Embed Size (px)
Citation preview

Artificial Intelligence in Medicine (2008) 43, 75—85
http://www.intl.elsevierhealth.com/journals/aiim
Assessment of classification improvement inpatients with Alzheimer’s disease based onmagnetoencephalogram blind source separation
Javier Escudero a,*, Roberto Hornero a, Jesus Poza a, Daniel Abasolo a,Alberto Fernandez b
aGrupo de Ingenierıa Biomedica, E.T.S. Ingenieros de Telecomunicacion, University of Valladolid,47011 Valladolid, SpainbCentro de Magnetoencefalografıa Dr. Perez-Modrego, Complutense University of Madrid,28040 Madrid, Spain
Received 14 February 2007; received in revised form 31 December 2007; accepted 20 January 2008
KEYWORDSAlzheimer’s disease;Algorithm formultiple unknownsignals extraction(AMUSE);Blind sourceseparation(BSS);Magnetoencepha-logram (MEG);Median frequency;Spectral entropy
Summary
Objectives: In this pilot study, we intended to assess whether a procedure based onblind source separation (BSS) and subsequent partial reconstruction of magnetoen-cephalogram (MEG) recordings might enhance the differences between MEGs fromAlzheimer’s disease (AD) patients and elderly control subjects.Materials and methods: We analysed MEG background activity recordings acquiredwith a 148-channel whole-head magnetometer from 21 AD patients and 21 controlsubjects. Artefact-free epochs of 20 s were blindly decomposed using the algorithmfor multiple unknown signals extraction (AMUSE), which arranges the extractedcomponents by decreasing linear predictability. Thus, the components of diverseepochs and subjects could be easily compared. Every component was characterisedwith its median frequency and spectral entropy (denoted by fmedian and SpecEn,respectively). The differences between subject groups in these variables werestatistically evaluated to find out which components could improve the subjectclassification. Then, these significant components were used to partially reconstructthe MEG recordings.Results: The statistical analysis showed that the AMUSE components which providedthe largest differences between demented patients and control subjects were orderedtogether. Considering this analysis, we defined two subsets, denoted by BSS-{15,35} andBSS-{20,30}, which included 21 components (15—35) and 11 components (20—30),respectively. We partially reconstructed the MEGs with these subsets. Then, the
* Corresponding author. Present address: E.T.S. Ingenieros de Telecomunicacion, University of Valladolid, Campus Miguel Delibes,Camino del Cementerio s/n, 47011 Valladolid, Spain. Tel.: +34 983 423000x5589; fax: +34 983 423667.
E-mail addresses: [email protected], [email protected] (J. Escudero).
0933-3657/$ — see front matter # 2008 Elsevier B.V. All rights reserved.doi:10.1016/j.artmed.2008.01.001

76 J. Escudero et al.
classification performance was computed with a leave-one-out cross-validation pro-cedure for the case where no BSS was applied and for the partial reconstructions BSS-{15,35} and BSS-{20,30}. The BSS and component selection procedure improved theclassification accuracy from 69.05% to 83.33% using fmedian with BSS-{15,35} and from61.91% to 73.81% using SpecEn with BSS-{20,30}.Conclusion: These preliminary results lead us to think that the proposed procedurebased on BSS and selection of significant components may improve the classification ofAD patients using straightforward features from MEG recordings.# 2008 Elsevier B.V. All rights reserved.
1. Introduction
Life expectancy has risen considerably during thelast decades. In this new situation, increasing num-bers of people reach ages at which mental diseasesbecome widespread [1,2]. Among these, Alzhei-mer’s disease (AD) is considered the most frequentcause of dementia in western countries [1,3]. More-over, the prevalence of AD increases rapidly withage [1].
AD causes progressive and irreversible impair-ment of mental functions [3]. Eventually, ADpatients need complete care. This dementia is char-acterised by neural loss. Moreover, neuritic plaquesand neurofibrillary tangles also appear [1]. Whereasthe former are microscopic extra-cellular deposi-tions composed of insoluble amyloid beta-protein,the latter are intra-cellular twisted fibres producedby protein tau [1]. The only definitive method for ADdiagnosis is direct pathological examination of braintissue [2]. Nevertheless, a probable diagnosis basedon neuroimaging techniques, medical history stu-dies and several mental tests — e.g., Mini-MentalState Examination (MMSE) [4] — is attempted.
Due to its relevance and difficult diagnosis, theutility of the electromagnetic brain activity in thedetection of AD has been widely researched in thelast decades (for recent reviews, we refer to Refs.[5,6]). Both electroencephalogram (EEG) and mag-netoencephalogram (MEG) record the electromag-netic oscillations produced by the pyramidalneurons non-invasively [7]. In AD, these signals showabnormalities that reflect anatomical and func-tional deficits of the brain cortex damaged by thedementia. Thus, the investigation of EEG and MEGsignals may provide useful insights into AD [5,6].
EEG and MEG have higher temporal resolutionthan other brain imaging techniques, like positronemission tomography or functional magnetic reso-nance imaging (fMRI) [7—9]. However, there areseveral differences between EEG and MEG. Firstly,MEG is blind to radial currents and most sensitive totangential dipoles. On the contrary, EEG records allprimary currents [8,9]. Secondly, since EEG record-ings measure the difference between the electric
potential at two locations, they require to define anelectrical reference electrode [7]. The selection ofthis electrode is a crucial matter [10]. In contrast,MEG does not need to define a reference sensor torecord the brain magnetic field [8]. Finally, MEG isnot affected by the conductivity of the skull andscalp, while EEG is distorted by these tissues [8,9].Due to these characteristics, MEG is considered acomplementary signal to EEG [8] that may provide auseful insight into the electromagnetic brain activ-ity [6].
Visual inspection of the electromagnetic brainrecordings from AD patients at rest with eyes closedshows a reduction in beta and alpha activity and aslowing of the cortical posterior rhythm, amongother abnormalities [5]. Moreover, diverse researchworks confirmed this slowing applying computerisedspectral analysis to EEG and MEG data. For instance,several studies quantified the changes that AD pro-duces in the power of different frequency bands[5,11—13]. These findings agree with the fact thatAD patients’ EEG and MEG recordings have a lowermean frequency than those of healthy control sub-jects [11,13—16]. AD also causes other abnormal-ities in the electromagnetic brain activity, such as adecrease in the functional connectivity among cor-tical areas. This reduction can be measured per-forming a coherence analysis of brain recordings[5,10,12].
