Embed Size (px)
Citation preview

206 Abstracts / Cardiovascular Revasculariza
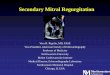
Fig. 1. (A) One day specimen with EC attaching to the stent strut (arrows) atthe interface between the endothelium and the lateral strut surface. (B) Two-day specimen with EC mounting the lateral strut surface. (C) Four-dayspecimen with EC covering a portion of the strut. (D) Ten-day specimen withstrut coverage except where the strut spans a side branch orifice.
doi:10.1016/j.carrev.2009.04.039
Percutaneous Valve Intervention
Cerebral microemboli during percutaneous mitral valvotomy forrheumatic mitral stenosisDeepak Natarajan, Vivek Prakash, Sachin Upadhyaya, Anoop KohliIndraprastha Apollo Hospital, New Delhi, India
Background: Cerebral microemboli detected by transcranial Doppler(TCD) occur systematically during cardiac angiography and surgery buttheir clinical significance are yet to be determined during percutaneousballoon mitral valvotomy for rheumatic mitral stenosis.Methods: We attempted percutaneous transvenous mitral commissurotomy(PTMC) in seven (18–60 years) patients with severe rheumatic mitralstenosis (five were females). An Inoue balloon catheter was employed (sizes24–28 mm) in all cases. There was decrease in mean end diastolic mitralgradient (from 20.2±3 mm Hg to 2+/2 mm Hg) and increase in calculatedmitral valve area from (0.7 +/− 0.6 to 1.9± 0.2 cm2).One patient was in atrialfibrillation and no patient had severe mitral valve calcification. During andimmediately after the procedure, all patients were monitored for cranialmicroemboli by a 2-MHz transcranial Doppler TCD probe, which was usedto interrogate the right middle cerebral artery.Results: Immediately after Inoue balloon inflation, single to multiplemicroemboli were detected in 5 patients. The interventions were uncompli-cated and no patient developed cognitive alteration following the procedure.Conclusion: The cranial microemboli observed during PTMC must havedislodged from the stenosed mitral leaflets during the process ofcommissurotomy by the Inoue balloon. The exact mechanism of PTMC isthe splitting of the fused mitral leraflet commissures by inflation of the Inoueballoon across the mitral valve. These microemboli must have been solid.Microemboli have, not uncommonly, also been observed during percutaneoustransluminal coronary angioplasty. These are considered gaseous and do notresult in any neurological sequelae. All seven patients were discharged thenext day in stable condition and did not experience any neurological sequelae.Further studies are necessary to determine the ramifications of silent braininjury if any following percutaneous balloon valvotomy for mitral stenosis.
doi:10.1016/j.carrev.2009.04.040
Probability of improvement in severe left ventricular systolicdysfunction following balloon aortic valvuloplasty for aortic stenosisChristopher W Pedersen, Robert S Schwartz, Michael Anderson,Michael R Mooney, Anil K Poulose, Sara Olson, Charlene R Boisjolie,Irvin F Goldenberg, Timothy D Henry, Wes R PedersenMinneapolis Heart Institute Foundation at Abbott Northwestern Hospital,Minneapolis, MN
Background: Patients with severe aortic stenosis (AS) and severe leftventricular dysfunction have a poor prognosis and are often refused surgicalaortic valve replacement. Outcomes following balloon aortic valvuloplasty(BAV) in this subgroup of patients have not been well characterized.Methods: Between June 03 and February 08, a total of 210 BAV procedureswere performed at our institution, 19 of which had baseline left ventricularejection fractions (LVEF) of ≤25%. These 19 patients were divided into twogroups based on success of BAV. Group 1 included 12 patients (63%) whounderwent successful BAV defined by increase in aortic valve area (AVA)≥35% on predischarge echo. Group 2 included the remaining 7 unsuccessfulBAV patients. Pre- and postoperative echocardiographic LVEFs weredetermined by averaging estimates of two independent and blinded reviewers.Results: Combined procedural mortality was 0%. Medications, pre and postBAV, were not significantly different between groups. Improvement inLVEF was more likely following successful BAV, with 5 (42%) of 12patients demonstrating postoperative LVEFs ≥30%, and (25%) 3 of 12,≥40%. Only 1 (14%) of 7 patients following unsuccessful BAVdemonstrated a LVEF ≥30%, none of which were ≥40%.Conclusion: BAV in nonsurgical AS patients with LVEFs ≤25% can beperformed safely. Successful BAV in this small series resulted in a strongtrend toward greater improvement in LVEF but no significant improvementin 6-month survival.
