Embed Size (px)
Citation preview

Assessment of Children’s Health System and UAB Department of Pediatrics Transition of Care of Children and Youth with Special
Health Care Needs
Cynthia C. deSa, BA (MPH and MSW Candidate, August 2009)

ABSTRACT: Purpose: Although the 1989 Surgeon General’s report Growing Up and Getting Medical Care: Youth with Special Health Care Needs championed a goal for successful transitioning of adolescents and youth to adult centers of care, the practice of doing so has been slow to catch on across pediatric health care delivery systems. Recently, however, transitioning of care from pediatrics to adult health care has become a focus of medical providers, professional organizations, and national policy makers. The scope of this project is to assess the current capacity and willingness of Children’s Health System (CHS) and UAB Department of Pediatrics’ [UAB PEDS] service delivery system to prepare children and youth with special health care needs (CYSHCN) for successful transition and to assess perceived need for institutional support for continuity of transitioning across all CHS and UAB PEDS’ divisions. Methods: A three-part questionnaire with 11 questions was developed and distributed to 52 physicians, nurses and social workers within UAB PEDS and Pediatric Surgery. Results: A total of 26 surveys were returned (50%). Most reported that their practice considered the transition process to be important; however, they had not received transition training, did not have a transition policy although their practice was considered as the medical home to their most complex patients. The unwillingness of families to leave the pediatric practice as well as the lack of adult providers to accept the CYSHCN were the two largest barriers identified. Two transition models were ranked as equally suitable: Training and guidance to develop unique transition models for each Division; and, funding for a transition coordinator for each Division to design and implement transition. Conclusions: This survey indicates the need for training for key personnel in UAB PEDS and Pediatric Surgery divisions if transition is to become a successful part of CHS/UAB PEDS’ system of care. Forging strong relationships with adult care providers will facilitate successful transition is also paramount. _____________________________________________________________________________________ ABBREVIATIONS MCHB – Maternal and Child Health Bureau; CYSHCN – children and youth with special health care needs; CHS – Children’s Health System of Alabama; UAB PEDS - University of Alabama Department of Pediatrics _____________________________________________________________________________________ INTRODUCTION The Maternal and Child Health Bureau defines CYSHCN as, “Those who have or are at increased risk for chronic physical, developmental, behavioral, or emotional conditions and who require health and related services of a type or amount beyond that required by children generally”.1 The 2005-2006 National Survey of Children with Special Health Care Needs finds that 10.2 million children ages 0-17 years have special health care needs, which is approximately 14% of the U.S. child population. 2 In 1993, the Society for Adolescent Medicine defined transition as, “the purposeful planned movement of adolescents and young adults with chronic conditions from childhood to adult-centered care.3 The Society’s 2003 position paper further identifies the goals of transition to adult care for young adults with special health care needs as measures to “optimize health and to facilitate each young persons’ attaining his or her maximum potential....[encouraging] young people to be successfully integrated into a comprehensive care system to meet their complex needs”.4 Research shows, however, that most CYSHCN enter adulthood without a clear transition plan, and the barriers to successful transition are well documented in the literature.5-12 For some, the familiarity and comfort of the pediatric practice, and the pediatrician’s willingness to continue the provision of care serves as reinforcement to remain with the practice. Studies show that the span of care provided to CYSHCN by pediatricians often exceeds the age at which most young adults move to adult providers5-13. For others, the medical complexity and vulnerability of patients whose fragile states of health might worsen with a change in care delivery dictates that these patients remain with the pediatrician solely because of the lack of qualified and willing adult providers to assume their care.13 Considerable investigation into the “patient and family” aspect of transition has occurred, and the need for timed, planned transition is widely recognized as the
cornerstone concept. Model transition programs focus, based on the concept of age-appropriate care, include key elements such as the discussion of transition at diagnosis, encouragement of the autonomous adolescent in the multidisciplinary team, and utilization of bridging clinics to connect the patient to the adult medical world.15 The Children’s Hospital of Alabama is the state’s only hospital committed solely to children, is the state’s single, largest provider of specialized pediatric services, and houses one of the largest pediatric outpatient centers in the nation14. According to the 2005/06 National Survey of Children with Special Health Care Needs the state of Alabama has 17.1% of children with special health care needs, which is 4.8% more than the nationwide total of 13.9%2. It is estimated that approximately 500,000 CYSHCN turn 18 every year, and 61.7% of Alabama’s children report that they have not received services needed for transition to adult health care2 . Recognizing that successful transition of Alabama’s CYSHCN to adult medical care largely depends upon the transition practice of CHS/UAB PEDS, a survey was distributed to physicians, nurses, social workers, and other direct care providers in UAB PEDS and UAB Pediatric Surgery to determine the present state of the health care transition process from the perspective of pediatric medical providers. The survey reported here also examines barriers to successful transition, and possible systemwide improvement. METHODS Survey Instrument Design A three-part survey instrument with 11 questions was developed to examine the current state of transition practices within CHS/UAB PEDS. The questions were derived from review of current literature and feedback from discussions with key personnel at CHS/UAB PEDS. The survey questions were not validated nor were their reliability established before distribution. The first section of questions, shown in Table 1, pertains to commitment to transition. These questions were intended to gain an understanding of the current state of transition within the respective practice of each respondent and a more clear picture of the level of care provided to adolescent and adult patients through special staffing/clinic accommodations for transitioning patients. This section also sought to determine if the responder had undergone training regarding transition, or if policies outlined by an accrediting body or professional organization, such as the Cystic Fibrosis Foundation or Juvenile Diabetes Research Foundation guided their practice’s transitioning methods. Table 1: Survey questions related to commitment to transition

