Embed Size (px)
Citation preview

Archives of Disease in Childhood 1995; 72: F71-F76 F71
Assessment and management of immunethrombocytopenia in pregnancy and in neonates
D L Cohen, T P Baglin
Department ofPaediatrics,Addenbrooke'sHospital, Cambridge,and 48th MedicalGroup (USAF) RAFLakenheath, SuffolkD L Cohen
Department ofHaematology,Addenbrooke'sHospital, CambridgeT P Baglin
Correspondence to:Dr D L Cohen, Departmentof Paediatrics,Addenbrooke's Hospital,Hills Road, CambridgeCB2 2QQ.
The use of electronic cell counters has led tothe recognition that pregnancy is frequentlyassociated with thrombocytopenia. As well asdisorders that cause thrombocytopenia in thenon-pregnant state, a reduction in the circulat-ing platelet count may result from thepregnancy itself, either as an incidental conse-quence, so-called 'gestational thrombocyto-penia', or as a manifestation of pregnancyassociated pathology, such as pre-eclampsia.Until recently autoimmune thrombocytopenia(ATP or ITP) was regarded as a commoncause of a low platelet count in pregnancy, butit now seems that most mild thrombocyto-penias in pregnancy are simply benign gesta-tional thrombocytopenia, with no implicationsfor morbidity in either mother or fetus.'Furthermore, it is now apparent that ITP inpregnancy is associated with considerably
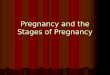
Thrombocytopenia in pregnancy
YesIs there evidence of systemic disease? - r Treat accordingly
No
Is there occult systemic disease Yeseg: antiphospholipid syndrome, HIV infection? Treat accordingly
No
Is platelet count No Gestational thrombocytopenia or<70? mild ITP- no intervention required
Yes
Bone marrow examination
YesIsthere primary marrow pathology? Treat accordingly
No
ITP
r l ~NoIs platelet count * No intervention
<50?
|Yes
Treat mother according tomaternal haemorrhagic risk
Figure 1
less morbidity to the fetus or neonate than waspreviously realised.
Neonatal illness is frequently and non-specifically associated with thrombocytopeniawhilst the distinct entity of neonatal allo-immune thrombocytopenia (NAIT) has beenwell characterised, and the high morbidity andmortality of this condition has been clarified.2
Understanding the complex associationbetween maternal and fetal-neonatal thrombo-cytopenia and the distinction between auto- andalloimmune platelet destruction is critical to themanagement of affected mothers and infants.Several papers published during the past fewyears have clarified many confusing issues relat-ing to the diagnosis and management of theseconditions.' 3-12 The purpose of this reviewis to summarise current concepts of immunethrombocytopenia in pregnancy and in the fetusor neonate, and in particular to emphasise thedistinction between auto-and alloimmunethrombocytopenia and the implications of thisknowledge for management.
Maternal thrombocytopenia andimplications for neonatal morbidityThe assessment and management of throm-bocytopenia in pregnancy is summarised infig 1.
Thrombocytopenia of less than 150X 109/1occurs in about 6-8% of pregnancies.3-5 If aplatelet count above 70X 109/1 is detected in ahealthy pregnant woman with no evidence ofsystemic disease or a history of ITP, the mostlikely diagnosis is benign gestational thrombo-cytopenia. This thrombocytopenic syndrome isnon-immune and is not associated with eithermaternal or fetal or neonatal morbidity or mor-tality. Affected pregnancies are not complicatedby excessive haemorrhage, and the infants arenot thrombocytopenic. The condition resolveswithin a few weeks of delivery. A recent largestudy of 15 932 neonates identified only oneinfant with a platelet count of less than50X 109/1 born to 756 mothers with presumedbenign gestational thrombocytopenia.3 Theplatelet count was greater than 20X109/1and the infant had Down's syndrome andcongenital marrow dysfunction.
