Embed Size (px)
Citation preview

The Evolution of Tracheal Injury Due to VentilatoryAssistance Through Cuffed Tubes:
A Pathologic Study
JOEL D. COOPER, M.D., HERMES C. GRILLO, M.D.
From the General Surgical Services and Department of Surgery, the HarvardMedical School and the Massachusetts General Hospital,
Boston, Massachusetts 02114
SEVERE clinical symptoms arising fromdamage to the trachea in patients who havebeen treated for respiratory failure bymechanical ventilatory assistance throughcuffed tracheostomy tubes have been in-creasingly recognized.1' 8,10,13 The symp-toms are those of airway obstruction, mas-sive hemorrhage or aspiration pneumonia.Symptoms arise from lesions which resultfrom a relative balance of ulcerative andreparative processes; the lesions includetracheal stenosis, tracheal malacia and lo-calized erosion. Similar complications havelong been recognized to arise from the tra-cheal stoma itself. The lesions which char-acteristically result from assistance throughcuffed tubes, however, are usually found afew centimeters below the stoma.10' 13
This report describes the pathology ofthe characteristic injuries which occurredin 30 patients who had received respiratoryassistance through cuffed tubes but whodied from causes other than upper airwaydamage. Lesions found at the site of thetracheostomy are not specifically discussed,since these occur independently of respira-tor assistance. The varying duration of res-piratory assistance prior to death providesinformation on the evolution of the lesions.
Submitted for publication September 18, 1968.Supported by Research Grant F.R.05486 from
the United States Public Health Service.Address for reprints: Dr. H. C. Grillo, Massa-
chusetts General Hospital, Boston, Massachusetts02114.
334
A small number of injuries related to ven-tilatory assistance through endotrachealtubes is also presented for comparison.
Surgically resected specimens were alsostudied from an additional group of pa-tients who had developed tracheal stenosisin the segment located from one to 3.5 cm.below the stoma. We have previously de-scribed the management of such benigntracheal stenosis and have also brieflynoted the pathology of these fully devel-oped stenotic lesions.l0 11
Specimens
Tracheas were removed at autopsy frompatients who had been receiving assistedrespiration through a cuffed tracheostomytube or an endotracheal tube at the timeof death. When possible, specimens wereremoved with the tubes in place in orderto correlate the site of damage to the tra-chea with the location of the tube and itscuff. The trachea was removed intact, in-cluding the larynx and carina. The dura-tion of intubation and assisted ventilationwas noted from the hospital records. In the30 patients who received respiratory assist-ance through a tracheostomy, the durationof intubation ranged from 1 day to 8 weeks(Table 1). In some cases, an endotrachealtube had been in place for several daysprior to the insertion of a tracheostomytube. Four specimens were studied frompatients who had received respiratory as-
TRACHEAL INJURY BY CUFFED TUBES 335
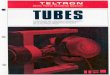
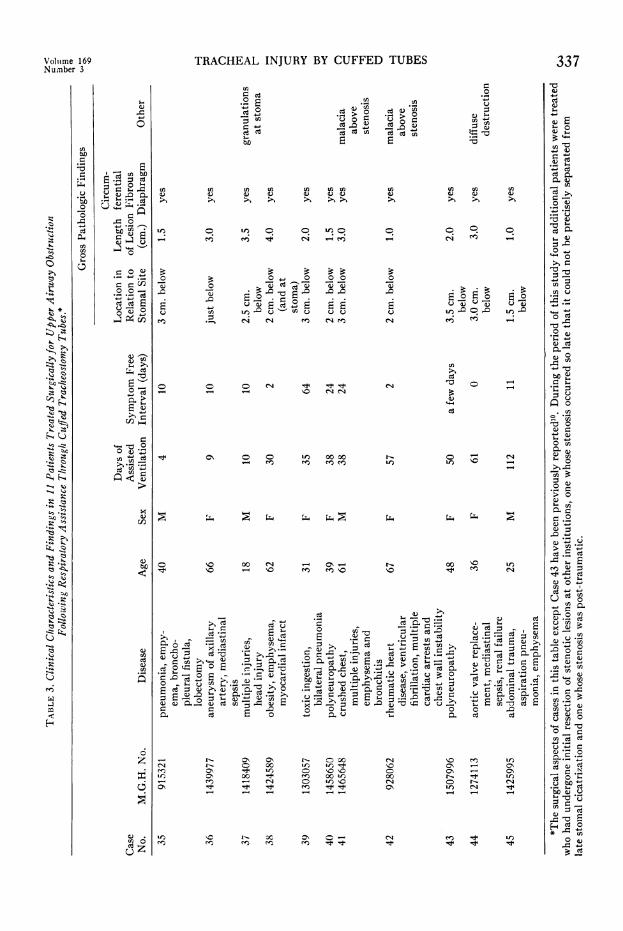
TABLE 1. Pat hologic Changes in Tracheas of 30 Patients Who Received Respiratory AssistanceThrough Cuffed Tracheostomy Tubes for Varying Periods of Time.*
Autopsy Specimens
M.G.H. Duration ofCase Pathology TracheostomyNo. No. Tube (days) Gross Pathologic Findings
2345
67
89
10
31623316553161631628316543186231629
317803182331651
11 3181012 3182813 31946
14 3202215 31967
16 31818
17 3177918 31825
19 3172520 3200421 32038
22 3164623 31806
24 31851
25 31890
26 32028
27 31944
28 3182129 31694
30 31594
1 Superficial changes-tracheitis1 Circumferential ring of hemorrhagic change2 Small anterior tracheal ulceration at cuff site2 Early anterior ulcerations2 Circumferential band of fibrin at cuff site3 Three cartilaginous rings exposed anteriorly at the cuff site3 Circumferential discoloration and one exposed cartilaginous ring
at cuff site3 Small area of exposed cartilage anteriorly at the cuff site3 Cartilaginous rings exposed anteriorly at the cuff site4 Discoloration of the anterior tracheal wall with superficial erosions
over the cartilaginous rings4 Fibrin deposition and superficial ulcerations anteriorly4 Small anterior ulcerations5 Exposed cartilaginous rings at the cuff site and a small anterior
erosion at site of tracheostomy tube tip6 Scattered erosions in the cuff area7 Extensive baring of cartilage and small perforation through the
posterior tracheal wall at the cuff site7 One cartilaginous ring widely exposed with several erosions above
and below this level. Tracheitis from the cuff site down8 Four cartilaginous rings widely exposed anteriorly at the cuff site9 Ballooning out of the trachea at the cuff site with severe exposure
of cartilage. Perforation of the membranous portion of thetrachea with local reaction in the esophageal wall
9 Ulcerations in the tracheal wall in the region of the cuff9 Several rings exposed at various points in the region of the cuff10 Severe exposure of numerous cartilaginous rings in the region of
the cuff with extensive fragmentation of cartilage. Large per-foration through posterior wall of trachea with local reactionin adjacent esophagus
12 Baring and softening of cartilage in the region of cuff16 Severely eroded and fragmented cartilage at the cuff site. Numer-
ous pieces of cartilage missing. Severe loss of tracheal wallsupport
18 Several cartilaginous rings widely exposed and thinned in theregion of the cuff
19 Two exposed, thinned and fragmented cartilaginous rings at cuffsite. Small anterior ulceration at the site of the tip of the tube
19 Extensive baring, fragmentation and exposure of cartilaginousrings at the stomal site as well as in the region of the cuff belowthe stoma
21 Extensive damage to cartilaginous rings with ulceration, baringof cartilage and fragmentation of cartilage at the cuff site.Small shallow ulcer located at the tip of the tracheostomy tube
21 Almost no visible damage except for slight discoloration42 Extensive fragmentation of cartilage, many areas devoid of
cartilage, marked loss of support in tracheal wall at the cuff site60 One centimeter segment of trachea totally devoid of cartilage and
totally flexible
* None of these patients had symptoms of upper airway obstruction at the time of death.