1. Have you ever received training regarding transition of adolescents with special health care needs to adult care? 2. Is transition to adult care for your patients guided by policies set forth by an accrediting body or professional organization (i.e., CF Foundation, Juvenile Diabetes Foundation, etc) 3. Does your practice have a written policy on the transition of adolescents with special health care needs to adult care? 4. Is there a person within your practice who functions as a transition coordinator? 5. How important does your practice consider the transition process of youth with special health care needs to adult care an important part of helping adolescents and their families achieve adult milestones? Not very important 1 2 3 4 5 Very important 6. Would your practice be considered the medical home for your most complex patients? 7. Do you have a special clinic time for your adolescent patients who are in the process of transitioning out of your practice? 8. Do you have a specific adult medical care provider to whom you transition your patients? 9. Estimate the percentage of adolescents with special health care needs leaving your practice by each of the following methods: AGE OUT _____% Leaves practice upon reaching an age determined by the practice
DROP OUT _____% Stops coming for care and is lost to followup
FORCED OUT _____% Leaves for reasons not controlled by patient or practice
HANGS OUT _____% Continue with practice after age limit of practice
MOVE OUT _____% Leaves practice to seek care from other provider
TRANSITION OUT _____% Coordinated transition to adult health care provider Section two of the survey, as shown in Table 2, lists ten possible barriers to transition, and asks the responder to indicate whether or not they consider each item a barrier to their patients’ successful transition. The ten barriers listed were drawn from those identified and discussed in published literature. Table 2: Survey questions related to barriers to transition Please indicate which of the following barriers are present within your practice that interfere with the successful transition of your special health care needs patients to adult care: _____ Lack of training for personnel regarding transition
_____ No written transition policy within the practice
_____ No institutional-wide transition policy
_____ No recognizable CHS/UAB Department of Pediatrics system infrastructure supporting transition
_____ Lack of individual division infrastructure to support transition program
_____ Time constraints of existing personnel
_____ Lack of funding for transition coordinator position
_____ Unwillingness of families to leave pediatric practice
_____ Lack of available, appropriately trained, or willing adult providers for complex patients
_____ Concerns of financial impact of losing patients
The third section of the survey, Table 3, offers four transition models to be ranked in order of suitability to the responder’s practice. These models reflect varying methods of institutional support to transition, and have been discussed in published literature.