However, thrombocytopenia associated withsystemic disease must always be excludedbefore diagnosing gestational thrombocyto-penia, because an alternative diagnosis mayhave major implications for mother and child.Maternal hypertensive disorders (including
on May 11, 2020 by guest. P
rotected by copyright.http://fn.bm
j.com/
Arch D
is Child F
etal Neonatal E
d: first published as 10.1136/fn.72.1.F71 on 1 January 1995. D
ownloaded from

F72 Cohen, Baglin
pre-eclampsia), diabetes mellitus, systemiclupus erythematosus, hyperthyroidism, throm-botic thrombocytopenic purpura (TTP),haemolytic uraemic syndrome (HUS), HIVinfection, and sepsis must be considered.Consumption coagulopathy caused byamniotic fluid embolism or intrauterine fetaldeath should be considered in thrombo-cytopenic women who are ill. Occasionallyprimary haematological disease such asleukaemia may present in pregnancy.'3 Bonemarrow examination is not necessary inpatients with stable thrombocytopenia of>70X 109/1 and no other features suggestive ofprimary marrow pathology. However, patientswith platelet counts of less than 70X 109/1, orwith any other haematological abnormality,should have a bone marrow examination toexclude marrow disease such as acuteleukaemia.ITP should be considered in otherwise
healthy women with thrombocytopenia, partic-ularly if there is a history of this disorder. ITPis a common disorder in young women. Withisolated thrombocytopenia for which there isno apparent cause, the diagnosis is primarilyone of exclusion. A rapid increase in plateletsfollowing administration of corticosteroid orhigh dose immunoglobulin confirms theimmune mechanism of platelet destruction,but immune thrombocytopenia secondaryto HIV infection or the antiphospholipidsyndrome is also responsive, and theseconditions should be considered before diag-nosing isolated primary platelet specific auto-immunity. Measurement of platelet associatedimmunoglobulin does not reliably differentiateITP from gestational thrombocytopenia as itis neither sensitive nor specific. Increasedplatelet associated immunoglobulin is fre-quently detected in normal women with nohaematological abnormality as well as inwomen with gestational thrombocytopenia andother thrombocytopenic syndromes. Thesemeasurements are therefore of little if anyvalue in the assessment of mild or moderatethrombocytopenia.'4 Women with a history ofITP which precedes pregnancy or who haveincidentally detected thrombocytopenia witha platelet count of <70X109/l should not beregarded as having simple gestationalthrombocytopenia because ITP is more likelyat this level of thrombocytopenia. Womenwith suspected ITP should be managed inaccordance with haematological guidelinesdesigned to prevent morbidity. Pregnantwomen with platelet counts of >50X 109/1 haveminimal bleeding risk and rarely require activeintervention. When the platelet count is<50X i09/1 an assessment must be maderegarding the degree of bleeding risk for thelevel of thrombocytopenia with respect to thestage of pregnancy, the anticipated mode ofdelivery, the need for epidural anaesthesiaand the presence of other complications. Ourpractice is to use standard corticosteroid treat-ment with prednisolone at 0*25 mg/kg as firstline treatment for pregnant women at risk ofbleeding.'5 Most women are responsive andtolerate this relatively low steroid dose without
any subsequent side effects. A maintenancedose that will achieve a haemostatic plateletcount can then be used until delivery. It isimportant to appreciate that complete normal-isation of the maternal platelet count is notrequired and low steroid doses can therefore bemaintained. Patients who are at risk of bleed-ing and who do not respond or tolerate steroidsmay require alternative treatment.'6ITP in pregnancy is caused by the production
of maternal autoantibodies specific for distinctepitopes on platelet membrane glycoproteins,particularly the IIb/IIIa and Ib/IX/V com-plexes.'7 The immune sensitised platelets areremoved from the circulation via bindingto Fc receptors expressed on the surface ofreticuloendothelial cells, primarily in the spleen.The fetus is at risk of immune platelet destruc-tion as the maternal autoantibody is activelytransported to the fetal circulation via Fcreceptors on the cells ofthe syncytiotrophoblast.However, the degree of fetal thrombocytopeniadoes not correlate with the amount of plateletreactive antibody in cord blood.'8 Clearly, thedegree of immune sensitisation of the plateletsurface is not the only factor that determines thecirculating platelet count, and the productivecapacity of the fetal marrow and maturity ofthe reticuloendothelial system are likely to beinfluential factors. Fetal thrombocytopenia iscommon, but only rarely have well documentedcases of intracranial haemorrhage been reportedin neonates born to mothers with ITP.8