Volume 169Number 3
COOPER AND GRILLO Annals of SurgeryMarch 1969
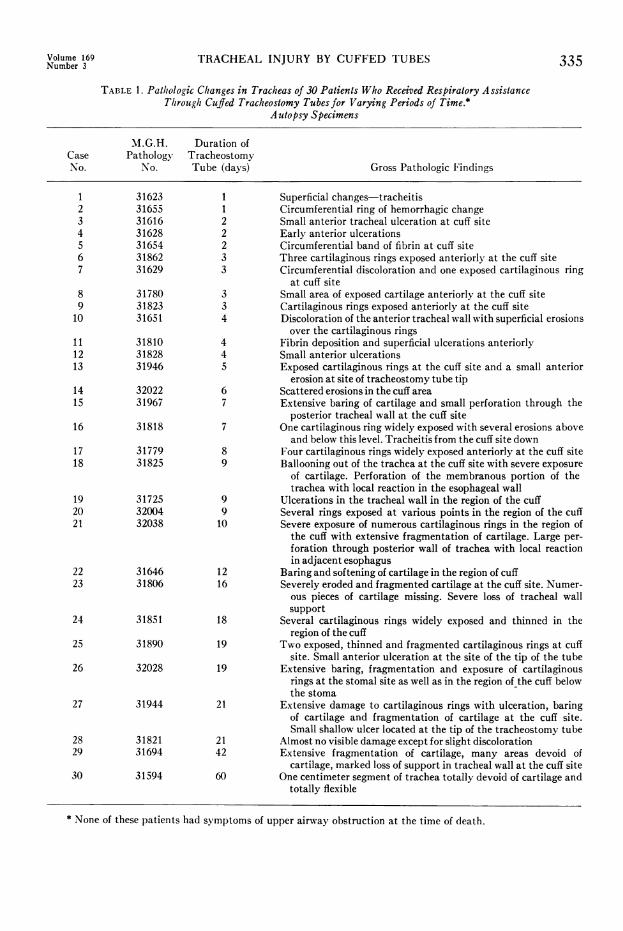
TABLE 2. Pathologic Changes in Tracheas of 4 Patients Who Received Respiratory AssistanceThrough Cuffed Endotracheal Tubes only for Short Periods.* Autopsy Specimens.
M.G.H. Duration ofCase Pathology EndotrachealNo. No. Tube (days) Gross Pathological Findings
31 31643 4 Fibrin deposition and superficial ulcerations32 31798 4 Fibrin deposition at cuff site with superficial shaggy ulcerations33 31625 5 Circumferential band of discoloration and fibrin deposition with
ulcerations exposing several cartilaginous rings34 31750 7 Minor erosions at cuff site. (The cuff of this Portex tube was
pre-stretched)
* None of these patients had symptoms of upper airway obstruction at the time of death.
sistance for 4 to 7 days through an endo-tracheal tube only (Table 2).The tracheas were opened along the
membranous portion with the tracheostomy
tube in place, when possible. The locationof the tracheostomy was noted and used as
a reference point from which to measure
the location of the distal damage to the
FIG. 1. (Case 25) Trachea shows moderate damage to cartilages at balloon site. Tube wasin place for 19 days. a. (left) The portex tracheostomy tube is in place, deflated. The lateraltracheal walls are thinned and expanded at the balloon site. b. (right) Several rings of carti-lage have been exposed and fragmented at the cuff site. There is, also, a small ulcer down tothe cartilage located at the site of the tip of the tracheostomy tube.
336
TRACHEAL INJURY BY CUFFED TUBES
En= Ce
*- E-6-- o-C
b,C
vz (n v) En En EnC C.) .) C.)C
>1 >% >1 >1 1>
C.0
* -
En C. cn cnv
:^cu 4
9) tu 9 9 I 9 9 0 0 CC-i e6 4 C-4 _ e#) -4 -'
a) ZEoE°'a d 2 = 04*0v_i) ir)=C c e.0
C '
0 0
V0 (L
Cl4
o Co It ttw -.4 \0 ClCl
C\ -CoIf 00 00CC) mme
'I 00 Cl -4 0-C-\'w - '0 e enC )'I
1- 0% t-- O 00
CN) t- a) co) tr In0en
Cf) -'i CL 1'IC0% aC + 1O)00 I0 0_ cC O r) \C\ I!t I! m It -.1
tn 9 t- oc O -1 Cen en en n t It
0
.0
C.)
CN
~ ~.:20
u LL mCC) 4ctn~
En
CdCN la O
C4.)cd
LO ur) 'I
1'- 00\0 oot w )
r- ceQ C e- 0;
0 CI. 0
ZE 7 Ce°S0 C0
'C C\ CSNOC 0 I.
00 t- 0101 0%t- 0%4
C\ CO CI0%e I) dC
CN 1.C tf)
Volu(me 169Number 3
> 0 .d > En
ceCdDA° d Q
bcr.-0
C.)
to
0
0
C.)
s00
0d C e03-
C.)tO 0.
00 000-
4--S0;
if)
_O
Eum
0
-0
of
*t 0
0 -0
tofa
0 o
-C a
0s
4H
C.)