tion Medicine 10 (2009) 195–212
Variable
Group 1,successfulBAV (n=12)(mean±SD)
Group 2,unsuccessfulBA (n=8)(mean±SD)
PAge (years)
85.1±6.8 83.7±3.9 .63 Coronary artery disease,n (%)
8 (66.7) 3 (42.9) .38STS score
14±6.0 20±5.1 .29 ΔAVA (cm2) 0.39±0.17 0.06±0.10 .002 Pre-BAV % LVEF 19.8±4.7 19.6±4.2 .95 Post-BAV % LVEF 30.8±12.3 23.9±1.8 .20 Δ% LVEF 11.3±12.0 4.6±7.8 .21 6-month mortality, n (%) 3 (25) 3 (42.9) .62STS, Society of Thoracic Surgeons.
doi:10.1016/j.carrev.2009.04.041
Assessment of paravalvular prosthetic mitral regurgitation with multi-modality imaging: procedural, inhospital, and follow-up resultsAkshay Mishra, Richard Slaughter, Christian Hamilton-Craig, Tau Boga,Greg Scalia, Darryl Burstow, Darren WaltersPrince Charles Hospital, Brisbane, Australia
Background: Paravalvular mitral regurgitation is a complication of mitralvalve replacement surgery. These patients often develop haemolytic anaemiarequiring transfusions. Treatment of these is usually with a repeat surgicalprocedure; however, percutaneous device closure may be offered in caseswith high surgical risk.Methods: We retrospectively reviewed our institutional data on percuta-neous mitral paravalvular leak closures over the last 2 years. Procedural,inhospital, and follow-up results were analysed.Results: A total of six percutaneous paravalvular leak closures wereperformed. The primary interventionalist was the same in all cases (DW). The

207Abstracts / Cardiovascular Revascularization Medicine 10 (2009) 195–212
mean age was 68.7 years. The mean duration of the procedure after the initialsurgery was 8.3 years (range, 8months to 19 years). Haemolytic anaemiawasa feature in all cases. Percutaneous intervention was the chosen modality dueto high surgical risk in three patients, complications during previous surgeryin two, and patient preference in one. The patients were evaluated withtransthoracic and transesophageal echocardiography (TEE) in all cases. Livethree-dimensional TEE was an additional modality used in five cases.Patients had preprocedure cardiac magnetic resonance imaging (MRI) scansin four cases. There was good correlation with the TEE and MRI findings,and both were useful in assessing the paravalvular geometry and suitabilityfor percutaneous closure. There were no deaths or MACE during theprocedure. Implantation of the devicewas technically successful in five out ofsix patients. One patient had entrapment of the mitral valve replacementlateral disc with the occluder device, which was retrieved percutaneously andpatient referred for surgery. One patient had significant residual (thoughimproved) leak post procedure andwas operated on 3weeks later. All patientswithout MACE at a mean follow-up of 7 months (range, 1–16 months).Conclusions: Transcatheter percutaneous paravalvular leak closure is atechnically demanding but feasible procedure. Cardiac imaging using TEE,3D TEE and MRI allows for accurate evaluation of paravalvular geometryand aid intraprocedural guidance to achieve the best possible results.
doi:10.1016/j.carrev.2009.04.042
Population characteristics, treatment assignment, and clinical outcomeof patients with severe aortic stenosis who were not eligible toparticipate in a clinical trial evaluation percutaneous aorticvalve replacementItsik Ben-Dor, Augusto D Pichard, Lowell F Satler, Petros Okubagzi,Rebecca Torguson, Zhenyi Xue, Asmir I Syed, Sara D Collins,Kimberly Kaneshige, William O Suddath, Kenneth M Kent, Ron WaksmanWashington Hospital Center, Washington, DC
Background: Percutaneous aortic valve replacement (PAVR) is currentlyevaluated in clinical trial for patients with severe aortic stenosis (AS), whoare considered high-risk surgical candidates. However, many patients are noteligible to participate in the trial. The aim of the present study was study thedemographics and the outcome of the patients that could not enter the trial.Methods: The study cohort was consisted of 231 patients with severe ASwho were referred to participate in the clinical trial of PAVR. All patientswere evaluated based on the protocol inclusion/exclusion criteria, and thegroup deferred from the study was continued to be followed clinically.