Until recently there has been considerableconcern regarding the prevention of intra-partum or postpartum neonatal intracranialhaemorrhage but no method of assessing fetalwellbeing in terms of thrombocytopenia hasproved useful in this setting. However, it isnow clear that although 5-10% of infants bornto women with ITP may have platelet countsof <50X109/1, they rarely if ever have anydisease.3 The incidence of intracranialhaemorrhage in infants born to mothers withITP has been considered to be as high as1-2%8 but this may be an overestimate. Thisevent now seems to be so unusual in thrombo-cytopenic infants born to mothers with ITPthat the possibility of coexistent NAIT shouldbe considered. Maternal platelet antigen andalloantibody response should be determined ina reference laboratory to identify a cause forsevere thrombocytopenia other than thetransplacental passage of maternal autoanti-body in neonates with severe thrombo-cytopenia born to mothers with ITP. This isparticularly important as the incidence ofNAIT has probably been underestimated.2
There is now a rational basis for minimalintervention in women with ITP in pregnancy.Fetal morbidity is low but intrauterine assess-ment and treatment are difficult. There is noconsistent correlation between neonatal plateletcounts and maternal platelet antibody titres ormaternal platelet counts.18 Furthermore,administration of corticosteroids or high doseimmunoglobulin to the mother has not beenshown conclusively to affect fetal platelet countsor outcome.12 1920 Similarly, removal of thespleen may result in normalisation of maternal
on May 11, 2020 by guest. P
rotected by copyright.http://fn.bm
j.com/
Arch D
is Child F
etal Neonatal E
d: first published as 10.1136/fn.72.1.F71 on 1 January 1995. D
ownloaded from

Assessment and management ofimmune thrombocytopenia in pregnancy and in neonates F73
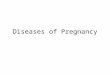
Neonatal thrombocytopenia
Is there recognisable congenital Yes Transfuse random plateletssyndrome i eesreg: TAR, haemangioma? if necessary
| No
Is there systemic illness Yes Treat underlying diseaseeg: sepsis? and support with randomdonor platelets if necessary
No
IF rProbable ITPIs mother thrombocytopenic Yes Treat with steroids orwithout systemic illness? intravenous Ig if platelets
<20 or if haemorrhageNo Exclude coexistent NAIT
Probable NAITTransfuse antigen-negative plateletsIf major haemorrhage infuse intravenous 1g andrandom donor platelets whilst awaitingselected platelets
Figure 2
platelet counts but the autoantibody may stillbe produced and the fetus or neonate may stillbe affected. The measurement of fetal scalpplatelet counts during labour is unreliable andoften underestimates the fetal platelet count,possibly leading to inappropriate intervention.21Given the exceedingly small risk of spontaneousintrauterine haemorrhage percutaneous umbili-cal blood sampling (PUBS) is not justified, par-ticularly as there is no effective therapeuticproduct that can be administered in utero iffetal bleeding occurs as the panspecific auto-antibody renders all platelets incom-patible. Caesarean section may not be less trau-matic than vaginal delivery and would beunwarranted for most infants with normal ormildly reduced platelet counts. The needfor caesarean section should be an obstetricdecision based on the haemostatic and obstetriccondition of the mother and the progress of thelabour. The relative safety of this procedure inthe context of fetal thrombocytopenia is notknown. While contention regarding the risk andoptimal therapeutic strategy remains,8 1l thereis increasing conservatism with respectto both investigation and intervention.1 12Mothers and obstetricians who wish to bereassured must understand that even thoughdetermination of fetal platelet counts can beaccomplished during pregnancy, without aspecific treatment such as exists for alloimmunethrombocytopenia, the risk of the diagnosticprocedure - for example, PUBS - may out-weigh any benefit should severe thrombo-cytopenia be detected.