10
Cd u
¢)blo 0
337
.4
"0
cd
cd Q
0-._1
Cf0U2C..)
'm
oo
.12 c)
'-0
0cn
.0
i._o0 0
o- Q
Q-0
C.V)
0._
,<i -0
0.
.0
.C)o .~_
> 0
0 CfS.o
U cd
C)) EnC
0Q e
C.)
cn.
o En
u 0
oL
E*n 0
cn
-0 .
En °c°
Ce01
OCo
*_ 0v0-°
0C.
t.r
C.)u01.0S0
00.
a;rnC)
C.6
z:
COOPER AND GRILLO Annals of SurgeryMarch 1969
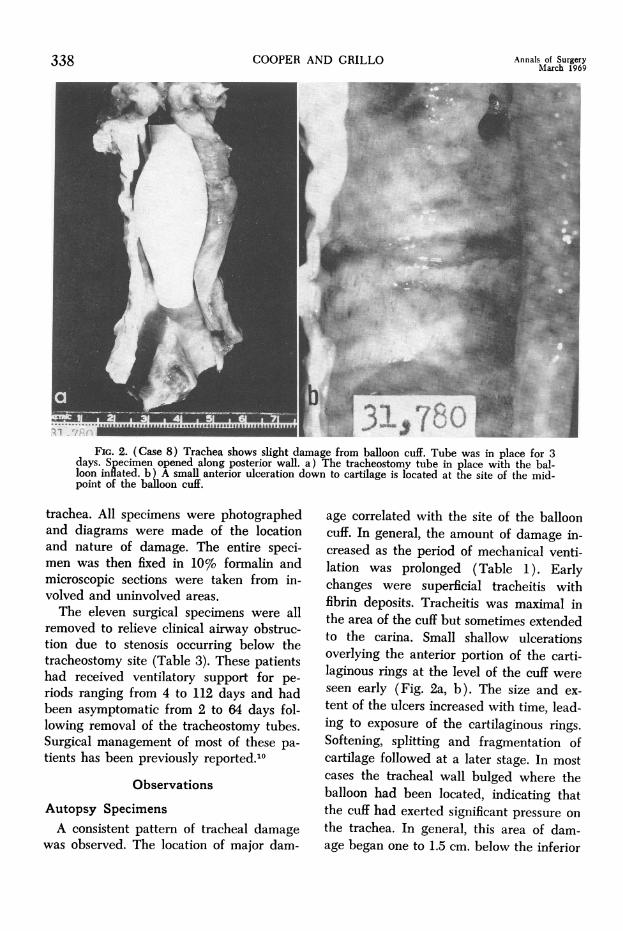
FIG. 2. (Case 8) Trachea shows slight damage from balloon cuff. Tube was in place for 3days. Specimen opened along posterior wall. a) The tracheostomy tube in place with the bal-loon inflated. b) A small anterior ulceration down to cartilage is located at the site of the mid-point of the balloon cuff.
trachea. All specimens were photographedand diagrams were made of the locationand nature of damage. The entire speci-men was then fixed in 10% formalin andmicroscopic sections were taken from in-volved and uninvolved areas.The eleven surgical specimens were all
removed to relieve clinical airway obstruc-tion due to stenosis occurring below thetracheostomy site (Table 3). These patientshad received ventilatory support for pe-riods ranging from 4 to 112 days and hadbeen asymptomatic from 2 to 64 days fol-lowing removal of the tracheostomy tubes.Surgical management of most of these pa-tients has been previously reported.10
Observations
Autopsy SpecimensA consistent pattern of tracheal damage
was observed. The location of major dam-
age correlated with the site of the ballooncuff. In general, the amount of damage in-creased as the period of mechanical venti-lation was prolonged (Table 1). Earlychanges were superficial tracheitis withfibrin deposits. Tracheitis was maximal inthe area of the cuff but sometimes extendedto the carina. Small shallow ulcerationsoverlying the anterior portion of the carti-laginous rings at the level of the cuff wereseen early (Fig. 2a, b). The size and ex-tent of the ulcers increased with time, lead-ing to exposure of the cartilaginous rings.Softening, splitting and fragmentation ofcartilage followed at a later stage. In mostcases the tracheal wall bulged where theballoon had been located, indicating thatthe cuff had exerted significant pressure onthe trachea. In general, this area of dam-age began one to 1.5 cm. below the inferior
338
TRACHEAL INJURY BY CUFFED TUBES 339
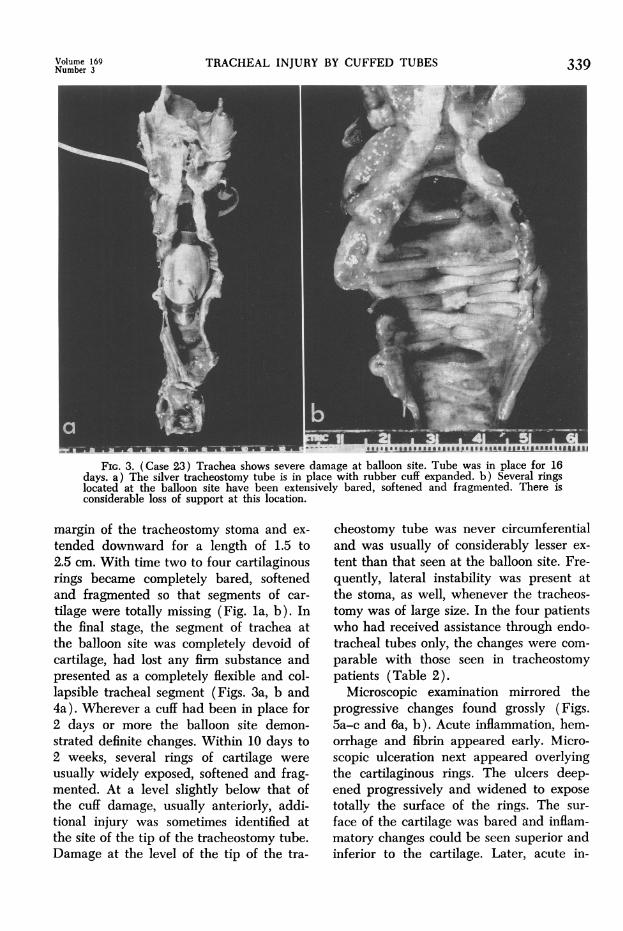
FIG. 3. (Case 23) Trachea shows severe damage at balloon site. Tube was in place for 16days. a) The silver tracheostomy tube is in place with rubber cuff expanded. b) Several ringslocated at the balloon site have been extensively bared, softened and fragmented. There isconsiderable loss of support at this location.