In addition to the aforementioned changes, theirregularity of the AD patients’ EEG and MEG spectraalso decreases [16,17]. This reduction can be eval-uated using spectral entropy [18,19], which is com-puted applying the Shannon entropy to thenormalised power spectral density (PSD) function.Moreover, the AD patients’ EEG and MEG data havealso been studiedwith various non-linear techniques[5,6,17,20] like complexity estimators [21—23] orconnectivity measures [24,25]. Other works havefocused on the internal equivalent generator dipolesof MEG activity in AD [26].
Nevertheless, there is room for further improve-ment in those methodologies [27]. A technique thatmay improve the subject classification based onfeatures extracted from EEG and MEG data is blind

Assessment of classification improvement in patients with Alzheimer’s disease based on MEG BSS 77
source separation (BSS) [28,29], since this metho-dology allows us to examine these signals fromanother point of view [27,30].
Typically, BSS techniques are applied to a set oftemporally and spatially correlated measurements,like EEGs and MEGs, although they can also be usedwith single channel recordings [31]. From the cor-related recordings, the BSS methods estimate anumber of underlying components, or sources,blindly (i.e., the components themselves and themixing process that produced the observed mea-surements from the components are unknown)[28,29,32]. To estimate the underlying components,it is assumed that they are mutually independent or,alternatively, that their waveforms have no spatialand temporal correlations [29].
It should be noted that the BSS components areneither equivalent current dipoles nor fMRI acti-vated zones. Instead, they are concurrent, spatiallyand temporally decorrelated electromagnetic activ-ities which were added over the scalp to originatethe measured recordings [28,33].
Given the fact that BSS is able to isolate dissimilarkinds of activity into different components [29,32],this technique has been used to reject artefactsfrom EEG [33—36] and MEG [37,38] data. OnceBSS has isolated the artefacts into a few compo-nents, the brain recording is reconstructed usingonly the non-artefactual components [29,36]. In thisway, artefacts can be removed from EEG or MEGdata with minimal interference in brain activity.Likewise, BSS can be used to separate specific brainactivity, such as epileptiform discharges, in order toassist in further analyses [39]. Moreover, BSS meth-ods can be applied to brain recordings using anotherapproach. Considering the intrinsic complexity ofthe brain recordings, some BSS components mayhave certain features that could make them moresensitive to particular brain states, such as AD [27]or audiovisual stimulation [30]. Hence, the mostrelevant components may be selected and the brainrecordings may be partially reconstructed using onlythese components [27]. Thus, diverse brain statesmight be better differentiated in comparison to thesituation where BSS is not used. Nevertheless,despite the advantages that this approach mayprovide, few studies have implemented it. To ourknowledge, this methodology has only been appliedto EEG data in [27,40].
In this study, we applied a BSS algorithm to back-ground MEG recordings from AD patients and controlsubjects. Two spectral variables (median frequencyand spectral entropy, denoted by fmedian andSpecEn, respectively) were used to characteriseevery MEG channel and BSS component. The BSScomponents of both groups were analysed to assess
how fmedian and SpecEn varied within them and todecidewhich provided themost relevant informationto classify the subjects. In addition, the classificationaccuracies achieved with and without the BSS pre-processing were compared. We wanted to test thehypothesis that this procedure of BSS and subsequentselection of AD-relevant components might improvethe classification of AD patients versus control sub-jects based on MEG background activity.
2. Subjects and signals
2.1. Subjects
Twenty-one AD patients participated in this study.The average age of this subject group, which wasformed by 13 women and 8 men, was 73.19 � 9.22years, mean � standard deviation (S.D.). All ADpatients were recruited from the ‘‘Asociacion deFamiliares de Enfermos de Alzheimer’’ (Spain) andfulfilled the criteria of probable AD according to theguidelines provided by the National Institute ofNeurological and Communicative Disorders andStroke—Alzheimer’s Disease and Related DisordersAssociation (NINCDS-ADRDA) [41]. The diagnosis wasbased on brain scans and thorough medical, physi-cal, neurological, psychiatric and neurophysiologi-cal examinations. MMSE was used to assess theseverity of AD [4]. The patients’ average MMSE scorewas 17.95 � 3.97 (mean � S.D.). The MEG recordingwas carried out when AD was diagnosed. No patientreceived medication that could affect the MEGsignals.
In addition, 21 control subjects (age = 70.19 �6.96 years, mean � S.D.; 13 women) without pastor present neurological or psychiatric diseases wererecruited to participate in this study. The differencein age between both subject groups was not signi-ficant ( p-value = 0.1861, Mann—Whitney U-test).The average MMSE score for the controls was29.05 � 0.97 (mean � S.D.).
All AD patients’ caregivers and all control sub-jects gave their informed consent to participate inthis study, which was approved by the local ethicscommittee.
2.2. Magnetoencephalogram recording
MEGs were recorded in a magnetically shieldedroom using a 148-channel whole-head magnet-ometer (MAGNES 2500 WH, 4D Neuroimaging). Dur-ing the recording process, the subjects lay on apatient bed with eyes closed. In order to avoidartefactual contamination, they were asked to stayawake and not to move eyes and head. Five minutes

78 J. Escudero et al.
of MEG recording were acquired from each subjectat a sampling frequency of 678.17 Hz using a hard-ware band-pass filter with cut-off frequencies at 0.1and 200 Hz. To reduce data length, these recordingswere decimated to 169.55 Hz. This procedure con-sisted of filtering the recordings according to theNyquist criterion and down-sampling them by afactor of four. Then, the recordings were copiedas ASCII files to a personal computer. They wereprocessed with a 50 Hz notch filter and a band-passfinite impulse response filter designed with a Ham-ming window with cut-off frequencies at 1.5 and40 Hz. MEG epochs of 20 s (3390 samples) that weresimultaneously artefact-free at all channels wereselected for analysis.