In contrast to ITP, in which mothers andtheir fetuses may both be affected to somedegree, women who become sensitised to theirfetuses' dissimilar platelet antigens do notgenerally have thrombocytopenia during theirpregnancies, although the alloantibodies can,and often do, cause severe fetal andneonatal thrombocytopenia with associatedhaemorrhagic morbidity, including intracranial
haemorrhage and death - NAIT. Thus gesta-tional thrombocytopenia, maternal autoim-mune thrombocytopenia with transplacentalpassage of platelet autoantibody, and preg-nancy related maternal allosensitisation ofwomen against fetal platelet antigens withconsequent NAIT are very distinct entitieswith vastly different implications for manage-ment.
Neonatal immune thrombocytopeniaThe assessment and management of thrombo-cytopenia in the neonate is summarised infig2.The mean (SEM) platelet count in fetuses is
187 (47) X 109/1 at 15 weeks' gestation andincreases to 274 (47) X 109/1 at 40 weeks' gesta-tion.22 The normal infant at birth should havea platelet count which falls within the normaladult range and which therefore should be inexcess of 150)x 109/1. The incidence of throm-bocytopenia (defined as a platelet count<15OX109/l) in non-selected neonates isabout 0 8-1 0%.23 Though thrombocytopeniacan be a manifestation of many disorders,the mechanisms responsible are often multifac-torial and not fully understood. Elements ofproduction, destruction, intravascular aggrega-tion, sequestration or endothelial marginationmay all have some role in producing thrombo-cytopenia. Thrombocytopenia, substantialenough to cause morbidity (<50X 109/1),occurs much less frequently, with an incidenceof 0d12% (95% confidence interval 0 07 to0.19%).3 On the other hand, at least 20% ofinfants in special care baby units have plateletcounts of less than 15OX 109/l and about 4%have counts of less than 5OX 109/.7 About halfof these infants have increased platelet associ-ated IgG. This is due to various mechanisms,including specific targeting of platelet antigensin the minority and non-specific adherencein the majority. It is not known what con-tribution, if any, the platelet associatedimmunoglobulin makes to platelet survival inmost of these cases. Generally, the thrombo-cytopenia worsens after two to three days butresolves by day 10 in most infants whoseunderlying medical conditions are improving.
Neonatal thrombocytopenia has been associ-ated with many conditions.7 Sepsis (with orwithout disseminated intravascular coagula-tion), congenital infections, intrauterine growthretardation, necrotising enterocolitis, poly-cythaemia, pre-eclampsia, asphyxia, respiratorydistress syndrome, persistent pulmonary hyper-tension, mechanical ventilation, phototherapy,hyperalimentation, exchange transfusion,haemolytic disease and other conditionscharacterised by clinical instability in sickneonates are frequently associated withthrombocytopenia. HIV infection can causethrombocytopenia in infants, though theincidence of this in neonates without othercauses of thrombocytopenia has not yet beenclarified. Rare congenital marrow disordersmay result in amegakaryocytic thrombo-cytopenia - for example, the syndrome ofthrombocytopenia and absent radii (TAR).24
on May 11, 2020 by guest. P
rotected by copyright.http://fn.bm
j.com/
Arch D
is Child F
etal Neonatal E
d: first published as 10.1136/fn.72.1.F71 on 1 January 1995. D
ownloaded from

F74 Cohen, Baglin
The Kasabach-Merritt syndrome with con-sumptive thrombocytopenia may occur withvisceral haemangiomas in the absence ofcutaneous manifestations. Fetal or neonatalthrombocytopenia has also been reported inassociation with maternal disease, includinghypertension, thyroid disease, diabetes mellitusand systemic lupus erythematosus.Immune thrombocytopenia should be consid-
ered in any infant with bleeding in whomcommonly associated illnesses associated withthrombocytopenia have been excluded. Itshould also be considered in well term infantswith isolated thrombocytopenia. Most infantsidentified as having thrombocytopenia inthe absence of systemic disease or a definedcongenital syndrome associated with thrombo-cytopenia usually have either autoimmune oralloimmune thrombocytopenia. The plateletserves as a target for antibody, usually IgGderived from the mother via transplacentaltransfer. Mild or moderate thrombocytopeniain a neonate whose mother has thrombocyto-penia suggests autoimmune thrombocytopeniaand hence a low risk of morbidity. However,women whose spleens have been removed mayhave persistent antibody production but lowclearance of platelets while clinically importantplatelet destruction can occur in the fetus. It isalso now recognised that infants may haveautoimmune thrombocytopenia in the absenceof maternal autoimmune thrombocytopenia,so-called occult autoimmunity.25 Nevertheless,neonatal thrombocytopenia with a normalmaternal platelet count in the absence ofprevious spleen removal in the mother stronglysuggests alloimmune thrombocytopenia.NAIT is very different from autoimmune
