Embed Size (px)
Citation preview

The Egyptian Journal of Radiology and Nuclear Medicine (2016) 47, 431–438
Egyptian Society of Radiology and Nuclear Medicine
The Egyptian Journal of Radiology andNuclearMedicine
www.elsevier.com/locate/ejrnmwww.sciencedirect.com
ORIGINAL ARTICLE
Assessment of postoperative local and distant
recurrence in colorectal cancer patients:
Comparison between PET/CT and CECT
* Corresponding author. Tel.: +20 1115666504.
E-mail addresses: [email protected] (A.M. Hussein),
[email protected] (M.A. Nassef).1 Address: 6 Abdel Azeem Awadallah Street, Heliopolis, Cairo,
Egypt. Tel.: +20 (002)1005048866, +20 (02)24150449.
Peer review under responsibility of The Egyptian Society of Radiology
and Nuclear Medicine.
http://dx.doi.org/10.1016/j.ejrnm.2016.02.0020378-603X � 2016 The Egyptian Society of Radiology and Nuclear Medicine. Production and hosting by Elsevier B.V.This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Ahmed Mohamed Hussein *, Mohamed Amin Nassef1
Radiology Department, Faculty of Medicine, Ain Shams University, Cairo, Egypt
Received 15 December 2015; accepted 5 February 2016Available online 22 February 2016
KEYWORDS
Cancer colon;
18F-FDG PET/CT;
Recurrence
Abstract Objective: To assess the diagnostic performance of 18F-FDG PET/CT scan in the detec-
tion of recurrent disease in CRC patients who have suspected local and/or distant recurrent disease
compared to contrast enhanced CT scan (CECT).
Material and method: 96 CRC treated patients with suspected recurrence were examined by CECT
and 18F-FDG PET/CT. Pathological results, clinical or imaging follow-up, or the responsiveness of
the lesion to the treatment with chemotherapy or radiation therapy were reviewed for gold stan-
dard.
Results: Recurrent or metastatic disease was found in 74 (77.1%) of 96 patients. Calculated sensi-
tivity, specificity, and accuracy of 18F-FDG PET/CT were 92%, 72.7%, and 88.5%. The specificity
of 18F-FDG PET/CT was statistically significantly better than that of CECT as it can reduce the
false positive results of CECT in 13 patients, however regarding the sensitivity.
18F-FDG PET/CT showed better value but without statistical significance.
Conclusion: 18F-FDG PET/CT is a better method to evaluate postoperative CRC patients with
suspected tumor recurrence or distant metastasis than CT with significantly higher specificity.� 2016 The Egyptian Society of Radiology andNuclearMedicine. Production and hosting by Elsevier B.V.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-
nd/4.0/).
1. Introduction
Colorectal carcinoma (CRC) is considered one of the most
common types of cancer in men and women (1). About fifthof the cancer patients present with distant metastases if leftuntreated with a five-year survival rate of less than 10% (2).
During follow-up after primary surgery approximately40% of patients develop local and distant recurrences (3).
Patient survival and quality of life might be improved by
surgery, radiotherapy and chemotherapy; thus, early detectionof recurrence is of great importance. Resection of the metas-

432 A.M. Hussein, M.A. Nassef
tases in selected patients has been reported to result in 5-yearsurvival rates exceeding 30% (4).
Metastatic disease in colorectal cancer is most common in
liver and lung, but can affect the whole body. Imaging of thewhole-body is of great importance during staging to detectlocal or distal tumor spread and as a part of surveillance pro-
gram after surgery or when a recurrence is suspected on clinicalbasis. Most accurate modality for whole-body staging is stillunclear. Currently, computed tomography (CT) is used to
detect recurrence, however having high false-negative rate forextrahepatic intra-abdominal lesions (e.g. para-aortic nodes)and a high false-positive rate for pulmonary lesions (5,6).
