Embed Size (px)
Citation preview

Digestive Endoscopy
(2005)
17
, 159–163
Blackwell Science, LtdOxford, UKDENDigestive Endoscopy0915-56352005 Blackwell Publishing Asia Pty LtdApril 2005172159163Original Article
SONOGRAPHIC ASSESSMENT OF ESOPHAGEAL CANCERH IWASE Et al.
Correspondence: Hiroaki Iwase, Department of Gastroenterology,Nagoya Medical Center, 4-1-1 Sannomaru, Naka-ku, Nagoya 460-0001,Japan. Email: [email protected]
Received 5 October 2004; accepted 6 December 2004.
ORIGINAL ARTICLE
ASSESSMENT OF TRANSENDOSCOPIC MINIATURE ULTRASONIC PROBE FOR CHEMORADIOTHERAPY OUTCOME IN PATIENTS WITH
LOCALLY ADVANCED ESOPHAGEAL CANCER
H
IROAKI
I
WASE
, M
ASAAKI
S
HIMADA
, T
OMOYUKI
T
SUZUKI
, R
EIKO
D
OI
, M
ASAYUKI
O
KEYAAND
K
EIKO
K
OBAYASHI
Department of Gastroenterology, Nagoya Medical Center, Nagoya, Japan
Background
: Assessment of the response of esophageal cancer to chemoradiotherapy is difficult. We investigated the valueof a transendoscopic miniature ultrasonic probe (USP) in assessing response to chemoradiotherapy in patients with locallyadvanced esophageal cancer.
Methods
: A total of 33 patients were entered in this prospective study. Response to treatment was evaluated according toWorld Health Organization criteria. According to the sonographic image, complete response (CR) of the primary lesionwas divided into two subcategories: confirmed CR (cCR) and unconfirmed CR (uCR).
Results
: Initial sonographic criteria for evaluating tumor depth and lymph nodes in the 33 patients before therapy showedtwo cases of T2N0, four of T3N0, 15 of T3N1, four of T4N0, and eight of T4N1. Following chemoradiotherapy, CR wasobtained in 18 (54.5%): seven cCR and 11 uCR. Eleven were partial response (PR) (33.3%), while three were stable disease(SD) and one was progressive disease (PD). High frequency USP (20 MHz) was able to detect tumor disappearance andrestoration of the esophageal wall. One-year survival rates among CR (cCR
+
uCR), PR and SD
+
PD were 100%, 70%and 0%, respectively. A significant difference in survival was evident among CR, PR and SD
+
PD (
P
<
0.001). Three-yearsurvival rates between cCR and uCR were 100% and 40%, respectively. A significant difference in survival was evidentbetween cCR and uCR (
P
<
0.001). In seven cases of uCR, local recurrence and distant metastasis appeared within 1 year,and five died of disease progression. Not one cCR case has relapsed.
Conclusion
: USP, which can be accomplished with a standard endoscopy, including biopsy, in one procedure, is a usefulmethod for objectively assessing the response to chemoradiotherapy in patients with locally advanced esophageal cancer.
Key words: chemoradiotherapy, confirmed complete response (cCR), esophageal cancer, ultrasonic probe.
INTRODUCTION
Despite recent increased feasibility and efficacy of che-moradiotherapy for locally advanced esophageal cancer,assessment of the response of esophageal cancer to chemo-radiotherapy is difficult. Thoracic computed tomography(CT) does not sensitively reflect major reductions of localdisease. Endoscopy and barium esophagogram demonstrateonly intraluminal changes. Endoscopic ultrasonography(EUS) can image the infiltration depth of the tumor andregional lymph node involvement. It is considered the besttechnique for staging of local esophageal cancer and has beenused for assessing tumor regression after neoadjuvant ther-apy.
1–5
Measurement of tumor size by EUS is a reliablemethod for assessing tumor regression before surgery,
1–3
andit can detect residual tumor infiltration after chemoradiother-apy of esophageal cancer even in the absence of endoscopiclesions.