TableCharacteristics and outcomes of the study population
Medicallytreated(n=61)
Balloonvalvuloplasty(n= 75)
Surgicalaortic valvereplacement(n=35) P
Age (years) 82.3±8.6 81.0±9.7 81.3±9.2 .41Thoracic surgeons
score (%)11.2±5.6 12.1±5.9 7.6±5.2 b.001
Logistic EuroSCORE(%)
36.7±23.1 45.0±21.5 19.9±12.3 b.001
Ejection fraction (%) 50.1±16.6 47.6±18.4 59.0±11.9 b.001Aortic valve area (cm2) 0.80±0.21 0.69±0.12 0.71±0.19 .001Mean gradient (mmHg) 37.5±14.7 40.9±12.3 48.8±20.8 .008Mean duration of
follow-up (days)185±182 211±192 249±169 .17
Mean time fromscreening tomortality (days)
93.8±101.6 122.7±155.1 27.6±27.9 .04
Mortality (%) 26.2 41.3 17.1 .003
Results: Of the 231 patients referred for PAVR, 171 (74.0%) were rejected.The major reasons for rejection were peripheral vascular disease 25.1%,Society of Thoracic Surgeons b10%–21.6%, AVA N0.8 cm2 11.7%, andcoronary artery disease 11.1%. This cohort was divided in three: (1)medically treated 35.7%, (2) balloon aortic valvuloplasty (BAV) 43.8%, and(3) surgery 20.5%. There was no difference between groups in the mean age.The STS and EuroSCORE were significantly lower in the surgical group.The mean aortic valve area was higher and the mean gradients were lower inthe medically treated group. The ejection fraction was lower in the BAVgroup. Death was lower in surgical group (Table).Conclusion: Most of the patients refereed for PAVR are not eligible for theprocedure mainly due to concomitant peripheral artery disease or failing oneor more of the inclusion criteria for the protocol. The mortality among thisgroup is very high with currently available options for treatment.
doi:10.1016/j.carrev.2009.04.043
Severity of aortic stenosis, not STS score, predicts procedural mortalityin elderly patients undergoing balloon aortic valvuloplastyMichael Anderson, Robert S Schwartz, Christopher Pedersen,Anil K Poulose, Michael R Mooney, Charlene R Boisjolie, Peg Demmer,Timothy D Henry, Wes R PedersenMinneapolis Heart Institute Foundation at Abbott Northwestern Hospital,Minneapolis, MN
Background: Balloon Aortic Valvuloplasty (BAV) for aortic stenosis isrequired as an essential step in the delivery of percutaneous aortic valvesand, on occasion, is used as stand alone therapy. BAV is not withoutprocedural mortality and requires a better understanding to minimize the riskas these procedures increase in frequency.Methods: Between June 2003 and July 2008, 210 BAVs were performedresulting in 7 (3.3%) procedural mortalities (PMs). Medical records,operative reports, and when available, autopsy findings were reviewed todetermine cause of death. Patient and procedural characteristics wereanalyzed for comparison between PM and non-PM patient groups.Results: PM was determined to be aortic root tear in four patients, electricalmechanical dissociation in one, pulmonary hemorrhage in one, andirreversible hemodynamic collapse of undetermined etiology in the finalpatient. Abrupt release in residual indentation of the inflated balloon contourat the annulus with progressive inflation beyond moderate resistance wasdocumented on final inflation in three of four aortic root tear patientsfollowed by abrupt hemodynamic collapse.Conclusion: The most common cause of PM following BAV was aortic rootdissection. Predictors of PM included measures of AS severity, not Societyof Thoracic Surgeons score, left ventricular outflow tract, or balloondiameter. Overly aggressive balloon inflations beyond moderate manualresistance to fully expand residual balloon indentation at the annulus shouldbe avoided, especially in patients with extremely stenotic valves.
Variable
PM group(n=7)(mean±SD)
Non-PM group(n=203)(mean±SD)
PAge (years), mean (SD)
88.3±3.1 86.8±6.4 .55 STS score 11.1±4.6% 12.6±5.7% .36 Pre-BAV LVEF (%) 53.6±13.7 49.0±16.6 .58 Pre-BAV mean gradient(mmHg)
64.3±20.3 40±18.8 .051Pre-BAVAVA (cm2)
0.4±0.11 0.6±0.4 .009 LVOT diameter (mm) 19.8±1.9 20.0±1.6 .45 Max balloon diameter (mm) 23.3±0.5 23.0±1.5 .14 No. of inflations 4.0±2.7 3.8±2.2 .90doi:10.1016/j.carrev.2009.04.044