Embed Size (px)
Citation preview

hagcssehr
Assessment of Topical Hemostats in a Renal HemorrhageModel in Heparinized Rats
David D. Tuthill, D.V.M.,1 Vladislav Bayer, B.S., Anne M. Gallagher, B.S.,William N. Drohan, Ph.D., and Martin J. MacPhee, Ph.D.
American Red Cross, Holland Laboratory, Rockville, Maryland 20855
Journal of Surgical Research 95, 126–132 (2001)doi:10.1006/jsre.2000.6027, available online at http://www.idealibrary.com on
00;
Submitted for publication May 18, 20Various topical hemostatic agents or devices havebeen employed to address the challenges associatedwith hemorrhage from parenchymal organs duringsurgery or trauma. Their relative efficacy, however,has not been assessed in a single animal model. Theobjective of this study was to develop a small animalrenal hemorrhage model for comparing hemostatic ef-ficacy of various topical agents, and then to comparefibrin sealant (FS) to an existing standard of care fortopical hemostasis. A left heminephrectomy was per-formed in anesthetized adult male Sprague–Dawleyrats. Animals were anticoagulated with 2000 IU/kgheparin IV and various topical hemostatic agents wereapplied to the injury. Treatment groups included FSapplied as a spray; FS applied through a cannula; gel-atin sponge (GS) soaked in 1000 IU/mL thrombin solu-tion; GS soaked in 300 IU/mL thrombin; dry GS; andfibrinogen without thrombin applied as a spray. Themain endpoints of the study were incidence of hemo-stasis, blood loss, acute survival trends, and mainte-nance of mean arterial pressure (MAP). Three treat-ment groups, the two FS groups and the GS soaked in1000 IU/mL thrombin, afforded significant hemostasiscompared to the controls (P < 0.01). Both FS groups
ad significantly less blood loss, longer survival times,nd maintained higher MAPs than the GS-treatedroups. Quantitative dose effects and functional defi-iencies in topical hemostatic products could be as-essed using this animal model. The study demon-trated that liquid FS was significantly morefficacious than a GS soaked in thrombin for abatingemorrhage from a renal excision in a heparinizedat. © 2000 Academic Press
1
To whom correspondence should be addressed at American RedCross, Holland Laboratory, PDL, 15601 Crabbs Branch Way, Rock-ville, MD 20855. Fax: (301) 738-0764. E-mail: [email protected].1260022-4804/00 $35.00Copyright © 2000 by Academic PressAll rights of reproduction in any form reserved.
published online December 13, 2000
Key Words: animal model; hemorrhage; fibrin seal-ant; fibrinogen; Gelfoam; heparin; hemostasis; surgi-cal; rats; thrombin.
INTRODUCTION
Injuries to parenchymal organs represent a specialchallenge for surgical hemostasis. Hemorrhage fromparenchymal organs may be life-threatening if the in-jury is severe, especially in the presence of coagulopa-thies [1]. Conventional hemostatic techniques such aspressure, ligature, or cautery may have limited effec-tiveness and are often impractical. Passive topical he-mostatic agents provide an attractive matrix for endog-enous clot formation, but are not highly effective ifclotting mechanisms are impaired. In contrast, activetopical hemostats provide exogenous clotting agents tothe injury site.
Fibrin sealants are active hemostatic agents utiliz-ing the mixture of a fibrinogen concentrate with athrombin preparation to form fibrin at the site of in-jury. The intrinsic ability of fibrin sealants to formfibrin clots irrespective of endogenous coagulationmechanisms offers a means for effective topical hemo-stasis of injuries in coagulopathic patients [2, 3]. Whilefibrin sealants represent the most effective topical he-mostatic technology yet developed, an assessment ofthe relative potency of these and other topical hemo-static agents has been difficult as their disparate effi-cacies have been demonstrated in different animalmodels, precluding their comparison using a singletechnique.