6
However, the limited manual control and the narrowfield of view make the assessment difficult, while failure to
transverse a highly stenotic lesion prevents full assessment ofthe lesion. A recently developed transendoscopic miniatureultrasonic probe (USP) has been shown to have importantpotential in the diagnosis of esophageal disease.
7
It can beused with standard endoscopy, easily allowing both endo-scopic evaluation and biopsy in a single procedure. Com-pared to conventional EUS, high-frequency USP mightassess even more correctly and in greater detail the completeresponse (CR) to multimodality therapy for esophageal can-cer. The purpose of this prospective study was to determinewhether the assessment of USP of chemoradiotherapy-induced tumor regression or disappearance was of prognosticrelevance in patients with locally advanced esophagealcancer.
PATIENTS AND METHODS
Patients
We studied patients with locally advanced esophageal cancerwho were treated with chemoradiotherapy. All patientsunderwent sonographic T (depth of tumor invasion) and N(regional lymph node metastasis) staging with USP. Theyunderwent abdomen and chest CT scanning to rule out met-astatic disease that was not detected with USP. Patients withdistant metastases on CT scanning were excluded.

160 H IWASE
ET AL.
Instruments
The USP used in this study was the Sp 701 (radial ultrasoundin a single system made by Fujinon Company, Utsunomiya,Japan). There are four switchable types of USP: 7.5 MHz,12 MHz, 15 MHz and 20 MHz; selection depends on tumorsize. In general, the 7.5 MHz or 12 MHz USP were used toassess the whole tumor before treatment and regional lymphnode disease. The 15 MHz USP was used for detecting resid-ual tumor and the 20 MHz USP was used for determiningtumor disappearance and restoration of the esophageal wallafter treatment. USP was carried out by two professionalexaminers.
Method
Patients were prepared for endoscopy in the usual manner.Transendoscopic USP examination was carried out with thewater-repletion method. TNM classification according to thesonographic image was initially carried out before treatment.The second examination was performed 2 weeks after thelast chemoradiation treatment to allow inflammation to sub-side. A third evaluation was done 2 months after the secondevaluation. Responses to treatment were evaluated accord-ing to World Health Organization criteria. CR was definedas complete disappearance of tumor by ultrasound imageand endoscopic assessment, including biopsy. According tothe ultrasound image, CR of the primary lesion was dividedinto two subcategories: confirmed CR (cCR) and uncon-firmed CR (uCR). cCR was defined as complete restorationof the over six-layered wall (Fig. 1): the hyperechoic outermembrane, three layers of hypo-, hyper- and hypoechoicmaking up the muscularis propria, and two or three layers ofhyper- (hypo-) and hyperechoic making up the mucosa andsubmucosa. Complete covering of the lesion by cicatricialtissue after tumor disappearance was evaluated as cCR(Fig. 2). uCR is defined as restoration of undistinguishablewall layers (Fig. 3). Partial response (PR) was defined as agreater than 50% reduction in the sum of the products of the
perpendicular diameters of lesions on sonographic image. Anew lesion or enlargement exceeding the original tumor sizeby 25% was defined as progressive disease (PD). All otherpatients were categorized as having stable disease (SD).Regional lymph nodes were assessed when the primarylesion was evaluated.
The data for tumor in all responders were reviewed byother doctors.
Fig. 1.
Sonographic image is the complete restoration of theover six-layered wall which showed confirmed completeresponse (cCR).
Fig. 2.
After tumor disappearance, the lesion was completelycovered by cicatricial tissue (
↓
). Sonographic image wasdiagnosed as confirmed complete response (cCR).
Fig. 3.
Sonographic image is the restoration ofundistinguishable wall layers that showed unconfirmed completeresponse (uCR).