3. Methods
3.1. Blind source separation
Briefly, BSS techniques attempt to find the set of nunknown underlying components, s(t) = [s1(t), s2(t),. . ., sn(t)]
T, where T denotes the transpose of avector or matrix and t is the discrete time index,which form the m temporally and spatially corre-lated measured signals, x(t) = [x1(t), x2(t), . . .,xm(t)]
T [28,29,32]. Hence, in this study, s(t) repre-sents the BSS components, whereas the MEG record-ings are denoted by x(t). The mixing process isassumed to be linear [28,34,35]. Mathematically:
xðtÞ ¼ AsðtÞ; (1)
where A is a full rank m � n mixing matrix and x(t)and s(t) are centred [28,29].
External noise may be included in the model[36,38]. However, for the sake of simplicity, thenoise term has not been incorporated in this study[34,35]. In addition, the number of BSS componentsmust be less than or equal to the number of recordedsignals (m � n) [29]. Taking into account that onlythe most relevant components will be retained forfurther MEG reconstruction and classification ana-lysis, we set m = n instead of applying a dimension-ality reduction technique in advance.
In order to estimate s(t) and A, several hypoth-eses are made [28,29]. The most important assump-tion may be that the BSS components are mutuallyindependent or, on the other hand, that they shouldbe decorrelated at any time delay. In addition, it ishypothesised that the mixing process is linear andinstantaneous. All these requirements are suitablymet by EEG and MEG data [29].
Under these hypotheses, some BSS algorithms usethe temporal dependences of the recordings to finda demixing matrix, W, [28,29]. Using W, the recov-
ered BSS components vector, y(t) = [y1(t), y2(t), . . .,ym(t)]
T, which estimates s(t), is computed by:
yðtÞ ¼ WxðtÞ: (2)
Some BSS components of the MEG recordings maybe more affected by AD than others [27]. Thus, avector formed by the subset of the most sensitivecomponents — ysubset(t) — could be used to computea partial reconstruction of the MEG recordings,xpartial(t):
xpartialðtÞ ¼ W�1ysubsetðtÞ: (3)
Hence, it could be assumed that some remarkablefeatures of AD may be enhanced in xpartial(t) bycomparison with the raw recordings, x(t) [27].
However, it should be noted that a certain orderor clustering is needed to compare BSS componentsextracted from different MEG epochs and subjects[27,30]. Thus, among the BSS algorithms available,we used the algorithm for multiple unknown signalsextraction (AMUSE) [28,42] to decompose the MEGs.This algorithm orders the extracted components bydecreasing linear predictability [27].
3.2. Algorithm for multiple unknownsignals extraction
Several BSS algorithms are based on the hypothesisthat BSS components should have no temporal andspatial correlations [28]. Consequently, this kind ofalgorithms find W by minimising the cross-correla-tions between components at certain time delays[29]. One of these algorithms is AMUSE, which dec-orrelates the signals at two time lags (typically, t = 0and 1) [27,29,36,42]. Since only two time delays areconsidered inAMUSE, its computational complexity islow [27,28]. Furthermore, AMUSE always offers thesame separation when it is applied to the same inputdata set and it orders the components by decreasinglinear predictability [27]. This inherent order enablesus to compare AMUSE components from differentepochs and subjects straightforwardly. Thus, thedefinition of the subsets ysubset(t) can be done byremoving the AMUSE components whose index ishigher and/or lower than certain thresholds.
First of all, AMUSE applies a principal componentanalysis to the input data, x(t), in order to whitenthem [27,42]. Let E{�} be the expectation value of avariable. Then, the covariance matrix of x(t) is:
Rxð0Þ ¼ EfxðtÞxðtÞTg: (4)
The whitened data, z(t), are computed by [27]:
zðtÞ ¼ QxðtÞ; (5)
where Q = [Rx(0)]�1/2.

Assessment of classification improvement in patients with Alzheimer’s disease based on MEG BSS 79
Afterwards, the signals are decorrelated at aparticular time delay, t (usually t = 1) [27,28,36].A time-delayed covariance matrix is computed [42]as:
RzðtÞ ¼ EfzðtÞzðt� tÞTg (6)
and the eigenvalue decomposition of (Rz(t) +Rz(t)
T)/2 is calculated. If V denotes the eigenmatrixcomputed from this decomposition, the demixingmatrix W is estimated as [42]:
W ¼ VTQ: (7)
As it has been described, AMUSE consists of awhitening process followed by a singular valuedecomposition. Thus, the computational complexityof this algorithm is low [27]. In a Matlab1 7.0environment running on a personal computer witha Intel Pentium Duo1 2.80 GHz processor and 2GB RAM, the decomposition of the 148 MEGchannels into the 148 AMUSE components took0.4023 � 0.0088 s/epoch (mean � S.D.).
3.3. Feature extraction
Two spectral features were used to characterise theMEG signals and the AMUSE components: fmedian andSpecEn. Firstly, we computed the PSD of each MEGchannel or AMUSE component for every epoch. PSDswere calculated as the Fourier transforms of thecorresponding autocorrelation functions. Then, thePSDs estimated from the epochs available wereaveraged for each subject and MEG channel orAMUSE component. Finally, fmedian and SpecEnvalues were computed from the mean PSDs.
fmedian is accepted as a simple way to summarisethe spectral content of the PSD [16]. It has beenused to study the spectra of AD, mild cognitiveimpairment (MCI) or vascular dementia patients’brain recordings [11,13—16], among other mentaldiseases. fmedian is defined as the frequency whichcontains half the PSD power. Taking into considera-tion the cut-off frequencies of the band-pass filterapplied to the MEG signals (1.5 and 40 Hz), fmedian
was computed as:
1
2
X40Hzf¼1:5Hz
PSD ð fÞ" #
¼Xfmedian
f¼1:5HzPSD ð fÞ: (8)
Additionally, we estimated the SpecEn in order toquantify the flatness of the PSD. SpecEn is computedapplying the Shannon’s entropy to the normalisedPSD (PSDn) [18,19]:
SpecEn ¼ � 1
logðNÞX40Hz
f¼1:5HzPSDnð fÞ log½PSDnð fÞ�;
(9)
where N is the number of frequency bins and thedivision by log(N) normalises the SpecEn to a scalefrom 0 to 1.