The animal model described in this report was de-veloped as an assay to gauge the relative performance
of topical hemostatic agents, especially the fibrin seal-ants, in a challenging surgical setting. These goalshave traditionally been carried out in medium-to-
wsgup
aswas
OS
large-sized animals such as dogs, pigs, and sheep, be-cause small animal hemostasis models are difficult todevelop. The small total body blood volume, limitedsurgical field, anesthetic considerations, and highly ef-ficient clotting profiles of many smaller mammals havelimited their use as animal models for surgical or trau-matic hemorrhage control. In contrast to other renalhemorrhage models in the rat [4, 5] a goal in thedevelopment of this model was to produce a consis-tently lethal parenchymal organ injury by inducing ahighly coagulopathic state. This was accomplished bythe use of a high dose of intravenous heparin thatexaggerated blood loss and allowed acute survivaltrends to be used as an experimental endpoint.
The purpose of the study was twofold: to evaluate theutility of the animal model for its intended purpose,and to compare a fibrin sealant to another topical he-mostatic technique. The study was designed to assessthe capability of the animal model to distinguish vary-ing degrees of topical hemostasis by testing a fibrinsealant product applied by two different methodsagainst clinically relevant comparators (gelatin spongeused dry or soaked in thrombin) and appropriate con-trol groups.
The animal model was shown to be a sensitive andefficient means of comparing topical hemostaticagents. This study demonstrated the superior efficacyof a fibrin sealant preparation in controlling hemor-rhage from parenchymal organ injuries in the presenceof marked coagulopathy compared to the use of gelatinsponges alone or in combination with thrombin. Theresults also provided some insight into the appropriateapplication of fibrin sealant in such settings.
MATERIALS AND METHODS
Animals
Male Sprague–Dawley rats (Harlan Sprague–Dawley, Indianapo-lis, IN) 120–180 days old and weighing between 400 and 500 g wereused in this study. They were held in the AALAC-accredited animalfacility at the American Red Cross (ARC) Holland Laboratory andwere handled in accordance with the Animal Welfare Act and theNIH Guide for the Care and Use of Laboratory Animals. This projectwas approved by the Institutional Animal Care and Use Committeeof the ARC Holland Lab.
Experimental Design
Model development included groups of sham operations (full sur-gical procedure including all steps except the renal injury and treat-ment) with either 2000 IU/kg heparin or an equivalent volume (0.2mL) of saline administered iv, and nontreated groups (injury pro-duced but no treatment applied) with the animals given either salineor heparin at 500, 1000, or 2000 IU/kg iv, in the same solutionvolumes (0.2 mL). Nontreated animals were randomly assigned theirheparin dosage and the surgeons were unaware which dose of hep-
TUTHILL ET AL.: TOPICAL HEM
arin was administered. All animals in the treatment groups weregiven 2000 IU/kg heparin iv. The renal injury was treated with oneof the following agents: (1) dry Gelfoam; (2) Gelfoam soaked in 300IU/mL thrombin solution; (3) Gelfoam soaked in 1000 IU/mL throm-
bin solution; (4) fibrinogen solution applied as a spray in combinationwith a CaCl2 solution with no thrombin; (5) fibrin sealant applied
ith a cannula-tip applicator; and (6) fibrin sealant applied with apray-tip applicator. Animals were randomly assigned to treatmentroups and investigators performing the procedures were blindedntil the moment treatment was applied, and were blinded whereossible to variations in treatments.
Hemostatic Agent Preparation
The fibrin sealant used in this study consisted of clinical grade,virally inactivated, human plasma-derived, topical fibrinogen com-plex (TFC) and thrombin, provided by the American Red Cross. TheTFC was packaged in vials containing 400 mg TFC, which weredissolved in 3.3 mL sterile water to make the protein concentration120 mg/mL. Separate vials containing 1000 IU/vial of thrombin weredissolved in 3.3 mL of aqueous 40 mM CaCl2 to make a solution of300 IU/mL thrombin. Two separate syringes (3 cc) were used to drawup 1.5 mL of each component solution. The two syringes were at-tached to a Y-shaped Duoflo (Haemedics, Inc., Malibu, CA) device inwhich the solutions were mixed as they passed through either aspray-tip or a cannula-tip applicator. Equal mixing of the compo-nents as they were applied to the injury site produced final concen-trations of 60 mg/mL TFC and 150 IU/mL thrombin in the fibrinsealant (FS) solution. The fully loaded apparatus was kept at 37°Cuntil ready for use, although for no more than 4 h. Fibrinogensolution at 120 mg/mL was applied in the absence of thrombin, but inconjunction with the 40 mM CaCl2 solution, using the spray-tippplicator in the same manner as with the fibrin sealant. A hemo-tatic gelatin sponge (GS) (Gelfoam 100, Upjohn Co., Kalamazoo, MI)as cut into rectangular pieces approximately 15 by 20 mm. Thegent was applied either dry or soaked in the appropriate thrombinolution—300 or 1000 IU/mL thrombin in 40 mM CaCl2. The throm-
bin solutions were the same as were used in the FS preparations. The1000 IU/mL concentration was chosen to represent the standard forsurgeons who clinically use gelatin sponges soaked in bovine throm-bin preparations. When used dry, the Gelfoam was gently flattenedbetween fingertips before application. When used wetted, the Gel-foam was submerged in a thrombin solution, gently squeezed toremove air bubbles, and resubmerged in the solution at 37°C untilready for use. Just before application the soaked Gelfoam was gentlyblotted and weighed.