SONOGRAPHIC ASSESSMENT OF ESOPHAGEAL CANCER 161
RESULTS
A total of 33 patients (30 men, three women) who metstudy criteria were identified during the period from April1999 to May 2003. The mean age was 65 (range, 51–81)years. All patients had histologically confirmed squamouscell carcinoma. Twenty-four patients had several malignantstructures in the lesion. The USP was able to pass thestenosis and display the whole tumor. The sonographicimage of the tumor (Fig. 4) was relatively homogeneousand hypoechoic with irregular outer borders, distinctly dif-ferent from the adjacent aorta, left ventricle and bronchus.The 7.5 MHz USP could detect the tumor depth andregional lymph node diseases more clearly compared tochest CT scanning.
Initial sonographic criteria for evaluating T and N in the33 patients before therapy showed two cases of T2N0, fourof T3N0, 15 of T3N1, four of T4N0, and eight of T4N1. Allpatients completed chemotherapy and concurrent mediasti-nal radiation of over 40 Gy; 10 patients underwent chemo-therapy with cisplatin and the oral 5-FU agent, UFT (tegafurin combination with uracil), while 23 patients received cispl-atin and a different oral 5-FU agent, S-1 (tegafur in combi-nation with gimestat and otastat potassium). Informedconsent was obtained from all patients. For patients whoshowed response to chemoradiotherapy, additional chemo-therapy (UFT/CDDP or S-1/CDDP) was given two timesevery 4 weeks. All patients were followed for a minimum of12 months or until death.
Sonographic assessment after chemoradiotherapy
The second USP evaluation was done in 32 patients. Onepatient could not be examined because of clinically progres-
sive disease. In tumors responding to chemoradiotherapy,transmural lesions and malignant stenosis were reduced.The USP was able to measure the reduced tumor (Fig. 5),even if it was within the muscularis propria. The high fre-quency USP (20 MHz) detected T1 stage residual tumorand restoration of the esophageal wall with disappearanceof the tumor. At the second evaluation, restaging showed 18cases of T0N0, one of T1N1, three of T2N0, five of T2N1,one of T3N0, three of T3N1, and one of T4N1. In responseto chemoradiotherapy, 18 were CR (54.5%): seven cCR and11 uCR. Eleven were PR (33.3%), while three were SD,and one was PD. Stage T0 meant cCR or uCR. All uCRcases showed two layers of the outside hypoechoic andinside hypoechoic thickening wall. A third evaluation wasdone in 26 patients. Six patients could not be examinedbecause of progression of disease, which was assessed byCT and their general condition. Restaging was as follows:14 T0N0, one T1M1, three T2M1, one T3N0, two T3N1, andfive T4N1. Five of 11 uCR patients at second evaluationbecame cCR.