thrombocytopenia, with major morbidity and asubstantial risk of mortality. Up to 30% ormore of fetuses or neonates may experienceintracranial haemorrhage and die, or survivewith variable long term morbidity as sequelaeto porencephaly, hydrocephalus, develop-mental retardation or seizure disorders.26Improved laboratory techniques are useful fordifferentiating autoimmune from alloimmunethrombocytopenia.27 28 The HPA plateletalloantigen system is responsible for 75% ofcases of NAIT in Caucasians29 with otherplatelet membrane glycoproteins with biallelicautosomal dominant inheritance involved inother cases. Class II MHC molecules functionas immune response modifiers to plateletalloantigens with the risk of development ofNAIT closely linked to the DRW52 locus.2 Ithas also been suggested that HLA antigensmay serve as primary targets for alloantibodymediated fetal thrombocytopenia although thisproposal requires further study.30 While analo-gous to Rhesus isosensitisation of red cells interms of antibody production, the condition isdifferent in its effects as it frequently occurs inthe first pregnancy. About 50% of infants withNAIT are first births and 97% of subsequentpregnancies are affected.2 Thus recurrence insubsequent siblings is very common and is therule rather than the exception. As maternalthrombocytopenia is not present and plateletantigen and alloantibody screening are not
yet routinely performed the only predictivefactor for this condition may be a history of apreviously affected child or a more remotepositive family history.The true incidence of HPA alloimmunisa-
tion has been presumed to be of the order of1 in 500-1 in 2000, but comprehensive popu-lation data are only now becoming available.Similarly, the actual morbidity and mortalitycaused by this disorder are now being clarified.In contrast to autoimmune thrombocytopenia,specific treatment is available for affectedfetuses. Protocols using fetal ultrasoundexaminations beginning early in gestation,blood sampling (via percutaneous umbilicalblood sampling), fetal platelet transfusions,maternal steroids and intravenous gamma-globulin have been developed and haveresulted in improved outcomes, both in termsof platelet counts and morbidity in fetuses andinfants born to mothers with a previouslyaffected pregnancy.31-35 Early delivery as soonas fetal maturity is achieved shortens the riskperiod for haemorrhage. Administration ofhigh dose immunoglobulin to the motherresults in an increase in the fetal plateletcount.32 Intrauterine platelet transfusion iseffective in increasing fetal platelet counts andpreventing haemorrhage but may have to bestarted as early as 18 weeks.36 Prospectivescreening programmes have now shown thatNAIT usually develops in neonates born towomen with detectable antiplatelet antibody.37On the basis of these recent observations, Fluget al have suggested that all pregnant womenshould have their HPA status determined.2Those who are homozygous for HPA2with detectable anti-HPAI antibody shouldhave PUBS performed at 20 weeks. If thefetal platelet count is <100X 1I09/1 themother should receive weekly intravenousimmunoglobulin. If the repeat PUBS six weekslater reveals a count of >30X 109/l treatmentshould be continued; if it is <30x 109/1intrauterine antigen negative platelet trans-fusions should be administered to the fetus atweekly intervals. Homozygous HPA2 womenwithout detectable antibody should be retestedat monthly intervals and if antibody becomesdetectable they should be managed in theabove manner. A count of 50x 109/1 has beensuggested as a discriminant level for decidingon vaginal delivery or elective section.2Ongoing studies should determine if this is afeasible approach but there may be logisticproblems of access to PUBS and the costeffectiveness of this approach may have to beproved.
