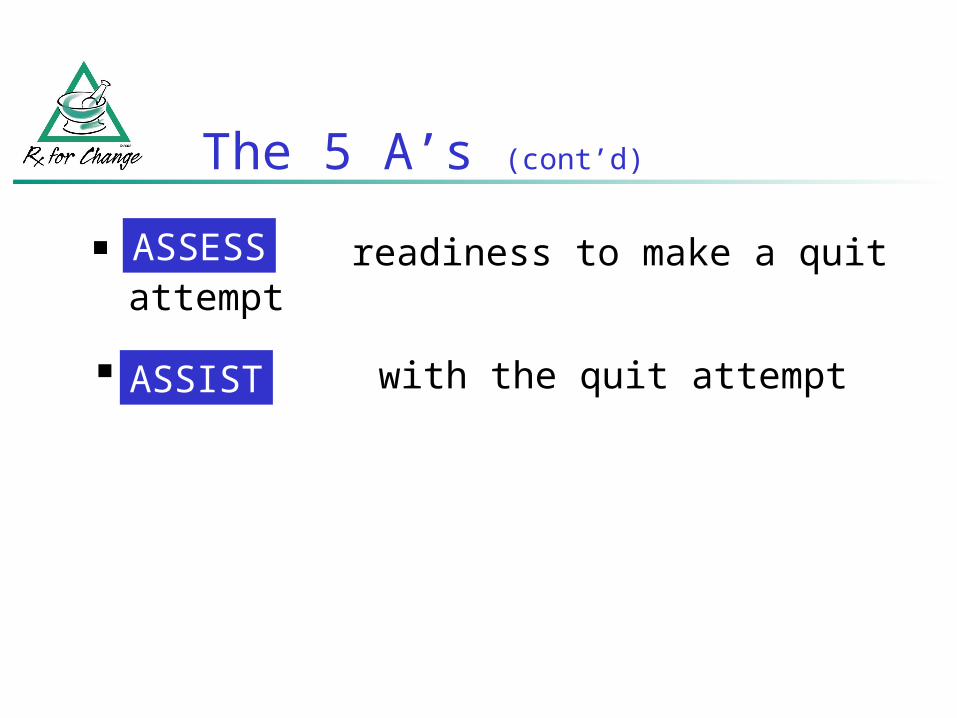
Maintenance
ContemplationAction
Preparation
Pre-contemplation
Termination
Relapse*
* Patients can relapse out of the maintenance or action stages, reverting to earlier stages.
ASSESS READINESS TO QUIT: STAGES of CHANGE, CYCLICAL VIEW
Not ready to quit
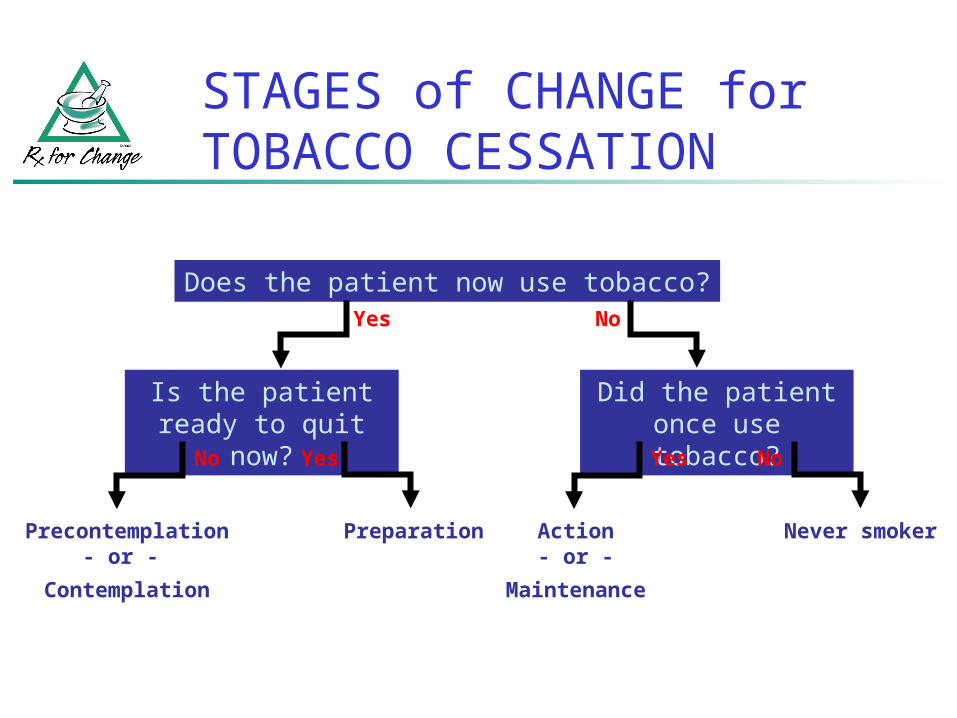
STAGES of CHANGE for TOBACCO CESSATION
Does the patient now use tobacco?
Is the patient ready to quit now?
PreparationPrecontemplation- or -
Contemplation
Yes
YesNo
Did the patient once use tobacco?
Action- or -
Maintenance
Never smoker
Yes
No
No