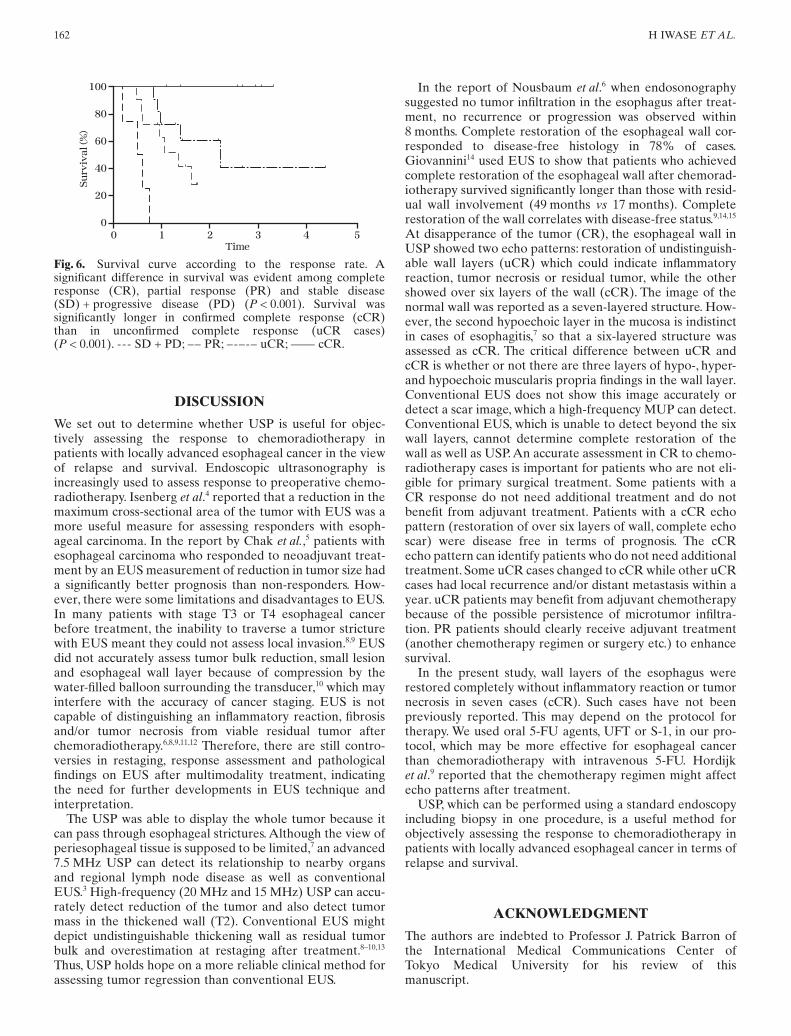
Survival
Figure 6 shows the survival curve including all cases accord-ing to the response rate at the second evaluation. One-yearsurvival rates among CR (cCR
+
uCR), PR and SD
+
PDwere 100% 70%, and 0%, respectvely. A significant differ-ence in survival was evident among CR, PR and SD
+
PD(
P
<
0.001). Three-year survival rates between cCR and uCRwere 100% and 40%, respectively. A significant difference insurvival was evident between cCR and uCR (
P
<
0.001). Inseven cases of uCR, local recurrence and distant metastasisappeared within 1 year, and five died of disease progression.Not one cCR case has relapsed.
Fig. 4.
Sonographic image of esophageal cancer is relativelyhomogeneous and hypoechoic with irregular outer borders.Tumor is apparently separate from adjacent organs.
Fig. 5.
Reduced tumor after chemoradiotheray is measured inthe sonographic image (
↓
).
162 H IWASE
ET AL.
DISCUSSION
We set out to determine whether USP is useful for objec-tively assessing the response to chemoradiotherapy inpatients with locally advanced esophageal cancer in the viewof relapse and survival. Endoscopic ultrasonography isincreasingly used to assess response to preoperative chemo-radiotherapy. Isenberg
et al
.
4
reported that a reduction in themaximum cross-sectional area of the tumor with EUS was amore useful measure for assessing responders with esoph-ageal carcinoma. In the report by Chak
et al.
,
5
patients withesophageal carcinoma who responded to neoadjuvant treat-ment by an EUS measurement of reduction in tumor size hada significantly better prognosis than non-responders. How-ever, there were some limitations and disadvantages to EUS.In many patients with stage T3 or T4 esophageal cancerbefore treatment, the inability to traverse a tumor stricturewith EUS meant they could not assess local invasion.
8,9
EUSdid not accurately assess tumor bulk reduction, small lesionand esophageal wall layer because of compression by thewater-filled balloon surrounding the transducer,
10
which mayinterfere with the accuracy of cancer staging. EUS is notcapable of distinguishing an inflammatory reaction, fibrosisand/or tumor necrosis from viable residual tumor afterchemoradiotherapy.
6,8,9,11,12
Therefore, there are still contro-versies in restaging, response assessment and pathologicalfindings on EUS after multimodality treatment, indicatingthe need for further developments in EUS technique andinterpretation.
The USP was able to display the whole tumor because itcan pass through esophageal strictures. Although the view ofperiesophageal tissue is supposed to be limited,
7
an advanced7.5 MHz USP can detect its relationship to nearby organsand regional lymph node disease as well as conventionalEUS.