Surgical and Experimental Procedure
Anesthesia was induced and maintained with intraperitoneal in-jection of urethane (Sigma; 50% weight per volume aqueous solutionprepared daily) at a dose of 1.0 g/kg, followed by buprenorphine(Buprenex, Reckitt and Colman Pharmaceuticals, Richmond, VA) at0.15 mg/kg and atropine sulfate (Phoenix Pharmaceuticals, Inc., St.Joseph, MO) at 0.06 mg/kg administered together intramuscularly.If surgical plane of anesthesia was not reached within 15 min anadditional dose of urethane up to one-half of the initial dose wasadministered intraperitoneally. Once anesthetized, the animal’s hairwas shaved on the ventral neck and the left paralumbar region andthe skin swabbed with alcohol. A rectal thermoprobe was insertedand the body temperature of the animal was brought to between 38and 40°C and maintained with the aid of a heating pad and a heatinglamp connected to a thermoregulating control unit (Phystemp,Clifton, NJ). A pressure microtransducer (Millar Instruments, Inc.,Houston, TX) was introduced approximately 2 cm into the rightcommon carotid artery through a ventral neck incision and bloodpressure data collection was initiated. Pressures were observed for atleast 5 min and the surgical procedure continued only if the meanarterial pressures were above 90 mm Hg and the heart rates between
127TATS IN RENAL HEMORRHAGE
350 and 550 bpm for 3 consecutive min. The left kidney was exposedvia a left paralumbar incision. Two stay sutures were placed bilat-erally in the fatty tissue proximal to the renal poles to maintaindistraction of the kidney. Any blood loss occurring up to this point

tgfltbkchfsTwotkwtwgsififhto
Sl
.7
.0
.3
was blotted with preweighed gauze and its weight recorded as pre-treatment blood loss. The procedure was continued after an obser-vation period of at least 5 min, or when the core body temperaturereached at least 38°C. Heparin (Heparin Sodium Injection, USP frombeef lung, Upjohn Co.) was administered via a lateral tail veininjection. The animal was placed in right dorsolateral recumbency,the left kidney was distracted with the stay sutures, and a thinflexible plastic tray (35 3 50 3 0.5 mm) was placed under the kidneyo direct blood flow from the injury onto a small stack of preweighedauze pads. A soft vascular clamp was used to occlude renal bloodow by clamping the arteriovenous complex. A sagittal heminephrec-omy was performed and the cut surface of the remaining kidneylotted dry with gauze. The cut surface of the excised portion of theidney was blotted onto filter paper three times and circumscribed toompare the surface area of the injuries. The treatment was thenanded to the surgeon and applied to the injury in the appropriateashion. If the treatment was a liquid preparation such as fibrinealant, 2 cc of total solution (1 cc from each syringe) was applied.he agent was allowed to polymerize for 3 min before the renal clampas released, returning blood flow to the kidney. If bleeding wasbserved after clamp release, the remaining hemostatic agent (1 ccotal) was applied over the bleeding area without reclamping theidney. In the case of solid preparations such as Gelfoam the productas applied either dry or soaked in the designated thrombin solu-
ion, according to the manufacturer’s label instructions. The agentas applied to the cut renal surface, the clamp was released, andentle pressure was maintained for 3 min as the sponge slowlyoaked with blood. In the event of continued hemorrhage, repeatedntermittent pressure was applied for a few minutes at a time for therst 10 min of the observation period. The animals were monitoredor up to 60 min or until death from exsanguination occurred. Theemostatic agents were removed at the end of the 60-min observa-ion period in any surviving animals to confirm copious renal hem-rrhage in the absence of the agent.