This disadvantage has led to the increased use of 18F-
fluorodeoxyglucose (18F-FDG)-positron emission tomogra-phy (PET)/CT as an imaging modality, in both preoperativeassessment and during follow-up. 18F-FDG PET has pre-
sented high accuracy in the detection of recurrent and meta-static CRC (7), however, being cost-effective only in thestaging of recurrent/metastatic colorectal cancers (8).
The purpose of the current study was to evaluate the diag-nostic performance of 18F-FDG PET/CT scan in the detectionof local or distal recurrence in suspected colorectal cancer
patients compared to contrast enhanced CT scan (CECT).
2. Materials and methods
This prospective study was conducted during the periodbetween February 2014 and September 2015 at a private Radi-ology centre in Cairo on 96 patients (62 males and 34 females),who were treated for colorectal cancer with suspected recur-
rence. Written and verbal consents were obtained from allpatients as well as an agreement of the local ethics committee.
2.1. FDG-PET/CT examinations
The patients were examined from base of skull to midthighusing a Philips Gemini Time of-Flight PET/CT machine
equipped with LYSO crystals (Philips, Holland). Manufac-turer’s review station (Brilliance, Philips, Holland) was usedto draw regions of interest (ROIs).
Table 1 Ninty-six patient characteristics.
Patient characteristics Value
Sex
Male 62
Female 34
Mean age (range)
Male 61.4(42–76)
Female 58.6(33–81)
Primary lesions
Colon 55
Rectum 41
Indication for 18F-FDG PET/CT scan
Assessment of resectability 41
Abnormal conventional imaging 35
Elevated serum CEA >7 ng/ml or rising
CEA level
23
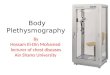
Fig. 1 Male patient with history of colon cancer and partial
colectomy; Study performed on June 2014, CECT (A) showed no
definite focal lesions, however the PET/CT (B) showed multiple
metabolically active hepatic lesions. Follow-up study done on
December 2014, CECT (C) showed small left lobe focal lesion,
while the PET/CT (D) revealed predominantly disease progression
with newly developed FDG avid lesions more pronounced on the
left lobe.

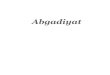
Fig. 2 Male patient with history of cancer colon operated upon with postoperative radiotherapy and chemotherapy. (A) CECT showing
sternal expansible osteolytic lesion with multiple fractures and multiple vertebral osteolytic lesions. (B) PET/CT detected metabolic
activity at the sternum, C1–C3, D1–D7, D11-L5 most active at D3 and D4. (C) CECT revealed multiple enlarged para-aortic and
mesenteric lymph nodes. (D) PET/CT showed metabolic activity in the detected lymph nodes with the mesenteric being the most active.
(E) CECT showed multiple bilateral common iliac and external iliac LNs. The largest on the right external iliac group. (F) PET/CT
detected marked metabolic activity in the iliac lymph nodes. (G) CECT showed sheet like and nodular thickening of the pelvic peritoneal
reflection. (H) PET/CT detected increased FDG uptake in the peritoneal reflections with the most active nodule seen in the midline
‘‘supra-pubic region”, from which biopsy was done and revealed its metastatic nature.
Assessment of postoperative local and distant recurrence in colorectal cancer patients 433

Table 2 Regions of recurrences or metastases.
Region Number of patients
Local 15
Liver 25
Chest 20
Bone 3
Intraabdominal extrahepatic 31
Table 3 CECT and 18F-FDG PET/CT result for recurrence
by patient-based analysis.
Study Patient based analysis (n= 96)
Positive by
golden standard
Negative by
golden standard
18F FDG PET/CT
Positive 69 6
Negative 5 16
CECT
Positive 65 19
Negative 9 3
434 A.M. Hussein, M.A. Nassef
The applied tracer was 18F-FDG. It was injected intra-venously (i.v.) with an aimed dose of 0.1–0.14 mCi/kg adjustedaccording to patient’s weight.
The patients fasted for at least 6 h before imaging and theirblood glucose level was kept below 160 mg/dl at the time oftracer injection.
Uptake time from tracer injection to onset of emission scanwas aimed at 60 ± 10% min.