The STAGES of CHANGE
STAGE 1: Precontemplation
Not thinking about quitting in the next 6 months
Patients might not be aware of the need to quit. They might be aware of the need but resist quitting. Pros of smoking outweigh the cons.
GOAL: Move the patient into the contemplation stage.
STRATEGIES for COUNSELING during PRECONTEMPLATION
DON’Ts
Persuade
“Cheerlead”
Tell patient how bad smoking is, in a judgmental manner
DOs Strongly advise to quit
Ask noninvasive questions “Envelope”
Raise awareness of health consequences/concerns
Demonstrate empathy, foster communication
Leave decision up to patient

Considering quitting in the next 6 months but not in the next 30 days
Patients are aware of the need to quit.
They are aware of the benefits of quitting.
But they struggle with ambivalence about change.
STAGE 2: Contemplation
The STAGES of CHANGE (cont’d)
GOAL: Move the patient into the preparation stage.

STRATEGIES for COUNSELING during CONTEMPLATION
DON’Ts
Apply action-oriented interventions
DOs Strongly advise to quit
Provide information
Identify reasons for tobacco use
Demonstrate empathy; increase motivation
Encourage self-reevaluation of concerns
Offer encouragement

METHODS for INCREASING MOTIVATION—5 R’s
For patients who are not yet ready to quit:
Relevance Risks Rewards Roadblocks Repetition
Fiore et al. Treating Tobacco Use and Dependence. Clinical Practice Guideline. Rockville, MD: USDHHS, PHS, 2000.
TAILORED
INTERVENTION
MESSAGES

A DEMONSTRATION: COUNSELING a PATIENT who is NOT READY TO QUIT
CASE SCENARIO: MS. STEWART
You are a clinician providing care to Ms. Stewart, a 55-year-old patient with emphysema.
She uses two different inhalers for her emphysema.
COUNSELING SCENARIO: KEY POINTS
Ask about tobacco use Link inquiry to knowledge of disease
Assess readiness to quit Aware of need to quit; not ready yet
Advise to quit Discuss implications for disease progression
“I will help you, when you are ready”

The clinician has
Established a relationship
Established yourself as a resource
Planted a seed to move patient forward
Opened a door to facilitate further
counseling
COUNSELING SCENARIO:SUMMATION

The STAGES of CHANGE (cont’d)
Ready to quit in the next 30 days Patients are aware of the need to, and the
benefits of, making the behavioral change.
Getting ready to take action.
Goal: Move the patient to the action stage.
STAGE 3: Preparation
STRATEGIES for COUNSELING DURING PREPARATION
DOs Praise the patient’s readiness Assess tobacco use history
Current use: Type(s) of tobacco, brand, amount
Past use: duration, recent changes Past quit attempts:
Number, date, length Methods used, compliance, duration Reasons for relapse
DOs Discuss key issues
Reasons/motivation to quit Confidence in ability to quit Triggers for tobacco use Routines/situations associated with tobacco
use Stress-related smoking Social support for quitting Concerns about post-cessation weight gain Concerns about withdrawal symptoms
STRATEGIES for COUNSELING DURING PREPARATION