Data Collection and Analysis
At the end of the procedure resulting blood loss was measured byreweighing the blood-soaked gauze along with the hemostatic agentand, after subtracting for the agent, recorded as grams of blood lost.Time of death was recorded in minutes and defined as when themean arterial pressure fell below 10 mm Hg with no pulse or respi-ration for 1 min. Incidence of complete hemostasis was noted whenno further measurable post-treatment blood loss from the injury sitewas observed. Blood pressures (systolic, diastolic, and mean arterial)
TAB
Hemostasis an
Group N M
Sham operation: no renal excisionW/physiologic saline iv 6W/2000 IU/kg heparin iv 6
Negative Control: renal injury with no treatmentW/physiologic saline iv 12 5W/500 IU/kg heparin iv 6 6W/1000 IU/kg heparin iv 6 8W/2000 IU/kg heparin iv 11 7
128 JOURNAL OF SURGICAL RESEARC
and heart rates were updated every half-second in computerizedformat that recorded the data each minute as an average of thereadings during that minute. The blood pressures in nonsurvivinganimals were recorded as zero for the remainder of the observation 0
period. The surface areas of the three renal imprints were measuredand averaged for each kidney to ensure consistency of the injuryamong groups.
Procedural criteria were developed to include only animals thatrepresented a consistent challenge to the hemostatic agent. Animalswere eliminated from the study if any of the following criteria ap-plied: (1) a mean arterial pressure (MAP) of less than 90 mm Hgbefore beginning surgery; (2) a MAP of less than 70 mm Hg beforethe heparin injection; (3) a MAP of less than 50 mm Hg beforereleasing the renal vascular clamp to begin the observation period;(4) a rectal temperature above 40°C for longer than 20 min; (5)copious uncontrolled bleeding from a site other than the kidney; (6)death due to some identifiable reason other than renal blood loss; (7)accidental disruption of the hemostatic agent during the test periodor other irreparable procedural error; and (8) failure to bleed pro-fusely once the agent was removed in surviving animals.
The endpoints compared for the experiment were weight of bloodshed, survival trends, maintenance of blood pressure, and incidenceof complete renal hemostasis. The mean blood loss for each groupwas analyzed for significance using a two-tailed Mann–Whitney ttest. Survival was analyzed using a log-rank trend comparison of theproportion of animals surviving at a given time. Maintenance ofmean arterial pressure was averaged within a group and analyzedusing a two-tailed, one-way ANOVA (Kruskal–Wallis) with Dunn’smultiple column comparison test over the entire 60-min observationperiod, the first 30 min, the last 30 min, and the last 10 min of theperiod. Incidence of complete hemostasis was compared using atwo-tailed Fisher’s Exact test. The renal injury surface areas werecompared using a one-way ANOVA and unpaired t test of the means.
ignificance in all tests was assigned at greater than 95% confidenceevel (P , 0.05).
RESULTS
The results of sham-operated and negative controlgroups are summarized in Table 1. The results for thetreatment groups regarding maintenance of mean ar-terial pressure, blood loss, and survival trends aresummarized in Figs. 1–3, respectively.
No statistical difference was found among the aver-age surface areas of the renal excision sites for any ofthe experimental groups (data not shown).
For the negative control groups, all three of the hep-
1
urvival Data
nal blood loss (mL)No. survived
60 min
Survival time(min)
6 SD Range Mean Range
0 6 60 600 6 60 60
6 2.1 1.0–8.2 4 48.8 30–606 2.0 3.2–8.8 1 24.8 12–606 1.3 6.5–9.8 0 19.0 5–496 0.8 6.0–8.5 0 15.4 6–34
VOL. 95, NO. 2, FEBRUARY 2001
LE
d S
Re
ean
.4
H:
arinized groups exhibited significantly lower survivaltrends compared to the saline-injected group (P ,
.01). With respect to blood loss, only the 1000 and the

rrhat
2000 IU/kg heparin groups differed significantly fromthe saline group (P , 0.01), and these two high-doseheparin groups had statistically similar blood loss andsurvival trends. All sham-operated animals were ad-ministered either saline or 2000 IU/kg heparin iv. Theysurvived the surgery with statistically similar bloodpressure trends throughout the procedure.