A 64 integrated multi-slice CT machine was used to per-
form the standard diagnostic contrast-enhanced examinationscovering the thorax, abdomen, and pelvis. Iodinated contrastagent (Omnipaque 350) was given orally: 20 mL in 500 mLbottled water (4% solution), 30 min before scan start, and
i.v.: 100 mL with an injection flow of 5 mL/s immediatelybefore scan start.
Imaging parameters: 120 kVp, 300 mAs, 512 � 512 matrix
size, acquiring field of view (FOV) of 500 mm using dose auto-mated modulation in the Z direction.
2.2. Diagnostic criteria
The diagnosis of recurrent disease was made by pathologicallyproven malignancy, the progression of clinical or imaging
follow-up, or the responsiveness of the lesion to the treatmentwith chemotherapy or radiation therapy.
The diagnosis of non-recurrent disease was made by thepathologically proven benign lesion, no interval change of
the lesion without treatment on follow-up imaging or noabnormal finding on follow-up imaging for more one year atleast after 18F-FDG PET/CT scans.
2.3. Data interpretation
The fused PET/CT and Ce-CT images were separately inter-
preted by a team of one nuclear medicine physician and oneradiologist with knowledge of aim of the study.
2.4. Statistical analysis
Sensitivity, specificity and accuracy of 18F-FDG PET/CTscan, compared to the gold standard (pathophysiology, clinicalor imaging follow-up for at least one year) and contrast
enhanced CT scan (CECT) were calculated and analyzed onpatient bases and lesion bases.
Statistical significance between the two imaging modalities
was calculated by McNemar, in which p-value of less than0.05 was considered statistically significant.
3. Results
Patient characteristics and demographic data are shown inTable 1.
Recurrent disease was found in 74 patients (77.1%), ofwhich 46 patients were pathologically proven and 28 patientsdemonstrated progression of disease or response to treatment
on follow-up imaging (Figs. 1 and 2).Ninety-four regions in 74 patients with recurrent disease are
shown in Table 2.We found that 18F-FDG PET/CT scan could reduce false
positive result of CECT in thirteen patients (local, chest, liver
and peritoneal lesions); therefore, the specificity of 18F-FDG
PET/CT scan was better than CECT (p= 0.012). However,there was no significant difference between the sensitivityand the accuracy of these two modalities (p= 0.696 and0.263) (Table 3).
18F-FDG PET/CT was falsely negative in 6 patients(Fig. 3).
Regarding the 23 patients with elevated CEA 18F-FDG
PET/CT detected recurrence/metastases in 21 patients(91.3%) (Fig. 4), however one patient was missed by CECT.
There were 178 lesions detected by CECT or 18F-FDG
PET/CT, 128 of which showed recurrence. 18F-FDG PET/CT scan can reduce false positive of CECT for 16 lesions (5local recurrences, 4 intraabdominal lymph nodes, 3 peritoneal
nodules, 2 pulmonary nodules and 2 liver lesions) (Table 4).However, 18F-FDG PET/CT scan also gives false positive
for nineteen lesions (Fig. 5) (5 local recurrences, 5 mediastinallymph nodes, 5 peritoneal nodules, and 4 liver lesions).
18F-FDG PET/CT scan provided the better sensitivityspecificity, and accuracy than that of CECT but did not reachthe statistical significance (Table 5).
4. Discussion
Computed tomography (CT), has an important role in the
detection of early recurrence in patients with CRC, howeverdepending on size criteria in the diagnosis of malignancy limitsits reliability. Though the larger the mass the more likely to be
malignant, yet some benign masses composed by fibrous tissuetend to reach large sizes.
Inability to differentiate viable from nonviable tumor lesion
is another drawback. 18F-FDG PET/CT has an importantrole in the detection of local and distant recurrence and inthe differentiation of malignant and non-malignant masses,by cellular glucose metabolism detection (9).

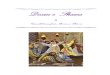
Fig. 3 70 years old male patient with history of colorectal cancer, underwent surgical excision. Known to have polycythaemia rubra
vera. Study done on January 2015; (A) CECT showed a tiny left upper lobe subpleural nodule. (B) PET/CT detected no metabolic activity
in the nodule. (C) CECT showed small peritoneal nodule lateral to the enlarged spleen. (D) PET/CT no metabolic activity in the nodule.