DOs Facilitate quitting process
Discuss methods for quitting (pros, cons)
Pharmacotherapy: a treatment, not a crutch! Behavioral counseling
Set a quit date! Recommend Tobacco Use Log (see
handout)
STRATEGIES for COUNSELING DURING PREPARATION

TOBACCO USE LOG
The Tobacco Use Log is most appropriate for patients who are getting ready to quit.
Documenting tobacco use helps patients to understand when and why they use tobacco.
Identifies activities or situations that trigger tobacco use.
Information can be used to develop coping strategies to overcome the temptation to use tobacco.

TOBACCO USE LOG: INSTRUCTIONS for USE
Patient should continue regular tobacco use for a period of 3 or more days
Each time any form of tobacco is used, the following information should be recorded on the log:
Time of day Brief description of activity or
situation during use “Importance” rating (scale of 1–3) Review log sheets to identify situations that trigger tobacco use
Develop coping strategies to prevent relapse

DOs
Discuss and develop coping strategies
Cognitive
Behavioral
STRATEGIES for COUNSELING DURING PREPARATION

COPING with QUITTING (cont’d)
Cognitive strategies
Review of commitment to quitting
Distractive thinking
Positive self-talks
Relaxation through imagery
Mental rehearsal and visualization

COPING with QUITTING (cont’d)
Examples: Thinking about cigarettes doesn’t mean you have to
smoke one. “Just because you think about something doesn’t mean you
have to do it!” Tell yourself “It’s just a thought,” or “I am in control.” Say the word STOP! out loud, or visualize a stop sign.
When you have a craving, remind yourself that: “The urge for a cigarette will only go away if I don’t smoke.”
As soon as you get up in the morning, look in the mirror and say to yourself
“I am proud that I made it through another day without smoking.”
COPING with QUITTING (cont’d)
Behavioral strategies Control your environment
Smoke-free home and workplace Alter or remove cues to tobacco use Modify behaviors that you associate with tobacco: when,
what, where, how, with whom Actively avoid trigger situations
Substitutes for smoking Water, chewing gum or hard candies (oral substitute)
Take a walk, diaphragmatic breathing, self-massage
Rely on social support Actively work to alleviate withdrawal symptoms

STRESS MANAGEMENT
Smoking gets rid of all my stress
I can’t relax without a cigarette
There will always be stress in one’s life
There are many ways to relax without a cigarette
The Myths The Facts
STRESS MANAGEMENT SUGGESTIONS:Deep breathing, shifting focus, taking a break.
Smokers confuse the relief of withdrawal with the feeling of relaxation

SOCIAL SUPPORT for QUITTING
Key ingredients for successful quitting: Social support as part of treatment (intra-
treatment) Social support outside of treatment (extra-
treatment)
Patients who receive social support and encouragement are more successful in quitting
PATIENTS SHOULD BE ADVISED TO: Ask family, friends, and coworkers for support – ask
them not to smoke around you, and not to leave cigarettes out
Talk with your health-care provider
Get individual, group, or telephone counseling
HERMAN ® is reprinted with permission from LaughingStock Licensing Inc., Ottawa, Canada
All rights reserved.
ADDRESSING CONCERNS about POSTCESSATION WEIGHT GAIN
Most quitters gain weight Most gain < 10 pounds, but there is a wide range
Discourage strict dieting while quitting Recommend physical activity Encourage healthy diet, plan meals, eat fruits Increase water intake Chew sugarless gum Select nonfood rewards
Maintain patient on pharmacotherapy shown to delay weight gain
Refer patient to specialist or program

Restlessness
Drowsiness
Fatigue
Impaired task performance
Nervousness
Sleep disturbances
Anger/irritability
Anxiety
Cravings
Difficulty concentrating
Hunger/weight gain
Impatience
ADDRESS CONCERNS about WITHDRAWAL SYMPTOMS
Hughes et al. Arch Gen Psychiatry 1991;48:52–59.