margin of the tracheostomy stoma and ex-
tended downward for a length of 1.5 to2.5 cm. With time two to four cartilaginousrings became completely bared, softenedand fragmented so that segments of car-
tilage were totally missing (Fig. la, b). Inthe final stage, the segment of trachea atthe balloon site was completely devoid ofcartilage, had lost any firm substance andpresented as a completely flexible and col-lapsible tracheal segment (Figs. 3a, b and4a). Wherever a cuff had been in place for2 days or more the balloon site demon-strated definite changes. Within 10 days to2 weeks, several rings of cartilage were
usually widely exposed, softened and frag-mented. At a level slightly below that ofthe cuff damage, usually anteriorly, addi-tional injury was sometimes identified atthe site of the tip of the tracheostomy tube.Damage at the level of the tip of the tra-
cheostomy tube was never circumferentialand was usually of considerably lesser ex-
tent than that seen at the balloon site. Fre-quently, lateral instability was present atthe stoma, as well, whenever the tracheos-tomy was of large size. In the four patientswho had received assistance through endo-tracheal tubes only, the changes were com-
parable with those seen in tracheostomypatients (Table 2).
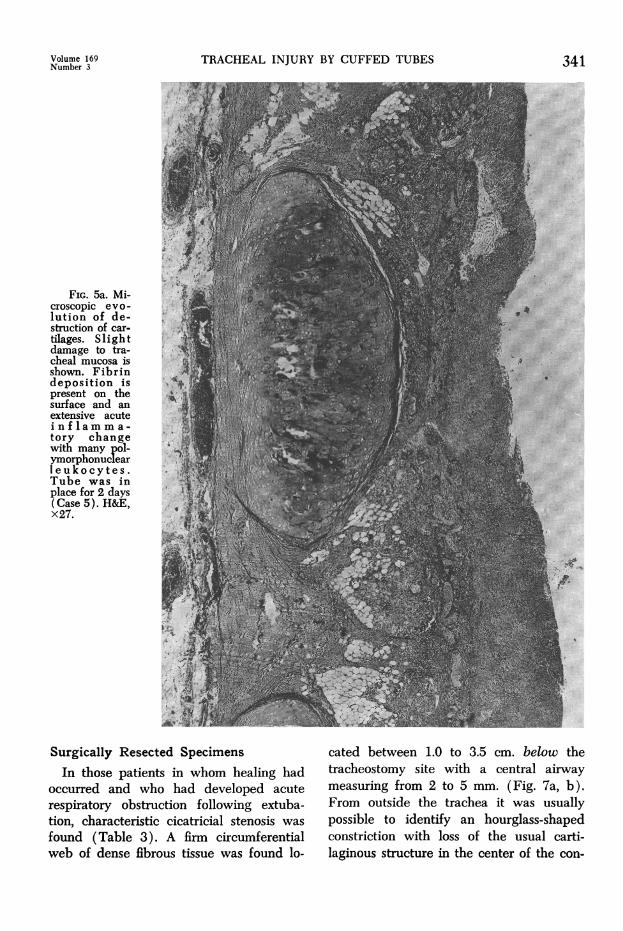
Microscopic examination mirrored theprogressive changes found grossly (Figs.5a-c and 6a, b). Acute inflammation, hem-orrhage and fibrin appeared early. Micro-scopic ulceration next appeared overlyingthe cartilaginous rings. The ulcers deep-ened progressively and widened to exposetotally the surface of the rings. The sur-
face of the cartilage was bared and inflam-matory changes could be seen superior andinferior to the cartilage. Later, acute in-
Volume 169Number 3
COOPER AND GRILLO Annals of SurgeryMarch 1969
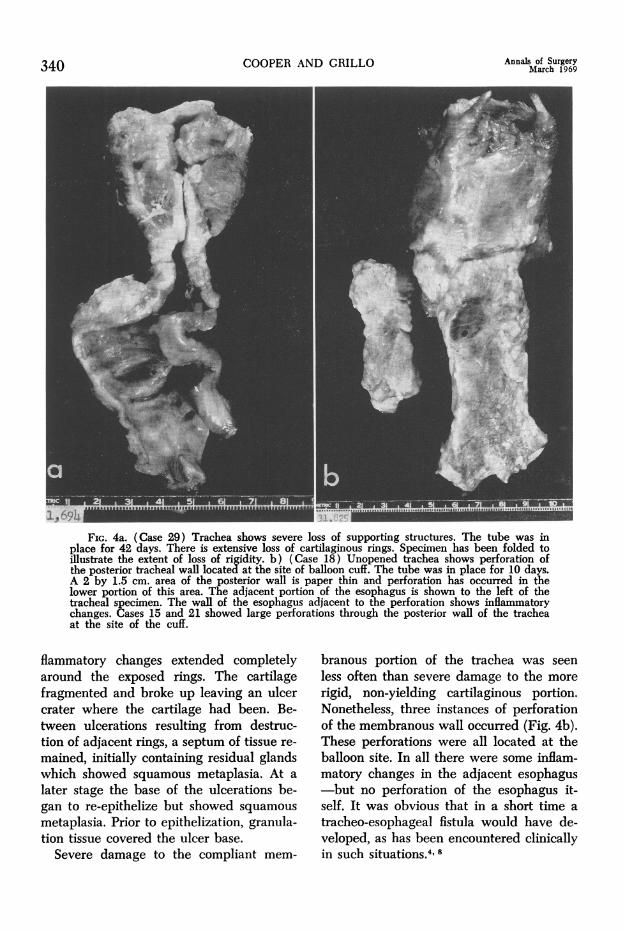
Fic. 4a. (Case 29) Trachea shows severe loss of supporting structures. The tube was inplace for 42 days. There is extensive loss of cartilaginous rings. Specimen has been folded toillustrate the extent of loss of rigidity. b) (Case 18) Unopened trachea shows perforation ofthe posterior tracheal wall located at the site of balloon cuff. The tube was in place for 10 days.A 2 by 1.5 cm. area of the posterior wall is paper thin and perforation has occurred in thelower portion of this area. The adjacent portion of the esophagus is shown to the left of thetracheal specimen. The wall of the esophagus adjacent to the perforation shows inflammatorychanges. Cases 15 and 21 showed large perforations through the posterior wall of the tracheaat the site of the cuff.
flammatory changes extended completelyaround the exposed rings. The cartilagefragmented and broke up leaving an ulcercrater where the cartilage had been. Be-tween ulcerations resulting from destruc-tion of adjacent rings, a septum of tissue re-
mained, initially containing residual glandswhich showed squamous metaplasia. At a
later stage the base of the ulcerations be-gan to re-epithelize but showed squamous
metaplasia. Prior to epithelization, granula-tion tissue covered the ulcer base.