Follow-up study done on June 2015. (E) CECT showed increased size of the nodule. (F) PET/CT detected increased metabolic activity in
the nodule which was not detected in the previous study. (G) CECT showed increased size of the peritoneal nodule. (H) PET/CT detected
increased metabolic activity in the nodule. Thus the PET/CT missed the pulmonary and peritoneal nodules in the previous study.
Assessment of postoperative local and distant recurrence in colorectal cancer patients 435
In the present study recurrent disease was found in 77.1%
of the patients, while in the previous study by Chiewvit et al.(9) 75% of the patients had disease recurrence.
In our study we found that 18F-FDG PET/CT scan couldreduce false positive results of CECT in thirteen patients;
therefore, the specificity of 18F-FDG PET/CT scan was betterthan CECT (p= 0.012). However, there was no significant
difference between the sensitivity and the accuracy of these
two modalities (p= 0.696 and 0.263).Maas et al. (10) in their meta-analysis found that PET/CT
has a high diagnostic performance with an area area undercurve (AUC) of 0.94. CT had a significantly lower diagnostic
performance than PET/CT with an AUC of 0.83. PET/CTwas the most accurate modality utilizing metabolic imaging

Fig. 4 72 years old female patient with history of cancer colon,
underwent partial colectomy and chemotherapeutic treatment,
and the patient reported previous hysterectomy. (A) CECT
showed bulky non-homogenous uterine cervix stump seen pro-
truding into the fluid filled distended vagina. (B) PET/CT detected
increased metabolic activity at the stump as well as the lower anal
canal with no CT correlate. Biopsy was done and revealed local
recurrence.
Table 4 CECT and 18F-FDG PET/CT result for recurrence
by lesion-based analysis.
Study Lesion based analysis (n = 178)
Positive by
golden standard
Negative by
golden standard
18F FDG PET/CT
Positive 113 19
Negative 15 31
CECT
Positive 99 35
Negative 29 15
Fig. 5 A 54-year-old female patient with history of cancer
rectum underwent surgical excision. (A) CECT showed mural
thickening with few diverticular outpouching along the recto-colic
anastomosis with associated pre-sacral and left para rectal soft
tissue sheet and edema. (B) PET/CT detected increased FDG
uptake is seen along recto-colic anastomosis, pre-sacral and left
para rectal soft tissue. Biopsy was performed and revealed
postoperative changes with no malignancy.
436 A.M. Hussein, M.A. Nassef

Table 5 Diagnostic performance of CECT compared with
18F-FDG PET/CT by patient based analysis and lesion based
analysis.
Sensitivity Specificity Accuracy
Study by patient based analysis
18F FDG PET/CT 92% 72.7% 88.5%
CECT 87.8% 13.6% 70.8%
p-value 0.696 0.012 0.263
Study by lesion based analysis
18F FDG PET/CT 88.3% 67.4% 64.1%
CECT 77.3% 30% 80.9%
p-value 0.188 0.085 0.998
Assessment of postoperative local and distant recurrence in colorectal cancer patients 437
techniques that provide information on the nature of a lesionbased on differences in glucose metabolism. The metabolicchanges precede the morphological changes (examined by
CT), giving the higher sensitivity for PET/CT for detectionof small malignant lesions.
Meta-analysis data of 11 articles by Huebner et al. (11)
found overall sensitivity of 97% and an overall specificity of76% for 18F-FDG PET in the detecting recurrent CRCthroughout the whole body altering the patient managementin about 30% of cases.
In the study by Lee et al. (12) on postoperative patientswith suspected recurrence, 107 suspicious recurrent lesionswere detected in the 63 cases examined by 18F-FDG PET/
CT. The result showed that the overall sensitivity, specificityand accuracy were 94.7%, 86.4%, and 92.4% for PET/CT,and 98.2%, 4.5 and 72.2% for conventional imaging.