High SpecEn values are due to broad and flatspectra (e.g., white noise), whereas this entropyestimator provides low values for spectra whoseenergy is mainly focused round a narrow frequencyband (e.g., a sine wave). Thus, SpecEn measures thedisorder of the spectrum, estimating the signalirregularity [18]. Several studies have appliedSpecEn to electromagnetic brain signals [18,19],including the analysis of AD patients’ EEGs [17]and MEGs [16].
3.4. Statistical analysis
Mann—Whitney U-test was used to decide whetherthere were statistically significant differencesbetween both subject groups in the fmedian andSpecEn values of the AMUSE components. The Bon-ferroni correction was applied to the Mann—WhitneyU-test p-values in order to avoid spurious positives.Previously, homoscedasticity was verified with theBrown—Forsythe test, and Kolmogorov—Smirnovtest assessed whether the differences in the shapeof the distributions were negligible.
A leave-one-out cross-validation procedure,together with receiver operating characteristics(ROC) curves [43], was used to measure the abilityof fmedian and SpecEn to distinguish AD patients fromcontrol subjects when different AMUSE componentsubsets were retained. ROC plots analyse the per-formance of a certain variable in classifying twogroups. In this study, sensitivity is defined as the rateof AD patients properly classified, whereas specifi-city represents the percentage of control subjectscorrectly detected. Accuracy denotes the total frac-tion of subjects precisely identified. ROC curves alsooffer visual information about the quality of theclassification rule, as they plot the sensitivity/{1 � specificity} pair of values for all possible cut-off points. Furthermore, leave-one-out cross-vali-dation avoids the appearance of over-fitting andbias in the analysis. The leave-one-out cross-valida-tion classifies each single case using the decisionrule obtained from the ROC analysis of all remainingdata. Then, this process is repeated for all cases.Although this procedure typically reduces the sen-sitivity, specificity and accuracy values, it increasesthe reproducibility of the results [27].
In addition, correlations between AD patients andcontrol subjects’ MMSE scores and their averagevalues of fmedian and SpecEn were assessed withSpearman’s rank correlation coefficient (r) whendifferent AMUSE component subsets were retained.Thecorrespondingp-values for testing thehypothesis

80 J. Escudero et al.
Figure 2 Average SpecEn values of every AMUSE com-ponent for AD patients and control subjects.
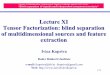
Figure 1 Average fmedian values of every AMUSE compo-nent for AD patients and control subjects.
of no correlation against the alternative that there isa non-zero correlation were also estimated. Correla-tion was considered significant when the p-value wasbelow 0.01.
Figure 3 Bonferroni-corrected p-values of fmedian andSpecEn for every AMUSE component.
4. Results
First of all, we used AMUSE to decompose MEGbackground activity epochs of 20 s (3390 samples)from 21 AD patients and 21 control subjects. Thanksto the inherent order of the AMUSE components, itwas straightforward to compare them betweengroups. Thus, mean PSDs were calculated for eachsubject and each AMUSE component index. Theseaverage PSDs were characterised with fmedian andSpecEn. Fig. 1 shows the average fmedian values foreach AMUSE component and subject group. Thefmedian increased with the AMUSE component index.This suggests that the decreasing linear predictabil-ity order provided by AMUSE is indeed determinedarranging the components by their spectral content,from low to high frequency oscillations. Moreover,the typical slowing of AD patients’ brain recordingscan also be observed in Fig. 1, since the averagefmedian values were lower for the dementedpatients’ components than for those of the controlsubjects. In addition, Fig. 2 depicts the meanSpecEn values of both groups for each AMUSE com-ponent. SpecEn evolved similarly for both kinds ofsubjects. Moreover, since this entropy estimatormeasures the spectral irregularity and AMUSE ordersthe components by decreasing linear predictability,the SpecEn of the components rose with the AMUSEindex, until it reached values close to 1. In addition,SpecEn values were usually higher in control sub-jects than in AD patients. This illustrates that ADpatients have a MEG background activity with anarrower spectral content than control subjects.
Visual inspection of both Figs. 1 and 2 suggestedthat the most AD-sensitive components had indexeswhich varied from 5 to 60, approximately. In order toevaluate the statistical significance of the differ-ences between groups, we carried out a Mann—Whitney U-test with a Bonferroni correction.Fig. 3 summarises the results of this analysis. Dif-ferences were usually more significant using fmedian
than SpecEn. Moreover, it can be seen that thelargest differences were focused around indexesranging from 10 to 40 with SpecEn and from 15 to55 using fmedian. Taking this into consideration, wechose two small subsets of AMUSE components topartially reconstruct the MEG recordings. The firstone contained 21 components (15—35), and it wasdenoted by BSS-{15,35}. The second subset wasformed by 11 AMUSE components: from 20 to 30(BSS-{20,30}). The classification results achievedwith the selection of these two subsets were com-pared to those provided by the MEG recordingswithout BSS.

Assessment of classification improvement in patients with Alzheimer’s disease based on MEG BSS 81
Table 1 Results from the ROC analysis with a leave-one-out cross-validation procedure for the average fmedian values
Without BSS BSS-{15,35} BSS-{20,30}
Control subjects, mean � S.D. (Hz) 13.08 � 2.95 12.60 � 1.32 12.57 � 1.24AD patients, mean � S.D. (Hz) 8.98 � 2.32 9.76 � 1.69 9.83 � 1.71Sensitivity (%) 71.43 85.71 80.95Specificity (%) 66.67 80.95 80.95Accuracy (%) 69.05 83.33 80.95
Figure 4 ROC curves computed with a leave-one-outcross-validation procedure for AD patients versus controlsubjects classification with fmedian. The comparisonbetween MEG epochs with and without the BSS componentselection procedure is shown.