Severe damage to the compliant mem-
branous portion of the trachea was seen
less often than severe damage to the more
rigid, non-yielding cartilaginous portion.Nonetheless, three instances of perforationof the membranous wall occurred (Fig. 4b).These perforations were all located at theballoon site. In all there were some inflam-matory changes in the adjacent esophagus-but no perforation of the esophagus it-self. It was obvious that in a short time a
tracheo-esophageal fistula would have de-veloped, as has been encountered clinicallyin such situations.4' 8
340
Volume 169Number 3
FIG. 5a. Mi-croscopic evo-lution of de-struction of car-tilages. Slightdamage to tra-cheal mucosa isshown. Fibrindeposition ispresent on thesurface and anextensive acutei n f Iam m a -tory changewith many pol-ymorphonuciearleukocytes.Tube was inplace for 2 days(Case 5). H&E,x27.
TRACHEAL INJURY BY CUFFED TUBES
Surgically Resected SpecimensIn those patients in whom healing had
occurred and who had developed acuterespiratory obstruction following extuba-tion, characteristic cicatricial stenosis wasfound (Table 3). A firm circumferentialweb of dense fibrous tissue was found lo-
341
*-s
cated between 1.0 to 3.5 cm. below thetracheostomy site with a central airwaymeasuring from 2 to 5 mm. (Fig. 7a, b).From outside the trachea it was usuallypossible to identify an hourglass-shapedconstriction with loss of the usual carti-laginous structure in the center of the con-
342*f..4. ... !.
COOPER AND GRILLO
striction and lesser degrees of damage forone centimeter proximal and distal to themid-point of the narrowing. Within, therewas further airway narrowing by the denseweb of scar tissue. The superior and in-ferior surfaces of this cicatricial tissue wereusually unepithelized, although in some ofthe prolonged cases metaplastic epitheliumcrept close to the remaining lumen. Inmany cases there was some degree of dam-age between the tracheostomy site and thelevel of this cicatricial web. This consisted
Annals of SurgeryMarch 1969
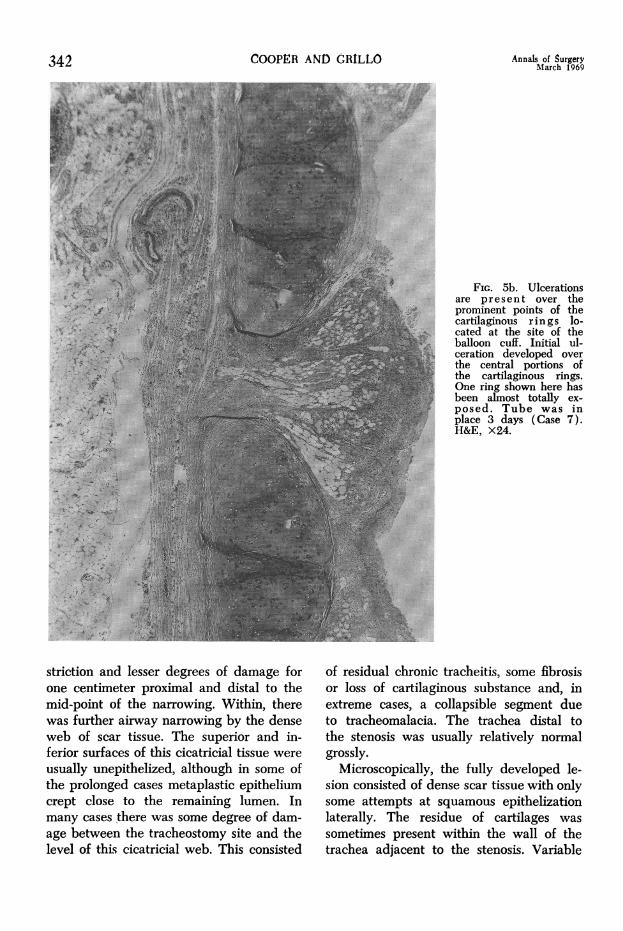
FIG. 5b. Ulcerationsare present over theprominent points of thecartilaginous r in gs lo-cated at the site of theballoon cuff. Initial ul-ceration developed overthe central portions ofthe cartilaginous rings.One ring shown here hasbeen almost totally ex-posed. Tube was inplace 3 days (Case 7).H&E, X24.
of residual chronic tracheitis, some fibrosisor loss of cartilaginous substance and, inextreme cases, a collapsible segment dueto tracheomalacia. The trachea distal tothe stenosis was usually relatively normalgrossly.
Microscopically, the fully developed le-sion consisted of dense scar tissue with onlysome attempts at squamous epithelizationlaterally. The residue of cartilages wassometimes present within the wall of thetrachea adjacent to the stenosis. Variable
Volume 160Number 3
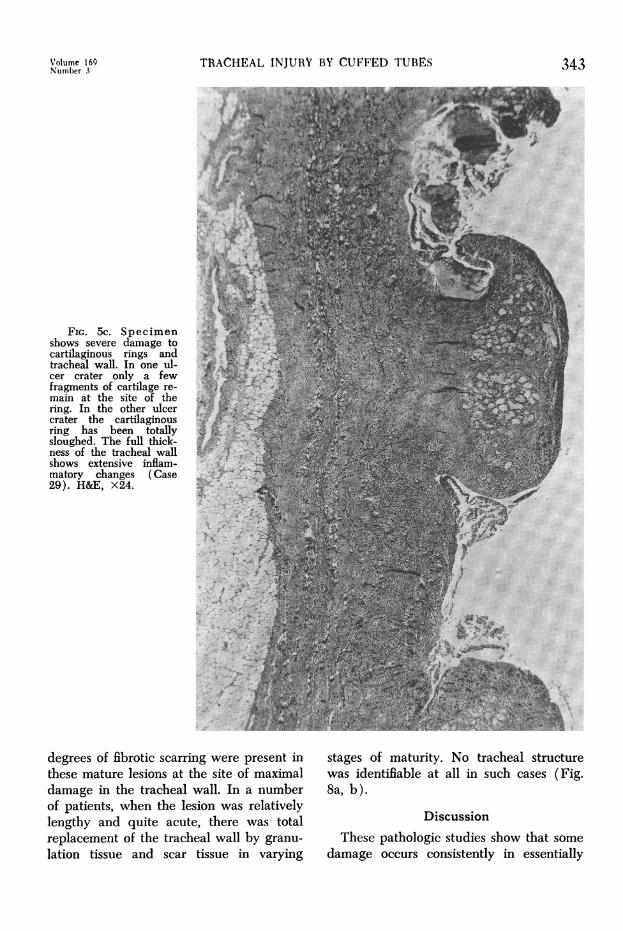
FIG. 5c. Specimenshows severe damage tocartilaginous rings andtracheal wall. In one ul-cer crater only a fewfragments of cartilage re-main at the site of thering. In the other ulcercrater the cartilaginousring has been totallysloughed. The full thick-ness of the tracheal wallshows extensive inflam-matory changes (Case29). H&E, X24.