CT had a lower diagnostic performance than PET/CT. Thecause may be that the accuracy of CT for extrahepatic metas-tasis detection is lower than that of PET/CT. CT is known to
be more accurate in the detection of hepatic being less sensitivefor extrahepatic metastases, making it less ideal for whole-body staging. Studies have shown that with respect to thedetection of extrahepatic lesions CT performs worse with sen-
sitivities ranging between 50%–70% and specificities rangingbetween 50%–80% compared to PET/CT having sensitivitiesranging between 70%–100% and specificities ranging between
40%–100% (13).In a study by Stuckle et al. (14) with multislice CT acknowl-
edged the low sensitivity (38–82%) for local recurrence
detection.In our current study 18F-FDG PET/CT detected recur-
rence/metastases in 21 patients (91.3%) of the 23 patients withelevated CEA while one patient was missed by CECT.
The previous study by Metser et al. (15) included 158patients who had a history of CRC, elevated or increasingCEA levels. The sensitivities of PET/CT and CT for patient
base were 97.3% and 70.3% (p = 0.002) and that the specifici-ties for patient base were 94.4% and 94.4% (p = 1.0). Thetumor site-based analysis showed the sensitivities of PET/CT
andMDCT were 98.1% and 66.7% (p < 0.0001) and the speci-ficities were 75% and 62.5% (p = 0.56). The specificity in Met-ser U study by PET/CT and CT was higher than our study.
The study by Mittal et al. (16) analyzed histopathologicallyproven patients with CRC.
After treatment in relation to CEA, PET/CT was 100%positive in cases that had CEA level of more than 50 ng/ml.
In the study by Chen et al. (17) in 56 recurrence and/ormetastasis CRC patients, PET/CT had a sensitivity of94.6%, and a specificity of 83.3% for recurrence/metastases,
detecting one or more occult malignant lesions in eight caseswhere abdominal/pelvic CT showed negative findings. Fur-thermore, it detected more lesions than CT did about 30%
of cases. Recurrence and/or metastasis were detected in about90% of cases with elevated serum CEA levels by 18F-FDGPET/CT imaging.
In the study by Choi et al. (18) 269 CRC patients were oper-ated for colorectal cancer, and PET/CT detected more lesionsthan conventional imaging in local recurrence and peritonealcarcinomatosis, however detecting the same number of lesions
in abdominal lymph nodes and hepatic metastases.
5. Conclusion
PET-CT has significant role in the assessment of patients withCRC, detecting previously unrecognized sites of metastaticdisease.
This study demonstrates that, when undertaken in selectedcolorectal cancer patients, 18F-FDG-PET/CT imaging pro-vides useful information and has a considerable impact on dis-
ease management in a significant proportion of patientsavoiding unnecessary surgeries, enabling the identification ofrecurrent disease as early as possible enabling curative surgery
for the patient.18F-FDG PET/CT is a better method to evaluate postoper-
ative CRC patients with suspected tumor recurrence or distantmetastasis than CT with significantly higher specificity.
Conflict of interest
The authors declare that there are no conflict of interest.
References
(1) Huguier M, Houry S, Barrier A. Local recurrence of cancer of the
rectum. Am J Surg 2001;182:437–9.
(2) Cancer Research UK. Cancer incidence statistics. <www.can-
cerresearchuk.org/cancer-info/cancerstats/incidence/ukcancer-
incidence-statistics> [accessed December 2012].
(3) Chen LB, Tong JL, Song HZ, Zhu H, Wang YC. (18)F-DG PET/
CT in detection of recurrence and metastasis of colorectal cancer.
World J Gastroenterol 2007;13:5025–9. http://dx.doi.org/10.3748/
wjg.v13.i37.5025.
(4) Elias D, Sideris L, Pocard M, Ouellet JF, Boige V, Lasser P, et al.
Results of R0 resection for colorectal liver metastases associated
with extrahepatic disease. Ann Surg Oncol 2004;11:274–80. http://
dx.doi.org/10.1245/ASO.2004.03.085.