Table 3: Survey questions related to institutional support Please rank the following transition program models in order of suitability to your Division _____ UAB Department of Peds/CHS systemwide plan for transition using standardized protocol All Divisions would follow the same systemwide transition protocol. _____ UAB Department of Peds/CHS systemwide transition coordinator All Divisions would refer patients ready to begin the transition process to a systemwide transition coordinator who would coordinate an individualized transition process. _____ Training for practice personnel to develop transition program Each Division would receive training on transition and guidance regarding the development of their own unique transition program. _____ Funding for transition coordinator within practice Each Division would receive funding for a transi on coordinator to design, implement and ti maintain a Division-specific transition program.
Survey Administration A total of 52 surveys were distributed via campus mail to physicians, nurses and social workers within UAB Department of Pediatrics and Pediatric Surgery using convenience sampling methodology. A reminder email was sent 10 days later to encourage participation. Data Analysis Data were entered into an Excel database (Microsoft, Redmond, Washington). Due to the low sample size (n = 27), raw percentages were used. RESULTS Responses were received from 27 of the 52 distributed questionnaires, for a response rate of 52%. Of those responders, 11 (41%) identified themselves as physicians, 8 (30%) identified themselves as nurses, 2 (7%) were social workers, 2 (7%) listed themselves as clinic coordinators, and 4 (15%) did not answer this question. (Figure 1).
Figure 1: Distribution of Survey Respondentsn=27
MD - 41% (11)
Nurse - 30% (8)
Social Worker - 7% (2)
Clinical Coordinator - 7% (2)
Unidentified - 15% (4)
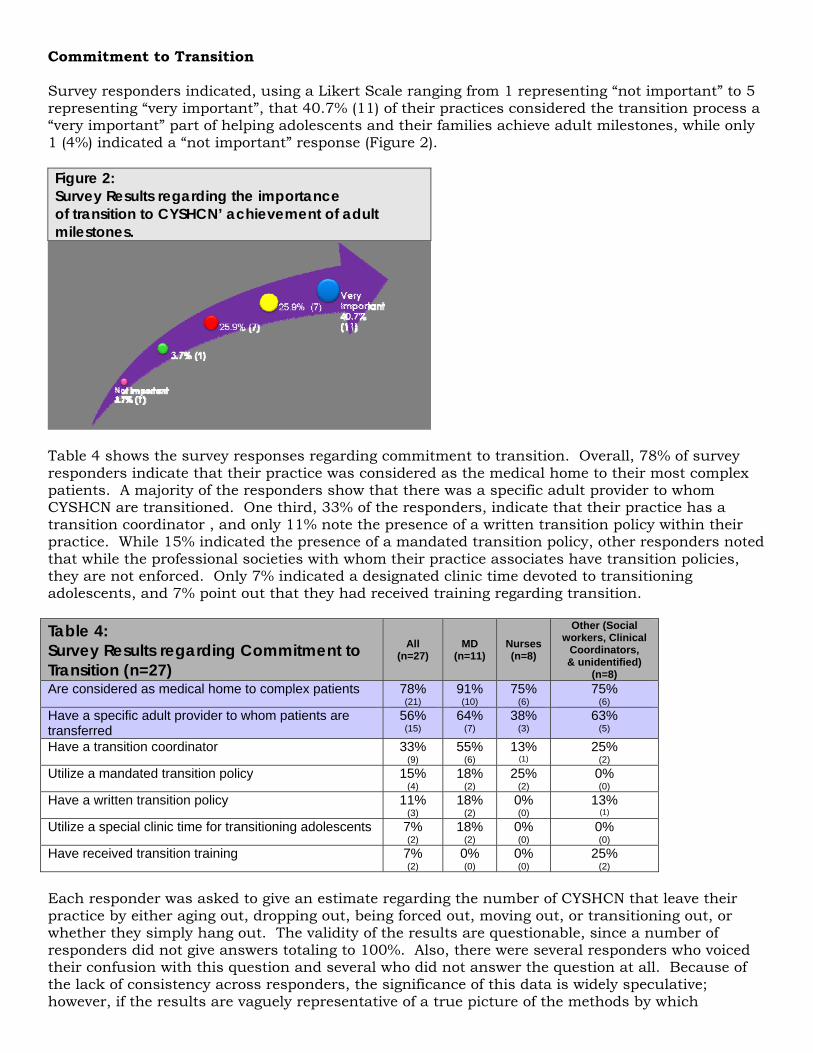
Commitment to Transition Survey responders indicated, using a Likert Scale ranging from 1 representing “not important” to 5 representing “very important”, that 40.7% (11) of their practices considered the transition process a “very important” part of helping adolescents and their families achieve adult milestones, while only 1 (4%) indicated a “not important” response (Figure 2). Figure 2: Survey Results regarding the importance of transition to CYSHCN’ achievement of adult milestones.
Table 4 shows the survey responses regarding commitment to transition. Overall, 78% of survey responders indicate that their practice was considered as the medical home to their most complex patients. A majority of the responders show that there was a specific adult provider to whom CYSHCN are transitioned. One third, 33% of the responders, indicate that their practice has a transition coordinator , and only 11% note the presence of a written transition policy within their practice. While 15% indicated the presence of a mandated transition policy, other responders noted that while the professional societies with whom their practice associates have transition policies, they are not enforced. Only 7% indicated a designated clinic time devoted to transitioning adolescents, and 7% point out that they had received training regarding transition. Table 4: Survey Results regarding Commitment to Transition (n=27)
All (n=27)
MD (n=11)
Nurses (n=8)
Other (Social workers, Clinical
Coordinators, & unidentified)
(n=8) Are considered as medical home to complex patients 78%
(21) 91% (10)
75% (6)
75% (6)
Have a specific adult provider to whom patients are transferred
56% (15)
64% (7)
38% (3)
63% (5)
Have a transition coordinator 33% (9)
55% (6)
13% (1)
25% (2)
Utilize a mandated transition policy 15% (4)
18% (2)
25% (2)
0% (0)
Have a written transition policy 11% (3)
18% (2)
0% (0)
13% (1)
Utilize a special clinic time for transitioning adolescents 7% (2)
18% (2)
0% (0)
0% (0)
Have received transition training 7% (2)
0% (0)
0% (0)
25% (2)
Each responder was asked to give an estimate regarding the number of CYSHCN that leave their practice by either aging out, dropping out, being forced out, moving out, or transitioning out, or whether they simply hang out. The validity of the results are questionable, since a number of responders did not give answers totaling to 100%. Also, there were several responders who voiced their confusion with this question and several who did not answer the question at all. Because of the lack of consistency across responders, the significance of this data is widely speculative; however, if the results are vaguely representative of a true picture of the methods by which