3
High-frequency (20 MHz and 15 MHz) USP can accu-rately detect reduction of the tumor and also detect tumormass in the thickened wall (T2). Conventional EUS mightdepict undistinguishable thickening wall as residual tumorbulk and overestimation at restaging after treatment.
8–10,13
Thus, USP holds hope on a more reliable clinical method forassessing tumor regression than conventional EUS.
In the report of Nousbaum
et al
.
6
when endosonographysuggested no tumor infiltration in the esophagus after treat-ment, no recurrence or progression was observed within8 months. Complete restoration of the esophageal wall cor-responded to disease-free histology in 78% of cases.Giovannini
14
used EUS to show that patients who achievedcomplete restoration of the esophageal wall after chemorad-iotherapy survived significantly longer than those with resid-ual wall involvement (49 months
vs
17 months). Completerestoration of the wall correlates with disease-free status.
9,14,15
At disapperance of the tumor (CR), the esophageal wall inUSP showed two echo patterns: restoration of undistinguish-able wall layers (uCR) which could indicate inflammatoryreaction, tumor necrosis or residual tumor, while the othershowed over six layers of the wall (cCR). The image of thenormal wall was reported as a seven-layered structure. How-ever, the second hypoechoic layer in the mucosa is indistinctin cases of esophagitis,
7
so that a six-layered structure wasassessed as cCR. The critical difference between uCR andcCR is whether or not there are three layers of hypo-, hyper-and hypoechoic muscularis propria findings in the wall layer.Conventional EUS does not show this image accurately ordetect a scar image, which a high-frequency MUP can detect.Conventional EUS, which is unable to detect beyond the sixwall layers, cannot determine complete restoration of thewall as well as USP. An accurate assessment in CR to chemo-radiotherapy cases is important for patients who are not eli-gible for primary surgical treatment. Some patients with aCR response do not need additional treatment and do notbenefit from adjuvant treatment. Patients with a cCR echopattern (restoration of over six layers of wall, complete echoscar) were disease free in terms of prognosis. The cCRecho pattern can identify patients who do not need additionaltreatment. Some uCR cases changed to cCR while other uCRcases had local recurrence and/or distant metastasis within ayear. uCR patients may benefit from adjuvant chemotherapybecause of the possible persistence of microtumor infiltra-tion. PR patients should clearly receive adjuvant treatment(another chemotherapy regimen or surgery etc.) to enhancesurvival.
In the present study, wall layers of the esophagus wererestored completely without inflammatory reaction or tumornecrosis in seven cases (cCR). Such cases have not beenpreviously reported. This may depend on the protocol fortherapy. We used oral 5-FU agents, UFT or S-1, in our pro-tocol, which may be more effective for esophageal cancerthan chemoradiotherapy with intravenous 5-FU. Hordijk
et al
.
9
reported that the chemotherapy regimen might affectecho patterns after treatment.
USP, which can be performed using a standard endoscopyincluding biopsy in one procedure, is a useful method forobjectively assessing the response to chemoradiotherapy inpatients with locally advanced esophageal cancer in terms ofrelapse and survival.
ACKNOWLEDGMENT
The authors are indebted to Professor J. Patrick Barron ofthe International Medical Communications Center ofTokyo Medical University for his review of thismanuscript.
Fig. 6.
Survival curve according to the response rate. Asignificant difference in survival was evident among completeresponse (CR), partial response (PR) and stable disease(SD) + progressive disease (PD) (
P
< 0.001). Survival wassignificantly longer in confirmed complete response (cCR)than in unconfirmed complete response (uCR cases)(
P
< 0.001). --- SD + PD; –– PR; –-–-– uCR; —— cCR.

SONOGRAPHIC ASSESSMENT OF ESOPHAGEAL CANCER 163
REFERENCES
1. Botet JF, Lightdale CJA, Zauber G, Gerdes H, UrmacherC, Brennan MF. Preoperative staging of esophageal cancer:comparison of endoscopic US and dynamic CT.