(5) Pfannschmidt J, Bischoff M, Muley T, Kunz J, Zamecnik P,
Schnabel PA, et al. Diagnosis of pulmonary metastases with
helical CT: the effect of imaging techniques. Thorac Cardiovasc
Surg 2008;56:471–5.
(6) Wiering B, Ruers TJ, Krabbe PF, Dekker HM, Oyen WJ.
Comparison of multiphase CT, FDG-PET and intra-operative
ultrasound in patients with colorectal liver metastases selected for
surgery. Ann Surg Oncol 2007;14:818–26.
(7) Scott AM. Current status of positron emission tomography in
oncology. Intern Med J 2001;31:27–36.
(8) Brush J, Boyd K, Chappell F, Crawford F, Dozier M, Fenwick E,
et al. The value of FDG positron emission tomography/comput-
erised tomography (PET/CT) in pre-operative staging of colorec-

438 A.M. Hussein, M.A. Nassef
tal cancer: a systematic review and economic evaluation. Health
Technol Assess 2011;15:1–192. http://dx.doi.org/10.3310/
hta15350.
(9) Chiewvit S, Jiranantanakorn T, Apisarnthanarak P, Kan-
chaanapiboon P, Hannanthawiwat C, Ubolnuch K, et al. Detec-
tion of recurrent colorectal cancer by 18F-FDG PET/CT
comparison with contrast enhanced CT scan. J Med Assoc Thai
2013;96(6):703–8.
(10) Maas M, Rutten IJ, Nelemans PJ, Lambregts DM, Cappendijk
VC, Beets GL, et al. What is the most accurate whole-body
imaging modality for assessment of local and distant recurrent
disease in colorectal cancer? A meta-analysis imaging for recur-
rent colorectal cancer. Eur J Nucl Med Mol Imaging
2011;38:1560–71.
(11) Huebner RH, Park KC, Shepherd JE, Schwimmer J, Czernin J,
Phelps ME, et al. A meta-analysis of the literature for whole-body
FDG PET detection of recurrent colorectal cancer. J Nucl Med
2000;41:1177–89.
(12) Lee JH, Park SG, Jee KN, Park DG, Namgung H, Song IH.
Performance of FDG PET/CT in postoperative colorectal cancer
patients with a suspected recurrence and a normal CEA level.
Nucl Med Commun 2010;31:576–82.
(13) Nakamoto Y, Sakamoto S, Okada T, Senda M, Higashi T, Saga
T, et al. Clinical value of manual fusion of PET and CT images in
patients with suspected recurrent colorectal cancer. AJR Am J
Roentgenol 2007;188:257–67.
(14) Stuckle CA, Haegele KF, Jendreck M, Kickuth R, Schneider O,
Hohlbach G, et al. Improvements in detection of rectal cancer
recurrence by multiplanar reconstruction. Radiologe 2005;45:
930–4, 936.71.
(15) Metser U, You J, McSweeney S, Freeman M, Hendler A.
Assessment of tumor recurrence in patients with colorectal cancer
and elevated carcinoembryonic antigen level: FDG PET/CT
versus contrast-enhanced 64-MDCT of the chest and abdomen.
AJR Am J Roentgenol 2010;194:766–71.
(16) Mittal BR, Senthil R, Kashyap R, Bhattacharya A, Singh B,
Kapoor R, et al. 18F-FDG PET-CT in evaluation of postoper-
ative colorectal cancer patients with rising CEA level. Nucl Med
Commun 2011;32:789–93.
(17) Chen LB, Tong JL, Song HZ, Zhu H, Wang YC. (18)F-DG PET/
CT in detection of recurrence and metastasis of colorectal cancer.
World J Gastroenterol 2007;13:5025–9.
(18) Choi EK, Yoo LR, Han EJ, Oo JH, Kim SH, Chung SK. Value
of surveillance F-18 FDG PET/CT in colorectal cancer: compar-
ison with conventional imaging studies. J Nucl Med 2010;51(2
Suppl):1208 [abstract].