CYSHCN leave the pediatric practice, to state that a significant number (35.2%) of patients age out of the system without a transition plan in place, while another one third (30%) hang out and remain with the pediatric practice.
*Based on estimates made by survey responders
Barriers to Transition The survey results regarding barriers to transition are shown in Table 5. Most responders (67%) acknowledged that their biggest barrier to transition was the lack of available, appropriately trained, or willing adult providers. Similarly, a large number (63%) indicated that the unwillingness of families to leave their practice was a barrier. The lack of transition-supportive CHS/UAB PEDS system infrastructure was acknowledged by 48% of responders, while the lack of divisional infrastructure was listed as a barrier to 37%. The lack of an institutional-wide transition policy was barrier to 44%. Lack of transition training for personnel was identified as a barrier for 37% of the responders, and lack of funding for a transition coordinator position was considered a barrier by 37%. Only 4% specified that the financial impact to their practice of losing patients through transition was a concern.

Table 5: Survey Responses Regarding Barriers to Transition (n=27)
All (n=27)
MD (n=11)
Nurses (n=8)
Other (Social workers, Clinical Coordinators, & unidentified) (n=8)
Lack of available, appropriately trained, or willing adult providers for complex patients
67% (18)
64% (7)
75% (6)
75% (6)
Unwillingness of families to leave pediatric practice
63% (17)
45% (5)
88% (7)
75% (6)
No written transition policy within the practice 56% (15)
45% (5)
63% (5)
50% (4)
No recognizable CHS/UAB PEDS system infrastructure supporting transition
48% (13)
55% (6)
25% (2)
63% (5)
No institutional-wide transition policy 44% (12)
45% (5)
38% (3)
63% (5)
Time constraints of existing personnel 41% (11)
45% (5)
38% (3)
38% (3)
Lack of training for personnel regarding transition 37% (10)
36% (4)
38% (3)
38% (3)
Lack of individual division infrastructure to support transition program
37% (10)
36% (4)
25% (2)
50% (4)
Lack of funding for transition coordinator position 37% (10)
45% (5)
25% (2)
38% (3)
Concerns of financial impact of losing patients 4% (1)
0% (0)
13% (1)
0% (0)
Institutional Support The last question on the survey focused on four models of transition and asked the responder to rank the models from 1 to 4, indicating the order in which the models would work best for their practice. The results of this question are shown in Figure 3. The model preferred by the largest number of responders, 29.6%, provides funding for division coordinators who would design, implement, and coordinate a unique transition program. This was the preferred model by a majority of the MD responders (36.3%). The second preferred choice, ranked first by 26% of responders, is division training for transition, in which each division would receive training and guidance through which a unique transition program is designed. The social workers, clinic coordinators, and unidentified responders (as categorized as “other” in Figure 3), indicated that this model as their preference. The third choice, a CHS/UAB PEDS systemwide transition coordinator, was preferred by 22.2% of responders overall; however, this choice was considered the first choice for nurses, with 37.5% of them considering this as their ideal model. Lastly, a CHS/UAB PEDS systemwide protocol, was chosen by 18.5% as the ideal model.