Complete hemostasis occurred only in the fibrinsealant-treated groups; 7 of 12 for the spray group and4 of 12 for the cannula group. Incidence of completehemostasis in the FS spray group (7 of 12) was signif-icantly higher than all the non-FS treatment groups(no complete hemostasis, P , 0.025).
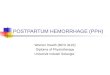
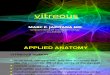
The results demonstrated significant differences inboth the survival trends and the amount of blood shedthat were manifested similarly among the varioustreatment groups. FS applied as a spray was the mosteffective treatment, with significantly less blood loss(P , 0.006) and improved survival trends (P , 0.005)compared to all the gelatin sponge groups and controlgroups. Fibrin sealant applied with a cannula wassignificantly more effective than treatment with a gel-atin sponge dry or soaked in 300 IU/mL (P , 0.002 forsurvival). Cannula application was intermediate be-
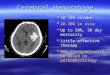
FIG. 1. Maintenance of mean arterial pressure in rat renal hemois omitted from the graph for clarity. It follows a trend similar to th
TUTHILL ET AL.: TOPICAL HEM
tween the gelatin sponge soaked in 1000 IU/mL throm-bin and the fibrin sealant spray treatment. Survivaltrends for the 1000 IU/mL thrombin-soaked gelatin
sponge were significantly prolonged compared to thetwo other gelatin sponge groups (P 5 0.045). Gelatinsponge soaked with 300 IU/mL thrombin, dry gelatinsponge, and fibrinogen alone were ineffective treat-ments in this model. In general a clear trend was seensuch that in this animal model, the most effective he-mostasis was provided by fibrin sealant applied as aspray, followed by fibrin sealant applied through acannula, followed by gelatin sponge soaked in 1000IU/mL thrombin, all of which afforded significantlymore effective hemostasis compared to the remaininggroups.
With respect to maintenance of MAP, all treatmentgroups were significantly different than the sham-operated groups for all time intervals compared. BothFS-treated groups maintained significantly higherpressures than all the other treatment groups includ-ing the GS soaked in 1000 IU/mL thrombin. Mainte-nance of MAP exhibited similar trends between the FSspray and cannula-treated groups until the last 10 minof the observation period, when a more rapid decline inthe cannula group became statistically distinct. Of noteis that the GS-treated groups, with or without thethrombin, were not statistically different from each
age model: treatment groups. Gelfoam 1 300 U/mL thrombin groupof the dry Gelfoam group.
129TATS IN RENAL HEMORRHAGE
OSother with respect to maintenance of blood pressure,although GS treatment maintained low blood pres-sures longer than no treatment.

mfi
t r
DISCUSSION
This renal hemorrhage model in the rat providedreproducible blood loss and survival trends, and proved
FIG. 2. Blood loss in ra
130 JOURNAL OF SURGICAL RESEARC
FIG. 3. Survival trends in rat renal he
to be an efficient in vivo assay for testing topical he-ostatic agents. Obvious differences in hemostatic ef-
cacy were demonstrated with group sizes of 6 to 8nimals, while more subtle differences could be de-
enal hemorrhage model.
VOL. 95, NO. 2, FEBRUARY 2001
a
H:
morrhage model: treatment groups.

OS
tected with as few as 12 animals in a group. The entiresurgical procedure takes less than 2 h. This animalmodel is appropriate for testing the relative efficacy ofboth passive and active topical hemostats, rangingfrom gelatin sponges to fibrin sealant formulations. Itis capable of detecting quantitative dose effects as wellas functional deficiencies in fibrinogen preparationsusing objective, quantified endpoints. The model maybe used to guide the development of topical hemostaticagents by distinguishing differences in compositionand formulation as well as delivery mechanisms.