For each of the three cases (without BSS, BSS-{15,35} and BSS-{20,30}), an average PSD perchannel and subject was computed. Two variables,fmedian and SpecEn, were calculated from the PSDfunctions. After computing them, we obtained 148values for each of the 21 AD patients and 21 healthycontrols. Owing to the high spatial density of theMEG channels, it may be helpful to reduce theproblem dimensionality in order to simplifythe analysis and the interpretation of the results.Thus, we averaged the 148 fmedian or SpecEn vari-ables for each subject. Hence, the classificationanalysis was carried out using one mean value offmedian or SpecEn per subject.
A ROC analysis combined with a leave-one-outcross-validation procedure was used to evaluate theclassification achieved by fmedian and SpecEn in eachof the three cases (without BSS, BSS-{15,35} andBSS-{20,30}). Table 1 shows the sensitivity, specifi-city and accuracy values obtained with fmedian. Theaverage values for each subject group are alsodisplayed. AD patients had lower fmedian values thancontrol subjects. It can be noticed that the S.D. waslarger for the case where no BSS was used than forBSS-{15,35} or BSS-{20,30}. This suggests that thecomponent selection procedure reduced the inter-subject group variability of fmedian. Furthermore,both cases, BSS-{15,35} and BSS-{20,30}, improvedthe accuracy of the subject classification more than11%. The accuracy without BSS was 69.05%. In con-trast, it reached 80.95% for BSS-{20,30} and 83.33%when the subset BSS-{15,35} was used. In addition,Fig. 4 illustrates the average ROC curves associatedwith these analyses. The ROC plots related to BSS-{15,35} and BSS-{20,30} are akin. The areas undertheir ROC curves are larger than that obtained with-out BSS, indicating a better diagnostic test when thecomponent selection preprocessing is used.
The ability of SpecEn to distinguish AD patientsfrom control subjects was also evaluated in thethree studied cases. The classification results (sen-sitivity, specificity, accuracy and mean � S.D. forboth groups) are summarised in Table 2. AD patients’MEG background activity is more regular than con-trol subjects’ one, as the SpecEn values were lowerfor the former. Likewise fmedian, the S.D. of theSpecEn values decreased when the MEG was par-
tially reconstructed. For this variable, the BSS andcomponent selection procedure provided an accu-racy improvement about 10% (71.43 and 73.81% forBSS-{15,35} and BSS-{20,30}, in that order, against61.91% for raw MEG recordings). Furthermore, thecorresponding ROC plots are depicted in Fig. 5. Theyconfirm the higher quality of the diagnostic testapplied to BSS-processed signals than that basedon MEG recordings without the BSS preprocessing.
Finally, we assessed whether the severity of thedementia, measured with the MMSE, was correlatedwith the average values of fmedian and SpecEn foreach case. All the computed r values, which areshown in Table 3, were significant ( p-value < 0.01).There were slight increases in the correlation coefi-cients when the BSS and partial reconstruction wasapplied (BSS-{15,35} and BSS-{20,30}) in comparisonwith the case where no BSS was used.
5. Discussion and conclusions
In this study, we used the AMUSE algorithm [28,42]to decompose artefact-free MEG epochs of 21 ADpatients and 21 control subjects. Every AMUSE com-ponent was characterised with fmedian [16] andSpecEn [18,19], and the evolution of these spectral

82 J. Escudero et al.
Table 2 Results from the ROC analysis with a leave-one-out cross-validation procedure for the average SpecEn values
Without BSS BSS-{15,35} BSS-{20,30}
Control subjects (mean � S.D.) 0.9346 � 0.0281 0.9549 � 0.0127 0.9585 � 0.0111AD patients (mean � S.D.) 0.8962 � 0.0539 0.9303 � 0.0203 0.9351 � 0.0189Sensitivity (%) 66.67 80.95 76.19Specificity (%) 57.14 61.91 71.43Accuracy (%) 61.91 71.43 73.81
features with the AMUSE component index wasanalysed. Mann—Whitney U-test determined whichcomponents offered the most significant differencesbetween both subject groups. Afterwards, two com-ponent subsets were selected to partially recon-struct the MEG recordings. These subsets wereformed by the components BSS-{15,35} and BSS-{20,30}. Finally, the accuracy achieved in each ofthese two cases, when either fmedian or SpecEn wasused to classify the subjects, was compared to thatobtained from the MEG recordings without BSS.
BSS techniques estimate the set of componentsthat originated the recorded brain activity blindly[28]. It should be noted that the BSS components arenot equivalent generator dipoles, but mutually inde-pendent and simultaneous electromagnetic activitymeasuredover the scalp [29,33]. In the last years,BSSalgorithms have been increasingly applied to EEG andMEGdata in order to isolate the artefacts that usuallyappear in these signals [29,33—38]. Once the arte-facts have been identified and detached, the braincomponents are projected back to the channels toobtain the clean recordings [34,38]. On the otherhand, the approach taken in this study is different.We did not aim to remove artefacts fromMEG record-ings with minimal brain activity distortion. Instead,we attempted to emphasise the differences between
Figure 5 ROC curves computed with a leave-one-outcross-validation procedure for AD patients versus controlsubjects classification with SpecEn. The comparisonbetween MEG epochs with and without the BSS componentselection procedure is shown.
AD patients and control subjects’ MEG recordings byretaining only the components which account for themost relevant differences between groups. Thus, thepartially reconstructedMEG recordings do not reflectthe brain activity accurately, but they should havemore different values of fmedian and SpecEn than theMEG data without BSS.
Moreover, it is worth noting that, previously tothe BSS, the MEG epochs with clear artefacts wererejected. We applied the epoch rejection method inorder to avoid surplus complexity and to assess theclassification improvement without any other kindof preprocessing. Moreover, the same artefact-freeraw MEG recordings were used to compute thefmedian and SpecEn with and without the BSS andcomponent selection procedure. Therefore, thediverse classification results could be directly com-pared to evaluate the relative classificationimprovement.