Figure 3: Reported Preference of Transition Model
05
1015202530354045
CHS/UABPEDSsystemwide plan
CHS/UABPEDSsystemwide
transitioncoordinator
Div ision trainingfor transition
Funding fordiv ision
coordinators
Transition Models
Perc
enta
ge ALLMDNurseOther
DISCUSSION OF FINDINGS Transition is taking place at CHS/UAB PEDS, but without structure at the institutional level. Several responders report some sort of transition activity in their practice areas with varying levels of success, and a listing of all the comments are found in Table 6. There were reports of successful relationships with specialists to whom most all patients are transferred, as well as practices who struggle to find adult physicians to accept their medically complex patients. The lack of formal CHS policies regarding transition and aging out results in divisional autonomy, and for those patients who are seen in several specialty clinics, this lack of formal policy results in mixed messages sent to the patient. For instance, a family seen in a clinic that ages out the patient at age 21 might be confused if another clinic within the CHS/UAB PEDS system continues to see the patient past that same age. There does not seem to be a forum through which personnel involved with transitioning can share their strategies and method. Dialogue could result to collaborative programs across divisions that could lead to policy formulation. Moreover, discussion regarding strategies and methods of transition that work could assist those divisions who are struggling. Transitional training is needed at multiple levels. One of the most striking findings of the survey is that only two responders have received transition training. The environment in which CHS/UAB PEDS exists offers multiple opportunities for training to take place. Grand Rounds lectures, division-sponsored workshops, professional development workshops, and CME/CEU workshops take place at CHS/UAB PEDS on a weekly basis. UAB School of Medicine is also a ripe forum for transition lectures to take place; planting the seeds early, while young physicians are learning, could eventually lead to medical providers whose awareness of pediatric diseases across the lifespan opens future doors for adult medical care for CYSHCN. Certainly, training programs that focus on the healthy and respectful inclusion of patients and families in the transition process will result in families who do not resist transition. Strong collaboration and community building with adult medicine is needed. The most consistent message sent by survey responders was that, even if they understood transition and had a solid program in place, the willingness of adult providers to receive CYSHCN into their care is a bigger problem needing to be resolved. It is suggested that perhaps looking outside of the adult physicians in the UAB network, and reaching into the communities in which the CYSHCN resides to find an adult medical care provider might be an ideal solution; however, this would require collaboration with various service providers in communities across the state. Another suggestion is that the use of adult general internists or family practice physicians may be an option rather than