Most pass within 2 to 4 weeks after quitting
Cravings can last longer, up to several months or years
Often can be ameliorated with cognitive or behavioral coping strategies
Refer to Withdrawal Symptoms Information Sheet
Symptom, cause, duration, relief
ADDRESS CONCERNS about WITHDRAWAL SYMPTOMS (cont’d)

DOs Discuss concept of slip versus
relapse “Let a slip slide”
Medication counseling Proper use, with demonstration Promote compliance
Arrange follow-up Offer to assist throughout quit attempt Provide resources and referrals Congratulate the patient!
STRATEGIES for COUNSELING DURING PREPARATION

The STAGES of CHANGE (cont’d)
Actively trying to quit for good Patients have quit using tobacco sometime in
the past 6 months and are taking steps to increase their success.
Withdrawal symptoms occur.
At high risk for relapse.
STAGE 4: Action
GOAL: Remain tobacco-free for at least 6 months.
HERMAN ® is reprinted with permission from LaughingStock Licensing Inc., Ottawa, Canada
All rights reserved.

STRATEGIES for COUNSELING during ACTION
DOs Praise progress - solicit commitment to quit for good Evaluate current quit attempt:
Status of attempt “Slips” or relapse Medication use, plans for termination
Ask about social support Identify temptations and triggers for relapse
Negative affect, smokers, eating, alcohol, cravings, stress
Encourage healthful alternative behaviors to replace tobacco use
Offer tips for relapse prevention

RELAPSE PREVENTION Congratulate success! Encourage continued abstinence
Promote smoke-free environments Discuss benefits of quitting and successes achieved Discuss problems encountered and potential barriers to
continued abstinence Strong or prolonged withdrawal symptoms?
Add, combine, or extend use of pharmacotherapy agents
Social support Discuss ongoing sources of support Schedule follow-up visits or calls; refer to support groups

The STAGES of CHANGE (cont’d)
Tobacco-free for 6 months Patients remain vulnerable to relapse.
STAGE 5: Maintenance
GOAL: Remain tobacco-free for life.

HERMAN ® is reprinted with permission from LaughingStock Licensing Inc., Ottawa, Canada
All rights reserved.

STRATEGIES for COUNSELING DURING MAINTENANCE
DOs
Congratulate continued success Continue to offer tips for relapse prevention
Assess temptations and triggers
Discuss and suggest coping strategies
Encourage alternative behaviors Provide positive reinforcement

STAGES of CHANGE: A REVIEW
Precontemplation ActionContemplation Maintenance
Quit date
Preparation
- 30 days- 6 months + 6 months
Routinely identify tobacco users (ASK) Strongly ADVISE patients to quit ASSESS stage at each contact Tailor intervention messages (ASSIST)
Be a good listener Minimal intervention in absence of time
for more intensive intervention ARRANGE follow-up
Use the referral process, if needed
CESSATION COUNSELING: SUMMARY

WHAT IF…
a patient asks you about your use of tobacco?

Courtesy of Mell Lazarus and Creators Syndicate. Copyright 2000, Mell Lazarus.

The RESPONSIBILITY of HEALTH PROFESSIONALS
It is inconsistent
to provide health care and
—at the same time—
remain silent (or inactive)
about a major health risk.
TOBACCO CESSATION is an important component of
THERAPY.
DR. GRO HARLEM BRUNTLAND,
DIRECTOR-GENERAL of the WHO:
“If we do not act decisively, a hundred years from now our grandchildren and their children will look back and seriously question how people claiming to be committed to public health and social justice allowed the tobacco epidemic to unfold unchecked.”
US Department of Health and Human Services. Women and Smoking: A Report of the Surgeon General. Washington, DC: Public Health Service, 2001.