The procedural inclusion criteria were developed assafeguards to ensure that all agents were subjected toa similar challenge. For example, model developmentrevealed that rats tend to clot more efficiently if mildlyhypothermic from the anesthesia, yet are prone to ab-errant deaths if overheated, so strict regulation of bodytemperature was important to the reproducibility ofthe model. Blood pressure monitoring was used to iden-tify abnormal physiologic responses to the anesthesiaor procedure. In the final analysis, 27 of 128 animals(21%) were excluded, resulting in 101 animals in thestudy. Eleven of these exclusions were based on bloodpressure criteria, 11 were due to surgical mishaps/technical errors, 2 were for overheating, and 3 wereaberrant deaths not due to bleeding (one of these was arat found to have cardiomyopathy and pulmonary hy-pertension upon necropsy with histopathology). Sincehalf of the exclusions were associated with technicaldevelopment of the model (errors, overheating) an ex-clusion rate as low as 10%, primarily due to physiologicvariability, could be achieved and expected in futurestudies. In essence, the blood pressure criteria ex-cluded the bottom 10% of the animals whose poor car-diovascular responses to the anesthetic/surgical proce-dure were likely to diminish the challenge to thehemostatic agent and thus would confound the resultswith animals that died for reasons other than bloodloss, or that may have survived due to aberrantly lowblood pressures producing a diminished hemostaticchallenge.
Both blood loss and survival trends served as suit-able endpoints for the model. Survival trends wereprobably the more objective and reliable endpoint assurvival times were easily and accurately determinedand generated very high confidence levels. Blood lossdata collection was subject to variability by loss ofunmeasured blood into the abdominal cavity, evapora-tion during the observation period, and extraneousfluid or blood from surrounding tissues. These vari-ables were controlled for to the extent possible by goodexposure and distraction of the kidney, careful place-ment of the gauze, and placement of blotted gauze into
TUTHILL ET AL.: TOPICAL HEM
plastic bags to limit evaporation. Maintenance of bloodpressure was also an appropriate and objective end-point that allowed the data to be compared over vari-
ous times during the procedure. Blood pressure trendswere the most sensitive endpoint for comparing themore effective FS treatments but did not meaningfullydistinguish the GS soaked in 1000 IU/mL thrombinfrom the other GS treatment groups in the same waythat blood loss and survival trends did. This observa-tion is probably related to intrinsic limits of the com-pensatory mechanisms to maintain pressure beyond acertain threshold of blood loss, leading to a binarytrend of BP maintenance between the more effectiveFS groups and the less effective GS groups. One wouldexpect the survival trends to become more stronglycorrelated to the blood pressure maintenance if theobservation period were extended further. Anotherendpoint considered was time to hemostasis, but thiswas very difficult to ascertain accurately when thesmall injury site was covered by a gelatin sponge or anopaque mass of fibrin. The heparin dosage titrationconfirmed the need for heparinization in rats to pro-duce consistently reproducible hemorrhage from a he-misected kidney. Placebo injections of saline resultedin one-third of the animals surviving a 1-h observationperiod, and widely scattered renal blood loss data. Hep-arin dosages in rats of between 300 and 1000 IU/kghave been used for antithrombotic effect in survivalcardiovascular and microsurgical procedures [6, 7]. Ad-ministration of 2000 IU/kg in has been found to prolongcoagulation time for more than 5 h and effectivelyprevent renal thrombosis in a rat model [8]. A dose of500 IU/kg heparin sulfate given by tail vein injection inthis model allowed one of six animals to survive thehour. Both the 1000 and 2000 IU/kg heparin doseswere effective in producing coagulopathy with 100%mortality, yet the survival times had a narrower rangeand the blood loss data were grouped more tightly inthe 2000 IU/kg dose group. Thus, to remain well be-yond the plateau of variation in heparin effect, thehighest dose of 2000 IU/kg iv was chosen to completethe study.
The investigators noted more difficulty in providinghemostasis with the cannula tip, as opposed to thespray tip, to apply fibrin sealant in this setting. Sub-jectively, a longer learning time was required for ap-plying the fibrin sealant in a uniform layer with thecannula tip. This assessment was somewhat evident inthe data. For example, in the blood loss results for thecannula tip, the four largest values above the medianwere generated in the first six rats. Also, an interimanalysis revealed a significant difference in survivaltrends between the spray and cannula tip for the firsthalf of the study; a gap that had narrowed by the endof the study to less than 95% confidence limits. Indeed,spray- and cannula-tip devices serve different surgical
131TATS IN RENAL HEMORRHAGE
needs, and this study demonstrates why a spray tipswould be generally recommended for applying FS overlarge flat surfaces. These results also suggest that sur-

H:
geons should be trained in the technical use of fibrinsealants and in the selection of the optimal applicationdevice. This should not obscure the fact that in thehands of experienced animal surgeons, the Haemedicsdevice with the appropriate applicator (spray tip) wasthe most effective topical hemostat tested.