Radiology
1991;
181
: 419–25.2. Willis J, Cooper GS, Isenberg G
et al.
Correlation of EUSmeasurement with pathologic assessment of neoadjuvanttherapy response in esophageal cancer.
Gastrointest.Endosc.
2002;
55
: 655–61.3. Ota M, Murata Y, Ide H
et al.
Useful endoscopic ultrasonog-raphy to assess the efficacy of neoadjuvant therapy foradvanced esophageal carcinoma: Based on the responseevaluation criteria in solid tumors.
Dig. Endosc.
2005;
17
: 59–63.
4. Isenberg G, Chak A, Canto MI
et al.
Endoscopic ultrasoundin restaging of esophageal cancer after neoadjuvant chemo-radiation.
Gastrointest. Endosc.
1998;
48
: 158–63.5. Chak A, Canto MI, Cooper GS
et al.
Endosonographicassessment of multimodality therapy predicts survival ofesophageal carcinoma patients.
Cancer
2000;
88
: 1788–95.6. Nousbaum JB, Robasezkiewies M, Cauvin JM, Calament G,
Gouerou H. Endosonography can detect residual tumorinfiltration after chemoradiotherapy of esophageal cancer inthe absence of endoscopic lesions.
Gut
1992;
33
: 1459–61.7. Xu GM, Niu YL, Zuo XP
et al.
The diagnostic value oftransendoscopic miniature ultrasonic probe for esophagealdisease.
Endoscopy
1998;
30
(Suppl.): A28–32.8. Souquel JC, Napoleon B, Descos F, Vallete PJ, Lambert
R. Contribution of endosonography to the follow up
esophageal squamous cell carcinoma treated by multimo-del protocol.
Gastrointest. Endosc.
1991;
48
: 243(Abstract).
9. Hordijk ML, Kok TC, Wilson HP, Milder AH. Assessmentof response of esophageal carcinoma to induction chemo-therapy.
Endoscopy
1993;
25
: 592–3.10. Kawano T, Ohshima M, Iwai T. Early esophageal carci-
noma: endoscopic ultrasonography using the sonoprobe.
Abdom. Imaging
2003;
28
: 477–85.11. Dittler HJ, Fink U, Siewert GR. Response to chemotherapy
in esophageal cancer.
Endoscopy
1994;
26
: 769–71.12. Roubein D, DuBrow R, David C
et al.
Endoscopic ultra-sonography in the quantitative assessment of response tochemotherapy in patients with adenocarcinoma of theesophagus and esophagogastric junction.
Endoscopy
1993;
25
: 587–91.13. Murata Y, Suzuki S, Ohta M
et al.
Small ultrasonic probefor determination of the depth of superficial esophageal can-cer.
Gastrointest. Endosc.
1996;
44
: 23–8.14. Giovannini M, Seitz JF, Thomas P
et al.
Endoscopic ultra-sonography for assessment of response to combined radio-therapy and chemotherapy in patients with esophagealcancer.
Endoscopy
1997;
29
: 4–9.15. Giovannini M, Seitz JF, Perrier H, Fourdan O, Rabbia I,
Gouvernet J. Locoregional involvement evaluated by endo-scopic ultrasound (EUS) is a useful factor for predictingsurvival in patients with inoperable squamous cell esoph-ageal carcinoma (SEC) treated by concomitant radiationtherapy and chemotherapy (RT-CT): results of 67 patients.
Gastroenterology
1995;
108
: A474 (Abstract).























![[C2] Preoperative radiotherapy and chemoradiotherapy for](https://img.pdfslide.us/doc/110x75/6159a52ce5e78c2242485b77/c2-preoperative-radiotherapy-and-chemoradiotherapy-for-.jpg)