specialists, and might be more willing partners in transition, particularly if the patient is medically stable. This model would be very similar to the pediatric model of care and might offer a different perspective to the process. It is impressive that transition takes place at CHS/UAB PEDS, without policies or mandates; however, the addition of such could lend a unifying process to the existing structure, fortifying the care given to CYSHCN and their families. Currently, each practice functions as an independent silo, with little communication and collaboration. Policies regarding transition, age of care parameters, and training will strengthen the system, and allow CHS/UAB PEDS to offer CYSHCN a bridge into adulthood that encourages and supports these young adults in their desire for success in the adult medical world.
TABLE 6: Comments and Responses from Survey Responders MD We have a protocol in place but no specific written policy. We are working on creating a binder for patients as they transition out. MD We have a transition team for diabetes, but not other endocrinology patients. MD Have not received specific training, but have dealt with these issues on a regular basis in my clinical practice. MD No special clinic time, but do coordinate these issues on an individual basis. Nurse We have a specific group of providers that we transition our patients to. MD This survey is missing the target. It is the adult MD’s who don’t want complex difficult patients with little to no compensation. MD No one on the adult side wants to care for these complex patients with chronic conditions. Nurse The majority of our complex patients stay with us longer than they should. Nurse In our division, the nurses and social workers collaborate to help identified patients move to adult care. MD We follow a population of neurologically devastated individuals, many in their 20’s. Despite their chronologic age, their neurologic status
remains unchanged. This population probably needs more help with primary care transitioning. SW Unwillingness of families to leave pediatric practice plus the unwillingness of the doctors to transition these that don’t want to leave. MD NASPGHAN has come out with guidelines, but they are not mandatory. MD A transition coordinator would be nice, but there are no resources available. MD Transition is an important aspect of my practice. Mostly hampered by lack of a coordinated effort, funding and a willing and available
partner on the adult side. Funding/billing for a transition visit is also a significant barrier (who will bill for the visit – adult or peds practice, and where to house the transition program?)
CC Insurance is a big issue – the kids age out of their insurance and have now way to finance healthcare. Nurse We have a great relationship with UAB Epilepsy Center and Dept. of Neurology for transition. Typically this is arranged by the patient’s
primary care physician or staff nurse. I don’t think we have enough patients to justify hiring a full-time transition coordinator. Nurse We have no set age limit for when we will stop seeing patients. Nurse The patients with spina bifida and hydrocephalus are harder to transition because adult neurosurgeons do not want to deal with
pediatric diseases. MD No forced age – We leave it up to the patient to decide when to transfer care and to what doctor. Do agree this should be a planned
process and not just an “event”. Getting pregnant, though, is an automatic referral to UAB.
REFERENCES 1. McPherson M, Arango P, Fox H, Lauver C, McManus M, Newacheck P, Perrin J, Shonkoff J, Strickland B. A new definition of children with special health care needs. Pediatrics,
102(1):137–140, 1998. 2. Child and Adolescent Health Measurement Initiative. 2005/06 National Survey of Children with Special Health Care Needs, Data Resource Center for Child and Adolescent Health
website. Retrieved 07/15/09 from www.chscndata.org. 3. Blum RW, Garell D, Hodgman CH, et al. Transition from child-centered to adult health-care systems for adolescents with chronic conditions: a position paper of the Society of Adolescent Medicine. J Adolesc Health 1993;14:570-6. 4. Society for Adolescent Medicine. Transition to Adult Health Care for Adolescents and Young Adults with Chronic Conditions. J Adolesc Health 2003;33:309-11. 5. Burdo-Hartman WA, Patel DR. Medical home and transition planning for children and youth with special health care needs. Pediatr Clin N Am 2008;55:1287-1297. 6. Geenen SJ, Powers LE, Sells W. Understanding the role of health care providers during the transition of adolescents with disabilities and special health care needs. J Adolesc
Health 2003;32:225-33. 7. Lotstein DS, Inkelas M, Hays RD, Halfon N, Brook R. Access to care of youth with special health
care needs in the transition to adulthood. J Adolesc Health 2008;43:23-29. 8. Lotstein DS, McPherson M, Strickland B, Newacheck PW. Transition planning for youth with
special health care needs: results from the National Survey of Children with Special Health Care Needs. Pediatrics. 2005;115:1562-68.
9. McPherson M, Weissman G, Strickland BB, van Dyck PC, Blumberg SJ, Newacheck PW. Implementing community-based systems of services for children and youths with special health care needs: how well are we doing? Pediatrics. 2004;113:1538-44.
10. Reiss J, Gibson R. Health care transition: destination unknown. Pediatrics. 2002;110:1307-17. 11. Reiss J, Walker LR, Walker GR. Health care transition for young adults with disabilities and
special health care needs. Abstr Acad Health Serv Res Health Policy Meet. 2002;19:21. 12. Scal P. Transition for youth with chronic conditions: primary care physicians’ approaches.
Pediatrics. 2002;110:1315-21. 13. Burke R, Spoerri M, Price A, Cardosi A-M, Flanagan P. Survey of primary care pediatricians on
the transition and trasfer of adolescents to adult health care. Clin Pediatr. 2008;47(4):347-354. 14. Children’s Health System. http://www.chsys.org/body.cfm?id=15 15. Surgeon General’s Conference. Growing Up and Getting Medical Care: Youth with Special
Health Care Needs. A Summary of Conference Proceedings. March 13-15, 1989.