There is a wide range of BSS algorithms that canbe applied to decompose EEGs or MEGs [29]. Amongthese, we employed AMUSE [27,36,42], which isbased on second order statistics [29] likewise otherBSS algorithms, such as the second order blindidentification (SOBI) algorithm [28,32]. SOBI mini-mises the cross-correlations at a much denser set oftime delays than AMUSE [32]. Although AMUSE mightnot separate the components as completely as SOBI[32], the computational complexity of AMUSE islower than in most BSS algorithms [36]. Further-more, AMUSE has other advantages: it always offersthe same separation when applied to the same inputdata set and orders the components by decreasinglinear predictability [27,42]. This inherent order isone of the key points of this component selectionprocedure, since it enables us to straightforwardlycompare AMUSE components from different epochsand subjects. On the other hand, due to the factthat AMUSE only uses two time delays to decorrelatethe signals, the AMUSE decomposition may be lessrobust to additive white noise than that computedusing SOBI or other BSS algorithms [32,36]. Never-theless, the simplicity of AMUSE makes the inter-pretation of the component order in terms of fmedian
or SpecEn plain.The features used for classification were fmedian
and SpecEn. Both variables try to characterise the

Assessment of classification improvement in patients with Alzheimer’s disease based on MEG BSS 83
Table 3 Spearman’s rank correlation coefficients (r) between the MMSE scores and the average values of fmedian andSpecEn for each case: ‘‘Without BSS’’, ‘‘BSS-{15,35}’’ and ‘‘BSS-{20,30}’’
Without BSS BSS-{15,35} BSS-{20,30}
fmedian SpecEn fmedian SpecEn fmedian SpecEn
r 0.5414 * 0.3933 * 0.6176 * 0.4934 * 0.6068 * 0.5485 *
*Correlation was significant ( p-value < 0.01).
whole spectrum with a single value. The formerassesses the slowing of the PSD [16], whereas thelatter measures the flatness of the spectrum [19].Moreover, both fmedian and SpecEn have alreadybeen applied to the analysis of AD patients’ EEGand MEG data. Our results were in agreement withthese previous studies [13—17]. Firstly, the fmedian
values were lower for AD patients than for controlsubjects in both AMUSE components and MEG chan-nels. This slowing was also found when differentfrequency bands and severity degrees of AD wereanalysed [11,13,14]. Secondly, AD patients hadlower SpecEn than control subjects. This suggeststhat the AD patients’ brain activity is more regularthan in control subjects. This result was also foundin EEG [17] and MEG data [16], although the differ-ences between both groups were not significant inthe EEG study. Moreover, other non-linear analysismethods support the hypothesis of decreased irre-gularity and complexity in AD patients’ EEGs andMEGs [5,6,17,20,22—24]. Nevertheless, the origin ofthese changes is not yet clear, due to the hetero-geneity of AD [1,5].
The Mann—Whitney U-test showed that the dif-ferences between both groups were more significantfor fmedian than for SpecEn. These results agree witha previous study where these variables were appliedto MEG recordings [16]. Nevertheless, the p-valuesevolved in a similar way with the AMUSE index forboth fmedian and SpecEn. Furthermore, the mostsignificant components were gathered together.Inspecting the p-values, we could evaluate the abil-ity of every AMUSE component to distinguish ADpatients from control subjects. We decided to keepthe subsets BSS-{15,35} (21 components) and BSS-{20,30} (11 components) to partially reconstruct theMEGs. Moreover, the projection of a componentsubset implies a kind of model order selection inthe BSS methodology. Furthermore, we did not esti-mate a fixed value for n a priori to reduce thedimensionality [29]. Instead, the most significantcomponents were projected to rebuild the record-ings. In addition, we classified the subjects using theaverage value of fmedian or SpecEn for the 148 MEGchannels.
Whereas the significance of each component wasevaluated with a Mann—Whitney U-test, the classi-
fication rate improvement was measured using aROC analysis with a leave-one-out cross-validationprocess. We found that the BSS and componentselection procedure provided an accuracy improve-ment between 9.52 and 14.28%. Additionally, thisprocedure also increased the correlation betweenthe MMSE scores and the average values of fmedian
and SpecEn slightly. This suggests that the partialreconstruction of MEG recordings may increase theconcordance between the severity of the mentalimpairments described by MMSE and the fmedian andSpecEn values.
A previous study where a subset of five AMUSEcomponents extracted from 21 EEG channels wereretained reported maximum accuracy improve-ments of 10% [27]. They tried to classify 22 MCIpatients who later proceeded to AD against 38 con-trol subjects. Our selection of the subsets BSS-{15,35} and BSS-{20,30} contrasts with their division[27], since in that previous work only the compo-nents below a certain index were taken into accountfor projection. Nevertheless, observing the p-valuesplotted in Fig. 3, it is clear that our first componentsprovided little differentiation between groups.Thus, as it was also suggested in Ref. [27], retainingan intermediate component subset, rather than justselecting the first AMUSE components, was benefi-cial in our case. A linear discriminant analysis with across-validation procedure applied to the relativepower in six frequency bands was used to classify the22 MCI patients and the 38 control subjects in [27].Thus, the settings of that study are different fromours, as a more elaborated classification rule wasused to distinguish the MCI patients. Nevertheless,that research work did not measure the improve-ment in each variable separately [27]. In contrast,our straightforward classification method helps toassess the improvement in each variable, fmedian orSpecEn. However, both studies have reported apromising accuracy increase of about 10%. In addi-tion, a later study used the partially reconstructedEEGs obtained in Ref. [27] to further improve theclassification of the MCI patients [40]. This subse-quent study achieved an additional rise of about 13%over the accuracy reported in [27] using a ‘‘bumpmodelling’’ of the EEG wavelet time-frequencytransform and a neural network classifier [40].

84 J. Escudero et al.
Therefore, it can be seen that the component selec-tion procedure not only improves the results ofsimple classification methods, but it also may pro-vide high classification rates when complex discri-minant techniques are used.