TRACHEAL INJURY BY CUFFED TUBES
degrees of fibrotic scarring were present inthese mature lesions at the site of maximaldamage in the tracheal wall. In a numberof patients, when the lesion was relativelylengthy and quite acute, there was totalreplacement of the tracheal wall by granu-lation tissue and scar tissue in varying
343
stages of maturity. No tracheal structurewas identifiable at all in such cases (Fig.8a, b).
DiscussionThese pathologic studies show that some
damage occurs consistently in essentially
344 COOPER AND CRILLO Annals of SurgeryMarch 1969
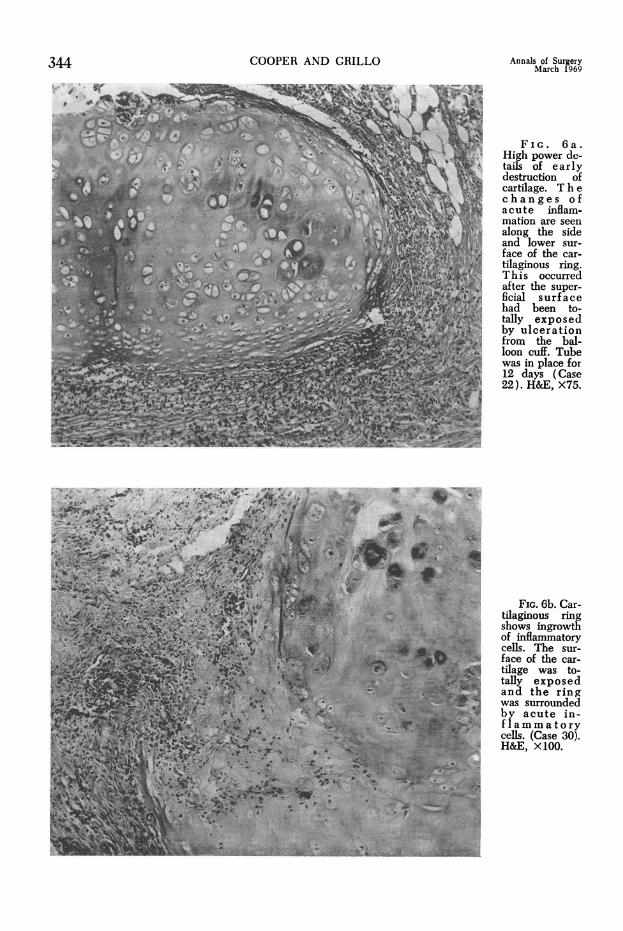
High power de-tails of earlydestruction ofcartilage. Thechanges of
X ~~~~~~~acute inflam-A ~~~~~~~~~~~~~mationare seen
along the sideand lower sur-face of the car-tilaginous ring.This occurredafter the super-ficial surfacehad been to-tally exposedby ulcerationfrom the bal-loon cuff. Tubewas in place for12 days (Case
1~~~~~~.. ~~~~~~~~~~~*75ic b.C r
4,;~~ ~ ~ ~ ~ ~ ~ '~~tlgiosrn-A ~~~ ~ ~ ~ ~ ~ ~~ ~hw inrot
cell. The sur-
i face of the car-tilage was to-tally exposedand the ringwas surroundedby acute in-ELr ~~ ~ ~~~~~~~~~~ ~~cells. (Case 30).H&E, x100.
Volume 169Number 3
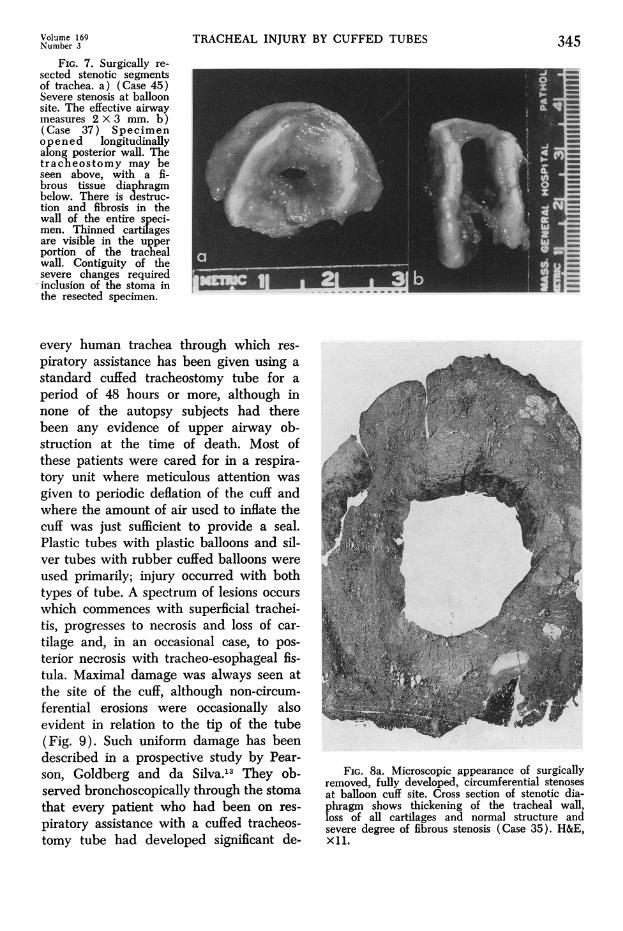
FIG. 7. Surgically re-sected stenotic segmentsof trachea. a) (Case 45)Severe stenosis at balloonsite. The effective airwaymeasures 2 X 3 mm. b)(Case 37) Specimenopened longitudinallyalong posterior wall. Thetracheostomy may beseen above, with a fi-brous tissue diaphragmbelow. There is destruc-tion and fibrosis in thewall of the entire speci-men. Thinned cartiTagesare visible in the upperportion of the trachealwall. Contiguity of thesevere changes requiredinclusion of the stoma inthe resected specimen.