ATTACHMENTS
QUESTIONNAIRE SUMMARY OF FINDINGS

COMMITMENT TO TRANSITION Have you ever received training regarding transition of adolescents with special health care needs to adult care?
o Yes o No o Comments __________________________________________________________________________________
Is transition to adult care for your patients guided by policies set forth by an accrediting body or professional organization (i.e., CF Foundation, Juvenile Diabetes Foundation, etc)
o Yes o No o Comments __________________________________________________________________________________
Does your practice have a written policy on the transition of adolescents with special health care needs to adult health care?
o Yes o No o Comments __________________________________________________________________________________
Is there a person within your practice who functions as a transition coordinator?
o Yes o No o Comments __________________________________________________________________________________
How important does your practice consider the transition process of youth with special health care needs to adult care an important part of helping adolescents and their families achieve adult milestones? Not very important 1 2 3 4 5 Very important
Would your practice be considered the medical home for your most complex patients?
o Yes o No o Comments __________________________________________________________________________________
Do you have a special clinic time for your adolescent patients who are in the process of transitioning out of your practice?
o Yes o No o Comments __________________________________________________________________________________
Do you have a specific adult medical care provider to whom you transition your patients? o Yes o No o Comments __________________________________________________________________________________
Estimate the percentage of adolescents with special health care needs leaving your practice by each of the following methods: AGE OUT _____% Leaves practice upon reaching an age determined by the practice
DROP OUT _____% Stops coming for care and is lost to followup
FORCED OUT _____% Leaves for reasons not controlled by patient or practice
HANGS OUT _____% Continue with practice after age limit of practice
MOVE OUT _____% Leaves practice to seek care from other provider
TRANSITION OUT _____% Coordinated transition to adult health care provider

BARRIERS TO TRANSITION Please indicate which of the following barriers are present within your practice that interfere with the successful transition of your special health care needs patients to adult care: _____ Lack of training for personnel regarding transition
_____ No written transition policy within the practice
_____ No institutional-wide transition policy
_____ No recognizable CHS/UAB Department of Pediatrics system infrastructure supporting transition
_____ Lack of individual division infrastructure to support transition program
_____ Time constraints of existing personnel
_____ Lack of funding for transition coordinator position
_____ Unwillingness of families to leave pediatric practice
_____ Lack of available, appropriately trained, or willing adult providers for complex patients
_____ Concerns of financial impact of losing patients
INSTITUTIONAL SUPPORT Please rank the following transition program models in order of suitability to your Division _____ UAB Department of Peds/CHS systemwide plan for transition using standardized protocol All Divisions would follow the same systemwide transition protocol. _____ UAB Department of Peds/CHS systemwide transition coordinator
All Divisions would refer patients ready to begin the transition process to a systemwide transition coordinator who would coordinate an individualized transition process.
_____ Training for practice personnel to develop transition program
Each Division would receive training on transition and guidance regarding the development of their own unique transition program.
_____ Funding for transition coordinator within practice
Each Division would receive funding for a transition coordinator to design, implement and maintain a Division-specific transition program.
PLEASE USE THE SPACE BELOW TO SHARE ANY ADDITIONAL COMMENTS, THOUGHTS, CONCERNS OR EXPERIENCES YOU HAVE REGARDING TRANSITION: What is your job title? _____________________________________

ASSESSMENT OF CHILDREN’S HEALTH SYSTEM AND UAB DEPARTMENT OF PEDIATRICS TRANSITION OF CARE OF
CHILDREN AND YOUTH WITH SPECIAL HEALTH CARE NEEDS Cynthia Carlson deSa, BA Pediatric Pulmonary Center Social Work Trainee MSW/MPH Candidate August 2009
ABOUT THIS SURVEY
• Survey was distributed to 52 physicians, nurses and social workers in the Department of Pediatrics and Pediatric Surgery in June 2009
• A total of 27 surveys were returned for a response rate of 52% • Distribution of responders: 11 MDs (41%), 8 nurses (30%), 2 social workers (7%), 2 clinic coordinators (7%), and
4 unidentified (15%)

COMMITMENT TO TRANSITION
How important does your practice consider the transition process of youth with special health care needs to adult care an important part of helping adolescents and their families achieve adult milestones?
Survey Results regarding Commitment to Transition
All (n=27)
MD (n=11)
Nurses (n=8)
Other (Social workers, Clinical
Coordinators, & unidentified)
(n=8) Are considered as medical home to complex patients 78%
(21) 91% (10)
75% (6)
75% (6)
Have a specific adult provider to whom patients are transferred
56% (15)
64% (7)
38% (3)
63% (5)
Have a transition coordinator 33% (9)
55% (6)
13% (1)
25% (2)
Utilize a mandated transition policy 15% (4)
18% (2)
25% (2)
0% (0)
Have a written transition policy 11% (3)
18% (2)
0% (0)
13% (1)
Utilize a special clinic time for transitioning adolescents 7% (2)
18% (2)
0% (0)
0% (0)
Have received transition training 7% (2)
0% (0)
0% (0)
25% (2)
AGES OUT – Leaves practice upon reaching an age determined by the practice DROPS OUT – Stops coming for care and is lost to followup FORCED OUT – Leaves for reasons not controlled by patient or practice HANGS OUT – Continues with practice after age limit of practice MOVES OUT – Leaves practice to seek care from other provider TRANSFERS OUT – Coordinated transfer to adult health care provider
*Based on estimates made by survey responders