This procedure based on BSS and subsequentpartial reconstruction of the electromagnetic brainrecordings has been tested using only spectral andtime-frequency features [27,40]. Nevertheless, thiscomponent selection procedure could also beapplied when the brain activity is characterised withother kinds of measures, such as complexity orconnectivity estimators. Non-linear complexityparameters may complement the information pro-vided by spectral features about the brain signals[5,6]. Abnormal patterns have been found in ADpatients’ EEGs and MEGs with different complexityestimators [21—23]. Additionally, since AD isthought to be a syndrome of neocortical disconnec-tion [5,6], connectivity measures may reflect animpairment of functional connectivity among cor-tical areas [24,25]. Consequently, future researchshould assess whether these or othermeasures couldbe suitably introduced into the component selectionprocedure. Additionally, it should be studiedwhether the subset of components with significantdifferences between AD patients and controlschanges when different features are used to char-acterise the signals. These studies might contributeto help in clinical AD diagnosis and to increase ourinsight into this dementia.
Certain limitations of our study merit attention.Firstly, the sample size was small. In addition, othermental diseases, such as MCI [13,15] or other typesof dementia [10,14], can produce a similar slowingin the brain activity. Thus, additional analyses with alarger database including MEG recordings frompatients with other mental diseases should be car-ried out to confirm our results. Secondly, althoughthe epochs used in this study have a length similar tothat analysed in previous works [27,36], it should beevaluated if different epoch lengths affect the per-formance of our methodology. Finally, due to thesimplicity of the BSS algorithm and the spectralfeatures studied, the classification performancemight be further improved using other BSS algo-rithms to decompose the recordings or features tocharacterise them.
In summary, this paper proposes a method toimprove the classification of AD patients and controlsubjects when MEG background activity recordingsare analysed. This method is based on a simpleBSS algorithm — AMUSE — [42] which orders theextracted components by decreasing linear predict-ability [27]. Afterwards, the components which mayoffer a significant differentiation between subject
groups are projected back to the MEG channels, andthese partially reconstructed signals are charac-terised with fmedian [16] and SpecEn [18,19]. Theimprovement in the classification performance wascompared to the case where no BSS preprocessingwas applied to the same MEG signals. Although thismethodology must be applied to a larger database inorder to validate our preliminary findings, theresults showed that the classification accuracyincreased between 9.52 and 14.28%, suggestingthe possible usefulness of this approach to help inthe AD diagnosis.
Acknowledgements
This study was supported in part by the ‘‘Ministeriode Educacion y Ciencia’’ and FEDER grant MTM 2005-08519-C02-01 and by the grant project VA108A06from ‘‘Consejerıa de Educacion de Castilla y Leon’’.The authors are thankful to the ‘‘Asociacion deEnfermos de Alzheimer’’ in Spain for supplying thepatients who took part in this study and to thereferees for their critical feedback on the originalmanuscript.
Conflict of interest
Authors have no conflicts of interest that couldinappropriately influence this research work.
References
[1] Selkoe DJ. Alzheimer’s disease: genes, proteins, and ther-apy. Physiol Rev 2001;81(2):741—66.
[2] Masters CL, Cappai R, Barnham KJ, Villemagne VL. Molecularmechanisms for Alzheimer’s disease: implications forneuroimaging and therapeutics. J Neurochem 2006;97(6):1700—25.
[3] Bird TD. Alzheimer’s disease and other primary dementias.In: Braunwald E, Fauci AS, Kasper DL, Hauser SL, Longo DL,Jameson JL, editors. Harrison’s principles of internal med-icine. New York: The McGraw-Hill Companies Inc.; 2001. p.2391—9.
[4] Folstein MF, Folstein SE, McHugh PR. Minimental state. Apractical method for grading the cognitive state of patientsfor the clinician. J Psychiat Res 1975;12(3):189—98.
[5] Jeong J. EEG dynamics in patients with Alzheimer’s disease.Clin Neurophysiol 2004;115(7):1490—505.
[6] StamCJ.Nonlineardynamical analysisofEEGandMEG:reviewof an emerging field. Clin Neurophysiol 2005;116(10):2266—301.
[7] Darvas F, Pantazis D, Kucukaltun-Yildirim E, Leahy RM. Map-ping human brain function with MEG and EEG: methods andvalidation. Neuroimage 2004;23(Suppl. 1):S289—99.
[8] Hari R. Magnetoencephalography in clinical neurophysiologi-cal assessment of human cortical functions. In: Niedermeyer

Assessment of classification improvement in patients with Alzheimer’s disease based on MEG BSS 85
E, Lopes da Silva F, editors. Electroencephalography:Basic Principles, Clinical Applications, and RelatedFields. Philadelphia: Lippincott Williams & Wilkins; 2005. p.1165—97.
[9] Hamalainen M, Hari R, Ilmoniemi RJ, Knuutila J, LounasmaaOV. Magnetoencephalography–—theory, instrumentation,and applications to noninvasive studies of the workinghuman brain. Rev Mod Phys 1993;65(2):413—97.
[10] Franciotti R, Iacono D, Della Penna S, Pizzella V, Torquati K,Onofrj M, et al. Cortical rhythms reactivity in AD, LBD andnormal subjects: a quantitative study. Neurobiol Aging2006;27(8):1100—9.
[11] Penttila M, Partanen JV, Soininen H, Riekkinen PJ. Quanti-tative analysis of occipital EEG in different stages of Alzhei-mer’s disease. Electroencephalogr Clin Neurophysiol1985;60(1):1—6.
[12] Berendse HW, Verbunt JPA, Scheltens Ph, van Dijk BW,Jonkman EJ. Magnetoencephalographic analysis of corticalactivity in Alzheimer’s disease: a pilot study. Clin Neuro-physiol 2000;111(4):604—12.
[13] Jelic V, Johansson SE, Almkvist O, Shigeta M, Julin P, Nord-berg A, et al. Quantitative electroencephalogram in mildcognitive impairment: longitudinal changes and possibleprediction of Alzheimer’s disease. Neurobiol Aging2000;21(4):533—40.
[14] Signorino M, Pucci E, Belardinelli N, Nolfe G, Angeleri F. EEGspectral analysis in vascular and Alzheimer dementia. Elec-troencephalogr Clin Neurophysiol 1995;94(5):313—25.
[15] Fernandez A, Hornero R, Mayo A, Poza J, Gil-Gregorio P,Ortiz T. MEG spectral profile in Alzheimer’s disease and mildcognitive impairment. Clin Neurophysiol 2006;117(2):306—14.