TRACHEAL INJURY BY CUFFED TUBES
every human trachea through which res-piratory assistance has been given using astandard cuffed tracheostomy tube for aperiod of 48 hours or more, although innone of the autopsy subjects had therebeen any evidence of upper airway ob-struction at the time of death. Most ofthese patients were cared for in a respira-tory unit where meticulous attention wasgiven to periodic deflation of the cuff andwhere the amount of air used to inflate thecuff was just sufficient to provide a seal.Plastic tubes with plastic balloons and sil-ver tubes with rubber cuffed balloons wereused primarily; injury occurred with bothtypes of tube. A spectrum of lesions occurswhich commences with superficial trachei-tis, progresses to necrosis and loss of car-tilage and, in an occasional case, to pos-terior necrosis with tracheo-esophageal fis-tula. Maximal damage was always seen atthe site of the cuff, although non-circum-ferential erosions were occasionally alsoevident in relation to the tip of the tube(Fig. 9). Such uniform damage has beendescribed in a prospective study by Pear-son, Goldberg and da Silva.13 They ob-served bronchoscopically through the stomathat every patient who had been on res-piratory assistance with a cuffed tracheos-tomy tube had developed significant de-
345
FiG. 8a. Microscopic appearance of surgicallyremoved, fully developed, circumferential stenosesat balloon cuff site. Cross section of stenotic dia-phragm shows thickening of the tracheal wall,loss of all cartilages and normal structure andsevere degree of fibrous stenosis (Case 35). H&E,Xli.
346 COOPER AND CRILLO
grees of damage primarily at the site of thecuff. Tracheal damage due to cuffed tubeshas also been described by numerous ob-servers 1, 6, 9,15-17 and the pathology hasbeen described by Florange, Muller andForster.5 Damage due to erosion by thepressure of the cuff is of a much greatermagnitude than the superficial changes fol-lowing tracheostomy alone.2' 7, 14These present observations confirm that
pressure necrosis is the primary cause ofdamage. With shorter periods of injury,recovery may occur more easily. The de-
Annals of SurgeryMarch 1969
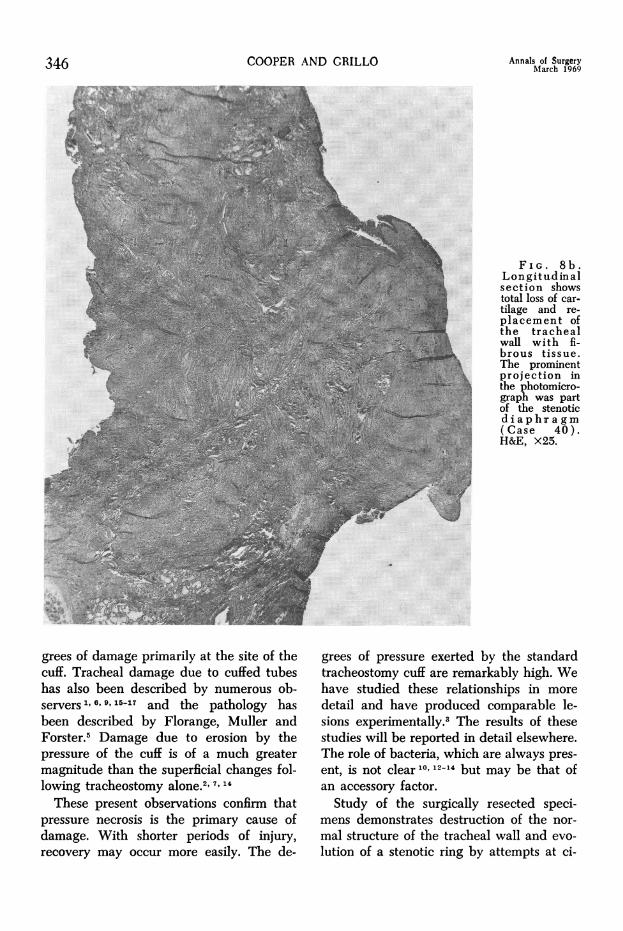
FIG. 8b.Lon gitu.d in alsection showstotal loss of car-tilage and re-placement ofthe trachealwall with fi-brous tissue.The prominentprojection inthe photomicro-graph was partof the stenoticdiaphragm( Case 40).H&E, X25.
grees of pressure exerted by the standardtracheostomy cuff are remarkably high. Wehave studied these relationships in moredetail and have produced comparable le-sions experimentally.3 The results of thesestudies will be reported in detail elsewhere.The role of bacteria, which are always pres-ent, is not clear'0, 12-14 but may be that ofan accessory factor.Study of the surgically resected speci-
mens demonstrates destruction of the nor-mal structure of the tracheal wall and evo-lution of a stenotic ring by attempts at ci-
TRACHEAL INJURY BY CUFFED TUBES
catricial healing (Fig. 9). Total loss ofstructure with replacement by granulationtissue permits no alternative to a concentriccicatrix which tends to contract with time.The process explains the general failure ofdilatation as a method of treatment-unlessthe lesion is not circumferential. The loca-tion and nature of the fully developedstenosis correlates with the location andnature of the tracheal injury found at theballoon site in the 30 autopsy specimens.It is clear that stenosis is the end stage ofhealing of the erosive processes seen in theautopsy specimens.