BARRIERS TO TRANSITION
Survey Responses Regarding Barriers to Transition
All (n=27)
MD (n=11)
Nurses (n=8)
Other (Social workers, Clinical Coordinators, & unidentified) (n=8)
Lack of available, appropriately trained, or willing adult providers for complex patients
67% (18)
64% (7)
75% (6)
75% (6)
Unwillingness of families to leave pediatric practice
63% (17)
45% (5)
88% (7)
75% (6)
No written transition policy within the practice 56% (15)
45% (5)
63% (5)
50% (4)
No recognizable CHS/UAB PEDS system infrastructure supporting transition
48% (13)
55% (6)
25% (2)
63% (5)
No institutional-wide transition policy 44% (12)
45% (5)
38% (3)
63% (5)
Time constraints of existing personnel 41% (11)
45% (5)
38% (3)
38% (3)
Lack of training for personnel regarding transition 37% (10)
36% (4)
38% (3)
38% (3)
Lack of individual division infrastructure to support transition program
37% (10)
36% (4)
25% (2)
50% (4)
Lack of funding for transition coordinator position 37% (10)
45% (5)
25% (2)
38% (3)
Concerns of financial impact of losing patients 4% (1)
0% (0)
13% (1)
0% (0)
INSTITUTIONAL SUPPORT
Figure 3: Reported Preference of Transition Model
05
1015202530354045
CHS/UABPEDSsystemwide plan
CHS/UABPEDSsystemwide
transitioncoordinator
Div ision trainingfor transition
Funding fordiv ision
coordinators
Transition Models
Perc
enta
ge ALLMDNurseOther

IMPLICATIONS OF FINDINGS
AREAS FOR FURTHER EXPLORATION
Surveys of adult medical care providers to gain insight into their views of transition Surveys of families of CYSHCN regarding their attitudes towards transition Review of CHS/UAB PEDS policies that relate to the care of older adolescents/young adults, particularly
those with special health care needs Medical school curriculum review regarding transition of CYSHCN to adult medical care Review of transition programs in place at other children’s hospitals and pediatric departments similar
in size and scope to CHS/UAB PEDS

Comments and Responses from Survey Responders
MD We have a protocol in place but no specific written policy. We are working on creating a binder for patients as they transition out.
MD We have a transition team for diabetes, but not other endocrinology patients. MD Have not received specific training, but have dealt with these issues on a regular basis in my clinical
practice. MD No special clinic time, but do coordinate these issues on an individual basis. Nurse We have a specific group of providers that we transition our patients to. MD This survey is missing the target. It is the adult MD’s who don’t want complex difficult patients with little to
no compensation. MD No one on the adult side wants to care for these complex patients with chronic conditions. Nurse The majority of our complex patients stay with us longer than they should. Nurse In our division, the nurses and social workers collaborate to help identified patients move to adult care. MD We follow a population of neurologically devastated individuals, many in their 20’s. Despite their
chronologic age, their neurologic status remains unchanged. This population probably needs more help with primary care transitioning.
SW Unwillingness of families to leave pediatric practice plus the unwillingness of the doctors to transition these that don’t want to leave.
MD NASPGHAN has come out with guidelines, but they are not mandatory. MD A transition coordinator would be nice, but there are no resources available. MD Transition is an important aspect of my practice. Mostly hampered by lack of a coordinated effort,
funding and a willing and available partner on the adult side. Funding/billing for a transition visit is also a significant barrier (who will bill for the visit – adult or peds practice, and where to house the transition program?)
CC Insurance is a big issue – the kids age out of their insurance and have now way to finance healthcare. Nurse We have a great relationship with UAB Epilepsy Center and Dept. of Neurology for transition. Typically this
is arranged by the patient’s primary care physician or staff nurse. I don’t think we have enough patients to justify hiring a full-time transition coordinator.
Nurse We have no set age limit for when we will stop seeing patients. Nurse The patients with spina bifida and hydrocephalus are harder to transition because adult neurosurgeons do
not want to deal with pediatric diseases. MD No forced age – We leave it up to the patient to decide when to transfer care and to what doctor. Do
agree this should be a planned process and not just an “event”. Getting pregnant, though, is an automatic referral to UAB.