[16] Poza J, Hornero R, Abasolo D, Fernandez A, Garcıa M.Extraction of spectral basedmeasures from MEG backgroundoscillations in Alzheimer’s disease. Med Eng Phys2007;29(10):1073—83.
[17] Abasolo D, Hornero R, Espino P, Alvarez D, Poza J. Entropyanalysis of the EEG background activity in Alzheimer’s dis-ease patients. Physiol Meas 2006;27(3):241—53.
[18] Inouye T, Shinosaki K, Sakamoto H, Toi S, Ukai S, Iyama A,et al. Quantification of EEG irregularity by use of the entropyof the power spectrum. Electroencephalogr Clin Neurophy-siol 1991;79(3):204—10.
[19] Sleigh JW, Steyn-Ross DA, Grant C, Ludbrook G. Corticalentropy changes with general anaesthesia: theory andexperiment. Physiol Meas 2004;25(4):921—34.
[20] Gomez C, Hornero R, Abasolo D, Fernandez A, Escudero J.Analysis of the magnetoencephalogram background activityin Alzheimer’s disease patients with auto-mutual informa-tion. Comput Meth Programs Biomed 2007;87(3):239—47.
[21] van Cappellen van Walsum AM, Pijnenburg YAL, BerendseHW, van Dijk BW, Know DL, Scheltens Ph, et al. A neuralcomplexity measure applied to MEG data in Alzheimer’sdisease. Clin Neurophysiol 2003;114(6):1034—40.
[22] Gomez C, Hornero R, Abasolo D, Fernandez A, Lopez M.Complexity analysis of the magnetoencephalogram back-ground activity in Alzheimer’s disease patients. Med EngPhys 2006;28(9):851—9.
[23] Escudero J, Abasolo D, Hornero R, Espino P, Lopez M. Analysisof electroencephalograms in Alzheimer’s disease patientswith multiscale entropy. Physiol Meas 2006;27(11):1091—106.
[24] Jeong J, Gore JC, Peterson BS. Mutual information analysisof the EEG in patients with Alzheimer’s disease. Clin Neu-rophysiol 2001;112(5):827—35.
[25] Stam CJ, Montez T, Jones BF, Rombouts SARB, van der MadeY, Pijnenburg YAL, et al. Disturbed fluctuations of resting
state EEG synchronization in Alzheimer’s disease. Clin Neu-rophysiol 2005;116(3):708—15.
[26] Osipova D, Ahveninen J, Jensen O, Ylikoski A, Pekkonen E.Altered generation of spontaneous oscillations in Alzhei-mer’s disease. Neuroimage 2005;27(4):835—41.
[27] Cichocki A, Shishkin SL, Musha T, Leonowicz Z, Asada T,Karachi T. EEG filtering based on blind source separation(BSS) for early detection of Alzheimer’s disease. Clin Neu-rophysiol 2005;116(3):729—37.
[28] Cichocki A, Amari S. Adaptive blind signal and image proces-sing: learning algorithms and applications. Chichester (UK):John Wiley and Sons; 2003.
[29] James CJ, Hesse CW. Independent component analysis forbiomedical signals. Physiol Meas 2005;26(1):R15—39.
[30] Jin SH, Jeong J, Jeong DG, Kim DJ, Kim SY. Nonlineardynamics of the EEG separated by independent componentanalysis after sound and light stimulation. Biol Cybern2002;86(5):395—401.
[31] James CJ, Gibson O, Davies M. On the analysis of singleversus multiple channels of electromagnetic brain signals.Artif Intell Med 2006;37(2):131—43.
[32] Tang AC, Liu JY, Sutherland MT. Recovery of correlatedneuronal sources from EEG: the good and bad ways of usingSOBI. NeuroImage 2005;28(2):507—19.
[33] Vorobyov S, Cichocki A. Blind noise reduction for multi-sensory signals using ICA and subspace filtering, withapplication to EEG analysis. Biol Cybern 2002;86(4):293—303.
[34] Joyce CA, Gorodnitsky IF, Kutas M. Automatic removal ofeye movement and blink artifacts from EEG data usingblind component separation. Psychophysiology 2004;41(2):313—25.
[35] Melissant C, Ypma A, Frietman EEE, Stam CJ. A methodfor detection of Alzheimer’s disease using ICA-enhancedEEG measurements. Artif Intell Med 2005;33(3):209—22.
[36] Ting KH, Fung PCW, Chang CQ, Chan FHY. Automatic correc-tion of artefact from single-trial event-related potentials byblind source separation using second order statistics only.Med Eng Phys 2006;28(8):780—94.
[37] Sander TH, Wubbeler G, Lueschow A, Curio G, Trahms L.Cardiac artifact subspace identification and elimination incognitive MEG data using time-delayed decorrelation. IEEETrans Biomed Eng 2002;49(4):345—54.
[38] Escudero J, Hornero R, Abasolo D, Fernandez A, Lopez-Coronado M. Artifact removal in magnetoencephalogrambackground activity with independent component analysis.IEEE Trans Biomed Eng 2007;54(11):1965—73.
[39] Kobayashi K, James CJ, Nakatori T, Akiyama T, Gotman J.Isolation of epileptiform discharges from unaveraged EEG byindependent component analysis. Clin Neurophysiol1999;110(10):1755—63.
[40] Vialatte F, Cichocki A, Dreyfus G, Musha T, Gervais R. Earlydetection of Alzheimer’s disease by blind source separationand bump modelling of EEG signals. Lect Notes ComputScience 2005;3696:683—92.
[41] McKhann G, Drachman D, Folstein M, Katzman R, Price D,Stadlan EM. Clinical diagnosis of Alzheimer’s disease: reportof the NINCDS-ADRDA Work Group under the auspices ofDepartment of Health and Human Services Task Force onAlzheimer’s disease. Neurology 1984;34(7):939—44.
[42] Tong L, Liu R, Soon VC, Huang Y-F. Indeterminacy andidentifiability of blind identification. IEEE Trans Circuits Syst1991;38(5):499—509.
[43] Zweig MH, Campbell G. Receiver-operating characteristic(ROC) plots: a fundamental evaluation tool in clinical med-icine. Clin Chem 1993;39(4):561—77.