Since the lesion occurs at the site of thecuff it is not surprising that prolonged intu-bation with an endotracheal tube led to thesame type of erosion. The endotrachealtube itself may also cause pressure erosionat a narrow point of the airway-at cricoidlevel. Significant lesions may also occur atthe tracheostomy sites; such lesions are notnecessarily related to respiratory assistanceand have been well identified in the past.As more patients with respiratory failure
survive as a result of expert care and as
awareness of this clinical syndrome in-creases, the number of patients recognizedto have serious degrees of stenotic or ma-
lacic tracheal damage has increased stead-ily. The incidence of recognized clinicalsymptoms has risen as high as 15% of pa-tients surviving treatment for respiratoryfailure by these methods.8' 13 A remarkabledegree of narrowing may be accepted bythe relatively sedentary patient withoutsymptoms. Various attempts have beenmade to prevent these lesions, includinguse of alternately inflated double-cuffedtubes, intermittently inflated cuffs cycledto the respirator, serial readjustment of thelevel of the cuffed tube using spacers ofvarious types and the use of large boretubes with a respirator of high volumeflow. Each of these methods presents cer-
tain difficulties and complexities. We haverecently demonstrated that these lesionscan be prevented experimentally by use of
b
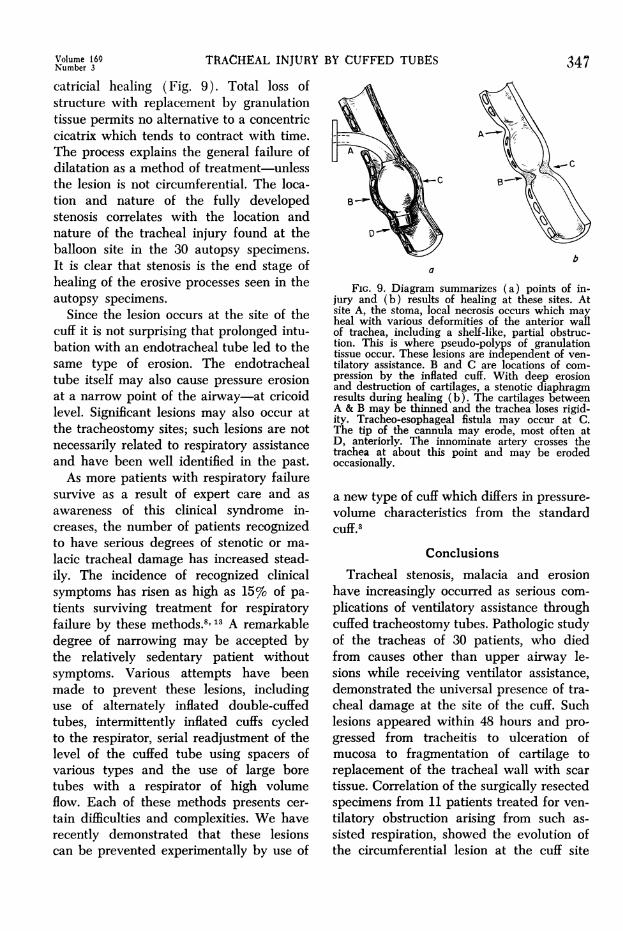
FIG. 9. Diagram summarizes (a) points of in-jury and (b) results of healing at these sites. Atsite A, the stoma, local necrosis occurs which mayheal with various deformities of the anterior wallof trachea, including a shelf-like, partial obstruc-tion. This is where pseudo-polyps of granulationtissue occur. These lesions are independent of ven-tilatory assistance. B and C are locations of com-pression by the inflated cuff. With deep erosionand destruction of cartilages, a stenotic diaphragmresults during healing (b). The cartilages betweenA & B may be thinned and the trachea loses rigid-ity. Tracheo-esophageal fistula may occur at C.The tip of the cannula may erode, most often atD, anteriorly. The innominate artery crosses thetrachea at about this point and may be erodedoccasionally.
a new type of cuff which differs in pressure-
volume characteristics from the standardcuff.3
ConclusionsTracheal stenosis, malacia and erosion
have increasingly occurred as serious com-
plications of ventilatory assistance throughcuffed tracheostomy tubes. Pathologic studyof the tracheas of 30 patients, who diedfrom causes other than upper airway le-sions while receiving ventilator assistance,demonstrated the universal presence of tra-cheal damage at the site of the cuff. Suchlesions appeared within 48 hours and pro-
gressed from tracheitis to ulceration ofmucosa to fragmentation of cartilage toreplacement of the tracheal wall with scar
tissue. Correlation of the surgically resectedspecimens from 11 patients treated for ven-tilatory obstruction arising from such as-
sisted respiration, showed the evolution ofthe circumferential lesion at the cuff site
Volume 169Number 3 347
COOPER AND GRILLO Annals of Surgery348 March 1969
into a tight, infrastomal stenosis by theusual processes of wound healing. The le-sions clearly result from pressure necrosiseven with well-managed conventional cuffs.Preventive measures must be based uponthese facts.
References1. Aboulker, P., Lissac, J. and Saint-Paul, O.:
De quelques accidents respiratoires dus anretrecissement du calibre laryngo-trachealapres tracheotomie. Acta Chir. Belg., 59:553,1960.
2. Bignon, J. and Chretien, J.: etude post-mortem des alterations laryngo-tracheo-bronchiques au cours de la tracheotomieavec respiration assistee. J. Franc. Med.Chir. Thor., 16:125, 1962.
3. Cooper, J. D. and Grillo, H. C.: ExperimentalProduction and Prevention of Injury Due toCuffed Tracheostomy Tubes, in preparation.
4. Flege, J. B., Jr.: Tracheo-Esophageal FistulaCaused by Cuffed Tracheostomy Tube. Ann.Surg., 166:153, 1967.
5. Florange, W., Muller, V. and Forster, E.:Morphologie de la necrose tracheale aprestracheotomie et utilisation d'une protheserespiratoire. Anesth. Analg., 22:693, 1965.
6. Foley, F. D., Moncrief, V. A. and Mason, A.D., Jr.: Pathology of the Lung in FatallyBurned Patients. Ann. Surg., 167:251, 1968.
7. Friedberg, S. A., Griffith, T. E. and Hass, G.M.: Histologic Changes in the Trachea Fol-lowing Tracheostomy. Ann. Otol., 74:785,1965.
8. Geffin, B. and Grullo, H. C.: Unpublished.9. Gibson, P.: Aetiology and Repair of Tracheal
Stenosis Following Tracheostomy and Inter-mittent Positive Pressure Respiration. Thorax,22:1, 1967.
10. Grillo, H. C.: The Management of TrachealStenosis Following Assisted Respiration. J.Thorac. Cardiovasc. Surg., Jan. 1969.
11. Grillo, H. C.: Comment, Symposium on Pul-monary Effects of Non-Thoracic Trauma.J. Trauma, 8:946, 1968.
12. Johnston, J. B., Wright, J. S. and Hercus, V.:Tracheal Stenosis Following Tracheostomy.J. Thorac. Cardiovasc. Surg., 53:206, 1967.
13. Pearson, F. G., Goldberg, M. and da Silva,A. J.: Tracheal Stenosis Complicating Tra-cheostomy with Cuffed Tubes: Clinical Ex-perience and Observations from a Prospec-tive Study. Arch. Surg., 97:380, 1968.
14. Sara, C.: Histological Change in the Tracheaand Bronchi with Tracheostomy. Med J.Australia, 6:1174, 1967.
15. Stiles, P. J.: Tracheal Lesions after Tracheos-tomy. Thorax 20:517, 1965.
16. Watts, J. McK.: Tracheostomy in ModemPractice. Brit. J. Surg., 50:954, 1963.
17. Yamasigawa, E. and Kirchner, J. A.: TheCuffed Tracheotomy Tube. Arch. Otolaryng.,79:80, 1964.