Affected infants usually present at birth orsoon after with purpura or evidence ofintracranial haemorrhage. It has been assumedthat outcome following intracranial haemor-rhage subsequent to immune thrombocyto-penia usually has a poor prognosis but a morefavourable outcome in neonates affected byimmune thrombocytopenia has recently beenreported.38 When a neonate is found to haveNAIT an urgent management decision isrequired based on the degree of thrombo-cytopenia and the extent of haemorrhage.
on May 11, 2020 by guest. P
rotected by copyright.http://fn.bm
j.com/
Arch D
is Child F
etal Neonatal E
d: first published as 10.1136/fn.72.1.F71 on 1 January 1995. D
ownloaded from

Assessment and management ofimmune thrombocytopenia in pregnancy and in neonates F75
Infants with severe thrombocytopenia andhaemorrhagic manifestations should receiveantigen negative platelets using either themother's washed platelets or antigen typed,non-maternal, donor platelets. Intravenousimmunoglobulin should also be consideredand may be effective in increasing the plateletcount.39 An infant with purpura and severethrombocytopenia requires rapid interventionand a cranial computed tomography scan.Platelet products should ideally be irradiatedto prevent graft versus host disease GvHD andshould preferably be from a cytomegalovirus(CMV) negative donor. The use of irradiatedplatelets or CMV negative blood will be deter-mined by the degree of thrombocytopenia andinstitutional guidelines.Autoimmune neonatal thrombocytopenia is
essentially a maternal disease which occurs inthe neonate as a result of the transplacentalpassage of maternally produced autoantibodydirected against various glycoproteins on theplatelet surface. Thrombocytopenia in affectedinfants is usually mild and the rare instances ofsevere morbidity nearly always occur in infantswhose mother's ITP produced the currentpregnancy. Intracranial haemorrhage is rare.Treatment of the affected infants is rarelynecessary or advisable in the absence ofbleeding. If treatment is necessary then intra-venous immunoglobulin or oral prednisoloneshould be considered in the first instance.Platelet transfusions are unlikely to be helpful asthe antibody target is common to all plateletsbut may be useful adjunctively after intravenousimmunoglobulin in a few patients with severehaemorrhage.
ConclusionITP in pregnant women is essentially a mater-nal disease with a very low risk of morbidity tothe fetus. Intervention should be in response tothe needs of the mother, recognising thatsevere thrombocytopenia caused by transfer ofmaternal autoantibody to the fetus or neonateis exceptional. In contrast, in NAIT alloimmu-nisation ofthe maternal immune system resultsin transplacental transfer of alloantibody withhigh affinity typically for the platelet mem-brane glycoprotein IIIa. Platelet destruction issevere and thrombocytopenia with a high riskof major haemorrhage is common. Specificeffective treatment is available and thereforeNAIT should be diagnosed and treatedas soon as possible to prevent neonatalmorbidity and mortality. Screening women intheir first pregnancy for HPA2 homozygosityand detection of anti-HPAl antibody maypermit identification of high risk fetuses andintervention in utero to prevent antepartumintracranial haemorrhage.
1 Aster R. Gestational thrombocytopenia, a plea for conserva-five management. NEnglJrMed 1990; 323: 264-6.
2 Flug F, Karpatkin M, Karpatkin S. Should all pregnantwomen be tested for their platelet PLA (Zw, HPA-1)phenotype? BrJ Haematol 1994; 86: 1-5.
3 Burrows R, Kelton J. Fetal thrombocytopenia and itsrelation to maternal thrombocytopenia. N Engi J Med1993; 329: 1463-6.
4 Burrows R, Kelton J. Incidentally detected thrombocyto-penis in healthy mothers and their infants. N EnglJ3 Med1988; 319: 142-5.