This study demonstrated that neither thrombinsoaked into a matrix or a fibrinogen spray alone couldprovide the active hemostatic capability of the combi-nation of fibrinogen and thrombin when applied prop-erly as a fibrin sealant formulation. The experimentalso showed that fibrin sealant can provide effectivehemostasis in an animal severely anticoagulated withheparin. This has implications for its use in humans asa surgical hemostat, especially in cardiothoracic sur-gery where patients are routinely heparinized, or inany patient whose coagulation state has been compro-mised. Coagulopathies secondary to hypothermia orblood dilution are not uncommon in trauma settings [9,10], underscoring the importance of demonstrating ef-ficacy for topical hemostats in the absence of normalendogenous clot formation.
The goal of the study was to develop an efficient andreliable small-animal hemorrhage model that could ob-jectively and quantifiably assess the performance ofvarious topical hemostats, and then to test a fibrinsealant against some other existing standard of care.The results of this study confirmed that the animalmodel met the goals set forth, providing a basis forcomparing the effectiveness of topical hemostaticagents, and demonstrating that fibrin sealant deliv-
132 JOURNAL OF SURGICAL RESEARC
ered by an effective applicator is highly efficacious as atopical hemostat in heparinized animals compared to apassive matrix soaked in thrombin.
1
REFERENCES
1. Burch, J. M., Ortiz, V. B., Richardson, R. J., Martin, R. R.,Mattox, K. L., and Jordan, G. L. J. Abbreviated laparotomy andplanned reoperation for critically injured patients. Ann. Surg.215: 476, 1992.
2. Martinowitz, U., and Schulman, S. Fibrin sealant in surgery ofpatients with a hemorrhagic diathesis. Thromb. Haemost. 74:486, 1995.
3. Martinowitz, U., Schulman, S., Horoszowski, H., and Heim, M.Role of fibrin sealants in surgical procedures on patients withhemostatic disorders. Clin. Orthop. 65: 1996.
4. Jackson, M. R., Taher, M. M., Burge, J. R., Krishnamurti, C.,Reid, T. J., and Alving, B. M. Hemostatic efficacy of a fibrinsealant dressing in an animal model of kidney injury.J. Trauma. 45: 662, 1998.
5. Raccuia, J. S., Simonian, G., Dardik, M., Hallac, D., Raccuia,S. V., Stahl, R., and Dardik, H. Comparative efficacy of topicalhemostatic agents in a rat kidney model. Am. J. Surg. 163: 234,1992.
6. Koyama, H., and Reidy, M. A. Reinjury of arterial lesions in-duces intimal smooth muscle cell replication that is not con-trolled by fibroblast growth factor 2. Circ. Res. 80: 408, 1997.
7. Smith, L. J., Schaible, K. L., Fessler, R. G., Rachlin, J. R., andBrown, F. D. Examination of the utility of the rat as an animalmodel for human anticoagulation. Haemostasis 17: 206, 1987.
8. Tsuchida, A., Kanai, H., Ogawa, S., Yano, S., and Naruse, T.Effect of drug administration on experimental renal glomerularthrombosis. Res. Commun. Chem. Pathol. Pharmacol. 59: 201,1988.
9. Watts, D. D., Trask, A., Soeken, K., Perdue, P., Dols, S., andKaufmann, C. Hypothermic coagulopathy in trauma: Effect ofvarying levels of hypothermia on enzyme speed, platelet func-tion, and fibrinolytic activity. J. Trauma. 44: 846, 1998.
VOL. 95, NO. 2, FEBRUARY 2001
0. Cosgriff, N., Moore, E. E., Sauaia, A., Kenny-Moynihan, M.,Burch, J. M., and Galloway, B. Predicting life-threatening co-agulopathy in the massively transfused trauma patient: Hypo-thermia and acidoses revisited. J. Trauma. 42: 857, 1997.