5 Burrows R, Kelton J. Thrombocytopenia at delivery. Am JfObstet Gynecol 1990; 162: 731-4.
6 Bussel J, Kaplan C, McFarland J. Recommendation for theevaluation and treatment of neonatal autoimmune andalloimmune thrombocytopenia. Thromb Haemastas 1991;65: 631-4.
7 Andrew M. The hemostatic system in the infant. In: NathanD, Oski F, eds. Hematology of infancy and childhood.4th edn. Philadelphia: WB Saunders & Co, 1993:115-27.
8 Samuels P, Bussel J, Braitman L, Tomaski A, Druzin M,Mennuti M, et al. Estimation of the risk of thrombo-cytopenia in the offspring of pregnant women with pre-sumed immune thrombocytopenic purpura. N EnglJ Med1990; 323: 229-35.
9 Kaplan C, Daffos F, Forestier F, Tertian G, Catherine N,Pons J, et al. Fetal platelet counts in thrombocytopenicpregnancy. Lancet 1991; 336: 979-82.
10 Bussel J, Druzin M, Cines D, Samuels P.Thrombocytopenia in pregnancy. Lancet 1991; 337: 251.
11 McCrae K, Samuels P, Schreiber A. Pregnancy-associatedthrombocytopenia: pathogenesis and management. Blood1992; 80: 2697-714.
12 Burrows R, Kelton J. Thrombocytopenia in pregnancy. In:Greer I, Turpie A, Forbes C, eds. Haemostasis and throm-bosis in obstetrics and gynaecology. London: Chapman &Hall, 1992: 407-29.
13 Roy V, Gutteridge C, Nysenbaum A, Newland A.Combination chemotherapy with conservative obstetricmanagement in the treatment of pregnant patients withacute myeloblastic leukaemia. Clin Lab Haematol 1989;11: 171-8.
14 Kelton J, Powers P, Carter C. A prospective study of theusefulness of the measurement of platelet-associated IgGfor the diagnosis of idiopathic thrombocytopenic purpura.Blood 1982; 60: 1050-3.
15 Bellucci S, Charpak Y, Chastang C, Tobelem G, PurpuraC, and the Cooperative Group on Immune Thrombo-cytopenic Purpura. Low doses v conventional doses ofcorticoids in immune thrombocytopenic purpura (ITP).Blood 1988; 71: 1165-9.
16 Manoharan A. Treatment of refractory idiopathic thrombo-cytopenic purpura in adults. Br Jf Haematol 1991; 79:143-7.
17 Van Leeuwan E, Van der Van J, Engelfriet C, von demBorne A. Specificity of autoantibodies in autoimmunethrombocytopenia. Blood 1982; 59: 23-6.
18 Scott J, Rote N, Cruikshank D. Antiplatelet antibodies andplatelet counts in pregnancies complicated by autoimmunethrombocytopenia. Am J7 Obstet Gynecol 1983; 145: 932-9.
19 Karpatkin M, Porges R, Karpatkin S. Platelet counts ininfants of women with autoimmune thrombocytopenia,effect of steroid administration to the mother. N Engl JfMed 1981; 305: 936-8.
20 Christiaens G, Niewenhuis H, Von den Borne A,Ouwehand W, Helmerhorst F, Van Dalen C, et al.Idiopathic thrombocytopenic purpura in pregnancy: arandomised trial on the effect of antenatal low dose corti-coids on neonatal platelet count. Br J Obstet Gynaecol1990; 97: 893-8.
21 Christiaens G, Helmerhorst F. Validity of intrapartum diag-nosis of fetal thrombocytopenia. Am 7 Obstet Gynecol1987; 157: 864-5.
22 Van den Hof M, Nicolaides K. Platelet count in normal,small and anemic fetuses. Am J Obstet Gynecol 1990; 162:735-9.
23 Dreyfus M, Morel-Kopp M, Verdy E, Schlegel N, KaplanC, Tchernia G. Immune neonatal thrombocytopenia:Unexpected results of a multicentric prospective study innon selected patients. Blood 1993; 82 (suppl 1): 582a.
24 Hall J, Levin J, Kuhn J, et al. Thrombocytopenia withabsent radius. Medicine 1969; 48: 411-39.
25 Tchernia G, Morel-Kopp M, Yvart J, Kaplan C. Neonatalthrombocytopenia and hidden maternal autoimmunity.BrJHaematol 1993; 84: 457-63.
26 Naidu S. Central nervous system lesions in neonatalisoimmune thrombocytopenia. Arch Neurol 1983; 40:552-4.
27 Clemenceau S, Perichon B, Elion J, Kaplan C,Krishnamoorthy R. An improved DNA based identifica-tion of fetuses at risk for HPA-la (PLA1) neonatal allo-immune thrombocytopenia. Br J Haematol 1994; 86:198-200.
28 Pao M, Karlowicz M, Kickler T, Zinchan W. Importance ofplatelet serologic testing for defining the cause of neonatalthrombocytopenia. Am J Ped Hematol Oncol 1991; 13:71-6.
29 Von Dem Borne A, Van Leeuwan W, Von Riesz I, VanBoxtel C, Engelfriet C. Neonatal alloimmune thrombo-cytopenia: Detection and characterisation of the respon-sible antibodies by the platelet immunofluorescence test.Blood 1981; 57: 649-56.
30 Lalezari P, Dimitrova A, Diwan A, Einarson M. HLAincompatibility is the most common cause of neonatalalloimmune thrombocytopenia. Blood 1993; 82 (suppl 1):203a.
31 Bussel J, Berkowitz R, McFarland J, Lynch L, Chitkara U.Antenatal treatment of neonatal alloimmune thrombo-cytopenia. NEnglJ3Med 1988; 319: 1374-8.
32 Lynch L, Bussel J, McFariand J, Chitkara U, Berkowitz R.Antenatal treatment of neonatal alloimmune thrombo-cytopenia. Obstet Gynecol 1992; 80: 67-71.
33 Bussel J, McFarland J, Berkowitz R. Antenatal managementof fetal alloimmune and autoimmune thrombocytopenia.Transfusion Medicine Review 1990; 2: 49-62.
on May 11, 2020 by guest. P
rotected by copyright.http://fn.bm
j.com/
Arch D
is Child F
etal Neonatal E
d: first published as 10.1136/fn.72.1.F71 on 1 January 1995. D
ownloaded from

F76 Cohen, Baglin
34 Nicolini U, Rodeck C, Kochenour N, Greco P, Fisk NM,Letsky E, et al. In-utero platelet transfusion for allo-immune thrombocytopenia. Lancet 1988; ii: 506.
35 Daffos F, Forestier F, Muller J, Reznikoff-Etievant MF,Habibi B, Capella-Parlovsky M, et al. Prenatal treatment ofalloimmune thrombocytopenia. Lancet 1984; ii: 632.
36 Murphy M, Metcalfe P, Waters A, Ord J, Hambley H,Nicolaides K. Antenatal management of severe feto-maternal alloimmune thrombocytopenia: HLA incompat-ibility may affect responses to platelet transfusions. Blood1993; 81: 2174-9.
37 McFarland J, Frenzke M, Aster R. Testing of maternal serain pregnancies at risk for neonatal alloimmune thrombo-cytopenia. Transfusion 1989; 29: 128-33.
38 Bussel J, Tanli S, Peterson Hart de C. Favourable outcomein 7 cases of perinatal intracranial haemorrhage due toimmune thrombocytopenia. Am J Ped Hematol Oncol1991; 13: 156-9.
39 Uinder N, Shapiro S, Moser A, Roitman J, Engelhard D.Treatment of thrombocytopenia with high dose intra-venous gamma globulin. Dev Pharmacol Ther 1990; 14:205-8.ii8
on May 11, 2020 by guest. P
rotected by copyright.http://fn.bm
j.com/
Arch D
is Child F
etal Neonatal E
d: first published as 10.1136/fn.72.1.F71 on 1 January 1995. D
ownloaded from